First-line tumor necrosis factor inhibitor versus abatacept treatment choice in real-world patients with anticitrullinated protein antibody- and rheumatoid factor-positive rheumatoid arthritis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare characteristics of patients with anticitrullinated protein antibody-positive (ACPA+) and rheumatoid factor-positive (RF+) rheumatoid arthritis (RA) who initiated abatacept or a tumor necrosis factor inhibitor (TNFi) as a first-line biologic disease-modifying antirheumatic drug (bDMARD), and to identify factors associated with first-line bDMARD selection. Materials & methods: This retrospective cohort study abstracted data for patients with ACPA+/RF+ RA initiating abatacept or a TNFi as a first-line bDMARD between 1 January 2015 and 19 February 2020. Patient characteristics were compared using chi-square/Fisher exact tests (categorical variables) and Wilcoxon tests (continuous variables). Adjusted odds ratios (OR; 95% confidence interval [CI]) of initiating abatacept versus TNFi were estimated using 2-level logistic regression. Results: The analysis cohort included 301 patients who initiated abatacept and 203 patients who initiated a TNFi. Time from RA diagnosis to first-line initiation (>2 years vs <1 year; OR [95% CI] 2.9 [1.4–6.1]), high and moderate disease activity (versus low; 5.0 [1.8–13.9] and 4.2 [1.5–11.6], respectively), and conventional synthetic (cs) DMARD use within 12 months prior to initiation (versus no csDMARD use; 2.0 [1.1–3.6]) were associated with higher odds of initiating abatacept versus a TNFi (all p < 0.05). Patients with Medicare/other insurance had increased odds of initiating abatacept (versus TNFi) as age increased. Baseline ACPA >250 AU/ml was associated with lower odds of initiating abatacept over a TNFi (versus ACPA 20–250 AU/ml; 0.4 [0.2–0.8]; p < 0.01). Conclusion: In this real-world study, patients with ACPA+/RF+ RA were more likely to initiate abatacept over TNFi as a first-line bDMARD if they had delayed first-line bDMARD initiation, high/moderate disease activity, prior csDMARD use, or were of an older age. There is a need for better understanding of treatment selection and to account for these variables in future studies.
Plain language summary
What was the aim of this research?
The study looked at patient or disease factors affecting doctors' choice of treatments for patients with seropositive rheumatoid arthritis (RA).
How was the research done?
The analysis compared data from patient medical records for two groups of patients with RA: one group started their first targeted treatment with abatacept and the other started with a drug from a group called tumor necrosis factor inhibitors (TNFis).
What were the results?
The research team studied data from the medical records of 301 patients who started abatacept and 203 patients who started a TNFi. The results showed that patients were more likely to start abatacept than a TNFi if they started treatment later after their diagnosis, had more severe disease, had used corticosteroid treatment previously, or were older. As patient age increased, they were more likely to start abatacept than a TNFi if they had Medicare or other insurance. Patients were more likely to be prescribed a TNFi than abatacept if they had higher levels of anticitrullinated protein antibody before starting treatment.
Why is this important?
This study showed that many patient and disease factors may affect treatment choice for patients with seropositive RA. Further studies will be important to improve our understanding of the reasons behind treatment decisions. This research may help to ensure that patients receive the right treatment for them with the most benefit.
Rheumatoid arthritis (RA) is a chronic autoimmune disease that is estimated to affect around 1.3 million adults in the US [1–4]. Autoantibodies, such as anticitrullinated protein antibodies (ACPAs) and rheumatoid factor (RF) are often indicative of a more severe and erosive form of RA and an increased risk of extra-articular manifestations/comorbidities [5–7]. For example, patients with RA who are ACPA and RF-positive have a greater risk of RA-related interstitial lung disease (RA-ILD) [8]. However, research has shown that the presence of ACPA and RF may also serve as prognostic and pharmacodynamic biomarkers to predict disease progression and treatment response, respectively, in patients with RA [9–14].
Treatment options for RA initially include conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), such as methotrexate (MTX), sulfasalazine, leflunomide and hydroxychloroquine [15,16]. Second-line treatments in cases where symptoms do not improve include switching to a different csDMARD, adding a second csDMARD, or adding a biologic DMARD (bDMARD), such as tumor necrosis factor inhibitors (TNFis), interleukin-6 inhibitors (IL-6is), or the T-cell co-stimulation modulator abatacept [15–17].
Treatment with abatacept has demonstrated favorable outcomes in adult patients with ACPA+ and/or RF+ RA and has shown benefit when used early in a subset of adults at high risk of developing RA [18–21]. Additionally, improved responses have been documented with abatacept compared with the TNFi adalimumab [22,23].
Guidelines for optimal bDMARD selection and sequencing following inadequate response to csDMARDs are not established, and there is a lack of information regarding which treatments may be suitable for specific patients. Thus, a better understanding of factors associated with first-line bDMARD selection for patients with ACPA+/RF+ RA in the real-world setting may help clinicians to optimize treatment decision-making. Therefore, this analysis aimed to compare demographic, clinical, and treatment-related characteristics of adult patients with RA who were both ACPA+ and RF+ and were treated with abatacept or a TNFi as a first-line bDMARD, as well as to identify factors associated with first-line bDMARD selection in the real-world setting.
Materials & methods
Study design & data source
This was a retrospective, observational cohort study of patients with ACPA+ and RF+ RA who initiated first-line bDMARD treatment with abatacept (intravenous [IV] or subcutaneous [SC] formulations) or a TNFi in rheumatology clinics in the US [21]. TNFis included SC adalimumab, SC certolizumab pegol, SC etanercept, IV or SC golimumab and IV infliximab. These medications were prescribed by treating rheumatologists at their own discretion as part of individualized decision-making processes. Eligible patients were identified by their treating rheumatologists in the Cardinal Health Rheumatology Provider Extended Network. As of February 2021, Cornerstone represented approximately 1100 practices comprising 2300 rheumatologists across 48 US states. Purposive sampling provided data for this analysis from 28 rheumatology practices across the US.
