An international observational study assessing conservative management in hemorrhoidal disease: results of CHORALIS (aCute HemORrhoidal disease evALuation International Study)
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Real-world evidence on the management of hemorrhoidal disease (HD) is limited. This international study collected clinical practice data on the effectiveness of conservative treatments for acute HD on symptoms and quality of life (QoL), providing perspectives of treatment modalities from different continents. Patients & methods: The 4-week observational prospective CHORALIS study involved adult outpatients consulting for spontaneous complaints of hemorrhoids (graded using Goligher classification) and prescribed conservative treatments according to usual clinical practice. Assessments were: anal pain/discomfort (visual analog scale [VAS]), other signs/symptoms (patient questionnaire), Patient Global Impression of Change (PGI-C) questionnaire and disease-specific QoL (HEMO-FISS-QoL questionnaire). Results: Of 3592 participants, 3505 were analyzed (58.4% male; age 40.5 ± 13.7 years; history of HD in 48.4%; 72.1% Goligher grade I and II). Pain and discomfort were the most common symptoms. Most treatments were venoactive drugs (VADs; 90.9%), particularly micronized purified flavonoid fraction (MPFF; 73.7%) and diosmin (14.6%). All VAD-based therapies improved signs/symptoms (number/intensity/frequency of pain, discomfort, bleeding, swelling, itching and soiling) and QoL. MPFF was associated with a significantly greater proportion of patients with no symptoms (48.8 vs diosmin 34.4%, p < 0.001), pain disappearance (69.7 vs diosmin 52.8%, p < 0.001), treatment impact at 1 week rated on PGI-C as ‘very much better’ (30.5 vs diosmin 17.9%, p < 0.001) and shorter times to improvement (mean ± SD 3.9 ± 1.5 days vs diosmin 4.2 ± 1.7 days). Conclusion: In this prospective real-world study of patients with acute HD, conservative therapies consisting mainly of VADs, including MPFF, improved the clinical signs and symptoms of disease, as well as QoL. This study evidence supports clinical advantages associated with VADs, mostly MPFF, for effectively managing acute HD.
Plain language summary of the results of the CHORALIS study, an international observational study assessing non-surgical treatments in hemorrhoidal disease
What is this article about?
Hemorrhoids, also called piles, are vessels located in the anus. They can cause symptoms like pain, bleeding, swelling and itching and soiling and can affect a person's quality of life. The treatment given for hemorrhoids depends on how bad they are. This study looked at how well non-surgical hemorrhoid treatments prescribed in medical practice work, by asking nearly 3600 people with hemorrhoids.
What were the results?
Most of the people who took part in the study were treated with venoactive drugs (medicines that act on the blood vessels), which were mostly micronized purified flavonoid fraction (MPFF). The results showed that the venoactive drug treatments helped to improve the symptoms of hemorrhoids and quality of life and that the treatment based on MPFF seemed to work better than another type of treatment based on a medicine called diosmin. People who took MPFF said that they felt “very much better” and their symptoms got better faster than people taking other treatments. Both the people being treated and their doctors were satisfied with the effectiveness of the hemorrhoid treatments.
What do the results mean?
Overall, the results of the study suggest that using treatments that include venoactive drugs, especially MPFF, can make a positive difference for people with hemorrhoids by reducing their symptoms and improving their quality of life.
Hemorrhoidal disease (HD) is a common anal condition, defined as the symptomatic enlargement and distal displacement of the normal anal cushions [1]. HD is one of the most common causes of anal pathology, with a peak incidence between the ages of 45 and 65 years in both males and females [2]. However, the exact incidence of HD is difficult to determine, because affected individuals are often reluctant to present for medical attention [3,4]. For example, data from France showed that 85% of individuals with anal symptoms who were seen by general practitioners did not spontaneously share these symptoms with their physician, despite experiencing related discomfort [3].
Currently available data from Europe and Japan have reported the general prevalence of HD as 3–27% [3–6]. In general, prevalence data are limited, with the absence of data in some regions quite striking, such as in parts of Africa [7]. Prevalence rates are usually higher when data are captured as part of screening or diagnosis of other diseases. For example, HD was prevalent in 39% of individuals undergoing colorectal cancer screening in a study in Austria [8].
HD is generally mild, making its recognition and diagnosis difficult. Bleeding, itching, soiling and pain are the most common presentations, although symptoms can vary widely [8,9]. The pathophysiology underlying the development of HD remains to be fully elucidated, but it is widely accepted that sliding of the anal canal lining plays a major role, with hemorrhoids developing when the supporting tissues of the anal cushions disintegrate or deteriorate [10]. This is supported by data from individuals with HD who show significant pathological changes to the anal cushions [10,11]. In addition, there appears to be a vascular component to the pathogenesis of hemorrhoids involving both arterial and vascular systems. Vascular hyperplasia of both the submucosal rectal arteries and transmural branches of the superior rectal artery have been shown to correlate with the appearance of hemorrhoids [12]. Based on the histological findings of abnormal venous dilatation and distortion in individuals with hemorrhoids, dysregulation of vascular tone might also play a role in the development of hemorrhoids due to failure in draining of the hemorrhoidal plexus leading to engorgement [1]. Factors thought to exacerbate changes associated with the development of HD include those causing increased intra-abdominal pressure, such as constipation, straining during defecation, pregnancy and obesity, although there is currently insufficient evidence to allow causal relationships to be established for many of these factors [13–15].
Depending on its severity, HD can be managed by lifestyle modification (including dietary changes, regular exercise and avoidance of straining while passing stools) and non-invasive medical treatments (oral and topical medications) and by invasive non-surgical (sclerotherapy, rubber band ligation, infrared coagulation and cryotherapy) and surgical (hemorrhoidectomy, hemorrhoidal artery ligation and stapled hemorrhoidopexy) approaches [16,17]. The use of the latter invasive treatments has been well studied; however, the impact of lifestyle modifications and non-invasive interventions on various aspects of HD (such as symptoms and quality of life across HD grades) has received less detailed investigation.
Recently, the Chronic venous and HemORrhoidal diseases evalUation and Scientific research (CHORUS) study provided up-to-date international data on patients presenting with HD in clinical practice across the world, and explored the frequency with which HD coexists with chronic venous disease [18]. However, CHORUS did not include follow-up visits, preventing determination of the effectiveness of strategies used to manage HD. Furthermore, to the best of our knowledge, there are no published large-scale studies describing real-world conservative treatment approaches to HD or the quality of life (QoL) of patients with HD that include different geographic areas across the world. Therefore, the aim of the aCute HemORrhoidal disease evALuation International Study (CHORALIS) was to collect large-scale data from clinical practice to evaluate the effectiveness of conservative treatments (i.e., lifestyle modifications and/or non-invasive interventions) in individuals presenting in the acute phase of HD. Areas of interest were patient-reported signs and symptoms, quality of life and management of HD in a real-world setting.
Participants & methods
Study design
CHORALIS was an international, observational, prospective, longitudinal study (NCT04578730) conducted in nine different countries that enrolled consecutive individuals who presented with spontaneous complaints of hemorrhoids to different healthcare professionals (such as proctologists, surgeons, gastroenterologists and general practitioners) in a variety of settings (hospitals, clinics and private practice) between 16 April 2021 and 25 November 2022. The study protocol received ethical approval in each country where participants were enrolled, and, when applicable, at each study center. All study procedures were conducted in accordance with the principles of the Declaration of Helsinki, and all participants provided written informed consent.
