Acthar Gel versus standard of care for adults with proteinuria in nephrotic syndrome due to focal segmental glomerulosclerosis: cost-per-response analysis from the US healthcare perspective
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Proteinuria poses a significant challenge in focal segmental glomerulosclerosis (FSGS), particularly when resistant to standard treatments. Acthar® Gel, a Food and Drug Administration (FDA)-approved treatment, may be a potential option for proteinuria in nephrotic syndrome (NS) due to FSGS, particularly given the limited alternative therapies. This study assessed the cost-per-response of Acthar Gel versus standard of care (SoC) for the treatment of refractory proteinuria in NS due to FSGS among adults from a US healthcare payer perspective over a 1- to 3-year horizon. Materials & methods: A probabilistic, cohort-based state-transition model tracked adults with nephrotic-range proteinuria due to FSGS through clinically relevant health states in 6-month cycles. All patients entered in relapse and received either Acthar Gel or SoC. At each cycle, individuals could transition to response or remain uncontrolled, progress to renal failure, or continue in relapse; death was permitted from any state. Responders were allowed to either sustain response or experience relapse in subsequent cycles. Model inputs for clinical event rates, healthcare utilization and medical costs were sourced from the published literature, and drug costs were valued using wholesale acquisition cost. Cost-per-response was defined as total healthcare costs (drug and nondrug medical costs) per patient divided by the response rate. Results: Acthar Gel showed a lower cost-per-response ($469,735) versus cyclophosphamide ($2,140,400) and rituximab ($1,272,477) over 1 year. This advantage for Acthar Gel was sustained for 2 and 3 years. Acthar Gel was potentially a dominant treatment option at 2 and 3 years, with a lower overall cost of care and higher response rates than SoC. Conclusion: From a US healthcare payer perspective, Acthar Gel appears to be a cost-effective, value-based treatment option for adults with proteinuria in NS due to FSGS over 1 to 3 years. These findings may aid providers and payers in making informed treatment decisions when conventional therapies are ineffective for these patients.
Plain language summary
What is this article about?
This study looks at whether Acthar Gel provides good value compared with usual treatments for adults with focal segmental glomerulosclerosis who still have high protein in their urine despite prior care. High protein in the urine (proteinuria) is a sign that the kidneys are damaged and can lead to worse health. The study compared the costs and effectiveness of Acthar Gel with standard options used in the US, such as cyclophosphamide or rituximab, over a 1- to 3-year period, considering the perspective of healthcare payers.
What were the results?
Acthar Gel resulted in more patients responding to treatment and, in many cases, reduced overall medical spending. After 1 year, the cost to achieve one responder was lower with Acthar Gel than with usual treatments. This advantage persisted for 2–3 years.
What do the results mean?
For adults with difficult-to-treat focal segmental glomerulosclerosis, Acthar Gel appears to be a cost-effective choice. Its higher chance of response and lower use of other healthcare services can reduce total costs over time. These findings can help clinicians and health plans choose treatments when standard therapies have not worked.
Focal segmental glomerulosclerosis (FSGS) stands as a leading cause of nephrotic syndrome (NS), categorized as either primary (idiopathic) or secondary to underlying disease processes or genetic mutations [1,2]. Untreated, FSGS frequently progresses to end-stage renal disease (ESRD), with 10-year survival rates ranging from 40 to 60% [1,2].
Proteinuria, a hallmark of glomerulopathies, is a crucial marker in FSGS [2]. Proteinuria in NS is a risk indicator of progressive kidney disease [3]. Its presence in NS signifies a heightened risk for progressive kidney disease, underscoring the importance of achieving proteinuria remission as a key therapeutic objective [2]. Studies consistently show that patients achieving complete or partial remission experience a slower decline in renal function and a reduced risk of renal failure, with complete remission predicting improved long-term kidney and patient survival [2]. Complete remission of proteinuria in NS due to FSGS predicts excellent long-term outcomes for both kidney and patient survival [2]. A partial remission also significantly reduces the risk of progression to ESRD [2]. However, FSGS is also characterized by a substantial relapse rate, with up to 40% of patients experiencing recurrence [4].
Managing proteinuria in NS due to FSGS, particularly in cases resistant to conventional therapies, poses a significant clinical challenge [3–5]. Although the treatment landscape for proteinuria in NS due to FSGS in adults includes well-established recommendations, specifically, high-dose glucocorticoids as first-line therapy and calcineurin inhibitors as second-line agents per the 2021 Kidney Disease: Improving Global Outcomes (KDIGO) Clinical Practice Guideline for Glomerular Diseases, there remains limited consensus regarding optimal treatment alternatives for adults with refractory proteinuria who have failed these standard treatments. Guidelines further note that adults with refractory proteinuria should be referred to specialized centers for consideration of alternative treatment options [4–6]. While glucocorticoids remain the cornerstone of first-line therapy for many proteinuric glomerular diseases, their long-term use is associated with significant morbidities, including steroid-induced diabetes, metabolic bone disease and weight gain [7,8]. Multiple subsequent therapeutic agents, such as calcineurin inhibitors, mycophenolate mofetil, cyclophosphamide and rituximab, have been employed with varying degrees of success, but are often accompanied by significant side effects, notably increased infection risk and potential relapse upon withdrawal, ultimately contributing to disease progression [4,5]. Given the limitations of current treatment approaches, there is a need for alternative therapies to address proteinuria in NS due to FSGS.
Despite standard immunosuppressive therapy, roughly two-thirds of patients with NS due to FSGS relapse and continue to exhibit persistent or recurrent proteinuria, making them prime candidates for alternative treatments. Acthar® Gel (repository corticotropin injection, Mallinckrodt Pharmaceuticals) is approved by the US FDA to induce a diuresis or a remission of proteinuria in the NS without uremia of the idiopathic type or due to lupus erythematosus [9]. It is a naturally sourced complex mixture of adrenocorticotropic hormone analogues and other pituitary peptides [9]. Its therapeutic effects may be mediated through multiple anti-inflammatory pathways [9]. Acthar Gel is also reported to bind to melanocortin receptors [9]. The trophic effects of endogenous adrenocorticotropic hormone and Acthar Gel on the adrenal cortex are not well understood beyond the fact that they appear to be mediated by cyclic adenosine monophosphate [9]. Clinical studies have reported the effectiveness of Acthar Gel in reducing or inducing remission of proteinuria in NS due to FSGS, with safety outcomes characterized [1,5,10–13]. With an established side effect profile and a higher likelihood of inducing remission [1,5,10–13], Acthar Gel may help appropriate patients with proteinuria in NS due to FSGS.
Despite several observational studies describing the clinical effects of Acthar Gel in NS, there is a notable evidence gap in economic evaluations for adults with refractory proteinuria in NS due to FSGS. Payers and clinicians increasingly require value-focused analyses (e.g., cost-per-outcome metrics) to guide treatment selection when conventional therapies fail; however, no model-based studies have compared Acthar Gel with alternative treatments in this population. This study addressed this gap by evaluating the cost-per-response of Acthar Gel compared with the standard of care (SoC; cyclophosphamide or rituximab) for the treatment of refractory proteinuria in NS due to FSGS among adults who have not responded to conventional therapies from a US healthcare payer perspective over a 1- to 3-year horizon.
Materials & methods
Model structure
A probabilistic, cohort-level state-transition model was constructed to evaluate the economic value of Acthar Gel in managing proteinuria in NS due to FSGS among adults who have not responded to conventional therapies (steroid-resistant or intolerant/contraindicated and those with steroid-dependent or frequently relapsing disease). Specifically, the model compared the cost-per-response of Acthar Gel to SoC, which included cyclophosphamide and rituximab, each evaluated separately. Although cyclophosphamide and rituximab are recommended as alternative treatment options for adults with refractory proteinuria who have failed on two or more treatments, these recommendations are grounded primarily in limited observational data rather than randomized controlled trials [4,6,14]. Given that their supporting data are limited, they are used as off-label medications [15–18]. The 2021 KDIGO guideline for primary FSGS in adults recommends high-dose glucocorticoids as first-line therapy, with calcineurin inhibitors (cyclosporine or tacrolimus) as the preferred alternative agents in patients who are steroid-resistant or intolerant [4]. However, it does not explicitly endorse cyclophosphamide or rituximab for adult FSGS due to the paucity of randomized trial data [4]. In the KDIGO executive summary, it is noted more broadly that in patients who do not tolerate or can no longer use cyclophosphamide, rituximab could be offered; however, this recommendation is conditional as it is based mainly on observational studies rather than RCTs [14]. A US commentary on the KDIGO 2021 guideline (KDOQI) further suggests that, for frequently relapsing disease (including FSGS), clinicians may consider alternative treatment options, such as cyclophosphamide, rituximab or adrenocorticotropic hormone [6]. Because there is no prior adult-focused economic evaluation study comparing these agents in FSGS, the model’s selection of cyclophosphamide and rituximab as off-label SoC comparators reflects both expert consensus in practice guidelines and published case series regarding their use in refractory adult FSGS. Therefore, their safety and efficacy have not been established by the FDA for this indication. The analysis was conducted from a US healthcare payer perspective over a 1- to 3-year timeframe. The analytical model was built within Microsoft® Excel 2024.
Patient trajectories were modeled across discrete health states with parameter uncertainty handled probabilistically (Figure 1). All patients entered in relapse and received Acthar Gel or SoC. Transitions were evaluated every 6 months in line with contemporary clinical practice. At the end of each cycle, patients could achieve a response, remain in relapse, transition to persistent NS, or develop acute renal failure (ARF). ‘Persistent NS’ health state was defined as failure to achieve a clinically meaningful reduction in proteinuria after a full initial treatment course. Patients showing improvement that did not meet response criteria were assumed to continue therapy while remaining in the relapse state. Responders could maintain a durable response or experience relapse. Patients in the persistent NS health state accrued ongoing treatment and healthcare costs and could progress to kidney failure (ARF or ESRD), at which point dialysis or a renal transplant was initiated. Death was permitted from any health state.
