Treatment burden and healthcare resource utilization in patients with chronic rhinosinusitis with nasal polyps who did or did not undergo functional endoscopic sinus surgery: a US real-world retrospective cohort study
Publication: Journal of Comparative Effectiveness Research
Abstract
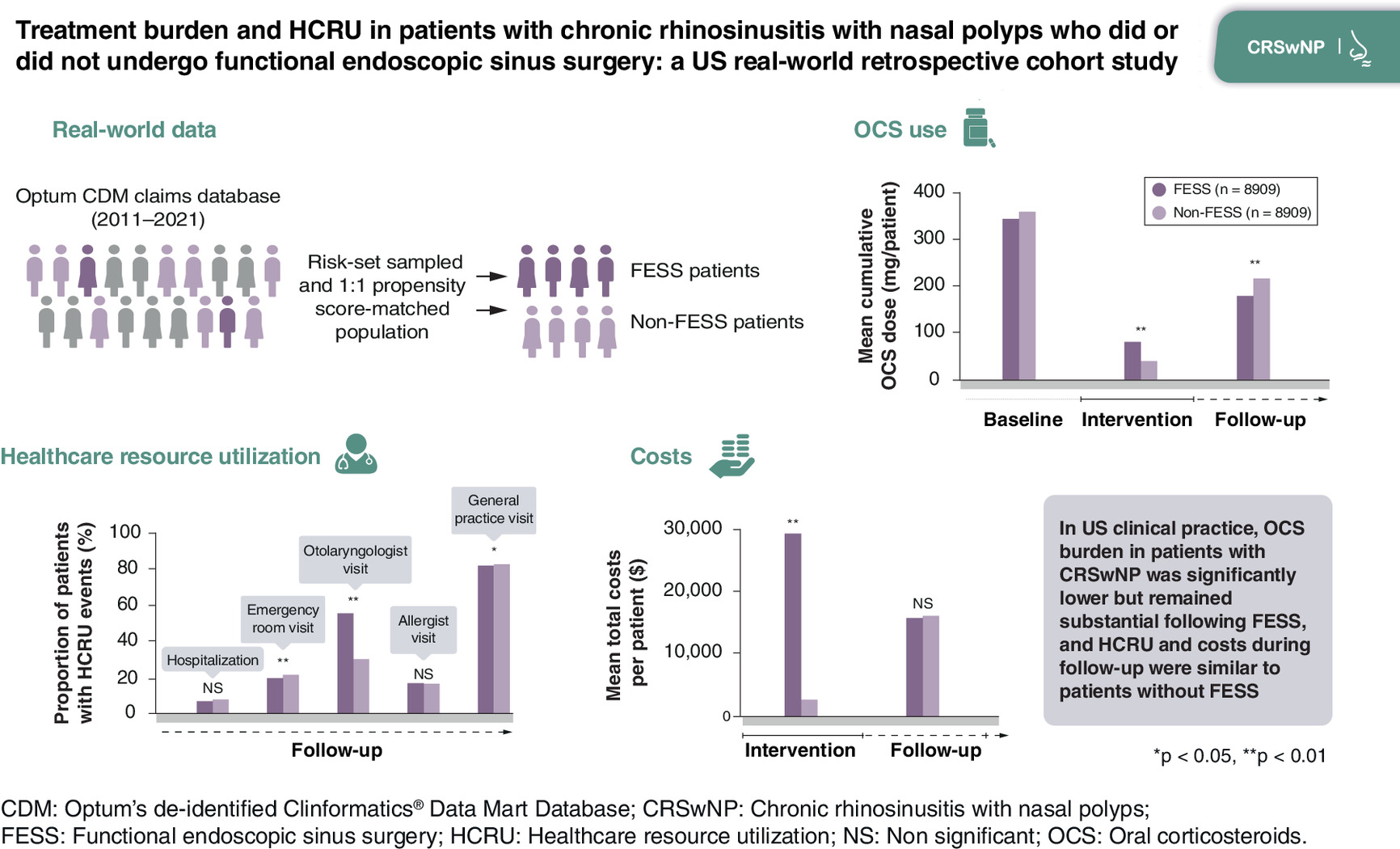
Aim: To compare oral corticosteroid (OCS) burden and healthcare resource utilization (HCRU) in patients with chronic rhinosinusitis with nasal polyps undergoing functional endoscopic sinus surgery (FESS; intervention) versus not undergoing FESS. Materials & methods: Retrospective cohort study using US claims data (Optum’s de-identified Clinformatics® Data Mart Database; 2011–2021). Groups were propensity score (PS) matched to adjust for confounding. OCS burden (cumulative dose in mg prednisone equivalents) and HCRU were assessed during baseline (365 days pre-index), intervention (days 0–44), and follow-up (days 45–365); costs during intervention and follow-up. Results: Before PS-matching, both groups had substantial comorbidity burden (>50% allergic rhinitis; >25% asthma) and over half of patients had used OCS (65% [FESS] vs 52% [non-FESS]; p < 0.01). After PS-matching (n = 8909 per group), OCS cumulative dose during follow-up was 18% lower among FESS versus non-FESS patients (mean difference: -40 mg per patient [95% CI: -57, -23; p < 0.01]). Similar proportions of patients filled OCS prescriptions during follow-up (35% [FESS], 36% [non-FESS]) and in these patients, OCS burden remained high (mean [SD] cumulative dose 521 [786] vs 612 [906] mg, respectively). Mean total healthcare costs per patient during the intervention period were $28,832 (FESS) and $2537 (non-FESS), but similar during follow-up ($15,659 and $15,926, respectively). HCRU was similar in follow-up, except more FESS patients visited an otolaryngologist (57% vs 32%, p < 0.01). Conclusion: In US clinical practice, OCS burden in patients with chronic rhinosinusitis with nasal polyps was significantly lower but remained substantial following FESS, and HCRU and costs during follow-up were similar to matched patients without FESS.
Plain language summary
What was the aim of this research?
To compare the burden of medications, visits, procedures and costs between patients with chronic rhinosinusitis with nasal polyps who did nor did not undergo polyp removal surgery.
How was the research carried out?
Anonymized administrative health-claim data were analyzed through the year before and up to 3 years after surgery. To allow for a fair comparison between patients who did and did not have surgery, patients were matched according to a range of factors including age, gender, race and prior use of medications.
What were the results?
Between 45 and 365 days after surgery, patients had an 18% lower average cumulative dose of oral corticosteroids (OCS) compared with patients who did not have surgery. The proportion of patients with prescriptions for OCS was similar between the surgery and nonsurgery groups (35% and 36%, respectively). Similarly, there was little difference in the use of other medications. Otolaryngologist visits were more common for patients who had surgery than those who did not. Costs were similar after surgery between the surgery and no-surgery groups through 3 years of follow-up.
What do the results of the study mean?
This study found that OCS use was lower over the 3 years after sinus surgery but remained substantial for both the surgery and nonsurgery patient groups. Further, surgery only marginally reduced costs during the follow-up period. These results serve as evidence for policymakers and healthcare providers when deciding the most cost-effective way to treat patients with chronic rhinosinusitis with nasal polyps.
Graphical and video abstract
Chronic rhinosinusitis with nasal polyps (CRSwNP) is an inflammatory disease of the nose and paranasal sinuses that is associated with significant clinical burden and poor health-related quality of life (HRQoL) due to its negative impact on mental health, sleep, work and productivity [1–3]. CRSwNP is also associated with significant economic burden in terms of direct and indirect costs and overall healthcare resource utilization (HCRU) [4–8].
Recommended first-line treatment for CRSwNP includes saline washes and intranasal corticosteroids, with short courses of oral corticosteroids (OCS) introduced for patients with severe disease [9]. A recent US claims database analysis found that 61% of patients with CRSwNP received OCS over a 2-year period (79% in patients with coexisting asthma) [10]. However, OCS are associated with a range of potential short-term and long-term adverse effects, including complications such as infections, cardiovascular disease, venous thromboembolism and fractures [11–13], restricting their chronic use [14]. In patients not responding to medical therapy, functional endoscopic sinus surgery (FESS) may be considered [9]. FESS is a generally well-tolerated procedure aiming to restore sinus ventilation and normal sinus function, and to facilitate local access for intranasal corticosteroids post-surgery [15,16]. Although FESS alleviates symptoms in most patients, recurrence is common [17,18], which may result in the need for additional surgeries and/or courses of OCS and other medications, with attendant increased healthcare costs. Prior research indicates that patients continue to use OCS post-surgery, and OCS burden may remain high [19,20]. However, real-world evidence on OCS use and HCRU in patients with CRSwNP who undergo FESS compared with those who do not is limited.
The primary objective of this real-world study was to describe and compare OCS use among patients with CRSwNP who underwent FESS versus those who did not. Secondary objectives were to describe and compare the burden of other CRSwNP-related medications and procedures, as well as HCRU and costs, in these groups of patients.
