Dosing patterns, healthcare resource utilization and costs among acromegaly patients who consistently use lanreotide and injectable octreotide
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: In the US, lanreotide and injectable octreotide are commonly used to treat acromegaly. For most patients, the recommended injection administration regimen is every 4 weeks, or 13-times over the course of 1 year. The study aimed to quantify the proportion of patients who used a number of injections that is beyond the standard recommended regimen and to assess whether high frequency (HF) use is associated with higher healthcare resource utilization and costs. Materials & methods: IQVIA Pharmetrics Plus data between 1 January 2013 and 30 June 2023 was used to conduct a retrospective, observational study of acromegaly patients who used injectable octreotide or lanreotide for at least 2 years. The primary study outcomes were the number of injections and HF use. HF use is defined as having observed more than 13 injections over a 1-year observation period. Results: There were 420 patients with acromegaly who used injectable octreotide (n = 250) or lanreotide (n = 170) for a median of 4 years. HF use was observed in 32.4% of injectable octreotide users and 30.6% of lanreotide users. Over the course of 1 year, mean total healthcare costs were significantly higher among HF users compared with non-HF users among patients treated with injectable octreotide ($130,238 vs $85,964, p < 0.001) or lanreotide ($143,975 vs $96,518, p < 0.001). Additionally, 10% of HF users incurred $238,070–$281,167 or more. Based on the average cost per injection, patients with HF use had an additional $12,803–$13,480 in injection costs each year. Conclusion: Among those who are consistently treated, nearly a third of patients with acromegaly are HF users of lanreotide or injectable octreotide. The economic burden of HF use is high. Given the high proportion of patients who require administration beyond what is indicated on approved drug labels, further evaluation of new therapies is warranted.
Plain language summary
What is this article about?
We conducted this study to understand how often patients with acromegaly use more injections than the standard recommended dose on the US FDA approved drug labels and whether there is an association between high injection frequency, healthcare resources utilization and costs. The standard dosing regimen for lanreotide and for injectable octreotide is 1 injection every 4 weeks or 13 injections over the course of 1 year.
What were the results?
In this study we defined high frequency (HF) use as having more than 13 injections over 1 year. Nearly a third of patients who consistently use injectable octreotide or lanreotide to treat acromegaly were observed to have HF use. HF use is associated with higher all-cause total healthcare costs compared with non-HF use and 10% of HF users incurred $238,070–$281,167 or more in total healthcare costs over 1 year. HF use is also associated with higher healthcare resource utilization compared with non-HF user. For example, patients with HF use had higher rates of outpatient services, IGF-1 tests and pituitary MRIs compared with patients without HF use.
Why is this important?
HF use is higher than what has been reported in previous real-world evidence studies. An understanding of the relationship between higher-than-expected injection frequency and healthcare utilization and costs will inform healthcare decision-making. Given the high proportion of patients who require administration beyond what is indicated on approved drug labels and the increased costs associated with HF use, further evaluation of new therapies is warranted.
Acromegaly is a rare chronic condition characterized by excess growth hormone (GH) and insulin-like growth factor 1 (IGF-1) production, which leads to abnormal bone and soft tissue growth. Abnormally high GH and IGF-1 levels in patients with acromegaly is typically the results of a of a pituitary tumor [1]. Surgery is the standard first-line treatment [2]. However, not all patients are eligible for surgery and some patients do not achieve postoperative biochemical control from surgery alone. For these patients, long-term pharmacologic management may be necessary to control disease progression and symptoms. Between 45–64% of medically treated acromegaly patients use injectable octreotide or lanreotide in an effort to achieve biochemical control [3–5]. These therapies are typically administered every 4 weeks or approximately 13-times per year.
Some patients may remain on the standard dosing schedule while other patients escalate to a higher injection frequency, beyond the standard dosing schedule, due to inadequate biochemical control [6–8]. Recent evidence suggests that while high injection frequency can improve biochemical control, it may also increase side effects and introduce safety concerns. Clinical trials evaluating the efficacy and safety of high-frequency or high-dose treatment regimens found that between 50–63% of patients with acromegaly reported adverse events that were not present at baseline [9,10]. This suggests that patients who are high frequency (HF) users of lanreotide or injectable octreotide may be at greater risk of side effects. The studies did not report whether, and to what extent, HF dosing regimens influenced healthcare resource utilization and costs. The clinical and economic burden associated with HF use remains unclear, particularly in real-world settings.
The study aimed to quantify the prevalence of HF use among patients treated with lanreotide or injectable octreotide and to compare HF users to non-HF users in terms of healthcare utilization and costs. Oral octreotide was not included in this study due to the relatively low number of patients observed to have a claim for oral octreotide in administrative datasets and because the study’s definition of HF use is not applicable to a twice daily oral formulation [5,11]. It was hypothesized that patients who had more than 13 injections per year would have higher healthcare utilization and costs compared with patients who had 13 injections or fewer per year. By identifying patients who may be at higher risk for adverse events and evaluating their healthcare utilization and total healthcare costs compared with patients on standard-use or low-use regimens, this study provides valuable insights into the burden of HF use. Given the substantial clinical and economic burden associated with current treatment options, even among patients on the standard dose, newer therapeutic options may help address the challenges faced by the acromegaly patient population.
Materials & methods
In this study, IQVIA Pharmetrics Plus was used between 1 January 2013 and 30 June 2023 to conduct a retrospective, observational study of acromegaly patients who consistently used lanreotide or injectable octreotide for at least 2 years. IQVIA Pharmetrics Plus is a longitudinal, administrative dataset composed of the medical and pharmaceutical claims of individuals who are insured in the US. Adult patients (≥18 years) with at least two medical claims with acromegaly (International Classification of Diseases, 9th Revision, Clinical Modification [ICD-9-CM] diagnosis code: 253.0 and International Classification of Diseases, 10th Revision, Clinical Modification [ICD-10-CM]: diagnosis code E22.0) in any diagnosis field or at least one medical claim with an acromegaly diagnosis code in combination with one other claim for a pituitary tumor, pituitary surgery (hypophysectomy) or cranial stereotactic radiosurgery (for ICD-9 and ICD-10 codes, see Supplementary Table A1) were identified. Patients were identified as having consistently used a medical treatment if there were at least 2 years between the first and last observed claims (while continuously enrolled in a health insurance plan) for injectable octreotide or lanreotide (i.e., somatostatin receptor ligands [SRLs]).
