The effect of infertility support education on treatment outcomes in women with unexplained infertility
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To study the effect of infertility support education on treatment outcomes in women with unexplained infertility. Materials & methods: This quasi-experimental study with a pretest–posttest comparison group was conducted on women aged 19–45 years who were admitted to EO University Health, Practice and Research Hospital Department of Reproductive Endocrinology and Private D Health Hospital IVF Clinic with the diagnosis of unexplained infertility and decided to undergo in vitro fertilization (IVF)/intracytoplasmic sperm injection (ICSI) and were included in the treatment plan. A study group and a control group were formed by randomization method with at least 25 infertile women for each group. Data were collected using the Introductory questionnaire, Fertility Readiness Scale for women receiving fertility support, Healthy Lifestyle Behaviors Scale II and post-IVF/ICSI success evaluation form. The pretest scales were administered to the education and control groups at the first interview. Infertility support training was given to the education group in three sessions at 15-day intervals. Post-test data were obtained at the interview on the day of ovum pickup. Embryo transfer was performed in 25 infertile women in both groups, and human chorionic gonadotropic hormone evaluation was performed on day 12. Approximately 4 weeks later the presence of a fetal heartbeat was analyzed by reviewing the medical records, and the post-IVF/ICSI success evaluation form was completed. Results: Fetal heartbeat was detected in 15 women in the training group and only in 10 women in the control group, although the pregnancy rate increased after training and this difference was not statistically significant. Conclusion: Infertility support education has been found to have positive effects on fertility as well as general health.
Plain language summary: Supportive education may help women feel more prepared and improve healthy lifestyle habits during the tube-baby (IVF) process
What is this article about?
This study explored whether ‘infertility support education’ can help women with unexplained infertility during their tube-baby (IVF) treatment. The education program aimed to increase women’s emotional readiness, support their healthy lifestyle habits and possibly improve early pregnancy results.
What did the researchers do?
Women with unexplained infertility were randomly placed into two groups. Education group: received three sessions of infertility support education over 45 days; control group: continued routine care. Before and after the program, both groups completed questionnaires about fertility readiness and healthy lifestyle behaviors. After the tube-baby treatment, pregnancy outcomes (fetal heartbeat) were checked.
What were the results?
Women who received the education showed increase in fertility readiness and healthy lifestyle scores. A fetal heartbeat was found in 15 women in the education group and 10 women in the control group. Although the education group had a higher pregnancy rate, the difference was not statistically significant.
What do the results mean and why is this important?
The supportive education helped women feel more prepared for treatment and adopt healthier lifestyle habits – two important factors in coping with the emotional and physical challenges of infertility.
Although pregnancy results did not differ significantly, the program may still provide meaningful psychological and behavioral benefits for women undergoing tube-baby (IVF) treatment. Further research with larger groups is needed to determine its full impact on pregnancy outcomes.
Infertility is defined as the inability to conceive within 12 months despite regular unprotected sexual intercourse in women aged 15–49 years who are not using any contraceptive method. Although it is not classified as a life-threatening disease, infertility is a significant life crisis that affects couples psychologically, socially, economically, culturally and within the family context. Several studies emphasize that during the crisis created by infertility and throughout the treatment process, women’s health is more negatively affected compared with men. These studies report psychological problems in women such as stress, anxiety, depression, low self-esteem, frustration, isolation, identity disturbances, sexual dysfunction and dissatisfaction in marital relationships [1–4].
Today, various patient education interventions – including cognitive behavioral therapy, mind–body approaches, counseling and positive coping strategies – are implemented to improve mental health, pregnancy rates, sexual life and marital relationships in women undergoing in vitro fertilization (IVF) treatment. It is becoming increasingly important to include women experiencing this challenging process in supportive educational programs before, during and after treatment [3,5,6]. However, such educational programs for infertile women must be grounded in well-established and evidence-based interventions [7].
The conceptual foundations of patient education in infertility care can be traced back to the incorporation of psychosomatic principles into obstetrics and gynecology practice in the 1930s. During this period, psychological and emotional processes – particularly in infertility cases without an identifiable organic etiology – were recognized as closely linked to clinical outcomes. In the 1970s, with the development of nursing advocacy frameworks, counseling practices began to address more comprehensively the grief responses, social isolation and psychosocial burden experienced by infertile couples. The widespread introduction of IVF technologies in the 1980s increased the need for mental-health professionals within fertility clinics, making psychological assessment and support a routine component of technologically intensive reproductive treatments. In the 1990s, the rise of evidence-based practice stimulated the systematic evaluation of psychosocial interventions, leading to the development of structured, standardized and clinically validated educational and counseling models for individuals undergoing infertility treatment. By the 2000s, holistic and multidisciplinary care approaches – integrating psychological support, lifestyle modifications, stress-management strategies and behavioral techniques – had gained prominence. This historical progression paved the way for psychological support, counseling, lifestyle modification and mind–body interaction to become integral components of infertility care [8].
Infertility support education (ISE) has emerged as a contemporary extension of this integrated care framework. ISE goes beyond traditional lifestyle education by enhancing psychological motivation, utilizing conscious and subconscious affirmation strategies and promoting healthy lifestyle behaviors within a multidimensional educational structure. Thus, ISE builds upon earlier educational and counseling models and represents a holistic, patient-centered and integrative paradigm in modern infertility care. Accordingly, ISE is an educational program designed to strengthen psychological motivation to increase the chance of conception, incorporate conscious and unconscious affirmation techniques and promote healthy lifestyle behaviors [6,9,10]. ISE is considered an approach that may influence the likelihood of achieving pregnancy among individuals diagnosed with infertility.
Although there is one study in the literature examining the effect of healthy lifestyle education on treatment success [11], there is no comprehensive study investigating the effect of ISE in addition to healthy lifestyle behaviors on treatment outcomes. Therefore, considering the increasing prevalence of unexplained infertility and the importance of individualized education in shortening the process, facilitating coping, reducing costs and increasing the likelihood of treatment success, this study aims to investigate the effect of ISE on treatment outcomes among women with unexplained infertility.
Materials & methods
Ethical approval, place & time of the study
The Ethics Committee approval for the study was obtained from the Clinical Research Ethics Committee of Eskisehir Osmangazi University with the letter dated 7 April 2022 and numbered E-80558721-050.99-321998. Institutional approval was granted by the Chief Physician of Eskişehir Osmangazi University Health, Practice and Research Hospital with the letter numbered E-31568761-044-368190 on 19 August 2022. The research was completed as a doctoral thesis registered at the University’s Institute of Health Sciences, Department of Nursing, and was supported by a University’s Scientific Research Projects Coordination Unit with decision number TDK-2022-2350 dated 28 November 2022.
For the inclusion of Denizli Private Health Hospital IVF Center in the study, institutional approval was obtained from the Chief Physician of Denizli Private Health Hospital on 30 May 2023. Subsequently, a petition was submitted for the inclusion of this center, and the Ethics Committee approval dated 7 April 2022 and numbered E-80558721-050.99-321998 was revised with the letter dated 22 June 2023 and numbered E-80558721-050.99-2300141102. Following the approval of the Ethics Committee by the Clinical Research Ethics Committee of Eskisehir Osmangazi University with the letter dated 22 June 2023 and numbered E-80558721-050.99-2300141102, and the approval by the Chief Physician of Eskisehir Osmangazi University Health, Practice, and Research Hospital with the letter numbered E-31568761-044-368190, as well as the institutional approval by the Chief Physician of Denizli private health hospital on 30 May 2023, the quasi-experimental study with a pretest–posttest comparison group was conducted between November 2022 and November 2023.
