Indirect comparisons of tucatinib in combination with trastuzumab for patients with previously treated HER2–positive metastatic colorectal cancer
Abstract
Aim: In the single-arm MOUNTAINEER trial (NCT03043313) tucatinib in combination with trastuzumab showed an objective response rate (ORR) of 39.3% in patients with previously treated, HER2+ unresectable or metastatic colorectal cancer (mCRC). This study compared the efficacy of tucatinib in combination with trastuzumab with other treatment options in this population. Materials & methods: An unanchored, matching-adjusted indirect comparison was conducted following a systematic literature review that identified the CORRECT trial (NCT01103323), which investigated regorafenib, and the RECOURSE trial (NCT01607957), which investigated trifluridine–tipiracil, as comparators for tucatinib in combination with trastuzumab. Patient and study characteristics, overall survival (OS), progression-free survival (PFS) and ORR data were extracted and compared assuming HER2 status was not prognostic. Differences in adjusted covariates across analyses included patient age, performance status, time since metastatic diagnosis and prior lines of therapy. OS and PFS were compared using Cox proportional hazard models to generate match-adjusted hazard ratios (HRs) and 95% CI. ORR was compared via match-adjusted odds ratios and 95% CIs. As MOUNTAINEER only included patients from Europe and North America, sensitivity analyses used non-Japanese patients from CORRECT and European and US patients from RECOURSE. Results: In the main analysis, the estimated adjusted HR (95% CI) for tucatinib in combination with trastuzumab versus regorafenib was 0.26 (0.14–0.46) for OS and 0.32 (0.23–0.46) for PFS; versus trifluridine–tipiracil, this was 0.34 (0.22–0.51) for OS and 0.38 (0.20–0.58) for PFS. Similar results were seen for OS and PFS in sensitivity analyses. ORR also favored tucatinib in combination with trastuzumab across analyses. Conclusion: These data support that tucatinib in combination with trastuzumab is an effective therapy option in patients with previously treated mCRC.
Plain language summary
What was the aim of this research?
This article compares the effect of tucatinib, which is given together with trastuzumab, with other treatments for patients with metastatic colorectal cancer (mCRC).
How was the research carried out?
The researchers first reviewed available scientific publications and identified the CORRECT clinical trial, which investigated regorafenib, and the RECOURSE clinical trial, which investigated trifluridine–tipiracil, as suitable studies to compare with the MOUNTAINEER clinical trial which investigated tucatinib together with trastuzumab. Results from the three clinical trials were compared using a matching-adjusted indirect comparison.
What were the results?
On average, patients with previously treated mCRC who received tucatinib together with trastuzumab survived for longer, had more time until their cancer got worse and were more likely to respond positively to their treatment than patients with previously treated mCRC who received either regorafenib or trifluridine–tipiracil.
What do the results of the study mean?
This study suggests that tucatinib together with trastuzumab is an effective treatment option for patients with previously treated mCRC.
Globally, colorectal cancer (CRC) is the third most common cancer and second leading cause of cancer death, with an estimated 1.9 million new cases and 904,000 deaths worldwide in 2022 [1]. Approximately 23% of patients with CRC have metastatic CRC (mCRC) at initial diagnosis [2], and about 50% of patients with CRC will develop metastases [3].
First-line treatments for mCRC include multiagent chemotherapy in combination with targeted therapy (antivascular endothelial growth factor [VEGF] or antiepidermal growth factor receptor [EGFR]) or immunotherapy, depending on mutation status, tumor location and microsatellite stability status. Despite available treatment options, the prognosis for mCRC is poor, with an estimated 5-year survival rate of 15.7% [2]. Amplification and/or overexpression of erb-B2 receptor tyrosine kinase 2 (ERBB2), the gene encoding human epidermal growth factor receptor 2 (HER2), occurs in around 3% of all patients with mCRC, increasing to around 5% in patients with rat sarcoma virus (RAS) wild-type tumors [4]. National Comprehensive Cancer Network (NCCN) guidelines now recommend HER2-targeted therapies as treatment options in the second-line or later for patients with HER2-positive (HER2+) mCRC or patients with previously untreated HER2+ mCRC who are not suitable for intensive therapy [5].
Tucatinib is an oral tyrosine kinase inhibitor that is highly selective for the kinase domain of HER2 [6]. Following the release of efficacy data from the phase II, open-label MOUNTAINEER trial, tucatinib in combination with trastuzumab was the first regimen targeting HER2 to receive US FDA approval in adult patients with RAS wild-type, HER2+ unresectable CRC or mCRC that has progressed following treatment with fluoropyrimidine, oxaliplatin and irinotecan-based chemotherapy [7]. In MOUNTAINEER, the confirmed objective response rate (ORR) as of the November 2023 data cut was 39.3% (95% CI: 28.8–50.5), and the median duration of response was 15.2 months (95% CI: 8.9–20.5) in the 84 patients with HER2+ mCRC who received tucatinib in combination with trastuzumab [8,9].
As MOUNTAINEER was a noncomparative study, no head-to-head data comparing tucatinib in combination with trastuzumab to other second-line or later therapies in mCRC are currently available. Population-adjusted indirect treatment comparisons, such as matching-adjusted indirect comparisons (MAIC), can be used to evaluate the effectiveness of treatments across studies when individual patient data is available for 1 study and summary or aggregate-level data is available for another [10].
The objective of this analysis was to compare the efficacy of tucatinib in combination with trastuzumab to regorafenib and to trifluridine–tipiracil for the treatment of patients with mCRC who have received 1 or more treatments for metastatic disease or who are not considered candidates for available therapy.
Materials & methods
Data sources
Individual patient data for tucatinib in combination with trastuzumab were from MOUNTAINEER, which was a phase II, open-label clinical trial (NCT03043313) conducted to evaluate tucatinib in combination with trastuzumab in patients with chemotherapy-refractory HER2+ mCRC (tucatinib in combination with trastuzumab: n = 84), with a data cutoff date of 2 November 2023 [8,9].
A systematic literature review was conducted in March 2023 to identify suitable studies to inform the MAICs with tucatinib in combination with trastuzumab [11]. Studies were identified via the EMBASE, Medline, and EBMR databases and were screened for inclusion in the SLR against the criteria listed in Supplementary Figure 1 & Supplementary Table 1. Upon reviewing studies included in the SLR and subsequent feasibility assessment, the best candidate studies identified for the indirect comparisons were the CORRECT trial (NCT01103323), which investigated regorafenib, and the RECOURSE trial (NCT01607957), which investigated trifluridine–tipiracil. The treatments used in these studies are potential comparators for tucatinib in combination with trastuzumab in the treatment of patients with mCRC who have received 1 or more treatments for metastatic disease or are not considered candidates for available therapy.
