Racial and ethnic differences in diagnosis, healthcare utilization and 1-year outcomes for patients with significant tricuspid regurgitation
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: The impact of race and ethnicity on prognosis and clinical outcomes in patients with significant tricuspid regurgitation (sTR) is not well understood. Aim: Describe healthcare utilization trends preceding the development of sTR and assess clinical outcomes 1-year post-sTR status by race and ethnicity. Materials & methods: We conducted a retrospective, longitudinal descriptive study using data from a large database containing electronic health record and insurance claims information. We employed multivariate modeling to assess the relationship between 1-year clinical outcomes and mutually exclusive race/ethnicity groups and other baseline factors. Results: Black patients were more likely to be identified as having sTR as inpatients when compared with White patients (p < 0.001) and had fewer outpatient visits to cardiac specialists before and after developing sTR (p < 0.01). Black and Hispanic patients with sTR were at increased risk of heart failure hospitalization compared with White patients at 1 year (adjusted HR: 1.21, 95% CI: 1.16–1.26, p < 0.001 and adjusted HR: 1.10, 95% CI: 1.02–1.19, p < 0.05 respectively). However, both Black and Hispanic patients had lower 1-year mortality than White patients in the adjusted model. Conclusion: Black and Hispanic patients are less likely to have received outpatient care by a cardiac specialist prior to the development of sTR, and have higher rates of heart failure hospitalization after diagnosis. In contrast, their mortality rates following sTR identification are lower than White patients. Further investigation into the underlying mechanisms of these observations is needed to improve TR-related outcomes.
Plain language summary
What is this article about?
Tricuspid regurgitation (TR) is a heart valve condition that can progress in terms of symptoms and severity over time. The purpose of this article is to understand if there are differences in healthcare pathways leading up to and clinical outcomes after significant symptoms and severity are present that are related to race and ethnicity.
What methodology was used in this study?
This a retrospective observational study. Researchers identified a group of patients with significant TR (sTR) in a real-world database that has information from medical records and insurance claims and examined their demographic and clinical characteristics as well as 1-year health outcomes.
What were the results?
Race and ethnicity categories were related to the kind of healthcare patients received leading up to a time point when their TR was identified as significant and to how often patients were hospitalized for heart failure or died in the year after. Before sTR, Black and Hispanic patients received more acute care compared with White patients and White patients received more outpatient cardiac specialist care compared with Black and Hispanic patients. After significant TR, Black and Hispanic patients were at increased risk of heart failure hospitalization compared with White patients, while White patients were at increased risk of death compared with Black and Hispanic patients.
Why are these results important?
These results suggest that race and ethnicity may play a role in healthcare experiences and outcomes for people with sTR. The findings highlight differences in care and outcomes, emphasizing the need for healthcare providers and systems to address these differences. Understanding and reducing such differences is important for making sure all patients receive high-quality, equitable care for sTR, ultimately improving health for everyone.
Tricuspid regurgitation (TR) is a common valve disorder that frequently co-occurs with other valve disease and increases in prevalence with age [1]. Once TR is present, the risk of mortality increases in parallel with progression in its severity [2,3]. Surgical treatment is infrequent and postoperative outcomes remain poor, due to at least in part to the late presentation and surgical management of advanced disease [4,5]. Our understanding of the pathophysiology and clinical outcomes for patients with TR continues to evolve, with recent research highlighting increasing prevalence with age and anatomic differences, higher prevalence, and poorer prognosis for women than for men [5].
The impact of race and ethnicity on prognosis and clinical outcomes in patients with TR is not as well understood. Racial/ethnic disparities in the burden and outcomes of cardiovascular disease, in general, have been studied and are especially pronounced among non-Hispanic Black Americans [6,7]. These disparities have persisted despite decades of research and public policy efforts [8,9], driven by a complex interplay of clinical, social, and structural factors [7,10]. For TR specifically, while a recent study looked at racial/ethnic differences in the clinical course of severe TR within a single healthcare system in New York City, nationwide data remain limited [11].
Given the diverse US population, understanding healthcare use – including timeliness of evaluation and diagnosis – and outcomes across different patient racial and ethnic groups holds important clinical and health policy implications. Accordingly, we conducted a descriptive analysis of real-world patterns of healthcare utilization and cost for patients developing significant TR (sTR) across the US. In that study [12], we observed a high intensity of care for sTR across all demographic groups, with increased risk of hospitalization in the post-sTR period for Black and Hispanic patients. The current analysis examines clinical outcomes in the year after sTR status by race and ethnicity in greater depth, with adjustment for baseline covariates.
Materials & methods
This study is a retrospective, longitudinal cohort study using patient records from linked claims and electronic health record (EHR) data to identify and follow sTR patients.
Data source
This study used Optum’s de-identified Market Clarity Data (years 2007–2023). The data source is one of the largest repositories of longitudinal data from real-world patients in the US, containing medical and pharmacy claims from a large national payer and additional third-party payers, linked with clinical data from EHRs [13]. Patient data used to perform this analysis were de-identified and accessed in compliance with the Health Insurance Portability and Accountability Act. Institutional review board approval was not required for this study due to its retrospective, observational and anonymized nature. To categorize patients’ race and ethnicity, Market Clarity incorporates patient self-reported values as captured in the EHR.
Patient selection
The analysis was conducted in a population of adults aged 50 years and above with TR who developed sTR between January 2018 and December 2023. As in the related analysis [12], sTR was defined by criteria generated in consultation with expert physicians; patients with either severe, massive or torrential TR in physician notes, or a TR diagnosis (International Classification of Diseases, 10th revision [ICD-10]: I36.1 non-rheumatic tricuspid valve insufficiency) and subsequent development of at least three of seven conditions – ascites, edema, liver disease, chronic kidney disease, extreme fatigue, weight loss and/or right ventricular dysfunction were classified as having sTR. Continuous health plan enrollment was required for the 12 months prior to patients meeting the definition of sTR (year -1) to give adequate time to capture comorbidities and TR-related symptoms. For year -2 and year -3, patients were included if they had continuous enrollment for the full year. Patients were also required to be alive and enrolled for at least 1 day after meeting criteria for sTR. Patients with missing race or ethnicity information, or those from categories with very low counts in the database (e.g., Asian) were excluded from the analysis.
Patient characteristics
Patients were grouped by race and ethnicity using three mutually exclusive categories: Hispanic (regardless of concurrent race category), White non-Hispanic and Black non-Hispanic. Baseline characteristics were assessed at the time of meeting the sTR definition. Comorbidities were captured using ICD-10 codes as previously described [12]. To give an assessment of overall comorbidity burden, the Elixhauser comorbidity index was computed according to established procedures [14]. Inpatient status at the time of sTR identification was also captured.
Outcomes
The primary outcomes were all-cause death and heart failure hospitalization during the year after identification of sTR. Mortality data are captured from EHR and claims data sources and supplemented with external data sources including the Social Security Death Master File, Centers for Medicare and Medicaid services data and obituaries. Linkages to external mortality data are incorporated into the patient record by the database provider for high degree of confidence matches. In addition to the two main outcomes, we examined measures of healthcare utilization both 3 years before and 1 year after sTR: urgent or emergent hospital admissions, emergency department visits and outpatient cardiac specialist visits.
