Effectiveness of motor relearning program in sit-to-stand transfer and activities of daily living among chronic stroke patients – a prospective, multicenter, randomized controlled trial
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Stroke is a clinically defined syndrome characterized by an acute, focal neurological deficit due to vascular injury. Strokes can result in various disabilities, including sensory and motor abnormalities, leading to difficulties with motor control, balance and posture. Physical therapists use various neurorehabilitation approaches to enhance the functional abilities and independence of stroke patients. The motor relearning program (MRP) is a task-oriented, self-monitored, structured program based on motor control theories and neuroplasticity used in the rehabilitation of stroke patients. Therefore, this study aimed to evaluate the effectiveness of MRP in improving sit-to-stand transfer and activities of daily living in individuals with chronic stroke. Materials & methods: A prospective, single-blinded, multi-centered randomized controlled trial was conducted in Saudi Arabia involving 32 chronic stroke patients randomly assigned to experimental (n = 16) and control (n = 16) groups. The experimental group received 45 minutes of MRP combined with conventional physical therapy, while the control group received conventional physical therapy alone. Interventions were delivered thrice weekly over 6 weeks (18 sessions). Outcome measures included the Barthel Index (BI) and the sit-to-stand component of the motor assessment scale (MAS), assessed pre- and post-intervention. Results: The experimental group demonstrated statistically significant improvements in both MAS and BI scores (p < 0.001), with large effect sizes (r = -0.865; for MAS, Cohen’s d = 1.46 for BI). ANCOVA analyses revealed that baseline MAS scores (MAS_pre) significantly influenced post-intervention outcomes (F[1, 29] = 65.33, p < 0.001), and the group effect remained significant after adjusting for MAS_pre (F[1, 29] = 41.89, p < 0.001). The model explained 72.6% of the variance in MAS_post scores (adjusted R2 = 0.707), confirming the predictive strength of MRP. Similarly, BI_post scores were significantly predicted by BI_pre and group assignment (F[1, 29] = 21.15, p < 0.001), with the model accounting for 85.8% of the variance (Adjusted R2 = 0.849). Conclusion: The motor relearning program significantly improves sit-to-stand transfer and activities of daily living performance in chronic stroke patients. Despite the small sample size and baseline MAS imbalance, these improvements remained robust after statistical adjustment, underscoring MRP’s clinical utility in neurorehabilitation. Clinical trial registration was done prospectively at https://clinicaltrials.gov/ with the registration no: NCT06690073
Plain language summary
Background:
Stroke is a medical condition that can cause problems with movement, balance and daily activities. Physical therapy helps stroke survivors regain their independence. One approach called the motor relearning program (MRP) focuses on practicing everyday tasks to improve movement and brain recovery.
Purpose:
This study looked at whether MRP could help people who had a stroke improve their ability to stand up from a sitting position and perform daily activities.
What was done?
Thirty-two stroke survivors in Saudi Arabia were divided into two groups. One group received MRP along with regular physical therapy, while the other group received only regular therapy. Both groups had 45-minute sessions, three times a week, for 6 weeks. Researchers measured how well participants could stand up and carry out daily tasks before and after the treatment.
What was found?
People who received MRP showed much better improvement in standing up and doing daily activities compared with those who had regular therapy alone.
Conclusion:
The motor relearning program is a powerful tool that can help stroke survivors improve their movement and independence in daily life. It may be especially useful for people recovering from the long-term effects of a stroke.
Stroke is a clinically defined syndrome marked by an acute, focal neurological deficit due to vascular injury, such as infarction or hemorrhage, in the central nervous system [1]. Globally, stroke is recognized as the third leading cause of physical disabilities in adults and the second leading cause of death in high-middle income countries [2]. The reported stroke burden in Saudi Arabia ranges from 19 to 57 cases per 100,000 population, with ischemic stroke being the most prevalent type, followed by intracerebral hemorrhage and subarachnoid hemorrhage [3].
Stroke can result in a range of disabilities that present significant challenges for physical therapists. Common impairments include sensory and motor dysfunctions, particularly involving the proprioceptive system, which affect motor control, balance and postural stability. Muscle weakness is a prominent issue that compromises the ability to sit, stand or walk, and its severity often depends on the location and extent of the brain injury. Alterations in muscle tone are frequently observed due to damage to the cerebral cortex, leading to diminished regulation by the spinal cord. Additional complications may include aphasia, impaired coordination and balance, convulsions, hydrocephalus, abnormal reflexes and disruptions in motor programming [4].
Physical therapy is a common rehabilitation method following a stroke. Its main goal is to enhance patients’ functional abilities and independence, ultimately improving their overall quality of life [5]. Physical therapists employ a range of neurorehabilitation approaches to support stroke recovery, including neurodevelopmental treatment (NDT), motor relearning program (MRP), proprioceptive neuromuscular facilitation (PNF), the Brunnstrom technique, task-oriented strategies and constraint-induced movement therapy (CIMT). The effectiveness of each approach may vary depending on factors such as the timing and duration of therapy, the availability of specialized stroke rehabilitation services and the therapist’s clinical preferences and expertise [6,7].
MRP is a rehabilitation approach used for post-stroke rehabilitation to retrain functional skills based on motor retraining theory. It is a structured, self-monitored practice which involves caregivers and rehabilitation staff. MRP divides the tasks into four distinct stages: first, analyzing and observing the task; second, practicing the missing components of the task with the help of verbal or visual instructions and manual guidance; third, practicing the entire task, including the previously practiced missing component; and finally, training for transference [8,9].
A recent systematic review evaluating the effectiveness of the motor relearning program on upper limb function post-stroke concluded that MRP yields short-term improvements in upper limb function among adults. However, current evidence remains insufficient to establish its superiority over other rehabilitation interventions [7]. Additionally, a randomized controlled trial investigating the impact of MRP on post-stroke balance reported a clinically meaningful enhancement in patient balance following MRP training [10]. Nevertheless, the effectiveness of MRP in improving sit-to-stand performance and activities of daily living (ADL) has not been comprehensively explored in existing literature [10–12].
Alqahtani et al., through a cross-sectional survey conducted among physiotherapists in the Riyadh region of Saudi Arabia, reported that the MRP was not a widely adopted approach for stroke rehabilitation, with only 21.7% of respondents indicating its use in clinical practice [13]. Recently, Alatawi F investigated the prevailing clinical practices among Saudi physiotherapists in stroke rehabilitation and found that the MRP was the third most commonly utilized approach, accounting for 25.38% of usage – following the Bobath/NDT and Brunnstrom methods [14]. Both studies concluded that Saudi physiotherapists tend to use mixed methods instead of a single rehabilitation approach for stroke rehabilitation.
Accordingly, this study was designed to offer evidence regarding the impact of MRP on enhancing sit-to-stand transfer and ADL following a stroke. The primary objective is to evaluate the effectiveness of MRP in improving these functional outcomes among individuals with chronic stroke.
Materials & methods
This study was a prospective, single-blinded, multicentered, randomized controlled trial design. The study took place at the stroke units of King Saud Medical City and Prince Sultan Bin Abdul-Aziz Humanitarian City in Riyadh, as well as the Ministry of Health Hospital in the Al-Jouf region, Saudi Arabia. The study included hemiplegic stroke patients who had experienced a stroke for more than 6 months, aged between 45 and 65 years, of both genders, with a minimum score of 24 on the Mini-Mental State Examination, and with normal vision. Patients with unilateral neglect, cognitive impairments or visual impairments were excluded. Assessors were blinded to the group assignment, and written consent was obtained from all patients for this study.