| Patient characteristics | Lanreotide | Injectable octreotide | ||||||
|---|---|---|---|---|---|---|---|---|
| HF users | Non-HF users | All | p-value | HF users | Non-HF users | All | p-value | |
| n (%) | 52 (30.6) | 118 (69.4) | 170 (100) | 81 (32.4) | 169 (67.6) | 250 (100) | ||
| Age, years, mean (SD) [median] | 48.1 (13.6) [50] | 48.1 (11.5) [50] | 48.1 (12.2) [50] | 0.980 | 51.0 (15.7) [50] | 52.7 (13.7) [54] | 52.1 (14.4) [53] | 0.371 |
| Female, n (%) | 27 (51.9) | 45 (38.1) | 72 (42.4) | 0.094 | 44 (54.3) | 74 (43.8) | 118 (47.2) | 0.118 |
| Geographic region, n (%) | 0.125 | 0.045 | ||||||
| Midwest | 18 (34.6) | 35 (29.7) | 53 (31.2) | 22 (27.2) | 33 (19.5) | 55 (22.0) | ||
| Northeast | 12 (23.1) | 24 (20.3) | 36 (21.2) | 30 (37.0) | 42 (24.9) | 72 (28.8) | ||
| South | 8 (15.4) | 35 (29.7) | 43 (25.3) | 19 (23.5) | 52 (30.8) | 71 (28.4) | ||
| West | 14 (26.9) | 24 (20.3) | 38 (22.4) | 10 (12.3) | 42 (24.9) | 52 (20.8) | ||
| Insurance type | 0.956 | 0.698 | ||||||
| Commercial | 35 (67.3) | 79 (66.9) | 114 (67.1) | 58 (71.6) | 117 (69.2) | 175 (70.0) | ||
| Medicare | 2 (3.8) | 3 (2.5) | 5 (2.9) | 6 (7.4) | 18 (10.7) | 24 (9.6) | ||
| Other | 15 (28.8) | 36 (30.5) | 51 (30.0) | 17 (21.0) | 34 (20.1) | 51 (20.4) | ||
| Duration of injection use, years, mean [median] | – | – | 4.2 [4] | – | – | 4.6 [4] | ||
Data source: IQVIA Pharmetrics Plus® claims database, from 1 January 2013 to 30 June 2023.
HF: High frequency; SD: Standard deviation.
The period over which patients with consistent use of SRLs was used to select a 1-year observation period for each patient during which all study measures were observed.
The primary study outcomes were the number of injections and HF use during the 1-year observation period. HF use was defined as having used more than 13 injections in any 1-year window. To identify HF users, a 1-year window was started at the date of the first claim for an SRL. The number of injections were counted during the observation window. Then, the start of the 1-year window was moved forward to the next SRL claim and the number of injections was observed for the new 1-year window. This process was repeated during the period of consistent use of an SRL. Patients who had at least one window of HF use were categorized as HF users and this window was used as the 1-year observation period. For non-HF users, a claim for an injection was randomly picked to be the start of the 1-year observation period. Beginning the observation period on the first date of consistent use may have resulted in selection bias towards patients with earlier stages of acromegaly, thus, a random claim was selected to mitigate this risk. Patient characteristics and healthcare utilization and costs were estimated during the 1-year observation period.
Patient demographics (age, sex), US geographic region and insurance type were summarized.
Comorbidity burden was measured using the Charlson Comorbidity Index (CCI) and specific comorbidities of interest [12]. These comorbidities were selected because of a known association with acromegaly or acromegaly-related treatment [4,13–16]. The list of patient comorbidities included cardiomyopathy, congestive heart failure, depression, hypertension, obesity, osteoarthritis, psychoses, sleep apnea, thyroid goiter/thyroid and valvular heart disease nodules. Patient comorbidities and CCI scores were identified using ICD-10 and ICD-9 diagnosis codes (Supplementary Table A2).
| Costs measures | Lanreotide | Injectable octreotide | ||||||
|---|---|---|---|---|---|---|---|---|
| HF users | Non-HF users | All | p-value | HF users | Non-HF users | All | p-value | |
| n (%) | 52 (30.6) | 118 (69.4) | 170 (100) | 81 (32.4) | 169 (67.6) | 250 (100) | ||
| Injections, mean | 14.7 | 9.2 | 10.9 | <0.001 | 15.3 | 9.0 | 11.0 | <0.001 |
| Total healthcare costs, mean (SD) [median] | $143,975 (81,131.1) [120,083] | $96,518 (60,857.4) [80,124] | $111,035 (70,932.4) [93,924] | <0.001 | $130,238 (101,481.7) [99,980] | $85,964 (72,478.4) [66,488] | $100,309 (85,346.9) [74,069] | <0.001 |
| Total healthcare costs, 75th percentile | $148,125 | $112,767 | $126,770 | $148,169 | $108,669 | $122,909 | ||
| Total healthcare costs, 90th percentile | $281,167 | $174,985 | $210,927 | $238,070 | $174,550 | $196,365 | ||
| Total healthcare costs, range | $51,528 – $410,307 | $15,008 – $419,598 | $15,008 – $419,598 | $18,015 – $681,235 | $973 – $415,973 | $973 – $681,235 | ||
Data source: IQVIA Pharmetrics Plus® claims database, from 1 January 2013 to 30 June 2023. All costs are adjusted to 2023 US dollars.
HF: High frequency; SD: Standard deviation.
The following relevant healthcare utilization and costs measures were reported: all-cause and acromegaly-related healthcare utilization included inpatient admissions, emergency department (ED) visits, office visits, use of cabergoline therapy, use of therapies, use of laboratory and imaging tests (i.e., IGF-1, glucose tolerance and GH tests and pituitary MRI) and total healthcare costs. All-cause total healthcare costs were calculated by summing the total expenditures from the inpatient, outpatient and other services and outpatient pharmacy files. To assess how the outcome changed under an alternative definition of HF use, all-cause total healthcare costs were also measured for consistent users with >14 injections during the 1-year observation period.
To estimate the additional costs incurred by HF users, the mean cost of a single lanreotide or injectable octreotide injection was multiplied by the average number of injections beyond 13 injections. To account for potential differences cost per injection differences between HF users and non-HF users, the cost per injection was estimated separately for each group.
Dose strength was measured per 28 days for claims which had dosing information. Dosing strength categories for lanreotide were of ≤60, >60–90, >90–120 and >120 mg. Dosing strength categories for injectable octreotide were ≤10, >10–20, >20–30, >30–40 and >40 mg. These dosing strength categories were chosen based on each medication’s prescribing information that states that the injections should be administered at 4 week intervals at 60, 90 or 120 mg doses or at 10, 20, 30 and 40 mg doses depending on GH level, IGF-1 level and symptom management for lanreotide and injectable octreotide, respectively [17,18]. Additionally, prescribing information for injectable octreotide recommends that patients do not exceed 40 mg per dose [19]. Any claims that were >180 mg for lanreotide or >60 mg for injectable octreotide were considered out of range and excluded from the dosing analysis.
Descriptive statistics were conducted to examine patient characteristics, healthcare utilization and healthcare costs among acromegaly patients who consistently used lanreotide or injectable octreotide for at least 2 years. Additionally, patient characteristics and healthcare utilization and costs outcomes among HF users and non-HF users were reported using data in 1-year observation period. Means, standard deviations and relative frequencies and percentages for continuous and categorical data, respectively, were reported. All data transformations and statistical analyses were performed using SAS© version 9.4.
