Comparison treatments for basal ganglia hemorrhage: minimally invasive puncture and drainage versus craniotomy versus conservative treatment
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The optimal management strategies for spontaneous intracerebral hemorrhage in the basal ganglia region are still controversial. The purpose of the present study is to evaluate the clinical benefits of craniotomy, minimally invasive puncture and drainage (MIPD) and conservative treatment in patients with basal ganglia hematoma. Materials & methods: This study retrospectively enrolled consecutive patients with hematoma ≥20 ml in the basal ganglia hemorrhage and onset to admission within 24 h. Primary outcome was the proportion of favorable outcome (modified Rankin scale score 0–3) at 3 months. Secondary outcomes included excellent outcome (modified Rankin scale score 0–2) and mortality at 3 months and 1 year. Sensitive analysis was performed in patients with hematoma ≥ 30 ml. Results: A total of 481 patients were included and divided into three groups: 146 received craniotomy, 211 underwent MIPD and 124 were managed with conservative treatment. The proportion of primary outcome was lower in the craniotomy (23.24%) than in the MIPD (35.41%) and conservative treatment (41.94%) groups. Among patients with hematoma ≥30 ml, MIPD has higher rates of favorable outcome at 3 months (37.32 vs 25.98%, p = 0.05) and 1 year (52.82 vs 40.16%, p = 0.04) compared with craniotomy; albeit. The short-term and long-term mortality was similar in three groups. Conclusion: MIPD was found to be associated with both short- and long-term favorable outcomes in patients with spontaneous intracerebral hemorrhage in the basal ganglia region. Moreover, neither MIPD nor craniotomy showed an association with increased risk of short- or long-term mortality.
Plain language summary: Which treatment works best for deep brain bleeds: minimally invasive drainage, open surgery or medication-only care?
What is this article about?
Patients with sudden bleeding in deep brain regions (basal ganglia hemorrhage) face high risks of disability. This study compared three treatments: open brain surgery (craniotomy), a less invasive drainage procedure (MIPD) and medication-only care (conservative treatment), to see which best preserves patients' independence.
What were the results?
MIPD was found to be associated with both short- and long-term favorable outcomes in patients with spontaneous intracerebral hemorrhage in the basal ganglia region. Moreover, neither MIPD nor craniotomy showed an association with increased risk of short- or long-term mortality.
Why is this important?
Doctors often debate whether surgery helps deep brain bleeds. This study shows that less invasive options (minimally invasive drainage or careful monitoring) may improve recovery more than open surgery, without increasing death risk. For large bleeds, minimally invasive drainage appears to offer the best chance for independence. These findings could potentially steer treatment toward safer, more effective approaches – especially where resources for complex surgery are limited.
Spontaneous intracerebral hemorrhage (sICH) is a devastating disease, accounting for 10–15% of all stroke cases [1,2]. Particularly, the hematomas in the area of basal ganglia are common, constituting approximately 65% of all sICH [3]. sICH has greater mortality and disability than ischemic stroke [2,4,5]. However, the optimal treatment for sICH remains uncertain and controversial.
Surgery and conservative treatment are dominant treatments for sICH. The STICH [3] and STICH II [6] trials, two randomized clinical trials, have failed to demonstrate patients with sICH can get benefits from craniotomy. While craniotomy effectively removes hematomas, the procedure may also cause damage to healthy brain tissue during the process. Minimally invasive surgery has advantages to decrease the blood loss during operation, shorten anesthetic time, and reduce the rates of complications for craniotomy [7]. The MISTIE-III trial [8], which investigated the use of catheter-associated thrombolysis for hematoma evacuation, did not demonstrate that minimally invasive surgery improved the proportion of favorable outcome at 1 year in patients with sICH. Recently, the ENRICH trial suggested that minimally invasive hematoma evacuation could increase the proportion of favorable outcome at 6 months for lobar hemorrhages [9]. The basal ganglia, a deep-seated anatomical structure within the brain, suffer severe damage during hematoma evacuation procedures [10,11]. A prospective nonrandomized comparative study supported that patient who underwent minimally invasive puncture and drainage (MIPD) for basal ganglia hematoma had higher rates of functional independence and lower rates of mortality than depressive craniotomy at 1 year [5].
MIPD is a safe surgical procedure characterized by rapid hematoma removal, reduced blood loss and low cost, which is widely used in China. Few studies have comprehensively compared the clinical outcomes among craniotomy, MIPD and conservative treatment in patients with basal ganglia hematoma. The aim of our study was to assess and compare the functional outcomes at 3 months and 1 year among three groups by conducting a retrospective study of basal ganglia hemorrhage.
Materials & methods
Patients
The study consecutively enrolled patients with sICH in the basal ganglia region from the First Hospital of Yulin, Xianyang Hospital of Yan'an University and the Yan'an University Affiliated Hospital between 1 August 2019 and 18 September 2023. The study protocol was approved by the local ethics committees. Those patients were included who were 18–90 years of age, identified with hemorrhage volume ≥20 ml based on CT, admitted to the hospital within 24 h after ICH symptom onset, keeping the drainage catheter less than 7 days after operation, and recorded without neurological deficit (Glasgow Coma Scale [GCS] score ≤5 and modified Rankin scale [mRS] score >1) before ICH symptom onset. Hemorrhage volume was calculated utilizing the ellipsoid volume approximation method, employing the Coniglobus formula [12] = A × B × C × 1/2. The exclusion criteria included the following: hemorrhage due to trauma, ruptured aneurysm, cerebral arteriovenous malformation and vascular anomaly; coagulation disorders; cerebral tumor; brain stem failure at admission; pregnancy and incomplete follow-up information. We also collected those data of patients, including age, sex, disease history (hypertension, diabetes, coronary heart disease), current smoking, GCS score at admission, hemorrhage volume, systolic blood pressure at admission, diastolic blood pressure at admission, the time of onset to admission, the time of admission to surgery and surgery procedure during time based on previous medical records.
Treatment procedures
Minimally invasive puncture & drainage
The puncture site was determined by locating the maximum cross-sectional area of the hematoma on preoperative CT scans, while carefully avoiding critical functional brain regions and major vessels. After general anesthesia, drainage catheter was placed into the hematoma center. The hematoma evacuation was performed with a 10 ml syringe to aspirate uncoagulated blood until no longer fluid in the syringe. The hematoma was then continuously liquefied via an extracranial drainage system, with daily administration of 10,000 units of urokinase (reconstituted in 5 ml normal saline) into the hematoma cavity through the catheter. Patients were re-examined by CT on the first, third, fifth and seventh days post-operation. Removing the drainage catheter was determined by the remaining hematoma volume less 10 ml on follow-up CT and patients with a stable condition. The decision to remove the drainage catheter was determined by three criteria: a residual hematoma volume of less than 10 ml on follow-up CT scans, the patient’s stable clinical condition and no severe hydrocephalus.
