Difference in hospital readmission among patients with atrial fibrillation undergoing ablation using nonintegrated pulsed field catheter with CARTO™ 3 versus EnSite™ electroanatomical mapping system
Publication: Journal of Comparative Effectiveness Research
Abstract
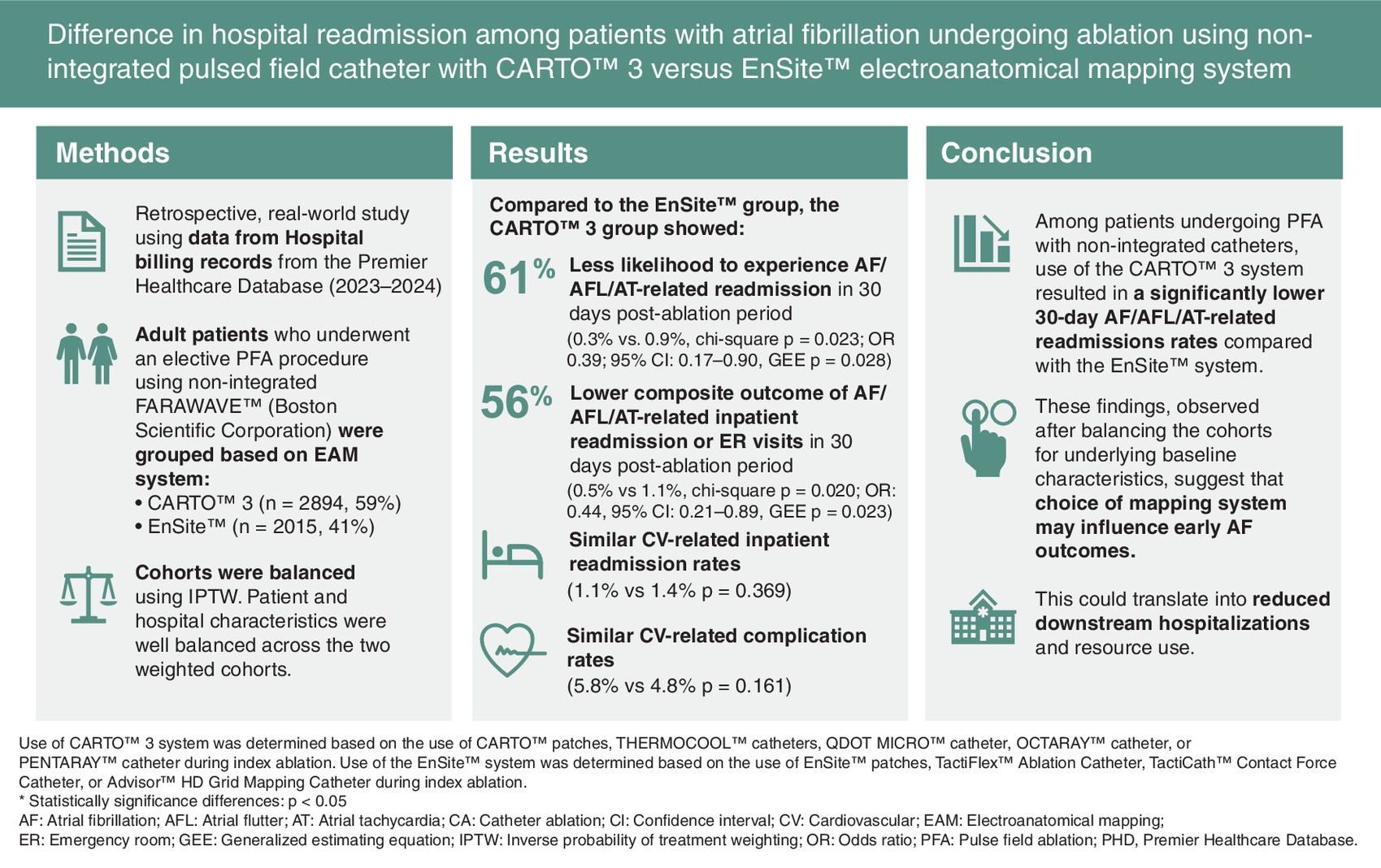
Aim: Pulsed field ablation (PFA) is a minimally thermal alternative to traditional thermal catheter ablation for atrial fibrillation (AF), with comparable efficacy and minimal risk of collateral tissue injury. Three-dimensional (3D) electroanatomical mapping systems have been adopted with nonintegrated PFA catheters to improve precision and procedural efficiency. This study compared arrhythmia-related hospital readmissions and procedure-related complications among patients with AF treated with PFA, using either the CARTO™ 3 or EnSite™ electroanatomical mapping system. Materials & methods: Patients who underwent PFA for AF using nonintegrated pulsed field catheters with either CARTO 3 or EnSite were identified from the 2023–2024 Premier Healthcare Database (PHD). The primary outcome was 30-day inpatient readmission and emergency room (ER) visit for AF/atrial flutter (AFL)/atrial tachycardia following the index PFA procedure. Secondary outcomes included 30-day cardiovascular-related readmissions and procedure-related complications. Cohorts were balanced using inverse probability of treatment weighting. Descriptive analyses and a weighted Generalized Estimating Equation (GEE) model were used to assess differences in outcomes between groups. Results: A total of 2894 patients were treated using CARTO 3 and 2015 using EnSite. After weighting, patient and hospital characteristics were well balanced across cohorts. The CARTO 3 group was significantly less likely to experience AF/AFL/atrial tachycardia-related readmissions (0.3% vs 0.9%, chi-square p = 0.023; odds ratio [OR], 0.39; 95% CI, 0.17–0.90, GEE p = 0.028) and a composite outcome of AF/AFL/atrial tachycardia-related inpatient readmission or ER visits (0.5% vs 1.1%, chi-square p = 0.020; OR: 0.44, 95% CI: 0.21–0.89, GEE p = 0.023) within 30 days of PFA procedure than the EnSite group. No differences were observed in cardiovascular-related readmission or complications. Conclusion: In this retrospective, real-world study, patients with AF who underwent PFA using CARTO 3 had lower 30-day AF/AFL/atrial tachycardia-related readmissions rates than those treated with EnSite suggesting that choice of mapping system may influence early AF outcomes and could translate into reduced downstream hospitalizations and resource use.
