Overall survival in patients with metastatic castration-sensitive prostate cancer treated with apalutamide versus abiraterone acetate: a head-to-head analysis of real-world patients in the USA
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Head-to-head studies of survival outcomes associated with different androgen receptor pathway inhibitor (ARPI) treatments for metastatic castration (hormone)-sensitive prostate cancer have not been conducted. The purpose of this study was to compare 24-month overall survival among ARPI-naive patients with metastatic castration-sensitive prostate cancer (mCSPC) who initiated apalutamide or abiraterone acetate. Materials & methods: Linked de-identified clinical and claims healthcare databases were used to compare overall survival between patients with mCSPC initiating apalutamide or abiraterone acetate treated in community-based urology practices in the USA. Overall survival at 24 months post-treatment initiation (primary analyses) was compared between apalutamide and abiraterone acetate initiators using weighted Cox proportional hazards models (exploratory analyses used all available follow-up). Results: Overall, 1879 and 2073 patients had initiated apalutamide or abiraterone acetate, respectively (both cohorts: weighted mean age 72 years, 62% were white, and 66% had bone metastasis). At 24 months post-index, patients in the apalutamide cohort had a 26% lower risk of mortality compared with those in the abiraterone acetate cohort (hazard ratio: 0.74; 95% confidence interval: 0.59, 0.93; p = 0.010), with the difference maintained when outcomes were evaluated using all available follow-up (hazard ratio: 0.72; 95% confidence interval: 0.59, 0.88; nominal p < 0.001). Conclusion: In this nationally representative, real-world head-to-head analysis of nearly 4000 ARPI-naive patients with mCSPC, apalutamide was associated with a 26% reduction in the risk of mortality compared with abiraterone acetate by 24 months post-treatment initiation.
Graphical abstract

Plain language summary
What was the aim of the study?
This retrospective longitudinal study compared 24-month overall survival between patients with metastatic castration-sensitive prostate cancer who were treated with apalutamide versus abiraterone acetate in the USA.
How was the research carried out?
A head-to-head, comparative effectiveness analysis was conducted between androgen receptor pathway inhibitor-naive patients treated with apalutamide versus abiraterone acetate using linked de-identified clinical and claims healthcare databases. Inverse probability of treatment weighting was used to balance patient baseline characteristics.
What were the results?
By 24 months after treatment initiation, there was a statistically significant 26% reduction in the risk of mortality among patients who initiated apalutamide (n = 1879) compared with abiraterone acetate (n = 2073; p = 0.010), which remained consistent in the exploratory analysis using all available follow-up data.
Why are findings important?
The results of this study show that compared with abiraterone acetate, initial treatment with apalutamide resulted in better real-world survival outcomes for patients with metastatic castration-sensitive prostate cancer and may provide a superior treatment option in clinical practice.
The addition of oral androgen receptor pathway inhibitors (ARPIs) to frontline androgen deprivation therapy (ADT) has become increasingly recommended for the treatment of metastatic castration-sensitive prostate cancer (mCSPC), which is also known as metastatic hormone-sensitive prostate cancer, given superior patient outcomes as compared with treatment with ADT alone [1–3].
Apalutamide is an ARPI that was approved in combination with ADT by the US FDA for the treatment of patients with mCSPC based on the results of the phase III TITAN clinical trial [4–6]. Based on the final survival analyses from TITAN, the combination of apalutamide and ADT was found to be associated with a 35% reduction in the risk of mortality relative to placebo and ADT (p < 0.001) [5]. Abiraterone acetate is another ARPI approved in combination with prednisone and ADT by the US FDA for the treatment of patients with high-risk mCSPC (i.e., Gleason score ≥8, ≥3 bone lesions or the presence of measurable visceral metastasis) based on the results of the phase III LATITUDE clinical trial [7–9]. Survival analyses from LATITUDE demonstrated that the combination of abiraterone acetate plus prednisone and ADT was associated with a 34% reduction in the risk of mortality compared with placebo and ADT (p < 0.001) [8].
In a recent real-world study of patients with mCSPC, those who initiated apalutamide were 68% more likely to achieve a prostate-specific antigen (PSA) decline of ≥90% (PSA90) by 6 months in comparison to those who initiated abiraterone acetate (hazard ratio [HR]: 1.68; 95% confidence interval [CI]: 1.42, 2.00; p < 0.001) [10]. These findings are meaningful in the context of numerous studies including the TITAN and LATITUDE trials demonstrating deep, early PSA response as a clinically important indicator of treatment efficacy in this population, including long-term survival outcomes [11–15].
Currently, overall survival in patients with mCSPC initiating either of these two ARPIs has not been compared in the context of clinical trials or real-world studies. Increasingly, the use of real-world evidence has helped inform regulatory authorities and population health decision-makers with regards to treatment effectiveness given the lack of head-to-head clinical trials [16]. Given the availability of multiple ARPIs for the initial treatment of mCSPC, comparative data of important clinical outcomes are needed to guide treatment choice in clinical practice. To address this gap in knowledge, this study aimed to test the hypothesis that there was no difference in overall survival at 24 months between ARPI-naive patients with mCSPC who initiated treatment with either apalutamide or abiraterone acetate.
Materials & methods
The study was designed following FDA guidance on real-world evidence [17].
Data source
This study combined patient-level data from two sources: a clinical urology database (Precision Point Specialty Analytics; PPS) and an administrative claims database (Komodo Research Database; KRD). PPS is a proprietary software which collects a broad range of demographic and routine clinical data from collaborating private community-based urology practices in the USA, including PSA testing results and prostate cancer (PC)-specific medication details not found in standard databases. KRD, an insurance claims database covering over 320 million US patients, includes insurance eligibility, diagnoses, procedures and prescription information.
Overall survival analyses used mortality data reported in the KRD. Data on patient mortality are updated monthly and are obtained from multiple third-party sources, therefore not relying solely on data from healthcare providers. From an external validation, the KRD has identified >90% of all deaths reported in oncology settings between 2018 and 2023 to the US Centers for Disease Control [18]. Data from both sources were linked by Datavant using their patent-pending, machine-learning validated, de-identification technology. This algorithm substitutes confidential patient data with an encrypted token that cannot be decoded back into the original information.
This study was considered exempt research under 45 CFR § 46.104(d)(4) as it involved only the secondary use of data that were de-identified in compliance with the Health Insurance Portability and Accountability Act (HIPAA), specifically, 45 CFR § 164.514.
Study design
A retrospective, longitudinal analysis was performed using propensity score-weighted cohorts of ARPI-naive patients who began treatment with apalutamide or abiraterone acetate. This study employed an intention-to-treat design and covered the period from 17 September 2018 to 31 December 2023. Patients diagnosed with mCSPC were classified into mutually exclusive cohorts based on their first dispensation in PPS or a paid pharmacy claim in the KRD for apalutamide or abiraterone acetate, with the date of treatment initiation serving as the index date. Only patients who initiated treatment on or after 17 September 2019 [6] (i.e., FDA approval date for apalutamide) were selected, to ensure that both treatment options had been approved for use in patients with mCSPC (abiraterone acetate was approved by the FDA for use in high-risk mCSPC on 7 February 2018) [9].