Sampling calculation & technique
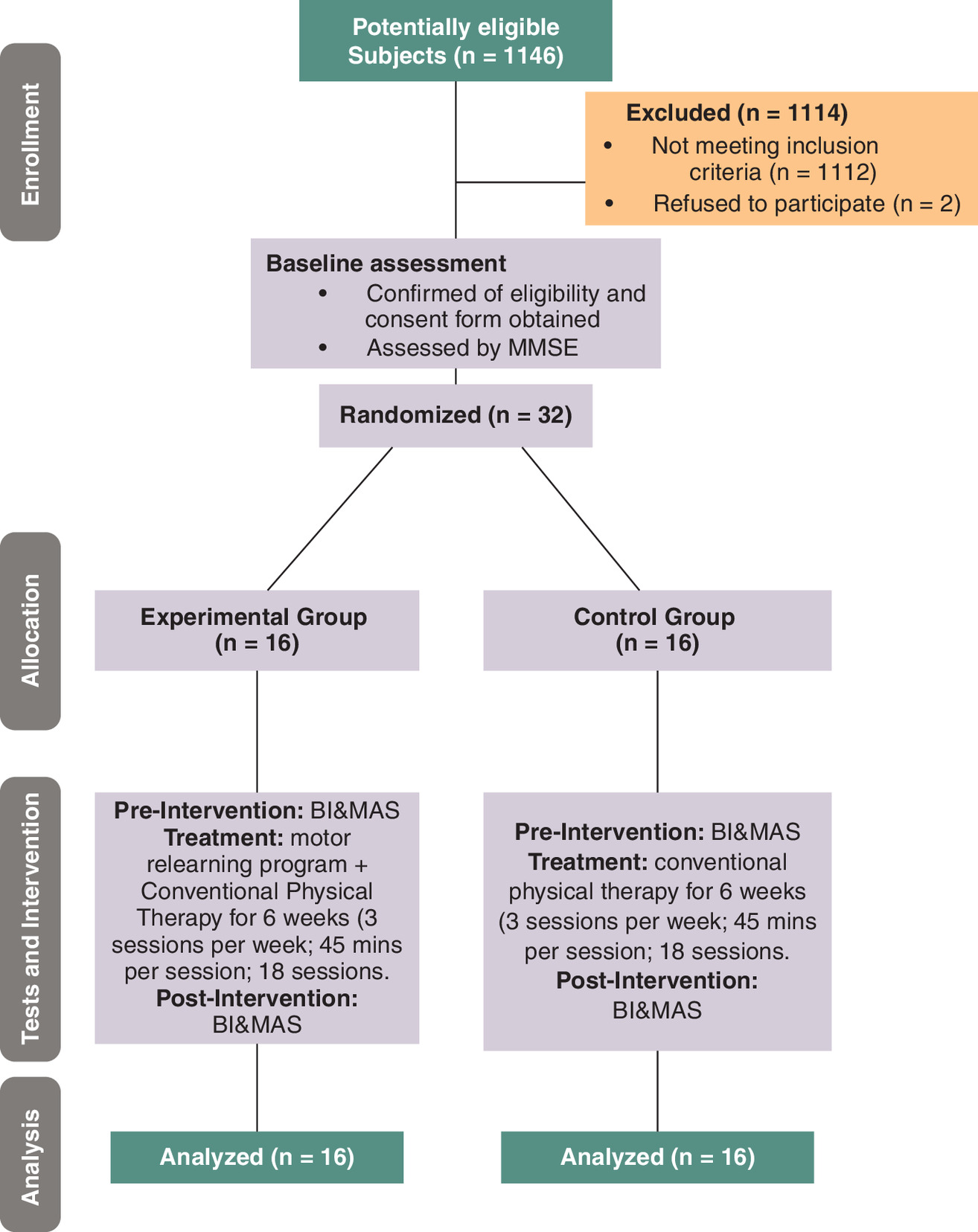
The non-probability convenience sampling technique was used. Based on the previous study [11], we calculated the sample size of the current study. The following method was applied to obtain the size of the sample. The sample size we got was 16 in each group, making the total sample required for the study 32.
The CONSORT diagram is shown in Figure 1, explaining the flow of participants in this study.
Ethical considerations
The study was conducted after obtaining the institutional review board approval from the following hospitals: King Saud Medical City (KSMC); approval no.: H1RE-24-May22-01, Al-Jouf Health Affairs; approval no.: 2022.19 and Prince Sultan Bin Abdul-Aziz Humanitarian City (SBAHC); approval no: 85-2022-IRB. The study was registered at ClinicalTrials.gov (registration ID: NCT06690073).
Randomization & blinding
Chronic stroke patients from the three aforementioned hospitals were screened based on inclusion and exclusion criteria. Written informed consent was obtained from individuals who met the eligibility criteria and agreed to participate in the study. Eligible participants were then randomly assigned to either the experimental or control group using a lottery method. Sealed envelopes were used to ensure an equal probability of group assignment. To maintain allocation concealment, opaque, sequentially numbered envelopes were prepared by an independent researcher not involved in participant recruitment or assessment. Importantly, outcome assessors at all three study sites were blinded to group allocation to minimize assessment bias. They were not involved in any aspect of participant recruitment, treatment administration or the randomization process, thereby ensuring the integrity of the blinding procedure throughout the study.
Interventions
The control group received conventional physical therapy (CPT) for 45 minutes/session, three times per week for 6 weeks (18 sessions). CPT treatments include mat activities, assisted movements, weight-bearing strategies, stretching exercises, strengthening exercises and gait training [15]. At the same time, the experimental group received the previously mentioned CPT treatment as well as MRP for sitting to standing and standing to sitting for 6 weeks, for a total duration of 45 min per session (30 min of CPT treatment followed by 15 min MRP), three sessions per week (18 sessions). The participants did not receive any concurrent therapies during the study period.
MRP of sitting and standing activities: During the MRP sessions focused on sit-to-stand training, the physical therapist positioned themselves in front of the participant, who was seated in a chair with armrests. Participants were guided to place their feet backwards and lean their trunk forward to initiate the movement. The therapist provided manual assistance by supporting the participant’s hand and shoulder, encouraging a swift anterior trunk flexion.
Once the forward lean was achieved, participants were instructed to press down through the affected foot and rise quickly to a standing position while shifting their hips forward. To facilitate this movement, the therapist applied gentle pressure through the participant’s knee along the shaft of the leg, promoting anterior displacement and weight transfer during the transition.
MRP of standing to sitting: During the stand-to-sit training, the physiotherapist assisted the participant by facilitating anterior shoulder movement and guiding knee flexion at the initiation of the descent. Participants were instructed to maintain weight-bearing on the affected leg throughout the sitting motion to promote symmetrical loading.
The exercise protocol included variations in seat height, controlled pauses at different points within the movement range, and adjustments in speed – all tailored by the therapist to challenge motor control and functional stability. Repetitions and intensity were individualized based on each participant’s physical capacity and progressively increased over time. Throughout the sessions, therapists provided verbal feedback on weight distribution, movement speed and performance quality to reinforce correct technique and encourage active participation [9,12].
Progression was standardized across the participants based on predefined performance benchmarks, such as task completion accuracy and movement quality, assessed weekly. To ensure consistency in intervention delivery, the principal investigator conducted weekly fidelity checks by reviewing session logs and directly observing selected therapy sessions. Constructive feedback was provided to therapists as needed to maintain adherence to the protocol.
