Adherence, duration and healthcare costs in a real-world population of patients with acromegaly
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The aim of this study was to describe treatment patterns among patients with acromegaly who are newly treated with acromegaly medical therapy. Materials & methods: Data from IQVIA Pharmetrics Plus® Database from 1 January 2013 to 30 June 2023 were used to identify patients with acromegaly who started a new acromegaly medical therapy and observe their treatment patterns. Patients were required to have at least 12 months of data without any acromegaly therapy (medication or surgery) prior to the index date and at least 6 months of follow-up. Comorbidities were measured during the baseline period. Adherence, persistence, medication and switching were measured during follow-up. Results: A total of 453 patients with acromegaly who were newly treated with acromegaly medical therapy and had no evidence of acromegaly therapy for at least 12 months were identified. Among these patients, 46.1% (n = 206) were treated with cabergoline as their index treatment, 24.5% (n = 111) with injectable octreotide, 15.0% (n = 68) with lanreotide, 5.5% (n = 25) with bromocriptine, 4.9% (n = 22) with pegvisomant, 2.2% (n = 10) with pasireotide, 1.1% (n = 5) with oral octreotide, 0.4% (n = 2) with cabergoline + octreotide, and 0.2% (n = 1) with cabergoline + lanreotide. By the end of the follow-up period, 54.3% (n = 246) were not on any treatment, 19.6% (n = 89) remained on the index treatment, and the remaining 26.0% (n = 118) switched to another treatment. Conclusion: This study contributed to the growing evidence that patients with acromegaly are not well-served by current therapeutic options, as indicated by high rates of treatment discontinuation, switching and add-on therapy. However, treatment switching and add-on therapy represent ongoing efforts to optimize patient care toward more effective and tolerable treatments. Expanded treatment options may serve an unmet need in this patient population.
Plain language summary
What is this article about?
Acromegaly is a rare, chronic condition caused by high hormone levels and results in soft tissue growth, joint pain, hypertension, diabetes and increased risk of mortality. In this study, the aim was to investigate medication persistence (i.e., how long patients stay on a medication), medication adherence (i.e., how consistently patients take their medication as prescribed) and medication switching/add-on therapy (i.e., how often patients use a different medication from the one they were initially prescribed).
What were the results?
We used health insurance claims data from the IQVIA Pharmetrics Plus Database to understand treatments patterns. Patients were not treated with any acromegaly medical therapy for at least 12 months prior to starting the new treatment. All patients were observed for at least 6 months with varying lengths of follow-up. Nearly 80% of patients did not persist with their initial therapy (discontinued [54%] or switched/added-on a medical treatment [26%]) by the end of follow-up.
What do the results mean?
Medication persistence and adherence are important in the management of chronic disease. However, we found that about 80% of patients with acromegaly who were newly treated with medication do not persist with medical therapy. Lack of persistence, when either discontinuing, switching or adding-on, represents opportunities for providers and patients to select therapies that better serve patient needs. These findings highlight the need for expanded treatment options.
In patients with acromegaly, a pituitary tumor releases excess growth hormone (GH) which stimulates the liver to produce high levels of insulin-like growth factor (IGF-1) [1]. Elevated GH and IGF-1 levels result in pathological changes, such as bone growth, soft tissue swelling, nerve entrapment and alternations in facial features, and higher rates of comorbidities such as cardiovascular disease, endocrine disorders, arthritis, cancer and mortality [2,3]. The goal of treatment is to reduce GH and/or IGF-1 levels, limit disease progression, and alleviate the symptoms and comorbidities associated with the disease [4,5]. Despite the availability of surgical treatment and pharmacological therapies, real-world evidence suggests that a large proportion of patients discontinue or modify their treatment regimens due to ineffectiveness, side effects, or other barriers [6–10].
Although there are numerous treatment options, many patients with acromegaly continue to struggle with uncontrolled disease. Surgery to remove the pituitary tumor is usually the primary intervention but about half of patients require additional treatment [11]. Pharmacologic therapy consists of somatostatin receptor ligands (SRLs; i.e., octreotide, lanreotide and pasireotide) that inhibit GH secretion, dopamine agonists (i.e., cabergoline and bromocriptine) that reduce GH levels, or GH receptor antagonist (i.e., pegvisomant) that block GH by binding to its receptor. Clinical trial data indicate that the therapeutic efficacy varies greatly between individual therapies with an average biochemical response rate of approximately 17–97% across most large studies [12–14]. Patients who partially respond to a particular therapy may increase the medication’s administration frequency or dose strength [5,15,16]. However, higher intensity medication regimens are associated with 50–63% of patients reporting side effects that were not present on the standard regimen [17,18]. Other patients may achieve better disease management by trying a different treatment and closely monitoring GH and IGF-1 laboratory values. These patients may switch to a new therapy, add a second medication to their regimen, undergo an additional pituitary surgery, or undergo radiotherapy [19]. A long-term, retrospective, single-center study found that 93.2% of patients achieved biochemical control and 69.9% of those patients received a second-line treatment following surgery [20]. However, both negative outcomes following radiotherapy and surgery and lack of persistence with medication may be barriers to safe and effective acromegaly therapy. For example, studies that assessed complications following repeated pituitary surgery or radiotherapy have reported negative outcomes including hormone deficits (e.g., panhypopituitarism, corticotroph deficiency, transient vasopressin deficiency), meningitis, vision loss, and cerebrospinal fluid leakage [21–23]. Real-world evidence studies report that discontinuation of acromegaly medical therapy is high [6,8,24,25]. Lack of medication persistence is of particular concern because once medical therapy stops, IGF-1 levels typically begin to rise. In a study of patients who were previously controlled on medication, 63% experienced biochemical disease recurrence 3 months after discontinuing SRLs; the rate of recurrence increased to 81% after 1 year [26]. Uncontrolled disease is associated with increase morbidity and mortality [27–29].
While evidence from claims-based analyses reveal widespread discontinuation and treatment switching, evidence from surveys and patient interviews highlight challenges with tolerability, treatment burden, lack of perceived efficacy and negative impacts of quality of life [8,30,31]. Patients who are prescribed injectable SRLs, report experiencing reluctance toward injectable treatments due to pain at the injection site, feelings of sadness and/or anxiety, side effects including fatigue, join pain, sweating and headaches, interference with work activities and leisure activities, and challenges related to scheduling and traveling for injection administration [32–34]. Tolerability issues and side effects are not limited to the SRLs. A multicenter study of patients treated with a dopamine agonist found that 52% of patients experienced at least one impulse control disorder [35].
Selecting an effective and well-tolerated acromegaly therapy remains a complex problem for many patients. This study assessed first-line medical therapy, persistence, and treatment modification in newly treated patients with acromegaly. Several studies have provided valuable treatment patterns insights using administrative claims data [7,8,36,37]. However, most existing claims-based analyses were conducted before the 2020 US FDA approval of oral octreotide and have little information about infrequently used therapies. The aim of this study was to add to the literature on real-world management of acromegaly by analyzing recent data, measuring utilization of less commonly used therapies and exploring the association between medical therapy and pituitary surgery.
Materials & methods
Data spanning from 1 January 2013 to 30 June 2023 from the IQVIA Pharmetrics Plus® Database were used to identify patients with acromegaly who started a new acromegaly medical therapy and observe their treatment patterns. The IQVIA Pharmetrics Plus® Database is a longitudinal closed claims dataset of administrative health insurance reimbursement records covering more than 210 million lives since 2006; it is primarily composed of private health insurance plans (i.e., commercial plans and self-funded plans) [38]. Between 1 January 2014 and 31 December 2022 (identification period), patients with existing or newly diagnosed acromegaly and newly starting a medical treatment with a 12-month washout period were identified based on the inclusion criteria. Patients who started a new medical therapy were selected so that the treatment history could be observed from medication initiation until the end of follow-up. The date on which patients started a new medical therapy was the index date. The baseline (pre-index) period was 12 months long and patients were followed for at least 6 months after the index date or the end of study period, whichever occurred later (follow-up period). Patients were required to have continuous enrollment during the baseline and follow-up periods.