Data collection was initiated in November 2022 following the initial ethics approval on 7 April 2022. An additional institution was included with a second ethics approval granted on 22 June 2023. The data collection process, including participants from the newly added institution, continued until November 2023. The study included women aged 19–45 years who were diagnosed with unexplained infertility at a reproductive health center and an IVF center, had decided to undergo in vitro fertilization (IVF)/intracytoplasmic sperm injection (ICSI), and were included in the treatment plan.
All participants were informed about the purpose and procedures of the study, and written informed consent was obtained from each participant.
Human ethics & consent to participate declarations
All procedures performed in this study involving human participants were conducted in compliance with the Declaration of Helsinki. Written informed consent was obtained from all individual participants included in the study.
Calculation of the sample size
After reviewing similar studies [10,12], a power analysis was performed to determine the sample size of the study. It was calculated as a minimum of 25 for each group and a total of 50 infertile women (25 study, 25 control) as study and control groups with a 5.0% bias level, 95.0% confidence interval, 80.0% power to represent the universe and d = 0.322 effect size [12]. A simple randomization method was preferred to ensure equality of sampling between both groups. Randomization was performed using a random number generator program called Research Randomizer (https://www.randomizer.org). Considering the losses that may occur over time in both groups, data collection continued until the number of infertile women who underwent the ET procedure reached 25. In this program, the study group was coded as “1” and the control group was coded as “2”. In total, 71 infertile women were initially assessed for eligibility. Two women declined participation, resulting in 69 women being randomized (study group n = 35, control group n = 34). Among the study group, 32 women received ISE, while three women did not attend the sessions. Subsequently, two participants discontinued the training midway and one discontinued treatment during the training period. In the control group, two women were lost at the post-test stage. During follow-up, seven participants (study: n = 6 without embryo transfer; control: n = 1 discontinued treatment) did not reach the embryo-transfer stage and were therefore excluded from the final analysis. Ultimately, 25 women in each group completed the full protocol and were included in the final analysis. These steps have been fully clarified and integrated into the flow diagram (Figure 1) to ensure transparent reporting of participant inclusion, exclusions, and losses to follow-up. Verbal and written informed consent were obtained from the women for participation in the study.
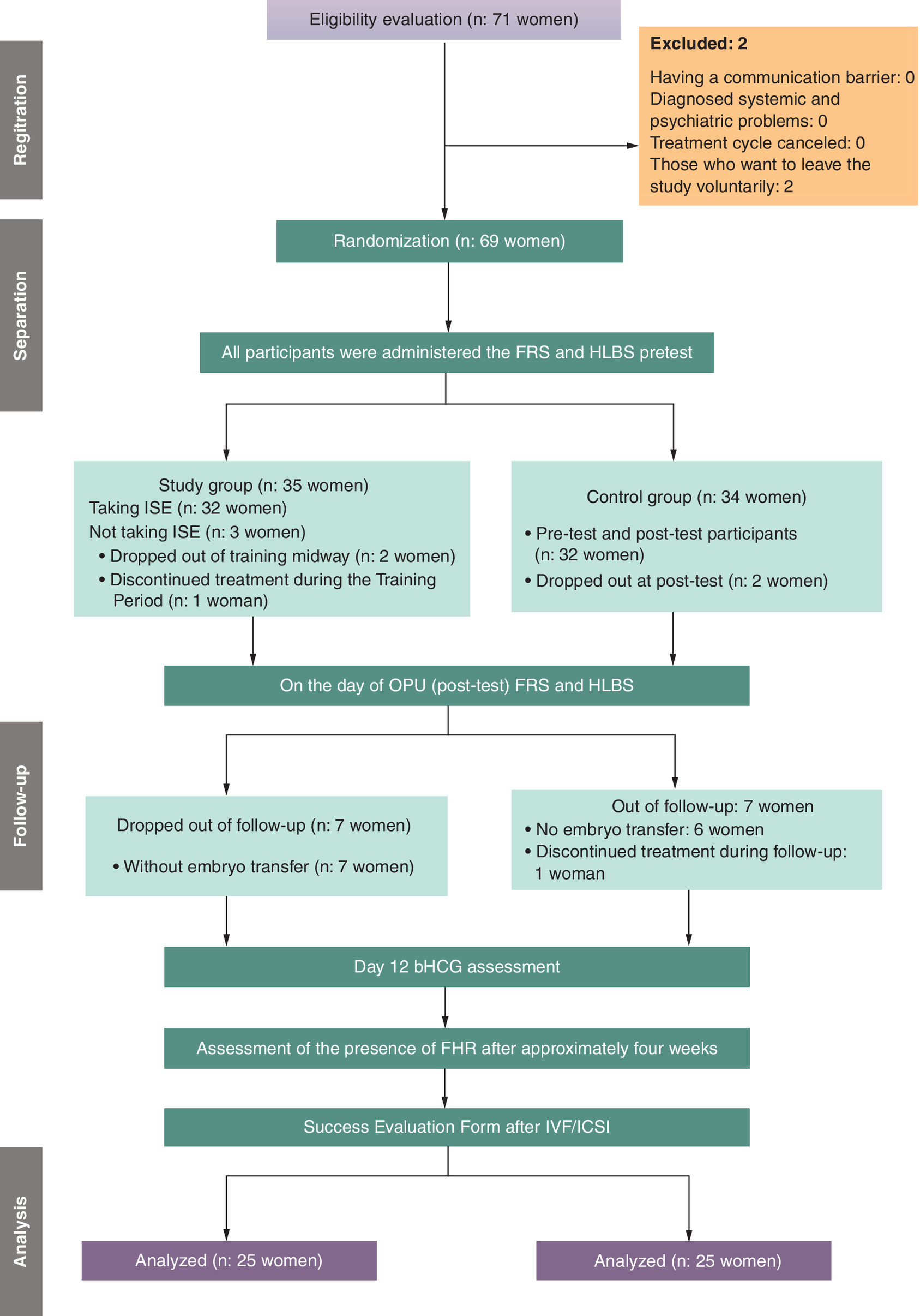
Figure 1. Research scheme.
FRS: Fertility Readiness Scale; HLBS: Healthy Lifestyle Behaviors Scale II; ICSI: Intracytoplasmic sperm injection; ISE: Infertility support education; IVF: in vitro fertilization; OPU: Ovum pickup.
Data collection forms
Data were collected using the Introductory questionnaire, the Fertility Readiness Scale (FRS) for women receiving fertility support (RFS), the Healthy Lifestyle Behaviors Scale II (HLBS), the post-IVF/ICSI success evaluation form and the evaluation of the appropriateness of written materials, DISCERN.
Introductory questionnaire
This questionnaire was created by the researcher after the literature review and consisted of a total of 13 questions, including sociodemographic information such as age, education level, occupation, income level, family type, place of residence, length of marriage and obstetric history of the participants [11].
