Comparison of deep prostate-specific antigen response in Black patients with metastatic castration-sensitive prostate cancer initiated on apalutamide or enzalutamide
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: There is limited real-world evidence about prostate-specific antigen (PSA) response to androgen receptor pathway inhibitor treatment in Black patients with metastatic castration-sensitive prostate cancer (mCSPC). This study compared PSA90 (≥90% reduction from baseline PSA level) between apalutamide and enzalutamide among Black patients with mCSPC. Materials & methods: Electronic medical record data (Precision Point Specialty Analytics) were linked to claims data (Komodo Research Database) and used to select cohorts of Black patients with mCSPC treated with either apalutamide or enzalutamide. Inverse probability of treatment weighting was used to balance treatment cohorts. PSA90 response was assessed using weighted Kaplan–Meier curves and hazard ratios with 95% CIs. Results: The study included 451 patients (apalutamide: 230, enzalutamide: 221) with balanced baseline characteristics after inverse probability of treatment weighting. Patients treated with apalutamide had a 42% higher rate of PSA90 response within 6 months post-index compared with those treated with enzalutamide (hazard ratio: 1.42, 95% CI: 1.06, 1.91; p = 0.020). Median time to first PSA90 response was shorter among patients treated with apalutamide (3.3 months) compared with enzalutamide (5.5 months). Conclusion: In Black patients with mCSPC, apalutamide led to faster and significantly deeper PSA responses than enzalutamide, suggesting potential clinical advantages in optimizing early treatment response in this population. Future research should assess PSA90 as a prognostic indicator of overall survival among Black patients.
Plain language summary
What is already known about this topic?
Apalutamide and enzalutamide are two treatments that can be used along with standard hormone therapy to treat patients with metastatic castration-sensitive prostate cancer (mCSPC). A blood protein called prostate-specific antigen (PSA) can be used to measure how well patients respond to treatment with a drop of 90% or more indicating that the treatment is highly effective. Black patients with mCSPC often have worse outcomes compared with White patients with mCSPC.
What was the aim of this research?
In this study, patient medical records and insurance claims information were used to study how many patients had a drop of 90% or more in their PSA levels within 6 months after starting treatment with either apalutamide or enzalutamide.
What are the results?
The results showed that more patients treated with apalutamide had a 90% drop in PSA levels compared with patients treated with enzalutamide. This drop also happened faster for patients treated with apalutamide compared with patients treated with enzalutamide.
Why is this research important?
This study helps to fill a gap in understanding how well these treatments work in Black patients with mCSPC. A strong and early drop in PSA levels is associated with better long-term results for patients, and these findings may help doctors make treatment decisions for Black patients with mCSPC.
Background
Prostate cancer (PC) is the most commonly diagnosed cancer among men, with an estimated 313,780 new cases and 35,770 deaths in the US in 2025 [1]. PC disproportionately affects Black men, who experience both higher incidence and mortality rates compared with White men. These disparities within the Black population stem from a combination of earlier disease presentation, more aggressive disease tumor biology at diagnosis, lower rates of cancer screening, and reduced access to timely and effective treatments [1–3]. This disproportionate burden underscores the critical need to examine the effects of PC within the Black population, who face greater barriers to care and worse outcomes.
Most cases of PC are diagnosed during the localized stage when PC is confined to the prostate; however, some patients may experience progression to metastatic castration-sensitive PC (mCSPC), also referred to as metastatic hormone-sensitive prostate cancer (mHSPC), despite treatment, which is associated with worse survival outcomes [4]. Guideline recommended treatment for mCSPC involves the use of androgen deprivation therapy (ADT), with the addition of androgen receptor pathway inhibitors (ARPIs) with ADT treatment recently shown to improve survival outcomes [5]. Apalutamide and enzalutamide are next generation ARPIs that received US FDA approval in 2019 for use in patients with mCSPC based on results of the TITAN and ARCHES trials, respectively [6–9]. Both Phase III randomized, double-blind, placebo-controlled trials demonstrated that adding either apalutamide or enzalutamide to ADT improved radiographic progression free survival in patients with mCSPC compared with ADT alone.
Prostate-specific antigen (PSA) levels are commonly used to evaluate PC treatment response, with PSA90 responses (i.e., ≥90% reduction in PSA from pretreatment levels) associated with superior long-term outcomes [10–12]. Previous real-world studies have evaluated PSA90 responses to ARPI treatment in patients with mCSPC [13,14]; however, there is limited real-world data among Black patients with mCSPC. Only one previous study has evaluated real-world PSA responses among Black patients with mCSPC following ARPI treatment, which reported that approximately 75% of patients achieved a PSA90 response following administration of apalutamide [15]. Furthermore, no previous real-world studies have compared PSA responses between ARPIs among Black patients with mCSPC.
Given the underrepresentation of Black patients in clinical trials [2] and the poor survival outcomes observed for Black patients with PC [16], a better understanding of real-world ARPI treatment response within this subpopulation of patients with mCSPC is critical for optimizing treatment for patients with mCSPC. Therefore, this study aimed to compare real-world PSA responses between Black patients with mCSPC treated with either apalutamide or enzalutamide.
Materials & methods
Data source
Demographic and clinical variables used in this study were obtained from the Precision Point Specialty (PPS) Analytics database, which is composed of electronic medical record (EMR) data routinely collected in US community-based urology practices (1 February 2017 to 31 December 2023). Available PPS clinical data included laboratory test results, details of PC-related medications and procedures, dispensing information for next-generation ARPIs, and International Classifications of Disease, 9th/10th Revision, Clinical Modification (ICD-9/10-CM) diagnostic codes.
The PPS dataset was linked to the Komodo Research Database (KRD), which contains insurance claims for over 330 million US patients covered by Commercial, Medicaid, and Medicare insurers (1 January 2016 to 31 December 2023). The KRD includes both open and closed claims with information on prescription fills, inpatient and outpatient procedures, and billing and reimbursements. The two databases were linked by Datavant using patent-pending de-identification technology which supplements patient information with an encrypted token that cannot be reversed to reveal the original information. Data regarding patients' race was obtained from the KRD from a Race and Ethnicity field, which largely uses self-reported data supplemented with modeling information that is highly concordant with 2020 census data. Institutional review board approval for this study was not required as all unlinked and linked data were de-identified and Health Insurance Portability and Accountability Act compliant.