Results
A total of 420 patients with acromegaly who met the study’s inclusion criteria were identified (Figure 1). The cohort of 170 consistent lanreotide users (mean age: 48.1 years; median age: 50 years) were majority male (57.6%), covered by commercial health insurance (67.1%) and used lanreotide for an average of 4.2 years (Table 1). Similarly, the cohort of 250 consistent injectable octreotide users (mean age: 52.1 years; median age: 53 years) were slightly more often male (52.8%), covered by commercial health insurance (70.0%) and used injectable octreotide for average of 4.6 years.
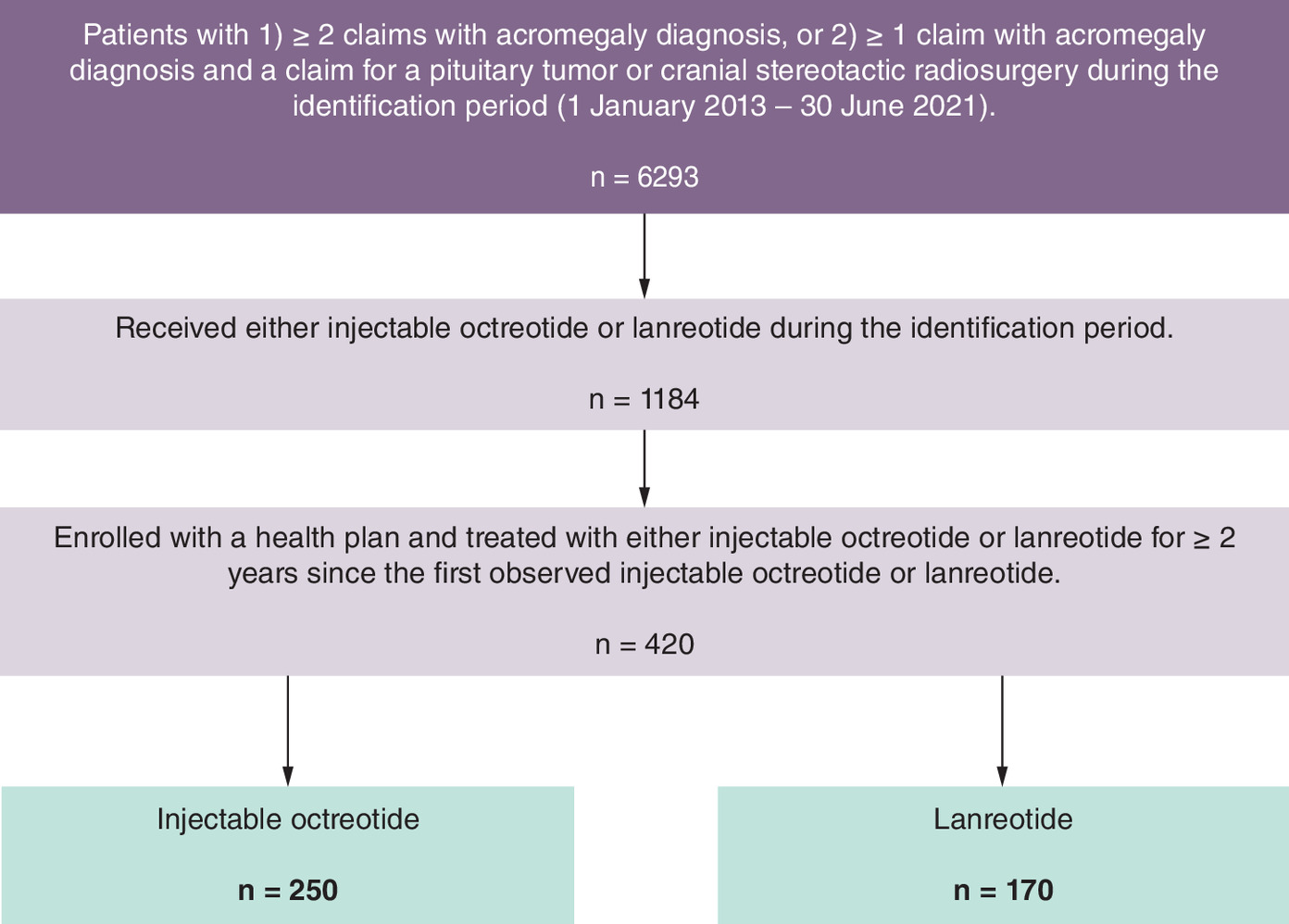
Figure 1. Patient attrition.
IQVIA Pharmetrics Plus claims database.
The distribution of the number of injections was similar for both therapies (Figure 2). There was wide variation in the number of injections among lanreotide users (range = 1–22 injections) and injectable octreotide users (1–28 injections). Nearly a third of patients exhibited HF use (Figure 2 & Table 2). Only about 7.6% of patients on either therapy used exactly 13 injections (Figure 2). Among HF users, patients prescribed lanreotide used an average of 14.7 injections and patients prescribed injectable octreotide used an average of 15.3 injections (Table 2).