Fertility Readiness Scale for women receiving fertility support
It is a scale developed by Fata and Aluş Tokat [13] and is used to assess the level of readiness of women receiving fertility support regarding reproductive health processes and also the effectiveness of fertility support programs. The 23-item scale consists of three sub-dimensions: ‘hope and awareness’, ‘relaxed body and mind’ and ‘positive feelings and thoughts’. Since the items in the scale contain only positive statements, the scores are calculated directly. Responses are given on a 5-point Likert scale: ‘Strongly agree’ = 5, ‘Agree’ = 4, ‘Neutral’ = 3, ‘Disagree’ = 2, ‘Strongly disagree’ = 1. Scores range from 23 to 115, and the median of the scale is 56, which can be considered a cut-off: scores ≥56 indicate higher readiness for pregnancy, while lower scores indicate less readiness. The Cronbach’s α coefficient of the scale was determined to be 0.84. The median of the scale is 56. This score indicates that the woman is more ready for pregnancy, while a lower score indicates that the woman is less ready for pregnancy.
Healthy Lifestyle Behaviors Scale II (HLBS)
The HLBS was first developed by Walker et al. in 1987 based on Pender’s health promotion model and was revised again by Walker et al. [14], in 1995 into a new version called the HLBS II consisting of 52 questions. It is a scale used to assess healthy lifestyle behaviors of individuals. Its validity and reliability in Turkey have been conducted by Bahar et al. [15]. The subscales of the scale consist of six categories: self-actualization, health responsibility, exercise, diet, interpersonal support and stress management. Each subscale can be scored independently and the total score of the scale makes up the total score of the HLBS. All items are positive statements and contain no reverse items. Responses are given on a 4-point Likert scale: 1 = ‘Never’, 2 = ‘Sometimes’, 3 = ‘Often’, 4 = ‘Always’. Scores range from 52 to 216, with higher scores indicating that the individual is practicing the health behaviors at a high level. Subscale item distribution:
•
Self-actualization: 3, 9, 15, 21, 27, 33, 39, 45, 51
•
Health responsibility: 3, 9, 15, 21, 27, 33, 39, 45, 51
•
Physical activity: 4, 10, 16, 22, 28, 34, 40, 46
•
Nutrition: 2, 8, 14, 20, 26, 32, 38, 44, 50
•
Interpersonal support: 1, 7, 13, 19, 25, 31, 37, 43, 49
•
Stress management: 5, 11, 17, 23, 29, 35, 41, 47
•
The Cronbach’s α value for the reliability of the scale was found to be 0.92.
Post-IVF/ICSI success evaluation form
This form, created by Kaya et al. [11], assesses the number of oocytes retrieved, number of meiosis II (MII) oocytes, fertilization rate, number of embryos transferred and presence of fetal heart rate (FHR). Approximately 4 weeks after embryo transfer, patient records were reviewed, and this form was completed.
Evaluation of the appropriateness of written materials, DISCERN (Quality criteria for consumer health information)
The DISCERN measurement tool, which is used to evaluate the reliability and quality of information in written educational materials, was developed by Charnock et al. [16] and translated into Turkish by Gökdoğan et al. [17]. The DISCERN measurement tool consists of a total of 16 questions. The first eight questions assess the reliability of the information provided, the next seven questions assess the quality of the information about treatment and care options, and the last 1 question assesses the overall evaluation of the material. A score between 1 and 5 is given for each question. A low total score indicates low quality, while a high total score indicates high quality. In order to evaluate the training content prepared for infertile women, the training content was sent to 10 experts in the field. The educational content was prepared in Word file format, and the experts were asked to evaluate it according to the DISCERN measurement tool. The experts rated each question with a score between 1 and 5 (1 = not suitable, 5 = suitable). According to the evaluation of 10 experts, necessary corrections in the training content were made and finalized. Questions 1, 2, 3, 4, and 7 received the highest scores among questions 1–8, indicating reliability. Among questions 9–15, which reflect the quality of information, questions 10, 13 and 15 received the highest score. As a result of the general evaluation made by the researchers, the average score of the 16th question was determined as 5 out of 5. In this case, the total evaluation score was calculated as 73 out of 75.
Study plan
Women in the study and control groups had not previously participated in ISE. All women enrolled in the study received routine education and counseling services at the clinic. The researcher (T.T.), who had a 12-module ISE certificate consisting of 92 h of online training given by Sevcan Fata and Merlinda Aluş Tokat, received information on the design and implementation of ISE from this training (https://ileriegitim.com/kurs/infertilite-dogurganlik-destek-sertifika-programi/). In addition, the researcher also participated in the trainings “One Breath, One Life Breath, You are in Control” and “Coping with Challenging Thoughts and Acceptance” of the Women Physicians Education Support Foundation to increase professionalism in the delivery of ISE. As part of the ISE, a special training plan was created after evaluating the intensity and applicability of the program following interviews with the expert who provided the training. This customized plan covers the topics of knowing the body, managing mind–body perception and preparing the lifestyle for pregnancy.
Previous studies evaluating hypnofertility-based interventions have mainly focused on hypnosis-derived techniques, including positive affirmations, imagination, visualization and relaxation to influence conscious and subconscious processes and reduce stress [10]. While these techniques aim to support fertility by decreasing psychological tension and modifying negative cognitive patterns, the scope of hypnofertility remains limited to mind-based strategies and does not include structured educational content or behavioral change components. In contrast, the ISE used in the present study is a broader and more structured program that integrates both cognitive-emotional techniques and comprehensive body-mind awareness, reproductive health education and lifestyle regulation. Unlike hypnofertility, ISE includes modules on anatomy-physiology, infertility knowledge, brain–body mapping, consciousness–subconscious mechanisms, diaphragmatic breathing, as well as lifestyle modifications such as diet, exercise, caffeine use, smoking, stress management and general preconception health behaviors. Therefore, ISE combines evidence-based education with targeted mind–body practices and behavioral interventions. The training plan is divided into three sessions and eight modules and includes the following topics. A detailed description of the session is shown in Table 1.
| First session Emotional exploration, information gathering and body awareness | Second session Brain–body perception management | Third session Preparing your lifestyle for pregnancy |
| *Module 1: Introduction Aim: At the stage of the meeting between the researcher and the infertile woman, the aim is for the woman to express her expectations of the training. | *Module 5: Brain–body map Aim: The aim is to provide women with information about the functioning of the brain, right and left-brain functions, consciousness, and subconscious mechanisms. | *Module 8: Healthy lifestyle behaviors Aim: The aim is to help women learn healthy lifestyle changes. - Cigarette use - Alcohol use - Diet - Stress - Exercise - Caffeine use |
| *Module 2: Positive, negative experiences with infertility Aim: To systematically discuss women's perceptions, thoughts and experiences of infertility. | *Module 6: Consciousness affirmation Aim: The aim is to help women transform negative concepts and statements about infertility into positive ones. | |
| *Module 3: Definition of infertility, literature information Aim: Aim is to learn about the definition of infertility and the global incidence of infertility. | *Module 7: Subconscious affirmation Aim: The aim is to help women learn visualization, imagination, and relaxation techniques. | |
| *Module 4: Anatomy and physiology of the women reproductive system Aim: The aim is to learn about women's reproductive organs, physiology and hormones. |
*Diaphragmatic breathing was preferred among relaxation exercises in our study.