Study design
This was a retrospective longitudinal cohort study. The index date was defined as the date of the first record for apalutamide or enzalutamide, determined by the earliest of either the first in-office dispensing in PPS or the first paid pharmacy claim in the KRD on or after 16 December 2019 (the latter date of apalutamide and enzalutamide’s mCSPC FDA approval [6,7]). Patients were assigned to mutually exclusive treatment cohorts of apalutamide or enzalutamide based on the ARPI initiated on the index date (Figure 1). The baseline period was composed of the 12 months prior to the index date. The observation period spanned from the index date until the earliest of index treatment discontinuation (defined by a 90-day treatment gap), initiation of a new ARPI (i.e., treatment switch, excluding first-generation antiandrogens), initiation of a radiopharmaceutical, end of clinical activity in PPS, or the end of open insurance claim activity in the KRD (i.e., 31 December 2023).
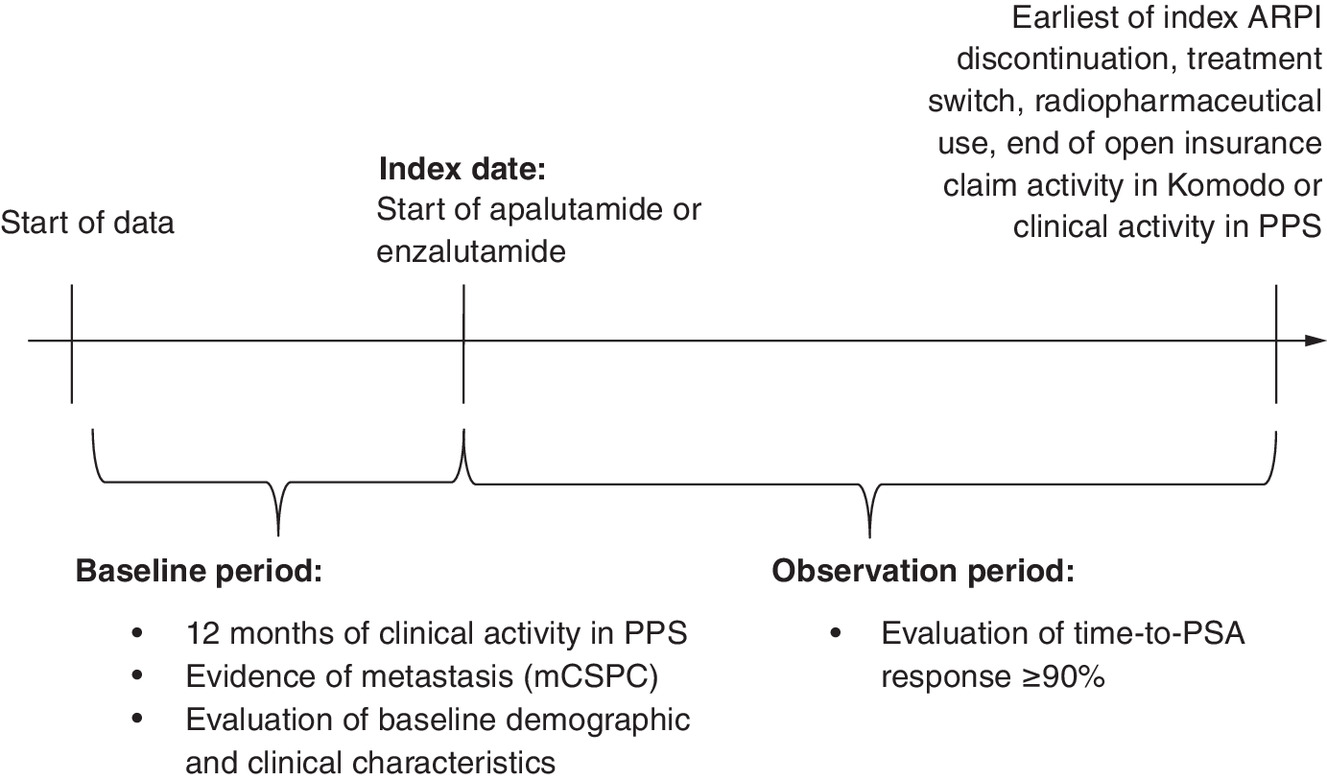
Figure 1. Study Design.
ARPI: Androgen receptor pathway inhibitor; mCSPC: Metastatic castration-sensitive prostate cancer; PPS: Precision Point Specialty; PSA: Prostate-specific antigen.
Sample selection
Black adult patients were required to have ≥1 pharmacy claim or dispensation for apalutamide or enzalutamide, confirmed metastasis on or prior to the index date, ≥1 PSA measurement in the 13-week period prior to and including the index date, and ≥12 months of clinical activity in PPS prior to the index date. Patients were excluded if they initiated the index ARPI prior to 16 December 2019, had a prescription for an ARPI other than the index ARPI prior to or on the index date, had evidence of castration resistance prior to or on the index date, or received treatment with radiopharmaceuticals prior to or on the index date. Previously published algorithms based on diagnosis codes and clinical indicators were used to assess metastatic disease and castration resistance [17]. Patients in this study were not required to have concurrent ADT use.
Study measures & outcomes
The primary study outcome was the proportion of patients who achieved a ≥90% reduction in PSA (i.e., PSA90 response) from the most recent baseline PSA observed. Baseline PSA was defined as the most recent value recorded within the 13 weeks prior to and including the index date, and PSA90 response was determined using a follow-up PSA measurement obtained within 6 months after the index date. The proportion of patients with a PSA90 response within the entire observation period (i.e., not restricting to the first 6 months post-index) and the median time-to-first PSA90 response were also reported. Post-index PSA measurement patterns during the observation period were also evaluated.
Baseline demographic and clinical characteristics included age, race, payer type, geographic region, index year, time between metastasis and the index date, time between initial PC diagnosis and the index date, metastasis type (nodal, bone or visceral), prior first-generation antiandrogen, ADT or chemotherapy use, baseline PSA and testosterone levels, and initial Gleason score.
Statistical analyses
The null hypothesis for the study was that there were no differences in PSA90 response rates by 6 months post-index between Black patients treated with apalutamide or enzalutamide. The alternative hypothesis was that there was a difference in PSA90 response rates by 6 months post-index between patients treated with apalutamide or enzalutamide. Potential confounders in both patient cohorts were balanced using inverse probability of treatment weighting (IPTW). Probability estimates from logistic regression models were used to generate propensity scores (PSs), in which the dependent variable was apalutamide initiation. The logistic regression model included the following independent variables: age, geographic region, index year, payer type, time between metastasis and the index date, time between initial PC diagnosis and the index date, metastasis type, de novo metastatic PC, prior ADT use, first-generation antiandrogen use, chemotherapy use, most recent baseline PSA level, most recent baseline testosterone level, and earliest Gleason score. Patients treated with apalutamide were attributed a weight of 1/PS and patients treated with enzalutamide were attributed a weight of 1/(1-PS), with weights normalized using the mean weight of each respective cohort [18]. Weights were truncated at the 95th percentile to reduce the impact of extreme weights. No patients were removed from the study analyses following IPTW weighting. Standardized differences were used to assess the balance of baseline characteristics between patients treated with apalutamide and enzalutamide in both the unweighted and weighted cohorts (differences <10% were considered well balanced) [19].
