Performance of stenting in femoropopliteal disease: a systematic literature review and meta-analysis of proportions
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To evaluate the performance of four stent types (BMS, bare metal stents; Eluvia, a polymer-based paclitaxel-eluting stent; Viabahn, a covered stent; and Zilver PTX, a polymer-free paclitaxel-coated stent) in femoropopliteal lesions at 12 and 24 months using a meta-analysis of proportions. Materials & methods: This systematic review (PROSPERO CRD42024528559) used PubMed to identify relevant single-arm and comparative studies (with ≥50 patients/study) published between 1 January 2009 and 1 July 2024. Data on patient/lesion characteristics and outcomes were extracted. Subgroup analyses were based on lesion length (<150 mm vs ≥150 mm) and study quality. A random-intercept logistic regression model was used to pool the data. The 95% CI around the pooled effect was calculated using Knapp–Hartung adjustments. Results: Data were extracted from 141 of the 870 screened studies, corresponding to 35,897 patients. The mean patient age was 70.9 (range: 63.3–80.0) years; 69.6% were male. The overall mean lesion length was 153.1 (range: 37–330) mm. Although all stent types performed well in the main analysis, Eluvia exhibited consistently high primary patency and low target lesion revascularization rates at both timepoints and across lesion lengths. Mortality rates for all stent types were stable for short lesions but more variable for long lesions. Conclusion: All stents used in short lesions performed well; however, Eluvia also demonstrated reliable performance in long lesions.
Plain language summary: How well do stents work for blocked arteries between the hip & the knee: an overview of published evidence
What is this article about?
Stenting is one of the treatments available for narrowed or blocked leg arteries. This study focused on four different stent types that are used in the artery that runs between the hip and the knee. We reviewed the available scientific literature on these stents and then combined the results from different studies to find out how often stenting is successful at keeping the artery open for 1 year and for 2 years. We also looked at the success of stents used in long or short sections of closed off artery.
What were the results?
We combined the results from 141 studies that looked at 35,897 patients overall. The average performance and a range where 95% of the results would fall (the 95% CI) was calculated. Although all stents performed well, one stent infused with a drug had a range that did not overlap with the other stents, this could mean that this stent has a better performance.
Why is this important?
The results of this analysis provide a summary of the performance of the different stent types which can help physicians understand the options available to them.
Peripheral arterial disease (PAD), a chronic vascular condition, is a substantial cause of morbidity, leading to mobility impairment, pain, limb amputation and death [1,2]. Treatment options include lifestyle modifications, pharmacological therapies and revascularization [3].
The femoropopliteal artery is frequently affected in PAD [4]. Endovascular interventions, including plain old balloon angioplasty (POBA) and stent placement, restore blood flow to stenotic or occluded femoropopliteal arteries. Drug-coated balloons are associated with higher patency rates than POBA, reducing the need for reintervention [5]. However, both strategies result in a frequent need for scaffolding to manage acute procedural complications [6]. The requirement for provisional stenting increases with lesion complexity and exceeds 40% in long lesions and chronic total occlusions (CTOs), highlighting the necessity for stent placement in these cases [7].
Despite the widespread use of stents in the treatment of femoropopliteal disease, clinicians face challenges in selecting the most appropriate stent due to limited comparative data. Numerous clinical trials have evaluated self-expanding nitinol stents, drug-eluting stents and covered stents in shorter to moderate-length lesions (reviewed in [8–10]). However, the evidence for longer, more complex real-world lesions is sparse. Additionally, there is a lack of randomized controlled trials (RCTs) directly comparing the effectiveness of different stent types in femoropopliteal lesions [11–13]. Thus, there is a pressing need to systematically evaluate the available evidence on stent performance in femoropopliteal disease. Understanding how different stent types perform across key clinical outcomes will be essential to improving treatment decisions and optimizing patient care.
The present study aimed to systematically review and synthesize the available literature on the four stent types commonly used to treat femoropopliteal disease: bare metal stents (BMS; specifically self-expanding nitinol stents); Eluvia™ (Boston Scientific, MA, USA), a polymer-based paclitaxel-eluting stent; Viabahn® (W. L. Gore and Associates, AZ, USA), a covered stent; and Zilver® PTX® (Cook Medical, IN, USA), a polymer-free paclitaxel-coated stent.
Materials & methods
The protocol was registered with PROSPERO (CRD42024528559). The findings were reported according to the PRISMA checklist (Supplementary Table 1) [14].
A systematic search of PubMed was performed on 30 January 2024 and updated on 8 July 2024. The final search included studies published between January 2009 and July 2024. The PICOS (population, intervention, comparison, outcome, study type) framework was adopted to guide the literature selection process. The full search strategy was published in the PROSPERO protocol. The identified studies were screened for duplicates and relevance using Laser AI (Evidence Prime Inc., Hamilton, Canada; https://www.laser.ai/) and PICO Portal (NY, USA; www.picoportal.org) and organized using the Citavi reference manager (Lumivero, CO, USA).
Studies meeting the following criteria were selected: evaluating the use of a vascular stent of interest in femoropopliteal arteries; reporting at least one primary outcome; patients with superficial femoral artery lesions or PAD; minimum of 50 participants per study. Abstract-only publications, commentaries, editorials, nonoriginal research articles (including reviews) and case reports were excluded.
Two reviewers independently screened titles and abstracts, followed by full-text assessment of eligible studies. Data were extracted using a standardized Excel (Microsoft, WA, USA) sheet. Disagreements regarding study eligibility or data extraction were resolved by a third reviewer. The extracted data included patient characteristics: age, sex, comorbidities, claudication, chronic limb-threatening ischemia (CLTI) and renal function; lesion characteristics: length, calcification, location and CTO; outcomes: primary patency, target lesion revascularization (TLR), all-cause mortality, major amputation, clinical improvement, stent fractures, walking distance and the ankle-brachial index. Outcomes were assessed at 12 and 24 months. The term ‘data points’ was used to indicate the number of study arms.
Outcome definitions
The primary outcomes were primary patency and all TLR events. The secondary outcomes were mortality, major amputations, stent fractures, walking distance and clinical improvement. Primary patency was included as defined in the papers. Restenosis was not analyzed as an independent outcome but instead converted to primary patency rate by inverting the value. This was only done if a study did not report primary patency and if restenosis was defined using duplex ultrasound and angiographic assessments. If no TLR was reported, it was calculated from the inversion of freedom from TLR. If only clinically driven (CD)-TLR was reported, this outcome was used as the primary measure. Major amputations were defined as occurring above the ankle; if the study only reported freedom from major amputation, the inverse was calculated. Walking distance was assessed using the walking impairment questionnaire score. Clinical improvement was defined as improvement in the Rutherford classification from baseline.
Statistical analysis & interpretation of results
Meta-analyses were conducted using R (version 4.4.2; R Core Team, 2024; R Foundation, Vienna, Austria), specifically the ‘metafor’ [15] and ‘meta’ [16] packages. A random-effects model was applied to account for the expected heterogeneity. Pooled proportions were calculated using a random-intercept logistic regression model. The Knapp–Hartung adjustment was applied to determine the 95% CI around the pooled effect.
The outcomes of a meta-analysis of proportion provides no direct comparison between interventions. What the outcome of each analysis shows, is an indication of the average effect and the underlying distribution of that effect for each stent type. As noted by Knol et al. [17], nonoverlapping 95% CIs from independent samples (as provided in this meta-analysis of proportions) could be considered statistically significant as the probability of it occurring at random is 0.0056, a factor of 10 smaller than the commonly used p-value cut-off of 0.05. These findings were validated in a study of clinical chemistry laboratory results, with the real data matching closely to the limits calculated by Knol et al. [18]. As such, we consider meta-analysis of proportion results that do not have overlapping 95% CIs to come from different underlying effect distributions. Superiority or inferiority is not implied, as potential confounders that impact on the underlying distribution cannot be discounted.
Due to the large number of studies and the resulting size of the forest plots, the pooled proportions are presented in condensed forest plots in the main body of the manuscript. The detailed forest plots are in the Supplementary Material.
Risk of bias & additional analyses
Risk of bias was assessed using the Downs and Black Quality Appraisal tool [19]. This appraisal tool is suitable for all included study types. Scores were rated as ‘excellent’ (25–27), ‘good’ (20–24), ‘fair’ (15–19) or ‘poor’ (≤14).
Subgroup analyses were performed based on the mean lesion length reported in the study (short <150 mm vs long ≥150 mm). Post hoc sensitivity analyses were done based on the use of core laboratory adjudication by excluding studies that did not use this, and based on the risk of bias scores by excluding all studies rated ‘poor’ in Downs and Black Quality Appraisal [19].
Results
Study selection & characteristics
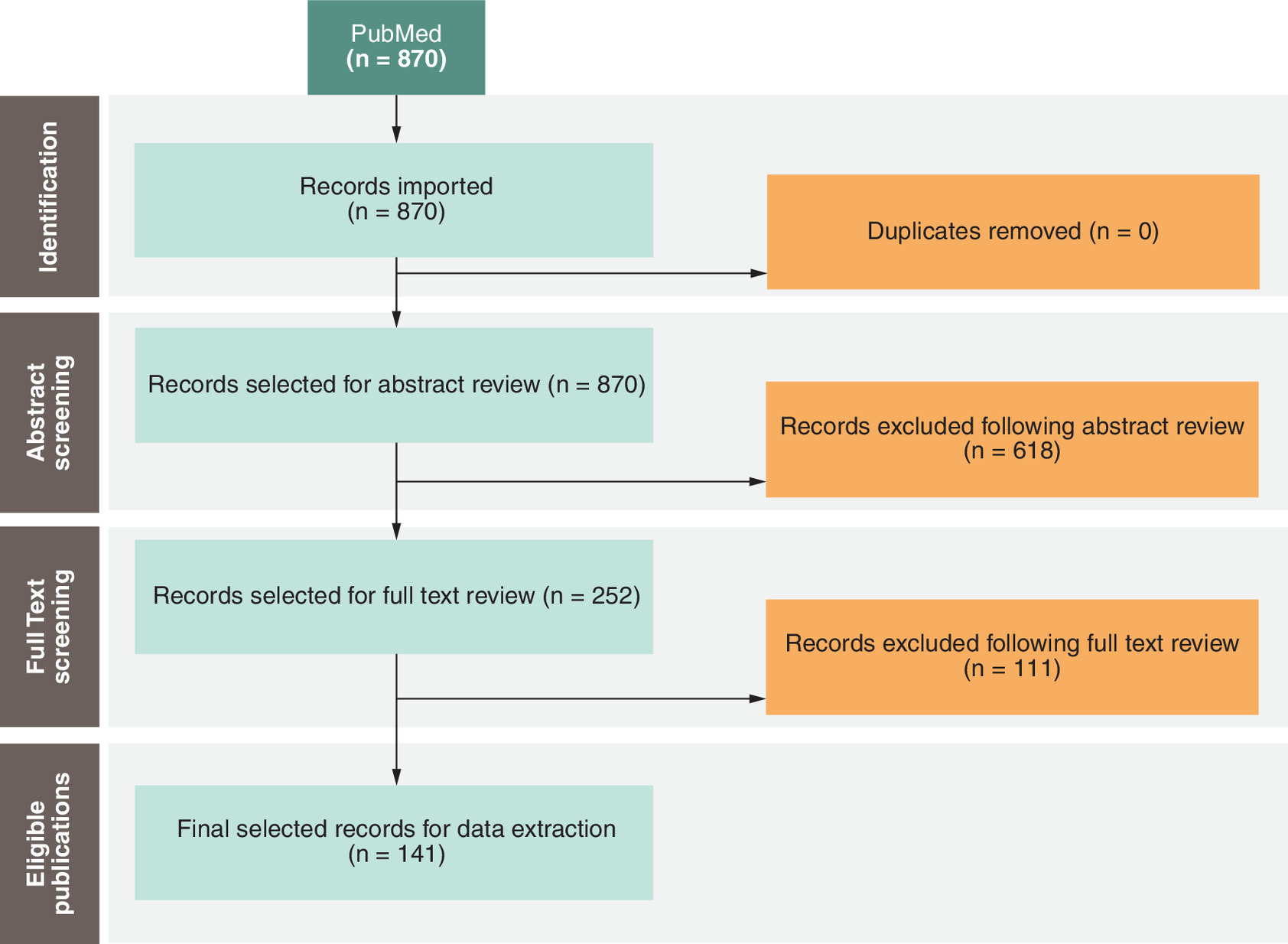
The study selection process is summarized in the PRISMA diagram (Figure 1). The initial search retrieved 870 unique articles, of which 252 were selected for full-text review. A total of 111 studies did not meet the inclusion criteria during full-text screening; consequently, 141 studies comprising 35,897 patients were selected for data extraction.