Study population
Eligible participants were aged ≥18 years and had either sought physician consultation spontaneously or were referred during the symptomatic acute phase of HD (<48 h after the beginning of symptoms), and the investigator had confirmed the diagnosis of HD. Individuals were excluded if they were consulting for an emergency not related to HD; were currently taking any treatment for HD; had undergone any anorectal procedure/surgery in the previous 6 months or had an anorectal procedure/surgery planned during the study; had incomplete convalescence after previous anorectal procedure/surgery; had known present perianal sepsis, inflammatory bowel disease, colorectal malignancy, pre-existing sphincter injury, diseases of the anal canal (fissures, fistulas, proctitis), coagulation disorders, or severe systemic disease likely to interfere with the study evaluation; or were pregnant or breastfeeding (for females). The complete study exclusion and inclusion criteria are provided in the Supplementary Materials (Supplementary Table 1).
Participant management & data collection
Investigators were instructed to continue to manage and treat participants according to their usual practice. At baseline (visit 0), participant demographic, clinical and lifestyle characteristics were recorded, and medical and medication history related to HD was taken. Participants were also asked to rate the severity of their anal pain and discomfort on 10-cm visual analog scales (VAS) from 0 (no pain/discomfort at all) to 10 (worst pain/discomfort ever experienced); to indicate the type and frequency of pain/discomfort; to indicate the presence and severity of bleeding, swelling, itching and soiling, and the frequency of bleeding; and to complete the HEMOrrhoid and FISSure QoL (HEMO-FISS-QoL) questionnaire, a disease-specific quality-of-life questionnaire [19]. The severity of the current HD episode was graded by the investigator using the Goligher classification [20].
A telephone ‘visit’ was scheduled 7 days after inclusion (visit 1), during which short questionnaires relating to patient-reported outcomes were completed. These included the Patient Global Impression of Change (PGI-C) questionnaire, which includes questions relating to symptom improvement and time to symptom improvement.
A face-to-face consultation was planned at 4 weeks after study inclusion (visit 2), during which participants repeated the PGI-C and HEMO-FISS-QoL questionnaires, the questionnaire relating to HD-related pain and discomfort (including the VAS) and the questionnaire regarding bleeding, swelling, itching and soiling (including severity and frequency). In addition, time to improvement was documented, and overall patient- and physician-rated satisfaction with prescribed treatment using a 5-point scale (from very unsatisfied to very satisfied), and any new prescriptions or need for additional follow-up were determined.
Outcomes
The primary objective of CHORALIS was to assess the effectiveness of conservative treatment of HD on patient-reported signs, symptoms and quality of life. This was determined using data from the PGI-C (global improvement score), time to improvement, evaluation of HD pain/discomfort and symptoms and responses on the HEMO-FISS-QoL questionnaire. Secondary objectives were as follows: assessment of patient and physician satisfaction with prescribed treatment and assessment of characteristics and management of HD in a real-world setting.
Statistical methods
Quantitative data are reported as mean with standard deviation (SD) or median with interquartile range and qualitative data are expressed as the number (n) and percentage (%) of participants. Within-group differences were evaluated using a paired t-test or Wilcoxon signed-rank test for continuous variables with normal or skewed distribution, respectively. McNemar's test or Cochran's Q test were used for categorical variables, according to the number of modalities of the variable.
Treatment effectiveness parameters for the two most commonly used venoactive drugs (VADs), i.e., micronized purified flavonoid fraction (MPFF)-based treatment and diosmin-based treatment, were compared using ranked analysis of covariance (ANCOVA) and Quade's method was used to transform the rank of the response variable and the covariate (baseline). The model was adjusted for country of enrolment and baseline characteristics (sex, age, ethnicity, body mass index, HD grade and intake of painkillers, laxatives, or topical agents) to improve inter-group comparability. Comparisons of proportions were performed using the Chi squared test.
Statistical significance was defined as a two-sided p-value of <0.05. All statistical analyses were performed with SAS® software version 9.4 or higher.
Results
Participants
A total of 3592 participants were included, 3505 of whom had available data for the main variables (age, sex, weight, height and HD grade) and completed at least one follow-up visit (analysis set). This included participants from China (n = 268), Hungary (n = 71), Kenya (n = 22), Nigeria (n = 902), Russia (n = 499), Saudi Arabia (n = 200), Senegal (n = 662), Ukraine (n = 679) and Vietnam (n = 202). Mean ± SD study duration per participant was 4.1 ± 0.6 weeks.
The study population (analysis set) included more males than females (58.4% vs 41.6%), the most common ethnicities were Caucasian/White and Black (40.2% and 45.0% vs 14.7% Asian, respectively) and the majority of participants (53.2%) reported moderate levels of physical activity while 30.1% were sedentary (Table 1). Just over two-thirds of female participants had previously given birth (mean number of births 2.7 ± 2.1; Table 1). The proportion of women who had ever given birth increased as HD severity increased, being 56.3% for those with grade I disease, 69.5% for grade II, 76.4% for grade III and 78.1% for grade IV. Water intake was <1.5 l/day in 60.5% of participants, and the majority of participants (63.4%) had poor fiber intake (fruit/vegetables making up less than a third of a meal). Almost half of study participants (48.4%) had a history of HD; of these, more than a third had experienced hemorrhoidal crisis in the previous 12 months (Table 1). The duration of the previous hemorrhoidal crisis was less than 1 week in 61.6% of participants.
