Comparative safety and effectiveness of direct oral anticoagulants and warfarin in patients with venous thromboembolism in Finland, Norway and Sweden
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Clinical trial data have demonstrated that direct oral anticoagulants (DOACs) are both noninferior to and safer than conventional therapy for the treatment of venous thromboembolism (VTE). This study aimed to compare the effectiveness and safety of DOACs versus warfarin using Nordic population-based registries. Materials & methods: This observational cohort study used Swedish, Norwegian and Finnish national administrative data from 2012 to 2018. We identified treatment-naive adult patients with noncancer-related VTE treated with either a DOAC (apixaban or rivaroxaban) or warfarin. We employed inverse probability of treatment weighting for each DOAC-warfarin comparison and assessed the risks of bleeding (overall and by site: gastrointestinal bleeding [GI], intracranial bleeding [ICH], or other bleeding) and recurrent VTE within 6 months after treatment initiation. Cox proportional hazards models estimated the adjusted hazard ratios of each end point. Country estimates were combined using meta-analyses. Results: After inverse probability of treatment weighting, 22,450 warfarin, 14,542 apixaban and 23,002 rivaroxaban patients were included. At 6 months, for apixaban versus warfarin, the risk of bleeding was lower overall (hazard ratio: 0.51 [95% CI: 0.43, 0.61]) and by site (GI: 0.65 [0.45, 0.93]; ICH: 0.58 [0.34, 0.97]; other: 0.45 [0.34, 0.58]). For recurrent VTE the risk was similar for apixaban versus warfarin (0.85 [0.71, 1.02]). For rivaroxaban versus warfarin the risk of bleeding was lower for overall and other bleeding (0.86 [0.75, 0.99]; 0.81 [0.69, 0.95], respectively), but similar for GI and ICH bleeding (1.06 [0.84, 1.34]; 0.68 [0.47, 1.00], respectively). For recurrent VTE the risk was lower for rivaroxaban versus warfarin (0.74 [0.63, 0.87]). Conclusion: DOACs showed improved safety and at least similar effectiveness compared with warfarin, which is in line with clinical trial estimates.
Venous thromboembolism (VTE) is a major cause of mortality and morbidity [1]. A broad array of populations, including older people, those undergoing surgery, and those experiencing periods of immobilization, have an increased risk of VTE (includes pulmonary embolism [PE] and deep vein thrombosis [DVT]); therefore, it is a major public health concern [2]. The annual incidence rates for PE vary between 39 and 115 cases per 100,000 population, and reports from the Nordics estimate an incidence of 60–67 cases per 100,00 population [3,4]. Similarly, the incidence rates for DVT range from 53 to 162 cases per 100,000 population [5,6]. A recent systematic literature review and meta-analysis reported that among individuals presenting with an initial episode of unprovoked VTE, 10% would experience a VTE recurrence within the first year after treatment, 16% within 2 years, 25% within 5 years and 36% within 10 years. It is noteworthy that 4% of these recurrent VTE (rVTE) occurrences resulted in death [7].
Oral anticoagulant (OAC) therapy using vitamin K antagonists (VKAs), particularly warfarin, has traditionally been the established method of treatment for VTE. However, these agents require routine monitoring of the international normalized ratio (INR), have food and drug interactions, and are linked to increased risks of major bleeding and clinically relevant nonmajor bleeding [8]. In more recent years, direct-acting non-VKA OACs (DOACs), including apixaban, dabigatran, edoxaban and rivaroxaban, have received global approval as viable alternatives to warfarin. Clinical trials have demonstrated that these medications are noninferior to VKAs in terms of reducing the risk of rVTE and VTE related death, and also offer a comparable or reduced risk of bleeding. Unlike warfarin, DOACs do not necessitate INR monitoring and have fewer interactions with drugs and food. The European Society of Cardiology guidelines published in 2019 [8], the American Society of Hematology guidelines published in 2020 [9], The American College of Chest Physicians published in 2021 [10], the European Society for Vascular Surgery guidelines published in 2021 [11], recommend DOACs as the preferred initial treatment for VTE rather than VKAs.
Although clinical trial data suggest comparable effectiveness and safety of DOACs relative to VKAs, it is imperative to obtain evidence from real-world studies to validate these findings within a broader demographic and in routine clinical settings. Two recent real-world effectiveness studies, one conducted in France [12] and one conducted in the US [13], both reported lower hazard ratios (HR) for the risk of bleeding and VTE recurrence in apixaban versus VKAs. Additional evidence in the European setting is required to support or refute these findings.
This study aimed to compare the safety and effectiveness of DOACs and conventional therapy in a real-world setting in Sweden, Norway and Finland.
Materials & methods
Study design
Data sources
Data from nationwide administrative registers in Finland, Norway and Sweden were used to conduct a retrospective cohort study (EU PASS registration number EUPAS29910). Patient registers include information on inpatient and outpatient visits, primary and secondary diagnoses (coded as International Statistical Classification of Diseases, 10th revision [ICD-10] codes) and procedures (recorded as Nordic Classification of Surgical Procedures [NCSP] codes). Prescription registers include dates, strength, quantity within a package and number of packages of medications dispensed in community pharmacies, which are organized according to Anatomical Therapeutic Chemical (ATC) classification. Death registries include dates and immediate and underlying causes of death, recorded using ICD-10 codes.
The patient registers were prelinked to prescription and death registries using a unique personal identification number. All directly identifiable information was removed from these data sets by the register holders before data release. The study was approved by the University of Eastern Finland Committee on Research Ethics, the Regional Committees for Medical and Health Research Ethics in Norway (ref. no. 2017/1328), and the Swedish Ethical Review Authority (ref. no. 2018/2719-31 [2019-00604]).
Study period
The index date was the first dispensation of each OAC on or after 1 January 2013. The preindex period included all available time before the index date, whereas follow-up extended from the index date until 6 months after the index date (to reflect treatment duration for VTE), patient death, until the patient experienced the outcome of interest, until treatment discontinuation (defined later), or 31 December 2018, whichever came first. Patients were classified into treatment groups according to their first index OAC dispensation.
Study population
The following inclusion criteria were applied:
•
Inpatient or outpatient ICD-10 diagnosis (primary position only) of DVT or PE identified in the patient registers that occurred between 1 December 2012 and 30 September 2018. The ICD-10 codes used to identify DVT and PE can be found in Supplementary Table 1.
•
A dispensation of warfarin, apixaban, rivaroxaban, dabigatran or edoxaban identified within 30 days after the index VTE via an ATC code in the prescription registries between 1 January 2013 and 30 September 2018.
The following exclusion criteria were applied:
•
Prior VTE diagnosis, atrial fibrillation, mechanical heart valve replacement, mitral stenosis or inferior vena cava filter, or a previous OAC from 1 January 2008 until the index date.
•
Pregnancy at the time of OAC index date.
•
Record of immigration in the 1 year before index VTE.
•
Receipt of more than one OAC on index date.
•
Cancer in the 90 days before or after patients' first VTE diagnosis; traditionally, these patients have been excluded from DOAC clinical trials [14].
Subgroups
Subgroups were defined according to the type of VTE (DVT or PE), etiology of the incident VTE (provoked or unprovoked), and diagnostic setting (inpatient or outpatient). If any transient or persistent (identified in preindex period, Supplementary Table 2) risk factors for VTE were identified using ICD-10, ATC, or NCSP codes, the cause of the incident VTE was identified as provoked. Otherwise, the cause was identified as unprovoked.
Outcomes
The safety outcome of interest was bleeding, which was defined as an inpatient hospitalization with at least one overnight stay and a primary or secondary ICD-10 diagnosis of bleeding. The positive predictive value of bleeding requiring hospitalization has been validated and has been estimated in the range of 89–99% [15]. Bleeding was categorized overall and by site (gastrointestinal [GI] bleeding, intracranial bleeding or other bleeding) according to the categories provided by Halvorsen et al. [16]. rVTE was also an outcome of interest, defined as any primary inpatient VTE code occurring after initiation of the index treatment, excluding those events that occurred within 7 days of the hospital discharge date for the corresponding index VTE.