The studies were prospective (25/141), nonrandomized prospective (47/141) and retrospective (69/141). Their patient and lesion characteristics are summarized in Table 1. The mean patient age was 70.9 (range: 63.3–80.0) years; 69.6% (range: 44.1–100.0%) of the patients were male. The most frequently reported comorbidities were hypertension (80.8% [range: 22.9–99.0%]) and diabetes mellitus (49.8% [range: 19.5–100.0%]). Although reduced kidney function and cardiovascular disease were also prevalent, they had broad definitions and were heterogeneously reported. The reported rate of CLTI was 35.2% (range: 0–100%). The overall mean lesion length was 153.1 mm (range: 37.0–330.0) (Eluvia: 159.4 mm [range: 70.8–230.0]; Zilver PTX: 159.6 mm [range: 64.2–330.0]; Viabahn: 229.7 mm [range: 173.0–290.0]; BMS: 140.5 mm [range: 37.0–330.0]) (Supplementary Table 2). The mean CTO rate was 55.7% (range: 16.4–100.0%).
| Article | Stent type | Population | Lesion characteristics | Patient characteristics | Ref. | |||
|---|---|---|---|---|---|---|---|---|
| Patients per intervention group (n) | Mean lesion length (mm) | CTO (%) | Mean age (years) | Male sex (%) | CLTI (%) | |||
| Abi-Khalil et al. 2022 | BMS | 35 | 65.5 | NR | 70.9 | 77.1 | NR | [20] |
| Abi-Khalil et al. 2022 | Eluvia | 27 | 72.6 | NR | 67.7 | 81.5 | NR | [20] |
| AbuRahma et al. 2022 | Zilver PTX | 94 | 208 | 68 | 69.3 | 57 | 68 | [21] |
| Armstrong et al. 2014 | BMS | 64 | 93 | 31 | 67 | 50 | NR | [22] |
| Armstrong et al. 2014 | BMS | 84 | 257 | 63 | 70 | 56 | NR | [22] |
| Armstrong et al. 2020 | BMS | 118 | 144.5 | 59.3 | 68.7 | 77.1 | 23.7 | [23] |
| Astarcıoglu et al. 2017 | BMS | 53 | 330 | 100 | 69 | 79.2 | 0 | [24] |
| Bausback et al. 2019† | Zilver PTX | 75 | 155.5 | 52 | 69.5 | 76 | 16 | [25] |
| Bertges et al. 2021 | BMS | 2113 | 230 | 56 | 71 | 58 | 69 | [26] |
| Bianchini Massoni et al. 2023 | Zilver PTX | 203 | 107 | 75.4 | 73.5 | 66.5 | 75.9 | [27] |
| Bisdas et al. 2018 | Eluvia | 62 | 200 | 79 | 71 | 63 | 58 | [28] |
| Bosiers et al. 2009 | BMS | 151 | 96.4 | 40 | 67.8 | 73.5 | NR | [29] |
| Bosiers et al. 2011 | BMS | 100 | 242 | NR | 70 | 66 | 29 | [30] |
| Bosiers et al. 2015† | Viabahn | 39 | 173 | 23.1 | 67.7 | 74.4 | NR | [31] |
| Bosiers et al. 2023† | Zilver PTX | 113 | 241.7 | 92 | 69.6 | 69 | 29.2 | [32] |
| Bunte et al. 2018 | BMS | 250 | 77.3 | 23.6 | 67.7 | 61.6 | NR | [33] |
| Chan et al. 2015 | BMS | 153 | 105.6 | 34 | 76.7 | 62.7 | NR | [34] |
| Cheban et al. 2023† | Zilver PTX | 30 | 220 | 100 | 63.3 | 83.3 | NR | [35] |
| Dake et al. 2013 | Zilver PTX | 787 | 99.5 | 38.3 | 67.1 | 73.4 | 11 | [36] |
| Dake et al. 2016† | Zilver PTX | 236 | 66.4 | 32.8 | 67.9 | 65.7 | 8.9 | [37] |
| Davaine et al. 2012 | BMS | 58 | 220 | NR | 71.4 | 72.4 | 59.7 | [38] |
| Davaine et al. 2013 | BMS | 58 | 210 | NR | 70.5 | 73.2 | 62 | [39] |
| Dearing et al. 2009 | BMS | 219 | 129 | 43 | 76.2 | 44.1 | NR | [40] |
| Dick et al. 2009† | BMS | 34 | 82 | 38 | 69 | 74 | NR | [41] |
| Elmahdy et al. 2017 | BMS | 213 | 179 | 100 | 70.9 | 66.2 | 33.8 | [42] |
| Falkowski et al. 2020† | Zilver PTX | 126 | 93.8 | NR | 66.6 | 64 | NR | [43] |
| Falkowski et al. 2020† | BMS | 130 | 127.6 | NR | 64.9 | 63 | NR | [43] |
| Fujihara et al. 2016 | Zilver PTX | 60 | 188.1 | 48.3 | 72.5 | 65 | 31.6 | [44] |
| Fujihara et al. 2023 | BMS | 299 | 97.1 | 33.4 | 75 | 72.9 | 34.3 | [45] |
| Gabrielli et al. 2015 | BMS | 30 | 80 | 100 | NR | 70 | 20 | [46] |
| Gabrielli et al. 2015 | BMS | 41 | 80 | 100 | NR | 61 | 17 | [46] |
| Garcia et al. 2015 | BMS | 264 | 78.1 | 25 | 68.7 | 63.6 | NR | [47] |
| Geraghty et al. 2013† | Viabahn | 72 | 190 | 61.1 | 69 | 62.5 | NR | [48] |
| Golzar et al. 2020 | Eluvia | 50 | 162.8 | 32 | 68.2 | 64 | NR | [49] |
| Gostev et al. 2022 | BMS | 143 | 250 | NR | 63.5 | 81.1 | NR | [50] |
| Gostev et al. 2023 | BMS | 52 | 198 | 100 | 67 | 74.5 | 16.3 | [51] |
| Gouëffic et al. 2020† | Zilver PTX | 86 | 69 | 38 | 71 | 72 | NR | [13] |
| Gouëffic et al. 2020† | BMS | 85 | 76 | 35 | 68 | 73 | NR | [13] |
| Gouëffic et al. 2022† | BMS | 267 | 72.2 | 39.9 | 68.9 | 67.4 | NR | [12] |
| Gouëffic et al. 2022† | Eluvia | 508 | 75.6 | 42.3 | 68.9 | 71.5 | NR | [12] |
| Gray et al. 2018† | Zilver PTX | 156 | 81.8 | 30 | 67.8 | 67 | NR | [11] |
| Gray et al. 2018† | Eluvia | 309 | 86.5 | 31 | 68.5 | 66 | NR | [11] |
| Gray et al. 2022 | BMS | 257 | 71 | 28 | 68 | 66.1 | NR | [52] |
| Guo et al. 2015 | BMS | 53 | 314.8 | NR | 74.2 | 67.9 | Nr | [53] |
| Guzzardi et al. 2021 | BMS | 99 | 150.4 | 41.9 | 74.5 | 69.7 | 64.4 | [54] |
| Haine et al. 2019 | Zilver PTX | 77 | 116 | 71.6 | 72.3 | 64.1 | 36.2 | [55] |
| Hendriks et al. 2020 | BMS | 117 | 71.4 | 30.6 | 69.4 | 70.9 | NR | [56] |
| Horie et al. 2024a | BMS | 204 | 155 | 42.2 | 75 | 75 | NR | [57] |
| Horie et al. 2024a | Viabahn | 137 | 265 | 67.9 | 77 | 65.7 | NR | [57] |
| Horie et al. 2024b | BMS | 177 | 37 | 59.7 | 77 | 60.5 | 31.6 | [58] |
| Hu et al. 2011 | BMS | 138 | 203.5 | 100 | 74.35 | 71.01 | NR | [59] |
| Ichihashi et al. 2019 | Zilver PTX | 220 | 164 | 45.2 | 73.1 | 79.5 | 26.5 | [60] |
| Ichihashi et al. 2022 | Eluvia | 211 | 230 | 64 | 75 | 72.5 | NR | [61] |
| Ichihashi et al. 2022 | Viabahn | 293 | 242 | 77.5 | 74 | 78.2 | NR | [61] |
| Iida et al. 2009 | BMS | 126 | 83 | 17 | 72 | 73 | 26 | [62] |
| Iida et al. 2011a | BMS | 861 | 152 | 54 | 72 | 70 | 26 | [63] |
| Iida et al. 2011b | BMS | 585 | 142 | 53 | 72 | 72 | 23 | [64] |
| Iida et al. 2015 | Zilver PTX | 690 | 170 | 45 | 73.6 | 71 | 32 | [65] |
| Iida et al. 2019† | BMS | 52 | 92 | 29 | 74 | 71 | NR | [66] |
| Iida et al. 2024 | Eluvia | 1097 | 186 | 53.2 | 75 | 69.4 | 34.8 | [67] |
| Ito et al. 2021a | BMS | 427 | NR | NR | 70 | 69.8 | 43 | [68] |
| Ito et al. 2021a | BMS | 157 | NR | NR | 76 | 62.4 | 46.8 | [68] |
| Ito et al. 2021b | BMS | 701 | 141 | 58.2 | 74 | 70.2 | 27.2 | [69] |
| Jeon-Slaughter et al. 2018 | BMS | 784 | 156.5 | 63.65 | 64.09 | 82.65 | 22.83 | [70] |
| Jeon-Slaughter et al. 2018 | Zilver PTX | 174 | 162.5 | 63.79 | 64.67 | 80.46 | 22.99 | [70] |
| Kang et al. 2016 | Zilver PTX | 63 | 218.9 | 69.8 | 66.3 | 57.1 | NR | [71] |
| Karashima et al. 2021 | BMS | 453 | 180 | 54 | 74 | 70 | 37 | [72] |
| Karpenko et al. 2022† | BMS | 35 | 229.2 | 65.7 | 65 | 71.43 | NR | [73] |
| Katsuki et al. 2019 | BMS | 1250 | 143 | 40.3 | 73 | 69.8 | NR | [74] |
| Katsuki et al. 2019 | Zilver PTX | 285 | 146 | 40.7 | 73 | 74.7 | NR | [74] |
| Katsuki et al. 2020 | Viabahn | 53 | 217.5 | 83 | 77.7 | 72 | NR | [75] |
| Kawamura et al. 2009 | BMS | 80 | NR | NR | 65 | 55 | NR | [76] |
| Kichikawa et al. 2019 | Zilver PTX | 905 | 146 | 41.5 | 73.5 | 70.3 | 21.4 | [77] |
| Kim et al. 2024 | Eluvia | 104 | 168.3 | 57.7 | 68.2 | 82.7 | 30.1 | [78] |
| Ko et al. 2019† | BMS | 66 | 238 | 87.9 | 70.3 | 81.8 | 30.3 | [79] |
| Ko et al. 2019† | BMS | 59 | 245 | 89.8 | 70 | 89.8 | 18.6 | [79] |
| Kum et al. 2021 | Eluvia | NR‡ | 201 | NR | NR | NR | NR | [80] |
| Labed et al. 2021 | BMS | 64 | 295 | 85.9 | 80 | 62.5 | 76.6 | [81] |
| Laird et al. 2012† | BMS | 134 | 70 | 17 | 68 | 70.9 | NR | [82] |
| Laird et al. 2014 | BMS | 196 | 60.7 | 29.9 | 68.7 | 63.3 | NR | [83] |
| Laird et al. 2018† | BMS | 197 | 107.6 | 42.1 | 66.7 | 71.6 | NR | [84] |
| Laird et al. 2018† | BMS | 70 | 117.9 | 37.1 | 67.9 | 70 | NR | [84] |
| Lammer et al. 2013† | BMS | 69 | 173.2 | 70 | 69.44 | 75 | NR | [85] |
| Lammer et al. 2013† | Viabahn | 72 | 189.8 | 79 | 68.85 | 67 | NR | [85] |
| Lammer et al. 2015† | BMS | 69 | 173.2 | 70 | 69.44 | 75 | NR | [86] |
| Lammer et al. 2015† | Viabahn | 72 | 189.8 | 79 | 68.85 | 67 | NR | [86] |
| Lee et al. 2021 | Zilver PTX | 93 | 194.8 | 77.5 | 70.8 | 77.5 | 50 | [87] |
| Leopardi et al. 2014 | Zilver PTX | 69 | 130.7 | NR | 70.4 | 81.1 | 18.8 | [88] |
| Lichtenberg et al. 2014 | BMS | 118 | 111.5 | 56.7 | 71.9 | 54.2 | NR | [89] |
| Lichtenberg et al. 2019 | BMS | 60 | 81.6 | 16.4 | 70.3 | 63.3 | 15.8 | [90] |
| Liistro et al. 2019† | Zilver PTX | 96 | 140.7 | 64 | 74.2 | 76 | 59.4 | [91] |
| Loureiro et al. 2024 | BMS | 79 | NR | NR | 66.9 | 72.2 | NR | [92] |
| Low et al. 2022 | BMS | 62 | 150 | NR | 76 | 69 | NR | [93] |
| Ma et al. 2022 | BMS | 157 | 187 | 79.4 | 71.9 | 69.4 | 52.86 | [94] |
| Marples et al. 2022 | Viabahn | 36 | 254.7 | 53 | 76 | 55 | NR | [95] |
| Matsumi et al. 2016a | BMS | 68 | 244 | 100 | 72.5 | 70.6 | 20.8 | [96] |
| Matsumi et al. 2016b | BMS | 107 | 114.3 | 31.4 | 70.4 | 73.8 | 33.5 | [97] |
| Matsumi et al. 2016b | BMS | 325 | 117.3 | 42.5 | 74.2 | 74.5 | 7.2 | [97] |
| Matsumura et al. 2013 | BMS | 287 | 89.1 | 48.1 | 67.7 | 66.2 | NR | [98] |
