Comparative safety of B/F/TAF versus other antiretroviral therapy regimens for treatment-naïve people with HIV-1: a systematic literature review and network meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Bictegravir, emtricitabine and tenofovir alafenamide (B/F/TAF) is a single-tablet regimen approved for the treatment of HIV-1 in treatment-naive (TN) and virologically suppressed people with HIV-1 (PWH). While the efficacy of antiretroviral therapy (ART) regimens in TN PWH is well established, regimen selection is often influenced by safety and tolerability concerns. This systematic literature review and network meta-analysis compares the safety outcomes of B/F/TAF with other ART regimens in TN PWH, addressing a key aspect of therapeutic decision-making. Materials & methods: A systematic literature review was performed to identify phase III and IV RCTs assessing B/F/TAF and comparator regimens in TN adults (≥18 years) with HIV-1. MEDLINE, Embase, Cochrane Database of Systematic Reviews and CENTRAL databases were last searched on 14 June 2023. Study design, population and outcome definitions were evaluated to ensure consistency across studies. Bayesian network meta-analyses were conducted where feasible, following key methodological guidelines. Results: Nineteen studies were included in indirect comparisons following assessments of heterogeneity and network connectivity. B/F/TAF performed better than the majority of interventions in safety and tolerability outcomes, notably discontinuation due to adverse events (AEs), treatment-related AEs and nausea. Additionally, with comparable risk of experiencing grade 3/4 treatment-emergent AEs, diarrhea and all-cause discontinuation rates to other interventions, B/F/TAF was non-inferior to any other regimen for all outcomes. B/F/TAF typically outperformed interventions containing non-nucleoside reverse transcriptase inhibitor third agents in terms of treatment-related AEs, nausea, and discontinuation due to AEs, although treatment class effects were not estimated separately. Conclusion: This analysis highlights the favorable safety profile of B/F/TAF compared with other ART regimens in TN PWH, demonstrating that B/F/TAF remains a safe and well-tolerated ART option for most TN PWH.
Plain language summary: comparative safety of B/F/TAF in people with HIV-1 who have not yet received any treatment
What is this article about?
B/F/TAF is a single-tablet treatment for HIV-1 which combines three medications – bictegravir (B), emtricitabine (F) and tenofovir alafenamide (TAF). B/F/TAF is recommended by US and international guidelines for the treatment of HIV-1 in people who may or may not have received any treatment before starting B/F/TAF.
This article compares B/F/TAF with other available HIV-1 treatments to see how they differ in terms of safety for people newly diagnosed with HIV-1.
Why is this important?
HIV-1 is a serious global health issue, and a major cause of death and illness worldwide. Finding safe and effective treatments is crucial for people with HIV-1.
What methods were used in the research?
The researchers reviewed a large number of studies that looked at B/F/TAF and other treatments. The data were then analyzed to compare how safe these treatments are for people who are starting HIV-1 therapy for the first time.
What were the results?
The analysis found that B/F/TAF has a favorable safety profile compared with many other HIV-1 treatments, particularly in terms of treatment-related adverse events, nausea and treatment discontinuation due to adverse events.
What do the results mean?
These findings suggest that B/F/TAF is a safe and tolerable option for most people newly diagnosed with HIV-1. It may be preferable for many patients, as it has fewer side effects compared with other available HIV-1 treatments.
HIV type 1 (HIV-1) is the causative agent of AIDS, a life-threatening and serious infection of global public health interest, which caused 1.3 million (range: 1.0–1.7 million) new infections and 630,000 (500,000–820,000) AIDS-related deaths in 2023 according to the WHO [1].
Current therapeutic strategies for HIV-1 are centered around the use of modern, effective antiretroviral therapies (ARTs). While these are not able to eradicate HIV-1 from the human body because of the persistence of a viral reservoir [2], initiation of guideline-recommended ART can suppress viral replication, preserving CD4 cells and preventing the onset of AIDS [3]. This enables people with HIV-1 (PWH) to have a life expectancy similar to that of the general population [4]. Combination ART, comprising multiple active agents from distinct mechanistic classes, is a proven strategy to achieve and maintain an undetectable viral load. When adhered to as prescribed, this treatment approach effectively eliminates the risk of sexual HIV-1 transmission, supporting the undetectable = untransmittable (U = U) strategy, and minimizes the risks of developing drug resistance [5].
Bictegravir, emtricitabine and tenofovir alafenamide (B/F/TAF), is a single-tablet regimen (STR) indicated in the management of HIV-1 infection in adults and children with HIV-1 who are treatment-naïve (TN) or treatment-experienced (TE) and virologically suppressed on a stable ART regimen with no known or suspected substitutions associated with resistance to bictegravir or tenofovir [6]. This STR offers a complete HIV-1 treatment option, combining the integrase strand transfer inhibitor (INSTI) bictegravir with the established nucleoside reverse transcriptase inhibitors (NRTIs) emtricitabine and tenofovir alafenamide [6].
B/F/TAF has demonstrated efficacy and safety as an ART regimen in the TN population in multiple clinical trials [7,8,9,10,11]. Notably, the GS-US-380-1489 and GS-US-380-1490 trials are randomized, double-blind, active-controlled phase III trials evaluating the efficacy and safety of B/F/TAF in TN adults with HIV-1 infection with a five-year follow-up. Long-term data from these pivotal trials demonstrate the durable efficacy and favorable safety profile of B/F/TAF in TN adults with HIV-1 infection [8,10].
Additionally, the real-world BICSTaR study is an ongoing, multinational, prospective, observational cohort study evaluating the real-world effectiveness, safety and tolerability of B/F/TAF in TN and TE populations [12]. The results from BICSTaR further support the findings of the clinical trials by demonstrating high levels of effectiveness and safety of B/F/TAF in the TN population [12]. Furthermore, B/F/TAF is recommended as first-line ART for PWH in international guidelines [13,14,15].
Objective
While the comparative virologic efficacy of ART regimens in TN PWH is well-established, the choice of ART regimen is partly driven by concerns about the safety and tolerability profile of each regimen. Given the ubiquity of effective ART options, these factors have become critical in determining optimal treatment regimens [4]. This systematic literature review (SLR) and network meta-analysis (NMA) aims to address this critical aspect in therapeutic strategies for HIV-1 by comparing safety outcomes of B/F/TAF versus other ART regimens in TN PWH.
Materials & methods
SLR methods
A comprehensive SLR was conducted to identify relevant B/F/TAF and comparator studies. MEDLINE, Embase and The Cochrane Library, including Cochrane Database of Systematic Reviews and Cochrane Central Register of Controlled Trials (CENTRAL) were last searched on 14 June 2023 using search terms detailed in Supplementary Table 1. Database searches were supplemented by manual searches of key conference proceedings and ClinicalTrials.gov to ensure that no studies were missed. Predefined eligibility criteria based on the population, intervention, comparators, outcomes and study design were used to review all studies identified from these searches in two stages: an abstract screening stage, followed by a more comprehensive full-text review stage. The SLR included phase III and IV randomized control trials (RCTs) investigating B/F/TAF and relevant comparators in individuals with HIV-1 infection, reporting on safety and efficacy outcomes at or around Weeks 24, 48, 96 or 144. Detailed eligibility criteria are provided in Supplementary Table 2. Two independent reviewers assessed each title, abstract and full text against the eligibility criteria. The methods and results of all included studies were extracted into pre-specified data extraction tables in Microsoft Excel by a single individual and independently verified by a second individual, in line with guidelines from the University of York Centre of Reviews and Dissemination [16]. These included information on study and patient characteristics, efficacy, safety and resistance outcomes. The quality of all included RCTs in the SLR was assessed using the criteria provided by the Cochrane Collaboration’s tool for assessing risk of bias [17].
Feasibility assessment for indirect comparisons
When conducting indirect treatment comparisons, it is important to consider any variation between the studies included in the analysis to determine whether there are any meaningful differences in the study design, population and outcome definitions between the studies, which may lead to differences in the observed intervention effects [18].
Heterogeneity assessment
As an NMA estimates relative treatment effects, effect-modifying characteristics are required to be balanced across studies for an NMA to accurately estimate true treatment effects. However, since, to our knowledge, limited clinical consensus and literature identifying effect-modifiers in first-line HIV-1 exists, we considered heterogeneity in the following potentially clinically meaningful baseline characteristics: viral load, CD4 cell count, age, race/ethnicity, hepatitis B/C co-infection, weight, comorbidities and eGFR/renal outcomes.
Interventions, outcomes & timepoints assessed
All relevant ARTs were considered for comparison with B/F/TAF (Supplementary Table 3). Regimens containing elvitegravir (EVG) were not considered of relevance for these analyses. While EVG-containing regimens were initially recommended as preferred third agents for TN patients, alongside DTG and RAL, current clinical practice now prioritizes second-generation INSTIs, such as DTG-containing regimens and B/F/TAF, due to their higher genetic barrier to resistance and reduced risk of virologic failure [19,20]. A key pharmacokinetic limitation of EVG is its requirement for coadministration with the booster cobicistat, which inhibits CYP3A and causes significant drug–drug interactions, complicating use in TN patients who may require polypharmacy [21,22]. Consequently, while it was included in the search terms in the SLR and its updates for comprehensiveness, EVG was excluded from these analyses in line with evolving treatment guidelines. Other treatments such as RAL are less typically used presently, however was retained since unlike EVG, RAL does not require boosting and has fewer drug interactions, and remains a key option in rescue regimens and in clinical scenarios where drug interactions are a concern [21,22]. Similarly, treatment arms pooling multiple unique regimens were excluded.
The outcomes assessed based on intention-to-treat population results were treatment-related adverse events (TRAEs; adverse events causally related to the study treatment), grade 3/4 treatment-emergent adverse events (TEAEs; adverse events that occur or worsen after treatment initiation, regardless of their perceived relationship to the study drug), diarrhea, nausea, all-cause treatment discontinuation, discontinuation due to adverse events (AEs), and treatment-emergent resistance mutations (see Supplementary Table 4 for definitions). The specific adverse event outcomes analyzed in this NMA were selected based on their clinical relevance and alignment with the summary of product characteristics for B/F/TAF [23]. Nausea and diarrhea were selected as AEs of interest because they are among the most commonly reported for B/F/TAF, as noted in the summary of product characteristics. Other AEs, such as depression, dizziness, fatigue and abnormal dreams, are less common for B/F/TAF, with incidence rates below 5% for depression and dizziness and below 10% for fatigue across both the GS-US-380-1489 and GS-US-380-1490 trials [8,10].
