Healthcare cost and utilization before and after the development of significant tricuspid regurgitation by age, sex and race
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: The impact of significant tricuspid regurgitation (sTR) on healthcare costs and utilization in real-world populations remains understudied. Aim: Describe healthcare costs and utilization before and after development of sTR and describe differences by patient demographic characteristics. Materials & methods: We conducted a retrospective, longitudinal descriptive study using a large database containing electronic health record and insurance claims data for US patients. Healthcare costs and utilization are summarized for up to 3 years prior to sTR and for 1 year after sTR. Results: Costs and utilization increased in the 3 years leading up to and the year after sTR. Costs were higher for patients who were: aged 50–79 years, male, and Black or Hispanic (p < 0.01). Cardiovascular hospitalizations were an important driver of costs in all groups. Patients aged 80 years and over, women, and Black nonHispanic patients had fewer outpatient visits to cardiac specialists in the year following sTR (p < 0.01). Conclusion: Healthcare costs and utilization of patients with TR increase as clinical disease progresses, with important differences by age, sex and race. Increasing recognition of signs of TR progression and improved outpatient cardiac specialty access may be important means to reduce heart failure hospitalization duration as well as overall costs.
Plain language summary
What is this article about?
Tricuspid regurgitation (TR) is a heart valve condition that can progress in terms of symptoms and severity over time. The purpose of this article is to understand if there are differences by age, sex and race/ethnicity in healthcare cost and visits leading up to and after severe or symptomatic (significant) TR disease.
What methodology was used in this study?
This is a retrospective observational study. Researchers identified a group of patients with significant tricuspid regurgitation (sTR) in a real-world database that has information from medical records and insurance claims and examined their demographic, baseline comorbidities, costs and healthcare visits in the study period.
What were the results?
Descriptive trends showed that healthcare costs and visits increased leading up to a patient’s sTR status date. There were differences in trends by demographic subgroup leading up to significant disease, specifically patients under age 80 years had higher costs and days in hospital but fewer outpatient cardiology visits than patients over age 80 years. Male patients had higher costs and healthcare visits overall compared with female patients. Lastly, Black and Hispanic patients had higher costs and healthcare utilization in most visit types compared with White patients. Most of these trends were consistent across demographic subgroups the year after clinical significance was reached for TR.
Why are these results important?
These results suggest that cost and healthcare visit patterns for patients with sTR are not the same for all patients and that some patients may experience a higher cost and healthcare visit burden than others. Understanding differences in patient cost and healthcare history may help improve clinical decision making at the time of sTR disease identification.
Tricuspid regurgitation (TR) is an increasingly common heart valve disease [1], with clinically significant disease most prevalent in older adults and women [2]. A recent study estimated 700,000 Medicare beneficiaries had a record of nonrheumatic tricuspid valve disease between 2011 and 2019 [3]. TR has long been considered the ‘innocent bystander’ to other valve diseases with which it frequently co-occurs, but this concept has been challenged in recent years with evidence that TR is independently associated with higher all-cause and cardiovascular mortality [4]. Furthermore, the progression of TR is not straightforward, and not all patients with TR identified by echocardiography will go on to develop severe TR. However, once severe TR develops, it is associated with higher mortality [5,6]. Additionally, a diagnosis of severe TR is often associated with typical heart failure symptoms including shortness of breath, fatigue, decreased exercise tolerance, abdominal distension, early satiety and edema. Once symptoms are present, prognosis and quality of life are markedly reduced [7,8].
Evidence regarding the impact of TR on healthcare costs and utilization is limited [9]. In particular, more information is needed on how healthcare costs and utilization patterns change in patients with TR both preceding and following severe or symptomatic (significant) TR status. Demographic subgroup analyses are also needed to identify how these patterns differ by age, sex, race and ethnicity categories. In this study, we describe the healthcare costs and utilization of sTR patients in the 3 years prior to and the year after development of sTR both overall and by demographic subgroups. Early identification of utilization and cost patterns in TR patients by demographic categories may have important clinical and economic implications.
Materials & methods
Data source
This retrospective cohort study used data from the Optum Market Clarity database (years 2007–2023), one of the largest repositories of longitudinal, de-identified, multipayer data from real-world patients in the US. The data source contains medical and pharmacy claims from UnitedHealthcare covered members (including Medicare Advantage beneficiaries) and clearinghouse data from other payers that are linked with electronic health records which include physician notes that are converted to semi-structured fields via natural language processing [10]. Patient data used to perform this analysis contained no identifiers and were accessed in compliance with the Health Insurance Portability and Accountability Act. Institutional review board approval was not required for this study.
Patient selection
Our analysis included TR patients, age 50 and older, who reached significant tricuspid regurgitation (sTR) status between January 2018 and December 2023. We defined the sTR population as those patients who had either a record of severe, massive or torrential TR in physician notes, or patients with a record of TR diagnosis (ICD-10: I36.1 nonrheumatic tricuspid valve insufficiency) who subsequently developed at least three of seven characteristic signs and symptoms (ascites, edema, liver disease, chronic kidney disease, extreme fatigue, weight loss and right ventricular dysfunction), as recorded in electronic health records or claims data (diagnostic codes, lab values or physician notes and findings as available). The list was generated in consultation with expert physicians and has been used to identify clinically sTR patients in previous research [11]. Details of the patient identification algorithm are provided in Supplementary Table 1A.
The index date for the analysis was the date on which the sTR definition was first met. Measures were assessed for a look-back period of up to 3 years, and a follow-up period of up to 1 year from index (Figure 1). Continuous enrollment for the 12 months preceding the index date (Year -1) was required. For Year -2 and Year -3, patients were included if they had continuous enrollment for the full year. For the year after index (Year +1), patients were included in the estimates if they had at least 1 day of enrollment past the index date.