Materials & methods
Study design & patients
This was a retrospective, observational study using Optums de-identified Clinformatics® Data Mart Database (CDM) claims data from 1 November 2011 to 31 August 2021. The database included commercially insured individuals and Medicare Advantage enrollees but did not capture uninsured patients or those covered by Medicaid. The analyzed population included patients with CRSwNP who underwent FESS (exposed [FESS] group) or did not undergo FESS (referent [non-FESS] group). Exposed patients entered the cohort on the date of their first recorded FESS (index date) between 1 November 2012 and 31 August 2020 and were 1:4 matched on index date to referent patients using risk-set sampling. This matching ensured that exposed and referent patients were sampled from the same time period, controlling for temporal changes such as the introduction of biologics and evolving FESS practices. Eligible patients were aged ≥18 years at the index date, had a CRSwNP diagnosis within the past 12 months (defined as ≥1 claim for chronic rhinosinusitis [CRS] [International Classification of Disease (ICD)-9 dx code: 473.x; ICD-10 dx code: J32.x] and ≥1 claim for NP [ICD-9 dx code: 471.x; ICD-10 dx code: J33.x] at least 1–365 days apart, within ≤365 days prior to and inclusive of the index date) (see Supplementary Material for list of procedural codes), and ≥12 months of health plan enrollment before and after the index date. Patients were excluded if in the year prior to the index date they had FESS or polypectomy, use of biologics or a diagnosis of nasal or sinus cancer. Patients were also excluded if they had FESS in follow-up; this was to avoid a potential source of artificial imbalance in follow-up time between groups due to censoring on post-index FESS.
The study design is illustrated in Supplementary Figure 1: the baseline period extended to 365 days pre-index; the intervention period covered days 0–44 starting from index date; and the follow-up period extended from days 45–365 post-index. Consistent with published literature, the 45-day period for the intervention was chosen to separate outcomes related to the surgical intervention itself (i.e., the index FESS event) and immediate post-operative healing/debridement in the exposed group [8].
Study objectives & end points
The primary objective was to describe and compare real-world OCS use among patients with CRSwNP who did versus did not undergo FESS. The primary end points were cumulative prednisone-equivalent OCS dose during follow-up (mg per patient); proportion of patients with any OCS use; number of OCS prescriptions filled per patient; and average daily prednisone-equivalent OCS dose. The secondary objectives were to compare real-world HCRU, costs and treatment burden and procedures related to CRSwNP in the FESS and non-FESS groups.
Assessments
Patient demographics, comorbidities and medications were assessed during the baseline period. The comorbidities assessed are listed in the Supplementary Material. OCS use and all-cause HCRU were evaluated during the baseline, intervention and follow-up periods; all-cause costs were assessed during the intervention and follow-up periods.
Statistical analyses
Sample size calculations were performed for the primary study end point of cumulative OCS dose in mg of prednisone equivalents. Calculations used 225.52 (611.2) mg as the mean (standard deviation [SD]) cumulative OCS dose in prednisone equivalents, derived from a combined sample of exposed and referent patients in CDM who met the study eligibility criteria. At 80% power and assuming an α = 0.05, a minimum total sample size of 5125 exposed and 5125 referent patients was required to detect a difference of 15% in cumulative OCS dose between the study groups.
All study end points were compared between the FESS and non-FESS groups through baseline-adjusted analyses using 1:1 propensity-score (PS) matching to control for confounding. The PS was defined as the predicted probability of receiving the treatment of interest (i.e., FESS) conditional on baseline covariates. A PS was derived for each patient using a multivariate logistic regression. Covariates included in the PS model were age, gender, race, insurance type, household income range, education level, baseline use of OCS and other treatments, comorbidities and baseline HCRU. Additional details of the PS-matching and full list of covariates included in the final model are provided in the Supplementary Material. The magnitude of difference in baseline characteristics between groups was expressed as absolute standard difference.
Primary end points were summarized using descriptive statistics. For OCS burden and cost, differences in means during the intervention and follow-up periods were estimated using a two-part model, consisting of a logistic model to estimate the odds ratio (OR) of having a nonzero value and a Gamma generalized linear model with log link to estimate the mean difference in nonzero values. Results from both parts of the model were combined to estimate the overall mean difference. The 95% CI and p-value for the overall mean difference were calculated based on 10,000 bootstrapped samples. For all-cause HCRU end points, differences between groups were assumed to be associated with the FESS procedure. Hospitalizations were measured by the number of inpatient admissions and cumulative inpatient days. Outpatient, emergency room, and specialist visits were calculated based on the number of events on different days, allowing a maximum of one event per day to reduce the possibility of overestimating HCRU. Differences in means for HCRU were estimated from generalized linear models with an identity link and negative binomial error distribution, with 95% CI. For treatment and procedure burden end points, differences between the two groups were assessed using ORs and 95% CI. Missing data were not imputed. Feasibility analyses indicated the mean daily OCS dose in prednisone equivalents was ≤48 mg for 95% of patients meeting the study eligibility criteria. To exclude outliers due to errors existing in the raw data, daily prednisone-equivalent values >100 mg were reassigned as missing.
Results
Cohort attrition
A total of 43,751 patients met the study eligibility criteria (9305 [FESS group] and 34,446 [non-FESS group]). The final PS-matched population comprised 17,818 patients (8909 in each group) (see Figure 1).
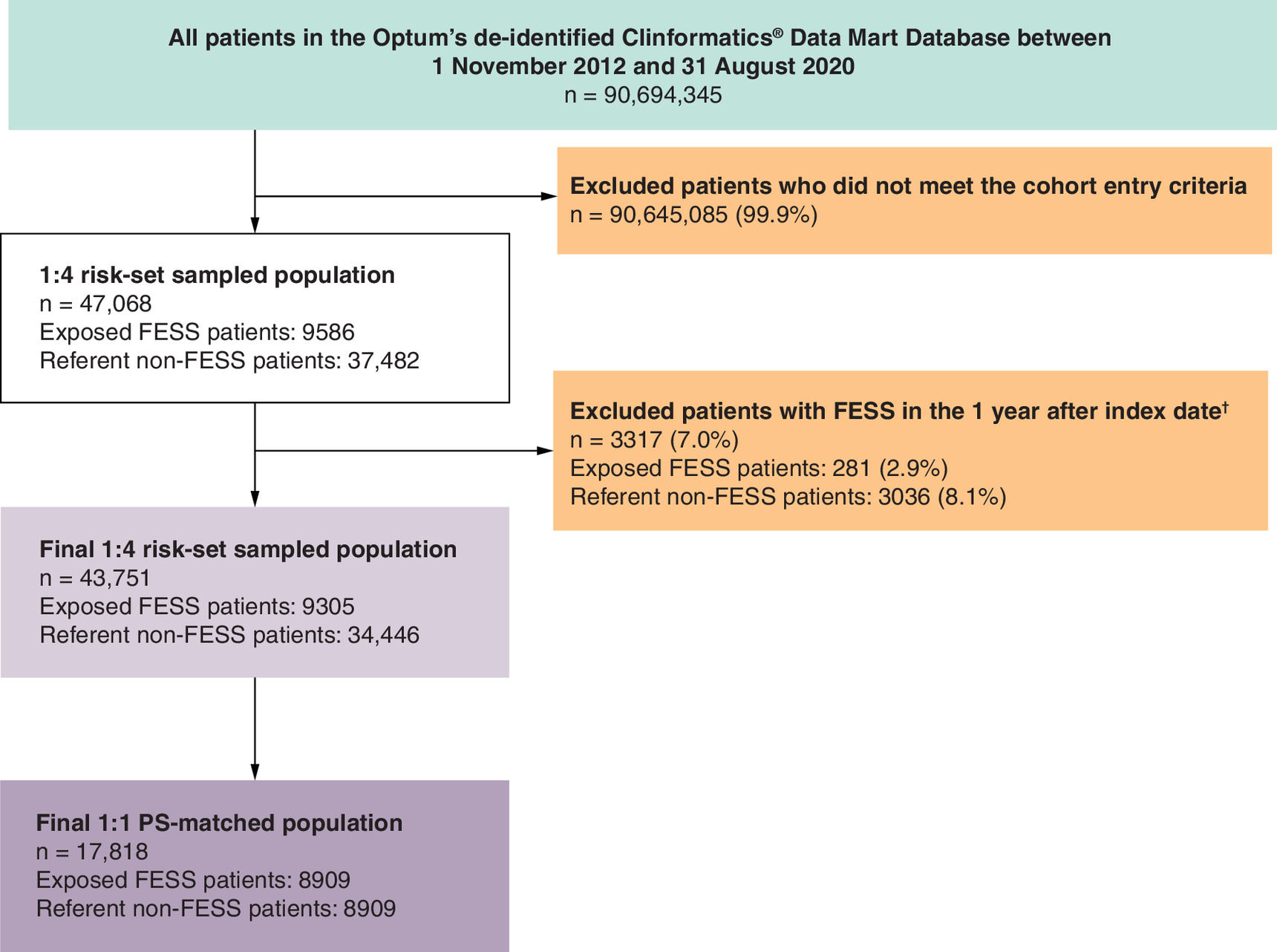
Figure 1. Cohort attrition.