| Treatment group | Overall (n = 3505) | |||
|---|---|---|---|---|
| Oral VAD based (including MPFF; n = 3168) | MPFF based (n = 2583) | Diosmin based (n = 511) | ||
| Demographic and clinical characteristics | ||||
| Female, n (%) | 1303 (41.1) | 1091 (42.2) | 174 (34.1) | 1458 (41.6) |
| Age, years, mean ± SD | 40.4 ± 13.6 | 40.7 ± 13.6 | 40.0 ± 13.7 | 40.5 ± 13.7 |
| Age group, n (%) | ||||
| 18–35 years | 1233 (38.9) | 990 (38.3) | 207 (40.5) | 1370 (39.1) |
| 35–50 years | 1200 (37.9) | 977 (37.8) | 192 (37.6) | 1310 (37.4) |
| 50–65 years | 521 (16.4) | 444 (17.2) | 72 (14.1) | 589 (16.8) |
| 65–80 years | 195 (6.2) | 155 (6.0) | 38 (7.4) | 214 (6.1) |
| ≥80 years | 19 (0.6) | 17 (0.7) | 2 (0.4) | 22 (0.6) |
| BMI, kg/m2, mean ± SD | 25.0 ± 4.2 | 25.0 ± 4.2 | 24.9 ± 4.1 | 24.9 ± 4.2 |
| Physical activity level†, n (%) | ||||
| Sedentary | 966 (30.5) | 796 (30.8) | 150 (29.4) | 1056 (30.1) |
| Moderate | 1682 (53.1) | 1375 (53.2) | 267 (52.3) | 1866 (53.2) |
| Intermediate | 420 (13.3) | 330 (12.8) | 76 (14.9) | 473 (13.5) |
| Intensive | 100 (3.2) | 82 (3.2) | 18 (3.5) | 110 (3.1) |
| Prolonged sitting (>5 h/day) during occupation | 731 (23.1) | 546 (21.1) | 154 (30.1) | 826 (23.6) |
| Smoking status, n (%) | ||||
| Never smoked | 2175 (68.7) | 1792 (69.4) | 331 (64.8) | 2453 (70.0) |
| Current smoker | 754 (23.8) | 597 (23.1) | 139 (27.2) | 789 (22.5) |
| Former smoker (>1 month ago) | 239 (7.5) | 194 (7.5) | 41 (8.0) | 263 (7.5) |
| Females only | ||||
| Given birth, yes, n (%) | 883/1303 (67.8) | 752/1091 (68.9) | 111/174 (63.8) | 983/1458 (67.4) |
| Births (n), mean ± SD | 2.7 ± 2.2 | 2.8 ± 2.3 | 2.2 ± 1.1 | 2.7 ± 2.1 |
| HD history | ||||
| History of hemorrhoids, n (%) | 1531 (48.3) | 1274 (49.3) | 218 (42.7) | 1697 (48.4) |
| Hemorrhoidal crisis in past 12 months, n (%) | 541/1531 (35.3) | 414/1274 (32.5) | 102/218 (46.8) | 627/1697 (36.9) |
| Duration of last hemorrhoidal crisis, n (%) | ||||
| <1 week | 323/541 (59.7) | 244/414 (58.9) | 61/102 (59.8) | 386/627 (61.6) |
| 1–2 weeks | 108/541 (33.3) | 138/414 (33.3) | 35/102 (34.3) | 195/627 (31.1) |
| 3 weeks | 38/541 (7.0) | 32/414 (7.7) | 6/102 (5.9) | 46/627 (7.3) |
| Treated for hemorrhoidal crisis, n (%) | 405/541 (74.9) | 319/414 (77.1) | 77/102 (75.5) | 438/627 (69.9) |
| Current presentation | ||||
| Hemorrhoid grade, n (%) | ||||
| I | 903 (28.5) | 768 (29.7) | 113 (22.1) | 1028 (29.3) |
| II | 1393 (44.0) | 1155 (44.7) | 212 (41.5) | 1501 (42.8) |
| III | 691 (21.8) | 540 (20.9) | 134 (26.2) | 777 (22.2) |
| IV | 163 (5.1) | 109 (4.2) | 48 (9.4) | 174 (5.0) |
| Constipation‡, n (%) | 872 (27.5) | 719 (27.8) | 135 (26.4) | 992 (28.3) |
†
Physical activity level: sedentary = reading, watching TV, or other sedentary activity; moderate = walking, cycling or other forms of exercise at least 4 h per week (including walking or cycling to the workplace, Sunday walking, etc.); intermediate = participation in recreational sports, heavy gardening, or similar activity for at least 4 h per week; intensive = participation in hard training or sport competitions, regularly and several times per week for at least 8 h per week.
‡
Constipation according to Rome IV criteria for Functional Constipation.
HD: Hemorrhoidal disease; MPFF: Micronized purified flavonoid fraction; SD: Standard deviation; VAD: Venoactive drug.
For the current presentation of acute HD, the diagnosis was confirmed by visual examination (68.6% of participants), digital examination (66.9%; primarily for differential diagnostic purposes), and/or anoscopy (46.8%). Hemorrhoid severity based on the Goligher classification was grade I in 29.3% of participants, grade II in 42.8%, grade III in 22.2% and grade IV in 5.0%. Just over a quarter of study participants (28.3%) had constipation based on the Rome IV criteria (Table 1).
At visit 0, individuals reported a mean of 4.5 ± 1.6 symptoms each. The mean number of symptoms was greater in participants with higher grade HD, i.e., 3.4 ± 1.4 in those with grade I HD, compared with 4.9 ± 1.4 to 5.4 ± 1.4 in those with grade II–IV HD.