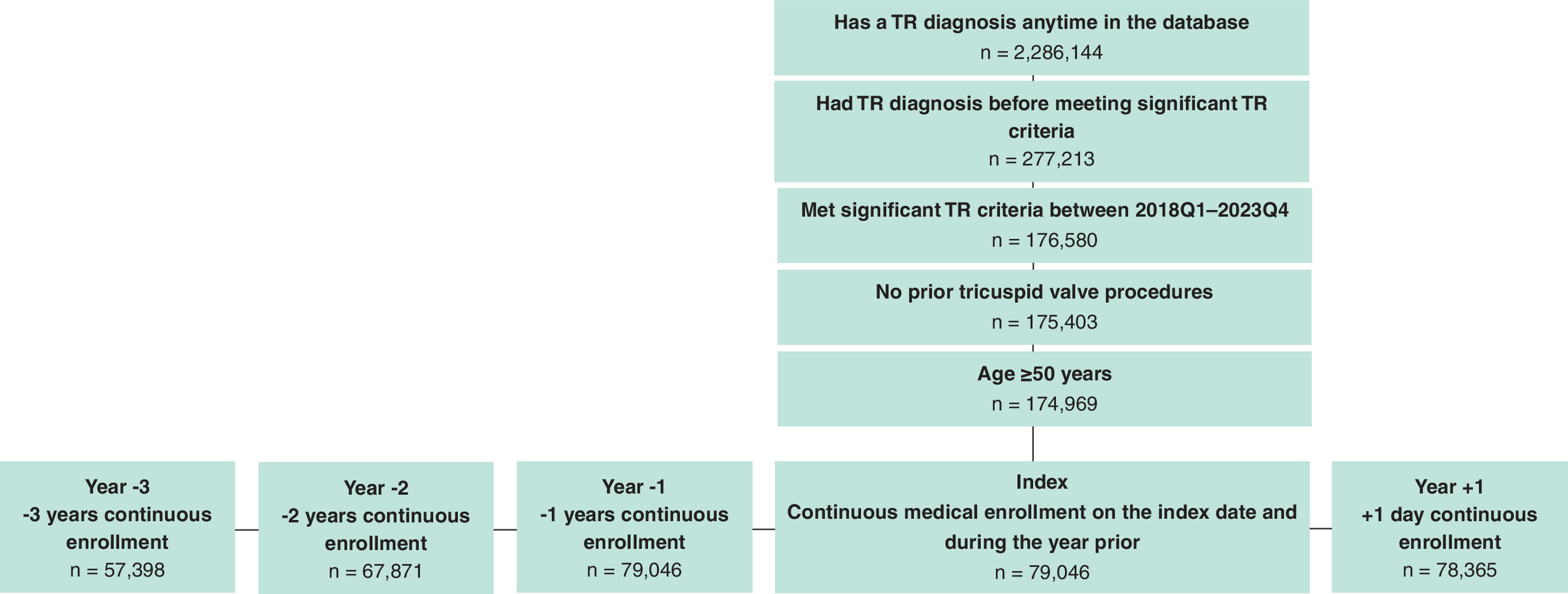
Figure 1. Cohort attrition.
TR: Tricuspid regurgitation.
Measures
Cost measures included total healthcare costs, total inpatient costs and inpatient costs attributed to cardiac disease or heart failure. Index encounter costs were not included since patients could reach an sTR status through a range of visit intensity types and visit reasons. Medication costs were not included in the analysis. Utilization measures consisted of the yearly number of all-cause, cardiovascular, heart failure, and urgent/emergent inpatient admissions, days in the hospital, emergency department encounters, outpatient visits overall and outpatient cardiac specialist visits specifically. Comorbidities were captured using ICD-10 codes. The Elixhauser comorbidity index was computed according to established methods to assess overall comorbidity burden [12].
Statistical analysis
This was a descriptive, longitudinal analysis of retrospective data. Summary statistics were generated using means and standard deviations for continuous variables and frequency and percentage of patients for categorical variables. Patient characteristics of age, sex and race/ethnicity are reported as mutually exclusive categories: 50–79 years and ≥80 years for age, male and female for sex, White nonHispanic, Black nonHispanic and Hispanic for race/ethnicity. Elixhauser comorbidity index scores and specific comorbidities are reported overall and stratified by age, sex and race/ethnicity categories.
Costs, number of inpatient admissions, and all other utilization measures were trimmed at the 99th percentile to reduce the influence of outlying values. Measures were annualized for Year +1 patients who died or did not have a full year of medical enrollment. All costs were inflation-adjusted to 2023 constant US dollar values [13]. Differences in means between demographic cohorts were tested using t-tests (age, sex) or ANOVA with subsequent Tukey tests for each pairwise comparison (race/ethnicity).
Results
A total of 79,046 patients with sTR were included in the analysis at index and Year -1 (Figure 1). Most (99.4%) patients met sTR criteria by having a TR diagnosis and 3 or more clinical findings while only 0.5% of patients entered via physician note of severity alone (Supplementary Table 1B). Chronic kidney disease, liver disease and edema were present in ≥90% of patients, whereas few patients had a record of ascites (16.7%), weight loss (7.8%), right heart dysfunction (0.1%) or fatigue (0.1%). Over half (56.8%) of patients had a TR diagnosis for at least 3 years prior to reaching sTR status, and 86.9% had a TR diagnosis at any time before the index encounter.
Patient characteristics
Table 1 displays patient characteristics present in the data during the index encounter for sTR. Slightly more than half of patients were female (54.3%), with a mean age of 72 years. Most patients were White nonHispanic (73.3%) and had Medicare coverage (69.5%). The mean Elixhauser score was 9.5. Sixty-seven percent of patients had congestive heart failure and most patients (80.3%) had one or more additional valvular pathologies, with mitral regurgitation being the most prevalent (75%).
| All sTR patients | |
|---|---|
| Patients, n | 79,046 |
| Age, mean (SD) | 72.4 (10.5) |
| Female, n (%) | 42,959 (54.3) |
| Race/ethnicity, n (%) | |
| White, nonHispanic | 57,960 (73.3) |
| Black, nonHispanic | 11,950 (15.1) |
| Hispanic | 2720 (3.4) |
| Other/unknown* | 6416 (8.1) |
| Payor | |
| Medicare | 54,968 (69.5%) |
| Commercial | 18,129 (22.9%) |
| Medicaid | 5663 (7.2%) |
| Unknown | 286 (0.4%) |
| Elixhauser score, mean (SD) | 9.5 (3.9) |
| Comorbidities, n (%) | |
| Atrial fibrillation | 41,110 (52.0) |
| Other valve disease | 63,456 (80.3) |
| Aortic stenosis | 27,794 (27.6) |
| Aortic regurgitation | 19,631 (24.8) |
| Mitral stenosis | 24,587 (31.1) |
| Mitral regurgitation | 59,286 (75.0) |
| Congestive heart failure | 52,721 (66.7) |
| Kidney disease | 46,368 (58.7) |
| On dialysis | 3751 (4.7) |
| Diabetes | 46,637 (59.0) |
| Stroke or TIA | 28,526 (36.1) |
| Dementia | 11,962 (15.1) |
| Cancer | 8613 (10.9) |
| COPD | 37,753 (47.8) |
| Oxygen dependence | 11,605 (14.7) |
COPD: Chronic obstructive pulmonary disease; sTR: Significant tricuspid regurgitation; SD: Standard deviation; TIA: Transient ischemic attack.
