Comparative safety of direct oral anticoagulants and low-molecular-weight heparin in patients with venous thromboembolism and cancer in Europe
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study aimed to compare the safety and effectiveness of direct oral anticoagulants (DOACs) with low-molecular-weight heparin (LMWH) in patients with venous thromboembolism (VTE) and active cancer in a real-world setting in Sweden, Norway, Finland, the UK and Germany. Materials & methods: This observational cohort study used datasets from Sweden, Norway, Finland (National Patient and Prescription Registers) the UK (Clinical Practice Research Datalink and Hospital Episode Statistics) and Germany (AOK Plus and GWQ) from 2013 to 2020. We identified treatment-naive adult patients with cancer-related VTE treated with a DOAC or LMWH. We employed inverse probability of treatment weighting for each DOAC-LMWH comparison and assessed recurrent VTE and bleeding risk (overall and by site: gastrointestinal [GI], intracranial hemorrhage [ICH] or other) within 6 months of treatment initiation. Fine–Gray models were fitted to estimate adjusted hazard ratios and country level estimates were meta-analyzed. Results: After inverse probability of treatment weighting, 30,002 and 2892 patients were included in the LMWH-apixaban comparison, and 29,976 and 4321 in the LMWH-rivaroxaban comparison, respectively. Recurrent VTE could not be assessed comparatively because of low numbers. At 6 months, apixaban was associated with a lower risk of overall and other (HR: 0.67 [95% CI: 0.53,0.86]; 0.64 [0.41,0.998]) bleeding compared with LMWH, with similar risks for GI and ICH bleeding (0.89 [0.61,1.29]; 0.67 [0.31,1.44], respectively). Rivaroxaban had a similar risk of overall, GI, and other bleeding (0.98 [0.83, 1.15]; 0.86 [0.47,1.58]; 0.89 [0.74,1.08]) compared with LMWH, but a lower risk of ICH (0.32 [0.13, 0.82]). Conclusion: These findings suggest that apixaban may offer a safer bleeding profile than LMWH for patients with cancer-associated VTE, particularly in reducing overall and other types of bleeding. Rivaroxaban also appears to be a viable alternative to LMWH, with a notably lower risk of ICH. These results provide valuable real-world insights in an area where evidence remains very limited and support the role of DOACs as a safe alternative to LMWH in patients with VTE and cancer.
Plain language summary
What was the aim of this research?
To compare the safety of blood thinners among patients with cancer and blood clots in Sweden, Norway, Finland, the UK and Germany.
How was the research carried out?
This study used data from Sweden, Finland, Norway, the UK and Germany between 2013 and 2020 from adults with cancer and blood clots who were prescribed either a direct oral anticoagulant (DOAC) or low-molecular-weight heparin (LMWH). Weighting methods were used to balance patient characteristics. We then compared the risk of bleeding within 6 months after starting treatment, combining results from different countries.
What were the results?
The study compared 30,002 patients taking LMWH with 2892 patients taking apixaban and also compared 29,976 patients taking LMWH with 4321 patients taking rivaroxaban. Patients taking apixaban showed an improved safety profile compared with LMWH for overall bleeding, whereas the overall bleeding risk was similar for rivaroxaban compared with LMWH.
What do the results of the study mean?
In patients with VTE and cancer, apixaban was associated with a lower risk of overall bleeding compared with LMWHs, whereas rivaroxaban had a similar risk of overall bleeding. This information can be used by doctors to help them choose the safest blood thinner for patients with cancer who have blood clots, potentially reducing the risk of dangerous bleeding complications.
Venous thromboembolism (VTE) represents a major cause of mortality and morbidity among patients with cancer [1], who are approximately five to nine-times more likely to develop VTE than people without cancer [2,3]. VTE is the second leading cause of death in this patient group [4–6]. The risk of VTE varies by cancer site, with the highest rates observed in cancers of the pancreas, noncolorectal abdominal sites, kidney, ovary, lung and stomach, as well as hematologic malignancies like myeloma and lymphoma [7]. Managing cancer patients with VTE is quite challenging due the dual risk of recurrent VTE in this patient population combined with the high risk of bleeding associated with anticoagulation [8].
Low-molecular-weight heparin (LMWH) has been the standard of care for treating VTE in patients with cancer for many years, following the results of the CLOT trial, which demonstrated its superior efficacy over vitamin K antagonists (VKAs) [9]. Direct oral anticoagulants (DOACs), including dabigatran, apixaban, rivaroxaban and edoxaban, have emerged as standard therapies for the treatment for VTE and prevention of recurrent VTE in the general population. DOACs offer a more convenient oral administration compared with the injectable LMWH [10,11]. Clinical trials have shown that DOACs are at least noninferior to LMWH in preventing recurrent VTE (rVTE) in patients with cancer, with comparable risks of major bleeding (MB). For example, the Caravaggio trial demonstrated that apixaban was noninferior to LMWH (dalteparin) for rVTE, with similar MB events between both cohorts [12], and the SELECT-D trial showed that rivaroxaban had a reduced risk of rVTE compared with LMWH (dalteparin), and comparable MB risk [13].
International guidelines recommend DOACs as an alternative to LMWH for most cancer patients, except those at high risk of bleeding, particularly those with unresected gastrointestinal (GI) and genitourinary malignancies [14–18]. While clinical trials have established the comparative efficacy and safety of DOACs versus LMWH, real-world evidence assessing these therapies in European clinical practice for cancer-associated VTE remains limited. This study aimed to compare the effectiveness and safety of DOACs with LMWH in patients with VTE and active cancer in a real-world setting in Sweden, Norway, Finland, the UK and Germany (NCT04618913; VICTORIE study).
Materials & methods
Data sources
The study included data from two nationwide registries in Sweden, Finland, and Norway: the National Patient Registry (NPR) and the National Prescription Database (NPD) [19]. The NPRs includes information on all hospital episodes (inpatient, outpatient and emergency visits), admission and discharge dates and hospital procedures. Diagnoses are recorded using International Classification of Diseases, 10th Revision (ICD-10) codes. Procedures are coded using the Nordic Classification of Surgical Procedures (NCSP). The NPD covers all prescriptions dispensed from nationwide pharmacies. Each medication is coded using the Anatomical Therapeutic Chemical (ATC) system. Each record also includes information on the date, strength and quantity of dispensations. These data sets are linked using unique patient identifiers assigned to each resident in each of the countries.
In the UK, the Clinical Practice Research Datalink (CPRD) Aurum linked to Hospital Episode Statistics (HES) was used. Diagnoses in CPRD are recorded by Systematized Nomenclature of Medicine, Read Coded Clinical Terms version 3, or local EMIS codes, each internally mapped to an individual ‘medcode’. Drugs are recorded using prescription codes (recorded per the Dictionary of Medicines and Devices codes), diagnoses using ICD-10 codes, and procedures using Operating Procedure Codes Supplement (OPCS).
In Germany, two Social Health Insurance funds databases were used (Allgemeine Ortskrankenkasse [AOK] Plus and Gesellschaft für Wirtschaftlichkeit und Qualität bei Krankenkassen [GWQ]), covering approximately 8.5 million people combined. Diagnoses are recorded using ICD-10, prescriptions using ATC, and procedures using Einheitlicher Bewertungsmaßstab (EBM) or Operationen-und Prozedurenschlüssel (OPS) codes. Deaths in all the datasets are also recorded as dates and immediate and underlying causes of death, recorded using ICD-10 codes.
All patient data were anonymized prior to data delivery. The study was approved by the Swedish Ethical Review Authority (ref. no. 2020-04155), the Regional Committees for Medical and Health Research Ethics in Norway (ref. no. 167093), University of Eastern Finland Committee on Research Ethics (ref. no. THL/4321/14.05.00/2021), and CPRD’s expert review and central advisory committee (ref. no. 20_000163). German claims data were analyzed under the formal agreement and legal basis of §75, Tenth Book of the Social Code. Accordingly, no informed consent or ethical approval from an institutional review board was required.
Study period
The study period was from 1 January 2013 until 31 March 2020 in Sweden, Norway, Germany and the UK and 31 December 2019 in Finland (for Sweden, Norway, Germany and the UK, the study period ended on 31 March 2020, to prevent overlap with the COVID-19 pandemic period. For Finland, the study period ended on 31 December 2019, since this was the latest available data at the time the research was conducted). Patients were included in the study if their first DOAC, VKA or LMWH dispensation (‘index date’) occurred between 1 January 2013 until 3 months before the end of the study period (‘cohort enrollment period’). A VTE diagnosis was required to occur up to 30 days prior to index date. The pre-index period included all available time before the index date. The follow-up extended from the day after index date until the earliest of 6 months after the index date (to align with clinical trials for VTE and cancer [12,13,20,21]), patient death, outcome of interest, index treatment discontinuation (defined later), emigration (Sweden and Finland only due to variable availability), inferior vena cava (IVC) filter insertion, pregnancy start, or 31 March 2020 (to prevent overlap with the start of the COVID pandemic in Europe). Patients were classified into treatment groups according to their index DOAC, VKA or LMWH dispensation.
Study population
The following inclusion criteria were applied:
•
A diagnosis (inpatient or outpatient in any position) of deep vein thrombosis (DVT) or pulmonary embolism (PE) identified <30 days before and including the cohort enrollment period. The ICD-10 codes and medcodes used to identify DVT and PE can be found in Supplementary Material 1. We assigned the hospital discharge date as the date of VTE if identified in the hospital setting
•
A diagnosis of cancer (ICD-10 codes) in the primary position (any setting of care) that occurred in the 6 months before the VTE diagnosis and up to the index date, or 2 or more diagnoses codes in secondary position or one cancer diagnoses in the secondary position plus a cancer related procedure in the same hospital admission or outpatient visit.
•
A prescription of LMWH, VKA, apixaban, rivaroxaban, dabigatran or edoxaban identified within 30 days after a VTE via an ATC or prescription code in the cohort enrollment period.
•
Age ≥ 18 years at VTE index date.
•
Linkage to secondary care data (UK only).
The following exclusion criteria were applied:
•
A VTE diagnosis that occurred <30 days before the identified VTE diagnosis using all available data.
•
An atrial fibrillation, mechanical heart valve replacement, mitral stenosis or IVC filter insertion that occurred before index date using all available data.
•
An anticoagulant that occurred before index date using all available data, unless administered prophylactically (duration for ≤42 days and either within 7 days of a knee/hip replacement or a hospital admission for ≥3 days with a primary position diagnosis considered ‘medically ill’ ref).
•
Pregnant at the time of index date.
•
Record of immigration <365 days prior to VTE diagnosis (Sweden and Finland only due to variable availability).
•
Receipt of more than one anticoagulant on index date.
•
<1 day of follow-up.
Outcomes
The primary safety outcome of interest was bleeding, which was defined as an inpatient hospitalization with at least one overnight stay and a primary or secondary ICD-10 diagnosis of bleeding. This definition was validated previously and the positive predictive value was estimated in the range of 89–99% [22]. Bleeding was categorized overall and by site (GI bleeding, intracranial bleeding [ICH] or other bleeding) according to the administrative claims definition and categories provided by Halvorsen et al. [23], which has previously been used in other real-world studies [24]. rVTE was defined as any primary inpatient VTE code occurring after initiation of the index treatment, excluding events that occurred within 7 days of the discharge date of the VTE diagnosis (to exclude hospital follow-up attendances).