The timepoints assessed for this analysis were Week 48 and Week 96, which are key timepoints reported in HIV-1 trials. All the outcomes were assessed separately at each timepoint. Only evidence at these timepoints was included in the networks and studies which did not report on any of these timepoints were excluded (Supplementary Table 5). Where differences in reporting meant that NMAs were not feasible, a qualitative comparison was conducted instead, in accordance with Cochrane guidelines [24].
Indirect comparison methods
Analyses conducted
Where feasible, Bayesian NMAs were conducted. NMAs extend the principles of meta-analysis and indirect treatment comparisons to allow for a connected network of treatments to be quantitatively synthesized [25].
Analyses followed methodology outlined in key methodological guidance documents, in particular, National Institute of Health and Care Excellence (NICE) Decision Support Unit (DSU) Technical Support Documents (TSD) 2, 3 and 4 [26,27,28]. Both random effects (RE) and fixed effects (FE) models were fitted. Due to a limited number of studies per treatment comparison, informative priors for between-study heterogeneity were also implemented [29].
Networks were generated and assessed by outcome and timepoint, with each treatment represented as a distinct node. To aid network connectivity, simplifying assumptions were required. In particular, STRs and multitablet regimens were considered equivalent in the safety networks. This assumption was based on evidence from prior real-world studies comparing STRs and multitablet regimens [30]. Additionally, different dosages of each individual backbone were also considered equivalent: tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) (300 mg/200 mg QD or 245 mg/200 mg QD) and F/TAF (200 mg/25 mg QD or 200 mg/10 mg QD). However, different dosages for third agents efavirenz (EFV) (600 and 400 mg) and raltegravir (RAL) (1200 and 400 mg) were not considered equivalent and were retained as separate regimens. All items of the PRISMA-NMA extension statement are reported in this manuscript (see Supplementary Table 6) [31].
Data input
Treatment-arm level inputs in terms of number of events and sample size were used for each analysis (see Supplementary Table 7).
Model specification & selection
Binomial distributions with a logit link were fitted for all outcomes. The deviance information criterion was used for model selection [32]. Further details are provided in the Supplementary Materials (Model Specification).
Results output
For all outcomes, risk differences (RDs) are presented with 95% credible intervals (CrIs) and statistical evidence of a difference between treatment was determined by whether the CrIs included the value of no effect. Furthermore, the mean surface area under the cumulative ranking curve (SUCRA) was computed for each treatment.
Software implementation
All analyses were conducted using statistical software R, version 4.3.0 or later, where NMAs were conducted using the software OpenBUGS version 3.2.3, through the R package R2OpenBUGS [33,34,35]. The OpenBUGS analysis code is provided in the Supplementary Materials (Model Specification).
Results
SLR & feasibility assessment
Eligibility assessment
Of the 79 RCTs identified in the SLR, 39 were performed in TN PWH. Two studies investigated B/F/TAF in TN PWH. The flow of records through the various review stages is presented in Figure 1.
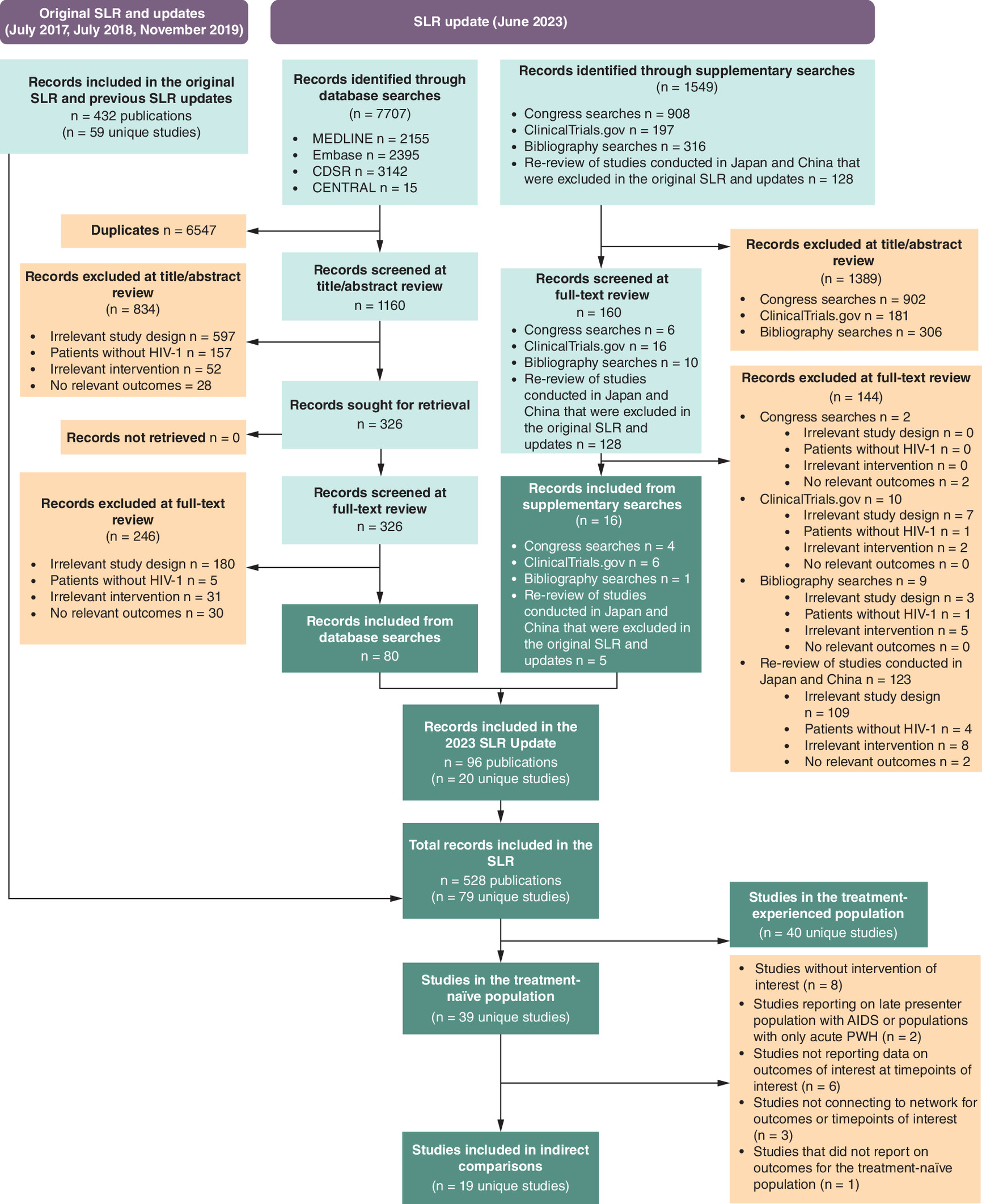
Figure 1. PRISMA flowchart for inclusion in systematic literature review and indirect treatment comparisons.
CDSR: Cochrane Database of Systematic Reviews; ITC: Indirect treatment comparison; PRISMA: Preferred reporting items for systematic reviews and meta-analyses; PWH: People with HIV-1; SLR: Systematic literature review.
The following exclusions were made when assessing eligibility of studies for the NMA:
•
•
One study reporting on a non-randomized pooled backbone was excluded [39]
•
•
•
•
One study that recruited TN PWH, but did not report outcomes for the TN population was excluded (patients who demonstrated virologic suppression following an induction phase were randomized to receive treatment, and outcomes were only reported for virologically suppressed patients) [54]
Overall, 19 studies were eligible for inclusion in indirect comparisons, with 14 studies reporting on outcomes of interest at Week 48 and 14 studies reporting Week 96 results. A list of studies excluded from the NMA is provided in Supplementary Table 5.
Study characteristics
All 19 studies eligible for inclusion in indirect comparisons were published between 2009 and 2021. Of these 19 studies, 14 were conducted in multiple countries whereas five trials took place in a single country. The majority of studies (13/19) were phase III or IIIb studies, with the remaining studies being phase IV studies. Blinding was carried out in 8/19 studies, and 5/19 studies were reported as being noninferiority studies. Further details can be found in Supplementary Table 8.
Quality assessment
Top-line summaries of the quality assessments for the 19 studies included in indirect comparisons are presented in the Supplementary Materials (Supplementary Tables 9 & 10). Quality assessments were based solely on data from published studies identified in the SLR. Overall, randomization and treatment allocation were carried out appropriately, and treatment arms were well-balanced in terms of prognostic factors at baseline. However, it was common for not all measured outcomes to be reported. The most substantial limitation of the RCTs overall was a lack of blinding (11/19 studies were not blinded), which may have led to bias in the ascertainment and reporting of safety outcomes. However, the inclusion of unblinded studies was deemed necessary to form the network between key treatment nodes, including DRV (+ or /) r + TDF/FTC, ATV (+ or /) + TDF/FTC, EFV + ABC/3TC and RPV (+ or /) TDF/FTC.
Patient baseline characteristics
Heterogeneity in patient baseline characteristics was assessed for studies eligible for analysis. Patient baseline characteristics are summarized below and presented in Supplementary Table 11. Study populations had mean ages between 34 and 38 years and were predominantly male. One study (ARIA) was conducted only in female participants. There was some evidence of heterogeneity in the ethnicity of the participants recruited. For most studies (10/19), White PWH made up the majority of the participants. However, two studies (ENCORE1 and ACTG5257) had a higher proportion of Black participants and there was one study where only Asian participants were recruited (Epzicom-Truvada).
For all included studies, reported mean viral loads were between low (i.e., 10,000 copies/ml [4 log10 copies/ml) and high (i.e., 100,000 copies/ml [5 log10 copies/ml]) viral loads and mean CD4 cell counts were above the 200 cells/ul threshold for AIDS. However, there was some heterogeneity across studies in both characteristics. Hepatitis B status was poorly reported (6/19), whereas hepatitis C status was reported more frequently (13/19). Where reported, the prevalence of hepatitis B and C was typically low, with some small differences across studies.
Summary of feasibility assessment
Due to differences in reporting of resistance mutations across studies, the low incidence and the agent-specific nature of resistance, NMAs were not feasible for treatment-emergent resistance mutations, and a qualitative comparison was conducted instead.
Aside from resistance mutations, which were only assessed in participants with protocol-defined virologic failure, NMAs were deemed feasible for all outcomes of interest. Despite some differences in patient characteristics across trials (ethnicity, age, viral load and baseline CD4 cell counts), it was deemed suitable to compare differences in safety events across trials via NMAs, as per previous indirect comparisons in this field [55,56,57]. Most treatment regimens connected indirectly to B/F/TAF in the network at Week 48 and Week 96; however, many of these connections were via two or more studies. As such, these comparisons may be less robust than those that connect to B/F/TAF either directly or via one common comparator.