Study measures
Baseline demographic characteristics, including age in years (18–29, 30–44, 45–64, ≥65) and sex, were identified at the index date. Clinical characteristics, such as comorbidities (identified in the preindex period: myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, rheumatic disease, diabetes without chronic complications, diabetes with chronic complications, renal disease, any malignancy, hypertension, obesity and ischemic heart disease; identified any time in the 3-month preindex period: pneumonia), concomitant medications (identified in the 3-month preindex period: platelet aggregation inhibitors and nonsteroidal anti-inflammatory drugs), and bleeding history (identified in the preindex period: overall, GI, intracerebral hemorrhage [ICH], and other) were identified using ICD-10 or ATC codes in the patient or prescription registries. Validated code lists were used to identify comorbidities within the Charlson Comorbidity Index (CCI) [17]. The validated weights from Quan et al. [18] were used to calculate the CCI score.
All analyses were conducted on-treatment only. In order to estimate on-treatment time for the DOACs, the duration of supply of each medication was calculated using the number of packages, the quantity contained in each packet, and dosage information from each DOAC label. Because warfarin dosage information differs significantly according to patients' INR, the median time between warfarin prescriptions was calculated for each patient in different age bands. The median time for that age group was then applied to each patient within that age band to estimate the duration of an average prescription. Patients were identified as having discontinued their treatment if there was no new dispensation of the same medication within 60 days of the last dispensation. Patients were also censored at date of switch to another OAC that occurred within a 60 day grace period and who discontinued the first OAC.
Inverse probability of treatment weighting
Potential confounding in the treatment effect on effectiveness and safety outcomes was controlled for using inverse probability of treatment weighing (IPTW). This method has previously been detailed by Austin et al. [19]; in brief, the method controls for confounding by giving patients a propensity score (PS) based on their probability of treatment selection, conditional on their baseline characteristics. Patients are then weighted by the inverse of the PS, which creates a synthetic sample in which treatment is independent of baseline covariates. This method is commonly used in comparative effectiveness and safety studies [20] and has benefits over PS-matching methods, as it utilizes all patients in the analysis through weighting, avoiding the exclusion of unmatched individuals. Baseline demographics, comorbidities with a prevalence ≥1%, concomitant medications, bleeding history and cause, and setting of the incident VTE were included in the PS model. For subgroup matching, the overall IPTW-matched cohorts were split into subgroups, and standardized mean differences were used to assess if cohorts were still balanced.
Statistical analyses
Patient demographics and clinical characteristics were summarized using counts and percentages. Event rates of bleeding outcomes and rVTE were reported per 100 person-years. Analyses of time-to-bleeding and rVTE events were conducted using both mean time-to-event and cumulative incidence methods. Schoenfeld residuals were checked to confirm assumptions of proportionality were held. Separate outcome-specific Cox regression analyses were performed for the hazards of overall bleeding, ICH, GI bleeding, other bleeding and rVTE. Analyses were conducted at the country level in the IPTW matched cohorts and then frequentist meta-analysis was performed across the three countries; cumulative incidence analyses were not meta-analyzed. Random- and fixed-effects models were both implemented in the meta-analyses, but only the random-effects models are presented, as this is preferred in instances of small sample sizes and few data sources [21]. Because of the small sample sizes, apixaban and rivaroxaban were the only DOACs included in the comparative and meta-analyses. All analyses were repeated within each subgroup.
Results
Description of selected population
Across the three countries and before IPTW, we identified 22,454 warfarin, 14,542 apixaban, 23,149 rivaroxaban, 747 dabigatran and 51 edoxaban patients (Figure 1). The dabigatran and edoxaban cohorts were excluded from further analyses because of low patient numbers. After IPTW, the weighted sample sizes for the comparative analyses and meta-analyses were 22,450 warfarin, 14,533 apixaban and 23,002 rivaroxaban patients.
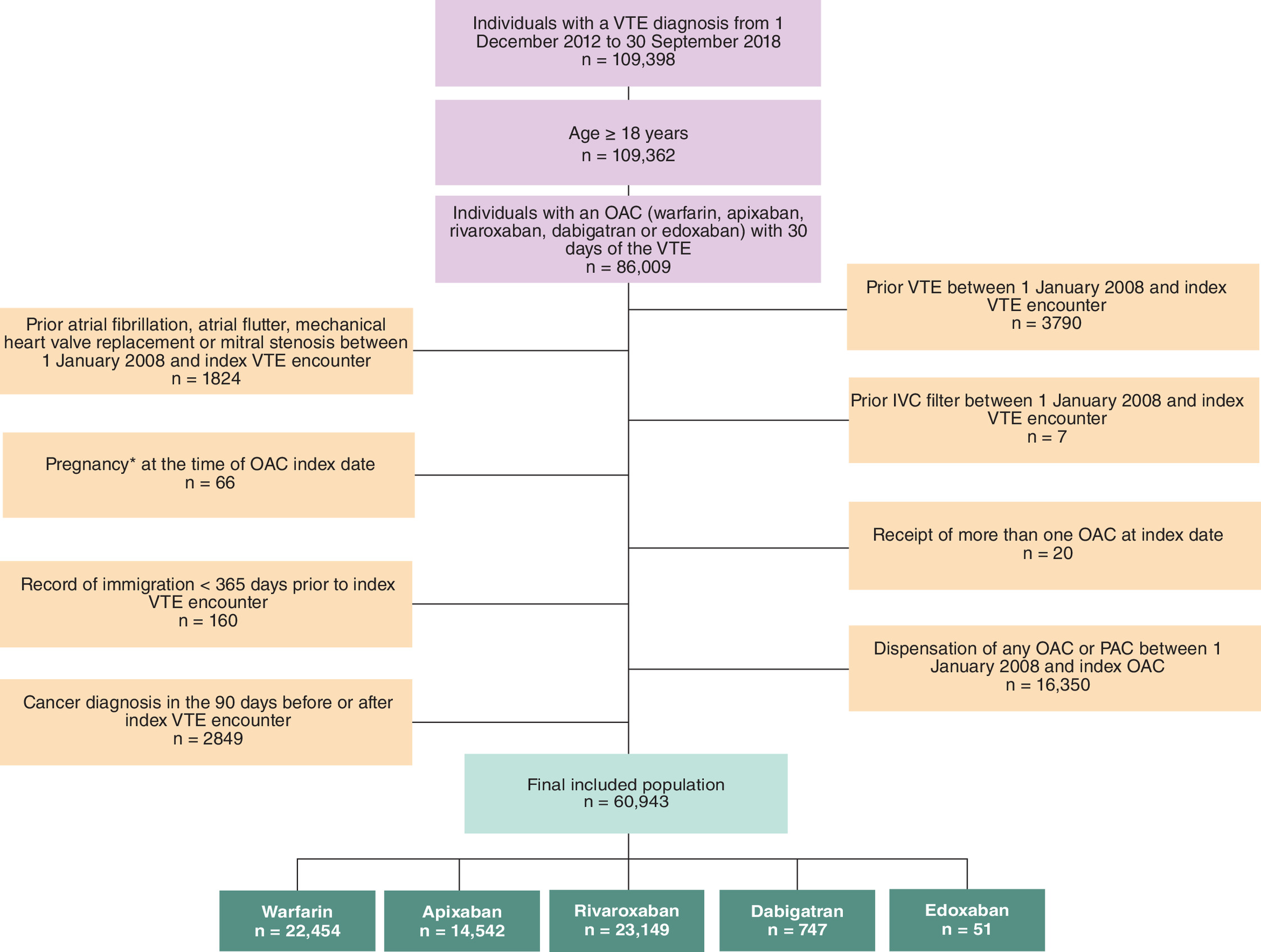
Figure 1. Flow diagram for patient selection.
Dabigatran and edoxaban were removed from further analyses because of low patient numbers.
