Real-world evidence on the use of hospital resources for subcutaneous and intravenous trastuzumab administration in breast cancer patients at a referral public hospital in Mexico
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The availability of subcutaneous (SC) trastuzumab has introduced a practical alternative to traditional intravenous (IV) delivery for HER2-positive breast cancer. Beyond clinical equivalence, the shift toward SC administration offers the possibility of reorganizing workflow, reducing the pressure on infusion units and improving the treatment experience for both patients and healthcare professionals. This study provides real-world evidence from a large public oncology hospital in Mexico City, examining how SC and IV trastuzumab compare in everyday practice with respect to treatment times, resources use and the perceptions of patients and staff. Materials & methods: A prospective time and motion study was conducted to compare the efficiency and operational impact of SC and IV routes of trastuzumab administered as monotherapy in women with HER2-positive breast cancer at a public hospital in Mexico City. Sixty administrations (30 SC and 30 IV) were analyzed, recorded in real time using a digital system specifically developed for this study. The system documented waiting times, preparation, administration and time spent in the treatment room. Resource utilization was estimated based on the average number of supplies required for each route. In addition, patients and healthcare personnel completed structured questionnaires on comfort, satisfaction and overall experience. Results: Treatment using the SC route was noticeably shorter. Compared with the IV route, median chair time and overall procedure duration dropped by close to 94%, and treatment room occupancy decreased by approximately 83%. This route also required fewer materials and avoided the drug loss due to weight-based IV dosing. Patients described the SC injection as more comfortable and less fatiguing, while healthcare professionals noted less physical effort, lower stress levels and a more manageable workflow. Conclusion: In a routine public oncology setting with limited resources, the use of SC trastuzumab was associated with clear advantages in terms of efficiency and the treatment experience while also mitigating the workload of infusion areas. These results provide practical, context-specific evidence that could help healthcare systems to improve the organization of oncology services and make better use of scarce hospital resources.
Plain language summary: Intravenous or subcutaneous trastuzumab for women with cancer? A choice with impact on time, resources & comfort
What is this article about?
This article examines the time, hospital resources and overall experience involved in giving trastuzumab intravenously (IV) or subcutaneously (SC) to women with breast cancer in a large public hospital in Mexico. The study reflects real daily practice in a resource-limited setting.
What did the study do & what were the results?
Using a real-world time-and-motion approach, the study observed how trastuzumab is delivered during routine clinic operations. A digital system was used to document each step without placing observers in treatment areas or interrupting normal workflow.
Across 60 treatment sessions, the SC route showed clear advantages: shorter chair and preparation times, reduced staff workload, fewer supplies required and no drug waste.
Patients and healthcare staff also reported that the SC option felt more comfortable and less tiring.
What do these results mean & why are they important?
These findings highlight that choosing between IV and SC trastuzumab can meaningfully influence daily care. In public hospitals with limited resources, the SC route can ease pressure on staff, free up treatment chairs and help clinics run more efficiency.
For patients, shorter and simpler visits reduce fatigue; for staff, less preparation allows them to focus on essential tasks. Although the medication is the same, how it is delivery can make a real difference, especially in resource-constrained health systems. The results provided practical, real-world evidence to support more efficient and patient-centered care.
Breast cancer is the most common malignancy among women in Mexico and around the world [1]. For patients with human epidermal growth factor receptor 2-positive (HER2+) early breast cancer, trastuzumab has become a key component of treatment, offering substantial improvements in survival. Although it has long been administered intravenously (IV), a subcutaneous (SC) formulation is available. This alternative maintain comparable efficacy and bioavailability while requiring considerably less time to administer.
Several international studies – including HannaH and PrefHer and other studies comparing SC and IV administration – have shown that SC formulations reduces patient chair time and healthcare provider (HCP) workload while also yielding high satisfaction among both patients and HCPs [2–7]. One of the most illustrative examples is the work by De Cock et al. [8], which reported a marked reduction in both patient chair time and active HCP time with SC trastuzumab compared with IV administration. These studies suggest that using the subcutaneous administration route could help to streamline clinical workflows and reduce some of the operational costs associated with oncology services.
Another highly relevant aspect is patient preference. Reports suggest that patients generally find SC trastuzumab more convenient, especially in high-demand cancer centers. Nevertheless, evidence from routine settings in public hospitals in low- and middle-income countries with limited resources still needs to be gathered. Understanding how SC versus IV administration affects real clinical settings is therefore crucial for planning, evaluating and improving service delivery.
Our study addresses this gap by analyzing how the two routes of administration differ in terms of hospital resource use, treatment time and overall experience among patients and HCPs in a public oncology hospital in Mexico City.
Materials & methods
Study design
We conducted a prospective, observational time-and-motion study in adult women (≥18 years) with HER2-positive breast cancer who were receiving trastuzumab as monotherapy – either in the adjuvant setting or as part of palliative care. Eligibility was confirmed using clinical records to ensure that participants were on single-agent trastuzumab. Patients receiving concurrent chemotherapy or pertuzumab were not included. All participants provided informed consent prior to being included in the observational study.
Data collection platform (SMAM system)
Data were collected through the Time, Mobility, and Acceptance in Drug Administration Monitoring System (SMAM, for its initials in Spanish), a digital tool we developed specifically for this project. The platform was created to allow real-time and nonintrusive recording of each step of the administration process, so that information could be captured as the workflow naturally unfolded. Rather than relying on external observers, SMAM was operated directly by the clinical staff, which helped avoid interruptions and reduced the influence of having someone watch over the process.
SMAM brings together three complementary components. First, the Hospital-Reported Outcomes (HROMS) module documented practical aspects of the workflow, such as treatment room occupancy and the sequence of logistical steps. Second, Medical-Reported Outcomes (MROMS) module, consisted of short, standardized Likert-scale questionnaires completed by HCP, where they rated their levels of stress, fatigue, comfort and satisfaction while administering either IV or SC trastuzumab. Finally, the patient-reported outcomes (PROMs) module drew on data from post-treatment administration satisfaction questionnaires for intravenous (IV) and subcutaneous (SC) routes, capturing patients, perceptions of tolerability, convenience, and satisfaction. Because the objective of the study was strictly operational, we did not collect safety information, and questions regarding pain or local reactions were intentionally excluded. Our focus was to document the workflow as accurately as possible and to understand how both patients and clinical staff experienced each route of administration.
Participant & hospital characteristics
A total of 60 trastuzumab administrations were analyzed at the National Cancer Institute (INCan), Mexico City: 30 SC and 30 IV, all carried out according to standard institutional procedures. The unit of analysis in this study was the observed administration rather than the individual patient. Because the objective was to evaluate workflow processes under routine conditions, administrations were treated as independent operational events, and some participants may have contributed more than one observation.