Outcome measures
Motor assessment scale: The motor assessment scale (MAS) is a clinical tool designed to evaluate motor function in stroke patients. It evaluates eight functional activities: turning in bed, sitting, standing up, walking, balance in sitting and activities of the upper arm, the wrist and the hand. The ninth item notes the general tone of the body. Each item is scaled from 0 to 6, with a total possible score of 54, indicating normal function. The MAS is considered a reliable and valid tool, making it a valuable tool for assessing disability levels according to WHO criteria [9,16]. In this study, the ‘standing up’ component of the MAS was specifically used to evaluate participants’ ability to perform sit-to-stand transfers.
Barthel Index: The Barthel Index (BI) is a widely used 10-item assessment tool that evaluates the level of assistance required by stroke patients for mobility and daily living activities. Individual item scores are weighted and combined to yield a total score ranging from 0 to 100, where a score of ‘0’ signifies complete independence in all ten activities. The assessment typically takes 5–10 minutes to complete and is recognized for its strong validity and reliability in the stroke population [17].
Data collection
The demographic data of the subjects were recorded on individual data entry sheets. The Mini-Mental State Examination assessment was conducted for screening purposes, and regular neurological evaluations were performed to inform treatment decisions. Outcome measures, including the MAS and BI, were assessed before and after 6 weeks of treatment.
Data analysis
All statistical analyses were performed using SPSS version 28. Descriptive statistics were calculated for all outcome variables. Assumptions of normality were assessed using the Shapiro–Wilk test. BI scores were normally distributed, allowing for the use of parametric tests. Within-group changes from pre- to post-intervention were analyzed using paired-samples t-tests, and between-group comparisons of post-intervention scores were conducted using independent-samples t-tests. Effect sizes were calculated using Cohen’s d, interpreted according to conventional benchmarks (small: 0.2, medium: 0.5, large: 0.8). MAS scores were not normally distributed, necessitating the use of nonparametric tests. Within-group changes were evaluated using the Wilcoxon Signed-Rank Test, and between-group comparisons of post-intervention scores were assessed using the Mann–Whitney U test. Effect sizes were calculated using r, with values interpreted as small (0.1), medium (0.3) and large (0.5). To control for baseline differences and assess the independent effect of group assignment, analysis of covariance (ANCOVA) was conducted for both BI and MAS post-intervention scores, using pre-intervention scores as covariates, respectively. Model fit was evaluated using R2 and adjusted R2, and statistical significance was set at p < 0.05 for all analyses.
Results
A total of 32 patients were included in this study, and they were randomly allocated into two groups. The participants’ demographic and baseline characteristics are given in Table 1.
| Variables | Mean ± SD, frequency (%), median (range) | |
|---|---|---|
| Experimental | Control | |
| Gender Male Female | 9 (56.2%) 7 (43.8%) | 14 (87.5%) 2 (12.5%) |
| Type of stroke Ischemic Hemorrhagic | 13 (81.2%) 3 (18.8%) | 12 (75%) 4 (25%) |
| Post-stroke duration (months) | 8 (6–95) | 16 (6–84) |
| Affected side Left Right | 5 (31.2%) 11 (68.8%) | 8 (50%) 8 (50%) |
| Hypertension Yes No | 12 (75%) 4 (25%) | 13 (81.2%) 3 (18.8%) |
| Diabetes Yes No | 13 (81.2%) 3 (18.8%) | 10 (62.5%) 6 (37.5%) |
| Smoking Yes No | 6 (37.5%) 10 (62.5%) | 4 (25%) 12 (75%) |
| Age (years) | 57.31 ± 5.86 | 52.31 ± 6.37 |
| BMI (kg/m2) | 30.2 ± 7.24 | 28.48 ± 5.39 |
| MMSE score | 26.56 ± 2.8 | 28.47 ± 5.39 |
| Barthel Index Pre-test Post-test | 58.75 ± 15.21 71.56 ± 17.86 | 63.13 ± 15.04 65.01 ± 17.22 |
| MAS score Pre-test Post-test | 2 (1–4) 5 (2–6) | 4 (1–5) 4 (1–5) |
BMI: Body mass index; MAS: Motor assessment scale; MMSE: Mini-mental state examination; SD: Standard deviation.
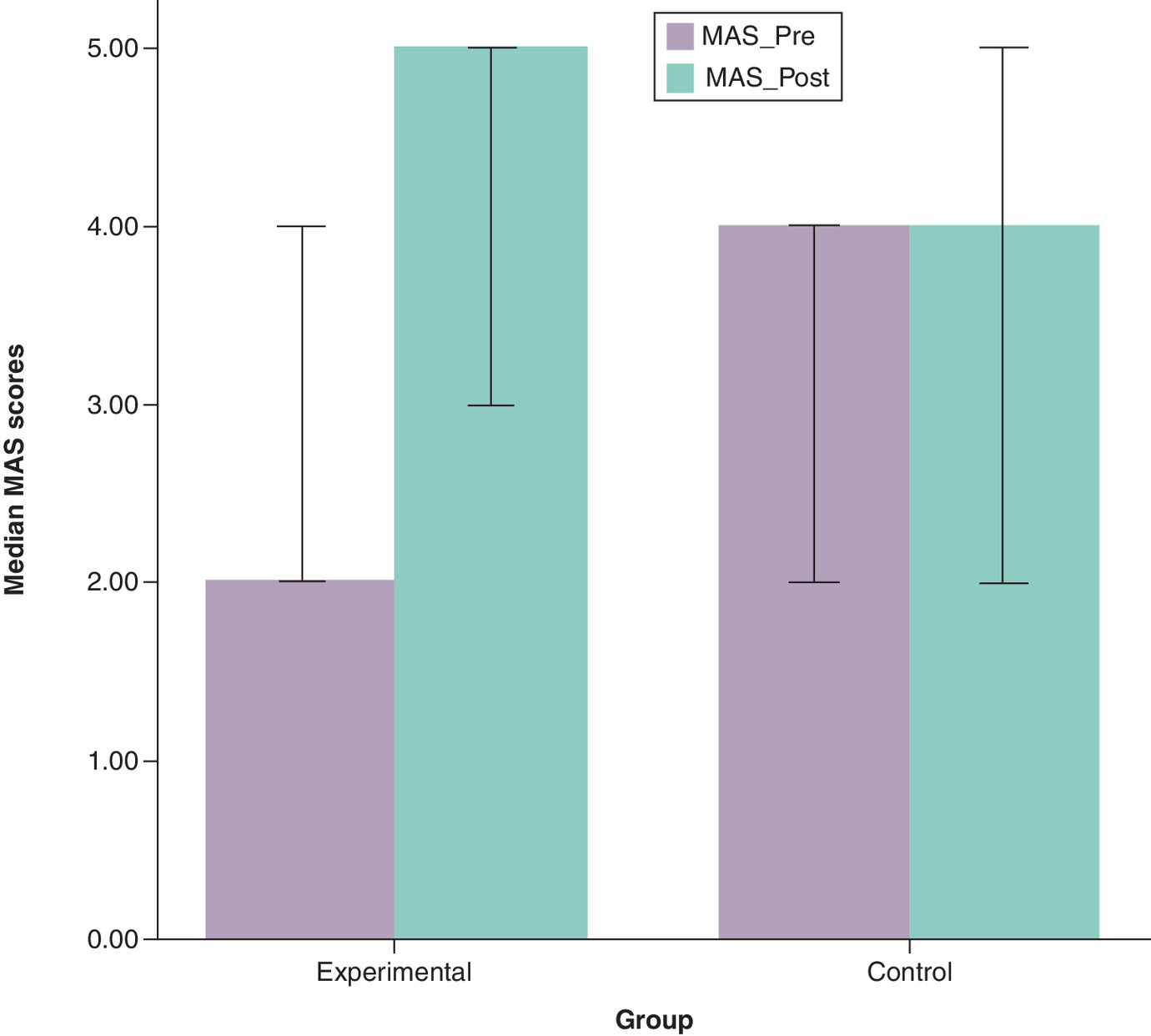
A Wilcoxon signed-rank test was conducted to compare the pre- and post-intervention MAS scores within each group (Table 2 & Figure 2). The experimental group revealed a statistically significant change in MAS scores from pre- to post-intervention, Z = -3.46, p = 0.001. Out of 16 participants, 15 showed improvements in MAS score, a positive rank and 1 no change (tie). The mean rank of the positive differences was 8.00, and a total sum of ranks of 120.00, indicating a consistent and meaningful change in MAS score after MRP. The effect size (r) was calculated to assess the magnitude of the change, which yields a value of -0.865, reflecting a larger effect size, suggesting MRP has a substantial effect in improving MAS scores. In contrast, the control group showed no statistically significant change in MAS scores from pre- to post-intervention, Z = -1.73, p = 0.083. Out of 16 participants, 3 showed improvement (positive rank) and 13 showed no change (tie). The mean rank of the positive differences was 2.00, and a total sum of ranks of 6.00, indicating a limited improvement in MAS score after CPT. The calculated effect size was -0.43, reflecting a moderate effect, suggesting that CPT may have had a meaningful but statistically inconclusive impact on MAS scores
| Group | Mean difference | SD | t (df) | 95% CI | p-value | Cohen’s d |
|---|---|---|---|---|---|---|
| Experimental | 12.81 | 75 | 5.86 (15) | 8.15, 17.48 | <0.001 | 1.46 |
| Control | 1.88 | 03 | 1.86 (15) | -0.27, 4.02 | 0.083 | 0.47 |
df: Degrees of freedom; SD: Standard deviation; CI: Confidence interval.
