Real-word evidence on healthcare resource use and associated costs in on-demand users of replacement therapies in von Willebrand disease in France: the FORvWARD study
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: Real-world data about use of Von Willebrand factor (VWF) concentrates to manage on-demand patients with Von Willebrand disease (VWD) are scarce. Aim: To describe and compare patients' characteristics, treatment patterns, healthcare resource use and associated costs of patients with VWD using VWF concentrates. Materials & methods: Using the French healthcare claims database, we included adult patients with ≥1 reimbursement for a replacement therapy (RT) containing VWF concentrate between 1 January 2017 and 30 September 2021 and followed them from first RT dispensation to 31 December 2021. Treatment patterns, healthcare resource use and associated costs of RT on-demand users were evaluated over each 30-days exposure period (EP) starting the first day of each hospital stay with ≥1 RT administration. In- and out-hospital RT doses and FVIII, number of general practitioner and nurse visits, in- and out-hospital RT dispensings and length of hospitalizations and their costs were described and compared across RTs using adjusted Generalized Estimating Equation models accounting for confounding factors. Results: Among 2540 on-demand RT users, WILFACTIN® was the main RT used, followed by VONCENTO®, VEYVONDI®, EQWILATE® and WILSTART®. Overall, the mean total RT dose was 12,962 IU and the mean cost was €21,034/EP. Compared with VEYVONDI®-treated EP, WILFACTIN®-treated EP had significantly longer stay duration, had more out-hospital RT dose and had higher overall and in-hospital costs; VONCENTO®-treated EP had more overall and in-hospital RT dose, and had higher in-hospital and RT-related costs. Conclusion: This first real-world study suggests that VEYVONDI® seems to be a cost-saving RT compared with other RT. Future studies including clinical data should provide further evidence.
Plain language summary
What is this article about?
Von Willebrand disease (VWD) is a rare genetic disorder caused by missing or defective Von Willebrand factors (VWF), leading to increased bleeding risk. The disease presents various severity forms, from type 1 to 3, i.e., from absent or mild symptoms to severe and spontaneous bleedings episodes. VWD therapeutic management varies widely with disease severity, from abstaining therapy to complex treatments including replacement therapies (RT) containing Von Willebrand factor (VWF). They can be used on-demand (most cases) or in prophylaxis. They are delivered intravenously at hospital (in-hospital use) or dispensed through the hospital pharmacy for home use (i.e., out-hospital use).
Including patients between 2017 and 2021, the FORvWARD study describes real-life use of VWF concentrates in VWD patients treated on-demand, i.e., for acute bleeding events or prior to invasive medical act such asa surgery. It describes and compares the healthcare consumption and costs associated to the use of the five RT available in France to date: WILFACTIN®, VONCENTO®, EQWILATE®, WILSTART® and VEYVONDI®. Costs analyzed covered RT medications (in- and out-hospital), hospitalizations, general practitioner and nurse visits. The study used the data from the French national healthcare claims database.
What were the results?
Main results show that fewer RT doses were used in patients treated with VEYVONDI® than with WILFACTIN® or VONCENTO®. They also show that the overall costs were lower for patients treated with VEYVONDI®, compared with those treated with WILFACTIN® or VONCENTO®.
What do the results mean?
Future studies are needed to better account for clinical data, which were not all available in the database used in this study.
Von Willebrand Disease (VWD) varies from type 1 to 3, i.e., from absent or mild symptoms to severe and spontaneous bleedings episodes, potentially into joints, muscles or mucous membranes [1]. VWD therapeutic management varies widely according to disease severity [1–3], including replacement therapies (RT) containing Von Willebrand Factor (VWF) with (dual concentrates) or without Factor VIII (FVIII) (pure concentrates). They can be used either on-demand (most cases) or in prophylaxis. When they are used on-demand (the focus of this paper), they intend to treat acute bleeding events or to prevent them in prevision of an invasive medical procedure, e.g., surgery, whereas when they are used in prophylaxis, they are dispensed permanently to prevent severe and/or recurrent bleeding events.
In France, five medications are available to treat on-demand VWD patients: plasma-derived (pd) combinations of VWF with varying quantities of FVIII: pdVWF/pdFVIII, ratio 2.4:1 (VONCENTO®), pdVWF/pdFVIII, ratio 1 (EQWILATE®), pdVWF/pdFVIII, ratio 1 (WILSTART®) and medications containing only VWF or neglectable quantity of FVIII: either pdVWF with low FVIII (WILFACTIN®) or the recombinant VWF (rVWF) VEYVONDI®. They are all currently indicated on-demand (for patients aged 18 or over only for VEYVONDI®) when treatment with desmopressin alone is ineffective or not indicated, for the treatment of bleedings and surgical bleedings, or in prevention of surgical bleeding [1]. They are delivered intravenously at hospitals (in-hospital use) or dispensed through the hospital pharmacy for use at home (i.e., out-hospital use). To date, there is no clinical trial comparing the efficacy of the various RT: in France, Health Technology Assessment considers their clinical benefits as similar [4]. Various international or regional guidelines about VWD monitoring exist [1–3,5], but the choice of VWF concentrates remains challenging and heterogeneous across centers and clinicians [6,7] because no data exist about VWD management using various RT, by indication (i.e., surgery or bleeding event).
In the field of VWD, real-world evidence mainly concerns safety and efficacy and focus on one specific concentrate [8–13]. Furthermore, despite the economic burden associated to the management of VWD and especially to the cost of VWF concentrates, little is known about the associated costs and the healthcare resource use (HCRU) associated to each of them and how it differentiates across RT [14,15].
In this context, the main aim of the present study was to describe characteristics of French adult patients with VWD using on-demand VWF concentrates, their treatment patterns, HCRU and associated costs. The secondary objective was to compare HCRU and associated costs across various RT.
Materials & methods
Data source
This retrospective cohort study was based on the French National Health System (NHS) claims database (Système National des Données de Santé [SNDS]) [16]. It contains anonymous individual information on sociodemographic characteristics, all nonhospital reimbursed healthcare costs (without corresponding medical diagnoses), and all hospital discharge summaries (ICD10-code-based). The SNDS does not provide direct information on behavioral or clinical baseline characteristics (tobacco smoking, body mass index, etc.), nor laboratory results, information on drug dispensed during a hospital stay (except for specific costly medications, such as coagulation factors), or data on cause of death. This claims database currently covers more than 98% of the population of France [16].
Study population
We included all patients identified in the SNDS with an in- or out-hospital dispensing of a VWF concentrate with or without additional FVIII between 1 January 2017 and 30 September 2021, i.e., the inclusion period. RT considered included WILFACTIN®, WILSTART®, VONCENTO®, EQWILATE® and VEYVONDI®. The date of the first in-hospital dispensing of any of them during the inclusion period was defined as the index date. To avoid including patients with hemophilia, we excluded patients with only hemophilia codes without any ICD-10 VWD diagnosis code (i.e., D68.0) related to hospitalizations or long-term disease status (i.e., full cares coverage in case of costly chronic condition) found during the study period (1 January 2017 to 31 December 2021) or in the three preceding years. We followed up patients from index date until death, last patient health record, or end of the study period.
In the absence of indication for drug prescription and clinical data in the database, an algorithm was developed to distinguish on-demand and prophylaxis RT users within the SNDS database. Specifically, prophylaxis RT users were identified as the patients with at least 1 year of follow-up, and at least one out-hospital RT dispensing, and at least 80% of days covered by RT, and all the other patients were considered ad occasional users (Figure 1).In the present study, we analyzed patients aged 18 years or more identified as on-demand RT users who received RT dispensing during a hospitalization (Figure 2).