CORRECT was a randomized, double-blind, placebo-controlled multicenter phase III trial conducted to evaluate the efficacy and safety of regorafenib in patients with mCRC who have progressed on, or after, all approved treatment for mCRC (regorafenib: n = 505 in efficacy population) [12].
RECOURSE was a double-blind, 2-arm, parallel, multicenter, randomized phase III trial that evaluated the efficacy and safety of trifluridine–tipiracil versus placebo in patients with refractory mCRC (trifluridine–tipiracil: n = 534) [13,14].
CORRECT and RECOURSE were determined to be the most suitable trials for inclusion in the MAICs versus regorafenib and trifluridine–tipiracil, respectively, because like MOUNTAINEER, both CORRECT and RECOURSE were multinational studies that included patients from Europe and North America, mostly with an Eastern Cooperative Oncology Group (ECOG) performance status of 0. Definitions of ORR, overall survival (OS), and progression-free survival (PFS) in both studies were also aligned with those used in MOUNTAINEER, enabling greater comparability across included studies.
Other potential comparator studies included CONCUR [15] for the regorafenib comparison and TERRA [16] and Yoshino et al. [17] for the trifluridine–tipiracil comparison. However, these were not included in the MAIC because TERRA and Yoshino et al. exclusively enrolled patients in Asian countries, and the majority of patients enrolled in TERRA had an ECOG of ≥1. Consequently, their enrolled populations were not considered to be comparable to the population in MOUNTAINEER.
Published aggregate data, including patient and study characteristics as well as outcomes of interest, were extracted from the published CORRECT and RECOURSE studies [12–14].
Outcomes
Outcomes of interest were OS, PFS, and ORR. PFS and ORR were evaluated using both blinded independent central review (BICR) and investigator-assessed for tucatinib in combination with trastuzumab. For patients receiving regorafenib and trifluridine–tipiracil, only investigator-assessed PFS and ORR data were available.
For the comparators' time-to-event outcomes, Kaplan–Meier (KM) curves were digitized, and the Guyot method was then used to generate pseudo-individual patient-event data from the digitized KM curves [18]. Comparisons for the primary analysis were based on the population used to report the key results of the study.
As MOUNTAINEER included patients from only Europe and North America, sensitivity analyses were conducted to report outcomes from a more geographically aligned population. For CORRECT, the non-Japanese subset (n = 438) was used for the sensitivity analysis [12]. For RECOURSE, the Europe (n = 271) and US (n = 64) subsets were used for the sensitivity analysis [14].
Statistical analysis
In the absence of a common comparator, unanchored indirect comparisons of individual treatment arms from the different studies were performed. A MAIC approach was used to adjust for imbalances in effect modifiers or prognostic variables between the studies.
Patients from MOUNTAINEER were matched to those from CORRECT and RECOURSE using inverse probability of treatment weighting obtained from method of moments propensity score estimation, where patients from the individual patient data trial (MOUNTAINEER) were weighted by their inverse propensity score to balance the covariate distribution with that of the aggregate-level study (CORRECT or RECOURSE) [10,19]. The key assumption of an unanchored MAIC is that all effect modifiers and prognostic variables are accounted for.
An initial list of potential effect modifiers/prognostic variables to use in the match adjustment was generated, and clinical opinion was then sought from four expert oncologists with professional experience in treating patients with mCRC to identify variables that could potentially impact patient outcomes. The following variables were identified by at least 1 expert and used (where reported) in the matching model: age, ECOG performance status, number of metastatic sites, presence of liver metastases, presence of lung metastases, time since diagnosis of metastatic disease, number of prior lines of therapy, site of primary tumor, and prior anti-EGFR therapy.
The MOUNTAINEER population included only patients with HER2+ mCRC; however, HER2 status was not reported in the comparator studies. In addition, the MOUNTAINEER population included only patients with RAS wild-type mCRC, whereas the comparator studies enrolled mixed populations of patients with RAS wild-type mCRC and patients with mCRC with RAS mutations. It was not possible to adjust MAICs for covariates such as these, where there are categories in the aggregate study that do not exist in the individual patient data study.
OS and PFS outcomes were compared using Cox proportional hazards models that were fitted to the weighted individual patient data or pseudo-individual patient data generated from the KM curves to generate match-adjusted HRs. The weight of comparator patients was set as 1, and 95% CIs were calculated using bootstrapping. Each bootstrap used 10,000 samples. The weighted number of patients and events for each study were tabulated, and match-adjusted KM curves were produced including numbers at risk.
Similarly, ORR was compared by generating match-adjusted odds ratios (OR) from the weighted data, and 95% CIs were calculated via bootstrapping. Each bootstrap used 10,000 samples.
An unadjusted indirect comparison was also performed to assess the impact of the matching adjustment in the same way as described for the MAIC but using nonweighted data for tucatinib in combination with trastuzumab.
For the sensitivity analysis of the RECOURSE study, the Europe and US subsets were pooled using standard meta-analytical methods for patient characteristics following the Cochrane handbook guidance [20]. These methods used weighted means or medians, summed numbers of patients for binary or categorical data, and combined standard deviations. For OS and PFS, the pseudo-individual patient data generated for each subset from the Guyot algorithm were pooled. In these subsets, unlike in the overall randomized population, the number of prior lines of therapy received was not reported. As this is a key prognostic covariate, it was imputed assuming the same proportions of patients for each line of therapy in the Europe and US subset as in the overall randomized population.
All analyses were conducted using R software version 4.3.1.
