Comparative effectiveness of oral antibiotics to treat uncomplicated urinary tract infections in male outpatients
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: New IDSA guidelines define uncomplicated UTI (uUTI) as infection limited to the bladder in both men and women. This study compared the effectiveness of β-lactams, nitrofurantoin and trimethoprim/sulfamethoxazole (TMP/SMX) to fluoroquinolones for outpatient uUTI treatment in men. Materials & methods: A retrospective cohort of adult male outpatients diagnosed with uUTI during 2019–2021 in the Department of Veterans Affairs system was created. Inclusion required an Emergency Department, Urgent/Primary Care visit with ICD-10 documentation of UTI and a prescription of interest dispensed. Patients with recent UTI, hospitalization, infectious co-diagnosis, temperature >99.9 F, pyelonephritis or prostatitis, or for whom asymptomatic bacteriuria treatment was appropriate were excluded. Overlap weighting propensity scores and generalized estimating equation models assessed the relative risk of a subsequent UTI-related visit or hospitalization within 3–30 days with a new antibiotic dispensed. Results: A total of 45,442 males (mean [SD]) age 71.6 (12.7) years were treated at 130 VA medical centers. Treatment n (%) included: β-lactams 17,655 (38.9%), nitrofurantoin 8394 (18.5%), TMP/SMX 9709 (21.4%) and fluoroquinolones 9684 (21.3%). UTI-related return visits occurred in 5453 (12.0%) and UTI-related hospitalization occurred in 1431 (3.1%). The adjusted relative risk (aRR, [95% CI]) of a return visit compared with fluoroquinolones was higher for β-lactams (1.22, [1.02, 1.48]) and nitrofurantoin (1.47, [1.23, 1.74]) but not for TMP/SMX (0.99, [0.80, 1.23]). The aRR for UTI-related hospitalization was not different for β-lactams (1.06, [0.80, 1.40] or TMP/SMX [0.80, [0.56, 1.15], but was lower for nitrofurantoin [0.60, [0.41, 0.89]). Conclusion: Compared with fluoroquinolones, β-lactam and nitrofurantoin prescribed for outpatient uUTI were associated with modestly increased UTI-related return visits but not hospitalization in men.
Plain language summary
Historically, urinary tract infection (UTI) in men have been considered to be complicated and to require prolonged treatment with antibiotics that achieve high systemic concentrations. New treatment guidelines classify infection limited to the bladder as uncomplicated (uUTI) in men which can be treated with shortened courses of select antibiotics. This study compared the effectiveness of commonly prescribed antibiotics for outpatient uUTI in men. A retrospective cohort of outpatients diagnosed with uUTI in the U.S. Department of Veterans Affairs system was conducted. Propensity score methods and generalized estimating equation models assessed the relative risk for subsequent UTI-related visit or hospitalization. The findings indicate that the commonly prescribed oral antibiotics nitrofurantoin, aminopencillins, and cephalosporins, but not trimethoprim/sulfamethoxazole were associated with a higher UTI return visit rate than fluoroquinolones and that shortened course treatment was not associated with a worse outcome. These findings generally support the new guideline recommendations for antibiotic selection and treatment duration in men.
Prior Infectious Diseases Society of America (IDSA) guidelines for urinary tract infection (UTI) management were limited to treatment of pre-menopausal women with uncomplicated infection [1]. Historically, UTI that occurs in men have been considered to be complicated due to anatomical abnormalities such as prostatic hyperplasia which may lead to bladder outlet obstruction and increased risk for prostate infection [2,3].
Newly released IDSA Guidelines on the Management of Complicated UTI redefine uncomplicated and complicated UTIs [4]. The new definitions classify uncomplicated UTI (uUTI) as infection limited to the bladder in both men and women; whereas, complicated UTI (cUTI) refers to infection beyond the bladder (i.e., pyelonephritis, febrile or other signs and symptoms of systematic illness, bacteremia, catheter-related or prostatitis in men). For patients without clinical instability or sepsis, risk factors for antibiotic resistance, or other contraindications, these guidelines and others recommend oral fluoroquinolones or trimethoprim/sulfamethoxazole (TMP/SMX) as preferred therapy with cephalosporins or amoxicillin/clavulanate as alternatives [5–7]. Further, these guidelines recommend that patients with cUTI who exhibit a clinical response to treatment can be treated with 5–7 days of therapy except for febrile men in whom acute bacterial prostatitis is suspected. This recommendation is primarily supported by evidence obtained from afebrile men treated with fluoroquinolones and TMP/SMX that found no difference between 7 and 14 days of treatment [8]. The IDSA guideline authors appropriately acknowledge that some of the recommendations are conditional and based on low certainty in evidence.
Alternatives such as oral β-lactams and nitrofurantoin are increasingly being used to treat outpatient UTIs [8–10]. Their widespread use, except for nitrofurantoin in women, has occurred in the absence of guideline recommendations endorsing their use as first-line therapy [1]. Nitrofurantoin is recommended as a first-line therapy for uUTI in women due to the high frequency (∼80%) of Escherichia coli as a pathogen, its favorable activity against this species, and low risk for toxicity [1]. A shorter duration of treatment is also increasingly used to treat male UTIs, many times with nonfluoroquinolone alternatives [10]. No comparative effectiveness research has evaluated antibiotic treatment recommendations utilizing the new uUTI definition in men.
The aim of this study was to compare the effectiveness of β-lactams, nitrofurantoin and TMP/SMX to fluoroquinolones for the outpatient treatment of uUTI in men. A secondary aim sought to determine if the effectiveness of these antibiotic classes was modified by a shortened duration of therapy.
Materials & methods
A national retrospective cohort study of outpatient male veterans diagnosed with UTI during calendar years 2019–2022 was conducted. Inclusion criteria required that patients received in-person care in an emergency department (ED), urgent care (UC) or primary care (PC) setting; that an International Classification of Diseases-Clinical Modification 10th revision (ICD-CM 10) for cystitis, related codes or UTI-NOS (Supplement 1) was coded for the index visit [11], and that a prescription for an oral antibiotic of interest was released to the patient on days 0–3 after the index visit. Antibiotics of interest included: β-lactams (amoxicillin, amoxicillin/clavulanate, cephalexin, cefuroxime, cefpodoxime, cefdinir), fluoroquinolones (levofloxacin, ciprofloxacin), nitrofurantoin and TMP/SMX. Fosfomycin was excluded due to sparse prescription for index visits. A single dose of intravenous or intramuscular antibiotics prior to initiation of oral antibiotics was allowed. Patients were excluded based on the following criteria (Supplement 1): UTI diagnosis within 30 days prior to the index visit; hospitalization within 7 days prior to the index visit; hospitalization or death within 2 days after the index visit; active prescription indicating treatment with antibiotics at the time of index visit; a temperature of >99.9 F or presence of more than one systemic inflammatory response criteria ± 1 day of visit; a co-diagnosis of infection (including acute prostatitis or pyelonephritis) for which antibiotics may have been indicated on the day of index visit; an antibiotic fill of >15 days as these likely represented intent to treat complicated infection or given for prophylaxis; release of multiple antibiotics within 2 days of index visit; a scheduled urological procedure 1 day before to 7 days after their index visit; or a patient with urinalyses that indicated collection via catheter [4,10–14].
Data were extracted from the VA Corporate Data Warehouse (CDW) [15]: patient demographics; vital signs; laboratory values including urine culture and susceptibility results; acute co-diagnoses; chronic comorbidities; antibiotic resistance risk factor history (prior hospitalizations/skilled nursing facility residence, antibiotic exposures, antibiotic resistant bacteria reported from prior cultures); the antibiotic dosage and duration prescribed; visit provider, practice setting, VA facility; and clinical outcomes of interest.