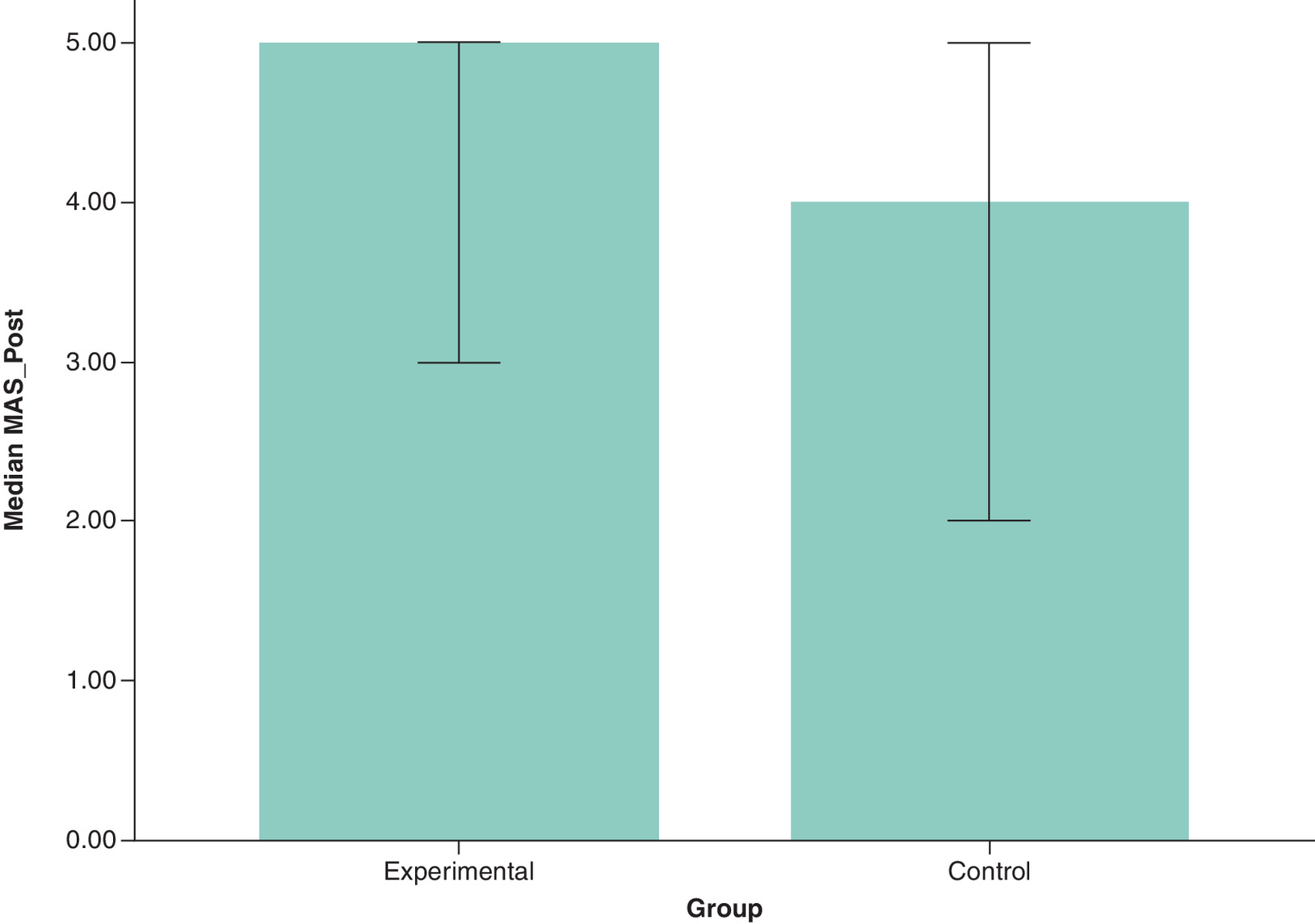
To compare post-intervention MAS scores (MAS_post) between groups, a Mann–Whitney U test was performed (Table 3 & Figure 3). The results indicated no statistically significant difference, U = 81.00, Z = -1.85, p = 0.065. The experimental group had a higher mean rank (19.44) compared with the control group (13.56), suggesting a trend toward greater improvement in MAS scores following MRP. The effect size (r) was calculated as -0.33, indicating a small to moderate effect, although the difference in MAS_post scores between groups was not statistically significant (p = 0.065), the effect size suggests a potentially meaningful clinical difference favoring the experimental group.
| Comparison | Mean Difference | SE | 95% CI | t (df) | p-value | Cohen's d |
|---|---|---|---|---|---|---|
| BI_post (experimental vs control) | 6.56 | 6.20 | -6.11, 19.23] | 1.06 (30) | 0.299 | 0.37 |
df: Degrees of freedom; SD: Standard deviation; CI: Confidence interval; BI: Barthel index.
An ANCOVA was conducted to compare post-intervention MAS scores between the experimental and control groups, while controlling for baseline MAS scores (MAS_pre). The overall model was statistically significant, F(2, 29) = 38.47, p < 0.001, indicating that the combination of group assignment and baseline motor function significantly predicted MAS_post outcomes. The covariate MAS_pre had a strong and statistically significant effect on MAS_post, F(1, 29) = 65.33, p < 0.001, confirming that baseline motor ability was a major determinant of post-intervention scores. Importantly, the group effect was statistically significant, F(1, 29) = 41.89, p < 0.001, suggesting that participants in the experimental group achieved significantly greater improvements compared with those in the control group, even after adjusting for baseline differences. The model explained 72.6% of the variance in MAS_post scores (R2 = 0.726, Adjusted R2 = 0.707), indicating strong predictive power and excellent model fit (Table 4).
| F (df) | p-value | |
|---|---|---|
| Overall model | 87.83 (2, 29) | <0.001 |
| BI_pre (covariate) | 168.29 (1, 29) | <0.001 |
| Group (effect) | 21.15 (1, 29) | <0.001 |
| R2/adjusted R2 | 0.858/0.849 | — |
df: Degrees of freedom.