The women in the study group were given the FRS and HLBS pretest at the first interview. The first stage of the ISE was carried out in a total of three stages by providing training at the first interview with the woman who decided to undergo IVF/ICSI and every 15 days after the first interview. Verbal, written and visual training materials were used during the training process. For each woman in the study group, the ISE was conducted in a specially prepared separate room using the face-to-face interview method and lasted approximately 20–25 min. To support each participant and help them recognize the empowering consequences of positive health behaviors, develop a positive perspective on behaviors, and improve self-monitoring, pamphlets on the topic were given after each session to remind and reinforce the information. At the end of each session, goals were set to successfully maintain the affirmation and health-promoting behaviors until the next session. After the ISE was administered in three sessions 15 days apart, the study group was administered the FRS and HLBS again during the OPU phase. The study group underwent bHCG evaluation on the 12th day after ET following the OPU phase. Women with a positive bHCG were evaluated by a physician for the presence of FHR approximately 4-weeks later, and the researcher scanned the patient records and completed the post-IVF/ICSI success evaluation form. Of the women in the education group (n = 35), two women dropped out of the education program and one woman dropped out of treatment. Another seven women who received ISE education but whose IVF/ICSI procedure was aborted for various reasons (low follicle count, insufficient follicle development, low quality or number of oocytes, endometrial incompatibilities, hormonal irregularities, health problems, etc.) were excluded from the study. In the study group, 25 women underwent ET.
Women in the control group were administered the pretest FRS and HLBS at the first interview. FRS and HLBS were administered again at the interview on the day of OPU. The control group underwent bHCG evaluation on the 12th day after the ET, which was performed after the ovum pickup (OPU) stage. Women with positive bHCG were evaluated by a physician for the presence of FHR approximately 4 weeks after the IVF/ICSI procedure, and the researcher scanned the patient records and completed the post-IVF/ICSI success evaluation form. In the control group (n = 34), two women were excluded from the study because two women withdrew from the study and one woman discontinued treatment during the follow-up period. Another six women whose IVF/ICSI procedure was terminated for various reasons (low follicular count, insufficient follicular development, low quality or number of oocytes, endometrial incompatibilities, hormonal irregularities, health problems, etc.) were excluded from the study. In the control group, 25 women underwent ET. The detailed description of the research scheme is shown in Figure 1.
Statistical methods
The statistical methods used in the study were as follows: Data were analyzed using IBM SPSS V23. Normality of the data was assessed using Kolmogorov–Smirnov and Shapiro–Wilk tests. Independent samples t-test was used for normally distributed data in comparisons between two groups. Mann–Whitney U test was used for data that did not follow normal distribution in comparisons between two groups. For comparisons of categorical data, Yates correction, Fisher-Freeman-Halton test, and Pearson’s chi-square test were used, and multiple comparisons were assessed using Bonferroni correction. Spearman’s rho correlation coefficient was used to examine the relationship of non-normally distributed scale scores. Generalized Linear Models were used for comparisons of normally distributed data by group and time, and Tukey test was used for multiple comparisons. Robust ANOVA test was used for comparisons of data not following normal distribution by group and time, with Bonferroni correction applied for multiple comparisons. Analysis results were presented as frequency (percentage) for categorical variables, mean ± standard deviation for quantitative variables, median (minimum - maximum), and trimmed mean ± standard error. A significance level of p < 0.050 was considered.
Results
When the socio-demographic data between the two groups were compared, the mean age of the study group was 29.63 ± 3.18 years and that of the control group was 30.22 ± 2.73 years. In addition, the mean duration of marriage in the study group was 6.25 ± 2.03 years, while the mean duration of marriage in the control group was 6.28 ± 1.61 years. When the smoking data between both groups were analyzed, 37.50% of the study group and 50.0% of the control group were found to be smokers. No statistically significant relationship was found between the sociodemographic parameters according to the groups (p > 0.05). When the data on infertility status between both groups were analyzed, it was found that the mean duration of infertility was 4.94 ± 2 years in the study group and 5 ± 1.48 years in the control group. In addition, it was found that the sources of information about infertility in both groups were mostly health personnel (50.0%, 56.30%). There was no statistically significant difference between the mean values of infertility duration and infertility sources according to the groups (p > 0.05).
There was a statistically significant difference between the mean scores of the total score, hope and awareness sub-dimension score, positive emotions and thoughts sub-dimension score, and ready body and brain sub-dimension score of the FRS after ISE (p < 0.001) (Table 2).
| Variables | Study (n = 32) | Control (n = 32) | Total | Analysis between groups |
|---|---|---|---|---|
| Avrg ± SD/median§ (min–max) | Avrg ± SD/median§ (min–max) | Avrg ± SD/median§ (min–max) | t/z;p | |
| Hope and awareness | ||||
| Pre-test | 33 (30–40) | 33 (30–40) | 33 (30–40) | 0.942‡ |
| Post-test | 36 (36–41) | 33 (30–40) | 36 (30–41) | p < 0.001‡,** |
| Total | 36 (30–41) | 33 (30–40) | 34 (30–41) | |
| Difference | 3.5 ± 1.14 | -0.28 ± 2.9 | 1.61 ± 2.9 | p < 0.001‡,** |
| 4 (1–6) | -1 (-8–6) | 3 (-8–6) | ||
| Group§ time | p < 0.001§ | |||
| Positive emotions and thoughts | ||||
| Pre-test | 17.1 ± 0.26 | 17 ± 0.35 | 17.1 ± 0.19 | 0.313† |
| Post-test | 20 ± 0.16 | 16.9 ± 0.27 | 18.5 ± 0.26 | p < 0.001†,** |
| Total | 18.7 ± 0.26 | 16.9 ± 0.2 | 17.8 ± 0.18 | |
| Difference | 2.88 ± 1.1 | -0.16 ± 1.97 | 1.36 ± 2.2 | p < 0.001‡,** |
| 3 (0–5) | 0 (-4–4) | 2 (-4–5) | ||
| Group§ time | p < 0.001§ | |||
| Ready body and mind | ||||
| Pre-test | 30 (27–34) | 29 (27–34) | 29.5 (27–34) | 0.642‡ |
| Post-test | 36 (34–38) | 29 (27–34) | 34 (27–38) | p < 0.001‡,** |
| Total | 34 (27–38) | 29 (27–34) | 31 (27–38) | |
| Difference | 5.66 ± 1.21 | -0.34 ± 2.25 | 2.66 ± 3.52 | p < 0.001†,** |
| 6 (3–8) | -0.5 (-5–6) | 3.5 (-5–8) | ||
| Group§ time | p < 0.001§ | |||
| FRS total | ||||
| Pre-test | 79 (75–91) | 78.5 (75–91) | 79 (75–91) | 0.751‡ |
| Post-test | 88 (84–94) | 75 (71–86) | 85 (71–94) | p < 0.001‡,** |
| Total | 86 (75–94) | 77 (71–91) | 80 (71–94) | |
| Difference | 7.75 ± 2.77 | -4.94 ± 5.19 | 1.41 ± 7.61 | p < 0.001‡,** |
| 8 (1–11) | -4 (-16–4) | 3 (-16–11) | ||
| Group§ time | p < 0.001§ | |||
†
Independent samples t-test.
‡
Mann–Whitney U test; median (minimum–maximum); SD.
§
Robust ANOVA; median method was used as the comparison method.
**Statistical significance at p < 0.001.
Avrg: Average; FRS: Fertility Readiness Scale; SD: Standard deviation.