Study measures
Baseline demographic characteristics, including age in years and sex, were identified at index date. Type of VTE (DVT or PE) was also described using ICD-10 codes. The year of anticoagulant initiation (index year; 2013–2019) was also described. Clinical characteristics were identified using diagnoses or prescription codes from each of the datasets. Clinical characteristics included:
•
Prior bleeding (identified in the pre-index period).
•
Comorbidities
○
Identified any time in the pre-index period: congestive heart failure, peripheral vascular disease, cerebrovascular disease, chronic obstructive pulmonary disease and/or asthma, rheumatic disease, diabetes without chronic complications, diabetes with chronic complications, renal disease, hypertension, anemia obesity, varicose veins, ischemic heart disease, coagulation defects, dyspepsia and hyperlipemia.
○
Identified in the 3-month pre-index period: pneumonia, concomitant medications (platelet aggregation inhibitors and nonsteroidal anti-inflammatory drugs).
•
Diagnostic setting (inpatient or outpatient).
•
Cancer type (including metastatic solid tumor, solid tumor and hematological malignancy).
•
•
Cancer site (leukemia, multiple myeloma, bladder, brain, gynecologic, lung, lymphoma, urinary tract, prostate, digestive organ, upper GI, lower GI, pancreatic, breast and melanoma).
All analyses were conducted on-treatment only. To estimate on-treatment time for the DOACs, the duration of supply of each medication was calculated using the number of packages, the quantity contained in each packet, and dosage information from each DOAC label. For LMWH, on-treatment time was estimated using information on the number of syringes in the pack dispensed and assuming the dosing plan of one syringe a day. LMWH was only considered as an index treatment if the dispensed duration was ≥14 days.
Patients were identified as having discontinued their treatment if there was no new dispensation of the same medication within 60 days of the end of the days of supply of the last dispensation.
Inverse probability of treatment weighting
Potential confounding was controlled for using inverse probability of treatment weighting (IPTW) in each of the respective country datasets. This method has previously been detailed by Austin et al. [29]; the method controls for confounding by assigning patients a propensity score (PS) based on their probability of treatment selection, conditional on their baseline characteristics. Patients are then weighted by the inverse of the PS, which creates a synthetic sample in which treatment is independent of baseline covariates. This method is commonly used in comparative safety studies [30] and has benefits over PS-matching methods because patient numbers are retained. Baseline demographics, comorbidities with a prevalence ≥1%, concomitant medications, bleeding history and cause, and setting of the incident VTE were included in the PS model. Following IPTW, some cohorts were not balanced because of extreme weights. Weight trimming was applied to handle extreme weights, and variables that remained unbalanced following trimming were adjusted for in the Fine–Gray models. If any weight exceeded 10 or standardized differences of baseline characteristics after IPTW exceeded 0.10, we trimmed the PS at the first and 99th percentiles for each group separately, and if balance was not achieved, further trimming was done at the fifth and 95th percentiles. For comparisons involving LMWH versus apixaban and LMWH versus rivaroxaban in Sweden, Norway and the UK, trimming was specifically applied at the fifth and 95th percentiles.
Statistical analyses
Patient demographics and clinical characteristics were summarized using counts and percentages. Patients with missing age and gender were not provided by any of the data vendors; otherwise missing data were described in the baseline tables. Patients were censored when they reached the end of study follow-up. Event rates of bleeding outcomes and death were reported per 100 person-years (PY). Analyses of time-to-bleeding were conducted by deriving the cumulative incidence function from applying Fine–Gray models using the subdistribution hazard function. Use of the Fine–Gray model allowed for death to be considered as a competing risk. Separate outcome-specific Fine–Gray models were performed for the hazards of overall bleeding, ICH, GI bleeding and other bleeding. Analyses were conducted at the country level in the IPTW matched cohorts, and then frequentist meta-analysis was performed across four countries (five datasets). Baseline characteristics and other noncomparative data were summarized using sample-size weighted pooling to generate means. Random- and fixed-effects models were implemented in the meta-analyses, but only the random-effects models are presented, as they assume between-country heterogeneity and account for this variation through wider effect size confidence intervals [31].
Results
Description of selected population
Across the five countries and before IPTW 34,687 LMWH users, 3176 VKA users, 3045 apixaban users, 4537 rivaroxaban users, 145 dabigatran users and 580 edoxaban users were identified. VKA use declined substantially over the study period; approximately 30% of patients in each country were prescribed VKA in 2013, declining to less than 5% by 2019. Use of DOACs appeared to increase over time across all countries, whereas use of LMWH was consistent over the study period. After IPTW, the weighted sample sizes for the comparative analyses and meta-analyses were 30,002 and 2892 in the LMWH-apixaban weighted comparison, respectively, and 29,976 and 4321 in the LMWH-rivaroxaban weighted comparison, respectively (Figure 1). Finland was excluded because of a limited sample size, preventing adequate balance after IPTW. The edoxaban and dabigatran groups were also too small to allow analyses and hence were excluded from further analyses. VKA was originally considered as a potential comparator group for the DOACs; however, because of the low number of patients taking VKA in later years, it became a nonrelevant comparator. rVTE was underpowered for comparative analyses; power calculations are presented in Supplementary Material 3.
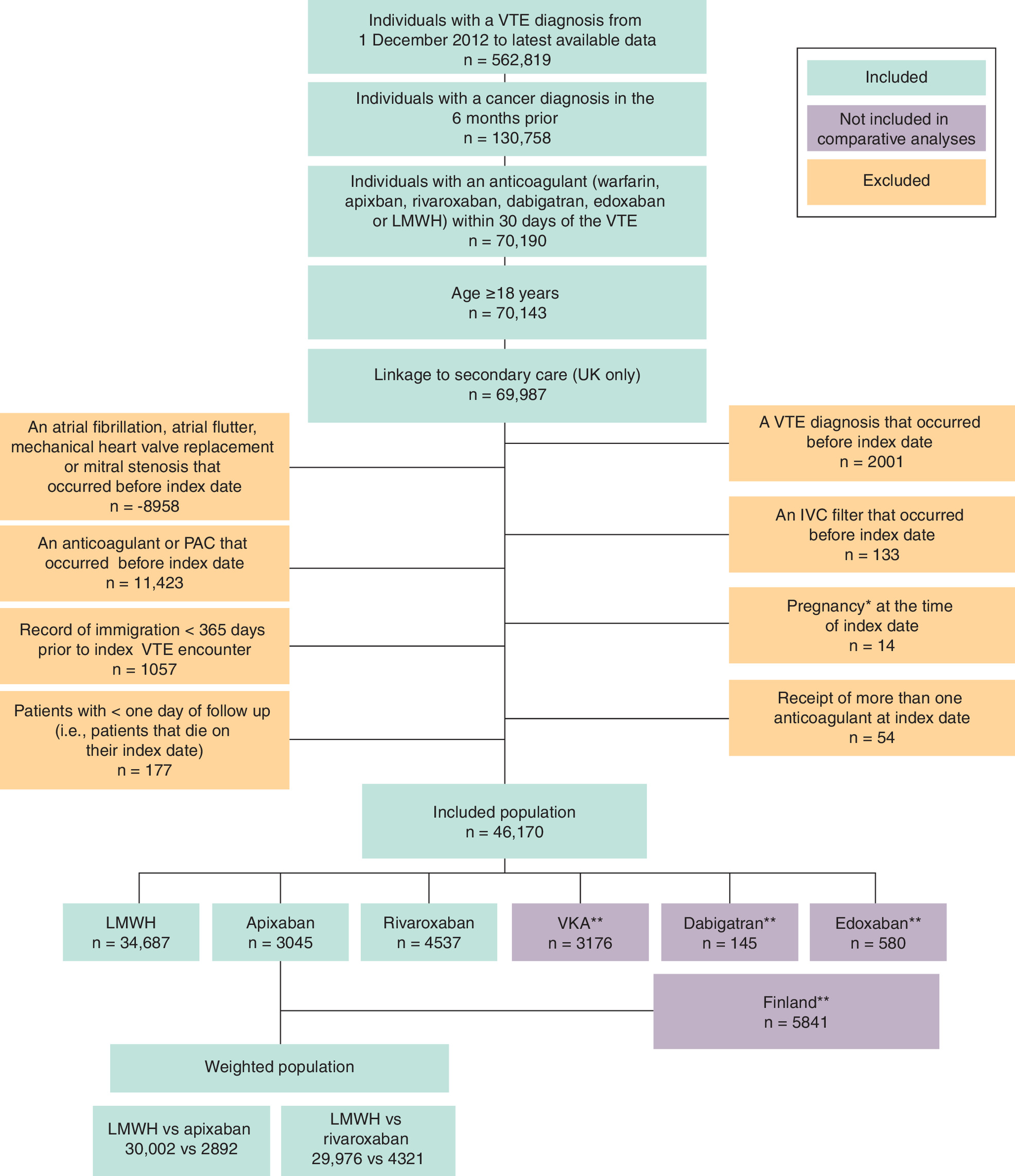
Figure 1. Flow diagram for patient selection.
*Pregnancy periods were estimated using International Classification of Diseases, 10th Revision and procedure codes for pregnancy end dates for pregnancy deliveries, cessations and preterm, and then patients were deemed to be pregnant in the 42, 13 and 36 weeks before end dates for each, respectively.
**It should be noted that dabigatran-treated patients, edoxaban-treated patients and patients from Finland were removed from further analyses because limited sample size prevented adequate balance after IPTW. VKA was not included in further analyses because of a decline in use over the study period.
DOAC: Direct oral anticoagulant; IPTW: Inverse probability of treatment weighting; IVC: Inferior vena cava; LMWH: Low-molecular-weight heparin; PAC: Parenteral anticoagulant; VKA: Vitamin K antagonist; VTE: Venous thromboembolism.
