Availability of secondary healthcare data for conducting pharmacoepidemiology studies in Mexico: a systematic review
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To investigate the data sources available in Mexico for real-world research. Materials & methods: A systematic literature review on PubMed, EMBASE and VHL using a combination of controlled vocabulary and keywords for the concepts of electronic health records, epidemiologic studies and Mexico was performed. Results: A total of 331 articles and 89 conference abstracts reporting real-world studies were identified. These included 320 data sources: 142 unique named databases, 172 unnamed databases from specified providers, and 26 electronic medical record datasets. The main data sources came from healthcare institutions (35%), followed by government agencies (26%). The most frequent database design corresponded to surveys (34%) and disease registries (20%). Most databases included cohort studies (43%), population-based (25%) and cross-sectional studies (18%). Specific diagnostic tests (28%), access (22%) and pharmacological treatment (21%) were the most common issues analyzed in databases at patient-level data. Neoplasms, cardiac disorders and infections/infestations were the most common therapeutic areas analyzed in databases. Conclusion: In Mexico, the use of databases has increased, driven by governmental and nongovernmental organisations and companies. However, further efforts are still needed to improve the quality and knowledge of real-world evidence.
Clinical trials currently represent the gold standard for analyzing the efficacy and safety of a new drug or strategy in a controlled environment, with a well-defined population, with specific inclusion and exclusion criteria and strict follow-up [1]. However, as the population included in clinical trials is somewhat selected in experimental conditions, the information provided by these studies cannot always be extended to patients daily attended in clinical practice. For example, real-world pharmacoepidemiology studies include people who are often excluded from clinical trials, such as those with multiple chronic conditions or disabilities that may limit them. Furthermore, the extensive monitoring that takes place during clinical trials is not representative of routine clinical practice, nor would its implementation be practical due to the associated costs. This statement highlights that, in certain cases, variations in the effectiveness and safety of specific medications among individual patients may not be identified during clinical trials. There are other reasons why clinical trials may not be feasible. For example, it is unethical to randomly assign participants to a drug with a poor safety profile when comparing medicines. In summary, real-world evidence (RWE) may provide complementary information that is important to determine which treatment is more suitable for certain subgroups of patients not well-represented in clinical trials [2,3].
In this context, drug makers, regulatory agencies, healthcare professionals and payers are progressively turning to real-world data to response questions that cannot be evaluated in clinical trials, such as everyday safety, effectiveness and cost-effectiveness of the different therapeutic approaches [4–6]. RWE research using secondary data sources, including electronic health records, pharmacy or insurance claims, among others is useful to better understand how a drug is being used in clinical practice [7,8], the safety profile across all subpopulations [9], comparative effectiveness [10,11] and intervention related healthcare costs [12,13].
The majority of healthcare-related data sources of RWE comes from United States and Europe [14–16]. Although this information is relevant, it cannot necessarily be translated into Latin America population. Despite in Latin America a continuous evaluation of safety and effectiveness of new treatments is required, there is a great variability in the amount, quality and standardization of patient-level data resources [17–19]. In this context, it is important to generate local data on disease epidemiology, drug utilization, effectiveness, safety and/or customers preferences.
Although hospitals and healthcare centers in Mexico are adopting electronic medical record systems that may facilitate the collection of patient data, diagnoses, treatments and outcomes, it is still unknown the data sources available in Mexico for real-world research. Recognizing these data sources would facilitate tailoring the medical strategy based on local evidence and building strong relationships with stakeholders based on collaborative initiatives. The objective of this study was to investigate the data sources available in Mexico for real-world research by conducting a literature review of real-world studies and extracting the details of the data sources (registries and databases) utilized in these studies.
Materials & methods
To address the primary objective of the study, the methodology for all literature reviews involved conducting comprehensive literature searches, systematically screening publications to identify those relevant, and subsequently extracting data regarding the information sources used in real-world research.
Search strategy
A systematic literature review was conducted following PRISMA guidelines [20,21]. A comprehensive search strategy for peer-reviewed articles was conducted to identify literature published prior to the start of 2020 in the following bibliographic databases: PubMed, Embase and Virtual Health Library (VHS, Biblioteca Virtual en Salud [BVS] in Spanish), which includes Latin American sources. A combination of controlled vocabulary and keywords was used to perform the search strategy and included electronic health records (EHR), databases, epidemiologic studies (with different designs) and Mexico. The operators “AND” and “OR” were used to combine these concepts (Supplementary Material Search strategy). English and Spanish manuscripts, from journal articles and congress materials were included in the search without any other limits. All citations were introduced into a citation management system and duplicates were eliminated.
Eligibility criteria
Analytical studies performed on secondary data sources originating from Mexico were considered for inclusion into the study. These involved publications reporting real-world studies (observational studies, including database studies, cross-sectional studies, registry studies, pharmacoepidemiologic studies, pharmacoeconomic studies, population-based studies and safety studies, among others). Secondary data sources were considered as articles that analyzed data already collected for other purposes (e.g., EHR, administrative and commercial databases, insurance records, disease and drug registries). If the database covered different countries, this was considered if information from Mexican patients was available. The reported data sources should meet one of the following criteria: EHR plus named hospital/institute source, unnamed ‘database’ or ‘registry’ plus named hospital/institute source, named database or registry (e.g., ‘GARFIELD-AF registry’) and/or a database or registry, as part of the study reported in the publication.
By contrast, studies performed under a ‘primary data collection’ approach [22], case reports, case series, pharmacoeconomic models, review articles, editorials, policy-related articles and studies not involving Mexican data were excluded from the search.
An external qualified organization (PGA Farma) performed an initial screening of titles to select the eligible articles for abstract review and full-text data extraction by the authors. After exclusion of articles based on information in the title and abstract, full text screening was performed by the authors to determine the final inclusion.
Data extraction & analysis
For each publication, data were extracted into prespecified extraction tables using a standardized collection form. Two independent reviewers performed the search strategy and extracted each study. In case of disparities, consensus was reached after discussion. Key data for extraction included the following: publication metrics (e.g., full citation, authors, and article type), details of the real-world study reported in the article (e.g., study design, study aim, and types of data gathered from databases), and details of the real-world data sources described in the study methods (e.g., database name, size, description, data contents, and hyperlinks to the database online). For articles that reported multiple data sources of interest, each database was extracted as a separate row in the spreadsheet. Each publication reporting on the same data source was compared side-by-side to cross-check the database-specific information. All information was harmonized between such publications. For each identified database, the data extraction was supplemented by searches online. The authors performed the data extraction on Microsoft Excel. Subsequent quality assurance was performed in order to verify data quality.
Results
The PubMed, EMBASE and VHL searches yielded a total of 3617 publications. Of these, 399 corresponded to duplicates, and thus, the titles/abstracts of 3218 articles were screened. Among these, 2486 articles were excluded, and 595 articles were fully text screened, of which 20 were related to congress material, 198 were excluded and 46 articles were not available. As a result, 331 full text references were included. Additionally, 157 congress abstracts were considered, but after exclusion of 68, 89 were finally included. Therefore, overall, 331 articles and 89 conference abstracts reporting real-world studies were identified (231 articles were reported in English and 100 articles were reported in Spanish), had interpretable data, fulfilled the eligibility criteria and were used for data extraction (Figure 1).
