Single-use endoscopy for the evaluation of swallowing: a performance survey
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Single-use endoscopes have become of interest across a multitude of procedure types given the risk of cross-contamination and availability of scopes; the performance capability of a single-use scope has not formally been evaluated for the flexible endoscopic evaluation of swallowing (FEES) indication. The primary objective was to measure FEES procedural success with single-use rhinolaryngoscopes without the need for a secondary scope, while the secondary objective was to evaluate the overall performance and usability of the single-use platform. Materials & methods: Twenty-three speech–language pathologists across 16 sites performed FEES procedures with the Ambu aScope 4 RhinoLaryngo Slim. After the procedures, participants completed a nine-question survey questionnaire. A five-point rating system was used to quantify scope performance. Mean ratings were calculated and a one-sample t-test was performed. Results: The primary end point of procedural success was achieved in 100% of procedures. Of the nine performance metrics captured for aScope 4 RhinoLaryngo Slim, six received a score of excellent by 100% of participants with the lowest score being a 4.2. Conclusion: Single-use rhinolaryngoscopes can successfully perform FEES procedures without additional scoping needed, and received high performance ratings among users. Level of evidence: 4.
Plain language summary
What is this article about?
This study measured the ability of single-use rhinolaryngoscopes to successfully complete flexible endoscopic evaluation of swallowing (FEES) procedures. The performance and evaluation of single-use rhinolaryngoscopes for these procedures had not been formally evaluated, and this study aims to show that these scopes can successfully perform FEES without the need of additional equipment, or secondary endoscopes. Additionally, this study evaluates the endoscope user’s opinions on the performance of the single-use rhinolaryngoscope for these procedures.
What were the methods & results?
Twenty-three speech–language pathologists participated in this study, and each performed a FEES procedure using the single-use scope. One hundred percent of the procedures performed with single-use rhinolaryngoscopes were successfully completed without the need for a secondary reusable rhinolaryngoscope. Additionally, users completed qualitative performance surveys after the procedure and gave strong ratings for the single-use scope, with 6 of 9 performance metrics receiving an average score of 4 or higher (out of 5).
Why is this important?
By showing the user’s perspective on the scope’s performance, other speech–language pathologists and users of flexible rhinolaryngoscopes can reference this data when considering implementing a single-use endoscopy system to alleviate workflow and scope availability issues, to more readily perform FEES when needed.
Flexible endoscopic evaluation of swallowing, or FEES, is a frequently performed procedure to assess and diagnose issues with swallowing, known as ‘oropharyngeal dysphagia.’ Oropharyngeal dysphagia describes issues with swallowing that occur in the mouth and throat, and most commonly result from impaired muscle or sensory changes, growths and obstructions of the mouth or throat [1]. During the procedure, a physician, or more commonly a speech–language pathologist, passes a thin, flexible endoscope through a patient’s nose to observe the pharynx and larynx during the swallowing function [2]. The speech–language pathologist will initially observe the pharynx and larynx structure during a patient’s swallow function, followed by an introduction of foods and liquids to assess how well the patient swallows different textures and sizes of items [2]. Traditionally, these procedures were primarily lead by ear, nose and throat (ENT) physicians with the assistance of an speech–language pathologist and were viewed as ‘fringe procedures’ [3]. In 2001, as more evidence solidified the instrumental role of FEES in dysphagia management, the American Speech Language Hearing Association added the FEES procedure to the scope of practice for speech–language pathologists [3], opening the door for the expansion of this procedure to more patients and settings. Since this expansion, coupled with growing evidence of the advantages of FEES [4,5], the demand for the procedure has grown significantly [6]. Between 2003 and 2018, the number of FEES procedures billed to Medicare grew from 2549 to 8442, respectively [6]. As the demand for FEES continues to grow – including increased patient populations and expanding points of care, it is important for clinicians to have the equipment and processes in place in order to provide timely diagnoses for patients.