Plain language summary
What is this article about?
Atrial fibrillation (AF) is a common heart rhythm disorder that can be treated with a procedure called pulsed field ablation (PFA), which uses electrical pulses to target and destroy heart muscle cells responsible for the abnormal rhythm. During the procedure, electroanatomical mapping systems help guide the treatment by creating a detailed map of the heart. This study compared hospital readmission rates and complications after PFA procedures performed using two different electroanatomical mapping systems: CARTO™ 3 and EnSite™.
What were the results?
This study analyzed the data of 4909 patients with AF treated with PFA in 2023–2024. Patients treated using the CARTO 3 system were 56% less likely to be readmitted to the hospital or emergency room within 30 days for AF, atrial flutter, or atrial tachycardia compared with those treated using the EnSite system. Both groups had similar rates of cardiovascular-related hospital readmissions and procedure-related complications.
What do the results mean?
These findings suggest that the choice of mapping system used to guide PFA may influence early heart rhythm-related hospital readmissions. The CARTO 3 system may offer an advantage in preventing recurrence of arrhythmia after the procedure.
Graphical abstract
Atrial fibrillation (AF) is the most common type of cardiac arrhythmia, affecting an estimated 6 million individuals in the US and is expected to reach 16 million by 2050 [1]. Approximately half a million hospitalizations are related to AF annually, imposing a significant burden on patients, providers, and payers [2]. Catheter ablation (CA) is an established and effective treatment option for patients with AF, and has been shown to reduce AF burden (percentage of time spent in AF, number of episodes, duration of episodes or density), improve quality of life and decrease cardiovascular (CV) hospitalizations and death [3–6].
The recent introduction of pulsed field ablation (PFA), which utilizes ultra-short high voltage pulses to create irreversible electroporation and necrosis in cardiac cells, offers an alternative to traditional radiofrequency (RF) or cryoenergy ablation [7–10]. This minimally thermal approach reduces the risk of damage to neighboring structures, a complication that may occur with conventional thermal CA techniques [11].
Three dimensional electroanatomical mapping (EAM) systems have been adopted with nonintegrated (i.e., catheters that do not have in-built navigation capabilities) PFA catheter for AF ablation to improve efficiency. Early clinical evidence has indicated that 3D mapping combined with PFA ablation provides a more accurate visualization of the anatomical location and positioning of PFA catheter, leading to minimal collateral tissue damage [12–14]. Additionally, EAM allows real-time visualization of the devices as they are navigated along the planned path, to minimize the risk of inadvertent injury and lower the likelihood of procedural complications [12].
CARTO™ 3 (Biosense Webster, Inc., CA, USA) and EnSite™ (Abbott, MN, USA) are the most commonly used 3D EAM systems for CA, and both are compatible with nonintegrated PFA catheters. Each system includes software modules that provide real-time feedback on the anatomical location and extent of energy delivery during ablation. Although there have been some studies conducted in the radiofrequency (RF) CA era [15,16], data are limited regarding direct comparisons of the efficacy of the CARTO 3 and EnSite systems during AF PFA procedure.
Given the increasing use of PFA in AF treatment, it is important to assess the differential in patient outcomes associated with the choice of EAM system. In this study, we compared outcomes in patients with AF who underwent CA using nonintegrated PFA guided by either the CARTO 3 or the EnSite EAM system. To the best of our knowledge, this is the first study to examine if patient outcome differences exist based on the underlying EAM system used during a PFA procedure.
Materials & methods
Data source
This retrospective cohort study used hospital billing records from the 2023–2024 Premier Healthcare Database (PHD), which contains complete clinical coding, hospital cost, and patient billing data from more than 1000 hospitals throughout the US. Premier collects data from voluntarily participating hospitals in its healthcare alliance. Although the database excludes federally funded hospitals (e.g., Veterans Affairs), the hospitals included are nationwide and reflective of different bed size, geographic region, location (urban/rural) and teaching hospital status. The database contains a date-stamped log of all billed items by cost-accounting department including medications; laboratory, diagnostic and therapeutic services; and primary and secondary diagnoses for each patient’s hospitalization. Identifier-linked enrollment files provide demographic and payer information. Detailed service level information for each hospital day is recorded; this includes details on medication and devices received. Institutional Review Board (IRB) oversight was not required for our analysis using the PHD, as per Title 45 Code of Federal Regulations (45 CFR 46.101(b)(4))) (https://www.govinfo.gov/content/pkg/CFR-2011-title45-vol1/pdf/CFR-2011-title45-vol1.pdf). No individuals were identified in the aggregated data.
Study design
Patients ≥18 years of age who underwent an elective PFA procedure using nonintegrated FARAWAVE™ (Boston Scientific Corporation, MA, USA) pulsed field catheter, with a primary diagnosis of AF (International Classification of Diseases, Tenth Revision, Clinical Modification [ICD-10-CM] codes: I48.0, I48.1, I48.2, and I48.91) were included. The first observed ablation meeting these criteria during the year 2024 was designated as the ‘index ablation’. Patients were included if they underwent their index ablation with providers (hospitals) that contributed inpatient data to the Premier database during the 6-month pre-index and the 1-month post-index periods. Patients were then classified into two cohorts based on the underlying EAM system used during the PFA procedure: CARTO 3 or EnSite EAM system cohort. The use of CARTO 3 system was determined based on the use of CARTO patches, THERMOCOOL™ catheters, QDOT MICRO™ catheter, OCTARAY™ catheter, or PENTARAY™ catheter during index ablation. The use of the EnSite system was determined based on the use of EnSite patches, TactiFlex catheter, Tacticath catheter, or Advisor HD Grid catheter during index ablation.