The proportion of patients treated with apalutamide and enzalutamide who achieved a PSA90 response by 6 months post-index was described using weighted Kaplan–Meier analyses. The association between index ARPI and PSA90 response by 6 months (primary outcome) and over the entire observation period (exploratory outcome) was assessed using hazard ratios (HRs) and 95% CIs calculated using weighted Cox proportional hazards models. All analyses were conducted using SAS Enterprise Guide software version 7.1 (SAS Institute, NC, USA).
Results
Study sample
Overall, 230 patients treated with apalutamide and 221 patients treated with enzalutamide were included in the study (Figure 2).
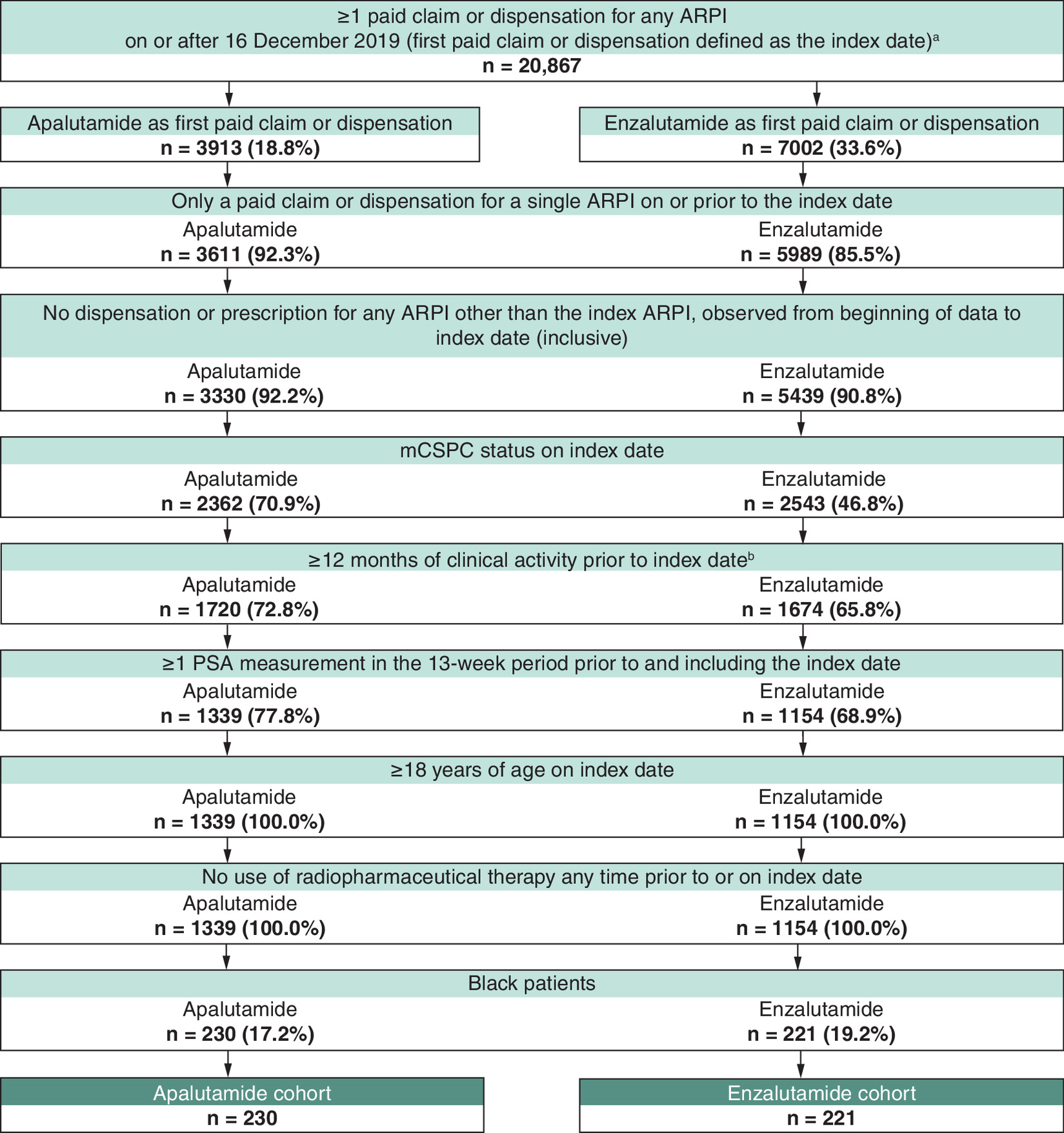
Figure 2. Patient identification flowchart.
aThe US FDA approved enzalutamide as treatment for mCSPC on 16 December 2019.
bClinical activity was defined as the period from the first to the last record in the Precision Point Specialty Analytics electronic health record database.
ARPI: Androgen receptor pathway inhibitor; mCSPC: Metastatic castration-sensitive prostate cancer; PSA: Prostate-specific antigen.
Baseline characteristics
After IPTW, baseline demographic and clinical characteristics were generally well-balanced between Black patients with mCSPC who received treatment with either apalutamide or enzalutamide (Table 1). The mean age was 71.0 years for patients treated with apalutamide and 71.4 years for patients treated with enzalutamide. Most patients were from the South region (apalutamide: 68.4%; enzalutamide: 66.1%) and insured with Medicare (apalutamide: 76.5%; enzalutamide: 78.1%). The time between metastatic diagnosis and initiation of the index ARPI was similar between patients treated with apalutamide and enzalutamide, with a median time of 3.4 months for both cohorts. The mean baseline PSA level was 23.6 μg/l for patients who received treatment with apalutamide and 23.4 μg/l for patients who received treatment with enzalutamide.