Statistical analysis
Black and Hispanic patient groups were compared with the White group on all baseline characteristics using t-tests for continuous variables and chi-square tests for categorical variables. Categorical variables are reported as counts and percentages and continuous variables as means and standard deviations (SD). Survival analysis curves were calculated for 1-year all-cause death (Kaplan–Meier) and heart failure hospitalization (cumulative incidence function for a competing risk of death). Unadjusted and adjusted hazard ratios comparing Black and Hispanic to White patients were calculated for all 1-year events with hazard models (Cox proportional or Fine–Gray subdistribution, as appropriate). Model adjustment included all baseline characteristics included in Table 1. Finally, baseline characteristics were examined as explanatory variables for all-cause death and heart failure hospitalization using Cox proportional and Fine–Gray subdistribution hazard models respectively. Eight explanatory variable models were run – four each for all-cause death and heart failure hospitalization (overall, White, Black, Hispanic). Values of p less than 0.05 were considered significant. All statistics were calculated in R.
| White | Black† | Hispanic† | |
|---|---|---|---|
| n | 57,960 | 11,950 | 2720 |
| Age, mean (SD) | 73.2 (10.3) | 69.5 (10.6) | 70.0 (10.8) |
| Sex-Female, n (%) | 30,722 (53.0) | 7318 (61.2) | 1494 (54.9) |
| Census region, n (%) | |||
| Midwest | 32,586 (56.2) | 5685 (47.6) | 719 (26.4) |
| South | 12,478 (21.5) | 3194 (26.7) | 940 (34.6) |
| Northeast | 9563 (16.5) | 2770 (23.2) | 760 (27.9) |
| West | 3333 (5.8) | 302 (2.5) | 301 (11.1) |
| Payor, n (%) | |||
| Medicare | 41,458 (71.5) | 7630 (63.8) | 1721 (63.3) |
| Commercial | 13,760 (23.7) | 2575 (21.5) | 625 (23.0) |
| Medicaid | 2742 (4.7) | 1745 (14.6) | 374 (13.8) |
| Elixhauser score, mean (SD) | 9.3 (3.8) | 10.2 (4.0) | 9.8 (4.0) |
| Comorbidities, n (%) | |||
| Atrial fibrillation | 31,901 (55.0) | 4796 (40.1) | 1168 (42.9) |
| Other valve disease | 49,436 (85.3) | 9575 (80.1) | 2185 (80.3) |
| Coronary artery disease | 40,377 (69.7) | 8070 (67.5) | 1877 (69.0) |
| Peripheral artery disease | 35,821 (61.8) | 7700 (64.4) | 1836 (67.5) |
| Congestive heart failure | 37,966 (65.5) | 8454 (70.7) | 1794 (66.0) |
| Hypertension | 56,073 (96.7) | 11,795 (98.7) | 2650 (97.4) |
| Pulmonary hypertension | 19,074 (32.9) | 4479 (37.5) | 823 (30.3) |
| Liver disease | 54,184 (93.5) | 11,052 (92.5) | 2563 (94.2) |
| Kidney disease | 32,420 (55.9) | 7903 (66.1) | 1675 (61.6) |
| CKD 5 or ESRD | 3095 (5.3) | 1577 (13.2) | 339 (12.5) |
| Diabetes | 31,606 (54.5) | 8452 (70.7) | 2021 (74.3) |
| Stroke or TIA | 20,181 (34.8) | 4770 (39.9) | 1023 (37.6) |
| Dementia | 8419 (14.5) | 2013 (16.8) | 458 (16.8) |
| Cancer | 6394 (11.0) | 1278 (10.7) | 225 (8.3) |
| COPD | 27,734 (47.9) | 5934 (49.7) | 1145 (42.1) |
| Other | |||
| Prior valve intervention (non-tricuspid), n (%) | 3390 (5.8) | 272 (2.3) | 114 (4.2) |
| Pacemaker, n (%) | 2798 (4.8) | 388 (3.2) | 112 (4.1) |
| Oxygen dependence, n (%) | 8543 (14.7) | 1750 (14.6) | 349 (12.8) |
| Inpatient at time of sTR, n (%) | 28,002 (48.3) | 6578 (55.0) | 1312 (48.2) |
| OP cardiac specialist visits in year prior to sTR, M (SD) | 3.35 (4.42) | 2.66 (3.98) | 2.84 (4.03) |
†
Bold values are significantly different from values for White patients at p < 0.05.
CKD 5: Chronic kidney disease stage 5; COPD: Chronic obstructive pulmonary disease; ESRD: End-stage renal disease; OP: Outpatient; SD: Standard deviation; sTR: Significant tricuspid regurgitation; TIA: Transient ischemic attack.
Results
In total, 72,630 patients met all inclusion and exclusion criteria for this study at the time they reached sTR status (Figure 1 for attrition details). The vast majority of patients met sTR criteria due to concomitant comorbid conditions such as chronic kidney disease, liver disease and edema following a previous TR diagnosis – the number of patients meeting sTR criteria with a physician’s note indicating severe or torrential TR was small (less than 2% for all race/ethnicity groups; Supplementary Table 1).
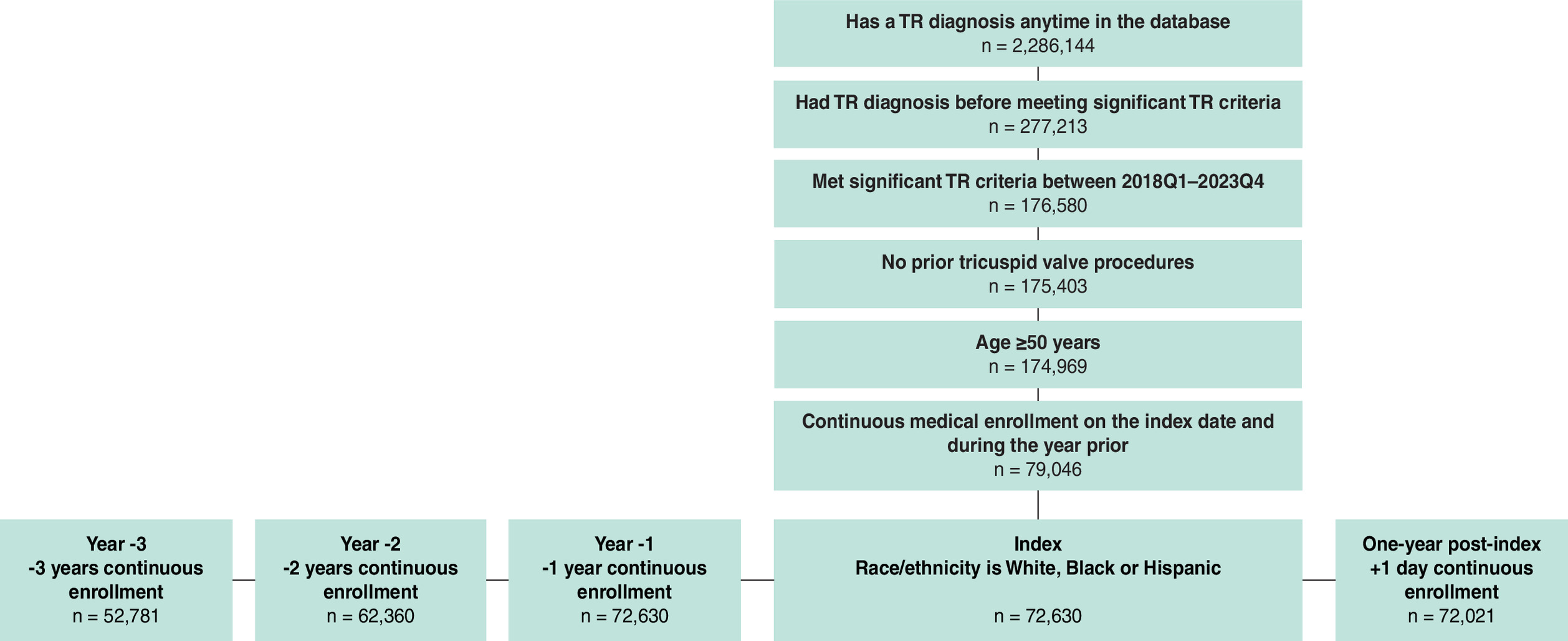
Figure 1. Cohort attrition.