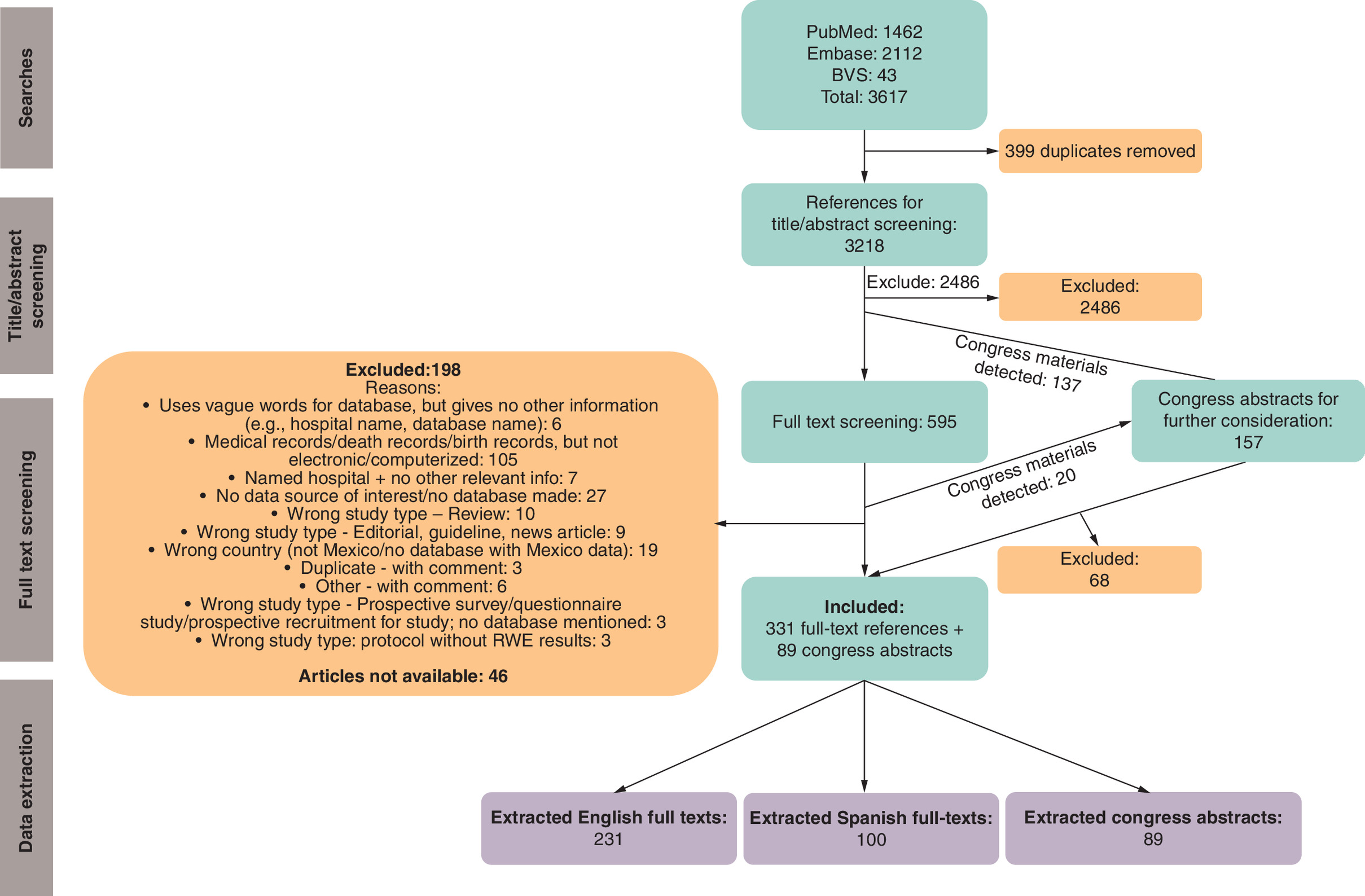
Figure 1. Flowchart of article selection.
BVS = VHL: Virtual Health Library.
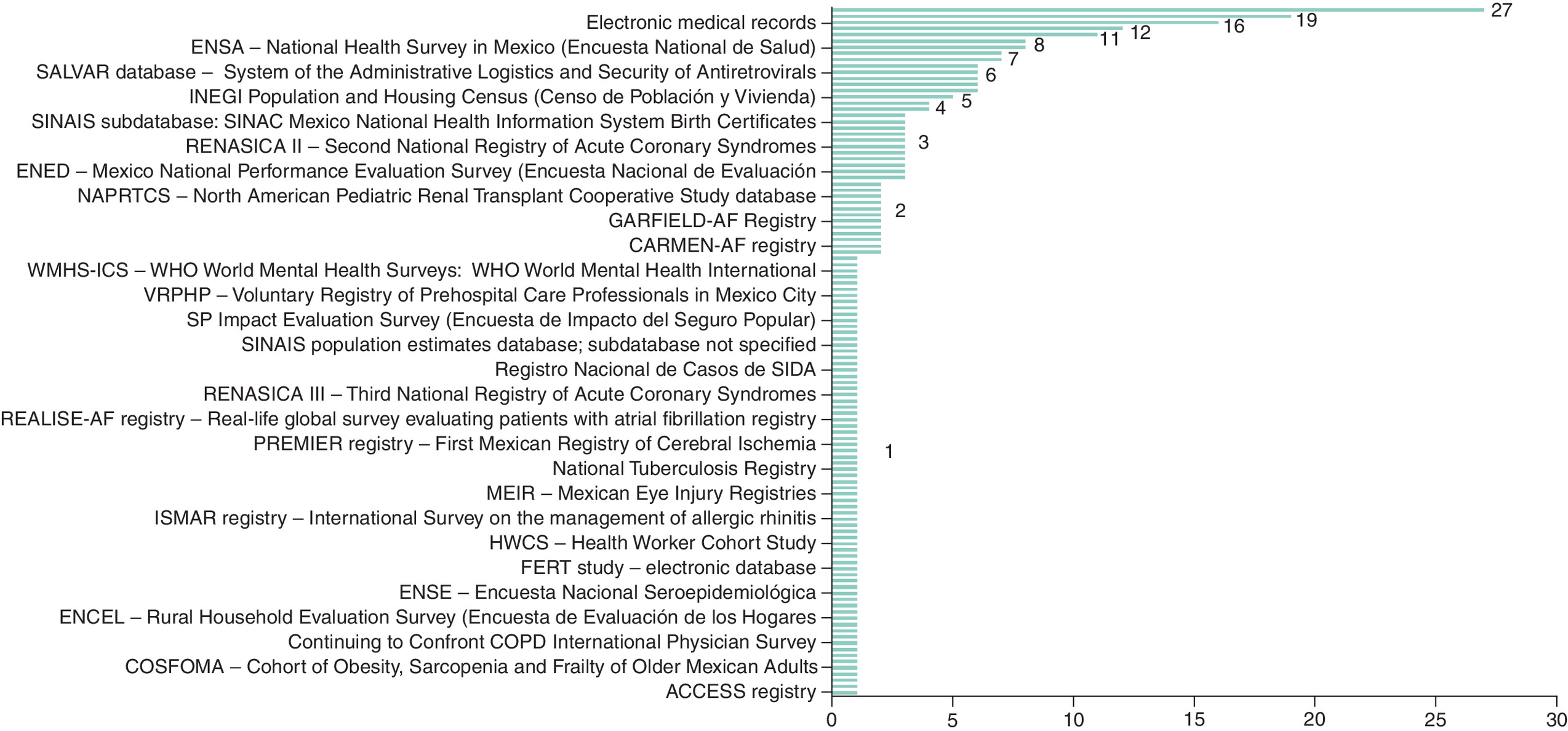
Regarding secondary healthcare databases in Mexico, 518 data sources were reported. Across the database descriptions extracted, 137/518 were supplemented with online information and 81/518 were supplemented with information from other publications extracted in the review. Among the 518 data sources extracted, there were numerous duplicates; for example, 27/518 of the extracted sources corresponded to the ENSANUT – Mexican National Survey of Health and Nutrition (‘Encuesta Nacional de Salud y Nutrición Cuernavaca, México: Instituto Nacional de Salud Pública), 320 data sources, covered 142 distinct named databases, there were 172 unnamed databases from specified providers and 26 electronic medical record datasets from specified providers. Patient-level information was available in 110 databases and were used by in the 420 articles as the data source. The most frequently-reported data source types were unnamed databases followed by ENSANUT, MHAS/ENASEM - Mexican Health and Aging Study (Estudio Nacional de Salud y Envejecimiento), CONAPO – database of population projections – (Datos de Proyecciones de la población) and ENIGH – National Survey of Household Income and Expenditures – (Encuesta Nacional de Ingresos y Gastos de los Hogares) (Supplementary Table 1). Additionally, the most frequently reported data source types at specified hospitals or institutions were unnamed database, followed by IMSS – Mexican Social Security Institute (Instituto Mexicano del Seguro Social) and INCMNSZ – Salvador Zubirán National Institute of Health Sciences and Nutrition, Mexico City (Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán) (Supplementary Table 2). Electronic medical records were the most common databases used for pharmacoepidemiology studies (Figure 2).