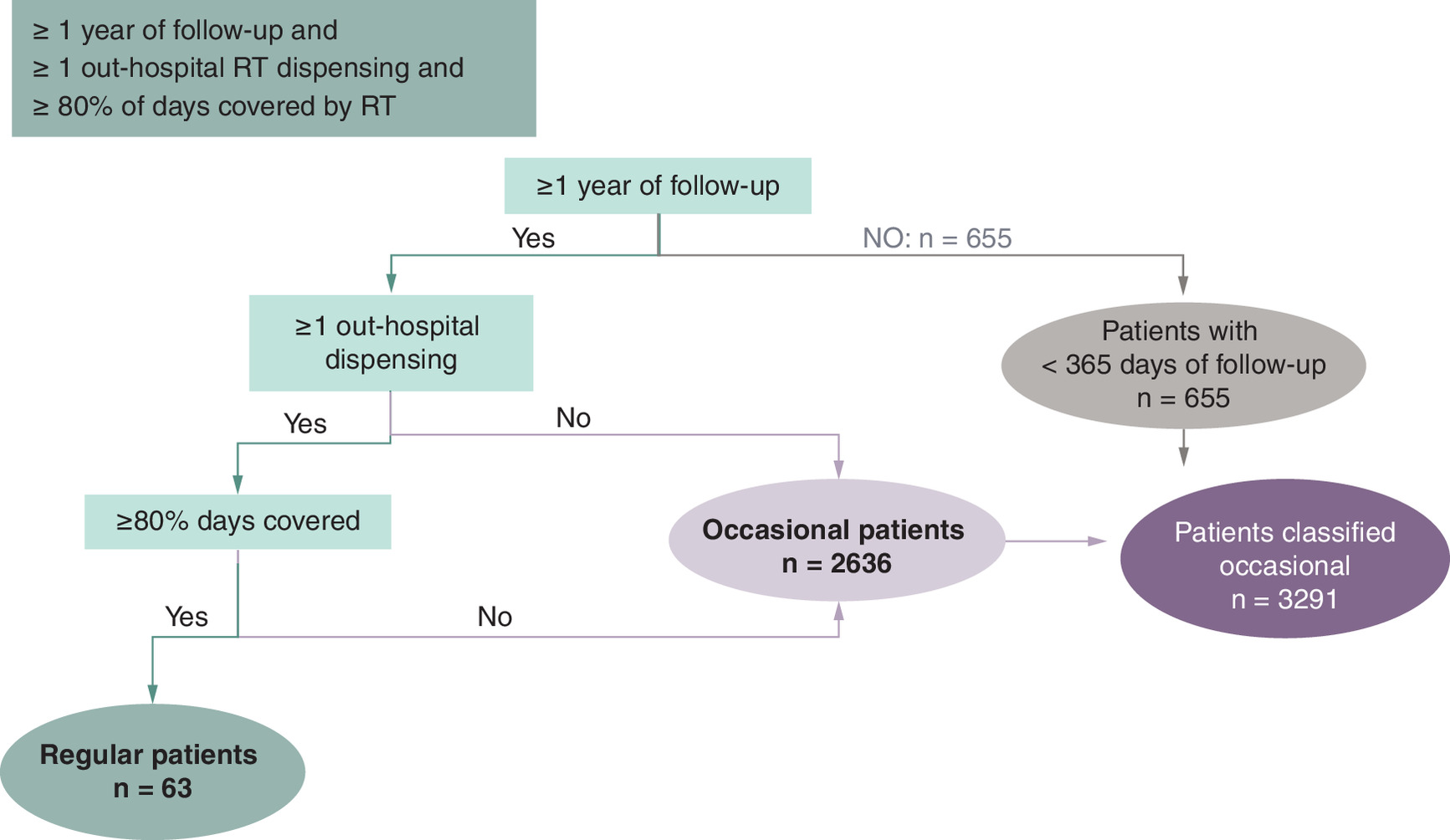
Figure 1. Algorithm used to identify on-demand versus in prophylaxis replacement therapy users in the SNDS database.
RT: Replacement therapy.
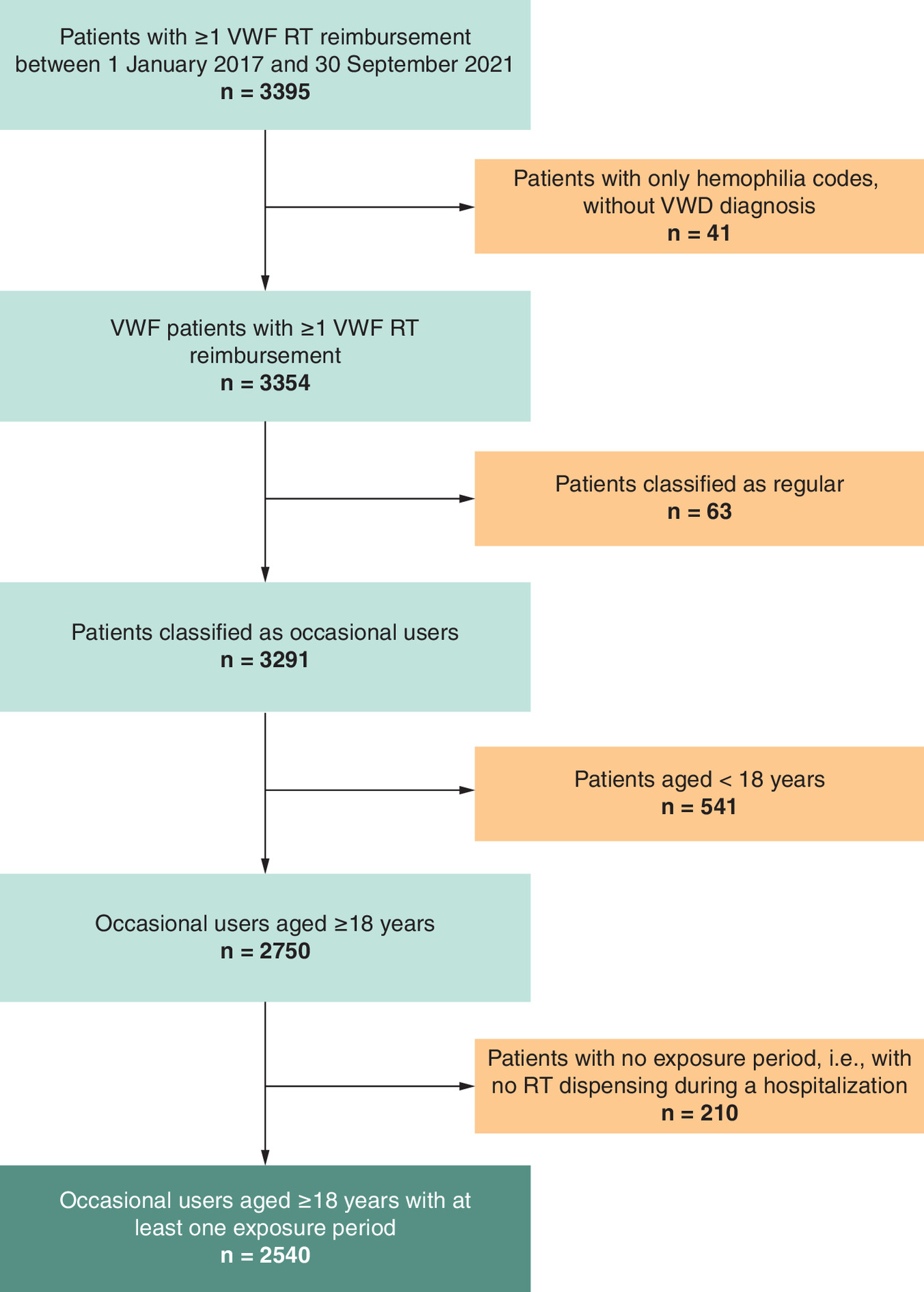
Figure 2. Flowchart of the study population.
RT: Replacement therapy; VWD: Von Willebrand disease; VWF: Von Willebrand factor.