†Owing to the imbalance between the proportion of patients excluded by this criterion, demographics and baseline characteristics were compared between referent patients with vs without post-index FESS to assess potential selection bias. Differences were not large. Referent patients with post-index FESS were slightly younger than patients with no surgery after index (mean [SD] age 53 [16] vs 57 [17] years, respectively), less likely to have Medicare coverage (32% vs 41%), and more likely to have asthma (34% vs 30%), acute sinusitis (41% vs 34%), and baseline OCS use (66% vs 52%). All other baseline characteristics were similar between those with vs without post-index FESS.
FESS: Functional endoscopic sinus surgery; PS: Propensity score.
Patient characteristics & baseline treatment burden
Demographics and comorbidities in the risk-set sampled population before PS matching are shown in Supplementary Table 1. Overall, 57% of all patients were male and 75% were White. Patients in the FESS group were younger on average than patients in the non-FESS group (52 vs 57 years); 29% versus 39%, respectively, were ≥65 years old. More patients in the FESS group had commercial insurance (69% vs 59%). Patients in both groups had a substantial burden of comorbidities, including allergic rhinitis (52% [FESS group] and 53% [non-FESS group]), acute sinusitis (47% and 34%), asthma (26% and 30%), sleep disorders (21% and 20%), anxiety (14% and 14%) and depression (13% and 12%).
More than half of the patients in each group used OCS, although OCS use was significantly greater (p < 0.01) among FESS than non-FESS patients across the 1-year baseline period (65% vs 52%, respectively) and during the 60 days (41% vs 18%) and 30 days (29% vs 10%) preceding index (Supplementary Table 2). Mean annual cumulative OCS dose was 78 (95% CI: 64, 91; p < 0.01) mg higher per patient in the FESS versus non-FESS group; among baseline OCS users, the difference was 16 (-5, 37; p = 0.11) mg. The FESS group had greater use of oral antibiotics than the non-FESS group (45% vs 39%; p < 0.01), but less frequent use of leukotriene receptor antagonists (LTRAs) (21% vs 25%; p < 0.01) and inhaled corticosteroids (9% vs 12%; p < 0.01) (Supplementary Table 2).
After PS matching, demographics and baseline characteristics including baseline OCS use were well balanced between FESS and non-FESS patients (Tables 1 & 2). While HCRU was well balanced between groups overall due to PS matching, more FESS than non-FESS patients had an otolaryngologist visit in baseline (85% vs 72%, respectively). The greater likelihood of FESS patients visiting an otolaryngologist in baseline was similar in the risk-set sampled population before PS matching (85% vs 70%).
| FESS (n = 8909) | No FESS (n = 8909) | ASD post-PS matching | ASD pre-PS matching | |
|---|---|---|---|---|
| Demographics | ||||
| Age (years) | 0.004 | 0.264 | ||
| Mean (SD) | 52.95 (16.42) | 53.01 (16.71) | ||
| Median (IQR) | 54 (41, 67) | 53 (40, 67) | ||
| Age category (years), n (%) | 0.020 | 0.245 | ||
| 18–34 | 1393 (15.6) | 1404 (15.8) | ||
| 35–44 | 1463 (16.4) | 1489 (16.7) | ||
| 45–54 | 1721 (19.3) | 1750 (19.6) | ||
| 55–64 | 1674 (18.8) | 1608 (18.0) | ||
| ≥65 | 2658 (29.8) | 2658 (29.8) | ||
| Gender, n (%)† | 0.008 | 0.047 | ||
| Female | 3689 (41.4) | 3726 (41.8) | ||
| Male | 5219 (58.6) | 5182 (58.2) | ||
| Race, n (%) | 0.014 | 0.071 | ||
| Asian | 322 (3.6) | 337 (3.8) | ||
| Black or African American | 663 (7.4) | 667 (7.5) | ||
| Hispanic | 768 (8.6) | 789 (8.9) | ||
| White | 6836 (76.7) | 6790 (76.2) | ||
| Missing/unknown | 320 (3.6) | 326 (3.7) | ||
| Insurance type, n (%) | 0.009 | 0.209 | ||
| Commercial | 6102 (68.5) | 6064 (68.1) | ||
| Medicare | 2807 (31.5) | 2845 (31.9) | ||
| Household income categories, n (%) | 0.020 | 0.036 | ||
| <$40k | 372 (4.2) | 369 (4.1) | ||
| $40k–49k | 123 (1.4) | 122 (1.4) | ||
| $50k–59k | 173 (1.9) | 157 (1.8) | ||
| $60k–74k | 233 (2.6) | 237 (2.7) | ||
| $75k–99k | 349 (3.9) | 351 (3.9) | ||
| $100k+ | 1020 (11.4) | 983 (11.0) | ||
| Missing/unknown | 6639 (74.5) | 6690 (75.1) | ||
| Education level categories, n (%) | 0.014 | 0.043 | ||
| Less than 12th grade | 20 (0.2) | 16 (0.2) | ||
| High school diploma | 1584 (17.8) | 1571 (17.6) | ||
| Less than bachelor’s degree | 4884 (54.8) | 4905 (55.1) | ||
| Bachelor’s degree or above | 2285 (25.6) | 2272 (25.5) | ||
| Missing/unknown | 136 (1.5) | 145 (1.6) | ||
| Comorbidities | ||||
| Type 2 comorbidities, n (%) | ||||
| Asthma | 2282 (25.6) | 2248 (25.2) | 0.009 | 0.091 |
| Allergic conjunctivitis | 340 (3.8) | 352 (4.0) | 0.007 | 0.056 |
| Allergic rhinitis | 4622 (51.9) | 4681 (52.5) | 0.013 | 0.023 |
| Atopic dermatitis | 106 (1.2) | 106 (1.2) | 0.000 | 0.036 |
| Chronic spontaneous urticaria | 100 (1.1) | 113 (1.3) | 0.013 | 0.013 |
| Eosinophilic esophagitis | 32 (0.4) | 29 (0.3) | 0.006 | 0.005 |
| Food allergy | 123 (1.4) | 121 (1.4) | 0.002 | 0.023 |
| Other comorbidities, n (%) | ||||
| Charlson comorbidity index | 0.008 | 0.146 | ||
| 0 | 6086 (68.3) | 6115 (68.6) | ||
| 1 | 1843 (20.7) | 1815 (20.4) | ||
| 2 | 537 (6.0) | 536 (6.0) | ||
| ≥3 | 443 (5.0) | 443 (5.0) | ||
| Acute sinusitis‡ | 4046 (45.4) | 4091 (45.9) | 0.010 | 0.282 |
| Anxiety | 1228 (13.8) | 1253 (14.1) | 0.008 | 0.002 |
| COPD | 825 (9.3) | 829 (9.3) | 0.002 | 0.077 |
| Cystic fibrosis | 39 (0.4) | 43 (0.5) | 0.007 | 0.007 |
| Depression | 1141 (12.8) | 1154 (13.0) | 0.004 | 0.025 |
| Diabetes | 1270 (14.3) | 1256 (14.1) | 0.005 | 0.069 |
| GERD | 755 (8.5) | 791 (8.9) | 0.014 | 0.043 |
| Obesity | 338 (3.8) | 322 (3.6) | 0.010 | 0.010 |
| Osteoporosis | 829 (9.3) | 804 (9.0) | 0.010 | 0.104 |
| Pneumonia | 348 (3.9) | 367 (4.1) | 0.011 | 0.020 |
| Rheumatoid arthritis | 190 (2.1) | 199 (2.2) | 0.007 | 0.004 |
| Sleep disorders§ | 1879 (21.1) | 1903 (21.4) | 0.007 | 0.028 |
†
Rows containing cells with 10 or fewer observations in either treatment group were redacted.
‡
Included acute maxillary, frontal, ethmoidal and sphenoidal sinusitis; unspecified and other acute sinusitis; acute pansinusitis.
§
Including but not limited to insomnia, somnambulism, night terrors, nightmare disorder, hypersomnia, circadian rhythm sleep disorder, sleep apnea, narcolepsy, parasomnia and sleep-related movement disorders.