Results
Patient characteristics
Among a total of 32 studies included in the SLR, five studies were included in the feasibility assessment (27 studies were excluded due to lack of an appropriate comparator, not being a full publication, or being either an observational, nonrandomized, or single-arm study), and two were considered for the MAIC (three studies were excluded due to reported study characteristics and inclusion criteria, patient characteristics or outcomes reported), resulting in inclusion of the CORRECT and RECOURSE studies in the MAIC (Supplementary Figure 1). Patient characteristics before and after adjustment are presented in Tables 1 & 2. The CORRECT study of regorafenib did not enroll patients with ECOG performance status ≥2; therefore, patients with an ECOG performance status ≥2 were excluded from the MOUNTAINEER study population in the MAIC versus regorafenib to improve comparability between studies. The RECOURSE study of trifluridine–tipiracil did not enroll patients who had an ECOG performance status ≥2 or who had ≤1 prior line of therapy. Consequently, such patients were also excluded from the MOUNTAINEER study population in the MAIC versus trifluridine–tipiracil to improve comparability between studies.
| Characteristic | Tucatinib in combination with trastuzumab | Tucatinib in combination with trastuzumab (adjusted) | Regorafenib |
|---|---|---|---|
| N | 81.0 | 48.7 | 505.0 |
| ECOG PS, % (n/N) | |||
| 0 | 61.7 (50/81) | 52.5 (25.5/48.7) | 52.5 (265/505) |
| 1 | 38.3 (31/81) | 47.5 (23.1/48.7) | 47.5 (240/505) |
| Prior lines of therapy, % (n/N) | |||
| ≤1 | 23.5 (19/81) | 3.2 (1.5/48.7) | 3.2 (16/505) |
| 2 | 38.3 (31/81) | 23.6 (11.5/48.7) | 23.6 (119/505) |
| ≥3 | 38.3 (31/81) | 73.3 (35.7/48.7) | 73.3 (370/505) |
| Site of primary tumor, % (n/N) | |||
| Colon | 46.9 (38/81) | 64.1 (31.2/48.7) | 64.1 (323/504) |
| Rectum | 32.1 (26/81) | 30 (14.6/48.7) | 30 (151/504) |
| Colon and rectum | 21 (17/81) | 6 (2.9/48.7) | 6 (30/504) |
| Age, years | |||
| Median | 55.0 | 61.3 | 61.0 |
| Proportion greater than comparator median, % (n/N) | 28.4 (23/81) | 50 (24.3/48.7) | 50 (252.5/505) |
| Time since metastatic diagnosis, months | |||
| Median | 27.2 | 31.3 | 31.0 |
| Proportion greater than comparator median, % (n/N) | 40.7 (33/81) | 50 (24.3/48.7) | 50 (252.5/505) |
ECOG: Eastern Cooperative Oncology Group; PS: Performance status.
| Characteristic | Tucatinib in combination with trastuzumab | Tucatinib in combination with trastuzumab (adjusted) | Trifluridine–tipiracil |
|---|---|---|---|
| N | 62.0 | 36.5 | 534.0 |
| ECOG PS, % (n/N) | |||
| 0 | 64.5 (40/62) | 56.4 (20.6/36.5) | 56.4 (301/534) |
| 1 | 35.5 (22/62) | 43.6 (15.9/36.5) | 43.6 (233/534) |
| Time since metastatic diagnosis <18 months, % (n/N) | 25.8 (16/62) | 20.8 (7.6/36.5) | 20.8 (111/534) |
| Prior lines of therapy, % (n/N) | |||
| 2 | 50 (31/62) | 17.8 (6.5/36.5) | 17.8 (95/534) |
| ≥3 | 50 (31/62) | 82.2 (30/36.5) | 82.2 (439/534) |
| Prior anti-EGFR, % (n/N) | 59.7 (37/62) | 52.1 (19/36.5) | 52.1 (278/534) |
| Age, years | |||
| Median | 54.0 | 63.4 | 63.0 |
| Proportion greater than comparator median, % (n/N) | 22.6 (14/62) | 50 (18.3/36.5) | 50 (267/534) |
ECOG: Eastern Cooperative Oncology Group; EGFR: Epidermal growth factor receptor; PS: Performance status.
The presence of liver and lung metastases could not be included in the match adjustment, because the CORRECT and RECOURSE publications did not report these data. In addition, the site of the primary tumor was not reported for the RECOURSE population, and prior anti-EGFR therapy use was not reported for the CORRECT population or for the Europe and US populations in RECOURSE. Hence, these covariates could only be adjusted for in the CORRECT and overall RECOURSE populations, respectively. All other planned matching covariates were reported in the comparator study populations and were included in generation of the matching weights of the MOUNTAINEER population (Supplementary Table 2).
The MAIC effective sample size was 35.20 for tucatinib in combination with trastuzumab versus regorafenib and was 24.12 for tucatinib in combination with trastuzumab versus trifluridine–tipiracil (Supplementary Table 3).
Indirect comparisons of tucatinib in combination with trastuzumab versus regorafenib
Median OS for patients receiving tucatinib in combination with trastuzumab was 19.9 months adjusted (n = 48.7) and 24.1 months unadjusted (n = 81) compared with 6.6 months for patients receiving regorafenib (n = 505) (adjusted HR [95% CI, bootstrap]: 0.26 [0.14–0.46]; unadjusted HR [95% CI]: 0.23 [0.15–0.37]) (Figure 1A).
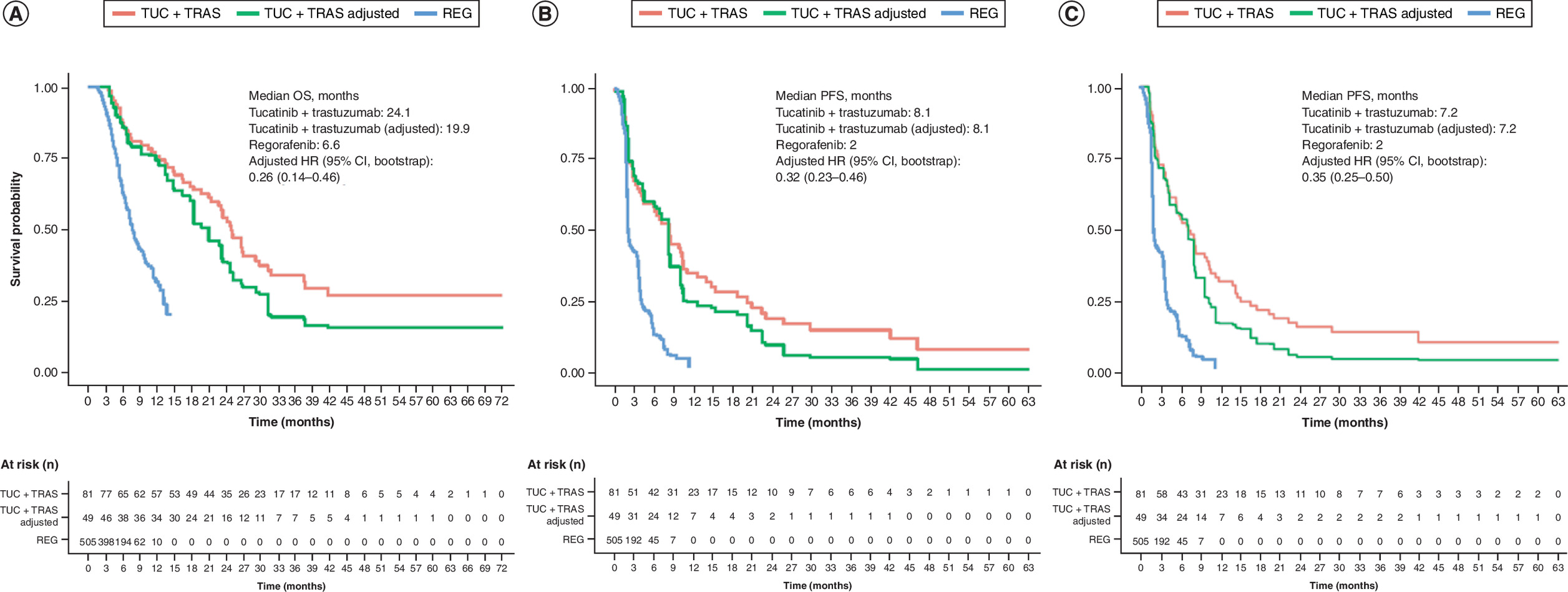
Figure 1. Comparison of overall survival and progression-free survival between tucatinib in combination with trastuzumab versus regorafenib in patients with mCRC.