Indirect comparisons
Week 48 results
Network diagrams at Week 48 for all safety outcomes are displayed in Figures 2, 3 & 4 and all Week 48 results are summarized in Table 1, and presented as forest plots in Figures 5, 6 & 7. Additional results such as absolute risk, mean SUCRA scores and probability best are presented in the Supplementary Materials (Supplementary Tables 12–14). With no substantial difference in deviance information criterion between the FE and informative prior RE models and comparable residual deviances, the informative prior RE model was selected as the favored model for all outcomes of interest (see Supplementary Tables 15–20 for model fit). Use of RE models was also considered to be suitable from a clinical perspective in incorporating between-study heterogeneity.
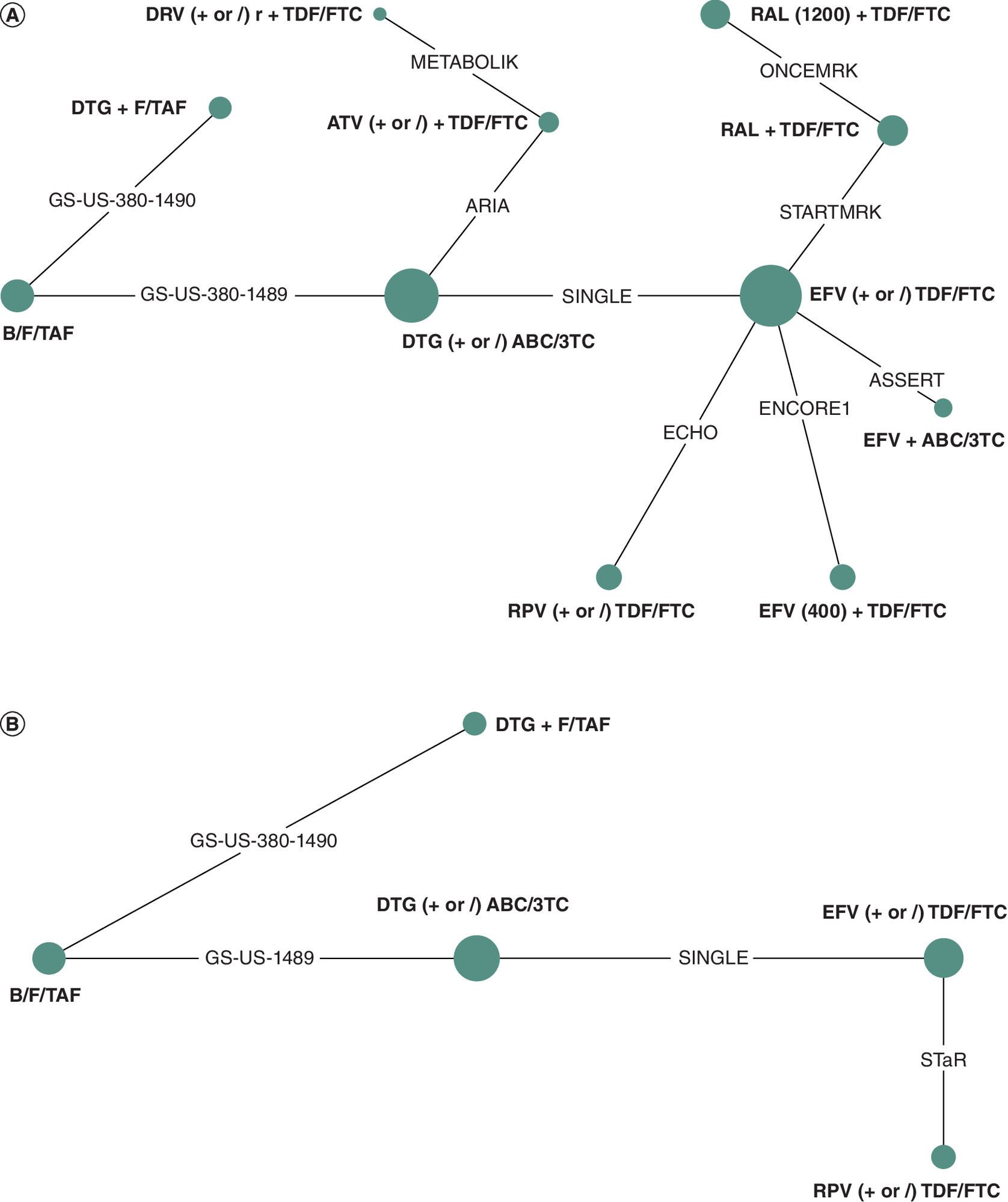
Figure 2. Analysis networks at Week 48: AE outcomes.
(A) TRAE. (B) Grade 3/4 TEAE. Green indicates two-arm trials; node size indicates the number of PWH receiving each intervention; edge width indicates the number of trials informing a given comparison. The network includes 11 comparators for TRAEs, and five comparators for grade 3/4 TEAEs.
AE: Adverse event; PWH: People with HIV-1; TEAE: Treatment emergent adverse event; TRAE: Treatment-related adverse event.
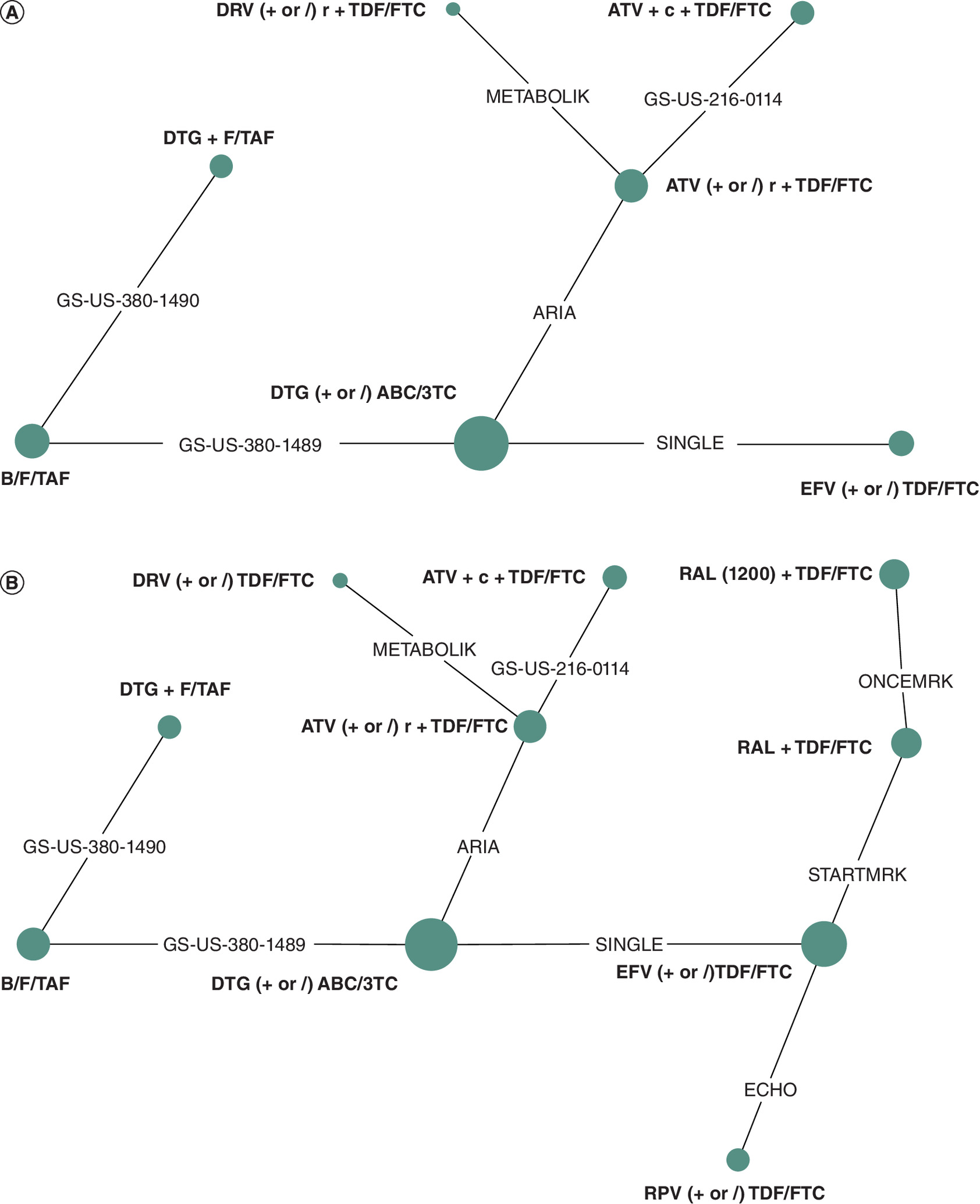
Figure 3. Analysis networks at Week 48: specific AE outcomes.
(A) Diarrhea. (B) Nausea. Green indicates two-arm trials; node size indicates the number of PWH receiving each intervention; edge width indicates the number of trials informing a given comparison. The network includes seven comparators for diarrhea, and ten comparators for nausea. RAL (1200) refers to the 1200 mg dosage of raltegravir, while RAL refers to the 400 mg dosage of raltegravir.
AE: Adverse event; PWH: People with HIV-1.