The inclusion criteria for this study included evidence of an acromegaly diagnosis, an age threshold, acromegaly treatment with medical therapy and continuous enrollment. Patients with existing or newly diagnosed acromegaly were included if they had ≥2 medical claims with acromegaly (International Classification of Diseases, 9th Revision, Clinical Modification [ICD-9-CM] diagnosis code: 253.0; ICD-10-CM: E22.0) in any diagnosis field or if they had ≥1 medical claim with an acromegaly diagnosis code in combination with one other claim for a pituitary tumor (ICD-9-CM: 227.3, 237.0; ICD-10-CM: D35.2, D44.3), pituitary surgery (hypophysectomy; see Appendix Table A for procedure codes), or cranial stereotactic radiosurgery (CSR; see Appendix Table A for procedure codes). Patients had either an existing diagnosis (i.e., prevalent cases of acromegaly which have been ongoing for an extended time) or a new diagnosis (i.e., incident cases that were diagnosed on or near the index date). Both existing and new diagnoses were included so that the study had a large enough sample size to make meaningful inferences about the treatment patterns described. All patients were required to be ≥18 years old during the year of identification. Patients were required to have started a new acromegaly medical therapy (mono or combination treatment) as the index date. A therapy was defined as a new medical therapy if it was not used during the 12-month baseline period. The 12-month baseline period was chosen as a balance between having a long enough baseline during where no acromegaly therapies were observed and having a short enough baseline so that study cohort size was not limited by unnecessarily strict continuous enrollment criteria at baseline. Patients who are commercially insured have high levels of disenrollment; 21.5% of members in a commercial health insurance plan disenroll each year [39]. Patients could have had acromegaly therapy (medication, surgery or medical therapy) prior to the baseline period. Acromegaly medical therapies included SRLs (octreotide, lanreotide and pasireotide), dopamine receptor agonists (cabergoline, bromocriptine) and a GH receptor antagonist (pegvisomant). Acromegaly medical therapies were identified using a combination of National Drug Code (NDC) codes and Healthcare Common Procedure Coding System (HCPCS) codes.
Patient socio-demographics (age and gender), insurance and geographic region at index date were reported. Patients in this cohort were identified as having a baseline comorbidity if a claim with a diagnosis for that comorbidity was observed during the 1-year baseline period. Baseline comorbidities were selected due to their association with acromegaly [40–43]. The selected baseline comorbidities included musculoskeletal conditions (osteoarthritis, arthropathy/arthralgia/synovitis, kyphosis and scoliosis, vertebral fracture, carpal tunnel syndrome, myopathy/myalgia), cardiovascular conditions (hypertension, cardiomyopathy, cardiac hypertrophy, heart failure, valvular heart disease and cardiac dysrhythmia/arrhythmia), endocrine/metabolic conditions (diabetes [including impaired glucose tolerance], obesity, galactorrhea, menstrual abnormality, impaired libido/impotence and hypothyroidism), chronic obstructive pulmonary disease, sleep apnea, deficiency anemia, psychoses and depression (see Appendix Table B for diagnosis codes).
The following medical treatment patterns were measured during the follow-up period. The index treatment was defined as the acromegaly therapy patients received at index date, including mono or combination treatment (defined as treatment with ≥2 medications overlapping for >3 months). The second observed treatment was defined as the different treatment patients received after the index treatment, including mono or combination treatment. Treatment switch or add-on was defined as patients who switched their medication from index to subsequent treatments, including mono or combination treatment. Persistence of index treatment was defined as continuous use from the index treatment to the end of available days’ supply of the medication without a gap of ≥60 days. Patients were not considered to have persisted on index therapy if they continued with the index medication and added on a new therapy. Data were censored at the end of follow-up. Adherence to index treatment was defined as patients with a proportion of days covered (PDC) ≥80% while they were persistent with the index treatment. PDC was calculated by number of days with the medication available divided by days of duration.
The cost of acromegaly medical therapy per prescription fill or per injection for 28 days of supply were reported. Costs were reported from claims with NDC or HCPCS codes where applicable. NDCs and HCPCS codes are included on claims for reimbursement purposes when medications or vaccines are billed. Costs were adjusted to 2023 US Dollars using the medical component of the Consumer Price Index [44].
Additionally, patients with non-medical intervention (pituitary surgery or CSR; see procedure codes in Appendix A) during the 1-year pre-index period and at any time 1-year post-index period and annualized inpatient hospitalization during the entire post-index period were reported. The proportion of patients with acromegaly surgery during the follow-up period was stratified by treatment pattern (continued, discontinued or switched/added-on). For patients who stopped medication, the proportion of patients who had acromegaly surgery before stopping medication and the proportion of patients who had surgery after stopping medication were reported.
Descriptive statistics including mean, standard deviation (SD) and relative frequencies and percentages for continuous and categorical data, respectively, were reported. All data transformations and statistical analyses were performed using SAS© version 9.4.
Results
A total of 453 patients with acromegaly who were newly treated with medication were identified (Table 1). The overall cohort had mean (SD) age was 46.6 (14.1) years, and the greatest proportion of patients belong to the 35–54 years age group (44.8%, n = 203), 50.6% (n = 229) were female and 62.5% (n = 283) were covered by commercial insurance (Table 2). During baseline, newly treated patients had a mean (SD) Charlson Comorbidity Index of 1.4 (2.2). The most common comorbidities were endocrine/metabolic disorders (70.4% [n = 319] of patients) and cardiovascular disorders (50.6% [n = 229] of patients) (Table 3). Pituitary surgery was found in 26.7% and CSR in 1.7% of patients in the baseline period (Table 3).
| Criteria for identifying study cohorts | n |
|---|---|
| A. Patients with ≥2 claims with acromegaly diagnosis, or ≥1 claim with acromegaly diagnosis and a claim for a pituitary tumor or cranial stereotactic radiosurgery during the identification period (1 January 2014 to 31 December 2022). | 7269 |
| B. Among A, who used one of the medical treatments during the study period (1 January 2013 to 30 June 2023). The first medication treatment date during the identification period is defined as the index date. | 2178 |
| C. Among B, who were continuously enrolled with health plan during baseline period (1 year prior to the index date) – patients with acromegaly newly started a medical treatment. | 518 |
| D. Among C, who were continuously enrolled with health plan for ≥6 months after the index date. | 468 |
| E. Among D, who were 18 years or older. | 453 |
Data source: IQVIA Pharmetrics Plus® claims database, 1 January 2013 to 30 June 2023.
| Patients with acromegaly newly treated with medical therapy | ||
|---|---|---|
| n (%) | 453 (100%) | |
| Age range, years | Mean (SD) [median] | 46.6 (14.1) [45] |
| 18–34 | n (%) | 106 (23.4) |
| 35–54 | n (%) | 203 (44.8) |
| 55–64 | n (%) | 109 (24.1) |
| 65+ | n (%) | 35 (7.7) |
| Female | n (%) | 229 (50.6) |
| Geographic region | ||
| Midwest | n (%) | 109 (24.1) |
| Northeast | n (%) | 86 (19.0) |
| South | n (%) | 185 (40.8) |
| West | n (%) | 73 (16.1) |
| Insurance type | ||
| Commercial | n (%) | 283 (62.5) |
| Medicare | n (%) | 26 (5.7) |
| Other | n (%) | 144 (31.8) |
Data source: IQVIA Pharmetrics Plus® claims database, 1 January 2013 to 30 June 2023.