Craniotomy
Under the general anesthesia, the bone flap was removed and dura was opened in a cruciate manner. Under microscopic visualization, the hematoma was evacuated using suction device and active bleeding was controlled employing bipolar electrocautery and local hemostatic agents. An external hematoma catheter was placed into the hematoma cavity for drainage for residual hematoma. In all cases, bone flap decompression was routinely performed in combination with hematoma evacuation to prevent postoperative brain herniation caused by severe hemorrhage or cerebral edema. Postoperative follow-up assessments were systematically conducted on postoperative days 1, 3, 5 and 7.
Conservative treatment
All enrolled patients received standardized medical management in strict accordance with the 2022 American Heart Association/American Stroke Association (AHA/ASA) guidelines for sICH management [13]. And standard acute-phase management for intracerebral hemorrhage were consistently implemented in patients [14].
Outcomes
The primary outcome was the proportion of patients with favorable functional outcomes (modified Rankin Scale [mRS] score 0–3) at 3 months [15]. Secondary outcomes included GCS and mRS scores at hospital discharge; the proportion of patients with excellent outcomes (mRS 0–2) and mortality at 3 months post-onset; and the rates of excellent outcomes, favorable outcomes and mortality at 1-year follow-up.
Statistical analysis
Categorical variables were presented as percentages and analyzed using the Chi-square test or Fisher exact test, appropriately. Continuous variables were shown using the median (interquartile range, IQR) and Mann–Whitney U test to analyze the difference in the craniotomy versus conservative treatment group and minimally invasive surgery versus conservative treatment group.
An inverse probability treatment weighting (IPTW) analysis was performed, adjusted for variables selected according to their p-value in univariate analysis and on their potential influence on outcome. The selected variables included age, sex, current smoking, diabetes, GCS score at admission, ICH volume, SBP and time from onset to admission. Additionally, sensitivity analysis was performed, stratified by ICH volume, time from onset to admission and GCS score at admission, to assess the association between the three treatments and clinical outcomes. Further, the effects of different treatments for outcomes also were explored in patients with hematoma volume ≥30 ml in the basal ganglia region. The proportion of clinical outcomes also were compared between craniotomy and MIPD group. Logistic regression analysis was conducted to examine the association between MIPD and clinical prognostics and adjusted age, GCS at admission, hematoma volume, time from admission to surgery and surgery procedure during time.
Statistical analysis was performed with the IBM SPSS Statistics, Version 26.0 program. Figures were drawn with the use of Excel software 2019 (Microsoft). Statistical significance was defined as p < 0.05 (two-tailed).
Result
Clinical characteristic
A total of 481 consecutive patients with sICH in the basal ganglia region were enrolled in our study. 300 patients were male, and ages ranged from 28 to 90 years, with a median of 62 years (IQR 54–69). Among those patients, 146 patients received craniotomy, 211 patients underwent MIPD, and 124 patients were managed with conservative treatment. Patients who underwent conservative treatment were observed to have higher GCS scores, smaller hematoma volumes and lower systolic blood pressure at admission compare to both the craniotomy and MIPD groups (in Table 1). Compared with craniotomy group, patients in the MIPD group had a high proportion of diabetes and current smoking, a smaller hematoma volume, a longer time from symptom onset to admission and a shorter surgical procedure duration.
| Craniotomy (n = 146) | MIPD (n = 211) | Conservative treatment (n = 124) | Pa | Pb | Pc | |
|---|---|---|---|---|---|---|
| Demographics | ||||||
| Age, years, median (IQR) | 61 (54–68) | 62 (54–69) | 63 (55–70) | 0.13 | 0.47 | 0.31 |
| Male, n (%) | 97 (66.44) | 133 (63.03) | 70 (56.45) | 0.09 | 0.23 | 0.51 |
| Disease history, n (%) | ||||||
| Hypertension | 98 (67.12) | 151 (71.56) | 89 (71.77) | 0.41 | 0.97 | 0.37 |
| Diabetes | 8 (5.48) | 26 (12.32) | 9 (7.26) | 0.55 | 0.14 | 0.03 |
| Coronary heart disease | 6 (4.11) | 15 (7.11) | 8 (6.45) | 0.39 | 0.82 | 0.24 |
| Current smoking | 13 (8.90) | 36 (17.06) | 16 (12.90) | 0.29 | 0.31 | 0.03 |
| Clinical features | ||||||
| GCS score at admission, median (IQR) | 9 (6–11) | 9 (7–11) | 10 (8–12) | <0.001 | <0.001 | 0.32 |
| GCS score at admission degree, n (%) | 0.01 | 0.01 | 0.94 | |||
| 3–8 | 66 (45.21) | 94 (44.55) | 34 (27.42) | |||
| 9–12 | 57 (39.04) | 86 (40.76) | 61 (49.19) | |||
| 13–15 | 23 (15.75) | 31 (14.69) | 29 (23.39) | |||
| ICH volume, median (ml) | 49.50 (40.00–60.00) | 34.00 (27.00–40.00) | 26.00 (22.00–30.00) | <0.001 | <0.001 | <0.001 |
| ICH volume > 30 (ml) | 130 (89.04) | 142 (67.30) | 41 (33.06) | <0.001 | <0.001 | <0.001 |
| Blood pressure at admission, median (IQR) | ||||||
| Systolic BP (mm Hg) | 179 (158–190) | 171 (155–189) | 160 (145–174) | <0.001 | <0.001 | 0.37 |
| Diastolic BP (mm Hg) | 98 (88–107) | 96 (86–108) | 91 (83–100) | 0.004 | 0.02 | 0.50 |
| Time variables, median (IQR) | ||||||
| Time from onset to admission (h) | 3.00 (2.00–5.00) | 4.00 (3.00–7.00) | 4.00 (3.00–7.00) | 0.001 | 0.40 | 0.003 |
| Time from admission to surgery (h) | 3.00 (2.00–7.00) | 15.30 (6.00–29.10) | NA | NA | NA | <0.001 |
| Surgery procedure during time (m) | 180.00 (120.00–300.00) | 31.00 (30.00–60.00) | NA | NA | NA | <0.001 |
Pa, craniotomy vs conservative treatment.