ASD: Absolute standard difference; COPD: Chronic obstructive pulmonary disease; CRSwNP: Chronic rhinosinusitis with nasal polyps; FESS: Functional endoscopic sinus surgery; GERD: Gastroesophageal reflux disease; IQR: Interquartile range; PS: Propensity score; SD: Standard deviation.
| FESS (n = 8909) | No FESS (n = 8909) | ASD post-PS matching | ASD pre-PS matching | |
|---|---|---|---|---|
| Baseline OCS use, n (%) | ||||
| OCS anytime in baseline | 5636 (63.3) | 5728 (64.3) | 0.021 | 0.255 |
| OCS within 30 days before index | 2457 (27.6) | 1541 (17.3) | 0.248† | 0.475 |
| OCS within 60 days before index | 3508 (39.4) | 2694 (30.2) | 0.193† | 0.510 |
| Acute OCS use, n (%)‡ | 79 (0.9) | 80 (0.9) | 0.001 | 0.031 |
| Chronic OCS use, n (%)‡ | 229 (2.6) | 248 (2.8) | 0.013 | 0.004 |
| Cumulative OCS dose (mg) per patient | 0.023 | 0.126 | ||
| Mean (SD) | 342.10 (621.55) | 356.82 (664.86) | ||
| Median (IQR) | 150 (0, 435) | 147 (0, 420) | ||
| Cumulative OCS days' supply per patient | 0.056 | 0.057 | ||
| Mean (SD) | 14.65 (32.21) | 16.71 (39.84) | ||
| Median (IQR) | 6 (0, 17) | 6 (0, 16) | ||
| OCS fills per patient | 0.017 | 0.246 | ||
| Mean (SD) | 1.32 (1.56) | 1.35 (1.70) | ||
| Median (IQR) | 1 (0, 2) | 1 (0, 2) | ||
| Subgroup: baseline OCS users | ||||
| Number of patients in subgroup | 5636 | 5728 | ||
| Cumulative OCS dose (mg) per patient | 0.020 | 0.023 | ||
| Mean (SD) | 540.32 (709.00) | 554.98 (759.98) | ||
| Median (IQR) | 350 (200, 640) | 315 (180, 605) | ||
| Cumulative OCS days' supply per patient | 0.045 | 0.066 | ||
| Mean (SD) | 23.16 (37.98) | 25.98 (47.20) | ||
| Median (IQR) | 13 (6, 24) | 12 (6, 23) | ||
| OCS fills per patient | 0.006 | 0.139 | ||
| Mean (SD) | 2.09 (1.49) | 2.10 (1.71) | ||
| Median (IQR) | 2 (1, 3) | 1 (1, 3) | ||
| Medications for CRSwNP§, n (%) | ||||
| Intranasal corticosteroids | 795 (8.9) | 819 (9.2) | 0.009 | 0.084 |
| Inhaled corticosteroids | 838 (9.4) | 870 (9.8) | 0.012 | 0.098 |
| Leukotriene receptor antagonists | 1881 (21.1) | 1889 (21.2) | 0.002 | 0.088 |
| Antihistamines | 1895 (21.3) | 1935 (21.7) | 0.011 | 0.026 |
| NSAIDs | 2177 (24.4) | 2187 (24.5) | 0.003 | 0.027 |
| Oral antibiotics | 3910 (43.9) | 3943 (44.3) | 0.007 | 0.111 |
| Oral macrolides¶ | 2795 (31.4) | 2913 (32.7) | 0.028 | 0.079 |
| HCRU#, mean (SD) | ||||
| Hospitalizations, n | 0.09 (0.38) | 0.10 (0.38) | 0.009 | 0.072 |
| Inpatient days, n | 0.45 (2.58) | 0.51 (3.58) | 0.017 | 0.070 |
| ER visits, n | 0.42 (1.07) | 0.43 (1.04) | 0.010 | 0.036 |
| Outpatient visits, n | 17.22 (11.96) | 17.36 (13.64) | 0.010 | 0.060 |
| Ambulatory visits, n | 16.84 (11.66) | 16.98 (13.27) | 0.012 | 0.058 |
| Unique drug fills (by generic name), n | 9.70 (6.70) | 9.85 (6.88) | 0.022 | 0.083 |
| Days since the first CRS or NP claim in the database, n (%) | 0.018 | 0.857 | ||
| <92 | 4733 (53.1) | 4666 (52.4) | ||
| ≥92–<183 | 2011 (22.6) | 2071 (23.2) | ||
| ≥183–<274 | 909 (10.2) | 916 (10.3) | ||
| ≥274 | 1256 (14.1) | 1256 (14.1) | ||
†
ASD not balanced across groups as these variables were not included in PS models. It is common practice for OCS to be prescribed in preparation of FESS.
‡
Acute and chronic OCS use defined as cumulative days' supply of <3 days or >30 days, respectively.
§
Some medications, such as inhaled corticosteroids, NSAIDs and antihistamines, may be underestimated in the pharmacy claims data due to over-the-counter availability.
¶
Oral macrolide use reported among all patients; approximately 73% of antibiotic users were treated with macrolides.
#
HCRU events are given per patient for all patients in the group.
ASD: Absolute standard difference; CRS: Chronic rhinosinusitis; CRSwNP: Chronic rhinosinusitis with nasal polyps; FESS: Functional endoscopic sinus surgery; HCRU: Healthcare resource utilization; IQR: Interquartile range; NP: Nasal polyp; NSAID: Non-steroidal anti-inflammatory drug; OCS: Oral corticosteroid; PS: Propensity score; SD: Standard deviation.
OCS burden during the intervention period (PS-matched population)
During the intervention period, more FESS than non-FESS patients used OCS (35% vs 16%, respectively), leading to a mean difference in cumulative OCS dose of 42 (95% CI: 37, 46; p < 0.01) mg prednisone equivalents higher per patient in the FESS group than the non-FESS group. However, among patients who used OCS, the cumulative dose per patient was lower in FESS patients than in non-FESS patients: mean (SD) 245 (221) mg versus 271 (273) mg (Table 3).
| Baseline period (365 days pre-index) | Intervention period (index to 45 days post-index) | Follow-up period (45–365 days post-index) | ||||
|---|---|---|---|---|---|---|
| FESS (n = 8909) | No FESS (n = 8909) | FESS (n = 8909) | No FESS (n = 8909) | FESS (n = 8909) | No FESS (n = 8909) | |
| Cumulative OCS dose per patient† | 342 (622) | 357 (665) | 85 (175) | 44 (148) | 179 (523) | 219 (616) |
| Days' supply (number of days) | 15 (32) | 17 (40) | 4 (8) | 2 (7) | 9 (30) | 11 (38) |
| Proportion of patients with OCS use | 63.3% | 64.3% | 35.0% | 16.2% | 34.6% | 36.0% |
| Cumulative OCS dose† among users‡ | 540 (709) | 555 (760) | 245 (221) | 271 (273) | 521 (786) | 612 (906) |
| Fills among users, n‡ | 2.09 (1.49) | 2.10 (1.71) | 1.18 (0.45) | 1.23 (0.54) | 2.14 (2.01) | 2.42 (2.40) |
| Cumulative days' supply among users‡ (number of days) | 23 (38) | 26 (47) | 11 (9) | 13 (12) | 25 (47) | 32 (57) |
Data are mean (standard deviation) unless otherwise stated. Index is the date of FESS (FESS group) or risk-set matching (non-FESS group).
†
Dose was reported as mg per patient in prednisone equivalents. Daily dose of >100 mg was recoded as missing.
‡
Data are for the patients who had OCS use during the denoted study period.
CRSwNP: Chronic rhinosinusitis with nasal polyps; FESS: Functional endoscopic sinus surgery; OCS: Oral corticosteroid; PS: Propensity score.
OCS burden during the follow-up period (PS-matched population)
Among all patients, the mean (SD) cumulative OCS dose per patient was 179 (523) mg in the FESS group versus 219 (616) mg in the non-FESS group (mean difference in cumulative dose: -40 [95% CI: -57, -23; p < 0.01] mg), corresponding to an 18% difference in OCS burden. FESS patients had an average of 3 (95% CI: -4, -2; p <0.01) fewer cumulative days’ supply of OCS versus non-FESS patients (mean [SD]: 9 [30] vs 11 [38]).
During the follow-up period, similar proportions of patients used OCS in the FESS and non-FESS groups (35% and 36%, respectively) (Table 3). Among OCS users, mean (SD) cumulative OCS dose per patient was 521 (786) mg in the FESS group versus 612 (906) mg in the non-FESS group. Mean (SD) cumulative OCS days’ supply per OCS user was 25 (47) days and 32 (57) days in the FESS and non-FESS groups, respectively.
Among baseline OCS users, the mean (SD) change in cumulative OCS dose from baseline to follow-up was -257 (723) mg in the FESS group and -203 (718) mg in the non-FESS group; FESS patients had an additional average decrease in cumulative OCS dose of 54 (95% CI: 27, 80) mg from baseline to follow-up compared with non-FESS patients. More than three-quarters of baseline OCS users in both groups had a decrease in cumulative dose from baseline to follow-up (Supplementary Table 3).
