The impact of socioeconomic crisis on cancer patient outcomes in Lebanon, 2018–2020
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The goal of this study was to assess the impact of economic and social crisis on access to cancer care in Lebanon. Materials & methods: A cancer Drug Access Program in Lebanon was launched, covering 80–90% of treatment costs. The program included three drugs for breast cancer, renal cancer, and lung cancer. A longitudinal follow-up of patients was conducted. The Multidimensional Poverty Measure (MPI) was used by year (2019 or 2021), i.e., before and after the onset of the economic crisis. Results: A total of 613 cancer patients were included in 50 hospitals. Mean patient age was 58.5 years (standard deviation = 12.3). The proportion of cancer types was 79.3% breast, 10.6% renal, and 7.3% lung cancer. Treatment with palbociclib (hazard ration [HR]: 1.64; 95% confidence interval [CI]: 1.53–1.76, p < 0.0004), enrollment prior to 1 January 2019 (HR: 1.24; 95% CI: 1.07–1.44, p = 0.004), treatment at a hospital with fewer than five physicians (HR: 1.11; 95% CI: 1.00–1.23, p = 0.04), and lower 2019 MPI (HR: 1.69; 95% CI: 1.30–2.20) were significant predictive factors associated with survival. Higher governorate-level MPI was associated with increased mortality (adjusted rate ratio per 0.1-unit, HR: 2.88; 95% CI: 0.95–8.77, p = 0.06). Conclusion: Economic crises have negative impacts on health outcomes, and we identified a change in survival pre/post crisis onset. This study argues strongly for coordinated efforts to mitigate the negative effects of poverty on health.
Plain language summary: How did the economic crisis in Lebanon impact the health of patients treated for cancer between 2018 and 2020?
What is this article about?
Since 2019, several events (an ongoing economic crisis, war in a neighboring country, severe wildfires, a massive explosion at a large port, the COVID-19 pandemic and political unrest) have negatively impacted Lebanon’s economy and made it difficult for patients to receive care. This study identified factors that impacted survival for cancer patients who began treatment before the start of Lebanon’s economic crisis in 2019 and those who started treatment once the crisis had begun.
What were the results?
This study found that patients who began cancer treatment before the start of the 2019 crisis were more likely to survive than patients who started treatment in 2019 or 2020. Other factors associated with being more likely to survive were treatment with a specific drug for breast cancer, treatment at a hospital with fewer than five physicians, and lower levels of poverty in 2019.
What do the results mean?
The results mean that factors unrelated to a cancer patients’ disease – when they started treatment, staffing at the hospital where they were treated, and their poverty level – can impact how likely they are to survive. These findings add to other data that show how poverty can negatively impact health. They also suggest that reducing poverty is important for improving survival in patients with cancer.
The incidence of cancer in Lebanon doubled between 1968 and 2018 [1], but has remained stable over the more recent period of 2008–2015 [2]. Breast, colorectal, and lung cancer are the most common cancer in Lebanese patients [2,3] and the incidence of all three cancers is expected to increase significantly by 2025 [2]. The cost of cancer medications in Lebanon is also on the rise, with the average cost of cancer medication increasing more than 50% between 2008 and 2013 in response to the growing use of more expensive targeted cancer therapies [1]. The introduction of new immunotherapies resulted in an additional 20% increase between 2014 and 2016 [1].
Approximately half the Lebanese population lacks sufficient access to healthcare and insurance coverage and must pay out-of-pocket for some or all of their medical care [4]. Since 1999, the Lebanese Ministry of Public Health has provided free cancer medication to all Lebanese patients who lack health coverage [1]. Total spending by Ministry of Public Health on cancer medications in the 2014–2016 period was US$140 million [1]. While government coverage of cancer medication for patients who lack formal health coverage is important for increasing access to life-saving therapy, this approach poses a significant financial burden to the Lebanese economy and does not address the needs of those patients who have insufficient coverage.
The start of the Syrian armed conflict in 2011 led to a years-long displacement of Syrian residents. By the end of 2019, Lebanon was home to 928,000 Syrian refugees [5], which placed a significant burden on national services [6]. Several other events in 2019 and 2020, including Lebanon’s worst wildfire in 50 years, a revolutionary uprising against the government in response to a severe and ongoing economic crisis, the COVID-19 pandemic, and the massive explosion in the port of Beirut in 2020 that displaced 300,000 people and injured more than 7000 [7,8] resulted in a liquidity crisis that upended every aspect of the country’s economy, including its healthcare system [9]. In 2019, the Lebanese government owed US$1.3 billion to private hospitals [9] While these hospitals comprise 82% of Lebanon’s healthcare capacity, they had received no government funding in 2019 [9]. Medical supply companies struggled to import needed medical equipment, many nurses were working for half or no pay, medical institutions laid off employees, and doctors provided free services where they could [9,10]. As the economy collapsed, people within Lebanon began to forgo nonessential healthcare, and necessary care became unaffordable for many [9].
Several studies have already identified associations between economic crises and worse health outcomes, including increases in rates of mental health hospitalizations [11] and dissociative experiences (absorption and dissociative amnesia/depersonalization) [12]; risk of cancer [13], diagnosis of breast cancer at later stages [14] and excess cancer-related deaths [15]; all-cause and disease-specific mortality [16]; and social and mortality inequalities [17]. Austerity measures imposed in response to these crises have led to reductions in government healthcare spending while simultaneously increasing poverty, deregulation of healthcare services and out-of-pocket costs for patients. These changes in the healthcare landscape have been associated with deterioration of public health and with increased rates of mental health issues, self-reported unmet medical needs, substance abuse, epidemics, suicide, mortality and disparities in health outcomes [18–23].