Pb, MIPD vs conservative treatment.
Pc, craniotomy vs MIPD.
BP: Blood pressure; GCS: Glasgow Coma Scale; ICH: Intracranial hemorrhage; IQR: Interquartile range; MIPD: Indicated minimally invasive puncture and drainage; NA: Not applicable.
Functional outcomes
Figure 1 illustrates the distribution of mRS at both 3 months and 1 year. The proportion of primary outcome was more frequent in patients who underwent conservative treatment and MIPD than in those who underwent craniotomy (41.94% vs 35.41% vs 23.24%, P (conservative treatment vs craniotomy) <0.001, P (MIPD vs craniotomy) = 0.02) (in Table 2). Patients who received conservative treatment and MIPD were significantly more likely to achieve a favorable outcome at the 1-year follow-up compared with those in the craniotomy group (62.10% vs 51.67% vs 35.92%, P [conservative treatment vs craniotomy] <0.001, P [MIPD vs craniotomy] = 0.004). No significant differences were observed between the MIPD and conservative treatment groups in favorable outcome and excellent outcome at 3 months and 1 year. The mortality rates at 3 months were 21.77%, 25.84% and 24.65% for conservative treatment, MIPD and craniotomy, respectively. At 1 year, the rates were 24.19, 31.58 and 30.99% for the same treatments. No significant differences in mortality were observed among the three groups. There were no significant differences in the rate of postoperative hemorrhage among the three groups (craniotomy: 1.30%, MIPD: 2.67%, conservative treatment: 3.57%; p > 0.05).
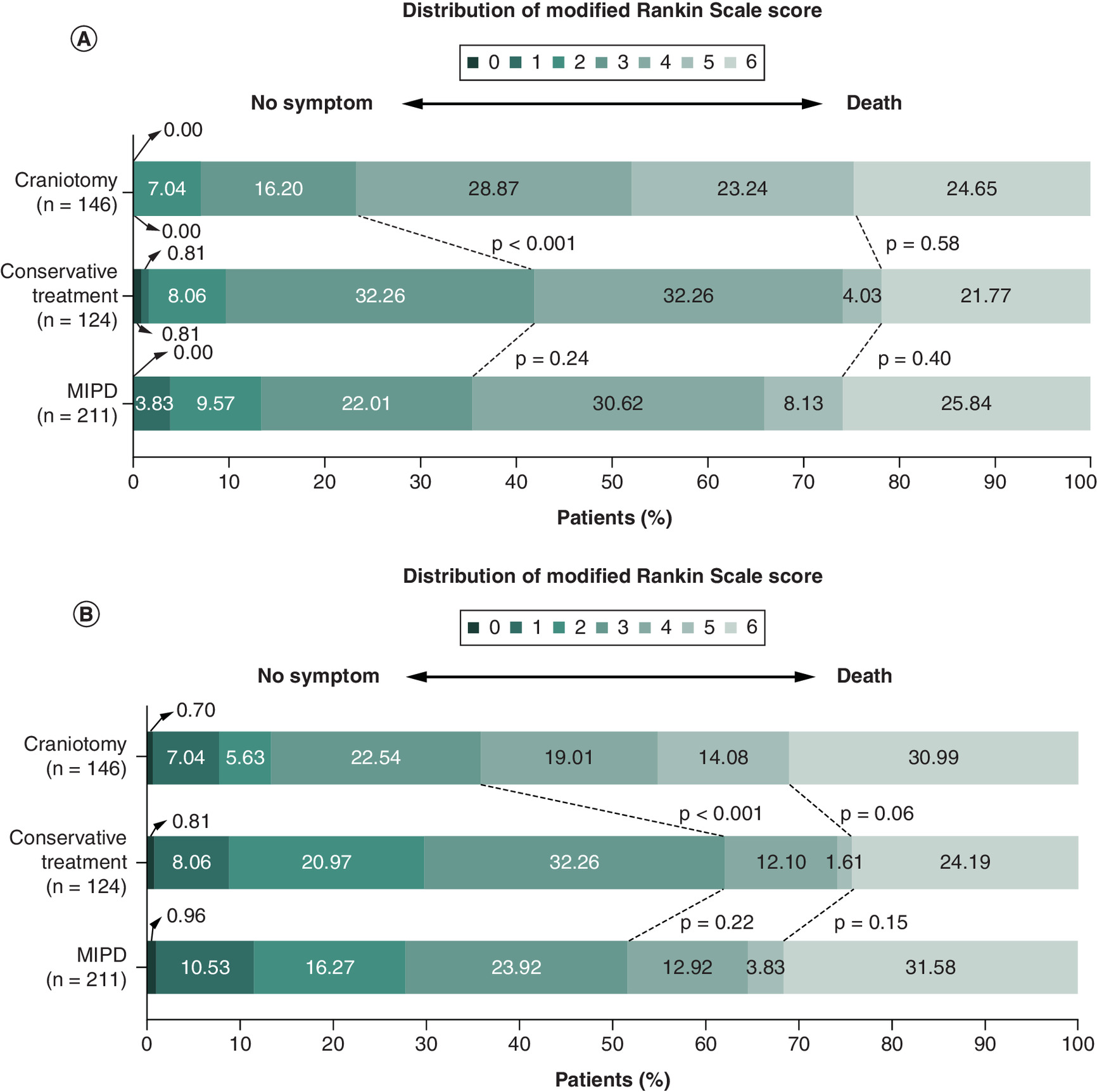
Figure 1. Distribution of treatment effects on the modified Rankin scale at 3-month and 1-year follow-up.
The distribution of scores for disability on the modified Rankin scale at 3 months (A) and 1 year (B) was displayed according to treatment group.