Patients who had undergone a CA procedure with primary or secondary diagnosis of AF, surgical ablation, valvular procedure, or left atrial appendage occlusion in the 6-month pre-index ablation period were excluded. Patients who had unknown baseline characteristics information (e.g., race) were also excluded from the study.
Study variables & outcomes
The primary independent variable was CARTO 3 versus EnSite EAM system, based on the underlying system that was used during the index ablation procedure. The following covariates were included in the study: patient demographic and clinical characteristics, procedural characteristics and hospital characteristics. Patient demographics included age, sex, race/ethnicity and payer type. Age was recorded in integer years as of the day of the index ablation, and was grouped into the following categories: 18–49 years, 50–59 years, 60–69 years, 70–79 years, and 80 years and above. Sex was categorized as either male or female. Race/ethnicity was categorized as White or non-White. Payer type was either Commercial, Medicare, Medicaid or Other. Procedural characteristics including ablation setting (inpatient or outpatient) and the use of intracardiac echocardiography (ICE) during index PFA were also assessed.
Patient clinical characteristics included the Elixhauser comorbidity index (0–1, 2–3, 4+), the CHA2DS2-VASc score (0–1, 2–3, 4+), AF subtype (paroxysmal, persistent, chronic and unspecified), history of electrical cardioversion and AF-related inpatient admission in the 6 months pre-index ablation period, sleep apnea and obesity.
Hospital and provider characteristics included hospital size (0–299, 300–499, and 500+ beds), geographic location (Midwest, South, Northeast and West), hospital type (teaching, or nonteaching) and ablation volume (number of admissions with ablation in the 6 months pre-index).
The primary outcome of interest was AF/AFL/atrial tachycardia-related inpatient readmissions (with a primary diagnosis of AF, AFL or atrial tachycardia), AF/AFL/atrial tachycardia-related emergency room (ER) visit, and a composite of these two outcomes in the 30-day post-index ablation period. We chose 30-day outcomes due to the recent adoption of PFA, which limited our ability to assess long-term outcomes (e.g., 12-month AF recurrence). It should be noted though that early AF recurrence after ablation has shown to be predictive of long-term AF recurrence [17–19]. The secondary outcomes of interest were 30-day post-index CV-related inpatient readmissions (i.e., inpatient admission with a primary diagnosis of CV conditions [conditions and corresponding codes have been listed in Supplementary Table 1]), and 30-day procedure-related complications (with a secondary diagnosis of the events during the index admission but not present at the time of admission, or with an admission [any setting] post-index discharge but within 30 days of index admission with a primary diagnosis). The procedure-related complications included laryngospasm, mandibular joint dislocation, acute coronary syndrome, ischemic stroke, hemorrhagic stroke, thromboembolism, transient ischemic attack, phrenic nerve damage, pericarditis, bleeding, blood transfusion, atrio-esophageal fistula, severe pulmonary vein stenosis requiring intervention, vagal nerve injury, vascular access complication requiring repair and cardiac tamponade/perforation, hematuria, organ failure, anemia, acute kidney injury, acute heart failure, pulmonary edema and vasovagal response.
Data analysis
Descriptive statistics are reported for all study covariates. Mean and standard deviation are reported for continuous variables/outcomes, and proportions are reported for categorical variables. To minimize the confounding effect of potential confounders, the inverse probability of treatment weighting (IPTW) approach was used [20]. The IPTW method allows for balancing patients covariates (i.e., patient demographics, patient clinical characteristics, procedural characteristics and hospital characteristics), resulting in a pseudo-population with a comparable group of patients who had CA using the CARTO 3 versus the EnSite system [16]. Each patient was assigned a weight by using the IPTW technique along with an estimation of the average treatment effect [20]. Stabilized IPTW weights were calculated for each patient and applied in the analysis. Standardized mean differences (SMDs) were used to assess if the distribution of these covariates were balanced after weighting, with SMD >0.10 or <-0.10 considered as imbalanced distribution. Bivariate analyses were performed for all study outcomes.
For multivariable analyses, weighted generalized estimated equation (GEE) model with logit link and binomial distribution function was used to examine differential in outcomes among study groups. GEE analyses adjusted for hospital clustering effect for the patients who were treated in the same hospital post-weighting. Sensitivity analyses were performed among hospitals with top five volumes of CA sites dropped and among patients with paroxysmal and persistent AF.
Results
Patient & hospital characteristics
A total of 4909 patients were included in this study, with 2894 (59.0%) undergoing the PFA procedure using the CARTO 3 system and 2015 (41.0%) using the EnSite EAM system. Patient attrition is illustrated in Figure 1.