*Pregnancy periods were estimated using ICD-10 and procedure codes for pregnancy end dates for pregnancy deliveries, cessations, and preterm, and then patients were deemed to be pregnant in the 42 weeks, 13 weeks and 36 weeks before end dates for each, respectively.
IVC: Inferior vena cava; OAC: Oral anticoagulant; VTE: Venous thromboembolism.
Description of the weighted cohorts
Many differences were observed in the cohorts before IPTW (see Supplementary Tables 3 & 4 for country-level descriptions within treatment groups). After IPTW, patient demographics and clinical characteristics were similar across treatment groups (Table 1).
| Characteristic | Apixaban vs warfarin weighted cohort | Rivaroxaban vs warfarin weighted cohort | ||
|---|---|---|---|---|
| Warfarin (n = 22,450) | Apixaban (n = 14,533) | Warfarin (n = 22,450) | Rivaroxaban (n = 23,002) | |
| Age at index VTE (years) | ||||
| Mean (SD) | 64.7 (16.8) | 64.6 (16.7) | 63.3 (17.1) | 63.1 (16.6) |
| Minimum, maximum | 18, 101 | 18, 104 | 18, 101 | 18, 103 |
| Gender, n (%) | ||||
| Male | 11,533 (51.4) | 7707 (53.0) | 11,786 (52.5) | 12,390 (53.9) |
| Female | 10,917 (48.7) | 6826 (47.0) | 10,663 (47.5) | 10,612 (46.1) |
| Index year, n (%) | ||||
| 2013 | 9216 (41.1) | <5 | 9384 (41.8) | 1842 (8.0) |
| 2014 | 6245 (27.8) | ⱡ | 6254 (27.9) | 4065 (17.7) |
| 2015 | 3441 (15.3) | 1648 (11.3) | 3390 (15.1) | 5101 (22.1) |
| 2016 | 1966 (8.8) | 3730 (25.7) | 1911 (8.51) | 4715 (20.5) |
| 2017 | 1119 (5.0) | 4913 (33.8) | 1068 (4.8) | 4217 (18.3) |
| 2018 | 464 (2.1) | 4080 (28.1) | 443 (2.0) | 3064 (13.3) |
| CCI, n (%) | ||||
| 0 | 15,371 (68.5) | 9,842 (67.7) | 15,970 (71.1) | 16,384 (71.2) |
| 1 | 3012 (13.4) | 2064 (14.2) | 2802 (12.5) | 2949 (12.8) |
| 2 | 2489 (11.1) | 1612 (11.1) | 2305 (10.3) | 2257 (9.8) |
| 3 | 821 (3.7) | 554 (3.8) | 716 (3.2) | 760 (3.3) |
| ≥4 | 758 (3.4) | 461 (3.2) | 658 (2.9) | 654 (2.8) |
| Specific comorbidities, n (%) | ||||
| AIDS/HIV | 24 (0.1) | 14 (0.1) | 24 (0.1) | 13 (0.1) |
| Any malignancy† | 1216 (5.4) | 893 (6.1) | 1131 (5.0) | 1262 (5.5) |
| Cerebrovascular disease | 1634 (7.3) | 1036 (7.1) | 1437 (6.4) | 1405 (6.1) |
| Chronic pulmonary disease | 2453 (10.9) | 1635 (11.3) | 2258 (10.1) | 2366 (10.3) |
| Dementia | 1001 (4.5) | 486 (3.3) | 901 (4.0) | 724 (3.2) |
| Diabetes without chronic complications | 1216 (5.4) | 788 (5.4) | 1167 (5.2) | 1177 (5.1) |
| Diabetes with chronic complications | 792 (3.5) | 504 (3.4) | 685 (3.1) | 698 (3.0) |
| Hemiplegia or paraplegia | 157 (0.7) | 137 (0.9) | 152 (0.7) | 187 (0.8) |
| Hypertension | 12,829 (57.1) | 7924 (54.5) | 12,110 (53.9) | 11,897 (51.72) |
| Inflammatory bowel disease | 346 (1.5) | 238 (1.6) | 350 (1.6) | 367 (1.6) |
| Ischemic heart disease | 2100 (9.4) | 1345 (9.3) | 1903 (8.5) | 1909 (8.3) |
| Metastatic solid tumor | 89 (0.4) | 55 (0.4) | 85 (0.4) | 84 (0.37) |
| Mild liver disease | 174 (0.8) | 126 (0.9) | 186 (0.8) | 202 (0.88) |
| Myocardial infarction | 617 (2.8) | 468 (3.2) | 539 (2.4) | 626 (2.72) |
| Obesity | 745 (3.3) | 482 (3.3) | 736 (3.3) | 752 (3.27) |
| Peptic ulcer disease | 337 (1.5) | 272 (1.9) | 302 (1.4) | 357 (1.55) |
| Peripheral vascular disease | 831 (3.7) | 620 (4.3) | 735 (3.3) | 825 (3.59) |
| Pneumonia‡ | 1410 (6.3) | 861 (5.9) | 1316 (5.9) | 1296 (5.63) |
| Renal disease | 1106 (4.93) | 837 (5.76) | 866 (3.86) | 983 (4.27) |
| Rheumatic disease | ||||
| Stroke (within 3 months prior to index) | 699 (3.11) | 383 (2.64) | 598 (2.66) | 511 (2.22) |
| Varicose veins | 687 (3.06) | 503 (3.46) | 692 (3.08) | 760 (3.3) |
| Prior bleeding, n (%) | ||||
| Bleeding overall | 877 (3.91) | 649 (4.47) | 772 (3.44) | 866 (3.76) |
| GI bleeding | 277 (1.23) | 203 (1.4) | 240 (1.07) | 267 (1.16) |
| Intracerebral hemorrhage | 177 (0.79) | 123 (0.85) | 157 (0.7) | 163 (0.71) |
| Other bleeding | 504 (2.24) | 382 (2.63) | 442 (1.97) | 516 (2.24) |
| Concomitant treatment | ||||
| Platelet aggregation inhibitors | 2647 (11.79) | 2044 (14.06) | 2445 (10.89) | 2861 (12.44) |
| NSAIDs | 3067 (13.66) | 1799 (12.38) | 3238 (14.42) | 3111 (13.52) |
| Transient risk factors for VTE | ||||
| Major surgery | 3463 (15.43) | 2179 (14.99) | 3439 (15.32) | 3237 (14.07) |
| Immobilization | 2542 (11.32) | 1390 (9.56) | 2392 (10.65) | 1993 (8.66) |
| Hormone therapy | 2556 (11.39) | 1713 (11.79) | 2571 (11.45) | 2788 (12.12) |
| Fracture/trauma | 1357 (6.04) | 1025 (7.05) | 1411 (6.29) | 1746 (7.59) |
| Central venous catheter | 42 (0.19) | 19 (0.13) | 41 (0.18) | 16 (0.07) |
| Specified medications (tamoxifen, thalidomide, lenalidomide) | 122 (0.54) | 84 (0.58) | 122 (0.54) | 91 (0.4) |
| Persistent risk factors for VTE | ||||
| Nephrotic syndrome | 25 (0.11) | 17 (0.12) | 21 (0.09) | 14 (0.06) |
| Inherited thrombophilia | 18 (0.08) | 12 (0.08) | 18 (0.08) | 20 (0.09) |
| Congestive heart failure | 911 (4.06) | 601 (4.14) | 792 (3.53) | 794 (3.45) |
| Antiphospholipid antibody syndrome | <5 | <5 | <5 | <5 |
| Lupus erythematosus | 27 (0.12) | 17 (0.12) | 26 (0.12) | 28 (0.12) |
| Myeloproliferative disorders | 77 (0.34) | 45 (0.31) | 72 (0.32) | 69 (0.3) |
| Inflammatory bowel disease | 346 (1.54) | 238 (1.64) | 350 (1.56) | 367 (1.6) |
| Myocardial infarction | 617 (2.75) | 468 (3.22) | 539 (2.4) | 626 (2.72) |
| Paroxysmal nocturnal hemoglobinuria | <5 | 0 (0) | <5 | 0 (0) |
| Type of VTE | ||||
| DVT | 10,548 (47.0) | 7141 (49.1) | 11,245 (50.1) | 11,944 (51.9) |
| PE | 11,903 (53.0) | 7391 (50.9) | 11,204 (49.9) | 11,058 (48.1) |
| Diagnostic setting | ||||
| Inpatient | 13,676 (60.9) | 8589 (59.1) | 12,916 (57.5) | 13,041 (56.7) |
| Outpatient | 8776 (39.1) | 5943 (40.9) | 9533 (42.5) | 9962 (43.3) |
| VTE etiology | ||||
| Provoked | 8823 (39.3) | 5751 (39.6) | 8636 (38.5) | 8882 (38.6) |
| Unprovoked | 6952 (31.0) | 5622 (38.7) | 7052 (31.4) | 8252 (35.9) |
†
Individuals with a cancer diagnosis in the 90 days before or after index were excluded.