Data were collected as previously described [21]. In brief, Cardinal Health developed and tested an electronic case report form (eCRF), which was then utilized by 28 rheumatologists who each selected a maximum of 20 consecutive potentially eligible patients for chart abstraction, starting with the earliest eligible (to minimize selection bias and to maximize follow-up time). Patient demographic, clinical and treatment-related data were abstracted from the date of RA diagnosis through the date of last follow-up or death (if known or applicable). In an attempt to minimize unmeasured confounding bias, the collection of numerous data points of clinical relevance to the treatment patterns of patients was required.
Patient identification spanned from 1 January 2015 to 19 February 2020, which defined the index period for patients initiating abatacept or a TNFi as a first-line bDMARD [21]. All data for patients treated with abatacept as a first-line bDMARD were abstracted from patient medical records, and data collection occurred between 19 February 2021 and 15 April 2021. Data for patients treated with a TNFi were collected between 17 November 2021 and 29 November 2021.
Patient population
Eligible patients had a confirmed diagnosis of RA; were aged ≥18 years; were bDMARD- and Janus kinase inhibitor treatment-naive; responded inadequately to MTX and subsequently initiated first-line abatacept or TNFi therapy on or after 1 January 2015; were ACPA+ (anticyclic citrullinated peptide 2 >20 AU/ml) and RF+ at or within 12 months prior to initiation; had one clinical disease activity index (CDAI) score [24] within 3 months prior to initiation and one CDAI score within 3–12 months following initiation; and were followed by participating rheumatologists for at least 12 months after first-line abatacept or TNFi initiation.
Patients were excluded if they had discontinued abatacept or a TNFi as a first-line bDMARD within 3 months of initiation or were treated with abatacept or a TNFi for RA in a clinical trial between 1 January 2015 and 19 February 2020 [21].
Study conduct & ethical considerations
This study was conducted in accordance with International Society for Pharmacoepidemiology Guidelines for Good Epidemiology Practices [25], the Professional Society for Health Economics and Outcomes Research [26], the Strengthening the Reporting of Observational Studies in Epidemiology guidelines [27] and the ethical principles in the Declaration of Helsinki [28]. Rheumatologists were required to be able to participate in research monitored by a central institutional review board (IRB; 20204039). The protocol, amendments, eCRF and waiver of patient informed consent (due to the minimal amount of protected health information collected) received IRB approval from the Western Institutional Review Board.
Outcomes
This analysis aimed to identify demographic and clinical characteristics associated with first-line bDMARD selection among US patients with ACPA+/RF+ RA in a real-world setting.
Statistical analysis
Demographic and clinical characteristics were summarized using descriptive statistics. Unadjusted comparisons of demographic, clinical and treatment characteristics across the abatacept and TNFi treatment cohorts were conducted using chi-square tests (or Fisher exact tests where n < 5) for categorical variables and Wilcoxon rank-sum tests for continuous variables. Adjusted odds ratios (ORs) of receiving abatacept versus TNFi as a first-line bDMARD were calculated using logistic regression. Given that patient data provided from the same provider may have high intra-class correlation at the provider level, 2-level logistic regression was utilized to adjust for the clustering effect. Analyses were adjusted for numerous demographic and disease characteristics.
All independent variables that had a p < 0.2 in univariate modeling were included in the initial multivariable model. Independent variables with the highest p-values were dropped from subsequent multivariable model iterations until all variables included in the model were significant. All analyses were conducted in SAS v9.4 (SAS Institute, NC, USA) and 2-sided test p ≤ 0.05 were considered statistically significant.
Results
Study population
In total, 504 patients identified by 28 rheumatologists were included in this analysis: 301 patients initiated abatacept (IV, n = 178; SC, n = 125 [not mutually exclusive]) and 203 patients initiated a TNFi (adalimumab, n = 69; certolizumab pegol, n = 41; etanercept, n = 38; infliximab, n = 34; golimumab, n = 21) as a first-line bDMARD. The rheumatologists had a median of 13.5 years in practice, with 71.4% practicing in the community setting and 53.6% being in urban locations. Participating rheumatologists had a broad geographic distribution across the US, with 32.1% in the Northeast, 28.6% in the South, 25.0% in the West and 14.3% in the Midwest.
Demographic, clinical & treatment-related characteristics at initiation of abatacept or TNFi as a first-line bDMARD
Patients who initiated abatacept as a first-line bDMARD were older at initiation, a greater proportion were >2 years post RA diagnosis, and a greater proportion had Medicare coverage compared with patients who initiated a TNFi (all p < 0.001; Table 1). A greater proportion of patients who initiated a TNFi had commercial insurance, compared with patients who initiated abatacept (p < 0.001).