The study populations consisted of adult women with HER2-positive breast cancer who were receiving trastuzumab as single-agent therapy, as outlined previously in the methods. Most patients had stage III disease at the time of observation. A small number of stage IV cases were also included, which reflects the day-to-day reality of a public oncology hospital. Because the focus of the study was operational-time metrics, resource use and user experience – these clinical differences did not influence the outcomes.
For patients receiving IV trastuzumab, vascular access varied: around 70% had a Por-a-Cath, 20% had peripherally inserted central catheters and roughly 10% received treatment through peripheral access. Although access type was registered because it can occasionally influence preparation time, no clear pattern suggesting a systematic impact on overall administration duration was apparent across the IV observations.
Measured end points
The primary end points of the study were designed to evaluate the efficiency and operational impact of each trastuzumab administration route. Before any data were collected, we worked with oncologists, nurses and pharmacy personnel from the preparation and infusion areas to map the full sequence of steps involved in both IV and SC administration. This collaborative review helped ensure that each step – beginning with patient arrival and ending with discharge – accurately reflected routine practice and minimized variability between observations. In parallel, clinical staff received brief, standardized training on the SMAM time-stamping interface and procedures. SMAM does not automatically infer HCP time per task; instead, time stamps were recorded in real time by staff through a simple usability-oriented workflow in which they selected the corresponding task template and actively confirmed task start and task completion (start/end). To minimize errors and support timely updates in a resource-constrained public hospital, the interface was designed for rapid input (few clicks, clear labels), and staff were instructed to record time stamps immediately at the point of care. Prior to study launch, we conducted short pilot tests to verify correct use of the system and proper functioning of the time-stamp recording process.
Once the workflow was validated, these steps were incorporated into the SMAM system as standardized templates for real-time time stamping and direct comparison between routes. Both treatments involve the same general workflow steps. However, the different routes of administration require specific tasks, so the number of tasks is not identical for the two treatments. Time metrics were defined using the workflow illustrated in Figure 1:
•
The waiting time (0–1): corresponds to the period between the patient’s arrival and admission to the treatment area.
•
Preparation time (2–6): this includes the time taken for verification processes and preparation of the formulation. In the case of IV treatment only, it also includes the time taken for venous access placement. This refers only to venous access procedures performed as part of routine same-day preparation, such as placement of peripheral venous access, and does not include surgical placement of long-term central access devices performed outside the treatment workflow.
•
Treatment administration time (7–9): corresponds to the interval between the start and end of drug administration.
•
Treatment room time (2–14): total time spent in the treatment area, encompassing preparation, treatment administration, monitoring (10–13) and patient exit (14).
•
Total hospital time (0–14): total time the patient spends undergoing treatment, from waiting time to exit.
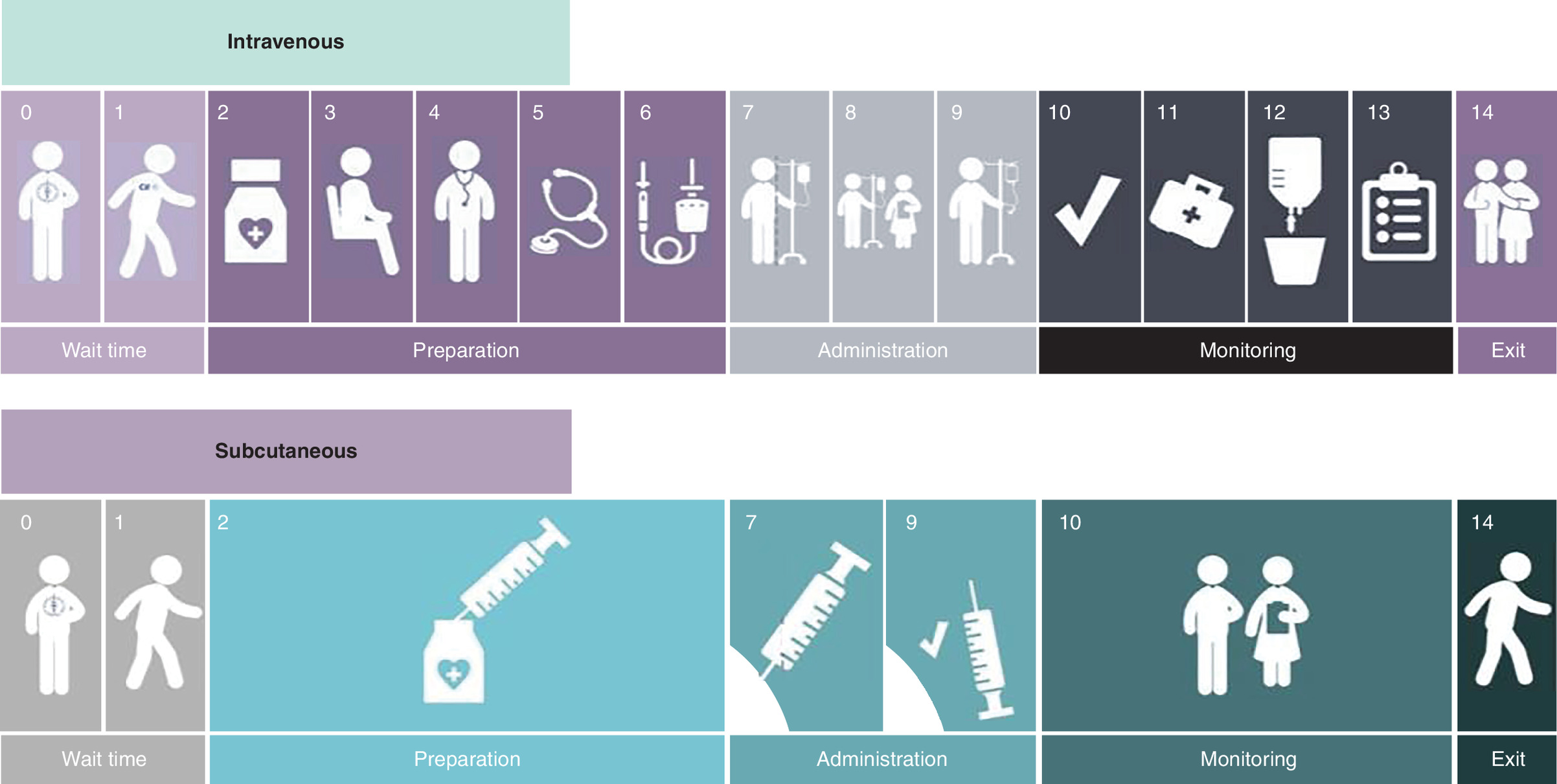
Figure 1. Workflow for intravenous and subcutaneous trastuzumab administration at a referral public hospital in Mexico.