| McQuade et al. 2010† | Viabahn | 40 | NR | NR | 72 | 80 | NR | [99] |
| Meng et al. 2018 | Zilver PTX | 24 | 105.4 | NR | 70.92 | 79.2 | 83.3 | [100] |
| Meng et al. 2018 | BMS | 70 | 107.9 | NR | 70.86 | 74.3 | 97.1 | [100] |
| Miura et al. 2018† | BMS | 85 | 96 | 36.5 | 73.4 | 64.7 | NR | [101] |
| Miura et al. 2018† | Zilver PTX | 85 | 110.5 | 50.6 | 73.1 | 70.6 | NR | [101] |
| Montero-Baker et al. 2016 | BMS | 147 | 184.5 | 53 | 72.2 | 51 | 0.7 | [102] |
| Mori et al. 2017 | BMS | 279 | 156 | 56 | 73.1 | 67 | 33 | [103] |
| Mori et al. 2017 | Zilver PTX | 27 | NR | NR | NR | 72 | 15 | [103] |
| Müller-Hülsbeck et al. 2016 | Eluvia | 57 | 70.8 | 46 | 69.3 | 82 | NR | [104] |
| Müller-Hülsbeck et al. 2017 | Eluvia | 57 | 70.8 | 46 | 69.3 | 82 | NR | [105] |
| Myint et al. 2016 | BMS | 97 | 151.5 | 43 | 75.3 | 70.10309 | 19 | [106] |
| Nakamura et al. 2018 | BMS | 74 | 80.7 | 20.8 | 72.8 | 75.7 | 0 | [107] |
| Nakao et al. 2024 | Eluvia | 173 | 201 | 41 | 76 | 66 | 59 | [108] |
| Nanto et al. 2015 | BMS | 1476 | NR | NR | 73 | 68.09 | 29.67 | [109] |
| Oberto et al. 2017 | Zilver PTX | 67 | 104 | 46.3 | 70.1 | 79 | NR | [110] |
| Okuno et al. 2019 | BMS | 260 | NR | NR | 73.6 | 66.1 | 39.4 | [111] |
| Palena et al. 2024 | BMS | 92 | 261 | 100 | 73.2 | 88 | 100 | [112] |
| Park et al. 2022† | Zilver PTX | 48 | 238.6 | 72.9 | 71.1 | 79.2 | 22.9 | [113] |
| Park et al. 2022† | Zilver PTX | 55 | 245.1 | 85.2 | 70.8 | 85.5 | 31.5 | [113] |
| Phair et al. 2020a | Zilver PTX | 56 | 64.15 | 41.1 | 70.5 | 60.7 | NR | [114] |
| Phair et al. 2020b | Zilver PTX | 97 | 115 | 41.2 | 68.2 | 56.7 | NR | [115] |
| Phillips et al. 2018 | Zilver PTX | 41 | 139 | 34 | 69.7 | 71 | NR | [116] |
| Phillips et al. 2018 | Zilver PTX | 48 | 330 | 83 | 67.9 | 54 | NR | [116] |
| Powell et al. 2017 | BMS | 299 | 93.2 | 44.7 | 67.4 | 74.2 | NR | [117] |
| Rammos et al. 2024 | BMS | 121 | 125.8 | 64 | 72.2 | 61.2 | 100 | [118] |
| Rammos et al. 2024 | BMS | 381 | 126.2 | 54.4 | 69.4 | 66.9 | 0 | [118] |
| Rastan et al. 2013† | BMS | 119 | 41.3 | 32.9 | 72 | 63.9 | NR | [119] |
| Salamaga et al. 2023 | BMS | 77 | 152.8 | 66 | 71 | 75 | 57 | [120] |
| Saratzis et al. 2019 | BMS | 136 | 150 | 78 | 76 | 63 | NR | [121] |
| Saxon et al. 2013 | Viabahn | 113 | 190 | 56 | 67 | 61.1 | NR | [122] |
| Scheinert et al. 2011 | BMS | 107 | 90.2 | 30.8 | 68.9 | 71.9 | 16.8 | [123] |
| Scheinert et al. 2013 | BMS | 101 | 58.4 | 47.5 | 73.1 | 52.5 | NR | [124] |
| Schulte et al. 2012 | BMS | 744 | 63.9 | 37.6 | 68.6 | 66.7 | NR | [125] |
| Shehada et al. 2022 | Eluvia | 75 | 140 | 71 | 72 | 59 | 27 | [126] |
| Shehada et al. 2022 | BMS | 124 | 160 | 84 | 74 | 59 | 16 | [126] |
| Shibata et al. 2023 | Eluvia | 98 | 160 | 56.7 | 76.9 | 68.3 | 28.8 | [127] |
| Shibata et al. 2023 | Zilver PTX | 86 | 185.7 | 53.1 | 75.3 | 71.9 | 32.3 | [127] |
| Soga et al. 2010 | BMS | 511 | 150.5 | 50 | 72 | 71 | 24 | [128] |
| Soga et al. 2011 | BMS | 807 | 145.3 | 54.4 | 72.3 | 68.9 | 25.8 | [129] |
| Stavroulakis et al. 2016 | BMS | 89 | 116 | 55 | 71 | 62 | NR | [130] |
| Stavroulakis et al. 2021 | Eluvia | 130 | 194 | 74 | 71 | 63 | NR | [131] |
| Steiner et al. 2016 | BMS | 470 | 125 | 53 | 70.5 | 67 | 19 | [132] |
| Steiner et al. 2016 | BMS | 432 | 148 | 58 | 67.6 | 70 | 25 | [132] |
| Stern et al. 2021 | Zilver PTX | 64 | 201.5 | NR | 70.46 | 71.9 | 29.7 | [133] |
| Sullivan et al. 2021 | BMS | 271 | 81.2 | 30 | 68.4 | 66.4 | NR | [134] |
| Suzuki et al. 2016 | BMS | 240 | 120 | 37 | 72 | 65 | 35 | [135] |
| Suzuki et al. 2016 | BMS | 1265 | 140 | 55 | 73 | 70 | 32 | [135] |
| Tan et al. 2022a | Zilver PTX | 65 | 171 | 53.8 | 73.8 | 72.3 | NR | [136] |
| Tan et al. 2022b | BMS | 250 | 200 | 58 | 75 | 60 | 45 | [137] |
| Teymen et al. 2018 | BMS | 49 | 147.02 | 49 | 64.35 | 71.4 | NR | [138] |
| Torsello et al. 2024 | Eluvia | 130 | 194 | 74 | 71 | 63 | 31 | [139] |
| Treitl et al. 2017 | BMS | 85 | 41.7 | NR | 70.5 | 58.8 | NR | [140] |
| Treitl et al. 2017 | BMS | 67 | 51.4 | NR | 72.5 | 64.2 | NR | [140] |
| Treitl et al. 2017 | BMS | 70 | 52.8 | NR | 74.7 | 70 | NR | [140] |
| Tsujimura et al. 2021 | Zilver PTX | 271 | 220 | 59 | 74 | 67.2 | NR | [141] |
| Tsujimura et al. 2021 | Viabahn | 174 | 255 | 69 | 75 | 74.1 | NR | [141] |
| Van Meirvenne et al. 2023 | BMS | 128 | 143 | NR | 75.5 | 53 | 45 | [142] |
| Vartanian et al. 2013 | BMS | NR‡ | NR | 30 | 72 | 76 | 52 | [143] |
| Vartanian et al. 2013 | Viabahn | NR‡ | NR | 59 | 68.5 | 75 | 33 | [143] |
| Vent et al. 2017 | BMS | 58 | 220 | NR | 71.4 | 72.4 | 59.7 | [144] |
| Vent et al. 2017 | Zilver PTX | 45 | 252 | NR | 67 | 71.1 | 46.7 | [144] |
| Watanabe et al. 2018 | BMS | 104 | 263 | 100 | 72.8 | 72.4 | 26 | [145] |
| Watanabe et al. 2018 | BMS | 95 | 269 | 100 | 74.4 | 65.8 | 48.6 | [145] |
| Werner et al. 2013 | BMS | 100 | 69.5 | 29 | 67.6 | 76 | NR | [146] |
| Werner et al. 2014 | BMS | 470 | 126.4 | 52.6 | 70.5 | 67.2 | 18.2 | [147] |
| Wittig et al. 2024† | Eluvia | 60 | 191.7 | 78.3 | 66.5 | 81.7 | NR | [148] |
| Yang et al. 2022 | BMS | 246 | 147.7 | 81.2 | 73.2 | 60.2 | 87.3 | [149] |
| Ye et al. 2022 | Zilver PTX | 178 | 79 | 50 | 67.4 | 78.8 | NR | [150] |
| Ye et al. 2023 | Viabahn | 65 | 290 | 71.6 | 73.1 | 77.6 | 61.2 | [151] |
| Yokoi et al. 2016 | Zilver PTX | 907 | 147 | 41.6 | 73.5 | 70.3 | 21.5 | [152] |
| Yoshioka et al. 2023 | Eluvia | 65 | 174.7 | 61.5 | 75.3 | 72.3 | NR | [153] |
| Zamani et al. 2021 | Zilver PTX | 57 | 200 | NR | 65.8 | 93 | 67 | [154] |
| Zamani et al. 2021 | Viabahn | 74 | 260 | NR | 64 | 100 | 31 | [154] |
| Zamani et al. 2021 | BMS | 95 | 280 | NR | 65.4 | 99 | 39 | [154] |
| Zeller et al. 2014 | Zilver PTX | 97 | 195 | 62.9 | 68.2 | 63.9 | NR | [155] |
| Zeller et al. 2016† | BMS | 26 | 63.3 | 46 | 66.8 | 65 | 0 | [156] |
| Zeller et al. 2016† | BMS | 50 | 65.8 | 44 | 68 | 66 | 4 | [156] |
| Zhao et al. 2021 | BMS | 39 | 187.8 | 61.9 | 66.5 | 61.5 | 23.6 | [157] |
†
Prospective randomized studies included in this analysis.
‡
Number of limbs reported instead of the number of patients.
In some cases, more than one arm in a study used the same stent type but different brands. A more detailed table of patient and lesion characteristics is included in the Supplementary Data (Supplementary Table 3).
BMS: Bare metal stent (specifically self-expanding nitinol stent); CLTI: Chronic limb-threatening ischemia; CTO: Chronic total occlusion; NR: Not reported.
Overall, 38 (27.0%) included studies reported using core laboratory adjudication. According to the Downs and Black Quality Appraisal tool [19] (Supplementary Table 4), 94/141 (66.7%) studies had a rating of ‘fair’ or above (‘excellent’: n = 2; ‘good’: n = 18; ‘fair’: n = 74; ‘poor’: n = 47).
Synthesis of results for the primary outcomes
Primary patency was reported in 129/141 (91%) studies. The total patient population across all stent types included 27,496 patients (153 data points) at 12 months and 17,656 patients (96 data points) at 24 months. Eluvia exhibited primary patency rates with the lower bound of its 95% CI exceeding the upper bound of that of the other stent types at both timepoints (Figure 2).
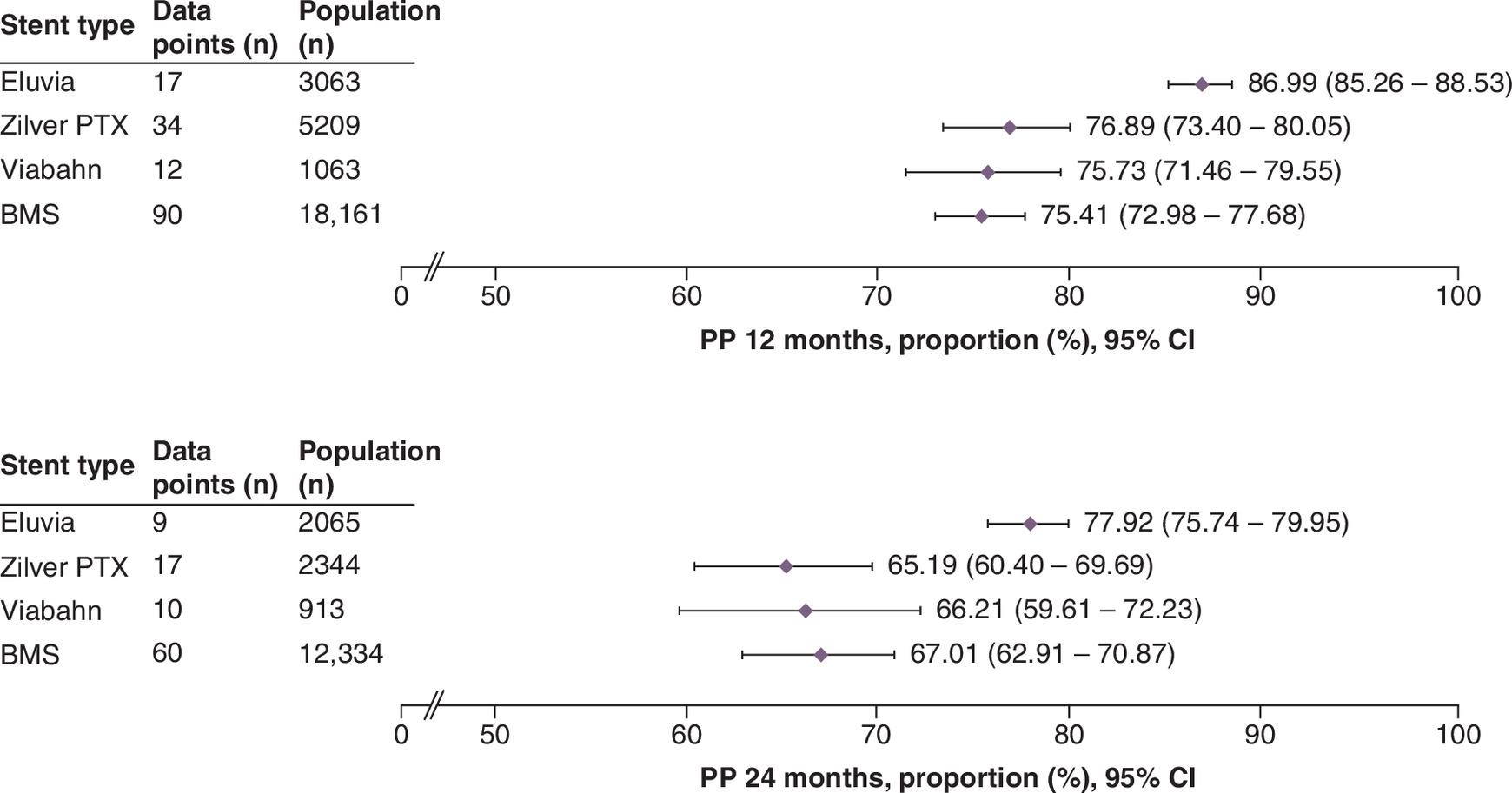
Figure 2. Summary forest plots showing primary patency at 12 and 24 months post stenting.
The pooled estimates of primary patency (and the corresponding 95% CI values) are shown for each stent type at 12 months (top panel) or 24 months (bottom panel). The full forest plot for each stent type at each time point can be found in Supplementary Figures 1–8. These data were extracted from the following references: Eluvia [11,12,20,28,49,61,67,78,80,104,105,108,126,127,131,139,148,153]; Zilver PTX [11,13,21,25,27,35,37,44,60,65,71,77,87,88,91,100,101,103,110,113–116,127,133,141,144,150,152,154,155,158]; Viabahn [48,57,61,75,85,86,95,99,122,141,151,154,158]; BMS [12,13,20,22,24,29,30,33,34,38–42,45–47,50,51,53,54,56–59,62–64,66,69,72,73,76,79,81–86,89,90,92–94,96–98,100–103,106,107,109,111,112,117,119–121,123–126,128–130,132,134,135,137,140,142,144–147,149,154,156,157].
BMS: Bare metal stent; CI: Confidence interval; PP: Primary patency.
In the subgroup analysis, Eluvia achieved consistently high primary patency in both short and long lesions at 12 and 24 months (Figure 3). Zilver PTX performed better in short than in long lesions at both timepoints. Viabahn was not used in short lesions; however, it achieved a primary patency of 75.93 (95% CI: 72.04–79.43) and 66.21 (95% CI: 59.61–72.23) at 24 months in long lesions. The performance of BMSs in both short lesions and long lesions declined at 24 versus 12 months.