| Characteristic | First-line bDMARD | ||
|---|---|---|---|
| Abatacept (n = 301) | TNFi (n = 203) | p-value | |
| Age at first-line bDMARD initiation, mean (SD), years | 53.3 (15.5) | 48.2 (14.2) | <0.001 |
| Female, n (%) | 214 (71.1) | 136 (67.0) | 0.416 |
| Race, n (%) White Black/African–American Asian Native Hawaiian or other Pacific Islander American Indian or Alaska Native Other | 208 (69.1) 50 (16.6) 27 (9.0) 6 (2.0) 4 (1.3) 6 (2.0) | 147 (72.4) 28 (13.8) 25 (12.3) 1 (0.5) 2 (1.0) 0 (0.0) | 0.141 |
| Ethnicity, n (%) Non-Hispanic/Non-Latino/Non-Latina Hispanic/Latino/Latina Unknown | 245 (81.4) 55 (18.3) 1 (0.3) | 169 (83.3) 34 (16.7) 0 (0.0) | 0.834 |
| Health insurance status at first-line bDMARD initiation, n (%) Commercial Medicare Other† | 165 (54.8) 110 (36.5) 26 (8.5) | 138 (68.0) 37 (18.2) 28 (13.8) | <0.001 |
| BMI at first-line bDMARD initiation, mean (SD) | 27.2 (5.7) | 27.4 (5.1) | 0.422 |
| Smoking status at first-line bDMARD initiation, n (%) Never smoked Current smoker History of smoking | 208 (69.1) 35 (11.6) 58 (19.3) | 135 (66.5) 31 (15.3) 37 (18.2) | 0.492 |
| Presence of extra-articular manifestations at first-line bDMARD initiation, n (%) | 144 (47.8) | 71 (35.0) | 0.004 |
| Charlson Comorbidity Index at first-line bDMARD initiation, n (%) 0 1 2 3+ | 227 (75.4) 59 (19.6) 13 (4.3) 2 (0.7) | 168 (82.8) 31 (15.3) 2 (1.0) 2 (1.0) | 0.060 |
| Presence of congestive heart failure at first-line bDMARD initiation, n (%) | 7 (2.3) | 0 (0.0) | 0.045 |
| Presence of chronic obstructive pulmonary disease at first-line bDMARD initiation, n (%) | 9 (3.0) | 1 (0.5) | 0.055 |
| Baseline ACPA‡ >250 AU/ml, n (%) | 78 (25.9) | 90 (44.3) | <0.001 |
| Baseline CDAI§, n (%) Remission/low disease activity (≤10) Moderate disease activity (>10 and ≤22) High disease activity (>22) | 18 (6.0) 112 (37.2) 171 (56.8) | 26 (12.8) 74 (36.5) 103 (50.7) | 0.026 |
| Time from RA diagnosis to first-line bDMARD initiation, n (%) <1 year 1–2 years >2 years | 179 (59.5) 47 (15.6) 75 (24.9) | 147 (72.4) 33 (16.3) 23 (11.3) | <0.001 |
| First-line bDMARD route of administration, n (%) Intravenous Subcutaneous | 178 (59.1) 125 (41.5) | 46 (22.7) 157 (77.3) | <0.001 <0.001 |
| Corticosteroid use within the 12 months prior to first-line bDMARD initiation, n (%) Yes No Unknown | 49 (16.3) 237 (78.7) 15 (5.0) | 21 (10.3) 166 (81.8) 16 (7.9) | 0.011 |
| Use of csDMARDs within the 12 months prior to first-line bDMARD initiation, n (%) | 135 (44.9) | 57 (28.1) | <0.001 |
| Use of NSAIDs within the 12 months prior to first-line bDMARD initiation, n (%) | 174 (57.8) | 129 (63.5) | 0.197 |
| Use of opioid/narcotic analgesics within the 12 months prior to first-line bDMARD initiation, n (%) | 31 (10.3) | 11 (5.4) | 0.052 |
Values of p were determined by unadjusted Wilcoxon test, chi-square test or Fisher’s exact test, as appropriate, and show TNFi vs abatacept.
Data from this table were previously presented at ACR Convergence 2022; 10–14 November 2022; Philadelphia, PA, USA (poster 1417).
†
Includes patients with Medicaid, military coverage (e.g., Tricare/Veterans Affairs) and self-pay patients.
‡
ACPA measured within 12-month period prior to/at initiation of first-line bDMARD, and value closest to initiation is reported (if more than one entered).
§
Baseline CDAI [24] assessed within 3 months prior to/at initiation of first-line bDMARD.
ACPA: Anticitrullinated protein antibody; bDMARD: Biologic disease-modifying antirheumatic drug; CDAI: Clinical Disease Activity Index; csDMARD: Conventional synthetic disease-modifying antirheumatic drug; NSAID: Non-steroidal anti-inflammatory drug; RA: Rheumatoid arthritis; SD: Standard deviation; TNFi: Tumor necrosis factor inhibitor.
A numerically higher proportion of patients who initiated abatacept had a Charlson Comorbidity Index (CCI) of 1 or 2 compared with patients who initiated a TNFi. The three most commonly reported comorbidities in the overall study population were reported in higher proportions among patients who initiated abatacept than a TNFi: Type 2 diabetes: 13.3 versus 8.9% (p = 0.127); mild liver disease 4.3 versus 3.9% (p = 0.835); and obesity (BMI ≥30) 7.0 versus 5.9% (p = 0.655). A higher proportion of patients who initiated abatacept had extra-articular manifestations and congestive heart failure compared with patients who initiated a TNFi (p = 0.004 and p = 0.045, respectively). A higher number of patients who initiated abatacept had chronic obstructive pulmonary disease at first-line bDMARD initiation, compared with patients who initiated a TNFi (3.0 vs 0.5%; p = 0.055).
Baseline CDAI differed between patients who initiated abatacept as a first-line bDMARD and those who initiated a TNFi. In the abatacept group, more patients had high disease activity (CDAI >22) than in the TNFi group, whereas in the TNFi group, more patients had remission/low disease activity (CDAI ≤10) than in the abatacept group. A greater proportion of patients who initiated abatacept (versus a TNFi) received the first-line bDMARD intravenously (p < 0.001) and used corticosteroids and csDMARDs within 12 months prior to first-line bDMARD initiation (p = 0.011 and p < 0.001, respectively).
At first-line bDMARD initiation, a lower proportion of patients who received abatacept had baseline ACPA levels >250 AU/ml than those who received a TNFi (p < 0.001).
Multivariate analysis: factors associated with first-line bDMARD selection
Patients with >2 years from the time of RA diagnosis to first-line bDMARD initiation had greater adjusted odds of initiating abatacept than a TNFi versus patients who initiated first-line <1 year from RA diagnosis (OR [95% CI]: 2.92 [1.39–6.13]; p = 0.005; Figure 1).