A paired-samples t-test was conducted to compare pre- and post-intervention BI scores within each group (Table 5 & Figure 4). In the experimental group, the analysis revealed a statistically significant improvement in BI scores, t(15) = 5.86, p < 0.001. The mean difference was 12.81 (SD = 8.75), with a 95% CI ranging from 8.15 to 17.48, indicating a reliable enhancement in functional independence. The magnitude of this change was quantified using Cohen’s d, which yielded a value of 1.46. This reflects a large effect size, suggesting that the MRP had a substantial positive impact on participants’ ability to perform ADLs.
| Group | Z-value | p-value | Positive ranks | Mean rank | Sum of ranks | Effect size (r) |
|---|---|---|---|---|---|---|
| Experimental | -3.46 | 0.001 | 15 | 8.00 | 120.00 | -0.865 |
| Control | -1.73 | 0.083 | 3 | 2.00 | 6.00 | -0.43 |
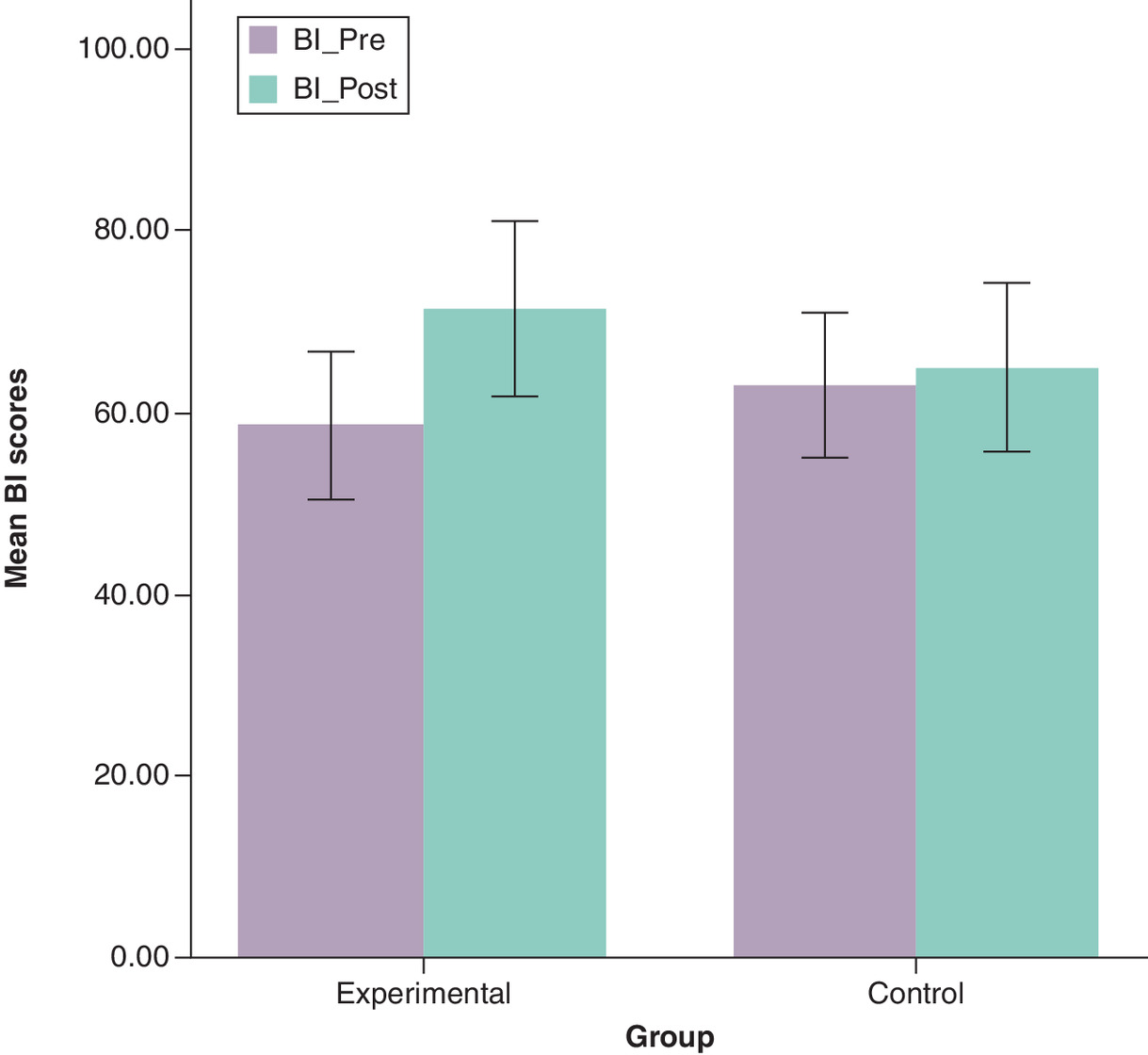
In contrast, the control group showed no statistically significant change in BI scores from pre- to post-intervention, t (15) = 1.86, p = 0.083. The mean difference was 1.88 (SD = 4.03), with a 95% CI ranging from -0.27 to 4.02. Although not statistically significant, the Cohen’s d of 0.47 suggests a moderate effect size, indicating a potentially meaningful improvement following CPT.