Exposure periods & variables
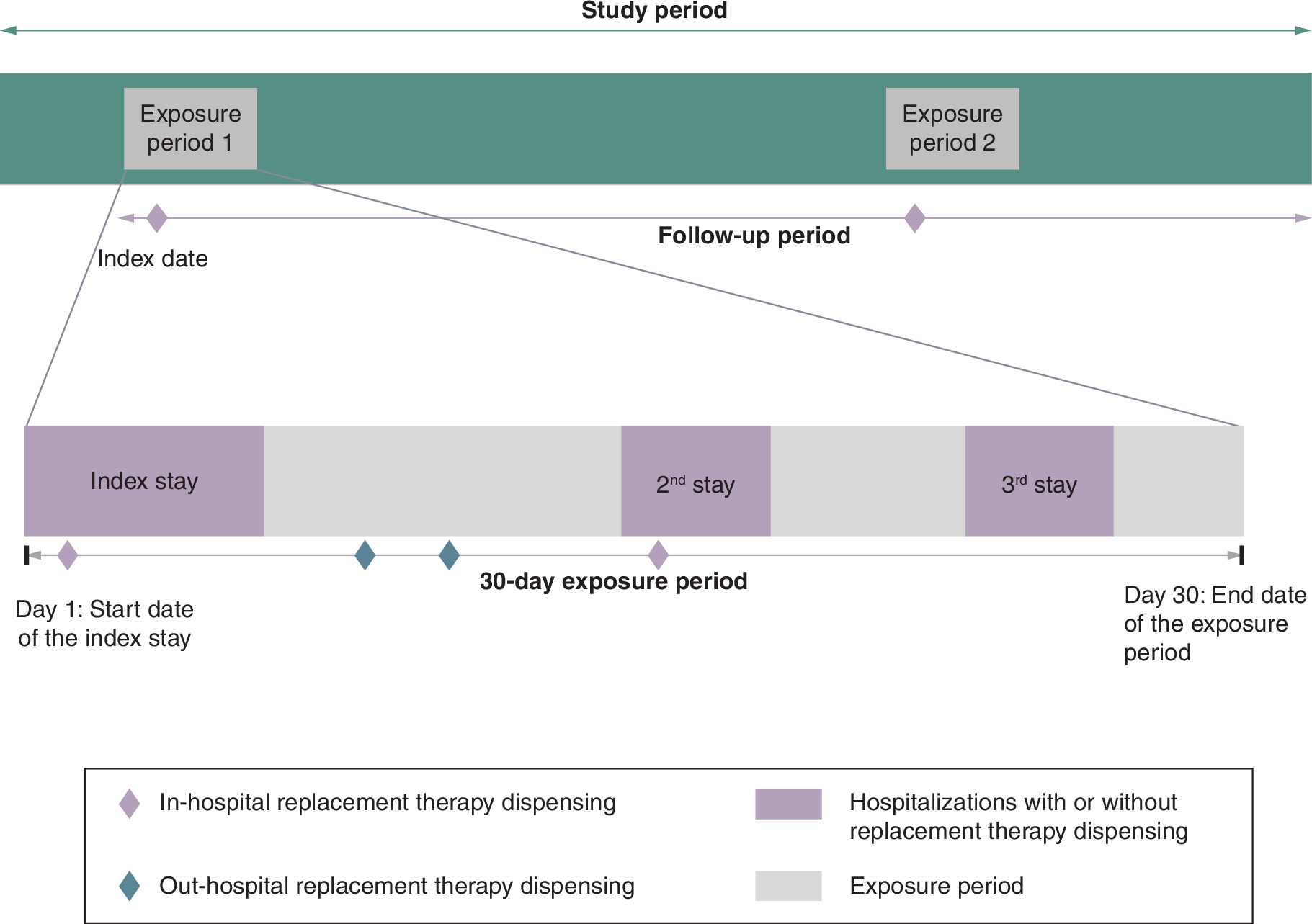
To assess HCRU and costs, we defined an exposure period (EP) as the period of 30 days starting on the first day of each hospitalization during which the RT was dispensed: the stay during which the RT was first dispensed was defined as the index hospitalization of the EP, even if other stays (i.e., not index) may have occurred during the EP (Figure 3). EPs during which multiple RT were dispensed were excluded. The 30-days duration was considered as the most relevant period to assess HCRU associated to the RT dispensing, HCRU occurring later being probably not linked to the event which led to the hospitalization.
Within the overall study population, we analyzed on-demand users sociodemographic characteristics, presence of comorbidities and Charlson Comorbidity Index at index date [17]. Within the study population having at least one EP, we described the number of EPs by patient over the follow-up period, and the proxy of the indication associated to the index stay by RT among bleeding, surgery or others, based on the main or related diagnosis or act-specific codes coded for the stay. In case where both bleeding and surgery codes were recorded for the same stay, bleeding was assumed to be a consequence of the surgery, and the indication ‘surgery’ was assigned to the stay. HCRU was analyzed using the EPs as the statistical unit. Consequently, HCRU of one given patient may be analyzed within several distinct EPs over the follow-up. The following HCRU variables and their associated costs were analyzed: number of general practitioner (GP) and nurse visits, index stay duration, number of RT dispensings and amount of in- and out- hospital RT units (in IU) and FVIII. Costs associated to these HCRU added to the costs of potential other hospitalizations during the EP were analyzed from a NHS perspective (i.e., the actual costs reimbursed by the NHS). In France, the price of VWF units is similar across various RT medications available.
Statistical analyses
All analyses were performed using SAS (SAS Institute, NC, USA), Version 9.4.
We provided descriptive statistics of patients' characteristics (number and relative percentages of patients by category of qualitative variables), and the mean, standard deviation (SD) of the number of EPs by patient, as well as of the number of cares and RT IU consumed over the EP and associated costs with their detailed distribution (Q1, Q3 and median). The reference year used for cost analysis was year 2021. All analyses were performed by EP, overall and by type of RT (WILFACTIN®, WILSTART®, VONCENTO®, EQWILATE® and VEYVONDI®).
To describe and compare HCRU and costs across RT, EPs in which only WILSTART® was identified were excluded, given this RT is indicated only for initial phases of treatment) [18]. We used Generalized Estimating models (GEE) to compare the mean number of cares, RT units and associated costs across RT, considering VEYVONDI® as the reference. Because patients could have more than one EP and to account for intra-patient correlation, GEE with a log link Negative Binomial or Poisson distribution and first-order autoregressive correlation matrix were used to estimate the rate ratio (RR) and the associated 95% confidence interval (CI95) of HCRU. As zero-inflated models are not supported within the GEE framework, standard Poisson or negative binomial GEE models were used instead. Overdispersion diagnostics based on the Pearson chi-square to degrees-of-freedom ratio guided the choice between Poisson and negative binomial distributions. GEE with a log link Gamma distribution and first-order autoregressive correlation matrix were used to estimate costs ratio (CR) and doses ratio (DR) and the associated CI95. This choice was based on empirical assessment of model fit for nonnormally distributed outcomes. The following confounding factors were considered in the GEE comparisons: age at index date, gender, geographical area, index stay duration (except for the comparison of stay duration), indication of the stay and the rank of the EP studied over the corresponding patient’s follow-up.
We conducted the same descriptive and comparative analyses, restricting the EPs to those with an indication of bleeding or surgery.