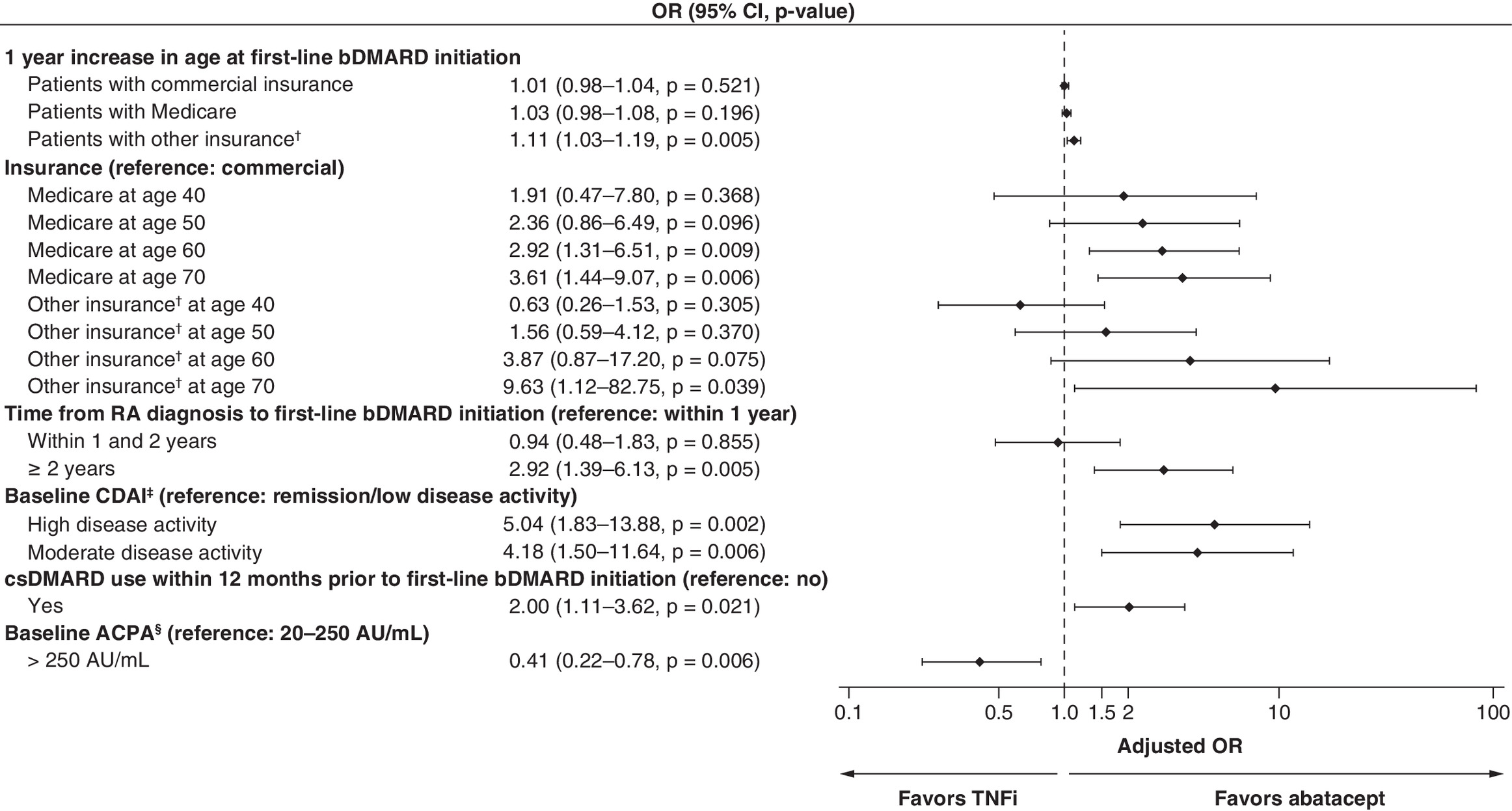
Figure 1. Odds ratios of receiving abatacept versus a tumor necrosis factor inhibitor as a first-line biologic disease-modifying antirheumatic drug.
The multivariate analysis adjusted for age at RA diagnosis, age at 1L initiation, sex, race, ethnicity, insurance, provider practice setting, provider regional location, time from RA diagnosis to 1L initiation, BMI, CCI, smoking, extra-articular manifestations, presence of congestive heart failure, presence of chronic obstructive pulmonary disease, corticosteroid use, baseline ACPA, baseline CDAI, baseline swollen joint count, baseline tender joint count, baseline evaluator global assessment, baseline Physician Global Assessment, csDMARD use within 12 months prior to first-line initiation, use of nonsteroidal anti-inflammatory drugs within 12 months prior to first-line initiation, use of opioids within the 12 months prior to first-line initiation, and route of administration. The reported OR and final model adjusted for the interaction of age and insurance (continuous) and age and insurance (categorical), time to diagnosis to 1L treatment, baseline ACPA (categorical), baseline CDAI (categorical) and csDMARD use within 12 months prior to first-line treatment.
†Includes patients with Medicaid, military coverage (e.g., Tricare/Veterans Affairs) and self-pay patients.
‡Baseline CDAI assessed within 3 months prior to/at initiation of first-line bDMARD, where remission/low disease activity is ≤10, moderate disease activity is >10 and ≤22 and high disease activity is >22 [24].
§ACPA measured within 12-month period prior to/at initiation of first-line bDMARD, and value closest to initiation is reported (if more than one entered).
ACPA: Anticitrullinated protein antibody; bDMARD: Biologic disease-modifying antirheumatic drug; CDAI: Clinical disease activity index; CI: Confidence interval; csDMARD: Conventional synthetic disease-modifying antirheumatic drug; OR: Odds ratio; RA: Rheumatoid arthritis; TNFi: Tumor necrosis factor inhibitor.
Data from this figure were previously presented at ACR Convergence 2022; 10–14 November 2022; PA, USA (poster 1417).
Patients with a high CDAI score at initiation of first-line bDMARD were more likely to initiate abatacept than a TNFi versus patients with low disease activity (OR [95% CI]: 5.04 [1.83–13.88]; p = 0.002). Similarly, patients with a moderate CDAI score were more likely to initiate abatacept than a TNFi versus patients with low disease activity (OR [95% CI]: 4.18 [1.50–11.64]; p = 0.006). Patients who used csDMARDs (other than MTX) within the 12 months prior to first-line bDMARD initiation were more likely to initiate abatacept than a TNFi versus patients who did not use csDMARDs (OR [95% CI]: 2.00 [1.11–3.62]; p = 0.021).
Additionally, patients with Medicare and other insurance (as opposed to commercial coverage) were more likely to initiate abatacept than a TNFi as a first-line bDMARD as age increased. For example, patients at 70 years of age with Medicare insurance were more likely to initiate abatacept than a TNFi (OR [95% CI]: 3.61 [1.44–9.07]; p = 0.006).
Patients with baseline ACPA levels >250 AU/ml had lower adjusted odds than patients with baseline ACPA levels 20–250 AU/ml of initiating abatacept than a TNFi as a first-line bDMARD (OR [95% CI]: 0.41 [0.22–0.78]; p = 0.006).