In addition to broad effects on diverse health outcomes, economic crises have also had specific negative effects on cancer care and outcomes. The Lebanese economic crisis has increased the cost of bladder cancer care by 768% [24]. This increase included a 61% increase in payments by third-party payers and a 2.74% increase in patients’ out-of-pocket expenses, which reduced overall third-party payers coverage to 17% of total bladder cancer costs. The burden of lung cancer increased after the onset of the Greek economic crisis in 2009, and the deprivation index was a significant predictor of increased risk of lung cancer mortality [25]. An analysis of unemployment rates during a period of economic recession found that increased rates of unemployment were associated with reductions in cancer diagnoses, cancer surgery and radiation therapy [26].
In addition to the effects of systemic economic crises, poverty at the individual level also impacts health outcomes. Since 2019, income poverty in Lebanon has increased due to decreased economic activity, political instability, inflation and currency depreciation [27]. Additionally, there is rising deprivation in areas beyond income, including healthcare, medicines, government services, education, employment, housing and assets. Recognizing that factors other than income poverty contribute to deprivation, the United Nations developed a Multidimensional Poverty Measure (MPI), which consists of 20 indicators across six dimensions (education, health, public utilities, housing, assets and property and employment and income) [27]. Households deprived in one or more dimensions are classified as living in multidimensional poverty, while those deprived in two or more dimensions are classified as living in extreme multidimensional poverty [27]. The multidimensional poverty level in Lebanon nearly doubled from 2019 (42% of the Lebanese population) to 2021 (82%), with 34% of the population living in extreme multidimensional poverty in 2021. From 2019 to 2021 the percentage of households deprived of healthcare increased from 9% to 33% [27].
Despite the high rates of health deprivation following the onset of the Lebanese liquidity crisis, cancer patients participating in the 2018–2020 Access Program continued to have access to their cancer medications for the duration of the Program. Approximately 80% of medication costs for patients participating in the program were covered by Social Security and the remainder of the cost was discounted. The elimination of financial barriers to accessing these therapies enabled evaluation of other factors (patient, physician, social determinants of health, etc.) that impacted health outcomes for patients in the Access Program. The goal of this study was to assess the impact of economic and social crisis on access to treatment and mortality in cancer patients in Lebanon.
Materials & methods
Study setting & design
In 2018, a Drug Access Program for cancer was implemented in Lebanon by Axios International. Social security paid for 80–90% of treatment costs, and the remaining costs were discounted so that patients participating in the Program had minimal out of pocket expenses for their cancer medications. The three drugs included in the Program were palbociclib (for breast cancer), crizotinib (renal cancer) or sunitinib (lung cancer). Patients diagnosed with other cancers that could be treated on-label with one of the three medications also were eligible to participate.
As part of its evaluation of the Access Program, Axios International conducted an anonymized longitudinal analysis of patients enrolled in the program from 2018 to 2020 in Lebanon. Incident case patients enrolled in the program and newly treated with one of the three specified cancer medications were included. The manufacturer of these medications had no role in the study conception, design, analyses or drafting of the manuscript.
Study population
The study included participants who met the following criteria: ≥18 years of age at program enrollment, confirmed cancer diagnosis consistent with the study drugs’ approved indications, initiation of treatment with palbociclib, crizotinib, or sunitinib and willingness to participate in the Access Program. The exclusion criteria were: <18 years of age at time of enrollment, diagnosis not compatible with approved indications of study drugs, cancer therapy initiated prior to program initiation, and unwillingness to participate in the Access Program. Patients participating in the Program received medication and healthcare at multiple public and private hospitals in different cities throughout Lebanon.
Data collection
An Axios Program Manager collected patient data at the time of entry into the Drug Access Program and throughout patient treatment and prospective follow-up. All information from patient files was extracted anonymously from medical program reports, and no information was collected directly from patients. Data were collected for sex, age, cancer diagnosis, cancer drugs, status of the hospital where the patient was treated (public vs private; university vs nonuniversity hospital, urban vs rural location), number of physicians at the hospital, and cash flow facilitation for the patient. The time of program enrollment was collected and categorized as before 1 January 2019 or after 1 January 2019, and governorate MPI was collected and characterized as 2019 or 2021 (i.e., before and after the onset of the economic and social crises). For the purposes of the study, relevant data were accessed from 1 January 22 to 30 June 2022.
The collected data were evaluated in the context of the primary outcome of patient survival in patients who remained on their cancer medication compared with patients who stopped treatment due to major adverse events, lack of clinical response, therapeutic escape with disease progression or patient death. Because drug dispensing and administrative monitoring were systematically recorded by the Access Program, all study participants had a documented last contact (death, discontinuation or ongoing treatment), and none were lost to follow-up during the study period.
Clinical staging, tumor burden and comorbidity data were not collected routinely in the Program’s dataset. Our analyses were adjusted for covariates available for all participants (sex, cancer type, enrollment period, governorate-level MPI and hospital staffing), and the findings of these analyses are interpreted as associations.
Multidimensional poverty index (MPI)
Multidimensional poverty was assessed using the World Bank’s Multidimensional Poverty Measure [28]. MPI was stratified by the five governorates within Lebanon (Beirut, Bekaa, Mount Lebanon, North and South) and by year (2019 or 2021, i.e., before and after the onset of the economic crisis).
Statistical analyses
Descriptive statistics were computed for the characteristics of patients included in the Program and are calculated as mean and standard deviation (SD), median (M) and range (R) for quantitative variables, and as percentage for qualitative variables. Chi-square test was used for qualitative data comparisons; ANOVA test was used for quantitative comparisons.
Overall survival time was measured from Program enrollment to death from any cause. Patients for whom no death was recorded were censored at their last follow-up contact or Program exit to determine the cause of discontinuation (e.g., disease progression or adverse events). In a small number of cases, data for specific variables were not available for all patients. In these cases, the patients with missing data were not included in the analysis of the variable.
For interpretability, MPI effects were expressed per 0.1-unit increase, corresponding to the approximate differences observed between Lebanese governorates.