SD: Standard deviation.
| Patients with acromegaly newly treated with medical therapy | ||
|---|---|---|
| n (%) | 453 (100.0) | |
| Charlson Comorbidity Index | Mean (SD) [median] | 1.4 (2.2) [0] |
| 0 | n (%) | 228 (50.3) |
| 1 | n (%) | 89 (19.6) |
| 2 | n (%) | 53 (11.7) |
| 3+ | n (%) | 83 (18.3) |
| Endocrine/metabolic | n (%) | 319 (70.4) |
| Diabetes (including impaired glucose intolerance) | n (%) | 138 (30.5) |
| Obesity | n (%) | 136 (30.0) |
| Galactorrhea | n (%) | 19 (4.2) |
| Menstrual abnormalities | n (%) | 67 (14.8) |
| Impaired libido/impotence | n (%) | 41 (9.1) |
| Hypothyroidism | n (%) | 104 (23.0) |
| Cardiovascular | n (%) | 229 (50.6) |
| Hypertension | n (%) | 194 (42.8) |
| Cardiomyopathy | n (%) | 18 (4.0) |
| Cardiac hypertrophy | n (%) | 29 (6.4) |
| Congestive heart failure | n (%) | 20 (4.4) |
| Valvular heart disease | n (%) | 40 (8.8) |
| Cardiac dysrhythmia/arrhythmia | n (%) | 46 (10.2) |
| Musculoskeletal | n (%) | 109 (24.1) |
| Osteoarthritis | n (%) | 56 (12.4) |
| Arthropathy/arthralgia/synovitis | n (%) | 24 (5.3) |
| Kyphosis and scoliosis | n (%) | 4 (0.9) |
| Vertebral fracture | n (%) | 2 (0.4) |
| Carpal tunnel syndrome | n (%) | 17 (3.8) |
| Myopathy/myalgia | n (%) | 33 (7.3) |
| Sleep apnea (obstructive and central) | n (%) | 119 (26.3) |
| Depression | n (%) | 68 (15.0) |
| Deficiency anemias | n (%) | 41 (9.1) |
| Chronic obstructive pulmonary disease | n (%) | 13 (2.9) |
| Psychoses | n (%) | 1 (0.2) |
| Non-medical intervention | n (%) | 123 (27.2) |
| Pituitary surgery (hypophysectomy) | n (%) | 121 (26.7) |
| CSR | n (%) | 7 (1.5) |
Data source: IQVIA Pharmetrics Plus® claims database, 1 January 2013 to 30 June 2023.
CSR: Cranial stereotactic radiosurgery; SD: Standard deviation.
Among these patients, 46.1% (n = 206) were treated with cabergoline as their index treatment, 24.5% (n = 111) with injectable octreotide, 15.0% (n = 68) with lanreotide, 5.5% (n = 25) with bromocriptine, 4.9% (n = 22) with pegvisomant, 2.2% (n = 10) with pasireotide, 1.1% (n = 5) with oral octreotide, 0.4% (n = 2) with cabergoline + octreotide and 0.2% (n = 1) with cabergoline + lanreotide (Table 4). The median follow-up time was 2.3 years, and the average follow-up time was 2.9 years with a standard deviation of 1.9 years (Table 4). The mean (SD) duration of the index treatment was 356.2 (414.5) days and 83.2% (n = 377) were adherent (PDC ≥80%) (Table 4, Figure 1). For patients on an index monotherapy, patients treated with pegvisomant had the longest mean duration (492.0 days, n = 22) and bromocriptine the shortest (235.2 days, n = 25).
| Index treatment | Patients with acromegaly newly treated with medical therapy | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cabergoline | Injectable octreotide | Lanreotide | Bromocriptine | Pegvisomant | Pasireotide | Oral octreotide | Caber + octreotide | Caber + lanreotide | |||
| n (%) | 209 (46.1) | 111 (24.5) | 68 (15.0) | 25 (5.5) | 22 (4.9) | 10 (2.2) | 5 (1.1) | 2 (0.4) | 1 (0.2) | 453 (100.0) | |
| Years of follow-up | Mean | 2.8 | 2.9 | 2.7 | 3.0 | 3.1 | 3.9 | 1.6 | 3.0 | 0.5 | 2.9 |
| SD | 1.9 | 1.8 | 1.9 | 2.3 | 2.3 | 2.6 | 0.7 | 1.6 | 0 | 1.9 | |
| Median | 2.3 | 2.6 | 2.0 | 2.3 | 2.5 | 2.9 | 1.2 | 3.0 | 0.5 | 2.3 | |
| Duration of index treatment without a gap ≥60 days during the follow-up period† | Mean | 331.2 | 332.8 | 458.2 | 235.2 | 492.0 | 396.7 | 404.0 | 596.5 | 180.0 | 356.2 |
| SD | 402.0 | 384.0 | 476.4 | 244.1 | 614.4 | 307.8 | 369.2 | 101.1 | n/a | 414.5 | |
| Median | 202 | 210 | 322 | 185 | 216 | 300 | 401 | 597 | 180 | 224 | |
| PDC (%) while persistent with the index treatment | Mean | 92.0 | 90.5 | 89.7 | 90.1 | 90.4 | 88.4 | 94.3 | 91.4 | 91.7 | 91.0 |
| SD | 12.3 | 10.6 | 9.9 | 13.8 | 10.8 | 8.2 | 7.8 | 3.7 | n/a | 11.4 | |
| Median | 98 | 94 | 91 | 98 | 93 | 90 | 98 | 91 | 92 | 95 | |
| PDC ≥80% while persistent with the index treatment | n (%) | 175 (83.7) | 91 (82.0) | 56 (82.4) | 19 (76.0) | 19 (86.4) | 9 (90.0) | 5 (100.0) | 2 (100.0) | 1 (100.0) | 377 (83.2) |
| Discontinued the index treatment by the end of follow-up† | n (%) | 166 (79.4) | 92 (82.9) | 53 (77.9) | 20 (80.0) | 19 (86.4) | 9 (90.0) | 4 (80.0) | 1 (50.0) | 0 (0.0) | 364 (80.4) |
| Stopped the index treatment and not on any treatment at the end of the follow-up† | n (%) | 129 (61.7) | 47 (42.3) | 34 (50.0) | 15 (60.0) | 15 (68.2) | 3 (30.0) | 2 (40.0) | 1 (50.0) | 0 (0.0) | 246 (54.3) |
| Switched during the follow-up period† | n (%) | 37 (17.7) | 45 (40.5) | 19 (27.9) | 5 (20.0) | 4 (18.2) | 6 (60.0) | 2 (40.0) | 0 (0.0) | 0 (0.0) | 118 (26.0) |
†
All patients were followed for at least 6 months with various lengths of follow-up.
Data source: IQVIA Pharmetrics Plus® claims database, 1 January 2013 to 30 June 2023.
PDC: Proportion of days covered; SD: Standard deviation.