Medication & procedure burden during the follow-up period (PS-matched population)
During the follow-up period, use of CRSwNP-related medications was similar in the PS-matched FESS and non-FESS groups, except for inhaled corticosteroids (used by 14% vs 8% of patients, respectively; OR 1.84 [95% CI: 1.67, 2.02]; p < 0.01) and oral antibiotics (28% vs 30%; OR 0.89 [0.84, 0.95]; p < 0.01) (Figure 2). Non-steroidal anti-inflammatory drugs (NSAIDs) were used by 22% versus 23% of FESS versus non-FESS patients; LTRAs were used by 22% versus 20%, respectively. Approximately 1% of each group used biologics.
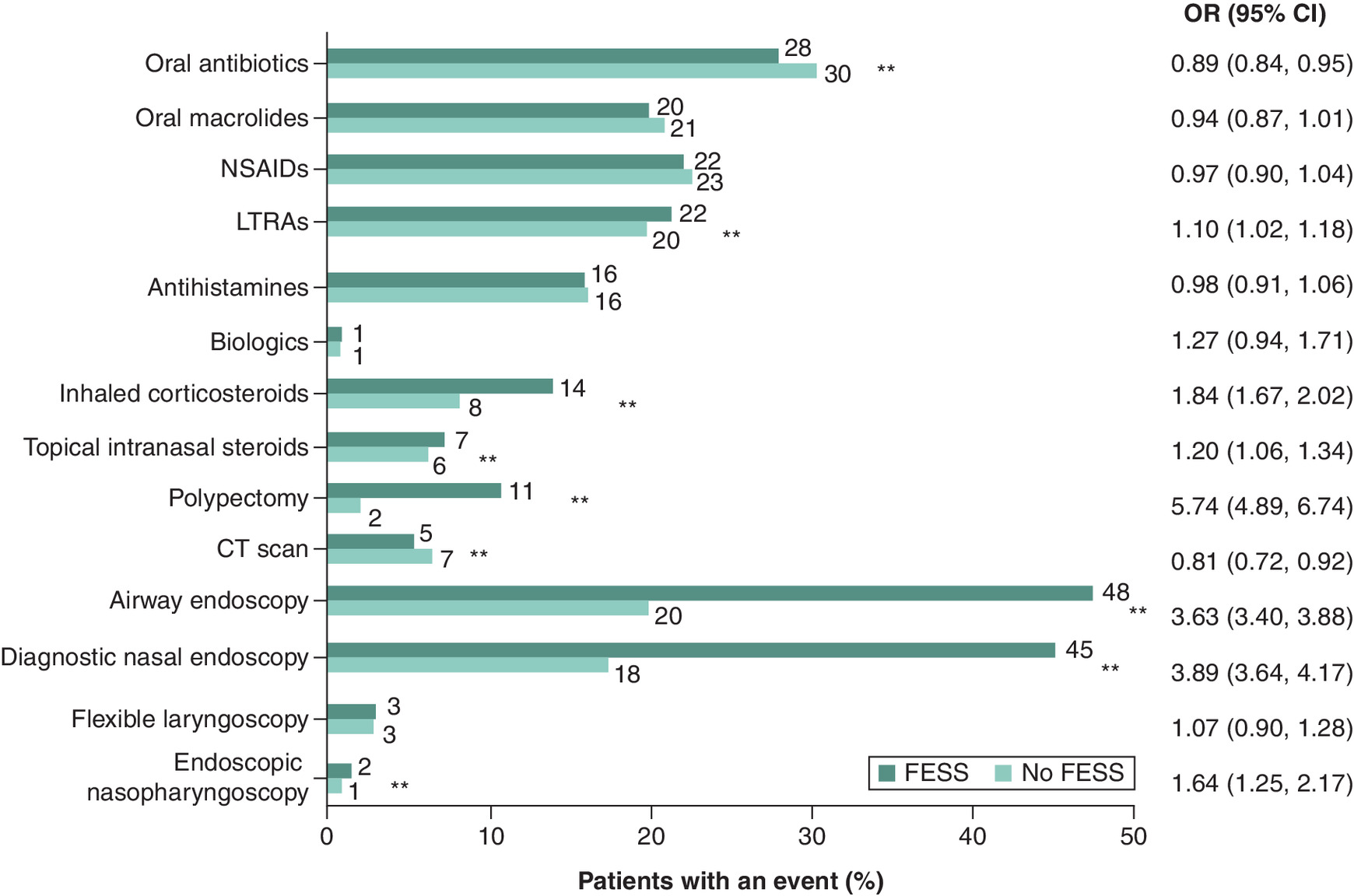
Figure 2. Treatment and procedure burden during the follow-up period in the propensity score-matched population of patients with chronic rhinosinusitis with nasal polyps with functional endoscopic sinus surgery versus no functional endoscopic sinus surgery.
**p < 0.01.
CT: Computed tomography; FESS: Functional endoscopic sinus surgery; LTRA: Leukotriene receptor antagonist; NSAID: Non-steroidal anti-inflammatory drug; OR: Odds ratio.
Additionally, more FESS than non-FESS patients had a polypectomy (11% vs 2%; OR 5.74 [95% CI: 4.89, 6.74]; p < 0.01) and diagnostic nasal endoscopy (45% vs 18%; 3.89 [3.64, 4.17]; p < 0.01). Fewer FESS than non-FESS patients had a computed tomography scan (5% vs 7%; 0.81 [0.72, 0.92]; p < 0.01) (Figure 2).
HCRU & costs (PS-matched population)
During follow-up, HCRU was similar between the PS-matched groups, except that more FESS than non-FESS patients visited an otolaryngologist (57% vs 32%; p < 0.01) (Figure 3). The mean number of otolaryngologist visits per patient was 2.0 in the FESS group and 1.0 in the non-FESS group (Table 4). Approximately 7.0% of patients in each group were hospitalized (Figure 3A); these patients had an average of 7 cumulative inpatient days throughout the follow-up period. Both groups had about 15 all-cause outpatient visits per patient on average (Table 4 & Figure 3B), though FESS patients were more likely to have visits with CRSwNP listed as the primary diagnosis (52% vs 27%; p < 0.01). In both groups, those who visited an otolaryngologist had a mean (SD) of 3 (6) visits per patient. Approximately 20% of patients in both groups had an emergency room visit.
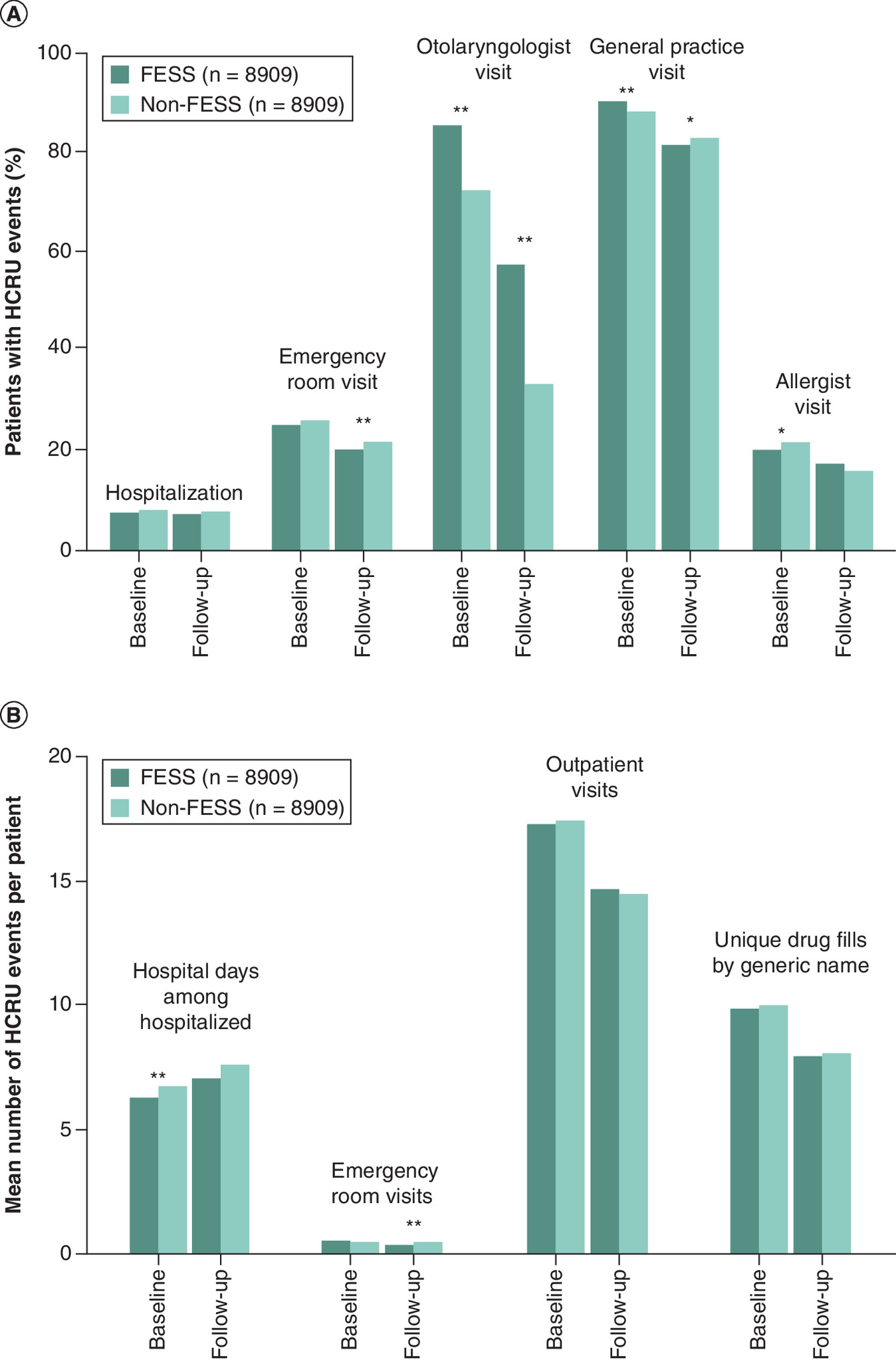
Figure 3. Healthcare resource utilization during the baseline and follow-up periods in the propensity score-matched population of patients with chronic rhinosinusitis with nasal polyps with functional endoscopic sinus surgery versus no functional endoscopic sinus surgery.