n: Number of patients; TR: Tricuspid regurgitation.
Baseline characteristics
Across race/ethnicity groups, the majority of patients were White (79.8%), female (54.4%), Medicare beneficiaries (70%) and from the Midwest (53.7%). Mean patient age was 72.5 years (SD 10.5 years), and mean Elixhauser comorbidity score was 9.5 (SD 3.9). Comorbidity burden increased over time, both in the years prior to the development of sTR and the year after (Supplementary Table 2).
Table 1 displays baseline characteristics by race/ethnicity category. Black and Hispanic patients were younger on average than White patients. Black and Hispanic patients had higher rates of diabetes and kidney disease, while White patients had higher rates of atrial fibrillation and valve diseases other than TR.
Healthcare utilization & TR diagnosis prior to meeting sTR criteria
Over half (56.8%) of patients had a TR diagnosis 3 years prior to developing sTR. Black patients were less likely to have a prior diagnosis of TR when compared with White (p < 0.001) and Hispanic (p < 0.001) patients. Black patients reached sTR status during inpatient admissions significantly more often than White patients (55 vs 48.3%, p < 0.001), but Hispanic patients (48.2%) did not differ significantly from White patients (p = 0.95).
Black patients had more urgent/emergent admissions and emergency department visits than White patients for all 3 years prior (year -3, year -2 and year -1) to the development of sTR (Figure 2). Black patients also had more urgent/emergent admissions than Hispanic patients for all prior years, and more emergency department visits in year -2 and year -1. Hispanic patients had more emergency department visits than White patients for all three prior years, but only differed on urgent/emergent admissions in year -1. White patients had more outpatient cardiac specialist visits than Black and Hispanic patients for all years prior to developing sTR. Hispanic patients also had more outpatient cardiac specialist visits than Black patients in year -3 but not in year -2 or year -1.
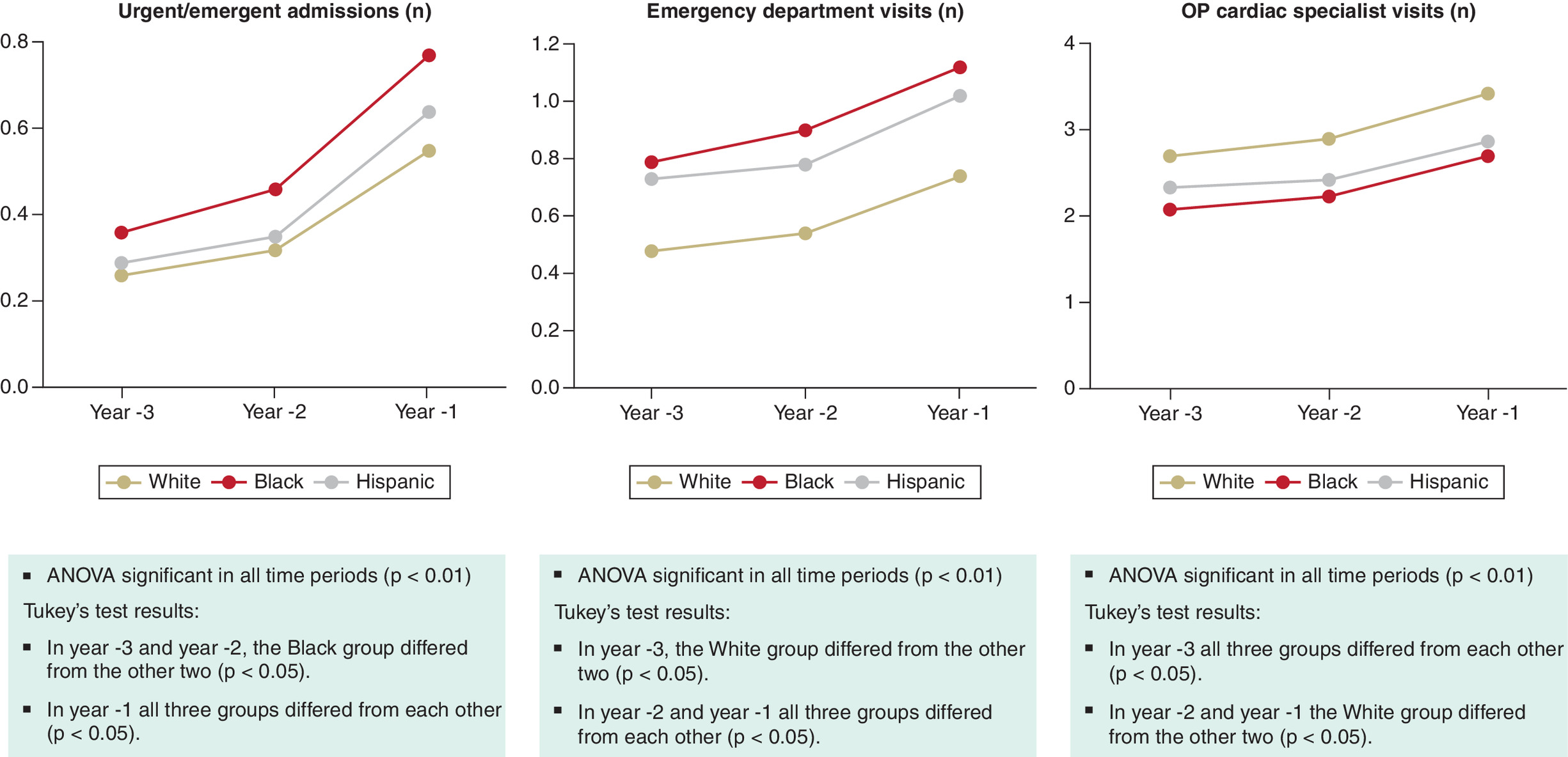
Figure 2. Healthcare utilization measures before significant tricuspid regurgitation, by race/ethnicity.
OP: Outpatient.