Pain and discomfort were the most frequently reported symptoms at visit 0, occurring in 89.4% and 94.9% of individuals, respectively (Figure 1). These were of moderate intensity (mean VAS score, 4.9 ± 3.0 for pain and 5.4 ± 2.7 for discomfort). Itching, swelling and bleeding were also common, with 60.8%, 60.6% and 57.9% of individuals reporting these symptoms. Soiling occurred less frequently, in 24.9% of individuals. All symptoms/signs were present as early as grade 1. A higher grade of HD was associated with a slight increased incidence of all symptoms, and with a greater intensity of pain and discomfort (Figure 2), a greater severity of bleeding, swelling, itching and soiling, and a greater frequency of bleeding, pain and discomfort.
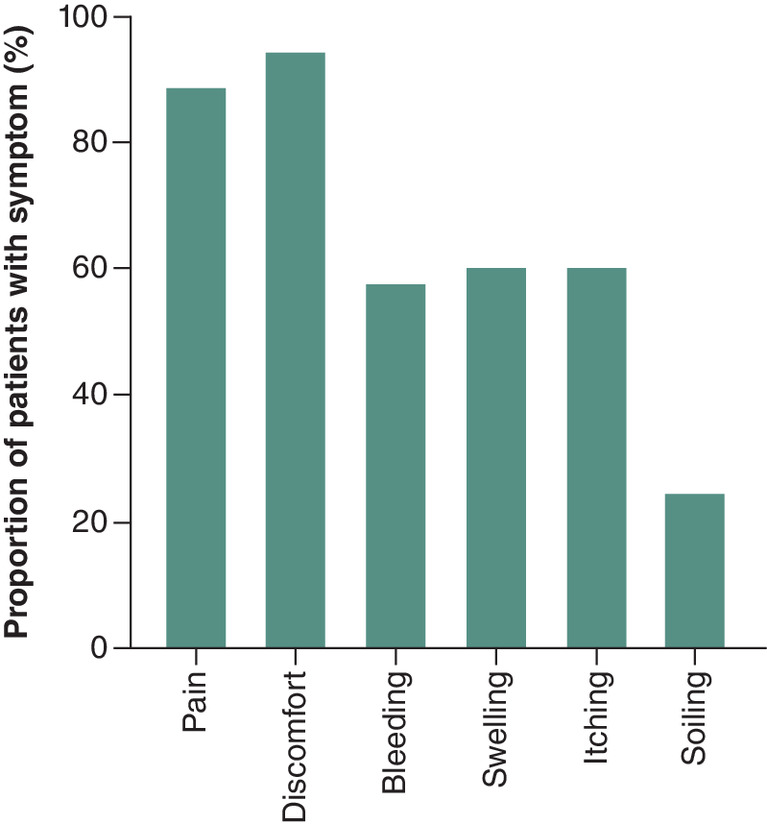
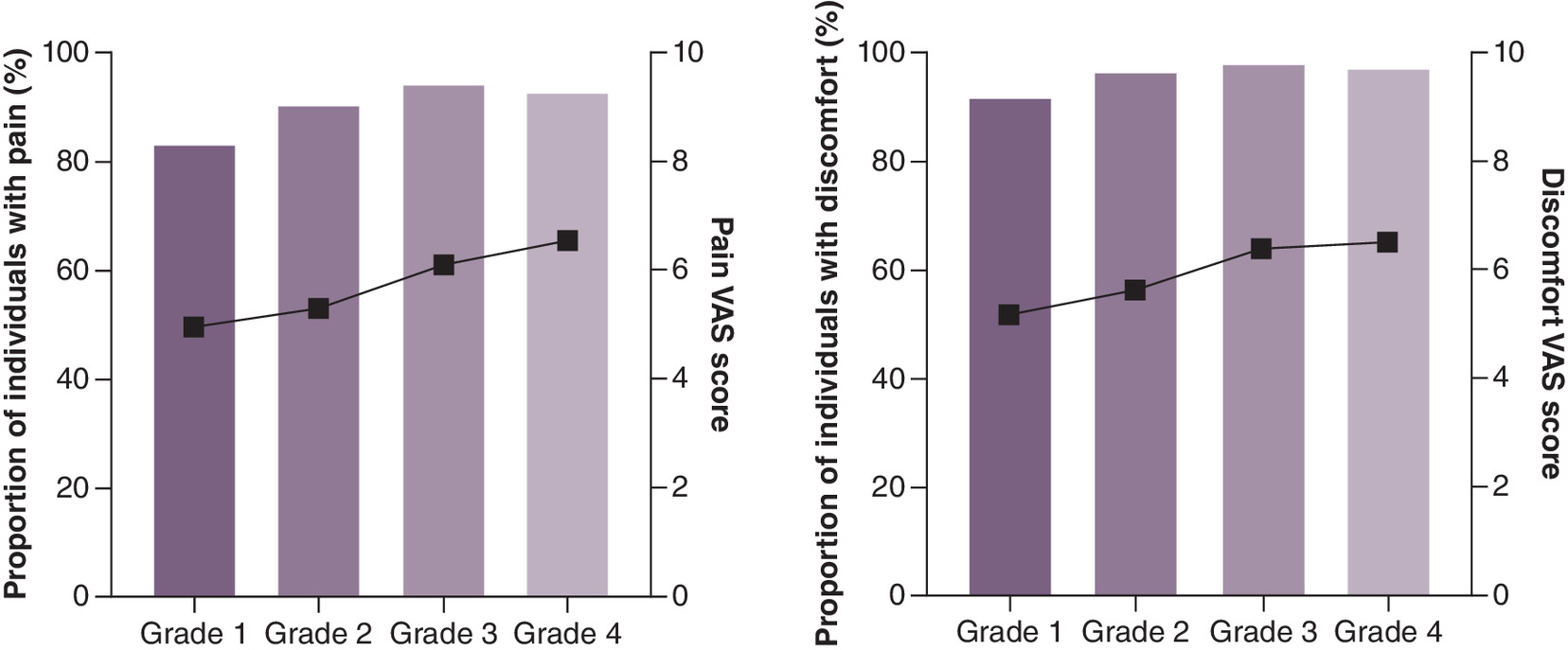
Figure 2. Proportion of participants with symptom and severity of pain and discomfort by grade of hemorrhoidal disease in the overall population at visit 0.
VAS: Visual analog scale.
The mean HEMO-FISS-QoL total score at visit 0 was 33.1 ± 21.3, indicating mild-to-moderate impact of HD on quality of life. Higher grade HD was associated with higher HEMO-FISS-QoL total score, indicating a greater impact on quality of life; mean score was 28.2 ± 20.5 for participants with grade I HD and 36.4 ± 23.1 in those with grade IV HD (p < 0.001). Baseline scores on the HEMO-FISS-QoL physical (31.8 ± 23.2), psychological (23.4 ± 22.3) and sexuality (25.8 ± 26.9) dimensions also showed the mild-to-moderate impact of HD on quality of life, while scores on the defecation dimension (51.5 ± 28.6) showed the greatest impact on quality of life. Grade III or IV HD was associated with worse QoL across all four HEMO-FISS-QoL dimensions.
No substantial or clinically relevant differences between subgroups based on the type of treatment received (i.e. between those receiving oral VAD-based, MPFF-based or diosmin-based therapy) were observed (Table 1).
Treatments
In addition to advice regarding lifestyle and dietary fiber intake, the most frequently prescribed treatment for HD was oral VAD-based treatments (n = 3185; 90.9%; Figure 3), including 2583 participants (73.7% of the analysis set; 81.1% of those receiving oral-VAD based treatments) who were receiving MPFF-based treatment and 511 (14.6%; 16.0%) receiving diosmin-based treatment. Topical treatments were used by 2055 (58.6%) participants (773 participants [22.1%] received both oral VAD and topical treatments), while 1375 (39.2%) participants received laxatives, 1348 (38.5%) analgesics and 471 (13.4%) other treatments (including traditional medicines, which were most popular in China and Vietnam; Figure 3).
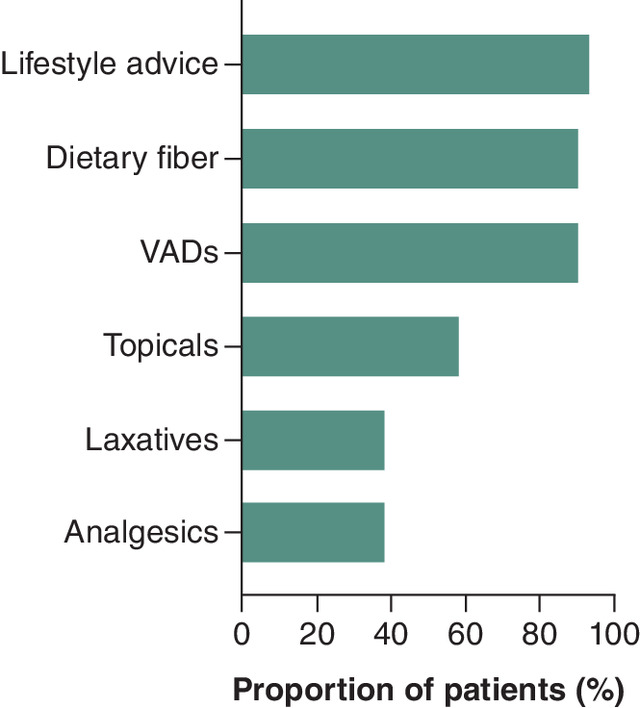
Figure 3. Prescribed treatments at visit 0, presented as proportion of individuals receiving each treatment.
VAD: Venoactive drug.
Of the treatment combinations compared in the current analysis, the most commonly prescribed treatment across all grades of HD was MPFF-based treatment. Individuals with grade IV HD were more likely to be treated with a combination of treatments, including VAD-based treatment added to topicals and laxatives. Conversely, VAD monotherapy was most commonly prescribed to individuals with grade I–II HD.
Treating physicians
Of the 121 physicians who contributed to this study, characteristics were available for 118. Most were proctologists (46.6%) or surgeons (33.8%; including vascular [0.8%], colorectal [9.3%] and general [22%] surgeons). The most common recommendation to individuals with HD was to consume more fiber (95.9% of physicians), followed by drink more water (95.0%); other common recommendations were to avoid spicy food (81.8%), avoid long periods of standing or sitting (77.7%), not strain during a bowel movement (72.7%), be careful with anoperineal hygiene (71.1%), get more exercise (70.2%) and lose weight (61.2%).