Description of the unweighted cohorts
Prior to IPTW, many differences were observed in the cohorts (Table 1). Mean age at initiation of index therapy ranged from 62.9 to 69.7 years across the countries, whereas for DOAC it ranged from 66.5 to 75.3 years. In addition, across all countries, the proportion of patients with high- or very high-risk cancer ranged from 46.1 to 55.4% for LMWH and from 26.6 to 42.8% for DOACs. Digestive cancer site ranged from 28.7 to 35.9% for LMWH across the countries and from 10.4 to 25.0% for DOACs. Mean CCI score appeared highest in patients from the UK and Germany (mean [SD]: 4.9 [2.3] and 6.2 [2.8]) when compared with the other countries (Supplementary Material 4).
| Characteristic | Sweden | Norway | Finland | UK | Germany (AOK) | Germany (GWQ) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| LMWH (n = 12,066) | Apixaban (n = 663) | Rivaroxaban (n = 779) | LMWH (n = 4751) | Apixaban (n = 562) | Rivaroxaban (n = 356) | LMWH (n = 4675) | Apixaban (n = 163) | Rivaroxaban (n = 252) | LMWH (n = 8388) | Apixaban (n = 635) | Rivaroxaban (n = 1056) | LMWH (n = 3192) | Apixaban (n = 461) | Rivaroxaban (n = 1225) | LMWH (n = 1615) | Apixaban (n = 561) | Rivaroxaban (n = 869) | |
| Age at index VTE (years) | ||||||||||||||||||
| Mean (SD) | 68.1 (12.2) | 72.3 (11.3) | 71.4 (11.1) | 67.4 (12.2) | 68.6 (11.8) | 69.6 (11.3) | 66.9 (11.5) | 70.4 (11.1) | 68.6 (11.5) | 66.8 (11.9) | 72.1 (12.3) | 71.0 (12.7) | 69.7 (13.2) | 75.3 (11.7) | 72.8 (11.8) | 62.9 (11.9) | 68.0 (12.0) | 66.5 (12.5) |
| Sex, n (%) | ||||||||||||||||||
| Female | 6479 (53.7) | 294 (44.3) | 316 (40.6) | 2334 (49.1) | 222 (39.5) | 146 (41.0) | 2540 (54.3) | 78 (47.9) | 127 (50.4) | 4615 (55.0) | 314 (49.4) | 516 (48.9) | 1752 (54.9) | 222 (48.2) | 623 (50.9) | 814 (50.4) | 257 (45.8) | 390 (44.9) |
| Index VTE type | ||||||||||||||||||
| DVT | 5267 (43.7) | 240 (36.2) | 328 (42.1) | 1346(28.3) | 189 (33.6) | 141(39.6) | 2685 (57.4) | 94 (57.7) | 121 (48.0) | 4885 (58.2) | 384 (60.5) | 541 (51.2) | 2194 (68.7) | 234 (50.8) | 696 (56.8) | 1013 (62.7) | 271 (48.3) | 434 (49.9) |
| PE | 6799 (56.3) | 423 (63.8) | 451 (57.9) | 3405 (71.7) | 373 (66.4) | 215 (60.4) | 1990 (42.6) | 69 (42.3) | 131 (52.0) | 3503 (41.8) | 251 (39.5) | 515 (48.8) | 616 (19.3) | 128 (27.8) | 313 (25.6) | 319 (19.8) | 171 (30.5) | 319 (19.8) |
| Index year, n (%) | ||||||||||||||||||
| 2013 | 1758 (14.6) | 0 (0) | 27 (3.5) | 659 (13.9) | 0 (0) | 40 (11.2) | 619 (13.2) | 0 | 11 (4.4) | 1230 (14.7) | 0 | 28 (2.7) | 501 (15.7) | 0 (0.0) | 177 (14.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| 2014 | 1751 (14.5) | <5 | 88 (11.3) | 706 (14.9) | <5 | 56 (15.7) | 672 (14.4) | 0 | 16 (6.3) | 1257 (15.0) | 0 | 90 (8.5) | 519 (16.3) | 8 (1.7) | 213 (17.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| 2015 | 1742 (14.4) | ‡ | 154(19.8) | 713 (15.0) | ‡ | 64 (18.0) | 663 (14.2) | <5 | 25 (9.9) | 1168 (13.9) | 14 (2.2) | 151 (14.3) | 476 (14.9) | 39 (8.5) | 210 (17.1) | 301 (18.6) | 39 (7.0) | 147 (16.9) |
| 2016 | 1752 (14.5) | 125 (18.9) | 131 (16.8) | 669 (14.1) | 99 (17.6) | 63 (17.7) | 763 (16.3) | ‡ | 45 (17.9) | 1229 (14.7) | 79 (12.4) | 236 (22.3) | 439 (13.8) | 68 (14.8) | 184 (15.0) | 337 (20.9) | 78 (13.9) | 200 (23.0) |
| 2017 | 1807 (15.0) | 135 (20.4) | 120 (15.4) | 668 (14.1) | 153 (27.2) | 44 (12.4) | 699 (15.0) | 26 (16.0) | 59 (23.4) | 1349 (16.1) | 156 (24.6) | 197 (18.7) | 427 (13.4) | 87 (18.9) | 140 (11.4) | 351 (21.7) | 117 (20.9) | 151 (17.4) |
| 2018 | 1637 (13.6) | 173 (26.1) | 129 (16.6) | 698 (14.7) | 124 (22.1) | 36 (10.1) | 748 (16.0) | 67 (41.1) | 53 (21.0) | 1171 (14.0) | 175 (27.6) | 172 (16.3) | 423 (13.3) | 108 (23.4) | 148 (12.1) | 308 (19.1) | 135 (24.1) | 188 (21.6) |
| 2019 | 1619 (13.4) | 166 (25.0) | 130 (16.7) | 638 (13.4) | 146 (26.0) | 53 (14.9) | 511 (10.9) | 47 (28.8) | 43 (17.1) | 984 (11.7) | 211 (33.2) | 182 (17.2) | 407 (12.8) | 151 (32.8) | 153 (12.5) | 318 (19.7) | 192 (34.2) | 183 (21.1) |
| Prior bleeding, n (%) | 1161 (9.6) | 53 (8.0) | 62 (8.0) | 594 (12.5) | 77 (13.7) | 44 (12.4) | 322 (6.9) | 19 (11.7) | 18 (7.1) | 1085 (12.9) | 94 (14.8) | 150 (14.2) | 736 (23.1) | 111 (24.1) | 246 (20.1) | 271 (16.8) | 87 (15.5) | 107 (12.3) |
| CCI, n (%) | ||||||||||||||||||
| Mean (SD) | 4.7 (2.1) | 3.5 (1.9) | 3.4 (1.9) | 4.8 (2.1) | 3.8 (2.0) | 3.4 (1.9) | 3.9 (2.1) | 3.0 (1.6) | 2.8 (1.4) | 5.6 (2.2) | 5.0 (2.4) | 4.9 (2.3) | 6.2 (2.8) | 6.1 (2.8) | 5.5 (2.7) | 5.6 (2.6) | 5.3 (2.7) | 5.1 (2.5) |
| Specific comorbidities, n (%) | ||||||||||||||||||
| Congestive heart failure | 553 (4.6) | 56 (8.4) | 56 (7.2) | 164 (3.5) | 23 (4.1) | 24 (6.7) | 172 (3.7) | 12 (7.4) | 10 (4.0) | 639 (7.6) | 87 (13.7) | 104 (9.8) | 801 (25.1) | 186 (40.4) | 382 (31.2) | 219 (13.6) | 109 (19.4) | 174 (20.0) |
| Peripheral vascular disease | 523 (4.3) | 29 (4.4) | 43 (5.5) | 270 (5.7) | 44 (7.8) | 28 (7.9) | 179 (3.8) | 11 (6.7) | 8 (3.2) | 25 (7.6) | 16 (6.8) | 33 (9.1) | 554 (17.4) | 95 (20.6) | 229 (18.7) | 224 (13.9) | 105 (18.7) | 118 (13.6) |
| Cerebrovascular disease | 862 (7.1) | 59 (8.9) | 77 (9.9) | 337 (7.1) | 47 (8.4) | 27 (7.6) | 366 (7.8) | 16 (9.8) | 22 (8.7) | 663 (7.9) | 88 (13.9) | 130 (12.3) | 523 (16.4) | 98 (21.3) | 247 (20.2) | 201 (12.4) | 93 (16.6) | 140 (16.1) |
| COPD and/or asthma | 1431 (11.9) | 93 (14.0) | 104 (13.4) | 571 (12.0) | 83 (14.8) | 52 (14.6) | 576 (12.3) | 27 (16.6) | 37 (14.7) | 2380 (28.4) | 235 (37.0) | 341 (32.3) | 828 (25.9) | 148 (32.1) | 354 (28.9) | 425 (26.3) | 183 (32.6) | 286 (32.9) |
| Rheumatic disease | 541 (4.5) | 55 (8.3) | 53 (6.8) | 217 (4.6) | 33 (5.9) | 26 (7.3) | 201 (4.3) | 13 (8.0) | 12 (4.8) | 1082 (12.9) | 110 (17.3) | 157 (14.9) | 253 (7.9) | 51 (11.1) | 113 (9.2) | 117 (7.2) | 48 (8.6) | 82 (9.4) |
| Diabetes without chronic complication | 1198 (9.9) | 62 (9.4) | 71 (9.1) | 297 (6.3) | 32 (5.7) | 19 (5.3) | 370 (7.9) | 13 (8.0) | 21 (8.3) | 833 (9.9) | 76 (12.0) | 98 (9.3) | 486 (15.2) | 72 (15.6) | 188 (15.3) | 176 (10.9) | 72 (12.8) | 88 (10.1) |
| Diabetes with chronic complication | 411 (3.4) | 25 (3.8) | 32 (4.1) | 154 (3.2) | 20 (3.6) | 10 (2.8) | 204 (4.4) | 12 (7.4) | 8 (3.2) | 550 (6.6) | 68 (10.7) | 92 (8.7) | 591 (18.5) | 99 (21.5) | 220 (18.0) | 150 (9.3) | 63 (11.2) | 78 (9.0) |
| Renal disease | 677 (5.6) | 39 (5.9) | 40 (5.1) | 500 (10.5) | 71 (12.6) | 38 (10.7) | 184 (3.9) | 10 (6.1) | 11 (4.4) | 102 (31.2) | 90 (38.0) | 116 (31.9) | 1071 (33.6) | 226 (49.0) | 475 (38.8) | 357 (22.1) | 177 (31.6) | 232 (26.7) |
| Hypertension | 7350 (60.9) | 435 (65.6) | 500 (64.2) | 2611 (55.0) | 313 (55.7) | 193 (54.2) | 3113 (66.6) | 121 (74.2) | 174 (69.0) | 5288 (63.0) | 463 (72.9) | 723 (68.5) | 2459 (77.0) | 400 (86.8) | 997 (81.4) | 944 (58.5) | 385 (68.6) | 558 (64.2) |
| Anemia | 2360 (19.6) | 113 (17.0) | 101 (13.0) | 784 (16.5) | 92 (16.4) | 43 (12.1) | 404 (8.6) | 16 (9.8) | 14 (5.6) | 2277 (27.1) | 219 (34.5) | 276 (26.1) | 934 (29.3) | 124 (26.9) | 274 (22.4) | 347 (21.5) | 112 (20.0) | 140 (16.1) |
| Obesity | 392 (3.2) | 22 (3.3) | 34 (4.4) | 118 (2.5) | 12 (2.1) | 9 (2.5) | 142 (3.0) | 8 (4.9) | 9 (3.6) | 80 (24.5) | 90 (38.0) | 119 (32.7) | 992 (31.1) | 162 (35.1) | 389 (31.8) | 373 (23.1) | 142 (25.3) | 209 (45.1) |
| Varicose veins | 327 (2.7) | 25 (3.8) | 22 (2.8) | 154 (3.2) | 30 (5.3) | 13 (3.7) | 150 (3.2) | 8 (4.9) | 11 (4.4) | 51 (15.6) | 60 (25.3) | 76 (20.9) | 865 (27.1) | 133 (28.9) | 334 (27.3) | 344 (21.3) | 121 (21.6) | 208 (23.9) |
