Indirect treatment comparison of iptacopan versus pegcetacoplan for patients with paroxysmal nocturnal hemoglobinuria and residual anemia despite C5 inhibitor treatment
Publication: Journal of Comparative Effectiveness Research
Abstract
This study conducted an indirect treatment comparison (ITC) of iptacopan, the first oral monotherapy targeting factor B, versus pegcetacoplan, a subcutaneous infusion targeting complement component 3, in patients with paroxysmal nocturnal hemoglobinuria (PNH) and residual anemia despite complement component 5 inhibitors (C5i). An unanchored matching adjusted ITC was performed, using phase III APPLY-PNH and PEGASUS studies, identified by a systematic literature review. The outcomes were: change from baseline (CfB) in hemoglobin (Hb), with and without post-transfusion data, CfB in lactate dehydrogenase (LDH), CfB in Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue score, transfusion avoidance, and serious adverse events. Two adjustment scenarios were analyzed: (A) baseline Hb, sex, transfusion history ≤12 months, and (B) scenario A plus reticulocyte count, baseline LDH and age. After matching and adjusting, baseline characteristics were similar across trials. Iptacopan showed greater Hb improvements than pegcetacoplan with post-transfusion data (mean difference – scenario A: 1.05 g/dl; p < 0.001, scenario B: 0.76 g/dl; p = 0.018) and without (A: 1.31 g/dl; p < 0.001, B: 1.01 g/dl; p = 0.014). Odds of transfusion avoidance were higher with iptacopan (A: odds ratio [OR] = 9.17, p = 0.013; B: OR = 12.71, p = 0.009). No significant difference was noted in CfB in LDH and FACIT-Fatigue score. These findings suggest that iptacopan may improve Hb levels and reduce transfusion dependency compared with pegcetacoplan in PNH patients with residual anemia despite C5i and must be interpreted in the context of ITCs.
Plain language summary
What is this article about?
This study compared two newer medications for paroxysmal nocturnal hemoglobinuria (PNH), iptacopan and pegcetacoplan, to see which works better for patients who are still experiencing anemia despite standard treatment. Because no clinical trial has compared these drugs directly, a statistical method was used to match patient data from two separate studies, ensuring the groups were as similar as possible in areas like starting hemoglobin levels and previous transfusion history.
What were the results?
The results showed that patients taking iptacopan had significantly greater improvements in their hemoglobin levels and were much more likely to avoid the need for blood transfusions compared with those on pegcetacoplan. However, there were no significant differences between the two drugs in reducing fatigue or hemolysis.
What do the results mean?
While these findings suggest iptacopan may be more effective at raising hemoglobin levels and reducing transfusion dependency, they are associated with limitations because they are based on a small number of patients and should be confirmed with future direct comparisons.
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare blood disorder caused by nonmalignant, acquired mutations in the PIGA gene in hematopoietic stem cells [1]. The mutations lead to uncontrolled complement activation and the production of CD55 and CD59 glycoprotein-deficient red blood cells that are particularly susceptible to destruction by the complement system [2]. PNH is characterized by hemolytic anemia, thrombosis and bone marrow failure [1]. The prognosis for PNH was poor prior to the availability of complement inhibitors, with thrombosis as the leading cause of death among these patients [3].
Since 2007 when eculizumab, an inhibitor targeting the complement component 5 (C5) of the complement cascade [4], was approved, survival rates for patients with PNH have improved and are now comparable to those of the general population [5]. Ravulizumab, a re-engineered C5 inhibitor (C5i) with an almost four-times longer terminal half-life than eculizumab [6] became the first alternative C5i treatment for PNH in 2018 [7,8]. Both eculizumab (biweekly dosing) and ravulizumab (every 8 weeks) are administered through intravenous infusions by a healthcare professional.
While clinical trials have shown that eculizumab [9] and ravulizumab [7] reduce the extent of intravascular hemolysis (IVH), improve hemoglobin (Hb), unmet needs persist [10]. Despite C5i treatment, many patients remain anemic due to emerging extravascular hemolysis and experience various symptoms including dyspnea, headaches and fatigue, with negative impact on health-related quality of life. The Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue scores remain below the population average norms [10–15].
Pegcetacoplan is a proximal complement 3 (C3) inhibitor administered as a twice weekly subcutaneous infusion and indicated for the treatment of adult patients with PNH [16] with hemolytic anemia [17]. Its efficacy and safety versus eculizumab were assessed in PNH patients with residual anemia in the PEGASUS trial [18].
Iptacopan is a first-in-class, twice daily oral proximal complement inhibitor monotherapy that targets Factor B to selectively inhibit C3 convertase activation in the alternative complement pathway [19,20]. Iptacopan is indicated for the treatment of adult PNH patients [21], with hemolytic anemia [21,22]. The efficacy and safety of iptacopan versus C5is in adult PNH patients with residual anemia despite previous C5i was assessed in APPLY-PNH [23]. To date, there are no head-to-head clinical trials comparing iptacopan with pegcetacoplan in this patient population.
Estimates of comparative efficacy and safety between treatment alternatives can be used to guide clinical decision making and are also an important component of the health technology assessments (HTA). The primary research question of this analysis was to assess the comparative efficacy and safety of iptacopan and pegcetacoplan for adult patients with PNH and residual anemia despite prior treatment with a C5i. In the absence of head-to-head clinical trials, indirect treatment comparisons (ITCs) can be used to estimate the relative efficacy of treatments [24,25]. Increasingly, ITCs are being included in submissions to regulators and HTA agencies such as National Institute of Health and Care Excellence [26]. While an ITC between these treatments using the Bucher method has been published and was unable to adjust for several key differences between APPLY-PNH and PEGASUS. The present analysis provides additional value by leveraging individual patient data (IPD) from APPLY-PNH to address these differences and analyzed additional outcomes of transfusion avoidance and serious adverse events, enabling a more comprehensive comparative assessment.
Materials & methods
Evidence base
A systematic literature review following methods outlined in the Cochrane Handbook for Systematic Reviews of Interventions v6.3 [27] was conducted to identify published studies that assessed the efficacy and safety of treatments for adults with PNH including those who remained anemic after treatment with any complement inhibitor [28]. Searches of EMBASE, MEDLINE and the Cochrane library were conducted up to 19 April 2023. Grey literature, including relevant conferences and clinical trial registries, were hand-searched. Two clinical trials were identified and considered relevant for the ITC: APPLY-PNH (NCT04558918; iptacopan vs C5i [eculizumab or ravulizumab]) [29] and PEGASUS (NCT03500549; pegcetacoplan vs eculizumab) [30].