The observation period spanned from the index date until the latter of open insurance claim activity in the KRD or clinical activity in PPS, both no later than 31 December 2023 (i.e., end of data). The baseline period was defined as the 12 month pre-index period. Following an intention-to-treat design, patients were not censored if they discontinued the index ARPI, switched to another ARPI, initiated therapy with another advanced PC treatment or developed castration resistance after the index date.
Patient selection criteria
Patients were included in this analysis if they met all of the following criteria: initiated apalutamide or abiraterone acetate on or after 17 September 2019, had ≥12 months of claims or clinical activity and had evidence of metastasis based on diagnosis codes or clinical indicators for bone, nodal or visceral metastasis in PPS. Patients were excluded from the study if they initiated index treatment prior to 17 September 2019, were treated with ≥2 ARPIs on the index date, were diagnosed with another primary cancer during the baseline period, had a prescription for a nonindex ARPI in PPS, were castration-resistant prior to or on the index date (for details see Supplementary Table 1) [19], used estrogens, immunotherapy, PARP inhibitors, radiopharmaceuticals or etoposide or used either cabazitaxel or carboplatin after docetaxel. Concurrent ADT use was not required for study inclusion and concurrent prednisone use was not required for inclusion in the abiraterone acetate cohort.
Study outcomes
Overall survival (i.e., time from the index date to the time of death from any cause) assessed at 24 months was the primary outcome. The following patient demographic and clinical characteristics were assessed prior to or on the index date: age, race, US geographic region, payer type, time between metastasis and index date, time between PC diagnosis and index date, metastases location, Quan-Charlson Comorbidity Index (Quan-CCI), de novo PC, ADT use overlapping the index date, prior first-generation ARPI use, prior chemotherapy, most recent PSA result and earliest Gleason score. ARPI treatment patterns were also assessed up to 24 months post-index.
Statistical analysis
The null hypothesis was that overall survival at 24 months was not different between patients initiating apalutamide or abiraterone acetate. The alternative hypothesis was that overall survival at 24 months was different between patients initiating apalutamide or abiraterone acetate. Inverse probability of treatment weighting (IPTW) was used to balance potentially confounding baseline variables between treatment cohorts. Propensity scores (PSs) were generated using a logistic regression model based on dependent (i.e., apalutamide initiation) and independent variables. Patients in the apalutamide and abiraterone acetate cohorts were attributed a weight of and , respectively, with weights normalized using the mean weight of each respective cohort and truncated to the 95th percentile [20]. No patients were removed from the study due to the IPTW model.
Baseline characteristics between treatment cohorts were considered balanced after weighting, as indicated by standardized differences of <10% [21]. Weighted Kaplan–Meier analyses were conducted to evaluate overall survival between treatment cohorts up to 48 months post-index. A weighted Cox proportional hazards model was used to calculate HRs and 95% CIs comparing overall survival between the apalutamide and abiraterone acetate cohorts at 24 months post-index (primary outcome) and using all follow-up data (exploratory outcome; nominal). As a sensitivity analysis, overall survival at 24 months post-index was compared between apalutamide and abiraterone acetate cohorts among a subgroup of patients who had a claim for ADT 180 days prior to the index date or within 180 days following the index date.
Results
Patient characteristics
This study of ARPI-naive patients with mCSPC included 1879 patients who initiated apalutamide and 2073 patients who initiated abiraterone acetate (Figure 1). Baseline characteristics were well-balanced between cohorts after IPTW weighting (i.e., standardized difference <10%; Table 1). In both cohorts, the median age was 72 years and most patients were white (apalutamide: 61.7%, abiraterone acetate: 62.5%) and insured with Medicare (apalutamide: 74.2%, abiraterone acetate: 73.5%). The majority of patients were diagnosed with bone metastasis (apalutamide: 66.5%, abiraterone acetate: 66.2%), with a median time between metastasis and ARPI initiation of <3 months (apalutamide: 2.5 months, abiraterone acetate: 2.8 months).
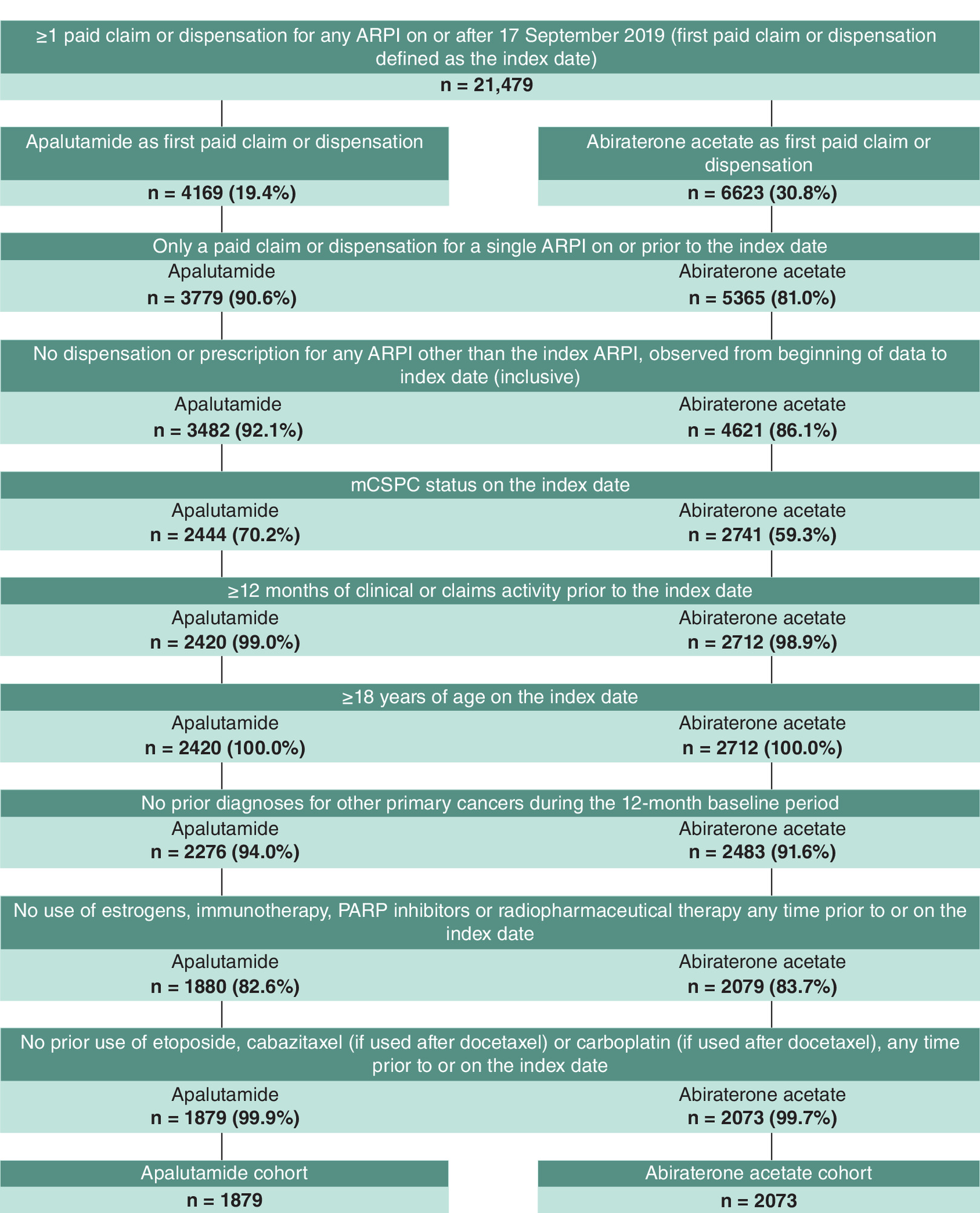
Figure 1. Sample selection.