The primary end point was a new outpatient acute care visit that occurred between 3 and 30 days after the initial antibiotic prescription release (i.e., dispensed) date in which the subsequent visit had ICD-10 documentation consistent with a UTI diagnosis (including pyelonephritis or prostatitis) and a new oral antibiotic prescription was released (i.e., UTI return visit). Return visits with documented competing tier 1 or 2 diagnosis codes where antibiotics may have been indicated were not classified as UTI return visits [12]. A secondary clinical end point included hospitalization with antibiotics administered within the same 3–30 day time-frame in which there was ICD-10 documentation of a UTI or a condition that could have arisen as a complicating genitourinary condition with a suspected urinary source (e.g., sepsis ICD-10 code PLUS UTI code) with an antibiotic prescribed (Supplement 1) [13,14].
Manual chart review was performed on 150 randomly selected index visit records from the CDW extracted cohort to validate that no exclusion criteria were present and that the clinician intent was to treat a UTI with antibiotics. Chart review was also performed on an additional 100 records defined as having a UTI outpatient return visit, but was not performed on UTI-related inpatient hospitalization as these were previously assessed [10,13]. Chart review was performed by the primary author using a standardized assessment process in which cases were first reviewed for prior/current exclusion criteria, followed by evaluation of the visit note assessment/plan where treatment allocation became apparent. Results were reported as the positive predictive value (PPV) along with the primary reasons for non-inclusion.
Regression models of treatment allocation were developed separately for each antibiotic class, (β-lactams, nitrofurantoin and TMP/SMX) relative to fluoroquinolones. For each model, the first patient-visit with either prescribed antibiotic class was selected and a logistic regression model was developed from factors deemed likely to be associated with antibiotic selection. These included race, ethnicity, age, indicators of chronic comorbidity (Charlson index) [16], vital signs, ICD-10 coded UTI diagnosis (cystitis versus UTI-NOS), antibiotic-resistant risk factors identified within the prior 90 days (prescription of antibiotic class of interest, recovery of study antibiotic class resistant organism from culture, hospitalization or nursing home residence) [10,13], time represented as a binary variable indicating pre/post COVID-19 onset (i.e., mid-March, 2020), and setting (ED/UC or PC) To account for potential correlation within the same facility, a generalized estimating equation model with clustering of patients by facility using an exchangeable correlation structure was fit [17,18]. Overlap weights [19,20] were calculated from model outputs and balance was checked (standardized mean difference and variance ratio) across variables included in both propensity and outcome models [21]. VA facility complexity, as an indicator of size and structure of the treating facility [22], and region of the country (VA VISN code) were not used in propensity models but balance on both of these variables was confirmed.
The overlap weights were applied in each antibiotic class comparison with UTI return visit as the outcome, using a Poisson regression with a log link to facilitate calculation of relative risk [23,24]. The three antibiotic classes were modeled relative to fluoroquinolones. An additional variable included the impact of treatment duration for each antibiotic class, which was categorized into 0–7 versus 8–15 day increments. The duration variable was not balanced in all models, so it was included in an interaction with each antibiotic class. A generalized estimating equation framework with clustered patients by facility and an exchangeable correlation structure was again employed for the outcome models. The same approach was used to assess relative risk for hospitalization, both for propensity and outcome models, for the same three antibiotic class comparisons.
Two different sensitivity analyses were performed. For all sets of models, E-values were calculated to address the magnitude of unidentified confounders which could potentially impact conclusions regarding treatment [25]. Simulations were also conducted to evaluate the change in the relative risk for an antibiotic that could potentially occur due to the inclusion of errant cases in the dataset (based on chart validation). For each antibiotic, based on chart review findings, 20% of the outcome (outpatient return visits) were randomly changed to treatment success. The outcome models were refit and the relative risk for the antibiotic was recorded. This was repeated 1000-times, and the 2.5th and 97.5th percentiles of relative risk were identified. These intervals were compared with the original relative risk for each antibiotic to evaluate whether inclusion of errant cases could have affected the magnitude and statistical significance of relative risk outcome. This sensitivity simulation was repeated for the hospitalization outcome. Additional post hoc analyses were conducted to better understand the findings. Specifically, we compared characteristics of patients prescribed nitrofurantoin across hospitalizations, return visits and treatment success, using one-way ANOVA or chi-square tests. We further compared these characteristics among hospitalizations and return visits using t-tests or chi-square tests.
All models were built using R version 4.3.1 [26] with RStudio [27], and using the libraries tidyverse [28], geepack [29], cobalt [30], gt summary [31], gt [32] and openxlsx [33].
This research was determined as exempt by the VA Puget Sound Investigational Review Board and complied with all federal guidelines and Department of Veterans Affairs policies relative to human subjects research.
Results
A total of 103,190 UTI patient-visits within 130 VA medical centers were identified, of which 45,442 patient-visits were analyzed after applying exclusions (Table 1 & Figure 1). Antibiotic treatments of interest included: β-lactams 17,655 (38.9%), nitrofurantoin 8394 (18.5%), TMP/SMX 9709 (21.4%) and fluoroquinolones 9684 (21.3%). Most patients were elderly, male, Caucasian, had normal vital signs and modest comorbidity. The aggregate 30-day UTI return visit rate was 5453 (12.0%) and the frequency of hospitalization was 1431 (3.1%).
| Characteristic | Fluoroquinolones (n = 9684) | β-lactam (n = 17,655) | Nitrofurantoin (n = 8394) | TMP/SMX (n = 9709) |
|---|---|---|---|---|
| Demographics | ||||
| Age (years), mean (SD) | 71.1 (12.8) | 73.0 (12.3) | 71.4 (12.1) | 69.6 (13.6) |
| <50 (%) | 6.5 | 4.8 | 5.7 | 8.8 |
| >50 <65 (%) | 17.5 | 14.8 | 16.9 | 19.5 |
| >65 (%) | 76.1 | 80.3 | 77.4 | 71.7 |
| Race (%) | 6.5 | 4.8 | 5.7 | 8.8 |
| Caucasian | 67.6 | 65.8 | 68.5 | 66.8 |
| African–American | 22.6 | 24.9 | 22.8 | 23.3 |
| Other | 9.8 | 9.3 | 8.8 | 9.9 |
| Hispanic/Latino (%) | 7.6 | 7.8 | 6.1 | 7.4 |
| Vital signs and comorbidity | ||||
| Temperature (F), mean (SD) | 98.0 (0.7) | 98.0 (0.7) | 98.0 (0.7) | 98.0 (0.8) |
| Heart rate (BPM), mean (SD) | 79.0 (14.6) | 79.5 (14.9) | 78.4 (14.6) | 79.1 (14.7) |
| Respiratory rate (BPM), mean (SD) | 17.6 (2.7) | 17.5 (2.5) | 17.5 (2.4) | 17.6 (2.8) |
| Systolic BP, mean (SD) | 138.0 (22.4) | 139.5 (23.3) | 137.6 (21.4) | 137.0 (21.3) |
| Charlson comorbidity, median (IQR) | 2.0 (3.0) | 2.0 (3.0) | 1.0 (3.0) | 1.0 (3.0) |
| Laboratory tests‡ | ||||
| WBC (mm3), mean (SD) | 8.7 (4.8) | 8.4 (3.7) | 8.0 (2.9) | 8.2 (3.6) |
| Urine culture collected (%) | 61.9 | 62.6 | 58.8 | 59.5 |
| Positive urine culture (% of UC) | 63.1 | 66.7 | 60.2 | 62.5 |
| Cultured organisms§ | ||||
| Escherichia coli | 39.0 | 40.1 | 44.1 | 41.4 |
| Other GNB | 42.8 | 40.2 | 34.1 | 40.4 |
| Other GPC | 19.4 | 18.9 | 24.1 | 18.7 |
| Treatment discordance¶,# | ||||
| Any cultured organism | 11.2 | 10.2 | 18.0 | 10.2 |
| Escherichia coli | 15.4 | 2.1 | 1.8 | 14.8 |
| Other GNB | 6.5 | 2.5 | 49.8 | 6.4 |
| Other GPC | 12.2 | 44.1 | 0.8 | 8.0 |
| Treatment location | ||||
| Emergency department | 54.6 | 75.5 | 50.0 | 48.6 |
| Primary care | 45.4 | 24.5 | 50.2 | 48.6 |
| Antibiotic resistance risk factors | ||||
| Inpatient stay in last 90 days (%) | 9.7 | 11.8 | 8.4 | 8.5 |
| UTI antibiotics in last 90 days (%) | 8.3 | 6.9 | 5.0 | 7.1 |
| Resistant organism in last 90 days (%) | 7.7 | 7.1 | 6.0 | 6.4 |
†
Demographic characteristic for cohort after exclusions applied (Figure 1).