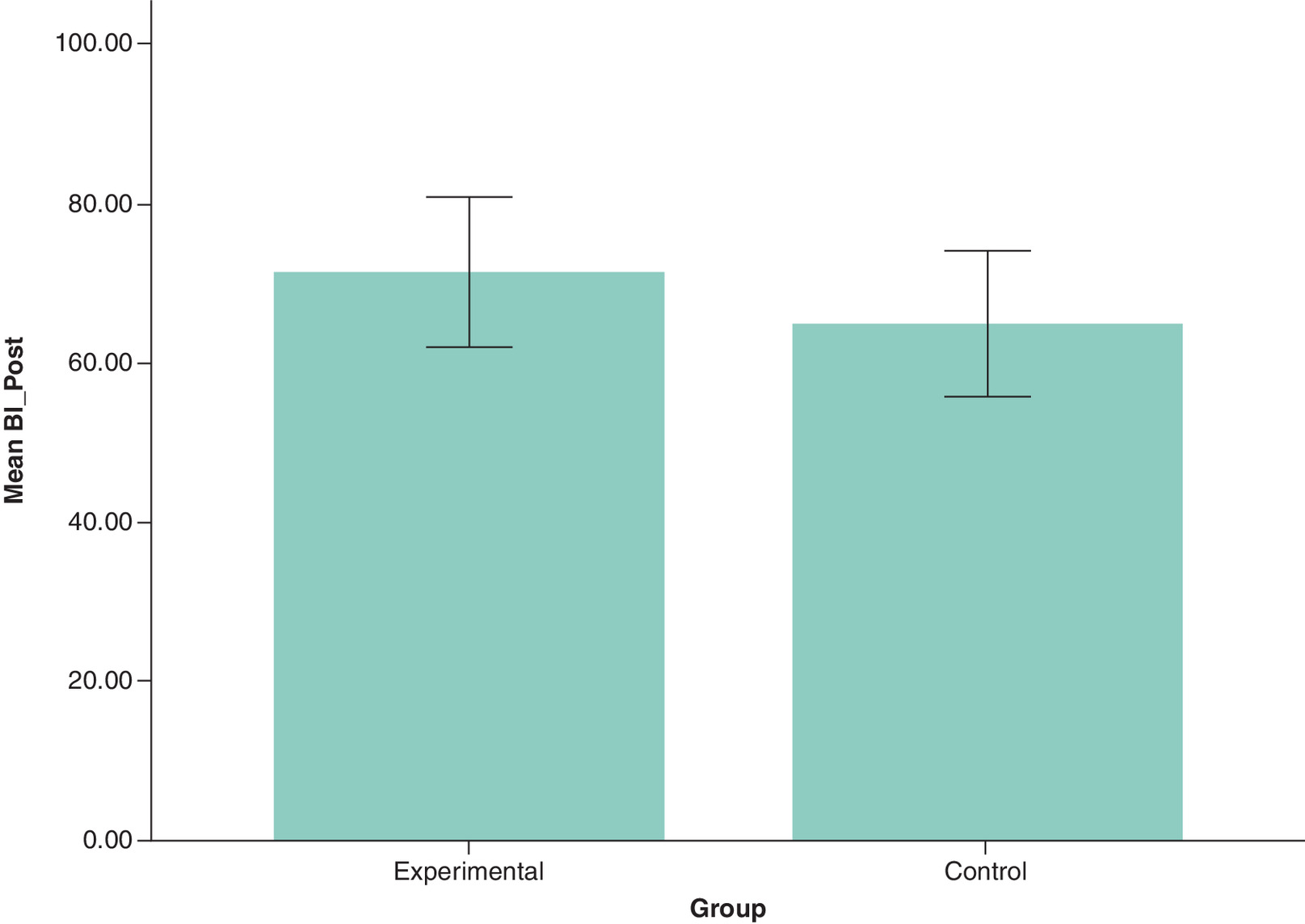
An independent-samples t-test was conducted to compare post-intervention BI scores (BI_post) between the experimental and control groups (Table 6 & Figure 5). The results showed no statistically significant difference in BI_post scores between groups, t(30) = 1.06, p = 0.299. The mean difference was 6.56 (SE = 6.20), with a 95% CI ranging from -6.11 to 19.23, suggesting that the true difference could range from a slight advantage for the control group to a moderate benefit for the experimental group. Cohen's d was approximately 0.37, indicating a small to moderate effect. Although the difference in BI_post scores was not statistically significant (p = 0.299) between the groups, the effect size suggests a potentially meaningful clinical difference favoring the experimental group.
| Comparison | U-value | Z-value | p-value | Mean rank | Effect size (r) | |
|---|---|---|---|---|---|---|
| Experimental | Control | |||||
| MAS_post | 81.00 | -1.85 | 0.065 | 19.44 | 13.56 | -0.33 |
An ANCOVA was conducted to compare BI_post scores between the experimental and control groups, while controlling for baseline BI scores (BI_pre). The overall model was statistically significant, F (2, 29) = 87.83, p < 0.001, indicating that the combination of group assignment and baseline BI_pre scores significantly predicted BI_post outcomes. The covariate BI_pre had a strong and significant effect on BI_post, F (1, 29) = 168.29, p < 0.001, confirming that baseline functional status was a major determinant of post-intervention scores. Importantly, the group effect was statistically significant, F (1, 29) = 21.15, p < 0.001, suggesting that participants in the experimental group achieved significantly higher BI_post scores compared with those in the control group, even after adjusting for baseline differences. The model explained 85.8% of the variance in BI_post scores (R2 = 0.858, Adjusted R2 = 0.849), indicating excellent model fit and strong predictive power (Table 7).
| F(df) | p-value | |
|---|---|---|
| Overall model | 38.47(2, 29) | <0.001 |
| MAS_pre (covariate) | 65.33(1, 29) | <0.001 |
| Group (effect) | 41.89(1, 29) | <0.001 |
| R2/adjusted R2 | 0.726/0.707 | — |
df: Degrees of freedom.
Discussion
Chronic stroke individuals often struggle with sit-to-stand transfers, a key activity of daily living, which increases their fall risk. ADL dependency affects 35% of stroke survivors within the first year [18], highlighting the importance of targeted rehabilitation for this population. This study is a single-blinded, multicenter, randomized controlled trial that aims to evaluate the effectiveness of MRP in improving sit-to-stand transfer and ADL of the chronic stroke population. The study group received 6 weeks of MRP, specifically sit-to-stand transfer training, and the control group received CPT, whereas both groups completed 18 sessions of treatment in total for a duration of 45 min per session. The results of this study found that MRP is more effective in improving sit-to-stand transfer and ADL than the CPT in chronic stroke patients, as evidenced by the improvements in the MAS and BI scores.
The MRP is a task-oriented rehabilitation approach that promotes purposeful movement through repetitive, focused practice of functional activities. It utilizes sensory feedback to help the brain ‘rewire’ itself and improve motor control [10,19]. In our study, we applied MRP specifically to the sit-to-stand transfer, a critical activity for daily living, in chronic stroke patients. The experimental group, which received MRP combined with CPT, showed significant improvements in both sit-to-stand performance and ADL compared with the control group, which received CPT alone. CPT interventions included mat activities, assisted movements, weight-bearing strategies, stretching, strengthening exercises and gait training. Our findings align with those of Sherin U et al., who evaluated MRP combined with mirror therapy and motor imagery techniques in chronic stroke patients. Their study demonstrated enhanced sit-to-stand performance, supporting the effectiveness of MRP-based interventions. Similarly, Ghrouz et al. investigated MRP's impact on balance and postural control when paired with CPT, concluding that MRP was more effective than CPT alone and had lasting benefits – further validating our results [10,12]. In our study, the mean difference in MAS scores for the sit-to-stand component of MRP between pre-test and post-test in the experimental group was 2.17. This is consistent with Sherin U et al.’s reported mean differences of 2.9, 1.1, and 2.17, reinforcing the reliability of our findings [12].
The specificity principle in the MRP for stroke rehabilitation emphasizes training in functional tasks that closely mirror everyday activities. In our study, this principle was applied through sit-to-stand transfers, which simulate routine movements such as adjusting seat heights, varying speeds, and performing stooping actions. This task-specific approach led to substantial improvements in lower limb function among post-stroke patients [9]. Several studies have highlighted sitting and standing as core components of MRP interventions, reinforcing the specificity principle of exercise training, which states that exercises resembling desired functional outcomes yield more effective results [20–23]. George Hornby et al. further emphasized the importance of specificity in post-stroke rehabilitation, noting that targeted training enhances neuroplasticity, cardiovascular function and lower limb performance. These findings support our study's conclusion that MRP-based, specificity-driven interventions significantly contribute to functional recovery in stroke patients [24].
Difficulty in performing ADL is a common challenge among chronic stroke patients, often contributing to physical, cognitive and emotional impairments [25,26]. In light of this, our study aimed to evaluate the effectiveness of the MRP in improving ADL performance in this population. Our findings revealed a significant improvement in ADL among participants in the experimental group, as measured by the BI. The experimental group demonstrated a mean difference of 12.81 in BI scores, compared with just 1.88 in the control group. This substantial improvement is likely attributed to the task-specific nature of MRP, which enhances motor control and functional capacity by targeting and reinforcing movement patterns relevant to daily activities [27]. To optimize post-stroke recovery, rehabilitation strategies must incorporate key elements such as task intensity, specificity of training and enriched sensorimotor experiences. MRP integrates all these components, particularly through sit-to-stand transfer training, which closely mirrors routine functional tasks. This targeted approach not only improves lower limb function but also translates into meaningful gains in ADL performance, reinforcing the clinical value of MRP [28]. Furthermore, the minimal clinically important difference for the BI, as reported by Hsieh et al., is 1.85, highlighting the clinical relevance of our observed improvement and supporting the efficacy of MRP in promoting functional recovery among chronic stroke patients [29].