(A) Proportion of patients with HCRU events and (B) Mean number of HCRU events per patient.
*p < 0.05; **p < 0.01.
FESS: Functional endoscopic sinus surgery; HCRU: Healthcare resource utilization.
| FESS (n = 8909) | No FESS (n = 8909) | Mean difference (95% CI) | p-value | |
|---|---|---|---|---|
| HCRU, mean (SD) number of events per patient | ||||
| Hospitalizations | 0.09 (0.40) | 0.10 (0.41) | -0.01 (-0.02, 0.01) | 0.29 |
| Outpatient visits | 14.74 (12.55) | 14.49 (13.15) | 0.24 (-0.13, 0.62) | 0.21 |
| Emergency room visits | 0.32 (0.93) | 0.36 (0.94) | -0.04 (-0.06, -0.01) | <0.01 |
| Unique drug fills by generic name | 7.78 (6.38) | 7.96 (6.54) | -0.18 (-0.38, 0.02) | 0.08 |
| Otolaryngologist visits | 2.00 (4.75) | 1.03 (3.56) | 0.96 (0.87, 1.05) | <0.01 |
| General practice visits | 4.48 (5.39) | 4.83 (5.90) | -0.35 (-0.50, -0.20) | <0.01 |
| Costs, mean (SD) per patient ($US) | ||||
| Total costs | 15,659 (37,237) | 15,926 (44,425) | -267 (-1437, 964) | 0.66 |
| Inpatient costs | 2678 (15,277) | 3025 (18,918) | -347 (-841, 180) | 0.18 |
| Outpatient costs | 8910 (23,903) | 8722 (32,599) | 188 (-614, 1055) | 0.66 |
| Emergency room costs | 562 (2096) | 650 (2191) | -88 (-151, -26) | <0.01 |
| Pharmacy costs | 3509 (15,197) | 3529 (14,165) | -20 (-453, 409) | 0.93 |
CRSwNP: Chronic rhinosinusitis with nasal polyps; FESS: Functional endoscopic sinus surgery; HCRU: Healthcare resource utilization; PS: Propensity score; SD: Standard deviation.
During the intervention period, mean (SD) total estimated costs per patient were $28,832 (19,676) and $2537 (9782) in the FESS and non-FESS groups, respectively (difference $26,295 [95% CI: 25,841, 26,747; p < 0.01]) (Supplementary Table 4). During the follow-up period, mean (SD) total estimated costs per patient were $15,659 (37,237) and $15,926 (44,425) in the FESS and non-FESS groups, respectively (difference -$267 [95% CI: -1437, 964; p = 0.66]) (Table 4). The main cost driver during the intervention period was incremental outpatient costs: $27,404 (17,991) and $1621 (8132) per patient on average in the FESS and non-FESS groups, respectively (difference $25,782 [95% CI: 25,370, 26,193; p < 0.01]). The main cost drivers during follow-up were incremental outpatient costs ($8910 [23,903] and $8722 [32,599] in the FESS and non-FESS groups, respectively; difference $188 [95% CI: -614, 1055; p = 0.66]) and inpatient costs ($2678 [15,277] and $3025 [18,918], respectively; difference -$347 [-841, 180], p = 0.18).
Sensitivity analysis: day 45 to year 3
To evaluate the long-term impact of FESS, a sensitivity analysis was conducted to assess OCS and economic burden outcomes over 3 years post-index. Overall, 3952 PS-matched patients in each group had continuous enrollment and no FESS in the 3 years post-index. There was little difference in cumulative OCS dose between FESS versus non-FESS patients in years 2 and 3 post-index. Mean (SD) cumulative OCS dose per patient was 186 (616) mg in the FESS group versus 198 (567) mg in the non-FESS group in year 2 (difference -12 [95% CI: -38, 14; p = 0.36] mg), and 186 (628) mg versus 203 (636) mg, respectively, in year 3 (difference -18 [95% CI: -45, 10; p = 0.21] mg) (Table 5). Between day 45 and year 3 post-index, 55% of FESS patients and 58% of non-FESS patients used OCS. Mean (SD) total costs per patient were $16,188 (41,536) in the FESS group versus $16,195 (36,431) in the non-FESS group in year 2 (difference -$6 [95% CI: -1785, 1713; p = 0.99]) and $17,470 (39,539) versus $18,430 (45,657), respectively, in year 3 (difference -$960 [95% CI: -2793, 928; p = 0.32]) (Table 5).
| FESS (n = 3952) | No FESS (n = 3952) | Mean difference (95% CI) | p-value | |
|---|---|---|---|---|
| Cumulative OCS dose, mean (SD) per patient | ||||
| Intervention (index–day 44) | 83 (174) | 39 (139) | 43 (36, 50) | <0.01 |
| Follow-up (day 45–year 3) | 548 (1486) | 603 (1567) | -55 (-122, 11) | 0.11 |
| Day 45–year 1 | 176 (532) | 202 (592) | -25 (-51, -1) | <0.05 |
| Year 2 | 186 (616) | 198 (567) | -12 (-38, 14) | 0.36 |
| Year 3 | 186 (628) | 203 (636) | -18 (-45, 10) | 0.21 |
| Total costs, mean (SD) per patient ($US) | ||||
| Intervention (index–day 44) | 27,461 (18,958) | 2120 (5977) | 25,341 (24,716, 25,952) | <0.01 |
| Follow-up (day 45–year 3) | 48,317 (92,613) | 48,593 (87,578) | -275 (-4196, 3635) | 0.89 |
| Day 45–year 1 | 14,659 (34,864) | 13,968 (29,327) | 691 (-736, 2070) | 0.34 |
| Year 2 | 16,188 (41,536) | 16,195 (36,431) | -6 (-1785, 1713) | 0.99 |
| Year 3 | 17,470 (39,539) | 18,430 (45,657) | -960 (-2793, 928) | 0.32 |
Index is the date of FESS (FESS group) or risk-set matching (non-FESS group).
CRSwNP: Chronic rhinosinusitis with nasal polyps; FESS: Functional endoscopic sinus surgery; OCS: Oral corticosteroid; PS: Propensity score; SD: Standard deviation.
Exploratory analysis: Impact of comorbid asthma
In patients with comorbid asthma in baseline, mean cumulative OCS dose during follow-up was -90 (95% CI: -136, -43) mg lower per patient in the FESS group versus the non-FESS group (p < 0.01). In patients without comorbid asthma, the corresponding difference between groups was -28 (95% CI: -44, -13; p < 0.01) mg per patient (Supplementary Table 5). The respective mean (SD) total costs for FESS and non-FESS patients during follow-up were $18,323 (35,200) and $18,692 (59,389) in those with comorbid asthma (difference -$369 [95% CI: -2806, 3086; p = 0.81]), and $14,805 (37,875) and $14,185 (33,542) in those without comorbid asthma (difference $620 [95% CI: -477, 1816; p = 0.31]).
Discussion
Overall, this study found that OCS burden was significantly lower after FESS, but remained substantial in patients with CRSwNP regardless of FESS up to 3 years post-surgery, indicating a continuing unmet need in both groups. Patients who underwent FESS between 2012 and 2020 had a modest reduction in subsequent OCS burden, with little difference in HCRU or burden of CRSwNP-related medications and procedures, compared with patients who did not undergo FESS. Furthermore, only marginal differences in costs were observed between FESS and non-FESS patients during follow-up, indicating that the costs associated with the FESS intervention were not balanced by subsequent savings over the following 3 years.