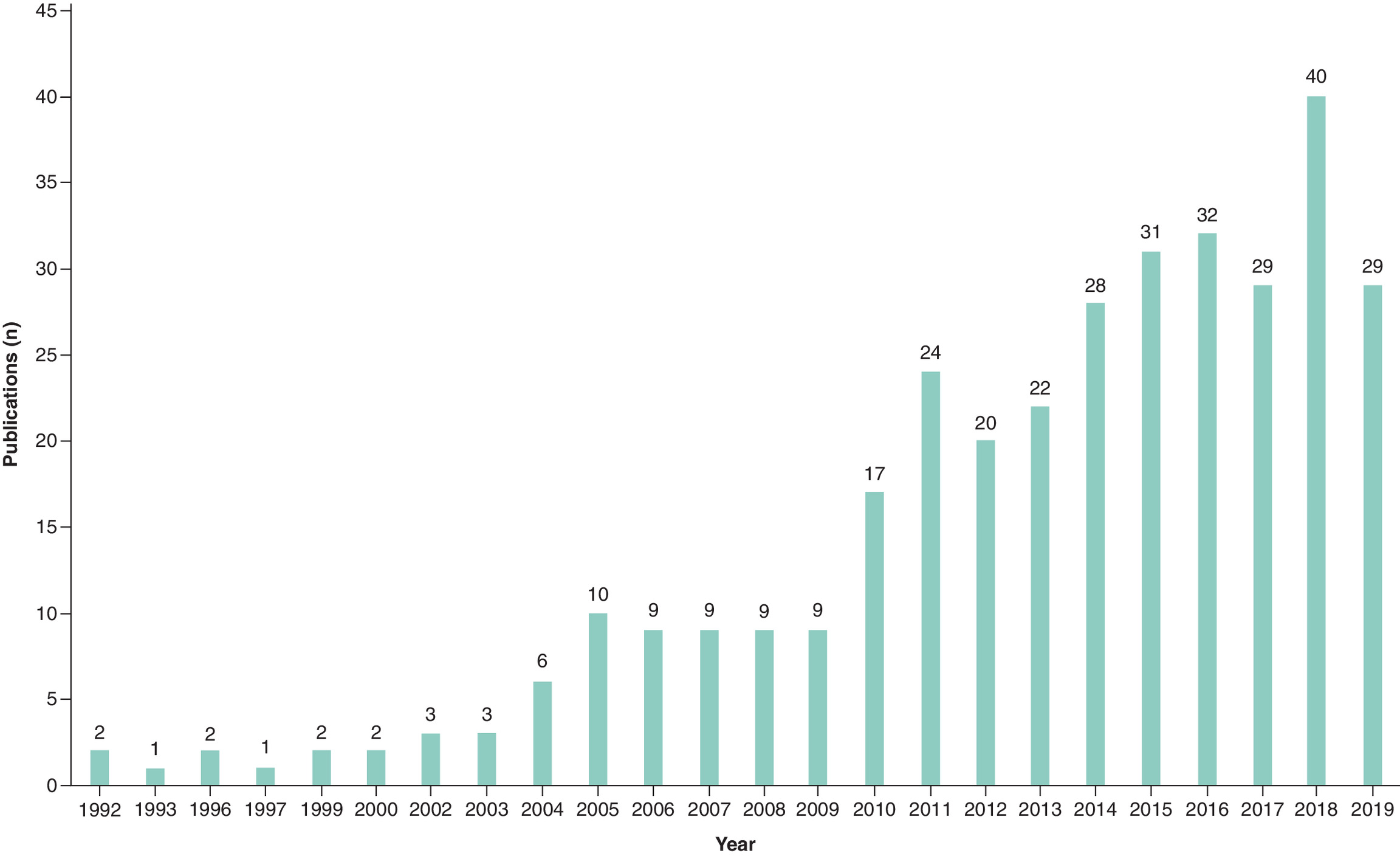
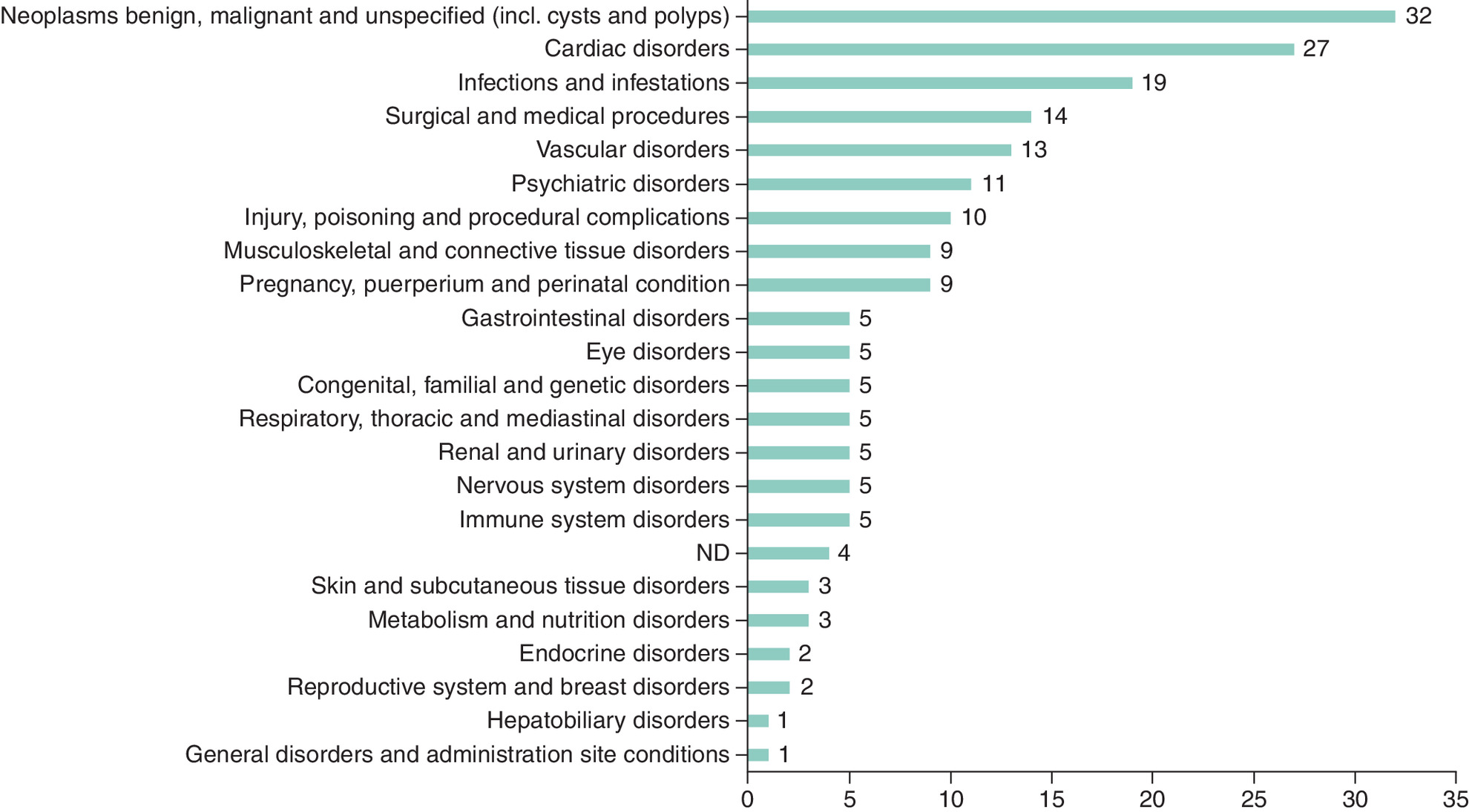
The number of publications using secondary data sources has progressively increased every year, from 1 to 2 per year in the early 90s to 40 per year in 2018 (Figure 3). The main characteristics of the databases identified are presented in Table 1. The main data sources came from healthcare institutions (35%), followed by government agencies (26%). The most frequent database design corresponded to surveys (34%) and disease registries (20%). Most of databases included cohort studies (43%), population-based (25%) and cross-sectional studies (18%). Specific diagnostic tests (28%), access (22%) and pharmacological treatment (21%) were the most common issues analyzed in the databases at patient-level data. Benign and malignant neoplasms, cardiac disorders and infections/infestations were the most common therapeutic areas analysed in databases (Supplementary Table 3 & Figure 4).