While ENT physicians may still perform FEES, one aspect that may contribute to procedure growth is the expansion of speech–language pathologists performing FEES across multiple departments and settings. In most instances, speech–language pathologists performing FEES have a small inventory and/or limited access to reusable endoscopes, which sometimes leads to inconvenient scheduling issues or procedural delays. Additionally, these endoscopes require significant cleaning and reprocessing of more than 100 individual steps [7,8] after each procedure to ensure a safe and patient ready device [6]. A full reprocessing cycle of a reusable endoscope has been estimated to require 76 min to complete [8] and may require additional time if the hospital or clinic adheres to updated guidelines such as the ANSI/AAMI ST91 endoscope reprocessing standards [9]. Mishandling of the endoscope during the reprocessing cycle can also lead to damages requiring repair, or even contamination of the device. Recent evidence showed visible damage and debris was observed with 100% of fully reprocessed endoscopes, which required repairs or full endoscope refurbishment [10] which can lead to significant equipment unavailability, impacting when and where clinicians can perform these procedures.
To address this issue, hospitals and clinics would need to invest in more reusable endoscopes for their speech–language pathologists or expand their reprocessing resources to keep up with instrument readiness needs. This capital outlay, compounded with reusable endoscope reprocessing, repairs and service contracts, may not be a feasible option for hospitals looking to expand the use of FEES. Given the cost and operational efficiency implications addressed above, single-use rhinolaryngoscopes may solve these issues and enable simple expansion of rhinolaryngoscopy points of care by providing a sterile, transportable endoscope that is always available. These single-use scopes also have an all-in-one imaging display for capturing images and video for documentation and review. Single-use rhinolaryngoscopes were first brought to market following US FDA approval in 2019 (Ambu A/S, Ballerup, Denmark) and were designed to clinically operate and function similarly to the reusable standard of care. As interest has grown in single-use endoscopy across specialties, other manufacturers such as Karl Storz [11] and Olympus [12] have brought their own single-use rhinolaryngoscopes to market. The performance capability of single-use rhinolaryngoscopes has not been formally evaluated for the FEES indication, where timely reprocessing and/or sterilization may not always be feasible or available. The primary objective of this study was to measure FEES procedural success with single-use rhinolaryngoscopes (Ambu aScope™ 4 RhinoLaryngo Slim), meaning the ability to perform the procedure without the use of a secondary endoscope. The secondary objective was to evaluate the overall performance and usability of the single-use rhinolaryngoscope (Ambu aScope™ 4 RhinoLaryngo Slim) platform.
Materials & methods
This study was reported following the Standards for Reporting Qualitative Research [13] guidelines for reporting qualitative research. A total of 23 speech–language pathologists and one speech–language pathologist student from 16 sites were identified to participate in this study. The facilities included represent a national sample including facilities in Alabama, Colorado, Kentucky, Maryland, Nevada, New York, Pennsylvania, Virginia, Texas, and Washington DC (USA) where clinicians worked across long-term acute care facilities, academic and nonacademic medical centers. All 23 clinicians, excluding the student, performed a FEES exam with the Ambu aScope™ 4 RhinoLaryngo Slim and the aView™ 2 Advance monitor (i.e., single-use rhinolaryngoscope and monitor), which were not provided by the manufacturer for the purpose of this study. Facilities that currently utilized the aScope™ 4 RhinoLaryngo Slim and performed FEES were identified. At each identified facility, speech–language pathologists who performed FEES previously, maintained their FEES competency and had previously used reusable flexible rhinolaryngoscopes for FEES exams were recruited. Each procedure was performed on a patient who previously met the parameters for a swallow study and had a FEES exam ordered by their physician. The speech–language pathologist student did not perform a FEES procedure with the single-use rhinolaryngoscope and is therefore not included in the primary outcome.