The Kaplan–Meier method was used to obtain the probability of overall survival. Statistical differences among the two groups (survivors and not survivors at end point) were tested using log-rank tests.
Multivariate Cox proportional-hazard model was fitted to identify predictive factors of survival. All variables tested in univariate analysis were included in the Cox models. Hazard-ratios (HRs) and 95% confidence intervals (CIs) were calculated for each variable. For all analyses, a significance level of ≤0.05 was used. Statistical analyses were performed using Excel Stat (Addinsoft). Model fit was summarized using the Akaike information criterion, and model discrimination was assessed using Harrell’s C-statistic. These measures illustrate adequate Cox model fit and moderate discrimination.
A robustness analysis was conducted using the rate-based model with log-exposure offset (approximating a piecewise-exponential hazard), yielding effect estimates consistent in direction with the main analysis. Additionally, variance inflation factors (VIFs) were calculated for all covariates (enrollment period, cancer type, hospital staffing, governorate-level MPI, sex), and no problematic multicollinearity was detected (all VIFs <2).
Results
A total of 613 patients were enrolled in the Program between January 2019 and December 2020. Of the 613 patients, 244 (39.8%) remained on treatment throughout the study, 87 (14.2%) died, and 282 (46.0%) discontinued treatment due to lack of clinical response or major adverse events. No patients were lost to follow-up. Baseline characteristics for patients, hospitals and governorate MPI are presented in Table 1. Mean patient age was 58.5 years (SD = 12.3) and the sex-ratio of males to females was 0.15. A total of 50 hospitals provided cancer care to patients in the Program, with a mean of 9.3 patients (SD = 4.2, R = 1–118) per hospital; 28 hospitals provided care to fewer than five patients enrolled in the program. A total of 86 physicians provided care to Program participants, with a mean of 19.1 patients (SD = 5.6, R = 1–50) per physician.
| Total (n = 613) | Beirut (n = 113) | Bekaa (n = 25) | Mount Lebanon (n = 373) | North (n = 52) | South (n = 50) | p-value | |
|---|---|---|---|---|---|---|---|
| Patients characteristics | |||||||
| Mean age (SD) | 58.5 (12.3) | 59.5 (12.2) | 57.0 (11.7) | 58.7 (12.5) | 55.8 (12.8) | 58.9 (±11.1) | 0.45 |
| Gender, % | |||||||
| Female | 87.3 | 90.3 | 92.0 | 87.1 | 88.5 | 78.0 | 0.25 |
| Male | 12.7 | 9.7 | 8.0 | 12.9 | 11.5 | 22.0 | |
| Cancer diagnosis % | |||||||
| Breast cancer | 79.3 | 81.4 | 88.0 | 77.5 | 84.6 | 78.0 | 0.81 |
| Renal cancer | 10.6 | 10.6 | 8.0 | 11.3 | 5.8 | 12.0 | |
| Lung cancer | 7.3 | 6.2 | 4.0 | 8.6 | 35.8 | 4.0 | |
| Other cancer | 2.8 | 1.8 | 0.0 | 2.7 | 3.8 | 6.0 | |
| Drug | |||||||
| Palbociclib | 79.3 | 81.4 | 88.0 | 77.5 | 84.6 | 78.0 | 0.76 |
| Crizotinib | 13.4 | 12.4 | 8.0 | 13.9 | 9.6 | 18.0 | |
| Sunitinib | 7.3 | 6.2 | 4.0 | 8.6 | 5.8 | 4.0 | |
| Time of enrollment | |||||||
| Before 1 Nov 2019 | 71.3 | 69.9 | 72.0 | 72.7 | 67.3 | 68.0 | 0.89 |
| After 1 Nov 2019 | 28.7 | 30.1 | 28.0 | 27.3 | 32.7 | 32.0 | |
| Cash-flow facilitation | |||||||
| No | 51.1 | 44.2 | 60.0 | 48.8 | 59.6 | 70.0 | 0.01 |
| Yes | 48.9 | 55.8 | 40.0 | 51.2 | 40.4 | 30.0 | |
| Hospital characteristics | |||||||
| Hospital status | |||||||
| Public | 70.5 | 78.8 | 72.0 | 71.0 | 48.1 | 70.0 | 0.003 |
| Private | 29.5 | 21.2 | 28.0 | 29.0 | 51.9 | 30.0 | |
| University hospital | |||||||
| University | 69.3 | 78.8 | 72.0 | 71.0 | 48.1 | 56.0 | 0.0001 |
| Nonuniversity | 30.7 | 21.2 | 28.0 | 29.0 | 51.9 | 44.0 | |
| Location status | |||||||
| Urban | 79.0 | 100.0 | 60.0 | 84.5 | 36.5 | 44.0 | 0.0001 |
| Rural | 21.0 | 0.0 | 40.0 | 15.5 | 63.5 | 56.0 | |
| MD/hospital (SD), n | 5.0 (2.0) | 5.0 (2.0) | 6.0 (1.0) | 5.0 (2.0) | 6.0 (4.0) | 2.0 (1.0) | 0.07 |
| MD/hospital median, n | |||||||
| ≤5 | 58.1 | 62.8 | 36.0 | 58.2 | 40.4 | 76.0 | 0.001 |
| >5 | 41.9 | 37.2 | 64.0 | 41.8 | 59.6 | 24.0 | |
| Governorate MPI | |||||||
| MPI (2019) | 0.09 | 0.10 | 0.15 | 0.08 | 0.11 | 0.10 | – |
| MPI (2021) | 0.23 | 0.22 | 0.30 | 0.22 | 0.26 | 0.27 | |
| Change in MPI 2019–2021 | 0.14 | 0.12 | 0.15 | 0.15 | 0.15 | 0.17 | |
MPI: Multidimensional Poverty Measure; MD: Medical doctor; Nov: November; SD: Standard deviation.