| Classification of data sources | Frequency |
|---|---|
| Healthcare institution | 35% |
| Government agency | 26% |
| Nongovernment agency | 9% |
| Health insurance company | 8% |
| Other | 18% |
| NA | 4% |
| Database design | Frequency |
| Survey | 34% |
| Disease registry | 20% |
| Administrative | 11% |
| Electronic health records | 8% |
| Drug registry | 2% |
| Others | 11% |
| NA | 14% |
| Study designs | Frequency |
| Cohort study | 43% |
| Population-based | 25% |
| Cross-sectional study | 18% |
| Pharmacoeconomic study | 6% |
| Drug utilization study | 5% |
| Case-control study | 3% |
| Patient-level data available | Frequency |
| Specific diagnostic tests | 28% |
| Access | 22% |
| Pharmacological treatment | 21% |
| Disease diagnosis codification by ICD-10 | 11% |
| Disease/Drug costs | 9% |
| Adverse event information | 6% |
| Quality of Life (QoL) | 2% |
| Drug codification by ATC | 1% |
ATC: Anatomical Therapeutic Chemical Classification System; ICD: International Classification of Diseases; NA: Not available.
The description of global and regional data sources is reported in Supplementary Table 4, with 38 articles, 61% reporting data only from Mexico and the remaining 39% not only from Mexico, but also from other countries. They were focused on disease epidemiology (82%), effectiveness (11%) and drug utilization (7%) [23–60]. The description of local disease and drug registries is reported in Supplementary Table 5, with 89 articles, 75% reporting data only from Mexico and the remaining 25% data not only from Mexico, but also from other countries. They were focused on disease epidemiology (65%), drug utilization (15%), effectiveness (8%) and drug safety (2%) (in 10% this information was not available) [23–111].
Discussion
This study was aimed to build and expand the capabilities to identify, acquire, maintain and use RWE in-house in Latin America with a particular focus on Mexico and to demonstrate the importance and impact of generating and disseminating local data on disease and product related access to medical care and treatment results for our internal and external stakeholders. Furthermore, our study may aid in developing a search strategy that other researchers can use as a template, and it offers a repository of data sources for generating RWE in Mexico that could benefit fellow researchers.
In order to reach these objectives, special care was taken in the methodology and data extraction. Thus, regarding the screening of the literature, since there was heterogeneity across publications in the level of methodological detail reported in the title and abstract, rules were developed to define the minimum requirements for inclusion of an abstract. Data sources were often described as named studies/surveys or acronyms. It was not always clear if there was an associated database for a named study. To ensure there was no associated database, research was conducted online prior to exclusion of any named studies/acronyms. In cases where it was not possible to verify if a database source was used, the study was excluded. Although some publications used the word ‘database’ as a general term to describe the results of a study, whether it was not possible to determine if a database of interest had been made as part of the study (and would be usable as a source for future work), the study was excluded. There were inconsistencies in the use of the term ‘registry’ across the literature. For instance, in some cases, the term ‘registry’ referred to a database source of interest, but in others ‘registry’ was used as a synonym for ‘registration’ and did not refer to a data source (this was very common in Spanish articles). Cases where it was not possible to verify if a database source was used, the study was excluded. To maintain the consistency for screening English and Spanish articles, because of differences in the terminology and key words, Spanish articles were screened using the same criteria as for English articles. In those cases, in which it was difficult to ascertain whether two publications were using the same database, cross-checks were performed to identify evidence for alternative names online or hyperlinks that led to the same database webpage. As some publications reported numerous database sources, the number of data sources associated with each publication was recorded in separate rows.
In our study, after an extensive search, a total of 331 articles (70% in English and 30% in Spanish) and 89 conference abstracts reporting real-world studies were identified. About secondary healthcare databases in Mexico, 518 data sources were initially reported, but after eliminating duplicities, 320 data sources, covered 142 distinct named databases, there were 172 unnamed databases from specified providers and 26 electronic medical record datasets from specified providers. Our study also showed that the number of publications using secondary data sources has progressively increased in the last decades. This does not only occur in Mexico, but also in other countries from Latin America [17–19]. In fact, secondary data sources provide important and extensive information that have become extensively used over the recent years worldwide [112–115].
In Mexico, the databases sources came from administrative data, electronic medical records and registries originating from government agencies, healthcare institutions and pharmacy dispensing companies, being surveys (34%) and disease registries (20%) the most frequent database designs. One of the main problems with secondary data sources is that the information from different sources is heterogeneous, without linkage between them. This occurs not only because of technical difficulties, but also due to privacy/property concerns [113,116]. This makes more difficult the interpretation of the data, as the differences in the results between sources may not be real, but the consequence of disparities in quality recording, confounding control, missing data or misclassification [113,117]. As a result, extensive quality control measures are required and interpretation of the data from different databases sources should be performed after an extensive analysis of the quality of the information.
The majority of data provided from Mexico sources and only a small amount as part of international data. Data sources mainly focused on disease epidemiology, drug utilization, drug effectiveness and drug safety and also covered the most relevant diseases, particularly cancer, cardiac disorders and infections. Therefore, these results emphasize the role of Mexico in collecting data from different sources and the use of this information to develop epidemiologic research with important impact on clinical practice. A recent analysis has shown that there are relevant differences in the quality of RWE in Latin America and that this RWE is not consistently used in healthcare decision making [17]. Our study showed that in Mexico, important efforts are being made to improve the quality of data sources in order to increase their application on healthcare decision making. In this setting, this research could assist in developing a database repository for RWE reporting in Mexico and help identify RWE studies within pharmacoepidemiology.
In Mexico, the most frequently reported data source types were unnamed databases followed by ENSANUT, MHAS/ENASEM, CONAPO and ENIGH. In addition, government main data sources provided from healthcare institutions (35%), and government agencies (26%). Therefore, government databases were commonly used as secondary data sources. RWE is important for physicians and payers to assess clinically relevant end points and estimate the impact of interventions on the quality of healthcare after the analysis of comparative effectiveness and safety of different approaches across therapeutic areas [118]. In this context, in Mexico the government is performing marked efforts to implement information systems that allows the capture of diverse health-related data at a population level [119,120]. In addition to government databases, disease registries actively enroll cases of disease from a well-defined demographic and therapeutic areas, and this could improve the data consistency [25,30–35,37–40,44,46–48,53,56–59]. Both, government and nongovernment databases, offer complementary information that may be very useful for decision making in clinical practice. In response to these efforts, we have shown an increase in the number of publications using secondary data sources in Mexico, which reached 40 per year in 2018, highlighting RWE growth.