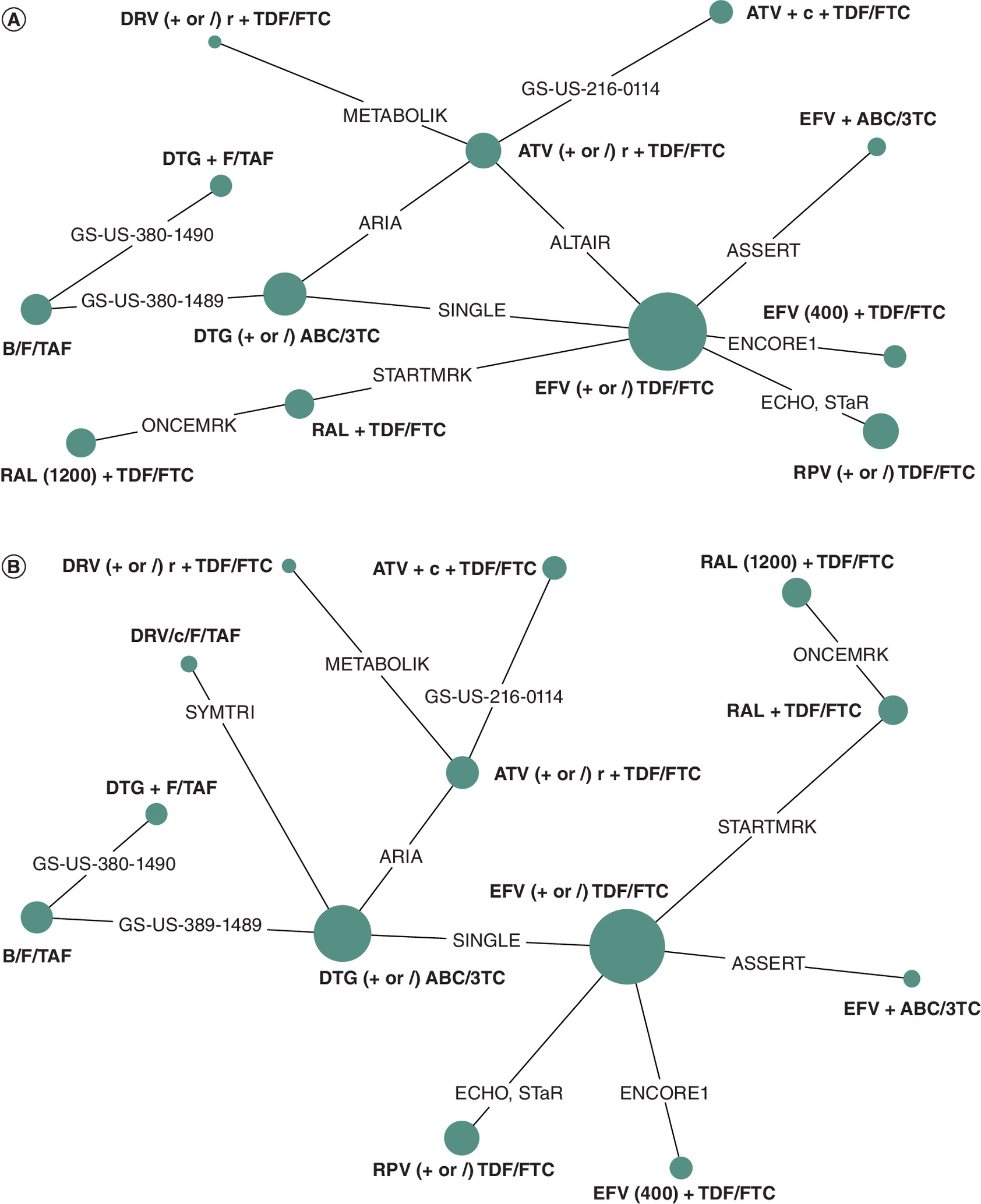
Figure 4. Analysis networks at Week 48: discontinuation outcomes.
(A) All-Cause discontinuation. (B) Discontinuation due to AE. Green indicates two-arm trials; node size indicates the number of PWH receiving each intervention; edge width indicates the number of trials informing a given comparison. The network includes 12 comparators for all-cause discontinuation and 13 comparators for discontinuation due to AE. RAL (1200) refers to the 1200 mg dosage of raltegravir, while RAL refers to the 400 mg dosage of raltegravir. EFV (400) refers to the 400 mg dosage of efavirenz, while EFV refers to the 600 mg dosage of efavirenz.
AE: Adverse event.
| Third agent class | Comparator | Risk difference (95% CrI) of B/F/TAF vs comparators | |||||
|---|---|---|---|---|---|---|---|
| TRAE | Grade 3/4 TEAE | Diarrhea | Nausea | All-cause discontinuation | Discontinuation due to AE | ||
| INSTI | B/F/TAF | – | – | – | – | – | – |
| DTG + F/TAF | -0.09 (-0.28, 0.06) | 0.02 (-0.06, 0.07) | -0.01 (-0.13, 0.07) | -0.01 (-0.13, 0.05) | 0.02 (-0.03, 0.05) | 0.00 (-0.00, 0.01) | |
| DTG (+ or /) ABC/3TC | -0.13 (-0.31, 0.03) | -0.00 (-0.11, 0.06) | -0.00 (-0.12, 0.07) | -0.11 (-0.27, -0.00)† | 0.01 (-0.05, 0.05) | -0.03 (-0.17, 0.00) | |
| RAL + TDF/FTC | -0.02 (-0.32, 0.15) | – | – | -0.07 (-0.38, 0.06) | 0.00 (-0.11, 0.06) | -0.07 (-0.42, -0.00)† | |
| RAL (1200) + TDF/FTC | -0.01 (-0.36, 0.17) | – | – | -0.08 (-0.46, 0.06) | 0.01 (-0.12, 0.06) | -0.03 (-0.33, 0.00) | |
| NNRTI | RPV (+ or /) TDF/FTC | -0.14 (-0.46, 0.10) | 0.01 (-0.19, 0.07) | – | 0.02 (-0.25, 0.08) | -0.01 (-0.12, 0.05) | -0.03 (-0.26, 0.00) |
| EFV (400) + TDF/FTC | -0.25 (-0.55, 0.05) | – | – | – | -0.00 (-0.13, 0.05) | -0.04 (-0.31, 0.00) | |
| EFV (+ or /) TDF/FTC | -0.36 (-0.58, -0.07) | -0.05 (-0.28, 0.05) | -0.01 (-0.20, 0.08) | -0.10 (-0.33, 0.03) | -0.03 (-0.14, 0.03) | -0.13 (-0.54, -0.02) | |
| EFV + ABC/3TC | -0.39 (-0.64, -0.05) | – | – | – | -0.09 (-0.28, 0.02) | -0.16 (-0.64, -0.02) | |
| PI | DRV/c/F/TAF | – | – | – | – | – | -0.02 (-0.16, 0.01) |
| DRV (+ or /) r + TDF/FTC | -0.02 (-0.40, 0.17) | – | -0.20 (-0.64, 0.06) | -0.50 (-0.85, -0.05) | 0.01 (-0.18, 0.07) | -0.00 (-0.17, 0.01) | |
| ATV (+ or /) r + TDF/FTC | -0.28 (-0.53, -0.01) | – | -0.04 (-0.27, 0.07) | -0.12 (-0.37, 0.02) | -0.01 (-0.12, 0.04) | -0.06 (-0.34, -0.00)† | |
| ATV + c + TDF/FTC | – | – | -0.00 (-0.25, 0.09) | -0.14 (-0.46, 0.03) | -0.04 (-0.20, 0.04) | -0.06 (-0.37, -0.00)† | |
The table shows risk differences for B/F/TAF vs comparators for all safety outcomes at Week 48. Bold highlighting indicates where risk differences showed a statically lower risk for B/F/TAF vs comparator. Results are presented as ‘-0.00’ if they were negative but round to 0 at two decimal places.
†
The credible interval of the risk difference does not include 0 when not rounded. RAL (1200) refers to the 1200 mg dosage of raltegravir, while RAL refers to the 400 mg dosage of raltegravir. EFV (400) refers to the 400 mg dosage of efavirenz, while EFV refers to the 600 mg dosage of efavirenz.
AE: Adverse event; CrI: Credible interval; DTR: Dual-therapy regimen; INSTI: Integrase strand transfer inhibitor; NMA: Network meta-analysis; NNRTI: Non-nucleoside reverse transcriptase inhibitors; PI: Protease inhibitors; TEAE: Treatment emergent adverse event; TRAE: Treatment-related adverse event.

Figure 5. Forest plots: AE outcomes (RD [95% CrI] of comparators vs B/F/TAF).
(A) TRAE (Week 48). (B) Grade 3/4 TEAE (Week 48). Forest plot showing how each comparator treatment (right) performed versus B/F/TAF; results are given as the RD and 95% CrIs. Orange indicates INSTI third agents, green indicates NNRTI third agents and purple indicates PI third agents. RAL (1200) refers to the 1200 mg dosage of raltegravir, while RAL refers to the 400 mg dosage of raltegravir.
AE: Adverse event; CrI: Credible interval; INSTI: Integrase strand transfer inhibitor; NNRTI: Non-nucleoside reverse transcriptase inhibitor; PI: Protease inhibitor; RD: Risk difference; TEAE: Treatment-emergent adverse event; TRAE: Treatment-related adverse event.
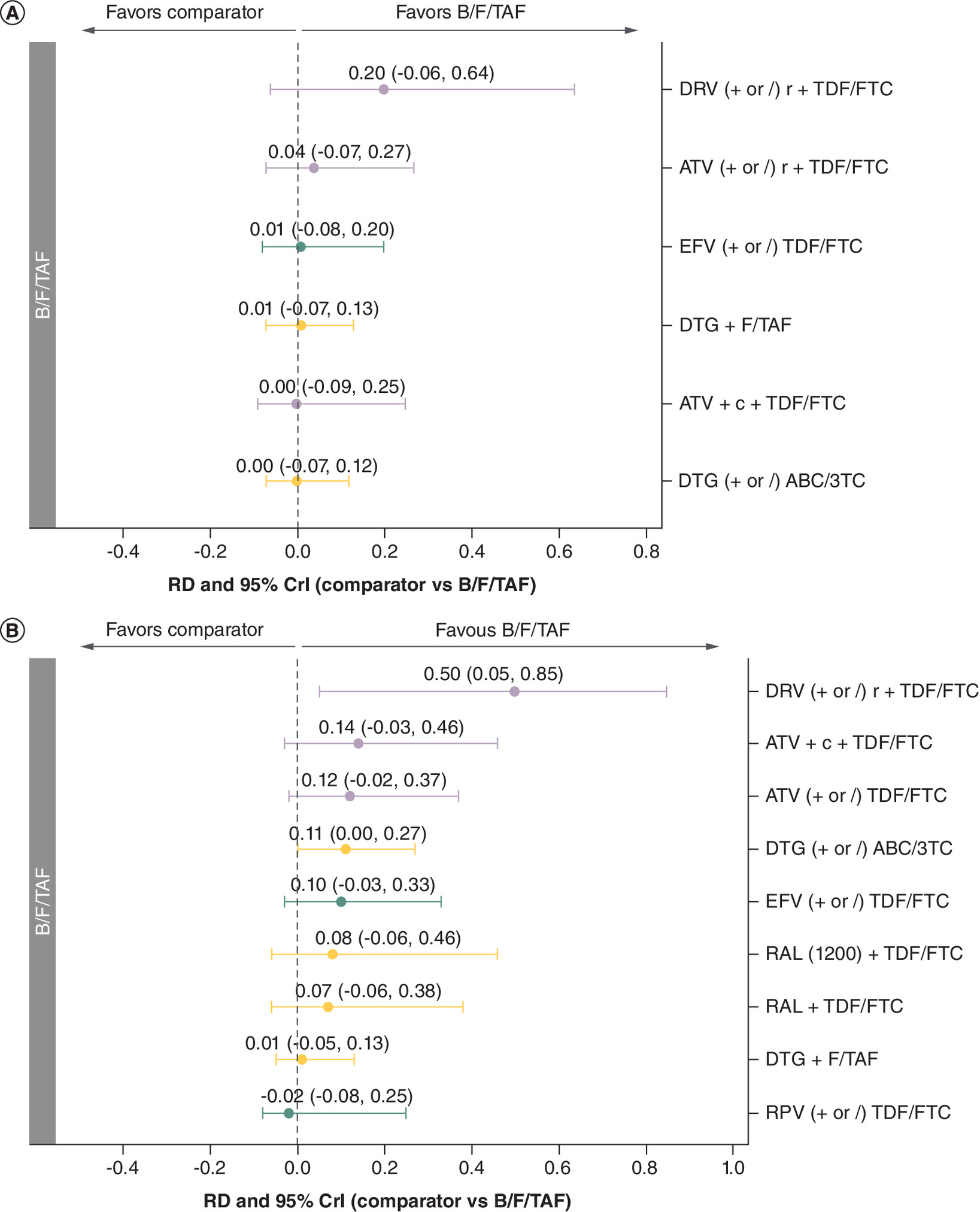
Figure 6. Forest plots: specific AE outcomes (RD [95% CrI] of comparators vs B/F/TAF).