‡
WBC obtained n = 23,190.
§
Urine culture obtained n = 27,769, positive urine culture (n = 17,749) if any bacterial species reported irrespective of organism quantity. E. coli was reported in 7244 (40.8%), other GNB organisms 7062 (39.8%) and other GPC organisms in 3519 (19.8%) of cultures.
¶
Discordance determined by a susceptibility result indicating intermediate/resistance or by expert rule (e.g., β-lactam resistant to all ESBL producing isolates) for prescribed antibiotic. Organism discordance based on total number of patient-visits treated with each drug class and total positive cultures.
#
Emergency department included fast track and Primary care Episodic Care which are considered to be Urgent care within the VA.
††
Definitions modified to include antibiotic exposure to any of the study antibiotics and organisms with non-susceptibility results reported to fluoroquinolones, 3rd or 4th generation cephalosporins, nitrofurantoin or TMP/SMX.
GNB: Gram negative bacilli.; GPC: Gram-positive cocci; IQR: Interquartile range; SD: Standard deviation; TMP/SMX: Trimethoprim/sulfamethoxazole; UTI: Urinary tract infection.
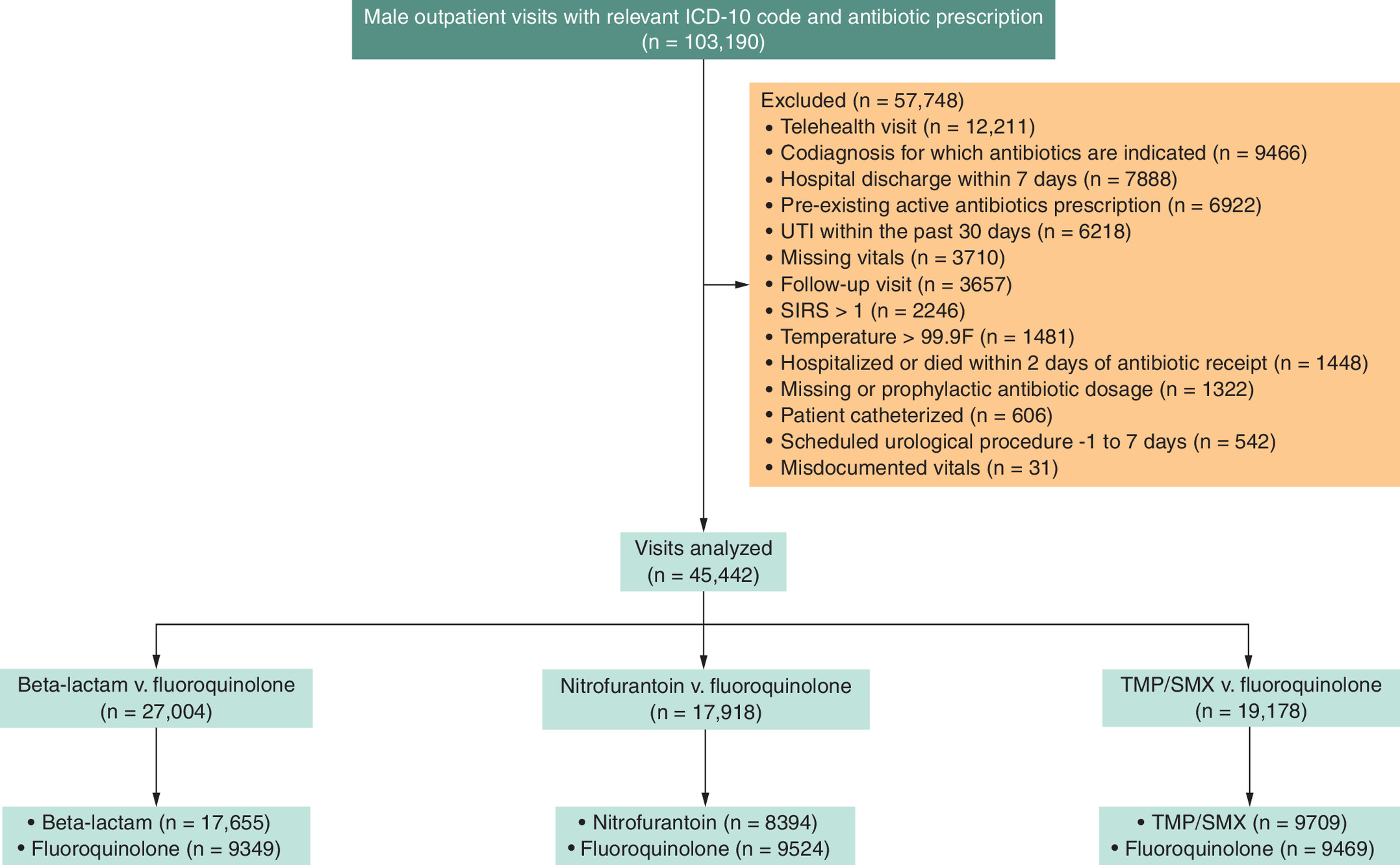
Figure 1. Study flow diagram for veterans treated for urinary tract infections with comparator antibiotic classes relative to fluoroquinolones.
TMP/SMX: Trimethoprim/sulfamethoxazole. Global exclusions: more than one exclusion criteria may have applied. Propensity weighting: Fluoroquinolone patient-visits could be utilized in more than one antibiotic comparison. Mis-documented vitals refers to physiological incompatible values defined as a value >10-fold different than the mean values.
After development of overlap weighting models, potential confounders in treatment groups were well balanced with the exception of duration of therapy (Supplement 2 & 3).