Results
A total of 2750 occasional RT users with VWD aged ≥18 years were identified (Table 1). Their mean age at index date was 51.2 +/- 18.7 years and 57.5% were females. There were no noticeable differences in patients' characteristics across RT used over the follow-up (Table 1). Among occasional users, 2540 patients had at least one EP, totalizing 4210 EPs, with a mean of 1.7 EPs per patient over the study period (Figure 2 & Table 2). WILFACTIN® was the RT used in more than three quarters of the EPs (n = 3250, 77.2%), followed by VONCENTO® (n = 472, 11.2%), VEYVONDI (n = 356, 8.5%), EQWILATE® (n = 55, 1.3%) and WILSTART® (n = 77, 1.8%). Supplementary figure 4 presents the switches between RT over the follow-up. The indication of the index hospitalization was mainly surgery (72.2%).
| Overall | VEYVONDI | WILFACTIN | VONCENTO | EQWILATE | WILSTART | |
|---|---|---|---|---|---|---|
| Patients, n (%) | 2750 (100.0%) | 159 (5.8%) | 2199 (80.0%) | 304 (11.0%) | 22 (0.8%) | 66 (2.4%) |
| Mean follow-up duration, years (SD) | 2.6 (1.5) | 1.2 (0.6) | 2.7 (1.5) | 2.8 (1.4) | 1.0 (0.6) | 3.3 (1.4) |
| Mean age, years (SD) | 51.2 (18.7) | 48.6 (17.7) | 51.5 (18.6) | 49.9 (19.2) | 50.3 (20.9) | 53.0 (19.9) |
| Females, % | 57.5% | 57.2% | 57.9% | 58.6% | 59.1% | 40.9% |
| Comorbidities, n (%) | ||||||
| Charlson Comorbidities Index, mean (SD) | 1.8 (2.0) | 1.4 (1.5) | 1.8 (2.1) | 1.5 (2.0) | 1.7 (1.7) | 1.9 (1.9) |
| Cardiovascular diseases | 552 (20.1%) | 19 (11.9%) | 484 (22.0%) | 39 (12.8%) | 0 | 10 (15.2%) |
| Mental illness | 445 (16.2%) | 15 (9.4%) | 379 (17.2%) | 40 (13.2%) | 3 (13.6%) | 8 (12.1%) |
| Cancer | 490 (17.8%) | 32 (20.1%) | 390 (17.7%) | 47 (15.5%) | 3 (13.6%) | 18 (27.3%) |
| Diabetes (types 1 and 2) | 213 (7.7%) | 12 (7.5%) | 183 (8.3%) | 11 (3.6%) | 0 | 7 (10.6%) |
SD: Standard deviation.
| Overall | VEYVONDI | WILFACTIN | VONCENTO | EQWILATE | WILSTART | |
|---|---|---|---|---|---|---|
| Exposure periods | ||||||
| Patients, n (%)† | 2540 (100%) | 252 (9.2%) | 2072 (75.3%) | 327 (11.9%) | 46 (1.7%) | 57 (2.1%) |
| EP, n (%) | 4210 (100%) | 356 (8.5%) | 3250 (77.2%) | 472 (11.2%) | 55 (1.3%) | 77 (1.8%) |
| EP/patient, n, mean (SD) | 1.7 (1.3) | 1.4 (0.8) | 1.6 (1.3) | 1.4 (0.9) | 1.2 (0.7) | 1.4 (0.9) |
| Indication of the index stay‡, n (%) | ||||||
| Surgery | 3038 (72.2%) | 243 (68.3%) | 2402 (73.9%) | 320 (67.8%) | 35 (63.6%) | 38 (49.4%) |
| Bleeding | 449 (10.7%) | 29 (8.1%) | 332 (10.2%) | 63 (13.3%) | 9 (16.4%) | 16 (20.8%) |
| Other | 723 (17.2%) | 84 (23.6%) | 516 (15.9%) | 89 (18.9%) | 11 (20.0%) | 23 (29.9%) |
†
Patients with at least one exposure period.
‡
Corresponds to the indication associated to the index stay, i.e., ICD-10 codes and surgery acts codes related to the index stay were reviewed to classify the index stay as a stay for bleeding, for surgery or for any other reason.
EP: Exposure period; SD: Standard deviation.
To perform the HCRU analysis, we excluded 77 periods in which only WILSTART® was used, resulting in 4,133 EPs of 2,505 patients to be compared. All RT combined, GP visits occurred in 40.6% of the EPs, and nurse visits in 45.1%. The mean index stay duration was 7.4 days and the mean number of RT dispensations by EP was 2.5. Overall, the mean dose of RT was 12,962 IU including both in- (mean dose was 10,666 IU) and out-hospital dispensings. Out-hospital RT dispensings occurred in 16.3% of the EPs, with a mean dose of 14,100 IU, all RT combined. Comedications with FVIII were identified with WILFACTIN® and VEYVONDI® in 14.3% and 21.6% of the EPs, respectively, mainly in-hospital. The mean total dose of FVIII used was 4,269 IU in WILFACTIN®-treated EP and 2,955 IU in VEYVONDI®-treated EP (Figure 4). The mean cost associated to one EP was €21,034 overall, mainly driven by in-hospital costs (€18,675). Within this cost, that of VWF concentrates represented 61% (i.e., €12,832). Detailed results by RT are presented in Figure 5 & Supplementary Table 1 (detailed distribution).
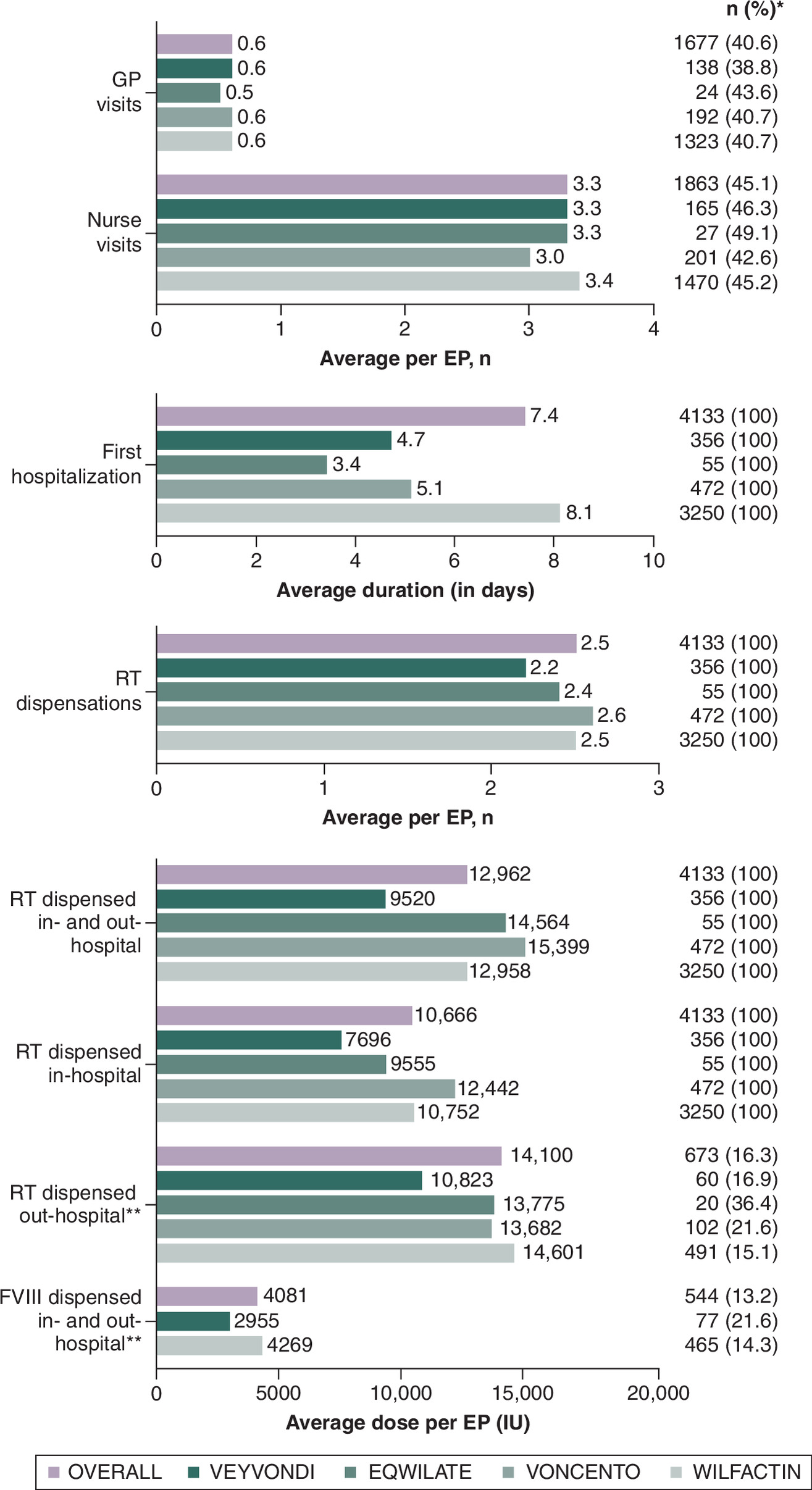
Figure 4. Description of mean healthcare resource use by exposure period, by replacement therapy.