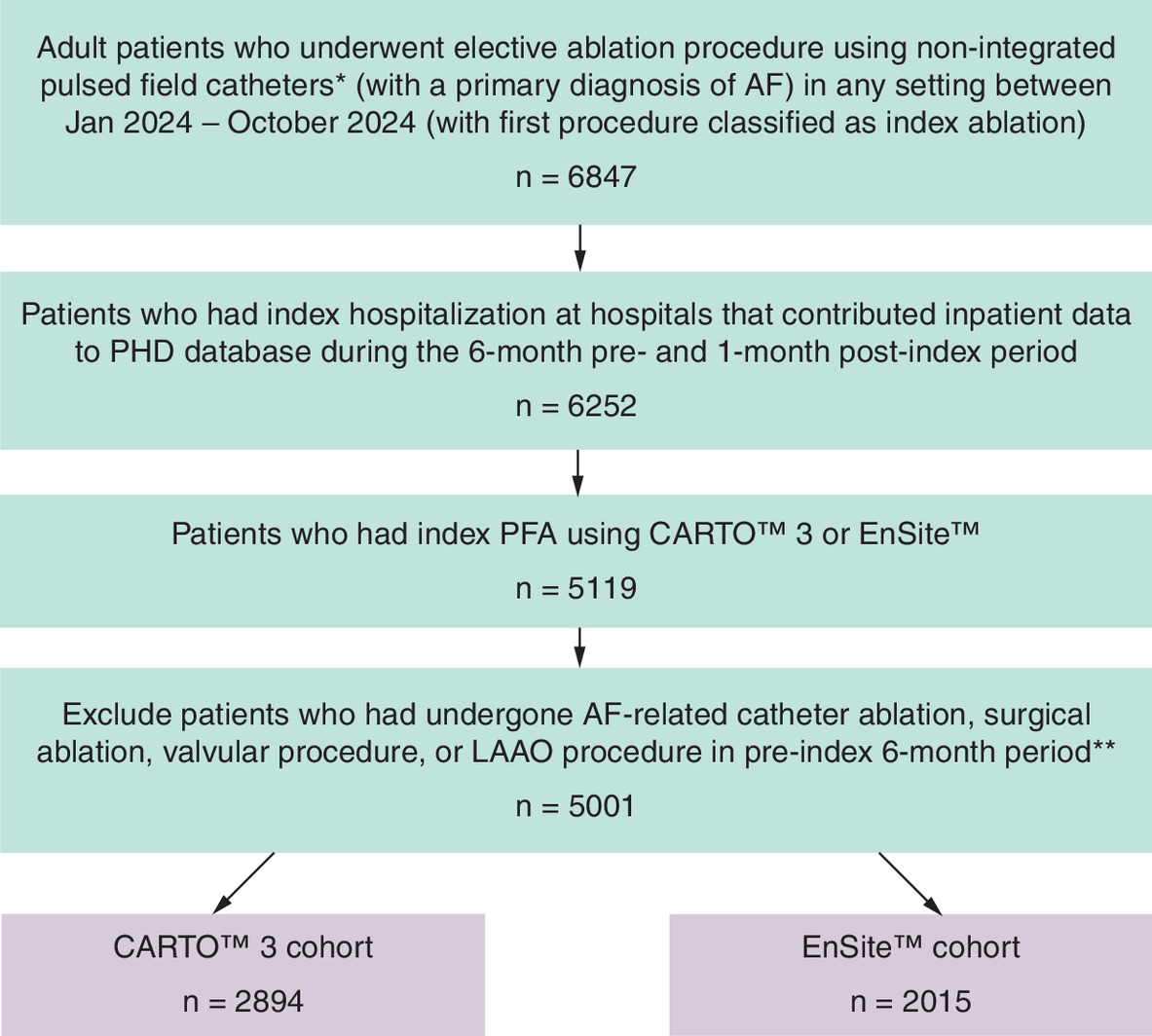
Figure 1. Patient attrition.
*PFA procedures were identified based on the use of FARAWAVE™ PFA catheter.
**92 patients were further removed due to lack of information in race.
AF: Atrial fibrillation; LAAO: Left atrial appendage occlusion; PHD: Premier Healthcare Database; PFA: Pulse field ablation.
Prior to applying the IPTW method, covariates including age (absolute SMD [aSMD] = 0.101), race (CARTO 3: 88.6% White, 11.4% non-White; EnSite: 92.3% White, 7.7% non-White; aSMD = 0.126), AF type during index (CARTO 3: 52.4% paroxysmal, 41.4% persistent; EnSite: 57.8% paroxysmal, 35.7% persistent; aSMD = 0.117), electrical cardioversion (CARTO 3: 5.4%; EnSite: 3.0%; aSMD = 0.122) and ICE use (CARTO 3: 94.4%%; EnSite: 99.0%; aSMD = 0.255) during index ablation were unbalanced among the study cohorts (Table 1). A larger percentage of patients in the CARTO 3 group were treated in teaching hospitals compared with the EnSite group (CARTO 3: 61.9%, EnSite: 53.1%; aSMD = 0.179). Patients in the CARTO 3 cohort had their index procedure in hospitals with higher mean ablation procedure volume as compared with the EnSite group (CARTO 3: 267.9, EnSite: 238.3, aSMD = 0.244). After applying the IPTW method, both groups were well balanced and the SMD for all covariates was within the -0.10–0.10 range (Table 1).