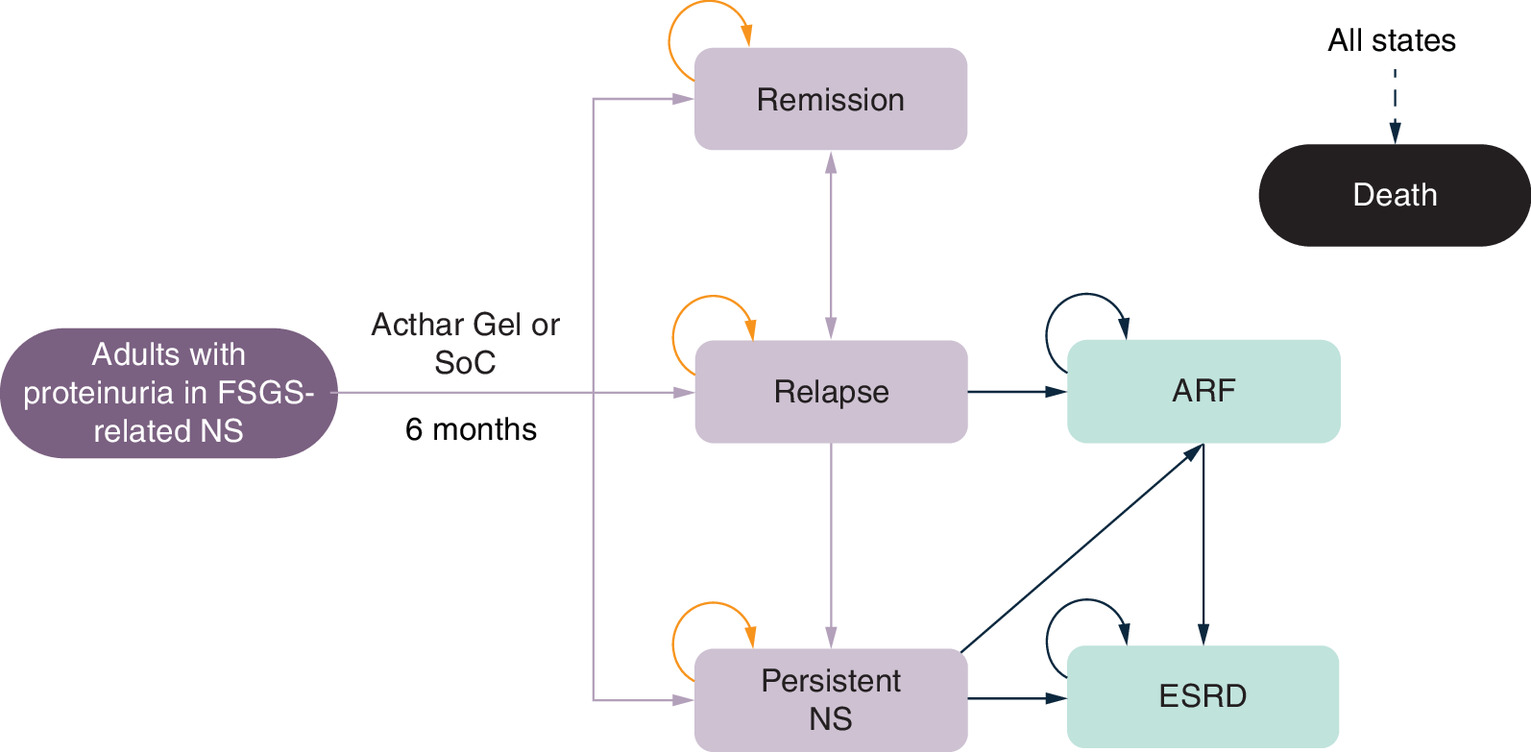
Figure 1. Schematic of the probabilistic cohort-level state-transition model for the treatment of proteinuria in nephrotic syndrome due to focal segmental glomerulosclerosis.
ARF: Acute renal failure; ESRD: End-stage renal disease; FSGS: Focal segmental glomerulosclerosis; NS: Nephrotic syndrome; SoC: Standard of care.
Model inputs
Clinical inputs
Clinical inputs, including clinical effectiveness, safety, clinical manifestations, disease progression and mortality, are provided in Table 1.
| Parameters† | Value (probability of event) | Source (year) | Ref. |
|---|---|---|---|
| Effectiveness | |||
| Acthar Gel | |||
| Response | 69.7% | Tumlin et al. (2017)¶ | [5] |
| No response‡ | 13.3% | Tumlin et al. (2017)¶ | [5] |
| Persistent NS§ | 17.0% | Tumlin et al. (2017)¶ | [5] |
| Relapse | 28.6% | Hogan et al. (2013) | [1] |
| Cyclophosphamide# | |||
| Response | 20.0% | Cattran et al. (1998) | [19] |
| No response‡ | 0.0% | Assumption†† | |
| Persistent NS§ | 80.0% | Assumption†† | |
| Relapse | 36.4% | Troyanov et al. (2005) | [2] |
| Rituximab# | |||
| Response | 25.0% | Fernandez-Fresnedo et al. (2009) | [20] |
| No response‡ | 12.5% | Fernandez-Fresnedo et al. (2009) | [20] |
| Persistent NS§ | 62.5% | Fernandez-Fresnedo et al. (2009) | [20] |
| Relapse | 25.0% | Ruggenenti et al. (2014) | [21] |
| Serious adverse events‡‡ | |||
| Cyclophosphamide | |||
| Anemia/leukopenia | 30.0% | Fernández-Juárez et al. (2021) | [22] |
| Venous thrombosis | 12.0% | Fernández-Juárez et al. (2021) | [22] |
| Acute kidney injury | 19.0% | Fernández-Juárez et al. (2021) | [22] |
| Infections | 23.0% | Fernández-Juárez et al. (2021) | [22] |
| Rituximab | |||
| Infusion-related adverse events | 25.0% | Fervenza et al. (2019) | [23] |
| Cardiovascular events | 1.5% | Fervenza et al. (2019) | [23] |
| Increased creatinine levels | 6.0% | Fervenza et al. (2019) | [23] |
| Endocrine/metabolic events | 3.1% | Fervenza et al. (2019) | [23] |
| Infections | 6.2% | Fervenza et al. (2019) | [23] |
| Clinical manifestations | |||
| Complications | |||
| Chronic kidney disease | 76.0% | Hayes et al. (2024) | [24] |
| Cardiac complications | 64.1% | Rice et al. (2021) | [25] |
| Pain | |||
| Relapse | 58.0% | Lambourg et al. (2021) | [26] |
| Persistent NS§ | 63.0% | Lambourg et al. (2021) | [26] |
| Hemodialysis | 57.1% | Moore et al. (2023) | [27] |
| Peritoneal dialysis | 58.3% | Moore et al. (2023) | [27] |
| Renal transplant | 46.0% | Lambourg et al. (2021) | [26] |
| Depression | |||
| Relapse | 7.0% | Hayes et al. (2024) | [24] |
| Persistent NS§ | 21.0% | Shirazian et al. (2017) | [28] |
| Renal failure | 22.8% | Shirazian et al. (2017) | [28] |
| Disease progression | |||
| Relapse to ARF | 5.0% | Troyanov et al. (2005) | [2] |
| Persistent NS§ to ARF | 10.0% | Troyanov et al. (2005) | [2] |
| Persistent NS§ to ESRD | 8.0% | Kolb et al. (2021) | [29] |
| ARF to ESRD | 4.2% | Coca et al. (2012) | [30] |
| Mortality | |||
| Remission | 1.3% | Kolb et al. (2021) | [29] |
| Relapse or persistent NS§ | 2.2% | Kolb et al. (2021) | [29] |
| ARF | 8.7% | US Renal Data System (2024) | [31] |
| ESRD | 7.2% | US Renal Data System (2024) | [31] |
†
All parameters from the literature were converted to a 6-month probability, where applicable.
‡
No response refers to patients who initially did not exhibit a therapeutic effect, but subsequently achieved a response and experienced resolution of their relapse.
§
Persistent NS health state refers to the state to which a patient transitions when a patient fails to show a significant clinical improvement following the full course of the prescribed initial treatment.
¶
Data on ‘Acthar Gel without tacrolimus’ was only considered; a complete remission was defined as a UP/Cr ratio less than 300 mg/g Cr, and a partial response was defined as a 50% reduction in the pre-Acthar Gel treated UP/Cr ratio to a value less than 3500 mg/g.
#
For both comparators, outcomes to ensure cross-arm comparability were standardized. The cyclophosphamide source defined complete but not partial response, while the rituximab series reported patient-level proteinuria reductions without prespecified complete and partial response thresholds. Accordingly, all interventions (including Acthar Gel) were harmonized to KDIGO-aligned criteria: proteinuria <0.3 g/day (or UP/Cr <0.3 g/g) with normal serum albumin for complete response and ≥50% reduction to a subnephrotic level (≤3.5 g/day or UP/Cr ≤3.5 g/g) for partial response. These standardized thresholds are widely used in contemporary adult FSGS studies and reviews. Studies lacking explicit thresholds were mapped to KDIGO categories (rule-based classification from patient-level proteinuria reductions).
††
Response probability was 20%; therefore, the probability of transitioning to a persistent NS health state was assumed to be 80%, and no response was assumed to be 0%.
‡‡
ARF: Acute renal failure; Cr: Creatinine; ESRD: End-stage renal disease; FSGS: Focal segmental glomerulosclerosis; g: Gram; mg: Milligram; NS: Nephrotic syndrome; UP: Urine protein.
Clinical effectiveness data were derived from prospective and retrospective studies on FSGS, selected based on study design, sample size and relevant factors. The effectiveness of Acthar Gel was sourced from a prospective, observational study of treatment-resistant FSGS, where patients received subcutaneous Acthar Gel (40–80 units) two- to three-times weekly for 6 months [5]. Relapse probability was obtained from an observational study of idiopathic FSGS patients treated with Acthar Gel at two academic medical centers between 2009 and 2012 [1]. There is limited data on the effectiveness of cyclophosphamide and rituximab in adult patients with FSGS who have failed conventional treatments. Cyclophosphamide effectiveness came from retrospective analyses of registry data from Toronto (population base of 4 million) [2,19], while rituximab effectiveness and relapse rates were obtained from prospective studies of biopsy-proven FSGS patients who failed conventional treatments or presented with steroid-dependent or frequently relapsing NS [20,21]. Only serious adverse events (SAEs) were considered for cyclophosphamide [22] and rituximab [23]. The reviewed studies reported no treatment-related SAEs for Acthar Gel; therefore, SAEs were not considered for Acthar Gel [1,5,10–13].
Pain in NS is multidimensional (nociceptive, neuropathic and non-neuropathic) [27]. Pain is also common in patients with ESRD and is the primary cause of depression, disturbed sleep patterns, impaired dialysis adequacy and the likelihood of withdrawal from dialysis [32]. Therefore, pain prevalence was incorporated into the model, with estimates sourced from the published literature [26,27]. Depression is similarly prevalent in chronic kidney disease, including ESRD, and is associated with poor quality of life and increased mortality [28]. Consequently, depression was also included in the model, with prevalence estimates derived from published literature [24,28].
Persistent proteinuria in NS due to FSGS elevates the risk of chronic conditions, such as venous thrombosis, hypertension and hyperlipidemia, leading to cardiac complications and further progression of chronic kidney disease [33–35]. Probabilities of these complications were sourced from published literature [24,25].
Disease progression to kidney failure occurs in both relapsing and persistent NS health states. Due to limited data on Acthar Gel and SoC, both treatment groups were assumed to have the same progression probability, based on published literature [2,29,30]. NS is also associated with increased mortality due to kidney failure, infection, thrombosis and cancer [29]. Six-month probabilities of excess mortality attributable to NS were derived from published literature [29,31].