Cancer diagnosis and treatment are shown in Table 1. Mean treatment duration for patients who remained on their cancer medication for the duration of the study was 30.7 months (SD = 10.2) compared with 11.5 months (SD = 9.9) for patients who discontinued treatment (p < 0.0004).
The country-level and governorate-specific numerical MPI values, all of which increased from 2019 to 2021, are summarized in Table 1. The country-level increase in MPI on a percentage basis between 2019 and 2021 was 155.6%. Governorate-specific MPI increases on a percentage basis were Beirut, 120.0%; Bekaa: 100.0%; Mount Lebanon, 175.0%; North, 136.4%; and South 170.0%. MPI was significantly higher in urban hospitals compared with rural hospitals in 2019 (0.088 vs 0.0096, respectively, p < 0.0004) and was significantly lower in 2021 (0.229 vs 0.242, p < 0.0006). Each 0.1-unit increase in 2019 MPI was associated with an almost threefold higher mortality rate (adjusted HR: 2.88; 95% CI: 0.95–8.77; p = 0.06), underscoring the adverse impact of contextual deprivation on survival. Evaluation of the interaction between MPI and pre-/post-crisis enrollment found that the interaction term was not statistically significant, and the direction of the effect was consistent with the main effects.
Figure 1 shows the probability of survival according to time of Access Program enrollment (before vs after onset of the 2019 crisis). Survival probability was lower for patients enrolled after the start of the 2019 crisis who remained on treatment (survival without dropout), compared with patients enrolled prior to the crisis (p = 0.06). No significant differences in survival before versus after 2019 were found when stratifying results based on cancer type (breast cancer, p = 0.22; renal cancer, p = 0.23; lung cancer, p = 0.33) (Supplementary Figures 1–3).
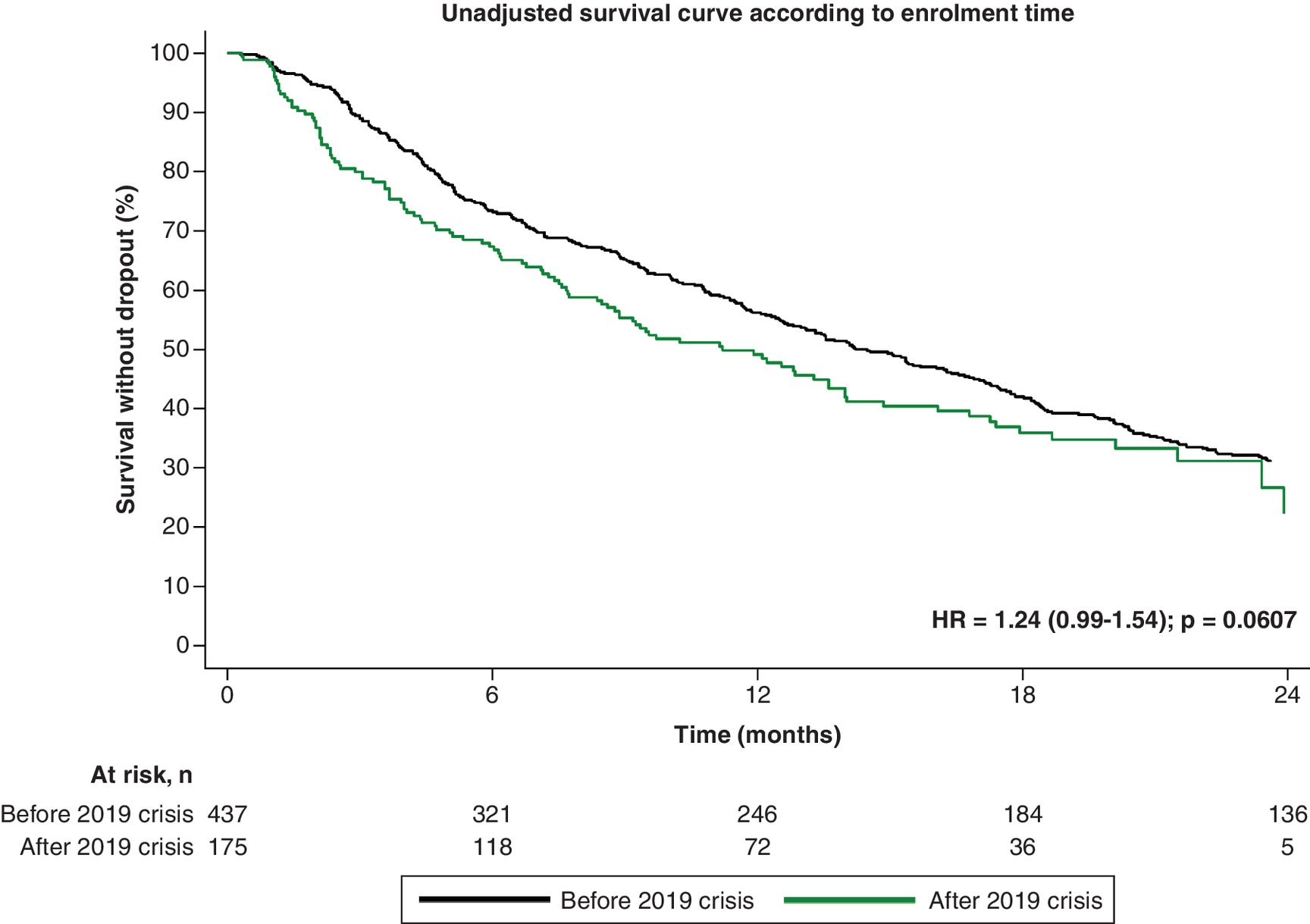
Figure 1. Probability of survival* according to time of Access Program enrollment, according the social-economic crisis (before vs after 2019).
*Stratified by cancer type (breast, renal, and lung cancer).