Once clinicians completed a FEES exam, a survey questionnaire with a five-point rating system to quantify the product performance from Unacceptable (1) to Excellent (4–5) was given, with the midpoint rating Acceptable (2–3). This survey (Appendix 1) was developed by the authors and included various performance characteristics commonly used in endoscope comparison including ease of use, overall quality and functionality, look and feel of the scope, ease of insertion/airway inspection, bending capabilities/maneuverability, stiffness of insertion cord, image quality and monitor performance, single-use concept, accessibility/convenience, and overall performance. Once the data were complete, simple averages and proportions were calculated for each of the variables. For summary and presentation purpose, ratings of 4 and 5 were considered excellent, 2 and 3 acceptable, and 1 as nonacceptable. The speech–language pathologist student completed the survey and provided feedback on the single-use rhinolaryngoscope. The results are displayed with and without the speech–language pathologist student’s responses, as they did not perform a FEES procedure prior to completing the survey. Mean ratings for each performance metric captured in the survey were calculated and a one-sample t-test was performed for each variable.
Institutional Review Board approval was deemed not necessary or sought after for this study, as no patient data were collected and the single-use rhinolaryngoscopes were already approved and in-use at the respective facilities.
Results
Of the 23 FEES evaluations performed with single-use rhinolaryngoscope and monitor, 23/23 were completed without the use of a secondary scope, resulting in 100% procedural success. The number of attempts to pass the single-use rhinolaryngoscope prior to procedural success were not captured, but it is of note that no secondary scopes were required to complete the procedure.
Results from the survey can be found in Table 1. Proportions of ratings were calculated for each metric and can be found in Figure 1.
| Attribute | Overall rating | Excellent (rating of 4–5) | Acceptable (rating of 3-2) | Less than acceptable (rating of 1) | p-value |
|---|---|---|---|---|---|
| Ease of use | 4.8 | 100% (23/23) | – | – | p < 0.001 |
| Overall quality and functionality | 4.4 | 95% (22/23) | 5% (1/23) | – | p < 0.001 |
| Look and feel | 4.7 | 95% (22/23) | 5% (1/23) | – | p < 0.001 |
| Ease of insertion/airway inspection | 4.8 | 100% (23/23) | – | – | p < 0.001 |
| Bending capability/maneuverability | 4.8 | 100% (23/23) | – | – | p < 0.001 |
| Stiffness of insertion cord | 4.5 | 90% (21/23) | 10% (2/23) | – | p < 0.001 |