ITC feasibility assessment
A comparison of APPLY-PNH and PEGASUS in terms of study design, patient eligibility criteria, end points definitions and timepoints assessed was conducted to explore the feasibility of an ITC and select the most appropriate methods (Supplementary Table 1). Both APPLY-PNH and PEGASUS were phase III, open-label, multicenter, randomized controlled trials comparing iptacopan (APPLY-PNH) or pegcetacoplan (PEGASUS) with an active C5i control arm (eculizumab or ravulizumab in APPLY-PNH and eculizumab in PEGASUS). Most of the study sites for both trials were in North America and Europe. All participants were adults with PNH with residual anemia despite treatment with a stable C5i regimen.
To be eligible for APPLY-PNH, which included patients with Hb <10 g/dL prior to screening, patients were required to have been on a stable C5i regimen for at least 6 months, while for PEGASUS, which included patients with Hb <10.5 g/dl, stable treatment on eculizumab was required for at least 3 months. All trial participants were required to have a PNH diagnosis confirmed via high-sensitivity flow cytometry. Eligibility cut-offs related to platelet, reticulocyte, neutrophil counts at screening and BMI differed between the trials (Supplementary Table 2).
While the key inclusion and exclusion criteria were largely similar between the two trials, there were moderate to substantial imbalances in some of the baseline characteristics, as determined by comparison of the standardized mean differences (SMD) between iptacopan and pegcetacoplan groups. Table 1 presents baseline characteristics for patients in both trials and the imbalances in parameters such as Hb, sex, proportion transfusion free within 12 months prior, etc. The presence of imbalances is an important consideration in the selection of an appropriate ITC method.
The APPLY-PNH trial consisted of a 24-week randomized controlled phase (from day 0 to day 168) during which participants were randomized to initiate iptacopan monotherapy or to continue treatment with their stable C5i regimen (either eculizumab or ravulizumab). In contrast, the PEGASUS trial included a 4-week run-in period (named day -28italic> to day 0italic> in the respective publication) of concomitant administration of pegcetacoplan and eculizumab, after which patients were randomized to receive either pegcetacoplan or eculizumab monotherapy for 16-weeks (named day 1 to day 112 in the publication). The naming of timepoints in PEGASUS trial was aligned to facilitate the comparison to APPLY timepoints with day -28 becoming day 0 and day 112 becoming day 140 (Figure 1). PEGASUS trial reported the key end points for the period of active treatments of 140 days from day -28 (renamed as day 0) to day 112 (renamed day 140).
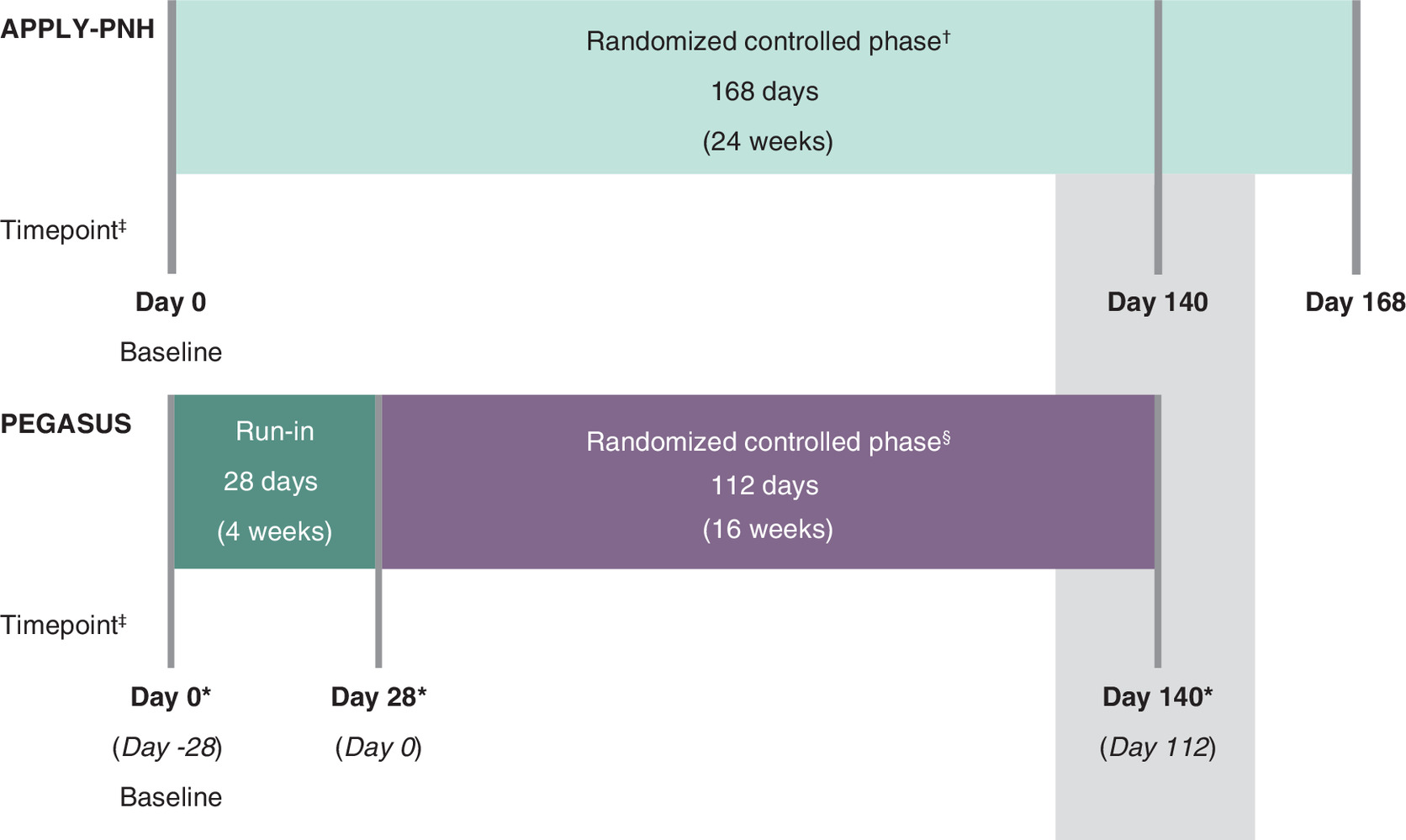
Figure 1. Alignment of assessment timepoints between APPLY-PNH and PEGASUS.
†Patients in the APPLY-PNH trial were randomized to either receive monotherapy with iptacopan or to continue treatment with their stable C5i (either eculizumab or ravulizumab) for the 168-day duration of the randomized controlled phase.
§Patients in the PEGASUS trial were randomized, after the 28-day run-in period, to receive either pegcetacoplan or eculizumab monotherapy for the duration of the 112-day randomized controlled phase.