‡
Identified in the 3 months before index.
Cells with values less than 5 have been suppressed for patient confidentiality reasons, and secondary suppression (ⱡ) has been conducted where necessary.
CCI: Charlson Comorbidity Index; DVT: Deep vein thrombosis; GI: Gastrointestinal; NSAID: Nonsteroidal anti-inflammatory drug; OAC: Oral anticoagulant; PE: Pulmonary embolism; VTE: Venous thromboembolism.
CCI scores were also consistent across treatment groups, and more than half of the patients had hypertension (warfarin vs apixaban: 57.14% vs 54.52%, respectively; warfarin vs rivaroxaban: 53.9% vs 51.7%, respectively). The prevalence of prior overall bleeding was similar in patients treated with apixaban versus warfarin (4.5% vs 3.9%, respectively) and similar in the rivaroxaban versus warfarin groups (3.8% vs 3.4%, respectively). Concomitant use of platelet aggregation inhibitors was also higher in patients treated with DOACs than in those treated with warfarin, and the prevalence of transient risk factors appeared similar (Table 1).
Occurrence & risk of bleeding & VTE recurrence After IPTW
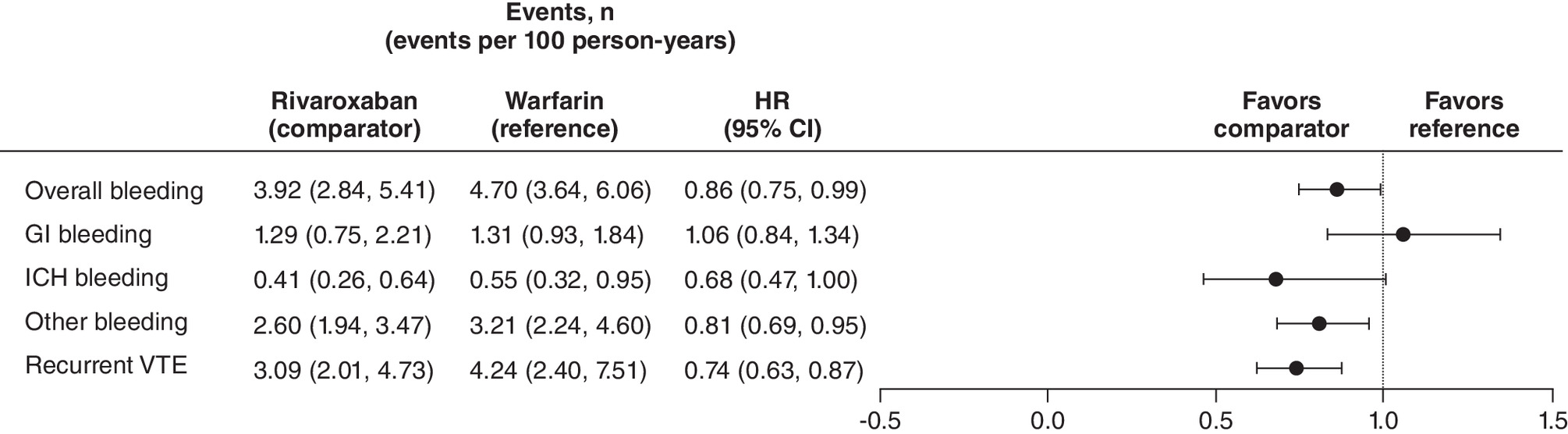
Event rates per 100 person-years (95% CI) for overall bleeding appeared higher in patients treated with warfarin than in those treated with DOAC: warfarin versus apixaban, 5.1 (4.6, 5.5) versus 2.8 (2.4, 3.2), respectively; warfarin versus rivaroxaban, 4.7 (4.3, 5.2) versus 3.9 (2.8, 5.4), respectively. Rates of bleeding by site are presented in Figures 2 & 3. The rate of rVTE was 3.6 per 100 person-years (2.2, 5.8) for patients treated with apixaban compared with 4.3 (2.5, 7.5) for patients treated with warfarin. In the rivaroxaban cohort, the rate of rVTE was 3.1 per 100 person-years (2.0, 4.7) compared with 4.2 (2.4, 7.5) for warfarin.
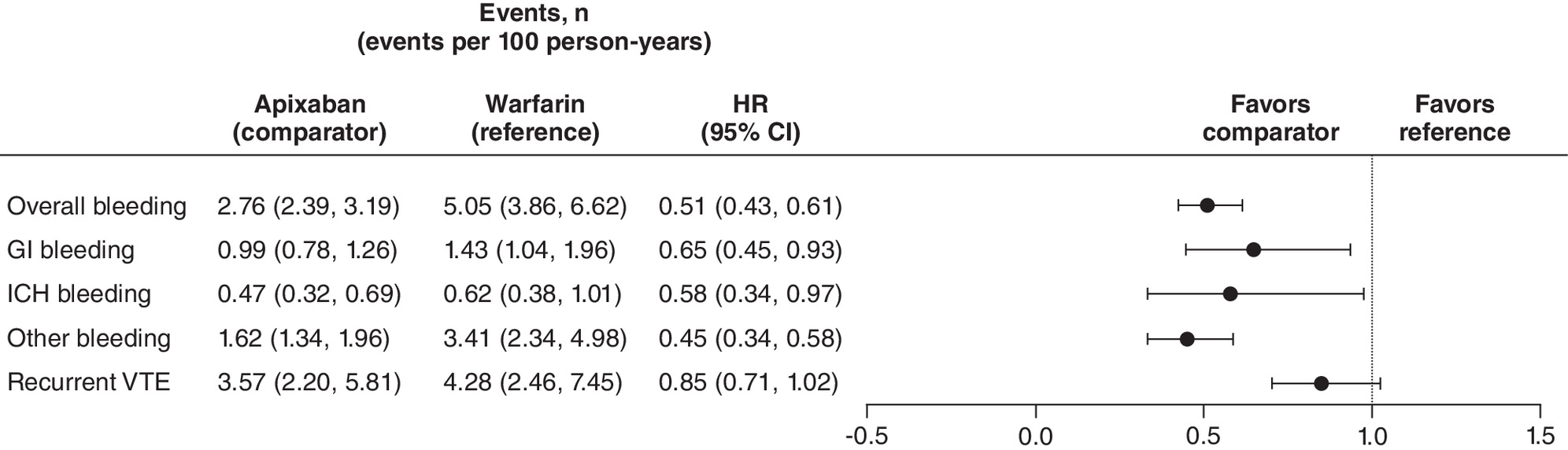
Results show that at 6 months, the risk of overall bleeding was lower for patients treated with apixaban than for those treated with warfarin (HR: 0.51 [95% CI: 0.43, 0.61]). The risk of other, GI and ICH bleeding were also lower for the apixaban cohort than for the warfarin cohort (HR: 0.45 [95% CI: 0.34, 0.58]; 0.65 [95% CI: 0.45, 0.93] and 0.58 [95% CI: 0.34, 0.97]), respectively. The risk of rVTE was similar (0.85 [95% CI: 0.71, 1.02]) (Figure 2).