ARPI: Androgen receptor pathway inhibitor; mCSPC: Metastatic castration-sensitive prostate cancer; PARP: Poly ADP-ribose polymerase.
| Nonweighted population | Weighted population† | |||||
|---|---|---|---|---|---|---|
| Apalutamide (n = 1879) | Abiraterone acetate (n = 2073) | Standardized difference, % | Apalutamide (n = 1879) | Abiraterone acetate (n = 2073) | Standardized difference, % | |
| Age, mean ± SD [Q1, median, Q3] | 72.9 ± 9.1 [67.0, 73.0, 80.0] | 71.2 ± 9.2 [65.0, 71.0, 78.0] | 18.4 | 72.1 ± 9.3 [66.0, 72.0, 79.0] | 71.9 ± 9.1 [65.0, 72.0, 78.0] | 2.5 |
| Race, n (%) | ||||||
| White | 1139 (60.6) | 1325 (63.9) | 6.8 | 1159 (61.7) | 1295 (62.5) | 1.6 |
| Black or African–American | 416 (22.1) | 317 (15.3) | 17.6 | 359 (19.1) | 374 (18.0) | 2.8 |
| Hispanic or Latino | 136 (7.2) | 151 (7.3) | 0.2 | 141 (7.5) | 152 (7.3) | 0.6 |
| Other | 71 (3.8) | 114 (5.5) | 8.2 | 85 (4.5) | 100 (4.8) | 1.3 |
| Unknown | 117 (6.2) | 166 (8.0) | 6.9 | 134 (7.1) | 152 (7.3) | 0.7 |
| Geographic region, n (%) | ||||||
| South | 1068 (56.8) | 744 (35.9) | 43.0 | 900 (47.9) | 923 (44.5) | 6.8 |
| Midwest | 421 (22.4) | 686 (33.1) | 24.0 | 515 (27.4) | 602 (29.0) | 3.6 |
| Northeast | 212 (11.3) | 353 (17.0) | 16.5 | 247 (13.1) | 296 (14.3) | 3.3 |
| West | 178 (9.5) | 290 (14.0) | 14.1 | 217 (11.5) | 253 (12.2) | 2.0 |
| Payer type, n (%) | ||||||
| Medicare | 1453 (77.3) | 1473 (71.1) | 14.4 | 1394 (74.2) | 1523 (73.5) | 1.7 |
| Commercial | 365 (19.4) | 506 (24.4) | 12.1 | 413 (22.0) | 462 (22.3) | 0.7 |
| Medicaid | 56 (3.0) | 82 (4.0) | 5.3 | 67 (3.6) | 73 (3.5) | 0.2 |
| Unknown | 5 (0.3) | 12 (0.6) | 0.0 | 5 (0.3) | 16 (0.8) | 0.0 |
| Index year, n (%) | ||||||
| 2019–2020 | 405 (21.6) | 504 (24.3) | 6.6 | 414 (22.0) | 473 (22.8) | 1.8 |
| 2021 | 447 (23.8) | 466 (22.5) | 3.1 | 444 (23.6) | 484 (23.3) | 0.8 |
| 2022 | 519 (27.6) | 528 (25.5) | 4.9 | 514 (27.4) | 555 (26.8) | 1.3 |
| 2023 | 508 (27.0) | 575 (27.7) | 1.6 | 506 (27.0) | 562 (27.1) | 0.4 |
| Time between metastasis and index date, months, mean ± SD [Q1, median, Q3] | 9.0 ± 17.9 [0.9, 2.3, 7.0] | 11.3 ± 17.6 [1.2, 3.4, 13.4] | 13.0 | 9.7 ± 17.6 [1.0, 2.5, 8.7] | 10.2 ± 17.1 [1.1, 2.8, 10.5] | 2.5 |
| Time between PC diagnosis and index date, months, mean ± SD [Q1, median, Q3] | 39.3 ± 46.9 [2.9, 14.9, 64.4] | 37.1 ± 46.9 [2.9, 13.3, 64.4] | 4.6 | 37.4 ± 45.5 [2.8, 14.1, 60.3] | 37.5 ± 47.7 [3.1, 12.8, 58.1] | 0.3 |
| Metastasis type‡, n (%) | ||||||
| Bone | 1311 (69.8) | 1339 (64.6) | 11.1 | 1249 (66.5) | 1373 (66.2) | 0.6 |
| Nodal | 960 (51.1) | 1,103 (53.2) | 4.2 | 994 (52.9) | 1097 (52.9) | 0.1 |
| Visceral | 335 (17.8) | 571 (27.5) | 23.4 | 396 (21.1) | 477 (23.0) | 4.7 |
| Metastasis in multiple sites | 536 (28.5) | 405 (19.5) | 21.2 | 477 (25.4) | 492 (23.7) | 3.9 |
| Quan-CCI, mean ± SD [Q1, median, Q3] | 8.5 ± 3.0 [8.0, 8.0, 10.0] | 8.6 ± 2.9 [8.0, 8.0, 10.0] | 1.4 | 8.5 ± 3.0 [8.0, 8.0, 10.0] | 8.5 ± 2.9 [8.0, 8.0, 10.0] | 0.7 |
| Any malignancy, including lymphoma and leukemia, except malignant neoplasm of skin, n (%) | 1869 (99.5) | 2040 (98.4) | 10.4 | 1865 (99.3) | 2048 (98.8) | 4.9 |
| Metastatic solid tumor, n (%) | 1595 (84.9) | 1793 (86.5) | 4.6 | 1589 (84.6) | 1783 (86.0) | 4.0 |
| Diabetes without chronic complication, n (%) | 451 (24.0) | 440 (21.2) | 6.6 | 452 (24.1) | 442 (21.3) | 6.6 |
| Renal disease, n (%) | 283 (15.1) | 307 (14.8) | 0.7 | 277 (14.7) | 304 (14.7) | 0.2 |
| Peripheral vascular disease, n (%) | 267 (14.2) | 314 (15.1) | 2.7 | 269 (14.3) | 307 (14.8) | 1.4 |
| Diabetes with chronic complication, n (%) | 235 (12.5) | 195 (9.4) | 9.9 | 237 (12.6) | 196 (9.5) | 10.0 |
| Chronic pulmonary disease, n (%) | 231 (12.3) | 272 (13.1) | 2.5 | 232 (12.4) | 262 (12.6) | 0.8 |
| Congestive heart failure, n (%) | 199 (10.6) | 196 (9.5) | 3.8 | 197 (10.5) | 192 (9.2) | 4.2 |
| Mild liver disease, n (%) | 164 (8.7) | 209 (10.1) | 4.6 | 177 (9.4) | 197 (9.5) | 0.3 |
| Cerebrovascular disease, n (%) | 128 (6.8) | 192 (9.3) | 9.0 | 122 (6.5) | 192 (9.3) | 10.2 |
| Myocardial infarction, n (%) | 81 (4.3) | 99 (4.8) | 2.2 | 81 (4.3) | 92 (4.4) | 0.7 |
| Dementia, n (%) | 41 (2.2) | 40 (1.9) | 1.8 | 41 (2.2) | 41 (2.0) | 1.4 |
| Rheumatic disease, n (%) | 38 (2.0) | 30 (1.4) | 4.4 | 34 (1.8) | 30 (1.5) | 2.7 |