The figure depicts the general workflow steps followed for intravenous and subcutaneous trastuzumab administration, as well as the differences in the number of tasks involved in the process.
Hospital resource utilization was documented as the average number of consumables and disposables required for each administration route. Descriptive analyses were also conducted for the patient-reported (PROMs) and medical staff-reported outcomes (MROMs) associated with each route.
Furthermore, exploratory analyses were also conducted to examine elements that could affect the efficiency of the workflow process under routine conditions. These include the level of experience and training of HCPs, the cycle number in which the observation took place and whether there were any interruptions or unusual events. Patient-related factors were also considered, such as whether the patient had venous access, and if so, what type (Port-a-Cath, peripherally inserted central catheters line or peripheral access). It was also considered whether the patient had any mobility limitations that could influence the progress of the workflow.
Sample size considerations
Given the variability that naturally arises in real-world hospital environments, no formal sample size calculation was attempted. Instead, we adopted a pragmatic target of 30 patients per group, an approach consistent with earlier time-and-motion studies [8], where sample sizes vary considerably depending on workflow availability and the number of observable administrations under real-world conditions, and sufficient for nonparametric group comparisons such as the Mann–Whitney U test. This sample size allowed us to capture the operational diversity of a public oncology service while keeping the study feasible and representative of routine practice in the Mexican public healthcare system.
Cost data
Consumable costs were estimated using average unit prices obtained from major medical supply distributors in Mexico during 2023–2024. For each item -syringes, needles, IV catheters, infusion sets, saline bags- we calculated a mean unit price and applied it to determine the per-procedure cost. This approach reflects typical procurement conditions in public hospitals, while acknowledging that prices may vary by institution, purchasing contracts or year. All costs are presented in Mexican pesos (MXN).
Statistical analysis
All statistical analyses were performed using Python. Data distribution was assessed with the Shapiro–Wilk test, and because variables did not follow a normal distribution, comparisons between IV and SC groups were carried out with the Mann–Whitney U test. Statistical significance was defined as p < 0.05. Descriptive statistics – median, interquartile range IQR, mean and standard deviation (SD) – were used to support interpretation of the findings.
Extrapolation into real-world numbers
To estimate the potential system-level impact, time and cost differences observed in the study were extrapolated to the population of HER2-positive early breast cancer patients treated in Mexico’s public healthcare institutions. The model assumed 18 trastuzumab cycles per patient and incorporated national epidemiologic data to approximate cumulative savings in patient time, HCP workload and hospital resources.
All data were collected as described using the SMAM digital platform and analyzed according to the predefined end points and statistical procedures.
Results
A total of 60 trastuzumab administrations were analyzed, 30 delivered SC and 30 IV, all carried out under standard institutional procedures. Baseline characteristics of the participating patients and the hospital setting are shown in Table 1. As planned, the study centered on operational outcomes – time metrics, resource utilization and satisfaction – rather than clinical efficacy or safety, since all treatments formed part of routine care.
| Cancer stage | IV | SC | Percentage (%) |
|---|---|---|---|
| I | 1 | 0 | 1.67 |
| II | 7 | 4 | 18.33 |
| III | 10 | 16 | 43.33 |
| IV | 12 | 10 | 36.67 |
| Total | 30 | 30 | 100 |
IV: Intravenous; SC: Subcutaneous.
Primary outcomes
Patient time metrics
SC administration of trastuzumab was noticeably faster than the IV route (Table 2). Median treatment chair time was 3.6 min for SC trastuzumab compared with 62.4 min for IV infusion, representing a 94% reduction (p < 0.0001). This large difference reflects the contrast between a single fixed-dose injection and the longer, weight-adjusted infusion required for IV delivery (Figure 2A).
| Stages | Description | IV | SC | Difference (h:min:s) |
|---|---|---|---|---|
| 2–6 | Preparation time | 0:17:32 | 0:02:51 | 0:14:41 |
| 7–9 | Treatment administration time | 1:02:24 | 0:03:36 | 0:58:48 |
| 2–14 | Treatment room time | 1:36:49 | 0:16:36 | 1:20:13 |
IV: Intravenous; SC: Subcutaneous.
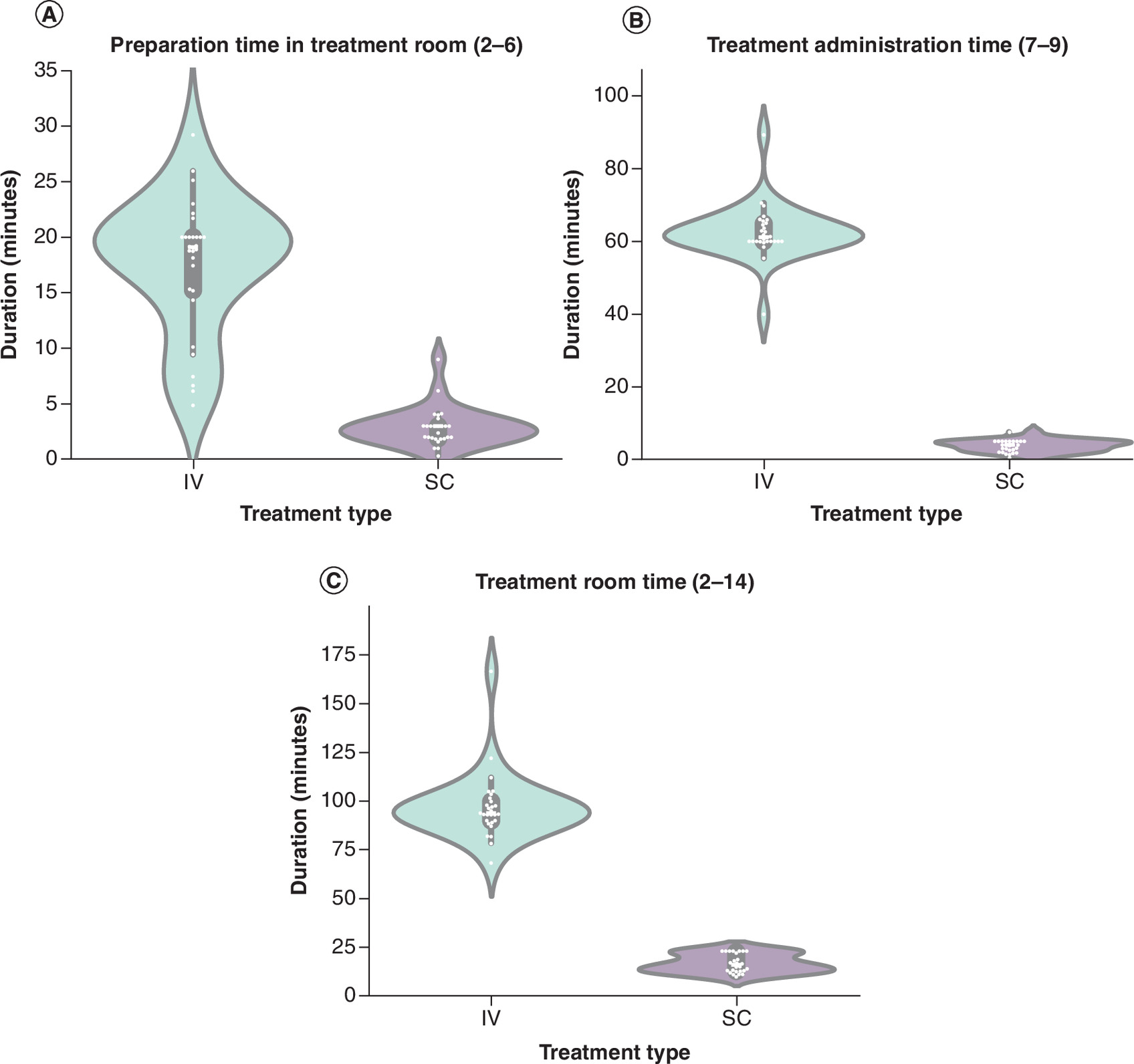
Figure 2. Comparison of patient time metrics between intravenous and subcutaneous trastuzumab administration.