A statistically significant difference was found between the mean values of the total score, health responsibility sub-dimension score, physical activity sub-dimension score, nutrition sub-dimension score, spiritual development sub-dimension score, interpersonal relationships sub-dimension score and stress management sub-dimension score of the HLBS after the ISE (p < 0.001) (Table 3).
| Variables | Study (n = 32) | Control (n = 32) | Total | Analysis between groups |
|---|---|---|---|---|
| Avrg ± SD/median§ (min–max) | Avrg ± SD/median§ (min–max) | Avrg ± SD/median§ (min–max) | t/z;p | |
| Health responsibility | ||||
| Pre-test | 20.5 (17–24) | 20 (17–24) | 20 (17–24) | 0.447‡ |
| Post-test | 25 (21–28) | 20 (17–24) | 23 (17–28) | p < 0.001‡,** |
| Total | 23 (17–28) | 20 (17–24) | 22 (17–28) | |
| Difference | 4 ± 1.81 | 0.31 ± 2.93 | 2.16 ± 3.05 | p < 0.001†,** |
| 4 (1–8) | 0 (-6–6) | 2.5 (-6–8) | ||
| Group§ time | p < 0.001§ | |||
| Physical activity | ||||
| Pre-test | 13.91 ± 3.25 | 13.84 ± 3 | 13.88 ± 3.1 | 0.942† |
| Post-test | 17.22 ± 4.55 | 13.22 ± 2.57 | 15.22 ± 4.18 | p < 0.001†,** |
| Total | 15.56 ± 4.26 | 13.53 ± 2.79 | 14.55 ± 3.73 | |
| Difference | 3.31 ± 1.94 | -0.63 ± 3.32 | 1.34 ± 3.35 | p < 0.001†,** |
| 3 (0–7) | -1 (-6–5) | 2 (-6–7) | ||
| Group§ time | p < 0.001§ | |||
| Diet | ||||
| Pre-test | 20 (17–31) | 20 (17–31) | 20 (17–31) | 0.543‡ |
| Post-test | 25 (21–31) | 20 (17–31) | 23 (17–31) | p < 0.001‡,** |
| Total | 23 (17–31) | 20 (17–31) | 21 (17–31) | |
| Difference | 4.75 ± 2.2 | -0.66 ± 4.55 | 2.05 ± 4.47 | p < 0.001‡,** |
| 5 (0–8) | -1 (-12–9) | 3 (-12–9) | ||
| Group§ time | p < 0.001§ | |||
| Spiritual development | ||||
| Pre-test | 22.78 ± 2.99 | 22.94 ± 2.69 | 22.86 ± 2.82 | |
| Post-test | 27 ± 1.74 | 22.75 ± 2.88 | 24.88 ± 3.19 | p < 0.001†,** |
| Total | 24.89 ± 3.23 | 22.84 ± 2.77 | 23.87 ± 3.17 | |
| Difference | 4.22 ± 2.12 | -0.19 ± 3.57 | 2.02 ± 3.66 | p < 0.001‡,** |
| 4 (1–8) | 0 (-10–7) | 2 (-10–8) | ||
| Group§ time | p < 0.001§ | |||
| Interpersonal relations | ||||
| Pre-test | 21.5 (18–27) | 22 (18–27) | 22 (18–27) | 0.242† |
| Post-test | 26 (19–29) | 21.5 (18–27) | 23.5 (18–29) | p < 0.001‡,** |
| Total | 24 (18–29) | 22 (18–27) | 23 (18–29) | |
| Difference | 4.03 ± 2.04 | -0.34 ± 3.29 | 1.84 ± 3.5 | p < 0.001‡,** |
| 3.5 (1–9) | -1 (-5–7) | 2.5 (-5–9) | ||
| Group§ time | p < 0.001§ | |||
| Stress management | ||||
| Pre-test | 17 (14–21) | 17 (14–21) | 17 (14–21) | 0.847‡ |
| Post-test | 22.5 (16–26) | 17 (14–21) | 19.5 (14–26) | p < 0.001‡,** |
| Total | 20 (14–26) | 17 (14–21) | 18 (14–26) | |
| Difference | 4.63 ± 1.58 | 0.19 ± 2.19 | 2.41 ± 2.93 | p < 0.001‡,** |
| 5 (2–7) | 0 (-4–4) | 3 (-4–7) | ||
| Group§ time | p < 0.001§ | |||
| HLBS total | ||||
| Pre-test | 115 (102–142) | 114 (102–142) | 114 (102–142) | 0.545‡ |
| Post-test | 145 (122–158) | 114 (102–142) | 125.5 (102–158) | p < 0.001‡,** |
| Total | 130.5 (102–158) | 114 (102–142) | 119 (102–158) | |
| Difference | 24.94 ± 8.18 | -1.31 ± 8.99 | 11.81 ± 15.74 | p < 0.001‡,** |
| 24 (12–44) | 0 (-26–17) | 13.5 (-26–44) | ||
| Group§ time | p < 0.001§ | |||
†
Independent samples t-test.
‡
Mann–Whitney U test; median (minimum–maximum); standard deviation (SD).
§
Robust ANOVA; median method was used as the comparison method.
**Statistical significance at p < 0.001.
Avrg: Average; HLBS: Healthy Lifestyle Behaviors Scale II; SD: Standard deviation; t/z: t-test/z statistic.
A statistically significant positive and very high correlation was found between the total post-test score of the FRS and the total post-test score of the HLBS (Table 4). A positive and statistically significant relationship was found between the post-test total FRS score and the post-test total HLBS score in the intervention group (Spearman's ρ = 0.424, p = 0.035). The scatter plot demonstrates that as FRS scores increase, HLBS scores also tend to increase, indicating a generally monotonic and upward trend (Figure 2). This finding suggests that as fertility readiness levels increase in the intervention group, post-test healthy lifestyle behavior scores also tend to rise (Table 4).
| HLBS post-test total | ||
|---|---|---|
| FRS post-test total | r | 0.424 |
| p | 0.035 |
FRS: Fertility Readiness Scale; HLBS: Healthy Lifestyle Behaviors Scale II; r: Spearman’s rho correlation coefficient.