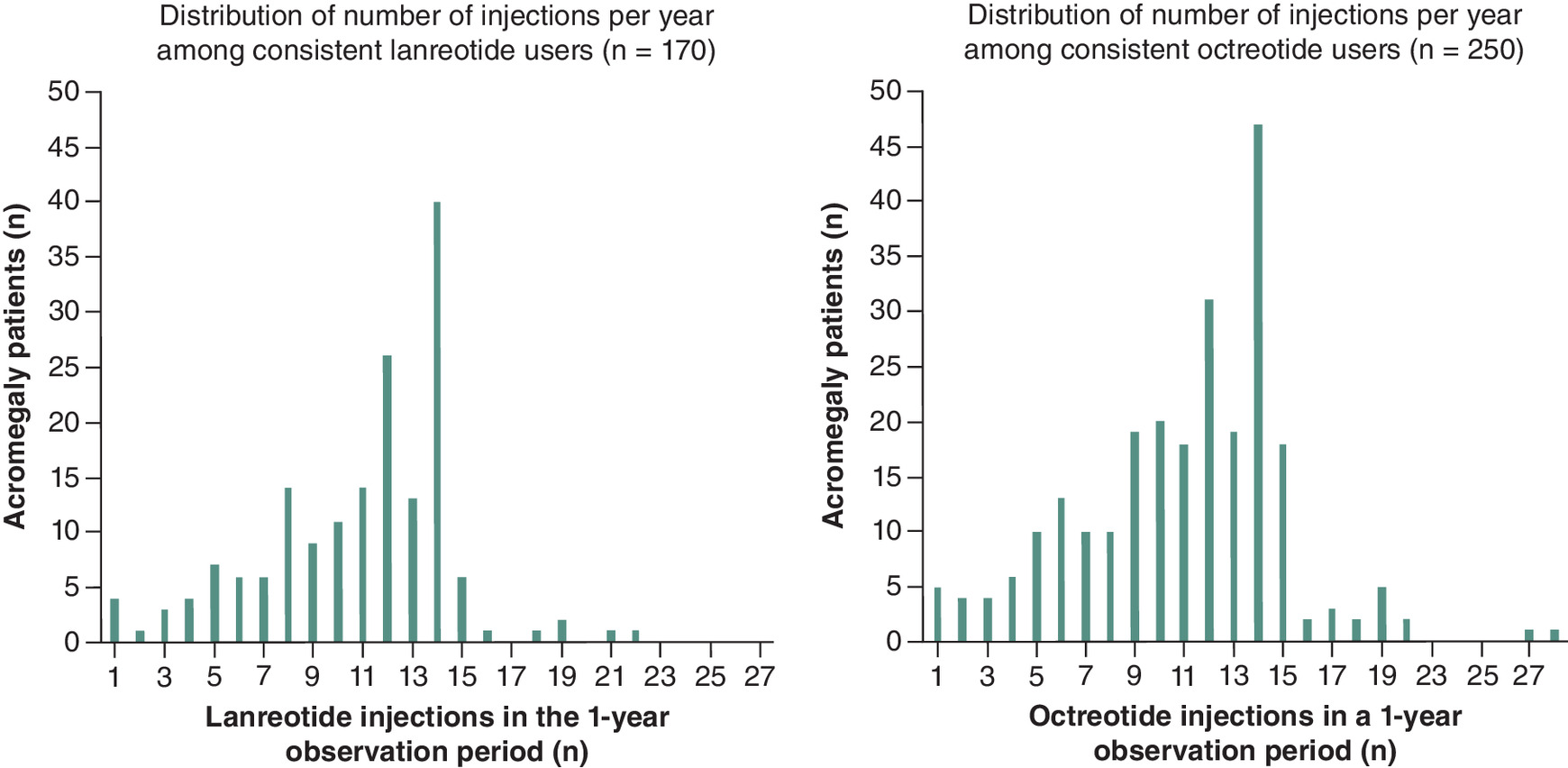
Figure 2. Distribution of the number of lanreotide and octreotide injections during the 1-year observation period.
IQVIA Pharmetrics Plus® claims database, from 1 January 2013 to 30 June 2023.
No statistically significant differences in CCI scores between HF user and non-HF users of either therapy were measured (Table 3). Similarly, there were no statistically significant differences in the proportion of patients with comorbidities between HF users and non-HF users. Among all patients who consistently used lanreotide, diagnoses of hypertension (40.6%), obesity (15.9%), sleep apnea (24.1%), osteoarthritis (12.4%), thyroid goiter/nodules (12.9%), depression (10.6%), valvular heart disease (6.5%), congestive heart failure (1.2%), cardiomyopathy (1.2%) and psychoses (0.6%) were observed during the 1-year observation period. Among all patients who consistently used injectable octreotide, diagnoses of hypertension (45.6%), obesity (23.2%), sleep apnea (14.8%), osteoarthritis (20.8%) and thyroid goiter/nodules (14.4%), depression (9.6%), valvular heart disease (7.2%), congestive heart failure (3.2%), cardiomyopathy (3.6%) and psychoses (0.0%) were observed during the 1-year observation period. There were no statistically significant differences between HF users and non-HF users in the number of comorbidities observed for either medication (Table 3). Lanreotide users had a higher proportion of patients with sleep apnea (24.1% vs 14.8%) relative to injectable octreotide users. Lanreotide users had a lower proportions of patients with osteoarthritis (12.4% vs 20.8%) and obesity (15.9% vs 23.2%) relative to injectable octreotide users.
| Comorbidity measures | Lanreotide | Injectable octreotide | ||||||
|---|---|---|---|---|---|---|---|---|
| HF users | Non-HF users | All | p-value | HF users | Non-HF users | All | p-value | |
| n (%) | 52 (30.6) | 118 (69.4) | 170 (100) | 81 (32.4) | 169 (67.6) | 250 (100) | ||
| CCI, continuous, mean (SD) [median] | 1.1 (1.6) [0] | 1.2 (1.8) [0] | 1.1 (1.8) [0] | 0.803 | 1.1 (1.7) [0] | 1.3 (2.1) [0] | 1.3 (2.0) [0] | 0.369 |
| CCI, categorical, n (%) | 0.314 | 0.765 | ||||||
| 0 | 27 (51.9) | 68 (57.6) | 95 (55.9) | 43 (53.1) | 86 (50.9) | 129 (51.6) | ||
| 1 | 13 (25.0) | 18 (15.3) | 31 (18.2) | 18 (22.2) | 34 (20.1) | 52 (20.8) | ||
| 2+ | 12 (23.1) | 32 (27.1) | 44 (25.9) | 20 (24.7) | 49 (29.0) | 69 (27.6) | ||
| Hypertension, n (%) | 21 (40.4) | 48 (40.7) | 69 (40.6) | 0.971 | 35 (43.2) | 79 (46.7) | 114 (45.6) | 0.599 |
| Obesity, n (%) | 9 (17.3) | 18 (15.3) | 27 (15.9) | 0.736 | 17 (21.0) | 41 (24.3) | 58 (23.2) | 0.566 |
| Sleep apnea, n (%) | 13 (25.0) | 28 (23.7) | 41 (24.1) | 0.858 | 9 (11.1) | 28 (16.6) | 37 (14.8) | 0.255 |
| Osteoarthritis, n (%) | 10 (19.2) | 11 (9.3) | 21 (12.4) | 0.070 | 17 (21.0) | 35 (20.7) | 52 (20.8) | 0.960 |
| Thyroid goiter/ thyroid nodules, n (%) | 9 (17.3) | 13 (11.0) | 22 (12.9) | 0.260 | 13 (16.0) | 23 (13.6) | 36 (14.4) | 0.607 |
| Depression, n (%) | 5 (9.6) | 13 (11.0) | 18 (10.6) | 0.784 | 7 (8.6) | 17 (10.1) | 24 (9.6) | 0.722 |
| Valvular heart disease, n (%) | 3 (5.8) | 8 (6.8) | 11 (6.5) | 1.000 | 6 (7.4) | 12 (7.1) | 18 (7.2) | 0.930 |
| Congestive heart failure, n (%) | 0 (0.0) | 2 (1.7) | 2 (1.2) | 1.000 | 0 (0.0) | 8 (4.7) | 8 (3.2) | 0.057 |
| Cardiomyopathy, n (%) | 0 (0.0) | 2 (1.7) | 2 (1.2) | 1.000 | 2 (2.5) | 7 (4.1) | 9 (3.6) | 0.722 |
| Psychoses, n (%) | 0 (0.0) | 1 (0.8) | 1 (0.6) | 1.000 | 0 (0.0) | 0 (0.0) | 0 (0.0) | n/a |
Data source: IQVIA Pharmetrics Plus® claims database, from 1 January 2013 to 30 June 2023.
CCI: Charlson Comorbidity Index; HF: High frequency; SD: Standard deviation.