| Ischemic heart disease/coronary artery disease | 1,026 (8.5) | 75 (11.3) | 105 (13.5) | 468 (9.9) | 74 (13.2) | 33 (9.3) | 424 (9.1) | 20 (12.3) | 34 (13.5) | 69 (21.1) | 67 (28.3) | 63 (17.3) | 773 (24.2) | 149 (32.3) | 360 (29.4) | 201 (12.4) | 98 (17.5) | 146 (16.8) |
| Coagulation defects | 321 (2.7) | 22 (3.3) | 24 (3.1) | 222 (4.7) | 23 (4.1) | 16 (4.5) | 84 (1.8) | <5 | <5 | 19 (5.8) | 12 (5.1) | 18 (4.9) | 464 (14.5) | 45 (9.8) | 139 (11.3) | 215 (13.3) | 58 (10.3) | 81 (9.3) |
| Dyspepsia | 542 (4.5) | 32 (4.8) | 30 (3.9) | 279 (5.9) | 31 (5.5) | 23 (6.5) | 368 (7.9) | 17 (10.4) | 29 (11.5) | 80 (24.5) | 56 (23.6) | 110 (30.2) | 584 (18.3) | 85 (18.4) | 214 (17.5) | 324 (20.1) | 119 (21.2) | 151 (17.4) |
| Hyperlipemia | 960 (8.0) | 59 (8.9) | 85 (10.9) | 70 (1.5) | 6 (1.1) | <5 | 135 (2.9) | 9 (5.5) | 5 (2.0) | 35 (10.7) | 27 (11.4) | 36 (9.9) | 1065 (33.4) | 174 (37.7) | 409 (33.4) | 365 (22.6) | 158 (28.2) | 226 (26.0) |
| Pneumonia 3 months before index date | 909 (7.5) | 66 (10.0) | 61 (7.8) | 623 (13.1) | 62 (11.0) | 31 (8.7) | 472 (10.1) | 18 (11.0) | 17 (6.7) | 976 (11.6) | 115 (18.1) | 148 (14.0) | 451 (14.1) | 86 (18.7) | 206 (16.8) | 137 (8.5) | 86 (15.3) | 128 (14.7) |
| Concomitant treatment, n (%) | ||||||||||||||||||
| Platelet aggregation inhibitors 3 months before index date | 1554 (12.9) | 134 (20.2) | 156 (20.0) | 681 (14.3) | 87 (15.5) | 66 (18.5) | 133 (2.8) | 9 (5.5) | 14 (5.6) | 296 (3.5) | 33 (5.2) | 58 (5.5) | 227 (7.1) | 46 (10.0) | 100 (8.2) | 69 (4.3) | 37 (6.6) | 48 (5.5) |
| NSAIDs 3 months before index date | 1372 (11.4) | 60 (9.0) | 76 (9.8) | 517 (10.9) | 59 (10.5) | 40 (11.2) | 779 (16.7) | 25 (15.3) | 42 (16.7) | 1252 (14.9) | 86 (13.5) | 161 (15.2) | 579 (18.1) | 79 (17.1) | 206 (16.8) | 310 (19.2) | 100 (17.8) | 165 (19.0) |
| Diagnostic setting, n (%) | ||||||||||||||||||
| Inpatient | 7759 (64.3) | 396 (59.7) | 444 (57.0) | 4039 (85.0) | 440 (78.3) | 256 (71.9) | 3140 (67.2) | 97 (59.5) | 134 (53.2) | 5271 (62.8) | 452 (71.2) | 593 (56.2) | 1425 (44.6) | 237 (51.4) | 573 (46.8) | 667 (41.3) | 270 (48.1) | 334 (38.4) |
| Outpatient | 4307 (35.7) | 267 (40.3) | 335 (43.0) | 712 (15.0) | 122 (21.7) | 100 (28.1) | 1408 (30.1) | 55 (33.7) | 109 (43.3) | 130 (1.5) | 11 (1.7) | 16 (1.5) | 1767 (55.4) | 224 (48.6) | 652 (53.2) | 948 (58.7) | 291 (51.9) | 535 (61.6) |
| Cancer type | ||||||||||||||||||
| Metastatic solid tumor | 6766 (56.1) | 148 (22.3) | 157 (20.2) | 2830 (59.6) | 180 (32.0) | 82 (23.0) | 1736 (37.1) | 13 (8.0) | 23 (9.1) | 5419 (64.6) | 218 (34.3) | 419 (39.7) | 1687 (52.9) | 156 (33.8) | 366 (29.9) | 913 (56.5) | 203 (36.2) | 308 (35.4) |
| Solid tumors | 11027 (91.4) | 503 (75.9) | 587 (75.4) | 4260 (89.7) | 467 (83.1) | 302 (84.8) | 4202 (89.9) | 139 (85.3) | 226 (89.7) | 7918 (94.4) | 543 (85.5) | 948 (89.8) | 2936 (92.0) | 402 (87.2) | 1110 (90.6) | 1466 (90.8) | 508 (90.6) | 787 (90.6) |
| Hematological malignancy | 1004 (8.3) | 160 (24.1) | 190 (24.4) | 475 (10.0) | 94 (16.7) | 54 (15.2) | 446 (9.5) | 24 (14.7) | ‡ | 405 (4.8) | 86 (13.5) | 101 (9.6) | 256 (8.0) | 59 (12.8) | 115 (9.4) | 149 (9.2) | 53 (9.4) | 82 (9.4) |
| Cancer risk type | ||||||||||||||||||
| Very high or high risk for VTE | 5563 (46.1) | 198 (29.8) | 249 (32.0) | 2339 (49.2) | 189 (33.6) | 112 (31.5) | 2202 (47.1) | 51 (31.3) | 67 (26.6) | 4132 (49.3) | 231 (36.4) | 379 (35.9) | 1602 (50.2) | 181 (39.3) | 512 (41.8) | 894 (55.4) | 237 (42.2) | 372 (42.8) |
| Other cancers | 6503 (53.9) | 465 (70.1) | 530 (68.0) | 2413 (50.8) | 373 (66.4) | 244 (68.5) | 2473 (52.9) | 112 (68.7) | 185 (73.4) | 4256 (50.7) | 404 (63.6) | 677 (64.1) | 1590 (49.8) | 280 (60.7) | 713 (58.2) | 721 (44.6) | 324 (57.8) | 497 (57.2) |
| Cancer site | ||||||||||||||||||
| Leukemia | 279 (2.3) | 45 (6.8) | 60 (7.7) | 88 (1.9) | 30 (5.3) | 8 (2.2) | 107 (2.3) | 9 (5.5) | 11 (4.4) | 86 (1.0) | 38 (6.0) | 44 (4.2) | 111 (3.5) | 30 (6.5) | 59 (4.8) | 50 (3.1) | 18 (3.2) | 26 (3.0) |
| Multiple myeloma | 247 (2.0) | 38 (5.7) | 34 (4.4) | 151 (3.2) | 32 (5.7) | 19 (5.3) | 104 (2.2) | <5 | <5 | 122 (1.5) | 20 (3.1) | 26 (2.5) | 77 (2.4) | 10 (2.2) | 10 (0.8) | 26 (1.6) | 13 (2.3) | 15 (1.7) |
| Bladder cancer | 438 (3.6) | 34 (5.1) | 51 (6.5) | 163 (3.4) | 45 (8.0) | 24 (6.7) | 133 (2.8) | 21 (12.9) | 12 (4.8) | 323 (3.9) | 31 (4.9) | 57 (5.4) | 198 (6.2) | 26 (5.6) | 80 (6.5) | 82 (5.1) | 27 (4.8) | 63 (7.2) |
| Brain tumor | 611 (5.1) | 17 (2.6) | 35 (4.5) | 179 (3.8) | 7 (1.2) | 8 (2.2) | 198 (4.2) | 5 (3.1) | <5 | 501 (6.0) | 21 (3.3) | 42 (4.0) | 88 (2.8) | 9 (2.0) | 18 (1.5) | 56 (3.5) | 15 (2.7) | 18 (2.1) |
| Gynecologic cancer | 837 (6.9) | 20 (3.0) | 28 (3.6) | 337 (7.1) | 11 (2.0) | 10 (2.8) | 416 (8.9) | <5 | 10 (4.0) | 779 (9.3) | 30 (4.7) | 66 (6.3) | 331 (10.4) | 23 (5.0) | 74 (6.0) | 168 (10.4) | 39 (7.0) | 64 (7.4) |
| Lung cancer | 1644 (13.6) | 53 (8.0) | 41 (5.3) | 778 (16.4) | 51 (9.1) | 29 (8.1) | 601 (12.9) | 7 (4.3) | 16 (6.3) | 1417 (16.9) | 82 (12.9) | 138 (13.1) | 333 (10.4) | 32 (6.9) | 96 (7.8) | 230 (14.2) | 58 (10.3) | 93 (10.7) |
| Lymphoma | 554 (4.6) | 53 (8.0) | 69 (8.9) | 291 (6.1) | 32 (5.7) | 24 (6.7) | 278 (5.9) | 7 (4.3) | 8 (3.2) | 279 (3.3) | 28 (4.4) | 35 (3.3) | 177 (5.5) | 32 (6.9) | 68 (5.6) | 115 (7.1) | 27 (4.8) | 39 (4.5) |
| Urinary tract cancer | 333 (2.8) | 10 (1.5) | 15 (1.9) | 139 (2.9) | 22 (3.9) | 8 (2.2) | 133 (2.8) | 10 (6.1) | 8 (3.2) | 231 (2.8) | 25 (3.9) | 24 (2.3) | 238 (7.5) | 37 (8.0) | 119 (9.7) | 100 (6.2) | 33 (5.9) | 63 (7.2) |
| Prostate cancer | 1106 (9.2) | 162 (24.4) | 199 (25.5) | 372 (7.8) | 86 (15.3) | 70 (19.7) | 428 (9.2) | 35 (21.5) | 60 (23.8) | 577 (6.9) | 117 (18.4) | 183 (17.3) | 314 (9.8) | 82 (17.8) | 198 (16.2) | 131 (8.1) | 101 (18.0) | 133 (15.3) |
| Digestive organ cancer | 3460 (28.7) | 79 (11.9) | 94 (12.1) | 1605 (33.8) | 137 (24.4) | 68 (19.1) | 1500 (32.1) | 17 (10.4) | 41 (16.3) | 3010 (35.9) | 127 (20.0) | 187 (17.7) | 1038 (32.5) | 115 (25.0) | 280 (23.0) | 472 (29.2) | 140 (25.0) | 195 (22.4) |
| Upper GI cancer† | 431 (3.6) | 0 (0) | <5 | 197 (4.1) | 7 (1.2) | <5 | 208 (4.4) | <5 | <5 | 698 (8.3) | 14 (2.2) | 30 (2.8) | 198 (6.2) | 16 (3.5) | 40 (3.3) | 85 (5.3) | 25 (4.5) | 34 (3.9) |
| Lower GI cancer† | 1879 (15.6) | 68 (10.3) | 78 (10.0) | 1037 (21.8) | 109 (19.4) | 64 (18.0) | 805 (17.2) | 15 (9.2) | 28 (11.1) | 1475 (17.6) | 84 (13.2) | 113 (10.7) | 522 (16.4) | 65 (14.1) | 179 (14.6) | 210 (13.0) | 69 (12.3) | 127 (14.6) |
| Pancreatic cancer† | 846 (7.0) | 9 (1.4) | 7 (0.9) | 311 (6.5) | 13 (2.3) | 2 (0.6) | 348 (7.4) | 0 (0.0) | 6 (2.4) | 511 (6.1) | 16 (2.5) | 23 (2.2) | 228 (7.1) | 23 (5.0) | 43 (3.5) | 141 (8.7) | 36 (6.4) | 28 (3.2) |
| Breast cancer | 1218 (10.1) | 75 (11.3) | 67 (8.6) | 457 (9.6) | 71 (12.6) | 42 (11.8) | 744 (15.9) | 36 (22.1) | 65 (25.8) | 1152 (13.7) | 83 (13.1) | 152 (14.4) | 474 (14.8) | 78 (16.9) | 220 (18.0) | 258 (16.0) | 93 (16.6) | 143 (16.5) |
| Melanoma | 207 (1.7) | 15 (2.3) | 25 (3.2) | 124 (2.6) | 30 (5.3) | 15 (4.2) | 98 (2.1) | <5 | <5 | 86 (1.0) | 12 (1.9) | 23 (2.2) | 90 (2.8) | 18 (3.9) | 29 (2.4) | 58 (3.6) | 20 (3.6) | 42 (4.8) |
| Other cancer† | 5638 (46.7) | 97 (14.6) | 98 (12.6) | 2109 (44.4) | 125 (22.2) | 42 (11.8) | 1580 (33.8) | 7 (4.3) | 18 (7.1) | 5410 (64.5) | 248 (39.1) | 493 (46.7) | 1721 (53.9) | 161 (34.92) | 379 (30.94) | 934 (57.83) | 211 (37.61) | 328 (37.74) |
†
Patients can have more than one cancer type, so numbers should not add to 100%.