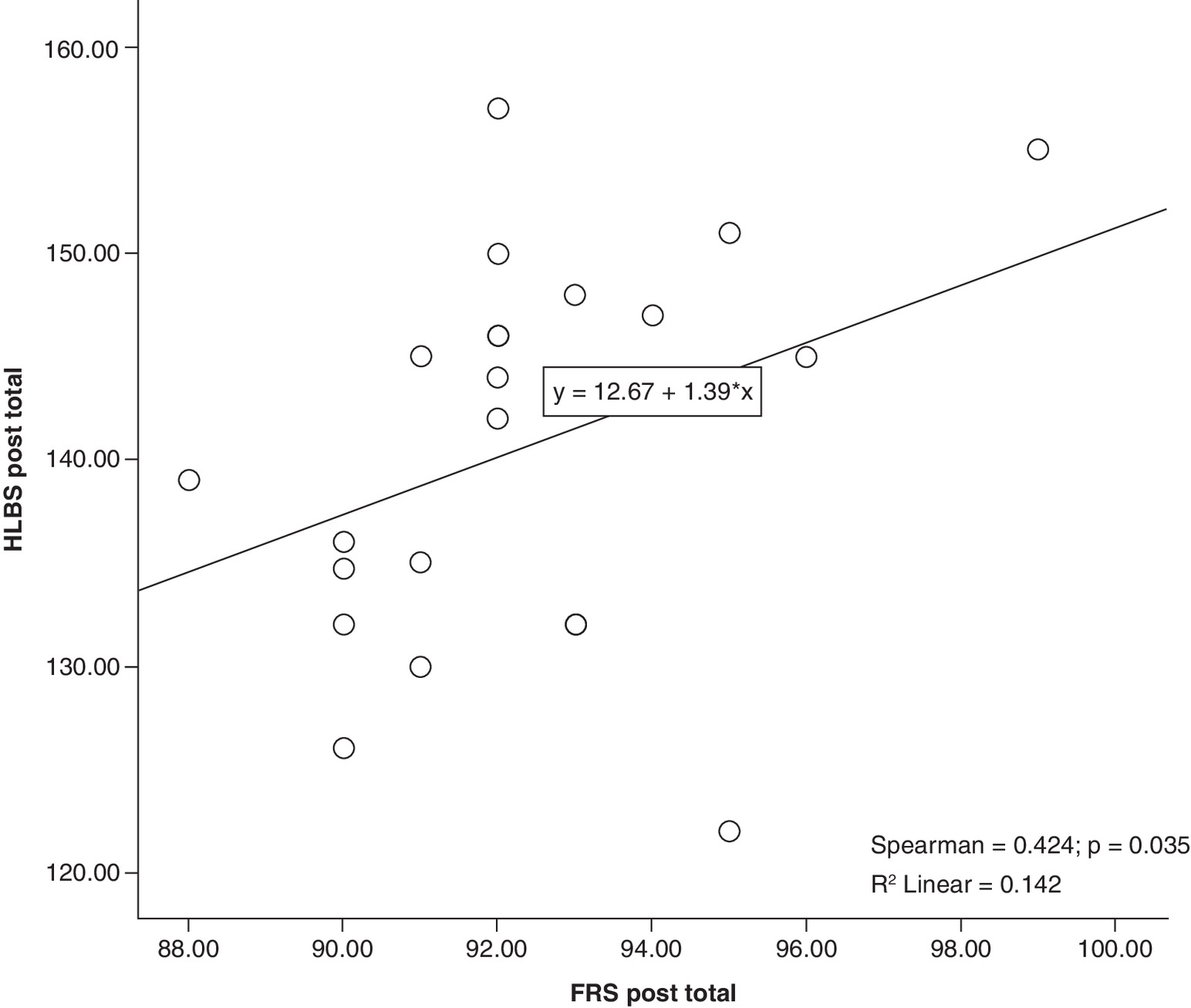
Figure 2. Scatter plot of the relationship between post-test total scores of the Fertility Readiness Scale and the Healthy Lifestyle Behavior Scale in the intervention group.
FRS: Fertility Readiness Scale; HLBS: Healthy Lifestyle Behaviors Scale II.
While FHR was detected in 15 women (60.0%) in the education group, FHR was detected in only 10 women (40.0%) in the control group. Although pregnancy rates increased in the education group, this difference was not statistically significant (p = 0.325) (Table 5).
| Group | Total | Test statistic | p-value | ||
|---|---|---|---|---|---|
| Study (n = 32) | Control (n = 32) | ||||
| Oocytes collected, n | 7.91 ± 1.82 | 7.91 ± 2.35 | 7.91 ± 2.08 | 0 | p > 0.999† |
| 8 (4–12) | 8 (4–13) | 8 (4–13) | |||
| Meiosis II oocyte count, n | 5.41 ± 1.5 | 5.09 ± 1.67 | 5.25 ± 1.58 | 448 | 0.380‡ |
| 5 (3–8) | 5 (3–9) | 5 (3–9) | |||
| Fertilization rate | 82.62 ± 4.74 | 81.66 ± 5 | 82.14 ± 4.86 | 458.5 | 0.470‡ |
| 81 (72–90) | 81 (72–90) | 81 (72–90) | |||
| Embryos transferred, n | 1.06 ± 0.25 | 1.06 ± 0.25 | 1.06 ± 0.24 | 512 | p > 0.999‡ |
| 1 (1–2) | 1 (1–2) | 1 (1–2) | |||
| Group | Total | Test statistic | p-value | ||
| Study (n = 25) | Control (n = 25) | ||||
| bHCG | |||||
| Positive | 25 (%100) | 25 (%100) | 50 | ||
| FHR | |||||
| Yes | 15 (60) | 10 (40) | 25 (50) | 0.621 | 0.325§ |
| No | 10 (40) | 15 (60) | 25 (50) | ||
†
Independent Samples t-test.
‡
Mann Whitney U test.
§
Yates Correction.
FHR: Fetal heart rate.
Discussion
It has been reported in various studies that negative choices such as healthy lifestyle factors, eating habits, stress, alcohol and smoking, excessive caffeine consumption and obesity may affect women’s physiology in the long term [11,18–21]. In this study, the scores of the education group that received the ISE increased on the post-ISE measures. In the studies of Kaya et al. [11] and Altıparmak [22], lifestyle training given to women diagnosed with infertility significantly increased the subscale and total scale scores of the HLBS. These results highlight that lifestyle training can have positive effects on fertility and the potential of training programs to increase fertility in infertile women. Improvements in the nutrition and physical activity sub-dimensions were noted to be associated with the infertility-specific dietary recommendations and behavioral strategies promoting regular activity that were included in the education program; these components have been supported in the literature as influencing IVF outcomes and reproductive health [20,23,24] The increases observed in stress management and spiritual growth were discussed as potentially related to the relaxation, mindfulness, affirmation and psychological well-being enhancing techniques incorporated into the education; these interventions are consistent with studies showing reductions in stress among infertile women [25,26]. The improvements in health responsibility and interpersonal relationships were explained as being associated with the provision of accurate infertility-related information, content supporting women’s active participation in healthcare and strengthened coping abilities for dealing with stigma [27,28].
In addition, studies in the literature show that technology-assisted healthy lifestyle training for infertile women has been developed, and personalized online and mobile programs have been used [29,30]. These studies demonstrate the diversity and effectiveness of healthy lifestyle education [30–32].
The infertility process can become a life crisis, causing long-term psychological distress and vulnerability. Psychosocial interventions for infertile individuals are recommended to reduce and reverse this negative impact [33]. In this study, the FRS scores of the education group that received ISE increased on post-ISE measures. The increase in fertility readiness was discussed as being linked to the components of the education that promote positive thinking, raise awareness, and support mind–body harmony; the literature indicates that readiness facilitates behavior change and the adoption of healthy lifestyle practices [7,10]. One study highlighted the need for evidence-based interventions that include patient-centered care and coping education to improve women’s well-being [7]. The need for patient-centered infertility care with a focus on the psychological needs of couples was also reported in another study [34]. A systematic review found that training provided before, during, and after ART is essential for managing the psychosocial aspects of infertile women. It is emphasized that trainings increase awareness among infertile women and these approaches should be translated into policies focused on health protection and promotion [35]. Yanık’s [26], study emphasizes the importance of educational programs in the treatment process to increase the psychological well-being and hope of women undergoing infertility treatment. However, in the studies of [10] and [12], no statistically significant difference was found in the level of fertility readiness after training between the groups that received hypnofertility-based training. These differences may be due to the differences in methodological approaches, such as the implementation methods, duration, and content of ISE and hypnofertility-based training. In this sense, future research may help to better elucidate the reasons for these differences by more closely examining the interactions and outcomes between different training programs.