This study has some limitations. Although our research employed stringent inclusion criteria, there remains a possibility that certain articles lacking methodological clarity may have been overlooked during the initial title and abstract screening process. Thus, as the search was performed at the article-level, rather than the database-level, only the data sources that were used for publication purposes were included in analysis, but not other data sources. Owing to the volume of literature, it was necessary to initially filter publications according to the information in the title/abstract. It is possible that some relevant articles were excluded owing to lack of methodological detail reported in the title/abstract. In addition, in cases where the location of the study (Mexico) was not specified in the title/abstract/index terms, (e.g., international studies) publications were not captured. Every effort was made to capture all named database or registries that were not clearly described in the publications. However, owing to inconsistencies in the descriptions and, in some cases, lack of information online, some relevant data sets may have been excluded.
Conclusions
Generating and disseminating local data through the access to secondary data sources to validate and contrast local research findings is mandatory to improve healthcare decision making for patients, healthcare professionals, regulatory agencies and internal and external stakeholders. In Mexico, in recent years there has been an increase in the use of these databases, promoted by government and nongovernment agencies/companies. Despite that, more efforts are required to expand the quality and knowledge of RWE. For instance, incorporating updated MeSH or lay terms to reflect the growth of RWE studies could improve the identification of relevant RWE.
Summary points
•
Real-world evidence (RWE) provides clinical and health information collected outside of controlled clinical trials.
•
In a real-world healthcare setting is a key component of post marketing drug evaluation, and plays a fundamental role in the access of drugs to health systems. Despite that, the availability of secondary data sources in Mexico is not well known.
•
In this study we investigated the data sources available in Mexico for real-world research by conducting a literature review of real-world studies and extracting the details of the data sources (registries and databases) used in these studies.
•
For this purpose, a systematic literature review on PubMed, EMBASE and VHL using a combination of controlled vocabulary and keywords for the concepts of electronic health records, epidemiologic studies and Mexico was performed.
•
A total of 331 articles and 89 conference abstracts reporting real-world studies were identified. These comprised 320 data sources, covered 142 distinct named databases, 172 unnamed databases from specified providers and 26 electronic medical record datasets from specified providers.
•
The main data sources came from healthcare institutions (35%), followed by government agencies (26%). The most frequent database design corresponded to surveys (34%) and disease registries (20%). Specific diagnostic tests (28%), access (22%) and pharmacological treatment (21%) were the most common issues analyzed in databases at patient-level data.
Financial disclosure
This study was supported by Bayer Mexico.
Competing interests disclosure
The authors are employees of Bayer Mexico. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Writing and editorial assistance was provided by Content Ed Net (Madrid, Spain) with funding from Bayer.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 385.71 KB
References
Papers of special note have been highlighted as: • of interest
1.
Novitzke JM. The significance of clinical trials. J. Vasc. Interv. Neurol. 1(1), 31 (2008).
2.
Eichler HG, Pignatti F, Schwarzer-Daum B et al. Randomized controlled trials versus real world evidence: neither magic nor myth. Clin. Pharmacol. Ther. 109(5), 1212–1218 (2021).
3.
Collins R, Bowman L, Landray M, Peto R. The magic of randomization versus the myth of real-world evidence. N. Engl. J. Med. 382(7), 674–678 (2020).
4.
Garrison LP, Neumann PJ, Erickson P, Marshall D, Mullins CD. Using real-world data for coverage and payment decisions: the ISPOR real-world data task force report. Value Health 10(5), 326–335 (2007).
• Although there are methodological challenges, real-world data are essential for making adequate reimbursement decisions.
5.
Zhang J, Symons J, Agapow P et al. Best practices in the real-world data life cycle. PLoS Digit. Health 1(1), e0000003 (2022).
6.
McGhan WF, Al M, Doshi JA, Kamae I, Marx SE, Rindress D. The ISPOR good practices for quality improvement of cost-effectiveness research task force report. Value Health 12(8), 1086–1099 (2009).
• To improve the quality of cost-effectiveness research, harmonization of guidelines and available instruments should be promoted.
7.
Lopes LC, Salas M, Osorio-de-Castro CGS et al. Data sources for drug utilization research in Latin American countries-a cross-national study: DASDUR-LATAM study. Pharmacoepidemiol. Drug Saf. 31(3), 343–352 (2022).
• Although multiple sources for drug utilization research are available in Latin American countries, the accessibility is limited in many places.
8.
Salas M, Lopes LC, Godman B et al. Challenges facing drug utilization research in the Latin American region. Pharmacoepidemiol. Drug Saf. 29(11), 1353–1363 (2020).
• In the Latin American countries there are relevant challenges regarding drug utilization research that are inherent to different healthcare and political systems.
9.
European Medicines Agency (EMA). Guideline on good pharmacovigilance practices (GVP) - Module VIII - Post-authorization safety studies (Rev. 3) EMA/813938/2011 Rev 3. First published 25 June 2012; last updated 12 October 2017. Available at: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-good-pharmacovigilance-practices-gvp-module-viii-post-authorisation-safety-studies-rev-3_en.pdf
10.
Stürmer T, Carey T, Poole C. ISPOR Health Policy Council proposed Good Research Practices for comparative effectiveness research: benefit or harm? Value Health 12(8), 1042–1043 (2009).
11.
Hunnicutt JN, Ulbricht CM, Chrysanthopoulou SA, Lapane KL. Probabilistic bias analysis in pharmacoepidemiology and comparative effectiveness research: a systematic review. Pharmacoepidemiol. Drug Saf. 25(12), 1343–1353 (2016).
12.
Donohue JM. A road map to rigor and relevance in pharmaceutical policy research. Milbank Q. 100(2), 341–344 (2022).
13.
Soumerai SB, Ross-Degnan D, Fortess EE, Abelson J. A critical analysis of studies of state drug reimbursement policies: research in need of discipline. Milbank Q. 71(2), 217–252 (1993).
14.
Khosla S, White R, Medina J et al. Real world evidence (RWE) – a disruptive innovation or the quiet evolution of medical evidence generation? F1000Research 7, 111 (2018).
15.
Deverka PA, Douglas MP, Phillips KA. Use of real-world evidence in US payer coverage decision-making for next-generation sequencing-based tests: challenges, opportunities, and potential solutions. Value Health 23(5), 540–550 (2020).
16.
Schad F, Thronicke A. Real-world evidence-current developments and perspectives. Int. J. Environ. Res. Public Health 19(16), 10159 (2022).
• Real-world evidence (RWE) has been included in various approval procedures of regulatory authorities, but there are important gaps and challenges to be resolved.
17.
Justo N, Espinoza MA, Ratto B et al. Real-world evidence in healthcare decision making: global trends and case studies from Latin America. Value Health 22(6), 739–749 (2019).
18.
Rodríguez-Tanta LY, Garavito Farro H, Freitas Leal L et al. Drug utilization research in Peru: is real-world data available? Front. Pharmacol. 13, 1047946 (2023).
19.
Franco JS, Vizcaya D. Availability of secondary healthcare data for conducting pharmacoepidemiology studies in Colombia: a systematic review. Pharmacol. Res. Perspect. 8(5), e00661 (2020).
20.
Liberati A, Altman DG, Tetzlaff J et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339, b2700 (2009).
21.
Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339, b2535 (2009).
22.
The European Centres for Pharmacoepidemiology and Pharmacovigilance. Guide on methodological standards in pharmacoepidemiology (Rev. 2). (2013). Available at: http://www.encepp.eu/standards_and_guidances
23.
Alcocer-Gamba MA, Martinez-Sanchez C, Verdejo-Paris J et al. Heart rate and use of beta-blockers in mexican stable outpatients with coronary artery disease. Arch. Cardiol. Mex. 85(4), 270–277 (2015).
24.
Leon-Jimenez C, Chiquete E, Cantu C et al. Citicoline for acute ischemic stroke in mexican hospitals: a retrospective postmarketing analysis. Methods Find. Exp. Clin. Pharmacol. 32(5), 325–330 (2010).