Only 5.3% of lanreotide users had at least one inpatient hospitalization (Table 4). The proportion of lanreotide users with at least one ED service utilization was higher among HF users compared with non-HF users (26.9% vs 13.6%, p < 0.05). About 12.4% of injectable octreotide users had at least one inpatient hospitalization. Among injectable octreotide users, the mean number of outpatient services was higher among HF users compared with non-HF users (15.7 services vs 11.7 services, p < 0.05). Among lanreotide users, a statistically significant difference in the proportion of patients who had at least one IGF-1 test (94.2% vs 77.1%, p = 0.007) or pituitary MRI (69.1% vs 48.8%, p < 0.001) between HF users and non-HF users was observed. Among injectable octreotide users, a statistically significant difference in the proportion of patients who had at least one IGF-1 test (88.9% vs 78.1%, p = 0.039) or pituitary MRI procedure (49.4% vs 34.3%, p = 0.022) between HF users and non-HF users was observed. Overall, cabergoline therapy was used by 24.1% of lanreotide users and 15.2% of injectable octreotide users (Table 4). Among lanreotide users, the proportion of HF users who used cabergoline was lower relative to non-HF users (21.2% vs 25.4%, p = 0.549). Among injectable octreotide users, the proportion of HF users who used cabergoline was higher relative to non-HF users (21.0% vs 12.4%, p = 0.078).
| Utilization measures | Lanreotide | Injectable octreotide | ||||||
|---|---|---|---|---|---|---|---|---|
| HF users | Non-HF users | All | p-value | HF users | Non-HF users | All | p-value | |
| n (%) | 52 (30.6) | 118 (69.4) | 170 (100) | 81 (32.4) | 169 (67.6) | 250 (100) | ||
| Had an inpatient hospitalization, n (%) | 1 (1.9) | 8 (6.8) | 9 (5.3) | 0.278 | 12 (14.8) | 19 (11.2) | 31 (12.4) | 0.423 |
| Had an ED service, n (%) | 14 (26.9) | 16 (13.6) | 30 (17.6) | 0.035 | 15 (18.5) | 28 (16.6) | 43 (17.2) | 0.702 |
| Office visits, mean (SD) [median] | 17.1 (12.9) [15] | 13.6 (11.9) [10] | 14.7 (12.2) [11] | 0.090 | 18.1 (11.2) [18] | 16.1 (15.4) [13] | 16.8 (14.2) [15] | 0.247 |
| Other outpatient services (non-ED/non-office), mean (SD) [median] | 13.4 (12.8) [10] | 9.8 (13.4) [7] | 10.9 (13.3) [8] | 0.107 | 15.7 (12.4) [15] | 11.7 (14.3) [7] | 13.0 (13.8) [10] | 0.032 |
| IGF-1 test, n (%) | 49 (94.2) | 91 (77.1) | 140 (82.4) | 0.007 | 72 (88.9) | 132 (78.1) | 204 (81.6) | 0.039 |
| Glucose tolerance test, n (%) | 3 (5.8) | 9 (7.6) | 12 (7.1) | 0.758 | 12 (14.8) | 13 (7.7) | 25 (10.0) | 0.079 |
| Growth hormone test, n (%) | 27 (51.9) | 44 (37.3) | 71 (41.8) | 0.075 | 40 (49.4) | 56 (33.1) | 96 (38.4) | 0.013 |
| Pituitary MRI, n (%) | 36 (69.2) | 47 (39.8) | 83 (48.8) | <0.001 | 40 (49.4) | 58 (34.3) | 98 (39.2) | 0.022 |
| Cabergoline use, n (%) | 11 (21.1) | 30 (25.4) | 41 (24.1) | 0.549 | 17 (21.0) | 21 (12.4) | 38 (15.2) | 0.078 |
Data source: IQVIA Pharmetrics Plus® claims database, from 1 January 2013 to 30 June 2023.
ED: Emergency department; HF: High frequency; IGF-1: Insulin-like growth factor 1; MRI: Magnetic resonance imaging; SD: Standard deviation.
Among consistent users of lanreotide, there were no statistically significant differences between HF users and non-HF users for patients with at least one dose of ≤60 mg (69.2% vs 69.5%, p = 0.973), >60–90 mg (17.3% vs 14.4%, p = 0.628), or >90–120 mg (23.1% vs 16.9%, p = 0.346) (Table 5). There were no consistent lanreotide users with an observed dosing strength of >120 mg. Among consistent users of injectable octreotide, there were no statistically significant differences between HF users and non-HF users for patients with at least one dose of ≤10 mg (32.1% vs 24.9%, p = 0.228), >10–20 mg (48.1% vs 41.4%, p = 0.315), >20–30 mg (33.3% vs 34.9%, p = 0.806), >30–40 mg (8.6% vs 8.9%, p = 0.951). There were 8 (3.2%) consistent injectable octreotide users who had at least one dose over 40 mg and there was a significant different in the number of HF users compared with non-HF users (7.4% vs 1.2%, p = 0.009).
| HF users | Non-HF users | All | p-value | |
|---|---|---|---|---|
| Lanreotide users, n (%) | 52 (30.6) | 118 (69.4) | 170 (100.0) | |
| Any claim with dose ≤60 mg, n (%) | 36 (69.2) | 82 (69.5) | 118 (69.4) | 0.973 |
| Any claim with dose >60–90 mg, n (%) | 9 (17.3) | 17 (14.4) | 26 (15.3) | 0.628 |
| Any claim with dose >90–120 mg, n (%) | 12 (23.1) | 20 (16.9) | 32 (18.8) | 0.346 |
| Any claim with dose >120 mg, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | – |
| Injectable octreotide users, n (%) | 81 (32.4) | 169 (67.6) | 250 (100.0) | |
| Any claim with dose ≤10 mg, n (%) | 26 (32.1) | 42 (24.9) | 68 (27.2) | 0.228 |
| Any claim with dose >10–20 mg, n (%) | 39 (48.1) | 70 (41.4) | 109 (43.6) | 0.315 |
| Any claim with dose >20–30 mg, n (%) | 27 (33.3) | 59 (34.9) | 86 (34.4) | 0.806 |
| Any claim with dose >30–40 mg, n (%) | 7 (8.6) | 15 (8.9) | 22 (8.8) | 0.951 |
| Any claim with dose >40 mg, n (%) | 6 (7.4) | 2 (1.2) | 8 (3.2) | 0.009 |
Data source: IQVIA Pharmetrics Plus® claims database, from 1 January 2013 to 30 June 2023.
HF: High-frequency.