Table 2 displays baseline characteristics by demographic subgroups. Patients aged 80 years and older had higher prevalence of most comorbidities, except diabetes, cancer and being on dialysis. Men and women had generally similar rates of comorbidities, with somewhat higher rates of dementia, oxygen dependence and stroke in women and most cardiovascular diagnoses in men. Black patients had higher prevalence of congestive heart failure, chronic obstructive pulmonary disorder, kidney disease and stroke. Hispanic patients had higher prevalence of diabetes. White patients had higher prevalence of atrial fibrillation and prior diagnosis of other valve diseases.
| Age (years) | Sex | Race/ethnicity | |||||
|---|---|---|---|---|---|---|---|
| 50–79 | 80+ | Female | Male | Black | Hispanic | White | |
| Patients, n† | 53,086 | 25,960 | 42,959 | 36,072 | 11,950 | 2720 | 57,960 |
| Age, mean (SD) | 66.8 (8.1) | 83.9 (2.3)§ | 73 (10.5) | 71.8 (10.4)§ | 69.5 (10.6)§ | 70 (10.8)§ | 73.2 (10.3) |
| Female, n (%) | 27,833 (52.4%) | 15,126 (58.3%) | 42,959 (100%) | 0 (0%) | 7317 (61.2%) | 1492 (54.9%) | 30,717 (53%) |
| Race/ethnicity, n (%) | |||||||
| White, nonHispanic | 37,329 (70.3%) | 20,631 (79.5%) | 30,717 (71.5%) | 27,238 (75.5%) | 0 (0%) | 0 (0%) | 57,960 (100%) |
| Black, nonHispanic | 9244 (17.4%) | 2706 (10.4%) | 7317 (17%) | 4632 (12.8%) | 11,950 (100%) | 0 (0%) | 0 (0%) |
| Hispanic | 2047 (3.9%) | 673 (2.6%) | 1492 (3.5%) | 1226 (3.4%) | 0 (0%) | 2720 (100%) | 0 (0%) |
| Other/unknown | 4466 (8.4%) | 1950 (7.5%) | 3433 (8.0%) | 2,976 (8.3%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Elixhauser, mean (SD) | 9.5 (4.0) | 9.6 (3.5)§ | 9.4 (3.9) | 9.7 (3.8)§ | 10.3 (4)§ | 9.8 (4)§ | 9.3 (3.8) |
| Comorbidities, % | |||||||
| Atrial fibrillation | 23,904 (45%) | 17,206 (66.3%)¶ | 20,400 (47.5%) | 20,700 (57.4%)¶ | 4796 (40.1%)¶ | 1168 (42.9%)¶ | 31,901 (55%) |
| Other valve disease‡ | 40,833 (76.9%) | 22,623 (87.1%)¶ | 34,177 (79.6%) | 29,268 (81.1%)¶ | 8989 (75.2%)¶ | 2072 (76.2%)¶ | 47,177 (81.4%) |
| Aortic stenosis | 11,251 (21.2%) | 10,543 (40.6%)¶ | 11,255 (26.2%) | 10,537 (29.2%)¶ | 2212 (18.5%)¶ | 630 (23.2%)¶ | 17,252 (29.8%) |
| Aortic regurgitation | 10,937 (20.6%) | 8694 (33.5%)¶ | 9870 (23%) | 9754 (27%)¶ | 2503 (20.9%)¶ | 588 (21.6%)¶ | 14,965 (25.8%) |
| Mitral stenosis | 14,405 (27.1%) | 10,182 (39.2%)¶ | 13,951 (32.5%) | 10,633 (29.5%)¶ | 2960 (24.8%)¶ | 755 (27.8%)¶ | 18,907 (32.6%) |
| Mitral regurgitation | 38,267 (72.1%) | 21,019 (81%)¶ | 32,111 (74.7%) | 27,164 (75.3%) | 8374 (70.1%)¶ | 1922 (70.7%)¶ | 44,110 (76.1%) |
| Congestive heart failure | 33,323 (62.8%) | 19,398 (74.7%)¶ | 27,303 (63.6%) | 25,404 (70.4%)¶ | 8454 (70.7%)¶ | 1794 (66%) | 37,966 (65.5%) |
| Kidney disease | 28,253 (53.2%) | 18,115 (69.8%)¶ | 24,192 (56.3%) | 22,163 (61.4%)¶ | 7903 (66.1%)¶ | 1675 (61.6%)¶ | 32,420 (55.9%) |
| On dialysis | 3041 (5.7%) | 710 (2.7%)¶ | 1657 (3.9%) | 2092 (5.8%)¶ | 1058 (8.9%)¶ | 254 (9.3%)¶ | 1940 (3.3%) |
| Diabetes | 32,438 (61.1%) | 14,199 (54.7%)¶ | 24,557 (57.2%) | 22,067 (61.2%)¶ | 8452 (70.7%)¶ | 2021 (74.3%)¶ | 31,606 (54.5%) |
| Stroke or TIA | 17,167 (32.3%) | 11,359 (43.8%)¶ | 15,804 (36.8%) | 12,714 (35.2%)¶ | 4770 (39.9%)¶ | 1023 (37.6%)¶ | 20,181 (34.8%) |
| Dementia | 4560 (8.6%) | 7402 (28.5%)¶ | 7037 (16.4%) | 4922 (13.6%)¶ | 2013 (16.8%)¶ | 458 (16.8%)¶ | 8419 (14.5%) |
| Cancer | 5972 (11.2%) | 2,641 (10.2%)¶ | 4703 (10.9%) | 3908 (10.8%)¶ | 1278 (10.7%) | 225 (8.3%)¶ | 6394 (11%) |
| COPD | 25,076 (47.2%) | 12,677 (48.8%)¶ | 20,349 (47.4%) | 17,400 (48.2%)¶ | 5934 (49.7%)¶ | 1145 (42.1%)¶ | 27,734 (47.9%) |
| Oxygen dependence | 7663 (14.4%) | 3942 (15.2%)¶ | 6730 (15.7%) | 4874 (13.5%)¶ | 1750 (14.6%) | 349 (12.8%)¶ | 8543 (14.7%) |
†
Patients with missing demographic data (sex, n = 15; race, n = 6416) were excluded.