25.
Martinez-Sanchez C, Borrayo G, Carrillo J et al. Clinical management and hospital outcomes of acute coronary syndrome patients in Mexico: The Third National Registry of Acute Coronary Syndromes (RENASICA III). Arch. Cardiol. Mex. 86(3), 221–232 (2016).
26.
Oh S, Goto S, Accetta G et al. Vitamin K antagonist control in patients with atrial fibrillation in Asia compared with other regions of the world: real-world data from the GARFIELD-AF registry. Int. J. Cardiol. 223, 543–547 (2016).
27.
Parissis JT, Mantziari L, Kaldoglou N et al. Gender-related differences in patients with acute heart failure: management and predictors of in-hospital mortality. Int. J. Cardiol. 168(1), 185–189 (2013).
28.
Parissis JT, Rafouli-Stergiou P, Mebazaa A et al. Acute heart failure in patients with diabetes mellitus: clinical characteristics and predictors of in-hospital mortality. Int. J. Cardiol. 157(1), 108–113 (2012).
29.
Perdomo CD, Rodríguez ER, Carrasco Magallanes H et al. Impact of a community program for child malnutrition. Rev. Chil. Pediatr. 90(4), 411–421 (2019).
30.
Portocarrero-Ortiz LA, Vergara-Lopez A, Vidrio-Velazquez M et al. The Mexican Acromegaly Registry: clinical and biochemical characteristics at diagnosis and therapeutic outcomes. J. Clin. Endocrinol. Metab. 101(11), 3997–4004 (2016).
31.
Ruiz-Sandoval JL, Cantú C, Chiquete E et al. Aneurysmal subarachnoid hemorrhage in a Mexican multicenter registry of cerebrovascular disease: the RENAMEVASC study. J. Stroke Cerebrovasc. Dis. 18(1), 48–55 (2009).
32.
Ruiz-Sandoval JL, Chiquete E, Bañuelos-Becerra LJ et al. Cerebral venous thrombosis in a Mexican multicenter registry of acute cerebrovascular disease: the RENAMEVASC study. J. Stroke Cerebrovasc. Dis. 21(5), 395–400 (2012).
33.
Herrera AL, Góngora-Rivera F, Muruet W et al. Implementation of a stroke registry is associated with an improvement in stroke performance measures in a tertiary hospital in Mexico. J. Stroke Cerebrovasc. Dis. 24(4), 725–730 (2015).
34.
Jerjes-Sanchez C, Corbalan R, Barretto ACP et al. Stroke prevention in patients from Latin American countries with non-valvular atrial fibrillation: insights from the GARFIELD-AF registry. Clin. Cardiol. 42(5), 553–560 (2019).
35.
Juárez-Herrera U, Jerjes Sánchez C, González-Pacheco H et al. In-hospital outcome in patients with ST elevation myocardial infarction and right bundle branch block. A sub-study from RENASICA II, a national multicenter registry. Arch. Cardiol. Mex. 80(3), 154–158 (2010).
36.
Gonzalez-Aquines A, Cordero-Perez AC, Ramirez-Martinez LA et al. Onset-to-alarm time in patients with acute stroke: results from a Mexican population. Int. J. Stroke 13(7), NP19–NP21 (2018).
37.
Suwaidi JA. RENASICA II: a Mexican acute myocardial infarction registry that highlights the importance of regional registries. Glob. Cardiol. Sci. Pract. 2014(3), 232–234 (2014).
38.
Sánchez-Diaz CJ, García-Badillo E, Sánchez-Ramírez CJ et al. Clinical characteristics, process of care and outcomes among Mexican, Hispanic and non-Hispanic white patients presenting with non-ST elevation acute coronary syndromes: data from RENASICA and CRUSADE registries. Arch. Cardiol. Mex. 82(1), 14–21 (2012).
39.
Al-Naamani N, Espitia HG, Velazquez-Moreno H et al. Chronic thromboembolic pulmonary hypertension: experience from a single center in Mexico. Lung 194(2), 315–323 (2016).
40.
Antonio Gonzalez-Hermosillo J, Banos-Gonzalez MA, Guevara-Valdivia ME et al. Gender differences and management of stroke risk of nonvalvular atrial fibrillation in an upper middle-income country: insights from the CARMEN-AF registry. Int. J. Cardiol. Heart Vasc. 22, 117–122 (2019).
41.
Arauz A, Romano JG, Ruiz-Franco A et al. Differences in lipid profiles in two Hispanic ischemic stroke populations. Int. J. Stroke 9(4), 394–399 (2014).
42.
Bistola V, Simitsis P, Farmakis D et al. Association of mineralocorticoid receptor antagonist use and in-hospital outcomes in patients with acute heart failure. Clin. Res. Cardiol. 107(1), 76–86 (2018).
43.
Borrayo-Sánchez G, Rosas-Peralta M, Ramírez-Arias E et al. STEMI and NSTEMI: real-world study in Mexico (RENASCA). Arch. Med. Res. 49(8), 609–619 (2018).
44.
Chiang CE, Naditch-Brûlé L, Murin J et al. Distribution and risk profile of paroxysmal, persistent, and permanent atrial fibrillation in routine clinical practice: insight from the real-life global survey evaluating patients with atrial fibrillation international registry. Circ. Arrhythm. Electrophysiol. 5(4), 632–639 (2012).
45.
Chiquete E, Ruiz-Sandoval JL, Murillo-Bonilla LM et al. Serum uric acid and outcome after acute ischemic stroke: PREMIER study. Cerebrovasc. Dis. 35(2), 168–174 (2013).
46.
Cohen M, Urban P, Christenson JT et al. Intra-aortic balloon counterpulsation in US and non-US centres: results of the Benchmark Registry. Eur. Heart J. 24(19), 1763–1770 (2003).
47.
Montalescot G, Sobhy M, Alam S et al. In-hospital management and outcome of Acute Coronary Syndromes (ACS) in developing countries: results of the ACCESS registry. Eur. Heart J. 30(Suppl. 1), 334–335 (2009).
48.
Parissis JT, Farmakis D, Ikonomidis I et al. Acute heart failure with preserved left ventricular ejection fraction in the ALARM-HF registry: predictors of in-hospital mortality. Eur. Heart J. 30(Suppl. 1), 838–839 (2009).
49.
Parissis JT, Fountoulaki K, Farmakis D et al. Body mass index and disease-modifying therapy in acute heart failure patients. Eur. Heart J. 34(Suppl. 1), 326 (2013).
50.
Rada FP, Suarez VP, Fernandez-Rangel E et al. Venous thromboembolic disease and thromboprophylaxis: experience in a medical-surgical ICU in Mexico. Crit. Care Med. 37(Suppl. 12), A377 (2009).
51.
Aguilera-Campos A, Asensio-Lafuente E, Fraga-Sastrías JM. [Analysis of the inclusion of police personnel on the out of hospital cardiac arrest emergency response]. Salud Publica Mex. 54(1), 60–67 (2012).
52.
Alcocer LA, Lozada O, Fanghänel G et al. Global cardiovascular risk stratification: comparison of the Framingham method with the SCORE method in the Mexican population. Cir. Cir. 79(2), 168–174 (2011).
53.
Arauz-Gongora A, Cantu C, Ruiz-Sandoval JL et al. Short-term prognosis of transient ischemic attacks. Mexican multicenter stroke registry. [Spanish]. Rev. Invest. Clin. 58(6), 530–539 (2006).
54.
Cantu-Brito C, Ruiz-Sandoval JL, Chiquete E et al. Risk factors, causes, and outcome in stroke types in Mexico. The RENAMEVASC Study. Rev. Mex. Neuroci. 12(5), 224–234 (2011).
55.