| Image quality and monitor performance | 4.2 | 90% (21/23) | 10% (2/23) | – | p < 0.001 |
| Single-use concept/no cross-contamination risk | 5.0 | 100% (23/23) | – | – | p < 0.001 |
| Accessibility/convenience/speed of setting up | 5.0 | 100% (23/23) | – | – | p < 0.001 |
| Overall performance (n = 23) | 4.6 | 100% (23/23) | – | – | p < 0.001 |
| Overall performance (n = 24)† | 4.6 | 100% (24/24) | – | – | p < 0.001 |
†
The student only completed ratings for ease of use, overall quality and functionality. With the inclusion of their rating for these 3 categories the overall ratings remained the same.
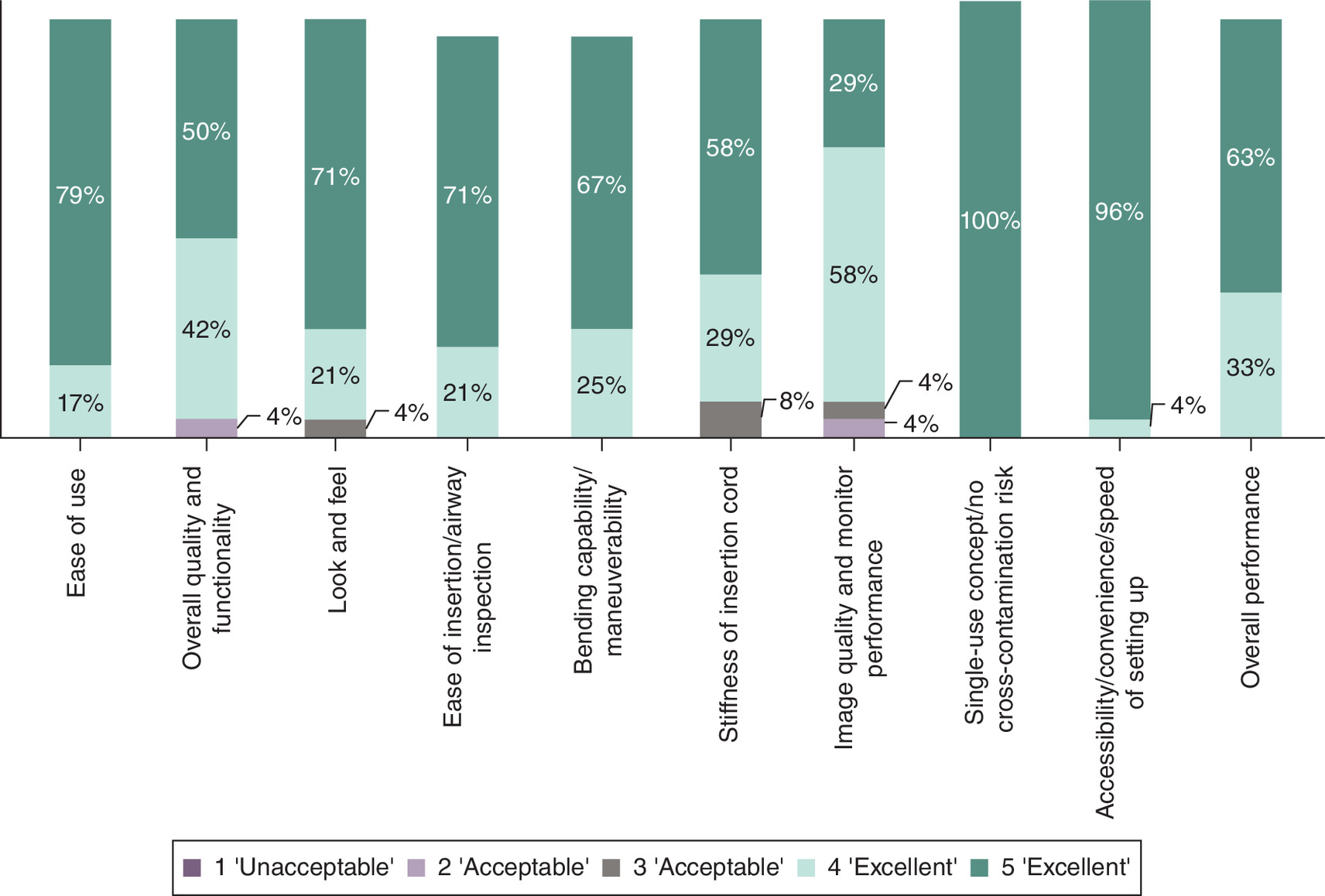
The overall rating of the single-use rhinolaryngoscope and monitor was 4.6 with 100% of participants rating the scope performance excellent. Furthermore, 100% of those who used the scope for a FEES procedure found the scope’s overall performance to be excellent (4.6). In addition to overall rating, ease of use (4.8), ease of insertion/airway inspection (4.8), bending capability/maneuverability (4.8), single-use concept/no cross-contamination risk (5.0), and accessibility/convenience/speed of setting up (5.0), were all rated as excellent with 100% of respondents rating these variables as either a 4 or a 5. Overall quality and functionality as well as look and feel were both rated excellent by 95% of participants (4.4 and 4.7, respectfully). At last, both stiffness of insertion cord (4.5) and image quality and monitor performance (4.2) were rated as excellent by 90% of participants.
Discussion
The introduction of single-use endoscopes for use in FEES procedures could play a key role in keeping up with the growing demand [6]. Speech–language pathologists and clinicians who utilize single-use endoscopes are enabled to take the procedure to the patient at any time, without being limited to specific procedure rooms with stationary endoscopy equipment, worrying about delays due to endoscope reprocessing, or having to transport burdensome endoscopy towers throughout the hospital. In addition to the ease and availability of the single-use scope, the portable high-powered display allows for necessary and required recording and documentation [6], further demonstrating the added compatibility and ease in utilizing single-use scopes for these procedures. Other areas in medicine that utilize endoscopes, such as endourology, have seen investigators investigate the workflow impact of single-use endoscopes. One investigation found that the utilization of single-use cystoscopes, with the ease-of-use and portability features, has enabled facilities to perform procedures in new settings while freeing up operating rooms for more elective surgeries and procedures [14].