MIPD: Indicated minimal invasive puncture and drainage.
| Craniotomy (n = 146) | MIPD (n = 211) | Conservative treatment (n = 124) | Pa | Pb | Pc | |
|---|---|---|---|---|---|---|
| GCS score at discharge, median (IQR) | 12 (9–14) | 12 (9–15) | 14 (11–15) | 0.003 | 0.03 | 0.49 |
| GCS score at discharge degree, n (%) | 0.01 | 0.07 | 0.49 | |||
| 3–8 | 32 (22.07) | 49 (23.22) | 25 (20.16) | |||
| 9–12 | 49 (33.79) | 59 (27.96) | 23 (18.55) | |||
| 13–15 | 64 (44.14) | 103 (48.82) | 76 (61.29) | |||
| mRS score at discharge, median (IQR) | 4 (3–4) | 4 (3–5) | 4 (3–5) | 0.11 | 0.71 | 0.17 |
| Excellent outcome at discharge, n (%) | 12 (8.22) | 15 (7.11) | 6 (4.84) | 0.27 | 0.41 | 0.70 |
| Favorable outcome at discharge, n (%) | 55 (37.67) | 65 (30.81) | 34 (27.42) | 0.07 | 0.51 | 0.18 |
| Mortality in hospital, n (%) | 1 (0.68) | 6 (2.84) | 3 (2.42) | 0.34† | >0.99 | 0.25 |
| mRS score at 3 months, median (IQR) | 4 (4–5) | 4 (3–6) | 4 (3–5) | 0.001 | 0.30 | 0.02 |
| Excellent outcome at 3 months, n (%) | 10 (7.04) | 28 (13.40) | 12 (9.68) | 0.44 | 0.31 | 0.06 |
| Favorable outcome at 3 months, n (%) | 33 (23.24) | 74 (35.41) | 52 (41.94) | <0.001 | 0.24 | 0.02 |
| Mortality within 3 months, n (%) | 35 (24.65) | 54 (25.84) | 27 (21.77) | 0.58 | 0.40 | 0.80 |
| mRS score at 1 year, median (IQR) | 4 (3–6) | 3 (2–6) | 3 (2–5) | <0.001 | 0.20 | 0.02 |
| Excellent outcome at 1 year, n (%) | 19 (13.38) | 58 (27.75) | 37 (29.84) | 0.001 | 0.68 | 0.001 |
| Favorable outcome at 1 year, n (%) | 51 (35.92) | 108 (51.67) | 77 (62.10) | <0.001 | 0.06 | 0.004 |
| Mortality within 1 year, n (%) | 44 (30.99) | 66 (31.58) | 30 (24.19) | 0.22 | 0.15 | 0.91 |
Pa, craniotomy vs Conservative treatment; Pb, MIPD vs conservative treatment; and Pc, craniotomy vs MIPD.
†
indicated the comparison between two groups using Fisher’s exact test.
GCS: Glasgow Coma Scale; IQR: Interquartile range; MIPD: Indicated minimally invasive puncture and drainage; mRS: Modified Rankin Scale.
IPTW-adjusted model (Table 3), we also assessed treatment effects on clinical outcomes. Compared with craniotomy, both MIPD (odds ratio (OR) = 3.730, 95% CI = 2.216–6.507, p < 0.001) and conservative treatment (OR = 2.796, 95% CI = 1.524–5.231, p = 0.001) were significantly associated with favorable 3-month outcomes. Compared with craniotomy, both MIPD and conservative treatment had significant associations with favorable and excellent functional outcomes at 1 year. However, no significant associations were observed between treatment groups and mortality at either short- or long-term follow-up. Furthermore, we explored pairwise treatment comparisons (MIPD vs conservative treatment, MIPD vs craniotomy and conservative treatment vs craniotomy) for associations with short- and long-term clinical outcomes using univariate and multivariate logistic regression models (Supplementary Tables 1–3).
| Craniotomy OR (95% CI) | MIPD OR (95% CI) | p-value | Conservative treatment OR (95% CI) | p-value | |
|---|---|---|---|---|---|
| GCS score at discharge | Reference | 0.705 (-0.128 to 1.538)† | 0.10 | -0.260 (-1.251 to 0.731)† | 0.61 |
| GCS score at discharge degree | Reference | 0.690 (0.471–1.010)‡ | 0.06 | 1.176 (0.736–1.879)‡ | 0.50 |
| mRS score at discharge | Reference | 1.347 (0.921–1.972)‡ | 0.13 | 0.712 (0.450–1.125)‡ | 0.15 |
| Excellent outcome at discharge | Reference | 0.998 (0.449–2.299)§ | 0.99 | 0.437 (0.108–1.377)§ | 0.19 |
| Favorable outcome at discharge | Reference | 1.451 (0.913–2.333)§ | 0.12 | 0.894 (0.494–1.598)§ | 0.71 |
| Mortality in hospital | Reference | 1.026 (0.252–4.731)§ | 0.97 | 1.140 (0.196–6.019)§ | 0.88 |
| mRS score at 3 months | Reference | 2.090 (1.442–3.037)‡ | <0.001 | 1.207 (0.769–1.892)‡ | 0.41 |
| Excellent outcome at 3 months | Reference | 2.379 (1.159–5.303)§ | 0.02 | 1.148 (0.424–3.027)§ | 0.78 |
| Favorable outcome at 3 months | Reference | 3.730 (2.216–6.507)§ | <0.001 | 2.796 (1.524–5.231)§ | 0.001 |
| Mortality within 3 months | Reference | 0.795 (0.498–1.274)§ | 0.33 | 1.578 (0.935–2.668)§ | 0.09 |
| mRS score at 1 year | Reference | 1.966 (1.358–2.853)‡ | <0.001 | 1.275 (0.814–1.995)‡ | 0.29 |
| Excellent outcome at 1 year | Reference | 3.947 (2.187–7.553)§ | <0.001 | 2.809 (1.407–5.791)§ | 0.004 |
| Favorable outcome at 1 year | Reference | 3.068 (1.962–4.866)§ | <0.001 | 2.409 (1.427–4.102)§ | 0.001 |
| Mortality within 1 year | Reference | 0.820 (0.524–1.287)§ | 0.39 | 1.368 (0.819–2.289)§ | 0.23 |
IPTW model taking the following variables into account: age, sex, current smoking, diabetes, GCS score at admission, intracranial hemorrhage volume, SBP and time from onset to admission.
†
The β values were estimated from a linear regression.
‡
The common odds ratios were estimated from a ordinal logistic regression.
§
The ORs were estimated from a binary logistic regression.
CI: Confidence interval; MIPD: Indicated minimally invasive puncture and drainage; GCS: Glasgow Coma Scale; mRS: Modified Rankin Scale; NA: Not applicable; OR: Odds ratio.