Panels show (A) preparation time in the treatment room, (B) treatment administration time and (C) total treatment room time. Median times and statistical comparisons were calculated using the Mann–Whitney U test; p < 0.0001 for all comparisons.
IV: Intravenous; SC Subcutaneous.
The time patients occupied the treatment room follow a similar pattern. Median treatment room time was 16.6 min for SC administration compared with 96.8 min for IV, representing an 83% reduction or roughly 80 min saved per session (p < 0.0001) (Figure 2B). Much of this gap stemmed from shorter preparation demands.
Mean preparation time, which includes verification steps and venous access setup for IV administration, was 17.5 min for IV compared with 2.9 min for SC, corresponding to an 84% reduction (p < 0.0001) (Figure 2C). The shorter preparation period and the brief injection time together explain the markedly reduced room occupancy for SC administration (Figure 2C).
Taken together, these findings show that the SC route simplifies several workflow phases – preparation, drug delivery and overall chair time – leading to meaningful reductions in technical demands and patient time on site. These differences have direct implications for patient experience, clinic throughput and operational efficiency
HCP time metrics
Nursing staff contributed the largest portion of administration time in both groups, but their involvement was substantially shorter in the SC arm because the procedure requires far fewer steps than IV delivery. In contrast, IV administration entails establishing venous access, initiating and supervising the infusion and completing line flushing, all of which extend nursing time considerably.
Pharmacist and pharmacy assistant workload showed a similar pattern. Since weight-based calculations or individual preparation of vials are not required for the SC trastuzumab administration, medication preparation time was reduced. The physician’s involvement was mainly limited to patient assessment and brief supervision for both routes, with no notable differences observed.
It is worth noting that much of the IV drug preparation occurred before the patient even arrived in the treatment area – often during early shifts – and those tasks were not fully captured by the patient-facing observation protocol. As a result, the estimates reported here may underestimate the actual preparation burden for the IV route, which further highlights the relative efficiency of SC administration.
Secondary outcomes
Hospital time metrics
Total hospital time spent in the hospital – from arrival to exit – was shorter for patients receiving SC trastuzumab than for those treated intravenously. Median total hospital time was 162.8 min for SC patients compared with 226.5 min for IV administration, a reduction of 63.6 min per visit (Figure 3A).
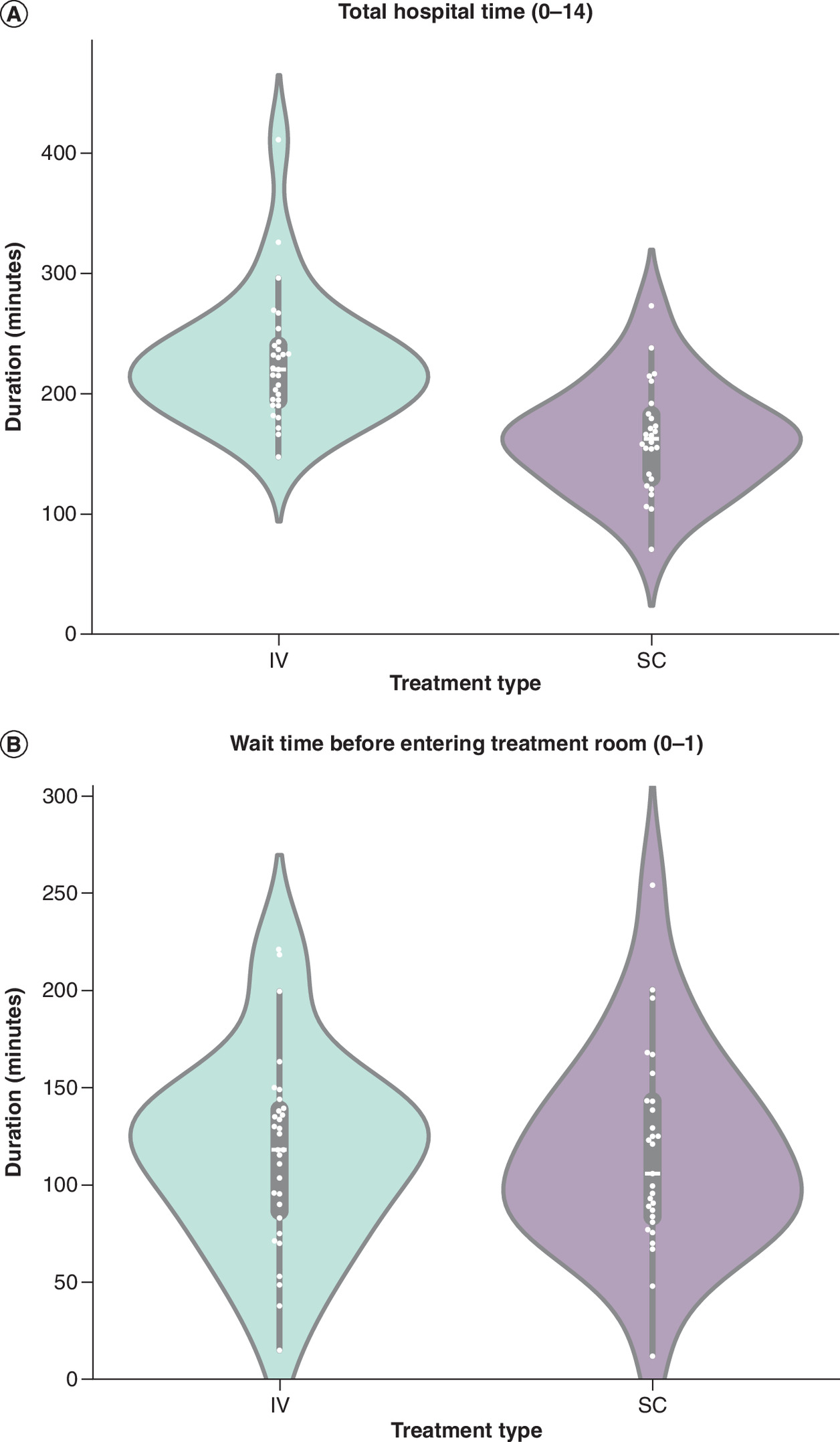
Figure 3. Comparison of total hospital time and waiting time between intravenous and subcutaneous trastuzumab administration.