Healthcare utilization & health outcomes 1-year post-sTR
Table 2 shows the adjusted hazard ratios (HRs) for healthcare utilization measures 1-year after the development of sTR. Trends were similar to those seen prior to meeting sTR criteria. After adjustment, Black patients had higher rates of urgent/emergent admissions (p < 0.001) and emergency department visits (p < 0.001) but fewer cardiac specialist visits (p < 0.01) compared with White patients. Hispanic patients did not differ from White patients for urgent/emergent admissions or outpatient cardiac specialist visits, but did have higher rates of emergency department visits (p < 0.001). See Supplementary Table 3 for unadjusted hazard ratios.
| 1-year measures | Black | Hispanic | ||||
|---|---|---|---|---|---|---|
| HR† | (95% CI) | p-value | HR† | (95% CI) | p-value | |
| Time to death (all-cause)‡ | 0.84 | (0.80, 0.88) | <0.001 | 0.86 | (0.78, 0.95) | <0.01 |
| Time to heart failure hospitalization§ | 1.21 | (1.16, 1.26) | <0.001 | 1.10 | (1.02, 1.19) | 0.014 |
| Time to urgent/emergent admission§ | 1.15 | (1.11, 1.19) | <0.001 | 0.97 | (0.91, 1.05) | 0.49 |
| Time to emergency department visit§ | 1.16 | (1.12, 1.20) | <0.001 | 1.13 | (1.05, 1.20) | <0.001 |
| Time to outpatient cardiac specialist visit§ | 0.96 | (0.93, 0.99) | <0.01 | 1.03 | (0.97, 1.08) | 0.34 |
†
Hazard ratios are adjusted for all baseline characteristics in Table 1, with White patients as the reference group.
‡
Calculated using Cox proportional hazards models.
§
Calculated using Fine–Gray subdistribution hazard models.
CI: Confidence interval; HR: Hazard ratio.
Figure 3 displays the Kaplan–Meier curve for death in the year after development of sTR by race/ethnicity. After adjustment for baseline characteristics (Table 1), Black and Hispanic patients both had a lower risk of death compared with White patients (p < 0.001 and p < 0.01 respectively; Table 2).
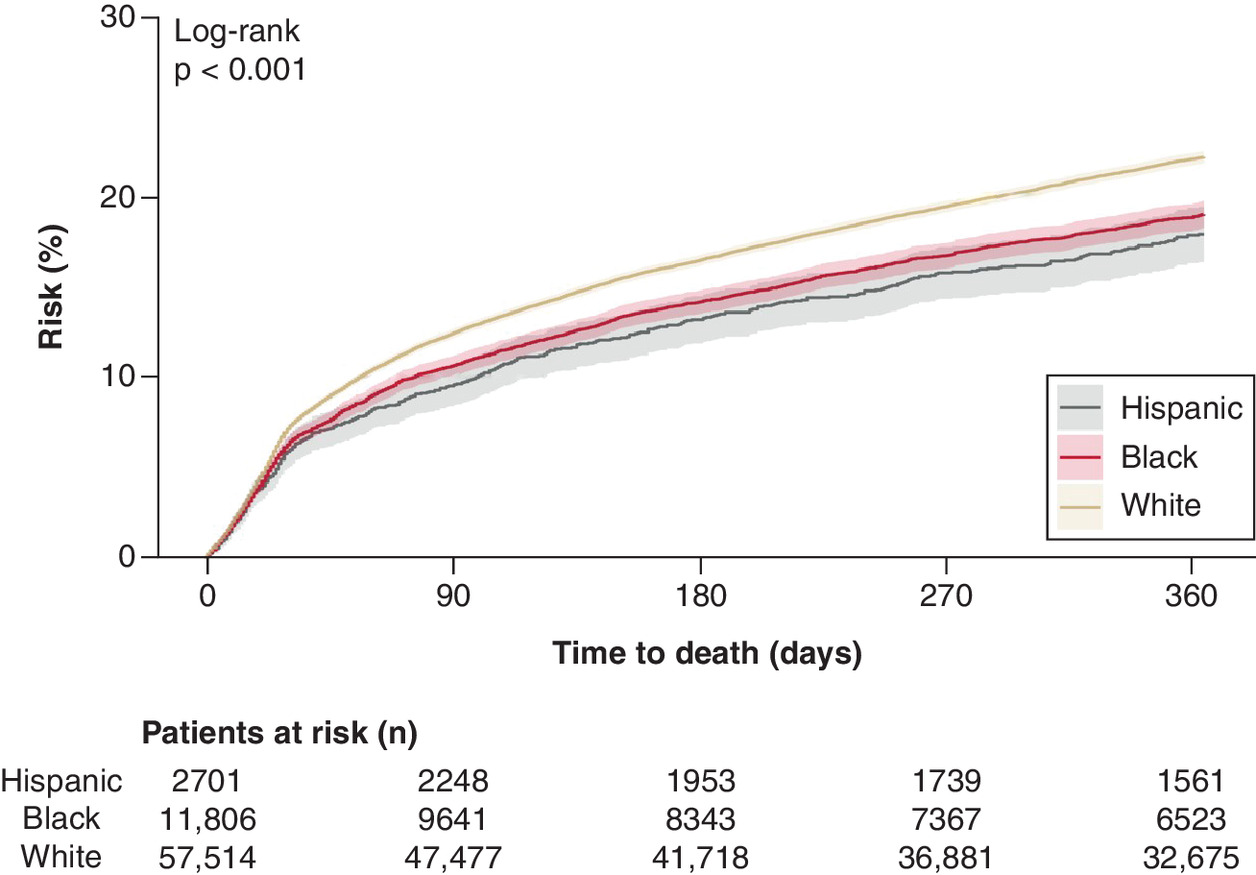
Figure 4 displays the cumulative incidence function for heart failure hospitalization in the year after development of sTR by race/ethnicity. After adjustment for baseline characteristics (Table 1), Black and Hispanic patients both had a greater risk of heart failure hospitalization compared with White patients (p < 0.001 and p < 0.05 respectively; Table 2).