In stroke rehabilitation, various physical therapy approaches have been employed, including the Bobath approach, PNF, Rood’s approach, CIMT and treadmill training [30,31]. Among these, the MRP has shown superior outcomes. For instance, Langhammer et al. compared MRP with the Bobath approach in tasks such as sitting and hand function, reporting better results in the MRP group. Supporting our findings, Kanase et al. demonstrated that MRP was more effective than CPT in improving both basic and functional mobility in chronic stroke patients. Similarly, Singha et al. found that MRP led to greater improvements in functional mobility compared with PNF techniques. While CPT includes therapeutic exercises such as flexibility and strength training, these interventions alone do not significantly enhance functional mobility [23]. Further evidence comes from studies evaluating treadmill and robotic-assisted therapies. Despite their emphasis on repetitive movement, these approaches have not consistently yielded significant functional improvements and are considered less effective than MRP in chronic stroke rehabilitation [32,33]. Our study is also supported by a recent systematic review by Brown et al., which examined the most effective physical rehabilitation strategies for post-stroke recovery. The review concluded that task-oriented interventions like MRP significantly improve ADL and motor function, with sustained long-term benefits, reinforcing the clinical relevance and efficacy of MRP in promoting recovery and functional independence among stroke patients [31].
Previous studies by Kashoo et al. and Alatawi et al. [14,34] reported that the Bobath/NDT approach remains the most widely used method among physical therapists in Saudi Arabia, often preferred over newer, evidence-based techniques. In contrast, our multicenter, prospective randomized trial – conducted across three tertiary hospitals in Saudi Arabia – demonstrated that the MRP significantly improves sit-to-stand transfers and enhances ADL in chronic stroke patients. By introducing and validating MRP within the Saudi clinical setting, our study offers a valuable contribution to stroke rehabilitation. These findings support the use of task-specific, evidence-based strategies and can help physical therapists improve functional recovery and ADL outcomes for stroke patients across the region.
Clinical implications
The findings of this multicenter trial support the integration of the MRP into stroke rehabilitation protocols in Saudi Arabia. Despite the widespread use of traditional approaches like Bobath/NDT among physical therapists, MRP demonstrated superior outcomes in improving sit-to-stand transfers and ADL in chronic stroke patients [14,34]. Introducing MRP into clinical practice offers a task-specific, evidence-based alternative that can enhance functional recovery and promote greater independence. These results highlight the need to update current rehabilitation guidelines to include MRP as a standard intervention for stroke care in the region.
Study limitations
This study has several limitations that should be considered when interpreting the findings. First, the small sample size of 32 participants may limit the statistical power to detect subtle but clinically meaningful differences between groups, and restricts the generalizability of results to the broader stroke population. Second, the use of convenience sampling from selected rehabilitation centers in Saudi Arabia may introduce selection bias and reduce the representativeness of the sample. Third, despite random assignment, there was a baseline imbalance in MAS scores between groups. Although ANCOVA was applied to adjust for this difference, the possibility of residual confounding cannot be entirely excluded. Additionally, the study was conducted within a specific cultural and healthcare context in Saudi Arabia, where factors such as cultural attitudes toward rehabilitation, family support systems and healthcare access may influence participation and outcomes, potentially limiting the applicability of findings to other regions. Future research should address these limitations by recruiting larger and more diverse samples, using stratified randomization to ensure baseline equivalence, and conducting multinational studies to enhance external validity.
Conclusion
In conclusion, the MRP demonstrates a significant improvement in sit-to-stand transfers and ADL among chronic stroke patients compared with CPT alone. Despite the small sample size and baseline MAS imbalance, these improvements remained robust after statistical adjustment, underscoring MRP’s clinical utility in neurorehabilitation. Our findings highlight the importance of integrating the MRP technique to enhance ADL in the chronic stroke population. This study also encourages physical therapists in Saudi Arabia to adopt MRP as part of their rehabilitation practices.
Summary points
•
Stroke impacts motor and sensory systems, often impairing balance, posture and independence in daily activities.
•
Motor relearning program (MRP) is a task-specific, neuroplasticity-driven approach that uses repetitive, functional training to restore purposeful movement.
•
A multicenter randomized controlled trial was conducted in Saudi Arabia with 32 chronic stroke patients to evaluate MRP’s effectiveness.
•
The experimental group received MRP plus conventional physical therapy, while the control group received conventional physical therapy alone; both completed 18 sessions over 6 weeks.
•
Outcome measures included the sit-to-stand item of the motor assessment scale and the Barthel Index (BI) for activities of daily living (ADL).
•
The MRP group showed significant improvements in the motor assessment scale and BI scores (p < 0.001), with a mean BI change of 12.81 versus 1.88 in the control group.
•
MRP’s task-specific training (e.g., sit-to-stand) aligns with the specificity principle, enhancing lower limb function and activities of daily living performance.
•
Compared with other approaches like Bobath, PNF and constraint-induced movement therapy, MRP demonstrated superior functional outcomes and practical clinical applicability.
•
Despite its effectiveness, MRP remains under-utilized in Saudi Arabia, likely due to limited awareness, training and cultural preferences for traditional methods.
•
Integrating MRP into clinical practice – via therapist education, updated guidelines and curriculum reform – may improve stroke rehabilitation outcomes regionally and globally.
Author contributions
Conceptualization: KA Alfaleh and AR Shaik; methodology: K Balasubramanian, MM Alshehri and RR Sanjeevi; formal analysis: K Balasubramanian, MM Alshehri and RR Sanjeevi; investigation: KA Alfaleh, AR Shaik, WO Alsalem and AM Shahhar; resources: KA Alfaleh, AR Shaik, WO Alsalem and AM Shahhar; data curation: KA Alfaleh, WO Alsalem and AM Shahhar; writing original draft preparation, K Balasubramanian and RR Sanjeevi; writing – review and editing, AR Shaik, MM Alshehri, V Esht, and SA Althoman; supervision: AR Shaik, MM Alshehri, V Esht, and SA Althoman; project administration: AR Shaik, and MA Alshehri; funding acquisition: MA Alshehri and SA Althoman. All authors have read and agreed to the submitted version of the manuscript.
Financial disclosure
This work was supported by a grant from Princess Nourah bint Abdulrahman University, Researchers Supporting Project no. PNURSP2025R714, Riyadh, Saudi Arabia. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This study was approved by the Ethics Committee of King Saud Medical City (KSMC); approval no.: H1RE-24-May22-01, Al-Jouf Health Affairs; approval no.: 2022.19 and Prince Sultan Bin AbdulAziz Humanitarian City (SBAHC); approval no.: 85-2022-IRB. All participants provided written informed consent prior to enrolment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. The data will not be made publicly available.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
Murphy SJX, Werring DJ. Stroke: causes and clinical features. Medicine (Abingdon) 48(9), 561–566 (2020).
2.
He Q, Wang W, Zhang Y et al. Global, regional, and national burden of stroke, 1990–2021: a systematic analysis for global burden of disease 2021. Stroke 55(12), 2815–2824 (2024).
3.
Mahfouz AA, Abdelmoneim SA, Abdu SMM et al. Understanding the stroke burden in Saudi Arabia: trends from 1990 to 2019 and forecasting through time series analysis. Neurosci. J. 30(1), 49–58 (2025).