‡Timepoints were measured from the first dose of the study drug.
*For the PEGASUS trial, the timepoints were re-named with day -28 becoming day 0 and day 112 becoming day 140. The published aggregated results of PEGASUS included the 28-day run-in period, so are reported from day -28 to day 112, therefore the renaming facilitates the understanding and better aligns with APPLY-PNH trial timepoints naming. The original study day naming for PEGASUS is presented in italics.
ITC methods & outcomes selection
The observed imbalances of baseline characteristics between the trials suggest that unadjusted ITCs, such as the Bucher method or network meta-analysis, were not feasible for this analysis. Consequently, population adjustment methods may yield less biased estimates. The availability of IPD from APPLY-PNH and published aggregated data from the PEGASUS trial [18] supported the selection of a matching-adjusted indirect comparison (MAIC), a commonly used ITC method where population adjustments are required. Anchored MAICs are typically preferred as they reduce bias from unmeasured factors; however, they require a common comparator that was administered similarly between trials to ‘anchor’ the analysis [31]. In this case, an anchored MAIC was rendered unfeasible by fundamental differences in the control arm designs of PEGASUS and APPLY-PNH.
While the comparator arm in APPLY-PNH included C5i monotherapy (ravulizumab or eculizumab), the comparator arm in PEGASUS included a run-in period where pegcetacoplan was administered with eculizumab for the first 4 weeks. This run-in likely confounded comparative efficacy; notably, transfusion avoidance in PEGASUS declined from 26 to 15% following pegcetacoplan withdrawal. This suggests that prior pegcetacoplan exposure may attenuate the observed benefit of subsequent C5i therapy on anemia-related end points, rendering the control arms noncomparable. Consequently, given these clinically pertinent differences and the potential for biased anchoring, an unanchored MAIC was considered more appropriate in this case. Anchored MAIC were performed for completeness and transparency, with the caveat that the results should be interpreted with caution due to potential bias arising from the PEGASUS study run-in (Supplementary Tables 3–8).
MAIC was possible in this case as the analysis of IPD available for APPLY-PNH allowed the matching of iptacopan patients by excluding those not meeting the inclusion criteria in PEGASUS and adjustment of imbalances in some baseline characteristics identified as potential treatment effect modifiers following consultation with clinical experts.
Outcomes & timepoints considered for the ITC
Efficacy outcomes of interest for the ITC were the change from baseline (CfB) to day 140 in Hb including all post-transfusion Hb values, CfB to day 140 in Hb excluding all post-transfusion Hb values and the mean difference between treatments was calculated. Similarly mean difference in CfB to day 140 in lactate dehydrogenase (LDH) and FACIT-Fatigue scores were calculated. The difference in transfusion avoidance between treatments is reported as odds ratio (OR) for transfusion avoidance from day 29 to day 140. In addition, serious adverse events (SAE) were compared considering those defined and reported during the active treatment period for each drug in their respective study [18,23] (Supplementary Table 1). No additional interpretation was made for SAEs. Difference in SAEs was reported as OR from day 29 to day 140. Definition of outcomes and alignment of timepoints were validated by clinicians and health economics experts.
Matching for trial eligibility criteria
To ensure that patients who would have been ineligible to enroll in PEGASUS did not contribute to iptacopan effect estimates, IPD from APPLY-PNH were matched to the PEGASUS trial by excluding patients who would not have met the PEGASUS eligibility criteria; APPLY-PNH patients who had a BMI ≥35.0 kg/m2, platelet count ≤ 50 × 109/l, neutrophil count ≤ 500/mm3, or absolute reticulocyte count < 1 x upper limit of normal (ULN) at screening were excluded from the analyses. The Hb eligibility criteria for PEGASUS were broader than for APPLY-PNH, so patients could not be matched for Hb (Supplementary Table 2).
Adjustment for baseline imbalances
After matching, patients in the iptacopan arm of APPLY-PNH were re-weighted via entropy balancing, an information-maximizing re-weighting algorithm that calculates weights so that a re-weighted group can satisfy balance conditions based on known means and standard deviations (SDs) of the comparison group. Histograms of the distribution of patient weights are presented in Supplementary Figures 1 & 2. In this analysis the proportions (for binary variables) and both means and SDs (for continuous variables) were aligned with the values of some baseline characteristics reported in PEGASUS considered as potential treatment effect modifiers [31,32]. These factors were selected following consultations with two UK-based clinical experts specializing in PNH, who were engaged through separate consultation calls to identify key treatment effect modifiers and prognostic factors. During these consultations, the experts identified baseline Hb, transfusion history, reticulocyte count, LDH and a history of major adverse vascular events (MAVE) as the most clinically important variables to be matched in an ideal analysis. However, the maximal set of variables was limited by data availability; specifically, history of MAVE was not reported in the published PEGASUS results and could not be included.
Two scenarios (scenario A and scenario B) adjusting for different factors were analyzed to validate the consistency and robustness of the reported outcomes. Scenario A adjusted for imbalances in three characteristics: baseline Hb, sex, and proportion of patients who were transfusion-free within 12 months prior to baseline. Scenario B adjusted for imbalances in six characteristics: baseline Hb, sex, proportion of patients transfusion-free within 12 months prior to baseline, reticulocyte count at screening, baseline LDH and age.
The performance and suitability of each MAIC scenario were evaluated based on effective sample size (ESS), which is interpreted as the number of independent, non-weighted individuals needed to obtain an equally precise estimate compared with that calculated from the weighted sample. ESS is calculated as the sum of patient weights squared divided by the sum of squared patient weights. The adjustment factors in scenario B represent the maximal feasible set available from reported data; further expansion of this list would have further reduced the ESS and further compromised the reliability of the comparative estimates.
Statistical analyses
For CfB outcomes, effect estimates for iptacopan were derived by fitting a mixed model for repeated measures to the reweighted IPD from APPLY-PNH. Estimates of the mean difference for iptacopan versus pegcetacoplan were derived as the difference between the adjusted mean CfB for iptacopan and the published adjusted mean CfB for pegcetacoplan. Corresponding 95% CIs were estimated using the sum of variances of the adjusted mean CfB for iptacopan and pegcetacoplan.
The effect estimates for transfusion avoidance and SAEs were derived for iptacopan using an intercept-only logistic regression model fitted to the reweighted IPD from APPLY-PNH. An estimate of the log OR for iptacopan versus pegcetacoplan was derived as the difference between the weighted log odds for iptacopan and the estimated log odds for pegcetacoplan based on published transfusions and serious adverse event data from PEGASUS. Corresponding 95% CIs were derived using the sum of variances for the log odds for iptacopan and pegcetacoplan. Point estimates and 95% CIs were transformed to the OR scale for reporting. Nominal significance for all MAIC results was assessed using a two-tailed p-value of <0.05.