The adjusted relative risk (aRR [±95% CI]) of 30-day outpatient UTI return visits for antibiotics of interest compared with fluoroquinolones was higher for β-lactams (1.22, [1.02, 1.48]) and nitrofurantoin (1.47, [1.23, 1.74]) but not for TMP/SMX (0.99, [0.80,1.21]). Relative risk for hospitalization associated with β-lactams (1.06, [0.80, 1.40]) and TMP/SMX (0.80, [0.56, 1.15]) was not different than the fluoroquinolones; whereas, relative risk of hospitalization was lower with nitrofurantoin (0.60, [0.41, 0.89]) (Tables 2 & 3 & Figure 2 & Supplement 4).
| Antibiotic class | UTI return visit (%)† | Hospital admission (%)† | Adjusted relative risk for UTI return visit | ±95% CI | Adjusted relative risk for hospital admission | +95% CI |
|---|---|---|---|---|---|---|
| Fluoroquinolones | 9.9 | 2.8 | Ref | Ref | Ref | Ref |
| β-lactams | 13.1 | 3.9 | 1.22 | 1.02,1.48 | 1.06 | 0.80,1.40 |
| Nitrofurantoin | 13.7 | 2.7 | 1.47 | 1.23,1.74 | 0.60 | 0.41, 0.89 |
| TMP/SMX | 10.6 | 2.5 | 0.99 | 0.80,1.23 | 0.80 | 0.56,1.15 |
Bold indicates statistically significant result.
†
UTI return visits and hospital admissions represent unadjusted percentages for these end points. Adjust relative risk for UTI return visits and hospital admission from models represented in Table 3 & Supplement 4, respectively.
CI: Confidence interval; Ref: Reference; TMP/SMX: Trimethoprim/sulfamethoxazole; UTI: Urinary tract infection.
| Antibiotic class | β-lactam | Nitrofurantoin | TMP/SMX |
|---|---|---|---|
| Variables | Adjusted risk ratio (±95% CI) | ||
| Intercept | 0.09 (0.07, 0.11) | 0.09 (0.07, 0.11) | 0.08 (0.07, 0.11) |
| Antibiotic comparator | 1.22 (1.02, 1.48) | 1.47 (1.23, 1.74) | 0.99 (0.80, 1.23) |
| Demographics | |||
| Age <50 years | Ref | Ref | Ref |
| Age 50–64 years | 1.20 (0.99, 1.45) | 1.18 (0.93, 1.49) | 1.23 (1.01, 1.49) |
| Age ≥65 years | 1.19 (0.99, 1.42) | 1.13 (0.91, 1.40) | 1.19 (1.00, 1.42) |
| Race, Caucasian | Ref | Ref | Ref |
| African–American | 0.87 (0.80, 0.95) | 0.81 (0.72, 0.91) | 0.86 (0.77, 0.95) |
| Other race/ethnicity | 0.94 (0.83, 1.07) | 0.88 (0.74, 1.03) | 0.91 (0.77, 1.08) |
| Hispanic/Latino | 0.84 (0.73, 0.96) | 0.87 (0.73, 1.04) | 0.85 (0.69, 1.04) |
| Charlson Index | 1.04 (0.99, 1.08) | 1.08 (1.03, 1.12) | 1.09 (1.04, 1.14) |
| Vital signs | |||
| Temperature | 1.03 (0.99, 1.06) | 1.01 (0.97, 1.06) | 1.05 (1.01, 1.09) |
| Heart rate | 1.06 (1.03, 1.10) | 1.05 (1.01, 1.09) | 1.03 (0.99, 1.07) |
| Respiration | 1.03 (1.00, 1.06) | 1.01 (0.96, 1.07) | 1.03 (0.99, 1.07) |
| Systolic BP | 0.98 (0.93, 1.03) | 1.00 (0.95, 1.05) | 0.95 (0.90, 1.01) |
| Diastolic BP | 1.00 (0.95, 1.05) | 1.03 (0.98, 1.08) | 1.01 (0.96, 1.07) |
| Antibiotic resistance risk in last 90 days | |||
| No antibiotic exposure | Ref | Ref | Ref |
| Fluoroquinolone | 1.74 (1.53, 2.00) | 1.55 (1.28, 1.87) | 1.62 (1.36, 1.94) |
| Comparator | 1.43 (1.24, 1.66) | 1.97 (1.67, 2.32) | 1.44 (1.19, 1.74) |
| Both antibiotic | 1.47 (1.17, 1.85) | 2.08 (1.55, 2.80) | 1.52 (1.08, 2.14) |
| No resistant isolate | Ref | Ref | Ref |
| Fluoroquinolone resist | 1.34 (1.02, 1.77) | 1.00 (0.74, 1.34) | 0.76 (0.50, 1.16) |
| Comparator resist | 1.23 (0.92, 1.64) | 1.19 (0.90, 1.59) | 2.06 (1.42, 2.99) |
| Resist to both | 1.32 (0.90, 1.94) | 1.35 (0.84, 2.15) | 2.55 (1.91, 3.42) |
| Inpatient stay relative to none | 1.18 (1.05, 1.33) | 1.29 (1.12, 1.48) | 1.22 (1.08, 1.38) |
| Other variables | |||
| Primary Care relative to ED | 0.70 (0.60, 0.82) | 0.74 (0.63, 0.87) | 0.73 (0.62, 0.86) |
| Post COVID-19 onset relative to prior | 1.01 (0.88, 1.17) | 1.03 (0.89, 1.20) | 1.02 (0.88, 1.17 |
| Treatment 8–15 days relative to 5–7 days | 0.86 (0.75, 0.98) | 0.87 (0.75, 0.99) | 0.83 (0.72, 0.95) |
| Interactions | |||
| Antibiotic* treatment duration | 1.11 (0.93, 1.31) | 1.16 (0.98, 1.38) | 1.15 (0.94, 1.39) |
| Antibiotic* pre/post COVID-19 onset | 1.01 (0.84, 1.21) | 1.02 (0.85, 1.22) | 1.13 (0.93, 1.38) |
| Antibiotic* PC/ED setting | 1.18 (0.96, 1.44) | 0.84 (0.68, 1.02) | 1.03 (0.86, 1.23) |
Bold indicates statistically significant result.
Models for outpatient revisits excluded patients with revisits with co-diagnoses for non-UTI infectious conditions: β-lactam (n = 247) vs fluoroquinolones (n = 111), nitrofurantoin (n = 125) vs fluoroquinolones (n = 239), TMP/SMX (n = 115) vs fluoroquinolones (n = 114). Sample sizes utilized in calculating interactions for antibiotic * treatment duration included: β-lactams (≤7 days n = 10,355, >7–15 days n = 6362) vs fluoroquinolones (≤7 days n = 5964, >7–15 days n = 2080), nitrofurantoin (≤7 days n = 5609, >7–15 days n = 3376) vs fluoroquinolones (≤7 days n = 5711, >7–15 days n = 3342), TMP/SMX (≤7 days n = 5785, >7–15 days n = 3564) vs fluoroquinolones (≤7 days n = 5680, >7–15 days n = 3412). Sample sizes utilized in calculating interactions for antibiotic * pre/post COVID-19 onset included: β-lactams (pre-COVID-19 n = 3578, post-COVID-19 n = 13,139) vs fluoroquinolones (pre-COVID-19 n = 3287, post-COVID-19 n = 5698), nitrofurantoin (pre-COVID-19 n = 2113, post-COVID-19 n = 5931) vs fluoroquinolones (pre-COVID-19 n = 3297, post-Covid n = 5846), TMP/SMX (pre-COVID-19 n = 2937, post-COVID-19 n = 6413) vs fluoroquinolones (pre-COVID-19 n = 3289, post-COVID-19 n = 5803). Sample sizes utilized in calculating interactions for antibiotic * setting included: β-lactams (ED n = 12,508, UC or PC n = 4209) vs fluoroquinolones ED n = 4762, UC or PC n = 4223), nitrofurantoin (ED n = 3947, UC or PC n = 4097) vs fluoroquinolones (ED n = 4911, UC or PC n = 4232), TMP/SMX (ED n = 4731, UC or PC n = 4619) vs fluoroquinolones (ED n = 4874, UC or PC n = 4218).