*Number and percentage of EP with at least one reimbursement for the mentioned care.
**Among users (i.e., EP with at least one reimbursement for the mentioned care).
EP: Exposure period; FVIII: Factor VIII; GP: General practioner; RT: Replacement therapy.
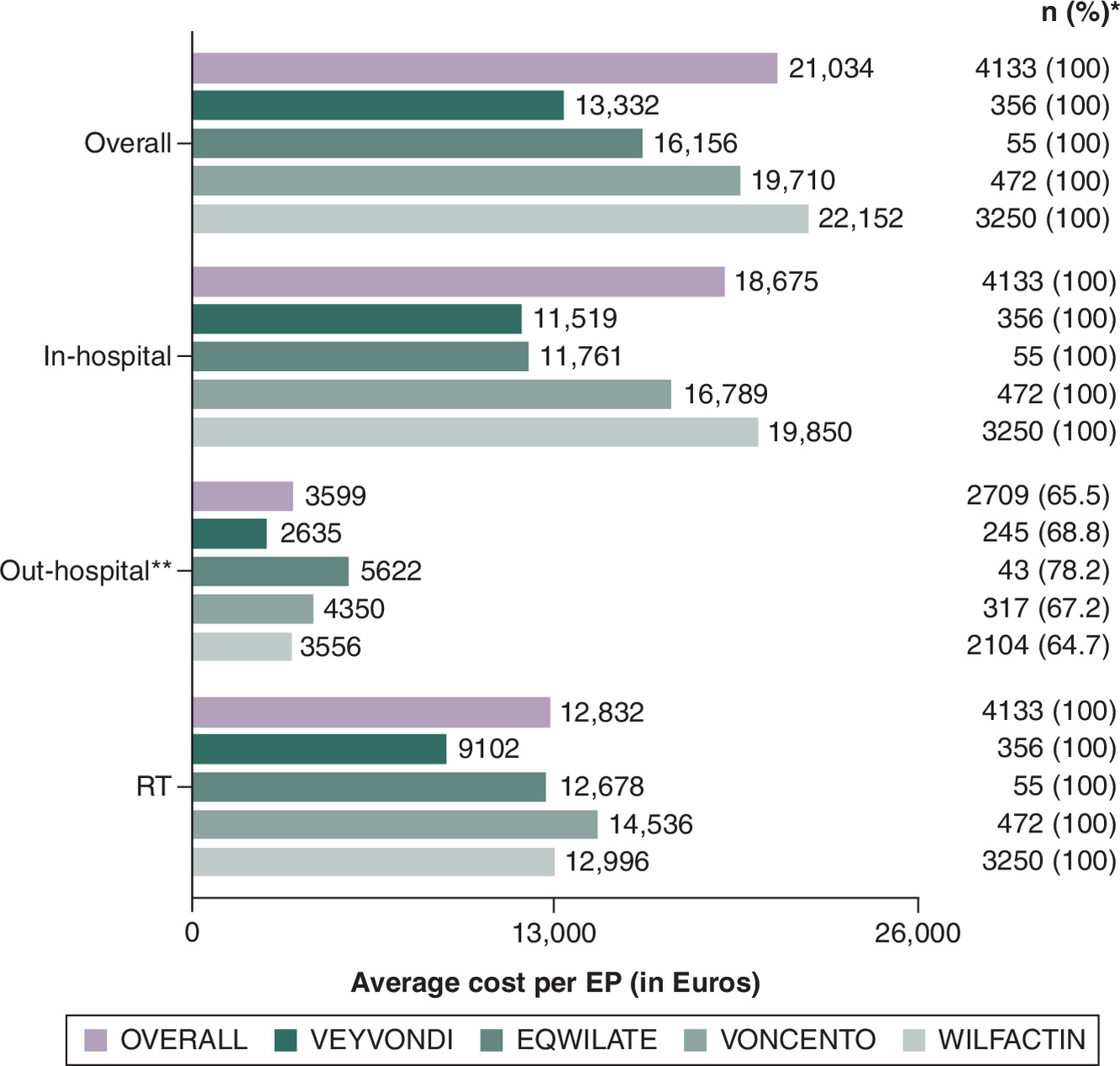
Figure 5. Description of mean costs associated to healthcare resource use by exposure period, by replacement therapy.
*Number and percentage of EP with at least one reimbursement for the mentioned care.
**Among users (i.e., EP with at least one reimbursement for the mentioned care).
EP: Exposure period; RT: Replacement therapy.
When comparing HCRU (Figure 6), we found that the duration of the index stay was significantly longer in WILFACTIN®-treated EPs than in VEYVONDI®-treated EPs (respectively, 8.1 and 4.7 days, RR = 1.39, CI95%: 1.18–1.63), whereas it was significantly lower in EQWILATE®-treated EPs than in VEYVONDI®-treated EPs (respectively, 3.4 and 4.7 days, RR = 0.67, CI95%: 0.53–0.85). Significantly more RT IU were dispensed in- and out-hospital within VONCENTO®-treated EPs than within VEYVONDI®-treated EPs (respectively, 15,399 IU and 9520.0 IU, DR = 1.28, CI95%: 1.06–1.54), and significantly more RT IU were also dispensed out- and in-hospital separately. Similarly, significantly more RT doses were dispensed out-hospital within WILFACTIN®-treated EPs than within VEYVONDI®-treated EPs (respectively, 14,601 IU and 10,823 IU, DR = 1.54, CI95%: 1.12–2.12).