Results
Baseline characteristics after matching & adjusting
Of the 62 patients randomized to the iptacopan arm of APPLY-PNH, 54 remained after excluding patients who did not meet key PEGASUS eligibility criteria (Supplementary Table 2). Adjustment for scenario A variables led to an ESS of 16 for the iptacopan arm, while adjustment for scenario B variables led to an ESS of 15. Baseline characteristics for matched patients were well balanced for the adjusted variables after reweighting (Table 1).
| Baseline characteristics† | Pegcetacoplan (PEGASUS) [18] | Iptacopan (APPLY-PNH) | |||||
|---|---|---|---|---|---|---|---|
| Unmatched and unadjusted [23] | Matched and adjusted | ||||||
| Scenario A‡ | Scenario B‡ | ||||||
| n = 41 | n = 62 | SMD | ESS = 16 | SMD | ESS = 15 | SMD | |
| Hb, g/dl, mean (SD) | 8.7 (1.1) | 8.9 (0.7) | 0.186 | 8.7 (1.1) | 0.000 | 8.7 (1.1) | 0.000 |
| Sex; female, n, (%) | 27 (65.9%) | 43 (69.4%) | 0.075 | 66.0% | 0.003 | 66.0% | 0.003 |
| Transfusion free previous 12 months, n, (%) | 10 (24.4%) | 25 (40.3%) | 0.346 | 24.0% | 0.008 | 24.0% | 0.008 |
| Reticulocyte count§, 10-9/l, mean (SD) | 217.5 (75.0) | 204.0 (84.1) | 0.169 | 211.7 (79.3) | 0.075 | 217.6 (76.3) | 0.002 |
| LDH, u/l, mean (SD) | 257.5 (97.6) | 269.1 (70.1) | 0.137 | 260.9 (54.4) | 0.044 | 257.5 (73.5) | 0.000 |
| Age, years, mean (SD) | 50.2 (16.3) | 51.7 (16.9) | 0.091 | 49.1 (14.6) | 0.068 | 50.2 (16.5) | 0.001 |
†
All characteristics were measured at baseline, except for those marked with §, which were measured at screening.
‡
Scenario A adjusted for imbalances in baseline hemoglobin, sex, and proportion transfusion-free within 12 months prior to baseline. Scenario B adjusted for imbalances in baseline hemoglobin, sex, proportion transfusion-free within 12 months prior to baseline, reticulocyte count at screening, baseline LDH and age.
ESS: Effective sample size; Hb: Hemoglobin; LDH: Lactate dehydrogenase; MAIC: Matching-adjusted indirect comparison; SD: Standard deviation; SMD: Standardized mean difference (SMDs ≤ 0.1 indicate a small difference, 0.1 > SMDs ≤ 0.2 indicate a moderate difference and SMDs > 0.2 indicate a substantial statistical, but not necessarily clinical, difference between treatment groups at the initial timepoint).
Clinical outcomes: change in Hb, transfusion avoidance & LDH
In the analysis including post-transfusion Hb values, in scenario A the mean (95% CI) CfB in Hb for patients treated with iptacopan was 3.71 g/dl (3.33, 4.09) compared with the published 2.66 g/dl (2.17, 3.15) among those treated with pegcetacoplan, resulting in a mean difference in CfB in Hb of 1.05 g/dl (0.43, 1.67), p < 0.001, in favor of iptacopan. Similarly, in scenario B iptacopan was also significantly better than pegcetacoplan with a mean difference in CfB in Hb of 0.76 g/dl (95% CI: 0.13, 1.39), p = 0.018 (Figure 2). When post-transfusion data were excluded from the analysis, in scenario A the mean CfB in Hb was 3.68 g/dl (3.33, 4.04) for iptacopan compared with the published 2.37 g/dl (1,66, 3.08) for pegcetacoplan, resulting in a mean difference in CfB in Hb of 1.31 g/dl (0.52, 2.10) p < 0.001 in favor of iptacopan. The CfB in Hb was significantly greater for iptacopan versus pegcetacoplan also in scenario B, with a mean difference in CfB in Hb of 1.01 g/dl (95% CI: 0.21, 1.82) p = 0.014 (Figure 2).
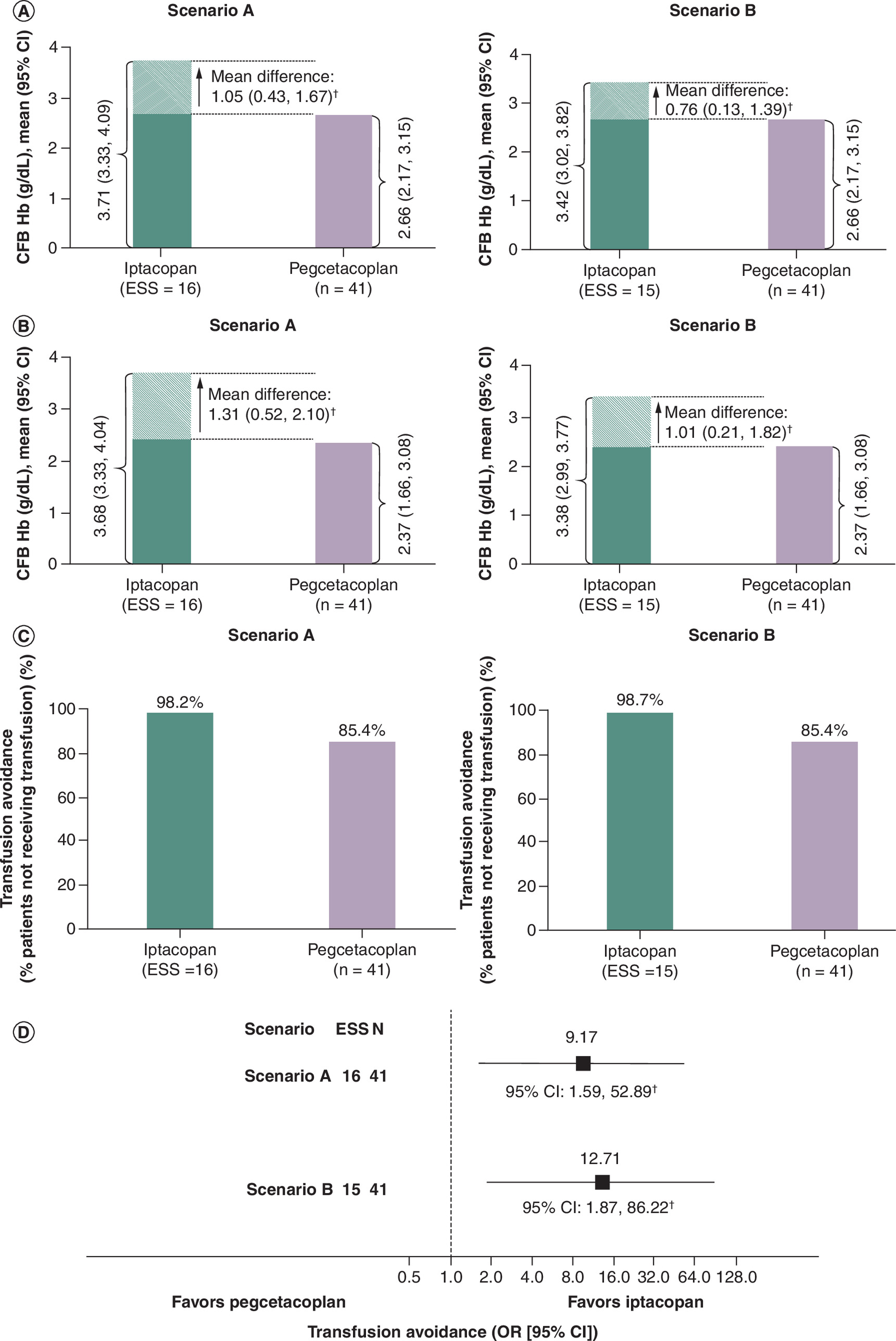
Figure 2. Matching-adjusted indirect comparison results for Hb outcomes and transfusion avoidance for iptacopan versus pegcetacoplan.