Cost inputs
Wholesale acquisition costs (WAC) as of 1 January 2025, were obtained from the Micromedex Red Book (Merative, Ann Arbor, MI) [36]. Specifically, the WAC for a 5 ml multidose vial of Acthar Gel was $45,304, and the average patient used 7.86 vials of Acthar Gel (based on the specialty pharmacy dispensing data for 12 months ending 31 December 2023), which incorporates real-world dose titration and treatment duration. The total cost of SoC, including cyclophosphamide and rituximab, was calculated using the dosing information, dosing strengths and WAC. The dosing information was sourced from the literature and based on guidelines [4,37]. An average body weight of 80.0 kg and a body surface area of 2.0 m2 were used for calculating the dosage. The cost calculation for rituximab also incorporated the cost and market share of both the biologic and its respective biosimilars. The resulting annual cost was $8554 for cyclophosphamide and $103,242 for rituximab.
Annual administration costs of $4170 were considered only for rituximab due to its intravenous administration [38]. Annual monitoring costs for both cyclophosphamide and rituximab were $480 [38]. As immunosuppressive agents necessitate antibiotic prophylaxis, trimethoprim/sulfamethoxazole was considered [39], with an annual cost of $250 [36]. Antiemetic costs were also factored into the overall administration expenses, with an annual cost of $877 [40].
The model incorporated a range of costs associated with FSGS management across different health states. These included costs for other treatments (supportive care medications, immunosuppressants, plasmapheresis, pain/depression medications), FSGS-related disease management (inpatient and outpatient), complications, end-of-life care and renal failure management (dialysis or renal transplant) [Table 2]. All costs were sourced from published literature. The costs were adjusted to 2025 US dollars using the US Consumer Price Index for Medical Care Services for Urban Consumers, where necessary [41].
| Parameters | Cost†,‡ | Source (year) | Ref. |
|---|---|---|---|
| Other treatments | Annual | ||
| Supportive care medications | |||
| ACEi/ARBs | $149 | Micromedex Red Book | [36] |
| Beta-blockers | $304 | Micromedex Red Book | [36] |
| Calcium channel blockers | $380 | Micromedex Red Book | [36] |
| Diuretics | $97 | Micromedex Red Book | [36] |
| Anticoagulants | $629 | Micromedex Red Book | [36] |
| Statins | $148 | Micromedex Red Book | [36] |
| Immunosuppressants | |||
| Systemic corticosteroids | $4383 | Micromedex Red Book | [36] |
| Cyclosporine | $16,810 | Micromedex Red Book | [36] |
| Tacrolimus | $16,843 | Micromedex Red Book | [36] |
| Mycophenolate Mofetil | $1527 | Micromedex Red Book | [36] |
| Plasmapheresis | $4888 | Micromedex Red Book; Heatwole et al. (2011); Winters et al. (2011); US BLS | [36,42–44] |
| Pain medications | |||
| Pain medication use | |||
| NSAIDs | $2242 | Katz et al. (2016) | [45] |
| Opioids | $4071 | Ding et al. (2020) | [46] |
| Pain medication-related toxicity | |||
| NSAIDs-related toxicity | $916 | Rahme et al. (2001) | [47] |
| Opioid-related substance abuse | $50,453 | White et al. (2005) | [48] |
| Antidepressants use | $3483 | Glassman et al. (2023) | [49] |
| FSGS-related disease management | Annual | ||
| Inpatient | $24,567 | Kalantar-Zadeh et al. (2022) | [50] |
| Outpatient | $45,468 | Kalantar-Zadeh et al. (2022) | [50] |
| Renal failure management | Annual | ||
| Dialysis | |||
| Hemodialysis | $188,520 | Bhatnagar et al. (2023) | [51] |
| Peritoneal dialysis | $174,188 | Bhatnagar et al. (2023) | [51] |
| Renal transplant | $487,836 | Bentley et al. (2020) | [52] |
| Complications | |||
| Chronic kidney disease | $17,664 | Jha et al. (2023) | [53] |
| Major cardiac complications | $21,683 | Jha et al. (2023) | [53] |
| End-of-life care | $105,124 | French et al. (2017) | [54] |
| Serious adverse events | Per event | ||
| Anemia/leukopenia | $23,872 | Weycker et al. (2008) | [55] |
| Venous thrombosis | $19,711 | Grosse et al. (2016) | [56] |
| Infections | $28,968 | Owens et al. (2024) | [57] |
| Infusion-related | $9386 | Foley et al. (2010) | [58] |
| Cardiovascular | $29,467 | Afana et al. (2015) | [59] |
| Endocrine/metabolic or impaired fasting glucose and diabetes mellitus | $15,519 | Fingar et al. (2021) | [60] |
| Acute kidney injury/increased creatinine level/reversible nephrotoxicity | $49,688 | Stottlemyer et al. (2024) | [61] |
| Irreversible nephrotoxicity | $180,819 | Stottlemyer et al. (2024) | [61] |
| Bleeding | $636 | Heatwole et al. (2011) | [42] |
| Catheter occlusion | $2477 | Heatwole et al. (2011) | [42] |
| Corticosteroid-related toxicity (annual) | $87,592 | Rice et al. (2018) | [62] |
†
All costs inflated to 2025 USD.
‡
Drug costs as of 1 January 2025.
ACEi: Angiotensin-converting enzyme inhibitor; ARB: Angiotensin receptor blocker; BLS, Bureau of Labor Statistics; FSGS: Focal segmental glomerulosclerosis; NSAID: Nonsteroidal anti-inflammatory drug; USD: US dollar.
Patients in all health states, except death, were assumed to receive supportive care medications for NS-related comorbidities such as hypertension, stroke, deep vein thrombosis and hyperlipidemia. The utilization rates of specific supportive care medications were angiotensin-converting enzyme inhibitors (ACEis) or angiotensin receptor blockers (ARBs) (69.4%), beta-blockers (31.9%), calcium channel blockers (18.1%), diuretics (62.5%), anticoagulants (9.7%) and statins (56.9%) (Symphony Health’s Integrated Dataverse [1 January 2016 to 31 December 2022]).
Patients in a persistent NS health state were assumed to receive immunosuppressants to manage proteinuria. The distribution of these treatments was as follows: systemic corticosteroids (chronic use): 44.0% [24], cyclosporine: 8.0% [63], tacrolimus: 12.3% [63] and mycophenolate mofetil: 0.3% [63]. Chronic corticosteroid use was assumed, resulting in all patients experiencing corticosteroid-related toxicity. Based on the published literature, the distribution of SAEs for cyclosporine was as follows: cardiovascular events: 10.8%, infections: 12.3%, nephrotoxicity: 3.1% and endocrine/metabolic events: 1.5% [23]. The distribution of SAEs for tacrolimus was as follows: reversible nephrotoxicity: 15.9%, irreversible nephrotoxicity: 9.0%, infections: 43.1% and impaired fasting glucose/diabetes mellitus: 22.7% [64]. In addition, 1.6% of patients were also assumed to receive plasmapheresis [63]. The data on the number of sessions [65] and costs were applied based on resources used for infusion to compute the cost per session, including the cost of acquisition, staff, equipment, materials costs and laboratory tests [36,42–44,66]. The distribution of SAEs for plasmapheresis was as follows: bleeding: 4.9%, catheter occlusion: 2.4%, deep vein thrombosis: 2.4% and infections: 2.4% [42].
Pain management included nonsteroidal anti-inflammatory drugs (NSAIDs) and/or opioids [45,46]. NSAID use was limited to patients in relapse due to the potential worsening of kidney function in persistent NS and renal failure health states [67]. Utilization rates and associated toxicity probabilities for both NSAIDs and opioids were sourced from the literature. Among patients in a relapse state, NSAID use was 50.0% and opioid use was 56.9% (Symphony Health’s Integrated Dataverse [1 January 2016 to 31 December 2022]). Opioid use among patients in the persistent NS health state was 20% [68], hemodialysis/peritoneal dialysis was 40.6% [69], and the kidney transplant was 60.0% [70]. The probability of NSAID-related toxicity was 25% [71]. Chronic opioid use was assumed to increase the risk of opioid-related abuse. The cost of pain-medication-related toxicity was also sourced from published literature [47,48]. Depression medication costs were considered for patients who did not achieve a treatment response [49].
FSGS management costs included inpatient and outpatient care for patients in a persistent NS health state [50], complication costs for persistent NS and disease progression health states [53], and end-of-life care costs for deceased patients [54]. ARF management involved dialysis (hemodialysis 89% and peritoneal dialysis 11%) [72,73]. ESRD management included dialysis (70%) or renal transplant (30%) [73]. Dialysis-related costs were applied to ARF patients, and dialysis and/or transplant costs were applied to ESRD patients [51,52].
Cost-per-response analysis
The primary analysis (base case) focused on determining the cost-per-response for Acthar Gel and SoC over 1 year. This was calculated by dividing the total healthcare costs per patient for a specific time horizon by the proportion of patients who achieved a resolved relapse within each treatment group. Total healthcare costs per patient include drug acquisition, administration/monitoring, SAEs, other treatments (supportive care and immunosuppressants), disease management and renal failure costs. Extended analyses were performed to assess cost-per-response at 2 and 3 years. Furthermore, the incremental cost-effectiveness was examined by calculating the difference in total healthcare costs per patient between interventions (incremental cost) divided by the difference in the proportion of patients responding to each intervention (incremental response) across the designated time frames. In base-case analyses, costs were discounted at 3.5% per year for the 2- and 3-year period.
Several key assumptions were made to reflect a population with refractory and persistent proteinuria in NS due to FSGS, and the best available data specific to this population were utilized. Acthar Gel was studied in patients who had failed at least two prior therapies (including corticosteroids), consistent with its real-world clinical practice. The model simulated a single, hypothetical cohort of adult steroid-resistant NS patients, defined by failure of prior conventional therapies, with identical baseline characteristics (including proteinuria levels and overall disease severity) across all three treatment arms. By assuming cohort homogeneity, it was ensured that observed differences in cost-per-response are driven by treatment effects rather than initial patient imbalances. Remaining variability in clinical and cost parameters was explicitly modeled through probability distributions and Monte Carlo simulation, thereby quantifying the impact of residual heterogeneity on the results. The model evaluated all interventions using KDIGO-aligned response criteria, proteinuria <0.3 g/day or urine protein-to-creatinine ratio <0.3 g/g with normal serum albumin for a complete response and ≥50% reduction in proteinuria to ≤3.5 g/day or urine protein-to-creatinine ratio ≤3.5 g/g for a partial response. Directional conclusions were unchanged in the sensitivity analyses. The response and relapse parameters used in the base case align with ranges reported in adult FSGS cohorts. After harmonizing source definitions to KDIGO thresholds, the 12 to 24-month complete/partial response rates assumed for Acthar Gel fall within the ranges observed in prospective and retrospective series of adults with primary FSGS under contemporary management [1,5,7,11]. Relapse probabilities applied in the model are also consistent with the recurrence patterns described in adult partial/complete remitters [2]. In the base-case model, identical probabilities of progression to renal failure were assumed for Acthar Gel and SoC because no long-term, head-to-head data exist demonstrating a differential impact of these agents on disease progression and ESRD onset. To ensure that this conservative simplification did not systematically underestimate the potential renal-protective benefit of Acthar Gel, sensitivity analyses were conducted. Moreover, disease progression did not emerge as a primary driver in the cost-per-response sensitivity analyses. Adverse event inputs were restricted to serious events requiring inpatient care, in line with regulatory definitions and common practice in economic evaluations. Accordingly, only hospitalization-level events (e.g., neutropenia and anemia) were modeled for cyclophosphamide and rituximab. Events described in Acthar Gel reports, such as weight gain, hypertension, edema, fatigue or seizures, were not consistently attributed to treatment and did not meet the hospitalization criterion, so they were not included. Notably, in sensitivity analyses, response and relapse parameters remained more influential than SAE assumptions for cost-per-response, indicating that study conclusions were not driven by SAE costing.