(A) Kaplan–Meier plots of overall survival, (B) progression-free survival by blinded independent central review for tucatinib and investigator assessed for regorafenib and (C) investigator-assessed progression-free survival for tucatinib and regorafenib for patients treated with tucatinib in combination with trastuzumab versus regorafenib.
BICR: Blinded independent central review; CI: Confidence interval; HR: Hazard ratio; KM: Kaplan–Meier; OS: Overall survival; PFS: Progression-free survival; REG: Regorafenib; TRAS: Trastuzumab; TUC: Tucatinib.
Survival probability at 12 months was 72.7% (adjusted) and 74.5% (unadjusted) in patients receiving tucatinib in combination with trastuzumab compared with 24.5% in patients receiving regorafenib (Table 3).
| Treatment arm | OS (12 months), % | PFS BICR (6 months), % | PFS investigator-assessed (6 months), % |
|---|---|---|---|
| Tucatinib in combination with trastuzumab vs regorafenib | |||
| Tucatinib in combination with trastuzumab (unadjusted) | 74.5 | 57.8 | 55 |
| Tucatinib in combination with trastuzumab (adjusted) | 72.7 | 58.9 | 55.7 |
| Regorafenib | 24.5 | 13.2 | 13.2 |
| Tucatinib in combination with trastuzumab vs trifluridine–tipiracil | |||
| Tucatinib in combination with trastuzumab (unadjusted) | 69.7 | 53.6 | 50.9 |
| Tucatinib in combination with trastuzumab (adjusted) | 72.8 | 60.7 | 58.9 |
| Trifluridine–tipiracil | 26.6 | 15.2 | 15.2 |
BICR: Blinded independent central review; OS: Overall survival; PFS: Progression-free survival.
Median PFS assessed using BICR for patients receiving tucatinib in combination with trastuzumab was 8.1 months (for both adjusted and unadjusted) compared with 2 months investigator assessed for patients receiving regorafenib (adjusted HR [95% CI, bootstrap]: 0.32 [0.23–0.46]; unadjusted HR [95% CI]: 0.30 [0.22–0.41]) (Figure 1B).
Median investigator-assessed PFS was 7.2 months (for both adjusted and unadjusted) for patients receiving tucatinib in combination with trastuzumab compared with 2 months for patients receiving regorafenib (adjusted HR [95% CI, bootstrap]: 0.35 [0.25–0.50]; unadjusted HR [95% CI]: 0.30 [0.22–0.41]) (Figure 1C).
The confirmed ORR per BICR for patients receiving tucatinib in combination with trastuzumab was 40.9% adjusted (n = 19.9/48.7) and 39.5% unadjusted (n = 32/81) compared with an investigator-assessed ORR of 1% (n = 5/505) for patients receiving regorafenib (adjusted OR [95% CI, bootstrap]: 69.1 [26.3–339.7]; unadjusted OR [95% CI]: 65.3 [24.3–175.2]).
In the sensitivity analysis limited to the non-Japanese population from the CORRECT study only (n = 438) (Supplementary Table 4 & Supplementary Figure 2) compared with covariates adjusted for in the overall randomized population, the non-Japanese population did not report data on the proportion of patients who received ≤1 prior line of therapy (i.e., they reported only the proportion with ≤2 prior lines of therapy). Median OS for tucatinib in combination with trastuzumab was 17.3 months adjusted and 24.1 months unadjusted compared with 6.3 months for regorafenib (adjusted HR [95% CI, bootstrap]: 0.29 [0.18–0.49]; unadjusted HR [95% CI]: 0.23 [0.14–0.35]) (Supplementary Figure 2). Median PFS assessed using BICR for tucatinib in combination with trastuzumab was 8.1 months (for both adjusted and unadjusted) compared with the 2.2 months investigator-assessed PFS for regorafenib (adjusted HR [95% CI, bootstrap]: 0.39 [0.27–0.58]; unadjusted HR [95% CI]: 0.34 [0.25–0.46]). Median investigator-assessed PFS for tucatinib in combination with trastuzumab was 7 months (adjusted) and 7.2 months (unadjusted) compared with 2.2 months for regorafenib (adjusted HR [95% CI, bootstrap]: 0.42 [0.31–0.59]; unadjusted HR [95% CI]: 0.34 [0.25–0.46]). The confirmed ORR per BICR for patients receiving tucatinib in combination with trastuzumab was 38.2% (adjusted) (n = 18.6/48.7) and 39.5% (unadjusted) (n = 32/81) compared with investigator-assessed ORR of 0.9% (n = 4/438) for patients receiving regorafenib (adjusted OR [95% CI, bootstrap]: 67.2 [21.7–407.9]; unadjusted OR [95% CI]: 70.9 [24.0–208.8]).
Indirect comparisons of tucatinib in combination with trastuzumab versus trifluridine–tipiracil
Median OS for patients receiving tucatinib in combination with trastuzumab was 22.2 months adjusted (n = 36.5) and 22.2 months unadjusted (n = 62) compared with 6.9 months in patients receiving trifluridine–tipiracil (n = 534) (adjusted HR [95% CI, bootstrap]: 0.34 [0.22–0.51]; unadjusted HR [95% CI]: 0.29 [0.21–0.42]) (Figure 2A).