Escudero-Lourdes GV, Morales-Romero LV, Valverde-Ocaña C et al. [Cardiovascular risk in children from 6 to 15 years with exogenous obesity]. Rev. Med. Inst. Mex. Seguro Soc. 52(Suppl. 1), S58–S63 (2014).
56.
González-Hermosillo JA, Márquez MF, Ocampo-Peña S. [Design of an atrial fibrillation and embolic risk registry in Mexico: CARMEN-AF]. Arch. Cardiol. Mex. 87(1), 5–12 (2017).
57.
González-Pliego JA, Gudiño-Amezcua DA, Celis A et al. [Registry of myocardial infarction in a tertiary hospital of the Instituto Mexicano del Seguro Social]. Rev. Med. Inst. Mex. Seguro Soc. 52(4), 382–387 (2014).
58.
Iturralde-Torres P, Lara-Vaca S, Cordero-Cabra A et al. [Design of a multicenter registry to evaluate rhythm versus rate control in atrial fibrillation: Atrial Fibrillation Mexican Registry (ReMeFA)]. Arch. Cardiol. Mex. 81(1), 13–17 (2011).
59.
Lupi Herrera E. [National registry of acute ischemic coronary syndromes (RENASICA). Mexican Cardiology Society. The RENASICA Cooperative Group]. Arch. Cardiol. Mex. 72(Suppl. 2), S45–S64 (2022).
60.
Santa Cruz-Ruiz JM, Sahagún-Sánchez G, González-Cabello D et al. [Analysis of clinical, echocardiographic, microbiological and cytopathological characteristics of pericardial effusions in a tertiary hospital care]. Arch. Cardiol. Mex. 84(2), 86–91 (2014).
61.
Beltrán-Sánchez H, Drumond-Andrade FC, Riosmena F. Contribution of socioeconomic factors and health care access to the awareness and treatment of diabetes and hypertension among older Mexican adults. Salud Publica Mex. 57 (Suppl. 1), S6–S14 (2015).
62.
Doubova SV, Borja-Aburto VH, Guerra YGG et al. Loss of job-related right to healthcare is associated with reduced quality and clinical outcomes of diabetic patients in Mexico. Int. J. Qual. Health Care 30(4), 283–290 (2018).
63.
Kumar A, Wong R, Ottenbacher KJ et al. Prediabetes, undiagnosed diabetes, and diabetes among Mexican adults: findings from the Mexican Health and Aging Study. Ann. Epidemiol. 26(3), 163–170 (2016).
64.
Lloyd-Sherlock P, Beard J, Minicuci N et al. Hypertension among older adults in low and middle-income countries: prevalence, awareness and control. Int. J. Epidemiol. 43(1), 116–128 (2014).
65.
Lopez-Garcia YK, Colunga-Pedraza PR, Tarin-Arzaga L et al. Iron deficiency anemia referral to the hematologist. Real-world data from Mexico: the need for targeted teaching in primary care. Hematology 23(9), 658–663 (2018).
66.
Mendoza R, Tolentino-Mayo L, Hernández-Barrera L et al. Modifications in the consumption of energy, sugar, and saturated fat among the Mexican adult population: simulation of the effect when replacing processed foods that comply with a front of package labeling system. Nutrients 10(1), 101 (2018).
67.
Jaspersen-Gastelum J, Rodríguez JA, Espinosa de los Monteros FJ et al. Prostatic profile, premature ejaculation, erectile function and andropause in an at-risk Mexican population. Int. Urol. Nephrol. 41(2), 303–312 (2009).
68.
Pagan JA, Puig A. Differences in access to health care services between insured and uninsured adults with diabetes in Mexico. Diabetes Care 28(2), 425–426 (2005).
69.
Jones K, Ramirez J, Papadimitropoulos M et al. Resource utilization and costs associated with percutaneous coronary intervention when treating patients with acute coronary syndrome in the Mexican National Institute of Cardiology “Ignacio Chavez”. Value Health Reg. Issues 20, 136–141 (2019).
70.
Rosa-Diez G, Gonzalez-Bedat M, Ferreiro A et al. Burden of end-stage renal disease (ESRD) in Latin America. Clin. Nephrol. 86(13), 29–33 (2016).
71.
Rontoyanni VG, Avila JC, Kaul S et al. Association between obesity and serum 25(OH)D concentrations in older Mexican adults. Nutrients 9(2), 97 (2017).
72.
Gonzalez-Gonzalez C, Tysinger B, Goldman DP et al. Projecting diabetes prevalence among Mexicans aged 50 years and older: the Future Elderly Model-Mexico (FEM-Mexico). BMJ Open 7(10), e017330 (2017).
73.
Guerra G, Gutierrez-Calderon E, Salgado de Snyder N et al. Loss of job-related right to healthcare associated with employment turnover: challenges for the Mexican health system. BMC Health Serv. Res. 18(1), 457 (2018).
74.
Villalpando S, Pérez-Expósito AB, Shamah-Levy T et al. Distribution of anemia associated with micronutrient deficiencies other than iron in a probabilistic sample of Mexican children. Ann. Nutr. Metab. 50(6), 506–511 (2006).
75.
Seuring T, Goryakin Y, Suhrcke M. The impact of diabetes on employment in Mexico. Econ. Hum. Biol. 18, 85–100 (2015).
76.
Sosa-Rubi SG, Galarraga O, Lopez-Ridaura R. Diabetes treatment and control: the effect of public health insurance for the poor in Mexico. Bull. World Health Organ. 87(7), 512–519 (2009).
77.
Stoddard P, Handley MA, Vargas Bustamante A et al. The influence of indigenous status and community indigenous composition on obesity and diabetes among Mexican adults. Soc. Sci. Med. 73(11), 1635–1643 (2011).
78.
Sepúlveda J, Bustreo F, Tapia R et al. [Improvement of child survival in Mexico: the diagonal approach]. Salud Publica Mex. 49(Suppl. 1), S110–S125 (2007).
79.
Araiza-Garaygordobil D, Gonzalez-Pacheco H, Sierra-Fernandez C et al. Pre-hospital delay of patients with ST-elevation myocardial infarction in Mexico City. Arch. Cardiol. Mex. 89(2), 174–176 (2019).
80.
Ascencio-Montiel IJ. 10 years analysis of diabetes-related major lower extremity amputations in Mexico. Arch. Med. Res. 49(1), 58–64 (2018).
81.
Barquera S, Tovar-Guzmán V, Campos-Nonato I et al. Geography of diabetes mellitus mortality in Mexico: an epidemiologic transition analysis. Arch. Med. Res. 34(5), 407–414 (2003).
82.
Yeatman SE, Potter JE, Grossman DA. Over-the-Counter access, changing who guidelines, and contraindicated oral contraceptive use in Mexico. Stud. Fam. Plann. 37(3), 197–204 (2006).
83.
You Y, Doubova SV, Pinto-Masis D et al. Application of machine learning methodology to assess the performance of DIABETIMSS program for patients with Type 2 diabetes in family medicine clinics in Mexico. BMC Med. Inform. Decis. Mak. 19(1), 221 (2019).
84.
Cruz C, Campuzano-Rincón JC, Calleja-Castillo JM et al. Temporal trends in mortality from ischemic and hemorrhagic stroke in Mexico, 1980–2012. J. Stroke Cerebrovasc. Dis. 26(4), 725–732 (2017).
85.
Cuanalo de la Cerda HE, Ochoa Estrada E, Tuz Poot FR et al. Food intake and nutrition in children 1–4 years of age in Yucatan, Mexico. Ann. Hum. Biol. 41(1), 46–52 (2014).
86.
Cusumano AM, Di Gioia C, Hermida O et al. The Latin American Dialysis and Renal Transplantation Registry Annual Report 2002. Kidney Int. Suppl. 97, S46–S52 (2005).
87.
Doubova SV, Lamadrid-Figueroa H, Pérez-Cuevas R. Use of electronic health records to evaluate the quality of care for hypertensive patients in Mexican family medicine clinics. J. Hypertens. 31(8), 1714–1723 (2013).