TMP/SMX: Trimethoprim/sulfamethoxazole; Resist.: Resistant; ED: Emergency department.
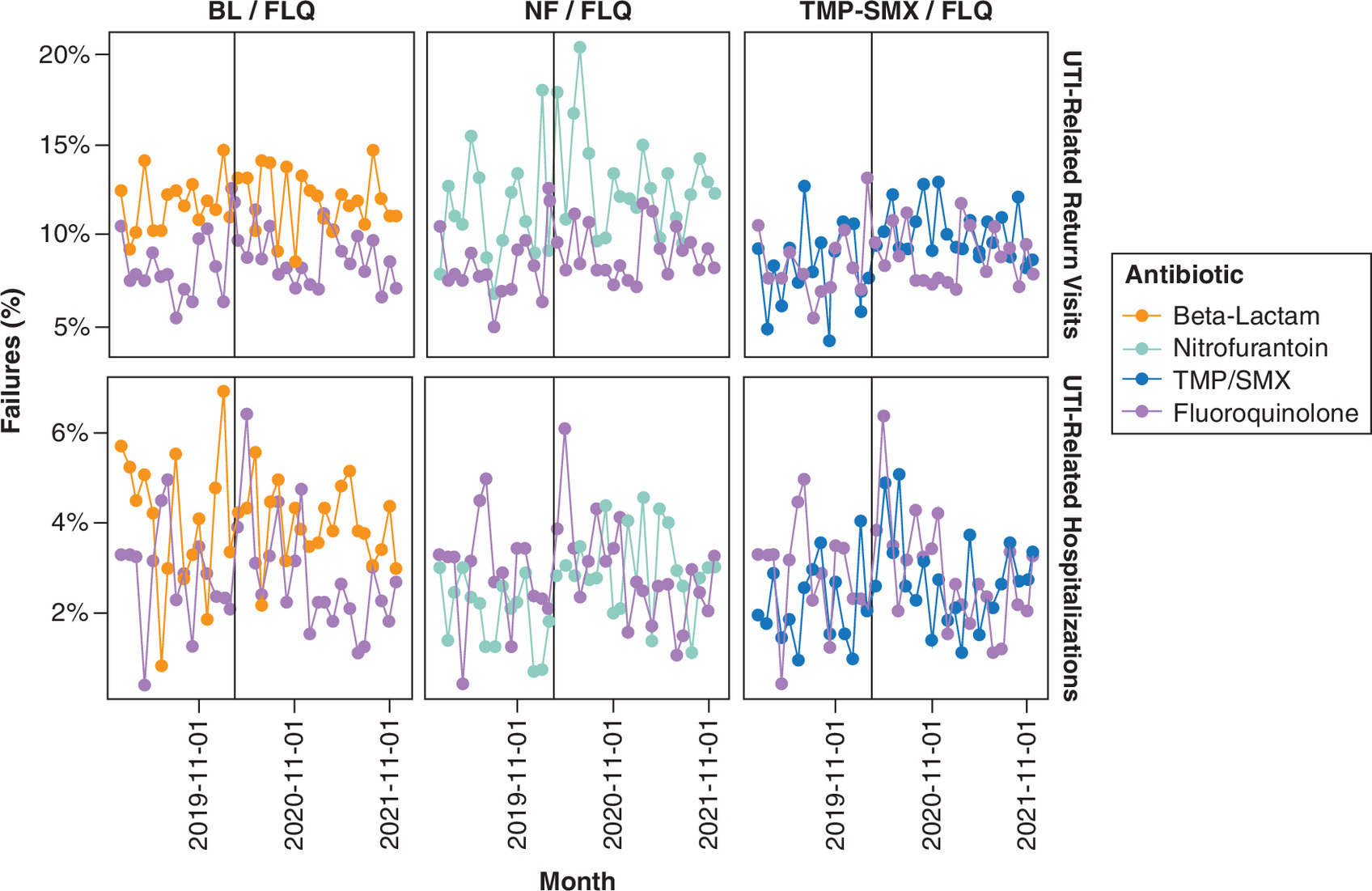
Figure 2. Cohort monthly return urinary tract infectionvisits and hospitalization for comparator and fluoroquinolone antibiotic classes.
Inpatient: admission between 3 and 30 days post-prescription release. Outpatient: return visit with urinary tract infection-coded encounter within 3–30 days post prescription release.
BL: β-lactam; FQ: Fluoroquinolone; NF: Nitrofurantoin; TMP/SMX: Trimethoprim/sulfamethoxazole.
An analysis of interactions in UTI return visits models indicated that neither treatment duration, practice setting, or visit time dichotomized by pre/post COVID-19 onset were associated with the outcome for any antibiotic comparison. Significant interactions between nitrofurantoin and treatment duration [1.54 (1.09, 2.22)] and pre/post COVID-19 onset [1.90 (1.3, 2.77)] were identified in the hospitalization model (Table 3 & Supplement 4). The interactions indicate that nitrofurantoin had large increase in aRR for hospitalization after COVID-19 onset [1.14 (0.89, 1.47)], (Figure 2) and with a longer nitrofurantoin treatment duration compared with the fluoroquinolones.
Manual chart review of index visits indicated a PPV of 88.0%; 132/150 cases had no exclusion criteria present and the clinician intent was to treat a UTI. The primary reasons for exclusion were that patients were treated for UTI external to the VA in the previous 30 days or had an un-coded concurrent tier 1 or 2 diagnosis where antibiotics may have been indicated. Manual chart review of the outpatient UTI-related return visit cases indicated that the PPV was 79.0%; 79/100 cases had a return visit in which the clinician prescribed further antibiotics for a UTI-related condition. The primary reason for exclusion was an un-coded concurrent tier 1 or 2 diagnosis where antibiotics may have been indicated. The possibility that as many as 21% of return visits could have been for something other than UTI was the basis of the sensitivity analysis performed for this study.
Sensitivity analyses indicated that E-values and lower confidence levels (LCLs) for outpatient UTI return visits were higher than observed covariate relative risks for the outpatient UTI-return visits reported in the β-lactam and nitrofurantoin models but not for the TMP/SMX models (Table 4). These findings indicate that a very large (aRR >1.75–2.25) unobserved confounding variable could alter results for β -lactam or nitrofurantoin outpatient revisit models. For inpatient admissions, point estimates for the E-values were higher than observed covariate relative risks for the nitrofurantoin and TMP/SMX models, but not for the β-lactam model. The point estimates of the E-values for the β-lactam and TMP/SMX are larger than most, but not all, of the model coefficients, suggesting relatively large unidentified covariates could potentially alter results.
| Analysis/model | β-lactam | Nitrofurantoin | TMP/SMX |
|---|---|---|---|
| E-values | |||
| UTI-related return visits | 1.75 (1.14, NA) | 2.29 (1.76, NA) | 1.10 (1.00, NA) |
| UTI-related hospitalizations | 1.31 (1.00, NA) | 2.72 (1.49, NA) | 1.81 (1.00, NA) |
| Simulated outcome | |||
| UTI-related return visits | (1.11, 1.34) | (1.31, 1.63) | (0.88, 1.11) |
| Treatment duration 8–15 days | (1.01, 1.21) | (1.05, 1.30) | (1.04, 1.27) |
| UTI-related hospitalizations | (0.91, 1.24) | (0.48, 0.73) | (0.65, 0.95) |
| Treatment duration 8–15 days | (0.77, 1.06) | (1.26, 1.88) | (1.08, 1.58) |
Bold indicates statistically significant result.