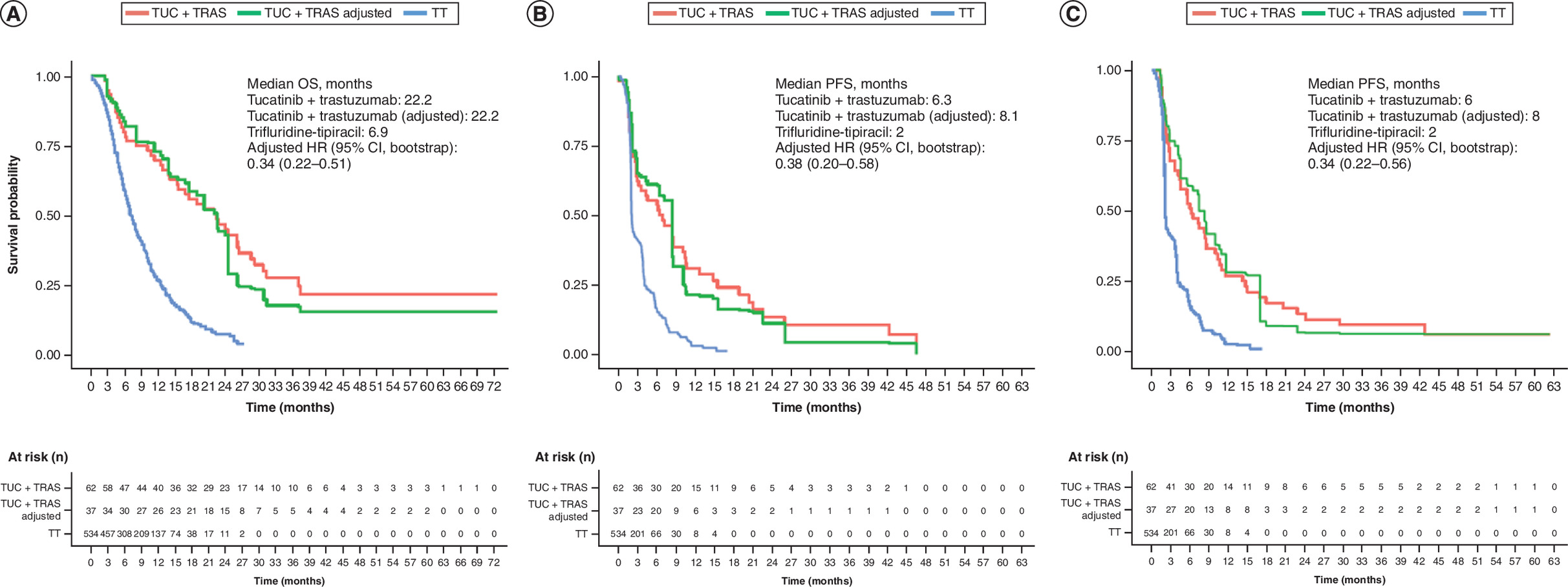
Figure 2. Comparison of overall survival and progression-free survival between tucatinib in combination with trastuzumab versus trifluridine-tipiracil in patients with mCRC.
(A) Kaplan–Meier plots of overall survival, (B) progression-free survival by blinded independent central review and (C) investigator-assessed PFS for patients treated with tucatinib in combination with trastuzumab versus trifluridine-tipiracil.
BICR: Blinded independent central review; CI: Confidence interval; HR: Hazard ratio; KM: Kaplan–Meier; OS: Overall survival; PFS: Progression-free survival; TRAS: Trastuzumab; TT: Trifluridine–tipiracil; TUC: Tucatinib.
Survival probability at 12 months was 72.8% (adjusted) and 69.7% (unadjusted) in patients receiving tucatinib in combination with trastuzumab compared with 26.6% in patients receiving trifluridine–tipiracil.
Median PFS assessed using BICR for patients receiving tucatinib in combination with trastuzumab was 8.1 months (adjusted) and 6.3 months (unadjusted) compared with the 2.0 months investigator-assessed PFS for patients receiving trifluridine–tipiracil (adjusted HR [95% CI, bootstrap]: 0.38 [0.20–0.58]; unadjusted HR [95% CI]: 0.37 [0.27–0.51]) (Figure 2B).
Median investigator-assessed PFS was 8 months (adjusted) and 6 months (unadjusted) for patients receiving tucatinib in combination with trastuzumab compared with 2 months for patients receiving trifluridine–tipiracil (adjusted HR [95% CI, bootstrap]: 0.34 [0.22–0.56]; unadjusted HR [95% CI]: 0.37 [0.27–0.51]) (Figure 2C).
The confirmed ORR per BICR for patients receiving tucatinib in combination with trastuzumab was 30.1% (adjusted) (n = 11/36.5) and 37.1% (unadjusted) (n = 23/62) compared with the investigator-assessed ORR of 1.6% (n = 8/502) for patients receiving trifluridine–tipiracil (adjusted OR [95% CI, bootstrap]: 26.6 [9.0–107.7]; unadjusted OR [95% CI]: 36.4 [15.3–86.8]).
In the sensitivity analysis that included the Europe and US populations from the RECOURSE study only (n = 335) (Supplementary Table 5 & Supplementary Figure 3) compared with covariates adjusted for in the overall randomized population, prior lines of therapy were not reported for this subset and were imputed from the overall randomized population; age was reported as mean (SD) instead of median, and prior EGFR therapy was not reported. Median OS for tucatinib in combination with trastuzumab was 19.9 months (adjusted) and 22.2 months (unadjusted) compared with the 6.7-month median OS for trifluridine–tipiracil (adjusted HR [95% CI, bootstrap]: 0.29 [0.15–0.50]; unadjusted HR [95% CI]: 0.33 [0.21–0.51]) (Supplementary Figure 3). Median PFS assessed using BICR for tucatinib in combination with trastuzumab was 8.1 months (adjusted) and 6.3 months (unadjusted) compared with the 2-month investigator-assessed median PFS for trifluridine–tipiracil (adjusted HR [95% CI, bootstrap]: 0.33 [0.20–0.50]; unadjusted HR [95% CI]: 0.37 [0.26–0.53]). Median investigator-assessed PFS for tucatinib in combination with trastuzumab was 7.2 months (adjusted) and 6 months (unadjusted) compared with 2 months for trifluridine–tipiracil (adjusted HR [95% CI, bootstrap]: 0.33 [0.19–0.52]; unadjusted HR [95% CI]: 0.37 [0.26–0.51]). ORR results were not reported for this population in the RECOURSE study.