| Non-weighted population | IPTW population† | |||||
|---|---|---|---|---|---|---|
| Apalutamide (n = 230) | Enzalutamide (n = 221) | Standardized difference (%) | Apalutamide (n = 230) | Enzalutamide (n = 221) | Standardized difference (%) | |
| Age, mean ± SD [median] | 70.3 ± 8.6 [69.5] | 72.4 ± 8.6 [71.0] | 24.7 | 71.0 ± 8.5 [70.0] | 71.4 ± 8.6 [71.0] | 4.7 |
| Age group, n (%) | ||||||
| ≤60 | 32 (13.9) | 16 (7.2) | 21.8 | 26 (11.2) | 21 (9.7) | 4.9 |
| 61–70 | 90 (39.1) | 81 (36.7) | 5.1 | 90 (39.3) | 85 (38.4) | 1.9 |
| 71–80 | 79 (34.3) | 81 (36.7) | 4.8 | 80 (34.8) | 79 (35.9) | 2.3 |
| ≥81 | 29 (12.6) | 43 (19.5) | 18.8 | 34 (14.7) | 35 (16.0) | 3.7 |
| Geographic region‡, n (%) | ||||||
| South | 165 (71.7) | 135 (61.1) | 22.7 | 157 (68.4) | 146 (66.1) | 4.8 |
| Midwest | 45 (19.6) | 62 (28.1) | 20.0 | 52 (22.6) | 54 (24.5) | 4.4 |
| Northeast | 18 (7.8) | 20 (9.0) | 4.4 | 18 (7.8) | 18 (8.0) | 0.9 |
| West | 2 (0.9) | 4 (1.8) | 8.2 | 3 (1.2) | 3 (1.3) | 1.3 |
| Payer type, n (%) | ||||||
| Medicare | 172 (74.8) | 180 (81.4) | 16.2 | 176 (76.5) | 173 (78.1) | 3.7 |
| Commercial | 48 (20.9) | 36 (16.3) | 11.8 | 46 (19.8) | 43 (19.3) | 1.2 |
| Medicaid | 9 (3.9) | 5 (2.3) | 9.6 | 8 (3.3) | 6 (2.5) | 4.6 |
| Unknown | 1 (0.4) | 0 (0.0) | 0.0 | 1 (0.3) | 0 (0.0) | 0.0 |
| Index year, n (%) | ||||||
| 2019–2020 | 43 (18.7) | 63 (28.5) | 23.3 | 49 (21.3) | 51 (23.1) | 4.4 |
| 2021 | 49 (21.3) | 60 (27.1) | 13.7 | 52 (22.8) | 52 (23.7) | 2.2 |
| 2022 | 78 (33.9) | 50 (22.6) | 25.3 | 70 (30.4) | 63 (28.4) | 4.4 |
| 2023 | 60 (26.1) | 48 (21.7) | 10.3 | 59 (25.6) | 55 (24.8) | 1.8 |
| Time between metastasis and index date, months, mean ± SD [median] | 9.2 ± 17.5 [3.0] | 13.1 ± 17.1 [6.0] | 22.8 | 11.3 ± 20.0 [3.4] | 11.8 ± 16.9 [3.4] | 2.6 |
| Time between PC diagnosis and index date, months, mean ± SD [median] | 51.1 ± 45.4 [45.4] | 56.3 ± 46.7 [47.5] | 11.3 | 52.7 ± 45.5 [47.6] | 54.0 ± 46.4 [45.3] | 2.9 |
| Metastasis type§, n (%) | ||||||
| Bone | 146 (63.5) | 142 (64.3) | 1.6 | 147 (63.9) | 142 (64.1) | 0.3 |
| Nodal | 131 (57.0) | 113 (51.1) | 11.7 | 127 (55.2) | 117 (53.0) | 4.4 |
| Visceral | 36 (15.7) | 54 (24.4) | 22.1 | 41 (17.7) | 43 (19.3) | 4.0 |
| De novo metastatic PC¶, n (%) | 82 (35.7) | 74 (33.5) | 4.6 | 81 (35.4) | 76 (34.4) | 2.0 |
| Concurrent use of ADT with index ARPI#, n (%) | 218 (94.8) | 203 (91.9) | 11.7 | 216 (93.8) | 206 (93.3) | 2.4 |
| Prior use of ADT††, n (%) | 209 (90.9) | 191 (86.4) | 14.0 | 206 (89.4) | 197 (89.1) | 0.9 |
| Prior use of first generation ARPI‡‡, n (%) | 34 (14.8) | 39 (17.6) | 7.8 | 35 (15.0) | 34 (15.2) | 0.5 |
| Prior use of chemotherapy§§, n (%) | 3 (1.3) | 6 (2.7) | 10.1 | 4 (1.5) | 4 (1.9) | 2.8 |
| Baseline PSA level¶¶, μg/l, mean ± SD [median] | 22.9 ± 52.0 [3.3] | 24.8 ± 52.1 [2.4] | 3.6 | 23.6 ± 54.8 [2.7] | 23.4 ± 48.1 [2.7] | 0.3 |
| Baseline testosterone tests##, n (%) | 171 (74.3) | 137 (62.0) | 26.8 | 168 (73.3) | 143 (64.9) | 18.3 |
| Testosterone <1.735 nmol/l††† | 109 (63.7) | 97 (70.8) | 15.1 | 115 (68.0) | 96 (66.7) | 2.8 |
| Initial Gleason score‡‡‡, n (%) | ||||||
| ≤6 | 22 (9.6) | 24 (10.9) | 4.3 | 25 (11.0) | 24 (11.0) | 0.0 |
| 7 | 71 (30.9) | 48 (21.7) | 20.9 | 66 (28.8) | 60 (27.2) | 3.5 |
| 8 | 24 (10.4) | 42 (19.0) | 24.4 | 28 (12.2) | 31 (14.0) | 5.3 |
| 9 | 48 (20.9) | 43 (19.5) | 3.5 | 47 (20.5) | 45 (20.3) | 0.5 |
| 10 | 2 (0.9) | 4 (1.8) | 8.2 | 3 (1.2) | 3 (1.5) | 1.8 |
| Unknown | 63 (27.4) | 60 (27.1) | 0.5 | 61 (26.3) | 58 (26.1) | 0.6 |
†
The number of patients reported in this weighted population represents the sum of weights for the corresponding non-weighted patients, rounded to the nearest integer. The proportions displayed were calculated prior to the rounding and may be slightly different than if they were calculated based on rounded numbers.
‡
Geographic region was defined by US census areas.
§
Types of metastases were defined at any time prior to (and including) the index date. Types of metastases were not mutually exclusive.
¶
De novo metastatic PC was defined as ≤180 days between first observed PC diagnosis and date of metastasis.