‡
Other valve disease defined as having any or all of the following: aortic stenosis, aortic regurgitation, mitral stenosis, mitral regurgitation.
§
Indicates significant differences at p < 0.05 compared with the reference group using a t-test.
¶
Indicates significant differences at p < 0.05 compared with the reference group using Fisher’s exact test.
COPD: Chronic obstructive pulmonary disease; sTR: Significant tricuspid regurgitation; SD: Standard deviation; TIA: Transient ischemic attack.
Measures in the total population
We observed an increase in the intensity of care prior to sTR status, with increases in costs and utilization outcomes throughout the study period (Table 3). Total costs increased each year from a mean of $30,887 in Year -3 to $95,276 (annualized) in Year +1. Cardiovascular-related hospitalizations accounted for most of the total inpatient costs in each year observed and were on average the most frequent type of admission per year. The average number of outpatient visits per patient per year increased from 20.4 in Year -3 to 28.6 in Year +1; outpatient visits to cardiac specialists comprised 12–13% of all outpatient visits on average for all years.
| Year -3 Mean (SD) | Year -2 Mean (SD) | Year -1 Mean (SD) | Year +1† Mean (SD) | |
|---|---|---|---|---|
| n | 57,398 | 67,871 | 79,046 | 78,365 |
| Total costs | $30,887 (55,291) | $36,974 (63,816) | $59,225 (86,195) | $95,276 (145,517) |
| $11,148 [3,797-33,468] | $13,741 [4,615-41,061] | $27,549 [8,819-73,351] | $33,887 [9,241-110,572] | |
| Inpatient costs | $13,918 (39,933) | $17,500 (46,990) | $32,299 (66,060) | $54,868 (110,618) |
| $0 [0–7,597] | $0[0–13,566] | $0 [0–36,109] | $0 [0–52,472] | |
| Cost of CV admissions | $9610 (33,580) | $12,513 (39,887) | $24,035 (56,616) | $38,927 (89,633) |
| $0 [0–0] | $0 [0–0] | $0 [0–22,173] | $0 [0–26,223] | |
| Cost of HF admissions | $2852 (17,585) | $4055 (21,636) | $8863 (32,741) | $15,567 (50,163) |
| $0 [0–0] | $0 [0–0] | $0 [0–0] | $0 [0–0] | |
| All cause admissions | 0.54 (1.16) | 0.63 (1.28) | 1.07 (1.65) | 1.84 (3.04) |
| % with any | 30.1% | 33.8% | 49.6% | 48.5% |
| CV admissions | 0.30 (0.74) | 0.37 (0.84) | 0.65 (1.14) | 1.02 (1.93) |
| 19.8% | 23.3% | 37.1% | 35.1% | |
| HF admissions | 0.04 (0.23) | 0.05 (0.28) | 0.12 (0.44) | 0.19 (0.63) |
| 3.1% | 4.3% | 9.0% | 10.4% | |
| Hospital days (all cause), n | 2.82 (8.46) | 3.72 (10.59) | 6.92 (14.21) | 13.88 (27.59) |
| 30.1% | 33.8% | 49.6% | 48.5% | |
| Emergency department visits | 0.52 (1.12) | 0.58 (1.19) | 0.78 (1.37) | 0.88 (1.78) |
| 28.8% | 31.4% | 39.6% | 33.6% | |
| Outpatient visits | 20.4 (18.8) | 21.6 (20.0) | 24.7 (21.9) | 28.6 (30.2) |
| 97.6% | 97.6% | 98.0% | 88.2% | |
| Outpatient visits to cardiac specialists | 2.54 (3.89) | 2.72 (4.02) | 3.20 (4.32) | 3.54 (5.44) |
| 58.2% | 60.7% | 66.8% | 57.4% |
All costs are reported in 2023 USD (United States dollar) and were trimmed at 99th percentile.
†
Cost and utilization measures in the year post-significant TR were annualized to a full year for patients without a full year of follow-up due to death or lack of continuous enrollment.
CV: Cardiovascular; HF: Heart failure; sTR: Significant tricuspid regurgitation; SD: Standard deviation.
Measures by age
Results by age are shown in Figure 2A. Total healthcare costs and number of days in the hospital were higher for patients under 80 years old for all years (p < 0.01). Patients 80 years or older had significantly more heart failure hospitalizations (HFHs) on average in Year +1 (p < 0.01), whereas age groups did not differ in the prior 3 years. For cardiac specialist visits, adults 80 years and older averaged significantly more visits per year for the 3 years prior to sTR but significantly fewer visits in Year +1 (p < 0.01 for all years).