Discussion
In this large, real-world study of patients with ACPA+/RF+ RA, factors potentially associated with greater odds of initiating abatacept as a first-line bDMARD over a TNFi included longer time (>2 years) from diagnosis to first-line bDMARD initiation, prior csDMARD use, and moderate/high baseline CDAI. Additionally, older patients and those who had Medicare/other noncommercial insurance were also more likely to receive abatacept than a TNFi.
Patient characteristics at the time of diagnosis have been explored for predicting response to treatment and for aiding treatment decisions [29–32]. In general, patients with RA who present with poor prognostic factors (such as seropositivity, either ACPA and/or RF; highly active disease, presence of erosions, presence of extra-articular manifestations and/or comorbidities) are at an increased risk of disease progression [6,33]. As such, it has been noted that poor prognostic factors were considered in the development of the most recent ACR guidelines for the treatment of RA. These factors may influence physicians and patients when deciding upon an appropriate treatment course [15,29,32]. However, clinical practice guidelines also refer to bDMARDs as a class and provide minimal guidance on the optimal selection, sequence or combinations of treatments for different patient populations.
Clinical trial and real-world evidence suggest that abatacept demonstrates greater improvements in clinical response compared with TNFis in patients with poor prognostic features, including dual seropositivity, high baseline ACPA titer and moderate-to-high disease activity [22,23,34–39]. TNFis, in contrast, are more commonly selected as the first-line bDMARD and may be a suitable option for patients with lower disease activity, those with negative or unknown biomarkers or patients with fewer medical comorbidities [40]. In the present analysis, influence of prognostic factors on treatment selection revealed mixed results. There was greater likelihood of initiating abatacept over a TNFi among patients with poorer prognostic factors, including moderate/high disease activity and delayed treatment initiation, and patients who initiated abatacept as a first-line bDMARD were more likely to have extra-articular manifestations and comorbidities/chronic conditions. However, patients with ACPA+/RF+ RA and baseline ACPA levels >250 AU/ml (versus 20–250 AU/ml) were less likely to initiate abatacept than a TNFi as a first-line bDMARD.
These data suggest that factors beyond patient characteristics and anticipated efficacy and safety – such as provider familiarity, insurance coverage and treatment adherence – have an influence on bDMARD selection. One of the most influential determinants of treatment choice, particularly for elderly patients, is insurance coverage. This can be a key deciding factor in the shared decision-making process [41]. In the US, persons aged ≥65 become eligible for one or more of four parts (A–D) of Medicare federal health insurance [42–44]. Because each Medicare part covers different services (inpatient versus outpatient services, drugs taken at home versus those received in clinic), the accessibility of abatacept versus TNFi to Medicare patients can depend on the type of Medicare coverage. In addition, insurance policies such as prior authorization and step therapy (or ‘fail first’) requirements in Medicare plans are prevalent, and these can also influence whether a TNFi or abatacept will be reimbursed as a first-line therapy [45]. Similarly, the joint US federal and state Medicaid insurance program for low-income individuals has prior authorization and ‘fail first’ step therapy requirements that influence the accessibility of abatacept versus TNFi [46]. Thus, societal factors (e.g., socioeconomic status) can play a key role in treatment choice. In patients with Medicare or Medicaid insurance, it may be that these requirements play a role in the prevalent access to TNFi as first-line biologic therapy (e.g., earlier in the course of disease) [47,48]. This aligns with the results of our analysis, which show that as patients increase in age, disease severity and treatment experience, abatacept becomes the first-line biologic of choice. Additional research is needed to understand the weight of these factors, for both patients and clinicians, in shared decision-making.
Limitations of this study include common inherent limitations of observational research studies and the potential introduction (by not accounting for all patient characteristics that may influence physician prescribing decisions) of unmeasured and residual confounding that cannot be accounted for in descriptive, univariate, multivariate, or subgroup analyses. The selection procedures for participating rheumatologists and patients potentially restrict the external generalizability of the results (data are not available to describe nonparticipating providers or nonselected patients). While this analysis included >500 patients across 28 rheumatology clinics, the purposive sampling used in this analysis meant that rheumatologists and patients were recruited based on prespecified criteria and therefore may not be representative of all patients with ACPA+/RF+ RA or of all rheumatologists, particularly outside of the US. As a medical chart review study, the accuracy and completeness of the data collected were limited by the quality of the data in the patient electronic medical records, and treatment adherence was not recorded. Selection bias (unequal probability of patient selection from all eligible charts), missing/incomplete data may also have occurred; however, selection bias was mitigated by advising rheumatologists to select all potentially eligible patients consecutively for chart abstraction. These data, while informative, reiterate the need to account for differences in patient demographic, clinical and treatment-related characteristics observed across treatment cohorts when assessing relative effectiveness of bDMARDs.
Strengths of this analysis include the retrospective medical chart review design, which provides in-depth data describing outcomes of treatment sequencing, including patient demographic and disease characteristics by using an efficient, reliable and verifiable method. The chart review approach allowed access to data contained in unstructured files in the patient electronic medical record (e.g., disease activity/response, clinical notes, radiologic assessments) and potentially, to contemporaneous data collection (as abstraction may occur using the patient’s most recent visit). Multiple clinically relevant data points were collected by treating rheumatologists. The data were abstracted by the patients’ treating rheumatologists, ensuring collection of high-quality data independent of assumptions by third-party abstractors.
Conclusion
In this real-world study of patients with ACPA+/RF+ RA, potential factors associated with greater odds of initiating abatacept as first-line bDMARD over a TNFi were identified. Patients with longer time (>2 years) from RA diagnosis, a higher burden of extra-articular manifestations and comorbidities, prescription of csDMARDs within 12 months, or moderate/high disease activity were more likely to initiate abatacept than a TNFi as a first-line bDMARD. An association between insurance status and increasing age was also observed. This analysis revealed a disconnect between evidence demonstrating increased benefit of abatacept treatment for patients with high ACPA levels at diagnosis and the observed lower likelihood of its use as first-line bDMARD. Results of this study underscore the need to understand better other potential drivers (e.g., tolerability, response and accessibility) behind associations observed between patient characteristics and first-line bDMARD treatment selection.