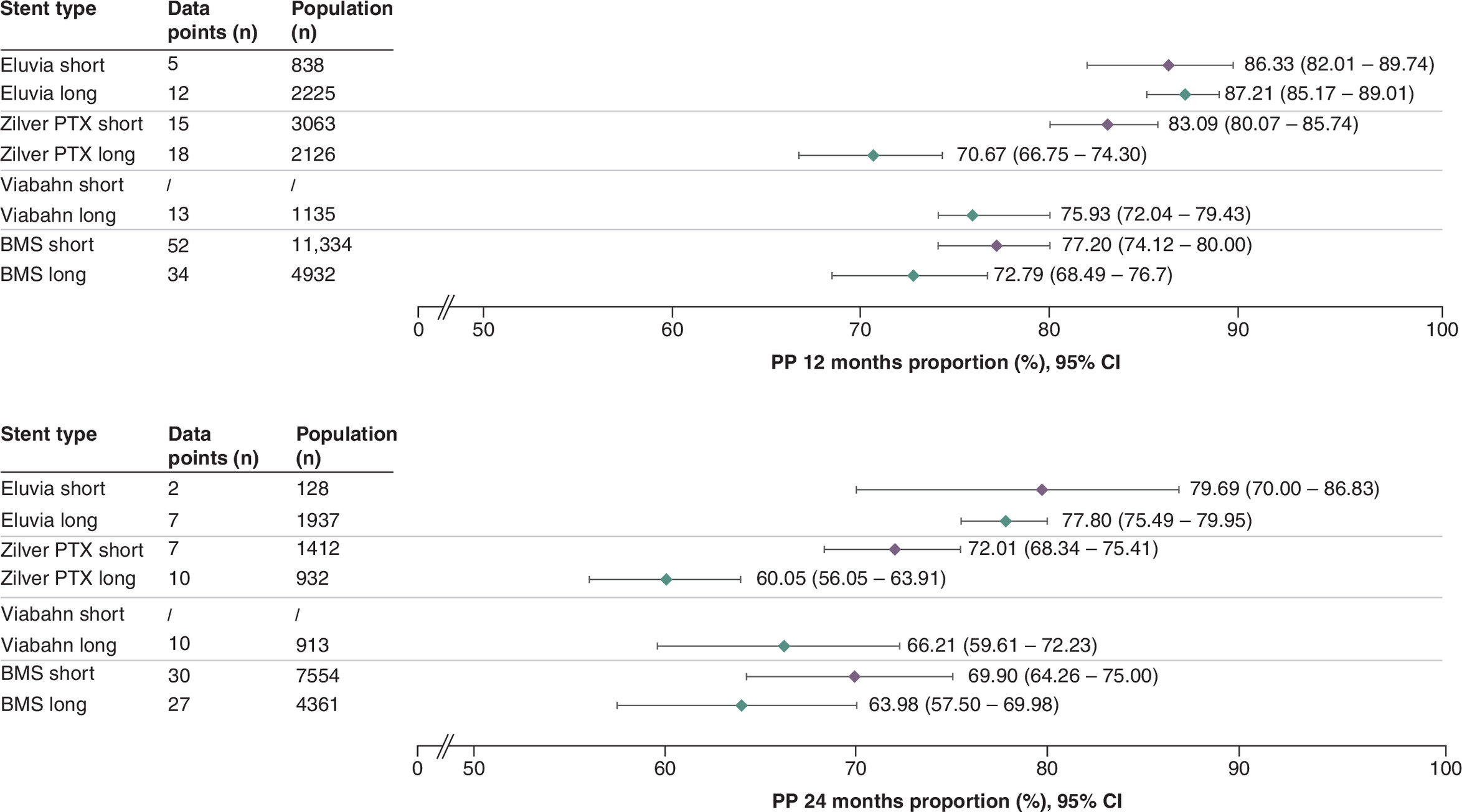
Figure 3. Summary forest plots showing primary patency for short and long lesions at 12 and 24 months post stenting.
The pooled estimates of primary patency (and the corresponding 95% CI values) are shown for each stent type in short (orange) or long (blue) lesions at 12 months (top panel) or 24 months (bottom panel). The full forest plot for each stent type at each time point can be found in Supplementary Figures 9–14.
BMS: Bare metal stent; CI: Confidence interval; PP: Primary patency.
TLR was reported in 85/141 (60%) studies. The total patient population included 18,272 patients (102 data points) at 12 months and 10,720 patients (62 data points) at 24 months. Eluvia exhibited the lowest TLR rates among the stent types at both timepoints, with the upper limit of its 95% CI staying below the lower limit of the 95% CI of the other stents (Figure 4).
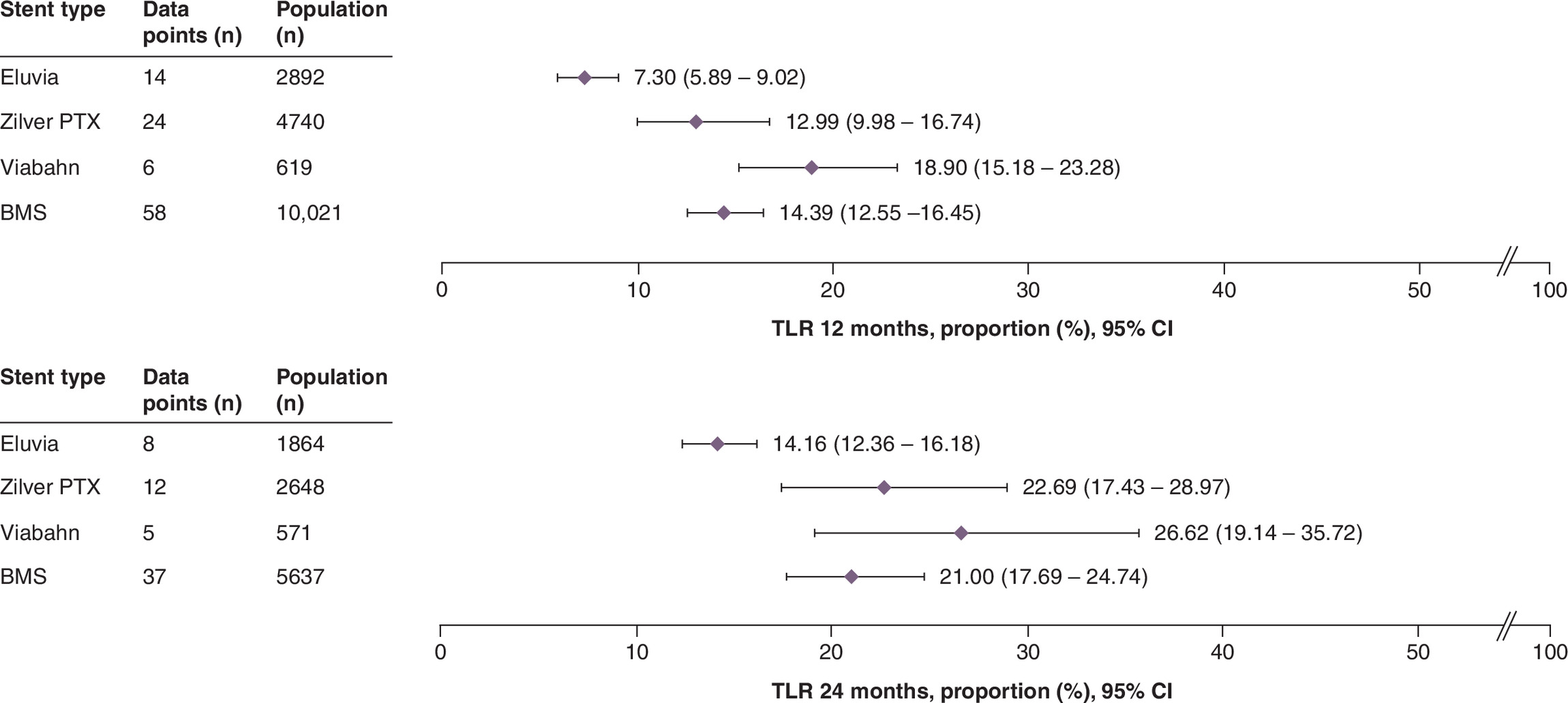
Figure 4. Summary forest plots showing target lesion revascularization at 12 and 24 months post stenting.
The pooled estimates of TLR (and the corresponding 95% CI values) are shown for each stent type at 12 months (top panel) or 24 months (bottom panel). The full forest plot for each stent type at each time point can be found in Supplementary Figures 30–37. These data were extracted from the following references: Eluvia [8,11,28,49,61,67,78,105,126,127,131,139,148,153]; Zilver PTX [11,13,25,27,35–37,44,55,60,70,77,87,91,100,101,113,114,127,144,150,152,154,155,158]; Viabahn [31,57,58,61,85,151,154]; BMS [12,13,23,24,29,30,33,38,45,47,51,52,54,56–58,66,68–70,76,81–86,89,90,94,97,98,100,101,106,107,112,117–119,121,125,126,130,134,140,142,144–147,154,156,157].
BMS: Bare metal stent; CI: Confidence interval; TLR: Target lesion revascularization.
The TLR rate was similar for long and short lesions treated with Eluvia (Figure 5). Meanwhile, the TLR rate for long lesions treated with Zilver PTX was higher than that for short lesions. As no studies reported the use of Viabahn in short lesions, no subgroup analysis was possible. Considerable overlap in 95% CIs was observed when comparing the performance of BMS in long and short lesions.
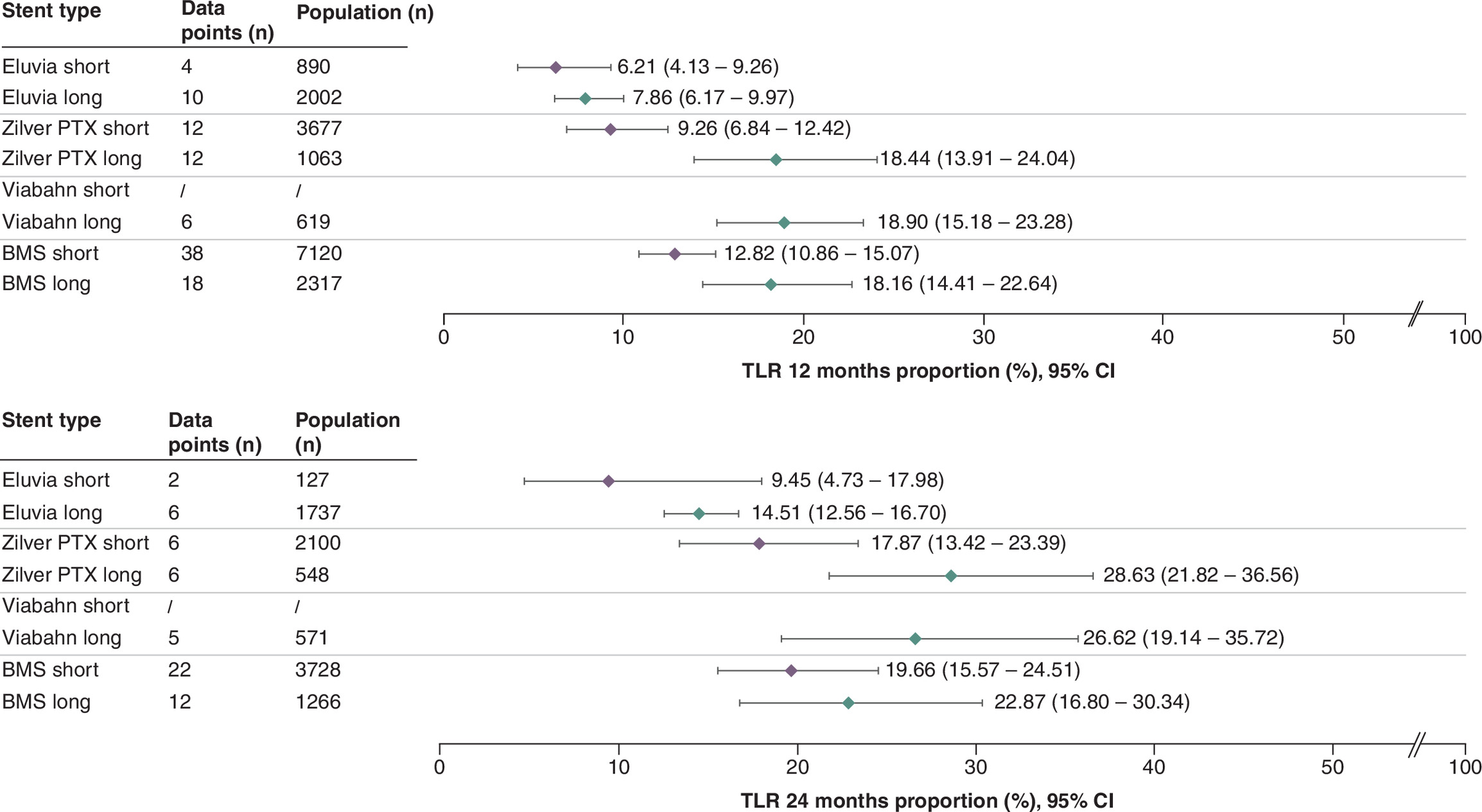
Figure 5. Summary forest plots showing target lesion revascularization for short and long lesions at 12 and 24 months post stenting.
The pooled estimates of TLR (and the corresponding 95% CI values) are shown for each stent type in short (orange) or long (blue) lesions at 12 months (top panel) or 24 months (bottom panel). The full forest plot for each stent type at each time point can be found in Supplementary Figures 38–43.
BMS: Bare metal stent; CI: Confidence interval; TLR: Target lesion revascularization.
The results of the sensitivity analyses, based on the reporting of core laboratory adjudication (primary patency: Supplementary Table 5 & Supplementary Figures 15–21, TLR: Supplementary Table 7 & Supplementary Figures 44–49) and Downs and Black quality assessment (primary patency: Supplementary Table 6 & Supplementary Figures 22–29, TLR: Supplementary Table 8 & Supplementary Figures 50–57), did not substantially alter the results of the main analysis. However, including only the studies that reported using core laboratory adjudication in the sensitivity analysis increased the variability of the estimated effect (i.e., widened the 95% CIs).
Synthesis of results for the secondary outcomes
Mortality was reported in 78/141 studies (55%) for 14,672 patients (81 data points) and 10,817 patients (44 data points) at 12 and 24 months, respectively. The performance of the stents appeared similar with regards to this outcome (Figure 6).