(A) Diarrhea (Week 48). (B) Nausea (Week 48).
Forest plot showing how each comparator treatment (right) performed versus B/F/TAF; results are given as the RD and 95% CrIs. Orange indicates INSTI third agents, green indicates NNRTI third agents and purple indicates PI third agents. RAL (1200) refers to the 1200 mg dosage of raltegravir, while RAL refers to the 400 mg dosage of raltegravir.
AE: Adverse event; CrI: Credible interval; INSTI: Integrase strand transfer inhibitor; NNRTI: Non-nucleoside reverse transcriptase inhibitor; PI: Protease inhibitor; RD: Risk difference.
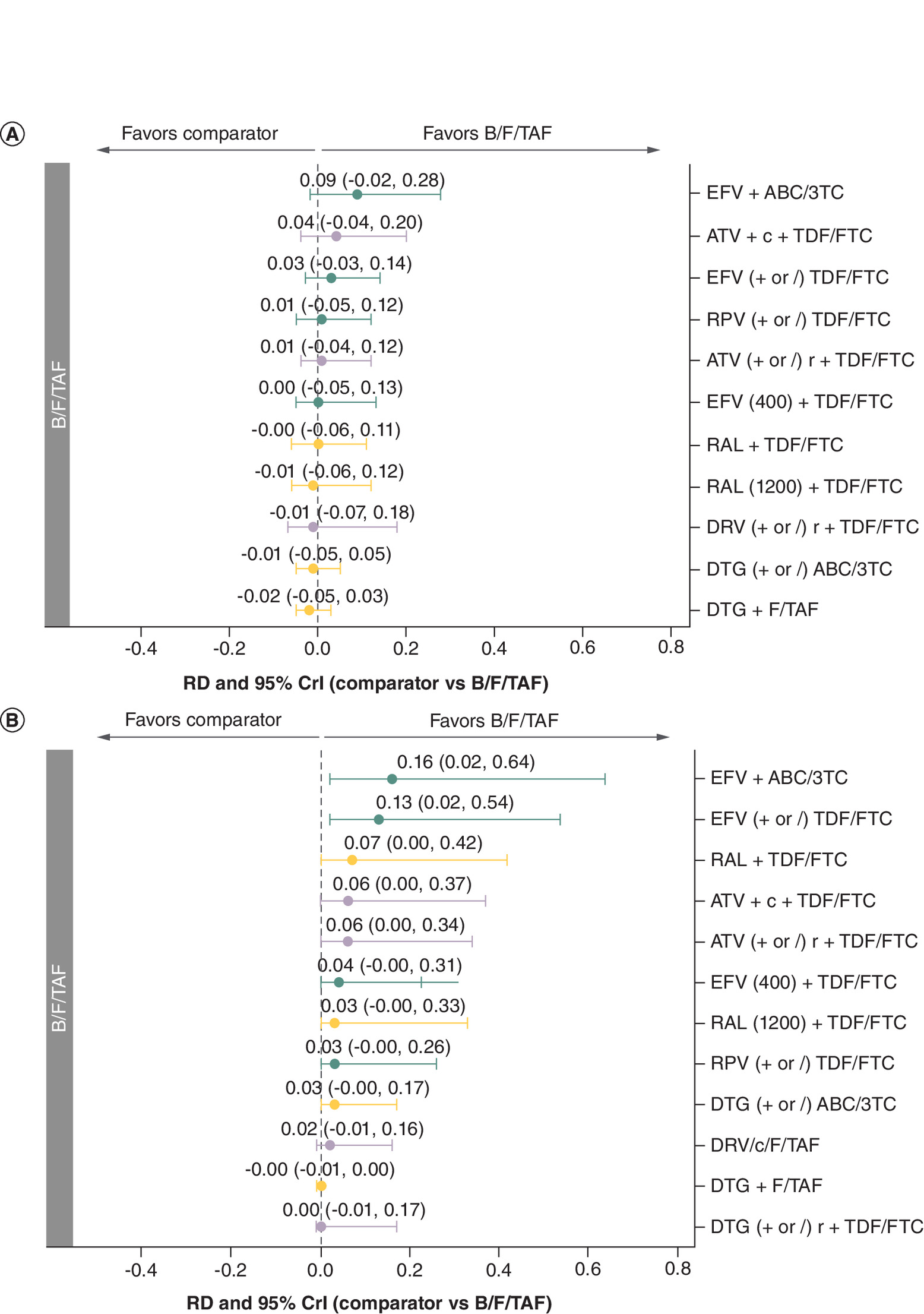
Figure 7. Forest plots: discontinuation outcomes (RD [95% CrI] of comparators vs B/F/TAF).
(A) All-cause discontinuation (Week 48). (B) Discontinuation due to AE (Week 48). Forest plot showing how each comparator treatment (right) performed versus B/F/TAF; results are given as the RD and 95% CrIs. Orange indicates INSTI third agents, green indicates NNRTI third agents and purple indicates PI third agents. RAL (1200) refers to the 1200 mg dosage of raltegravir, while RAL refers to the 400 mg dosage of raltegravir. EFV (400) refers to the 400 mg dosage of efavirenz, while EFV refers to the 600 mg dosage of efavirenz.
AE: Adverse event; CrI: Credible interval; INSTI: Integrase strand transfer inhibitor; NNRTI: Non-nucleoside reverse transcriptase inhibitor; PI: Protease inhibitor; RD: Risk difference.
Treatment-related adverse events
The estimated absolute risk of PWH experiencing any TRAE on B/F/TAF was 22% (Supplementary Table 12). This risk was statistically lower for B/F/TAF compared with EFV + ABC/3TC, EFV (+ or /) TDF/FTC and ATV (+ or /) r + TDF/FTC and numerically lower compared with all seven other interventions included in the network (A). B/F/TAF had a mean SUCRA of 0.84 (the highest mean SUCRA value of any intervention), suggesting that, on average, it outperformed 84% of interventions included in this network (Supplementary Table 13). Compared with B/F/TAF, the risk of experiencing TRAEs was between 14 and 39 percentage points higher for non-nucleoside reverse transcriptase inhibitor (NNRTI)-based regimens (RD between 0.14 [-0.10, 0.46] and 0.39 [0.05, 0.64]). For INSTI-based regimens, there was a less clear trend in favor of B/F/TAF. While RAL-containing regimens performed similarly to B/F/TAF, the risk of experiencing TRAEs was numerically higher for DTG-containing regimens compared with B/F/TAF. For PI-based regimens, the risk of TRAEs was higher for ATV (+ or /) r + TDF/FTC and similar for DRV (+ or /) r +TDF/FTC versus B/F/TAF.
Grade 3/4 TEAEs
The estimated absolute risk of PWH experiencing any grade 3/4 TEAE on B/F/TAF was 9% (Supplementary Table 12). This risk was numerically lower for B/F/TAF compared with EFV (+ or /) TDF/FTC, and comparable with the three other interventions (DTG (+ or /) ABC/3TC, RPV (+ or /) TDF/FTC and DTG + F/TAF) included in the network (B). B/F/TAF had a mean SUCRA of 0.50, suggesting that, on average, it performed better than half of the five interventions included in this network (Supplementary Table 13).
Diarrhea
The estimated absolute risk of PWH experiencing diarrhea on B/F/TAF was 12% (Supplementary Table 12). This risk was numerically lower for B/F/TAF compared with DRV (+ or /) r + TDF/FTC and ATV (+ or /) r + TDF/FTC, and similar to the four other treatments included in this analysis (A). B/F/TAF had a mean SUCRA of 0.64 (the joint highest mean SUCRA value of any intervention), suggesting that, on average, it performed better than 64% of the seven interventions included in this network (Supplementary Table 13). Compared with B/F/TAF, the risk of experiencing diarrhea was 20 percentage points higher for DRV (+ or /) r + TDF/FTC (RD: 0.20 [-0.06, 0.64]) and four percentage points higher for ATV (+ or /) r + TDF/FTC (RD: 0.04 [-0.07, 0.27]).
Nausea
The estimated absolute risk of PWH experiencing nausea on B/F/TAF was 9% (Supplementary Table 12). This risk was statistically lower for B/F/TAF compared with DRV (+ or /) r + TDF/FTC and DTG (+ or /) ABC/3TC and numerically lower compared with all other interventions except DTG + F/TAF and RPV (+ or /) TDF/FTC, which had a comparable risk of experiencing nausea (B). B/F/TAF had a mean SUCRA of 0.83 (the second-highest mean SUCRA value of any intervention), suggesting that, on average, it performed better than 83% of the ten interventions included in this network (Supplementary Table 13). Compared with B/F/TAF, the risk of experiencing nausea was 50 percentage points higher for the PI-based DRV (+ or /) r + TDF/FTC regimen (RD: 0.50 [0.05, 0.85]), and 11 percentage points higher for the INSTI-based DTG (+ or /) ABC/3TC regimen (RD: 0.11 [0.00, 0.27]). For other NNRTI- and INSTI-based regimens, the risk of nausea was similar or numerically higher compared with B/F/TAF (RD between -0.02 [-0.08, 0.25] and 0.10 [-0.03, 0.33] for NNRTI- and between 0.01 [-0.05, 0.13] and 0.08 [-0.06, 0.46] for INSTI-based regimens).