| Peptic ulcer disease, n (%) | 20 (1.1) | 22 (1.1) | 0.0 | 18 (1.0) | 22 (1.1) | 1.1 |
| Hemiplegia or paraplegia, n (%) | 10 (0.5) | 25 (1.2) | 7.3 | 10 (0.5) | 21 (1.0) | 5.4 |
| Moderate or severe liver disease, n (%) | 6 (0.3) | 11 (0.5) | 3.3 | 5 (0.2) | 10 (0.5) | 4.0 |
| AIDS/HIV, n (%) | 0 (0.0) | 0 (0.0) | 0.0 | 0 (0.0) | 0 (0.0) | 0.0 |
| De novo PC§, n (%) | 1040 (55.3) | 1259 (60.7) | 10.9 | 1100 (58.5) | 1223 (59.0) | 1.0 |
| Concurrent use of ADT with index ARPI¶, n (%) | 1542 (82.1) | 1395 (67.3) | 34.5 | 1443 (76.8) | 1535 (74.0) | 6.4 |
| Duration of ADT episode overlapping with index date, months, mean ± SD [Q1, median, Q3] | 4.4 ± 8.5 [0.7, 1.8, 4.4] | 5.1 ± 8.3 [0.8, 2.0, 5.7] | 8.6 | 4.5 ± 8.0 [0.7, 1.8, 4.7] | 5.0 ± 8.3 [0.8, 1.9, 5.2] | 6.4 |
| Prior use of first-generation ARPI#, n (%) | 297 (15.8) | 437 (21.1) | 13.6 | 343 (18.2) | 396 (19.1) | 2.2 |
| Prior use of chemotherapy††, n (%) | 30 (1.6) | 102 (4.9) | 18.8 | 51 (2.7) | 72 (3.5) | 4.6 |
| PSA level, ng/ml, n (%) | ||||||
| ≤0.2 | 325 (17.3) | 246 (11.9) | 15.4 | 288 (15.3) | 298 (14.4) | 2.7 |
| >0.2 to ≤2 | 309 (16.4) | 265 (12.8) | 10.4 | 286 (15.2) | 296 (14.3) | 2.7 |
| >2 to ≤5 | 214 (11.4) | 161 (7.8) | 12.3 | 186 (9.9) | 194 (9.3) | 1.9 |
| >5 to ≤10 | 194 (10.3) | 141 (6.8) | 12.6 | 168 (9.0) | 172 (8.3) | 2.3 |
| >10 | 558 (29.7) | 541 (26.1) | 8.0 | 533 (28.4) | 577 (27.8) | 1.3 |
| Unknown | 279 (14.8) | 719 (34.7) | 47.2 | 417 (22.2) | 537 (25.9) | 8.7 |
| Earliest Gleason score‡‡, n (%) | ||||||
| ≤6 | 110 (5.9) | 85 (4.1) | 8.1 | 94 (5.0) | 97 (4.7) | 1.6 |
| 7 | 370 (19.7) | 355 (17.1) | 6.6 | 355 (18.9) | 383 (18.5) | 1.1 |
| 8 | 263 (14.0) | 320 (15.4) | 4.1 | 276 (14.7) | 311 (15.0) | 0.9 |
| 9 | 405 (21.6) | 430 (20.7) | 2.0 | 408 (21.7) | 446 (21.5) | 0.6 |
| 10 | 56 (3.0) | 66 (3.2) | 1.2 | 60 (3.2) | 65 (3.2) | 0.3 |
| Unknown | 675 (35.9) | 817 (39.4) | 7.2 | 685 (36.5) | 771 (37.2) | 1.5 |
†
The number of patients reported in this weighted population represents the sum of weights for the corresponding nonweighted patients, rounded to the nearest integer. The proportions displayed were calculated before the rounding and may be slightly different than if they were calculated based on rounded numbers.
‡
Types of metastases were defined at any time prior to (and including) the index date. Types of metastases were not mutually exclusive.
§
De novo PC was defined as ≤180 days between first observed PC diagnosis and date of metastasis.
¶
Concurrent ADT use was defined as an episode of continuous ADT use overlapping with the index date (using a 60-day gap to define discontinuation).
#
Prior use of first-generation ARPI was defined as any prescription for bicalutamide, nilutamide or flutamide in the 12 months preceding the index date.
††
Prior chemotherapy use was defined as any administration in the 12 months preceding the index date.
‡‡
Gleason score was evaluated at any time prior to and including the index date.
ADT: Androgen deprivation therapy; ARPI: Androgen receptor pathway inhibitor; CCI: Charlson Comorbidity Index; PC: Prostate cancer; PSA: Prostate-specific antigen; Q1: First quartile; Q3: Third quartile; SD: Standard deviation.
Overall survival
Patients who initiated apalutamide were 26% less likely to have died at 24 months post-index compared with those treated with abiraterone acetate (HR: 0.74; 95% CI: 0.59, 0.93; p = 0.010; Figure 2). The trend toward a lower risk of mortality among patients who initiated apalutamide compared with those who initiated abiraterone acetate was consistent throughout the entire follow-up period (HR: 0.72; 95% CI: 0.59, 0.88; nominal p < 0.001). At 24 months post-index, 88.7% of patients in the apalutamide cohort and 85.8% of patients in the abiraterone acetate cohort remained alive. By 48 months post-index, 77.3% of patients in the apalutamide cohort and 69.4% of patients in the abiraterone acetate cohort remained alive (median overall survival was not reached in either cohort). Results from the sensitivity analysis of patients with a claim for ADT 180 days before or 180 days after the index date were largely consistent with the primary analysis (HR: 0.78; 95% CI: 0.62, 0.98; nominal p = 0.035).