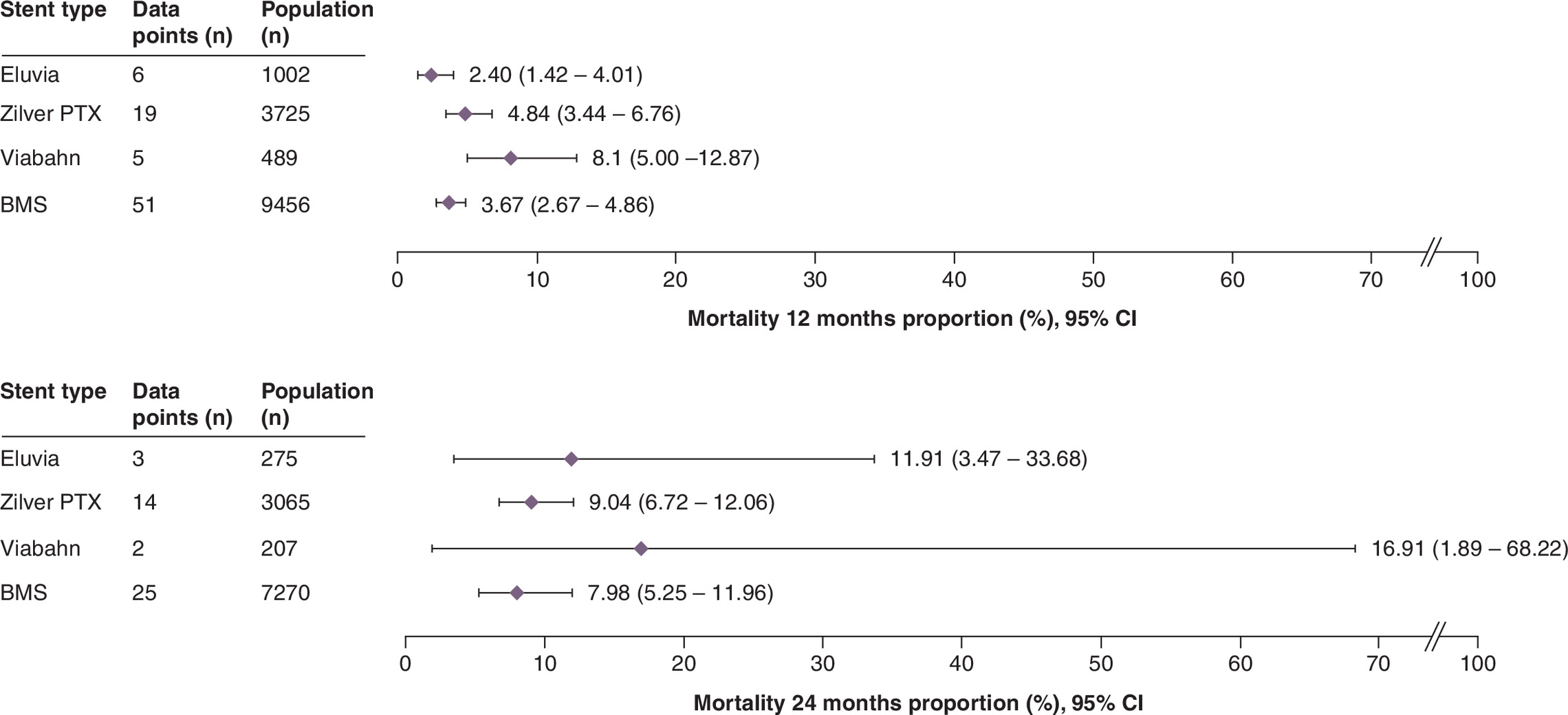
Figure 6. Summary forest plots showing mortality at 12 and 24 months post stenting.
The pooled estimates of mortality (and the corresponding 95% CI values) are shown for each stent type at 12 months (top panel) or 24 months (bottom panel). The full forest plot for each stent type at each time point can be found in Supplementary Figures 58–65. These data were extracted from the following references: Eluvia [11,12,28,49,78,126,131,148]; Zilver PTX [11,13,36,43,55,60,65,70,71,74,77,87,91,100,101,110,116,141,144,150,152,154,155,158]; Viabahn [31,58,122,141,154]; BMS [13,23,24,29,30,33,38,39,41,43,46,51,54,56–58,68,70,74,79,81,83,89,94,98,103,106,118,119,123–126,128,138,140,144,146,147,154,156,157].
BMS: Bare metal stent: CI: Confidence interval.
Fewer mortality data points were available for the subgroup analysis than in the main analysis (Supplementary Figures 66–70). At 12 months, mortality rates were comparable across lesion lengths for all stents. At 24 months, more variation in mortality rate was observed, with long lesions resulting in higher mortality rates than short lesions. The results of the sensitivity analysis, based on the reporting of core laboratory adjudication (Supplementary Table 9 & Supplementary Figures 71–76) and Downs and Black quality assessment, (Supplementary Table 10 & Supplementary Figures 77–84) were comparable to those of the main analysis.
The other secondary outcomes were inconsistently reported and did not generate meaningful results for all stent types. The incidence of major amputations was reported by 52/141 (37%) of studies and was higher at 24 months (range: 1.2–2.3%) than at 12 months (range: 0.5–1.4%) (Supplementary Table 11 & Supplementary Figures 85–92). The number of studies reporting stent fractures was also relatively low (45/141, 32%). This outcome was similar at 12 months (range: 0.2–4.8%) and 24 months (range: 0.0–4.4%) but was highly heterogeneous, likely due to the low number of data points (Supplementary Table 12 & Supplementary Figures 93–98). We also attempted to examine clinical improvement associated with each stent type (range: 79.7–91.0% at 12 months) at both timepoints (Supplementary Table 13 & Supplementary Figures 99–101); however, low study numbers reporting data in our timeframe (26/141, 18%) and the heterogeneity between studies in reporting this outcome limited the utility of the findings. The analysis of walking impairment questionnaire scores (reported by 10/141 [7%] studies) was also not informative due to insufficient data (data not shown).
Discussion
This meta-analysis of proportions included 141 studies evaluating the performance of four stent types in patients with femoropopliteal disease, with a focus on primary patency and TLR at 12- and 24-months post stenting. We found that Eluvia demonstrated consistent performance (i.e., similar primary patency and TLR rates) across lesion lengths and follow-up times, which was not the case for the other stents. As expected, stent performance decreased over time, with lower performance at 24 months than 12 months. Although the reasons for variability in stent performance were not investigated in this study, they may be linked to differences in stent, lesion and/or patient characteristics.
Long or complex lesions in the femoropopliteal segment are especially challenging to treat as they are subjected to continuous mechanical stress [159]. Such lesions are associated with an increased risk of intimal hyperplasia (with subsequent restenosis or reocclusion), stent fracture and ultimately, lower patency and freedom from TLR rates [6]. To date, few studies have demonstrated the successful application of nitinol stents in long, complex femoropopliteal lesions [42,49,160]. Paclitaxel-eluting stents may be especially important in the treatment of longer lesions at a high risk of restenosis [49]. Eluvia is designed to achieve controlled, sustained drug release over time [161], whereas Zilver PTX releases the drug at a faster rate [162]. This may be one explanation for the difference in the performance of these stents in long lesions observed in the present study.
Patient characteristics are an important factor during stent selection. Patients with long and/or complex femoropopliteal lesions often present with more severe disease, characterised by higher rates of CTO, and the presence of CLTI [81,160,163]. In accordance, we found that more patients with long than with short lesions presented with CTO (68.3 vs 44.2%) or CLTI (37.8 vs 34.5%). The overall characteristics of patients included in our study align with the femoropopliteal patient profile reported by patient registries [78,146]. However, the effect of patient characteristics on outcomes fell outside the scope of the present study and was not controlled for in our analysis. Ultimately, patient-level data will be required to address the true impact of patient characteristics on stent selection and performance. At present, our understanding of stent performance in diverse patient populations is also limited by the fact that many of the registry datasets presented at symposia are rarely formally disseminated. Greater access to this information would enable clinicians to make more informed treatment decisions and support evidence-based market access for new medical technologies.
Inconsistent outcome reporting emerged as a notable barrier in this analysis, particularly as it prevented a detailed evaluation of secondary outcomes. We found that primary patency and TLR often lacked clear definitions and required conversion for cross-study comparisons. For instance, TLR was reported as CD-TLR or any TLR and primary patency had to sometimes be derived from restenosis. The consistent reporting of outcomes such as CD-TLR is particularly important for patients with advanced femoropopliteal disease, as it provides a clinically meaningful measure of treatment failure and a reliable indicator of whether reintervention is required. Secondary outcomes, such as stent fractures and clinical improvement, were only reported sporadically. Although many studies presented walking distance scores, the heterogeneity in reporting prevented any meaningful analysis of this outcome. Overall, the current lack of consistent outcome reporting complicates the assessment of a stent’s true clinical benefit. We recommend the adoption of standardized definitions and uniform reporting criteria to enable more accurate medical device comparisons.
Considering that only around a third of the included studies used core laboratory adjudication, the need for the standardization of reporting practices is clear. Adjudication by an independent core laboratory reduces operator bias and ensures that key outcomes are accurately reported. As such, it is a key feature of RCT design. Discrepancies between operator- and core-laboratory-assessed outcomes have been documented [25,164]. Thus, the use of core laboratory adjudication in femoropopliteal stenting may help mitigate operator bias such as the underestimation of residual stenosis. However, because the use of core laboratory adjudication is still not routinely implemented, focusing on studies that included this quality assurance process paradoxically reduced the robustness of the reported data in the sensitivity analysis. Thus, future studies should prioritise core laboratory adjudication and standardized outcome definitions to enhance cross-study comparability. Establishing a Clinical Events Committee to align best practices for long-term outcome reporting represents a valuable next step, while supplementing RCT and real-word data with findings from Delphi consensus studies promises to further enhance collaboration among experts to improve patient outcomes [165].
Similarly, sensitivity analyses based on study quality (assessed using the Downs and Black Quality Appraisal tool) did not alter our overall conclusions. It is possible that studies rated as ‘poor’ may not have reported values that differed significantly from those originating from studies with a better rating. This may, in part, reflect a limitation of the Downs and Black Quality Appraisal tool, whereby single-arm studies are inherently penalised because of their design rather than the methodological rigour with which they were conducted. Given that this analysis was not restricted to comparative data, the inclusion of single-arm studies remains a valuable and appropriate source of information to characterise outcomes associated with specific stent types.
A key strength of this study is that it used a combination of randomized, prospective, nonrandomized and retrospective studies to provide a robust, yet generalisable, measure of stent performance in femoropopliteal lesions. Although the nature of a pooled rates meta-analysis prevents direct comparison, the lack of overlap between the 95% CIs of Eluvia and those of the other stents indicates that this stent may exhibit superior performance across lesion lengths and follow-up timepoints.
This study also had limitations. Key end points such as primary patency and TLR were not consistently defined across the included studies. The derivation of primary patency or TLR via conversion may have introduced some misclassification bias; however, these conversions were only performed when certain stringent conditions were met. Studies that did not report the mean/median lesion length (e.g., they reported the median lesion length or the mean lesion length for the whole population but not a subset treated with the stent of interest) could not be included in the subgroup analyses. Only 12- and 24-month follow-up durations were investigated. Moreover, outcomes were more frequently reported at 12 than at 24 months (152 vs 94 data points for primary patency; 106 vs 65 data points for TLR), reducing the robustness of the long-term data. We cannot guarantee the quality of the included data as only 27.5% of the studies reported using core laboratory adjudication and almost a third did not achieve a Downs and Black rating of ‘fair’ or above. The inclusion of single-arm studies may have reduced the reliability of the pooled estimates by introducing confounding in the patient and study characteristics that could not have been fully adjusted for in the absence of direct comparators. The BMS group comprises stents made by different manufacturers and with designs, which inevitably introduces intragroup heterogeneity. Nonetheless, previous studies have adopted the same grouping of BMSs, and specifically self-expanding bare nitinol stents [12,22,53,59,62–64,68–70,72,76,81,85,86,96,97,100,109,111,129,132,143,145,154,157]. The generalised linear mixed model used enabled the estimation of heterogeneity while considering variability across individual studies. Although this approach is robust, it is characterised by wide 95% CIs, particularly when one of the studies reports zero events for an outcome. An expected limitation of pooled analyses is that they rely on aggregate (i.e., cohort means) rather than primary patient-level data. Finally, we acknowledge that the results of this meta-analysis of proportions are not a substitute for direct, comparative data. As such, future studies should build on this work by comparing the performance of different stent types in RCTs and individual patients. In addition, an analysis of longer-term follow-up is needed to effectively capture data on stent durability and late-stage complications.
Conclusion
The lack of RCTs comparing stent performance in PAD limits the feasibility of conducting a head-to-head meta-analysis directly comparing stent effectiveness within the femoropopliteal segment. The present meta-analysis of proportions provides pooled estimates and corresponding CIs for outcomes related to the performance of four common stent types in both short and long femoropopliteal lesions across two key timepoints. The underlying distribution of effects did on occasion differ between the stent types. We found that Eluvia performed consistently well in both short and long lesions, even at 24-month follow-up. Although they are no substitute for direct, comparative data, our findings offer valuable insights into stent performance, helping clinicians make more informed, case-by-case treatment decisions based on lesion characteristics and long-term outcomes. Additionally, this study demonstrates how the inclusion of long-lesion data in clinical practice can help guide stent selection strategies. Conclusive comparative findings from RCTs and studies involving patient-level data are needed to build on this work.
Summary points
•
This systematic literature review included 141 studies on four stent types in femoropopliteal arterial disease and pooled their results in a meta-analysis of proportions.
•
The four stent types are bare metal stents (BMS), a polymer-based paclitaxel-eluting stent (Eluvia), a covered stent (Viabahn) and a polymer-free paclitaxel-coated stent (Zilver PTX).
•
Primary patency and target lesion revascularization were pooled at 12 and 24 months, and a subgroup analysis was done for short lesions (<150 mm) and long lesions (≥150 mm).
•
We found that only one stent, Eluvia, demonstrated consistent performance (i.e., similar primary patency and target lesion revascularization rates) across lesion lengths and follow-up times.
•
As expected, stent performance in general decreased over time, with lower performance at 24 months than 12 months.
•
Mortality rates for short lesions were stable for all stent types, but more variable for long lesions.
•
Inconsistent definitions were a potential barrier to the pooling of data across clinical studies.
•
Standardization in the reporting of outcomes and the use of core laboratory adjudication would allow for better, cross-study comparison.
Author contributions
Authors Y Gouëffic, S Steiner, R Saunders, J Hafermann and A Bosworth Smith were involved in the study conception and design. Authors R Saunders, A Bosworth Smith, J Hafermann, A Lissina and F Distler were involved in the data acquisition. Authors F Distler was responsible for the data analysis. Authors Y Gouëffic, S Steiner, A Holden, R Saunders, A Bosworth Smith, F Distler and A Lissina were involved in the interpretation of the data analysis results. Authors A Bosworth Smith and A Lissina were responsible for the drafting the manuscript with support from Y Gouëffic, S Steiner and A Holden. Authors Y Gouëffic, S Steiner, A Holden, R Saunders, J Hafermann, F Distler critically reviewed the manuscript. All authors gave final approval for the work to be published and agree to be accountable for the work contained within.
Financial disclosure
Boston Scientific (MA, USA) funded this work.