All-cause discontinuation
The estimated absolute risk of PWH discontinuing on B/F/TAF due to any cause (not specifically due to AEs alone) was 7% (Supplementary Table 12). Differences in risk were small; however, B/F/TAF showed numerically fewer all-cause discontinuations than EFV + ABC/3TC, ATV + c + TDF/FTC, and EFV (+ or /) TDF/FTC, and was comparable to the remaining eight regimens in the network (A). B/F/TAF had a mean SUCRA of 0.56, suggesting that, on average, it performed better than 56% of the 12 interventions included in this network (Supplementary Table 13).
Discontinuation due to AE
The estimated absolute risk of PWH discontinuing on B/F/TAF due to AE was 1% (Supplementary Table 12). This risk was statistically lower for B/F/TAF compared with EFV + ABC/3TC, EFV (+ or /) TDF/FTC, RAL + TDF/FTC, ATV + c + TDF/FTC and ATV (+ or /) r + TDF/FTC, and numerically lower or comparable to the seven other interventions including all remaining PI-based, INSTI-based, and NNRTI-based regimens (B). B/F/TAF had a mean SUCRA of 0.85 (the second-highest mean SUCRA of any intervention), suggesting that, on average, it performed better than 85% of the 13 interventions included in this network (Supplementary Table 13). Compared with B/F/TAF, the risk of PWH discontinuing due to AE was between 13 and 16 percentage points higher for the NNRTI-based regimens containing EFV 600 mg (RD between 0.13 [0.02, 0.54] and 0.16 [0.02, 0.64]) and between 6 and 7 percentage points higher for the INSTI-based RAL + TDF/FTC regimen and the PI-based regimens containing ATV.
Resistance mutations
Resistance mutations are summarised in Supplementary Table 21. Due to differences in reporting of resistance mutations across studies, the low incidence and the agent-specific nature of resistance, no NMA was feasible for treatment-emergent resistance mutations. As such, we summarise results qualitatively here. For the B/F/TAF arms in both the GS-US-380-1489 and GS-US-380-1490 trials, no subject developed treatment-emergent resistance to any study drug. This drug resistance profile was similar to DTG-containing regimens, which were commonly associated with no resistance mutations. In contrast, a small number of both INSTI- and NRTI-associated resistance mutations were generally observed for RAL-containing regimens. Similarly, a small number of NNRTI- and NRTI- associated resistance mutations were observed for EFV-containing regimens whereas RPV + TDF/FTC had a substantially larger number of NNRTI- and NRTI-associated resistance mutations. Finally, no or very few resistance mutations were typically observed for PI-containing regimens. In summary, B/F/TAF did not lead to the development of any resistance mutations, while RAL- or NNRTI-containing regimens had the largest number of resistance mutations.
Week 96 results
Results from Week 96 showed broad consistency with Week 48, indicating that similar safety profiles were sustained for this later timepoint (Supplementary Table 22).
Discussion
Summary of findings
SLR & feasibility assessment
This analysis of interventions in the treatment of HIV-1 in TN PWH was based on evidence from RCTs identified in an SLR, whose most recent update was conducted in June 2023. A total of 39 studies were identified in TN PWH. The feasibility of conducting indirect comparisons with the studies identified in the SLR was then assessed. Overall, 19 studies were eligible for indirect comparisons after application of suitable eligibility criteria and an assessment of network connectivity. Analyses were deemed to be feasible for all outcomes of interest (other than resistance mutations) at Week 48 and Week 96.
Indirect comparisons
The NMA revealed that B/F/TAF had superior safety compared with many other ART regimens and was not statistically inferior for any outcome versus any intervention.
In particular, the results showed that B/F/TAF had a more favorable safety profile compared with NNRTI-containing regimens. Compared with PI-containing regimens, B/F/TAF substantially reduced nausea alongside some improvements for other safety outcomes such as TRAEs and discontinuations due to AEs. While B/F/TAF generally had a similar safety profile to other INSTI-containing regimens, the risk of nausea and discontinuation due to AE was lower for B/F/TAF. Furthermore, B/F/TAF had a lower risk of TRAE compared with DTG-containing regimens. The estimated absolute risk of PWH discontinuing on B/F/TAF due to AEs was 1%, which was numerically lower than the majority of other ART regimens included in the analysis. Although PI regimens are generally associated with a high risk of diarrhea, only numerical differences were observed versus B/F/TAF [58]. In particular, the lack of statistical significance versus DRV (+ or /) r + TDF/FTC is likely due to the limited sample size of the METABOLIK study informing this comparison (n = 34 in the DRV/r arm, and n = 31 in the ATV/r arm) [59]. Furthermore, B/F/TAF was not associated with any resistance mutations, while RAL- and NNRTI-based regimens lead to substantially larger numbers of resistance mutations.
These findings collectively support the potential of B/F/TAF as a valuable treatment option for HIV-1 infection, and reaffirm the favorable safety and tolerability profile of B/F/TAF, which aligns with its status as a preferred first-line regimen in both US and UK HIV-1 treatment guidelines [12,60]. However, in resource-limited settings, access to B/F/TAF may be impeded by economic and access constraints. Despite these barriers, its simplified dosing regimen and fewer side effects could make B/F/TAF a promising option in these settings.
Previous NMAs in the TN population have considered regimens of different backbones but the same third agent as either distinct or equivalent within a network [56,57,61]. Our analysis was in line with Radford et al. and Zhang et al. in not assuming equivalency of backbones of regimens of the same third agent [56,58]. For instance, in our NMA, DTG (+ or /) ABC/3TC, DTG + 3TC, DTG + F/TAF and DTG + TDF/FTC were treated as separate treatment nodes. Additionally, the results of our NMA are consistent with earlier indirect comparisons of ARTs in TN PWH, demonstrating that B/F/TAF yields noninferior safety outcomes to other ARTs [56,57,58]. Notably, our NMA provides a more comprehensive overview of safety and is the first to provide comparative evidence on specific AEs, such as nausea and diarrhea, when comparing B/F/TAF to ART regimens.
Strengths & limitations
The strengths of this work include that the SLR was conducted conforming to Cochrane guidelines, and identified RCTs assessing the safety of complete ART regimens for the treatment of HIV-1, meaning that the evidence informing the analysis was systematically identified and up to date. Data extracted during the SLR included a range of study characteristics, patient baseline characteristics and outcomes, allowing a comprehensive feasibility assessment to be conducted, and a range of clinically relevant safety outcomes to be considered for analysis. A systematic feasibility assessment ensured that studies informing the indirect comparisons were broadly comparable in terms of study design, patient populations and reported outcomes.
Reporting on outcomes of interest was mostly consistent across included studies, which meant that connected networks were possible for most outcomes at the timepoints of interest. Some differences were observed in definition of discontinuation (with some studies only reporting on study rather than treatment discontinuation). However, these differences are expected to have limited impact on the discontinuation results.
Bayesian NMAs were conducted, with the methodology used in line with key methodological guidance documents (in particular, NICE DSU TSDs 2, 3 and 4) [26,27,58]. Multiple models were independently fitted for each outcome, allowing for an assessment of the most appropriate model for each outcome. Specifically, although both RE and FE models were fitted, RE models were selected to allow for between-study heterogeneity. Networks at Week 48 included evidence from most of the regimens of interest and included regimens with INSTI, NNRTI and PI third agents, allowing for comparisons across most key competitors and across different treatment classes.
Limitations of this work include that the SLR, on which the NMA was based, was restricted to publications written in English; hence, relevant publications in other languages would have been excluded, which may limit the global relevance of the results. In addition, only phase III RCTs and beyond were included, meaning that any study using observational data in a real-world setting would not have been captured. Future work may wish to explore longer-term data given the critical role of ART safety and tolerability in ensuring long-term adherence for sustained HIV-1 management. Another limitation of the studies included in this NMA was the lack of blinding, which may have introduced bias in the reporting of safety outcomes, particularly AEs, which are often subjective and susceptible to influence by awareness of treatment allocation among participants or investigators. Nonetheless, inclusion of unblinded studies was necessary to maintain network connectivity across key treatment nodes. Furthermore, the last searches for this SLR were conducted in June 2023; however, to our knowledge no critical new data on interventions and outcomes considered in the present NMA have been published since the search date.
While the feasibility assessment was thorough and identified suitable evidence, the heterogeneity assessment of clinically meaningful characteristics did show some potential imbalances across studies included in the NMA. In particular, there was evidence of differences in patient demographics across studies, particularly with regards to age and ethnicity. These differences could, for example, influence discontinuation events across studies. However, appropriate decisions were made to limit heterogeneity where feasible, namely, studies reporting on a late presenter population with AIDS or populations with only acute PWH were excluded in order to reduce the heterogeneity in baseline viral load and CD4 cell count across studies and ensure that all CD4 cell counts were above the 200 cells/ul threshold for AIDS. Furthermore, RE models were used to accommodate some degree of heterogeneity across studies, although it is worth noting that most treatment contrasts were informed primarily by single studies, and therefore limited information was available to robustly estimate the between-study heterogeneity parameter.
While the NMA was conducted on networks that included regimens with INSTI, NNRTI and PI third agent classes, the effect of treatment classes was not specifically estimated. Further work may wish to explore the effect of specific third agent classes, in addition to the effects of individual regimens explored via this analysis.
Conclusion
This analysis provides valuable insights into the comparative safety profile of B/F/TAF versus various ART regimens for HIV-1 infection in TN PWH. The analysis was based on a rigorous SLR and comprehensive feasibility assessment and included 20 high-quality RCTs.
B/F/TAF performed better than the majority of interventions in safety and tolerability outcomes, notably discontinuation due to AEs, TRAEs and nausea. Additionally, with comparable risk of experiencing grade 3/4 treatment-emergent AEs, diarrhea and all-cause discontinuation rates to other interventions, B/F/TAF was non-inferior to any other regimen for all outcomes.
While the heterogeneity in patient demographics may have some influence on the results, the findings of this NMA support the conclusion that B/F/TAF has a comparable or favorable safety profile over the majority of ART regimens for HIV-1 infection.
Summary points
•
HIV-1 continues to be a significant global health concern, with 1.3 million new infections and 630,000 AIDS-related deaths in 2023.