| Pre-weighted cohort | Post-weighted cohort | |||||
|---|---|---|---|---|---|---|
| CARTO 3 (n = 2894) | EnSite (n = 2015) | aSMD | CARTO 3, % | EnSite, % | aSMD | |
| n (%) | n (%) | |||||
| Age, years | 0.101 | 0.030 | ||||
| Mean (SD) | 67.7 (10.2) | 68.6 (10.0) | 68.1 (10.1) | 68.1 (10.3) | ||
| 18 to 49 | 155 (5.4%) | 83 (4.1%) | 4.8% | 5.4% | ||
| 50 to 59 | 376 (13.0%) | 256 (12.7%) | 12.6% | 12.2% | ||
| 60 to 69 | 983 (34.0%) | 656 (32.6%) | 33.6% | 33.5% | ||
| 70 to 79 | 1,099 (38.0%) | 771 (38.3%) | 37.9% | 37.9% | ||
| 80+ | 281 (9.6%) | 249 (12.3%) | 11.1% | 11.0% | ||
| Sex | 0.039 | 0.011 | ||||
| Male | 1,801 (62.2%) | 1,292 (64.1%) | 63.2% | 62.7% | ||
| Female | 1,093 (37.8%) | 723 (35.9%) | 36.8% | 37.3% | ||
| Race | 0.126 | 0.005 | ||||
| White | 2,563 (88.6%) | 1,859 (92.3%) | 90.0% | 90.1% | ||
| Non-White | 331 (11.4%) | 156 (7.7%) | 10.0% | 9.9% | ||
| Payor type | 0.059 | 0.015 | ||||
| Medicare | 1,819 (62.8%) | 1,291 (64.1%) | 63.5% | 62.8% | ||
| Commercial | 943 (32.6%) | 655 (32.5%) | 32.3% | 33.0% | ||
| Medicaid/other | 132 (4.6%) | 69 (3.4%) | 4.2% | 4.2% | ||
| AF type during index | 0.117 | 0.022 | ||||
| Paroxysmal | 1,517 (52.4%) | 1,164 (57.8%) | 54.1% | 53.0% | ||
| Persistent | 1,197 (41.4%) | 719 (35.7%) | 39.6% | 40.7% | ||
| Others | 180 (6.2%) | 132 (6.5%) | 6.3% | 6.3% | ||
| Electrical cardioversion | 157 (5.4%) | 60 (3.0%) | 0.122 | 4.2% | 4.3% | 0.004 |
| AF-related hospitalization | 407 (14.1%) | 227 (11.3%) | 0.084 | 12.7% | 13.3% | 0.016 |
| Index procedure setting | 0.026 | 0.012 | ||||
| Outpatient | 2,787 (96.3%) | 1,950 (96.8%) | 66.5% | 66.3% | ||
| Inpatient | 107 (3.7%) | 65 (3.2%) | 3.5% | 3.7% | ||
| ICE use during index procedure | 2,733 (94.4%) | 1,994 (99.0%) | 0.255 | 96.3% | 95.0% | 0.065 |
| Elixhauser score | 0.079 | 0.035 | ||||
| 0–1 | 583 (20.1%) | 373 (18.5%) | 18.9% | 17.8% | ||
| 2–3 | 1,354 (46.8%) | 1,022 (50.7%) | 48.7% | 48.5% | ||
| 4 and above | 957 (33.1%) | 620 (30.8%) | 32.4% | 33.7% | ||
| CHA2DS2-VASc score | 0.036 | 0.025 | ||||
| 0–1 | 782 (27.0%) | 513 (25.5%) | 25.8% | 26.1% | ||
| 2–3 | 1,453 (50.2%) | 1,029 (51.1%) | 50.7% | 49.6% | ||
| 4 and above | 659 (22.8%) | 473 (23.4%) | 23.5% | 24.3% | ||
| Obesity | 465 (16.1%) | 315 (15.6%) | 0.012 | 16.1% | 15.8% | 0.008 |
| Sleep apnea | 767 (26.5%) | 594 (29.5%) | 0.066 | 28.3% | 27.5% | 0.017 |
| Hospital bed size | 0.661 | 0.010 | ||||
| <300 | 330 (11.4%) | 522 (25.9%) | 16.9% | 17.3% | ||
| 300–499 | 626 (21.6%) | 771 (38.3%) | 29.3% | 28.9% | ||
| 500+ | 1,938 (67.0%) | 722 (35.8%) | 53.8% | 53.8% | ||
| Hospital region | 0.238 | 0.049 | ||||
| South | 1,509 (52.1%) | 910 (45.2%) | 48.5% | 50.9% | ||
| Midwest | 868 (30.0%) | 581 (28.8%) | 29.7% | 28.6% | ||
| West | 348 (12.0%) | 415 (20.6%) | 16.4% | 15.6% | ||
| Northeast | 169 (5.9%) | 109 (5.4%) | 5.4% | 4.9% | ||
| Hospital type | 0.179 | 0.016 | ||||
| Teaching | 1,792 (61.9%) | 1,070 (53.1%) | 58.5% | 59.3% | ||
| Nonteaching | 1,102 (38.1%) | 945 (46.9%) | 41.5% | 40.7% | ||
| Ablation volume (mean, SD) | 267.9 (134.1) | 238.3 (107.8) | 0.244 | 258.7 (132.4) | 255.4 (112.2) | 0.026 |
Bold aSMD values represents significant difference as they are outside the -0.1 to 0.1 range.
AF: Atrial fibrillation; aSMD: Absolute standardized mean difference; ICE: Intracardiac echocardiography; SD: Standard deviation.
Outcomes
In the weighted sample, patients who underwent PFA with CARTO 3 were observed to have significantly lower rate of AF/AFL/atrial tachycardia-related inpatient readmissions (0.34% vs 0.86%, chi-square p = 0.023) and a significantly lower rate of AF/AFL/atrial tachycardia-related inpatient readmissions or ER visits (0.47% vs 1.08%, p = 0.020) in the 30 days post-ablation period as compared with those who underwent PFA with the EnSite system. No significant differences in the rate of AF/AFL/atrial tachycardia-related ER visits (0.14% vs 0.21%, p = 0.482), CV-related inpatient readmissions (1.07% vs 1.37%, p = 0.369) and procedure-related complications (5.76% vs 4.76%, p = 0.161) were observed among patients who underwent PFA with CARTO 3 versus EnSite system (Table 2). The proportion of patients in each cohort who experienced complications within 30 days in the unweighted sample is shown in Supplementary Table 2.