Summary points
•
Rheumatoid arthritis (RA) is a chronic autoimmune disease that affects an estimated 1.3 million adults in the US and can be complicated by the presence of poor prognostic factors such as anticitrullinated protein antibodies (ACPA), rheumatoid factor (RF), extra-articular manifestations and comorbidities.
•
Although treatment guidelines are available for RA, there is little guidance for the sequence of biologic disease-modifying antirheumatic drugs (bDMARDs) following conventional synthetic (cs) DMARD failure.
•
This analysis aimed to compare demographic and clinical characteristics of patients with RA who were both ACPA+ and RF+ and initiated abatacept (n = 301) or a tumor necrosis factor inhibitor (TNFi) (n = 203) as a first-line bDMARD, and to identify factors associated with first-line bDMARD selection in the real-world setting.
•
Analysis showed that initiation of abatacept as a first-line bDMARD (versus a TNFi) was significantly associated with older age at bDMARD initiation, having Medicare insurance coverage, being >2 years since RA diagnosis (all p < 0.001), and the presence of extra-articular manifestations and congestive heart failure (p < 0.05 for each).
•
Additionally, a higher proportion of patients who initiated abatacept (versus a TNFi) had specific comorbidities: chronic obstructive pulmonary disease, Type 2 diabetes, mild liver disease and obesity.
•
The odds of initiating abatacept (versus a TNFi) were greater among patients with >2 years from RA diagnosis (odds ratio [OR] 2.9), patients with a high clinical disease activity index (CDAI) score (OR 5.0), patients with a moderate CDAI score (OR 4.2) and patients who used csDMARDs within the 12 months prior to bDMARD initiation (OR 2.0).
•
An association was also observed between insurance status and increasing age.
•
These data underscore the need for consideration of many different prognostic factors by clinicians when discussing and deciding on a treatment pathway with their patients.
•
Further analysis is required to understand potential drivers behind first-line bDMARD treatment selection for patients with ACPA+/RF+ RA fully.
Author contributions
G Lam, H Zheng, A Klink, V Patel, L N'Dri, K Wittstock, C Brown-Bickerstaff, V Khaychuk and B Feinberg were responsible for study conception and design of the analysis. P Asgarisabet, E Bland, C Brown-Bickerstaff, B Feinberg and A Klink were responsible for data acquisition. E Bland and P Asgarisabet were responsible for data analysis. G Lam, H Zheng, A Klink, V Patel, E Bland, L N'Dri, P Asgarisabet, C Brown-Bickerstaff, M Chaballa and B Feinberg were responsible for data interpretation. All authors were responsible for drafting the work or reviewing it critically for important intellectual content and final approval of the version to be published.
Acknowledgments
The authors thank the Cardinal Health Research Operations team for assistance with data acquisition and William John of Cardinal Health for assistance with early drafts of the manuscript.
Financial disclosure
This study was funded by Bristol Myers Squibb.
Competing interests disclosure
G Lam has received speaking and consulting fees from AbbVie, Bristol Myers Squibb, Cardinal Health, Janssen, Pfizer, Sanofi Genzyme, and UCB. H Zheng is a pre-doctoral fellow at Bristol Myers Squibb. A Klink is an employee of and owns equity stock in Cardinal Health. V Patel, L N'Dri, K Wittstock, M Chaballa and V Khaychuk are employees of and own equity stock in Bristol Myers Squibb. E Bland and P Asgarisabet are employees of Cardinal Health. C Brown-Bickerstaff was an employee of Cardinal Health at the time of the analysis and is currently employed at Ontada, Irving, TX, USA. B Feinberg has nothing to disclose. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Professional medical writing and editorial assistance was provided by Rachel Rankin at Caudex, a division of IPG Health Medical Communications, and was funded by Bristol Myers Squibb.
Ethical conduct of research
This study was conducted in accordance with International Society for Pharmacoepidemiology Guidelines for Good Epidemiology Practices, the Professional Society for Health Economics and Outcomes Research and the Strengthening the Reporting of Observational Studies in Epidemiology guidelines and the ethical principles in the Declaration of Helsinki. Rheumatologists were required to be able to participate in research monitored by a central institutional review board (IRB; 20204039). The protocol, amendments, eCRF and waiver of patient informed consent (due to the minimal amount of protected health information collected) received IRB approval from the Western Institutional Review Board.
Data sharing statement
All datasets on which the conclusions of the manuscript report are available on request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Almutairi K, Nossent J, Preen D, Keen H, Inderjeeth C. The global prevalence of rheumatoid arthritis: a meta-analysis based on a systematic review. Rheumatol. Int. 41(5), 863–877 (2021).
2.
Hunter TM, Boytsov NN, Zhang X, Schroeder K, Michaud K, Araujo AB. Prevalence of rheumatoid arthritis in the United States adult population in healthcare claims databases, 2004–2014. Rheumatol. Int. 37(9), 1551–1557 (2017).
3.
Xu Y, Wu Q. Prevalence trend and disparities in rheumatoid arthritis among US adults, 2005–2018. J. Clin. Med. 10(15), 3289 (2021).
4.
Helmick CG, Felson DT, Lawrence RC et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part I. Arthritis Rheum. 58(1), 15–25 (2008).
5.
Emery P, Gottenberg JE, Rubbert-Roth A et al. Rituximab versus an alternative TNF inhibitor in patients with rheumatoid arthritis who failed to respond to a single previous TNF inhibitor: SWITCH-RA, a global, observational, comparative effectiveness study. Ann. Rheum. Dis. 74(6), 979–984 (2015).
6.
Hecht C, Englbrecht M, Rech J et al. Additive effect of anti-citrullinated protein antibodies and rheumatoid factor on bone erosions in patients with RA. Ann. Rheum. Dis. 74(12), 2151–2156 (2015).
7.
Ajeganova S, Humphreys JH, Verheul MK et al. Anticitrullinated protein antibodies and rheumatoid factor are associated with increased mortality but with different causes of death in patients with rheumatoid arthritis: a longitudinal study in three European cohorts. Ann. Rheum. Dis. 75(11), 1924–1932 (2016).
8.