‡
Indicates that the data was secondary suppressed to prevent back calculation of the results.
AOK: Allgemeine Ortskrankenkasse; CCI: Charlson Comorbidity Index; COPD: Chronic obstructive pulmonary disease; DVT: Deep vein thrombosis; GI: Gastrointestinal; GWQ: Gesellschaft für Wirtschaftlichkeit und Qualität bei Krankenkassen; LMWH: Low-molecular-weight heparin; NSAID: Nonsteroidal anti-inflammatory drug; PE: Pulmonary embolism; VTE: Venous thromboembolism.
Description of the weighted cohorts
After IPTW in each country-specific analysis (Figure 1), averaged and weighted patient demographics and clinical characteristics at baseline were found to be similar across treatment groups (Table 2). CCI scores were consistent across treatment groups, and more than half of the patients had hypertension (apixaban vs LMWH: 63.6% vs 62.6%; rivaroxaban vs LMWH: 65.9% vs 62.5%). Prior bleeding was higher in both of the DOAC groups compared with LMWH (apixaban vs LMWH: 14.9% vs 12.6%; rivaroxaban vs LMWH: 16.7% vs 12.5%). The prevalence of non-GI cancer was the highest cancer type across all treatment groups and within the cancer sites digestive organ cancer had the highest prevalence (apixaban vs LMWH: 32.6% vs 31.2%; rivaroxaban vs LMWH: 29.8% vs 30.6%). Almost half of patients had a high- or very high-risk cancer type for VTE across all treatment groups (Table 2).
| Characteristic | LMWH vs apixaban weighted cohort | LMWH vs rivaroxaban weighted cohort | ||
|---|---|---|---|---|
| LMWH (n = 30,002) | Apixaban (n = 2892) | LMWH (n = 29,976) | Rivaroxaban (n = 4321) | |
| Age at index VTE (years) | ||||
| Mean (SD) | 67.72 (12.2) | 67.31 (12.7) | 67.79 (12.2) | 67.8 (12.7) |
| Sex, n (%) | ||||
| Female | 15,838 (52.8) | 1510 (52.2) | 15,780 (52.6) | 2287 (52.9) |
| Index VTE type, n (%) | ||||
| DVT | 12,867 (43.1) | 1300 (45.0) | 12,906 (43.1) | 2214 (51.2) |
| PE (with or without DVT) | 17,135 (57.1) | 1592 (55.1) | 17,071 (57.0) | 2107 (48.8) |
| Prior clinical characteristics, n (%) | ||||
| Prior bleeding | 3586 (12.6) | 345 (14.9) | 3548 (12.5) | 576 (16.7) |
| CCI, n (%) | ||||
| Mean (SD) | 5.11 (2.3) | 5.37 (2.4) | 5.09 (2.3) | 5.47 (2.4) |
| Specific comorbidities, n (%)† | ||||
| Congestive heart failure | 2488 (8.3) | 324 (11.2) | 2490 (8.3) | 620 (14.4) |
| Peripheral vascular disease | 2152 (7.2) | 242 (8.4) | 2125 (7.1) | 480 (11.1) |
| Cerebrovascular disease | 2648 (8.8) | 294 (10.2) | 2675 (8.9) | 533 (12.3) |
| COPD and/or asthma | 5741 (19.1) | 646 (22.3) | 5729 (19.1) | 1040 (24.1) |
| Rheumatic disease | 2261 (7.5) | 228 (7.9) | 2256 (7.5) | 356 (8.2) |
| Diabetes without chronic complication | 3004 (10.0) | 301 (10.4) | 2969 (9.9) | 498 (11.5) |
| Diabetes with chronic complication | 1894 (6.3) | 236 (8.2) | 1864 (6.2) | 426 (9.9) |
| Renal disease | 4636 (15.5) | 568 (19.6) | 4598 (15.3) | 1043 (24.1) |
| Hypertension | 18786 (62.6) | 1840 (63.6) | 18,736 (62.5) | 2846 (65.9) |
| Anemia | 6701 (22.3) | 652 (22.5) | 6548 (21.8) | 1036 (24.0) |
| Obesity | 3862 (12.9) | 469 (16.2) | 3853 (12.9) | 898 (20.8) |
| Varicose veins | 2815 (9.4) | 383 (13.2) | 2806 (9.4) | 738 (17.1) |
| Ischemic heart disease/coronary artery disease | 3640 (12.1) | 388 (13.4) | 3654 (12.2) | 691 (16.0) |
| Coagulation defects | 1511 (5.0) | 199 (7.0) | 1485 (5.0) | 372 (8.6) |
| Dyspepsia | 3880 (12.9) | 438 (15.2) | 3827 (13.0) | 669 (15.6) |
| Hyperlipidemia | 3155 (10.5) | 394 (13.6) | 3122 (10.4) | 776 (18.1) |
| Pneumonia 3 months before index date | 3161 (10.5) | 334 (11.6) | 3142 (10.5) | 514 (11.9) |
| Concomitant treatment, n (%) | ||||
| Platelet aggregation inhibitors 3 months before index date | 2880 (9.6) | 240 (8.3) | 2895 (9.7) | 340 (7.9) |
| NSAIDs 3 months before index date | 4003 (13.3) | 424 (14.7) | 4005 (13.4) | 662 (15.3) |
| Diagnostic setting, n (%) | ||||
| Inpatient | 19,176 (63.9) | 1724 (59.6) | 19,000 (63.4) | 2316 (53.6) |
| Outpatient | 7871 (26.2) | 940 (32.5) | 7943 (26.5) | 1587 (36.7) |
| Cancer type, n (%) | ||||
| Metastatic solid tumor | 17,026 (56.8) | 1641 (56.7) | 16,769 (55.9) | 2324 (53.8) |
| GI cancer | 9320 (31.1) | 935 (32.3) | 9143 (30.5) | 1277 (29.6) |
| Non-GI cancer | 18,200 (60.7) | 1687 (58.3) | 18,355 (61.2) | 2658 (61.5) |
| Hematological malignancy | 2482 (8.3) | 268 (9.3) | 2478 (8.3) | 386 (8.9) |
| Cancer risk type, n (%) | ||||
| High or very high risk for VTE | 14,244 (47.5) | 1410 (48.8) | 14,160 (47.2) | 2106 (48.7) |
| Other cancers | 15,758 (52.5) | 1482 (51.2) | 15,816 (52.8) | 2214 (51.2) |
| Cancer site, n (%) | ||||
| Leukemia | 666 (2.2) | 76 (2.6) | 665 (2.2) | 121 (2.8) |
| Multiple myeloma | 683 (2.3) | 57 (2.0) | 680 (2.3) | 68 (1.6) |
| Bladder cancer | 1211 (4.0) | 148 (5.1) | 1219 (4.1) | 280 (6.5) |
| Brain tumor | 1428 (4.8) | 86 (3.0) | 1439 (4.8) | 149 (3.5) |
| Gynecologic cancer | 2375 (7.9) | 217 (7.5) | 2358 (7.9) | 347 (8.0) |
| Lung cancer | 4327 (14.4) | 403 (13.9) | 4306 (14.4) | 544 (12.6) |
| Lymphoma | 1436 (4.8) | 163 (5.6) | 1425 (4.8) | 245 (5.7) |
| Urinary tract cancer | 1030 (3.4) | 125 (4.3) | 1029 (3.4) | 248 (5.7) |
| Prostate cancer | 2631 (8.8) | 312 (10.8) | 2700 (9.0) | 481 (11.1) |
| Digestive organ cancer | 9351 (31.2) | 943 (32.6) | 9172 (30.6) | 1289 (29.8) |
| Upper GI cancer | 1568 (5.2) | 109 (3.8) | 1529 (5.1) | 181 (4.2) |
| Lower GI cancer | 5037 (16.8) | 559 (19.3) | 4958 (16.5) | 814 (18.8) |
| Pancreatic cancer | 1940 (6.5) | 218 (7.5) | 1894 (6.3) | 225 (5.2) |
| Breast cancer | 3603 (12.0) | 360 (12.5) | 3654 (12.2) | 552 (12.8) |
| Melanoma | 575 (1.9) | 71 (2.5) | 582 (1.9) | 99 (2.3) |
| Other cancer | 15,326 (51.1) | 1411 (48.8) | 15,084 (50.3) | 2052 (47.5) |
†
To maintain clarity and conciseness of the table, only those comorbidities present in >5% of all groups have been presented. The following comorbidities were evaluated but not included in the table: dementia, peptic ulcer disease, mild liver disease, moderate or severe liver disease, hemiplegia or paraplegia, AIDS/HIV, sepsis, stroke, cardiac arrest, inflammatory bowel disease, sleep apnea, spinal cord injury and thrombophilia.