Sensitivity analysis
Our stratified analyses suggest that MIPD and conservative treatment may be associated with favorable outcomes in patients with smaller hematoma volumes (20–30 ml), longer time to admission (>4 h), or higher GCS scores at admission. In contrast, among patients with hematoma volumes >30 ml or higher GCS scores, only MIPD appeared to show an association with favorable outcomes, whereas conservative treatment did not. (Table 4). Hematoma volume was a decisive factor for treatment selection, therefore, our study focused on analyzing clinical prognosis in patients with hematoma volume over 30 ml.
| Craniotomy | MIPD | Conservative treatment | |||
|---|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | ||
| ICH volume (ml) | Reference | ||||
| 20–30 | Reference | 4.376 (1.806–11.914) | 0.002 | 4.902 (1.859–14.233) | 0.002 |
| >30 | Reference | 2.119 (1.186–3.886) | 0.01 | 1.168 (0.550–2.447) | 0.68 |
| Time from onset to admission (h) | Reference | ||||
| 0–4 | Reference | 1.741 (0.948–3.270) | 0.08 | 1.012 (0.467–2.158) | 0.97 |
| >4 | Reference | 5.466 (2.383–14.100) | <0.001 | 5.525 (2.156–15.498) | 0.001 |
| GCS score at admission | Reference | ||||
| 0–9 | Reference | 3.264 (1.669–7.762) | 0.001 | 1.515 (0.594–3.889) | 0.38 |
| 9–15 | Reference | 2.205 (1.136–4.398) | 0.02 | 2.766 (1.262–6.196) | 0.01 |
IPTW model taking the following variables into account: age, sex, current smoking, diabetes, GCS score at admission, intracranial hemorrhage volume, SBP and time from onset to admission.
CI: Confidence interval; GCS: Glasgow Coma Scale; ICH: Intracranial hemorrhage; MIPD: Indicated minimally invasive puncture and drainage; OR: Odds ratio.
The baseline characteristics of patients with hematoma volume over 30 ml were presented in Supplementary Table 4, which indicated that patients who underwent MIPD had higher rates of smoking, smaller hematoma volume, longer time from symptom onset to admission and shorter time for surgical procedure than craniotomy group. According to the following-up data, the distribution of mRS is also shown in Figure 2.
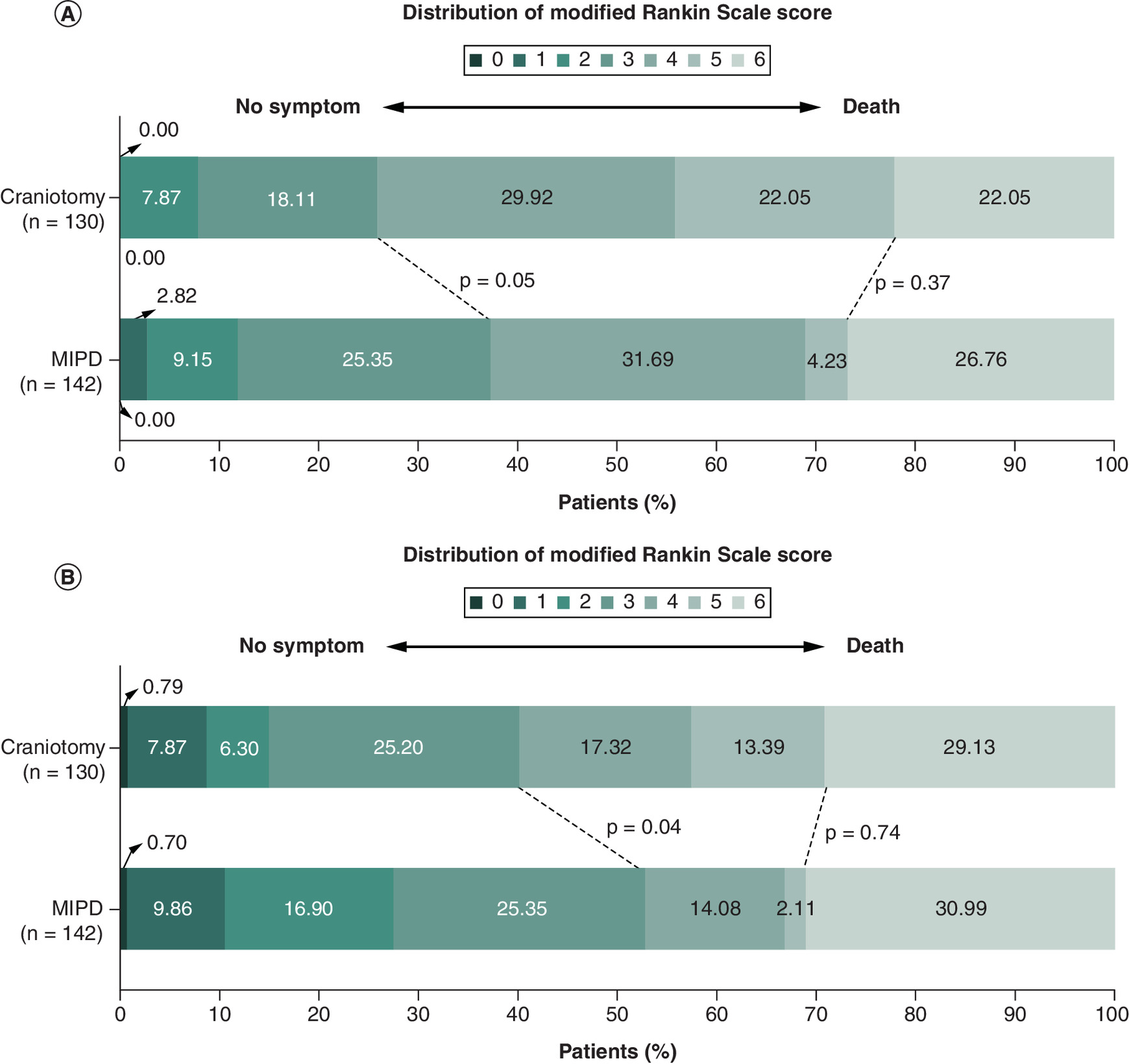
Figure 2. Distribution of minimal invasive puncture and drainage and craniotomy for hematoma of 30 ml or more on the modified Rankin scale at 3 months and 1 year.
The modified Rankin scale distribution (A) at 3 months and (B) 1 year showed the benefits of MIPD for basal ganglia hematomas larger than 30 ml.
MIPD: Indicated minimal invasive.