Among all consistent users, the average cost per injection was $7582 per lanreotide injection and $5861 per injectable octreotide injection (Table 6). Among HF users, the average cost per injection was $7528 per lanreotide injection and $5966 per injectable octreotide injection. Among HF users, there was an estimated $12,803 in additional spending on lanreotide and $13,772 in additional spending on injectable octreotide, relative to patients on the standard dosing regimen of 13 injections per year. Mean total healthcare costs were significantly higher for HF users compared with non-HF users among lanreotide users ($143,975 vs $96,518, p < 0.001) and among injectable octreotide users ($130,238 vs $85,964, p < 0.001) (Table 2). Among HF users with >14 injections during the observation period, mean total healthcare costs were $158,253 for HF lanreotide users and $146,738 for HF injectable octreotide users (Supplementary Table A3).
| HF use measures | Lanreotide | Injectable octreotide |
|---|---|---|
| Injections (n) | 7307 | 10,580 |
| Cost per injection, mean [median] | $7582 [7013] | $5861 [5074] |
| Cost per injection among HF users, mean [median] | $7528 [7180] | $5966 [4731] |
| Cost per injection, among non-HF users, mean [median] | $7624 [6951] | $5782 [5313] |
| Estimated annual costs per patient with 13 injections per year (every 4 weeks) among HF users | $97,864 | $77,558 |
| Consistent users (≥2 years of use), n | 170 | 250 |
| Observed duration of medication use (y), mean [median] | 4.2 [4] | 4.6 [4] |
| HF users: ever received >13 injections during any 1-year period, n (%) | 52 (30.6) | 81 (32.4) |
| Injections per year among HF users, mean [median] | 14.7 [14] | 15.3 [14] |
| Average annual costs per HF user | $110,662 | $91,280 |
| Average annual HF use costs per HF user | $12,798 | $13,722 |
Data source: IQVIA Pharmetrics Plus® claims database, from 1 January 2013 to 30 June 2023. All costs are adjusted to 2023 US dollars.
HF: High-frequency.
Discussion
Nearly a third of acromegaly patients consistently treated with lanreotide or injectable octreotide are HF users, defined as receiving more than 13 injections per year. Some HF users also use high doses of medical therapies and differences in dosing strength among HF users and non-HF users is minimal. HF users incur higher total healthcare costs compared with non-HF users over 1 year, highlighting the substantial economic burden associated with HF use.
Previous research on the burden of acromegaly has documented high economic burden, adverse events and side effects [9,10,20,21]. Furthermore, patients have reported concerns about pain, travel burden and how often acromegaly therapy interferes with daily life [22–24]. Given that HF users may have been more likely to have struggled to achieve biochemical control compared with non-HF users, it follows that HF users may experience these challenges to a greater degree. The current study’s results, along with the other studies that have documented the burden of lanreotide and injectable octreotide use, raise important questions about whether new treatment options could provide more effective and tolerable disease management.
A significant proportion of this study’s cohort exhibited HF use. Notably, HF use in this study was more common than what has been reported elsewhere. Fleseriu and colleagues observed few patients on a high-frequency injection regimen [5]. This study’s longer treatment requirement may have contributed to a higher observation of HF use relative to other studies. Fleseriu and colleagues required at least 3 months of medical treatment while this study design required at least 2 years between the first and last observed injection. However, that same treatment pattern study found that 22.1% of injectable octreotide users were administered more than the maximum approved dosing strength [5]. Over a relatively shorter study period, high-dose regimens may be more easily observed compared with high-frequency regimens because only one administration incident is required. With the exclusion of patients who had at least one >40 mg dose of injectable octreotide, there were no significant differences between HF users and non-HF users in the number of patients that had at least one dose administered at a particular dosing strength. This finding suggests that HF users are not consistently prescribed lower dosing strengths relative to non-HF users to compensate for increased frequency and result in similar amount of the medication being administered over a 28-day period.
In addition to HF use, HF users used cabergoline therapy and a wide range of dosing strengths of lanreotide and injectable octreotide. Cabergoline is recommended as an add-on therapy for patients with acromegaly who are partial responders to SRLs or who have treatment-resistant acromegaly [25,26]. Studies report that between 30–48% of patients achieved normalized IGF-1 levels following the addition of cabergoline add-on therapy [27–30]. The data used in this study does not contain any information on whether patients with HF use, high-dose use, or cabergoline add-on therapy achieved normal IGF-1 levels. Further investigation is warranted to understand whether patients with acromegaly who are on HF, high-dose and/or poly-pharmaceutical regimens are adequately controlled and whether those patients may be better served by new treatment options.
Healthcare utilization of inpatients hospitalizations, ED services and office visits was similar to utilization rates reported in previous research [3,5,31]. This study included measures of acromegaly-related testing which, the authors’ knowledge, has not been measured in a cohort of consistent medication users. This study measured high proportions of consistent users with an IGF-1 laboratory test (77.1–94.2%) compared with the rate of acromegaly-related laboratory testing reported in studies of the general acromegaly patient population (31.7–53.7%) [3]. Consensus guidelines recommend that patients with acromegaly are assessed for biochemical control every 6–12 months [7,32]. This study provides evidence that patients who were being treated for acromegaly were more likely to receive guideline-based care compared with cohorts of patients who were diagnosed with acromegaly but did not receive pharmacologic therapy. Patients who are being treated for acromegaly, particularly those who require additional injections beyond the standard dose, may interact with the healthcare system more frequently, providing more opportunities for disease monitoring.
This study measured higher mean total healthcare costs ($85,964–$143,975) compared with other studies on the economic burden on acromegaly ($35,281–$50,144; inflation adjusted 2023 USD) [3,20,31,33]. The relatively higher costs estimate is attributable to differences in study design. All patients included in the current study were required to have consistent medication use for at least 2 years. Due to design differences, the cost burden of acromegaly management among patients who persist with treatment may be underestimated if previous studies are used to project costs. For example, one study reported mean total healthcare costs for a population in which only 30.8% received pharmacologic treatment for acromegaly [3]. Another study reported total healthcare costs in a population of medically treated acromegaly patients; however, this study included other medical therapies (pegvisomant, bromocriptine, cabergoline) and did not report whether medical therapy was used consistently [31]. A third study did not report any information on whether its cohort was medically treated [20]. None of these studies examined total healthcare costs in a cohort that is comparable to consistent users of SRLs. Among patients with >14 injections, mean total healthcare costs were about $18,000 higher compared with patients with >13 injections. The difference in total healthcare costs was greater than the estimated cost of a single additional injection; therefore, patients may have additional costs that are not related to the cost and administration of an injection alone. Future research may assess healthcare cost drivers among HF users that are not directly related to therapy costs.
This study has several limitations. First, there is no validated, US-based algorithm to identify patients diagnosed with acromegaly in claims data. However, it is reasonable to assume that the majority of this study’s cohort was correctly identified; patients were required to have at least two acromegaly-related claims and to consistently use acromegaly therapies.
Second, the data elements included in claims data are limited in determining whether non-adherence to the US approved drug label resulted in higher or lower quality care as defined by well-established frameworks [34,35]. Clinical guidelines consider HF dosing appropriate for certain patient groups while acknowledging that not all patients will be well-served by this treatment regimen [6,8]. The proportion of patients for which HF use is appropriate is unanswered by the current study because outcomes such as safety, tolerability, effectiveness or any patient reported outcomes could not be directly measured.