#
Concurrent ADT use was defined as having a claim for any ADT medication from 180 days prior to 180 days after the index date.
††
Prior use of ADT medication was defined as any ADT administration at any time prior to (and excluding) the index date.
‡‡
Prior use of first-generation ARPI was defined as any prescription for bicalutamide, nilutamide or flutamide, at any time prior to (and excluding) the index date.
§§
Prior chemotherapy use was defined as any administration at any time prior to (and excluding) the index date.
¶¶
Baseline PSA was evaluated as the most recent value from 13 weeks pre-index up to, and including, the index date.
##
Testosterone testing was evaluated during the 12-month baseline period and included the index date, with the most recent value reported.
†††
Patients’ mCSPC status were evaluated using their records and baseline testosterone may not be synchronous with mCSPC designation.
‡‡‡
Gleason score was evaluated at any time prior to and including the index date.
ADT: Androgen deprivation therapy; ARPI: Androgen receptor pathway inhibitor; IPTW: Inverse probability of treatment weighting; mCSPC: Metastatic castration-sensitive prostate cancer; PC: Prostate cancer; PSA: Prostate-specific antigen; SD: Standard deviation.
PSA outcomes
The mean (median) on-treatment observation period was 11.2 (7.9) months for patients who received treatment with apalutamide and 9.5 (7.0) months for patients who received treatment with enzalutamide. The proportion of patients having achieved a PSA90 response by 6 months post-index was 63.1% in the apalutamide cohort and 52.4% in the enzalutamide cohort (Figure 3). Patients treated with apalutamide had a 42% higher rate of PSA90 response within 6 months post-index compared with those treated with enzalutamide (HR: 1.42 [95% CI: 1.06, 1.91]; p = 0.020). Patients who received treatment with apalutamide attained a PSA90 response after a median of 3.3 versus 5.5 months for patients treated with enzalutamide.
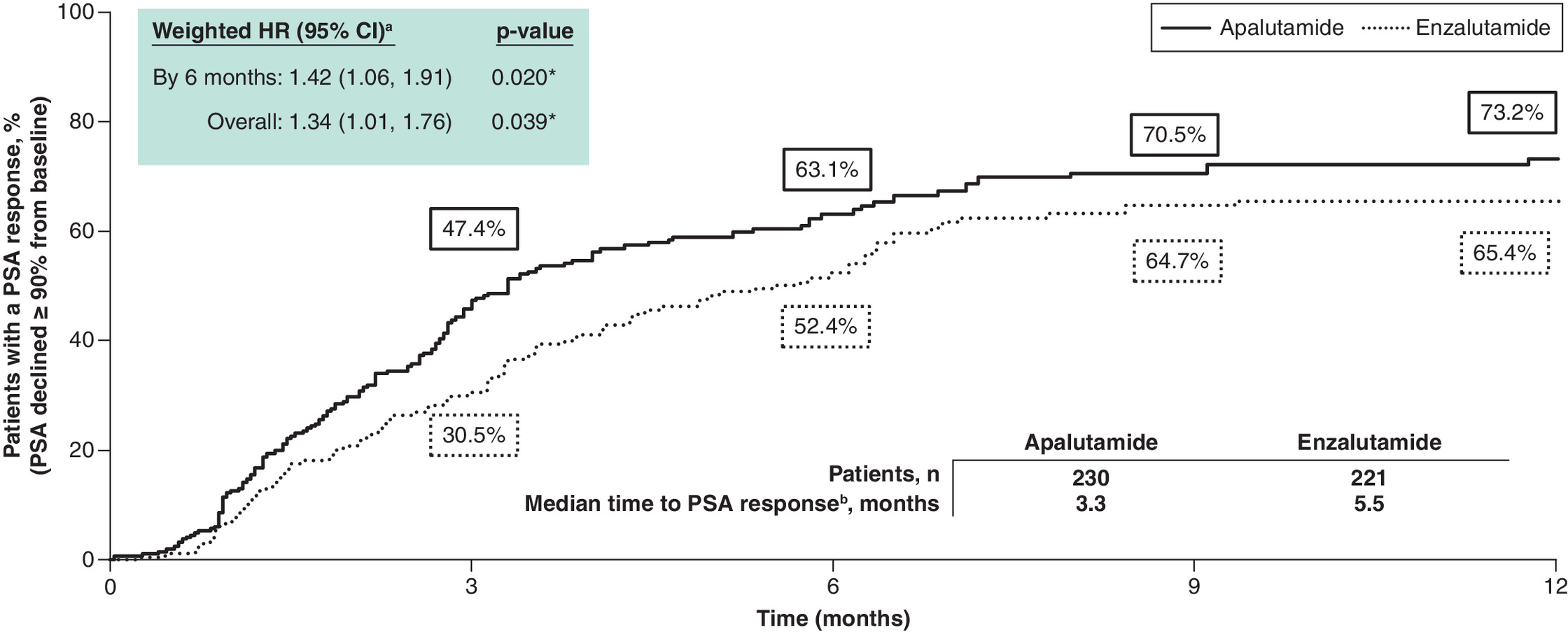
Figure 3. Comparison of time-to-PSA90 response among Black patients with metastatic castration-sensitive prostate cancer.
*Significant at the 5% level.
aA hazard ratio >1 indicates that the apalutamide cohort had a higher rate of PSA response ≥90% compared with the enzalutamide cohort.
bPSA90 response was defined as the first decline for a follow-up PSA value of 90% or more relative to the most recent baseline PSA value observed within 13 weeks up to and including the index date.
HR: Hazard ratio; mCSPC: Metastatic castration-sensitive prostate cancer; PSA: Prostate-specific antigen.
PSA-related measurements
Overall, 80.3% and 78.5% of patients who received treatment with apalutamide or enzalutamide, respectively, had ≥1 PSA measurement during the observation period (Table 2). A similar proportion of patients who received treatment with apalutamide or enzalutamide had ≥1 PSA measurement within 6 months of index ARPI treatment initiation (apalutamide: 77.0%; enzalutamide: 77.7%). Patients who received treatment with apalutamide were administered a mean (median) of number of 3.9 (3.4) PSA tests per year, relative to 3.9 (3.2) for patients who received treatment with enzalutamide.
| Apalutamide† (n = 230) | Enzalutamide† (n = 221) | |
|---|---|---|
| On-treatment observation period, months, mean ± SD [median] | 11.2 ± 10.3 [7.9] | 9.5 ± 9.4 [7.0] |
| Patients with ≥1 PSA test, n (%) | 185 (80.3) | 174 (78.5) |
| Within 3 months of observation | 159 (69.3) | 135 (61.3) |
| Within 6 months of observation | 177 (77.0) | 172 (77.7) |
| Follow-up PSA tests per year, mean ± SD [median] | 3.9 ± 3.5 [3.4] | 3.9 ± 3.8 [3.2] |
| Patients with a PSA test on average every 3 months, n (%) | 87 (38.0) | 72 (32.7) |
| Patients with a PSA test on average every 6 months, n (%) | 167 (72.8) | 168 (75.9) |
†
The number of patients reported in this weighted population represents the sum of weights for the corresponding non-weighted patients, rounded to the nearest integer. The proportions displayed were calculated prior to the rounding and may be slightly different than if they were calculated based on rounded numbers.