Sensitivity analyses were conducted to evaluate the robustness of the 1-year cost-per-response findings for Acthar Gel compared with SoC. Both deterministic and probabilistic methods were employed to assess the impact of variations in model parameters and base case assumptions. One-way deterministic sensitivity analysis (DSA) was performed by individually varying all key model inputs by ±30% and drug acquisition costs by ±10%. Additionally, a multivariable probabilistic sensitivity analysis was executed using 5000 simulations, in which the parameter values were randomly sampled from predefined probability distributions, allowing for a comprehensive evaluation of joint uncertainty. The selection of these distributions was driven by the inherent characteristics and limitations of the available data, ensuring that the full range of potential uncertainty was adequately represented.
Results
Over 1 year, Acthar Gel showed a lower cost-per-response ($469,735) compared with cyclophosphamide ($2,140,400) and rituximab ($1,272,477) [Figure 2]. Compared with cyclophosphamide, Acthar Gel, while costing $5836 more per patient, yielded a 45.7% higher response rate. Acthar Gel, despite having a $210,673 higher drug acquisition cost than cyclophosphamide, resulted in lower overall medical costs and incurred no treatment-related costs (administration/monitoring and adverse events) over the 1 year. Acthar Gel’s higher drug acquisition cost was offset by lower spending on other treatments (-$102,330), FSGS management (-$33,246), renal failure management (-$29,255), administration/monitoring (-$4188) and adverse events (-$35,818) compared with cyclophosphamide. Compared with rituximab, Acthar Gel resulted in cost savings of $1469 per patient and yielded a 36.6% higher response rate. Acthar Gel, despite having a $136,962 higher drug acquisition cost than rituximab, achieved cost offsets in other treatments (-$42,453), FSGS management (-$28,328), renal-failure management (-$22,538), administration/monitoring (-$7845) and adverse events (-$37,267) [Figure 3].
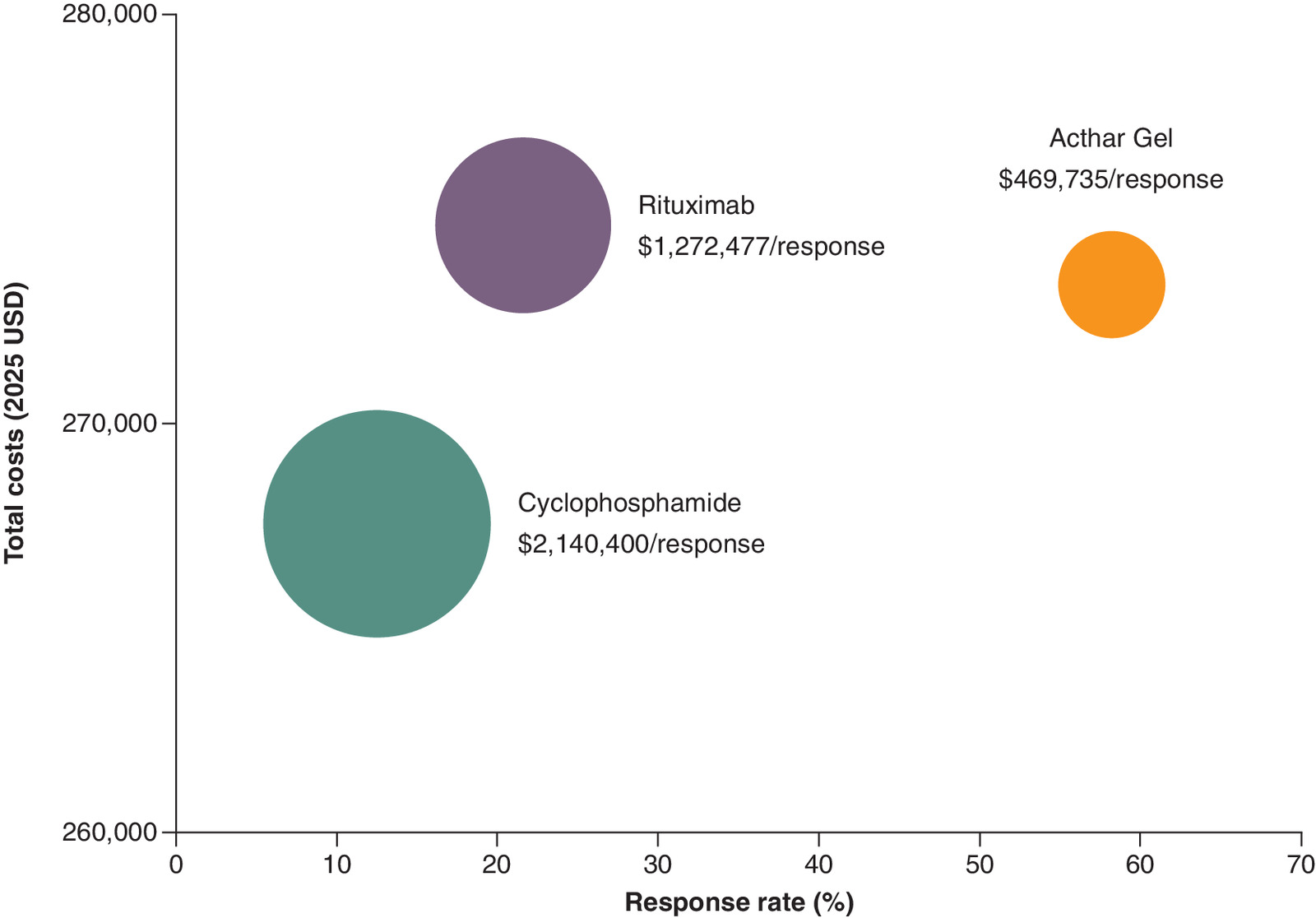
Figure 2. Cost-per-response over 1 year from a US payer perspective.
Results are presented on a per-person basis.
USD: United States dollar.
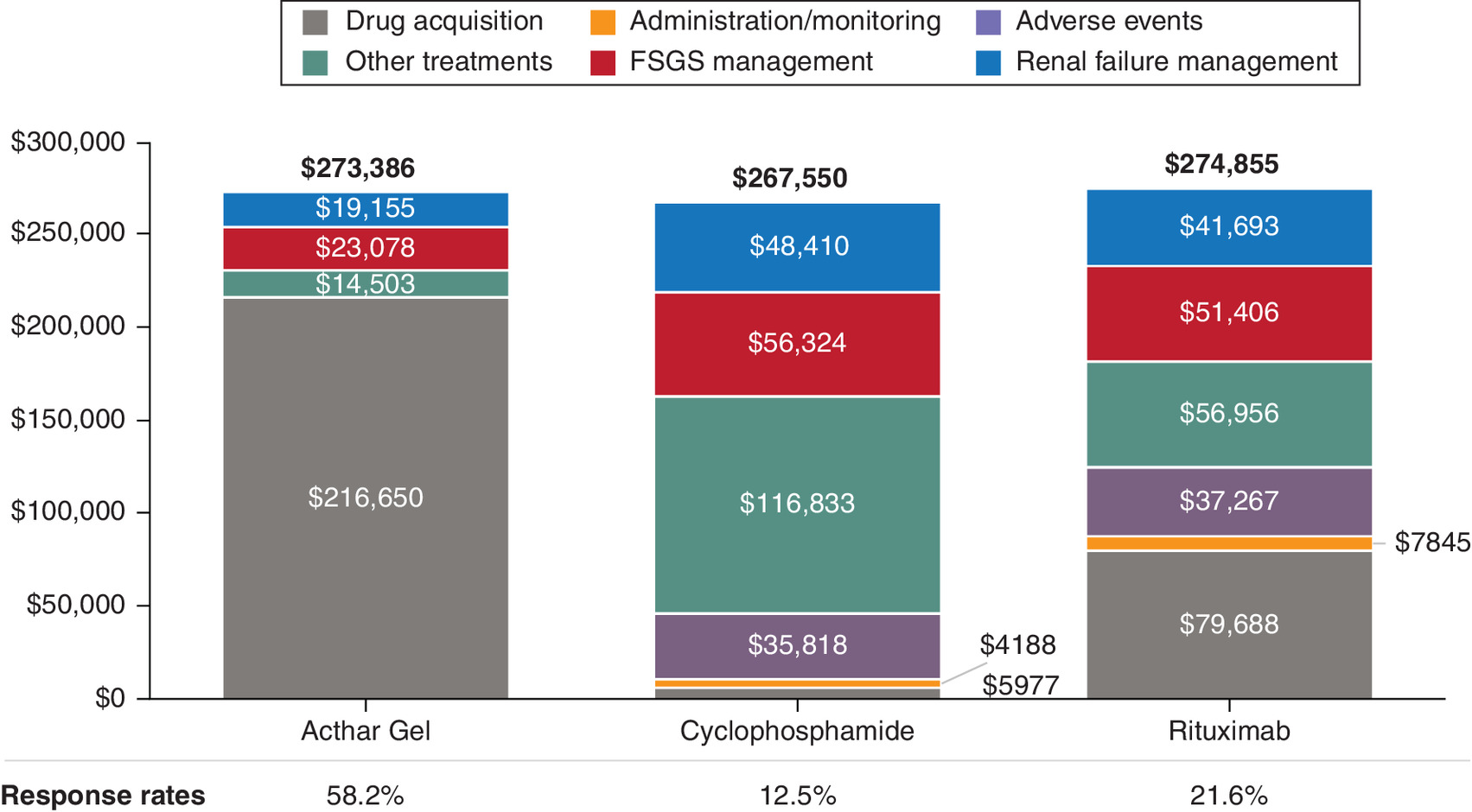
Figure 3. Overall cost of care and response rate over 1 year from a US payer perspective.
Numbers in bold represent total costs. Results are presented on a per-person basis; all costs inflated to 2025 US dollars. Other treatments include immunosuppressants (including monitoring and serious adverse events costs), supportive care treatments (antihypertensives, anticoagulants and statins), plasmapheresis, pain medications, antidepressants; disease management includes FSGS-related inpatient and outpatient (physician office visits, emergency department, other outpatient); renal failure management includes disease progression costs, including dialysis, renal transplant and complications.