Competing interests disclosure
Y Gouëffic has received research funding from Predisurge, Biotronik, WL Gore, GE Healthcare and Honoraria from Abbott, BD, Bentely, Biotronik, Boston Scientific, Cook, Eclevar Medtech, GE Healthcare, Ivascular, Medtronic, Penumbra, Sensome, Shockwave medical, WL Gore (consulting, medical advisory board, educational course, speaking). F Distler, J Hafermann, A Lissina and A Bosworth Smith are employees and R Saunders is the founder and CEO of Coreva Scientific GmbH & Co. KG, which received consultancy fees from Boston Scientific. A Holden has been a scientific advisory board member for Boston Scientific, Medtronic, WL Gore, and Phillips. S Steiner has consulted for iThera Medical, Biotronik, Boston Scientific, Cook Medical, Novartis, Angiodynamics, Medupdate. Boston Scientific funded this study and was involved in the review of the work. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Open access
This work is licensed under the Creative Commons Attribution 4.0 License. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 4.50 MB
References
Papers of special note have been highlighted as: • of interest
1.
Aronow WS. Peripheral arterial disease of the lower extremities. Arch. Med. Sci. 8(2), 375–388 (2012).
2.
Jones WS, Patel MR, Dai D et al. High mortality risks after major lower extremity amputation in Medicare patients with peripheral artery disease. Am. Heart J. 165(5), 809–815; 815.e1 (2013).
3.
Gerhard-Herman MD, Gornik HL, Barrett C et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 135(12), e726–e779 (2017).
4.
Johnson AP, Swaminathan RV, Minc SD, Gutierrez JA. Femoropopliteal interventions for peripheral artery disease: a review of current evidence and future directions. Int. Cardiol. Clin. 14(2), 243–256 (2025).
5.
Debing E, Aerden D, Vanhulle A, Gallala S, von Kemp K. Paclitaxel-coated versus plain old balloon angioplasty for the treatment of infrainguinal arterial disease in diabetic patients: the Belgian diabetic IN.PACT Trial. J. Cardiovasc. Surg. 58(4), 528–534 (2017).
6.
Mosarla RC, Armstrong E, Bitton-Faiwiszewski Y, Schneider PA, Secemsky EA. State-of-the-art endovascular therapies for the femoropopliteal segment: are we there yet? J. Soc. Cardiovasc. Angiogr. Interv. 1(5), 100439 (2022).
7.
Tepe G, Brodmann M, Micari A et al. 5-year outcomes of drug-coated balloons for peripheral artery in-stent restenosis, long lesions, and CTOs. JACC Cardiovasc. Interv. 16(9), 1065–1078 (2023).
8.
Gouëffic Y, Brodmann M, Deloose K, Dubosq-Lebaz M, Nordanstig J. Drug-eluting devices for lower limb peripheral arterial disease. EuroIntervention 20(18), e1136–e1153 (2024).
9.
Katsanos K, Spiliopoulos S, Karunanithy N, Krokidis M, Sabharwal T, Taylor P. Bayesian network meta-analysis of nitinol stents, covered stents, drug-eluting stents, and drug-coated balloons in the femoropopliteal artery. J. Vasc. Surg. 59(4), 1123–1133.e8 (2014).
10.
Zhou Y, Shu C, Zhang Z, Wang T, He H, Li Q. Optimal endovascular strategy for femoropopliteal claudication and infrapopliteal CLTI: a network meta-analysis stratified by lesion length. Cardiovasc. Interv. Ther. 41(1), 123–140 (2026).
11.
Gray WA, Keirse K, Soga Y et al. A polymer-coated, paclitaxel-eluting stent (Eluvia) versus a polymer-free, paclitaxel-coated stent (Zilver PTX) for endovascular femoropopliteal intervention (IMPERIAL): a randomised, non-inferiority trial. Lancet 392(10157), 1541–1551 (2018).
• This is a randomized, single-blinded study that compares the efficacy and safety of Zilver PTX and Eluvia. It is a multicentre study, that includes 465 patients. The study demonstrates noninferiority at 12 months.
12.
Gouëffic Y, Torsello G, Zeller T et al. Efficacy of a drug-eluting stent versus bare metal stents for symptomatic femoropopliteal peripheral artery disease: primary results of the EMINENT randomized trial. Circulation 146(21), 1564–1576 (2022).
• This is a multicentre randomized controlled trial, that compares drug-eluting stents to bare metal stents. It includes 775 patients overall and reports primary patency, target lesion revascularization, primary sustained clinical improvement and health-related quality of life measures.
13.
Gouëffic Y, Sauguet A, Desgranges P et al. A polymer-free paclitaxel-eluting stent versus a bare-metal stent for de novo femoropopliteal lesions: the BATTLE trial. JACC Cardiovasc. Interv. 13(4), 447–457 (2020).
14.
Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71 (2021).
15.
Viechtbauer W. Conducting meta-analyses in R with the metafor package. J. Stat. Soft. 36(3), 1–48. (2010).
16.
Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid. Based Ment. Health 22(4), 153–160 (2019).
17.
Knol MJ, Pestman WR, Grobbee DE. The (mis)use of overlap of confidence intervals to assess effect modification. Eur. J. Epidemiol. 26(4), 253–254 (2011).
18.
Cho J, Seo DM, Uh Y. Clinical application of overlapping confidence intervals for monitoring changes in serial clinical chemistry test results. Ann. Lab. Med. 40(3), 201–208 (2020).
19.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Commun. Health 52(6), 377–384 (1998).
20.
Abi-Khalil J, Astarci P, Elens M. Comparison of interwoven nitinol and drug-eluting stents for endovascular treatment of femoropopliteal artery disease. Surg. Tech. Int. 40, sti40/1532 (2022).
21.
AbuRahma AF, Beasley M, AbuRahma ZT et al. Clinical outcome of drug-eluted stenting (Zilver PTX) in patients with femoropopliteal occlusive disease a single center experience. J. Endovasc. Ther. 29(3), 350–360 (2022).
22.
Armstrong EJ, Saeed H, Alvandi B et al. Nitinol self-expanding stents vs. balloon angioplasty for very long femoropopliteal lesions. J. Endovasc. Ther. 21(1), 34–43 (2014).
23.
Armstrong EJ, Jeon-Slaughter H, Kahlon RS, Niazi KA, Shammas NW, Banerjee S. Comparative outcomes of supera interwoven nitinol vs bare nitinol stents for the treatment of femoropopliteal disease: insights from the XLPAD Registry. J. Endovasc. Ther. 27(1), 60–65 (2020).
24.
Astarcıoglu MA, Kılıt C, Sen T et al. One-year results of primary stenting for TASC II D lesions of the superficial femoral and popliteal arteries. Acta Cardiol. 72(1), 36–40 (2017).
25.
Bausback Y, Wittig T, Schmidt A et al. Drug-eluting stent versus drug-coated balloon revascularization in patients with femoropopliteal arterial disease. J. Am. Coll. Cardiol. 73(6), 667–679 (2019).
26.
Bertges DJ, Eldrup-Jorgensen J, Robbins S et al. Vascular quality initiative surveillance of femoropopliteal artery paclitaxel devices. JACC Cardiovasc. Interv. 14(23), 2598–2609 (2021).
27.
Bianchini Massoni C, Strozzi F, Epifani E et al. Real-world outcomes of Cook Zilver PTX in femoro-popliteal district from multicenter experience. Int. Angiol. 42(1), 9–18 (2023).
28.
Bisdas T, Beropoulis E, Argyriou A, Torsello G, Stavroulakis K. 1-year all-comers analysis of the Eluvia drug-eluting stent for long femoropopliteal lesions after suboptimal angioplasty. JACC Cardiovasc. Interv. 11(10), 957–966 (2018).
29.
Bosiers M, Torsello G, Gissler H-M et al. Nitinol stent implantation in long superficial femoral artery lesions: 12-month results of the DURABILITY I study. J. Endovasc. Ther. 16(3), 261–269 (2009).
30.
Bosiers M, Deloose K, Callaert J et al. Results of the Protégé EverFlex 200-mm-long nitinol stent (ev3) in TASC C and D femoropopliteal lesions. J. Vasc. Surg. 54(4), 1042–1050 (2011).
31.
Bosiers M, Deloose K, Callaert J et al. Superiority of stent-grafts for in-stent restenosis in the superficial femoral artery: twelve-month results from a multicenter randomized trial. J. Endovasc. Ther. 22(1), 1–10 (2015).
32.
Bosiers M, Donato G, Torsello G et al. ZILVERPASS Study: ZILVER PTX stent vs. bypass surgery in femoropopliteal lesions, 3 year results and economic analysis. J. Cardiovasc. Surg. 64(4), 413–421 (2023).
33.
Bunte MC, Cohen DJ, Jaff MR et al. Long-term clinical and quality of life outcomes after stenting of femoropopliteal artery stenosis: 3-year results from the STROLL study. Catheter Cardiovasc. Interv. 92(1), 106–114 (2018).
34.
Chan YC, Cheng SW, Cheung GC. Predictors of restenosis in the use of helical interwoven nitinol stents to treat femoropopliteal occlusive disease. J. Vasc. Surg. 62(5), 1201–1209 (2015).
35.
Cheban AV, Osipova OS, Ignatenko PV et al. One-year results of long femoropopliteal lesions stenting with fasciotomy lamina vastoadductoria. Ann. Vasc. Surg. 88, 100–107 (2023).
36.
Dake MD, Ansel GM, Jaff MR et al. Sustained safety and effectiveness of paclitaxel-eluting stents for femoropopliteal lesions: 2-year follow-up from the Zilver PTX randomized and single-arm clinical studies. J. Am. Coll. Cardiol. 61(24), 2417–2427 (2013).
37.
Dake MD, Ansel GM, Jaff MR et al. Durable clinical effectiveness with paclitaxel-eluting stents in the femoropopliteal artery: 5-year results of the Zilver PTX randomized trial. Circulation 133(15), 1472–1483; discussion 1483 (2016).
38.
Davaine J-M, Azéma L, Guyomarch B et al. One-year clinical outcome after primary stenting for Trans-Atlantic Inter-Society Consensus (TASC) C and D femoropopliteal lesions (the STELLA “STEnting Long de L'Artère fémorale superficielle” cohort). Eur. J. Vasc. Endovasc. Surg. 44(4), 432–441 (2012).
39.
Davaine JM, Quérat J, Guyomarch B et al. Incidence and the clinical impact of stent fractures after primary stenting for TASC C and D femoropopliteal lesions at 1 year. Eur. J. Vasc. Endovasc. Surg. 46(2), 201–212 (2013).
40.
Dearing DD, Patel KR, Compoginis JM, Kamel MA, Weaver FA, Katz SG. Primary stenting of the superficial femoral and popliteal artery. J. Vasc. Surg. 50(3), 542–547 (2009).
41.
Dick P, Wallner H, Sabeti S et al. Balloon angioplasty versus stenting with nitinol stents in intermediate length superficial femoral artery lesions. Catheter Cardiovasc. Interv. 74(7), 1090–1095 (2009).
42.
Elmahdy MF, Buonamici P, Trapani M et al. Long-term primary patency rate after nitinol self-expandable stents implantation in long, totally occluded femoropopliteal (TASC II C & D) lesions. Heart Lung Circ. 26(6), 604–611 (2017).
43.
Falkowski A, Bogacki H, Szemitko M. Assessment of mortality and factors affecting outcome of use of paclitaxel-coated stents and bare metal stents in femoropopliteal PAD. JCM 9(7), 2221 (2020).
44.
Fujihara M, Utsunomiya M, Higashimori A, Yokoi Y, Nakamura M. Outcomes of Zilver PTX stent implantation for the treatment of complex femoropopliteal artery disease. Heart Vessels 31(2), 152–157 (2016).
45.
Fujihara M, Takahara M, Iida O et al. Endovascular therapy with interwoven nitinol stent placement after predilation for heavily calcified femoropopliteal artery disease: results of the BURDOCK study. J. Vasc. Interv. Radiol. 34(11), 1929–1937 (2023).
46.
Gabrielli R, Rosati MS, Chiappa R et al. First clinical experience with the Innova versus the Protege EverFlex self-expanding bare metal stents in superficial femoral artery occlusions. Thorac. Cardiovasc. Surg. 63(2), 158–163 (2015).
47.
Garcia L, Jaff MR, Metzger C et al. Wire-interwoven nitinol stent outcome in the superficial femoral and proximal popliteal arteries: twelve-month results of the SUPERB trial. Circ. Cardiovasc. Interv. 8(5), e000937 (2015).
48.
Geraghty PJ, Mewissen MW, Jaff MR, Ansel GM. Three-year results of the VIBRANT trial of VIABAHN endoprosthesis versus bare nitinol stent implantation for complex superficial femoral artery occlusive disease. J. Vasc. Surg. 58(2), 386–95.e4 (2013).
49.
Golzar J, Soga Y, Babaev A et al. Effectiveness and safety of a paclitaxel-eluting stent for superficial femoral artery lesions up to 190 mm: one-year outcomes of the single-arm IMPERIAL long lesion substudy of the Eluvia drug-eluting stent. J. Endovasc. Ther. 27(2), 296–303 (2020).
50.
Gostev AA, Osipova OS, Saaya SB et al. Bypass versus interwoven nitinol stents for long femoro-popliteal occlusions: a propensity matched analysis. Cardiovasc. Interv. Radiol. 45(7), 929–938 (2022).
51.
Gostev AA, Osipova OO, Cheban AV et al. Treatment of long femoropopliteal occlusive lesions with self-expanding interwoven nitinol stent: 24 month outcomes of the STELLA-SUPERA-SIBERIA register trial. J. Endovasc. Ther. 32(1), 192–198 (2025).
52.
Gray WA, Cardenas J, Teigen CL. Evaluation of safety and efficacy of the S.M.A.R.T.® Flex Vascular Stent System (OPEN study). Catheter Cardiovasc. Interv. 100(6), 1078–1087 (2022).
53.
Guo X, Xue G, Huang X et al. Outcomes of endovascular treatment for patients with TASC II D femoropopliteal occlusive disease: a single center study. BMC Cardiovasc. Disord. 15, 44 (2015).
54.
Guzzardi G, Spinazzola A, Cangiano G et al. Endovascular treatment of femoro-popliteal disease with the Supera stent: results of a multicenter study. J. Public Health Res. 11(1), 2360 (2021).
55.
Haine A, Schmid MJ, Schindewolf M et al. Comparison between interwoven nitinol and drug eluting stents for endovascular treatment of femoropopliteal artery disease. Eur. J. Vasc. Endovasc. Surg. 58(6), 865–873 (2019).
56.
Hendriks JM, Dubois M, Lauwers P et al. Endovascular treatment of atherosclerotic lesions in the superficial femoral artery and proximal popliteal artery using the sinus-SuperFlex-635 stent: twelve-month results from the HERO Registry. J. Cardiovasc. Surg. 61(1), 84–92 (2020).
57.