•
Bictegravir, emtricitabine and tenofovir alafenamide (B/F/TAF) is a single-tablet regimen approved for managing HIV-1 infection in treatment-naïve (TN) and virologically suppressed people with HIV-1 (PWH) on a stable ART regimen with no known or suspected substitutions associated with resistance to bictegravir or tenofovir.
•
Clinical trials have demonstrated the efficacy and safety of B/F/TAF in TN populations, making it one of the recommended initial ART regimens for most PWH.
•
The aim of this systematic literature review (SLR) and network meta-analysis (NMA) was to compare the safety outcomes of B/F/TAF with other ART regimens in TN PWH, focusing on critical safety and tolerability outcomes.
•
A comprehensive search of MEDLINE, Embase, and The Cochrane Library was conducted, identifying relevant studies of B/F/TAF and comparator regimens. Bayesian NMAs were conducted to evaluate comparative safety profiles of included regimens.
•
Out of 39 identified studies in TN PWH, 19 studies were deemed suitable for indirect comparisons based on heterogeneity and network connectivity assessments.
•
The NMA revealed that B/F/TAF demonstrated superior safety compared with many other ART regimens and was not statistically inferior for any outcome versus any intervention.
•
The estimated risk of discontinuation due to adverse events (AEs) was 1%, with B/F/TAF particularly outperforming NNRTI-containing regimens and PI-containing regimens in terms of safety and tolerability.
•
B/F/TAF showed a favorable safety profile with reduced treatment-related AEs, discontinuations due to AEs, and nausea compared with other regimens, while being non-inferior for all assessed outcomes. B/F/TAF is therefore a comparatively safe and tolerable option for initial ART therapy in TN PWH.
Author contributions
M Chen, J Jarrett, B Gandhi-Patel, EG Scerpella, P Chaudhari, T Curteis, A Karlsson, H Luedke contributed to study design. H Luedke, LA Eddowes, M Rubinstein, A Karlsson, M Hempfling contributed to acquisition of data. LA Eddowes, M Rubinstein, A Karlsson, M Hempfling, T Curteis contributed to the analysis of data. All authors contributed to the interpretation of data. All authors contributed to drafting the article or revising it critically for important intellectual content. All authors provided final approval of the version of the article to be published. The authors wish to acknowledge and honor the significant contributions of EG Scerpella, who passed away prior to the submission of this manuscript. We express our deepest gratitude for his invaluable input and dedication to this work.
Acknowledgments
The authors thank Jonathan Gurney from Costello Medical (London, UK) for supporting statistical analyses, Ania Bobrowska from Costello Medical (Cambridge, UK) for leading the systematic literature review, Katherine Massey from Costello Medical (Singapore) for supporting the clinical interpretation of the findings and Sari Wright from Costello Medical (London, UK) for administrative and organizational support of the project.
Financial disclosure
This study was funded by Gilead Sciences.
Competing interests disclosure
M Chen, J Jarrett, B Gandhi-Patel, EG Scerpella are employees and shareholders of Gilead Sciences Inc. P Chaudhari was contracted to Gilead Sciences Inc during manuscript development. T Curteis, LA Eddowes, A Karlsson, H Luedke, M Rubinstein, M Hempfling are employees of Costello Medical, which was funded by Gilead to conduct the study. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support was provided by E Dinkar of Costello Medical (Cambridge, UK) and was funded by Gilead.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data that have been shared with them, and that the use of this shared data is in accordance with the terms (if any) agreed upon their receipt. The source of this data is: ACTG5257 (NCT00811954), ALTAIR (NCT00335322), ARIA (NCT01910402), ASSERT (NCT00549198), ATADAR (NCT01274780), ECHO (NCT00540449), ENCORE1 (NCT01011413), Epzicom-Truvada, GS-US216-0114 (NCT01108510), GS-US-380-1489 (NCT02607930), GS-US-380-1490 (NCT02607956), Honda 2011 (NCT00280969), METABOLIK (NCT00757783), NEAT001/ANRS143 (NCT01066962), ONCEMRK (NCT02131233), SINGLE (NCT01263015), STaR (NCT01309243), STARTMRK (NCT00369941), SYMTRI (EudraCT2018-001645-14). Please note, 20 further studies were identified in the SLR but no analyses were conducted on these.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.pdf)
- Download
- 745.56 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
World Health Organization (WHO). HIV data and statistics 2024 [14 August 2024]. Available from: https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/hiv/strategic-information/hiv-data-and-statistics
2.
Castro-Gonzalez S, Colomer-Lluch M, Serra-Moreno R. Barriers for HIV cure: the latent reservoir. AIDS Res. Hum. Retroviruses 34(9), 739–759 (2018).
3.
Trickey A, May MT, Vehreschild J-J et al. Survival of HIV-positive patients starting antiretroviral therapy between 1996 and 2013: a collaborative analysis of cohort studies. Lancet HIV 4(8), e349–e356 (2017).
4.
Waters L, Winston A, Reeves I et al. BHIVA guidelines on antiretroviral treatment for adults living with HIV-1 2022. HIV Med. 23(Suppl. 5), 3–115 (2022).
5.
Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in adults and adolescents living with HIV. (2022) Accessed: 2nd November 2023: https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-arv/what-start-initial-combination-regimens-antiretroviral-naive?view=full
6.
Food and Drug Administration (FDA). BIKTARVY® (bictegravir, emtricitabine, and tenofovir alafenamide) tablets, for oral use 2018. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/210251s000lbl.pdf
7.
Wohl DA, Yazdanpanah Y, Baumgarten A et al. Bictegravir combined with emtricitabine and tenofovir alafenamide versus dolutegravir, abacavir, and lamivudine for initial treatment of HIV-1 infection: week 96 results from a randomised, double-blind, multicentre, phase III, non-inferiority trial. Lancet HIV 6(6), e355–e363 (2019).
8.
Gallant J, Lazzarin A, Mills A et al. Bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir, abacavir, and lamivudine for initial treatment of HIV-1 infection (GS-US-380-1489): a double-blind, multicentre, phase III, randomised controlled non-inferiority trial. Lancet 390(10107), 2063–2072 (2017).
•• GS-US-380-1489 and GS-US-380-1490 are pivotal trials which compared B/F/TAF with other antiretroviral therapy (ART) regimens (ABC/DTG/3TC and DTG/F/TAF, respectively) in the treatment-naive (TN) population.
9.
Orkin C, DeJesus E, Sax PE et al. Fixed-dose combination bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir-containing regimens for initial treatment of HIV-1 infection: week 144 results from two randomised, double-blind, multicentre, phase III, non-inferiority trials. Lancet HIV 7(6), e389–e400 (2020).
10.
Sax PE, Pozniak A, Montes ML et al. Coformulated bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir with emtricitabine and tenofovir alafenamide, for initial treatment of HIV-1 infection (GS-US-380–1490): a randomised, double-blind, multicentre, phase III, non-inferiority trial. Lancet 390(10107), 2073–2082 (2017).
•• GS-US-380-1489 and GS-US-380-1490 are pivotal trials which compared B/F/TAF to other ART regimens (ABC/DTG/3TC and DTG/F/TAF respectively) in the TN population.
11.
Stellbrink HJ, Arribas JR, Stephens JL et al. Co-formulated bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir with emtricitabine and tenofovir alafenamide for initial treatment of HIV-1 infection: week 96 results from a randomised, double-blind, multicentre, phase III, non-inferiority trial. Lancet HIV 6(6), e364–e372 (2019).
12.
Esser S, Brunetta J, Inciarte A et al. Twelve-month effectiveness and safety of bictegravir/emtricitabine/tenofovir alafenamide in people with HIV: real-world insights from BICSTaR cohorts. HIV Med. 25(4), 440–453 (2024).
13.
Gandhi RT, Bedimo R, Hoy JF et al. Antiretroviral drugs for treatment and prevention of HIV infection in adults: 2022 recommendations of the international antiviral society–USA panel. JAMA 329(1), 63–84 (2023).
14.
Department of Health and Human Services. Panel on antiretroviral guidelines for adults and adolescents. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV 2024 [August 17, 2024]. Available from: https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-arv
15.
EACS Guidelines version 12.0 2023 [October 14, 2024]. Available from: https://www.eacsociety.org/media/guidelines-12.0.pdf
16.
Higgins J, Thomas J, Chandler J et al. Cochrane handbook for systematic reviews of interventions version 6.3 (updated February 2022). Cochrane. (2022) Available from: https://training.cochrane.org/handbook (
17.
Sterne JAC, Savović J, Page MJ et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. Brit. Med. J. 366, l4898 (2019).
18.
Sturtz S, Ligges U, Gelman A. R2WinBUGS: a package for running WinBUGS from R. J. Stat. Software 12, 1–16 (2005).
19.
Dunn D, Fink D, Gupta R et al. BHIVA guidelines on antiretroviral treatment for adults living with HIV-1 (2023 interim update).
20.
Waters L, Ahmed N, Angus B et al. BHIVA guidelines for the treatment of HIV-1-positive adults with antiretroviral therapy 2015 (2016 interim update). BHIVA, Royston, UK (2016).
21.
Scarsi KK, Havens JP, Podany AT, Avedissian SN, Fletcher CV. HIV-1 integrase inhibitors: a comparative review of efficacy and safety. Drugs 80(16), 1649–1676 (2020).
22.
Zhao AV, Crutchley RD, Guduru RC, Ton K, Lam T, Min AC. A clinical review of HIV integrase strand transfer inhibitors (INSTIs) for the prevention and treatment of HIV-1 infection. Retrovirology 19(1), 22 (2022).
23.
Electronic Medicines Compendium (EMC). Biktarvy 50 mg/200 mg/25 mg film-coated tablets 2023. Available from: https://www.medicines.org.uk/emc/product/9313/smpc/print
24.
Noyes J, Booth A, Cargo M et al. Qualitative evidence. Cochrane Handbook Syst. Rev. Intervent. 525–545 (2019).
25.
Rouse B, Chaimani A, Li T. Network meta-analysis: an introduction for clinicians. Int. Emerg. Med. 12, 103–111 (2017).
26.
Dias S, Welton NJ, Sutton AJ, Ades A. NICE DSU Technical Support Document 2: a generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. (2011).
27.
Dias S, Sutton AJ, Welton NJ, Ades AE. NICE DSU Technical Support Document 3: heterogeneity: subgroups, meta-regression, bias and bias-adjustment. (2011).
28.
Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. NICE DSU Technical Support Document 4: inconsistency in networks of evidence based on randomised controlled trials. (2014).
29.