Xie S, Li S, Chen B, Zhu Q, Xu L, Li F. Serum anti-citrullinated protein antibodies and rheumatoid factor increase the risk of rheumatoid arthritis-related interstitial lung disease: a meta-analysis. Clin. Rheumatol. 40(11), 4533–4543 (2021).
9.
Liu J, Gao J, Wu Z et al. Anti-citrullinated protein antibody generation, pathogenesis, clinical application, and prospects. Front. Med. (Lausanne) 8, 802934 (2022).
10.
Jilani AA, Mackworth-Young CG. The role of citrullinated protein antibodies in predicting erosive disease in rheumatoid arthritis: a systematic literature review and meta-analysis. Int. J. Rheumatol. 2015, 728610 (2015).
11.
Seegobin SD, Ma MH, Dahanayake C et al. ACPA-positive and ACPA-negative rheumatoid arthritis differ in their requirements for combination DMARDs and corticosteroids: secondary analysis of a randomized controlled trial. Arthritis Res. Ther. 16(1), R13 (2014).
12.
Endo Y, Koga T, Kawashiri SY et al. Anti-citrullinated protein antibody titre as a predictor of abatacept treatment persistence in patients with rheumatoid arthritis: a prospective cohort study in Japan. Scand. J. Rheumatol. 49(1), 13–17 (2020).
13.
Eloff E, Martinsson K, Ziegelasch M et al. Autoantibodies are major predictors of arthritis development in patients with anti-citrullinated protein antibodies and musculoskeletal pain. Scand. J. Rheumatol. 50(3), 189–197 (2021).
14.
Alten R, Mariette X, Flipo RM et al. Retention of subcutaneous abatacept for the treatment of rheumatoid arthritis: real-world results from the ASCORE study: an international 2-year observational study. Clin. Rheumatol. 41(8), 2361–2373 (2022).
15.
Fraenkel L, Bathon JM, England BR et al. 2021 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 73(7), 1108–1123 (2021).
16.
Smolen JS, Landewé RBM, Bergstra SA et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann. Rheum. Dis. 82(1), 3–18 (2022).
17.
Malmstrom V, Catrina AI, Klareskog L. The immunopathogenesis of seropositive rheumatoid arthritis: from triggering to targeting. Nat. Rev. Immunol. 17(1), 60–75 (2017).
18.
Westhovens R, Robles M, Ximenes AC et al. Clinical efficacy and safety of abatacept in methotrexate-naive patients with early rheumatoid arthritis and poor prognostic factors. Ann. Rheum. Dis. 68(12), 1870–1877 (2009).
19.
Rech J, Tascilar K, Hagen M et al. Abatacept inhibits inflammation and onset of rheumatoid arthritis in individuals at high risk (ARIAA): a randomised, international, multicentre, double-blind, placebo-controlled trial. Lancet 403(10429), 850–859 (2024).
20.
Cope AP, Jasenecova M, Vasconcelos JC et al. Abatacept in individuals at high risk of rheumatoid arthritis (APIPPRA): a randomised, double-blind, multicentre, parallel, placebo-controlled, phase 2b clinical trial. Lancet 403(10429), 838–849 (2024).
21.
Balanean A, Brown-Bickerstaff C, Klink A et al. Real-world clinical outcomes and rationale for initiating abatacept as a first-line biologic for patients with anticitrullinated protein antibody- and rheumatoid factor-positive rheumatoid arthritis. J. Comp. Eff. Res. 13(12), e230144 (2024).
22.
Fleischmann R, Weinblatt M, Ahmad H et al. Efficacy of abatacept and adalimumab in patients with early rheumatoid arthritis with multiple poor prognostic factors: post hoc analysis of a randomized controlled clinical trial (AMPLE). Rheumatol. Ther. 6(4), 559–571 (2019).
• This post hoc analysis of clinical trial data provided evidence of dual seropositivity (RF+ and ACPA+) as a predictive biomarker of greater improvements in disease activity and physical function with abatacept versus TNFi adalimumab.
23.
Sokolove J, Schiff M, Fleischmann R et al. Impact of baseline anti-cyclic citrullinated peptide 2 antibody titre on efficacy outcomes following treatment with subcutaneous abatacept or adalimumab: 2-year results from the AMPLE trial. Ann. Rheum. Dis. 74(Suppl. 2), 983–984 (2015).
• The AMPLE trial provided evidence that patients with rheumatoid arthritis (RA) with high baseline anti-CCP2 levels had better clinical response to abatacept compared with patients with lower levels, and anticitrullinated protein antibody (ACPA) positivity was associated with better clinical response to treatment with abatacept than adalimumab.
24.
Aletaha D, Smolen J. The Simplified Disease Activity Index (SDAI) and the Clinical Disease Activity Index (CDAI): a review of their usefulness and validity in rheumatoid arthritis. Clin. Exp. Rheumatol. 23(39 Suppl. 5), S100–S108 (2005).
25.
International Society for Pharmacoepidemiology. Guidelines for good pharmacoepidemiology practices (GPP). Pharmacoepidemiol. Drug Saf. 25(1), 2–10 (2016).
26.
Berger ML, Sox H, Willke RJ et al. Good practices for real-world data studies of treatment and/or comparative effectiveness: Recommendations from the joint ISPOR-ISPE special task force on real-world evidence in health care decision making. Value Health 20(8), 1003–1008 (2017).
27.
von Elm E, Altman DG, Egger M et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 4(10), e296 (2007).
28.
World Medical Association Declaration of Helsinki. Recommendations guiding physicians in biomedical research involving human subjects. JAMA 277(11), 925–926 (1997).
29.
Muñoz-Fernández S, Otón-Sánchez T, Carmona L et al. Use of prognostic factors of rheumatoid arthritis in clinical practice and perception of their predictive capacity before and after exposure to evidence. Rheumatol. Int. 38(12), 2289–2296 (2018).
30.
Jansen DTSL, Emery P, Smolen JS et al. Conversion to seronegative status after abatacept treatment in patients with early and poor prognostic rheumatoid arthritis is associated with better radiographic outcomes and sustained remission: post hoc analysis of the AGREE study. RMD Open 4(1), e000564 (2018).
31.