(A) Mean change and mean difference in Hb including post-transfusion data. (B) Mean change and mean difference in Hb excluding post-transfusion data. (C) Transfusion avoidance (proportion). (D) Transfusion avoidance (OR).
†Statistically significant, p < 0.05.
CI: Confidence interval; CFB: Change from baseline; ESS: Effective sample size; Hb: Hemoglobin; OR: Odds ratio.
After matching and adjusting the proportion of iptacopan patients who did not receive transfusions between day 29 to day 140 in scenario A were 98.7%, in scenario B 98.2%, compared with published 85.4% of patients without transfusion on pegcetacoplan. The odds of transfusion avoidance for patients treated with iptacopan were significantly greater than those for patients with pegcetacoplan in scenario A (OR: 9.17 [95% CI: 1.59, 52.89]) p = 0.013; and, scenario B (OR: 12.71 [1.87, 86.22]) p = 0.009; (Figure 2).
The mean (SD) baseline LDH levels in PEGASUS and APPLY-PNH (unmatched and unadjusted data) trials, were slightly above the ULN (defined as 226 u/l in PEGASUS and 250 u/l in APPLY-PNH). After matching and adjusting, the mean (SD) baseline LDH for iptacopan in scenario A was 260.9 (54.4) and in scenario B was 257.5 (73.5) (Table 1). The mean (95% CI) CfB to day 140 in LDH levels for iptacopan was 21.68 (-31.61, 74.97) in scenario A, and 19.59 (-31.27, 70.44) in scenario B, while for pegcetacoplan, it was -15.00 (-98.69, 68.69). In both the scenarios, the mean difference in CfB in LDH between iptacopan and pegcetacoplan was not significant (scenario A: 36.68 u/l (-62.54, 135.89), p = 0.469, and scenario B: 34.59 u/l (-63.35, 132.52), p = 0.489) (Table 2).
| CfB in FACIT-Fatigue | CfB in LDH | SAE | |
|---|---|---|---|
| Scenario A | Mean CfB | Mean CfB | Percentage with SAE |
| Iptacopan: ESS = 16 | 6.88 (4.37, 9.39) | 21.68 (-31.61, 74.97) | 4.8% |
| Pegcetacoplan: n = 41 | 9.20 (6.06, 12.34) | -15.00 (-98.69, 68.69) | 17.0% |
| Mean difference (95% CI) | Mean difference (95% CI) | OR (95% CI) | |
| -2.32 (-6.34, 1.70) p = 0.257 | 36.68 (-62.54, 135.89) p = 0.469 | 0.24 (0.06, 0.98) p = 0.047 | |
| Scenario B | Mean CfB | Mean CfB | Percentage with SAE |
| Iptacopan: ESS = 15 | 6.64 (4.20, 9.07) | 19.59 (-31.27, 70.44) | 5.6% |
| Pegcetacoplan: n = 41 | 9.20 (6.06, 12.34) | -15.00 (-98.69, 68.69) | 17.1% |
| Mean difference (95% CI) | Mean difference (95% CI) | OR (95% CI) | |
| -2.56 (-6.53, 1.41) p = 0.206 | 34.59 (-63.35, 132.52) p = 0.489 | 0.29 (0.06, 1.29) p = 0.103 |
CI: Confidence interval; CfB: Change from baseline; ESS: Effective sample size; FACIT-Fatigue: Functional Assessment of Chronic Illness Therapy – Fatigue; LDH: Lactate dehydrogenase; OR: Odds ratio; SAE: Serious adverse event.
Health related quality of life
The reported mean (SD) baseline FACIT-Fatigue score for patients on pegcetacoplan was 32.2 (11.4) [18] and on iptacopan it was 34.7 (9.8) [23]. In the matched and adjusted population, the baseline score in iptacopan arm was 35.1 (10.5) in both scenarios. The mean FACIT-Fatigue score at day 140 for pegcetacoplan was 41.4, and for matched and adjusted population on iptacopan the mean (SD) score was 42.0 (9.5) in scenario A and 41.7 (9.3) in scenario B. The published mean (95% CI) CfB in the score for pegcetacoplan at day 140 was 9.20 (6.06, 12.34), and in the matched and adjusted population for iptacopan 6.88 (4.37, 9.39) in scenario A and 6.64 (4.20, 9.07) in scenario B. The mean difference (95% CI) in CfB in FACIT-Fatigue scores showed no significant difference between iptacopan and pegcetacoplan in scenario A (-2.32 [-6.34, 1.70] p = 0.257) or scenario B (-2.56 [-6.53, 1.41] p = 0.206) (Table 2).
Safety
The percentage of patients who experienced an SAE as reported in pegcetacoplan trial was 17.0% [18] and for iptacopan was 9.7% [23], as per the trial-specific definitions. After matching and adjusting, the percentage of patients experiencing an SAE in iptacopan was 4.8% in scenario A and 5.6% in scenario B. This resulted in lower odds of experiencing an SAE for iptacopan compared with pegcetacoplan, scenario A: OR 0.24 (95% CI: 0.06, 0.98), p = 0.047 and scenario B: OR 0.29 (95% CI: 0.06, 1.29), p = 0.103 (Table 2).