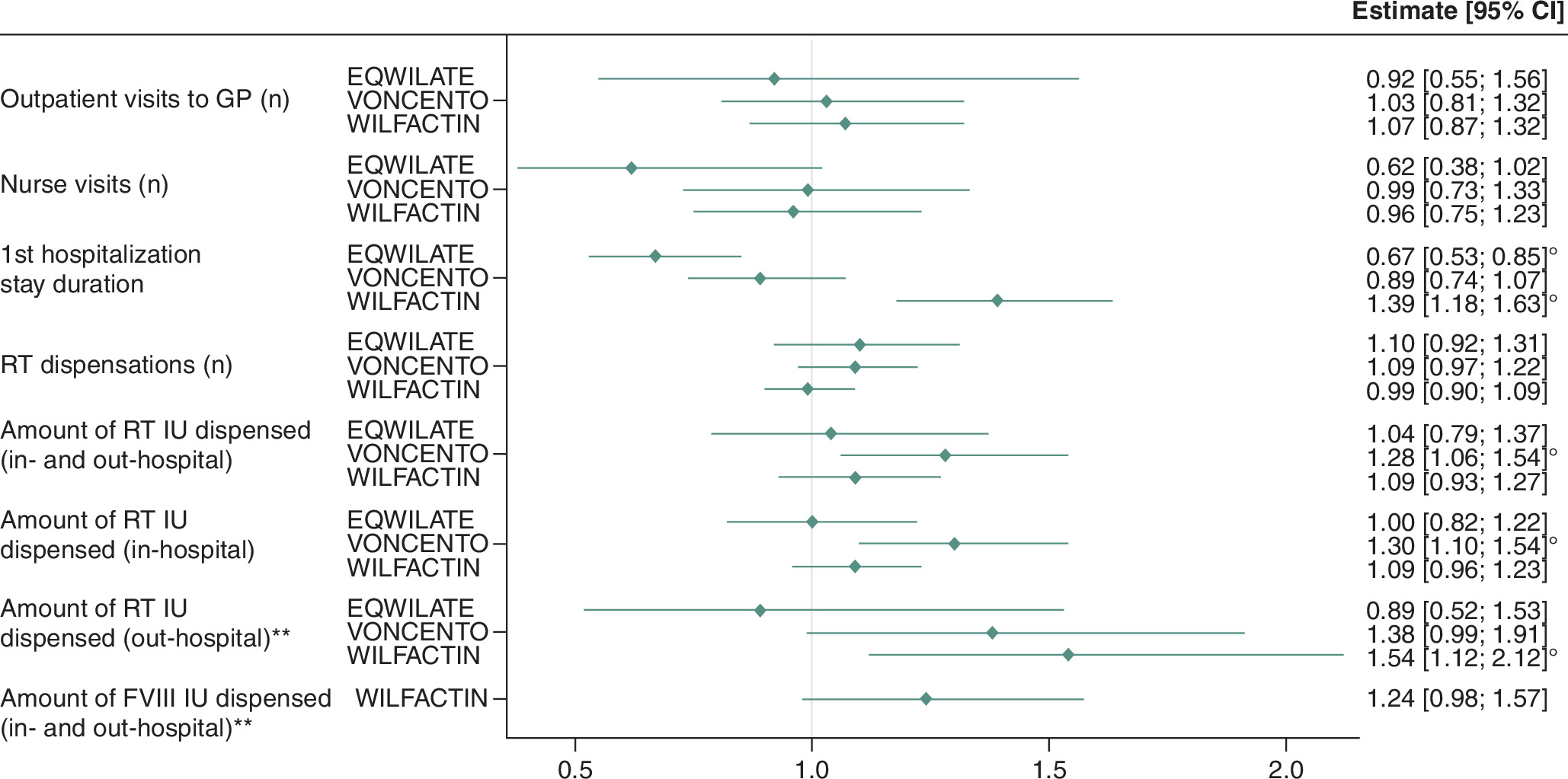
Figure 6. Comparison of mean healthcare resource used by exposure period across replacement therapies (exposure periods treated with VEYVONDI as a reference).
Models were adjusted on age, gender, geographical area, duration of the index stay (except for the comparison of stay duration), indication of the stay and history of RT exposure.
**Among users, i.e., in patients with at least one of the mentionned care.
CI: Confidence interval; EP: Exposure period; FVIII: Factor VIII; GP: General practioner; RT: Replacement therapy.
The mean costs associated to the use of VONCENTO® (€19,710; SD: 42,281) and WILFACTIN® (€22,152: SD: 34,405) were significantly higher than that of VEYVONDI® (€13,332, SD: 18,154) (respective CR of 1.21 [1.04–1.41] and 1.27 [1.13–1.42]), as were the in-hospital costs of €16,789 (SD: 38,949) for VONCENTO®-treated EPs, €19,850 (SD: 33,194) for WILFACTIN®-treated EPs, compared with €11,519 (SD: 16,367) for VEYVONDI®-treated EPs (respective CR: 1.19 [1.03–1.38] and 1.24 [1.11–1.39]) (Figure 7). The RT-related cost was significantly higher in VONCENTO®-treated EPs (€14,536, SD: 26,590) compared with VEYVONDI®-treated EPs (€9102, SD: 13,503) (CR = 1.29, CI95%: 1.07–1.55).
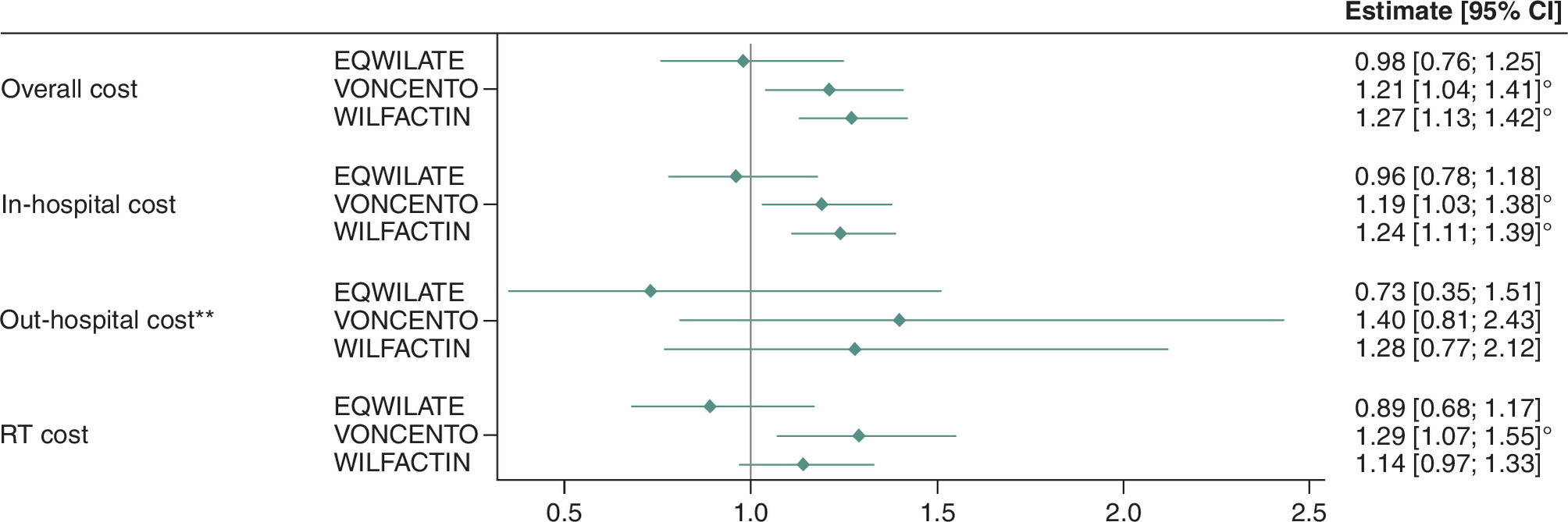
Figure 7. Comparison of mean costs associated with healthcare resource used by exposure period across replacement therapies (exposure periods treated with VEYVONDI as a reference).
**Among users, i.e., in patients with at least one of the mentionned care.
CI: Confidence interval; RT: Replacement therapy.
Among the 4133 EPs, 3433 were related to a surgery (n = 3000) or a bleeding event (n = 433). When restricting the HCRU and the cost analysis to those periods, the results were similar to the main analysis in terms of stay duration, RT dose dispensed and FVIII dispensation (Supplementary Table 2 & Supplementary Figure 3). The only differences observed concerned the amount of FVIII dispensed within WILFACTIN®-treated EPs (4503 IU) being significantly higher than in VEYVONDI®-treated EPs (2938 IU) (DR = 1.29, CI95%: 1.03–1.62), and the out-hospital cost being higher in VONCENTO®-treated EPs (€4954) than in VEYVONDI®-treated EPs (€2665) (CR = 1.83, CI95%: 1.08–3.12).
Discussion
Key findings
Our results provide detailed information about patients with VWD treated on-demand with VWF concentrates in France, their HCRU and associated costs. The most frequently used RT was WILFACTIN (77.2% of EP), and in most cases (72.2%), concentrates were used in the context of a surgery, in agreement with their labels. Over the 30 days following the index stay start, the patients consumed a total mean dose of 12,962 IU. By definition, each EP included in-hospital RT dispensing corresponding to 82% (mean = 10,666 IU) of the dose dispensed during the EP, while only 16% of the EP included out-hospital dispensings. FVIII was co-dispensed in 14.3% of the WILFACTIN®- and in 21.6% of the VEYVONDI®-treated EPs. The EP mean cost was €21,034 overall, driven by in-hospital costs (€18,675). After adjustment, the mean stay duration was shorter in VEYVONDI®-treated EPs (4.7 days) than in WILFACTIN®-treated EPs (8.1 days), but longer in EQWILATE-treated EPs (3.4 days). We also showed that compared with VEYVONDI-treated EPs, more RT doses were dispensed in VONCENTO®-treated EPs, and more RT doses were dispensed out-hospital in WILFACTIN®-treated EPs. Finally, overall and in-hospital costs of VONCENTO- and WILFACTIN®-treated EPs were higher than VEYVONDI®-treated EPs.