Alemao E, Litman HJ, Connolly SE et al. Do poor prognostic factors in rheumatoid arthritis affect treatment choices and outcomes? Analysis of a US rheumatoid arthritis registry. J. Rheumatol. 45(10), 1353–1360 (2018).
32.
Albrecht K, Zink A. Poor prognostic factors guiding treatment decisions in rheumatoid arthritis patients: a review of data from randomized clinical trials and cohort studies. Arthritis Res. Ther. 19(1), 68 (2017).
33.
Visser K, Goekoop-Ruiterman YP, de Vries-Bouwstra JK et al. A matrix risk model for the prediction of rapid radiographic progression in patients with rheumatoid arthritis receiving different dynamic treatment strategies: post hoc analyses from the BeSt study. Ann. Rheum. Dis. 69(7), 1333–1337 (2010).
34.
Harrold LR, Bryson J, Lehman T et al. Association between baseline anti-cyclic citrullinated peptide antibodies and 6-month clinical response following abatacept or TNF inhibitor treatment: a real-world analysis of biologic-experienced patients with RA. Rheumatol. Ther. 8(2), 937–953 (2021).
• Among a real-world cohort of patients treated with abatacept, higher baseline anti-CCP2 concentration was associated with greater improvements in Clinical Disease Activity Index (CDAI) score and patient-reported outcomes compared with patients who had low baseline anti-CCP2. No association between anti-CCP2 concentration and treatment response was observed among patients treated with tumor necrosis factor inhibitors (TNFis).
35.
Harrold LR, Wittstock K, Kelly S et al. Comparative effectiveness of abatacept versus TNF inhibitors in rheumatoid arthritis patients who are ACPA and shared epitope positive. Adv. Rheumatol. 64(1), 10 (2024).
• In this real-world cohort of patients with HLA-DRB1 shared epitope-positive and ACPA+ RA, patients treated with abatacept had better efficacy outcomes – in particular, greater improvements in CDAI scores – compared with patients who received TNFis.
36.
Harrold LR, Litman HJ, Connolly SE et al. Effect of anticitrullinated protein antibody status on response to abatacept or antitumor necrosis factor-alpha therapy in patients with rheumatoid arthritis: A US national observational study. J. Rheumatol. 45(1), 32–39 (2018).
• In this US-based registry analysis, patients with ACPA+ RA at baseline were more likely to achieve a CDAI response with abatacept – but not TNFis – compared with patients who were ACPA negative.
37.
Choy E, Groves L, Sugrue D et al. Outcomes in rheumatoid arthritis patients treated with abatacept: a UK multi-centre observational study. BMC Rheumatol. 5(1), 3 (2021).
38.
Mohamed Ahamada M, Wu X. Analysis of efficacy and safety of abatacept for rheumatoid arthritis: systematic review and meta-analysis. Clin. Exp. Rheumatol. 41(9), 1882–1900 (2023).
39.
Alemao E, Postema R, Elbez Y, Mamane C, Finckh A. Presence of anti-cyclic citrullinated peptide antibodies is associated with better treatment response to abatacept but not to TNF inhibitors in patients with rheumatoid arthritis: a meta-analysis. Clin. Exp. Rheumatol. 38(3), 455–466 (2020).
• This meta-analysis of 18 systematic literature reviews revealed that patients with ACPA-positive RA were more likely to achieve EULAR and ACR20 response compared with patients who had ACPA-negative RA; however, there was not an association between ACPA status and response to TNFi treatment.
40.
Frisell T, Bower H, Morin M et al. Safety of biological and targeted synthetic disease-modifying antirheumatic drugs for rheumatoid arthritis as used in clinical practice: results from the ARTIS programme. Ann. Rheum. Dis. 82(5), 601–610 (2023).
• Observational real-world data from this cohort of Swedish patients with RA support that approved tsDMARDs and bDMARDs have acceptable safety profiles, but there are important differences in treatment tolerability, infection risks, and specific rare, serious outcomes.
41.
Binder-Finnema P, Dzurilla K, Hsiao B, Fraenkel L. Qualitative exploration of triangulated, shared decision-making in rheumatoid arthritis. Arthritis Care Res. (Hoboken) 71(12), 1576–1582 (2019).
42.
U.S. Department of Health and Human Services. Medicare and Medicaid. (Accessed: 24 September 2025). https://www.hhs.gov/answers/medicare-and-medicaid/index.html
43.
U.S. Department of Health and Human Services. Medicare and Medicaid. Who's eligible for Medicare? (Accessed: 24 September 2025). https://www.hhs.gov/answers/medicare-and-medicaid/who-is-eligible-for-medicare/index.html
44.
U.S. Department of Health and Human Services. Medicare and Medicaid. Who's eligible for Medicaid? (Accessed: 24 September 2025). https://www.hhs.gov/answers/medicare-and-medicaid/who-is-eligible-for-medicaid/index.html
45.
Yazdany J, Dudley RA, Chen R, Lin GA, Tseng CW. Coverage for high-cost specialty drugs for rheumatoid arthritis in Medicare Part D. Arthritis Rheumatol. 67(6), 1474–1480 (2015).
46.
Medicaid and CHIP Payment and Access Commission (MACPAC). Prior authorization in Medicaid. (Accessed: 24 September 2025). https://www.macpac.gov/wp-content/uploads/2024/08/Prior-Authorization-in-Medicaid.pdf
47.
Zhang J, Xie F, Delzell E et al. Trends in the use of biologic agents among rheumatoid arthritis patients enrolled in the US Medicare program. Arthritis Care Res. (Hoboken) 65(11), 1743–1751 (2013).
48.
Jin Y, Desai RJ, Liu J, Choi NK, Kim SC. Factors associated with initial or subsequent choice of biologic disease-modifying antirheumatic drugs for treatment of rheumatoid arthritis. Arthritis Res. Ther. 19(1), 159 (2017).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 29 April 2025
Accepted: 22 December 2025
Published online: 27 January 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
First-line tumor necrosis factor inhibitor versus abatacept treatment choice in real-world patients with anticitrullinated protein antibody- and rheumatoid factor-positive rheumatoid arthritis. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0062
Export citation
Select the citation format you wish to export for this article or chapter.