A higher proportion of patients had baseline OCS use in the FESS compared with the non-FESS group within 30- and 60-days pre-index, at 27.6% versus 17.3%, and 39.4% versus 30.2%, respectively. These findings were expected, with OCS being routinely prescribed pre-operatively to reduce both blood loss and surgery times [19]. The proportion of patients needing OCS, which can be considered an indicator of uncontrolled disease, was similar during follow-up in the FESS and non-FESS groups (~35%). However, it should be noted that OCS can be used as a post-surgery additive treatment to improve patient endoscopic scores and post-surgery pain [19]. In this analysis, cumulative OCS dose during the intervention period (245 mg FESS and 271 mg non-FESS) was within the range of perioperative cumulative OCS doses reported in a recent literature review of OCS in CRS with and without polyps (150–352 mg) [21]. Additionally, a recent prospective randomized trial in the Netherlands showed a similar mean cumulative prednisone dose in the 12 months following FESS (266 mg per patient) [22] as the 12 months following FESS in the current study (combined intervention and follow-up periods 264 mg). The OCS burden for medical therapy alone in the Dutch trial was double the figure observed for non-FESS patients in the current analysis. While this difference may be due to variations in study design, setting, and local practice, recent literature has shown large disparities in steroid regimens and dosing among patients with CRSwNP [21]. Notwithstanding, the results consistently demonstrate high OCS burden in the CRSwNP population.
The clinical significance of the observed 40 mg (18%) difference in cumulative OCS dose is difficult to determine. Reported dose-response data for OCS-related adverse effects suggest a small absolute risk difference for this magnitude of difference in cumulative dose [23,24]. While even small reductions in risk may accumulate clinically significant benefits over many years, our findings over 3 years’ follow-up showed smaller and nonstatistically significant differences in cumulative OCS dose in years 2 and 3. Studies of longer duration would be needed to determine whether reductions in OCS use following FESS are sustained and whether they translate into lower incidence of OCS-related adverse events.
Results of this study show that while the cost of the intervention is high, FESS surgery does not lead to substantially lower total medical costs over a 3-year period. In the primary analysis, estimated cost of the intervention was $26,000, yet only $267 in cost savings were observed during follow-up. Average healthcare costs per patient were similar between the FESS and non-FESS groups during follow-up in the primary analysis ($14,000–15,000; days 45–365) and in each of years 2 ($16,000) and 3 ($17,000–18,000) in the sensitivity analysis in patients with 3 years of follow-up. Additionally, a higher rate of polypectomy procedures, as distinct from FESS, was observed during follow-up in the FESS cohort, which mirrors previous findings of common post-surgery polyp recurrence [17], particularly in patients with type 2 comorbidities such as asthma [9]. These findings illustrate the high economic burden associated with CRSwNP. A limitation of the current analysis was inability to assess quality of life and thus cost-effectiveness. An economic model that compared FESS with medical therapy in CRS in 2015 concluded that FESS became cost-effective in the third year after surgery, with incremental cost-effectiveness ratios versus medical therapy of $203,000, $85,000, and $49,000 per quality-adjusted life year in years 1, 2, and 3 post-surgery, respectively [25]. While that analysis reported FESS cost-effectiveness in CRSwNP, it is important to note that our analysis took a different approach. Our study focused on relative differences in healthcare costs between matched FESS and non-FESS groups over time, rather than conducting a formal cost-effectiveness analysis incorporating quality-adjusted life years. This real-world comparative cost analysis complements existing cost-effectiveness models by providing contemporary evidence on the relative economic impact of FESS in clinical practice. The ability to directly compare our findings to a cost-effectiveness model is limited. All-cause HCRU was similar between groups and there was little difference between baseline and follow-up. The observation of little change in all-cause HCRU in the 12-month periods before and after FESS is consistent with previously described costs [10] and supports the present analysis.
The comorbidity burden in the patients analyzed in this study was higher in comparison to that reported in other studies [4,5], and demonstrates multimorbidity that required medical care. In addition, we observed high prevalence of depression, anxiety and sleep disorders, consistent with previous findings in patients with CRSwNP [3,26,27]. Sources such as administrative claims may underestimate the true mental health burden in these patients. Loss of smell, a key symptom in patients with CRSwNP [28], has been implicated as an important contributor to the psychopathology of anxiety and depression [29].
A strength of this study is the use of a large claims database to provide pragmatic data in the context of real-world clinical practice. However, the limitations of administrative claims data should be considered when interpreting the findings. The CDM is considered generalizable to the commercially insured adults in the US but does not include patients covered by Medicaid or those without insurance cover. As is the nature of administrative claims databases, some misclassification of patients and their comorbidities is possible, due to limited observability of patients' medical history and rule-out codes used to bill for investigational services. While prescription claims data reflect medications dispensed at the pharmacy, it may not accurately reflect actual use of medications, such as inhaled corticosteroids, NSAIDs, and antihistamines, which may be underestimated in pharmacy claims due to over-the-counter availability. In addition, this analysis included OCS use for any cause but did not apply any method to ascertain CRSwNP-related OCS use, which would have added context to the all-cause OCS results, albeit with likely substantial imprecision and underestimation of the true rate of CRSwNP-related OCS use. We used PS matching to control for potential confounding, but the possibility of residual confounding factors cannot be excluded. While the cohorts were well matched on the known characteristics, this does not rule out differences in factors that are difficult to assess in the dataset, such as health-seeking behaviors not captured in the assessed HCRU metrics and disease severity not captured by all-cause OCS and CRSwNP medication use. Moreover, the analysis did not capture indirect costs, a known contributor to the economic burden associated with OCS use. The exclusion of patients with FESS during the follow-up period could have introduced selection bias by excluding referent patients with more severe disease. However, potential bias was minimal given there was little difference in demographics and baseline characteristics between the small proportion of patients with post-index FESS and those without (Figure 1). Lastly, traditional measures of severity of disease as reflected by symptom scores or radiologic scores could not be compared between the FESS and non-FESS groups.
Conclusion
This retrospective analysis of a large US administrative claims database indicates that real-world OCS burden for patients with CRSwNP who underwent FESS was significantly lower but remained substantial compared with matched patients who did not undergo FESS through up to 3 years of follow-up, indicating a continuing unmet need in both groups. Moreover, only marginal differences in costs were observed between FESS and non-FESS patients during follow-up, demonstrating that the high costs to the healthcare system of the FESS intervention resulted in minimal subsequent savings.
Summary points
•
This retrospective, observational study used claims data to compare oral corticosteroid (OCS) burden and healthcare resource utilization (HCRU) in patients with chronic rhinosinusitis with nasal polyps (CRSwNP) undergoing versus not undergoing functional endoscopic sinus surgery (FESS).
•
OCS burden and HCRU were assessed during baseline (365 days pre-index), intervention (days 0–44) and follow-up (days 45–365); costs were assessed during intervention and follow-up.
•
In the risk-set sampled population, patients undergoing FESS were younger on average than patients not undergoing FESS (52 vs 57 years) and more likely to have commercial insurance (69% vs 59%); both groups had substantial comorbidity burden (>50% allergic rhinitis; >25% asthma).
•
After propensity score matching (8909 patients in each group), mean OCS cumulative dose during follow-up was 18% lower among FESS versus non-FESS patients (mean difference: -40 mg per patient [95% CI: -57, -23; p < 0.01]).
•
Similar proportions of patients filled OCS prescriptions during follow-up (35% [FESS], 36% [non-FESS]), and in these patients, OCS burden remained high (mean [SD] cumulative dose 521 [786] vs 612 [906] mg, respectively).
•
HCRU was similar in follow-up, except more FESS patients visited an otolaryngologist (57% vs 32%, p < 0.01).
•
Mean total healthcare costs per patient during the intervention period were higher among FESS versus non-FESS patients ($28,832 vs $2537) but were similar during follow-up ($15,659 vs $15,926).
•
A sensitivity analysis in patients with data through 3 years post-index found that results in years 2 and 3 were similar to results in the primary follow-up period.
•
In US clinical practice, FESS leads to a significantly lower but persistent OCS burden, and does not lead to substantially lower costs through 3 years of follow-up in patients with CRSwNP.
Author contributions
DL Isaman and N Petruski-Ivleva contributed to study conception and design, data acquisition and analysis and drafting the manuscript. DL Isaman, M Corbett, SE Lee, AT Peters, PH Hwang, S Reitsma, N Petruski-Ivleva, S Nash, and JA Jacob-Nara contributed to data interpretation and critical review of the manuscript for important intellectual content. All authors approved the version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
The authors thank Asif H Khan (Sanofi) for insights and guidance.
Financial disclosure
Research sponsored by Sanofi, NJ, USA & Regeneron Pharmaceuticals Inc., NY, USA.