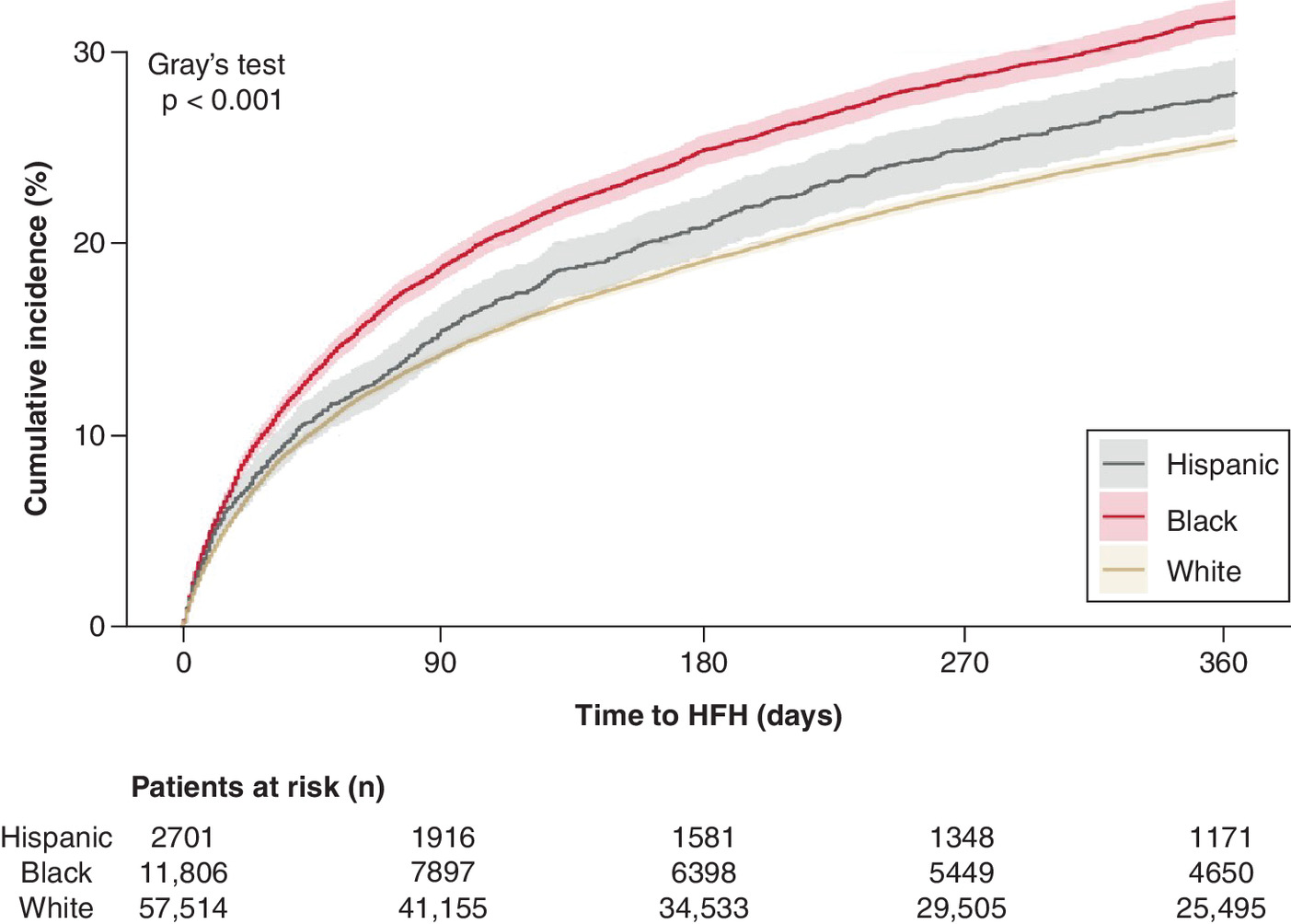
Figure 4. Heart failure hospitalization cumulative incidence in the year after significant tricuspid regurgitation, by race/ethnicity.
HFH: Heart failure hospitalization.
Explanatory variables
Figure 5 displays the HRs for potential explanatory variables for death (all baseline characteristics from Table 1), both overall and for each race/ethnicity category. Inpatient status at the time of meeting sTR criteria was the strongest predictor of death overall (HR: 2.39, 95% CI: 2.29–2.48, p < 0.001) and for each race/ethnicity category (Supplementary Table 4).
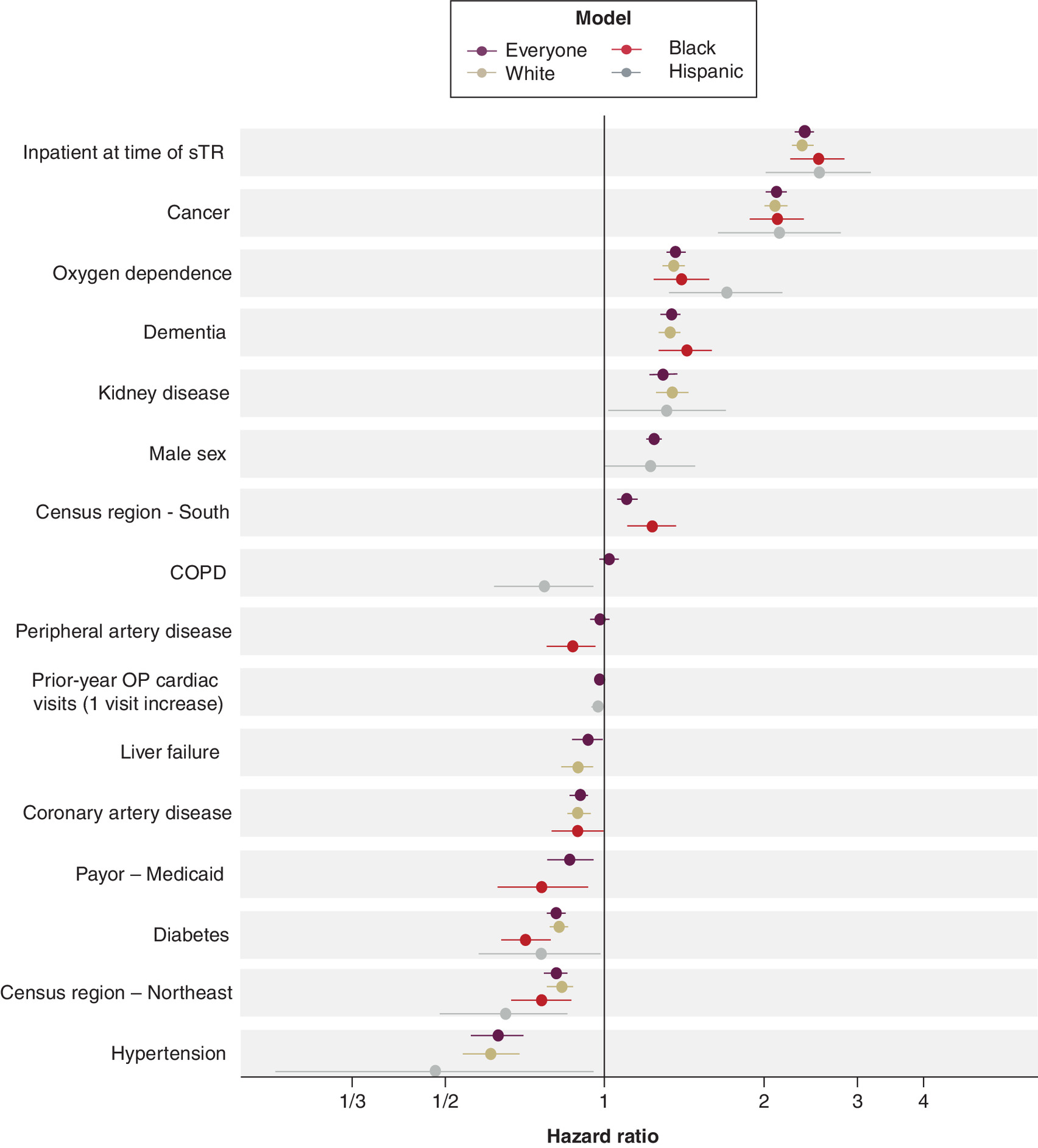
Figure 5. Hazard ratios for all-cause mortality explanatory variables* in the year after significant tricuspid regurgitation.