While our findings highlight the high rating and performance capability of single-use rhinolaryngoscopes for speech–language pathologists, this study is not without limitations.
First, the size of our study included 23 speech–language pathologists and did not evaluate multiple FEES procedures with the single-use platform which may impact the ratings provided. Additionally, participants did not evaluate a reusable flexible rhinolaryngoscope or other single-use comparator during the study. Therefore, these results may not be generalizable across all single-use manufacturers, users and facilities in the US and does not capture the comparative performance capability of reusable flexible rhinolarygnoscopes for FEES, which are commonly used in practice today.
Second, the cost to perform a FEES procedure will vary across facilities. In one recent study, one reusable flexible nasopharyngolaryngoscope and digital video tower with components amounted to more than $33,000 [15] alone, without including the costs of repairs or reprocessing annually. Cost to perform FEES with reusable endoscopes and accompanying equipment will depend on procedural volumes, quantity of reusable endoscopes available for FEES use, and method of reprocessing the reusable endoscopy equipment, among others. Single-use rhinolaryngoscopes offer a fixed cost per scope and avoid the variable costs associated with reprocessing, services and repairs. The cost per single-use scope may vary depending on volume agreements and contracts but has been shown to cost as much as $170.36 per procedure in peer-reviewed evidence [15].
Physicians and speech–language pathologists exploring the expansion of their FEES procedures or the option of developing a mobile FEES department or capability should evaluate the required equipment [3], the annual FEES case load and various procedure settings to better understand the respective costs. In addition to financial implications of single-use endoscopy related to FEES procedures, there has not been a published investigation into the impact on organizational workflow that speech–language pathologists could experience with single-use rhinolaryngoscopes. A full investigation evaluating procedure duration, transportation, set up, and annual patient throughput should be captured to measure the magnitude of impact that single-use rhinolaryngoscopes may have.
Conclusion
Speech–language pathologists successfully completed 100% of the FEES procedures with single-use rhinolaryngoscopes. The scopes received a high overall rating and scores across each performance measure in the survey, demonstrating that single-use rhinolaryngoscopes can be utilized for FEES procedures. By eliminating the availability and portability concerns of traditional endoscopy equipment and possessing the documentation capabilities required for FEES, single-use rhinolaryngoscopes can meet the growing demand of FEES procedures and create a streamlined workflow. A faster, more mobile procedure design could assist in the expansion of FEES into more diagnostic areas, such as an ENT indication for assessing laryngopharyngeal reflux or for patient assessment for discharge after extubation [6]. Laryngopharyngeal reflux is primarily an ENT indication but presents an area of potential expanded use of FEES across healthcare settings. Single-use rhinolaryngoscopes were shown to successfully complete FEES procedures, and may provide significant cost and workflow benefits for clinicians across multiple settings as the demand and utilization of FEES continues to grow.
Summary points
•
Single-use endoscopes are of interest across a multitude of procedure types given the risk of cross-contamination, and availability of scopes.
•
This study aimed to measure flexible endoscopic evaluation of swallowing (FEES) procedural success with single-use rhinolaryngoscopes without the need for a secondary scope.
•
It also evaluated the overall performance and usability of the single-use platform.
•
A total of 23 speech–language pathologists across 16 sites performed FEES procedures with the Ambu aScope 4 RhinoLaryngo Slim, after which participants completed a nine-question survey questionnaire. A five-point rating system was used to quantify scope performance.
•
The primary end point of procedural success was achieved in 100% of procedures.
•
Of the nine performance metrics captured for aScope 4 RhinoLaryngo Slim, six received a score of excellent by 100% of participants with the lowest score being a 4.2.
•
It was concluded that single-use rhinolaryngoscopes can successfully perform FEES procedures without additional scoping needed, and received high performance ratings among users.