Turner RM, Jackson D, Wei Y, Thompson SG, Higgins JP. Predictive distributions for between-study heterogeneity and simple methods for their application in Bayesian meta-analysis. Stat. Med. 34(6), 984–998 (2015).
30.
Drozd DR, Saag MS, Westfall AO et al. Comparative effectiveness of single versus multiple tablet antiretroviral therapy regimens in clinical HIV practice. Medicine 96(14), e6275 (2017).
31.
Hutton B, Catala-Lopez F, Moher D. The PRISMA statement extension for systematic reviews incorporating network meta-analysis: PRISMA-NMA. Medicina Clínica (English Edition) 147(6), 262–266 (2016).
32.
Spiegelhalter DJ, Best NG, Carlin BP, Van Der Linde A. Bayesian measures of model complexity and fit. J. Royal Stat. Soc. Series B 64(4), 583–639 (2002).
33.
R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing Vienna, Austria (2022).
34.
Lunn D, Jackson C, Best N, Thomas A, Spiegelhalter D. 8.6.4: DIC for model comparison, in The BUGS book: A practical introduction to Bayesian analysis. CRC Press (2012).
35.
Sturtz S, Ligges U, Gelman A. R2WinBUGS: A Package for Running WinBUGS from R. J. Stat. Software 12(3), 1–16 (2005).
36.
Suanzes P, Curran A, Torres F et al. CMV viremia and disease in very advanced late presenters: an Advanz-4 trial substudy. International Antiviral Society 49 (2022).
37.
Podzamczer D, Micán R, Tiraboschi J et al. Darunavir/cobicistat/emtricitabine/tenofovir alafenamide versus dolutegravir/abacavir/lamivudine in antiretroviral-naive adults (SYMTRI): a multicenter randomized open-label study (PReEC/RIS-57). Open Forum Infect. Dis. 9(3), ofab595 (2022).
38.
Squires K, Sax PE, Cahn P et al. Doravirine versus ritonavir-boosted darunavir in antiretroviral-naive adults with HIV-1 (DRIVE-FORWARD): 48-week results of a randomised, double-blind, phase III, non-inferiority trial. Lancet HIV 5(5), e211–e220 (2018).
39.
Orkin C, Molina JM, Lombaard J et al. Once-daily doravirine in human immunodeficiency virus type 1-infected, antiretroviral-naive adults: an integrated efficacy analysis. Clin. Infect. Dis. 70(7), 1344–1352 (2020).
40.
Sax PE, DeJesus E, Mills A et al. Co-formulated elvitegravir, cobicistat, emtricitabine, and tenofovir versus co-formulated efavirenz, emtricitabine, and tenofovir for initial treatment of HIV-1 infection: a randomised, double-blind, phase III trial, analysis of results after 48 weeks.[Erratum appears in Lancet. 2012 Aug 25;380(9843):730]. Lancet 379(9835), 2439–2448 (2012).
41.
DeJesus E, Rockstroh J, Henry K et al. Co-formulated elvitegravir, cobicistat, emtricitabine, and tenofovir disoproxil fumarate versus ritonavir-boosted atazanavir plus co-formulated emtricitabine and tenofovir disoproxil fumarate for initial treatment of HIV-1 infection: a randomised, double-blind, phase III, non-inferiority trial. Lancet 379(9835), 2429–2438 (2012).
42.
Sax PE, Wohl D, Yin MT et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate, coformulated with elvitegravir, cobicistat, and emtricitabine, for initial treatment of HIV-1 infection: two randomised, double-blind, phase III, non-inferiority trials. [Erratum appears in Lancet. 2016 Apr 30;387(10030):1816; PMID: 27091463]. Lancet 385(9987), 2606–2615 (2015).
43.
Squires K, Kityo C, Hodder S et al. Integrase inhibitor versus protease inhibitor based regimen for HIV-1 infected women (WAVES): a randomised, controlled, double-blind, phase III study. Lancet HIV 3(9), e410–e420 (2016).
44.
Chéret A, Bauer R, Meiffrédy V et al. Once-daily dolutegravir versus darunavir plus cobicistat in adults at the time of primary HIV-1 infection: the OPTIPRIM2-ANRS 169 randomized, open-label, phase III trial. J. Antimicrob. Chemother. 77(9), 2506–2515 (2022).
45.
Mussini C, Roncaglia E, Sighinolfi L et al. A prospective randomised trial on abacavir/lamivudine plus darunavir/r or raltegravir in patients with CD4 + <200 cells/ul (PRADAR study). J. Int. AIDS Soc. Conference: 2018 International Congress on Drug Therapy in HIV Infection, Glasgow, UK 21(Suppl. 8), 41–42 (2018).
46.
Imaz A, Scevola S, Niubo J et al. HIV-1 RNA decay in semen and rectum with DTG PLUS 3TC versus BIC/FTC/TAF.Conference on Retroviruses and Opportunistic Infections (2022). https://www.croiconference.org/abstract/hiv-1-rna-decay-in-semen-and-rectum-with-dtg-plus-3tc-versus-bic-ftc-taf/
47.
Daar E, Tierney C, Fischl M et al. Atazanavir plus ritonavir or efavirenz as part of a 3-drug regimen for initial treatment of HIV-1. Ann. Intern. Med. 154(7), 445–456 (2011).
48.
Bracchi M, Pagani N, Dalla Pria A et al. A phase IV, open-label three-arm study investigating the impact of a combination of tenofovir disoproxil fumarate/emtricitabine with raltegravir or dolutegravir or elvitegravir/cobicistat on renal function in HIV-1 antiretroviral naïve patients. HIV Res. Clin. Pract. 22(5), 128–139 (2021).
49.
GS-US-236-0140 clinical trials record, renal effect of stribild or other tenofovir DF-containing regimens compared to ritonavir-boosted atazanavir plus abacavir/lamivudine in antiretroviral treatment-naive HIV-1 infected adults. Accessed January 2020: https://clinicaltrials.gov/ct2/show/NCT02246998
50.
Clotet B, Feinberg J, Van Lunzen J et al. Once-daily dolutegravir versus darunavir plus ritonavir in antiretroviral-naive adults with HIV-1 infection (FLAMINGO): 48 week results from the randomised open-label phase IIIb study. Lancet 383(9936), 2222–2231 (2014).
51.
Raffi F, Rachlis A, Stellbrink H et al. Once-daily dolutegravir versus raltegravir in antiretroviral-naive adults with HIV-1 infection: 48 week results from the randomised, double-blind, non-inferiority SPRING-2 study. Lancet 381(9868), 735–743 (2013).
52.
Rashbaum B, Spinner CD, McDonald C et al. Darunavir/cobicistat/emtricitabine/tenofovir alafenamide in treatment-naïve patients with HIV-1: subgroup analyses of the phase III AMBER study. HIV Res. Clin. Pract. 20(1), 24–33 (2019).
53.
GEMINI I Clinical Trials Record, an efficacy, safety, and tolerability study comparing dolutegravir plus lamivudine with dolutegravir plus tenofovir/emtricitabine in treatment naïve HIV infected subjects. Accessed January 2020: https://clinicaltrials.gov/ct2/show/NCT02831673
54.
GEMINI II Clinical Trials Record, an efficacy, safety, and tolerability study comparing dolutegravir (DTG) plus lamivudine (3TC) with dolutegravir plus tenofovir/emtricitabine in treatment naïve HIV infected subjects. Accessed January 2020: https://clinicaltrials.gov/ct2/show/NCT02831764
55.
Orkin C, Arasteh K, Hernandez-Mora MG et al. Long-active cabotegravir + rilpivirine for HIV maintenance: FLAIR week-48 results. HIV Med. 20(Suppl. 5), 6–7 (2019).
56.
Radford M, Parks DC, Ferrante S, Punekar Y. Comparative efficacy and safety and dolutegravir and lamivudine in treatment naive HIV patients. AIDS 33(11), 1739–1749 (2019).
• Radford et al. (2019), Snedecor et al. (2019) and Zhang et al. (2022) are previous network meta-analysis (NMAs) in the TN population comparing the efficacy and safety profiles of various ARTs and providing key methodological insights.
57.
Snedecor SJ, Radford M, Kratochvil D, Grove R, Punekar YS. Comparative efficacy and safety of dolutegravir relative to common core agents in treatment-naïve patients infected with HIV-1: a systematic review and network meta-analysis. BMC Infect. Dis. 19, 1–14 (2019).
• Radford et al. (2019), Snedecor et al. (2019) and Zhang et al. (2022) are previous NMAs in the TN population comparing the efficacy and safety profiles of various ARTs and providing key methodological insights.
58.
Zhang K, Zhang Y, Zhou J et al. Comparison of the efficacy and safety of a doravirine-based, three-drug regimen in treatment-Naïve HIV-1 positive adults: a Bayesian network meta-analysis. Front. Pharmacol. 13, 676831 (2022).
• Radford et al. (2019), Snedecor et al. (2019) and Zhang et al. (2022) are previous NMAs in the TN population comparing the efficacy and safety profiles of various ARTs and providing key methodological insights.
59.
Gupta R, Ordonez RM, Koenig S. Global impact of antiretroviral therapy-associated diarrhea. AIDS Pat. Care STDs 26(12), 711–713 (2012).
60.
Aberg J, Tebas P, Overton E et al. Metabolic effects of darunavir/ritonavir versus atazanavir/ritonavir in treatment-naive, HIV type 1-infected subjects over 48 weeks. AIDS research and human retroviruses. AIDS Res. Hum. Retrovirus. 28(10), 1184–1195 (2012).
61.
Sax PE, Arribas JR, Orkin C et al. Bictegravir/emtricitabine/tenofovir alafenamide as initial treatment for HIV-1: five-year follow-up from two randomized trials. EClinicalMedicine 59, 101991 (2023).
Information & Authors
Information
Published In
Copyright
© 2025 Gilead Sciences Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 13 December 2024
Accepted: 9 May 2025
Published online: 30 May 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative safety of B/F/TAF versus other antiretroviral therapy regimens for treatment-naïve people with HIV-1: a systematic literature review and network meta-analysis. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0231
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Graeme Moyle, Joshua Gruber, Megan Dunbar, Janna Radtchenko, Isobel McEwen, Neia Prata Menezes, Travis Lim, Charles Walworth, Paul Sax, Steven Santiago, Hector Bolivar, Richard A. Elion, Persistence and virologic outcomes of people with HIV (PWH) with suboptimal adherence on B/F/TAF or dolutegravir-based single-tablet regimens, Future Virology, 10.1080/17460794.2026.2689295, 21, 7, (445-452), (2026).