Panels show (A) total hospital time, from arrival to discharge, and (B) waiting time prior to entering the treatment room. Median values and statistical comparisons were calculated using the Mann–Whitney U test.
IV: Intravenous; SC Subcutaneous.
In both groups, patients spent a significant amount of time waiting to enter the treatment room as median waiting time was approximately 2 h regardless of the route of administration (p = 0.784) (Figure 3B). Although administration time was shorter for SC, the total length of hospital stay was mainly determined by prior logistical steps rather than the administration procedure itself.
Together, these findings suggest that the operational advantages of SC trastuzumab are concentrated within the treatment unit, while total hospital time is more strongly influenced by institutional workflow and patient flow management.
Resource utilization
SC administration required far fewer consumables than the IV route, largely because it avoids the need for infusion lines, saline bags and flushing systems. On average, SC administration used nine material units per session, compared with 17 for IV administration. The cost difference was substantial as well: MXN $4.97 per SC application versus MXN $107.80 for IV (Table 3).
| Consumables | IV | SC | Cost per piece (MXN) |
|---|---|---|---|
| Swab | 3 | 4 | $0.065 |
| Syringe 1 ml | – | 1 | $0.93 |
| Needle 25 G x 16 | – | 1 | $0.90 |
| Sterile glove | 2 | 2 | $1.25 |
| Face mask | 1 | 1 | $0.38 |
| Sterile drape | 2 | – | $11.00 |
| Large gauze | 1 | – | $2.15 |
| Medium gauze | 2 | – | $0.49 |
| Small gauze | 1 | – | $0.45 |
| IV catheter 20–22 G | 1 | – | $12.50 |
| Patch | 1 | – | $1.50 |
| Infusion line with filter | 1 | – | $27.84 |
| Saline solution 0.9% 100 ml | 2 | – | $18.65 |
| Total | $107.795 | $4.970 |
G: Gauge; IV: Intravenous; SC: Subcutaneous.
Most of this gap came from IV-specific supplies – infusion tubing, saline solution, sterile drapes and venous catheters – none of which were needed for the SC injection. By contrast, the subcutaneous route requires only a 1 ml syringe and a fine-gauge needle, as well as the standard protective materials used by both groups.
Notable differences were also observed in terms of medication waste. With IV delivery, where the dose is adjusted according to the patient’s weight, it is common for part of the vial to remain unused after preparation. In contrast, the fixed dose used in the SC route did not generate product remnants. Consequently, the SC route was more economical in routine hospital practice as it required fewer materials and made better use of resources.
Satisfaction & acceptance in patients
Patient-reported satisfaction and convenience scores were higher for the SC route across all nine survey items. Four domains showed statistically significant differences (p < 0.05). Patients receiving SC trastuzumab were more likely to report gaining time for other daily activities (U = 634.5, p = 0.000009; Figure 4A) and expressed a stronger overall preference for SC over IV administration (U = 212.0, p = 0.0012; Figure 4B). They also felt they had more time available to communicate with healthcare professionals (U = 303.0, p = 0.030; Figure 4C) and were more inclined to recommend their mode of treatment to others (U = 525.0, p = 0.0011; Figure 4D).
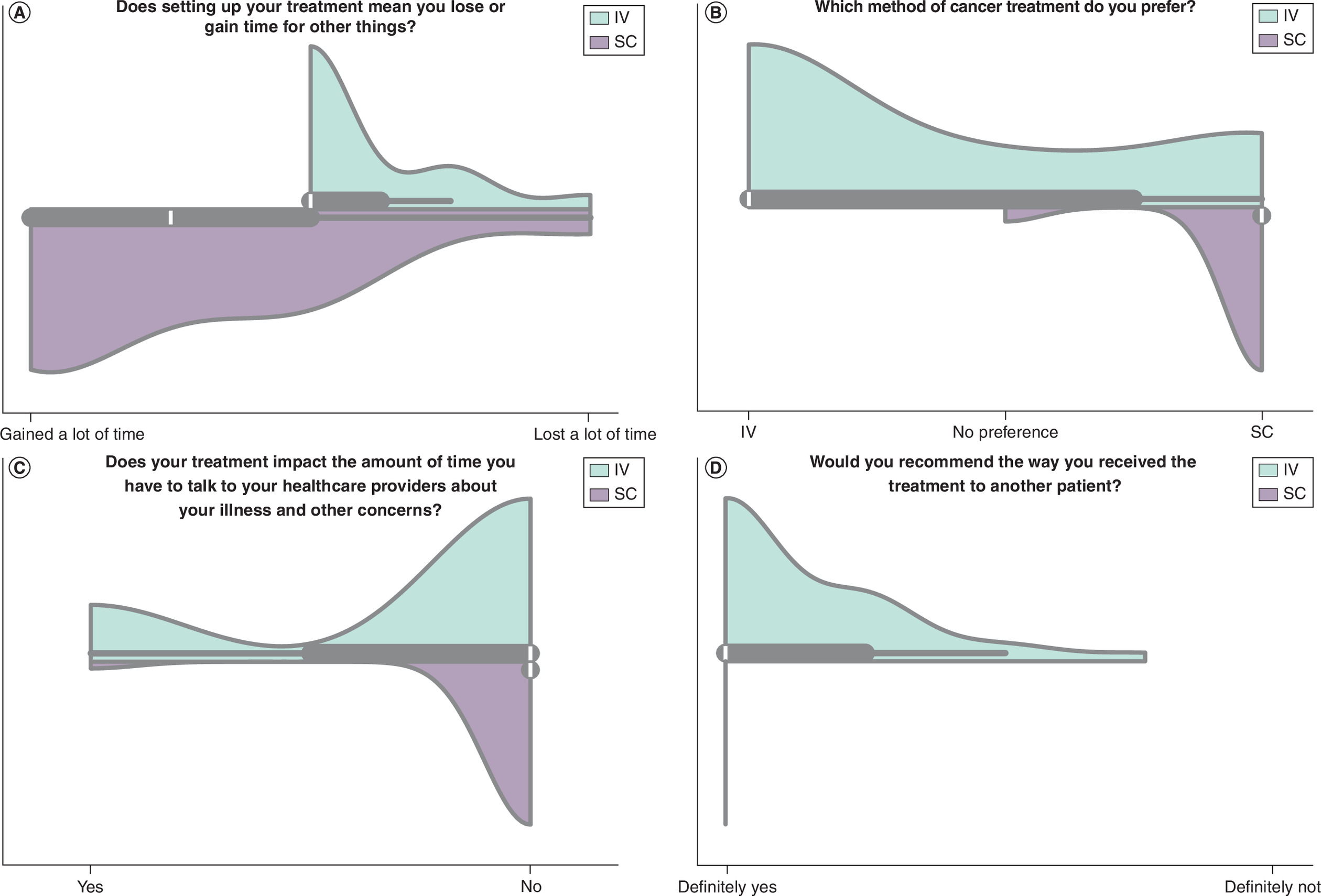
Figure 4. Patient-reported outcomes for intravenous and subcutaneous trastuzumab administration.