Competing interests disclosure
DL Isaman, M Corbett and N Petruski-Ivleva are employees of Sanofi and may hold stock and/or stock options in the company. SE Lee has received clinical trial funding from, and is an advisory board member for AstraZeneca, Genentech, GlaxoSmithKline and Sanofi, and is also an advisory board member for Novartis, Regeneron Pharmaceuticals Inc., and Sanofi. AT Peters is an advisory board member for AstraZeneca, Regeneron Pharmaceuticals Inc., and Sanofi, has received research grants from Optinose, Regeneron Pharmaceuticals Inc., and Sanofi, and is a consultant for GlaxoSmithKline and Optinose. PH Hwang has received speaker fees from GlaxoSmithKline and Regeneron Pharmaceuticals Inc., clinical trial funding from GlaxoSmithKline, is a consultant for Slate Therapeutics and Stryker, and has received equity interest from SoundHealth. S Reitsma is a consultant for and has received research grants and honoraria from GlaxoSmithKline, Novartis and Sanofi, and is a steering committee member for EPOS and European Chronic Rhinosinusitis Outcome Registry. S Nash is an employee and shareholder of Regeneron Pharmaceuticals Inc. JA Jacob-Nara is a former employee of Sanofi and may hold stock and/or stock options in the company. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support was provided by Sibyl Bertrand, PhD, and Sean Booth, MRes, of Adelphi Communications, Bollington, UK, and was funded by Sanofi and Regeneron Pharmaceuticals Inc. in accordance with Good Publication Practice.
Data sharing statement
Qualified researchers may request access to patient-level data and related documents (including, e.g., the clinical study report, study protocol with any amends, blank case report form, statistical analysis plan and dataset specifications). Patient-level data will be anonymized, and study documents will be redacted to protect the privacy of trial participants. Further details on Sanofi’s data sharing criteria, eligible studies and process for requesting access can be found at https://www.vivli.org.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 223.04 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Claeys N, Teeling MT, Legrand P et al. Patients unmet needs in chronic rhinosinusitis with nasal polyps care: a patient advisory board statement of EUFOREA. Front. Allergy 2, 761388 (2021).
2.
Khan A, Vandeplas G, Huynh TMT et al. The Global Allergy and Asthma European Network (GALEN) rhinosinusitis cohort: a large European cross-sectional study of chronic rhinosinusitis patients with and without nasal polyps. Rhinology 57(1), 32–42 (2019).
3.
Bachert C, Bhattacharyya N, Desrosiers M, Khan AH. Burden of disease in chronic rhinosinusitis with nasal polyps. J. Asthma Allergy 14, 127–134 (2021).
4.
Bhattacharyya N, Villeneuve S, Joish VN et al. Cost burden and resource utilization in patients with chronic rhinosinusitis and nasal polyps. Laryngoscope 129(9), 1969–1975 (2019).
5.
Benson VS, Germain G, Chan RH et al. Elucidating the real-world burden of chronic rhinosinusitis with nasal polyps in patients in the USA. OTO Open 6(4), 2473974X221128930 (2022).
6.
Lourijsen ES, Fokkens WJ, Reitsma S. Direct and indirect costs of adult patients with chronic rhinosinusitis with nasal polyps. Rhinology 58(3), 213–217 (2020).
7.
Wahid NW, Smith R, Clark A, Salam M, Philpott CM. The socioeconomic cost of chronic rhinosinusitis study. Rhinology 58(2), 112–125 (2020).
• Highlights the substantial healthcare resource utilization (HCRU), out-of-pocket expenditures and lost work time for patients with CRS.
8.
Bhattacharyya N. Incremental health care utilization and expenditures for chronic rhinosinusitis in the United States. Ann. Otol. Rhinol. Laryngol. 120(7), 423–427 (2011).
•• This study comparing HCRU of patients with and without CRS found that CRS is associated with substantial increases in HCRU owing to office-based and prescription expenditures, and imposes a high cost on national healthcare.
9.
Fokkens WJ, Lund VJ, Hopkins C et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology 58(Suppl. 29), 1–464 (2020).
10.
Peters AT, Bengtson LGS, Chung Y et al. Clinical and economic burden of chronic rhinosinusitis with nasal polyposis: a U.S. administrative claims analysis. Allergy Asthma Proc. 43(5), 435–445 (2022).
•• This administrative claims analysis highlights the prevalence of oral corticosteroid (OCS) use among patients with chronic rhinosinusitis with nasal polyps (CRSwNP).
11.
Hox V, Lourijsen E, Jordens A et al. Benefits and harm of systemic steroids for short- and long-term use in rhinitis and rhinosinusitis: an EAACI position paper. Clin. Transl. Allergy 10, 1 (2020).
12.
Waljee AK, Rogers MA, Lin P et al. Short term use of oral corticosteroids and related harms among adults in the United States: population based cohort study. BMJ 357, j1415 (2017).
13.
Yao TC, Huang YW, Chang SM et al. Association between oral corticosteroid bursts and severe adverse events: a nationwide population-based cohort study. Ann. Intern. Med. 173(5), 325–330 (2020).
14.
Yasir M, Goyal A, Sonthalia S. Corticosteroid adverse effects. Statpearls. StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC (2023).
15.
Slack R, Bates G. Functional endoscopic sinus surgery. Am. Fam. Physician 58(3), 707–718 (1998).
16.
Snidvongs K, Kalish L, Sacks R et al. Sinus surgery and delivery method influence the effectiveness of topical corticosteroids for chronic rhinosinusitis: systematic review and meta-analysis. Am. J. Rhinol. Allergy 27(3), 221–233 (2013).
17.
DeConde AS, Mace JC, Levy JM et al. Prevalence of polyp recurrence after endoscopic sinus surgery for chronic rhinosinusitis with nasal polyposis. Laryngoscope 127(3), 550–555 (2017).
18.
Loftus CA, Soler ZM, Koochakzadeh S et al. Revision surgery rates in chronic rhinosinusitis with nasal polyps: meta-analysis of risk factors. Int. Forum Allergy Rhinol. 10(2), 199–207 (2020).
19.
Pundir V, Pundir J, Lancaster G et al. Role of corticosteroids in functional endoscopic sinus surgery–a systematic review and meta-analysis. Rhinology 54(1), 3–19 (2016).
20.
Han JK, Silver J, Dhangar I, Veeranki P, Deb A. Quantifying corticosteroid burden in chronic rhinosinusitis with nasal polyps: a retrospective US database study. Ann. Allergy Asthma Immunol. 134(6), 685–693 (2024).
21.
Mansi A, Bui R, Chaaban MR. Oral corticosteroid regimens in the management of chronic rhinosinusitis. Ear Nose Throat J. 101(2), 123–130 (2022).
22.
Lourijsen ES, Reitsma S, Vleming M et al. Endoscopic sinus surgery with medical therapy versus medical therapy for chronic rhinosinusitis with nasal polyps: a multicentre, randomised, controlled trial. Lancet Respir. Med. 10(4), 337–346 (2022).
•• This randomized controlled trial from the Netherlands of ESS versus medical therapy alone found a similar substantial burden of OCS following surgery as found in our US study.
23.
Price DB, Trudo F, Voorham J et al. Adverse outcomes from initiation of systemic corticosteroids for asthma: long-term observational study. J. Asthma Allergy 11, 193–204 (2018).
24.
Davis GE, Zeiger RS, Emmanuel B et al. Systemic corticosteroid-related adverse outcomes and health care resource utilization and costs among patients with chronic rhinosinusitis with nasal polyposis. Clin. Ther. 44(9), 1187–1202 (2022).
25.
Rudmik L, Soler ZM, Mace JC, Schlosser RJ, Smith TL. Economic evaluation of endoscopic sinus surgery versus continued medical therapy for refractory chronic rhinosinusitis. Laryngoscope 125(1), 25–32 (2015).
•• This analysis concluded that functional endoscopic sinus surgery (FESS) becomes cost-effective versus continued medical therapy within the third year after surgery.
26.
Nanayakkara JP, Igwe C, Roberts D, Hopkins C. The impact of mental health on chronic rhinosinusitis symptom scores. Eur. Arch. Otorhinolaryngol. 270(4), 1361–1364 (2013).
27.
Schlosser RJ, Gage SE, Kohli P, Soler ZM. Burden of illness: a systematic review of depression in chronic rhinosinusitis. Am. J. Rhinol. Allergy 30(4), 250–256 (2016).
28.
Mullol J, Mariño-Sánchez F, Valls M, Alobid I, Marin C. The sense of smell in chronic rhinosinusitis. J. Allergy Clin. Immunol. 145(3), 773–776 (2020).
29.
Marin C, Alobid I, Fuentes M, López-Chacón M, Mullol J. Olfactory dysfunction in mental illness. Curr. Allergy Asthma Rep. 23(3), 153–164 (2023).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 1 May 2025
Accepted: 6 January 2026
Published online: 11 February 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Treatment burden and healthcare resource utilization in patients with chronic rhinosinusitis with nasal polyps who did or did not undergo functional endoscopic sinus surgery: a US real-world retrospective cohort study. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0065
Export citation
Select the citation format you wish to export for this article or chapter.