Horie K, Takahara M, Nakama T et al. Retrospective multicenter comparison between Viabahn covered stent-grafts and Supera Interwoven Nitinol Stents for endovascular treatment in severely calcified femoropopliteal artery disease: the ARMADILLO study (Adjusted Retrospective coMparison of scAffolDs In caLcified LesiOns). J. Endovasc. Ther. 31(3), 400–409 (2024).
58.
Horie K, Takahara M, Nakama T et al. Multicenter registry of common femoral artery disease treated with endovascular revascularization using interwoven nitinol stents: an observational retrospective study. J. Endovasc. Ther. 32(6), 2039–2049 (2025).
59.
Hu H, Zhang H, He Y et al. Endovascular nitinol stenting for long occlusive disease of the superficial femoral artery in critical limb ischemia: a single-center, mid-term result. Ann. Vasc. Surg. 25(2), 210–216 (2011).
60.
Ichihashi S, Shibata T, Fujimura N et al. Vessel calcification as a risk factor for in-stent restenosis in complex femoropopliteal lesions after Zilver PTX paclitaxel-coated stent placement. J. Endovasc. Ther. 26(5), 613–620 (2019).
61.
Ichihashi S, Takahara M, Yamaoka T et al. Drug eluting versus covered stent for femoropopliteal artery lesions: results of the ULTIMATE study. Eur. J. Vasc. Endovasc. Surg. 64(4), 359–366 (2022).
• This is a multicentre retrospective study that compares a drug eluting stents and a covered stent. This is an important direct comparison, and it indicated a higher patency for drug-eluting stents.
62.
Iida O, Nanto S, Uematsu M et al. Long-term results of endovascular therapy with nitinol stent implantation for TASC II A/B femoro-popliteal artery lesions: 4 years' experience. Circ. J. 73(11), 2143–2147 (2009).
63.
Iida O, Soga Y, Hirano K et al. Long-term outcomes and risk stratification of patency following nitinol stenting in the femoropopliteal segment: retrospective multicenter analysis. J. Endovasc. Ther. 18(6), 753–761 (2011).
64.
Iida O, Uematsu M, Soga Y et al. Timing of the restenosis following nitinol stenting in the superficial femoral artery and the factors associated with early and late restenoses. Catheter. Cardiovasc. Interv. 78(4), 611–617 (2011).
65.
Iida O, Takahara M, Soga Y et al. 1-year results of the ZEPHYR Registry (Zilver PTX for the Femoral Artery and Proximal Popliteal Artery): predictors of restenosis. JACC Cardiovasc. Interv. 8(8), 1105–1112 (2015).
66.
Iida O, Urasawa K, Komura Y et al. Self-expanding nitinol stent vs percutaneous transluminal angioplasty in the treatment of femoropopliteal lesions: 3-year data from the SM-01 trial. J. Endovasc. Ther. 26(2), 158–167 (2019).
67.
Iida O, Takahara M, Soga Y et al. Three-year clinical course after fluoropolymer-based drug-eluting stent implantation for femoropopliteal lesions. Vasc. Med. 29(2), 182–188 (2024).
• This is a multicentre, prospective, observational study with a large population. It includes 1204 limbs that had implantation of a drug-eluting stent. This study also includes 3-year follow-up data.
68.
Ito R, Ishii H, Oshima S et al. Long-term clinical outcomes after self-expandable bare nitinol stent implantation for femoropopliteal occlusive disease in hemodialysis patients. Catheter. Cardiovasc. Interv. 97(2), 318–324 (2021).
69.
Ito N, Takahara M, Soga Y et al. Lumen loss at 1 year after bare nitinol stent implantation in the superficial femoral artery. J. Endovasc. Ther. 28(1), 132–138 (2021).
70.
Jeon-Slaughter H, Khalili H, Tsai S et al. Comparative effectiveness study of drug-eluting and bare-metal peripheral artery stents in endovascular femoropopliteal artery revascularization. J. Invasive Cardiol. 30(10), 373–379 (2018).
71.
Kang WY, Campia U, Didier RJ et al. A single center experience of Zilver PTX for femoro-popliteal lesions. Cardiovasc. Revasc. Med. 17(6), 399–403 (2016).
72.
Karashima E, Takahara M, Hozawa K et al. Three-year clinical outcomes of the Innova™ self-expanding nitinol stent for the treatment of femoropopliteal lesions. Cardiovasc. Interv. Radiol. 44(11), 1722–1727 (2021).
73.
Karpenko AA, Rabtsun AA, Popova IV et al. Influence of lamina vastoadductoria dissection on the outcomes of femoral artery extensive lesion stenting: a pilot randomised investigation. J. Biomech. 136, 111053 (2022).
74.
Katsuki T, Takahara M, Soga Y et al. Mortality risk following application of a paclitaxel-coated stent in femoropopliteal lesions. J. Endovasc. Ther. 26(5), 593–599 (2019).
75.
Katsuki T, Tomoi Y, Yamaji K et al. Combination therapy of heparin-bonded covered stent and bare-nitinol stent assessed by intravascular ultrasound. Heart Vessels 35(11), 1502–1509 (2020).
76.
Kawamura Y, Ishii H, Aoyama T et al. Nitinol stenting improves primary patency of the superficial femoral artery after percutaneous transluminal angioplasty in hemodialysis patients: a propensity-matched analysis. J. Vasc. Surg. 50(5), 1057–1062 (2009).
77.
Kichikawa K, Ichihashi S, Yokoi H et al. Zilver PTX post-market surveillance study of paclitaxel-eluting stents for treating femoropopliteal artery disease in Japan: 2-year results. Cardiovasc. Interv. Radiol. 42(3), 358–364 (2019).
• This is a large prospective, multicentre study that includes 905 patients. This study reports two-year data on the safety and effectiveness of Zilver PTX.
78.
Kim J, Ko Y-G, Lee S-J et al. Korean Multicenter Registry of ELUVIA stent for femoropopliteal artery disease: K-ELUVIA Registry. Korean Circ. J. 54(9), 565–576 (2024).
79.
Ko Y-G, Ahn C-M, Rha S-W et al. Comparison of spot versus long stenting for femoropopliteal artery disease. Ann. Vasc. Surg. 58, 101–107 (2019).
80.
Kum S, Ipema J, Huizing E et al. Outcomes of the paclitaxel-eluting Eluvia stent for long femoropopliteal lesions in Asian patients with predominantly chronic limb-threatening ischemia. Vasc. Med. 26(3), 267–272 (2021).
81.
Labed P, Gonzalez F, Jayet J, Javerliat I, Coggia M, Coscas R. Endovascular treatment of long femoropopliteal lesions with contiguous bare metal stents. Ann. Vasc. Surg. 76, 276–284 (2021).
82.
Laird JR, Katzen BT, Scheinert D et al. Nitinol stent implantation vs. balloon angioplasty for lesions in the superficial femoral and proximal popliteal arteries of patients with claudication: three-year follow-up from the RESILIENT randomized trial. J. Endovasc. Ther. 19(1), 1–9 (2012).
83.
Laird JR, Jain A, Zeller T et al. Nitinol stent implantation in the superficial femoral artery and proximal popliteal artery: twelve-month results from the complete SE multicenter trial. J. Endovasc. Ther. 21(2), 202–212 (2014).
84.
Laird JR, Zeller T, Loewe C et al. Novel nitinol stent for lesions up to 24 cm in the superficial femoral and proximal popliteal arteries: 24-month results from the TIGRIS randomized trial. J. Endovasc. Ther. 25(1), 68–78 (2018).
85.
Lammer J, Zeller T, Hausegger KA et al. Heparin-bonded covered stents versus bare-metal stents for complex femoropopliteal artery lesions: the randomized VIASTAR trial (Viabahn endoprosthesis with PROPATEN bioactive surface VIA versus bare nitinol stent in the treatment of long lesions in superficial femoral artery occlusive disease). J. Am. Coll. Cardiol. 62(15), 1320–1327 (2013).
86.
Lammer J, Zeller T, Hausegger KA et al. Sustained benefit at 2 years for covered stents versus bare-metal stents in long SFA lesions: the VIASTAR trial. Cardiovasc. Interv. Radiol. 38(1), 25–32 (2015).
87.
Lee Y-J, Kook H, Ko Y-G et al. Drug eluting stent vs. drug coated balloon for native femoropopliteal artery disease: a two centre experience. Eur. J. Vasc. Endovasc. Surg. 61(2), 287–295 (2021).
88.
Leopardi M, Houbballah R, Becquemin JP. Effectiveness of Zilver PTX eluting stent in TASC C/D lesions and restenosis. J. Cardiovasc. Surg. 55(2), 229–234 (2014).
89.
Lichtenberg M, Kolks O, Hailer B et al. PEACE I all-comers registry: patency evaluation after implantation of the 4-French Pulsar-18 self-expanding nitinol stent in femoropopliteal lesions. J. Endovasc. Ther. 21(3), 373–380 (2014).
90.
Lichtenberg M, Breuckmann F, Kramer V et al. Effectiveness of the Pulsar-18 self-expanding stent with optional drug-coated balloon angioplasty in the treatment of femoropopliteal lesions – the BIOFLEX PEACE All-Comers Registry. VASA Zeitschrift fur Gefasskrankheiten 48(5), 425–432 (2019).
91.
Liistro F, Angioli P, Porto I et al. Drug-eluting balloon versus drug-eluting stent for complex femoropopliteal arterial lesions: the DRASTICO study. J. Am. Coll. Cardiol. 74(2), 205–215 (2019).
92.
Loureiro L, Pinelo A, Veterano C, Rocha H, Castro J, Machado R. Navigating complexity: the Supera's triumph in femoropopliteal lesions. Vascular 33(6), 1274–1281 (2025).
93.
Low J, Shih T, Lu E, Derubertis BG, Baril DT. Midterm results of the Supera stent for the treatment of femoropopliteal occlusive disease. Ann. Vasc. Surg. 86, 177–183 (2022).
94.
Ma H, Zhang X, Li J et al. Mid-term Efficacy and safety of drug-coated balloon versus nitinol bare metal stent for primary lesions in femoropopliteal artery disease. Ann. Vasc. Surg. 81, 316–323 (2022).
95.
Marples R, Binks M, Spina R, Wright M, Huilgol R. Prophylactic paclitaxel-eluting stent placement does not improve covered femoropopliteal stent patency. Surgery Open Sci. 7, 18–21 (2022).
96.
Matsumi J, Ochiai T, Tobita K et al. Long-term outcomes of self-expandable nitinol stent implantation with intraluminal angioplasty to treat chronic total occlusion in the superficial femoral artery (TransAtlantic Inter-Society Consensus Type D Lesions). J. Invasive Cardiol. 28(2), 58–64 (2016).
97.
Matsumi J, Takada T, Moriyama N et al. Long-term risks for patency loss in patients with hemodialysis after bare self-expandable nitinol stent implantation to femoropopliteal artery occlusive lesions. Int. J. Cardiol. 223, 268–275 (2016).
98.
Matsumura JS, Yamanouchi D, Goldstein JA et al. The United States StuDy for EvalUating EndovasculaR TreAtments of lesions in the superficial femoral artery and proximal popliteal by using the Protégé EverfLex NitInol STent SYstem II (DURABILITY II). J. Vasc. Surg. 58(1), 73–83.e1 (2013).
99.
McQuade K, Gable D, Pearl G, Theune B, Black S. Four-year randomized prospective comparison of percutaneous ePTFE/nitinol self-expanding stent graft versus prosthetic femoral-popliteal bypass in the treatment of superficial femoral artery occlusive disease. J. Vasc. Surg. 52(3), 584–590; discussion 590–591, 591.e1–591.e7 (2010).
100.
Meng F-C, Chen P-L, Lee C-Y, Shih C-C, Chen I-M. Real-world comparison of drug-eluting and bare-metal stents in superficial femoral artery occlusive disease with Trans-Atlantic Intersociety Consensus B Lesions: a 2-year, single-institute study. Acta Cardiologica Sinica 34(2), 130–136 (2018).
101.
Miura T, Miyashita Y, Soga Y et al. Drug-eluting versus bare-metal stent implantation with or without cilostazol in the treatment of the superficial femoral artery. Circ. Cardiovasc. Interv. 11(8), e006564 (2018).
102.
Montero-Baker M, Ziomek GJ, Leon L et al. Analysis of endovascular therapy for femoropopliteal disease with the Supera stent. J. Vasc. Surg. 64(4), 1002–1008 (2016).
103.
Mori S, Hirano K, Yamauchi Y et al. Penetration rate of the placement of a drug-eluting stent for the treatment of superficial femoral artery lesions in Japan. Heart Vessels 32(9), 1093–1098 (2017).
104.
Müller-Hülsbeck S, Keirse K, Zeller T, Schroë H, Diaz-Cartelle J. Twelve-month results from the MAJESTIC trial of the eluvia paclitaxel-eluting stent for treatment of obstructive femoropopliteal disease. J. Endovasc. Ther. 23(5), 701–707 (2016).
105.
Müller-Hülsbeck S, Keirse K, Zeller T, Schroë H, Diaz-Cartelle J. Long-term results from the majestic trial of the eluvia paclitaxel-eluting stent for femoropopliteal treatment: 3-year follow-up. Cardiovasc. Interv. Radiol. 40(12), 1832–1838 (2017).
106.
Myint M, Schouten O, Bourke V, Thomas SD, Lennox AF, Varcoe RL. A real-world experience with the Supera interwoven nitinol stent in femoropopliteal arteries: midterm patency results and failure analysis. J. Endovasc. Ther. 23(3), 433–441 (2016).
107.
Nakamura M, Jaff MR, Settlage RA, Kichikawa K. Nitinol self-expanding stents for the treatment of obstructive superficial femoral artery disease: three-year results of the RELIABLE Japanese multicenter study. Ann. Vasc. Dis. 11(3), 324–334 (2018).
108.
Nakao S, Iida O, Takahara M et al. Impact of procedural techniques on midterm patency of fluoropolymer-based drug-eluting stent placed in the femoropopliteal artery. J. Vasc. Interv. Radiol. 35(2), 259–268 (2024).
109.
Nanto K, Iida O, Takahara M et al. Effect of cilostazol following endovascular intervention for peripheral artery disease. Angiology 66(8), 774–778 (2015).
110.
Oberto S, Cetta F, Trabattoni P et al. Comparison of SFA lesion treatment with Zilver PTX in diabetics vs. non-diabetics: 2-year clinical and functional results. J. Cardiovasc. Surg. 58(4), 565–573 (2017).
111.
Okuno S, Iida O, Iida T et al. Comparison of clinical outcomes between endovascular therapy with self-expandable nitinol stent and femoral-popliteal bypass for Trans-Atlantic Inter-Society Consensus II C and D femoropopliteal lesions. Ann. Vasc. Surg. 57, 137–143 (2019).