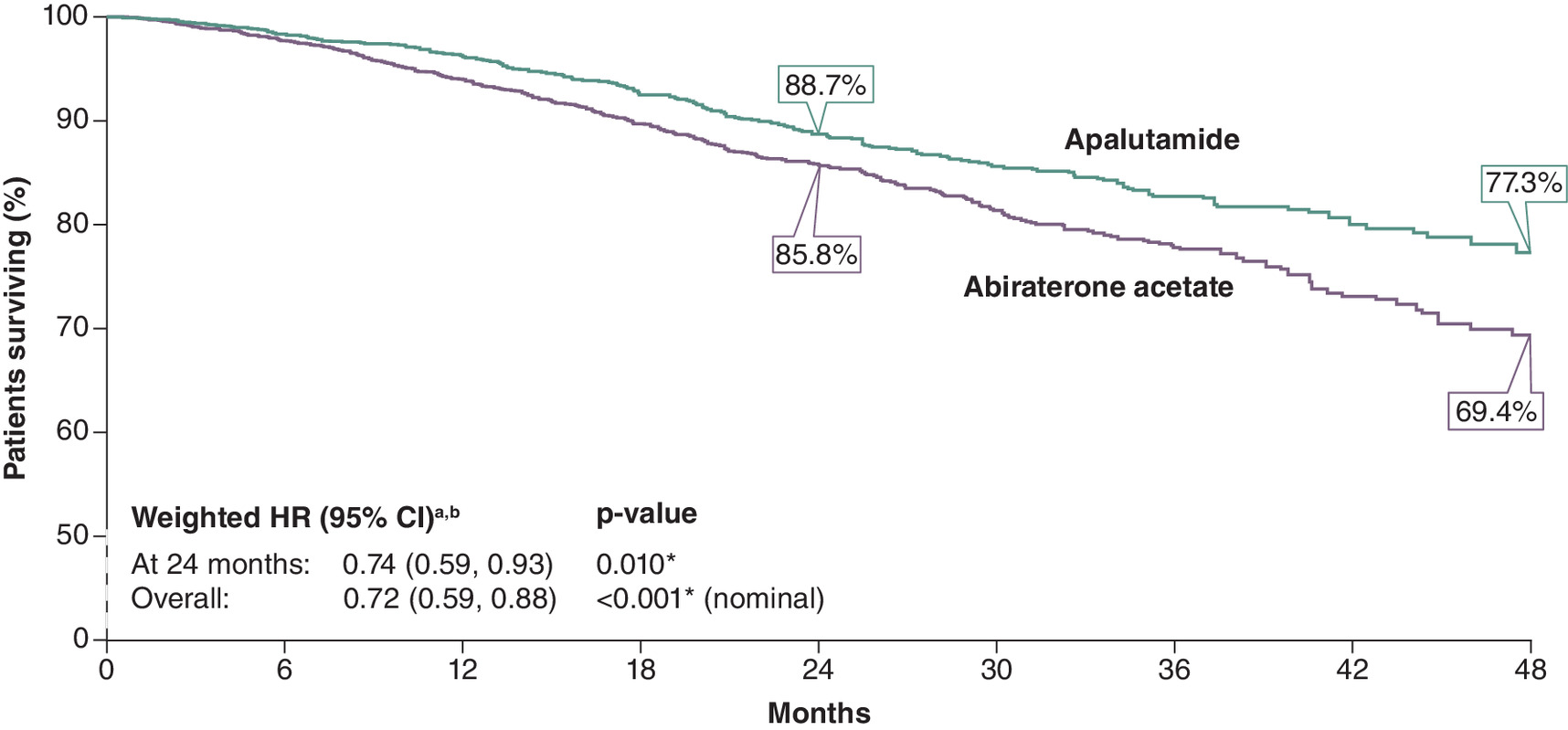
Figure 2. Overall survival between patients who initiated apalutamide versus abiraterone acetate.
aPropensity scores were generated using probability estimates from a logistic regression models using the following predictors: age (continuous), race, geographic region, payer type, year of index date, time between metastasis and index date (continuous and categorical), time between PC diagnosis and index date (continuous), de novo PC, ADT use overlapping with index date, first-generation androgen receptor pathway inhibitor use, chemotherapy use, metastases location (bone, nodal, visceral and metastasis in multiple sites), Quan–Charlson Comorbidity Index (continuous), most recent prostate-specific antigen level (categorical) and earliest Gleason score (categorical). Each patient was attributed an inverse-probability of treatment weight that was defined as follows: 1/(propensity score) for the apalutamide cohort and 1/(1-propensity score) for the abiraterone acetate cohort. Normalized inverse-probability of treatment weights were truncated at the 95th percentiles.
bAn HR <1 indicates that the apalutamide cohort had a lower rate of death compared with the abiraterone acetate cohort.
*Significant at the 5% level.
ADT: Androgen deprivation therapy; CI: Confidence interval; HR: Hazard ratio; PC: Prostate cancer.
Treatment patterns
The mean (median) follow-up period was 16.8 (19.5) months in the apalutamide cohort and 16.3 (19.0) months in the abiraterone acetate cohort (Table 2). The mean (median) duration of continuous index ARPI use was 9.3 (6.6) months among patients who initiated apalutamide and 10.7 (8.9) months among patients who initiated abiraterone acetate. The index treatment was discontinued by 55.6% of patients in the apalutamide cohort and 44.8% of patients in the abiraterone acetate cohort. In both cohorts, most patients who discontinued the index ARPI were re-treated with a different ARPI.
| Weighted population† | ||
|---|---|---|
| Apalutamide (n = 1879) | Abiraterone acetate (n = 2073) | |
| Follow-up length‡, months, mean ± SD [median] | 16.8 ± 7.5 [19.5] | 16.3 ± 7.8 [19.0] |
| Duration of continuous use of index ARPI§, months, mean ± SD [median] | 9.3 ± 7.9 [6.6] | 10.7 ± 7.4 [8.9] |
| Patients who discontinued index ARPI¶, n (%) | 1045 (55.6) | 929 (44.8) |
| Patients with no additional treatment after discontinuation, n (%) | 692 (36.8) | 636 (30.7) |
| Patients who received different advanced PC medication after discontinuation of index ARPI#, n (%) | 353 (18.8) | 294 (14.2) |
| Time to first advanced PC medication after discontinuation of index ARPI, months, mean ± SD [median] | 4.9 ± 5.4 [2.6] | 3.3 ± 4.3 [1.0] |
| First advanced PC medication received after discontinuation of index ARPI, n (%) | ||
| Non-index ARPI†† | 170 (9.0) | 144 (6.9) |
| Enzalutamide | 78 (4.2) | 93 (4.5) |
| Abiraterone acetate | 70 (3.7) | – |
| Darolutamide | 22 (1.2) | 14 (0.7) |
| Apalutamide | – | 37 (1.8) |
| Immunotherapies | 38 (2.0) | 18 (0.9) |
| Chemotherapies | 69 (3.7) | 77 (3.7) |
| Estrogens | 56 (3.0) | 19 (0.9) |
| Radiotherapy | 12 (0.6) | 26 (1.3) |
| PARP inhibitors | 9 (0.5) | 10 (0.5) |
†
The number of patients reported in this weighted population represents the sum of weights for the corresponding non-weighted patients, rounded to the nearest integer. The proportions displayed were calculated before the rounding and may be slightly different than if they were calculated based on rounded numbers.
‡
Follow-up length was defined as the index date until the latter of the end of open insurance claim activity in Komodo, clinical activity in PPS (both no later than 31 December 2023). The observation period was censored such that it is not longer than 24 months.
§
Continuous use was reported from the first ARPI episode observed in the observation period. Continuous use of ARPI was defined as the time from the date of the first paid pharmacy or dispensation claims to the last day of supply before a gap greater than 90 days.