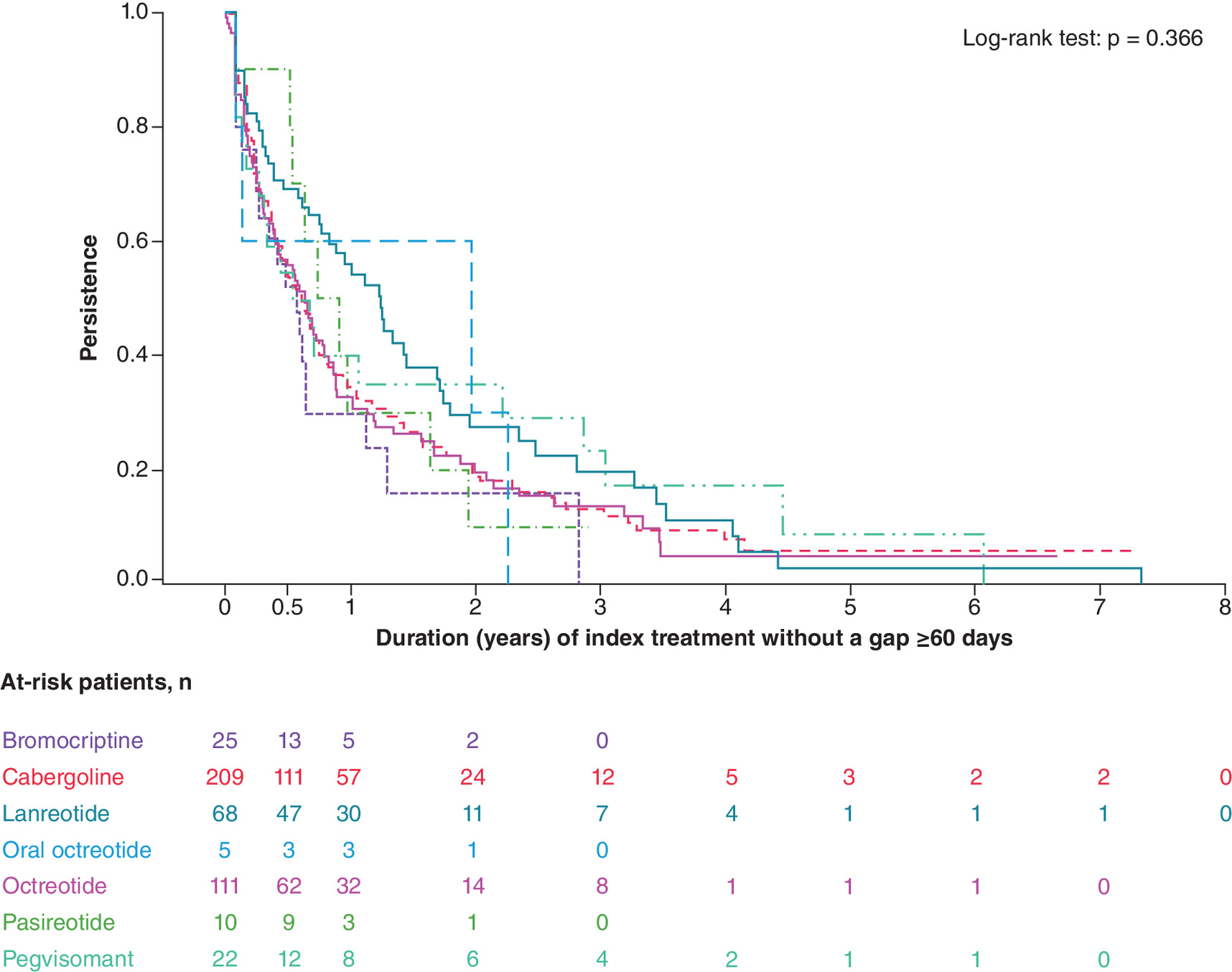
Figure 1. Persistence of index treatment among patients with mono index treatment.
All patients were followed for at least 6 months with various lengths of follow-up.
Data source: IQVIA Pharmetrics Plus® claims database, 1 January 2013 to 30 June 2023.
Of the 453 patients starting a new acromegaly medical therapy, 54.3% (n = 246) were not on any treatment at the end of follow-up, 19.6% (n = 89) remained on the index treatment and the remaining 26.0% (n = 118) switched to another treatment during follow-up (Table 4, Figure 2). Patients with the index treatment pasireotide had the most discontinuation (90.0% [n = 9] of patients), with 60.0% (n = 6) switching to a different therapy. The following index therapies had the largest proportion of patients who stopped their index treatment and were not on any treatment at the end of follow-up: pegvisomant (68.2%, n = 15), cabergoline (61.7%, n = 129) and bromocriptine (60.0%, n = 15). Among patients who switched (n = 118), the most common second treatments were cabergoline/cabergoline add-on therapy (33.1%, n = 39) and lanreotide (19.5%, n = 23) (Figure 2).
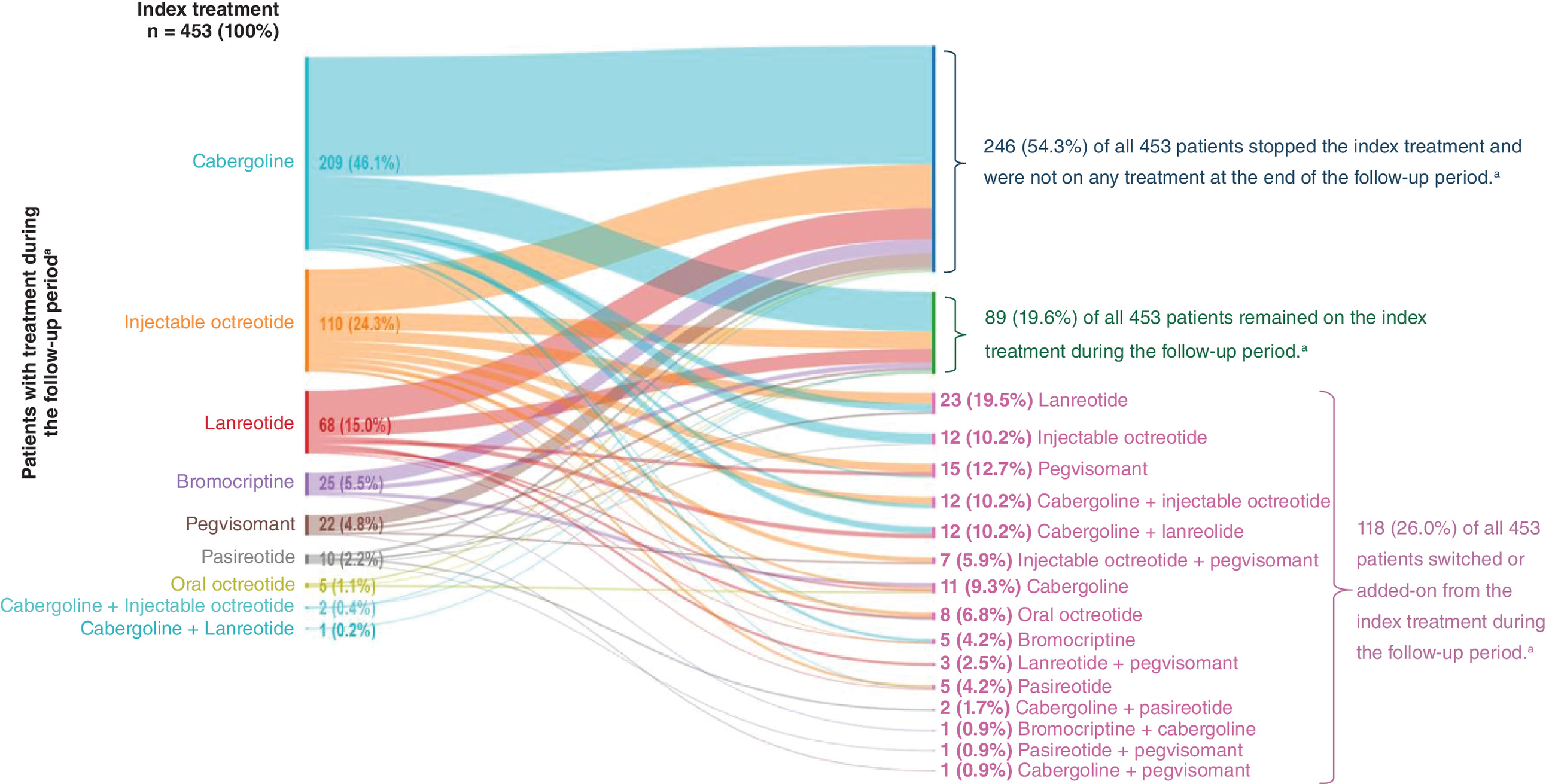
Figure 2. Treatment pattern among patients who stopped, remained on or switched/added-on an acromegaly medical therapy during the follow-up period.a
a All patients were followed for at least 6 months with various lengths of follow-up.
Data source: IQVIA Pharmetrics Plus® claims database, 1 January 2013 to 30 June 2023.
The average costs of each medical therapy per prescription fill or injection for 28 days of supply was measured for pasireotide ($14,681), pegvisomant ($12,379), lanreotide ($8133), oral octreotide ($7791), injectable octreotide ($5758), bromocriptine ($200), and cabergoline ($104) (Figure 3).