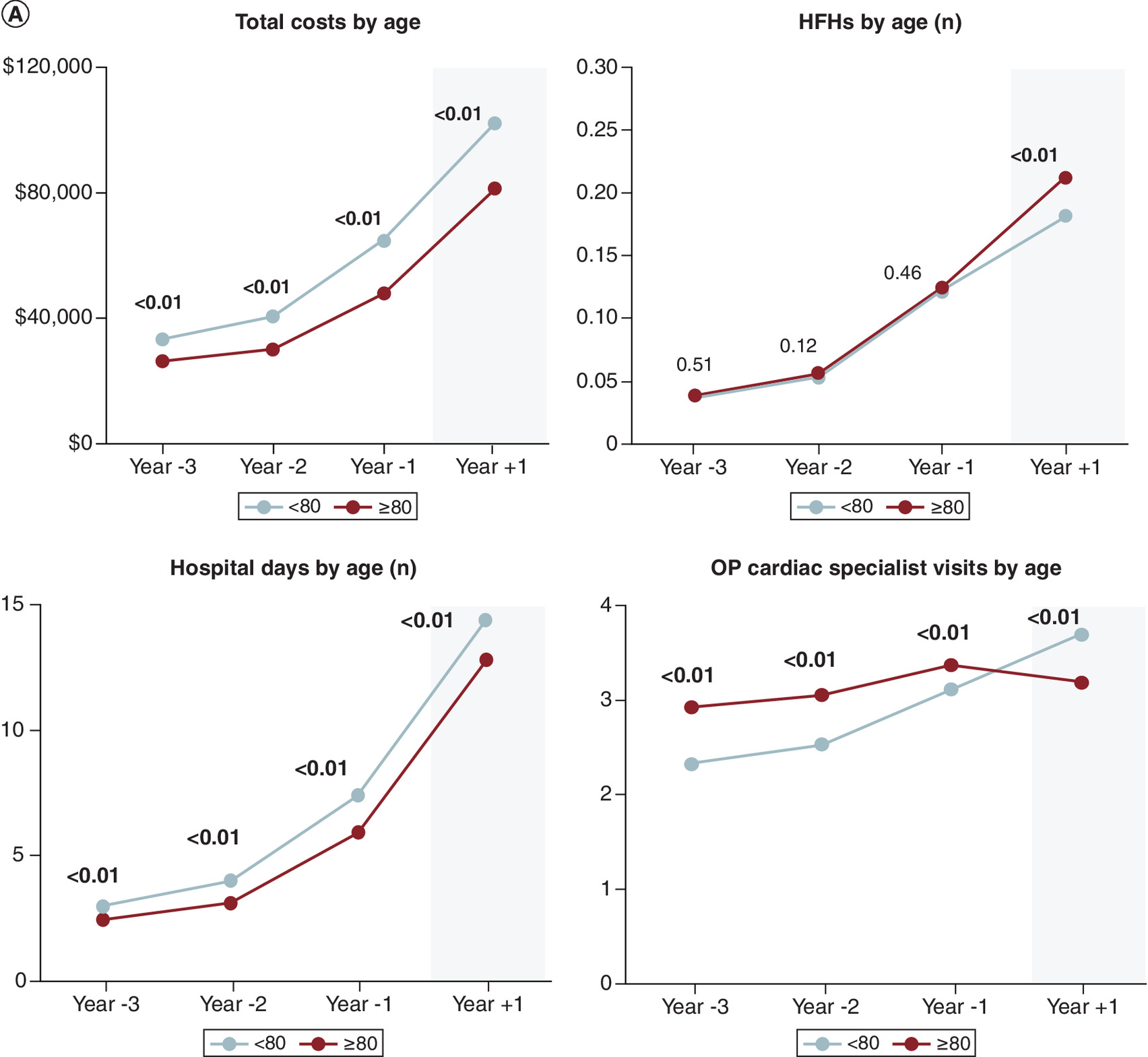
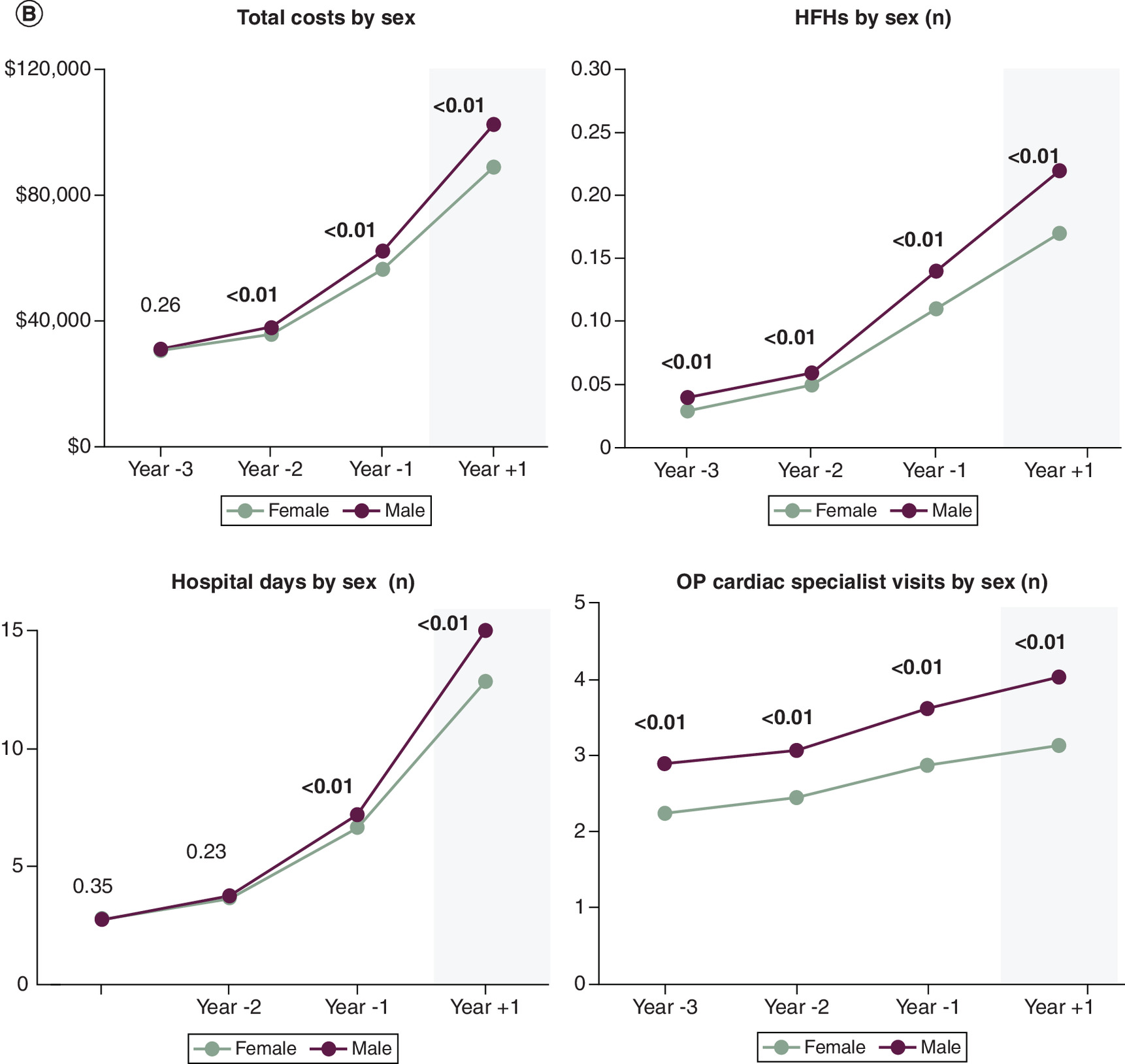
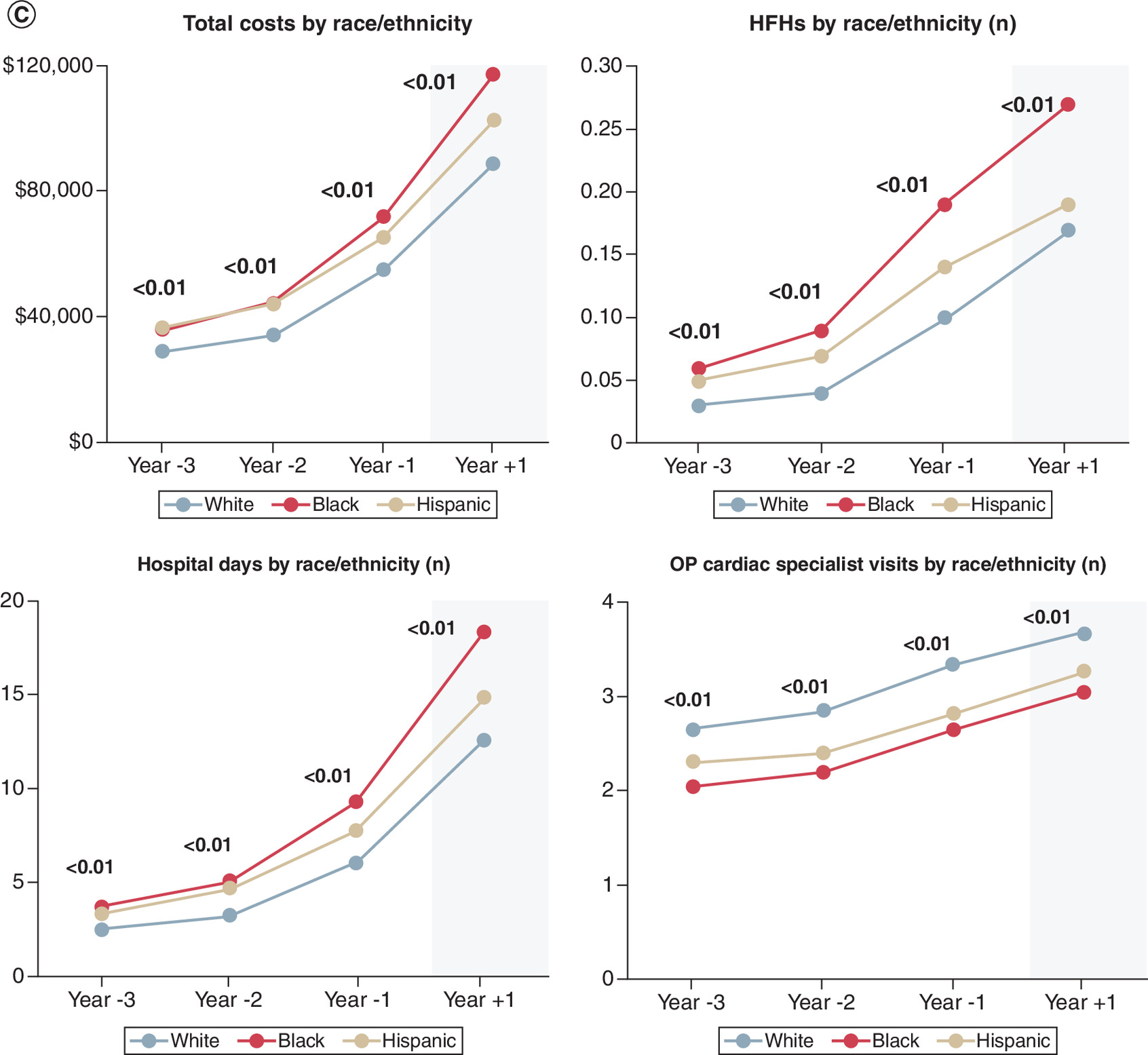
Figure 2. Healthcare cost and utilization before and after significant tricuspid regurgitation.
(A) Healthcare cost and utilization before and after significant TR by age. 95% CIs are on order of the graph point size and therefore not displayed. (B) Healthcare cost and utilization before and after significant TR by sex. 95% CIs are on order of the graph point size and therefore not displayed. (C) Healthcare cost and utilization before and after significant TR by race/ethnicity. 95% CIs are on order of the graph point size and therefore not displayed; see Supplementary Table 2 for Tukey’s test p-values.
HFH: Heart failure hospitalizations; OP: Outpatient; TR: Tricuspid regurgitation.
Measures by sex
Figure 2B displays results by sex. Male and female patients had similar costs in Year -3, but in all other years, costs for males were higher (p < 0.01). Male patients had significantly more HFHs and more outpatient visits to cardiac specialists than female patients in all years (p < 0.01 for all years). Male patients also had a significantly higher number of days in the hospital in Year -1 and Year +1 (p < 0.01 for both years).
Measures by race/ethnicity
Figure 2C displays results by race/ethnicity (Tukey’s test p-values in Supplementary Table 2). Black patients had higher total costs, more HFHs, more days in the hospital, and fewer cardiac specialist outpatient visits than White patients (p < 0.01 for all years). The pattern for Hispanic patients compared with White patients was similar, with the exception that there was no significant difference in HFHs during Year +1 (p = 0.64; all other p < 0.05). Compared with Hispanic patients, Black patients had higher total costs and more days in the hospital in Year -1 and Year +1 (p < 0.01 for both in both years) and more HFHs for all years (p < 0.01 for all). Black patients had fewer cardiac specialist visits than Hispanic patients during Year -3 only (p = 0.02).