¶
Discontinuation of index ARPI was assessed using >90-day gap in days of supply.
#
Includes patients with a record for an advanced PC medication different from the index ARPI; advanced PC medication use was assessed from the date of index ARPI discontinuation until the end of the observation period.
††
Defined as a record for another ARPI than the one initiated on the index date.
ARPI: Androgen receptor pathway inhibitor; PARP: Poly ADP-ribose polymerase; PC: Prostate cancer; SD: Standard deviation.
Discussion
This retrospective analysis performed in a large administrative and clinical-linked database in the USA presents the first comparative evidence of real-world overall survival between ARPI-naive patients with mCSPC who initiated treatment with apalutamide or abiraterone acetate. At 24 months post-treatment initiation, apalutamide was associated with a 26% statistically significant reduction in the risk of mortality compared with abiraterone acetate. This improvement in overall survival associated with apalutamide versus abiraterone acetate treatment among patients with mCSPC remained when assessed using all the available follow-up data. Given the greater diversity in the population in the current study in terms of demographics and clinical characteristics, these results are more generalizable to the broader mCSPC population than those enrolled in the TITAN [4] and LATITUDE [7] trials.
The findings of this study are consistent with those of an initial analysis of retrospective data from the Flatiron metastatic PC Core Registry (2013–2023) based on approximately 850 ARPI-naive patients with mCSPC [22]. Specifically, the study showed that by 24 months post-treatment initiation, apalutamide was associated with a 40% reduction in the risk of mortality compared with abiraterone acetate [22]. However, no adjustment between the two treatment cohorts was conducted and the authors noted the possible impact of confounding variables. By leveraging linked insurance claims and clinical data, the current study was able to evaluate PC-specific outcomes among a larger sample of nearly 2000 patients per treatment cohort. Additionally, the use of IPTW to balance potentially confounding baseline variables between the two treatment cohorts mitigated their impact and enabled a more accurate estimation of the comparative treatment effects.
The overall survival rates reported by 12 and 24 months post-treatment initiation among patients who initiated apalutamide in the current study (96.2% and 88.7%, respectively) are consistent with a recent descriptive study by Lowentritt et al. based on retrospective data, also from the Flatiron metastatic PC Core Registry, which reported overall survival rates of 91.0% by 12 months and 88.3% by 24 months post-apalutamide initiation [23]. Although to our knowledge, no studies outside the USA have compared overall survival between these treatments, the rates observed in our study are consistent with non-US studies reporting overall survival for each treatment, separately. For example, recent clinical studies from Japan and Spain among patients with mCSPC treated with apalutamide reported overall survival rates >80% by 24 months post-treatment initiation, which were similar to the current study [24,25]. Furthermore, aligned with the results from the current study, real-world overall survival rates among patients with mCSPC treated with abiraterone acetate were 89% by 12 months post-treatment initiation in a study from Belgium and >80% by 24 months in a study from Hong Kong [26,27].
The clinical benefit of apalutamide over abiraterone acetate for the treatment of ARPI-naive patients with mCSPC has been previously demonstrated in retrospective studies based on clinical data from community urology practices evaluating the attainment of a deep, rapid PSA response within 6 months of treatment initiation [10,28]. These studies showed that achieving a PSA90 response was 53–68% more likely among patients who initiated apalutamide compared with abiraterone acetate [10,28]. In post hoc analyses of the key ARPI phase III trials, deep PSA response, which is defined by ≥90% relative decline (i.e., PSA90), has been identified as an important indicator of long-term clinical outcomes, including overall survival [11–15]. Therefore, while the causal link between the improved overall survival observed with apalutamide versus abiraterone acetate cohorts in this study remains to be confirmed, the difference in PSA response achieved by patients with mCSPC who initiate apalutamide versus abiraterone acetate may be linked to the reduction in the risk of mortality observed in the current study and warrants consideration in clinical practices to guide treatment decision making.
Limitations
This study has potential limitations including the possibility of miscoding or misclassification in either database that could influence patient characterization or capture in death records. The IPTW analysis accounts for documented baseline covariates, however minimal adjustments were made to account for missing data (if present, missing values were included as a separate category for categorical variables in order to preserve the sample during IPTW), and potentially unknown confounders may be present. Abiraterone acetate with prednisone, which was not required for study inclusion and was observed at variable dosing, is indicated for high-risk mCSPC, which may result in residual differences relative to the apalutamide cohort after IPTW adjustments [9]. It is worth noting that the presence of visceral metastases, which can reflect high-risk disease, was well-balanced between the cohorts after IPTW. Additional studies with longer follow-up may be necessary to assess the full therapeutic effects of these medications.
Conclusion
This head-to-head analysis of real-world overall survival outcomes among ARPI-naive patients with mCSPC in the USA showed that patients who initiated treatment with apalutamide had a 26% statistically significant reduction in the risk of mortality compared with abiraterone acetate at 24 months post-treatment initiation. This finding remained consistent when overall survival was assessed using all available follow-up data. These results suggest that apalutamide may represent a superior treatment option compared with abiraterone acetate for patients with mCSPC.
Summary points
•
Apalutamide and abiraterone acetate are two androgen receptor pathway inhibitors (ARPIs) which were approved in combination with androgen deprivation therapy for the treatment of patients with metastatic castration-sensitive prostate cancer (mCSPC).
•
Outside of phase III clinical trials, there are limited real-world data reporting survival outcomes in patients with mCSPC treated with ARPIs, and no head-to-head studies have been performed.
•
This longitudinal study compared 24-month overall survival between ARPI-naive patients with mCSPC who initiated apalutamide versus abiraterone acetate in the USA.
•
The study linked de-identified patient-level data from a clinical urology database (Precision Point Specialty Analytics) and an administrative claims database (Komodo Research Database) between 17 September 2018 and 31 December 2023.
•
Comparisons between patients were conducted using weighted Cox proportional hazards models after inverse probability of treatment weighting was applied to balance baseline characteristics.
•
By 24 months after treatment initiation, there was a statistically significant 26% reduction in the risk of mortality among patients who initiated apalutamide (n = 1879) compared with abiraterone acetate (n = 2073; p = 0.010).
•
This survival benefit observed with apalutamide versus abiraterone acetate remained consistent in the exploratory analysis using all available follow-up data (hazard ratio: 0.72; nominal p < 0.001).
•
These findings suggest that apalutamide may represent a superior treatment option compared with abiraterone acetate among patients with mCSPC.
Author contributions
All authors have made substantial contributions to the conception or design of the study, or the acquisition, analysis or interpretation of data, drafting the manuscript and revising it critically for important intellectual content, and have provided final approval of this version to be published and agree to be accountable for all aspects of the work.
Acknowledgments
The authors thank David Caviedes Combita, an intern for Analysis Group, Inc. at the time the study was conducted, and Kruti Joshi and Sabree Burbage, employees of Johnson & Johnson, for their contributions to this study.
Financial disclosure
This study was funded by Johnson & Johnson. The study sponsor was involved in several aspects of the research, including the study design, interpretation of data and writing of the manuscript.