The risk of overall bleeding and other bleeding was lower for rivaroxaban than for warfarin (HR: 0.86 [95% CI: 0.75, 0.99] and HR: 0.81 [95% CI: 0.69, 0.95], respectively). The HRs for GI bleeding and ICH were similar (1.06 [95% CI: 0.84, 1.34] and 0.68 [95% CI: 0.47, 1.00], respectively). A lower risk of rVTE was observed for rivaroxaban than for warfarin (HR: 0.74 [95% CI: 0.63, 0.87]) (Figures 2 & 3). Trends in HRs stratified by subgroup (type of VTE, etiology of the incident VTE, and diagnostic setting) were consistent for both comparisons for all outcomes (Supplementary Figures 1 & 2). Country-specific estimates are provided in Supplementary Figures 3 & 4.
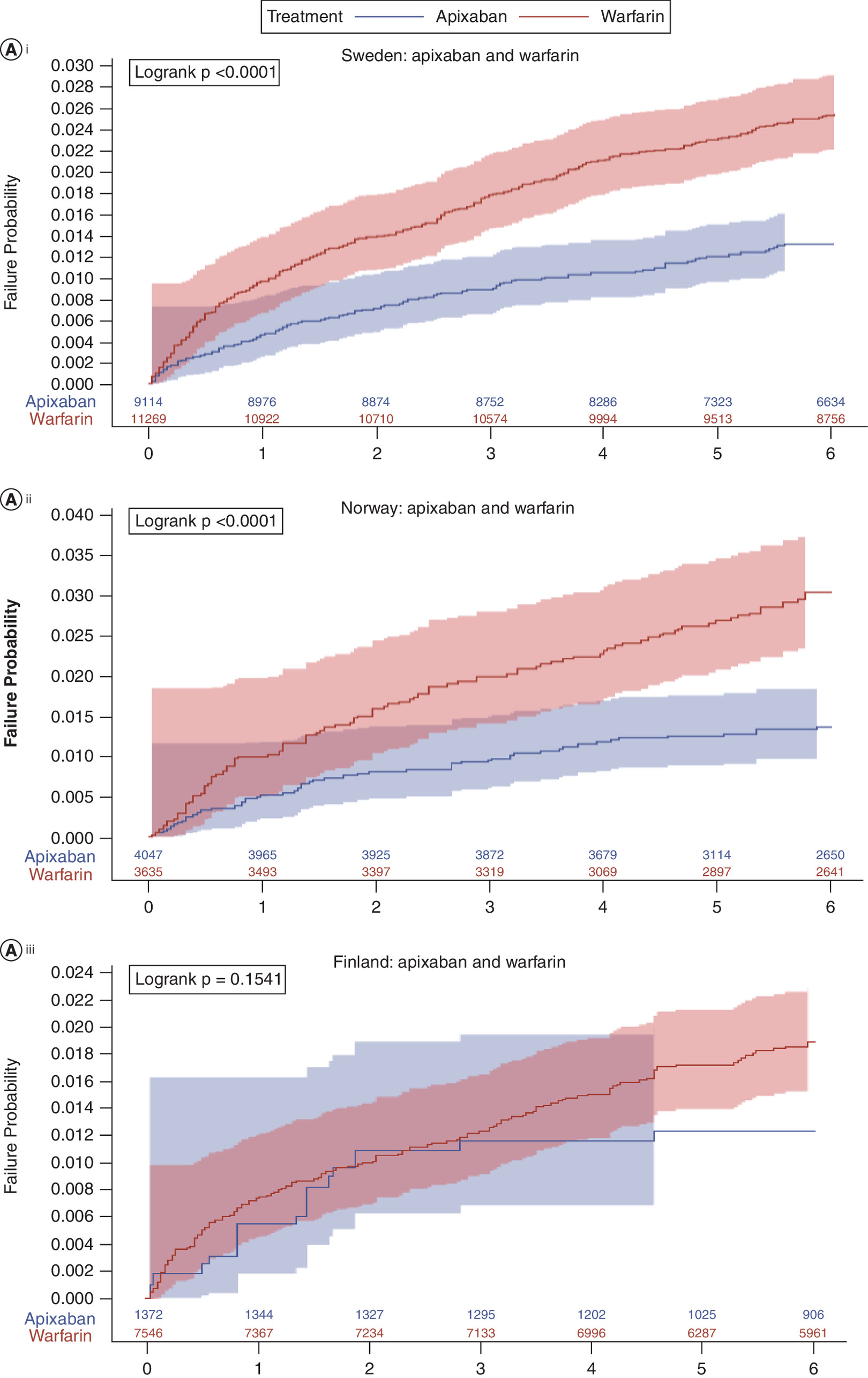
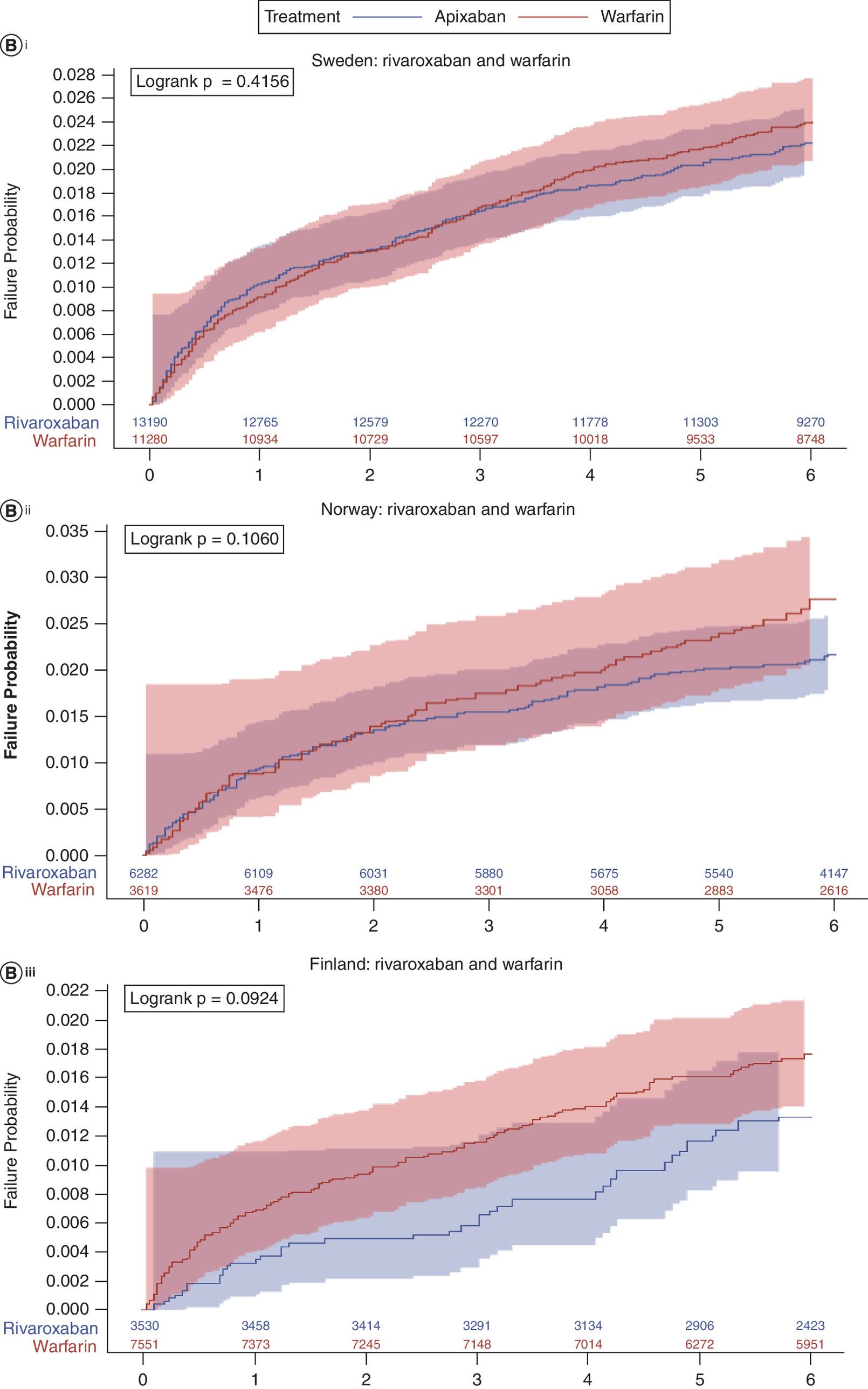
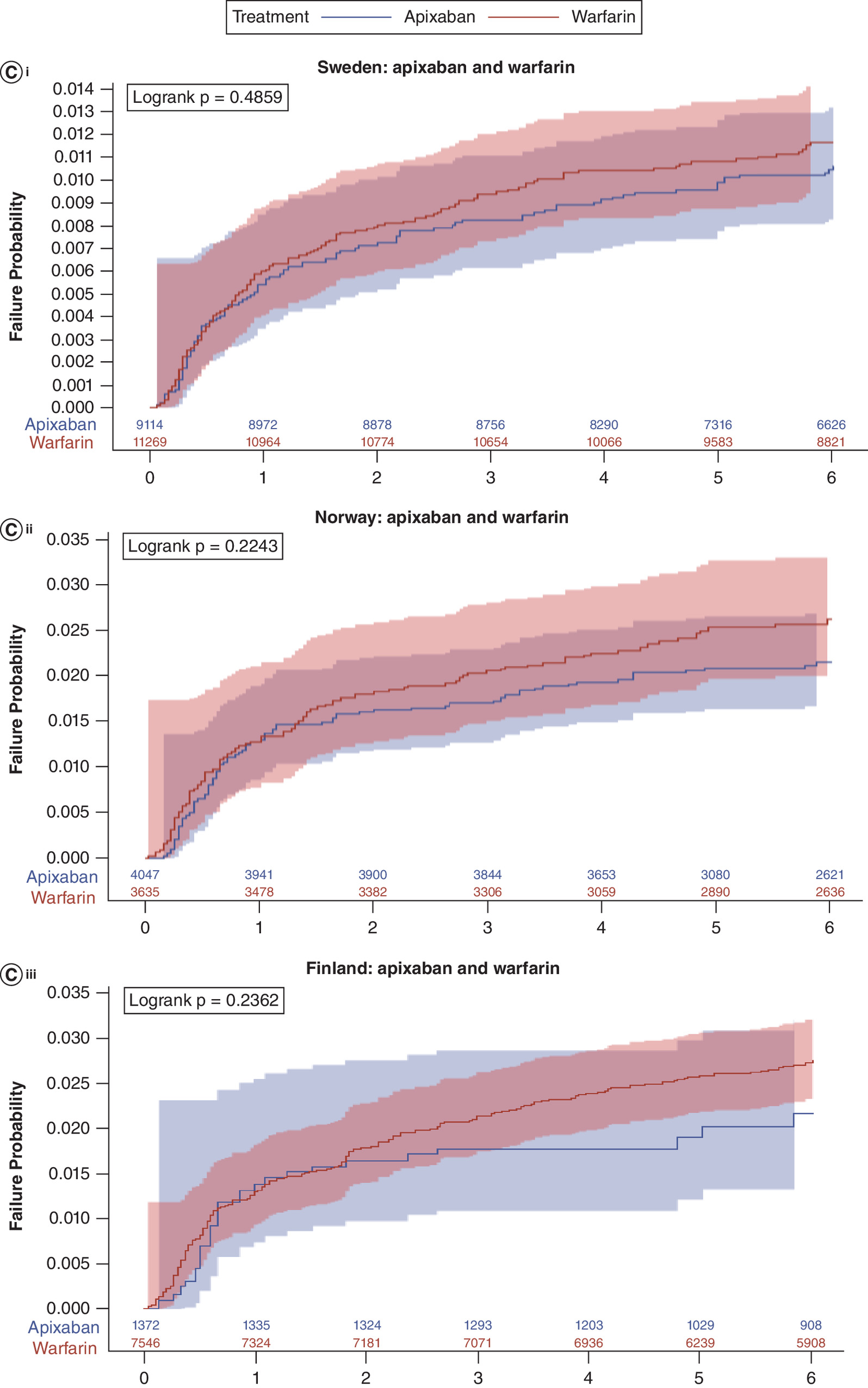
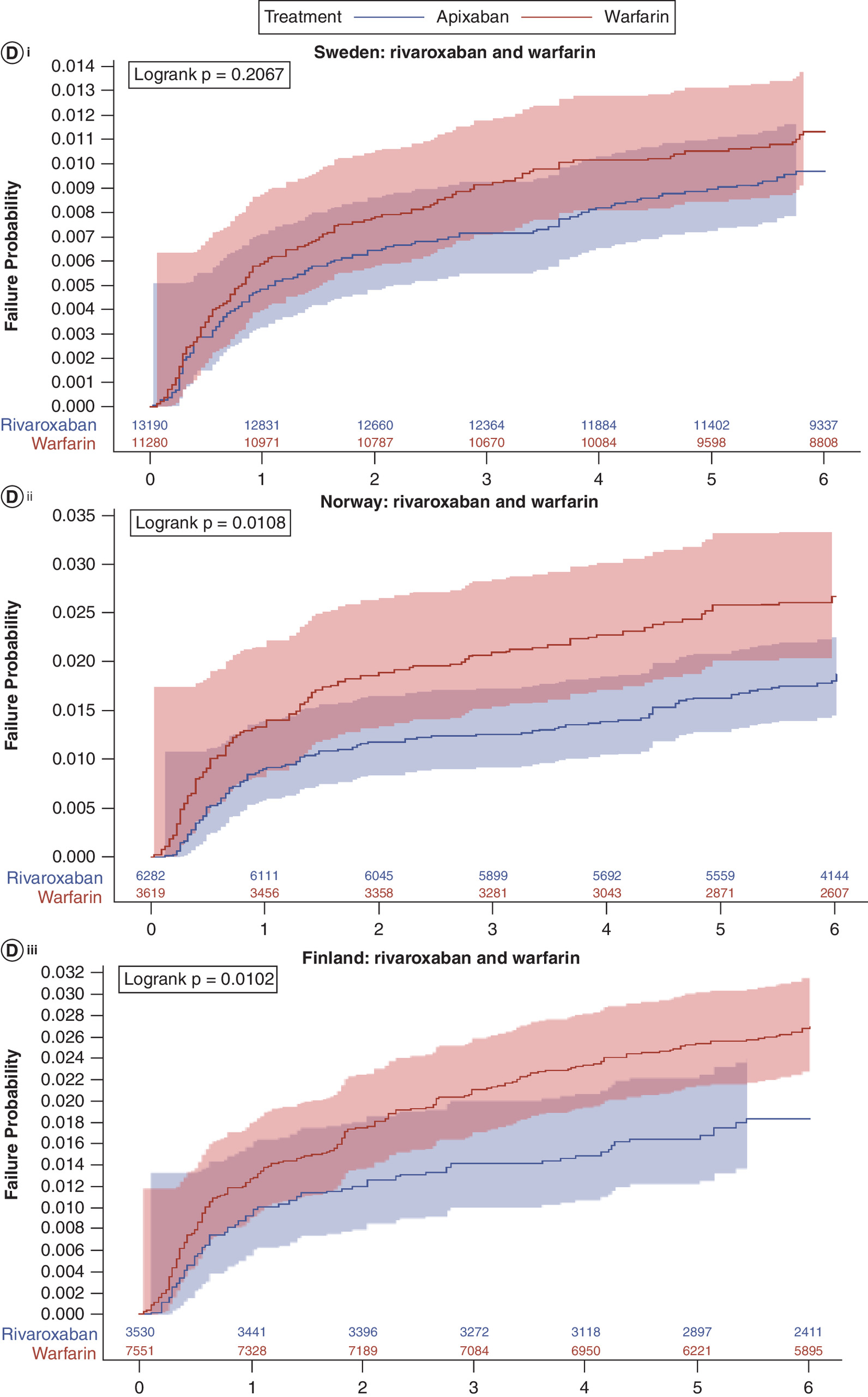
Country-specific cumulative incidence estimates for time to overall bleeding and rVTE are provided in Figures 4 & 5, respectively.