Univariate analysis found that gender, type of cancer, prescribed drug, Program enrollment after the onset of the social crisis, fewer than five physicians per hospital, and MPI value in 2019 were significant predictive factors of survival (Table 2). In multivariate Cox proportional hazard model, prescribed drug, enrollment before the 2019 crisis, fewer than five physicians per hospital, and living in multidimensional poverty in 2019 were significantly associated with survival (Table 2).
| Patients characteristics | n | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|---|
| HR (95% CI) | p-value | HR (95% CI) | p-value | ||
| Age | 602 | 0.99 (0.98–1.00) | 0.99 (0.98–1.01) | 0.34 | |
| Gender | |||||
| Female | 534 | ref | 0.01 | ||
| Male | 78 | 1.59 (1.10–2.32) | |||
| Cancer diagnosis | |||||
| Breast cancer | 485 | ref | <0.0004 | ||
| Renal cancer | 65 | 1.64 (1.53–1.76) | |||
| Lung cancer | 45 | 1.42 (1.05–1.94) | |||
| Other cancer | 17 | 0.92 (0.48–1.76) | |||
| Drug | |||||
| Palbociclib | 485 | ref | <0.0004 | ref | <0.0004 |
| Crizotinib | 82 | 1.44 (1.24–1.67) | 1.49 (1.22–1.83) | ||
| Sunitinib | 45 | 1.42 (1.04–1.95) | 1.41 (1.01–1.97) | ||
| Time of enrollment | |||||
| Before 1 Nov 2019 | 437 | ref | 0.002 | ref | 0.004 |
| After 1 Nov 2019 | 175 | 1.24 (1.08–1.41) | 1.24 (1.07–1.44) | ||
| Cash-flow facilitation | |||||
| No | 312 | ref | 0.40 | ||
| Yes | 300 | 0.94 (0.83–1.08) | |||
| Hospital characteristics | |||||
| Hospital status | |||||
| Public | 431 | ref | 0.37 | ||
| Private | 181 | 1.14 (0.86–1.49) | |||
| University hospital | |||||
| University | 424 | ref | 0.54 | ||
| Nonuniversity | 188 | 1.11 (0.80–1.53) | |||
| Location status | |||||
| Urban | 483 | ref | 0.14 | ||
| Rural | 129 | 1.09 (0.97–1.22) | |||
| MD/hospital (SD), | 612 | ||||
| MD/hospital median, n | 1.01 (0.99–1.03) | 0.11 | |||
| ≤5 | 355 | ref | 0.01 | ref | 0.04 |
| >5 | 257 | 1.14 (1.03–1.26) | 1.11 (1.00–1.23) | ||
| MPI Governorate | |||||
| MPI (2019) | 612 | 1.75 (1.42–2.16) | <0.0004 | 1.69 (1.30–2.20) | <0.0004 |
| MPI (2021) | 612 | 1.37 (0.96–1.97) | 0.08 | ||
| Change in MPI 2019–2021 | 612 | 0.80 (0.40–1.62) | 0.54 | ||
†
Stratified by cancer type (breast, renal, and lung cancer).
CI: Confidence interval; MD: Medical doctor; MPI: Multidimensional Poverty Measure; Nov: November; SD: standard deviation.
Discussion
The results of this study, which show a trend toward improved survival for patients enrolled in the Access Program prior to the onset of socioeconomic crisis, add to the body of data that associate economic crises with negative impacts on health outcomes. Even when hospital, physician and access to medication remained constant, our results continued to show an association between survival and pre-/post-crisis Program enrollment.
Multivariate analysis identified four factors associated with improved survival: treatment with palbociclib for breast cancer, enrollment in the Access Program prior to the liquidity crisis (1 January 2019), treatment at a hospital with fewer than five physicians, and lower 2019 MPI. The association of palbociclib treatment with improved survival is likely due to the fact that nearly all patients receiving palbociclib had breast cancer, which has better survival outcomes than lung or renal cancer. Interestingly, even though palbociclib, crizotinib and sunitinib were largely used in an indication-specific manner (for breast, renal and lung cancer, respectively). This analysis did not identify an association between breast cancer diagnosis and increased survival compared with other cancer types, even though the population of patients receiving palbociclib and those with breast cancer were largely identical.
In this study, physician, hospital and access to cancer medication remained constant before/after the onset of the crisis, while other aspects of patients' lives changed (displacement from area of care center, difficulty in traveling to appointments, increased stress, etc.). In this context, our finding that pre-crisis enrollment is associated with improved survival suggests that MPI factors have important impacts on survival.
A higher 2019 deprivation index was also associated with reduced survival. This suggests that reduced survival for patients enrolled in the program after the crisis began is likely associated with increased poverty. Poverty would be expected to negatively impact patients’ ability to attend appointments, maintain proper nutrition and stress levels, all of which would likely have a negative impact on health outcomes. Four general services indicators of a proposed MPI for Lebanon (electricity, drinking water, sanitation and waste collection) [27] would all be expected to impact health outcomes for cancer patients participating in the Access Program even if their cancer therapy remained unaffected by the liquidity crisis. It should be noted that the affordability of the medication provided through the Access Program was not modified during this period, as drug costs were largely reimbursed. This further underscores the association of increased poverty with survival outcomes.
These findings add to the growing body of evidence underscoring the impact of economic crises and deprivation on health outcomes. Economic crises have been associated with increases in all-cause mortality as well as with specific health conditions, including respiratory infections, chronic liver disease, infant mortality, and suicide [16]. Government fiscal responses to economic crisis – including reductions in healthcare spending, increases in patients' co-payments, and deregulation of healthcare services – have been associated with deterioration of public health, increased rates of mental health issues, substance abuse, epidemics, suicide, decreases in self-rated health and increased mortality in some age groups – especially by cancer, as found in our study [18–21].