PSA: Prostate-specific antigen; SD: Standard deviation.
Discussion
To our knowledge, this is the first study using real-world data to evaluate PSA responses after treatment initiation with either apalutamide or enzalutamide specifically among Black patients with mCSPC. Black patients treated with apalutamide achieved a PSA90 response within 6 months of treatment initiation at a significantly higher rate compared with those treated with enzalutamide. Median time to PSA90 response was also 2 months shorter in patients treated with apalutamide, relative to patients treated with enzalutamide. A key strength of this study was the use of EMR data linked with insurance claims data. Data from the EMR provided PC-related characteristics documented during the routine provision of care in urology practices, and insurance claims data provided complementary medical and pharmacy information for services received outside of these practices.
There is limited evidence regarding the impact of apalutamide versus enzalutamide on PSA outcomes in Black patients, as no head-to-head trials or previous comparisons of real-world data within this population have been conducted. One other retrospective cohort study by Bivins et al. has evaluated PSA responses following treatment with apalutamide among Black patients with mCSPC, also using urology EMR data obtained from PPS [15]. A PSA90 response was achieved by 76.5% of patients after apalutamide treatment initiation, with a median time-to-first PSA90 response of 2.9 months [15]. The proportion of Black patients who achieved a PSA90 response following apalutamide treatment was higher than that identified by the current analysis (54.6%). Differences in findings may reflect variations in sample size (44 patients vs 503 patients) and the urology-specific nature of the data in the Bivins et al. study. Previous real-world studies have reported that patients with mCSPC treated with apalutamide were between 21% and 56% more likely to attain a PSA90 response within 6 months of treatment initiation compared with patients treated with enzalutamide [13,20]. The patients treated with apalutamide also achieved a PSA90 response a median of approximately 1.5 to 2.0 months earlier than patients in the enzalutamide cohort [13,20]. Some of the differences in PSA response may reflect pharmacologic distinctions between these medications, including a higher androgen receptor affinity of apalutamide compared with enzalutamide [21]. Thus, while these results were not specific to Black patients with mCSPC, they identify a deeper and earlier response to apalutamide versus enzalutamide treatment among patients with mCSPC and are consistent with the PSA90 responses observed among the Black population in the current analysis.
Previous research evaluating real-world treatment patterns among Black patients with mCSPC initiating apalutamide identified exceptionally high persistence rates, with 97.8% of patients remaining on treatment at 12 months [22]. Given that high treatment persistence suggests a therapy is both tolerable and effective, these findings could help to further explain the higher PSA90 response rates observed with apalutamide versus enzalutamide treatment in the present study.
There is a sizable body of evidence demonstrating that early PSA response in patients with advanced PC is associated with improved progression-free survival and overall survival [10,11,23–27]. Relatedly, a recent real-world study reported that ARPI-naive patients initiated on apalutamide had better survival outcomes at 24 months compared with enzalutamide [28]. However, further evidence is needed to determine whether the higher rates of PSA response observed with apalutamide in this study would similarly translate to improved long-term outcomes among a Black population.
Several studies have demonstrated that Black men with PC in the US experience restricted access to care and treatment, which can negatively affect their survival outcomes [29–32]. In a large study of over 35,000 US men with PC, access-related variables accounted for nearly 85% of the excess risk of death observed in Black men relative to White men [31]. Additionally, as Black men have largely been underrepresented in PC clinical trials, more diverse and representative clinical studies in combination with real-world analyses of large patient cohorts are essential to understand clinical outcomes of mCSPC treatments within this population [2]. The results of the present study may help to inform clinical decision-making when selecting an initial ARPI for the treatment of Black patients with mCSPC, although further research is needed to determine the potential impact of early PSA90 response on long-term clinical outcomes among this population and to clarify the implications of these findings for future guideline development.
Limitations
Results from this study are subject to limitations. First, the selection of patients with mCSPC and/or detection of PSA testing patterns and responses may have been impacted by inaccuracies or omissions within the data source, a limitation common to all EMR and administrative claims databases. Despite balancing baseline characteristics using IPTW, residual confounding may have been present due to unmeasured factors. Comorbidities, in particular, were not assessed. Socioeconomic factors were not captured; however, as apalutamide and enzalutamide are similarly priced branded medications, and most patients in both treatment cohorts were insured through Medicare, these factors were unlikely to have differentially affected treatment selection or outcomes. This study also did not include uninsured patients, who may face greater barriers to accessing apalutamide and enzalutamide. Second, mis-linkages between the data sources may have led to misclassification or information bias. Third, if PSA testing was performed more frequently for one ARPI relative to the other, surveillance bias may have resulted. However, this is unlikely to affect results in this study as the mean number of follow-up PSA tests per year was 3.9 for patients in both treatment cohorts. Furthermore, patients who did not have a follow-up PSA test were assumed to not have achieved a PSA90 response; however, this may not have been true for all patients. Finally, all PSA data were sourced from the same urology network (PPS); thus, any PSA testing received outside of this network would not have been captured in the data source. However, most patients receive care through PPS (including medication dispensing); thus, this was unlikely to meaningfully impact data availability.
Conclusion
In this study among Black ARPI-naive patients with mCSPC, treatment with apalutamide was associated with a statistically significant 42% increase in the rate of achieving a PSA90 response within 6 months compared with enzalutamide. Patients initiating treatment with apalutamide had a median time to PSA90 response 2 months shorter compared with enzalutamide. Given that a deep and early PSA response has been associated with improved long-term clinical outcomes in patients with mCSPC, the shorter time to and higher likelihood of achieving PSA90 observed with apalutamide in this study suggests that apalutamide may provide greater long-term treatment efficacy than enzalutamide among Black patients with mCSPC. Future research evaluating PSA90 as a prognostic indicator of overall survival in this population is therefore warranted.