*Variables included in the figure represent the five strongest, statistically significant explanatory variables with increased risk and the five strongest, statistically significant explanatory variables with decreased risk for each race/ethnicity category.
CHF: Congestive heart failure; CKD 5: Chronic kidney disease stage 5; COPD: Chronic obstructive pulmonary disease; ESRD: End-stage renal disease; OP: Outpatient; TIA: Transient ischemic attack.
Figure 6 displays the HRs for the potential explanatory variables for heart failure hospitalization both overall and for each race/ethnicity category. Pre-existing congestive heart failure at baseline was the strongest predictor of heart failure hospitalization for all groups (HR: 3.60, 95% CI: 3.41–3.81; Supplementary Table 5).
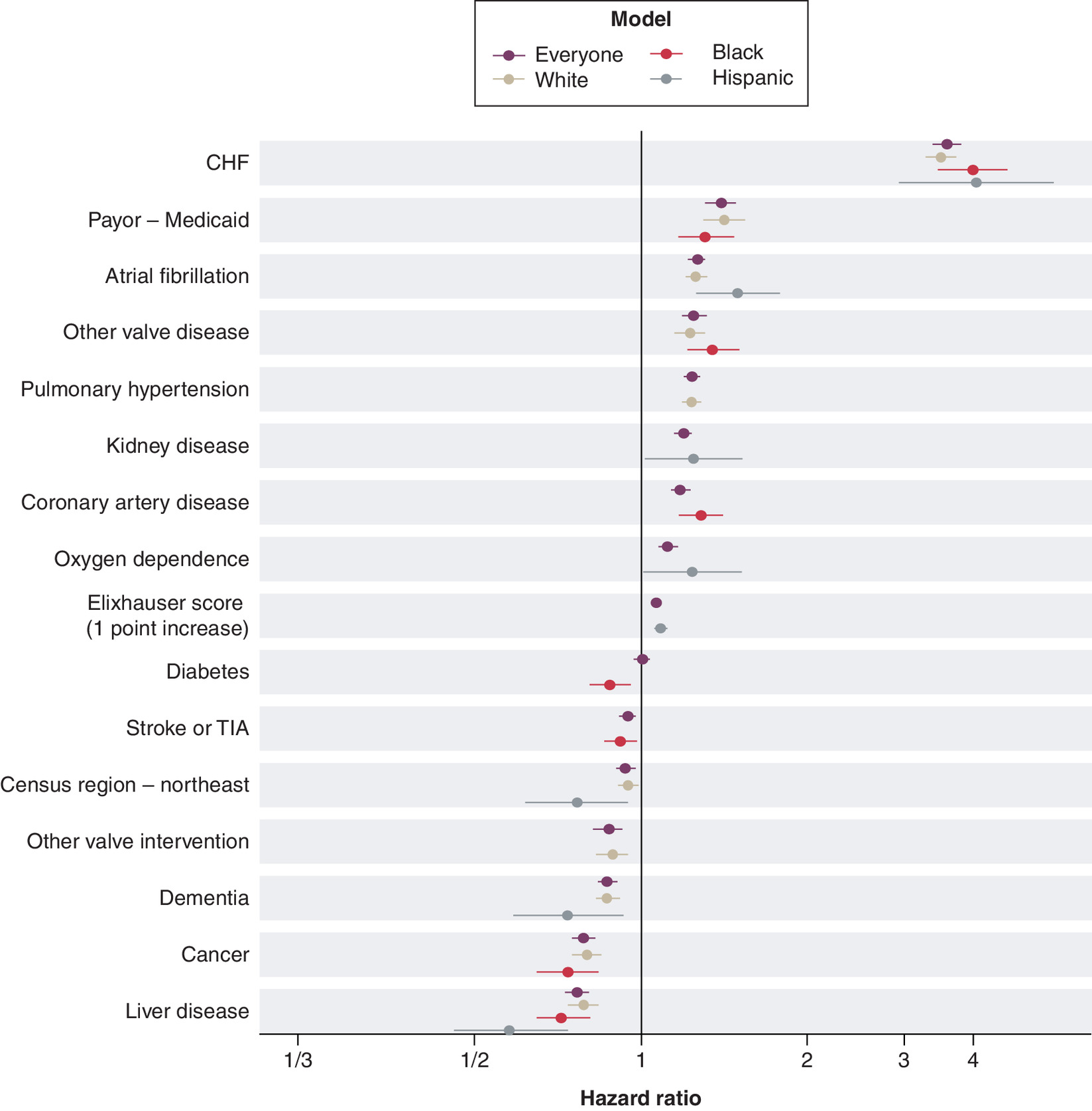
Figure 6. Hazard ratios for heart failure hospitalization explanatory variables* in the year after significant tricuspid regurgitation.
*Variables included in the figure represent the five strongest, statistically significant explanatory variables with increased risk and the five strongest, statistically significant explanatory variables with decreased risk for each race/ethnicity category.
CHF: Congestive heart failure; CKD 5: Chronic kidney disease stage 5; COPD: Chronic obstructive pulmonary disease; ESRD: End-stage renal disease; OP: Outpatient; TIA: Transient ischemic attack.
Overall, older age, male sex, higher Elixhauser score, atrial fibrillation, congestive heart failure, pulmonary hypertension, kidney disease, oxygen dependence and identification of sTR during an inpatient encounter were all associated with greater risk of death and heart failure hospitalization. Receiving prior intervention on other (i.e., non-tricuspid) valves was associated with lower hazard ratios for both death and heart failure hospitalization. Diabetes and a prior pacemaker were both associated with lower risk of death only. Peripheral artery disease, stage 5 chronic kidney disease and chronic obstructive pulmonary disease were associated with higher risk of heart failure hospitalization only. Medicaid enrollment, other valve diseases, coronary artery disease, hypertension and outpatient cardiac specialist visits in the year prior to sTR were all associated with lower risk of death but higher risk of heart failure hospitalization. Stroke and cancer were associated with higher risk of death and lower risk of heart failure hospitalization. Some associations such as census region, hypertension and diabetes varied by race/ethnicity (Supplemental Tables 4 & 5).
Discussion
This contemporary nationwide analysis of 72,630 patients who developed sTR between 2018 and 2023 provides critical insights into the current landscape of the progression and clinical manifestation of TR among different racial and ethnic patient groups. Compared with White patients, Black patients were less likely to have a preexisting TR diagnosis and were most often in an inpatient setting when they met sTR criteria. Prior to developing sTR, Black and Hispanic patients had higher rates of acute care utilization but fewer outpatient cardiac specialist visits, with consistent trends in the year following sTR status. One-year clinical outcomes revealed significant but contrasting patterns: Black and Hispanic patients had a higher risk of heart failure hospitalization, whereas White patients faced a greater risk of death even after adjustment for age and baseline clinical characteristics. Baseline characteristics and clinical comorbidities were associated with adverse outcomes. Inpatient admission at the time of meeting sTR criteria emerged as a strong predictor of subsequent death.