The health-related impacts of economic crises and privation is not limited to low- and middle-income countries. Austerity measures implemented across the European Union following the economic downturn that began in 2008 (the ‘Great Recession’) resulted in an increase in disparities in all health outcomes in 2010, which likely were due to an increase in socioeconomic inequalities [22]. Self-reported unmet medical needs also increased in European countries that reduced their health expenditures during the Great Recession [23].
Our findings also underscore the limitations of using income-based poverty assessments, which would likely not have been informative in this study. This is because income wasn't a factor in patients’ access to medication in the study and because income data in Lebanon are not reliable due to underreporting and tax evasion [29]. Similarly, a multivariate analysis of associations between multidimensional poverty, income poverty and youth depressive symptoms in Mexico, Colombia and South Africa found a significant association between multidimensional poverty and severity of depressive symptoms, but not between income and depressive symptoms [30].
The current study also found that treatment at a hospital with fewer than five physicians was associated with increased survival. This initially paradoxical association became less significant after adjustment and variable refinement, and should be interpreted cautiously. Possible explanations for this association include closer individualized care in smaller centers, differences in hospital case-mix or unmeasured contextual factors, such as urban–rural disparities in hospital burden and resources. These considerations highlight the need for cautious interpretation and underscore the importance of collecting more granular patient- and hospital-level data in future research. However, it should be noted that this finding is consistent with a trend observed in a prior study of patients in Egypt undergoing treatment for chronic bronchitis [31]. Reductions in mortality and 30-day readmission rates have also been reported for patients with heart failure treated at hospitals with more cardiologists or physicians per bed [32,33]. A lower bed number per medical staff has been associated with lower-than-expected mortality in acute care settings in England [34].
Outcomes for Lebanese patients with cancer are still a cause for concern given the ongoing nature of the liquidity crisis. Our results suggest that continued increases in MPI across Lebanon will have a correspondingly negative impact on survival for patients undergoing cancer therapy. They also suggest that improving socio-economic status may help to improve health outcomes and access to care and to reduce mortality. This previously has been demonstrated in an analysis of socioeconomic inequalities on cancer mortality in nine European countries during the Great Recession. This analysis found that, while disparities existed, they did not increase during the period of economic decline [35]. The authors suggest that this was due to the study being conducted in cities and metropolitan areas with strong public health components. This reinforces the importance of health system structure on the ability to mitigate adverse health outcomes during times of economic crises. Similarly, reducing out-of-pockets expenses and providing income replacement for the unemployed has been shown to mitigate loss of healthcare access during periods of recession [36].
Overall, our results align with the broader literature emphasizing the importance of absorbing shocks and sustaining essential services during crises on health system resilience [37–39]. The Lebanese experience illustrates how socioeconomic collapse can exacerbate existing inequities in cancer care, consistent with findings from other fragile and conflict-affected settings. These findings underscore the importance of embedding equity safeguards into crisis preparedness, including decentralization of oncology services and targeted financial protection.
Limitations
This study has several limitations. First, it included a relatively small study population that was followed for a limited period, and it was not powered to detect socio-demographic differences among patients. Significant differences were found despite the small sample size. Second, it focused on patient metrics, which do not provide insight into the impact of physician stress or hospital burden on survival of patients undergoing medical therapy for cancer. Third, it only evaluated a limited number of cancers and socioeconomic metrics, and it is possible that factors associated with survival in patients with other types of cancer or using different or additional socioeconomic assessments may differ from those identified here. Similarly, because data were retrospectively extracted from medical records, some clinical variables (e.g., disease stage and severity and comorbidities) may have been incompletely documented. Absence of these data could generate an information bias and/or confound the observed associations if these factors differed pre-/post 2019 or across governorates. However, survival status was systematically verified through the Program database, ensuring reliability of the main outcome.
The nonrandomized nature of the study also creates the opportunity for selection bias that could confound our results. We controlled for these potential biases by stratifying results by cancer type and conducting a robustness analysis. Another potential limitation is that MPI was assigned at the governorate level. This ecological measure may not reflect individual socioeconomic deprivation and could induce ecological bias. Additionally, our results identified an association between hospitals that had fewer physicians and improved survival, which is seemingly paradoxical. It should be noted that this analysis did not include several potentially confounding variables, such as hospital case mix, referral patterns and urban/rural context. Consequently, this finding could benefit from additional analysis and should not be over-interpreted.
Conclusion
Data from this study suggest that deprivation generated by an economic crisis has a negative impact on survival for patients treated for cancer in Lebanon. Our findings suggest that implementing specific health measures, (e.g., awareness campaigns, specific communication with patients designed to increase follow-up and decreasing poverty by improving relevant MPI indicators) may help alleviate the impact of economic crises on health outcomes. These results also highlight the potential impact of economic crisis on mortality in cancer patients and underscore the urgent need to evaluate and assess the health impacts of socioeconomic poverty in Lebanon and other countries with impoverished populations. This study and the growing body of evidence indicating that socioeconomic crisis leads to poor health outcomes, argue strongly for proactive and coordinated efforts to prevent – or respond rapidly and effectively – to these crises to mitigate the negative effects of poverty on health outcomes.
Mitigating socioeconomic barriers to oncology care during times of future crisis will require policies that prioritize decentralizing oncology services, supporting mobile outreach clinics and integrating social support such as transport vouchers and patient navigators. Protecting oncology drug budgets and linking access programs with social protection schemes could further enhance equity and resilience in cancer care during future crises.
Summary points
•
Since 2019, several events (an ongoing economic crisis, war in a neighboring country, severe wildfires, a massive explosion at a large port, the COVID-19 pandemic and political unrest) have negatively impacted Lebanon’s economy and made it difficult for patients to receive care.
•
Several studies have already identified associations between economic crises and worse outcomes across a variety of health metrics, including specific negative effects on cancer care and outcomes.