CCI: Charlson Comorbidity Index; COPD: Chronic obstructive pulmonary disease; DVT: Deep vein thrombosis; GI: Gastrointestinal; LMWH: Low-molecular-weight heparin; NSAID: Nonsteroidal anti-inflammatory drug; PE: Pulmonary embolism; VTE: Venous thromboembolism.
Occurrence & risk of bleeding & VTE recurrence after IPTW
Cumulative incidence estimates for the proportion of patients experiencing overall bleeding and bleeding by site at 3 and 6 months for both comparisons are provided in Figure 2.
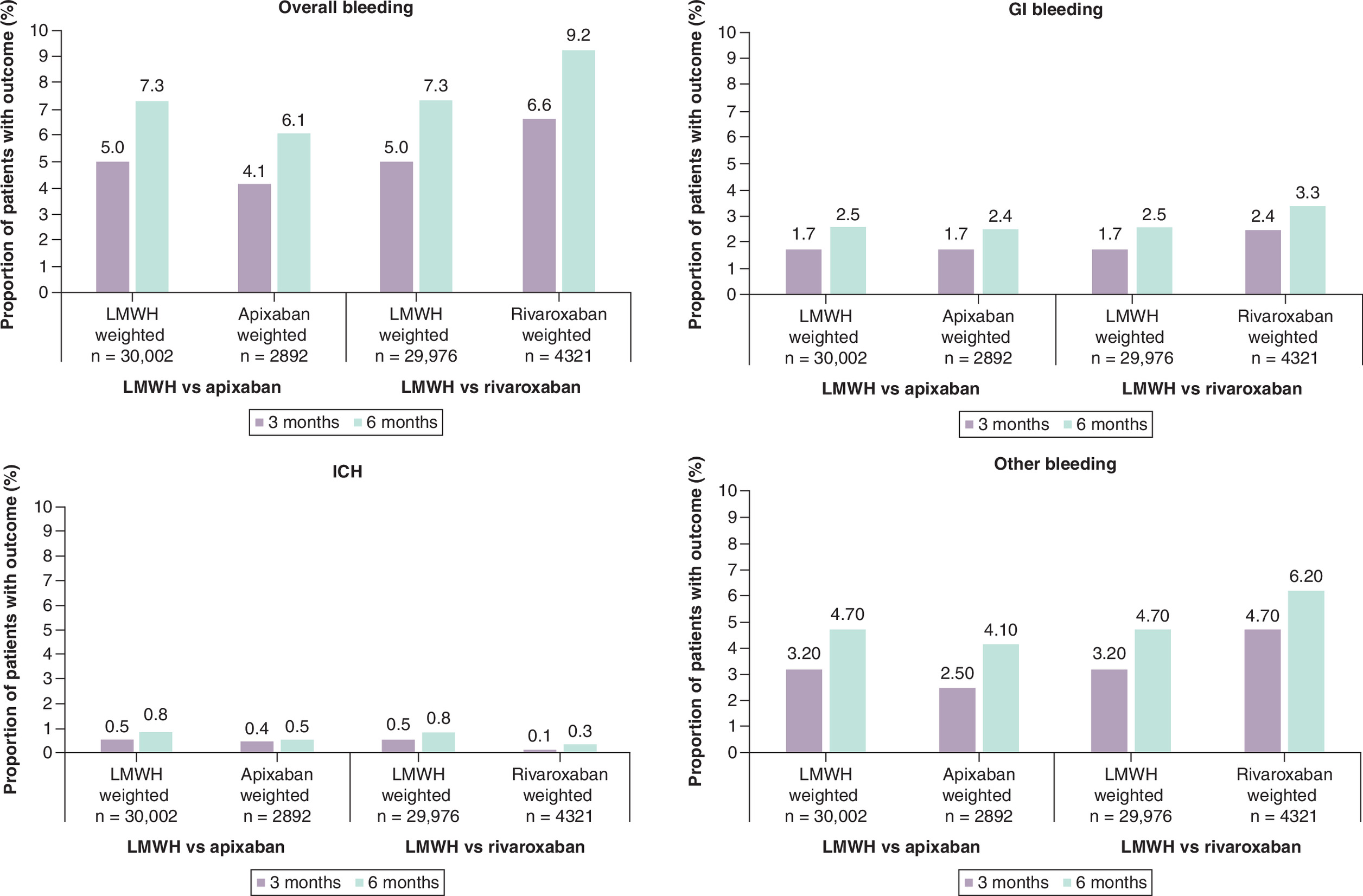
Figure 2. Cumulative incidence of bleeding outcomes (apixaban vs low-molecular-weight heparin and rivaroxaban vs low-molecular-weight heparin) at 3- and 6-month intervals.
Each of the country-specific estimates were conducted using Fine–Gray competing risk, and the weighted were estimated.
GI: Gastrointestinal; ICH: Intercranial hemorrhage; LMWH: Low-molecular-weight heparin.
The meta-analyzed country-specific incidence rates in the IPTW country-specific estimates and hazard ratios (HRs) using the random-effect estimates can be found in Table 3 for apixaban versus LMWH and Table 4 for rivaroxaban versus LMWH. As previously described, rVTE events were not powered for comparative analyses; however, descriptive pre-IPTW results for the rVTE and bleeding outcomes can be found in Supplementary Material 5.
| Apixaban | LMWH | HR | ||||||
|---|---|---|---|---|---|---|---|---|
| Events | PY | Rate per 100 PY [95%CI]† | Events | PY | Rate per 100 PY [95%CI]† | |||
| Overall bleeding | MA result | – | – | 14.94 [10.16–21.97] | – | – | 24.60 [15.37–39.37] | 0.67 [0.53–0.86] |
| Sweden | 29 | 225 | 12.70 [8.81–18.32] | 534 | 3680 | 14.51 [13.33–15.80] | 0.98 [0.56–1.72] | |
| Norway | 24 | 198 | 12.16 [8.16–18.12] | 312 | 1487 | 20.98 [18.78–23.44] | 0.64 [0.37–1.10] | |
| UK | 18 | 194 | 9.51 [6.02–15.00] | 364 | 2297 | 15.86 [14.31–17.57] | 0.62 [0.31–1.25] | |
| Germany - AOK | 40 | 137 | 29.48 [21.44–40.54] | 301 | 647 | 46.50 [41.52–52.08] | 0.75 [0.50–1.12] | |
| Germany - GWQ | 29 | 181 | 15.88 [10.82–23.30] | 130 | 319 | 40.57 [34.0-9–48.28] | 0.46 [0.28–0.76] | |
| GI bleeding | MA result | – | – | 6.37 [4.34–9.35] | – | – | 7.71 [5.61–10.61] | 0.89 [0.61–1.29] |
| Sweden | 10 | 228 | 4.32 [2.31–8.07] | 189 | 3743 | 5.04 [4.37–5.81] | 0.95 [0.34–2.71] | |
| Norway | 16 | 199 | 8.22 [5.07–13.34] | 111 | 1526 | 7.29 [6.06–8.78] | 1.20 [0.58–2.47] | |
| UK | 10 | 195 | 5.16 [2.78–9.57] | 150 | 2322 | 6.45 [5.49–7.57] | 0.84 [0.35–2.00] | |
| Germany - AOK | 15 | 140 | 10.75 [6.17–18.74] | 86 | 679 | 12.62 [10.18–15.65] | 1.03 [0.50–2.11] | |
| Germany - GWQ | 7 | 184 | 3.64 [1.36–9.76] | 32 | 333 | 9.75 [6.81–13.96] | 0.44 [0.18–1.09] | |
| ICH | MA result | – | – | 1.25 [0.76–2.05] | – | – | 2.21 [1.91–2.55] | 0.67 [0.31–1.44] |
| Sweden | 3 | 228 | 1.18 [0.36–3.90] | 87 | 3765 | 2.31 [1.87–2.85] | 0.57 [0.10–3.29] | |
| Norway | 3 | 202 | 1.37 [0.42–4.44] | 35 | 1544 | 2.26 [1.62–3.15] | 0.69 [0.20–2.35] | |
| UK | 0 | 196 | 0 | 47 | 2336 | 2.03 [1.53–2.70] | NE‡ | |
| Germany - AOK | 2 | 142 | 1.56 [0.67–3.62] | 15 | 687 | 2.18 [1.25–3.82] | 0.85 [0.18–4.03] | |
| Germany - GWQ | 2 | 185 | 0.94 [0.38–2.34] | 6 | 336 | 1.71 [0.54–5.42] | 0.55 [0.09–3.38] | |
| Other bleeding | MA result | – | – | 9.41 [5.74–15.44] | – | – | 16.06 [8.40–30.71] | 0.64 [0. 0.998] |
| Sweden | 22 | 226 | 9.82 [6.47–14.89] | 303 | 3715 | 8.15 [7.28–9.12] | 1.35 [0.72–2.53] | |
| Norway | 13 | 200 | 6.31 [3.64–10.96] | 205 | 1506 | 13.58 [11.84–15.58] | 0.52 [0.24–1.13] | |
| UK | 8 | 195 | 4.29 [2.18–8.44] | 184 | 2317 | 7.95 [6.88–9.19] | 0.55 [0.18–1.72] | |
| Germany - AOK | 27 | 139 | 19.52 [13.15–28.98] | 228 | 654 | 34.80 [30.54–39.66] | 0.65 [0.40–1.06] | |
| Germany - GWQ | 21 | 182 | 11.64 [7.39–18.34] | 113 | 321 | 35.08 [29.11–42.28] | 0.39 [0.22–0.70] | |
†
Reported per 100 PY.
‡
Cannot be computed due to 0 events in the apixaban group.
All analyses presented used a random-effects model due to sample size and few data sources being included in the meta-analyses.