Panels show the median scores across nine survey domains. Statistically significant differences were observed for (A) perceived time gained for other activities (U = 634.5, p < 0.000009); (B) preference for the route of administration (U = 212.0, p = 0.0012); (C) impact on communication time with healthcare professionals (U = 303.0, p = 0.030) and (D) likelihood of recommending the treatment to other patients (U = 525.0, p = 0.0011). Other survey items showed higher median values for the SC delivery, but these differences were not statistically significant (p > 0.05).
IV: Intravenous; SC Subcutaneous.
Although scores for satisfaction, convenience, perceived restrictions, time-related bother and communication tended to favor SC as well, these additional differences did not reach statistical significance (p > 0.05). Overall, patients viewed SC administration as the more practical option, with a smaller impact on their daily routines.
Satisfaction & acceptance in HCP
HCP responses followed the same pattern observed in patients, with all four survey items showing statistically significant differences in favor of SC administration. Compared with IV trastuzumab, HCPs reported feeling less fatigue during SC sessions (median score 9.57 vs 8.25; U = 625.0, p = 0.0011) and described lower levels of stress (9.31 vs 8.75; U = 576.5, p = 0.0234). They also rated SC administration as more comfortable (9.83 vs 7.58; U = 706.0, p = 0.000005) and expressed higher overall satisfaction with the procedure (10.0 vs 8.42; U = 609.0, p = 0.0005) (Table 4).
| Treatment type | IV | SC |
|---|---|---|
| When you applied the treatment, how tired did you feel? (10 = not tired at all) | 8.25 | 9.57 |
| When you applied the treatment, how stressed did you feel? (10 = not stressed at all) | 8.75 | 9.31 |
| How comfortable was applying the treatment for you? (10 = very comfortable) | 7.58 | 9.83 |
| How satisfied were you with applying treatment? (10 = very satisfied) | 8.42 | 10 |
IV: Intravenous; SC: Subcutaneous.
Taken together, these findings indicate that the benefits of SC delivery extend beyond patients. By reducing physical effort and stress for staff, SC administration supports a more manageable workload and contributes to a more sustainable and efficient care environment in oncology practice.
Discussion
This study demonstrates that SC administration of trastuzumab offers clear operational advantages over IV delivery in the Mexican public healthcare setting. The SC route was found to be associated with shorter preparation and administration times, greater patient acceptance and a more manageable workflow, as was also found in international studies including the HannaH and PrefHer trials. Our study contributes evidence generated under routine conditions in a Latin American public hospital. This setting differs markedly from those in which most comparative evaluations have been conducted, as it experiences infrastructure limitations and severe HCPs pressures.
The significant reduction in preparation and administration time, as seen with the SC route, has practical implications for both patients and the institution. According to our observations, patients who received SC trastuzumab had substantially shorter median treatment room times (-83%), resulting in shorter visits and a more manageable treatment experience. Reports from HCPs followed the same pattern: those involved in SC administration reported lower levels of fatigue and stress, and greater overall comfort. This suggests that the simpler procedure associated with switch in administrations routes may alleviate demands on both staff and patients.
When projected over the 18 cycles typically used in the adjuvant setting, the SC route results in an estimated saving of around 24 h of trastuzumab treatment-related time per patient. Furthermore, given the annual incidence of HER2-positive breast cancer in Mexican women, the potential benefit is significant: the public health system could liberate over 114,000 h of treatment annually, equivalent to around 1100 standard chemotherapy sessions. This estimate was derived from extrapolating the time differences observed in this study to national incident data for HER2-positive breast cancer reported in Mexican registries [9,10]. Although these calculations are based on the assumption of full adoption of the SC formulation and consistent efficiency across all institutions, they illustrate the potential magnitude of a widespread transition at system level. While our study did not include a formal economic evaluation, future work should consider the budgetary implications of wider use of the SC trastuzumab formulation.
These operational advantages align with the fundamental principles of value-based healthcare. By reducing time and resource requirements while maintaining clinical equivalence, the SC formulation offers patients meaningful benefits, such as greater comfort, ease of use and reduced interference with daily activities. It also contributes to a more manageable work environment for HCPs. The efficiency gains observed in our study suggest that changing the route of administration can promote patient-centered care and make better use of institutional resources in Mexico.
Importantly, our findings suggest that the benefits of SC administration are not limited to the individual treatment event but can influence how the entire treatment unit operates. Because SC trastuzumab requires shorter preparation and administration times and involves fewer personnel steps than IV workflows, treatment chairs can become available sooner and clinical staff can move more quickly between patients. In routine practice, waiting times often reflect the cumulative duration of multiple treatments in the unit. Therefore, reducing the time required for each administration may contribute to smoother patient flow and more efficient use of clinical resources. For public oncology services with limited resources, adopting SC formulations has the potential not only to reduce treatment-related time but also to facilitate more agile management of patient flow at the system level.