Discussion
Unanchored MAIC was used in this study to assess efficacy and safety outcomes of iptacopan compared with pegcetacoplan in PNH patients with residual anemia despite C5i treatment. This technique matched and adjusted IPD from APPLY-PNH for iptacopan to published data for pegcetacoplan from PEGASUS [18]. Two scenarios were analyzed by adjusting for several clinical characteristics considered by clinical experts as potential treatment effect modifiers. In both scenarios, the results showed a greater increase of Hb favoring iptacopan, when including or excluding post-transfusion data, as well as higher odds of remaining transfusion-free compared with pegcetacoplan. These are two important clinical outcomes when managing PNH patients who remain anemic despite C5i. In most cases these patients have a good control of IVH shown by LDH levels within the normal range but continue to present anemia due to extravascular hemolysis. Many require transfusions in order to manage residual anemia. Switching to a proximal inhibitor such as the oral monotherapy iptacopan may be more beneficial from clinical perspective and more convenient for patients, than using a therapy requiring subcutaneous infusions. More patients have chances to achieve normalized Hb levels in the absence of transfusions when treated with iptacopan.
When looking at results for LDH in this MAIC, the CfB (decrease) in LDH was comparable for both treatments in both scenarios as the difference was not statistically significant. The majority of patients on C5i who switched to pegcetacoplan in PEGASUS18 or iptacopan in APPLY-PNH23 had reasonable control of IVH as shown by the baseline LDH values. At the end of the treatment period the LDH values remained below the ULN suggesting that iptacopan and pegcetacoplan continue to control intravascular hemolysis in this population.
The difference in CfB in FACIT-Fatigue score between iptacopan and pegcetacoplan was not significant. This might be due to higher baseline FACIT-Fatigue score in the iptacopan adjusted and weighted population compared with the pegcetacoplan published baseline score. In addition, at day 140, a ceiling effect was noted as the scores achieved in both treatments were comparable to the general population. Both treatments have a positive impact on fatigue.
The predicted odds of experiencing an SAE were lower for adjusted and weighted population on iptacopan than for those published for pegcetacoplan in both scenarios (statistically significant only in scenario A). Events reported as SAE could differ across both trials, therefore this MAIC assessed SAE as odds of having an event and used the total proportion of patients experiencing any SAE (as per respective trial definition) within a same time frame.
To our knowledge this is the first ITC to use an unanchored MAIC approach to evaluate the efficacy and safety of iptacopan compared with pegcetacoplan in PNH patients with residual anemia despite C5i treatment. A previously published anchored ITC, which used the Bucher method with a confirmatory simulated treatment comparison and found no statistically significant differences between the treatments [35]. However, the analysis considered the control arms a suitable common comparator linking the trials, despite the presence of combination therapy of pegcetacoplan and eculizumab, which was required in the PEGASUS trial as part of the run-in period. The presence of combination therapy in the run-in period is the major difference in study design that impacts the suitability of conducting an anchored ITC using C5i treatment as a common comparator. Furthermore, the analysis was unable to assess transfusion avoidance, due to differences in follow-up times between trials. By leveraging IPD from APPLY-PNH this MAIC was able to align timepoints to compare this end point and address this limitation across all outcomes.
In this analysis comparing two products in an orphan disease, based on only two studies (one having IPD available and one having published aggregated data) the MAIC was determined to be a suitable approach. By leveraging IPD, MAIC provides the flexibility to reduce cross-trial heterogeneity in study design, patient populations, outcomes definitions and assessment timepoints. Overall, most of the key patient eligibility criteria of APPLY-PNH and PEGASUS were similar. Additionally, by excluding patients from the APPLY-PNH IPD who did not satisfy key PEGASUSs inclusion criteria the similarity of population increased. Of the prognostic factors and effect-modifiers identified through expert consultation a priori, many were reported for the APPLY-PNH and PEGASUS and could be adjusted for in the MAIC. Scenarios A and B were selected carefully to adjust for these factors while retaining sufficient ESS in iptacopan population.
The small ESS after matching and adjusting of the iptacopan population may be considered a limitation. However, the initial sample size of the iptacopan arm was small compared with what is generally seen in other diseases, reflecting the orphan status of PNH. Ultimately, the decrease in ESS was a necessary trade-off to allow for a better balance between the trial populations, though resulting estimates should be interpreted with caution. The inability to match for narrower eligibility criteria of the APPLY-PNH population with regards to Hb at baseline (patients with Hb <10.0 g/dl were eligible, whereas in PEGASUS patients with Hb <10.5 g/dl were eligible) is recognized as a limitation; furthermore, the unavailability of IPD for the comparator and potential bias due to cross-trial differences may impact the findings. Despite this, mean Hb levels at baseline were similar between the trials, and the present analyses were able to adjust for the remaining differences, ultimately producing an SMD of zero for both MAIC scenarios.
The present analyses were strengthened by aligning end point definitions including analysis timepoints, based on the date that first dose of study drug was received and with the time spent on the study treatments. Adjustments did produce well balanced prognostic factors in these analyses, with no SMDs over 0.08 for adjusted factors.
Although efforts were made to conduct robust and detailed analyses using unanchored MAIC, there is still potential for bias given the assumptions and limitations associated with all ITCs. In this case, anchored MAICs were deemed unsuitable due to significant differences in the control arms between trials. The PEGASUS trial included a run-in period with pegcetacoplan and eculizumab combination therapy, impacting subsequent eculizumab monotherapy efficacy. This pre-treatment exposure to pegcetacoplan potentially confounded the comparison of eculizumab monotherapy from PEGASUS to eculizumab or ravulizumab from APPLY-PNH leading to unreliable results in an anchored MAIC.
Ultimately, the results of this study cannot fully replace evidence derived from head-to-head trials. These results are hypothesis-generating and should be confirmed in head-to-head or real-world studies. In the context of HTA of rare diseases such as PNH, comparative efficacy data from ITCs are required due to small trial populations and a lack of direct comparison between treatments. Notably, since the systematic literature review search date that informed this study, new complement inhibitors, such as the danicopan, have been approved or become available in various markets. Consequently, separate analyses may be required to compare iptacopan and pegcetacoplan with these new treatments. In addition, future real-world studies could be considered to understand the effect of these drugs in a heterogeneous real-world population.