FSGS: Focal segmental glomerulosclerosis.
This study also assessed cost-per-response over a timeframe of 2 and 3 years. This cost-per-response advantage for Acthar Gel over cyclophosphamide and rituximab was sustained at 2 and 3 years (Table 3). Acthar Gel showed a lower overall cost of care and higher response rates compared with cyclophosphamide and rituximab at 2 and 3 years. The overall cost of care patterns at 2 and 3 years was consistent with those observed at 1 year (Table 4). At 2 years, larger cost offsets for patients on Acthar Gel versus cyclophosphamide and rituximab were from lower renal failure management (-$92,518 and -$73,967, respectively) and other treatments (-$145,593 and -$72,311, respectively). The same pattern persisted for 3 years, with larger cost offsets for Acthar Gel versus cyclophosphamide and rituximab were renal failure management (-$170,700 and -$138,810, respectively) and other treatment (-$178,123 and -$98,033, respectively), supporting the dominance finding.
| Timeframe and intervention | Costs per patient† | Response rate | Cost-per-response‡ |
|---|---|---|---|
| 2 years | |||
| Acthar Gel | $405,219 | 52.8% | $767,460 |
| Cyclophosphamide | $482,534 | 6.7% | $7,202,000 |
| Rituximab | $483,710 | 14.8% | $3,268,311 |
| 3 years | |||
| Acthar Gel | $536,671 | 47.3% | $1,134,611 |
| Cyclophosphamide | $702,598 | 3.5% | $20,074,229 |
| Rituximab | $695,556 | 10.1% | $6,886,693 |
†
All costs inflated to 2025 US dollars.
‡
Results are presented on a per-person basis.
| Cost components†,‡ | Acthar Gel | CTX | Acthar Gel vs CTX§ | RTX | Acthar Gel vs RTX§ |
|---|---|---|---|---|---|
| 2 years | |||||
| Drug acquisition | $274,834 | $6758 | $268,076 | $99,054 | $175,780 |
| Administration/monitoring | $0 | $4735 | -$4735 | $9751 | -$9751 |
| Adverse events | $0 | $40,497 | -$40,497 | $46,323 | -$46,323 |
| Other treatments¶ | $30,898 | $176,491 | -$145,593 | $103,209 | -$72,311 |
| Disease management# | $48,373 | $110,421 | -$62,048 | $100,292 | -$51,919 |
| Renal failure management†† | $51,114 | $143,632 | -$92,518 | $125,081 | -$73,967 |
| 3 years | |||||
| Drug acquisition | $322,382 | $7028 | $315,354 | $110,264 | $212,118 |
| Administration/monitoring | $0 | $4924 | -$4924 | $10,854 | -$10,854 |
| Adverse events | $0 | $42,117 | -$42,117 | $51,565 | -$51,565 |
| Other treatments¶ | $48,006 | $226,129 | -$178,123 | $146,039 | -$98,033 |
| Disease management# | $72,793 | $158,210 | -$85,417 | $144,534 | -$71,741 |
| Renal failure management†† | $93,490 | $264,190 | -$170,700 | $232,300 | -$138,810 |
†
Results are presented on a per-person basis.
‡
All costs inflated to 2025 US dollars.
§
Differences are calculated as Acthar Gel minus comparator. Negative values indicate lower costs with Acthar Gel (i.e., savings) and vice versa.
¶
Other treatments include immunosuppressants (including monitoring and serious adverse events costs), supportive care treatments (antihypertensives, anticoagulants and statins), plasmapheresis, pain medications and antidepressants.
#
Disease management includes FSGS-related inpatient and outpatient (physician office visits, emergency department and other outpatient).
††
Renal failure management includes disease progression costs, including dialysis, renal transplant and complications.
CTX: Cyclophosphamide; RTX: Rituximab.
Under the base-case assumptions and clinical inputs, Acthar Gel incurred lower costs and achieved a higher response rate; therefore, Acthar Gel emerged as a potential dominant treatment option compared with cyclophosphamide or rituximab at 2 and 3 years, exhibiting lower costs and higher response rates (Table 5).
| Timeframe and intervention | Incremental costs†,‡,§ | Incremental response | Incremental cost-per-response†,‡ |
|---|---|---|---|
| 1 year | |||
| Acthar Gel vs cyclophosphamide | $5836 | 45.7% | $12,770 |
| Acthar Gel vs rituximab | -$1469 | 36.6% | Dominant¶ |
| 2 years | |||
| Acthar Gel vs cyclophosphamide | -$77,315 | 46.1% | Dominant¶ |
| Acthar Gel vs rituximab | -$78,491 | 38.0% | Dominant¶ |
| 3 years | |||
| Acthar Gel vs cyclophosphamide | -$165,927 | 43.8% | Dominant¶ |
| Acthar Gel vs rituximab | -$158,885 | 37.2% | Dominant¶ |
†
All costs inflated to 2025 US dollars.
‡
Results are presented on a per-person basis.
§
Negative incremental costs indicate that Acthar Gel is cost-saving.
¶
Under the base-case assumptions and clinical inputs used in this model, Acthar Gel incurred lower costs and achieved a higher response rate than cyclophosphamide or rituximab and is therefore classified as ‘dominant’.
The DSA identified the major contributors to the cost-per-response over a 1-year period. For Acthar Gel versus cyclophosphamide, the major contributors to cost-per-response were the immunosuppressant-related toxicity, response rate of Acthar Gel, acquisition cost of Acthar Gel, relapse rate of Acthar Gel and cyclophosphamide-related SAEs. For Acthar Gel versus rituximab, the major contributors to cost-per-response were the response rate of Acthar Gel, the acquisition cost of Acthar Gel, the relapse rate of Acthar Gel, rituximab-related SAEs and immunosuppressant-related toxicity (Figure 4).
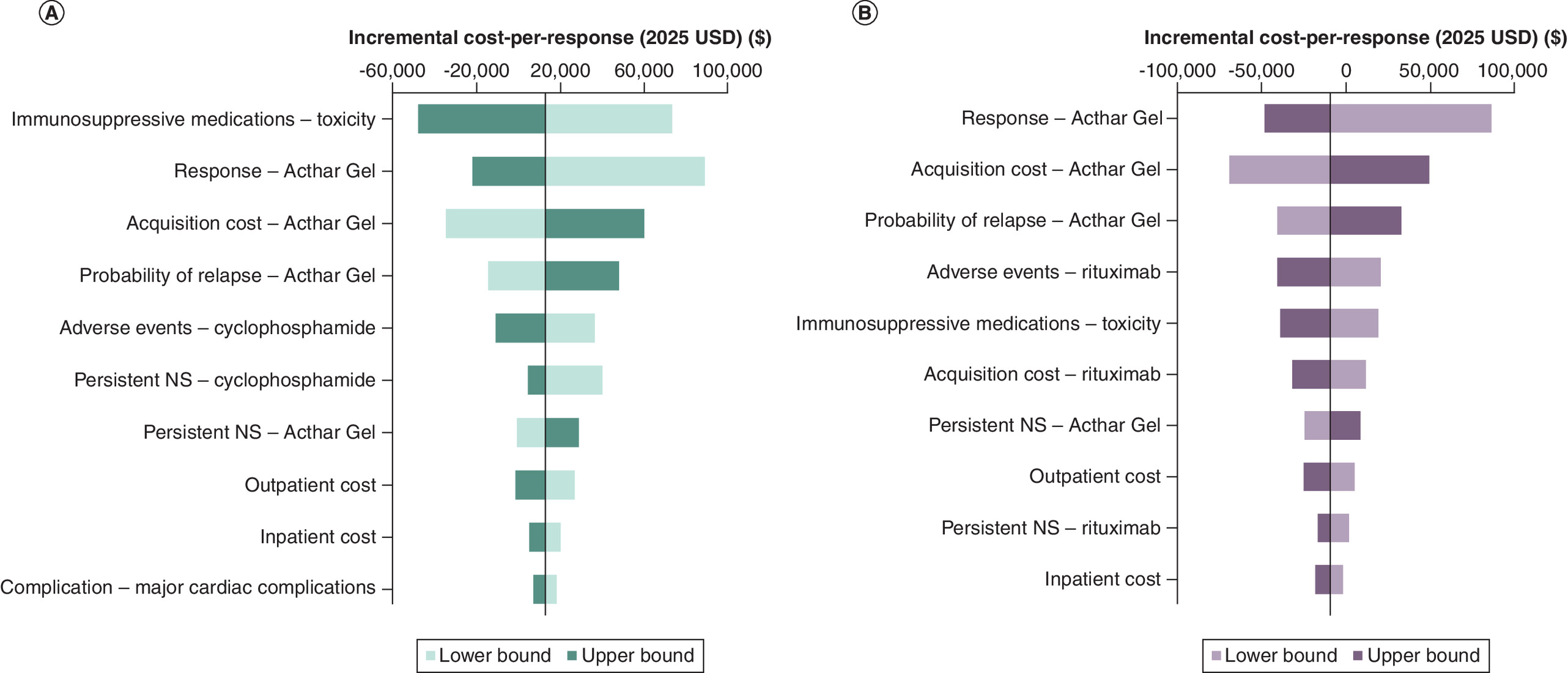
Figure 4. Key drivers of
cost-per-response: deterministic sensitivity analysis of Acthar Gel versus standard of care over 1 year from a US payer perspective. (A) Cyclophosphamide and (B) Rituximab. Persistent NS health state refers to the state to which a patient transitions when a patient fails to show a significant clinical improvement following the full course of the prescribed initial treatment. Bars represent the variation in the cost-per-response corresponding to high and low variation on a parameter’s point estimate. The ‘lower bound’ represents the model outcome when a specific parameter is set to its minimum value within the specified range, while holding all other parameters at their base or central values. The ‘upper bound’ represents the model outcome when a specific parameter is set to its maximum value within the specified range, while holding all other parameters at their base or central values. The vertical line dividing the lower and upper bound bars represents the base case cost-per-response when all inputs are set to their base case estimates. Parameters are presented in a ranked order, with the most influential variables at the top. The length of the bars represents the magnitude of impact, and their direction (left or right) indicates whether the impact is positive or negative. If the impact of an input is positively related, then increasing the input estimate increases the cost-per-response (upper bound bar extends to the right; lower bound bar to the left) and vice versa. Conversely, if the impact of an input is negatively related, then increasing the input estimate decreases the cost-per-response (upper bound bar extends to the left; lower bound bar to the right) and vice versa.
NS: Nephrotic syndrome; USD: United States dollar.
The probabilistic sensitivity analysis showed that, at a willingness-to-pay threshold of $150,000 per response over 1 year, Acthar Gel was cost-effective in 99.0% of iterations versus cyclophosphamide and 100.0% of iterations versus rituximab (Figure 5).