From a policy perspective, these results impact decisions regarding reimbursement, purchasing strategies and the distribution of resources within Mexico’s public oncology system. Although trastuzumab is already included in national clinical guidelines, our findings suggest that the SC formulation could be considered as an alternative that is more efficient than the IV route.
An additional consideration relates to the acquisition cost of SC trastuzumab compared with IV biosimilars currently available in México, which may influence the overall economic interpretation of these findings depending on local procurement conditions. Although drug acquisition costs were not available for direct analysis in this study due to institutional variability and restricted access to pricing information, it is important to recognize that IV administration typically involves additional resource utilization, including infusion materials, longer staff engagement and extended chair occupancy. While our study focused on operational efficiency and consumable use rather than cost modelling, future economic evaluations integrating acquisition costs and reimbursement structures would provide a more comprehensive assessment of value within the Mexican public healthcare system.
More broadly, this work underscores the potential of relatively simple innovations, such as changing the mode of administration, to generate measurable value, particularly in settings where staffing shortages and limited infusion capacity challenge the sustainability of oncology services.
Beyond time savings, SC administration was associated with reduced drug wastage and substantially lower consumable use. Fixed-dose SC trastuzumab eliminates the residual discard inherent to weight-based IV dosing and avoids the need for infusion lines, saline bags and venous access materials. In the present study, vial sharing was not observed during routine practice. However, coordinate scheduling strategies could theoretically enable vial sharing in settings where treatment sessions are aligned, which may further reduce medication wastage. Together, these efficiencies may strengthen the case for SC delivery as a cost-conscious strategy for resource-limited healthcare systems.
Patient and HCP feedback reinforced these operational findings. SC administration consistently achieved higher satisfaction scores across all survey items, with significant advantages in perceived time savings, communication opportunities, treatment preference and willingness to recommend the therapy. All HCP-reported domains – fatigue, stress, comfort and overall satisfaction – favored SC as well, echoing previous reports that associate SC formulations with reduced physical strain and improved professional well-being [11–14]. Within a value-based healthcare (VBHC) framework, such perceptions reflect outcomes that matter to both patients and professionals, contributing to higher-quality, more sustainable oncology services.
This study has limitations. Its observational design enhances real-world relevance but introduces potential confounders, including variability in nurse experience, patient comorbidities and institutional workflow dynamics. The two pathways were found to differ in several ways, but these results are only reliable to the extent that our sample size allowed us to detect them. It is possible that more subtle variations in patient reports would not have been detected even if we had had a larger sample size. The use of Likert-type items, which tend to generate high scores across all categories, may also have reduced our ability to identify statistically significant contrasts. As the study was conducted at a single, high-volume referral center, it is unclear to what extent these results can be applied to smaller or less well-resourced hospitals.
The workload associated with IV preparation may be underestimated as a substantial portion of these activities occurs before the patient arrives to the treatment area and was therefore not fully captured in the observation window. This limitation likely affects IV workflows more than SC administration, which requires minimal advance preparation and is typically performed at chairside. Consequently, the operational differences observed between SC and IV administration in this study likely represent a conservative estimate of the true system-level impact. Because IV processes generally involve broader personnel participation and longer preparation pathways, the real-world benefits of SC administration may be greater than those measured here, particularly in terms of staff utilization, chair turnover and overall treatment-unit efficiency. Moreover, differences in the number of treatment cycles between groups, reflecting actual scheduling rather than study design, may have influenced some aspects of patient satisfaction.
Even with these limitations, the results of this study provide real-world evidence that SC trastuzumab is a valuable treatment option for HER2-positive breast cancer in Mexico’s public healthcare system. In addition to maintaining clinical equivalence, it offers practical advantages such as a more efficient use of hospital resources, a better treatment experience for patients and a more manageable workload for HCPs. These are all crucial considerations for improving access, equity and efficiency in cancer care.
Our results are consistent with those of other studies which have reported a reduction in chair time and workload for HCPs when SC trastuzumab is used. López-Vivanco et al. [15] documented a reduction in HCP active time per cycle of around half, while De Cock et al. [8] described equally significant decreases in patient chair time and staff effort. Taken together, these studies suggest that the operational benefits of the subcutaneous route are consistent and can be replicated in various healthcare settings.
Equity and access would also be impacted by the transition to subcutaneous administration. Shorter treatment sessions could be a good solution for public systems that are operating at limited capacity. This is because they would mean more appointment slots and would help to reduce delays for patients. Despite our assessment focusing on trastuzumab, other monoclonal antibodies with SC formulations could offer comparable advantages. Hence, there is a broader opportunity to strengthen cancer care in settings with limited resources.
Conclusion
This study provides real-world evidence that SC administration of trastuzumab is an effective alternative to intravenous administration for treating HER2-positive breast cancer within Mexico’s public hospital system. In routine practice, this method was associated with significant reductions in treatment time, HCPs workload, consumable use and medication waste. Furthermore, both HCPs and patients reported a more comfortable and satisfactory experience with the subcutaneous route.
Although statistical significance was not reached by some comparisons, the overall pattern observed across operational measures and patient- and staff-reported experiences points to benefits of the subcutaneous route that extend beyond clinical equivalence. This study provides evidence that is directly relevant to the working conditions and limitations of public oncology services in Latin America by examining these effects in day-to-day practice rather than in a controlled trial environment.
Expanding the use of SC trastuzumab in routine cancer care could increase treatment capacity, reduce demand for infusion units and support the long-term sustainability of cancer services. From a health policy perspective, our findings suggest that subcutaneous formulations should be considered within reimbursement mechanisms, that HCPs should be strengthened, and that formal cost–effectiveness evaluations should be conducted to inform broader adoption. This could help Mexico’s public cancer system to make better use of scarce resources and promote greater efficiency, equity and value.
Summary points
•
This study compared the use of intravenous (IV) and subcutaneous (SC) trastuzumab in routine care at a large public hospital in Mexico.
•
A real-world time-and-motion approach and a digital system that was developed ad hoc were used to document how each formulation fits into everyday clinical workflow.
•
SC trastuzumab reduced both chair time and preparation time compared with the IV route.
•
The SC option resulted in a lighter workload for healthcare professionals.
•
SC administration required fewer supplies and resulted in no drug waste.
•
Patients and healthcare staff described the SC route as more comfortable and less tiring during busy clinic days.
•
As the study was conducted without controlled groups or disruption to normal operations, the findings reflect real conditions in a resource-limited oncology service.
•
These results provide practical evidence that SC trastuzumab can enhance efficiency and the overall care experience in public health systems.