AOK: Allgemeine Ortskrankenkasse; GI: Gastrointestinal; GWQ: Gesellschaft für Wirtschaftlichkeit und Qualität bei Krankenkassen; HR: Hazard ratio; ICH: Intracranial hemorrhage; LMWH: Low-molecular-weight heparin; MA: Meta-analysis; NE: Not Evaluable; PY: Person-year.
| Rivaroxaban | LMWH | HR | ||||||
|---|---|---|---|---|---|---|---|---|
| Events | PY | Rate per 100 PY [95%CI]† | Events | PY | Rate per 100 PY [95%CI]† | |||
| Overall bleeding | MA result | – | – | 20.54 [12.47–33.81] | – | – | 24.38 [15.32–38.79] | 0.98 [0.83–1.15] |
| Sweden | 30 | 269 | 11.11 [7.76–15.90] | 533 | 3681 | 14.48 [13.30–15.77] | 0.84 [0.46–1.53] | |
| Norway | 18 | 116 | 15.70 [9.92–24.84] | 312 | 1486 | 20.99 [18.78–23.45] | 0.81 [0.40–1.64] | |
| UK | 44 | 311 | 14.26 [10.63–19.14] | 363 | 2299 | 15.79 [14.25–17.50] | 0.94 [0.62–1.42] | |
| Germany - AOK | 134 | 354 | 37.83 [31.88–44.89] | 297 | 636 | 46.65 [41.61–52.30] | 0.97 [0.76–1.24] | |
| Germany - GWQ | 87 | 246 | 35.36 [28.56–43.77] | 123 | 317 | 38.92 [32.57–46.51] | 1.09 [0.80–1.48] | |
| GI bleeding | MA result | – | – | 6.05 [2.86–12.82] | – | – | 7.60 [5.57–10.36] | 0.86 [0.47–1.58] |
| Sweden | 7 | 270 | 2.41 [1.12–5.19] | 188 | 3743 | 5.01 [4.34–5.78] | 0.53 [0.17–1.65] | |
| Norway | 2 | 119 | 1.72 [0.44–6.76] | 111 | 1525 | 7.29 [6.06–8.78] | 0.26 [0.10–0.67] | |
| UK | 25 | 314 | 8.08 [5.47–11.92] | 148 | 2324 | 6.38 [5.43–7.49] | 1.31 [0.73–2.37] | |
| Germany - AOK | 58 | 365 | 15.80 [12.13–20.58] | 82 | 668 | 12.29 [9.87–15.31] | 1.54 [1.02–2.32] | |
| Germany - GWQ | 20 | 254 | 7.84 [4.89–12.57] | 31 | 330 | 9.47 [6.56–13.66] | 1.00 [0.53–1.90] | |
| ICH | MA result | – | – | 0.78 [0.38–1.63] | – | – | 2.21 [1.91–2.55] | 0.32 [0.13–0.82] |
| Sweden | 5 | 271 | 1.74 [0.70–4.28] | 87 | 3765 | 2.32 [1.88–2.86] | 0.83 [0.13–5.10] | |
| Norway | 2 | 119 | 1.63 [0.40–6.65] | 35 | 1543 | 2.24 [1.61–3.13] | 0.76 [0.17–3.35] | |
| UK | 0‡ | 316 | 0.11 [0.00–3.06] | 48 | 2338 | 2.04 [1.54–2.71] | 0.06 [0.01–0.40] | |
| Germany - AOK | 2 | 372 | 0.40 [0.15–1.05] | 15 | 676 | 2.19 [1.25–3.83] | 0.21 [0.05–0.92] | |
| Germany - GWQ | 1 | 256 | 0.57 [0.22–1.49] | 6 | 333 | 1.72 [0.54–5.46] | 0.33 [0.03–3.49] | |
| Other bleeding | MA result | – | – | 13.21 [7.01–24.91] | – | – | 15.94 [8.39–30.29] | 0.89 [0.74–1.08] |
| Sweden | 19 | 270 | 6.92 [4.40–10.89] | 302 | 3716 | 8.13 [7.27–9.10] | 0.91 [0.43–1.95] | |
| Norway | 14 | 116 | 12.41 [7. 20.79] | 205 | 1505 | 13.60 [11.86–15.59] | 0.98 [0.42–2.30] | |
| UK | 19 | 314 | 5.96 [3.79–9.38] | 184 | 2319 | 7.93 [6.86–9.16] | 0.78 [0.43–1.40] | |
| Germany - AOK | 86 | 359 | 23.90 [19.28–29.62] | 226 | 643 | 35.08 [30.76–40.00] | 0.81 [0.61–1.08] | |
| Germany - GWQ | 73 | 248 | 29.33 [23.20–37.08] | 108 | 319 | 33.70 [27.84–40.80] | 1.04 [0.75–1.44] | |
†
Reported per 100 PY.
‡
Full weighed number is 0.3 events.
All analyses presented used a random-effects model due to sample size and few data sources being included in the meta-analyses.
AOK: Allgemeine Ortskrankenkasse; GI: Gastrointestinal; GWQ: Gesellschaft für Wirtschaftlichkeit und Qualität bei Krankenkassen; HR: Hazard ratio; ICH: Intracranial hemorrhage; LMWH: Low-molecular-weight heparin; MA: Meta-analysis; PY: Person-year.
At 6 months, patients treated with apixaban had a significantly lower risk of overall bleeding compared with LMWH (rate per 100 PY: apixaban: 14.94 [95% CI: 10.16–21.97]; LMWH: 24.60 [95% CI: 15.37–39.37]; HR: 0.67 [95% CI: 0.53–0.86]). The risk of other bleeding was also lower for the apixaban cohort than for the LMWH cohort (rate per 100 PY: apixaban: 9.41 [95% CI: 5.74–15.44]; 16.06 [95% CI: 8.40–30.71]; HR: 0.64 [95% CI: 0.41–0.998]). There was no significant difference between apixaban and LMWH for GI or ICH bleeding risk (GI: rate per 100 PY: apixaban: 6.37 [95% CI: 4.34–9.35]; LMWH: 7.71 [95% CI: 5.61–10.61]; HR: 0.89 [95% CI: 0.61–1.29] and ICH: rate per 100 PY: apixaban: 1.25 [95% CI: 0.76–2.05]; LMWH: 2.21 [95% CI: 1.91–2.55]; HR: 0.67 [95% CI: 0.31–1.44]). The lower risk estimates for apixaban versus LMWH appeared to be driven by Germany GWQ and the UK (Table 3).
The risk of ICH bleeding was lower for rivaroxaban than for LMWH (rate per 100 PY: rivaroxaban: 0.78 [95% CI: 0.38–1.63]; LMWH: 2.21 [95% CI: 1.91–2.55]; HR: 0.32 [95% CI: 0.13–0.82]). The risks of overall, GI bleeding, and other bleeding were similar for the other rivaroxaban versus LMWH comparisons (overall bleeding: rate per 100 PY: rivaroxaban: 20.54 [95% CI: 12.47–33.81]; LMWH: 24.38 [95% CI: 15.32–38.79]; HR: 0.98 [95% CI: 0.83–1.15] GI bleeding: rate per 100 PY: rivaroxaban: 6.05 [95% CI: 2.86–12.82]; LMWH: 7.60 [95% CI: 5.57–10.36] HR: 0.86 [95% CI: 0.47–1.58], and other bleeding: rate per 100 PY: rivaroxaban: 13.21 [95% CI: 7.01–24.91]; LMWH: 15.94 [95% CI: 8.39–30.29]; HR: 0.89 [95% CI: 0.74–1.08]). Point estimates and trends were mostly consistent across countries with overlapping confidence intervals (Table 4).
Country-specific estimates before IPTW are provided in Supplementary Material 5.
Discussion
This large, multicountry European study analyzed real-world data from Sweden, Norway, Finland, the UK and Germany (2013–2020) to assess bleeding risks in patients with cancer-associated VTE treated with DOACs or LMWH. Treatment guidelines caution on the use of DOACs in patients with GI and genitourinary cancer due to higher rates of bleeding [14–18]. The descriptive results of our study reflected these recommendations – a higher proportion of patients with GI cancer or very high- or high-risk cancers were prescribed LMWH. When assessing bleeding risk in patients treated with apixaban compared with LMWHs, apixaban was associated with a lower risk of overall and other (i.e., not ICH or GI) bleeding, but had a similar risk for ICH and GI bleeding. Patients treated with rivaroxaban were found to have a similar risk of overall bleeding compared with LMWH, but a lower risk of ICH bleeding.
Our findings for apixaban are broadly consistent with Caravaggio [12] and ADAM VTE [20] clinical trials, which showed no excess risk of bleeding (MB or clinically relevant not MB) compared with LMWH, though our real-world data suggested lower overall bleeding (Caravaggio: MB: HR: 0.82 [95% CI: 0.40–1.69]; major GI bleeding: HR: 1.05 [95% CI: 0.44–2.50]; ADAM VTE: MB: 0% vs 1.4%). The SELECT-D [13] and CASTA DIVA [21] trials showed similar MB risks for rivaroxaban versus dalteparin, consistent with our findings of similar overall bleeding risk for rivaroxaban (SELECT-D: MB: 6% vs 4%; CASTA DIVA: MB: HR: 0.36 [95% CI: 0.04–3.43]).
A US retrospective study conducted in MarketScan Commercial Claims (2014–2017) [32–34] found lower risks of MB (HR: 0.63 [95% CI: 0.47–0.86]), ICH bleeding (HR: 0.22 [95% CI: 0.07–0.70]), and other bleeding (HR: 0.62 [95% CI: 0.41–0.92]), and a similar risk of GI bleeding with apixaban versus LMWH (HR: 0.97 [95% CI: 0.59–1.58]). With the exception of ICH bleeding which was underpowered in the current study, these results align with our findings. Another US retrospective study conducted in the Humana database (2007–2015) [35] reported comparable MB risks for rivaroxaban versus LMWH (HR: 1.03 [95% CI: 0.64–1.65]), similar to our results. Comparison with prior US retrospective studies further confirmed differences in risk by bleeding type, with some slight geographical differences.
This is the first study to compare the safety of DOACs and LMWH for the treatment of cancer-related VTE in a real-world European setting. Strengths include the large multicountry population and high quality data sources [36–40] and the categorization of the bleeding outcomes into sites (GI, ICH and other). The use of IPTW ensures that comparisons are made between similar populations, so any observed differences in outcomes are more likely attributable to the treatment rather than underlying differences between cohorts. However, since IPTW was conducted on the country-level, this did not account for between country heterogeneity.
A limitation of the study was that only the primary outcome (overall bleeding) was powered for comparative analyses, so bleeding by site comparisons should be interpreted with caution. The effectiveness outcome (rVTE) was underpowered – the definition used was restricted to the inpatient setting because it is not possible to differentiate between recurrent and incident VTE events in the outpatient setting in the datasets used. Future research could aim to conduct analyses better powered for detecting differences in bleeding by site and rVTE. Additionally, the assumption of one syringe per day might have resulted in an underestimation of the duration of LMWHs. Cancer treatments were not accurately recorded in all datasets, and therefore identification of patients with cancer using only diagnoses codes likely underestimated prevalence. Despite IPTW, residual and unmeasured confounding may still exist leading which could have under or overestimated risk of the study outcomes. Future research should leverage more recent data to capture the evolving treatment landscape following updated guidelines that increasingly recommend DOACs for cancer-associated VTE [15,16,41]. More recent data with increased sample sizes could also be used to perform DOAC versus DAOC comparisons in the real-world setting, since the current study was not designed for these types of comparisons.
Conclusion
In this multicountry European study, in patients with cancer who had a VTE, apixaban was associated with a lower risk of overall bleeding compared with LMWH. The risk of overall bleeding associated with rivaroxaban was similar to that associated with LMWH. Overall, these results provide valuable real-world insights in an area where evidence remains very limited and support the role of DOACs as a safe alternative to LMWH in patients with VTE and cancer.
Summary points
•
This study aimed to compare the safety of direct oral anticoagulant (DOACs) with low-molecular-weight heparin (LMWH) in patients with venous thromboembolism (VTE) and active cancer in a real-world setting in Sweden, Norway, Finland, the UK and Germany.
•
Treatment-naive adult patients with cancer-related VTE treated with a DOAC or LMWH were identified.
•
Inverse probability of treatment weighting (IPTW) was employed for each DOAC-LMWH comparison and assessed risk of bleeding (overall and by site: gastrointestinal, intracranial hemorrhage or other) within 6 months after treatment initiation.
•
Fine–Gray models were fitted to estimate adjusted hazard ratios. Country estimates were combined using meta-analyses.