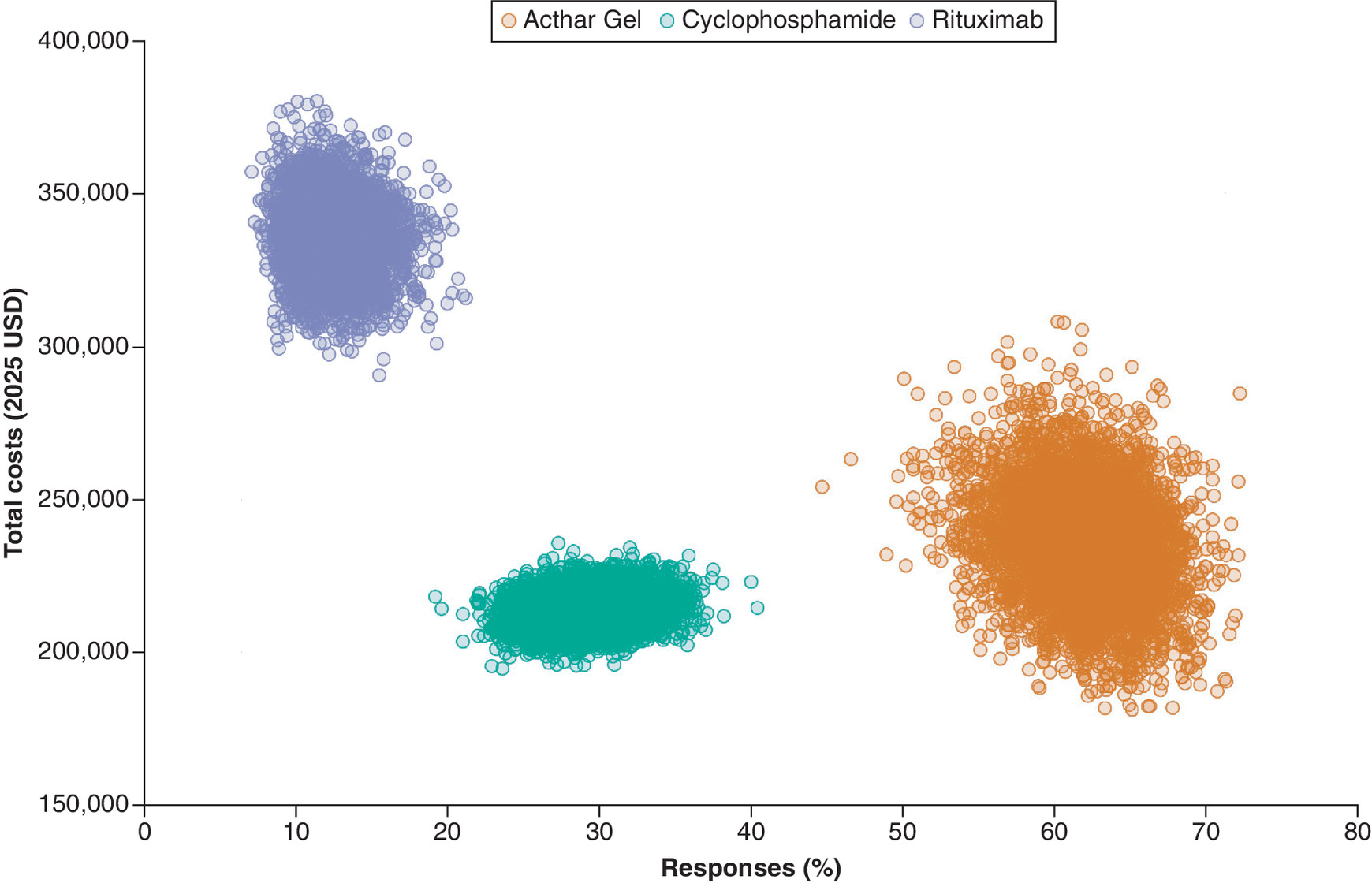
Figure 5. Scatter plot Acthar Gel versus cyclophosphamide and rituximab over 1 year from a US payer perspective.
USD: United States dollar.
Discussion
Proteinuria is a critical marker in FSGS and a risk factor for the progression of kidney disease [2,3,74]. Managing proteinuria in NS, particularly in cases that are difficult to treat, is challenging due to the lack of consensus on optimal treatment strategies [3–5]. This study evaluated the economic impact of treatment options for proteinuria in NS due to FSGS among adults who have previously failed conventional treatments.
Acthar Gel showed a more favorable cost-per-response profile compared with unapproved standard therapies, such as cyclophosphamide and rituximab, over a 1- to 3-year timeframe. Specifically, the cost-per-response with Acthar Gel was approximately five-times lower than cyclophosphamide and three-times lower than rituximab over a 1-year period. This advantageous cost-per-response for Acthar Gel remained consistent across various sensitivity analyses. DSA revealed that the higher response rate associated with Acthar Gel was a key factor driving its lower cost-per-response compared with SoC. Other significant cost drivers included the higher probability of immunosuppressant-related toxicity and SAEs related to SoC, as well as the lower relapse rate and higher acquisition costs of Acthar Gel. Furthermore, over the 2- and 3-year horizons, Acthar Gel emerged as a potential dominant strategy, exhibiting both reduced costs and improved response rates under the base-case assumptions and clinical inputs considered in this economic evaluation. Although the initial drug acquisition cost of Acthar Gel was higher than SoC, it was associated with reduced overall direct medical expenditures throughout the evaluation period. This cost reduction with Acthar Gel was attributed to its decreased need for immunosuppressant medications, plasmapheresis, pain/depression medications, disease management resources and resource-intensive interventions such as dialysis and renal transplant. Importantly, Acthar Gel incurred no treatment-related costs for administration, monitoring or adverse events.
This study is the first economic assessment comparing the clinical and cost implications of treatment options for adults with refractory proteinuria in NS due to FSGS among patients who have failed on conventional therapies within the US payer context. It contributes novel insights to the limited evidence addressing this challenging condition. By capturing these potential pathways, the model provides a comprehensive framework for evaluating the short-term clinical and economic consequences of different treatment strategies for managing proteinuria in NS due to FSGS. The possible transitions between health states in this model have significant implications for both patient outcomes and healthcare resource utilization. For instance, the potential for patients to transition from a relapse to a response state highlights the variability in treatment effectiveness and the need for individualized approaches. The possibility of cycling between relapse and response states underscores the chronic nature of proteinuria in NS due to FSGS and the potential for ongoing treatment needs. Additionally, the transitions to ARF or ESRD emphasize the potential severity of the disease and the possibility of requiring more intensive interventions like dialysis or transplantation. These transitions also carry substantial cost implications for payers. Further, the findings from this study may equip clinicians and payers with crucial data for informed decision-making among adults who fail conventional treatments. Given the challenges associated with proteinuria in NS due to FSGS, treatment selection should be guided by clinical acumen, available resources and individualized patient needs. Lastly, this analysis provides a basis for future investigations, including longitudinal studies and subgroup analyses aimed at identifying patient subgroups who may derive greater benefit from Acthar Gel.
Effective management of proteinuria in NS due to FSGS primarily focuses on achieving remission, reducing complications, and preventing renal failure, thereby minimizing economic burden. Further, evaluating treatments based on their ability to deliver positive outcomes cost-effectively is paramount [75]. This study underscores the pivotal role of improved response rate with Acthar Gel in shaping its cost-per-response profile for treating proteinuria in NS due to FSGS. Acthar Gel’s lower relapse rate, another key factor in this economic evaluation, contributed significantly to its favorable outcomes compared with cyclophosphamide. Though rituximab had a marginally lower rate, a higher response rate with Acthar Gel suggests notable clinical and economic advantages. Despite a higher drug acquisition cost, the observed reduction in overall costs highlights the potential of treatments with improved response rates to achieve treatment goals and generate cost savings. This emphasizes the potential use of treatments with better response rates to achieve treatment goals and provide cost savings for healthcare systems. Furthermore, the acquisition cost of Acthar Gel, while a significant factor, is mitigated by the reduced downstream costs. The observed favorable cost-per-response of Acthar Gel over SoC can be further enhanced through strategic pricing mechanisms, such as rebates, bolstering its value proposition as a potentially cost-effective treatment alternative.
A higher probability of immunosuppressant toxicities with cyclophosphamide and rituximab was also the primary cost driver in the Acthar Gel versus SoC comparison. Cyclophosphamide regimens, which typically also include systemic corticosteroids, pose a greater risk of long-term toxicity than other treatments [7,8]. SAEs associated with both of these SoC treatments also significantly impacted healthcare resource utilization and costs. Acthar Gel showed a favorable cost-per-response compared with these unapproved SoCs, suggesting potential reductions in healthcare expenditures and improved patient outcomes through lower treatment-related toxicity rates.
This economic evaluation acknowledges certain limitations. First, the analysis, framed from a US payer perspective, may not be entirely generalizable for healthcare systems with differing protocols for treating adults with proteinuria in NS due to FSGS. Second, relying on published observational data for clinical and cost inputs introduces the potential for variations from real-world scenarios. Clinical efficacy inputs for Acthar Gel are based on observational data, rather than head-to-head randomized comparisons with off-label therapies, which may limit the precision of transition probability estimates. Modeling heterogeneity as random variation may underestimate systematic biases stemming from divergent patient populations, study designs, or outcome definitions. Until head-to-head trials or individual-patient data meta-analyses become available, residual heterogeneity remains a potential source of uncertainty in the comparative findings. Furthermore, harmonizing response definitions across heterogeneous sources may lead to misclassification. Nonetheless, sensitivity analyses did not alter the directional conclusions. Due to the absence of comparative long-term data on ESRD progression under Acthar Gel versus SoC, equal progression probabilities were assumed across treatment arms. Sensitivity analyses were conducted to assess the impact of varying these rates and to confirm that potential underestimation of Acthar Gel’s renal-protective effects did not materially affect the conclusions. Third, accurately quantifying the nuanced implications of proteinuria in NS due to FSGS on health and resource utilization remains challenging due to data scarcity. Fourth, AEs reported in some Acthar Gel studies were not included because they did not meet the prespecified definition of SAEs (i.e., events requiring hospitalization). This selective inclusion may modestly underestimate total costs, particularly for Acthar Gel, however, the same SAE-only rule was applied to the off-label comparators. Importantly, sensitivity analyses did not alter the direction of the results, suggesting this limitation has limited impact on the study’s primary conclusions. Fifth, the model did not account for potential manufacturer pricing adjustments, such as discounts or rebates. Sixth, it was not possible to directly assess external validity by comparing findings from this study with those from existing economic evaluations in the same patient population. To date, no prior economic evaluation studies have been conducted specifically in adults with refractory proteinuria in NS due to FSGS who have failed two or more previous treatments. However, several steps were taken to strengthen the internal validity and contextualize the findings. The model’s clinical inputs, including treatment response rates, costs, and relapse rates, were derived from a comprehensive review of existing clinical literature, real-world claims data, and expert opinion. This ensured that the model accurately reflected the current standard of care and typical patient experiences to the extent possible. Furthermore, extensive sensitivity analyses were conducted to assess the robustness of the results, considering the inherent uncertainty in these parameters. Finally, uncertainty is introduced from the lack of randomized trials, the limited quality studies in difficult-to-treat proteinuria in FSGS, and the off-label use of SoC treatments. Hence, the robustness of the findings was tested through sensitivity analyses, which consistently supported Acthar Gel’s favorable cost-per-response profile, accounting for these limitations.