The MIPD group showed the advantage of achieving a favorable outcome at 3 months (37.32 vs 25.98%, p = 0.05) and 1 year (52.82 vs 40.16%, p = 0.04) (Table 5). Multivariate logistic regression analysis suggested that MIPD was associated with favorable outcome (odds ratio [OR] = 2.255; 95% CI = 1.172–4.342, p = 0.02) at 3 months and excellent outcome (OR = 2.191; 95% CI = 1.023–4.689, p = 0.04) at 1 year. IPTW model supported that the association between MIPD and favorable outcome was significant at 3 months and 1 year. However, mortality rates within 3 months and 1 year, discharge GCS score and discharge mRS score were similar between the MIPD and craniotomy groups.
| Craniotomy (n = 130) | MIPD (n = 142) | p-value | Crude odds ratio | Adjusted odds ratio | IPTW odds ratio | ||||
|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | OR (95% CI) | p-value | ||||
| GCS score at discharge, median (IQR) | 12 (9–15) | 13 (9–15) | 0.68 | -0.137 (-1.012 to 0.738)† | 0.76 | -0.406 (-1.328 to 0.516)† | 0.39 | 0.078 (-0.747 to 0.903)† | 0.85 |
| GCS score at discharge degree, n (%) | 0.82 | 1.082 (0.692–1.693)‡ | 0.73 | 1.037 (0.623–1.724)‡ | 0.89 | 0.845 (0.574–1.243)‡ | 0.39 | ||
| 3–8 | 26 (20.00) | 29 (20.42) | |||||||
| 9–12 | 43 (33.08) | 42 (29.58) | |||||||
| 13–15 | 61 (46.92) | 71 (50.00) | |||||||
| mRS score at discharge, median (IQR) | 4 (3–4) | 4 (3–5) | 0.06 | 0.661 (0.427–1.023)‡ | 0.06 | 0.551 (0.334–0.908)‡ | 0.02 | 0.966 (0.660–1.415)‡ | 0.86 |
| Excellent outcome at discharge, n (%) | 12 (9.23) | 10 (7.04) | 0.51 | 0.745 (0.310–1.787)§ | 0.51 | 0.482 (0.161–1.444)§ | 0.19 | 0.745 (0.323–1.727)§ | 0.49 |
| Favorable outcome at discharge, n (%) | 55 (42.31) | 45 (31.69) | 0.07 | 0.633 (0.385–1.039)§ | 0.07 | 0.602 (0.333–1.088)§ | 0.09 | 0.985 (0.623–1.564)§ | 0.95 |
| Mortality in hospital, n (%) | 0 | 4 (2.82) | 0.12 | NA | NA | NA | NA | NA | NA |
| mRS score at 3 months, median (IQR) | 4 (3–5) | 4 (3–6) | 0.10 | 1.444 (0.940–2.219)‡ | 0.09 | 1.314 (0.811–2.129)‡ | 0.27 | 1.574 (1.084–2.290)‡ | 0.02 |
| Excellent outcome at 3 months, n (%) | 10 (7.87) | 17 (11.97) | 0.26 | 1.591 (0.700–3.616)§ | 0.27 | 0.905 (0.327–2.507)§ | 0.85 | 1.423 (0.689–3.091)§ | 0.35 |
| Favorable outcome at 3 months, n (%) | 33 (25.98) | 53 (37.32) | 0.05 | 1.696 (1.006–2.860)§ | 0.05 | 2.255 (1.172–4.342)§ | 0.02 | 1.939 (1.211–3.154)§ | 0.01 |
| Mortality within 3 months, n (%) | 28 (22.05) | 38 (26.76) | 0.37 | 1.292 (0.738–2.263)§ | 0.37 | 1.365 (0.692–2.691)§ | 0.37 | 1.159 (0.725–1.866)§ | 0.54 |
| mRS score at 1 year, median (IQR) | 4 (3–6) | 3 (2–6) | 0.09 | 1.450 (0.945–2.225)‡ | 0.09 | 1.323 (0.816–2.147)‡ | 0.26 | 1.504 (1.037–2.185)‡ | 0.03 |
| Excellent outcome at 1 year, n (%) | 19 (14.96) | 39 (27.46) | 0.01 | 2.152 (1.168–3.966)§ | 0.01 | 2.191 (1.023–4.689)§ | 0.04 | 2.736 (1.554–5.024)§ | 0.001 |
| Favorable outcome at 1 year, n (%) | 51 (40.16) | 75 (52.82) | 0.04 | 1.668 (1.028–2.707)§ | 0.04 | 1.746 (0.968–3.148)§ | 0.06 | 2.260 (1.460–3.533)§ | <0.001 |
| Mortality within 1 year, n (%) | 37 (29.13) | 44 (30.99) | 0.74 | 1.092 (0.648–1.842)§ | 0.74 | 1.116 (0.602–2.066)§ | 0.73 | 1.095 (0.700–1.721)§ | 0.69 |
Adjusted estimates of outcome were calculated using multiple regression, taking the following variables into account: age, GCS at admission, intracranial hemorrhage volume, time from admission to surgery and surgery procedure during time.
IPTW was applied using a model that adjusted for age, sex, current smoking, diabetes, GCS score at admission, intracranial hemorrhage volume, SBP, time from admission to surgery and surgery procedure during time.
†
The β values were estimated from a multivariable linear regression model.
‡
The common odds ratios were estimated from a ordinal logistic regression model.
§
The odds ratios were estimated from a binary logistic regression model.
CI: Confidence interval; GCS: Glasgow Coma Scale; IPTW: Inverse probability treatment weighting; IQR: Interquartile range; MIPD: Indicated minimally invasive puncture and drainage; mRS: Modified Rankin scale; NA: Not applicable; OR: Odds ratio.