Author contributions
T Fiordelisio conceived the study, designed its overall structure, supervised all phases of the work, contributed to data interpretation and critically reviewed the manuscript. F Valdés-Souto, K Ramírez, C Escamilla, Y Correa, CI Gutiérrez and I Espino contributed to the development and implementation of the data acquisition system, participated in hospital-based data collection and took part in the critical revision of the manuscript; F Valdés-Souto and K Ramírez also contributed to data analysis and processing. D Zamarrón supported data acquisition, processing, analysis and interpretation, contributed to the methodological approach, and participated in the critical review of the manuscript. Diana del-Río contributed to the organization and interpretation of the data and collaborated in drafting and revising the manuscript. CH Arce facilitated coordination within the hospital, supervised on-site data acquisition activities and contributed to the critical review and validation of the manuscript. All authors reviewed and approved the final version of the manuscript and agree to take joint responsibility for the integrity of the work.
Acknowledgments
We are grateful to the Laboratorio Nacional de Soluciones Biomiméticas para Diagnóstico y Terapia (LANSBIODYT) for their technical assistance at diverse stages of this project. We would also like to thank the healthcare personnel at the National Institute of Cancerology, whose collaboration and commitment to patient care on a daily basis greatly facilitated the development of this study. Above all, we would like to acknowledge the patients who took part in this study and hope for their continued recovery and well-being.
Financial disclosure
This work was funded by F. Hoffmann–La Roche Ltd (México) under a contract with the Facultad de Ciencias, UNAM. The sponsor had no role in the design, conduct, data collection, analysis, interpretation, manuscript writing or decision to submit the manuscript. No author received personal payments for this work.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
We used artificial intelligence-assisted tool ChatGPT exclusively for language editing and style refinement.
Ethical conduct of research
The study relied on observational data from routine clinical practice. All participants provided informed consent. As this was a noninterventional time-and-motion study, formal ethics committee approval was deemed unnecessary by the institution.
Data availability statement
The authors certify that this manuscript reports the original results of a real-world evidence study. The protocol was not preregistered. De-identified data and analytical code can be requested from the corresponding author, subject to ethical and institutional requirements.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Ferlay J, Soerjomataram I, Dikshit R et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 136(5), E359–E386 (2015).
2.
Stoner KL, Harder H, Fallowfield LJ, Jenkins VA. Intravenous versus subcutaneous drug administration. Which do patients prefer? A systematic review. Patient doi: (2014) (Epub ahead of print).
3.
McCloskey C, Ortega MT, Nair S, Garcia MJ, Manevy F. A systematic review of time and resource use costs of subcutaneous versus intravenous administration of oncology biologics in a hospital setting. Pharmacoecon. Open 7(1), 3–36 (2023).
•• This systematic review analyses international evidence on time, resource use and operational efficiencies when oncology biologics are administered subcutaneously instead of intravenously.
4.
Shapiro RS. Why I use subcutaneous immunoglobulin (SCIG). J. Clin. Immunol. 33(Suppl. 2), S95–S98 (2013).
5.
Falanga M, Canzona A, Mazzoni D. Preference for subcutaneous injection or intravenous infusion of biological therapy among Italian patients with SLE. J. Patient Exp. 6(1), 41–45 (2019).
6.
Harvey MJ, Zhong Y, Morris E, Beverage JN, Epstein RS, Chawla AJ. Assessing the transition from intravenous to subcutaneous delivery of rituximab: benefits for payers, health care professionals, and patients with lymphoma. PLoS One 17(1), e0261336 (2022).
7.
De Cock E, Kritikou P, Sandoval M et al. Time savings with rituximab subcutaneous injection versus rituximab intravenous infusion: a time and motion study in eight countries. PLoS ONE 11(6), e0157957 (2016).
8.
De Cock E, Pivot X, Hauser N et al. A time and motion study of subcutaneous versus intravenous trastuzumab in patients with HER2-positive early breast cancer. Cancer Med. 5(3), 389–397 (2016).
•• This multinational, multicenter time-and-motion substudy of PrefHer compared subcutaneous (SC) and intravenous (IV) trastuzumab in controlled cohorts. Conducted in middle- to high-income healthcare systems, it provides a key operational benchmark for studies like ours.
9.
Arceo-Martínez MT, López-Meza JE, Ochoa-Zarzosa A, Palomera-Sanchez Z. Estado actual del cáncer de mama en México: principales tipos y factores de riesgo. Gac. Mex. Oncol. 20(3), (2021).
10.
Instituto Nacional de Estadística y Geografía (INEGI). Estadísticas a propósito del Día Internacional de la lucha contra el cáncer de mama (19 DE OCTUBRE). AguascalientesMéxico (2023). Available at: https://www.inegi.org.mx/contenidos/saladeprensa/aproposito/2023/EAP_CMAMA23.pdf
11.
Bittner B, Richter W, Schmidt J. Subcutaneous administration of biotherapeutics: an overview of current challenges and opportunities. BioDrugs 32(5), 425–440 (2018).
12.
Pivot X, Gligorov J, Müller V et al. Patients' preferences for subcutaneous trastuzumab versus conventional intravenous infusion for the adjuvant treatment of HER2-positive early breast cancer: final analysis of 488 patients in the international, randomized, two-cohort PrefHer study. Ann. Oncol. 25(10), 1979–1987 (2014).
13.
Jackisch C, Müller V, Dall P et al. Subcutaneous trastuzumab for HER2-positive breast cancer – evidence and practical experience in 7 German centers. Geburtshilfe Frauenheilkd. 75(6), 566–573 (2015).
14.
Cicin İ, Oukkal M, Mahfouf H et al. An open-label, multinational, multicenter, Phase IIIb study with subcutaneous administration of trastuzumab in patients with HER2-positive early breast cancer to evaluate patient satisfaction. Eur. J. Breast Health 18(1), 63–73 (2022).
15.
Lopez-Vivanco G, Salvador J, Diez R et al. Cost minimization analysis of treatment with intravenous or subcutaneous trastuzumab in patients with HER2-positive breast cancer in Spain. Clin. Transl. Oncol. 19(12), 1454–1461 (2017).
• This Spanish PrefHer substudy compared SC and IV trastuzumab by measuring healthcare provider time and calculating related staff costs, thereby highlighting differences in workflow-driven economics.
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 4 December 2025
Accepted: 23 March 2026
Published online: 20 April 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-world evidence on the use of hospital resources for subcutaneous and intravenous trastuzumab administration in breast cancer patients at a referral public hospital in Mexico. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0199
Export citation
Select the citation format you wish to export for this article or chapter.