| Outcomes in 30 days post-index | Unweighted sample | Weighted sample | |||||
|---|---|---|---|---|---|---|---|
| CARTO 3, % n = 2894 | EnSite, % n = 2015 | CARTO 3, %† n = 2906.7 | EnSite, %† n = 2007.3 | Absolute risk difference | Needed to treat, n | Chi-square test, p-value | |
| Primary outcomes | |||||||
| AF/AFL/atrial tachycardia-related inpatient readmission‡ | 11 (0.38%) | 14 (0.69%) | 9.8 (0.34%) | 17.3 (0.86%) | -0.52% (-1.06%, 0.01%) | 192 | 0.023 |
| AF/AFL/atrial tachycardia-related ER visit‡ | 4 (0.14%) | 6 (0.30%) | 4.0 (0.14%) | 4.3 (0.21%) | -0.08% (-0.30%, 0.14%) | 1,250 | 0.482 |
| Composite of AF/AFL/atrial tachycardia-related inpatient readmission or ER visit | 15 (0.52%) | 20 (0.99%) | 13.8 (0.47%) | 21.6 (1.08%) | -0.60% (-1.18%, -0.02%) | 167 | 0.020 |
| Secondary outcomes | |||||||
| CV-related inpatient readmission | 33 (1.14%) | 27 (1.34%) | 31.1 (1.07%) | 27.6 (1.37%) | -0.30% (-0.99%, 0.38%) | 33 | 0.369 |
| Procedure-related complications | 169 (5.84%) | 98 (4.86%) | 167.4 (5.76%) | 95.5 (4.76%) | 1.00% (-0.37%, 2.37%) | 100 | 0.161 |
†
Due to weighting, the reported patient count for the cohort may not be an integer.
‡
AF/AFL/atrial tachycardia-related inpatient readmission/ER visit was defined as hospitalization/ER visit with a primary diagnosis of AF, AFL or atrial tachycardia.
Bold p-values represent significant findings.
AF: Atrial fibrillation; AFL: Atrial flutter; CV: Cardiovascular, ER: Emergency room; GEE: Generalized estimating equation.
Results from GEE regression analysis demonstrated that patients who underwent PFA with CARTO 3 had 61% lower risk of AF/AFL/atrial tachycardia-related inpatient readmissions (odds ratio [OR] 0.39; 95% confidence interval [CI] 0.17–0.90) and 56% lower risk of composite of AF/AFL/atrial tachycardia-related inpatient readmission or ER visit (OR: 0.44; 95% CI: 0.21–0.89) in the 30-day post-procedure period than those who had PFA with EnSite system. No significant differences were observed for AF/AFL/atrial tachycardia-related ER visit, cardiovascular-related inpatient readmissions or procedure-related complications from regression analysis (Table 3).
| Outcomes in 30 days post-index | Odds ratio | 95% Confidence interval | GEE regression model, p-value |
|---|---|---|---|
| Primary outcomes | |||
| AF/AFL/atrial tachycardia-related inpatient readmission† | 0.39 | 0.17–0.90 | 0.028 |
| AF/AFL/atrial tachycardia-related ER visit† | 0.63 | 0.17–2.29 | 0.480 |
| Composite of AF/AFL/atrial tachycardia-related inpatient readmission or ER visit | 0.44 | 0.21–0.89 | 0.023 |
| Secondary outcomes | |||
| CV-related inpatient readmission | 0.78 | 0.45–1.35 | 0.380 |
| Procedure-related complications | 1.22 | 0.92–1.62 | 0.162 |
†
AF/AFL/atrial tachycardia-related inpatient readmission/ER visit was defined as hospitalization/ER visit with a primary diagnosis of AF, AFL or atrial tachycardia.
Bold p-values represent significant findings.
GEE: Generalized estimating equation; AF: Atrial fibrillation; AFL: Atrial flutter; CV: Cardiovascular.
Sensitivity analyses for hospitals with top five CA columns sites dropped and among patients with paroxysmal and persistent AF revealed consistent findings for the primary outcomes (Supplementary Tables 3 & 4).
Discussion
In this retrospective cohort study, patients with AF who underwent a CA procedure with nonintegrated PFA catheter using the CARTO 3 EAM system were 61% less likely to have AF/AFL/atrial tachycardia-related inpatient readmission and 56% less likely to have AF/AFL/atrial tachycardia-related inpatient readmission or ER visit in the 30 days following the procedure, compared with patients treated with the EnSite EAM system. In the 30-day period post-procedure, neither CV-related inpatient readmissions nor procedure-related complications were significantly different between the two groups. As PFA adoption is recent, we could not compare long-term recurrence among patients with PFA treated with CARTO 3 versus EnSite in our study; although prior studies have suggested early recurrence post-ablation to be predictive of long-term recurrence [17–19]. In particular, a recent study focusing on patients who underwent PFA-pulmonary vein isolation for AF found that over half of patients who experienced early recurrences of atrial tachyarrhythmia had a late recurrence of arrhythmia; the early recurrence of atrial tachyarrhythmia is a significant predictor of late recurrence [17]. As seen in our study, when considering the use of nonintegrated PFA catheters, the choice of the EAM system could have implications on patient outcomes, as well as downstream hospital resource burden and cost associated with repeat admissions.
EAM systems are now central to AF ablation workflows [21,22]. They facilitate 3D reconstruction of cardiac anatomy, catheter navigation and EAM, allowing the precise localization of the regions responsible for the abnormal electrical activity. By generating activation maps, color-coded reconstructions of electrical activation sequences across the cardiac surface, EAMs help identify precise targets for ablation. This guidance significantly reduces or eliminates the need for fluoroscopy, minimizing radiation exposure to both patients and providers. The clinical use of EAM systems has been associated with improved procedural outcomes, including reduced fluoroscopy, enhanced safety and lower rates of arrhythmia recurrence [22,23]. Additional benefits include shorter procedure time and improved efficacy by enabling better interpretation of complex arrhythmia mechanisms, more accurate targeting of ablation sites and continuous visualization of catheter [22–24]. The ability to generate high-resolution maps and integrate with advanced imaging modalities further refines anatomical understanding and guides effective lesion delivery, leading to improved overall success in treating a wide range of cardiac arrhythmias [22].