Most of the EPs used WILFACTIN. It was the first VWF concentrate to be launched in France, explaining the longer follow-up duration of WILFACTIN-treated patients (compared with patients treated with VEYVONDI or EQWILATE, both launched in 2018–2019). However, as the unit of analysis was the 30-day EP, the follow-up duration does not impact result interpretation. The shorter stay duration observed in VEYVONDI-treated EPs compared with WILFACTIN®-treated EPs may be explained by the presence of residual confounding related to clinical variables not available in the SNDS, which may reflect a potential channeling bias: VEYVONDI®, as the most recent RT launched in France, may tend to be prescribed to less comorbid patients. This is supported by the lower Charlson Comorbidity Index and the fewer presence of main comorbidities in patients treated with VEYVONDI®, although this was not statistically tested.
Comparison to existing studies
To our knowledge, this is the first European real-world study describing VWD patients' characteristics, RT management, and comparing HCRU and costs in real-life setting. Few other US studies based on claims data described HCRU and costs associated with VWD management. Thus, Swallow et al. described the number and duration of hospital stays, emergency department and outpatient visits of 396 patients with VWD over a 6-month period [19]. Oladapo et al. showed that the 12-months HCRU and associated costs of 2972 patients with VWD following major surgery were significantly higher than those of patients without VWD [20]. Lu et al. described the number of bleeding events over a median follow-up of 4 years in 19,785 patients, and compared associated costs to VWD patients without bleeding events [21]. However, none of these studies compared HCRU and costs associated to the use of various VWF concentrates. In France, some real-life studies described efficacy, safety and treatment patterns of VONCENTO® [22,23] and WILFACTIN® [11] based on observational data, but corresponding HCRU and costs were not reported. The BERLINGHO study also described the treatment patterns of various VWF concentrates in 153 hospitalized patients, showing that VWF concentrates use is influenced by basal levels of VWF and FVIII, by VWD type and by cause of hospitalization [14].
Strengths & limitations
Based on the French healthcare claims database representative and exhaustive to the French population, this study included almost all French patients treated with VWF concentrates. This allows to provide a robust and detailed description of this patients’ population, their treatment patterns, HCRU and costs, as well as to estimate the number of patients with Von Willebrand disease needing VWF concentrates in France. Our results are coherent with the VWD 3306 patients included in the French FranceCoag registry in December 2020 [24]. Despite different inclusion criteria, our patients’ characteristics are similar to those of registry’s patients: 80.6% of adult patients and 57.7% of females. However, our study population was limited to patients with a hospitalization with a dispensation of RT, which is not the case of all patients included in the registry.
The algorithm used to classify patients either as on-demand or as using prophylaxis has been developed with the study authors following a detailed exploration phase of all the variables available [25]. However, we may have considered patients as on-demand whereas they were actually using prophylaxis, as the algorithm was based on at least 1 year of follow-up availability for patients to be classified as using prophylaxis. Consequently, patients with less than 1 year of follow-up (n = 655) have automatically been classified as on-demand users of RT, while they may be using RT in prophylaxis. However, the proportion of patients identified as using prophylaxis was similar to expected, and a sensitivity analysis with a minimum follow-up time of 6 months instead of 1 year showed that only three additional patients would have been classified as prophylaxis users (data not shown). In addition, a differential inclusion bias cannot be excluded, as only WILFACTIN® was indicated in prophylaxis at these dates.
The GEE models used for HCRU and costs comparisons allowed to provide reliable results, as they account for major available cofounding factors and intra-patient correlation, i.e., the fact that one given patient may have been exposed to different RT. However, we cannot exclude residual confounding given the lack of clinical information such as the basal levels of VWF and FVIII, VWD type, events severity and the detailed cause of the hospitalization were missing in the database and could not be accounted for as cofounding factors. In addition, we compared EPs’ characteristics and not patients' characteristics, making the inclusion of patients’ comorbidities in the confounding factors impossible. We overcome these limitations using proxies of the severity of the stay, such as its duration and the 3-classes diagnoses associated to the index stay. We could classify 83% of them, the remaining being classified as ‘others’, which corresponded mainly to generic diagnosis codes such as ‘Von Willebrand Disease’, ‘coagulation disorder’ or ‘infusion session’.
Conclusion
Based on a large national French real-life database, our results provide new and robust evidence about the characteristics of patients with VWD treated in-hospital with VWF concentrates, their treatment patterns, the amount of cares consumed and associated costs. For the first time, they also allow to compare HCRU and costs associated with each of the RT currently available in France, which is key to inform decision-makers and clinicians to manage patients with VWD. Statistically significant results suggest that VEYVONDI® seems to be a cost-saving option in the management of on-demand VWD patients compared with historical treatment WILFACTIN® and to VONCENTO®. However, these findings need to be confirmed with the consideration of additional clinical outcomes such as bleeding control, safety and efficacy. Results also showed that concomitant use of FVIII was rare with the use of pure VWF concentrates. Additional observational studies including key clinical data as well as combined clinical-economic evaluations are now needed to further develop comparisons across RTs.
Summary points
•
Real-world data on the use of Von Willebrand factor (VWF) concentrates in the management of Von Willebrand disease (VWD) remain limited.
•
This study aimed to describe and compare patients' characteristics, treatment patterns, healthcare resource use (HCRU) and costs of VWD patients using on-demand VWF concentrates.
•
A retrospective cohort study was conducted using the French national healthcare claims database, including adult patients with at least one reimbursement for a VWF-containing replacement therapy (RT) between January 2017 and September 2021, with FU until December 2021.
•
A total of 2540 on-demand RT users were analyzed; WILFACTIN® was the most frequently used RT, followed by VONCENTO®, VEYVONDI®, EQWILATE® and WILSTART®.
•
The mean RT dose per 30-days exposure period (EP) was 12,962 +/- 19,474 IU, and the mean total cost was €21,034 +/- 34,253/EP, primarily driven by in-hospital care.
•
Compared with VEYVONDI®, WILFACTIN® episodes were associated with longer hospital stays, higher out-hospital RT use and greater overall and in-hospital costs. VONCENTO® episodes had higher in-hospital and RT-related doses and costs than VEYVONDI®.
•
The study suggests that VEYVONDI® may be a cost-saving alternative to older RTs, although further studies with clinical data are warranted.
Author contributions
C Lefèvre and CM Micallef were responsible for study design, project coordination, results interpretation and drafting the manuscript. N Bornier and M Née were involved in the study design, performed statistical analyses and reviewed the manuscript. M Belhassen was responsible for study design, results interpretation and reviewing the manuscript. B Polack, V Nerich, M Trossaërt, CB Andreani and G de Pouvourville were members of the scientific committee, providing consultancy to build the study design, interpret results and review the manuscript. J Beoletto was involved in results interpretation and reviewing the manuscript. FF Besse was involved in study design, results interpretation and reviewing the manuscript. C Chatelanaz was involved in results interpretation and reviewing the manuscript.
Acknowledgments
The authors thank the French NHS (Caisse Nationale de l'Assurance Maladie) for providing access to its claims data. The authors also thank Manon Walter (PELyon) for her strong support in the statistical analyses.
Financial disclosure
This study was funded by Takeda (France) and C Lefèvre, J Beoletto, FF Besse, C Chatelanaz were full-time employees of Takeda at the time of the study; none of them are Takeda shareholders.