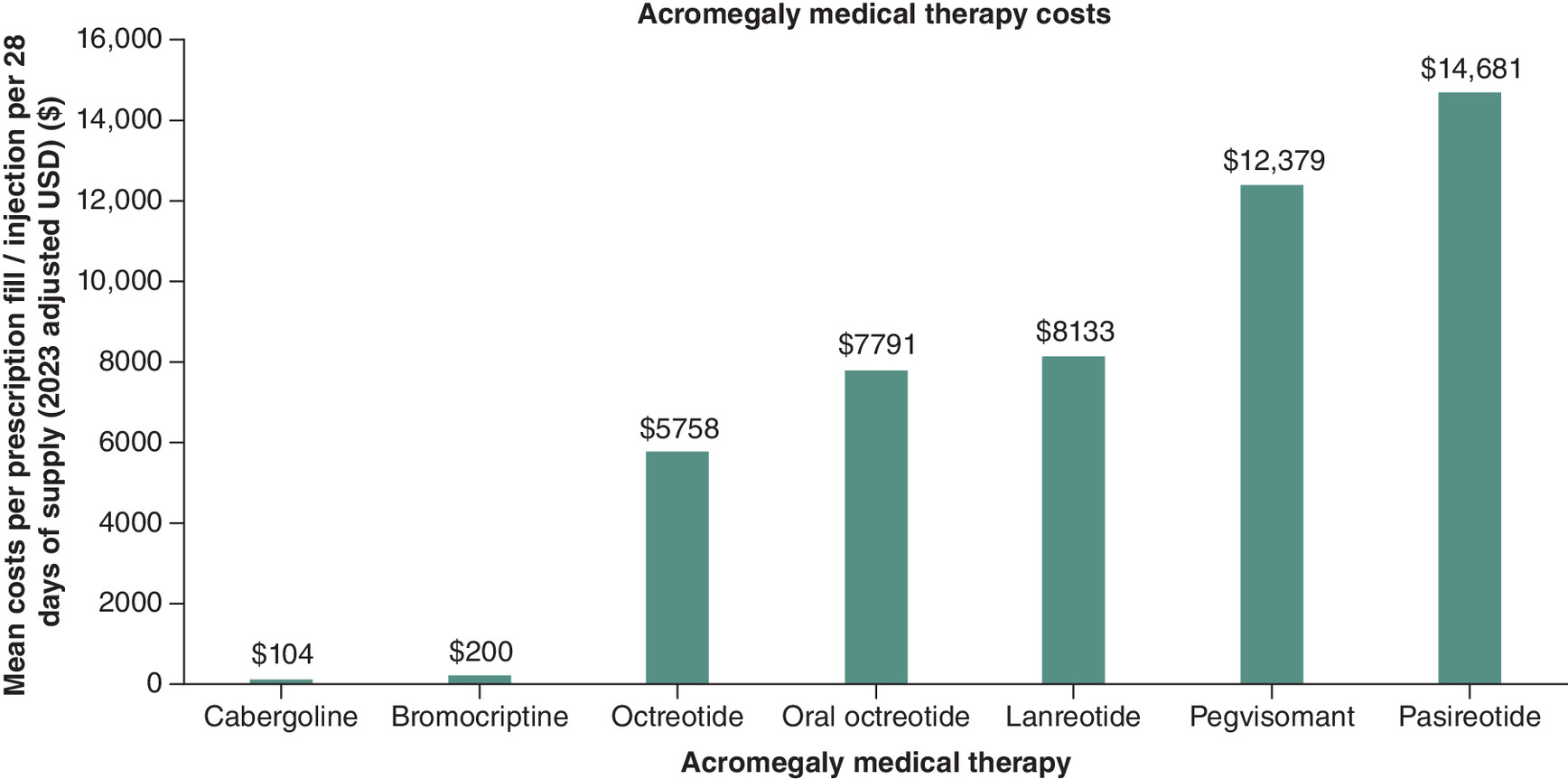
Figure 3. Acromegaly medical therapy costs (adjusted to Y2023 dollars) per fill/injection for 28 days of supply during the follow-up period.a
a All patients were followed for at least 6 months with various lengths of follow-up.
Data source: IQVIA Pharmetrics Plus® claims database, 1 January 2013 to 30 June 2023.
During the follow-up period, the proportion of patients who had non-medical intervention after newly initiating medical therapy was highest in patients who switched or added-on a therapy (19.5%, n = 23), followed by patients who discontinued therapy (16.3%, n = 40) and lowest for patients who remained on their index treatment (0.0%, n = 0) (Table 5). Patients who switched/added on therapy had higher rates of pituitary surgery (17.8%, n = 21) compared with CSR (1.7%, n = 2). Similarly, patients who discontinued therapy had higher rates of pituitary surgery (14.6%, n = 6) compared with CSR (2.4%, n = 6). Among patients who discontinued therapy and had surgery during the follow-up period, 25 patients (62.5%) stopped therapy prior to undergoing surgery. Among the 63 patients with non-medical intervention during follow-up, 16 patients also had evidence of prior non-medical intervention during baseline (Table 5). The proportion of patients with non-medical intervention during both the baseline and follow-up periods was highest among those who discontinued therapy (27.5%, n = 11), followed by patients who switched or added-on a therapy (21.7%, n = 5). When pituitary surgery was observed within 1 year of the index date (i.e., 1 year prior to the index and 1 year following the index date), surgery was observed in 35.8% of patients (results not shown). The mean (SD) number of annual inpatient hospitalizations was 0.26 (0.65) visits, with more visits among those who switched medical treatment compared with those without a switch (0.31 vs 0.24, p = 0.106; results not shown).
| Stopped the index treatment | Remained on the index treatment | Switched or added-on from the index treatment | Patients with acromegaly newly treated with medical therapy | ||
|---|---|---|---|---|---|
| n (%) | 246 (54.3) | 89 (19.6) | 118 (26.0) | 453 (100.0) | |
| Surgery (hypophysectomy or CSR) during follow-up period | n (%) | 40 (16.3) | 0 (0.0) | 23 (19.5) | 63 (13.9) |
| Pituitary surgery (hypophysectomy) during follow-up period | n (%) | 36 (14.6) | 0 (0.0) | 21 (17.8) | 57 (12.6) |
| CSR during follow-up period | n (%) | 6 (2.4) | 0 (0.0) | 2 (1.7) | 8 (1.8) |
| Non-medical intervention (hypophysectomy or CSR) during baseline and follow-up periods‡ | n (%) | 11 (27.5) | 0 (0.0) | 5 (21.7) | 16 (25.4) |
| Pituitary surgery (hypophysectomy) during baseline and follow-up periods | n (%) | 11 (27.5) | 0 (0.0) | 4 (17.4) | 15 (23.8) |
| CSR during baseline and follow-up periods | n (%) | 0 (0.0) | 0 (0.0) | 1 (43.3) | 1 (1.6) |
†
All patients were followed for at least 6 months with various lengths of follow-up.
‡
Subgroup of patients with at least one non-medical intervention in the baseline period among patients who had at least one non-medical intervention in the follow-up period.
Data source: IQVIA Pharmetrics Plus® claims database, 1 January 2013 to 30 June 2023.
CSR: Cranial stereotactic radiosurgery.
Discussion
This study of acromegaly patients, using data from 2013 to 2023, reveals that approximately 80% do not persist with their newly started medical therapy. Most patients rely on therapies such as cabergoline monotherapy, injectable octreotide, and lanreotide. Lack of persistence with these therapies may be due to the lack of efficacy or dissatisfaction with the route of administration. The uptake of newer therapies, such as oral octreotide, is low. These findings highlight the unmet need for more effective, better tolerated, and patient-centered treatment options for individuals with acromegaly. Furthermore, even patients who do persist with ineffective treatments may be better served by switching to a more effective therapy.