Simulated outcome results indicate the 2.5th and 97.5th percentiles for the aRR of each comparator based on random replacement of 20% of clinical failures with success in each model repeated 1000-times. Treatment duration reference group 5–7 days.
NA: Not applicable; TMP/SMX: Trimethoprim/sulfamethoxazole; UTI: Urinary tract infection.
The simulations utilizing altered outcome data indicated that even with a 20% drop in outpatient UTI-related return visits, the original aRR for each antibiotic relative to fluoroquinolone was within the simulated 95% confidence interval for aRR (Table 4). However, while the modelled aRR estimates for longer treatment duration lie within the 2.5th and 97.5th percentiles of the simulated coefficients, the results indicate that the aRR for longer treatment duration is higher for all comparators. Finally, a 20% drop in hospitalizations indicates that TMP/SMX could result in a significant lower aRR whereas a significant aRR for longer treatment is possible.
An assessment of positive culture results indicated that treatment discordance with nitrofurantoin was significantly higher (adjusted p < 0.05) compared with the other three antibiotic classes (Table 1). Discordance for patients with E. coli recovered was highest for fluoroquinolones and TMP/SMX and lowest for nitrofurantoin and β-lactams (adjusted p < 0.05). While E. coli was the most common organism recovered overall it was only identified in 40.8% of positive cultures. In contrast, other Gram-negative organisms were identified in 39.8% of positive cultures, and treatment discordance with β-lactams was higher (adjusted p < 0.001) compared with the other three antibiotic classes, primarily due to treatment with oral cephalosporins and the recovery of Enterococcus spp.
Comparison of the patient-level characteristics for fluoroquinolone or nitrofurantoin recipients who experienced treatment success or failure with an outpatient revisit or inpatient admission are presented in (Supplement 5). As expected patients experiencing treatment success were less acutely ill and had less chronic comorbidity than treatment failures. They were more likely to have been initially treated in primary care, less likely to have antibiotic resistance risk factors, have a UC collected, or receive discordant treatment. Differences in characteristics between inpatient and outpatient failures were few and sample size for some characteristics for inpatient admissions was limited. Patients who experienced inpatient admission had more comorbidity, more likely to have been initially seen in the ED, and were more likely to have been recently hospitalized than patients experiencing outpatient failure. Differences in microbiology or treatment discordance were not apparent between inpatient and outpatient failures.
Discussion
There are several notable findings from this comparative effectiveness analysis of oral antibiotics for the treatment of uUTI in males. First, modestly higher outpatient return visit rates were observed for treatment with β-lactams and nitrofurantoin relative to fluoroquinolones. Overall, UTI-related hospitalizations were low; and while no differences between β-lactam or TMP/SMX treatments and fluoroquinolones were observed, nitrofurantoin recipients had a reduced aRR for hospitalization. Assessment of the interaction between nitrofurantoin and post COVID-19 onset indicated a large increase in aRR for hospitalization, consistent with the estimated aRR for outpatient return visits. The interactions between antibiotic and treatment duration did not identify a modifying effect with a shorter versus longer treatment duration for either end point.
Plausible explanations for the increased outpatient return visits include treatment culture discordance, undiagnosed or mis-coded complicated infection, potentially combined with unfavorable pharmacokinetic properties of β-lactams and nitrofurantoin. Antibiotic resistance risk factors, particularly recent prior antibiotic exposure exhibited large aRR for both end points. In other VHA work we have demonstrated a protective effect for UC in patients with recent prior antibiotic exposures [13]. While positive UC were obtained in approximately 1/3rd of patients; E. coli was only identified in 40% of positive cultures. Additionally, discordance between nitrofurantoin and cultured Gram-negative organisms other than E. coli was high. A possible explanation for the higher return visit rate observed with nitrofurantoin includes the potential for non-E. coli pathogens to be intrinsically resistant to this antibiotic [34]. A second possibility is that clinicians have difficulty distinguishing between uUTI and acute prostatitis. In other work we have observed that documentation of acute prostatitis assessment and/or diagnosis in the eHR occurs in approximately 2% of ED/UC visits for UTI related presentations where an antibiotic is prescribed [35]. Both nitrofurantoin and oral β-lactam antibiotics possess unfavorable pharmacokinetics properties that contribute to low concentrations in prostate tissue or in systemic infections. While the study criteria attempted to restrict visits consistent with the new UTI guideline definition for uUTI it is plausible that not all patients with cUTI were identified during data extraction or that clinicians underdiagnosed cUTI. The outpatient return visit findings are also consistent with observations and guideline recommendations that nitrofurantoin should not be used to treat cUTI and that β-lactam therapy is associated with a higher relapse rate in men [4,6,10,36]. The observation that nitrofurantoin had a lower aRR for hospitalization was unanticipated, especially as the unadjusted rate was similar to fluoroquinolones. It is important to recognize that the baseline reported point estimate for nitrofurantoin represented the Pre-COVID-19 period, and when the interaction with COVID-19 is considered the point estimate for inpatient failures is non-significant [1.14 (0.89, 1.47)], Other relative changes in antibiotic prescription changed over time with reductions in fluoroquinolone use and increased for alternative antibiotics. For example, nitrofurantoin prescription increased from an average of 150/month prior to COVID-19 onset to 270/month post COVID-19 onset. One possibility is that as clinicians sought alternatives to fluoroquinolones they broadened patient selection for empirical nitrofurantoin use. Comparison of inpatient and outpatient failures indicated that treatment discordance was similar between end points, and admitted patients on average had more comorbidity, ED presentation, and antibiotic resistance risk factors; however, sample sizes for inpatient failures were limited in these strata. Finally, the potential for unmeasured confounding as represented by E-values was the highest for the nitrofurantoin hospitalization model and cannot be excluded.
Study strengths include the use of the nationwide VHA data warehouse for conducting the study, which allowed development of a detailed analysis including integration of outpatient visits and hospital admissions. Index visits were limited to those conducted in person with prescription of a single antibiotic to facilitate risk adjustment based on complete data. Another strength includes adjustment using overlap weighting which balances the mean of measured covariates [19,20]. Finally, the cohort criteria generally aligns with the new guideline definitions for uUTI in men.
Limitations are consistent with other retrospective database studies conducted within the VHA and elsewhere. Patients could have received diagnosis or treatment in non-VHA settings that would not be completely captured within the CDW, which may have biased risk adjustment or outcome. Second, UTI index visits were identified utilizing administrative data and in other work we observed that the specificity for UTI type (e.g., cystitis, pyelonephritis, prostatitis) within the VHA is poor as >85% of cases are classified as UTI-NOS and frequently other genitourinary diagnostic codes are used despite chart documentation of UTI treatment intent [10,13,37]. While most cases of cUTI were removed by applying other exclusion criteria including fever, we were unable to fully exclude catheterized patients with administrative data. In prior work we identified that ASB treatment occurs and it is likely that some patients were treated irrespective of symptoms [10]. In the current study, chart review demonstrated that in 88% of index cases, clinician prescribed an antibiotic with the intent to treat a UTI, irrespective of true diagnosis. The difference in return visits as an end point is meaningful in that the assumption on follow-up is that these patients were initially diagnosed with a UTI and were prescribed another antibiotic. An additional limitation was that chart review indicated that 78% of UTI return visits received antibiotics for a UTI-related condition. However, the sensitivity analysis with random replacement of cases did not identify an issue with inclusion of errant UTI return visits. Hospitalization was uncommon and the power to detect differences in this outcome and for select interactions was low. VHA patients could also have a higher portion of non- E. coli pathogens compared with other healthcare systems. However, A recent nationwide (n = 33,113) retrospective cohort study of UTIs in males (mean age = 70.7 years) in 15 French EDs reported a similar E. coli prevalence of 40.0%, and similar rates of non-E coli GNB and GPC [38]. Culture and susceptibility results were reported in less than half of the eligible visits, and each facility applies their own selective susceptibility reporting criteria. While not all susceptibility results performed are entered into the electronic health record (e.g., selective reporting) they are available in the VHA CDW. While discordant treatment with nitrofurantoin is a plausible explanation, caution is advised when extrapolating these results to other patient populations. Finally, we did not consider the downstream effects of the index visit therapy on subsequent antibiotic resistance or adverse events.