•
In addition to the effects of systemic economic crises, poverty at the individual level also impacts health outcomes. The multidimensional poverty level in Lebanon nearly doubled from 2019 to 2021, and the percentage of households deprived of healthcare over the same period grew from 9 to 33%.
•
Cancer patients participating in a drug access program between 2018 and 2020 that eliminated financial barriers continued to have access to their cancer medications, which enabled the evaluation of other factors (patient, physician, social determinants of health, etc.) that impact health outcomes for cancer patients during periods of economic crisis.
•
In this study we assessed the impact of economic and social crisis on access to care for cancer treatment in 613 cancer patients participating in the drug access program and identified factors that impacted survival for cancer patients who began treatment before the start of Lebanon’s economic crisis in 2019 and those who started treatment once the crisis had begun.
•
This study found that patients who began cancer treatment before the start of the 2019 crisis were more likely to survive than patients who started treatment in 2019 or 2020.
•
Other factors associated with being more likely to survive were treatment with a specific drug for breast cancer, treatment at a hospital with fewer than five physicians, and lower levels of poverty in 2019.
•
Study results show that deprivation generated by an economic crisis has a negative impact on survival for patients treated for cancer in Lebanon and the growing body of evidence indicating that socioeconomic crisis leads to poor health outcomes.
•
Our findings underscore the critical need to rapidly respond to economic crises to reduce the negative impact of poverty on health outcomes.
Author contributions
J Saba, A Sawsan, A Nofal, M Ammar, E Audureau and J Ladner were responsible for the study conception and design; M Rana, E Audureau, J Saba and J Ladner were responsible for the acquisition of data and data analysis; all authors critically reviewed and revised manuscript drafts; all authors have approved the final version of the manuscript for publication.
Acknowledgments
The authors give special thanks to S Seiler for editing and revision of the manuscript.
Financial disclosure
The authors received no financial and/or material support for this research or the creation of this work.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
Under the direction of authors, S Seiler provided writing assistance for the manuscript.
Ethical conduct of research
The Ethical Committee of Rouen University Hospital (CERDE-HLJ) approved the research (no. E2021-74). Patients provided written informed consent to enroll in the Access Program; research written consent was not required for collection of patient data because information from patient files was collected anonymously from medical reports, without collection of personal, patient-identifying information.
Data sharing statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable and justified request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary figures.docx)
- Download
- 37.15 KB
References
Papers of special note have been highlighted as: • of interest
1.
Elias F, Bou-Orm IR, Adib SM, Gebran S, Gebran A, Ammar W. Cost of oncology drugs in the Middle-Eastern country of Lebanon: an update (2014–2016). J. Glob. Oncol. 4, 1–7 (2018).
2.
Khachfe HH, Rahal Z, Sammouri J et al. Cancer in Lebanon: a review of incidence rates from 2008 to 2015 and projections till 2025. South Asian J. Cancer 9, 147–152 (2020).
• The top cancers in Lebanon are the breast, lung, colorectal, bladder and prostate. Lebanon had a steady incidence rate of cancer cases during the time of study.
3.
Salhab HA, Fares MY, Khachfe HH, Khachfe HM. Epidemiological study of lung cancer incidence in Lebanon. Medicina 55, 217 (2019).
4.
Yassoub R, Alameddine M, Saleh S. The path toward universal health coverage. Int. J. Health Serv. 47(2), 352–373 (2017).
5.
UNHCR. Global trends: forced displacement in 2019. Available from: https://www.unhcr.org/flagship-reports/globaltrends/globaltrends2019/
6.
Akik C, Asfahani F, Elghossain T et al. Healthcare system responses to non-communicable diseases' needs of Syrian refugees: the cases of Jordan and Lebanon. J. Migr. Health 6, 100136 (2022).
7.
Fleifel M, Abi Farraj K. The Lebanese healthcare crisis: an infinite calamity. Cureus 14(5), e25367 (2022).
8.
Nuwayhid I, Zurayk H. The political determinants of health and wellbeing in the Lebanese uprising. Lancet 394(10213), 1974–1975 (2019).
9.
Devi S. Economic crisis hits Lebanese health care. Lancet 395(10224), 548 (2020).
• The full impact of the economic crisis on public health would take time to become apparent, but it was a worrying sign that people were cutting back on their use of primary health care.
10.
Saliba AN, Taher AT. A land in agony: COVID-19, economic collapse, political corruption, and a deadly blast. Am. J. Hematol. 96, E1–E40 (2021).
11.
Kassab B, El Hachem C, Raad G, Cordahi C, Richa S. Effects of a multilayered crisis on psychiatric hospitalizations in a university hospital in Lebanon; a retrospective study. Psychiatry Res. 318, 114940 (2022).
12.
Mhanna M, El Zouki C-J, Chahine A, Obeid S, Hallit S. Dissociative experiences among Lebanese university students: association with mental health issues, the economic crisis, the COVID-19 pandemic, and the Beirut port explosion. PLoS ONE 17(11), e0277883 (2022).
13.
Jarroch R, Tajik B, Tuomainen T-P, Kauhanen J. Economic recession and the risk of cancer: a cohort study from Eastern Finland. J. Epidemiol. 32(8), 384–390 (2022).
14.
Petrovici I, Ionica M, Neagoe OC. Economic crisis: a factor the delayed diagnosis of breast cancer. Int. J. Environ. Res. Public Health 18(8), 3998 (2021).
15.
Maruthappu M, Watkins J, Noor AM et al. Economic downturns, universal health coverage, and cancer mortality in high-income and middle-income countries, 1990–2010: a longitudinal analysis. Lancet 388(10045), 684–695 (2016).
16.
Falagas ME, Vouloumanou EK, Mavros MN, Karageorgopoulos DE. Economic crises and mortality: a review of the literature. Int. J. Clin. Pract. 63(8), 1128–1135 (2009).