Both CARTO 3 and EnSite systems allow for real-time visualization and tailored ablation strategies in complex arrhythmia cases, contributing to improved efficacy and safety of these procedures [22]. The CARTO 3 system combines magnetic field and impedance-based localization with respiratory gating and high spatial accuracy (<1 mm), while EnSite primarily uses impedance-based tracking and incorporates optional magnetic sensors to improve mapping accuracy. Additionally, there are differences in the software and modules used with each system providing information and feedback on the lesion formed during the ablation procedure. First, the CARTO 3 system enables better positioning of the ablation catheter as well as understanding of where the ablations were performed including enhanced accuracy of the anatomy as well as position and visualization of the catheters. The EnSite system enables zero-exchange workflow, but only when working in impedance mode, which could potentially influence the accuracy of the map and visualizations. Second, the CARTOSOUND™ FAM Module uses artificial intelligence (AI) based on a deep learning (DL) algorithm which automatically constructs detailed three-dimensional left atrial anatomy using a series of ultrasound input [25]. In their assessment of the CARTOSOUND™ FAM Module DL algorithm among 28 patients undergoing AF ablation, Di Biase et al. reported that the algorithm demonstrated considerable accuracy compared with the gold standard computed tomography. This accuracy contributed to a more efficient workflow for anatomical map creation and its integration into the CARTO 3 system for catheter positioning and contact assessment [25]. Schwartz et al. compared the left atrial reconstruction of model-based FAM (m-FAM) of CARTO 3 system with cardiac computed tomography angiography of the same patient left atrium as the gold standard [26]. The authors reported 100% pulmonary vein isolation, with no significant complications. The left atrial reconstruction guided by CARTO 3 m-FAM was reported to be accurate in all patients irrespective of the mapping catheter, and resembled closely with cardiac computed tomography angiography. Machine data from the two mapping systems were not available in our study. As such, we could not delineate the impact of such features on study outcomes. Further research is needed to better understand the impact of different features among the two mapping systems and their potential role in outcomes differential.
Limitations
Some limitations should be noted for this study. Device identification was based on a search and text mining strategy using device names which could have resulted in misclassification. Unmeasured confounders, such as ablation technique, ablation on non-pulmonary vein, physician experience and other ablation-related devices (e.g., high-density mapping catheter), could have influenced study results. We did control for hospital ablation volume, which may serve as a reasonable proxy for physician experience. In PHD, readmissions are only captured if they occur in the same hospital; while we assumed most patients would return to the same facility within 30 days, this limitation could have led to an underestimation of readmission rates. However, it should be noted that this limitation is likely to lead to nondifferential bias so the treatment effect should be consistent. Finally, as the study population was drawn from a subset of hospitals included in the PHD, the findings may not be generalizable to all US hospitals or patients undergoing AF ablation using the underlying study devices.
Conclusion
Among patients undergoing PFA with nonintegrated catheters, use of the CARTO 3 system resulted in a significantly lower rate of arrhythmia-related readmissions compared with the EnSite system. These findings, observed after balancing the cohorts for underlying baseline characteristics, suggest that mapping system differences may influence early AF outcomes and should be considered in procedural planning for AF ablation. Given the link between early AF readmission and long-term reoccurrence which has been find among those who underwent PFA, future studies should evaluate whether the early advantages with CARTO 3 translate into durable clinical and meaningful economic benefits.
Summary points
•
Pulsed field ablation (PFA) has emerged as a promising minimally thermal alternative to conventional ablation techniques for atrial fibrillation (AF). Integration of electroanatomical mapping systems, such as CARTO™ 3 and EnSite™, with PFA may enhance procedural efficiency and safety, but comparative data on their performance in this setting are limited.
•
This retrospective cohort study investigated 30-day post-procedure AF/AFL/atrial tachycardia-related inpatient readmissions, 30-day CV-related inpatient readmissions and 30-complications in patients with AF who underwent ablation with nonintegrated pulsed field catheters with the CARTO 3 versus EnSite electroanatomical mapping systems.
•
Data from 4909 patients with AF and treated with PFA using CARTO 3 versus EnSite between 2023–2024 were identified from the Premier Healthcare Database.
•
Inverse probability of treatment weighting was used to balance covariates between the CARTO 3 and EnSite cohorts.
•
Patients who underwent PFA using CARTO 3 were 61% less likely to have AF/AFL/atrial tachycardia-related inpatient readmission and 56% less likely to have AF/AFL/atrial tachycardia-related inpatient readmission or ER visit in the 30 days post-procedure period versus those treated using the EnSite electroanatomical mapping system.
•
No significant differences in 30-day CV-related inpatient readmissions and 30-day complications were observed between the CARTO 3 cohort and EnSite cohort.
Author contributions
All authors were responsible for study conception and design; RK and YR were responsible for acquisition of data; RK and YR were responsible for data analysis. All authors contributed to draft review and revision of the manuscript.
Financial disclosure
This study was funded by Johnson & Johnson.
Competing interests disclosure
R Khanna, M Iglesias and Y Rong are employed by Johnson & Johnson. AI Costea is a speaker for Biosense Webster, Inc. and Biotronik. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
The authors acknowledge Superior Medical Experts for drafting and editorial assistance.
Ethical conduct of research
The authors state that the use of Premier Healthcare Database was reviewed by the New England Institutional Review Board and was determined to be exempt from broad IRB approval, as this study does not involve human subjects' research. Confidentiality of data subject records were maintained at all time. All study reports contained aggregate data only and did not identify individual data subjects or physicians.
Open access
This work is licensed under the CreativeCommons Attribution 4.0 License. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 121.29 KB
References
1.
Go AS, Hylek EM, Phillips KA et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 285(18), 2370–2375 (2001).
2.
Benjamin EJ, Muntner P, Alonso A et al. Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation 139(10), e56–e528 (2019).
3.
Asad ZUA, Yousif A, Khan MS, Al-Khatib SM, Stavrakis S. Catheter ablation versus medical therapy for atrial fibrillation: a systematic review and meta-analysis of randomized controlled trials. Circ. Arrhythm. Electrophysiol. 12(9), e007414 (2019).
4.
Mark DB, Anstrom KJ, Sheng S et al. Effect of catheter ablation vs medical therapy on quality of life among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA 321(13), 1275–1285 (2019).
5.