Summary points
•
Black men are disproportionately affected by prostate cancer (PC), including experiencing higher incidence and mortality rates compared with White men.
•
Treatment for metastatic castration-sensitive PC (mCSPC) may involve treatment with androgen receptor pathway inhibitors (ARPIs), including apalutamide or enzalutamide.
•
Prostate-specific antigen levels are often used to evaluate PC treatment response, and a PSA90 response (≥90% reduction in prostate-specific antigen [PSA] from pre-treatment levels) in particular is an important earlier indicator of treatment success.
•
This study aimed to compare PSA responses between Black patients with mCSPC treated with apalutamide or enzalutamide in real-world clinical practice.
•
Linked electronic medical record and claims data were analyzed for 230 patients treated with apalutamide and 221 patients treated with enzalutamide.
•
Within 6 months of treatment initiation, Black patients treated with apalutamide had a 42% higher PSA90 response rate compared with those treated with enzalutamide (HR: 1.42, 95% CI: 1.06, 1.91; p = 0.020).
•
The median time to PSA90 response was 2 months shorter among Black patients treated with apalutamide versus enzalutamide (3.3 vs 5.5 months).
•
Given that a deep and early PSA response is associated with better long-term clinical outcomes, Black patients with mCSPC may experience greater and more durable efficacy with apalutamide versus enzalutamide treatment.
Author contributions
B Lowentritt contributed to the conceptualization, investigation, methodology, writing – original draft, writing – review and editing. S Burbage contributed to the conceptualization, data curation, funding acquisition, methodology, project administration, resources, supervision, writing – original draft, writing – review and editing. I Khilfeh contributed to the conceptualization, data curation, funding acquisition, methodology, project administration, resources, supervision, writing – original draft, writing – review and editing. D Pilon contributed to the conceptualization, formal analysis, investigation, methodology, project administration, resources, supervision, validation, visualization, writing – original draft, writing – review and editing. S Du contributed to the conceptualization, data curation, funding acquisition, methodology, project administration, resources, supervision, writing – original draft, writing – review and editing. C Rossi contributed to the conceptualization, formal analysis, investigation, methodology, resources, supervision, writing – original, writing – review and editing. F Kinkead contributed to the formal analysis, investigation, software, validation, visualization, writing – original draft, writing – review and editing. L Diaz contributed to the formal analysis, investigation, software, validation, visualization, writing – original draft, writing – review and editing. G Brown contributed to the conceptualization, investigation, methodology, writing – original draft, writing – review and editing. All authors approved the final version of the manuscript to be published and agree to be accountable for all aspects of the work.
Acknowledgments
The authors thank Gordon Wong, BIE, an employee of Analysis Group, Inc., for his contribution to this study. Part of the material in this manuscript was presented at the American Society of Clinical Oncology (ASCO) conference, held from 30 May to 3 June 2024, in Chicago, Illinois.
Financial disclosure
This study was funded by Johnson & Johnson (PA, USA).
Competing interests disclosure
B Lowentritt is an employee of Chesapeake Urology Associates and has received consulting fees from Johnson & Johnson. S Burbage, I Khilfeh and S Du are employees and stockholders of Johnson & Johnson. D Pilon, C Rossi, F Kinkead and L Diaz are employees of Analysis Group, Inc., a consulting company that has provided paid consulting services to Johnson & Johnson. G Brown is an employee of New Jersey Urology and has received consulting fees from Johnson & Johnson. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing assistance was provided by professional medical writer, Molly Gingrich, MSc, an employee of Analysis Group, Inc., a consulting company that has provided paid consulting services to Johnson & Johnson, which funded the development and conduct of this study. Medical writing support was also provided by Cody Patton, BSc, an independent contractor working on behalf of Analysis Group, Inc.
Ethical conduct of research
Data were de-identified and comply with the patient requirements of the Health Insurance Portability and Accountability Act (HIPAA) of 1996; therefore, no review by an institutional review board was required per Title 45 of CFR, Part 46.101(b)(4) (https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr-46/#46.101).
Data availability statement
The data that support the findings of this study were used under license. These data cannot be shared as restrictions apply to their availability.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A. Cancer statistics, 2025. CA Cancer J. Clin. 75(1), 10–45 (2025).
2.
Lillard JW Jr, Moses KA, Mahal BA, George DJ. Racial disparities in Black men with prostate cancer: a literature review. Cancer 128(21), 3787–3795 (2022).
• This literature review describes racial inequalities among Black versus White men with prostate cancer and proposes soultions to address this health disparity.
3.
Devasia TP, Mariotto AB, Nyame YA, Etzioni R. Estimating the number of men living with metastatic prostate cancer in the United States. Cancer Epidemiol. Biomarkers Prev. 32(5), 659–665 (2023).
4.
National Cancer Institute Surveillance Epidemiology and End Results Progam. Cancer Stat Facts: prostate cancer 2025. (Accessed: 29 July 2025). Available from: https://seer.cancer.gov/statfacts/html/prost.html
5.
Sayegh N, Swami U, Agarwal N. Recent advances in the management of metastatic prostate cancer. JCO Oncol. Pract. 18(1), 45–55 (2022).
6.
FDA approves apalutamide for metastatic castration-sensitive prostate cancer. (2019). Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-apalutamide-metastatic-castration-sensitive-prostate-cancer
7.
FDA approves enzalutamide for metastatic castration-sensitive prostate cancer. (2019). Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-enzalutamide-metastatic-castration-sensitive-prostate-cancer
8.
Chi KN, Agarwal N, Bjartell A et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N. Engl. J. Med. 381(1), 13–24 (2019).
9.
Armstrong AJ, Szmulewitz RZ, Petrylak DP et al. ARCHES: a randomized, Phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J. Clin. Oncol. 37(32), 2974–2986 (2019).
10.
Chowdhury S, Bjartell A, Agarwal N et al. Deep, rapid, and durable prostate-specific antigen decline with apalutamide plus androgen deprivation therapy is associated with longer survival and improved clinical outcomes in TITAN patients with metastatic castration-sensitive prostate cancer. Ann. Oncol. 34(5), 477–485 (2023).
11.
Matsubara N, Chi KN, Özgüroğlu M et al. Correlation of prostate-specific antigen kinetics with overall survival and radiological progression-free survival in metastatic castration-sensitive prostate cancer treated with abiraterone acetate plus prednisone or placebos added to androgen deprivation therapy: post hoc analysis of Phase III LATITUDE study. Eur. Urol. 77(4), 494–500 (2020).