Hemorrhoidal disease symptoms
In participants receiving oral VADs (MPFF, diosmin and others), the number of symptoms per participant was significantly reduced from 4.6 at visit 0 to 1.4 at visit 2 (Table 2 and Figure 4). The number of symptoms per participant was reduced with both MPFF-based treatment (n = 2537; from 4.6 ± 1.6 at baseline to 1.3 ± 1.7 at visit 2), and diosmin-based treatment (n = 489; from 4.7 ± 1.7 to 1.7 ± 1.7, respectively; Table 2); this reduction was significantly greater with MPFF-based versus diosmin-based treatment (p = 0.018). At visit 2, a significant number of individuals (>90%) receiving VAD-based treatment showed improvement in their symptoms or even complete resolution in some cases. Significantly more individuals in the MPFF based-treatment group achieved symptom resolution at visit 2 compared with those receiving diosmin-based-treatment in regard to pain (69.7% vs 52.8%; p < 0.001), discomfort (57.6% vs 45.1%; p < 0.001) and itching (80.2% vs 73.7%; p = 0.012). Almost half (46.3%) of the VAD-based treatment group reported no more symptoms of HD at visit 2; the proportion was significantly higher with MPFF-based treatment (48.8%) than with diosmin-based treatment (34.4%, p < 0.001; Figure 5).
| Treatment group | |||
|---|---|---|---|
| Oral VAD-based (including MPFF; n = 3098) | MPFF-based (n = 2537) | Diosmin-based (n = 489) | |
| Participants reporting at least 1 symptom, n (%) | |||
| V0 | 3096 (99.9) | 2536 (100.0) | 488 (99.8) |
| V2 | 1664 (53.7) | 1300 (51.2) | 321 (65.6) |
| Symptoms per participant (n), mean ± SD | |||
| V0 | 4.6 ± 1.6 | 4.6 ± 1.6 | 4.7 ± 1.7 |
| V2 | 1.4 ± 1.7 | 1.3 ± 1.7 | 1.7 ± 1.7 |
| Change from V0–V2, mean ± SD | -3.2 ± 1.9§ | -3.3 ± 1.8§,¶ | -3.0 ± 2.1§ |
| VAS score, mean ± SD | |||
| Pain | |||
| V0 | 5.1 ± 2.9 | 5.1 ± 2.8 | 5.2 ± 3.2 |
| V2 | 0.7 ± 1.5 | 0.7 ± 1.4 | 0.9 ± 1.6 |
| Change from V0–V2 | -4.4 ± 2.8§ | -4.4 ± 2.7§,¶ | -4.3 ± 3.2§ |
| Discomfort | |||
| V0 | 5.6 ± 2.6 | 5.7 ± 2.5 | 5.4 ± 2.9 |
| V2 | 0.9 ± 1.5 | 0.9 ± 1.5 | 1.1 ± 1.6 |
| Change from V0–V2 | -4.7 ± 2.7§ | -4.8 ± 2.5§ | -4.4 ± 3.2§ |
| Proportion of participants with symptom, n (%) | |||
| Pain | |||
| V0 | 2816 (90.9) | 2322 (91.5) | 432 (88.3) |
| Resolution† | 1878 (66.7) | 1618 (69.7)†† | 228 (52.8) |
| Discomfort | |||
| V0 | 2977 (96.1) | 2453 (96.7) | 455 (93.0) |
| Resolution† | 1650 (55.4) | 1413 (57.6)†† | 205 (45.1) |
| Bleeding‡ | |||
| V0 | 1803 (58.2) | 1449 (57.1) | 307 (62.8) |
| Resolution† | 1624 (90.1) | 1310 (90.4) | 272 (88.6) |
| Swelling‡ | |||
| V0 | 1923 (62.1) | 1545 (60.9) | 329 (67.3) |
| Resolution† | 1444 (75.1) | 1149 (74.4) | 256 (77.8) |
| Itching‡ | |||
| V0 | 1969 (63.6) | 1653 (65.2) | 289 (59.1) |
| Resolution† | 1557 (79.1) | 1326 (80.2)# | 213 (73.7) |
| Soiling‡ | |||
| V0 | 800 (25.8) | 630 (24.8) | 153 (31.3) |
| Resolution† | 696 (87.0) | 553 (87.8) | 127 (83.0) |
†
In the subgroup of patients presenting the symptom at V0.
‡
At least one symptom at V0 and V2.
§
p < 0.001 for within-group comparison at visit 2 vs visit 0 (Wilcoxon signed rank test).
¶
p < 0.05 vs diosmin-based treatment (ranked ANCOVA performed using Quade's Method after transformation of rank of the response variable and the covariate [baseline]; the model was adjusted on Goligher grade, center, sex, BMI in category and analgesic, topical treatment and laxative use).
#
p < 0.05 vs diosmin-based treatment (Chi squared test).
††
p < 0.001 vs diosmin-based treatment (Chi squared test).
MPFF: Micronized purified flavonoid fraction; SD: Standard deviation; V0: Visit 0; V2: Visit 2; VAD: Venoactive drug; VAS: Visual analog scale.
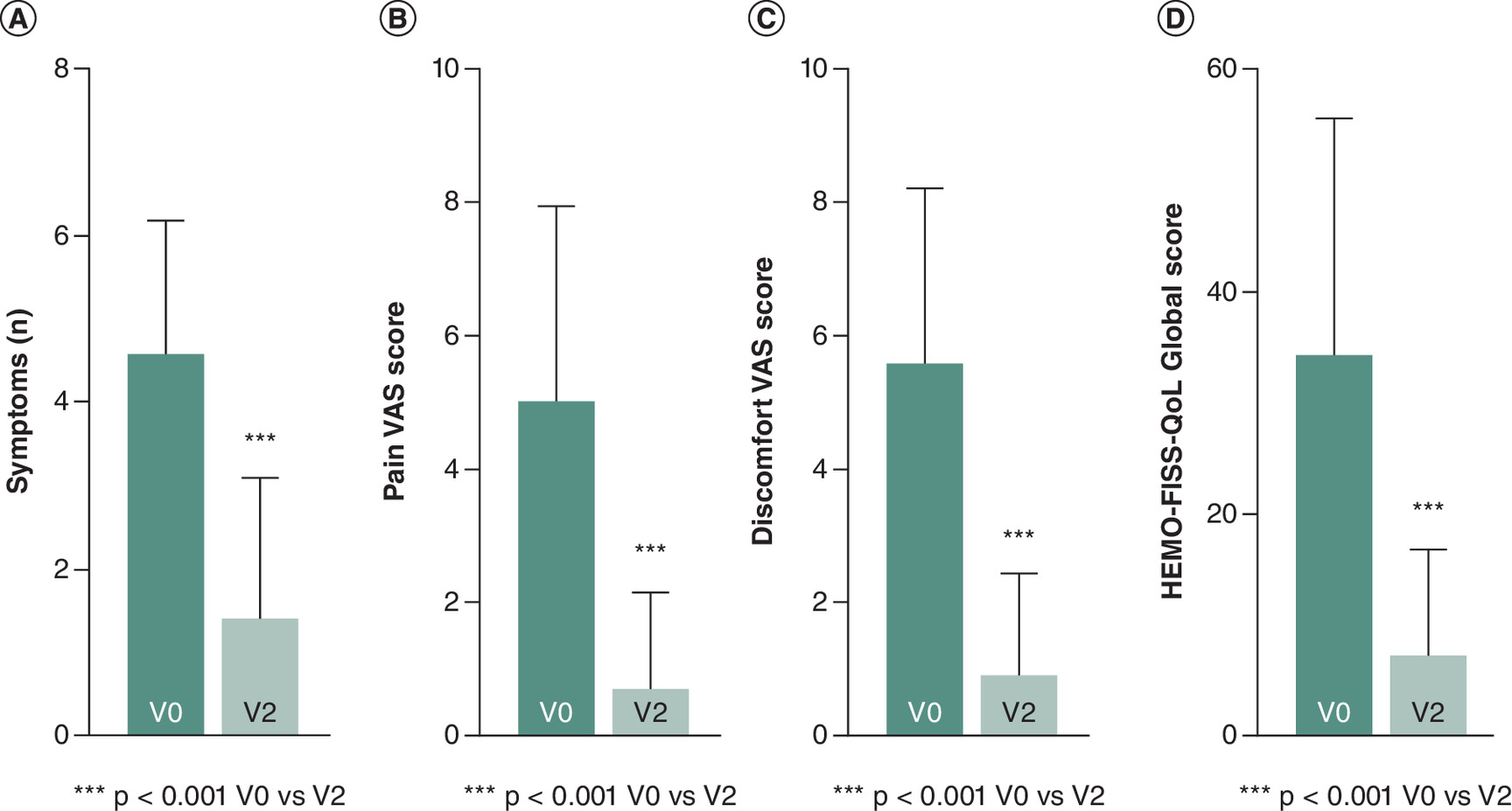
Figure 4. Effect of venoactive drugs on different catergories.