Consistent with previous claims-based studies examining treatment patterns in patients with acromegaly, cabergoline and the somatostatin analogs octreotide and lanreotide were the most common index treatments [8,36,37,45]. The high percentage of index cabergoline users suggests that the patient population may have more mild disease; consensus guidelines recommend first-line cabergoline treatment only in patients with IGF-1 levels that were no more than 2–2.5 times the upper limit of normal [5,19]. Other explanations for the high percentage of patients who were prescribed cabergoline include that patients were seeking a medication that was less expensive than alternative therapies, patients were required by their insurance plans to use cabergoline before advancing to other medical therapies, or that patients favored oral medications over injections [46,47]. A small proportion of patients (5.5%) received bromocriptine as index therapy. The evidence for bromocriptine's effectiveness is low and it has not been mentioned in any recent clinical guidelines [5,15,19,48]. Patients may be better served with newer therapeutic options that have been shown to be more effective under both regulatory-grade intervention trials and in real-world settings. Low utilization of medications like pegvisomant, pasereotide, and oral octreotide raises questions about access barriers or clinicians’ assessments of the efficacy and safety of these drugs.
In this study, over half of patients discontinued therapy by the end of the follow-up period. Nontreatment may have been due disease remission, successful reduction of IGF-1 and GH levels through surgery, healthcare barriers (e.g., cost) or patient dissatisfaction and/or tolerability with current treatment options [9]. This study found a higher proportion of patients who stopped their index treatment and a lower proportion who switched than a previously published study by Carmichael and colleagues which used 2002–2013 data from two claims databases [49]. In a more recent study, Fleseriu and colleagues found that 59.4% had only one line of therapy but did not specify whether these patients remained on treatment or if treatment was stopped completely [8]. The current study’s longer baseline period (12 months) during which no evidence of acromegaly therapy utilization was observed means that patients who may have only taken a break from treatment were more likely to have been excluded compared with Carmichael (no reported baseline) and Fleseriu (6 months baseline). Patients who recently started a new medical therapy may be earlier in the process of finding an individualized therapeutic regimen to continue using for disease management. Therefore, slightly higher rates of switching might be expected in a cohort that recently started a new medical therapy compared with a cohort that only took a short-term break from medical therapy.
Less than one-fifth of patients who discontinued treatment also had surgery during the follow-up period. Surgery rates increased to 35.8% of patients when healthcare utilization was observed for 1 year before and 1 year after the index date. Although we are unable to look at lifetime surgical history due to the lack of continuous enrollment in private health insurance plans, it is likely that surgery would be higher if we observed a longer baseline period. Among the patients who discontinued medical therapy and had surgery during the follow-up period, nearly two-thirds discontinued treatment prior to undergoing surgery. This study’s findings suggest that at least some patients with acromegaly undergo preoperative medical therapy, for which the benefits remain unclear [5,15,50,51]. The number of patients undergoing preoperative therapy may have been impacted by limits to healthcare utilization instituted during the coronavirus pandemic. Between 33.3 and 54.8% of patients reported delays in surgery during the early months of the pandemic [52,53] and may have been started on medication because of such a delay. Therefore, patients in this study who were observed during the coronavirus pandemic may have had have their treatment regimen impacted. Further research is needed to better understand the intentions around starting and then stopping medical therapy prior to pituitary surgery and to confirm the practice’s effectiveness in helping patients achieve biochemical control.
In addition to high rates of discontinuation, slightly more than one-fourth of patients newly treated with medication switched or added-on a therapy. Cabergoline, together with cabergoline add-on therapy, was the most common switched/added-on therapy. Clinical guidelines and meta-analyses consider cabergoline to be limited as acromegaly monotherapy but useful and effective as an add-on therapy, particularly when SRL monotherapy is ineffective [15,54,55]. The presence of multiple treatment modifications across studies reinforces the need for more effective and tolerable interventions for disease control among some subgroups of patients. Fleseriu and colleagues’ similar claims-based analysis observed two lines of therapy for 23.1% of patients and three or more lines medical therapy for 17.3% of patients [8]. Although this study was unable to determine why patients switched medications during the follow-up period, this study compared the number of inpatient hospitalizations between patients who switched medications and those who did not switch to understand whether an adverse event could precipitate a change in therapeutic management. This study did not find a statistically significant difference in the number of hospitalizations between switchers and nonswitchers. Future research may incorporate laboratory values to understand how often lack of biochemical control is the main reason for treatment modification compared with other rationales (e.g., patient dissatisfaction, adverse events and financial burden).
This study reported medication costs by individual therapy. Several surveys of patients and physicians reported that the financial burden of treatment was a significant factor in nonadherence [6,9,24,30,31]. Older medications, such as bromocriptine and cabergoline, were the least expensive medications taken in the cohort. Cabergoline’s relatively lower costs, in addition to its effectiveness when combined with other treatments, may contribute to it enduring and common usage [56,57]. Conversely, pegvisomant’s relative higher costs may be a barrier to uptake despite its high effectiveness in both clinical trials and real-world settings [14,58,59].
There are several limitations that should be considered when interpreting the results of this study. First, there are no validated, US-based algorithms to identify patients diagnosed with acromegaly in administrative health insurance claims data. However, the algorithm that was used in the analysis is commonly used across claims-based acromegaly epidemiologic, burden of illness, and treatment patterns studies [8,37,45,60,61]. All individuals included in this study had at least one claim that indicated use of an acromegaly therapy and were required to have at least two claims with a diagnosis for acromegaly or one claim with a diagnosis for acromegaly and one claim associated with an acromegaly related procedure. Therefore, it is likely that the individuals in our cohort have been treated for acromegaly. Second, the interpretation of the study’s results is limited by what is available in administrative billing records and subject to coding inaccuracies, misclassification, and missing data. Third, this study only included an average of 3 years of follow-up; therefore, the cohort’s lifetime acromegaly medical history and healthcare utilization may be incomplete. For example, patients who had first-line surgical intervention may be included in this cohort; however, their surgery was unobserved because it occurred years prior to those patients’ index date. Furthermore, we were unable to measure which line of therapy patients were on at index. Patients in this study cohort included both prevalent and incident cases of acromegaly that were indexed at the start of a new therapy which was not necessarily the first-line medical therapy. We included both prevalent and incident cases so that the study cohort's size was large enough to provide meaningful insights into treatment patterns among patients with acromegaly. Fourth, this study was unable to observe whether patients administered acromegaly therapy, whether medication administration adhered to a specific schedule, or if it was administered correctly. Therefore, there are dimensions of medication adherence that remain unexplored in this study. Fifth, information on why patients discontinued medical therapy is not available in claims data. Future research incorporating treatment patterns and patient treatment satisfaction is needed. Sixth, because our data did not include laboratory values, this study was unable to determine whether patients achieved biochemical control with or without acromegaly therapy.
Conclusion
Overall, a large proportion of patients with acromegaly who start a new medication therapy go on to stop treatment or switch therapies. High levels of treatment discontinuation among patients with a chronic condition that is most effectively treated with long-term management may indicate patients are underserved and dissatisfied with current therapy options. Treatment switching and add-on therapy, while signaling that patients are not well-served by their current treatment regimen, represent proactive efforts by healthcare providers and patients to find optimal treatment regimens. Continued innovation is needed to better serve patients with acromegaly and provide them with expanded treatment options that allow for sustained disease management.
Summary points
•
This study measured treatment patterns among patients with acromegaly who are newly treated with acromegaly medical therapy.
•
IQVIA Pharmetrics Plus Database from 1 January 2013 to 30 June 2023 was used to measure treatment patterns.
•
Patients were included if they were diagnosed with acromegaly, were 18 years or older, and were continuously enrolled for at least 12 months prior to the start of acromegaly medical therapy and at least 6 months after the start of acromegaly medical therapy. A total of 453 patients met the inclusion criteria.
•
Over one-half of patients discontinued medical therapy by the end of the follow-up period.
•
Over one-fourth of patients switched to a new medical therapy or added on an additional medical therapy by the end of the follow-up period.
•
The frequent discontinuation and switching of medication regimens observed in this study, together with high rates of patient-reported dissatisfaction with current treatment options, highlight the burden of unmet need among patients with acromegaly.
•
Treatment switching and discontinuation are opportunities to prescribe patients more effective, better tolerated therapies.
•
Innovation in the acromegaly treatment space may address gaps in medication persistence and adherence.
Author contributions
TP Quock, SK Rattana and IE Paulson: acquisition of data; design of the work; interpretation of data; revising the work for important intellectual content; final approval. E Chang, AK Das, A Speller, MH Tarbox and MS Broder: design of the work; analysis of data; interpretation of data; drafting and revising the work for important intellectual content; final approval.