Discussion
The results of this retrospective longitudinal analysis of multipayer data in the Optum Market Clarity database showed healthcare costs and utilization increased in the years leading up to and following sTR status. Cardiovascular hospitalizations were the primary driver of inpatient costs, but outpatient cardiac specialist care represented only a small proportion of total outpatient visits. There were also significant differences across demographic subgroups in terms of disease burden and healthcare utilization trends which impacted overall costs. Together, these data provide important insights into the clinical trajectory of TR, associated healthcare utilization patterns and demographic differences along the care pathway in patients with significant TR.
The findings of our analysis are consistent with past literature reporting the substantial impact of HFH in TR patients [1], and worsening TR severity with development of characteristic symptoms [7,14]. The current study illustrates a rising burden of costs associated with progression of TR and the development of clinically sTR. Nearly 87% of patients had a diagnosis of TR prior to the index encounter, many of them up to 3 years prior, consistent with progression of valvular heart disease that is often seen in clinical practice. Most patients in this study had additional valvular heart disease pathologies, with a predominance of mitral regurgitation (75%). Further, approximately two-thirds of patients were diagnosed with congestive heart failure before or at the time of meeting criteria for sTR, a finding frequently encountered clinically in the setting of hypervolemia that accompanies heart failure exacerbations. The presence of heart failure in patients with sTR has been shown to increase their healthcare utilization and costs compared with sTR patients without heart failure [15].
We observed a high intensity of care in the sTR cohort across all demographic groups. Increased medical care needs were identified leading up to sTR, with continued increases in costs and utilization once patients entered sTR status. Mean total costs more than tripled from Year -3 to Year +1 in the study, and cardiovascular-related inpatient hospitalization was a primary driver of increased cost associated with sTR. More than 50% of hospitalizations were urgent/emergent, and there were relatively low rates of outpatient cardiac specialist visits, suggesting patient cohorts with limited access to cardiac specialty care or those with frailty are underserved with regards to outpatient specialty access. More research is needed on whether improving outpatient specialty care for those patients with TR disease progression may be one avenue to avoid disruptive and expensive inpatient admissions.
Examining TR progression by age, sex and race/ethnicity revealed variable relationships between total healthcare costs and three utilization measures (HFHs, days in the hospital and outpatient visits to cardiac specialists). Specifically, by age, patients under 80 years had higher costs, equal HFHs, more days in the hospital and fewer outpatient cardiac specialist visits compared with those 80 years and over. By sex, male patients experienced higher costs, higher HFHs, more days in the hospital, and more outpatient cardiac specialist visits than female patients. By race/ethnicity, nonWhite patients had higher costs, more HFHs, more days in the hospital and fewer cardiac specialist visits compared with White patients. These results suggest that one mechanism of reducing costs may be via increased access to outpatient cardiac specialist visits, particularly among older and nonWhite patients, thereby reducing HFHs and days in the hospital. Further prospective work is needed to more comprehensively elucidate these relationships.
Understanding real-world patterns of TR progression to significant status may support clinical decision-making. For instance, older and more frail patients who may not be eligible for surgery are still at risk of hospitalization for heart failure and may benefit from minimally invasive transcatheter approaches [16]. Also, a consensus on risk stratification for patients to aid with clinical decision-making when faced with a patient with progressive TR is lacking. Treating patients before the development of severe right ventricular dysfunction and associated clinical symptomatology and heart failure risk may reduce heart failure related hospital admissions and associated costs. However, little guidance is presently available to consistently define and assess right ventricular dysfunction to help determine appropriate timing of intervention [17,18].
There are study limitations, including a lack of quality-of-life metrics and further clinical details, including specific cardiac testing results. Proxy definitions were required for disease severity as echocardiogram data is limited to small subset of patients in the Optum Market Clarity database. These proxy definitions are not intended to replicate TR severity classifications used in physician guidelines [19]. Valve disease has been found to be under-reported in community-based screening studies [20], and patients without a record of TR diagnosis would be missed by our proxy query. The study was observational and descriptive in nature, meaning that causal relationships between observed events cannot be assumed. Patients were not required to be enrolled during measurement Year -2 and Year -3 to be included in the study and therefore subject analysis across time periods was not conducted. Future trend research might evaluate the change in slope across demographic groups leading up to a sTR status. This study compares complete (pre years) to annualized (post year) costs; the accuracy of annualized costs diminishes with fewer months of available data and prior published work has found an absolute error between actual annual costs and annualized costs of $2700 for Medicare patients [21]. Additionally, annualizing costs may introduce bias by including patients with increased medical complexities and high short-term costs (but less than 12 months of follow-up) compared with patients who have all 12 months of follow-up available in the database. Finally, trends may be confounded by age, sex and race/ethnicity representativeness within each demographic category. A regression model adjusting for these differences would be relevant in future analyses assessing cost and clinical events in this population.
Conclusion
Annual costs before sTR increase over time and continue to increase as clinical disease progresses. Higher costs among Black patients as well as those 50–79 years old, were associated with more HFHs and an increased number of hospital days. Increasing recognition of TR progression in patients at high risk of sTR development, in addition to research on improved outpatient cardiac specialty access, may be an important means to reduce HFH duration as well as overall costs.
Summary points
•
Existing healthcare cost and utilization research on patients with significant tricuspid regurgitation (sTR) disease has not documented how trends differ based on demographic subgroups leading up to a significant disease status.
•
The study population of sTR had a high burden of comorbidities, with most patients experiencing congestive heart failure, kidney disease and other valve disease.
•
Healthcare costs and utilization for patients with sTR increased steadily in the 3 years before and the year after sTR status.
•
Costs were higher for patients aged 50–79 years, males and Black or Hispanic individuals, with cardiovascular hospitalizations being the main driver of inpatient expenses.
•
Patients under 80 years had more hospital days, while those 80 years and older had more heart failure hospitalizations after sTR.
•
Outpatient visits to cardiac specialists represented only a small proportion of total outpatient visits, and were especially low among patients aged 80+ years, women and Black nonHispanic patients after sTR.
•
Male patients had higher costs, more hospital days and more cardiac specialist visits than female patients in all years studied.
•
Research on improving outpatient cardiac specialty access, especially for older and nonWhite patients, may help researchers understand heart failure hospitalizations and overall healthcare costs in this population.
Acknowledgments
The authors thank D Frame for her assistance in writing the manuscript.
Financial disclosure
The present analysis and manuscript was supported by Edwards Lifesciences.