(A) Number of symptoms. (B) Severity of pain. (C) Severity of discomfort. (D) Quality of life.
HEMO-FISS-QoL: HEMOrrhoid and FISSure Quality of Life scale, SD: Standard deviation; V: Visit; VAS: Visual analog scale.
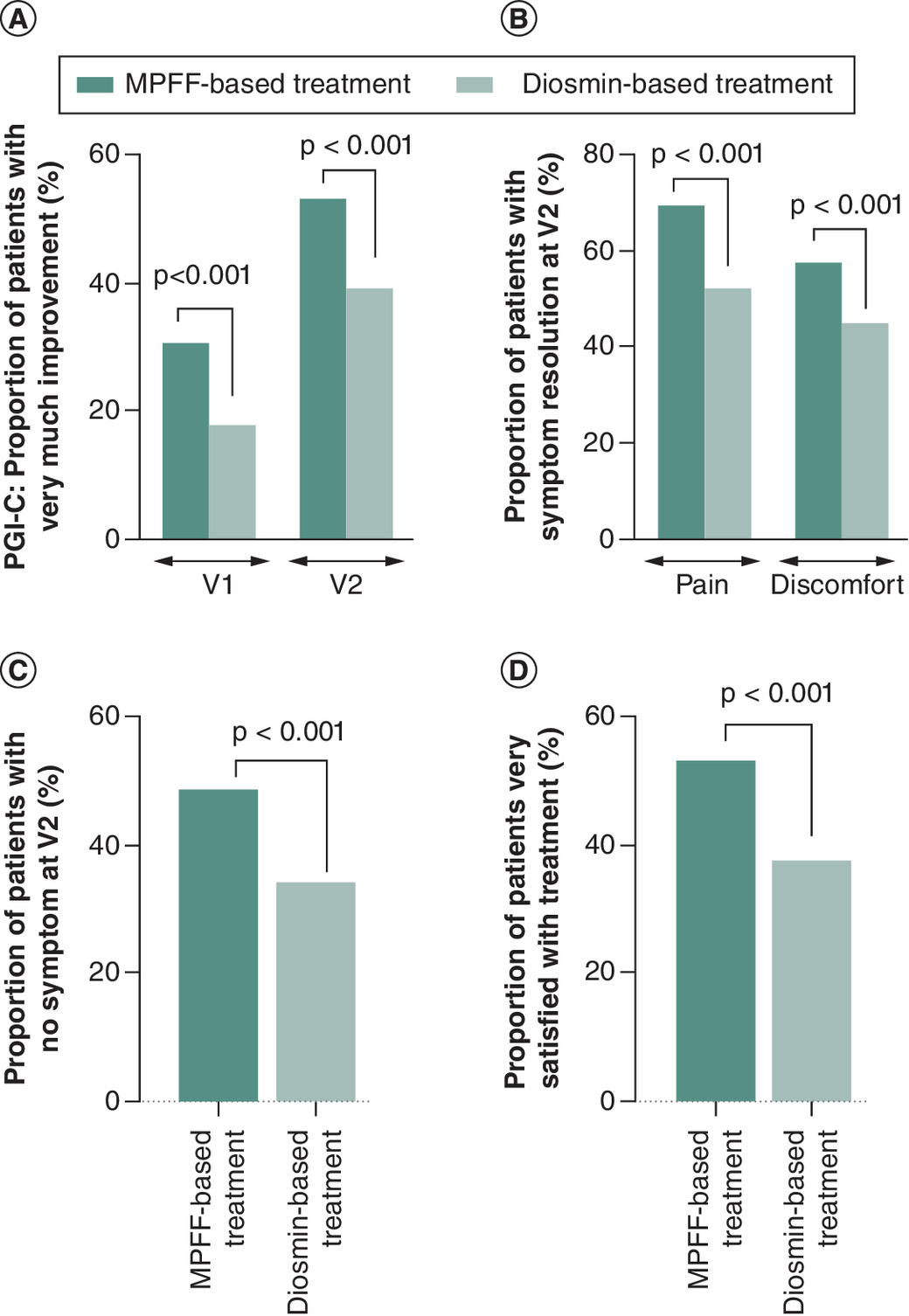
Figure 5. Effectiveness of micronized purified flavonoid fraction-based treatment versus diosmin-based treatment.
(A) Percentage of participants ‘very much improved’ according to the PGI-C at V1 and V2. (B) Percentage of participants with pain and discomfort resolution at V2. (C) Percentage of participants with no symptoms at V2. (D) Participant satisfaction with treatment.
MPFF: Micronized purified flavonoid fraction; PGI-C: Patient Global Impression of Change; V: Visit; VAS: Visual analog scale.
After 1 week (visit 1), the majority of participants reported an improvement in all symptoms, especially in pain, discomfort and bleeding; the proportion in the VAD-based treatment group who had improvements in these symptoms was 86.3, 75.3 and 64.8%, respectively. All symptoms improved whatever the baseline HD grade. VAS scores for both pain and discomfort decreased significantly from visit 0 to visit 2 (p < 0.001) in the VAD-based treatment group (Table 2 and Figure 4). The reduction from baseline in VAS pain score in the MPFF group was significantly greater than that in the diosmin-based treatment group (p = 0.035). In individuals who still had pain at visit 2, the majority (>80%) were experiencing pain during defecation, while spontaneous pain was less frequent across all treatment groups (p < 0.001 vs baseline). The frequency of pain also decreased significantly between baseline and visit 2 in all treatment groups (p < 0.001). Results were similar for the severity and frequency of discomfort (p < 0.05 vs baseline for all comparisons).
The proportion of participants reporting at least one bleeding symptom decreased substantially during treatment in all groups (Table 2). About 95% of individuals with bleeding at baseline had experienced symptom improvement at visit 2, with bleeding resolution achieved in approximately 90% (90.1%, 90.4% and 88.6% in the VAD-based, MPFF-based and diosmin-based treatment groups, respectively; Table 2).