Competing interests disclosure
B Polack, V Nerich, M Trossaert, C Biron-Adreani and G de Pouvourville received fees from Takeda France SAS to participate in the Scientific Committee of the study. CB Andreani also declared consulting fees from Roche, CSL (Commonwealth Serum Laboratories), LFB (Laboratoire français du Fractionnement et des Biotechnologies) and support for attending meetings and/or travel from SOBI. C Chatelanaz, FF Besse, J Beoletto and C Lefèvre are paid employees of Takeda. CM Micallef, N Bornier, M Née and M Belhassen are employees of PELyon, and received research funding from Takeda France SAS to perform the study. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No writing or editorial assistance was received for the preparation of this manuscript.
Ethical conduct of research
This study was reviewed by the French Health Data Hub (no. 5288335 from 14 October 2021). It was conducted using anonymized data, approved by the French Data Protection Authority (CNIL, approval no. 921402 from 17 November 2021). Written informed consent was not required for participation in this study, in accordance with national legislation and institutional requirements.
Data sharing statement
The dataset analyzed (i.e., the SNDS database) during the current study is not publicly available due data privacy. Data access is only granted to trained personnel upon request specific for the project and after approval from the Health Data Hub scientific committee and CNIL.
Data transparency statement
This manuscript reports the results of a database study. The study design and objectives are available in an open-access repository (https://www.health-data-hub.fr/projets).
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (desktop.ini)
- Download
- .08 KB
File (supplementary figure 1.jpg)
- Download
- 85.10 KB
{kind=link}
File (supplementary figure 2.jpg)
- Download
- 50.51 KB
{kind=link}
File (supplementary figure 3.jpg)
- Download
- 231.61 KB
{kind=link}
File (supplementary figure 4.eps)
- Download
- 3.01 MB
File (supplementary table 1.docx)
- Download
- 36.25 KB
File (supplementary table 2.docx)
- Download
- 30.38 KB
References
1.
Centre de Référence de la Maladie de Willebrand. Protocole National de Diagnostic et de Soins (PNDS): Maladie de Willebrand. Centre de Référence de la Maladie de Willebrand, Lille, France (2018).
2.
Connell NT, Flood VH, Brignardello-Petersen R et al. ASH ISTH NHF WFH 2021 guidelines on the management of Von Willebrand disease. Blood Adv. 5(1), 301–325 (2021).
3.
Centre de Référence de la Maladie de Willebrand. Protocole National de Diagnostic et de Soins (PNDS): Maladie de Willebrand – Argumentaire. Centre de Référence de la Maladie de Willebrand, Lille, France (2018).
4.
Haute Autorité de Santé. Avis – Commission de la Transparence: vonicog alfa (facteur Von Willebrand recombinant humain). VEYVONDI, 2018.
5.
Nowak-Göttl U, Miesbach W, Koscielny J et al. Replacement therapy in patients with Von Willebrand disease-indications and monitoring. Hamostaseologie 39(4), 326–338 (2019).
6.
Franchini M, Focosi D. Targeting Von Willebrand disease: the current status and future directions of management therapies. Expert Rev. Hematol. 16(11), 871–878 (2023).
7.
Peyvandi F, Kouides P, Turecek PL et al. Evolution of replacement therapy for Von Willebrand disease: from plasma fraction to recombinant Von Willebrand factor. Blood Rev. 38, 100572 (2019).
8.
Desprez D, Drillaud N, Flaujac C et al. Efficacy and safety of a recombinant Von Willebrand Factor treatment in patients with inherited Von Willebrand Disease requiring surgical procedures. Haemophilia 27(2), 270–276 (2021).
9.
Jiménez-Yuste V, Alvarez-Román MT, Palomo Bravo Á et al. Clinical efficacy and safety of Fanhdi(®), a plasma-derived VWF/factor VIII concentrate, in Von Willebrand disease in Spain: a retrospective study. Clin. App. Thromb. Hemost. 28, 10760296221074348 (2022).
10.
Windyga J, Dolan G, Altisent C et al. Practical aspects of factor concentrate use in patients with Von Willebrand disease undergoing invasive procedures: a European survey. Haemophilia 22(5), 739–751 (2016).
11.
Borel-Derlon A, Federici AB, Roussel-Robert V et al. Treatment of severe Von Willebrand disease with a high-purity Von Willebrand factor concentrate (Wilfactin): a prospective study of 50 patients. J. Thromb. Haemost. 5(6), 1115–1124 (2007).
12.
Miesbach W, Krekeler S, Wolf Z et al. Clinical use of Haemate® P in Von Willebrand disease: a 25-year retrospective observational study. Thromb. Res. 135(3), 479–484 (2015).
13.
Srivastava A, Serban M, Werner S et al. Efficacy and safety of a VWF/FVIII concentrate (wilate(®)) in inherited Von Willebrand disease patients undergoing surgical procedures. Haemophilia 23(2), 264–272 (2017).
14.
Horvais V, Beurrier P, Cussac V et al. Key drivers of coagulation factor use in Von Willebrand disease during hospitalization: an overview of the French BERHLINGO cohort. Clin. Drug. Invest. 44(1), 35–49 (2024).
15.
Morgan G, Brighton S, Laffan M et al. The cost of Von Willebrand disease in Europe: the CVESS Study. Clin. App. Thromb. Hemost. 28, 10760296221120583 (2022).
16.
Tuppin P, Rudant J, Constantinou P et al. Value of a national administrative database to guide public decisions: from the systeme national d'information interregimes de l'Assurance Maladie (SNIIRAM) to the systeme national des donnees de sante (SNDS) in France. Rev. Epidemiol. Sante Publique 65(Suppl. 4), S149–S167 (2017).
17.
Bannay A, Chaignot C, Blotiere PO et al. The best use of the Charlson Comorbidity Index with electronic health care database to predict mortality. Med. Care 54(2), 188–194 (2016).
18.
Haute Autorité de Santé. Avis - Commission de la Transparence. WILSTART, (2004). https://www.has-sante.fr/upload/docs/application/pdf/ct031519.pdf
19.
Swallow E, Marden JR, Billmyer E et al. Burden of illness and treatment patterns among patients with Von Willebrand disease in US clinical practice. Clin. App. Thromb. Hemost. 29, 10760296231177023 (2023).
20.
Oladapo A, Wu Y, Lu M et al. Economic burden associated with major surgery in patients with Von Willebrand disease: a United States retrospective administrative database analysis. J. Blood Med. 12, 699–708 (2021).
21.
Lu M, Oladapo A, Wu Y et al. Economic burden of major bleeding events in commercially insured patients with Von Willebrand disease based on claims data from the United States. J. Manag. Care Spec. Pharm. 27(2), 175–185 (2021).
22.
Rugeri L, d'Oiron R, Harroche A et al. Effectiveness and safety of hFVIII/VWF concentrate (Voncento(®)) in patients with inherited Von Willebrand disease requiring surgical procedures: the OPALE multicentre observational study. Blood Transfus. 19(2), 152–157 (2021).
23.
Rugeri L, Harroche A, Repessé Y et al. Effectiveness of long-term prophylaxis using pdFVIII/VWF concentrate in patients with inherited Von Willebrand disease. Eur. J. Haematol. 109(1), 109–117 (2022).
24.
FranceCoag. Cohorte française des patients vivant avec une maladie hémorragique constitutionnelle. Dispositif FranceCoag. Données descriptives 2021. FranceCoag (2020). https://www.francecoag.org/wp-content/uploads/2025/03/2021_Rapport_annuel_FC.pdf
25.
Nerich V, Trossaert M, Marant Micallef Cet al. et al. (Eds). A national analysis of Von Willebrand disease in France: preliminary results on replacement treatment patterns from the FORvWARD study. Congrès Français d'Hémotase, Saint-Malo, France. 10–12 May 2023.
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 2 September 2025
Accepted: 13 February 2026
Published online: 23 March 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-word evidence on healthcare resource use and associated costs in on-demand users of replacement therapies in von Willebrand disease in France: the FORvWARD study. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0128
Export citation
Select the citation format you wish to export for this article or chapter.