• Economic crises in less affluent countries are accompanied with the increase in all-cause mortality. Public health authorities should be aware of this issue and consider appropriate preventive and control measures.
17.
Benach J, Padilla-Pozo Á, Martínez-Herrera E et al. What do we know about the impact of economic recessions on mortality inequalities? A critical review. Soc. Sci. Med. 296, 114733 (2022).
• The economic recessions that occurred in the period 1980–2020 tended to increase mortality inequalities throughout the world. This strengthens the argument that those crises are especially detrimental to the health of the most vulnerable populations.
18.
Simou E, Koutsogeorgou E. Effects of the economic crisis on health and healthcare in Greece in the literature from 2009 to 2013: a systematic review. Health Policy 115(2–3), 111–119 (2014).
19.
Kondilis E, Giannakopoulos S, Gavana M, Ierodiakonou I, Waitzkin H, Benos A. Economic crisis, restrictive policies, and the population's health and health care: the Greek case. Am. J. Public Health 103(6), 973–979 (2013).
20.
Filippidis FT, Gerovasili V, Millett C, Tountas Y. Medium-term impact of the economic crisis on mortality, health-related behaviours and access to healthcare in Greece. Sci. Rep. 7, 46423 (2017).
21.
Vlachadis N, Vrachnis N, Ktenas E, Vlachadi M, Kornarou E. Mortality and the economic crisis in Greece. Lancet 383(9918), 691 (2014).
22.
Maynou L, Saez M. Economic crisis and health inequalities: evidence from the European Union. Int. J. Equity Health 15(1), 135 (2016).
23.
Torfs L, Adriaenssens S, Lagaert S, Willems S. The unequal effects of austerity measures between income-groups on the access to healthcare: a quasi-experimental approach. Int. J. Equity Health 20(1), 79 (2021).
24.
Raad E, Helou S, Hage K, Daou M, El Helou E. Cost of bladder cancer in Lebanon before and after the economic collapse: a probabilistic modeling study. Int. J. Equity Health 22(1), 77 (2023).
25.
Sifaki-Pistolla D, Chatzea VE, Mechili EA et al. Spatio-temporal variation of lung cancer in Crete, 1992–2013. Economic or health crisis? Int. J. Environ. Res. Public Health 19(19), 12161 (2022).
26.
Ennis KY, Chen MH, Smith GC et al. The impact of economic recession on the incidence and treatment of cancer. J. Cancer 6(8), 727–733 (2015).
• Highlights the broad implications of economic recessions on the welfare of people, ex-tending beyond income to health and cancer.
27.
United Nations Economic and Social Commission for Western Asia. Multidimensional poverty in Lebanon (2019–2021): painful reality and uncertain prospect. (2021). Available from: https://www.unescwa.org/publications/multidimensional-poverty-lebanon-2019-2021
28.
The World Bank. Multidimensional poverty measure. Available from: https://www.worldbank.org/en/topic/poverty/brief/multidimensional-poverty-measure
29.
Ashaal A, Bakri A. A multidimensional poverty analysis: evidence from Lebanese data. Int. J. Recent Tech. Eng. 7(6S5), 2277–3878 (2019).
30.
Zimmerman A, Lund C, Araya R et al. The relationship between multidimensional poverty, income poverty and youth depressive symptoms: cross-sectional evidence from Mexico, South Africa and Colombia. BMJ Glob. Health 7(1), e006960 (2022).
31.
Ladner J, El Badrawy M, Nofal A, Saba J, Audureau E. A cohort study of medication adherence among patients with chronic obstructive pulmonary disease in Egypt. NPJ Prim. Care. Respir. Med. 30(1), 31 (2020).
• Pharmacists are well positioned to play a role as an essential public health resource to improve adherence as well as social support to improve adherence to long-term therapy in chronic obstructive pulmonary disease (COPD) diseases in low- and middle-income countries.
32.
Lee JE, Park EC, Jang SY, Lee SA, Choy YS, Kim TH. Effects of physician volume on readmission and mortality in elderly patients with heart failure: nationwide cohort study. Yonsei Med. J. 59(2), 243–251 (2018).
33.
Kanaoka K, Okayama S, Nakai M et al. Number of cardiologists per cardiovascular beds and in-hospital mortality for acute heart failure: a nationwide study in Japan. J. Am. Heart Assoc. 8(18), e012282 (2019).
34.
Harvey PR, Trudgill NJ. The association between physician staff numbers and mortality in English hospitals. E. Clin. Med. 32, 100709 (2021).
35.
Palència L, Ferrando J, Marí-Dell'Olmo M et al. Socio-economic inequalities on cancer mortality in nine European areas: the effect of the last economic recession. Cancer Epidemiol. 69, 101827 (2020).
36.
Madureira-Lima J, Reeves A, Clair A, Stuckler D. The Great Recession and inequalities in access to health care: a study of unemployment and unmet medical need in Europe in the economic crisis. Int. J. Epidemiol. 47(1), 58–68 (2018).
37.
Blanchet K, Nam SL, Ramalingam B, Pozo-Martin F. Governance and capacity to manage resilience of health systems: towards a new conceptual framework. Int. J. Health Pol. Manag. 6, 431–435 (2017).
38.
Kruk ME, Ling EJ, Bitton A et al. Building resilient health systems: a proposal for a resilience index. Brit. Med. J. 357, j2323 (2017).
39.
O'Neill J, Tabish H, Welch V et al. Applying an equity lens to interventions: using PROGRESS-Plus. J. Clin. Epidemiol. 67, 56–64 (2014).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 17 June 2025
Accepted: 17 December 2025
Published online: 21 January 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The impact of socioeconomic crisis on cancer patient outcomes in Lebanon, 2018–2020. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0099
Export citation
Select the citation format you wish to export for this article or chapter.