112.
Palena LM, Isernia G, Parlani G et al. A multicenter prospective observational study appraising the effectiveness of the Supera stent after subintimal recanalization of femoro-popliteal artery occlusion: The SUPERSUB II study. Catheter Cardiovasc. Interv. 103(6), 963–971 (2024).
113.
Park J-I, Ko Y-G, Lee Y-J et al. Long coverage with drug-eluting stents is superior to spot coverage for long femoropopliteal artery disease: PARADE II study. Front. Cardiovasc. Med. 9, 1022071 (2022).
114.
Phair J, Carnevale M, Lipsitz EC, Shariff S, Scher L, Garg K. Amputation-free survival in patients with critical limb ischemia treated with paclitaxel-eluting stents and paclitaxel-coated balloons. Ann. Vasc. Surg. 62, 8–14 (2020).
115.
Phair J, Carnevale M, Lipsitz EC, Shariff S, Scher L, Garg K. Primary patency of long-segment femoropopliteal artery lesions in patients with peripheral arterial occlusive disease treated with paclitaxel-eluting technology. Ann. Vasc. Surg. 66, 595–600 (2020).
116.
Phillips JA, Falls A, Kolluri R et al. Full drug-eluting stent jacket: two-year results of a single-center experience with Zilver PTX stenting for long lesions in the femoropopliteal arteries. J. Endovasc. Ther. 25(3), 295–301 (2018).
117.
Powell RJ, Jaff MR, Schroë H, Benko A, Diaz-Cartelle J, Müller-Hülsbeck S. Stent placement in the superficial femoral and proximal popliteal arteries with the innova self-expanding bare metal stent system. Catheter Cardiovasc. Interv. 89(6), 1069–1077 (2017).
118.
Rammos C, Zeller T, Piorkowski M et al. The BioMimics 3D helical centreline nitinol stent in chronic limb threatening ischaemia and complex lesions: three year outcomes of the MIMICS-3D Registry. Eur. J. Vasc. Endovasc. Surg. 67(6), 923–932 (2024).
119.
Rastan A, Krankenberg H, Baumgartner I et al. Stent placement versus balloon angioplasty for the treatment of obstructive lesions of the popliteal artery: a prospective, multicenter, randomized trial. Circulation 127(25), 2535–2541 (2013).
120.
Salamaga S, Stępak H, Żołyński M et al. Three-year real-world outcomes of interwoven nitinol Supera stent implantation in long and complex femoropopliteal lesions. JCM 12(14), 4869 (2023).
121.
Saratzis A, Rudarakanchana N, Patel S et al. Interwoven nitinol stents versus drug eluting stents in the femoro-popliteal segment: a propensity matched analysis. Eur. J. Vasc. Endovasc. Surg. 58(5), 719–727 (2019).
122.
Saxon RR, Chervu A, Jones PA et al. Heparin-bonded, expanded polytetrafluoroethylene-lined stent graft in the treatment of femoropopliteal artery disease: 1-year results of the VIPER (Viabahn Endoprosthesis with Heparin Bioactive Surface in the Treatment of Superficial Femoral Artery Obstructive Disease) trial. J. Vasc. Interv. Radiol. 24(2), 165–73; quiz 174 (2013).
123.
Scheinert D, Grummt L, Piorkowski M et al. A novel self-expanding interwoven nitinol stent for complex femoropopliteal lesions: 24-month results of the SUPERA SFA registry. J. Endovasc. Ther. 18(6), 745–752 (2011).
124.
Scheinert D, Werner M, Scheinert S et al. Treatment of complex atherosclerotic popliteal artery disease with a new self-expanding interwoven nitinol stent: 12-month results of the Leipzig SUPERA popliteal artery stent registry. JACC Cardiovasc. Interv. 6(1), 65–71 (2013).
125.
Schulte K-L, Kralj I, Gissler HM et al. MISAGO 2: one-year outcomes after implantation of the Misago self-expanding nitinol stent in the superficial femoral and popliteal arteries of 744 patients. J. Endovasc. Ther. 19(6), 774–784 (2012).
126.
Shehada Y, Bisdas T, Argyriou A et al. Efficacy analysis following polymer coated drug eluting stent and bare metal stent deployment for femoropopliteal arterial disease. Vascular 32(1), 102–109 (2024).
127.
Shibata T, Iba Y, Shingaki M et al. One year outcomes of Zilver PTX versus Eluvia for femoropopliteal disease in real-world practice: REALDES study. J. Endovasc. Ther. 32(2), 490–497 (2025).
128.
Soga Y, Iida O, Hirano K, Yokoi H, Nanto S, Nobuyoshi M. Mid-term clinical outcome and predictors of vessel patency after femoropopliteal stenting with self-expandable nitinol stent. J. Vasc. Surg. 52(3), 608–615 (2010).
129.
Soga Y, Iida O, Hirano K et al. Utility of new classification based on clinical and lesional factors after self-expandable nitinol stenting in the superficial femoral artery. J. Vasc. Surg. 54(4), 1058–1066 (2011).
130.
Stavroulakis K, Torsello G, Manal A et al. Results of primary stent therapy for femoropopliteal peripheral arterial disease at 7 years. J. Vasc. Surg. 64(6), 1696–1702 (2016).
131.
Stavroulakis K, Torsello G, Bosiers MJ, Argyriou A, Tsilimparis N, Bisdas T. 2-year outcomes of the eluvia drug-eluting stent for the treatment of complex femoropopliteal lesions. JACC Cardiovasc. Interv. 14(6), 692–701 (2021).
132.
Steiner S, Schmidt A, Bausback Y et al. Midterm patency after femoropopliteal interventions: a comparison of standard and interwoven nitinol stents and drug-coated balloons in a single-center, propensity score-matched analysis. J. Endovasc. Ther. 23(2), 347–355 (2016).
133.
Stern JR, Tran K, Chandra V, Harris EJ, Lee JT. Paclitaxel exposure and long-term mortality of patients treated with the Zilver PTX drug-eluting stent. Vascular 29(4), 567–573 (2021).
134.
Sullivan TM, Zeller T, Nakamura M, Gaines PA. Treatment of femoropopliteal lesions with the BioMimics 3D vascular stent system: two-year results from the MIMICS-2 trial. J. Endovasc. Ther. 28(2), 236–245 (2021).
135.
Suzuki K, Takahara M, Shintani Y et al. Retrospective multicenter comparison of S.M.A.R.T. CONTROL and MISAGO stents in treatment of femoropopliteal lesions. J. Vasc. Interv. Radiol. 27(11), 1642–1649 (2016).
• This is a large multicentre, retrospective study with a large population, a total of 1505 cases. This study includes 2-year data on the performance of the two different stent types.
136.
Tan M, Urasawa K, Haraguchi T et al. Mortality risk after use of a paclitaxel-coated stent in femoropopliteal peripheral artery disease. Cardiovasc. Interv. Ther. 37(1), 136–144 (2022).
137.
Tan M, Takahara M, Soga Y et al. Three-year clinical outcomes following implantation of LifeStent self-expanding nitinol stents in patients with femoropopliteal artery lesions. Angiology 73(3), 244–251 (2022).
138.
Teymen B, Akturk S, Akturk U, Tdjani M. Comparison of drug-eluting balloon angioplasty with self-expanding interwoven nitinol stent deployment in patients with complex femoropopliteal lesions. Vascular 26(1), 54–61 (2018).
139.
Torsello GF, Stavroulakis K, Bisdas T, Cardona Y, Wichmann K, Torsello GB. Treatment of femoropopliteal artery disease with polymer-coated drug-eluting stent: 5-year results of a prospective, non-randomized study including the halo phenomenon. Cardiovasc. Interv. Radiol. 47(2), 177–185 (2024).
140.
Treitl KM, Woerner B, Schinner R et al. Evolution of patency rates of self-expandable bare metal stents for endovascular treatment of femoro-popliteal arterial occlusive disease: does stent design matter? Eur. Radiol. 27(9), 3947–3955 (2017).
141.
Tsujimura T, Takahara M, Iida O et al. Clinical outcomes of polymer-free, paclitaxel-coated stents vs stent grafts in peripheral arterial disease patients with femoropopliteal artery lesions. J. Vasc. Surg. 73(6), 1998–2008.e1 (2021).
142.
van Meirvenne E, Reyntjens P, Tielemans Y. Self-expanding interwoven nitinol stent in severe femoropopliteal arterial disease. Real life results of the Supera Peripheral Stent System®. Acta Chirurgica Belgica 123(5), 463–472 (2023).
143.
Vartanian SM, Johnston PC, Walker JP et al. Clinical consequence of bare metal stent and stent graft failure in femoropopliteal occlusive disease. J. Vasc. Surg. 58(6), 1525–1531 (2013).
144.
Vent P-A, Kaladji A, Davaine J-M et al. Bare metal versus paclitaxel-eluting stents for long femoropopliteal lesions: prospective cohorts comparison using a propensity score-matched analysis. Ann. Vasc. Surg. 43, 166–175 (2017).
145.
Watanabe Y, Hozawa K, Hiroyoshi K, Naganuma T, Ishiguro H, Nakamura S. The importance of patency of tibial run off arteries on clinical outcomes after stenting for chronic total occlusions in the superficial femoro-popliteal artery. Eur. J. Vasc. Endovasc. Surg. 56(6), 857–863 (2018).
146.
Werner M, Piorkowski M, Thieme M et al. SUMMIT registry: one-year outcomes after implantation of the EPIC self-expanding nitinol stent in the femoropopliteal segment. J. Endovasc. Ther. 20(6), 759–766 (2013).
147.
Werner M, Paetzold A, Banning-Eichenseer U et al. Treatment of complex atherosclerotic femoropopliteal artery disease with a self-expanding interwoven nitinol stent: midterm results from the Leipzig SUPERA 500 registry. Euro Intervention 10(7), 861–868 (2014).
148.
Wittig T, Schmidt A, Fuß T et al. Randomized trial comparing a stent-avoiding with a stent-preferred strategy in complex femoropopliteal lesions. JACC Cardiovasc. Interv. 17(9), 1134–1144 (2024).
149.
Yang M, Shi B, Ma L et al. Treatment of atherosclerotic femoropopliteal artery disease with supera interwoven nitinol stent: a real-world study in China. Ann. Vasc. Surg. 85, 183–189 (2022).
150.
Ye W, Böhme T, Fu W et al. First peripheral drug-eluting stent clinical results from China: 1-year outcomes of the Zilver PTX China study. Front. Cardiovasc. Med. 9, 877578 (2022).
151.
Ye M, Ni Q, Zhu Y et al. Stent graft vs drug-coated balloon in endovascular treatment of complex femoropopliteal artery lesions: a 2-center experience. J. Endovasc. Ther. 32(4), 1038–1046 (2025).
152.
Yokoi H, Ohki T, Kichikawa K et al. Zilver PTX post-market surveillance study of paclitaxel-eluting stents for treating femoropopliteal artery disease in Japan: 12-month results. JACC Cardiovasc. Interv. 9(3), 271–277 (2016).
153.
Yoshioka N, Tokuda T, Koyama A et al. Two-year clinical outcomes and predictors of restenosis following the use of polymer-coated paclitaxel-eluting stents or drug-coated balloons in patients with femoropopliteal artery disease. Heart Vessels 38(3), 429–437 (2023).
154.
Zamani N, Sharath SE, Browder RC et al. Outcomes after endovascular stent placement for long-segment superficial femoral artery lesions. Ann. Vasc. Surg. 71, 298–307 (2021).
155.
Zeller T, Rastan A, Macharzina R et al. Drug-coated balloons vs. drug-eluting stents for treatment of long femoropopliteal lesions. J. Endovasc. Ther. 21(3), 359–368 (2014).
156.
Zeller T, Gaines PA, Ansel GM, Caro CG. Helical centerline stent improves patency: two-year results from the randomized Mimics trial. Circ. Cardiovasc. Interv. 9(6), e002930 (2016).
157.
Zhao H, Ma B, Chen J et al. Drug-coated balloon versus bare nitinol stent in femoropopliteal artery: 12 months outcome from a single center in China. Ann. Vasc. Surg. 74, 367–381 (2021).
158.
Bosiers MJ, Donato G, Torsello G et al. ZILVERPASS Study: ZILVER PTX stent versus prosthetic above-the-knee bypass surgery in femoropopliteal lesions, 5-year results. Cardiovasc. Interv. Radiol. 46(10), 1348–1358 (2023).
159.
Maleckis K, Anttila E, Aylward P et al. Nitinol stents in the femoropopliteal artery: a mechanical perspective on material, design, and performance. Ann. Biomed. Eng. 46(5), 684–704 (2018).
160.
Nasr B, Gouailler F, Marret O et al. Treatment of long femoropopliteal lesions with self-expanding interwoven nitinol stent: 24 month outcomes of the STELLA-SUPERA trial. J. Endovasc. Ther. 30(1), 98–105 (2023).
161.
Müller-Hülsbeck S, Hopf-Jensen S, Keirse K et al. Eluvia drug-eluting vascular stent system for the treatment of symptomatic femoropopliteal lesions. Future Cardiol. 14(3), 207–213 (2018).
162.
Edwards CT, Schneider PA, Huynh C. Paclitaxel exposure and dosage of drug-coated devices for the treatment of femoropopliteal peripheral artery disease. Vasc. Endovasc. Rev. 4, e05 (2021).
163.
Palena LM, Diaz-Sandoval LJ, Sultato E et al. Feasibility and 1-year outcomes of subintimal revascularization with supera® stenting of long femoropopliteal occlusions in critical limb ischemia: the “Supersub” study. Catheter Cardiovasc. Interv. 89(5), 910–920 (2017).
164.
Tepe G, Brodmann M, Werner M et al. Intravascular lithotripsy for peripheral artery calcification: 30-day outcomes from the randomized disrupt PAD III trial. JACC Cardiovasc. Interv. 14(12), 1352–1361 (2021).
165.
Korosoglou G, Schmidt A, Lichtenberg M et al. Global algorithm for the endovascular treatment of chronic femoropopliteal lesions: an interdisciplinary expert opinion statement. JACC Cardiovasc. Interv. 18(5), 545–557 (2025).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Creative Commons Attribution 4.0 License
History
Received: 19 September 2025
Accepted: 26 January 2026
Published online: 10 March 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Performance of stenting in femoropopliteal disease: a systematic literature review and meta-analysis of proportions. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0152
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Viabahn Stent Graft and VBX Endoprosthesis: Scoping Review with ☸️SAIMSARA, SAIMSARA Journal, 10.62487/saimsarae1c09738, 1, 1, (2026).