Competing interests disclosure
D Cork, F Medina, P Gaba, R Yeh and C Barker report administrative support, article publishing charges, statistical analysis and writing assistance were provided by Edwards Lifesciences Corportion. L Kemp, A Dratch, R Horn, S Murphy and S Mollenkopf report financial support was provided by Edwards Lifesciences Corporation. L Kemp, A Dratch, R Horn, S Murphy and S Mollenkopf report a relationship with Edwards Lifesciences Corporation that includes: employment. R Yeh reports the following relationships: Abbott Vascular Inc, Boston Scientific, Edwards Lifesciences, Elixir Medical and Medtronic relationships include: consulting and research grants; JenaValve and Siemens relationships that include: research grants; CathWorks, FastWave, Magenta Medical and Shockwave relationships that include: consulting. C Barker reports relationships with Alleviant, Boston Scientific, Edwards Lifesciences Corporation and Medtronic that include: consulting. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical data that have been shared with them, and that the use of this shared data is in accordance with the terms (if any) agreed upon their receipt.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary data.docx)
- Download
- 28.27 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Kolte D, Kennedy KF, Passeri JJ, Inglessis I, Elmariah S. Temporal trends in prevalence of tricuspid valve disease in hospitalized patients in the United States. Am. J. Cardiol. 125(12), 1879–1883 (2020).
2.
Singh JP, Evans JC, Levy D et al. Prevalence and clinical determinants of mitral, tricuspid, and aortic regurgitation (the Framingham Heart Study). Am. J. Cardiol. 83, 897–902 (1999).
3.
Vemulapalli S, Kerr MSD, Roberts GJ, Prillinger JB, Meduri CU, McCarthy P. Tricuspid valve disease prevalence and the impact of tricuspid valve surgery on cardiovascular events and hospital resource use in Medicare beneficiaries. Am. Heart J. 245, 100–109 (2022).
4.
Tung M, Nah G, Tang J, Marcus G, Delling FN. Valvular disease burden in the modern era of percutaneous and surgical interventions: the UK Biobank. Open Heart 9(2), e002039 (2022).
5.
Topilsky Y, Maltais S, Medina Inojosa J et al. Burden of tricuspid regurgitation in patients diagnosed in the community setting. JACC Cardiovasc. Imaging 12, 433–442 (2019).
6.
Shahim A, Hourqueig M, Lund LH et al. Long-term outcomes in heart failure with preserved ejection fraction: predictors of cardiac and non-cardiac mortality. ESC Heart Fail. 10, 1835–1846 (2023).
7.
Sadeghpour A, Hassanzadeh M, Kyavar M et al. Impact of severe tricuspid regurgitation on long term survival. Res. Cardiovasc. Med. 2, 121–126 (2013).
8.
Barker CM, Cork DP, McCullough PA et al. Comparison of survival in patients with clinically significant tricuspid regurgitation with and without heart failure (from the Optum Integrated File). Am. J. Cardiol. 144, 125–130 (2021).
• Reports the overall clinical burden of patients with tricuspid regurgitation (TR) disease from a claims database.
9.
Cork DP, McCullough PA, Mehta HS et al. The economic impact of clinically significant tricuspid regurgitation in a large, administrative claims database. J. Med. Econ. 23, 521–528 (2020).
• Reports the overall economic burden of patients with TR disease from a claims database.
10.
Optum, Inc. (2025). Market Clarity: linked EHR and claims data. (Accessed: 28 January 2025). Available at: https://business.optum.com/en/data-analytics/life-sciences/real-world-data/market-clarity-data.html
11.
Madhavan MV, Barker CM, Kemp LS et al. Real-world clinical outcomes and health care utilization in patients with severe tricuspid regurgitation. Struct. Heart 9, 100463 (2025).
•• Follows clinical and cost outcomes in a similarly defined patient population as the current analysis for 3-years after the onset of a severe, symptomatic TR status.
12.
Moore BJ, White S, Washington R, Coenen N, Elixhauser A. Identifying increased risk of readmission and in-hospital mortality using hospital administrative data: the AHRQ Elixhauser Comorbidity Index. Med. Care 55, 698–705 (2017).
13.
U.S. Bureau of Labor Statistics. (2025). Consumer Price Index. (Accessed: 25 June 2025). Available at: https://www.bls.gov/cpi/
14.
Barker C, Kemp L, He S et al. SA70 Identifying early disease progression in tricuspid regurgitation when echocardiographic imaging data is unavailable. Value Health 27(Suppl. 6), S408 (2024).
15.
Chung CH. Healthcare utilization and expenditures in patients with tricuspid regurgitation: a population-based cohort study. Int. J. Cardiol. Heart Vasc. 54, 101495 (2024).
16.
Gröger M, Friedl S, Ouerghemmi D et al. TRI-SCORE is superior to EuroSCORE II and STS-Score in mortality prediction following transcatheter edge-to-edge tricuspid valve repair. Clin. Res. Cardiol. 112, 1436–1445 (2023).
17.
Ricci F, Bufano G, Galusko V et al. Tricuspid regurgitation management: a systematic review of clinical practice guidelines and recommendations. Eur. Heart J. Qual. Care Clin. Outcomes 8, 238–248 (2022).
18.
Anastasiou V, Bazmpani MA, Daios S et al. Unmet needs in the assessment of right ventricular function for severe tricuspid regurgitation. Diagnostics (Basel) 13(18), 2885 (2023).
19.
Writing Committee Members; Otto CM, Nishimura RA, Bonow RO et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 77(4), e25–e197 (2021).
• Provides the physician guidelines for identification, treatment and management of TR.
20.
d'Arcy JL, Coffey S, Loudon MA et al. Large-scale community echocardiographic screening reveals a major burden of undiagnosed valvular heart disease in older people: the OxVALVE Population Cohort Study. Eur. Heart J. 37, 3515–2522 (2016).
21.
Linden A, Samuels SJ. Estimating error when annualizing healthcare costs. J. Eval. Clin. Pract. 19, 933–937 (2013).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 12 September 2025
Accepted: 25 November 2025
Published online: 11 December 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Healthcare cost and utilization before and after the development of significant tricuspid regurgitation by age, sex and race. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0146
Export citation
Select the citation format you wish to export for this article or chapter.