Since this analysis relies on modeled assumptions and limited randomized trial data from heterogeneous populations, the findings should be interpreted as hypothesis-generating. To address these limitations, the robustness of the results was evaluated through sensitivity analyses, which consistently validated Acthar Gel’s advantageous cost-per-response profile. Building on these findings, future longitudinal studies should prioritize head-to-head trials comparing Acthar Gel with other treatments to assess proteinuria reduction, extended follow-up of at least 2–3 years to document response durability, incorporation of patient-reported outcome measures to evaluate treatment impact on quality of life and functional status, and real-world registry analyses integrated with economic evaluations.
Despite limitations, the study suggests that Acthar Gel may be a potentially value-driven therapeutic strategy for adults with proteinuria in NS due to FSGS. The observed favorable cost-per-response is mainly attributable to its improved response rate, which, in turn, diminishes the need for subsequent, resource-intensive interventions. This reduced healthcare resource utilization effectively counterbalances the initial investment in drug-related costs, leading to overall cost savings. This analysis underscores the importance of a value-centric approach to treatment decisions for therapies that improve patient outcomes and optimize the allocation of healthcare resources.
Conclusion
This analysis indicates that, based on the current assumptions and clinical inputs, from a US healthcare payer perspective, Acthar Gel appears to be a cost-effective, value-based treatment option for adults with refractory proteinuria in NS due to FSGS, particularly for those who have failed multiple treatments. While reliant on current model inputs, this economic analysis provides promising early insights and lays the groundwork for hypothesis-driven research, particularly in populations with limited data. This finding may inform provider and payer decision-making when conventional therapies prove ineffective for this patient population. Future research, including head-to-head trials or registry studies, is needed to validate the clinical evidence.
Summary points
•
Proteinuria, a hallmark of glomerulopathies, is a crucial marker in focal segmental glomerulosclerosis (FSGS).
•
Acthar® Gel is approved by the US FDA to induce a diuresis or a remission of proteinuria in the nephrotic syndrome (NS) without uremia of the idiopathic type or due to lupus erythematosus.
•
This study evaluated the cost-per-response of Acthar Gel compared with standard of care for the treatment of refractory proteinuria in NS due to FSGS among adults who have not responded to conventional therapies from a US healthcare payer perspective over a 1- to 3-year horizon.
•
A probabilistic, cohort-level state-transition decision-analytic model was developed to assess the economic value of Acthar Gel.
•
Over 1 year, Acthar Gel showed a lower cost-per-response ($469,735) versus cyclophosphamide ($2,140,400) and rituximab ($1,272,477).
•
Acthar Gel also demonstrated a lower overall cost of care and higher response rates compared with standard of care at 2 and 3 years.
•
Acthar Gel may be a cost-effective, value-based treatment option for selected patients with proteinuria in NS due to FSGS from a US healthcare payer perspective.
•
Further research is required to examine the long-term clinical effectiveness and economic benefit of Acthar Gel for proteinuria in NS due to FSGS.
Author contributions
All authors made a significant contribution to the work reported, including study conception, design, execution, acquisition of data, analysis and interpretation, and in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Financial disclosure
This study was sponsored by Mallinckrodt Pharmaceuticals (NJ, USA). The authors had complete editorial control of the paper and provided their final approval of all content. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interests disclosure
K Hayes, J Niewoehner and GJ Wan are employees of Mallinckrodt Pharmaceuticals. I Chopra, J Bindra and M Panaccio are paid research consultants for the study. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This economic analysis is based on data from the published literature and, therefore, did not involve any new studies of human or animal subjects.
Data sharing statement
The data used in the current study are available within the manuscript. The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Hogan J, Bomback AS, Mehta K et al. Treatment of idiopathic FSGS with adrenocorticotropic hormone gel. Clin. J. Am. Soc. Nephrol. 8(12), 2072–2081 (2013).
• Provides experience treating idiopathic focal and segmental glomerulosclerosis (FSGS) with Acthar Gel at two medical centers.
2.
Troyanov S, Wall CA, Miller JA, Scholey JW, Cattran DC. Toronto Glomerulonephritis Registry Group. Focal and segmental glomerulosclerosis: definition and relevance of a partial remission. J. Am. Soc. Nephrol. 16(4), 1061–1068 (2005).
• Provides data on rate of renal function decline (slope of creatinine clearance) and renal survival in nephrotic FSGS patients.
3.
Levey AS, Cattran D, Friedman A et al. Proteinuria as a surrogate outcome in CKD: report of a scientific workshop sponsored by the National Kidney Foundation and the US Food and Drug Administration. Am. J. Kidney Dis. 54(2), 205–226 (2009).
4.
Kidney Disease: Improving Global Outcomes Glomerular Diseases Work G. KDIGO 2021 clinical practice guideline for the management of glomerular diseases. Kidney Int. 100(Suppl. 4), S1–S276 (2021).
•• These guidelines provide recommendations for the management of proteinuria in nephrotic syndrome (NS) due to FSGS.
5.
Tumlin J, Galphin C, Santos R, Rovin B. Safety and efficacy of combination Acthar Gel and tacrolimus in treatment-resistant focal segmental glomerulosclerosis and membranous glomerulopathy. Kidney Int. Rep. 2(5), 924–932 (2017).
•• This prospective, observational study evaluated the efficacy and safety of Acthar Gel in treating proteinuria in NS due to FSGS.
6.
Beck LH Jr, Ayoub I, Caster D et al. KDOQI US Commentary on the 2021 KDIGO Clinical Practice Guideline for the Management of Glomerular Diseases. Am. J. Kidney Dis. 82(2), 121–175 (2023).
•• A US commentary on the KDIGO 2021 guideline (KDOQI) provides information on management with alternative treatment options for frequently relapsing FSGS.
7.
Korbet SM. Treatment of primary FSGS in adults. J. Am. Soc. Nephrol. 23(11), 1769–1776 (2012).
8.
Moghadam-Kia S, Werth VP. Prevention and treatment of systemic glucocorticoid side effects. Int. J. Dermatol. 49(3), 239–248 (2010).
9.
Mallinckrodt Pharmaceuticals. Acthar® Gel prescribing information. (1952). (Revised October 2021). https://www.acthar.com/pdf/Acthar-PI.pdf
10.
Bomback AS, Canetta PA, Beck LH Jr, Ayalon R, Radhakrishnan J, Appel GB. Treatment of resistant glomerular diseases with adrenocorticotropic hormone gel: a prospective trial. Am. J. Nephrol. 36(1), 58–67 (2012).
11.
Bomback AS, Tumlin JA, Baranski J et al. Treatment of nephrotic syndrome with adrenocorticotropic hormone (ACTH) gel. Drug Des. Devel. Ther. 5, 147–153 (2011).
12.
Filippone EJ, Dopson SJ, Rivers DM et al. Adrenocorticotropic hormone analog use for podocytopathies. Int. Med. Case Rep. J. 9, 125–133 (2016).
13.
Madan A, Mijovic-Das S, Stankovic A, Teehan G, Milward AS, Khastgir A. Acthar Gel in the treatment of nephrotic syndrome: a multicenter retrospective case series. BMC Nephrol. 17, 37 (2016).
14.
Rovin BH, Adler SG, Barratt J et al. Executive summary of the KDIGO 2021 Guideline for the Management of Glomerular Diseases. Kidney Int. 100(4), 753–779 (2021).
15.
AlSahow A, Al-Muhaiteeb A, Nawar H et al. Use of rituximab as an off-label medication in glomerular diseases: clinical perspective. Med. Princ. Pract. 31(2), 133–141 (2022).
16.
Genentech. Rituxan (rituximab): prescribing information. (2010). (cited 20 February 2025). https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/103705s5311lbl.pdf
17.
UNC Kidney Center. Cyclophosphamide (Cytoxan®). (2025). (cited 20 February 2025). https://unckidneycenter.org/kidneyhealthlibrary/drug-information/cyclophosphamide-cytoxan/
18.
Food and Drug Administration. Cyclophosphamide injection: prescribing information. (2020). (cited 20 February 2025). https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/212501s000lbl.pdf
19.
Cattran DC, Rao P. Long-term outcome in children and adults with classic focal segmental glomerulosclerosis. Am. J. Kidney Dis. 32(1), 72–79 (1998).
20.
Fernandez-Fresnedo G, Segarra A, Gonzalez E et al. Rituximab treatment of adult patients with steroid-resistant focal segmental glomerulosclerosis. Clin. J. Am. Soc. Nephrol. 4(8), 1317–1323 (2009).
21.
Ruggenenti P, Ruggiero B, Cravedi P et al. Rituximab in steroid-dependent or frequently relapsing idiopathic nephrotic syndrome. J. Am. Soc. Nephrol. 25(4), 850–863 (2014).
22.
Fernández-Juárez G, Rojas-Rivera J, Logt A-Evd et al. The STARMEN trial indicates that alternating treatment with corticosteroids and cyclophosphamide is superior to sequential treatment with tacrolimus and rituximab in primary membranous nephropathy. Kidney Int. 99(4), 986–998 (2021).
23.
Fervenza FC, Appel GB, Barbour SJ et al. Rituximab or cyclosporine in the treatment of membranous nephropathy. N. Engl. J. Med. 381(1), 36–46 (2019).
24.
Hayes K, Hu FS, Fahim M, Panaccio M, Niewoehner J, Wan GJ. SA27 Reduction in corticosteroid use among patients with focal segmental glomerulosclerosis, membranous nephropathy, or IgA nephropathy after Acthar® Gel in a large administrative claims database. Value Health 27(6), S400 (2024).
25.
Rice JB, Panaccio MP, White A et al. Consequences of insurance denials among U.S. patients prescribed repository corticotropin injection (Acthar Gel) for nephrotic syndrome. Curr. Med. Res. Opin. 37(3), 431–441 (2021).
26.
Lambourg E, Colvin L, Guthrie G et al. The prevalence of pain among patients with chronic kidney disease using systematic review and meta-analysis. Kidney Int. 100(3), 636–649 (2021).
27.
Moore I, Byrne P, Ilic N, Chen JH, Lambert K. The prevalence and lived experience of pain in people undertaking dialysis. Kidney Dialysis 3, 24–35 (2023).
28.
Shirazian S, Grant CD, Aina O, Mattana J, Khorassani F, Ricardo AC. Depression in chronic kidney disease and end-stage renal disease: similarities and differences in diagnosis, epidemiology, and management. Kidney Int. Rep. 2(1), 94–107 (2017).