Competing interests disclosure
B Lowentritt is an employee of Chesapeake Urology and has received consulting fees from Johnson & Johnson, Dendreon, Astellas Pharma, Bayer, AstraZeneca/MedImmune, Merck, Tolmar, Abbvie, Pfizer and Myovant Sciences. MA Bilen has acted as a paid consultant for and/or as a member of the advisory boards of Exelixis, Bayer, BMS, Eisai, Pfizer, AstraZeneca, Johnson & Johnson, Calithera Biosciences, Genomic Health, Nektar, EMD Serono, SeaGen and Sanofi and has received grants to his institution from Merck, Xencor, Bayer, Bristol-Myers Squibb, Genentech/Roche, SeaGen, Incyte, Nektar, AstraZeneca, Tricon Pharmaceuticals, Genome & Company, AAA, Peloton Therapeutics and Pfizer for work performed outside of the current study. I Khilfeh and S Du are employees and stockholders of Johnson & Johnson. C Rossi, F Kinkead, L Diaz and D Pilon are employees of Analysis Group, Inc., a consulting company that has provided paid consulting services to Johnson & Johnson. L Ellis was an employee of Johnson & Johnson at the time the study was conducted. ND Shore is an employee of the Carolina Urologic Research Center and has received consulting fees from Johnson & Johnson, Bayer, Dendreon, Tolmar, Ferring, Medivation/Astellas, Amgen, Pfizer, AstraZeneca, Astellas Pharma, AbbVie, Merck, Bristol Myers Squibb/Sanofi, Exact Imaging, FerGene, InVitae, MDxHealth, Myriad Genetics, Propella Therapeutics, Genzyme, Sanofi, CG Oncology, Genesis Cancer Care, Urogen pharma, Speciality Networks, PeerView, Clarity Pharmaceuticals, Lantheus Medical Imaging, Lilly, Photocure, Telix Pharmaceuticals, AIkido Pharma, Arquer Diagnostics, Asieris Pharmaceuticals, Minomic, Novartis, PlatformQ Health, Promaxo, Protara Therapeutics, Fize Medical, Accord Research, Antev, Aura Biosciences, Bioprotect and Sumitomo Pharma Oncology. ND Shore has received research funding from AbbVie, Amgen, Astellas Pharma, AstraZeneca, Bayer, Bristol Myers Squibb/Pfizer, Boston Scientific, Clovis Oncology, Dendreon, Exact Imaging, Ferring, Foundation Medicine, InVitae, Johnson & Johnson, MDxHealth, Merck, Myovant Sciences, Myriad Genetics, Nymox, Pfizer, Sanofi, Sesen Bio, Tolmar, CG Oncology, DisperSol, FORMA Therapeutics, Guardant Health, Jiangsu Yahong Meditech, Novartis, Pacific Edge, POINT Biopharma, Propella Therapeutics, SeaGen, MT Group, Theralase, Veru, Zenflow, Advantagene, Aragon Pharmaceuticals, Endocyte, Exelixis, FKD Therapies, Genentech, Istari Oncology, Medivation, OncoCellMDx, ORIC Pharmaceuticals, Palette Life Sciences, Plexxikon, RhoVac, Steba Biotech, Urogen pharma, Urotronic, US Biotest and Vaxiion for work performed outside of the current study. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing assistance was provided by professional medical writers, Molly Gingrich and Loraine Georgy, employees of Analysis Group, Inc., a consulting company that has provided paid consulting services to Johnson & Johnson, which funded the development and conduct of this study.
Ethical conduct of research
The study was considered exempt research under 45 CFR § 46.104(d)(4) as it involved only the secondary use of data that were de-identified in compliance with the Health Insurance Portability and Accountability Act (HIPAA), specifically, 45 CFR § 164.514.
Previous presentations
Part of the material in this manuscript was presented as a poster at the 6th European Conference of Oncology Pharmacy (ECOP) in Lisbon, Portugal (2–4 October 2024), the LUPGA 2025 Global Prostate Congress in Sun Valley, Idaho (18–21 January 2025) and at the 35th Annual International Prostate Cancer Update (IPCU) in Vail, Colorado (9–12 February 2025).
Data availability statement
The data that support the findings of this study are available from PPS Analytics and Komodo Health Solutions. Restrictions apply to the availability of these data, which were used under license for this study.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 30.95 KB
References
1.
Ng K, Smith S, Shamash J. Metastatic hormone-sensitive prostate cancer (mHSPC): advances and treatment strategies in the first-line setting. Oncol. Ther. 8(2), 209–230 (2020).
2.
Weiner AB, Nettey OS, Morgans AK. Management of metastatic hormone-sensitive prostate cancer (mHSPC): an evolving treatment paradigm. Curr. Treat. Options Oncol. 20(9), 69 (2019).
3.
Mitsiades N, Kaochar S. Androgen receptor signaling inhibitors: post-chemotherapy, pre-chemotherapy and now in castration-sensitive prostate cancer. Endocr. Relat. Cancer 28(8), T19–T38 (2021).
4.
Chi KN, Agarwal N, Bjartell A et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N. Engl. J. Med. 381(1), 13–24 (2019).
5.
Chi KN, Chowdhury S, Bjartell A et al. Apalutamide in patients with metastatic castration-sensitive prostate cancer: final survival analysis of the randomized, double-blind, Phase III TITAN study. J. Clin. Oncol. 39(20), 2294–2303 (2021).
6.
United States Food and Drug Administration. FDA approves apalutamide for metastatic castration-sensitive prostate cancer. Accessed: 29 July 2024: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-apalutamide-metastatic-castration-sensitive-prostate-cancer
7.
Fizazi K, Tran N, Fein L et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N. Engl. J. Med. 377(4), 352–360 (2017).
8.
Fizazi K, Tran N, Fein L et al. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): final overall survival analysis of a randomised, double-blind, Phase III trial. Lancet Oncol. 20(5), 686–700 (2019).
9.
United State Food and Drug Administration. FDA approves abiraterone acetate in combination with prednisone for high-risk metastatic castration-sensitive prostate cancer. Accessed: 21 August 2024: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-abiraterone-acetate-combination-prednisone-high-risk-metastatic-castration-sensitive
10.
Brown G, Khilfeh I, Rossi C et al. A comparison of prostate-specific antigen response in patients with metastatic castration-sensitive prostate cancer initiated on apalutamide vs abiraterone acetate in linked clinical and claims databases. Rev. Urol. 23(2), 15–27 (2024).
11.
Chowdhury S, Bjartell A, Agarwal N et al. Deep, rapid, and durable prostate-specific antigen decline with apalutamide plus androgen deprivation therapy is associated with longer survival and improved clinical outcomes in TITAN patients with metastatic castration-sensitive prostate cancer. Ann. Oncol. 34(5), 477–485 (2023).
12.
Saad F, Small EJ, Feng FY et al. Deep prostate-specific antigen response following addition of apalutamide to ongoing androgen deprivation therapy and long-term clinical benefit in SPARTAN. Eur. Urol. 81(2), 184–192 (2022).
13.
Hussain MHA, Sternberg CN, Efstathiou E et al. Overall survival (OS) and metastasis-free survival (MFS) by depth of prostate-specific antigen (PSA) decline in the Phase III PROSPER trial of men with nonmetastatic castration-resistant prostate cancer (nmCRPC) treated with enzalutamide (ENZA). J. Clin. Oncol. 39(Suppl. 6), 94 (2021).