In one prior study of patients with severe TR who were included in the Bronx-Valve registry (n = 989), results showed that Black and Hispanic patients presented with more advanced disease and higher comorbidity burdens compared with White patients, despite their younger age [11]. In addition, Black patients experienced a significantly higher risk of heart failure hospitalization [11]. Our study confirms these findings in a large national dataset, and offers insight into the influence of race and ethnicity on the clinical trajectories of patients who develop sTR. However, that study also found that 5-year mortality rates were not significantly different across racial and ethnic groups, a finding in contrast with the increased 1-year risk of death for White patients in the current study as well as a recent analysis of death certificate data that found higher tricuspid valve disorder-related mortality rates in White and American Indian populations than in Black populations [15]. Several important differences between the studies, including the clinical specificity and number of variables in the models, sample size, and sample definition (i.e., severe vs significant TR), are likely related to this variation in outcomes.
The paradox of lower mortality but higher hospitalization among Black patients has been seen in several studies of heart failure, a highly prevalent comorbid condition in our analysis. In a study of Medicare heart failure patients (n = 47,149), Black adults had higher rates of cardiovascular-related readmission but lower mortality at 30-days and 1-year after risk adjustment; Hispanic adults also had higher readmission rates, but comparable 1-year mortality to White patients [16]. In another real-world heart failure cohort (n = 34,621), Black patients had a higher rate of heart failure hospitalization but lower rate of death compared with White patients. The adjusted effect estimates for heart failure hospitalization (HR: 1.28, 95% CI: 1.18–1.38) and all-cause death (HR: 0.78, 95% CI: 0.72–0.8) were consistent with those observed in our analysis [17]. The elevated risk of hospitalization among Black patients may reflect unmeasured confounding variables such as differences in disease burden, patient–provider treatment dynamics, thresholds for inpatient admission, access to outpatient services, medication adherence and broader socioeconomic factors [17–19]. Similarly, the higher mortality observed in White patients may point to potential variations in confounding variables such as TR pathophysiology and limitations of current management strategies [17,18]. Notably, Medicaid enrollment was similarly associated with a higher risk of heart failure hospitalization but lower mortality in our analysis, highlighting the potential influence of insurance and healthcare delivery models on clinical outcomes [20].
A prior analysis of the Optum database did examine the impact of TR and race on mortality rates in heart failure patients [21]. Models comparing patients with severe TR to patients without TR showed an overall increased risk of 2-year mortality that varied in size between non-White (52%) and White (33%) patients; however, non-White and White patients were not compared directly. Thus, the current results fill a gap in reporting of differences between specific racial and ethnic subgroups among patients with sTR. Further investigation of confounding variables beyond the scope of the current study will be necessary to elucidate the mechanisms underlying these racial and ethnic differences in TR clinical outcomes.
In addition to ensuring timely detection of TR, effort should also be directed toward more inclusive outpatient care. Among Black and Hispanic patients, fewer follow-up visits with a cardiologist after meeting sTR criteria may reflect barriers to specialist care for non-White patients. Without regular outpatient specialty care, cardiovascular related adverse events that necessitate emergency department visits and unplanned hospitalizations may become more frequent [18]. Studies have shown that minority patient groups have lower rates of specialty provider follow-up compared with White patients [22]. To bridge these gaps, improving care delivery models will be necessary to attenuate these differences, particularly in vulnerable communities with fragmented healthcare infrastructures.
Overall, improvement in outcomes will heavily rely on early TR recognition by clinicians and referral to comprehensive valve centers with multidisciplinary expertise [23]. Management strategies for TR remain heterogeneous, with surgical or procedural intervention for isolated TR still infrequently performed [5,24,25]. The emergence of transcatheter tricuspid valve interventions is expanding therapeutic options, particularly for patients with high surgical-risk [26]. However, surgical and percutaneous treatment selection is often influenced by multiple factors including race, as Black patients have been reported to be less likely to receive any TR intervention compared with White patients [27]. As the clinical interest in TR continues to grow [28], tailored and patient-oriented strategies to ensure equitable distribution of care are needed [29].
Limitations
Our study utilized a large database that included a diverse payer mix, including commercial insurance, Medicaid and Medicare throughout the US The data source incorporated EHR data and physician notes as well as administrative claims, allowing for longitudinal analysis of TR progression and healthcare utilization. Despite these strengths, the findings from this analysis should be interpreted with the following limitations in mind. First, this was an observational study. Proxy definitions for clinical symptomatology were used to define our sTR population and only a small percentage of patients entered the cohort directly from a physician note of severe or greater TR, a point in contrast to prior literature where severity was known. Granular clinical details are missing from our analysis, including patient baseline laboratory results and echocardiographic parameters such as left ventricular ejection fraction, and severity ratings are not well populated in the physician notes. In addition, the cohort was restricted to patients with non-rheumatic TR, and TR etiology was not captured. Due to limitations in the data, concomitant medical therapy was not assessed nor were other important potential confounding variables, including lifestyle factors such as diet and exercise or socioeconomic characteristics aside from health insurance payor (which may be considered at best a proxy for socioeconomic status). Clustering of patients at the hospital level was not adjusted for in associations between race/ethnicity and outcomes. Finally, race and ethnicity categories were simplified to ensure mutually exclusive groups for analysis; if patients identified as Black or White and also identified as Hispanic, they were classified as Hispanic within the cohort.
Conclusion
Among adults with sTR in the US, we observed racial and ethnic differences in disease recognition, healthcare use and clinical outcomes that expand on prior findings from studies of patients with severe TR or heart failure. Black and Hispanic patients with sTR were at increased risk of heart failure hospitalization compared with White patients. Black patients used more acute healthcare services, received fewer outpatient cardiology services and more often met sTR criteria in an inpatient setting. White patients had higher rates of mortality at 1 year. Further investigation into the underlying mechanisms of these observations, including measurement of important additional confounding factors, is needed to better improve TR-related outcomes.
Summary points
•
Tricuspid regurgitation (TR) progresses over time, causing patients to seek healthcare more often and putting them at risk of being hospitalized for heart failure or dying.
•
The results of this study showed that patients from different race and ethnicity categories had different types of healthcare leading up to significant illness and different outcomes in the year after significant illness.
•
Black and Hispanic patients more often used acute care resources leading up to significant TR and were more at risk of heart failure hospitalization after, compared with White patients.
•
White patients more often used outpatient cardiac specialist care leading up to significant TR and were more at risk of death after, compared with Black and Hispanic patients.
•
Understanding how the healthcare pathway and clinical outcomes of patients with progressive conditions like TR vary by characteristics such as race is an important step in improving healthcare quality and equity.
Acknowledgments
The authors thank Diana Frame for her assistance in writing the manuscript.
Financial disclosure
This study was supported by Edwards Lifesciences.