29.
Kolb A, Gallacher PJ, Campbell J et al. A national registry study of patient and renal survival in adult nephrotic syndrome. Kidney Int. Rep. 6(2), 449–459 (2021).
30.
Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int. 81(5), 442–448 (2012).
31.
National Institute of Diabetes and Digestive and Kidney Diseases. United States Renal Data System. (2024). (cited 25 January 2025). https://usrds-adr.niddk.nih.gov/2024/end-stage-renal-disease/6-mortality
32.
Brkovic T, Burilovic E, Puljak L. Prevalence and severity of pain in adult end-stage renal disease patients on chronic intermittent hemodialysis: a systematic review. Patient Prefer. Adherence 10, 1131–1150 (2016).
33.
Kodner C. Diagnosis and management of nephrotic syndrome in adults. Am. Fam. Physician 93(6), 479–485 (2016).
34.
Ordonez JD, Hiatt RA, Killebrew EJ, Fireman BH. The increased risk of coronary heart disease associated with nephrotic syndrome. Kidney Int. 44(3), 638–642 (1993).
35.
Li SJ, Tu YM, Zhou CS, Zhang LH, Liu ZH. Risk factors of venous thromboembolism in focal segmental glomerulosclerosis with nephrotic syndrome. Clin. Exp. Nephrol. 20(2), 212–217 (2016).
36.
Merative LP. Micromedex® Red Book®. (2025). https://www.merative.com/documents/micromedex-red-book
37.
Osterholt T, Todorova P, Kuhne L et al. Repetitive administration of rituximab can achieve and maintain clinical remission in patients with MCD or FSGS. Sci. Rep. 13(1), 6980 (2023).
38.
Schmier J, Ogden K, Nickman N et al. Costs of providing infusion therapy for rheumatoid arthritis in a hospital-based infusion center setting. Clin. Ther. 39(8), 1600–1617 (2017).
39.
Chung JB, Armstrong K, Schwartz JS, Albert D. Cost-effectiveness of prophylaxis against Pneumocystis carinii pneumonia in patients with Wegner's granulomatosis undergoing immunosuppressive therapy. Arthritis Rheum. 43(8), 1841–1848 (2000).
40.
Gupta A, Nshuti L, Grewal US et al. Financial burden of drugs prescribed for cancer-associated symptoms. JCO Oncol. Pract. 18(2), 140–147 (2022).
41.
US Bureau of Labor Statistics. CPI for all urban consumers. Medical care in U.S. city average, all urban consumers, seasonally adjusted. (2025). (cited 31 March 2025). https://data.bls.gov/
42.
Heatwole C, Johnson N, Holloway R, Noyes K. Plasma exchange versus intravenous immunoglobulin for myasthenia gravis crisis: an acute hospital cost comparison study. J. Clin. Neuromuscul. Dis. 13(2), 85–94 (2011).
43.
Winters JL, Brown D, Hazard E, Chainani A, Andrzejewski C Jr. Cost-minimization analysis of the direct costs of TPE and IVIg in the treatment of Guillain-Barre syndrome. BMC Health Serv. Res. 11, 101 (2011).
44.
US Bureau of Labor Statistics. Occupational employment and wage statistics. (2024). (cited 20 January 2025). https://www.bls.gov/oes/
45.
Katz JN, Smith SR, Collins JE et al. Cost-effectiveness of nonsteroidal anti-inflammatory drugs and opioids in the treatment of knee osteoarthritis in older patients with multiple comorbidities. Osteoarthritis Cartilage 24(3), 409–418 (2016).
46.
Ding Y, Miller GE. Total expenses, total utilization, and sources of payment for outpatient prescription opioids in the U.S. Adult civilian noninstitutionalized population, 2017. HCUP Statistical Brief #529. Agency for Healthcare Research and Quality, MD, USA (April 2020).
47.
Rahme E, Joseph L, Kong SX, Watson DJ, LeLorier J. Cost of prescribed NSAID-related gastrointestinal adverse events in elderly patients. Br. J. Clin. Pharmacol. 52(2), 185–192 (2001).
48.
White AG, Birnbaum HG, Mareva MN et al. Direct costs of opioid abuse in an insured population in the United States. J. Manag. Care Pharm. 11(6), 469–479 (2005).
49.
Glassman JR, Jauregui A, Milstein A, Kaplan RM. Caring for people with depression: costs among 43 million commercially insured patients with or without comorbid illnesses. Ann. Behav. Med. 57(5), 380–385 (2023).
50.
Kalantar-Zadeh K, Baker CL, Copley JB et al. A retrospective study of clinical and economic burden of focal segmental glomerulosclerosis (FSGS) in the United States. Kidney Int. Rep. 6(10), 2679–2688 (2021).
51.
Bhatnagar A, Niu J, Ho V, Winkelmayer WC, Erickson KF. Hemodialysis versus peritoneal dialysis drug expenditures: a comparison within the private insurance market. Kidney Med. 5(8), 100678 (2023).
52.
Bentley TS, Ortner N. 2020 U.S. organ and tissue transplants: cost estimates, discussion, and emerging issues. (2020). (cited 3 December 2025). https://www.milliman.com/en/insight/2020-us-organ-and-tissue-transplants
53.
Jha V, Al-Ghamdi SMG, Li G et al. Global economic burden associated with chronic kidney disease: a pragmatic review of medical costs for the inside CKD Research Programme. Adv. Ther. 40(10), 4405–4420 (2023).
54.
French EB, McCauley J, Aragon M et al. End-of-life medical spending in last twelve months of life is lower than previously reported. Health Aff. (Millwood). 36(7), 1211–1217 (2017).
55.
Weycker D, Malin J, Edelsberg J, Glass A, Gokhale M, Oster G. Cost of neutropenic complications of chemotherapy. Ann. Oncol. 19(3), 454–460 (2008).
56.
Grosse SD, Nelson RE, Nyarko KA, Richardson LC, Raskob GE. The economic burden of incident venous thromboembolism in the United States: a review of estimated attributable healthcare costs. Thromb. Res. 137, 3–10 (2016).
57.
Owens PL, Miller MA, Barrett ML, Hensche M. Overview of outcomes for inpatient stays involving sepsis, 2016–2021. HCUP Statistical Brief #306. Agency for Healthcare Research and Quality, MD, USA (April 2024).
58.
Foley KA, Wang PF, Barber BL et al. Clinical and economic impact of infusion reactions in patients with colorectal cancer treated with cetuximab. Ann. Oncol. 21(7), 1455–1461 (2010).
59.
Afana M, Brinjikji W, Cloft H, Salka S. Hospitalization costs for acute myocardial infarction patients treated with percutaneous coronary intervention in the United States are substantially higher than Medicare payments. Clin. Cardiol. 38(1), 13–19 (2015).
60.
Fingar KR, Reid LD. Diabetes-related inpatient stays, 2018. HCUP Statistical Brief #279. Agency for Healthcare Research and Quality, MD, USA (July 2021).
61.
Stottlemyer BA, Tran T, Suh K, Kane-Gill SL. A systematic review of the costs of drug-associated acute kidney injury and potential cost savings with nephrotoxin stewardship prevention strategies. Clin. Pharmacol. Ther. 117(4), 989–1004 (2024).
62.
Rice JB, White AG, Johnson M et al. Healthcare resource use and cost associated with varying dosages of extended corticosteroid exposure in a US population. J. Med. Econ. 21(9), 846–852 (2018).
63.
Nazareth T, Kariburyo F, Kirkemo A et al. Patients with focal segmental glomerulosclerosis (FSGS): a claims analysis of clinical and economic outcomes. Abstract: TH-PO168. Presented at: American Society of Nephrology, Kidney Week, LA, USA (2017).
64.
Ramachandran R, Kumar V, Rathi M et al. Tacrolimus therapy in adult-onset steroid-resistant nephrotic syndrome due to a focal segmental glomerulosclerosis single-center experience. Nephrol. Dial. Transplant. 29(10), 1918–1924 (2014).
65.
Kashgary A, Sontrop JM, Li L et al. The role of plasma exchange in treating post-transplant focal segmental glomerulosclerosis: a systematic review and meta-analysis of 77 case-reports and case-series. BMC Nephrol. 17(1), 104 (2016).
66.
Klemencic Kozul T, Yudina A, Donovan C, Pinto A, Osman C. Cost-minimisation analysis of plasma exchange versus IVIg in the treatment of autoimmune neurological conditions. BMC Health Serv. Res. 22(1), 904 (2022).
67.
Lefebvre C, Hindie J, Zappitelli M, Platt RW, Filion KB. Non-steroidal anti-inflammatory drugs in chronic kidney disease: a systematic review of prescription practices and use in primary care. Clin. Kidney J. 13(1), 63–71 (2020).
68.
Lambourg E, Colvin L, Guthrie G, Walker H, Bell S. Analgesic use and associated adverse events in patients with chronic kidney disease: a systematic review and meta-analysis. Br. J. Anaesth. 128(3), 546–561 (2022).
69.
Coluzzi F, Caputi FF, Billeci D et al. Safe use of opioids in chronic kidney disease and hemodialysis patients: tips and tricks for non-pain specialists. Ther. Clin. Risk Manag. 16, 821–837 (2020).
70.
Lentine KL, Lam NN, Naik AS et al. Prescription opioid use before and after kidney transplant: implications for posttransplant outcomes. Am. J. Transplant. 18(12), 2987–2999 (2018).
71.
Bloom BS. Cost of treating arthritis and NSAID-related gastrointestinal side-effects. Aliment. Pharmacol. Ther. 2(Suppl. 1), 131–138 (1988).
72.
Fry AC, Farrington K. Management of acute renal failure. Postgrad. Med. J. 82(964), 106–116 (2006).
73.
Rha B, See I, Dunham L et al. Vital signs: health disparities in hemodialysis-associated staphylococcus aureus bloodstream infections - United States, 2017–2020. Am. J. Transplant. 23(5), 676–681 (2023).
74.
Troyanov S, Wall CA, Miller JA, Scholey JW, Cattran DC. Toronto Glomerulonephritis Registry Group. Idiopathic membranous nephropathy: definition and relevance of a partial remission. Kidney Int. 66(3), 1199–1205 (2004).
75.
Porter ME. What is value in health care? N. Engl. J. Med. 363(26), 2477–2481 (2010).
•• Offers insights into defining healthcare value, a key concept for stakeholders deciding interventions based on clinical and economic benefits.
Information & Authors
Information
Published In
Copyright
© 2026 Mallinckrodt Pharmaceuticals. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 24 September 2025
Accepted: 24 December 2025
Published online: 28 January 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Acthar Gel versus standard of care for adults with proteinuria in nephrotic syndrome due to focal segmental glomerulosclerosis: cost-per-response analysis from the US healthcare perspective. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0155
Export citation
Select the citation format you wish to export for this article or chapter.