•
Recurrent VTE could not be assessed in comparative analyses because of low numbers.
•
Across the five countries and before IPTW, 34,687 LMWH users, 3176 vitamin K antagonist users, 3045 apixaban users, 4537 rivaroxaban users, 145 dabigatran users and 580 edoxaban users were identified.
•
The descriptive results of our study suggest more patients with very high- or high-risk cancers were prescribed LMWH compared with DOACs.
•
After IPTW, patients with VTE and cancer initiating apixaban showed an improved safety profile compared with LMWH for overall bleeding, whereas the risk was similar for patients initiating rivaroxaban versus LMWH.
Author contributions
All authors contributed to the conception and design of this work and related manuscript. All authors read and approved the final manuscript.
Financial disclosure
This was a BMS/Pfizer UK sponsored study.
Competing interests disclosure
D Lambrelli, B Nordstrom, A Booth and S Graham are employees of Evidera. Evidera received funding from Bristol Myers Squibb in connection with the work reported in this manuscript. R Mokgokong, A Jenkins, J Chaves, F Dai, R Subash and D Fliegner are employees and shareholders of Pfizer. A Gottsäter has received consultancy fees from Bayer, Pfizer and Sanofi. E Brodin has received personal fees for lectures or consultancy from Bayer, Bristol Myers Squibb and Pfizer. F Langer has received personal fees for lectures or consultancy from Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo, LEO Pharma, Pfizer, Sanofi and Viatris. E Brodin, A Young, F Langer, R Alikhan, L Timo and A Gottsäter received honoraria paid by the Pfizer/BMS Alliance for the participation in the VICTORIE Study Steering Group. A Mevius is an employee of IPAM. M Ghiani and M Lehne are employees of Cytel. Cytel received funding from Evidera for analytic work for the German part of this study. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 151.59 KB
References
Papers of special note have been highlighted as: • of interest
1.
Lyman GH, Culakova E, Poniewierski MS, Kuderer NM. Morbidity, mortality and costs associated with venous thromboembolism in hospitalized patients with cancer. Thromb. Res. 164(Suppl. 1), S112–S118 (2018).
2.
Walker AJ, Card TR, West J et al. Incidence of venous thromboembolism in patients with cancer - a cohort study using linked United Kingdom databases. Eur. J. Cancer 49(6), 1404–1413 (2013).
3.
Mulder FI, Horvath-Puho E, van Es N et al. Venous thromboembolism in cancer patients: a population-based cohort study. Blood 137(14), 1959–1969 (2021).
4.
Donnellan E, Khorana AA. Cancer and venous thromboembolic disease: a review. Oncologist 22(2), 199–207 (2017).
5.
Chew HK, Wun T, Harvey D et al. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch. Intern. Med. 166(4), 458–464 (2006).
6.
Khorana AA, Francis CW, Culakova E et al. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J. Thromb. Haemost. 5(3), 632–634 (2007).
7.
Khorana AA, Francis CW, Culakova E et al. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer 110(10), 2339–2346 (2007).
8.
Wang TF, Billett HH, Connors JM, Soff GA. Approach to cancer-associated thrombosis: challenging situations and knowledge gaps. Oncologist 26(1), e17–e23 (2021).
9.
Lee AY, Levine MN, Baker RI et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N. Engl. J. Med. 349(2), 146–153 (2003).
10.
Muñoz A, Gallardo E, Agnelli G et al. Cost-effectiveness of direct oral anticoagulants compared to low-molecular-weight-heparins for treatment of cancer associated venous thromboembolism in Spain. J. Med. Econ. 25(1), 840–847 (2022).
11.
Shin YE, Kumar A, Hwang M et al. Cost-utility analysis comparing direct oral anticoagulant and low molecular weight heparin therapies for secondary prevention of cancer-associated thrombosis. Clin. Drug Investig. 42(12), 1075–1083 (2022).
12.
Agnelli G, Becattini C, Meyer G et al. Apixaban for the treatment of venous thromboembolism associated with cancer. N. Engl. J. Med. 382(17), 1599–1607 (2020).
13.
Young AM, Marshall A, Thirlwall J et al. Comparison of an oral factor Xa inhibitor with low molecular weight heparin in patients with cancer with venous thromboembolism: results of a randomized trial (SELECT-D). J. Clin. Oncol. 36(20), 2017–2023 (2018).
14.
Mazzolai L, Alatri A. Treatment of cancer-associated venous thromboembolism. (2023). (Accessed 11 November 2024). https://www.escardio.org/Councils/Council-for-Cardiology-Practice-(CCP)/Cardiopractice/treatment-of-cancer-associated-venous-thromboembolism
15.
Farge D, Frere C, Connors JM et al. 2022 International Clinical Practice Guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer, including patients with COVID-19. Lancet Oncol. 23(7), e334–e347 (2022).
• Provides insight on International Clinical Practice Guidelines from 2022 for the treatment and prophylaxis of venous thromboembolism (VTE) in patients with cancer.
16.
Falanga A, Ay C, Di Nisio M et al. Venous thromboembolism in cancer patients: ESMO clinical practice guideline. Ann. Oncol. 34(5), 452–467 (2023).
• Provides ESMO clinical practice guidelines for VTE in cancer patients.
17.
Key NS, Khorana AA, Kuderer NM et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO guideline update. J. Clin. Oncol. 41(16), 3063–3071 (2023).
• Provides information on the American Society of Clinical Oncology (ASCO) clinical practice guidelines for VTE prophylaxis and treatment in patients with cancer.
18.
Streiff MB, Holmstrom B, Angelini D et al. Cancer-associated venous thromboembolic disease, Version 2.2024, NCCN Clinical Practice Guidelines in Oncology. J. Natl Compr. Canc. Netw. 22(7), 483–506 (2024).
• Provides insight on the National Comprehensive Cancer Network (NCCN) Clinical practice guidelines in oncology, specifically regarding cancer associated with VTE.
19.
Wallerstedt SM, Wettermark B, Hoffmann M. The first decade with the Swedish Prescribed Drug Register – a systematic review of the output in the scientific literature. Basic Clin. Pharmacol. Toxicol. 119(5), 464–469 (2016).
20.
McBane RD 2nd, Wysokinski WE, Le-Rademacher JG et al. Apixaban and dalteparin in active malignancy-associated venous thromboembolism: the ADAM VTE trial. J. Thromb. Haemost. 18(2), 411–421 (2020).
21.
Planquette B, Bertoletti L, Charles-Nelson A et al. Rivaroxaban vs dalteparin in cancer-associated thromboembolism: a randomized trial. Chest 161(3), 781–790 (2022).
22.
Cunningham A, Stein CM, Chung CP et al. An automated database case definition for serious bleeding related to oral anticoagulant use. Pharmacoepidemiol. Drug Saf. 20(6), 560–566 (2011).
23.
Halvorsen S, Ghanima W, Fride Tvete I et al. A nationwide registry study to compare bleeding rates in patients with atrial fibrillation being prescribed oral anticoagulants. Eur. Heart J. Cardiovasc. Pharmacother. 3(1), 28–36 (2017).
24.
Halvorsen S, Johnsen SP, Madsen M et al. Effectiveness and safety of non-vitamin K antagonist oral anticoagulants and warfarin in atrial fibrillation: a Scandinavian population-based cohort study. Eur. Heart J. Qual. Care Clin. Outcomes 8(5), 577–587 (2022).
25.
Thygesen SK, Christiansen CF, Christensen S et al. The predictive value of ICD-10 diagnostic coding used to assess Charlson Comorbidity Index conditions in the population-based Danish National Registry of Patients. BMC Med. Res. Methodol. 11, 83 (2011).
26.
Quan H, Li B, Couris CM et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 173(6), 676–682 (2011).
27.
Khorana AA, Connolly GC. Assessing risk of venous thromboembolism in the patient with cancer. J. Clin. Oncol. 27(29), 4839–4847 (2009).
• Notes the importance of recognizing patients with cancer who are most at risk for VTE for effectively targeting thromboprophylaxis.
28.
Khorana AA, McCrae KR. Risk stratification strategies for cancer-associated thrombosis: an update. Thromb. Res. 133(Suppl. 2), S35–S38 (2014).
29.
Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 34(28), 3661–3679 (2015).
30.
Allan V, Ramagopalan SV, Mardekian J et al. Propensity score matching and inverse probability of treatment weighting to address confounding by indication in comparative effectiveness research of oral anticoagulants. J. Comp. Eff. Res. 9(9), 603–614 (2020).
31.
von Hippel PT. The heterogeneity statistic I(2) can be biased in small meta-analyses. BMC Med. Res. Methodol. 15, 35 (2015).
32.
Cohen AT, Dhamane AD, Liu X et al. Effectiveness and safety of extended treatment apixaban versus low-molecular-weight heparin in cancer-associated venous thromboembolism. J. Natl Compr. Canc. Netw. 22(6), 397–403 (2024).
33.
Cohen A, Keshishian A, Lee T et al. Effectiveness and safety of apixaban, low-molecular-weight heparin, and warfarin among venous thromboembolism patients with active cancer: a U.S. claims data analysis. Thromb. Haemost. 121(3), 383–395 (2021).
34.
Cohen AT, Keshishian A, Lee T et al. Effectiveness and safety of apixaban, LMWH, and warfarin among high-risk subgroups of VTE patients with active cancer. Curr. Med. Res. Opin. 37(9), 1467–1482 (2021).
35.
Streiff MB, Milentijevic D, McCrae K et al. Effectiveness and safety of anticoagulants for the treatment of venous thromboembolism in patients with cancer. Am. J. Hematol. 93(5), 664–671 (2018).
36.
Ludvigsson JF, Andersson E, Ekbom A et al. External review and validation of the Swedish national inpatient register. BMC Public Health 11, 450 (2011).
37.
Friberg L, Skeppholm M. Usefulness of health registers for detection of bleeding events in outcome studies. Thromb. Haemost. 116(6), 1131–1139 (2016).
38.
Herrett E, Thomas SL, Schoonen WM et al. Validation and validity of diagnoses in the General Practice Research Database: a systematic review. Br. J. Clin. Pharmacol. 69(1), 4–14 (2010).
39.
Knapp RK, Hardtstock F, Wilke T et al. Evaluating the economic burden of relapses in neuromyelitis optica spectrum disorder: a real-world analysis using German claims data. Neurol. Ther. 11(1), 247–263 (2022).
40.
Laugesen K, Ludvigsson JF, Schmidt M et al. Nordic health registry-based research: a review of health care systems and key registries. Clin. Epidemiol. 13, 533–554 (2021).
41.
Lyman GH, Carrier M, Ay C et al. American Society of Hematology 2021 guidelines for management of venous thromboembolism: prevention and treatment in patients with cancer. Blood Adv. 5(4), 927–974 (2021).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 13 May 2025
Accepted: 23 March 2026
Published online: 1 May 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative safety of direct oral anticoagulants and low-molecular-weight heparin in patients with venous thromboembolism and cancer in Europe. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0072
Export citation
Select the citation format you wish to export for this article or chapter.