Discussion
Our study performed an analysis of three treatments for patients with sICH in the basal ganglia region, which supported that MIPD and conservative treatment resulted in better functional outcome at 3 months and 1 year than craniotomy. Nevertheless, the short-term and long-term mortality rates were similar between the craniotomy, MIPD and conservative treatment groups. The advantages of MIPD over craniotomy seemed to be associated to treating patients with a basal ganglia hematoma of 30 ml or more. It is worth noting that the outcomes associated with craniotomy should be interpreted with caution, as they may in part reflect the more severe clinical presentation at baseline rather than the procedure per se. In the participating hospitals, craniotomy for hematoma evacuation was commonly performed in combination with decompressive craniectomy; therefore, our results should be understood as reflecting this combined approach rather than craniotomy alone. To our knowledge, sICH is recognized as a devastating event associated with significantly high rates of mortality and disability [3,6,16]. Craniotomy and conservative treatment are still the main treatments for patients suffering from sICH in many hospitals. Minimally invasive surgery, a novel treatment, has been demonstrated to effectively evacuate hematomas [8,17,18]. Removing hematoma at the acute period is vital to reduce mortality and improve long-term quality of life for patients with sICH. The STICH randomized trial failed to illustrate the hypothesized superiority of conventional surgery over conservative treatment [3]. Additionally, the STICH II trial demonstrated that early surgery did not increase the rate of favorable outcome and mortality at 6 months [6]. The core surgical principle for managing hemorrhagic hematoma patients involves achieving effective hematoma evacuation while minimizing iatrogenic brain tissue injury. Conventional surgery can effectively remove hematoma and control bleeding while healthy brain tissue is damaged during the process. Instead, minimally invasive surgery is considered as the alternative approach for hematoma. Recently, the ENRICH trial supported that patients with lobar hematoma could get benefits from minimally invasive surgery at the 6-months follow-up [9]. However, the benefit for basal ganglia hematoma was not significant in the trial. The clinical prognosis of sICH was associated with the hematoma volume and location [19]. Our study, focusing on basal ganglia hematoma, also observed that MIPD was not superior to conservative treatment, which were consistent with MISTIE III trial [8]. One plausible explanation is that patients presenting with large-volume hematoma were more likely to undergo surgical hematoma evacuation. The proportion of hematoma volume over 30 ml was lower in conservative treatment than in craniotomy and MIPD (33.06% vs 89.04% vs 67.30%, p < 0.001) in our study. To explain the problem clearly, we conducted an analysis in those patients with hematoma volume of 30 ml or more. Results indicated the proportion of favorable outcome at short-term and long-term was comparable, while the mortality seems to be low in patients underwent MIPD compared with the conservative treatment group, although the difference did not arrival at the threshold value (Supplementary Table 2). The discrepancies may be reasonably attributed to the limited sample size and substantial heterogeneity in hematoma volumes.
Besides, some studies have demonstrated minimally invasive surgery could result in a better outcome compared with craniotomy [5,20]. Higher rates of favorable outcome at 3 months and 1 year were found in our study. Conventional craniotomy causes considerable trauma to the brain tissue [21]. And the shortcomings of craniotomy included general anesthesia, long duration of surgery, and damage to the functional area due to electrocoagulation. The MIPD procedure demonstrates a substantially reduced level of invasiveness in brain tissue manipulation relative to craniotomy [17,22]. MIPD procedures can be successfully performed under local anesthesia, typically requiring approximately 30 min or less to complete [23]. Further, previous literature reported patients underwent MIPD with small blood loss and less occurrence of epilepsy [5,7]. Minimizing complications of hematoma evacuation may improve the functional outcome in patients with sICH.
The mortality was similar among the craniotomy, MIPD and conservative treatment groups based on our study follow-up. By comparison with conservative treatment, STICH [3] and STICH II [6] trials have revealed that craniotomy did not increase the rate of mortality at 6 months. The MISICH trial [18] also insisted that craniotomy has not increased the risk of long-term mortality. Craniotomy for hematoma evacuation is a vital life-saving approach, especially in patients with large-volume hematomas, altered levels of consciousness due to midline shift, or hematoma expansion. The open surgical technique remains the common approach for large-volume hematoma evacuation, as it provides exhaustive exposure of the hematoma cavity and facilitates complete evacuation. Albeit, craniotomy may result in severe damage to healthy brain tissue and can be effective in removing hematomas and controlling active bleeding sites.
The limitation of our work needs to be considered. First, a retrospective nature of the study could cause inevitable selective bias. Given the retrospective design and unavoidable selection bias, our conclusions must be interpreted with caution. Future prospective, multicenter randomized controlled trials are warranted to validate and strengthen our findings. Second, the results of conservative treatment should be interpreted with caution due to the small number of patients. Third, those data were not collected, including residue hematoma, anesthetic time, blood loss, pulmonary infection and epilepsy. In addition, prior studies (e.g., Delcourt et al.) have highlighted the prognostic importance of specific anatomical involvement, particularly the posterior limb of the internal capsule and thalamus [24]. However, our cohort included larger hematomas, where deep structural boundaries were often obscured on retrospective imaging, precluding reliable stratification. This limitation underscores the need for future studies using advanced, high-resolution imaging to clarify the prognostic role of key anatomical sites in basal ganglia hemorrhage. Fourth, the generalizability of our findings is limited due to carrying out the study at three centers. Fifth, data on survival time were not available during the follow-up period of our study.
Conclusion
The retrospective study demonstrated that, compared with craniotomy, MIPD and conservative treatment were associated with the short-term and long-term favorable outcome of patients with sICH in the basal ganglia region. In patients with a basal ganglia hematoma of ≥30 ml, MIPD was associated with a higher likelihood of achieving favorable outcomes at both 3 months and 1 year when compared with craniotomy. The mortality was similar among the craniotomy, MIPD and conservative treatment groups. These findings should be interpreted with caution, as the possibility of residual confounding and bias cannot be fully excluded. Validation through well-designed prospective randomized controlled trials will be essential.
Summary points
•
This study included 481 patients with basal ganglia hemorrhage who underwent craniotomy, minimally invasive puncture and drainage (MIPD), or conservative treatment, and compared the efficacy of the three methods.
•
At the 3-month follow-up, the favorable outcome rate (modified Rankin scale 0–3) was 41.9% in the conservative group and 35.4% in the MIPD group, both superior to 23.2% in the craniotomy group.
•
At the 1-year follow-up, the advantage persisted: 62.1% in the conservative group and 51.7% in the MIPD group, both superior to 35.9% in the craniotomy group.
•
In patients with large hematomas (≥30 ml), MIPD showed significantly better outcomes than craniotomy: 37.3 versus 26.0% at 3 months, and 52.8 versus 40.2% at 1 year.
•
Mortality rates did not differ significantly among the three groups: approximately 22–26% at 3 months and 24–32% at 1 year.
•
Craniotomy may cause greater damage to brain tissue, leading to worse functional recovery compared with minimally invasive and conservative treatment.
•
MIPD achieves effective hematoma evacuation while minimizing trauma, showing clear advantages especially in patients with large hematomas.
•
MIPD or conservative treatment showed a potential association with better outcomes than conventional craniotomy and could be regarded as important treatment alternatives for basal ganglia hemorrhage.
Author contributions
T Tang: conceptualization, data curation, formal analysis, investigation, methodology, writing – original draft. J Liu: data curation, investigation, resources, validation. B Gao: data curation, investigation, resources. Y Gao: data curation, resources, validation. G Zhang: data curation, resources, supervision. G Guo: conceptualization, funding acquisition, project administration, supervision, writing – review and editing.
Acknowledgments
The authors express their gratitude to all the patients who contributed to this study.