14.
Matsubara N, Chi KN, Ozguroglu M et al. Correlation of prostate-specific antigen kinetics with overall survival and radiological progression-free survival in metastatic castration-sensitive prostate cancer treated with abiraterone acetate plus prednisone or placebos added to androgen deprivation therapy: post hoc analysis of Phase III LATITUDE study. Eur. Urol. 77(4), 494–500 (2020).
15.
Saad F, Hussain MHA, Tombal BF et al. Association of prostate-specific antigen (PSA) response and overall survival (OS) in patients with metastatic hormone-sensitive prostate cancer (mHSPC) from the Phase III ARASENS trial. J. Clin. Oncol. 40(Suppl. 16), 5078–5078 (2022).
16.
Purpura CA, Garry EM, Honig N, Case A, Rassen JA. The role of real-world evidence in FDA-approved new drug and biologics license applications. Clin. Pharmacol. Ther. 111(1), 135–144 (2022).
17.
United States Food and Drug Administration. Considerations for the use of real-world data and real-world evidence to support regulatory decision-making for drug and biological products: guidance for industry. Accessed: 21 August 2024: https://www.fda.gov/media/171667/download
18.
Komodo Health Inc. Komodo Mortality Data User Guide. Version 23.8.
19.
Freedland SJ, Ke X, Lafeuille MH et al. Identification of patients with metastatic castration-sensitive or metastatic castration-resistant prostate cancer using administrative health claims and laboratory data. Curr. Med. Res. Opin. 37(4), 609–622 (2021).
20.
Dorfman AH, Valliant R. The Hajek Estimator Revisited. Proceedings of the Section on Survey Methods Research, American Statistical Association, USA. 760–765 (1997).
21.
Austin PC. Using the standardized difference to compare the prevalence of a binary variable between two groups in observational research. Commun. Stat. Simul. Comput. 38(6), 1228–1234 (2009).
22.
Bilen MA, Khilfeh I, Rossi C et al. Analysis of real-world survival for patients with metastatic castration-sensitive prostate cancer (mCSPC) treated with apalutamide (APA) or abiraterone acetate (ABI) in an oncology database: ROMA study. J. Clin. Oncol. 42(Suppl. 4), 58–58 (2024).
23.
Lowentritt BH, Du S, Rossi C et al. Real-world clinical outcomes among patients with metastatic castration-sensitive prostate cancer initiating apalutamide. Future Oncol. 20(27), 2005–2013 (2024).
24.
Ueda T, Shiraishi T, Miyashita M et al. Apalutamide versus bicalutamide in combination with androgen deprivation therapy for metastatic hormone sensitive prostate cancer. Sci. Rep. 14(1), 705 (2024).
25.
Hassi Roman M, Mate K, de Pablos-RodrIguez P et al. Apalutamide use in metastatic hormone-sensitive prostate cancer patients diagnosed by conventional and next-generation imaging. Real world data from 772 patients. Actas Urol. Esp. (Engl. Ed.) 501742 (2025).
26.
Lam BHW, Tsang VHM, Lee MP et al. A territory-wide real-world efficacy and toxicity analysis of abiraterone acetate versus docetaxel in 574 Asian patients with metastatic hormone-sensitive prostate cancer. Clin. Genitourin. Cancer 22(1), e75–e85; e71 (2024).
27.
Lambert E, Hollebosch S, van Praet C et al. Treatment of patients with newly diagnosed metastatic hormone sensitive prostate cancer (mHSPC) in Belgium: a real world data analysis. Acta Clin. Belg. 77(6), 897–905 (2022).
28.
Lowentritt B, Pilon D, Waters D et al. Comparison of prostate-specific antigen response in patients with metastatic castration-sensitive prostate cancer initiated on apalutamide or abiraterone acetate: a retrospective cohort study. Urol. Oncol. 41(5), 252.e219–252.e227 (2023).
Information & Authors
Information
Published In
Copyright
© 2025 Johnson & Johnson. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 4 March 2025
Accepted: 24 April 2025
Published online: 9 May 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Overall survival in patients with metastatic castration-sensitive prostate cancer treated with apalutamide versus abiraterone acetate: a head-to-head analysis of real-world patients in the USA. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0023
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Mehmet A. Bilen, Gordon Brown, Mukul Singhal, Carmine Rossi, Dominic Pilon, Courtney D. Longfield, Benjamin Lowentritt, Real-World PSA Response and Overall Survival Among Men with mCSPC Receiving Apalutamide Versus Darolutamide (Both Without Docetaxel) in the US, Advances in Therapy, 10.1007/s12325-026-03707-z, (2026).
- Srivatsa N, Chandrakanth Mv, Avinash Upadhyay, Pankaj Sonone, Shruti Dharmadhikari, Gaurav Puppalwar, Chintan Khandhedia, Amey Mane, Suyog Mehta, Apalutamide‑induced prostate‑specific antigen response and its association with clinical outcomes in metastatic castration sensitive prostate cancer (Review), Molecular and Clinical Oncology, 10.3892/mco.2026.2964, 25, 3, (1-8), (2026).
- Keita Hayakawa, Takashi Ueda, Masahiro Iehara, Yusuke Gabata, Junki Murashita, Hikaru Takahashi, Yumiko Saito, Masatsugu Miyashita, Yasuhiro Yamada, Takumi Shiraishi, Atsuko Fujihara, Masayoshi Okumi, Fumiya Hongo, Osamu Ukimura, Triplet versus doublet therapy in patients with metastatic hormone-sensitive prostate cancer, Scientific Reports, 10.1038/s41598-026-44627-w, 16, 1, (2026).
- Piotr Kawczak, Tomasz Bączek, Emerging Therapeutic Strategies in Prostate Cancer: Targeted Approaches Using PARP Inhibition, PSMA-Directed Therapy, and Androgen Receptor Blockade with Olaparib, Lutetium (177Lu)Vipivotide Tetraxetan, and Abiraterone, Journal of Clinical Medicine, 10.3390/jcm15020685, 15, 2, (685), (2026).
- Gordon Brown, Sabree Burbage, Ibrahim Khilfeh, Carmine Rossi, Shawn Du, Frederic Kinkead, Lilian Diaz, Dominic Pilon, Benjamin Lowentritt, Comparison of Prostate-Specific Antigen Response in Black Patients with Metastatic Castration-Sensitive Prostate Cancer Initiated on Apalutamide vs Abiraterone Acetate, Journal of Health Economics and Outcomes Research, 10.36469/jheor.2025.151273, (270-278), (2025).
- Gordon Brown, Sabree Burbage, Ibrahim Khilfeh, Carmine Rossi, Shawn Du, Frederic Kinkead, Lilian Diaz, Dominic Pilon, Benjamin Lowentritt, Comparison of Prostate-Specific Antigen Response in Black Patients with Metastatic Castration-Sensitive Prostate Cancer Initiated on Apalutamide vs Abiraterone Acetate, Journal of Health Economics and Outcomes Research, 10.36469/001c.151273, 12, 2, (2025).