In our study, a significant and positive correlation was found between the post-test total score of the FRS and the post-test total score of the HLBS after the ISE. A significant correlation indicates that there is a significant relationship between two variables. A positive correlation indicates that an increase in one variable is associated with an increase in the other variable [36]. The very high positive correlation between FRS and HLBS indicates that there is a strong and consistent relationship between the two measures. Our study results show that women’s readiness levels increase with ISE, which contributes to making healthy lifestyle behaviors more applicable. As women’s readiness increases, their scores on healthy lifestyle behaviors tend to increase. Readiness is a concept that shows how willing a woman is to adapt to a situation. If the ISE increases a woman's readiness by increasing her positive thinking habits, this may make it more likely that she will adopt the HLBS. Increased readiness with ISE can make healthy lifestyle behaviors more feasible and sustainable. However, it is important to note that correlation does not imply causation. The positive association observed between FRS and HLBS scores does not indicate that ISE directly causes improvements in either readiness or healthy lifestyle behaviors. These findings only show a relationship between the two variables, and further longitudinal or experimental studies are needed to establish any causal links.
Studies on the effect of healthy lifestyle behaviors and mind–body programs on live birth rates in infertile women are inconsistent in the literature. Therefore, there is no definitive information on the effectiveness of any particular training or program. A meta-analysis of infertile individuals suggests that preconception healthy lifestyle education may have little or no effect on live birth rates [31]. One study found that preconception healthy lifestyle education had no significant effect on live births or pregnancy rates compared with routine care [29]. Another study reported that hypnofertility-based interventions during the treatment process did not have the expected effect on pregnancy outcomes, although they did provide relief to the woman [10]. In our study, 15 women who received ISE had FHR, while 10 women in the control group had FHR. However, the difference between the groups was not statistically significant, indicating that although ISE resulted in increased pregnancy outcomes in the training group, it did not lead to a measurable improvement. In a study conducted by Rooney and Domar, it was observed that healthy lifestyle education in infertile women can have a significant impact on pregnancy rates [37]. Another study found that a healthy lifestyle is an important, modifiable, and influential factor in reproduction. To increase the success of ART, the importance of assessing the healthy lifestyle habits of couples with infertility problems and designing and implementing healthy lifestyle counseling programs is emphasized. It has been reported that such training before and during ART can significantly increase the chances of success of IVF/ICSI methods [38]. The results of some studies show that providing healthy lifestyle education before starting infertility treatment increases live birth and natural conception rates [39,40]. Factors such as study design, sample size, type, duration and intensity of healthy lifestyle interventions may cause variation in the results obtained. It is important for future studies that these interventions not only include a healthy lifestyle but also that educational programs such as hypnofertility or ISE are combined with a healthy lifestyle and the results are evaluated. Therefore, more research is needed to understand these differences. Future research focusing on large and diverse sample groups and using standardized methods may make IVF/ICSI outcomes more comparable.
This study has some methodological limitations that should be considered. First, the relatively small sample size may have limited the statistical power and affects the generalizability of the findings. Second, the study design does not allow for causal conclusions regarding the relationship between ISE, healthy lifestyle behaviors and fertility readiness. Future studies with larger sample sizes and rigorously designed randomized controlled trials are needed to provide stronger evidence and clarify the potential causal pathways through which ISE may impact reproductive outcomes.
Conclusion
In this study, the presence of FHR was observed in 60% of women in the ISE group and 40% of women in the control group. Although this difference was not statistically significant, it suggests that there may be a clinically significant improvement in early pregnancy outcomes in women receiving ISE. For women diagnosed with infertility, ISE should be personalized and tailored to women’s needs and become a routine practice. An appropriate and professional environment should be created in infertility clinics to successfully implement and effectively deliver ISE to women. Training programs such as ISE should also be offered on mobile platforms to provide easy access to information.
Summary points
•
This study is the first to evaluate the effect of structured infertility support education (ISE) on IVF/ICSI treatment outcomes in women with unexplained infertility.
•
Conducted as a quasi-experimental pretest–posttest study with randomized groups, including women aged 19–45 diagnosed with unexplained infertility.
•
ISE was delivered in three sessions over 15-day intervals, covering body awareness, mind–body perception and lifestyle preparation for pregnancy.
•
Standardized instruments were used: Fertility Readiness Scale, Healthy Lifestyle Behaviors Scale II and post-IVF/ICSI success evaluation form.
•
Post-intervention, the education group showed significant improvements in fertility readiness (hope, awareness, positive emotions and readiness of body and mind).
•
Significant gains were also observed in healthy lifestyle behaviors, including nutrition, physical activity, stress management, interpersonal relationships and spiritual development.
•
A strong positive correlation was found between fertility readiness and healthy lifestyle behaviors after ISE (p < 0.001).
•
Pregnancy outcomes improved: fetal heartbeat was detected in 60% of women in the education group compared with 40%.
•
The intervention highlights the value of psychosocial and behavioral support as a complementary component to medical infertility treatment.
•
Findings suggest that integrating ISE into clinical practice may enhance both psychological well-being and clinical success rates for women undergoing IVF/ICSI.
Author contributions
All the authors critically read the initial manuscript, commented on all parts of the text, and approved the final version of the manuscript. T Tahta: conceptualization, conception and design of study, data collection, writing – original draft, writing – review and editing. Y Kaya: writing – original draft, review and editing. VY Tokgöz: writing – review and editing. Y Aydın: writing – review and editing.
Financial disclosure
The research was completed as a doctoral thesis registered at Eskişehir Osmangazi University Institute of Health Sciences, Department of Nursing in Türkiye, and was supported by Eskişehir Osmangazi University Scientific Research Projects Coordination Unit with the scope of project number TDK-2022-2350, decision number 2022/13, dated 18 November 2022.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
Ethics approval for this study was obtained – please see the Materials and Methods section for details. All procedures performed in this study involving human participants were conducted in compliance with the Declaration of Helsinki. Written informed consent was obtained from all individual participants included in the study.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Reference
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Göker A, Yanikkerem E, Birge O, Kuscu NK. Quality of life in Turkish infertile couples and related factors. Hum. Fertil. 21(3), 195–203 (2018).
2.
Royani Z, Heidari M, Vatanparast M, Yaghmaei F, Sarcheshme AK, Majomerd JK. Predictors of quality of life in infertile couples. J. Menopausal Med. 25(1), 35–40 (2019).
3.
Namavar Jahromi B, Mansouri M, Forouhari S, Poordast T, Salehi A. Quality of life and its influencing factors of couples referred to an infertility center in Shiraz, Iran. Int. J. Fertil. Steril. 12(1), 91 (2018).
4.
Carson SA, Kallen AN. Diagnosis and management of infertility: a review. JAMA 326(1), 65–76 (2021).
5.
Furman I, Charlinn V. Calidad de vida de parejas infértiles en el sector público de Chile. Rev. Med. Chil. 145(11), 1378–1386 (2017).
6.
Fata S, Tokat MA, Doğan ÖE, Okyay RE. Effect of hypnofertility on in vitro fertilization treatment process: case report. Turkish Reproductive Health Association Izmir Symposium June 2-3, 8 (2018).
7.
Garre VFS, Rederiksen Y, Petersen KB. Recommended therapy for psychosocial consequences of infertility and fertility treatment. Ugeskr Laeger 182(11), V08190430 (2020).
8.
Boivin J, Gameiro S. Evolution of psychology and counseling in infertility. Fertil. Steril. 104(2), 251–259 (2015).
9.
Fata S, Tokat MA. Hypnofertility-based nursing care in relieving stress for women with need for fertility support. Biomed. J. Sci. Tech. Res. 33(4), 25946 (2021).
10.
Fata S, Tokat MA. Does hypnofertility-based nursing care affect cortisol levels, fertility preparedness, and pregnancy outcomes in women undergoing in vitro fertilization? A randomized controlled trial. Biol. Res. Nurs. 23(3), 418–429 (2021).