12.
Du S, Rossi C, Khilfeh I et al. Prostate-specific antigen reduction after androgen receptor pathway inhibitor initiation: real-world comparison of disease progression among patients with metastatic castration-sensitive prostate cancer. J. Health Econ. Outcomes Res. 12(2), 41–49 (2025).
13.
Lowentritt B, Pilon D, Khilfeh I et al. Attainment of early, deep prostate-specific antigen response in metastatic castration-sensitive prostate cancer: a comparison of patients initiated on apalutamide or enzalutamide. Urol. Oncol. 41(5), 253.e1–253.e9 (2023).
• In this real-world study, PSA90 responses were compared between patients with metastatic castration-sensitive prostate cancer (mCSPC) treated with apaltamide versus enzaluatmide. Apalutamide treatment was associated with a significantly higher likelihood of achieving PSA90 compared with enzalutamide treatment.
14.
Lowentritt B, Pilon D, Waters D et al. Comparison of prostate-specific antigen response in patients with metastatic castration-sensitive prostate cancer initiated on apalutamide or abiraterone acetate: a retrospective cohort study. Urol. Oncol. 41(5), 252.e19–252.e27 (2023).
15.
Bivins VM, Durkin M, Khilfeh I et al. Early prostate-specific antigen response among Black and non-Black patients with advanced prostate cancer treated with apalutamide. Future Oncol. 18(32), 3595–3607 (2022).
• This real-world study compared PSA90 responses between Black and non-Black patients with advanced PC treated with apalumatide, finding that apalutamide reduced prostate-specific antigen (PSA) levels in both populations.
16.
Dess RT, Hartman HE, Mahal BA et al. Association of Black race with prostate cancer–specific and other-cause mortality. JAMA Oncol. 5(7), 975–983 (2019).
• This multiple-cohort study included over 300,000 participants and found that Black race was not associated with inferior mortality after adjusting for access to care and standardized treatment.
17.
Freedland SJ, Ke X, Lafeuille MH et al. Identification of patients with metastatic castration-sensitive or metastatic castration-resistant prostate cancer using administrative health claims and laboratory data. Curr. Med. Res. Opin. 37(4), 609–622 (2021).
18.
Dorfman AH, Valliant R. (Eds). The Hajek Estimator revisited. Proceedings of the Section on Survey Methods Research. American Statistical Association, VA, USA (1997).
19.
Austin PC. Using the standardized difference to compare the prevalence of a binary variable between two groups in observational research. Commun. Stat. Simul. Comput. 38(6), 1228–1234 (2009).
20.
Lowentritt B, Khilfeh I, Pilon D et al. Real-world comparison of deep prostate-specific antigen response in patients with metastatic castration-sensitive prostate cancer treated with apalutamide or enzalutamide. Rev. Urol. 23(2), e29–e40 (2024).
• In this study, linked electronic medical record and claims data was used to compare PSA90 responses between patients with mCSPC treated with apalutamide versus enzalutamide. A PSA90 response was observed in a greater number of patients treated with apalutamide compared with enzalutamide.
21.
Park SJ, Yoder B, Li T. Comparison of second-generation antiandrogens for the treatment of prostate cancer. J. Hematol. Oncol. Pharm. 12(2), 92–98 (2022).
22.
Lowentritt BH, Rossi C, Muser E et al. Real-world clinical outcomes and treatment patterns among Black and non-Black patients with prostate cancer initiated on apalutamide in a urology setting. J. Health Econ. Outcomes Res. 11(2), 41–48 (2024).
23.
Hussain MH, Sternberg CN, Efstathiou E et al. Overall survival (OS) and metastasis-free survival (MFS) by depth of prostate-specific antigen (PSA) decline in the Phase III PROSPER trial of men with nonmetastatic castration-resistant prostate cancer (nmCRPC) treated with enzalutamide (ENZA). J. Clin. Oncol. 39, 94 (2021).
24.
Saad F, Hussain MH, Tombal BF et al. Association of prostate-specific antigen (PSA) response and overall survival (OS) in patients with metastatic hormone-sensitive prostate cancer (mHSPC) from the Phase III ARASENS trial. J. Clin. Oncol. 40, 5078 (2022).
25.
Saad F, Small EJ, Feng FY et al. Deep prostate-specific antigen response following addition of apalutamide to ongoing androgen deprivation therapy and long-term clinical benefit in SPARTAN. Eur. Urol. 81(2), 184–192 (2022).
26.
Harshman LC, Chen Y-H, Liu G et al. Seven-month prostate-specific antigen is prognostic in metastatic hormone-sensitive prostate cancer treated with androgen deprivation with or without docetaxel. J. Clin. Oncol. 36(4), 376–382 (2018).
27.
Hussain M, Goldman B, Tangen C et al. Prostate-specific antigen progression predicts overall survival in patients with metastatic prostate cancer: Data from Southwest Oncology Group Trials 9346 (Intergroup Study 0162) and 9916. J. Clin. Oncol. 27(15), 2450–2456 (2009).
28.
Bilen MA, Lowentritt B, Khilfeh I et al. Overall survival with apalutamide versus enzalutamide in metastatic castration-sensitive prostate cancer. Adv. Ther. 42(7), 3437–3454 (2025).
• Patients with mCSPC treated with apalutamide versus enzalutamide in real-world clinical practice experienced better survival outcomes at 24 months.
29.
Barocas DA, Penson DF. Racial variation in the pattern and quality of care for prostate cancer in the USA: mind the gap. BJU Int. 106(3), 322–328 (2010).
30.
Gong J, Kim DM, De Hoedt AM et al. Disparities with systemic therapies for Black men having advanced prostate cancer: where do we stand? J. Clin. Oncol. 42(2), 228–236 (2024).
31.
Krimphove MJ, Cole AP, Fletcher SA et al. Evaluation of the contribution of demographics, access to health care, treatment, and tumor characteristics to racial differences in survival of advanced prostate cancer. Prostate Cancer Prostatic Dis. 22(1), 125–136 (2019).
32.
Ma TM, Agarwal N, Mahal B et al. Racial and ethnic disparities in use of novel hormonal therapy agents in patients with prostate cancer. JAMA Netw. Open 6(12), e2345906 (2023).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 6 October 2025
Accepted: 18 December 2025
Published online: 16 January 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparison of deep prostate-specific antigen response in Black patients with metastatic castration-sensitive prostate cancer initiated on apalutamide or enzalutamide. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0161
Export citation
Select the citation format you wish to export for this article or chapter.