Discussion
In the absence of direct evidence from head-to-head studies, indirect treatment comparisons can be used to determine the relative efficacy of different treatments [10]. This study used MAICs of individual patient data from MOUNTAINEER and aggregate summary-level data from the CORRECT and RECOURSE studies to compare the efficacy of tucatinib in combination with trastuzumab with that of regorafenib and that of trifluridine–tipiracil in patients with previously treated mCRC. CORRECT and RECOURSE were selected for inclusion in the MAICs versus regorafenib and trifluridine–tipiracil, respectively, because they enrolled study populations with similar characteristics to the patients enrolled in MOUNTAINEER and because those studies used similar definitions of ORR, OS and PFS. These similarities enabled greater comparability across included studies. In addition, these were important comparators due to their utilization across healthcare systems. For instance, both trifluridine–tipiracil and regorafenib are widely used in the UK, where they are approved for use by patients with mCRC who have previously received other treatments, or if other available treatments are not suitable [21,22].
However, there were some differences between MOUNTAINEER and the comparator studies. The MOUNTAINEER population included only patients with HER2+ mCRC, whereas HER2 status was not reported in the comparator studies. Therefore, any indirect comparisons are valid only under the assumption that the comparator outcomes in the other populations would have been the same if the study were conducted in a population of patients who all had HER2+ mCRC. Supporting this assumption, a retrospective analysis of 7121 patients with HER2+ and HER2- mCRC who were treated with non-HER2-targeted therapy found no significant difference in OS between the groups [23], which, together with other similar findings [24–27], suggests that HER2 status is not prognostic in mCRC.
Additionally, MOUNTAINEER enrolled only patients with RAS wild-type mCRC. Therefore, all enrolled patients had Kirsten rat sarcoma (KRAS) wild-type mCRC, whereas the comparators enrolled mixed populations of patients with KRAS wild-type mCRC and mCRC with KRAS mutations. As above, indirect comparisons were conducted under the assumption that comparator outcomes in the mixed populations would have been the same if their population had all been KRAS wild-type. Since KRAS mutations are associated with poorer outcomes with treatment [28,29], this difference in population characteristics could have resulted in better outcomes in the MOUNTAINEER population than in comparator studies and may have influenced the analysis results.
The number of metastatic sites and presence of liver and lung metastases also could not be adjusted for because they were not reported in the comparator studies, and the site of the primary tumor and prior anti-EGFR therapy could not be adjusted for in all MAICs because these details were not reported for all study populations.
While it is possible that unknown imbalances in these characteristics between studies could have had some influence on the results, given the large magnitude of effect from the available analyses, these variables would have had to be very strong confounders to alter the conclusions. Overall, match-adjusted comparisons favored tucatinib in combination with trastuzumab for all available outcomes across all comparators included in the analysis.
Further, for the OS and PFS outcomes, the duration of follow-up was much shorter for CORRECT than MOUNTAINEER; as such, the estimated HR used only the earlier data from MOUNTAINEER and may not have captured the complete treatment effect over the study period. Hence, this analysis may not have been representative of the long-term benefit of tucatinib in combination with trastuzumab versus regorafenib.
The sensitivity analysis in patient populations geographically aligned with those in MOUNTAINEER were consistent with the main analysis. The MAIC comparisons also favored tucatinib in combination with trastuzumab for the unadjusted indirect comparisons. The magnitude of this effect was smaller in the adjusted comparisons than in the unadjusted comparisons. This may have been due to patients in MOUNTAINEER being younger, having better ECOG performance status, and having received fewer previous lines of therapy than comparator study populations resulting in improved clinical outcomes; the imbalance in these covariates was accounted for in the adjusted analysis.
Until recently, regorafenib and trifluridine–tipiracil have been standard-of-care subsequent-line treatment options in patients with mCRC who have progressed through available treatment regimens [5]. Several clinical studies, including MOUNTAINEER, have now demonstrated the efficacy of HER2-targeted therapy in patients with previously treated HER2+ mCRC [9,30–32]. HER2-directed therapies are now included as subsequent therapy options in HER2+ mCRC in the NCCN treatment guidelines, which also recommend testing for HER2 amplification/overexpression in patients with mCRC [5]. At the same time, new treatments and regimens for mCRC continue to be developed. For example, fruquintinib and trifluridine–tipiracil plus bevacizumab have been recently approved for the treatment of patients with previously treated mCRC based on data from the FRESCO/FRESCO-2 (NCT02314819 and NCT04322539) studies for fruquintinib [22,33] and the SUNLIGHT (NCT04737187) study for trifluridine–tipiracil plus bevacizumab [21,34].
Nevertheless, taken together, the MAIC data presented here, along with data from the primary efficacy analysis and final analysis of MOUNTAINEER data [8,9], suggest that tucatinib in combination with trastuzumab is an effective therapy option in patients with chemotherapy-refractory HER2+ mCRC. Additionally, these findings provide valuable insights, which can further inform the ongoing development of new therapies, as well as build upon the existing body of clinical and real-world evidence, which can collectively be used to inform future treatment recommendations. With the availability of new treatment options for mCRC, these results provide further information for clinicians to consider when selecting subsequent therapy for patients with previously treated HER2+ mCRC.
Limitations
These analyses are based on unanchored indirect comparisons, because no common comparator was available between the studies. This approach loses the protection of randomization that is inherent in a network meta-analysis or anchored indirect comparison and requires the assumption that all effect modifiers and prognostic factors are accounted for. The MAIC methodology can control only for the characteristics reported in the study publications of CORRECT and RECOURSE, and results may be confounded by other unreported factors. The number of prior lines of therapy received in the US and European subsets in the RECOURSE study were imputed from the overall population due to the absence of data for these subgroups. As the number of prior lines of therapy is a prognostic factor in the metastatic setting, our study is limited by this potential for bias that could be investigated in future studies. As HER2 status was not reported in the CORRECT and RECOURSE trials, it was not possible to control for HER2 status. While the assumption that HER2 status does not have a prognostic role in mCRC is supported by a number of studies [23–27], mixed results have also been reported [35,36] and, as such, this should be considered a limitation of this analysis.
The effective sample size after adjustment was small for most analyses in the study, which increases the uncertainty and may reduce the robustness of the results. OS and PFS for the CORRECT and RECOURSE studies were based on pseudo-individual patient data reconstructed from the digitized KM curves and are thus not exact. The comparator studies used investigator assessment of response, compared with confirmed BICR assessment in MOUNTAINEER, although this would have likely favored the comparator treatments, because a confirmed response is broadly considered to be more stringent [37].