Historically there has been a lack of consensus on the definition of cUTI in men with some guidelines recommending that all UTIs in males are complicated versus others that take a more selective approach [39,40]. The recently published IDSA guidelines for cUTI suggest that men without systemic signs of illness or signs or symptoms of prostatitis or pyelonephritis can be managed as uUTI [4]. Our findings are consistent with cUTI guideline recommendation that list fluoroquinolones or TMP/SMX as preferred oral therapy; reservation or β-lactams as alternatives, and avoidance of nitrofurantoin. Consistent with guideline recommendation, we did not observe additional benefit with therapy >7 days. These recommendations are supported in part by the findings of Drekonja et al. that found no difference between 7 versus 14 days of therapy for afebrile male veterans treated with ciprofloxacin or TMP/SMX [7]. In contrast, a recent multi-centered non-inferiority study of 7 versus 14 days of antibiotic therapy in febrile men determined that 7 days of treatment was inferior to 14 days of therapy [41]. Further, a recent analysis of male UTIs in Europe observed a higher clinical failure rate of UTI treatment with nitrofurantoin and β-lactams relative to fluoroquinolones which is similar to our findings [35].
Future work should include additional adequately powered comparative studies of outpatient antibiotic regimens in men for uUTI. Improved diagnostic strategies are also needed to assist in differentiating complicated from uUTI in men and assessment of the new IDSA guideline UTI definitions. Given the increasing frequency of discordant empirical antibiotic selection for UTI, additional diagnostic studies are also needed to aid clinicians in identifying patients at risk for therapeutic failure and selection of effective antibiotics. Finally, outpatient diagnostic and antimicrobial stewardship studies evaluating surrogate markers of improvement in UTI management should also evaluate patient outcomes.
In conclusion, in this large comparative effectiveness analysis of oral antibiotics for the treatment of outpatient uUTI in men a modestly higher risk of clinical failure with β-lactam and nitrofurantoin compared with fluoroquinolones was observed. Clinicians should carefully differentiate between complicated and uUTI and carefully select appropriate antibiotic treatment in male patients.
Summary points
•
Urinary tract infection (UTI) in men have been considered to be complicated due to increased risk for prostate infection which requires prolonged treatment with antibiotics that achieve high concentrations in prostate tissue or in systemic concentrations.
•
New complicated UTI treatment guidelines classify infection limited to the bladder as uncomplicated (uUTI) in men which can be treated with 7-day antibiotic courses.
•
These guidelines oral fluoroquinolones or trimethoprim/sulfamethoxazole (TMP/SMX) as preferred therapy with cephalosporins or amoxicillin/clavulanate as alternatives and avoidance of nitrofurantoin.
•
This study compared the effectiveness of commonly prescribed antibiotics for outpatient uUTI in men.
•
Commonly prescribed oral antibiotics nitrofurantoin, aminopenicillins, and cephalosporins, but not trimethoprim/sulfamethoxazole were associated with a higher UTI return visit rates than fluoroquinolones; although no meaningful differences in hospital admission were observed.
•
Short (5–7 day) treatment compared with longer (8–15 days) was not associated with worse outcome.
•
These findings generally support the new guideline recommendations for antibiotic selection and treatment duration in men.
Author contributions
K Madaras-Kelly: Conceptualization, obtaining funding, development of methods, data validation, initial draft of manuscript. J Boyd: Development of methods, data extraction, analysis, manuscript editing. L Bond: Development of methods, statistical analysis, manuscript editing
Acknowledgments
The findings and conclusions in this manuscript are those of the authors and do not necessarily represent the official position of the Department of Veterans Affairs.
Financial disclosure
This work was supported in part with resources and use of the Department of Veterans Affairs and was funded in part by an investigator-initiated research grant from BioMerieux, France (contract #E0358) to Idaho State University (Madaras-Kelly) with subcontracts awarded to the Idaho Veterans Research and Education Foundation (Boyd), and Boise State University (Bond). K Madaras-Kelly and L Bond also receive general support from the Institutional Development Awards (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under grants #P20GM103408 and #P20GM155898, and L Bond from the Biomolecular Research Center at Boise State, RRID: SCR_019174.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This research was determined as exempt by the VA Puget Sound Investigational Review Board and complied with all federal guidelines and Department of Veterans Affairs policies relative to human subjects research.
Data sharing statement
This manuscript reports the results of a real-world evidence study. The protocol was not publicly registered, and the data are not publicly available due to contractual restrictions. Select data and materials may be available from the authors upon reasonable request with the permission of Department of Veterans Affairs.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary data.docx)
- Download
- 6.12 MB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Gupta K, Hooton T, Naber K et al. Infectious Diseases Society of America; European Society for Microbiology and Infectious Diseases. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 52(5), e103–e120 (2011).
• Retired IDSA uncomplicated urinary tract infection (uUTI) guidelines that recommended nitrofurantoin as first line therapy for uUTI in women.
2.
Anon. Guidance document. Complicated urinary tract infections: developing drugs for treatment. Accessed 10 June 2024. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/complicated-urinary-tract-infections-developing-drugs-treatment
3.
D'Ancona C, Haylen B, Oelke M et al. Standardisation Steering Committee ICS and the ICS Working Group on Terminology for Male Lower Urinary Tract & Pelvic Floor Symptoms and Dysfunction. The International Continence Society (ICS) report on the terminology for adult male lower urinary tract and pelvic floor symptoms and dysfunction. Neurourol. Urodyn. 38(2), 433–477 (2019).
4.
Trautner B, Cortés-Penfield N, Gupta K et al. Clinical Practice Guideline by Infectious Diseases Society of America (IDSA): 2025 guideline on management and treatment of complicated urinary tract infections. Accessed 22 September 2025. https://www.idsociety.org/practice-guideline/complicated-urinary-tract-infections/
•• New IDSA practice guidelines for complicated urinary tract infection (UTI) that redefines complicated ad uUTI in men.
5.
Hooton T. Acute simple cystitis in men. Up to Date, 2023. Accessed 10 June 2024. https://www.uptodate.com/contents/acute-simple-cystits-in-men
6.
Hooton T, Gupta K. Acute complicated urinary tract infection (including pyelonephritis) in adults. Up to Date, 2023. (Accessed 10 June 2024). Available at: https://www.uptodate.com/contents/acute-complicated-urinary-tract-infection-including-pyelonephritis-in-adults
7.
Drekonja D, Trautner B, Amundson C, Kuskowski M, Johnson JR. Effect of 7 vs 14 days of antibiotic therapy on resolution of symptoms among afebrile men with urinary tract infection: a randomizedclinical trial. JAMA 326(4), 324–331 (2021).
• Randomized controlled trial of short course versus longer course therapy with fluoroquinolones and trimethoprim/sulfamethoxazole in afebrile men that demonstrated no difference in outcome.
8.