These exploratory results of this MAIC suggest that iptacopan could offer greater increases in Hb levels and higher odds of transfusion avoidance compared with pegcetacoplan. Thus, these analyses suggest that iptacopan may provide additional benefits for managing residual anemia in C5i-experienced patients with PNH. The comparative efficacy estimates were not significantly different between iptacopan and pegcetacoplan for CfB in FACIT-Fatigue and LDH, suggesting intravascular hemolysis are controlled by both treatments and fatigue was improved in a similar direction. In addition to the potential clinical benefits over pegcetacoplan indicated by these analyses, the oral administration of iptacopan may be a convenient option for patients.
Conclusion
Statistical analyses employing MAIC techniques provide a framework for estimating comparative efficacy in the absence of head-to-head clinical trials and are commonly used in HTA to inform drug reimbursement decision. Given the limitations of the unanchored design and a small ESS, the results suggest that iptacopan may be more effective than pegcetacoplan in improving clinically relevant outcomes for managing PNH, such as increasing Hb levels and allowing patients to be transfusion-free. Ultimately, the potential therapeutic advantages of iptacopan monotherapy should be confirmed in head-to-head clinical trials or real-world studies.
Summary points
•
This study conducted an indirect treatment comparison of iptacopan (an oral monotherapy) versus pegcetacoplan (a subcutaneous infusion) for patients with paroxysmal nocturnal hemoglobinuria (PNH) who still have anemia despite treatment with standard C5 inhibitors.
•
A method called matching-adjusted indirect comparison was used to align individual patient data from the APPLY-PNH trial with published results from the PEGASUS trial.
•
An unanchored design was chosen because differences in trial designs, specifically a 4-week period where PEGASUS patients received combination therapy, made the control groups noncomparable.
•
The comparison focused on several clinical outcomes, including hemoglobin (Hb) levels, transfusion avoidance, fatigue scores, change in lactate dehydrogenase (LDH) and serious adverse events.
•
Across two different adjustment scenarios, iptacopan was associated with significantly greater improvements in hemoglobin and higher odds of avoiding blood transfusions compared with pegcetacoplan.
•
There were no significant differences found between the two treatments regarding improvements in patient-reported fatigue, levels of LDH or serious adverse events.
•
The study is limited by a small effective sample size (15–16 patients) and the exploratory nature of indirect comparisons, meaning results should be confirmed by head-to-head clinical trials.
•
Ultimately, the findings suggest that the oral monotherapy iptacopan may offer clinical and convenience benefits for PNH patients who are not fully responding to standard C5 inhibitor therapy.
Financial disclosure
This research was funded by Novartis Pharma AG, Basel, Switzerland.
Competing interests disclosure
A Kulasekararaj has provided research support (to institution): Celgene/BMS and Novartis; acted as a consultant to: Samsung, NovoNordisk, Alexion/AstraZeneca, Arrowhead, Silence Therapeutics, AdaRx, and Ono Pharma; received speaker’s fees from: Alexion/AstraZeneca, Amgen, Celgene/BMS, Pfizer, Novartis, Ra Pharma/UCB, Roche, SOBI, and Janssen; and participated in scientific advisory boards or data monitoring committees for: Alexion/Astra Zeneca, Apellis, Amgen, Agios, Biocryst, Celgene/BMS, Geron, Novartis, Pfizer, Regeneron, Roche, SOBI, Janssen, and Samsung. P Scheinberg received consulting and speaker fees from AstraZeneca, Novartis, Pfizer, and F. Hoffmann-La Roche. RP de Latour received consulting or speaker fees from Alexion Pharmaceuticals, Amgen, Apellis Pharmaceuticals, Jazz Pharmaceuticals, Novartis, Pfizer, F. Hoffmann-La Roche, and Samsung; received research grants from Alexion Pharmaceuticals, Novartis, and Pfizer. M-M Balp, O Somenzi, J Snellman are employees of Novartis Pharma AG, Basel, Switzerland. A Wiyani is an employee of Novartis Pharmaceuticals UK Ltd, London, UK. S Walsh and J Steenkamp are employees of EVERSANA who received funding from Novartis for conducting the statistical analyses that informed this study. All authors contributed substantially to each component of this work, however, M-M Balp, O Somenzi, A Wiyani, J Snellman and K Pannagl were largely responsible for the conception and design of the study, RP de Latour, A Kulasekararaj and P Scheinberg verified the inputs from a clinical perspective and led the interpretation of the data while J Steenkamp and S Walsh were most responsible for the study selection and statistical analyses. Each author participated in drafting the manuscript and performed a critical review, making any required revisions for veracity and intellectual content. All authors have given their final approval to publish this version and accept accountability for its components. None of the authors have any unresolved questions related to the accuracy or integrity of the work. As of the time of publication, Katharina Pannagl is no longer an employee of Novartis Pharmaceuticals UK Ltd, London, UK. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support for this manuscript was provided by Amanda Griffin, EVERSANA, under the guidance of the authors and in accordance with Good Publication Practice 2022 (GPP 2022) guidelines (https://www.ismpp.org/gpp-2022). Funding for this medical writing assistance was provided by Novartis Pharma AG, Basel, Switzerland.
Acknowledgements
As of the time of publication, Katharina Pannagl is no longer an employee of Novartis Pharmaceuticals UK Ltd, London, UK.
Data sharing statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 211.35 KB
References
Papers of special note have been highlighted as: • of interest
1.
Brodsky R. Paroxysmal nocturnal hemoglobinuria. Blood 124(18), 2804–2811 (2014).
2.
Hill A, DeZern AE, Kinoshita T, Brodsky RA. Paroxysmal nocturnal haemoglobinuria. Nat. Rev. Dis. Primers 3(1), 1–14 (2017).
3.
Hillmen P, Lewis S, Bessler M, Luzzatto L, Dacie JV. Natural history of paroxysmal nocturnal hemoglobinuria. N. Engl. J. Med. 333(19), 1253–1258 (1995).
4.
Food and Drug Administration. Soliris. (2019).
5.
Kelly R, Hill A, Arnold L et al. Long-term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria: sustained efficacy and improved survival. Blood 117(25), 6786–6792 (2011).
6.
Lee J-W, Bachman ES, Aguzzi R et al. Immediate, complete, and sustained inhibition of C5 with ALXN1210 reduces complement-mediated hemolysis in patients with paroxysmal nocturnal hemoglobinuria (PNH): interim analysis of a dose-escalation study. Blood 128(22), 2428 (2016).
7.
Lee J, Sicre de Fontbrune F, Wong Lee Lee L et al. Ravulizumab (ALXN1210) vs eculizumab in adult patients with PNH naive to complement inhibitors: the 301 study. Blood 133(6), 530–539 (2019).
8.