For those who still had bleeding at visit 2, the frequency and severity of bleeding had improved in all treatment groups. The severity of bleeding decreased significantly in the VAD-based treatment group (p < 0.001), with 35.3, 19.2 and 3.7% of individuals reporting blood streaks on toilet paper, blood drops and a stream of blood, respectively, at visit 0, which decreased to 5.7, 0.6 and 0.0%, respectively, at visit 2. Similarly, significant (p < 0.001) reductions in bleeding severity between visit 0 and visit 2 were seen in the MPFF-based and diosmin-based treatment groups. Bleeding frequency also decreased significantly (p < 0.001 in all treatment groups); at visit 0, the most common bleeding frequency was once daily (in 41.7% of participants in the VAD-based treatment group), whereas at visit 2 the most common bleeding frequency was less than once a week (in 47.9% of participants in the VAD-based treatment group).
Results were consistent for the proportion of individuals with symptoms of swelling, itching and soiling, which decreased significantly from visit 0 to visit 2 in all treatment groups (Table 2). Of those participants who had at least one symptom of swelling, itching, or soiling at visit 0, an improvement in each of these symptoms was seen at visit 2 in over 90% of individuals in each treatment group, including complete resolution of symptoms in approximately 80%.
Patient global impression of change
After 1 week (visit 1), 95.8% of individuals in the VAD-based treatment group reported an improvement in their symptoms according to the patient global impression of change (PGI-C) scale, with 3.9% reporting no change and 0.3% a worsening. Further improvement was noted by visit 2 (98.8% improvement, 0.9% no change and 0.3% worsening). An improvement in symptoms according to the PGI-C was also seen at visit 1 and visit 2 in almost all participants in the MPFF-based and diosmin-based treatment groups.
As early as visit 1, the proportion of individuals who reported that they were ‘very much better’ was 28.3% in the VAD-based treatment group. The proportion was significantly higher in the MPFF-based treatment group (30.5%) compared with the diosmin-based treatment (17.9%, p < 0.001; Figure 5). By visit 2, the proportion of study participants reporting that they were ‘very much better’ had increased to 50.6% in the VAD-based treatment group and remained significantly higher in the MPFF-based compared with the diosmin-based group (53.3% and 39.3%, respectively, p < 0.001; Figure 5). Any kind of worsening over time was rare, being reported by <1% of individuals.
Improvement was reported to have taken a mean of 4.0 ± 1.5 days in the VAD-based treatment group. The mean time to improvement was significantly shorter in the MPFF-based treatment group (3.9 ± 1.5 days) than the diosmin-based treatment group (4.2 ± 1.7 days, p < 0.001).
Quality of life (HEMO-FISS-QoL)
Overall mean ± SD change in HEMO-FISS-QoL score from baseline to visit 2 was -26.0 ± 21.2 overall, -25.7 ± 23.2 for the physical dimension, -19.2 ± 21.5 for the psychological dimension, -38.6 ± 29.2 for the defecation dimension, and -20.4 ± 25.8 for the sexuality dimension (all p < 0.001). Changes in disease-specific quality of life over time by treatment group, as assessed by the median HEMO-FISS-QoL score, are summarized in Table 3. Consistent improvements were seen across all three treatment groups (VAD-based (Figure 4), MPFF-based and diosmin-based treatment). Reductions in the total HEMO-FISS-QoL score and scores on the physical, psychological, defecation and sexuality dimensions from visit 0 to visit 2 were statistically significant in all treatment groups (Table 3).
| Treatment group | |||
|---|---|---|---|
| Oral VAD-based (including MPFF; n = 3168) | MPFF-based (n = 2583) | Diosmin-based (n = 511) | |
| Change in HEMO-FISS-QoL score from V0–V2, median (Q1, Q3) | n = 2524 | n = 2117 | n = 345 |
| Total score | -22.8 (-39.4, -10.6)† | -23.3 (-40.3, -11.5)† | -20.1 (-36.9, -7.1)† |
| Physical dimension subscore | -22.4 (-41.7, -7.5)† | -22.5 (-42.5, -9.1)† | -20.8 (-38.9, -5.0)† |
| Psychological dimension subscore | -14.3 (-30.0, -3.6)† | -14.3 (-32.1, -3.6)† | -10.7 (-25.0, 0.0)† |
| Defecation dimension subscore | -33.3 (-58.3, -16.7)† | -37.5 (-58.3, -16.7)† | -33.3 (-58.3, -8.3)† |
| Sexuality dimension subscore | -19.5 (-25.5, 0.0)† | -20.1 (-37.5, 0.0)† | -12.5 (-25.0, 0.0)† |
†
p < 0.001 (Wilcoxon signed rank test).
HEMO-FISS-QoL: HEMOrrhoid and FISSure Quality of Life scale; MPFF: Micronized purified flavonoid fraction; Q1: Quartile 1; Q3: Quartile 3; QoL: Quality of life; V: Visit; VAD: Venoactive drug.
Patient & physician satisfaction
The majority of patients and physicians reported that they were satisfied or very satisfied with the treatment prescribed for HD (Table 4). The proportions of both patients and physicians who were very satisfied with treatment was significantly higher for MPFF-based (53.0 and 49.4%) than for diosmin-based treatment (37.5 and 37.9%, p < 0.001; Table 4 and Figure 5).
| Treatment group | |||
|---|---|---|---|
| Oral VAD-based (including MPFF; n = 3168) | MPFF-based (n = 2583) | Diosmin-based (n = 511) | |
| Patients | n = 3076 | n = 2516 | n = 488 |
| Very satisfied with prescribed treatment, n (%) | 1539 (50.0) | 1334 (53.0)† | 183 (37.5) |
| Satisfied with prescribed treatment, n (%) | 1325 (43.1) | 1021 (40.6) | 256 (52.5) |
| Physicians | n = 3076 | n = 2516 | n = 488 |
| Very satisfied with prescribed treatment, n (%) | 1466 (47.7) | 1244 (49.4)† | 185 (37.9) |
| Satisfied with prescribed treatment, n (%) | 1356 (44.1) | 1069 (42.5) | 255 (52.3) |
†
p < 0.001 vs diosmin-based treatment.
MPFF: Micronized purified flavonoid fraction; VAD: Venoactive drug.
Discussion
The results of this large (n = 3505), international, real-world study provide a detailed picture of the characteristics of individuals with HD, the impact of HD symptoms and the conservative treatments used to manage the condition as well as their effectiveness. In particular, several countries across different continents, including the African continent, were included in this study, providing valuable insights into the real-world management of HD in countries where such data are limited or nonexistent.
In terms of the occurrence of HD, both males and females were represented in the current study population, with a slight male predominance (58.4%), consistent with the findings of CHORUS [18]. The reasons underlying these findings are not completely clear. The slightly higher proportion of males with HD may reflect a higher likelihood that males will seek care for HD or that females are less likely to seek help for symptoms of HD (e.g., for cultural reasons). Alternatively, the differential rates in males versus females could simply be a consequence of underlying population demographics in the countries contributing individuals for this study.
The baseline data from CHORALIS also confirm the high rates of HD recurrence that have been reported previously [21]. Almost half of all CHORALIS participants reported previous episodes of hemorrhoids, and a third of these had experienced hemorrhoidal crisis in the previous 12 months.