Kikuchi JY, Banaag A, Koehlmoos TP. Antibiotic prescribing patterns and guideline concordance for uncomplicated urinary tract infections among adult women in the US military health system. JAMA Netw. Open 5(8), e2225730 (2022).
9.
Langner JL, Chiang KF, Stafford RS. Current prescribing practices and guideline concordance for the treatment of uncomplicated urinary tract infections in women. Am. J. Obstet. Gynecol. 225(3), 272.e1–272.e11 (2021).
10.
Rovelsky SA, Vu M, Barrett AK et al. UTI Management Improvement Group. Outpatient treatment and clinical outcomes of bacteriuria in veterans: a retrospective cohort analysis. Antimicrob. Steward Healthcare Epidemiol. 2(1), e168 (2022).
• Chart review of 3255 culture-positive veterans that identified and unadjusted increased risk for clinical failure with nitrofurantoin and β-lactam therapy relative to the fluoroquinolones.
11.
Germanos G, Light P, Zoorob R et al. Validating use of electronic health data to identify patients with urinary tract infections in outpatient settings. Antibiotics (Basel) 9(9), 536 (2020).
12.
Fleming-Dutra KE, Hersh AL, Shapiro DJ et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010–2011. JAMA 315(17), 1864–1873 (2016).
13.
Madaras-Kelly KJ, Boyd JK, Bond L. The comparative effectiveness of telehealth versus primary care and collection of urine cultures on outcome in urinary tract infection. Medicine (Baltimore) 104(29), e43172 (2025).
• Retrospective cohort study of veterans utilizing similar criteria and methodology that identified the benefit of urine culture collection in patients with recent UTI antibiotic exposure.
14.
Søgaard KK, Thomsen RW, Schønheyder HC, Søgaard M. Positive predictive values of the International Classification of Diseases, 10th revision diagnoses of Gram-negative septicemia/sepsis and urosepsis for presence of Gram-negative bacteremia. Clin. Epidemiol. 7, 195–199 (2025).
15.
Fihn SD, Francis J, Clancy C et al. Insights from advanced analytics at the Veterans Health Administration. Health Aff. (Millwood) 33(7), 1203–1211 (2014).
16.
Glasheen WP, Cordier T, Gumpina R, Haugh G, Davis J, Renda A. Charlson Comorbidity Index: ICD-9 Update and ICD-10 translation. Am. Health Drug Benefits 12(4), 188–197 (2019).
17.
Hardin JW, Hilbe JM. Generalized estimating equations. CRC Press (2012). Accessed 7 June 2024. https://books.google.com/books?id=7QrSBQAAQBAJ
18.
Liang KY, Zeger SL. Longitudinal data analysis using generalized linear models. Biometrika 73(1), 13–22 (1986).
19.
Li F, Thomas LE, Li F. Addressing extreme propensity scores via the overlap weights. Am. J. Epidemiol. 188(1), 250–257 (2019).
20.
Thomas LE, Li F, Pencina MJ. Overlap weighting: a propensity score method that mimics attributes of a randomized clinical trial. JAMA 323(23), 2417–2418 (2020).
21.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav. Res. 46(3), 399–424 (2011).
22.
National Academies of Sciences, Engineering, and Medicine. Facilities staffing requirements for the Veterans Health Administration—resource planning and methodology for the future: interim report. The National Academies Press. Accessed 11 June 2024. https://nap.nationalacademies.org/read/25455/chapter/2
23.
Chen W, Qian L, Shi J. Franklin M comparing performance between log-binomial and robust Poisson regression models for estimating risk ratios under model misspecification. BMC Med. Res. Methodol. 18(1), 63 (2018).
24.
Zou G. A modified poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 159(7), 702–706 (2004).
25.
Chung WT, Chung KC. Key concepts in clinical epidemiology: the use of the E-value for sensitivity analysis. J. Clin. Epidemiol. 163, 92–94 (2023).
26.
R Core Team. R: A language and environment for statistical computing [Internet]. Vienna, Austria (2023). Accessed 7 June 2024. https://www.R-project.org/
27.
Posit team. RStudio: Integrated development environment for R [Internet]. Boston, MA (2023). Accessed 7 June 2024. http://www.posit.co/
28.
Wickham H, Averick M, Bryan J et al. Welcome to the tidyverse. J. Open Source Softw. 4(43), 1686 (2019).
29.
Halekoh U, Højsgaard S, Yan J. The R Package geepack for generalized estimating equations. J. Stat. Softw. 15(2), 1–11 (2006).
30.
Greifer N. Cobalt: covariate balance tables and plots. (2023). Accessed 7 June 2024. https://CRAN.R-project.org/package=cobalt
31.
Sjoberg DD, Whiting K, Curry M et al. Reproducible summary tables with the gtsummary package. R J. 13(1), 570–580 (2021).
32.
Iannone R, Cheng J, Schloerke B et al. gt: easily create presentation-ready display tables. (2023). Accessed 7 June 2024. https://CRAN.R-project.org/package=gt
33.
Schauberger P, Walker A. _openxlsx: Read, Write, and Edit xlsx Files. (2024). R package version 4.2.7. Accessed 15 September 2025. https://CRAN-R-project.org/package=openxlsx
34.
Azar N, Khodor M, Choucair J et al. Susceptibility of urinary Enterobacteriaceae to selected antimicrobials in an out-patient setting in Wallonia-Belgium: retrospective analysis over 5 years period (2018–2022). Ann. Biol. Clin. (Paris) 81(1), 52–60 (2023).
35.
Bajema K, Strymish J, Jones M et al. P-848. Antibiotic prescribing in VA Healthcare System emergency departments and urgent care centers – a medication use evaluation. Open Forum Infect. Dis. 13(Suppl. 1), ofaf695.1056 (2026).
36.
Platteel TN, Beets MT, Teeuwissen HA et al. Nitrofurantoin failure in males with an uncomplicated urinary tract infection: a primary care observational cohort study. Br. J. Gen. Pract. 73(728), e204–e210 (2023).
• Observational cohort study conducted in Europe that identified and increased risk for failure with nitrofurantoin and β-lactams.
37.
Madaras-Kelly KJ, Nakasone T, Maghari S et al. A pilot intervention to improve the management of urinary tract infections in outpatient settings. Antimicrob. Steward Healthcare Epidemiol. 5(1), e338 (2025).
38.
Reissier S, Penven M, Amara M et al. Bacterial epidemiology and antibiotic resistance rates in male urinary tract infections in France, 2019–2023. Infect. Dis. Now 55(7), 105123 (2025).
39.
Soudais B, Ribeaucoup F, Schuers M. Guidelines for the management of male urinary tract infections in primary care: a lack of international consensus-a systematic review of the literature. Fam. Pract. 40(1), 152–175 (2023).
40.
Bilsen MP, Jongeneel RMH, Schneeberger C et al. Definitions of urinary tract infection in current research: a systematic review. Open Forum Infect. Dis. 10(7), ofad332 (2023).
41.
Lafaurie M, Chevret S, Fontaine JP et al. Antimicrobial for 7 or 14 days for febrile urinary tract infection in men: a multicenter noninferiority double-blind, placebo-controlled, randomized clinical trial. Clin. Infect. Dis. 76(12), 2154–2162 (2023).
• Randomized multicentered study of short versus longer duration of therapy in febrile men that identified benefit of longer duration of therapy.
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 9 October 2025
Accepted: 13 February 2026
Published online: 26 March 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative effectiveness of oral antibiotics to treat uncomplicated urinary tract infections in male outpatients. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0163
Export citation
Select the citation format you wish to export for this article or chapter.