Additional limitations included differences in study design, because MOUNTAINEER was a phase II, open-label, noncomparative study, whereas CORRECT and RECOURSE were both phase III, randomized, double-blind, placebo-controlled studies. The single-arm nature of MOUNTAINEER could have introduced open-label bias in contrast with the double-blind design of CORRECT and RECOURSE, potentially impacting treatment effects observed.
Conclusion
In this MAIC analysis, patients with previously treated HER2+ mCRC who were treated with tucatinib in combination with trastuzumab had more favorable PFS, ORR and OS outcomes than patients treated with regorafenib or trifluridine–tipiracil.
Summary points
•
Colorectal cancer (CRC) is the third most common cancer globally and is the second leading cause of cancer death.
•
Most patients with CRC either have metastatic CRC (mCRC) at their initial diagnosis or go on to develop metastases.
•
To compare the efficacy of tucatinib in combination with trastuzumab with other treatment options for patients with previously treated, unresectable mCRC, a systematic literature review (SLR) was conducted, followed by an unanchored, matching-adjusted indirect comparison (MAIC).
•
Two studies were identified by the SLR as suitable comparators for tucatinib in combination with trastuzumab and were included in the MAIC; the CORRECT trial, which investigated regorafenib, and the RECOURSE trial, which investigated trifluridine–tipiracil.
•
The MAIC estimated hazard ratio for overall survival was 0.26 (95% CI: 0.14–0.46) for tucatinib in combination with trastuzumab versus regorafenib and was 0.34 (95% CI: 0.22–0.51) versus trifluridine–tipiracil, favoring tucatinib in combination with trastuzumab in both comparisons.
•
The MAIC estimated hazard ratio for progression-free survival was 0.32 (0.23–0.46) for tucatinib in combination with trastuzumab versus regorafenib and was 0.38 (0.20–0.58) versus trifluridine–tipiracil, favoring tucatinib in combination with trastuzumab.
•
Sensitivity analyses by geographical region also favored tucatinib in combination with trastuzumab versus regorafenib and trifluridine–tipiracil.
•
These data support that tucatinib in combination with trastuzumab is an effective therapy option in patients with previously treated HER2+ unresectable or mCRC.
Author contributions
Conception and design: All authors; Provision of study materials: C Watkins, R Leadley, G Redhead; Collection and assembly of data: C Watkins, R Leadley, G Redhead, E Neuberger, K Bartley; Data analysis and interpretation: All authors; Manuscript writing: All authors; Final approval of manuscript: All authors.
Acknowledgments
Janine Ross from Mtech Access was responsible for the search strategy development and execution.
Financial disclosure
This study was sponsored by Seagen Inc. (WA, USA), which was acquired by Pfizer in December 2023, in collaboration with Merck Sharp & Dohme Corp, a subsidiary of Merck & Co, Inc. (NJ, USA).
Competing interests disclosure
C Watkins is an employee of Clarostat Consulting, which received funding from Pfizer Inc. C Simon is an employee of, and owns stock in, Pfizer Ltd. R Leadley and G Redhead were employees of Mtech Access, which has since been acquired by Petauri; Mtech Access received funding from Pfizer Inc. E Neuberger, P Martin and K Bartley were, at the time of this study, employees of, and held stock in, Pfizer Inc. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support was provided by Philip Ruane of Envision Value & Access, a part of Envision Medical Communications, and funded by Pfizer.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Bray F, Laversanne M, Sung H et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 74(3), 229–263 (2024).
2.
National Cancer Institute SEER program. Cancer Stat Facts: Colorectal Cancer (2024). Available from: https://seer.cancer.gov/statfacts/html/colorect.html
3.
Carrion-Alvarez L, Primavesi F, Søreide K et al. Liver metastases from colorectal cancer: a joint ESSO-EAHPBA-UEMS core curriculum collaboration. Eur. J. Surg. Oncol. 51(6), 109728 (2025).
4.
Pilati C, Soulabaille A, Gallois C et al. ERBB2 comprehensive profiling and prognostication in stage III colon cancer: findings from PETACC8 and IDEA-France cohorts. Gastroenterology 168(4), 714–724.e4 (2025).
5.
Malla M, Pedersen KS, Parikh AR. Updates in the treatment of metastatic colorectal cancer. J. Natl Comp. Cancer Network 21(5.5), 567–571 (2023).
• Provides recent key updates to NCCN guidelines on the testing and treatment of metastatic CRC (mCRC).
6.
Kulukian A, Lee P, Taylor J et al. Preclinical activity of HER2-selective tyrosine kinase inhibitor tucatinib as a single agent or in combination with trastuzumab or docetaxel in solid tumor models. Mol. Cancer Ther. 19(4), 976–987 (2020).
7.
FDA. FDA grants accelerated approval to tucatinib with trastuzumab for colorectal cancer (2023). Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-tucatinib-trastuzumab-colorectal-cancer
• Highlights the 2023 USFDA approval of tucatinib in combination with trastuzumab in patients with HER2+ RAS wild-type mCRC previously treated with fluoropyrimidine-, oxaliplatin-and irinotecan-based chemotherapy.
8.
Strickler JH, Cercek A, Siena S et al. Final results of a phase II study of tucatinib and trastuzumab for HER2-positive mCRC (MOUNTAINEER). J. Clin. Oncol. 42(Suppl. 16), 3509 (2024).
•• Pivotal publications reporting key results from the MOUNTAINEER trial showing the efficacy and safety of the HER2-targeted therapy tucatinib in combination with trastuzumab in previously treated patients with HER2+ RAS wild-type mCRC.
9.
Strickler JH, Cercek A, Siena S et al. Tucatinib plus trastuzumab for chemotherapy-refractory, HER2-positive, RAS wild-type unresectable or metastatic colorectal cancer (MOUNTAINEER): a multicentre, open-label, Phase II study. Lancet Oncol. 24(5), 496–508 (2023).
•• Pivotal publications reporting key results from the MOUNTAINEER trial showing the efficacy and safety of the HER2-targeted therapy tucatinib in combination with trastuzumab in previously treated patients with HER2+ RAS wild-type mCRC.
10.
Signorovitch JE, Sikirica V, Erder MH et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health 15(6), 940–947 (2012).
11.
Leadley R, Bhadti S, Ross J, Bartley K, Simon C, Martin P. Systematic literature reviews of clinical, economic evaluation, health state utility value, and cost/resource use studies in patients with human epidermal growth factor receptor 2 positive metastatic or unresectable colorectal carcinoma. PROSPERO 2023 CRD42023404442. (2023). Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023404442
12.