Marrouche NF, Brachmann J, Andresen D et al. Catheter ablation for atrial fibrillation with heart failure. N. Engl. J. Med. 378(5), 417–427 (2018).
6.
Packer DL, Piccini JP, Monahan KH et al. Ablation versus drug therapy for atrial fibrillation in heart failure: results from the CABANA trial. Circulation 143(14), 1377–1390 (2021).
7.
Batista Napotnik T, Polajžer T, Miklavčič D. Cell death due to electroporation - a review. Bioelectrochemistry 141, 107871 (2021).
8.
Bradley CJ, Haines DE. Pulsed field ablation for pulmonary vein isolation in the treatment of atrial fibrillation. J. Cardiovasc. Electrophysiol. 31(8), 2136–2147 (2020).
9.
Kotnik T, Rems L, Tarek M, Miklavčič D. Membrane electroporation and electropermeabilization: mechanisms and models. Annu. Rev. Biophys. 48, 63–91 (2019).
10.
Verma A, Haines DE, Boersma LV et al. Pulsed field ablation for the treatment of atrial fibrillation: PULSED AF pivotal trial. Circulation 147(19), 1422–1432 (2023).
11.
Muthalaly RG, John RM, Schaeffer B et al. Temporal trends in safety and complication rates of catheter ablation for atrial fibrillation. J. Cardiovasc. Electrophysiol. 29(6), 854–860 (2018).
12.
Falasca Zamponi A, Olson J, Scheel S, Englund A, Scorza R, Tabrizi F. Procedural efficiency is enhanced combining the pentaspline pulsed field ablation catheter with three-dimensional electroanatomical mapping system for pulmonary vein isolation. J. Interv. Card. Electrophysiol. 67(9), 1993–2001 (2024).
13.
Kueffer T, Seiler J, Madaffari A et al. Pulsed-field ablation for the treatment of left atrial reentry tachycardia. J. Interv. Card. Electrophysiol. 66(6), 1431–1440 (2023).
14.
Mittal A, Hong K, Fitzpatrick N et al. A hybrid approach using pulse field ablation and three-dimensional mapping in atrial fibrillation ablation: a relatively early worldwide experience. Heart 108(Suppl. 3), A4–A6 (2022).
15.
Costea AI, Khanna R, Iglesias M, Rong Y. Hospital readmissions following catheter ablation for atrial fibrillation with THERMOCOOL™ STSF/THERMOCOOL™ ST catheter with CARTO™ 3 system versus TactiCath™ catheter with EnSite™ system. J. Comp. Eff. Res. 14(1), e240075 (2025).
16.
Arai H, Miyazaki S, Nitta J et al. Acute procedural safety of the latest radiofrequency ablation catheters in atrial fibrillation ablation: data from a large prospective ablation registry. J. Cardiovasc. Electrophysiol. 35(11), 2109–2118 (2024).
17.
Plank K, Bordignon S, Urbanek L et al. Early recurrences predict late therapy failure after pulsed field ablation of atrial fibrillation. J. Cardiovasc. Electrophysiol. 34(12), 2425–2433 (2023).
18.
Li Z, Wang S, Hidru TH et al. Long atrial fibrillation duration and early recurrence are reliable predictors of late recurrence after radiofrequency catheter ablation. Front Cardiovasc. Med. 9, 864417 (2022).
19.
Kim YG, Boo KY, Choi JI et al. Early recurrence is reliable predictor of late recurrence after radiofrequency catheter ablation of atrial fibrillation. JACC Clin. Electrophysiol. 7(3), 343–351 (2021).
20.
Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 34(28), 3661–3679 (2015).
21.
Bazoukis G, Elkholey K, Stavrakis S, Heist EK, Armoundas AA. Efficacy of commonly used 3D mapping systems in acute success rates of catheter ablation procedures. Heart Int. 18(1), 9–25 (2024).
22.
Kim YH, Chen SA, Ernst S et al. 2019 APHRS expert consensus statement on three-dimensional mapping systems for tachycardia developed in collaboration with HRS, EHRA, and LAHRS. J. Arrhythm. 36(2), 215–270 (2020).
23.
Hofer D, Steffel J, Duru F et al. Feasibility, efficiency, and safety of zero-fluoroscopy catheter interventions for right-sided cardiac arrhythmias using only electroanatomic mapping. Cardiology 147(5–6), 547–556 (2022).
24.
Obeng-Gyimah E, Nazarian S. Advancements in imaging for atrial fibrillation ablation: is there a potential to improve procedural outcomes? J. Innov. Card. Rhythm. Manag. 11(7), 4172–4178 (2020).
25.
Di Biase L, Zou F, Lin AN et al. Feasibility of three-dimensional artificial intelligence algorithm integration with intracardiac echocardiography for left atrial imaging during atrial fibrillation catheter ablation. Europace 25(9), euad211 (2023).
26.
Schwartz AL, Chorin E, Mann T et al. Reconstruction of the left atrium for atrial fibrillation ablation using the machine learning CARTO 3 m-FAM software. J. Interv. Cardi. Electrophysiol. 64(1), 39–47 (2022).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Creative Commons Attribution 4.0 License
History
Received: 19 September 2025
Accepted: 4 December 2025
Published online: 8 January 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Difference in hospital readmission among patients with atrial fibrillation undergoing ablation using nonintegrated pulsed field catheter with CARTO™ 3 versus EnSite™ electroanatomical mapping system. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0151
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Benjamin J. Behers, Christoph A. Stephenson-Moe, Sammy Shihadeh, Tonya S. King, Omar Hozayen, Joseph Hozayen, Maria Moreno, Karen M. Hamad, Antonio Moretta, Effect of Pulsed Field Ablation System and Post-Ablation Mapping on Atrial Fibrillation Recurrence, Journal of Cardiovascular Development and Disease, 10.3390/jcdd13060243, 13, 6, (243), (2026).