88.
Aguilar-Frasco J, Arreola-Guerra J, Palau L et al. Evolution of GFR outcomes during the first year of transplant according to the kidney donor risk index transplantation in Mexico. The experience of a single center [abstract]. Am. J. Transplant. 15(Suppl. 3), C53 (2015).
89.
Chavez Palencia C, Arellano Gomez L. Eating habits of breakfast and lunch in Mexican children. Ann. Nutr. Metab. 71(Suppl. 2), 880–881 (2017).
90.
Galvan V, Jimenez GA, Moctezuma R et al. Cognitive function changes in patients with diabetes mellitus in Mexican population in ENASEM. J. Am. Geriatr. Soc. 66(Suppl. 2), S292 (2018).
91.
Godinez Olivas HF, Nader Kawachi JA, Cano Nigenda CV et al. Retrospective registry of cerebrovascular disease in a private third level referral academic hospital (Fundacion Clinica Medica Sur) in Mexico City. J. Neurol. Sci. 357(Suppl. 1), e379 (2015).
92.
Jimenez GA, Barragan A. Deficit-direct effect of insulin on cognitive impairment treatment. J. Am. Geriatr. Soc. 66 (Suppl. 2), S284 (2018).
93.
Jimenez P, Pastor V, Luna G. Estimating the cost of treating hypoglycemc events in the Mexican public health care system. Value Health 17(3), A129–A130 (2014).
94.
Lara MV, Rodriguez CM. Prevalence of cardiovascular risk factors in persons living with HIV at high activity antiretroviral therapy in Mexico City. J. Int. AIDS Soc. 18(2 Suppl. 3), 18–19 (2015).
95.
Magis-Rodriguez C, Casillas J, Alvarez-Wyssmann V et al. Cardiovascular risk assessment In HIV patients of an outpatient HIV clinic in Mexico City. J. Int. AIDS Soc. 16(2S1), 12 (2013).
96.
Oliva-Oropeza P, Quiroz Angulo ME, Marco Antonio AC. Cost-utility of sacral neuromodulation versus augmentation cystoplasty for treatment of refractory urge incontinence in Mexico. Value Health 14(7), A537 (2011).
97.
Panopoulou P, Garcia-Contreras F, Paladio-Hernandez JA et al. Economic impact of analogue insulin on health expenditure at the Mexican Institute of Social Security in 2012. An expenditure reduction proposal. Value Health 15(7), A497 (2012).
98.
Sanchez-Casillas JL, Ramirez-Lopez-De NMG. Cost-effectiveness of paricalcitol versus parathyroidectomy for secondary hyperparathyroidism to chronic kidney disease in Mexico. Value Health 16(7), A689 (2013).
99.
Noyola-Villalobos HF, Alberu-Gomez J, Gracida C et al. Fert results (results of the collaborative retrospective study in renal transplantation in Mexico. Transplantation 90, 926 (2010).
100.
Vieira D, Mehta S, Fernandez F et al. Synergy of artificial intelligence and single lead EKG to detect and localize STEMI. Eur. Heart J. 40(Suppl. 1), 1831 (2019).
101.
Arreola-Ornelas H, Rosado-Buzzo A, Garcia-Mollinedo M et al. Cost-effectiveness of tolterodine as treatment for overactive bladder (OAB) in adult mexican patients. Value Health 14(3), A76 (2011).
102.
Camacho ME, Saenz JL, McKey TA et al. Cardiovascular risk factors and lifestyles of older mexicans with cardiovascular events. J. Am. Geriatr. Soc. 62(Suppl. 1), S43 (2014).
103.
Aldrete-Velasco JA, Chiquete E, Rodriguez-Garcia JA et al. Chronic kidney disease mortality and its relation to diabetes in Mexico. Med. Interna Mex. 34(4), 536–550 (2018).
104.
Burboa-Noriega L, Burboa-Noriega J, Cristancho-Rojas C et al. Evaluation of the characteristics of aortic dissection by computed angio-tomography in the Mexican population. Arch. Cardiol. Mex. 88(5), 496–502 (2018).
105.
Calderón-Colmenero J, De-la-Llata M, Vizcaíno A et al. [Medical and surgical health care for congenital heart disease: a panoramic vision of the reality in Mexico. Inquiry 2009]. Rev. Invest. Clin. 63(4), 344–352 (2011).
106.
Chávez Valencia V, Orizaga de La Cruz C, Becerra Fuentes JG et al. [Epidemiology of glomerular disease in adults: a database review]. Gac. Med. Mex. 150(5), 403–408 (2014).
107.
Chavolla-Canal AJ, Gonzalez-Mercado MG, Ruiz-Larios OA. Prevalence of extensively drug-resistant bacteria isolated in urine cultures over an 8-year period at a secondary care hospital in Mexico. Rev. Mex. Urol. 76(4), 213–217 (2016).
108.
Sierra-Díaz E, Belmonte-Hernández MV, Villanueva-Pérez MA et al. [Non-traumatic spontaneous retroperitoneal bleeding: the effect of an early and accurate diagnosis]. Cir. Cir. 83(3), 206–210 (2015).
109.
Viramontes-Madrid JL, Jerjes-Sánchez C, Pelaez-Ballestas I et al. [Risk of drug interactions. Combinations of drugs associated with ventricular arrhythmias]. Rev. Invest. Clin. 54(3), 192–197 (2002).
110.
Gaytán-Hernández D, Díaz-Oviedo A, Gallegos-García V et al. [Future status of ischaemic heart disease in the state of San Luis Potosí: a predictive dynamic model]. Arch. Cardiol. Mex. 88(2), 140–147 (2018).
111.
Rizo Treviño S. Demographic and clinical characteristics, and adverse reactions of people with overweight and obesity consumers of orlistat, attended by a call center (2009–2017). Medwave 17(6), e7288 (2018).
112.
Murakami Y. Secondary data analysis of epidemiology in Asia. J. Epidemiol. 24(5), 345–346 (2014).
113.
Schneeweiss S. Learning from big health care data. N. Engl. J. Med. 370(23), 2161–2163 (2014).
114.
Chikwava F, Cordier R, Ferrante A, O'Donnell M, Speyer R, Parsons L. Research using population-based administration data integrated with longitudinal data in child protection settings: a systematic review. PLoS ONE 16(3), e0249088 (2021).
115.
Hinds A, Lix LM, Smith M, Quan H, Sanmartin C. Quality of administrative health databases in Canada: a scoping review. Can. J. Public Health 107(1), e56–e61 (2016).
116.
Cohen S, Gilutz H, Marelli AJ et al. Administrative health databases for addressing emerging issues in adults with CHD: a systematic review. Cardiol. Young 28(6), 844–853 (2018).
117.
Blayney DW. Transforming data from information to quality improvement: a panel discussion with electronic health record vendors. J. Oncol. Pract. 11(3), 174–175 (2015).
118.
Roberts MH, Ferguson GT. Real-world evidence: bridging gaps in evidence to guide payer decisions. Pharmacoecon. Open 5(1), 3–11 (2021).
119.
Csete J, Kamarulzaman A, Kazatchkine M et al. Public health and international drug policy. Lancet 387(10026), 1427–1480 (2016).
120.
Langlois EV, Becerril Montekio V, Young T, Song K, Alcalde-Rabanal J, Tran N. Enhancing evidence informed policymaking in complex health systems: lessons from multi-site collaborative approaches. Health Res. Policy Syst. 14, 20 (2016).
• A higher use of research in real-world policymaking is desirable, to better fit to the complex adaptive nature of health systems.
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 2 October 2025
Accepted: 26 January 2026
Published online: 5 March 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Availability of secondary healthcare data for conducting pharmacoepidemiology studies in Mexico: a systematic review. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0160
Export citation
Select the citation format you wish to export for this article or chapter.