Financial disclosure
Funding for this study and publication-related fees were received from Crinetics Pharmaceuticals.
Competing interests disclosure
TP Quock, SK Rattana and IE Paulson are employees of and hold stock in Crinetics Pharmaceuticals, Inc. at the time of this study. At the time this research was conducted, E Chang, AK Das, A Speller, MH Tarbox and MS Broder were employees of Partnership for Health Analytic Research, LLC (now ADVI Health), which was paid by Crinetics to perform the research described in this manuscript. PHAR also discloses financial relationships with the following commercial entities outside of the submitted work: Abbvie, Akcea, Amgen, Astellas, AstraZeneca, Delfi Diagnostics, Dompe, Exact Sciences Corporation, Genentech, Gilead, GRAIL, Ionis, Janssen, Nobelpharma, Novartis, Pfizer, Recordati, Regeneron and Sanofi US Services. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 31.16 KB
References
Papers of special note have been highlighted as: • of interest
1.
Adigun OO, Nguyen M, Fox TJ, Anastasopoulou C. Acromegaly. In: StatPearls. StatPearls Publishing, FL, USA (2024). Available from: https://www.ncbi.nlm.nih.gov/sites/books/NBK431086/
2.
Fleseriu M, Langlois F, Lim DST, Varlamov EV, Melmed S. Acromegaly: pathogenesis, diagnosis, and management. Lancet Diabetes Endocrinol. 10(11), 804–826 (2022).
3.
Bello MO, Garla VV. Gigantism and Acromegaly. In: StatPearls. StatPearls Publishing, FL, USA (2024). Available from: http://www.ncbi.nlm.nih.gov/books/NBK538261/
4.
Yedinak C, Pulaski-Liebert KJ, Adelman DT, Williams J. Acromegaly: current therapies benefits and burdens. Clin. Pract. 15(2), 499–511 (2018).
• This clinical practice review describes utilization, benefits and trade-offs of current and emerging acromegaly therapies as of 2018. The review considers clinical presentation, quality of life, drug administration issues, economic factors and patient-reported outcomes, treatment adherence and provider-related issues.
5.
Melmed S, Bronstein MD, Chanson P et al. A consensus statement on acromegaly therapeutic outcomes. Nat. Rev. Endocrinol. 14(9), 552–561 (2018).
6.
Plunkett C, Barkan AL. The care continuum in acromegaly: how patients, nurses, and physicians can collaborate for successful treatment experiences. Patient Prefer. Adher. 9, 1093–1099 (2015).
• This expert opinion article describes a dialog map to be used by nurses and physicians during acromegaly diagnosis, treatment decisions, treatment initiation and follow-up. The goal of the dialog map is to identify barriers to acromegaly treatment and address topics such as geographic, economic and psychological concerns.
7.
Chuang CC, Bhurke S, Chen SY, Dinet J, Brulais S, Gabriel S. Treatment patterns and economic burden in patients treated for acromegaly in the USA. Drugs – Real World Outcomes 2(3), 299–309 (2015).
• This claims-based analysis reports treatment patterns for patients with acromegaly who underwent surgery and/or who received medical therapy from 2007 to 2010.
8.
Fleseriu M, Barkan A, Brue T et al. Treatment patterns, adherence, persistence, and health care resource utilization in acromegaly: a real-world analysis. J. Endocr. Soc. 7(10), bvad104 (2023).
9.
Liu S, Xu Y, Begelman SM, Shi L. Barriers to treatment adherence associated with acromegaly in the United States: provider's perspective. Value Health 18(3), A64 (2015).
10.
Sisco J, Furumalm M, Yssing C, Okkels A, Zavisic S. Preferences for different treatment options among people living with acromegaly in the US. Curr. Med. Res. Opin. 40(4), 657–664 (2024).
11.
Ezzat S, Serri O, Chik CL et al. Canadian consensus guidelines for the diagnosis and management of acromegaly. Clin. Invest. Med. 29(1), 29–39 (2006).
12.
Carmichael JD, Bonert VS, Nuño M, Ly D, Melmed S. Acromegaly clinical trial methodology impact on reported biochemical efficacy rates of somatostatin receptor ligand treatments: a meta-analysis. J. Clin. Endocrinol. Metab. 99(5), 1825–1833 (2014).
13.
Colao A, Auriemma RS, Pivonello R, Kasuki L, Gadelha MR. Interpreting biochemical control response rates with first-generation somatostatin analogues in acromegaly. Pituitary 19(3), 235–247 (2016).
14.
Trainer PJ, Drake WM, Katznelson L et al. Treatment of acromegaly with the growth hormone–receptor antagonist pegvisomant. N. Engl. J. Med. 342(16), 1171–1177 (2000).
15.
Giustina A, Barkhoudarian G, Beckers A et al. Multidisciplinary management of acromegaly: a consensus. Rev. Endocr. Metab. Disord. 21(4), 667–678 (2020).
16.
Giustina A, Biermasz N, Casanueva FF et al. Consensus on criteria for acromegaly diagnosis and remission. Pituitary 27(1), 7–22 (2024).
17.
Giustina A, Mazziotti G, Cannavò S et al. High-dose and high-frequency lanreotide autogel in acromegaly: a randomized, multicenter study. J. Clin. Endocrinol. Metab. 102(7), 2454–2464 (2017).
• Reports the results of a prospective, open-label, interventional trial to test whether more frequent therapy or high dose therapy normalizes IGF-1 levels in patients with acromegaly who are partial responders to lanreotide.
18.
Giustina A, Bonadonna S, Bugari G et al. High-dose intramuscular octreotide in patients with acromegaly inadequately controlled on conventional somatostatin analogue therapy: a randomised controlled trial. Eur. J. Endocrinol. 161(2), 331–338 (2009).
19.
Giustina A, Chanson P, Kleinberg D et al. Expert consensus document: a consensus on the medical treatment of acromegaly. Nat. Rev. Endocrinol. 10(4), 243–248 (2014).
20.
Ghajar A, Jones PS, Guarda FJ et al. Biochemical control in acromegaly with multimodality therapies: outcomes from a pituitary center and changes over time. J. Clin. Endocrinol. Metab. 105(3), e532–e543 (2019).
21.
Palmisciano P, Ogasawara C, Ogasawara M et al. Endocrine disorders after primary gamma knife radiosurgery for pituitary adenomas: a systematic review and meta-analysis. Pituitary 25(3), 404–419 (2022).
22.
Wilson TJ, McKean EL, Barkan AL, Chandler WF, Sullivan SE. Repeat endoscopic transsphenoidal surgery for acromegaly: remission and complications. Pituitary 16(4), 459–464 (2013).
23.
Heringer LC, de Oliveira MF, Rotta JM, Botelho RV. Effect of repeated transsphenoidal surgery in recurrent or residual pituitary adenomas: a systematic review and meta-analysis. Surg. Neurol. Int. 7, 14 (2016).
24.
Polanco-Briceno S, Glass D, Plunkett C. Communication practices and awareness of resources for acromegaly patients among endocrinologists. Patient Prefer. Adher. 10, 2531–2541 (2016).
25.
Kamusheva M, Parvanova A, Rusenova Y, Vandeva S, Elenkova A. Do we need a specific guideline for assessment and improvement of acromegaly patients adherence? Front. Public Health 9, 693409 (2021).
26.
Hatipoglu E, Bozcan S, Kadioglu P. Discontinuation of somatostatin analogs while acromegaly is in long-term remission. Pituitary 18(4), 554–560 (2015).
• Aims to evaluate whether patients with acromegaly who were well-controlled with medical therapy continued to experience disease remission following therapy withdrawal.
27.
Esposito D, Ragnarsson O, Johannsson G, Olsson DS. Prolonged diagnostic delay in acromegaly is associated with increased morbidity and mortality. Eur. J. Endocrinol. 182(6), 523–531 (2020).
28.