Financial disclosure
This work was supported by the Yan'an Science and Technology Plan Project (grant no.: 2024-SFGG-178).
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Data sharing statement
The data that support the findings of this study are not publicly available but are available from the corresponding author or data sharing committee upon reasonable request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 36.06 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Keep RF, Hua Y, Xi G. Intracerebral haemorrhage: mechanisms of injury and therapeutic targets. Lancet Neurol. 11(8), 720–731 (2012).
2.
Krishnamurthi RV, Feigin VL, Forouzanfar MH et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990–2010: findings from the global burden of disease study 2010. Lancet Glob. Health 1(5), e259–e281 (2013).
3.
Mendelow AD, Gregson BA, Fernandes HM et al. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the international surgical trial in intracerebral haemorrhage (STICH): a randomised trial. Lancet 365(9457), 387–397 (2005).
4.
Krishnamurthi RV, Ikeda T, Feigin VL. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: a systematic analysis of the global burden of disease study 2017. Neuroepidemiology 54(2), 171–179 (2020).
5.
Wang GQ, Li SQ, Huang YH et al. Can minimally invasive puncture and drainage for hypertensive spontaneous basal ganglia intracerebral hemorrhage improve patient outcome: a prospective non-randomized comparative study. Mil. Med. Res. 1, 10 (2014).
• Provided early prospective evidence supporting the use of minimally invasive puncture and drainage (MIPD) in basal ganglia hemorrhage.
6.
Mendelow AD, Gregson BA, Rowan EN et al. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial lobar intracerebral haematomas (STICH II): a randomised trial. Lancet 382(9890), 397–408 (2013).
•• Landmark randomized controlled trial (STICH II) showing no significant advantage of craniotomy over conservative treatment.
7.
Li Z, Li Y, Xu F et al. Minimal invasive puncture and drainage versus endoscopic surgery for spontaneous intracerebral hemorrhage in basal ganglia. Neuropsychiatr. Dis. Treat. 13, 213–219 (2017).
8.
Hanley DF, Thompson RE, Rosenblum M et al. Efficacy and safety of minimally invasive surgery with thrombolysis in intracerebral haemorrhage evacuation (MISTIE III): a randomised, controlled, open-label, blinded endpoint phase 3 trial. Lancet 393(10175), 1021–1032 (2019).
•• Large multicenter randomized clinical trial (RCT) (MISTIE III) providing high-level evidence for minimally invasive hematoma evacuation.
9.
Pradilla G, Ratcliff JJ, Hall AJ et al. Trial of early minimally invasive removal of intracerebral hemorrhage. N. Engl. J. Med. 390(14), 1277–1289 (2024).
• Recent RCT suggesting potential benefits of early minimally invasive removal of ICH.
10.
Fazl A, Fleisher J. Anatomy, physiology, and clinical syndromes of the basal ganglia: a brief review. Semin. Pediatr. Neurol. 25, 2–9 (2018).
11.
Yanagisawa N. Functions and dysfunctions of the basal ganglia in humans. Proc. Jpn Acad. Ser. B Phys. Biol. Sci. 94(7), 275–304 (2018).
12.
Kwak R, Kadoya S, Suzuki T. Factors affecting the prognosis in thalamic hemorrhage. Stroke 14(4), 493–500 (1983).
13.
Greenberg SM, Ziai WC, Cordonnier C et al. 2022 guideline for the management of patients with spontaneous intracerebral hemorrhage: a guideline from the American Heart Association/American Stroke Association. Stroke 53(7), e282–e361 (2022).
•• Authoritative 2022 AHA/ASA guideline summarizing evidence-based management of spontaneous intracerebral hemorrhage.
14.
Cordonnier C, Demchuk A, Ziai W, Anderson CS. Intracerebral haemorrhage: current approaches to acute management. Lancet 392(10154), 1257–1268 (2018).
15.
Zi W, Qiu Z, Li F et al. Effect of endovascular treatment alone vs intravenous alteplase plus endovascular treatment on functional independence in patients with acute ischemic stroke: the DEVT randomized clinical trial. JAMA 325(3), 234–243 (2021).
16.
Fallenius M, Skrifvars MB, Reinikainen M et al. Spontaneous intracerebral hemorrhage. Stroke 50(9), 2336–2343 (2019).
17.
Mould WA, Carhuapoma JR, Muschelli J et al. Minimally invasive surgery plus recombinant tissue-type plasminogen activator for intracerebral hemorrhage evacuation decreases perihematomal edema. Stroke 44(3), 627–634 (2013).
18.
Xu X, Zhang H, Zhang J et al. Minimally invasive surgeries for spontaneous hypertensive intracerebral hemorrhage (MISICH): a multicenter randomized controlled trial. BMC Med. 22(1), 244 (2024).
• Recent multicenter RCT in China evaluating minimally invasive surgery, highly relevant to the study population.
19.
de Oliveira Manoel AL. Surgery for spontaneous intracerebral hemorrhage. Crit. Care 24(1), 45 (2020).
20.
Guo W, Liu H, Tan Z et al. Comparison of endoscopic evacuation, stereotactic aspiration, and craniotomy for treatment of basal ganglia hemorrhage. J. Neurointerv. Surg. 12(1), 55–61 (2020).
• Comparative study exploring different surgical strategies for basal ganglia hemorrhage.
21.
Zhu H, Wang Z, Shi W. Keyhole endoscopic hematoma evacuation in patients. Turk. Neurosurg. 22(3), 294–299 (2012).
22.
Beynon C, Schiebel P, Bosel J et al. Minimally invasive endoscopic surgery for treatment of spontaneous intracerebral haematomas. Neurosurg. Rev. 38(3), 421–428 (2015).
23.
Zhou H, Zhang Y, Liu L et al. Minimally invasive stereotactic puncture and thrombolysis therapy improves long-term outcome after acute intracerebral hemorrhage. J. Neurol. 258(4), 661–669 (2011).
• Demonstrated that minimally invasive stereotactic puncture combined with thrombolysis improved long-term outcomes.
24.
Delcourt C, Sato S, Zhang S et al. Intracerebral hemorrhage location and outcome among INTERACT2 participants. Neurology 88(15), 1408–1414 (2017).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 16 June 2025
Accepted: 23 October 2025
Published online: 27 November 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparison treatments for basal ganglia hemorrhage: minimally invasive puncture and drainage versus craniotomy versus conservative treatment. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0097
Export citation
Select the citation format you wish to export for this article or chapter.