Grothey A, Van Cutsem E, Sobrero A et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase III trial. Lancet 381(9863), 303–312 (2013).
•• Publications reporting key results from the CORRECT and RECOURSE trials that were included in the matching-adjusted indirect comparison (MAIC).
13.
Mayer RJ, Van Cutsem E, Falcone A et al. Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N. Engl. J. Med. 372(20), 1909–1919 (2015).
•• Publications reporting key results from the CORRECT and RECOURSE trials that were included in the MAIC.
14.
Van Cutsem E, Mayer RJ, Laurent S et al. The subgroups of the phase III RECOURSE trial of trifluridine/tipiracil (TAS-102) versus placebo with best supportive care in patients with metastatic colorectal cancer. Eur. J. Cancer 90, 63–72 (2018).
•• Publications reporting key results from the CORRECT and RECOURSE trials that were included in the MAIC.
15.
Li J, Qin S, Xu R et al. Regorafenib plus best supportive care versus placebo plus best supportive care in Asian patients with previously treated metastatic colorectal cancer (CONCUR): a randomised, double-blind, placebo-controlled, phase III trial. Lancet Oncol. 16(6), 619–629 (2015).
16.
Xu J, Kim TW, Shen L et al. Results of a randomized, double-blind, placebo-controlled, phase III trial of trifluridine/tipiracil (TAS-102) monotherapy in Asian patients with previously treated metastatic colorectal cancer: the TERRA study. J. Clin. Oncol. 36(4), 350–358 (2018).
17.
Yoshino T, Mizunuma N, Yamazaki K et al. TAS-102 monotherapy for pretreated metastatic colorectal cancer: a double-blind, randomised, placebo-controlled phase II trial. Lancet Oncol. 13(10), 993–1001 (2012).
18.
Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 12, 9 (2012).
19.
Signorovitch JE, Wu EQ, Yu AP et al. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. Pharmacoeconomics 28(10), 935–945 (2010).
20.
Higgins JPT, Thomas J, Chandler J et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.5 (updated August 2024) (2024). Available from: www.cochrane.org/handbook
• The most up-to-date version (2024) of the Cochrane Handbook for Systematic Reviews of Interventions.
21.
Medicines & Healthcare Products Regulatory Agency. LONSURF 20 MG/8.19 MG film-coated tablets (SPC). (2023).
22.
Medicines & Healthcare Products Regulatory Agency. Fruzaqla (SPC). (2023).
23.
Starling N, Snider J, Cho-Phan C et al. 75P. The prognostic impact of human epidermal growth factor receptor 2 (HER2) status in metastatic colorectal cancer (mCRC). Ann. Oncol. 35, S36–S37 (2024).
24.
Bartley K, Snider J, Cho-Phan C et al. The prognostic impact of human epidermal growth factor receptor 2 status in metastatic colorectal cancer. Future Sci. OA 11(1), 2527482 (2025).
25.
Schröder C, Gower-Page C, Reyes-Rivera I et al. Natural history of human epidermal growth factor receptor 2-amplified and human epidermal growth factor receptor 2 wild-type refractory metastatic colorectal cancer in US clinical practice. JCO Clin. Cancer Inform. 6, e2100133 (2022).
26.
Jang JY, Jeon YK, Jeong SY et al. Effect of human epidermal growth factor receptor 2 overexpression in metastatic colorectal cancer on standard chemotherapy outcomes. J. Gastrointest. Oncol. 14(5), 2097–2110 (2023).
27.
Sartore-Bianchi A, Amatu A, Porcu L et al. HER2 positivity predicts unresponsiveness to EGFR-targeted treatment in metastatic colorectal cancer. Oncologist 24(10), 1395–1402 (2019).
28.
Strickler JH, Yoshino T, Stevinson K et al. Prevalence of KRAS G12C mutation and co-mutations and associated clinical outcomes in patients with colorectal cancer: a systematic literature review. Oncologist 28(11), e981–e994 (2023).
29.
Zhu G, Pei L, Xia H, Tang Q, Bi F. Role of oncogenic KRAS in the prognosis, diagnosis and treatment of colorectal cancer. Mol. Cancer 20(1), 143 (2021).
30.
Sartore-Bianchi A, Trusolino L, Martino C et al. Dual-targeted therapy with trastuzumab and lapatinib in treatment-refractory, KRAS codon 12/13 wild-type, HER2-positive metastatic colorectal cancer (HERACLES): a proof-of-concept, multicentre, open-label, phase II trial. Lancet Oncol. 17(6), 738–746 (2016).
31.
Meric-Bernstam F, Hurwitz H, Raghav KPS et al. Pertuzumab plus trastuzumab for HER2-amplified metastatic colorectal cancer (MyPathway): an updated report from a multicentre, open-label, phase IIa, multiple basket study. Lancet Oncol. 20(4), 518–530 (2019).
32.
Siena S, Di Bartolomeo M, Raghav K et al. Trastuzumab deruxtecan (DS-8201) in patients with HER2-expressing metastatic colorectal cancer (DESTINY-CRC01): a multicentre, open-label, phase II trial. Lancet Oncol. 22(6), 779–789 (2021).
33.
FDA. Highlights of Prescribing Information (Fruzaqla). (2023). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217564s000lbl.pdf
34.
FDA. Highlights of Prescribing Information (Lonsurf). (2023). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/207981s012lbl.pdf
35.
Yagisawa M, Sawada K, Nakamura Y et al. Prognostic value and molecular landscape of HER2 low-expressing metastatic colorectal cancer. Clin. Colorectal Cancer 20(2), 113–120.e1 (2021).
36.
Takahashi N, Iwasa S, Taniguchi H et al. Prognostic role of ERBB2, MET and VEGFA expression in metastatic colorectal cancer patients treated with anti-EGFR antibodies. Br. J. Cancer 114(9), 1003–1011 (2016).
37.
Dello Russo C, Navarra P. Local investigators significantly overestimate overall response rates compared to blinded independent central reviews in uncontrolled oncology trials: a comprehensive review of the literature. Front. Pharmacol. 13, 858354 (2022).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 13 February 2025
Accepted: 24 December 2025
Published online: 28 January 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Indirect comparisons of tucatinib in combination with trastuzumab for patients with previously treated HER2–positive metastatic colorectal cancer. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0017
Export citation
Select the citation format you wish to export for this article or chapter.