Puder JJ, Nilavar S, Post KD, Freda PU. Relationship between disease-related morbidity and biochemical markers of activity in patients with acromegaly. J. Clin. Endocrinol. Metab. 90(4), 1972–1978 (2005).
29.
Gasco V, Prencipe N, Cuboni D et al. Diagnostic delay, older age, and hormonal levels at diagnosis affect disease burden and mortality in acromegaly. J. Endocrinol. Invest. 48(4), 919–929 (2024).
30.
Kamusheva M, Vandeva S, Mitov K et al. Adherence to acromegaly treatment and analysis of the related factors—a real-world study in Bulgaria. Pharmaceutics 15(2), 438 (2023).
31.
Siegel S, Giese S, Honegger J et al. Exploring potential influencing factors of inadherence to specialist aftercare and long-term medication in patients with acromegaly. Pituitary 27(4), 403–415 (2024).
32.
Fleseriu M, Molitch M, Dreval A et al. Disease and treatment-related burden in patients with acromegaly who are biochemically controlled on injectable somatostatin receptor ligands. Front. Endocrinol. 12, 627711 (2021).
33.
Strasburger CJ, Karavitaki N, Störmann S et al. Patient-reported outcomes of parenteral somatostatin analogue injections in 195 patients with acromegaly. Eur. J. Endocrinol. 174(3), 355–362 (2016).
• Reports the results from a survey of acromegaly patients who were treated with long-acting somatostatin analogs. The survey was conducted in Germany, the UK and the Netherlands and collected information on patient-reported symptoms, daily life impact and treatment satisfaction.
34.
Geer EB, Sisco J, Adelman DT et al. Patient reported outcome data from acromegaly patients treated with injectable somatostatin receptor ligands (SRLs) in routine clinical practice. BMC Endocr. Disord. 20(1), 117 (2020).
35.
Martinkova J, Trejbalova L, Sasikova M, Benetin J, Valkovic P. Impulse control disorders associated with dopaminergic medication in patients with pituitary adenomas. Clin. Neuropharmacol. 34(5), 179–181 (2011).
36.
Burton T, Le Nestour E, Bancroft T, Neary M. Real-world comorbidities and treatment patterns of patients with acromegaly in two large US health plan databases. Pituitary 16(3), 354–362 (2013).
37.
Broder MS, Chang E, Ludlam WH, Neary MP, Carmichael JD. Patterns of pharmacologic treatment in US patients with acromegaly. Curr. Med. Res. Opin. 32(5), 799–805 (2016).
38.
IQVIA. IQVIA PharMetrics® Plus Fact Sheet (2025). Available from: https://www.iqvia.com/-/media/iqvia/pdfs/library/fact-sheets/iqvia-pharmetrics-plus-fs.pdf
39.
Fang H, Frean M, Sylwestrzak G, Ukert B. Trends in disenrollment and reenrollment within US Commercial Health Insurance Plans, 2006–2018. JAMA Netw. Open 5(2), e220320 (2022).
40.
Abreu A, Tovar AP, Castellanos R et al. Challenges in the diagnosis and management of acromegaly: a focus on comorbidities. Pituitary 19(4), 448–457 (2016).
41.
Slagboom TNA, van Bunderen CC, De Vries R, Bisschop PH, Drent ML. Prevalence of clinical signs, symptoms and comorbidities at diagnosis of acromegaly: a systematic review in accordance with PRISMA guidelines. Pituitary 26(4), 319–332 (2023).
42.
Wolters TLC, Roerink SHPP, Drenthen LCA et al. The course of obstructive sleep apnea syndrome in patients with acromegaly during treatment. J. Clin. Endocrinol. Metab. 105(1), 290–304 (2020).
43.
Rolla M, Jawiarczyk-Przybyłowska A, Halupczok-Żyła J et al. Complications and comorbidities of acromegaly—retrospective study in Polish center. Front. Endocrinol. 12, 642131 (2021).
44.
US Bureau of Labor Statistics, Division of Consumer Prices and Price Indexes. Consumer Price Index (2021). Available from: https://www.bls.gov/cpi/
45.
Broder MS, Neary MP, Chang E, Cherepanov D, Katznelson L. Treatments, complications, and healthcare utilization associated with acromegaly: a study in two large United States databases. Pituitary 17(4), 333–341 (2014).
46.
Ogedegbe OJ, Cheema AY, Khan MA et al. A comprehensive review of four clinical practice guidelines of acromegaly. Cureus 14(9), e28722 (2022).
47.
Melmed S, Katznelson L. Treatment of acromegaly. UpToDate (2023). Available from: https://www.uptodate.com/contents/treatment-of-acromegaly
48.
Lindholm J, Riishede J, Vestergaard S, Hummer L, Faber O, Hagen C. No effect of bromocriptine in acromegaly. N. Engl. J. Med. 304(24), 1450–1454 (1981).
49.
Carmichael JD, Neary MP, Chang E, Broder MS, Cherepanov D, Ludlam WH. Patterns of pharmacotherapy changes and switches suggest unmet need in US patients with acromegaly. 2015 Annual SNO Meeting, TX, USA (2015).
50.
Albarel F, Cuny T, Graillon T, Dufour H, Brue T, Castinetti F. Preoperative medical treatment for patients with acromegaly: yes or no? J. Endocr. Soc. 6(9), bvac114 (2022).
51.
Papaioannou C, Druce M. Preoperative medical treatments and surgical approaches for acromegaly: a systematic review. Clin. Endocrinol. (Oxf). 98(1), 14–31 (2023).
52.
Varlamov EV, Fleseriu M. Acromegaly and COVID-19, lessons, and new opportunities. Pituitary 27(6), 935–944 (2024).
53.
Giustina A, Legg E, Cesana BM, Frara S, Mortini P, Fleseriu M. Results from ACROCOVID: an international survey on the care of acromegaly during the COVID-19 era. Endocrine 71(2), 273–280 (2021).
54.
Kizilgul M, Duger H, Nasiroglu NI et al. Efficacy of cabergoline add-on therapy in patients with acromegaly resistance to somatostatin analogs treatment and the review of literature. Arch. Endocrinol. Metab. 66(3), 278–285 (2022).
55.
Sandret L, Maison P, Chanson P. Place of cabergoline in acromegaly: a meta-analysis. J. Clin. Endocrinol. Metab. 96(5), 1327–1335 (2011).
56.
Marazuela M, Ramos-Leví A, Sampedro-Núñez M, Bernabeu I. Cabergoline treatment in acromegaly: pros. Endocrine 46(2), 215–219 (2014).
57.
Jallad RS, Bronstein MD. Optimizing medical therapy of acromegaly: beneficial effects of cabergoline in patients uncontrolled with long-acting release octreotide. Neuroendocrinology 90(1), 82–92 (2009).
58.
Fleseriu M, Führer-Sakel D, van der Lely AJ et al. More than a decade of real-world experience of pegvisomant for acromegaly: ACROSTUDY. Eur. J. Endocrinol. 185(4), 525–538 (2021).
59.
MacFarlane J, Korbonits M. Growth hormone receptor antagonist pegvisomant and its role in the medical therapy of growth hormone excess. Best Pract. Res. Clin. Endocrinol. Metab. 38(4), 101910 (2024).
60.
Broder MS, Chang E, Cherepanov D, Neary MP, Ludlam WH. Incidence and prevalence of acromegaly in the United States: a claims-based analysis. Endocr. Pract. 22(11), 1327–1335 (2016).
61.
Burton T, Le Nestour E, Neary M, Ludlam WH. Incidence and prevalence of acromegaly in a large US health plan database. Pituitary 19(3), 262–267 (2016).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 20 May 2025
Accepted: 26 June 2025
Published online: 8 July 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Adherence, duration and healthcare costs in a real-world population of patients with acromegaly. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0080
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Hayri Bostan, Iris C. M. Pelsma, Nienke R. Biermasz, Sex-related differences in healthcare utilization and costs among patients with pituitary adenomas, Pituitary, 10.1007/s11102-026-01638-0, 29, 1, (2026).