• Demonstrates how hypnofertility-based nursing interventions can positively influence both physiological (cortisol) and fertility outcomes in IVF patients.
11.
Kaya Y, Kizilkaya Beji N, Aydin Y, Hassa H. The effect of health-promoting lifestyle education on the treatment of unexplained female infertility. Eur. J. Obstet. Gynecol. Reprod. Biol. 207, 109–114 (2016).
•• One of the earliest studies to show that structured lifestyle education contributes to improved treatment outcomes in women with unexplained infertility.
12.
Erdemoğlu Ç, Aksoy Derya Y. The effect of hypnofertility on fertility preparedness, stress, and coping with stress in women having in vitro fertilization: a randomized controlled trial. J. Reprod. Infant Psychol. 13, 1–12 (2022).
• Highlights the effectiveness of hypnofertility interventions in reducing stress and enhancing psychological readiness in IVF candidates.
13.
Fata S, Tokat MA. Development of fertility preparedness scale for women receiving fertility treatment. J. Nurs. Res. 28(3), e95 (2020).
14.
Walker SN, Sechrist KR, Pender NJ. Health promotion model-instruments to measure health promoting lifestyle: Health-promoting lifestyle profile (HPLP II). (Adult Version) (1995).
15.
Bahar Z, Beşer A, Gördes N, Ersin F, Kıssal A. Validity and reliability study of the healthy lifestyle behavior scale II. Cumhuriyet Nurs. J. 12(1), 1–13 (2008).
16.
Charnock D, Shepperd S, Needham G, Gann R. DISCERN: an instrument for judging the quality of written consumer health information on treatment choices. J. Epidemiol. Community Health 53, 105–111 (1999).
17.
Gökdoğan F, Kır E, Özcan A, Cerit B, Yıldırım Y, Akbal S. Are educational booklets reliable? 2nd Int. & 9th Natl. Nursing Congress Proceedings, Antalya, Türkiye, 517–521 (2003).
18.
Hart RJ. Physiological aspects of female fertility: role of the environment, modern lifestyle, and genetics. Physiol. Rev. 96(3), 873–909 (2016).
19.
Deyhoul N, Mohamaddoost T, Hosseini M. Infertility-related risk factors: a systematic review. Int. J. Womens Health Reprod. Sci. 5(1), 24–29 (2017).
20.
Bala R, Singh V, Rajender S, Singh K. Environment, lifestyle, and female infertility. Reprod. Sci. 28(3), 617–638 (2021).
21.
Ma M, Guo L, Liu X, Zheng Y, Gu C, Li B. Genetic correlation between female infertility and mental health and lifestyle factors: a linkage disequilibrium score regression study. Health Sci. Rep. 5(5), e797 (2022).
22.
Altıparmak S. The effect of fertility supporting behavior recruiting training given to infertile women to healthy lifestyle behaviors and infertility self-efficacy. [Doctoral Thesis, İnönü University] (2018). Available from: https://tez.yok.gov.tr/UlusalTezMerkezi/
• Doctoral work demonstrating the role of fertility-supportive training in empowering infertile women’s self-efficacy and adoption of healthy lifestyle behaviors.
23.
Fabozzi G, Verdone G, Allori M et al. Personalized nutrition in the management of female infertility: new insights on chronic low-grade inflammation. Nutrients 14(9), 1918 (2022).
24.
van Elten TM, Karsten MDA, Geelen A et al. Preconception lifestyle intervention reduces long-term energy intake in women with obesity and infertility: a randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 16(3), (2019).
25.
Hill B, McPhie S, Fuller-Tyszkiewicz M, Gillman M, Skouteris H. Psychological health and lifestyle management preconception and in pregnancy. Semin. Reprod. Med. 34(2), 121–128 (2016).
26.
Yanık D, Kavak Budak F. The effect of positive psychotherapy-based training on stigma and self-efficacy in women receiving infertility treatment. J. Am. Psychiatr. Nurses Assoc. 30(2), 382–396 (2024).
27.
Bornstein M, Gipson JD, Failing G, Banda V, Norris A. Individual and community-level impact of infertility-related stigma in Malawi. Soc. Sci. Med. 251, 112910 (2020).
28.
Rouchou B. Consequences of infertility in developing countries. Perspect. Public Health 133(3), 174–179 (2013).
29.
Oostingh EC, Koster MPH, van Dijk MR et al. First effective mHealth nutrition and lifestyle coaching program for subfertile couples undergoing in vitro fertilization treatment: a single-blinded multicenter randomized controlled trial. Fertil. Steril. 114, 945–954 (2020).
30.
Boedt T, Vanhove AC, Vercoe MA, Matthys C, Dancet E, Lie Fong S. Preconception lifestyle advice for people with infertility. Cochrane Database Syst. Rev. 4(4), CD008189 (2021).
•• A high-level systematic review providing strong evidence that preconception lifestyle interventions are crucial in infertility management and outcomes.
31.
Ng KYB, Wellstead S, Cheong Y, Macklon NA. Randomised controlled trial of a personalised lifestyle coaching application in modifying periconceptional behaviours in women suffering from reproductive failures (iPLAN trial). BMC Womens Health 18(1), 196 (2018).
32.
Boedt T, Matthys C, Lie Fong S, De Neubourg D, Vereeck S, Seghers J et al. Systematic development of a mobile preconception lifestyle programme for couples undergoing IVF: the PreLiFe-programme. Hum. Reprod. 36(9), 2493–2505 (2021).
33.
Chow KM, Cheung M, Cheung IK. Psychosocial interventions for infertile couples: a critical review. J. Clin. Nurs. 25(15–16), 2101–2113 (2016).
34.
Borghi L, Menichetti J, Vegni E. Patient-centered infertility care: current research and future perspectives on psychosocial, relational, and communication aspects. Front. Psychol. 25(12), 712485 (2021).
35.
de Castro MHM, Mendonça CR, Noll M, de Abreu Tacon FS, do Amaral WN. Psychosocial aspects of gestational grief in women undergoing infertility treatment: a systematic review. Int. J. Environ. Res. Public Health 18(24), 13143 (2021).
36.
Hahs-Vaughn DL. Foundational methods: descriptive statistics: bivariate and multivariate data. Int. Encycl. Educ. 734–750 (2023).
37.
Rooney KL, Domar AD. The impact of lifestyle behaviors on infertility treatment outcome. Curr. Opin. Obstet. Gynecol. 26(3), 181–185 (2014).
38.
Zeinab H, Zohreh S, Samadaee Gelehkolaee K. Lifestyle and outcomes of assisted reproductive techniques: a narrative review. Glob. J. Health Sci. 7(5), 11–22 (2015).
39.
Hunter E, Avenell A, Maheshwari A, Stadler G, Best D. The effectiveness of weight-loss lifestyle interventions for improving fertility in women and men with overweight or obesity and infertility: a systematic review update. Obes. Rev. 22(12), e13325 (2021).
40.
Hoek A, Wang Z, van Oers AM, Groen H, Cantineau AEP. Effects of preconception weight loss after lifestyle intervention on fertility outcomes and pregnancy complications. Fertil. Steril. 118(3), 456–462 (2022).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 30 September 2025
Accepted: 14 January 2026
Published online: 18 February 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The effect of infertility support education on treatment outcomes in women with unexplained infertility. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0159
Export citation
Select the citation format you wish to export for this article or chapter.