Third, consistency of medication dosing is variable in claims data and dosing strength outcome may be difficult to intercept. Clinical consensus statements state that a higher injection frequency or a higher dosing strength, relative to what is recommended for most patients on the US FDA approved prescription label, may be considered for patients who are not well-controlled on the standard regimen [6]. A real-word evidence study by Fleseriu and colleagues found that 22.1% of patients using injectable octreotide were administered more than the maximum standard dosing strength while only 1.7% of patients using patients using lanreotide were administered more than the standard recommended dosing strength [5]. Similarly, in this study, 7.4% of HF injectable octreotide users and 0.0% of HF injectable octreotide users were observed to have dosing strengths above the maximum recommended dose. The current study found that there are some patients who are both HF users and use dosing strengths that were in the upper ranges of recommended values. Whether these patients were able to achieve biochemical control and the extent to which high dosing contributed to adverse events using those regimens is unknown within the context of the current study. However, in one randomized controlled trial that investigated the efficacy and safety of HF and high-dose treatment regimens, 63.3% of patients experienced an adverse event that was not present on the lower frequency and lower dose regimens [9].
Fourth, although whether patients had acromegaly-related laboratory testing was measured, claims data does not include laboratory values. Therefore, IGF-1 and GH levels were not measured in this study and whether patients are well-controlled on their current therapy regimen is unknown. HF users who achieved biochemical control may be effectively managed, while those who remain uncontrolled may be unnecessarily exposed to the risk of adverse events and high financial burden. Furthermore, without laboratory results and other important factors (e.g. patient preference and symptom burden), this study cannot determine whether HF use was appropriate.
Finally, healthcare claims data were used to define the cohort and to measure all the healthcare utilization and cost outcomes. The interpretation of the results is limited by what is available in administrative billing records and subject to coding inaccuracies, misclassification and missing data.
Conclusion
Patients with acromegaly who are HF users have higher total healthcare costs and higher utilization relative to non-HF users. Future research should investigate the clinical consequences of HF use, particularly the rate of adverse events, and the economic burden among consistent users. Given the challenges associated with current treatment regimens, further evaluation of new therapies is warranted. Optimizing treatment strategies to balance efficacy, safety, cost and patient preference remains a key priority.
Summary points
•
Acromegaly is a rare, chronic condition that results in excess IGF-1 and growth hormone in patients with pituitary tumors. Patients with acromegaly experience increased morbidity and mortality relative to patients without acromegaly.
•
Lanreotide and injectable octreotide are commonly used to treat patients with acromegaly. The standard administration regimen is every 4 weeks, or 13 injections per year.
•
Some patients with acromegaly may not achieve biochemical control on a standard regimen of lanreotide or injectable octreotide and may be prescribed a higher frequency dose.
•
In clinical intervention trials, high-frequency (HF) regimens have been associated with both increased biochemical control and higher rates adverse events relative to standard regimens.
•
This retrospective study used data from IQVIA Pharmetrics Plus, a health insurance claims database, to observe healthcare resource utilization and costs among patients with acromegaly who consistently used lanreotide or injectable octreotide for at least 2 years between 1 January 2013 and 30 June 2023.
•
Nearly a third of patients who were consistent users of lanreotide or injectable octreotide exhibited HF use.
•
The average cost per injection was $7582 per lanreotide injection and $5861 per injectable octreotide injection.
•
Mean total healthcare costs were significantly higher for HF users compared with non-HF users among lanreotide users ($143,975 vs $96,518, p < 0.001) and among injectable octreotide users ($130,238 vs $85,964, p < 0.001).
•
HF users used cabergoline therapy and a wide range of dosing strengths of lanreotide and injectable octreotide, underscoring the intensity of medical therapy even among patients already on HF regimens.
•
This study cannot determine whether HF use is appropriate because IGF-1 and growth hormone laboratory test results and other important patient and clinical factors are unavailable in health insurance claims.
Author contributions
TP Quock, SK Rattana and IE Paulson: Acquisition of data; design of the work; interpretation of data; revising the work for important intellectual content; final approval. E Chang, AK Das, A Speller, MH Tarbox and MS Broder: Design of the work; analysis of data; interpretation of data; drafting and revising the work for important intellectual content; final approval.
Financial disclosure
Funding for this study and publication-related fees was received from Crinetics Pharmaceuticals.
Competing interests disclosure
TP Quock, SK Rattana, IE Paulson are employees of and hold stock in Crinetics Pharmaceuticals, Inc. at the time of this study. At the time this research was conducted, E Chang, AK Das, A Speller, MH Tarbox and MS Broder were employees of Partnership for Health Analytic Research, LLC (now ADVI Health), which was paid by Crinetics to perform the research described in this manuscript. PHAR also discloses financial relationships with the following commercial entities outside of the submitted work: Abbvie, Akcea, Amgen, Astellas, AstraZeneca, Delfi Diagnostics, Dompe, Exact Sciences Corporation, Genentech, Gilead, GRAIL, Ionis, Janssen, Nobelpharma, Novartis, Pfizer, Recordati, Regeneron and Sanofi US Services. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 27.33 KB
References
Papers of special note have been highlighted as: • of interest
1.
Fleseriu M, Langlois F, Lim DST, Varlamov EV, Melmed S. Acromegaly: pathogenesis, diagnosis, and management. Lancet Diabetes Endocrinol. 10(11), 804–826 (2022).
2.
Ershadinia N, Tritos NA. Diagnosis and treatment of acromegaly: an update. Mayo Clin. Proc. 97(2), 333–346 (2022).
3.
Broder MS, Neary MP, Chang E, Cherepanov D, Katznelson L. Treatments, complications, and healthcare utilization associated with acromegaly: a study in two large United States databases. Pituitary 17(4), 333–341 (2014).
• This real-world evidence study assesses the burden of acromegaly by reporting the additional healthcare resource utilization and costs associated with complications of the disease.
4.
Burton T, Le Nestour E, Bancroft T, Neary M. Real-world comorbidities and treatment patterns of patients with acromegaly in two large US health plan databases. Pituitary 16(3), 354–362 (2013).
• This real-world evidence study found lower than expected rates of acromegaly treatment, considering that remission rates from surgery alone remain low.
5.
Fleseriu M, Barkan A, Brue T et al. Treatment patterns, adherence, persistence, and health care resource utilization in acromegaly: a real-world analysis. J. Endocr. Soc. 7(10), bvad104 (2023).
• This study used administrative claims data from MarketScan (2010–2022) and found that patient demographic characteristics are associated with treatment adherence, persistence and dosing patterns.
6.
Giustina A, Barkhoudarian G, Beckers A et al. Multidisciplinary management of acromegaly: a consensus. Rev. Endocr. Metab. Disord. 21(4), 667–678 (2020).
7.
Giustina A, Biermasz N, Casanueva FF et al. Consensus on criteria for acromegaly diagnosis and remission. Pituitary 27(1), 7–22 (2024).