Acknowledgments
Abstract presented at the Combined Otolaryngology Spring Meetings (MA, USA), 3–7 May 2023.
Financial disclosure
The authors received no financial and/or material support for this research or the creation of this work.
Competing interests disclosure
C Cool, I Haislip, and C Escobar are paid employees of Ambu USA. J Mojica is a paid contractor of Ambu USA. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This study did not require Institutional Review Board approval.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
Oropharyngeal dysphagia. UCLA Health, Accessed: 14 April 2025: https://www.uclahealth.org/medical-services/gastro/esophageal-health/diseases-we-treat/dysphagia/oropharyngeal-dysphagia
2.
Fiberoptic evaluation of swallowing. Johns Hopkins Medicine (2021). Accessed: 13 March 2023: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/fiberoptic-evaluation-of-swallowing
3.
Langmore SE. History of fiberoptic endoscopic evaluation of swallowing for evaluation and management of pharyngeal dysphagia: changes over the years. Dysphagia 32(1), 27–38 (2017).
4.
Helliwell K, Hughes VJ, Bennion CM, Manning-Stanley A. The use of videofluoroscopy (VFS) and fibreoptic endoscopic evaluation of swallowing (fees) in the investigation of oropharyngeal dysphagia in stroke patients: a narrative review. Radiography 29(2), 284–290 (2023).
5.
Jia L, Yan C, Liu R et al. Early application value of flexible laryngoscope swallowing function assessment in patients after partial laryngectomy. Sci. Rep. 15(1), 6040 (2025).
6.
Langmore SE, Scarborough DR, Kelchner LN et al. Tutorial on clinical practice for use of the fiberoptic endoscopic evaluation of swallowing procedure with adult populations: part 1. Am. J. Speech Lang. Pathol. 31(1), 163–187 (2022).
7.
Ofstead CL, Quick MR, Eiland JE, Adams SJ. A glimpse at the true cost of reprocessing endoscopes. Available at: https://www.bostonscientific.com/content/dam/bostonscientific/uro-wh/portfolio-group/LithoVue/pdfs/Sterilization-Resource-Handout.pdf
8.
Hoffman D, Cool C. Costs involved in compliance with new endoscope reprocessing guidelines. Clin. Endosc. 57(4), 534–541 (2024).
9.
Association for the Advancement of Medical Instrumentation (AAMI). ANSI/AAMI ST91:2021; Flexible and semi-rigid endoscope processing in health care facilities. Accessed: 14 November 2022: https://www.aami.org/st91
10.
Ofstead CL, Smart AG, Hopkins KM, Wetzler HP. The utility of lighted magnification and borescopes for visual inspection of flexible endoscopes. Am. J. Infect. Control. 51(1), 2–10 (2023).
11.
KARL STORZ Endoskope | United States. CMOS video rhino-laryngoscope SSU. Accessed: 11 April 2025: https://www.karlstorz.com/us/en/product-detail-page.htm?productID=1000134204&cat=1000248211
12.
E-SteriScope™ single-use Rhinolaryngoscope. Medical Accessed: 11 April 2025: https://medical.olympusamerica.com/products/e-steriscope
13.
O'Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad. Med. 89(9), 1245–1251 (2014).
14.
Oderda M, Antolini J, Falcone M, Lacquaniti S, Fasolis G. Cost-effectiveness analysis of a single-use digital flexible cystoscope for double J removal. Urologia 87(1), 29–34 (2020).
15.
Walczak R, Arnold M, Grewal J, Yuan X, Suryadevara A, Marzouk H. Reusable vs disposable nasopharyngolaryngoscopes: cost analysis and resident survey. Laryngoscope Investig. Otolaryngol. 6(1), 88–93 (2020).
Information & Authors
Information
Published In
Copyright
© 2025 Ambu USA. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 16 July 2024
Accepted: 30 April 2025
Published online: 4 June 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Single-use endoscopy for the evaluation of swallowing: a performance survey. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0113
Export citation
Select the citation format you wish to export for this article or chapter.