Discussion
In this large Nordic study among patients with VTE who were newly initiating OACs, treatment with apixaban was associated with a reduced risk of bleeding (overall and by type) and similar risk of rVTE compared with warfarin. Initiating rivaroxaban was associated with a reduced risk of overall and other bleeding, and a similar risk of GI bleeding and ICH compared with warfarin. Rivaroxaban was also associated with a reduced risk of rVTE compared with warfarin.
Our findings are generally consistent with previous clinical trial results and observational studies that showed a reduced risk of safety outcomes and comparable effectiveness between the DOACs and warfarin. In terms of prior RCTs, for apixaban versus warfarin, the AMPLIFY (Apixaban for the Initial Management of Pulmonary Embolism and Deep-Vein Thrombosis as First-Line Therapy) trial9 reported bleeding outcomes by severity (major and clinically relevant nonmajor bleeding), but as in the current study, all bleeding outcomes were lower for apixaban than for conventional therapy. Both the AMPLIFY trial and our study results showed noninferiority for rVTE compared with conventional therapy (current study estimate: HR: 0.85 [95% CI: 0.71, 1.02]; clinical trial: HR: 0.84 [95% CI: 0.60, 1.18]).
In comparison to previous observational studies, a 2014–2020 study by Sandblad et al. [22] used nationwide data in Sweden and included 45,114 VTE patients. They reported a reduction in the risk of major bleeds in patients treated with apixaban compared with warfarin during the initial 6 months (HR: 0.55 [95% CI: 0.43, 0.71]) and from 6 months to 5 years (HR: 0.72 [95% CI: 0.53, 0.99]). A 2013–2018 observational study by Bertoletti et al. [12] used nationwide data in France and included 58,137 VTE patients. They reported bleeding estimates at 6 months that were in line with those of our study: apixaban-treated patients had a lower risk of bleeding than warfarin-treated patients overall and by site (overall bleeding, HR: 0.43 [95% CI: 0.32, 0.59]; GI bleeding, HR: 0.51 [95% CI: 0.30, 0.87]; ICH, HR: 0.38 [95% CI: 0.21, 0.70]; other bleeding, HR: 0.41 [95% CI: 0.25, 0.65]) [12]. A 2014–2017 observational study by Weycker et al. [13] used four commercial claims data sources in the US and included 17,878 VTE patients. They reported a significant reduction in the rates of both major bleeding and rVTE. Another 2014–2017 claims-based study in the US by Cohen et al. [23] included 155,119 VTE patients. They observed a significantly lower risk of rVTE among patients aged ≥65 years when they were treated with apixaban rather than warfarin.
Although our study did not find a significant reduction in the risk of rVTE in apixaban-treated patients compared with warfarin-treated patients, it should be noted that the definition of rVTE for our study was restricted to the inpatient setting, given that it was not possible to differentiate between follow-up visits for the incident VTE and recurrent visits that occurred in the outpatient setting. To our knowledge, in the Nordics, a large number of rVTE events are diagnosed in the outpatient setting; as a result, this study likely underestimated the rate of rVTE. Because of this underestimation, the study was not sufficiently powered to confirm differences in the rate of rVTE between cohorts.
For rivaroxaban versus warfarin, the clinical trials EINSTEIN-DVT and EINSTEIN-PE also reported bleeding outcomes by severity, but only one reported a lower risk of bleeding with rivaroxaban than with conventional therapy (EINSTEIN-PE: major bleeding, HR: 0.49 [95% CI: 0.31, 0.79]). The EINSTEIN trials reported noninferiority for rVTE (recurrent DVT, HR: 0.68 [95% CI: 0.44, 1.04]; recurrent PE, 1.12 [95% CI: 0.75, 1.68]), whereas our study reported a lower risk of rVTE for rivaroxaban compared with conventional therapy (HR: 0.74 [95% CI: 0.63, 0.87]).
The observational study conducted by Sandblad et al. [22], found no evidence for a reduction in the risk of bleeding events in patients treated with rivaroxaban compared with warfarin in the 6 months following treatment initiation (HR: 0.89 [95% CI: 0.71, 1.12]). In addition, Bertoletti et al. [12] compared bleeding outcomes in patients treated with rivaroxaban versus warfarin and found similar bleeding risk overall and for all bleeding types except for the lower risk for ICH bleeding (overall bleeding: HR: 0.86 [95% CI: 0.69, 1.07]; GI bleeding: 1.26 [95% CI: 0.87, 1.83]; ICH bleeding: 0.48 [95% CI: 0.29, 0.79]; other bleeding: 0.84 [95% CI: 0.61, 1.17]).
To the best of our knowledge, this is the first study to compare the safety and effectiveness of DOACs and warfarin for the treatment of VTE in a real-world setting in the Nordics. This study is strengthened by the large multi-country population size (>60,000 VTE patients) and the use of the high-quality national Nordic registers, which allow patient-level linkage and complete follow-up [24,25]. Furthermore, the use of IPTW ensures that the comparisons made are between similar populations and that resulting differences in the outcomes are driven by the treatment rather than by any underlying differences in cohorts. Limitations of the study include the inability to identify warfarin dosage and INR, which could mean there were some inaccuracies with estimating warfarin duration of supply. Therefore, patients with significant time outside of their designated therapeutic range may be included in the analysis. Low time in therapeutic range may lead to poor outcomes in the warfarin population; however, this is reflective of real-world outcomes for patients treated with VKAs. A further limitation is that, although comparisons can be drawn between each DOAC and warfarin, the design does not allow for DOAC versus DOAC comparisons. Therefore, no conclusions can be made regarding the efficacy and safety of apixaban versus rivaroxaban. It should also be noted that despite IPTW, residual and unmeasured confounding may still exist. Finally, as explained previously, another limitation is the underpowering of the comparative analysis for the rVTE outcome. Future research validating definitions for identifying recurrent VTE events in the outpatient setting when using administrative data would be beneficial in order to allow for more complete ascertainment of rVTE events and improve power for comparative effectiveness analyses of this outcome.
Conclusion
In this large, retrospective, nationwide study that meta-analyzed data across three European countries, we identified improved safety and at least similar effectiveness of DOACs versus warfarin, with results in line with those of previous clinical trials and observational data. Overall, these results add to the real-world evidence supporting recommendations to use DOACs over warfarin for the treatment of VTE. Future research is warranted to accurately identify rVTE events in the outpatient setting.
Summary points
•
Clinical trial data has suggested comparable effectiveness and safety of direct oral anticoagulants relative to vitamin K antagonists for the treatment of patients with venous thromboembolism.
•
Real-world evidence studies in Europe are required to support or refute these findings.
•
This multi-country cohort study utilized national healthcare administrative data from Sweden, Norway and Finland from 2012 to 2018.
•
After population weighting methods were applied, 22,450 patients with warfarin, 14,542 apixaban and 23,002 rivaroxaban were included.
•
For patients with apixaban versus warfarin patients, risk of overall bleeding was lower (hazard ratio [HR]: 0.51 [95% CI: 0.43, 0.61]) and risk of recurrent venous thromboembolism was comparable (0.85 [0.71, 1.02]).
•
For patients with rivaroxaban versus warfarin patients, risk of overall bleeding (HR: 0.86 [0.75, 0.99]) and recurrent venous thromboembolism were lower (0.74 [0.63, 0.87]).