Kulasekararaj AG, Hill A, Rottinghaus ST et al. Ravulizumab (ALXN1210) vs eculizumab in C5-inhibitor–experienced adult patients with PNH: the 302 study. Blood 133(6), 540–549 (2019).
9.
Hillmen P, Hall C, Marsh JC et al. Effect of eculizumab on hemolysis and transfusion requirements in patients with paroxysmal nocturnal hemoglobinuria. N. Engl. J. Med. 350(6), 552–559 (2004).
10.
Risitano AM, Marotta S, Ricci P et al. Anti-complement treatment for paroxysmal nocturnal hemoglobinuria: time for proximal complement inhibition? A position paper from the SAAWP of the EBMT. Front. Immunol. 10, 1157 (2019).
11.
Dingli D, Matos JE, Lehrhaupt K et al. The burden of illness in patients with paroxysmal nocturnal hemoglobinuria receiving treatment with the C5-inhibitors eculizumab or ravulizumab: results from a US patient survey. Ann. Hematol. 101(2), 251–263 (2022).
12.
Panse J, Sicre de Fontbrune F, Burmester P et al. The burden of illness of patients with paroxysmal nocturnal haemoglobinuria receiving C5 inhibitors in France, Germany and the United Kingdom: patient-reported insights on symptoms and quality of life. Eur. J. Haematol. 109(4), 351–363 (2022).
13.
Hillmen P, Young NS, Schubert J et al. The complement inhibitor eculizumab in paroxysmal nocturnal hemoglobinuria. N. Engl. J. Med. 355(12), 1233–1243 (2006).
14.
Debureaux P-E, Kulasekararaj AG, Cacace F et al. Categorizing hematological response to eculizumab in paroxysmal nocturnal hemoglobinuria: a multicenter real-life study. Bone Marrow Transplant. 56(10), 2600–2602 (2021).
15.
Sicre de Fontbrune F, Burmester P, Piggin M et al. The burden of illness of patients with paroxysmal nocturnal haemoglobinuria receiving C5 inhibitors: clinical outcomes and medical encounters from the patient perspective. Hematology 27(1), 1140–1151 (2022).
16.
Food and Drug Administration. Empaveli highlights of prescribing information. (2023). Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2023/215014s002lbl.pdf
17.
European Medicines Agency. Aspaveli (pegcetacoplan) summary of product characteristics (SMPC). (2022). Last updated: 14 June 2022. Available from: Https://www.Ema.Europa.Eu/en/documents/product-information/aspaveli-epar-product-information_en.Pdf
18.
Hillmen P, Szer J, Weitz I et al. Pegcetacoplan versus eculizumab in paroxysmal nocturnal hemoglobinuria. N. Engl. J. Med. 384(11), 1028–1037 (2021).
• Primary publication of one of the clinical trials that informed this indirect treatment comparison (ITC).
19.
Schubart A, Anderson K, Mainolfi N et al. Small-molecule factor B inhibitor for the treatment of complement-mediated diseases. Proc. Natl Acad. Sci. USA 116(16), 7926–7931 (2019).
20.
Risitano AM, Röth A, Soret J et al. Addition of iptacopan, an oral factor B inhibitor, to eculizumab in patients with paroxysmal nocturnal haemoglobinuria and active haemolysis: an open-label, single-arm, Phase II, proof-of-concept trial. Lancet Haematol. 8(5), e344–e354 (2021).
21.
Food and Drug Administration. Fabhalta highlights of prescribing information. (2023). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/218276s001lbl.pdf
22.
European Medicines Agency. Fabhalta summary of product characteristics. (2023). Available from: https://www.ema.europa.eu/en/documents/product-information/fabhalta-epar-product-information_en.pdf
23.
Peffault de Latour R, Roth A, Kulasekararaj A et al. Oral iptacopan monotherapy in paroxysmal nocturnal hemoglobinuria. N. Engl. J. Med. 390(11), 994–1008 (2024).
• Primary publication of one of the clinical trials that informed this ITC.
24.
Phillippo D, Ades T, Dias S et al. NICE DSU TSD 18: Methods for population-adjusted indirect comparisons in submissions to NICE. NICE Decision Support Unit, UK (2016).
• The primary methodological approach used in this ITC.
25.
NICE. NICE Health Technology Evaluations: The Manual [PMG36]. 31 January 2023. Available from: https://www.nice.org.uk/process/pmg36/chapter/introduction-to-health-technology-evaluation
26.
Phillippo DM, Dias S, Elsada A, Ades A, Welton NJ. Population adjustment methods for indirect comparisons: a review of national institute for health and care excellence technology appraisals. Int. J. Technol. Assess. Health Care 35(3), 221–228 (2019).
27.
Higgins J, Thomas J, Chandler J et al. Cochrane Handbook for Systematic Reviews of Interventions, Version 6.3. (2022). Available from: http://www.training.cochrane.org/handbook
28.
Munro I, Shodimu V, Webb N et al. SA52 efficacy of clinical interventions in paroxysmal nocturnal hemoglobinuria patients previously treated with C5 inhibitors: a systematic literature review. Value Health 27(12), S624 (2024).
29.
Novartis Pharmaceuticals. Study of efficacy and safety of twice daily oral LNP023 in adult PNH patients with residual anemia despite anti-C5 antibody treatment (APPLY-PNH). (2020). Available from: https://clinicaltrials.gov/study/NCT04558918?a=7
30.
Apellis Pharmaceuticals Inc. Study to evaluate the efficacy and safety of APL-2 in patients with paroxysmal nocturnal hemoglobinuria (PNH). (2018). Available from: https://clinicaltrials.gov/study/NCT03500549
31.
Remiro-Azocar A, Heath A, Baio G. Methods for population adjustment with limited access to individual patient data: a review and simulation study. Res. Synth. Methods 12(6), 750–775 (2021).
32.
Signorovitch J, Sikirica V, Erder M et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health 15(6), 940–947 (2012).
33.
R Core Team. R: a language and environment for statistical computing. (2021). Available from: https://www.R-project.org/
34.
Hainmueller J. Ebal: entropy reweighting to create balanced samples. (2022). Available from: https://CRAN.R-project.org/package=ebal
35.
de Latour RP, Kulasekararaj A, Dingli D et al. Anchored indirect treatment comparison finds comparable effects of pegcetacoplan and iptacopan in paroxysmal nocturnal haemoglobinuria. Eur. J. Haematol. 115(2), 125–133 (2025).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 11 October 2025
Accepted: 12 February 2026
Published online: 19 March 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Indirect treatment comparison of iptacopan versus pegcetacoplan for patients with paroxysmal nocturnal hemoglobinuria and residual anemia despite C5 inhibitor treatment. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0167
Export citation
Select the citation format you wish to export for this article or chapter.