8.
Melmed S, Bronstein MD, Chanson P et al. A consensus statement on acromegaly therapeutic outcomes. Nat. Rev. Endocrinol. 14(9), 552–561 (2018).
9.
Giustina A, Mazziotti G, Cannavò S et al. High-dose and high-frequency lanreotide autogel in acromegaly: a randomized, multicenter study. J. Clin. Endocrinol. Metab. 102(7), 2454–2464 (2017).
10.
Giustina A, Bonadonna S, Bugari G et al. High-dose intramuscular octreotide in patients with acromegaly inadequately controlled on conventional somatostatin analogue therapy: a randomised controlled trial. Eur. J. Endocrinol. 161(2), 331–338 (2009).
• Reports the effectiveness of a randomized intervention for high-dosing strength or high-dosing frequency, and found that high dose octreotide was an effective and safe strategy for disease management.
11.
Uygur MM, Villanova M, Frara S, Giustina A. Clinical pharmacology of oral octreotide capsules for the treatment of acromegaly. Touch Rev. Endocrinol. 20(1), 37–42 (2024).
12.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40(5), 373–383 (1987).
13.
Abreu A, Tovar AP, Castellanos R et al. Challenges in the diagnosis and management of acromegaly: a focus on comorbidities. Pituitary 19(4), 448–457 (2016).
14.
Whittington MD, Munoz KA, Whalen JD, Ribeiro-Oliveira A, Campbell JD. Economic and clinical burden of comorbidities among patients with acromegaly. Growth Horm. IGF Res. 59, 101389 (2021).
15.
Vargas-Ortega G, Romero-Gameros CA, Rendón-Macias ME et al. Risk factors associated with thyroid nodular disease in acromegalic patients: a case-cohort study in a tertiary center. Growth Horm. IGF Res. 60–61, 101431 (2021).
16.
Tiemensma J, Biermasz NR, van der Mast RC et al. Increased psychopathology and maladaptive personality traits, but normal cognitive functioning, in patients after long-term cure of acromegaly. J. Clin. Endocrinol. Metab. 95(12), E392–E402 (2010).
17.
FDA. “Sandostatin LAR Depot, drug label” (2024). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/021008Orig1s047lbl.pdf
18.
FDA. “Somatuline Depot (lanreotide) drug label” (2014). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/022074s011lbl.pdf
19.
Novartis Pharmaceuticals Corporation. Sandostatin LAR® Depot (octreotide acetate for injectable suspension) [prescribing information] (2019). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/021008s043lbl.pdf
20.
Ribeiro-Oliveira A, Brook RA, Munoz KA et al. Burden of acromegaly in the United States: increased health services utilization, location of care, and costs of care. J. Med. Econ 24(1), 432–439 (2021).
21.
Placzek H, Xu Y, Mu Y, Begelman SM, Fisher M. Clinical and economic burden of commercially insured patients with acromegaly in the United States: a retrospective analysis. J. Manag. Care Spec. Pharm. 21(12), 1106–1112 (2015).
22.
Fleseriu M, Molitch M, Dreval A et al. Disease and treatment-related burden in patients with acromegaly who are biochemically controlled on injectable somatostatin receptor ligands. Front. Endocrinol. 12, 627711 (2021).
• Reports high disease and treatment burden among patients who are biochemically controlled with the use of injections. Patients experienced gastrointestinal symptoms, pain at the injection site and interference with daily life.
23.
Geer EB, Sisco J, Adelman DT et al. Patient reported outcome data from acromegaly patients treated with injectable somatostatin receptor ligands (SRLs) in routine clinical practice. BMC Endocr. Disord. 20(1), 117 (2020).
• This study used a one-time online survey of patients with acromegaly who were either on a stable dose of octreotide or lanreotide for at least 12-months. Most patients reported experiencing constant symptoms (e.g., tiredness, carpal tunnel syndrome, snoring and excessive sweating), while fewer patients reported experiencing symptoms only at the end of the injection cycle.
24.
Strasburger CJ, Karavitaki N, Störmann S et al. Patient-reported outcomes of parenteral somatostatin analogue injections in 195 patients with acromegaly. Eur. J. Endocrinol. 174(3), 355–362 (2016).
25.
Kyriakakis N, Seejore K, Hanafy A, Murray RD. Management of persistent acromegaly following primary therapy: the current landscape in the UK. Endocrinol. Diabetes Metab. 3(3), e00158 (2020).
26.
Ogedegbe OJ, Cheema AY, Khan MA et al. A comprehensive review of four clinical practice guidelines of acromegaly. Cureus 14(9), e28722 (2022).
27.
Mattar P, Alves Martins MR, Abucham J. Short- and long-term efficacy of combined cabergoline and octreotide treatment in controlling IGF-I levels in acromegaly. Neuroendocrinology 92(2), 120–127 (2010).
28.
Kizilgul M, Duger H, Nasiroglu NI et al. Efficacy of cabergoline add-on therapy in patients with acromegaly resistance to somatostatin analogs treatment and the review of literature. Arch. Endocrinol. Metab. 66(3), 278–285 (2022).
29.
Vilar L, Azevedo MF, Naves LA et al. Role of the addition of cabergoline to the management of acromegalic patients resistant to longterm treatment with octreotide LAR. Pituitary 14(2), 148–156 (2010).
30.
Suda K, Inoshita N, Iguchi G et al. Efficacy of combined octreotide and cabergoline treatment in patients with acromegaly: a retrospective clinical study and review of the literature. Endocr. J. 60(4), 507–515 (2013).
31.
Chuang C-C, Bhurke S, Chen S-Y, Dinet J, Brulais S, Gabriel S. Treatment patterns and economic burden in patients treated for acromegaly in the USA. Drugs - Real World Outcomes 2(3), 299–309 (2015).
32.
Lim EM, Pullan P. Biochemical assessment and long-term monitoring in patients with acromegaly: statement from a joint consensus conference of the growth hormone research society and the pituitary society. Clin. Biochem. Rev. 26(2), 41–43 (2005).
33.
U.S. Bureau of Labor Statistics. “CPI inflation calculator - consumer price index for all urban consumers (CPI-U)” (2024). Available from: https://www.bls.gov/data/inflation_calculator.htm
34.
Donabedian A. The quality of care: how can it be assessed? JAMA 260(12), 1743–1748 (1988).
35.
Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the quality chasm: a new health system for the 21st century. National Academies Press (US), DC, USA (2001).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 10 May 2025
Accepted: 9 July 2025
Published online: 17 July 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Dosing patterns, healthcare resource utilization and costs among acromegaly patients who consistently use lanreotide and injectable octreotide. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0070
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Hayri Bostan, Iris C. M. Pelsma, Nienke R. Biermasz, Sex-related differences in healthcare utilization and costs among patients with pituitary adenomas, Pituitary, 10.1007/s11102-026-01638-0, 29, 1, (2026).