4.
O'Sullivan SB, Schmitz TJ. O'Sullivan & Schmitz's Physical Rehabilitation (8th Edition). F. A. Davis Company, NY, USA (2024).
5.
Shahid J, Kashif A, Shahid MK. A comprehensive review of physical therapy interventions for stroke rehabilitation: impairment-based approaches and functional goals. Brain Sci. 13(5), 717 (2023).
6.
Alhusayni AI, Alzahrani AH. A systematic review of physical therapy rehabilitation for stroke survivors in Arab countries and Saudi Arabia: current approaches and future challenges. SMJ 46(9), 976–984 (2025).
7.
O'Rourke C, Edwards D. The effectiveness of the motor relearning program on upper limb function post-stroke: a systematized review. Phys. Ther. Rev. 29(1–3), 87–100 (2024).
8.
Ghrouz A, Marco E, Muñoz-Redondo E, Boza R, Ramirez-Fuentes C, Duarte E. The effect of motor relearning on balance, mobility and performance of activities of daily living among post-stroke patients: study protocol for a randomised controlled trial. Eur. Stroke J. 7(1), 76–84 (2022).
9.
Carr JH, Shepherd RB. A Motor Relearning Programme for Stroke (2nd edition ). Aspen Publishers, Inc, Oxford: MD, USA (1987).
10.
Ghrouz A, Guillen-Sola A, Morgado-Perez A et al. The effect of a motor relearning on balance and postural control in patients after stroke: an open-label randomized controlled trial. European Stroke J. 9(2), 303–311 (2024).
11.
Kanase SB. Effect of motor relearning programme and conventional training on functional mobility in post stroke patients. Ind. J. Public Health Res. Dev. 11(5), 496–501 (2020).
12.
Hitha Sherin U, Prem Kumar BN. Effect of motor re-learning program with motor imagery on sit-to-stand activity in stroke. J. Rehab. Pain Med. 1(1), doi: (2022).
13.
Alqahtani MM, Kashoo FZ, Ahmad F. Current scenario of evidence-based practice and rationale of preferred approach in stroke rehabilitation among physiotherapists in Saudi Arabia: a cross-sectional survey. Saudi J. Health Sci. 7(1), 53 (2018).
14.
Alatawi SF. Current clinical practices of saudi physiotherapists in stroke rehabilitation. J. Acute Care Phys. Ther. 12(4), 194 (2021).
15.
Esht V, Alshehri MM, Balasubramanian K et al. Transcranial direct current stimulation (tDCS) for neurological disability among subacute stroke survivors to improve multiple domains in health-related quality of life: randomized controlled trial protocol. Neurophysiologie Clinique 54(3), 102976 (2024).
16.
Conradsen I, Henriksen M, Rytter HM. Predictive validity of motor assessment scale on poststroke discharge destination. Rehab. Res. Pract. 2024(1), 2914252 (2024).
17.
Zhou M, Liu X, Zha F et al. Stroke outcome assessment: optimizing cutoff scores for the Longshi Scale, modified rankin scale and Barthel Index. PLoS ONE 16(5), e0251103 (2021).
18.
Appelros P, Nydevik I, Terént A. Living setting and utilisation of ADL assistance one year after a stroke with special reference to gender differences. Disabil. Rehabil. 28(1), 43–49 (2006).
19.
Maier M, Ballester BR, Verschure PFMJ. Principles of neurorehabilitation after stroke based on motor learning and brain plasticity mechanisms. Front. Syst. Neurosci. 13, 74 (2019).
20.
Ammann BC, Knols RH, Baschung P, de Bie RA, de Bruin ED. Application of principles of exercise training in sub-acute and chronic stroke survivors: a systematic review. BMC Neurol. 14, 167 (2014).
21.
Hawley JA. Specificity of training adaptation: time for a rethink? J. Physiol. 586(Pt 1), 1–2 (2008).
22.
Langhammer B, Stanghelle JK. Can physiotherapy after stroke based on the Bobath concept result in improved quality of movement compared to the motor relearning programme. Physiother. Res. Int. 16(2), 69–80 (2011).
23.
Singha R. Motor relearning program versus proprioceptive neuromuscular facilitation technique for improving basic mobility in chronic stroke patients-a comparative study. Int. J. Physiother. Res. 5, 2490–2500 (2017).
24.
George Hornby T, Straube DS, Kinnaird CR et al. Importance of specificity, amount, and intensity of locomotor training to improve ambulatory function in patients poststroke. Topics Stroke Rehab. 18(4), 293–307 (2011).
25.
Legg LA, Lewis SR, Schofield-Robinson OJ, Drummond A, Langhorne P. Occupational therapy for adults with problems in activities of daily living after stroke. Cochrane Database Syst. Rev. 2017(7), CD003585 (2017).
26.
Wurzinger HE, Abzhandadze T, Rafsten L, Sunnerhagen KS. Dependency in activities of daily living during the first year after stroke. Front. Neurol. 12, 736684 (2021).
27.
Bhalerao G, Kulkarni V, Doshi C, Rairikar S, Shyam A, Sancheti P. Comparison of motor relearning program versus bobath approach at every two weeks interval for improving activities of daily living and ambulation in acute stroke rehabilitation. Int. J. Sci. Basic App. Res. (IJSBAR) 3, 2277–210370 (2013).
28.
Fisher BE, Sullivan KJ. Activity-dependent factors affecting poststroke functional outcomes. Topics Stroke Rehab. 8(3), 31–44 (2001).
29.
Hsieh Y-W, Wang C-H, Wu S-C, Chen P-C, Sheu C-F, Hsieh C-L. Establishing the minimal clinically important difference of the Barthel Index in stroke patients. Neurorehabil. Neural. Repair 21(3), 233–238 (2007).
30.
Shahid J, Kashif A, Shahid MK. A comprehensive review of physical therapy interventions for stroke rehabilitation: impairment-based approaches and functional goals. Brain Sci. 13(5), 717 (2023).
31.
Todhunter-Brown A, Sellers CE, Baer GD et al. Physical rehabilitation approaches for the recovery of function and mobility following stroke. Cochrane Database Syst. Rev. 2(2), CD001920 (2025).
32.
Prange GB, Jannink MJA, Groothuis-Oudshoorn CGM, Hermens HJ, Ijzerman MJ. Systematic review of the effect of robot-aided therapy on recovery of the hemiparetic arm after stroke. J. Rehabil. Res. Dev. 43(2), 171–184 (2006).
33.
Eng JJ, Tang PF. Gait training strategies to optimize walking ability in people with stroke: a synthesis of the evidence. Expert Rev. Neurother. 7(10), 1417–1436 (2007).
34.
Alqahtani MM, Kashoo FZ, Ahmad F. Current scenario of evidence-based practice and rationale of preferred approach in stroke rehabilitation among physiotherapists in Saudi Arabia: a cross-sectional survey. Saudi J. Health Sci. 7(1), 53–64 (2018)
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 25 August 2025
Accepted: 5 November 2025
Published online: 9 December 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Effectiveness of motor relearning program in sit-to-stand transfer and activities of daily living among chronic stroke patients – a prospective, multicenter, randomized controlled trial. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0133
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yee Mah, Vassilios Tahtis, Abigail Beddard, Aryan Esfandiari, Jorge Cardoso, Parashkev Nachev, Toward automation of motor assessments in stroke: Proof-of-concept model to interpret balance and gait in stroke patients, Archives of Rehabilitation Research and Clinical Translation, 10.1016/j.arrct.2026.100673, (100673), (2026).