•
Direct oral anticoagulants showed improved safety and at least similar effectiveness compared with warfarin, in line with clinical trial estimates.
Financial disclosure
This was a BMS/Pfizer sponsored study.
Competing interests disclosure
W Ghanima reports fees for participation in advisory board from Amgen, Novartis, Pfizer, Principia Biopharma Inc. – a Sanofi Company, Sanofi, SOBI, Grifols, UCB, Argenx, Cellphire, Alpine, Kedrion, HiBio and Hutchmed. Lecture honoraria from Amgen, Novartis, Pfizer, Bristol Myers Squibb, SOBI, Grifols, Sanofi and Bayer. Research grants from Bayer, BMS/Pfizer and UCB. H Pohjantähti received consultancy fees from Pfizer, Amarin, AstraZeneca, Boehringer Ingelheim, BMS, Vifor Pharma and Bayer. D Lambrelli, B Nordstrom, A Booth and S Graham are employees of Evidera. Evidera received funding from the Bristol Myers Squibb and Pfizer Alliance in connection with the development of this manuscript and conduct of the study. R Mokgokong, A Jenkins, J Chaves, F Dai and R Subash are employees and shareholders of Pfizer. A Gottsäter has received consultancy fees from Bayer, Pfizer and Sanofi. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 947.54 KB
References
Papers of special note have been highlighted as: • of interest
1.
Raskob GE, Angchaisuksiri P, Blanco AN et al. Thrombosis: a major contributor to global disease burden. Arterioscler. Thromb. Vasc. Biol. 34(11), 2363–2371 (2014).
2.
McLendon K, Goyal A, Attia M. Deep venous thrombosis risk factors. StatPearls (2023). Available from: https://www.ncbi.nlm.nih.gov/books/NBK470215/
3.
Andersson T, Soderberg S. Incidence of acute pulmonary embolism, related comorbidities and survival; analysis of a Swedish national cohort. BMC Cardiovasc. Disord. 17(1), 155 (2017).
4.
Ghanima W, Brodin E, Schultze A et al. Incidence and prevalence of venous thromboembolism in Norway 2010–2017. Thromb. Res. 195, 165–168 (2020).
5.
Wendelboe AM, Raskob GE. Global burden of thrombosis: epidemiologic aspects. Circ. Res. 118(9), 1340–1347 (2016).
6.
Keller K, Hobohm L, Ebner M et al. Trends in thrombolytic treatment and outcomes of acute pulmonary embolism in germany. Eur. Heart J. 41(4), 522–529 (2020).
7.
Khan F, Rahman A, Carrier M et al. Long term risk of symptomatic recurrent venous thromboembolism after discontinuation of anticoagulant treatment for first unprovoked venous thromboembolism event: systematic review and meta-analysis. BMJ 366, l4363 (2019).
8.
Konstantinides SV, Meyer G, Becattini C et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 41(4), 543–603 (2020).
• The European treatment guidelines for patients with venous thromboembolism at the time this study was conducted.
9.
Ortel TL, Neumann I, Ageno W et al. American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism. Blood Adv. 4(19), 4693–4738 (2020).
10.
Stevens SM, Woller SC, Kreuziger LB et al. Antithrombotic therapy for VTE disease: second update of the Chest Guideline and Expert Panel Report. Chest 160(6), e545–e608 (2021).
11.
Kakkos SK, Gohel M, Baekgaard N et al. Editor's choice – European Society for Vascular Surgery (ESVS) 2021 clinical practice guidelines on the management of venous thrombosis. Eur. J. Vasc. Endovasc. Surg. 61(1), 9–82 (2021).
12.
Bertoletti L, Gusto G, Khachatryan A et al. Effectiveness and safety of oral anticoagulants in the treatment of acute venous thromboembolism: a nationwide comparative cohort study in France. Thromb. Haemost. 122(8), 1384–1396 (2022).
• This study was not published at the time of study conduct, but we have compared our study results to this regardless.
13.
Weycker D, Li X, Wygant GD et al. Effectiveness and safety of apixaban versus warfarin as outpatient treatment of venous thromboembolism in U.S. clinical practice. Thromb. Haemost. 118(11), 1951–1961 (2018).
• This was the only real-world study that was published at the time of study conduct and some of the study definitions were based on this article.
14.
Agnelli G, Buller HR, Cohen A et al. Oral apixaban for the treatment of acute venous thromboembolism. N. Engl. J. Med. 369(9), 799–808 (2013).
• This is the clinical trial for apixaban versus warfarin which we compared our study results to.
15.
Cunningham A, Stein CM, Chung CP, Daugherty JR, Smalley WE, Ray WA. An automated database case definition for serious bleeding related to oral anticoagulant use. Pharmacoepidemiol. Drug Saf. 20(6), 560–566 (2011).
16.
Halvorsen S, Ghanima W, Fride Tvete I et al. A nationwide registry study to compare bleeding rates in patients with atrial fibrillation being prescribed oral anticoagulants. Eur. Heart J. Cardiovasc. Pharmacother. 3(1), 28–36 (2017).
17.
Thygesen SK, Christiansen CF, Christensen S, Lash TL, Sorensen HT. The predictive value of ICD-10 diagnostic coding used to assess Charlson Comorbidity Index conditions in the population-based Danish National Registry of Patients. BMC Med. Res. Methodol. 11, 83 (2011).
18.
Quan H, Li B, Couris CM et al. Updating and validating the Charlson Comorbidity Index and Score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 173(6), 676–682 (2011).
19.
Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 34(28), 3661–3679 (2015).
20.
Allan V, Ramagopalan SV, Mardekian J et al. Propensity score matching and inverse probability of treatment weighting to address confounding by indication in comparative effectiveness research of oral anticoagulants. J. Comp. Eff. Res. 9(9), 603–614 (2020).
21.
von Hippel PT. The heterogeneity statistic i(2) can be biased in small meta-analyses. BMC Med. Res. Methodol. 15, 35 (2015).
22.
Glise Sandblad K, Schulman S, Rosengren A, Sorbo J, Philipson J, Hansson PO. Association of type of oral anticoagulation with risk of bleeding in 45,114 patients with venous thromboembolism during initial and extended treatment-a nationwide register-based study. J. Intern. Med. 294(6), 743–760 (2023).
23.
Cohen AT, Sah J, Dhamane AD et al. Effectiveness and safety of apixaban versus warfarin among older patients with venous thromboembolism with different demographics and socioeconomic status. Adv. Ther. 38(11), 5519–5533 (2021).
24.
Ludvigsson JF, Andersson E, Ekbom A et al. External review and validation of the Swedish National Inpatient Register. BMC Public Health 11, 450 (2011).
25.
Friberg L, Skeppholm M. Usefulness of health registers for detection of bleeding events in outcome studies. Thromb. Haemost. 116(6), 1131–1139 (2016).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 4 November 2024
Accepted: 21 August 2025
Published online: 25 September 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative safety and effectiveness of direct oral anticoagulants and warfarin in patients with venous thromboembolism in Finland, Norway and Sweden. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0207
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Omar Elmadhoun, Dinu V. Balanescu, Troy G. Seelhammer, Yahya Alwatari, Kevin G. Buda, Jamel P. Ortoleva, Sumera R. Ahmad, Sanjay Chaudhary, Krishnan Ramanujan, Pramod K. Guru, Sean M. Caples, Patrick M. Wieruszewski, Harish Ramakrishna, The 2026 Multisociety Acute Pulmonary Embolism Guidelines: An Expert Perspective, Journal of Cardiothoracic and Vascular Anesthesia, 10.1053/j.jvca.2026.06.003, (2026).
- Katarina Glise Sandblad, Mazdak Tavoly, Waleed Ghanima, Camilla T. Jørgensen, Bleeding and Recurrence in Patients with Venous Thromboembolism with Changing Anticoagulant Treatment Patterns: Findings from the TROLL Registry, TH Open, 10.1055/a-2832-8297, 10, CP, (2026).