Competing interests disclosure
F Medina, D Cork, P Gaba, C Barker and R Yeh report administrative support, article publishing charges, statistical analysis and writing assistance were provided by Edwards Lifesciences Corporation. R Horn, L Kemp, A Dratch, S Murphy and S Mollenkopf report financial support was provided by Edwards Lifesciences Corporation. L Kemp, A Dratch, R Horn, S Murphy and S Mollenkopf report a relationship with Edwards Lifesciences Corporation that includes: employment. R Yeh reports the following relationships: Abbott Vascular Inc, Boston Scientific, Edwards Lifesciences, Elixir Medical and Medtronic relationships include: consulting and research grants; JenaValve and Siemens relationships that include: research grants; CathWorks, FastWave, Magenta Medical and Shockwave relationships that include: consulting. C Barker reports relationships with Alleviant, Boston Scientific, Edwards Lifesciences Corporation and Medtronic that include: consulting. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical data that have been shared with them, and that the use of this shared data is in accordance with the terms (if any) agreed upon their receipt.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary data.docx)
- Download
- 54.60 KB
References
Papers of special note have been highlighted as: • of interest
1.
Kolte D, Kennedy KF, Passeri JJ, Inglessis I, Elmariah S. Temporal trends in prevalence of tricuspid valve disease in hospitalized patients in the United States. Am. J. Cardiol. 125, 1879–1883 (2020).
2.
Topilsky Y, Maltais S, Medina Inojosa J, Oguz D et al. Burden of tricuspid regurgitation in patients diagnosed in the community setting. JACC Cardiovasc. Imaging. 12, 433–442 (2019).
3.
Shahim A, Hourqueig M, Lund LH et al. Long-term outcomes in heart failure with preserved ejection fraction: predictors of cardiac and non-cardiac mortality. ESC Heart Fail. 10, 1835–1846 (2023).
4.
Vemulapalli S, Kerr MSD, Roberts GJ, Prillinger JB, Meduri CU, McCarthy P. Tricuspid valve disease prevalence and the impact of tricuspid valve surgery on cardiovascular events and hospital resource use in Medicare beneficiaries. Am. Heart J. 245, 100–109 (2022).
5.
Hahn RT. Tricuspid regurgitation. N. Engl. J. Med. 388, 1876–1891 (2023).
6.
Graham G. Disparities in cardiovascular disease risk in the United States. Curr. Cardiol. Rev. 11, 238–245 (2015).
7.
Carnethon MR, Pu J, Howard G et al. Cardiovascular health in African Americans: a scientific statement from the American Heart Association. Circulation 136, e393–e423 (2017).
8.
Mensah GA. Eliminating disparities in cardiovascular health: six strategic imperatives and a framework for action. Circulation 111, 1332–1336 (2005).
9.
Martin SS, Aday AW, Almarzooq ZI et al. 2024 heart disease and stroke statistics: a report of US and global data from the American Heart Association. Circulation 149, e347–e913 (2024).
10.
Mazimba S, Peterson PN. JAHA spotlight on racial and ethnic disparities in cardiovascular disease. J. Am. Heart Assoc. 10, e023650 (2021).
11.
Echarte-Morales J, Scotti A, Bonnet G et al. Racial and ethnic disparities in patients with severe tricuspid regurgitation: The Bronx-Valve registry. Int. J. Cardiol. 421, 132889 (2025).
• Results are the most directly comparable to the current study.
12.
Cork DP, Medina F, Kemp L et al. Healthcare cost and utilization by age, sex, and race: three years prior to and one year following a status of significant tricuspid regurgitation. (In press)
• Companion article to the current study.
13.
Optum, Inc. Market Clarity: linked EHR and claims data. (2025). (Accessed 28 January 2025). Available at: https://business.optum.com/en/data-analytics/life-sciences/real-world-data/market-clarity-data.html
14.
Moore BJ, White S, Washington R, Coenen N, Elixhauser A. Identifying increased risk of readmission and in-hospital mortality using hospital administrative data: The AHRQ Elixhauser Comorbidity Index. Med. Care 55, 698–705 (2017).
15.
Ansari Y, Raja A, Raja S et al. Investigating mortality trends and disparities in tricuspid valve disorder: a U.S. nationwide study from 1999 to 2023. BMC Cardiovasc. Disord. 25, 208 (2025).
16.
Vivo RP, Krim SR, Liang L et al. Short- and long-term rehospitalization and mortality for heart failure in 4 racial/ethnic populations. J. Am. Heart Assoc. 3, e001134 (2014).
• Article looks at the same main outcomes by race and ethnicity.
17.
Savitz ST, Leong T, Sung SH et al. Contemporary reevaluation of race and ethnicity with outcomes in heart failure. J. Am. Heart Assoc. 10, e016601 (2021).
18.
Durstenfeld MS, Ogedegbe O, Katz SD, Park H, Blecker S. Racial and ethnic differences in heart failure readmissions and mortality in a large municipal healthcare system. JACC Heart Fail. 4, 885–893 (2016).
19.
Kamath SA, Drazner MH, Wynne J, Fonarow GC, Yancy CW. Characteristics and outcomes in African American patients with decompensated heart failure. Arch. Intern. Med. 168, 1152–1158 (2008).
20.
Khatana SAM, Bhatla A, Nathan AS et al. Association of Medicaid expansion with cardiovascular mortality. JAMA Cardiol. 4, 671–679 (2019).
21.
Messika-Zeitoun D, Verta P, Gregson J et al. Impact of tricuspid regurgitation on survival in patients with heart failure: a large electronic health record patient-level database analysis. Eur. J. Heart Fail. 22, 1803–1813 (2020).
• Provides insight into the impact of tricuspid regurgitation on mortality in HF patients.
22.
Cai C, Gaffney A, McGregor A et al. Racial and ethnic disparities in outpatient visit rates across 29 specialties. JAMA Intern. Med. 181, 1525–1527 (2021).
23.
Otto CM, Nishimura RA, Bonow RO et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 77, e25–e197 (2021).
24.
Wang N, Fulcher J, Abeysuriya N et al. Tricuspid regurgitation is associated with increased mortality independent of pulmonary pressures and right heart failure: a systematic review and meta-analysis. Eur. Heart J. 40, 476–484 (2019).
25.
Wang TKM, Akyuz K, Mentias A et al. Contemporary etiologies, outcomes, and novel risk score for isolated tricuspid regurgitation. JACC Cardiovasc. Imaging. 15, 731–744 (2022).
26.
Sorajja P, Whisenant B, Hamid N et al. Transcatheter repair for patients with tricuspid regurgitation. N. Engl. J. Med. 388, 1833–1842 (2023).
27.
Villablanca P, Jabri A, Alhuneafat L et al. Trends in surgical and transcatheter interventions for tricuspid regurgitation: a national inpatient sample analysis from 2011 to 2020. Cardiovasc. Revasc. Med. 78, 91–103 (2025).
28.
Bax JJ, Chandrashekhar Y. Tricuspid regurgitation: what is missing? JACC Cardiovasc. Imaging. 17, 713–714 (2024).
29.
Small AM, Watson NW, Wadhera RK, Secemsky EA, Yeh RW. Advancing health equity in the cardiovascular device life cycle. Circ. Cardiovasc. Qual. Outcomes 18, e011310 (2025).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 24 September 2025
Accepted: 25 November 2025
Published online: 11 December 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Racial and ethnic differences in diagnosis, healthcare utilization and 1-year outcomes for patients with significant tricuspid regurgitation. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0156
Export citation
Select the citation format you wish to export for this article or chapter.