The CHORALIS study cohort also presented with other recognized risk factors for HD, such as lower levels of physical activity, having given birth in females, and poor fiber and low water intake; however, constipation was not a common observation. Constipation was reported in just over one-quarter of participants in CHORALIS compared with just under half of all individuals in CHORUS [18]. The difference in rates of constipation between the two studies may be due to the different definitions used in the studies, with the Rome IV criteria (the most reliable criteria for defining constipation) used in CHORALIS and the Bristol stool scale (which primarily measures stool consistency) used in CHORUS. Alternatively and additionally, the low rate of constipation in CHORALIS could reflect a lack of association between constipation and HD, as previously reported [22].
At baseline, there was a mean of 4.5 symptoms per participant. The most frequently reported symptoms were pain and discomfort reported by 89.4% and 94.9% of individuals, respectively. This is superior to the observation made in the previous observational study CHORUS [18] and might be explained by the fact that in the present study patients consulted for spontaneous complaints of hemorrhoids at the acute phase of the crisis. Itching, swelling and bleeding were also commonly reported (around 60% of individuals). The symptoms were consistently observed across all grades of Goligher classification, including among patients classified as less severe. Furthermore, a trend to an increase in the number and intensity of symptoms was noticed with higher grades. However, no strong correlation was observed between symptoms and Goligher grade, in line with the notion that this classification focuses on assessing the presence and severity of prolapse without considering the patient's symptomatology [23]. The presence of HD symptoms had a negative impact on quality of life in the study cohort, regardless of disease severity. This is consistent with previous findings, showing that health-specific quality of life measures and HD severity are poorly correlated, whereas higher HD symptom burden had a greater impact on quality of life [24]. This highlights the importance of including patient-reported measures in the evaluation of HD because objective data may not be a good indicator of the impact of disease on an individual. The impact of HD on quality of life and the associated large economic burden of the disease [25] emphasize the importance of effective treatment.
In terms of treatment for HD, the majority of participants in CHORALIS received, in addition to dietary and lifestyle recommendations, a combination of two or more treatments, mostly oral VAD-based, with or without topical therapies and/or laxatives and/or analgesics. MPFF-based treatment was the most frequently prescribed treatment across all grades of HD.
Oral VAD-based treatment was associated with a substantial decrease in symptoms, with almost half of the individuals treated reporting an absence of symptoms at visit 2. VAD-based treatment appeared to be particularly effective in managing pain, discomfort and bleeding. Overall, MPFF-based treatment appeared to be associated with a statistically significant higher benefit than diosmin-based treatment in promoting symptom resolution. The benefits of VADs in HD, including MPFF, diosmin, hydroxyethylrutosides and troxerutin have been reported in several systematic reviews [26–28]. One of these publications aggregated data from systematic reviews and meta-analyses and found that MPFF treatment could improve most of the symptoms of HD, including bleeding, discharge/leakage and/or itching [28]. In addition, combined data from 14 randomized clinical trials suggested that MPFF effectively reduced the recurrence of HD symptoms [28]. The current real-world data showed that 90.4% of individuals treated with MPFF-based therapy did not have bleeding at visit 2. This figure is higher than the proportion of participants (80.2%) who did not report any anal bleeding after 1 month of treatment with MPFF in a randomized controlled trial [29]. The aforementioned substantial body of high-level evidence from studies of robust design demonstrating the efficacy of MPFF treatment in alleviating symptoms and signs of HD, particularly bleeding, may help explain why MPFF seems to be the physician's treatment of choice for patients with HD, and consequently the most frequently prescribed VAD in the present study.
Improvements in symptoms, based on responses to the PGI-C scale, also suggested that VAD-based treatment is effective for individuals with HD. The proportion of patients reporting feeling “very much better” was significantly higher in the MPFF-based group compared with the diosmin-based treatment group. In addition, the time to improvement was significantly shorter in patients treated with a MPFF-based treatment. This difference between treatment groups was also reflected in patient and physician satisfaction with prescribed treatment, where the proportion of very satisfied patients was significantly higher with MPFF-based treatment than with diosmin-based treatment.
A key finding of the current study was an improvement in disease-specific quality of life during conservative treatment of HD. There was a reduction in the HEMO-FISS-QoL score from visit 0 to visit 2 (indicating a better quality of life) whatever the dimension in all treatment groups. A previous study has also shown improvement in quality of life in adults with HD treated with MPFF [30]. There was a significant improvement in physical, general health and total Short Form-12 scores 2 weeks after the addition of MPFF to conventional treatment (topical therapy/lifestyle modification) compared with conventional treatment alone; the bleeding rate was also significantly improved in the MPFF versus conventional therapy group [30].
The beneficial effect of MPFF observed could be attributed to its systemic effect on the pathogenesis of HD. Indeed, the mechanism of action of MPFF including beneficial effects on venous tone, inflammatory processes and microcirculatory permeability [31–33] may address the underlying causes of symptomatic hemorrhoids, such as diminished venous return and swelling that play prominent roles in HD.
Taken together, the results of the present study provide additional insights into the real-world outcomes of the conservative approach of using VADs, mostly MPFF, in the management of patients with acute HD in everyday clinical practice.
A number of limitations need to be considered when interpreting the study findings. These include those inherent to all studies with an observational design, such as the absence of randomization with respect to treatment assignment, sample bias, incomplete survey response data, the potential for inaccurate/incomplete self-reported data, as well as the potential role of possible concomitant treatments (fibers, laxatives, sitz baths, traditional medicines), which may have influenced the results. In addition, bias may arise from the selection of treating physicians in each participating country, and from the individuals who agreed to participate (who may differ from those choosing not to provide consent). Furthermore, therapeutic options and follow-up of patients may depend on treatment availability and specific characteristics of the individual health systems in participating countries, and the qualifications of the treating physician. Despite a lack of randomization/stratification, it was interesting that there did not appear to be any clinically meaningful differences between individuals who received the various treatments in this study that could explain the variation in clinical outcomes observed.
Another limitation was that a limited number of statistical comparisons were made, i.e., only between MPFF-based and diosmin-based treatments; this was because these compounds were the most frequently prescribed VADs. Further, the comparisons between MPFF and diosmin were not head-to-head randomized comparisons. While adjustments were made for country of enrolment and baseline characteristics (sex, age, ethnicity, body mass index, HD grade and intake of painkillers, laxatives, or topical agents) to improve inter-group comparability, there was no control for other variables such as dose and duration of therapy, etc., which may have led to bias. Therefore, the current findings should be considered hypothesis generating, and need to be confirmed in a randomized, controlled trial.
The strength of this real-world study lies in the collection of large-scale data obtained from about 3500 patients enrolled by practitioners from different continents with various specialties, including general practitioners and surgeons. Further, numerous countries typically underrepresented in HD clinical research were included, offering crucial insights into clinical practice, especially concerning conservative treatments. As such, the data collected were from a more heterogeneous patient population (that was likely to include patients with comorbidities) than could be expected from a randomized, controlled trial, bringing added value to the study. Another strength was the confirmation of disease by physician examination including digital exam and/or anoscopy. Unlike randomized, controlled trials which are conducted under controlled conditions, real-world studies collect data from real-world settings, including diverse patient populations, treatments and healthcare practices. This approach can offer valuable information for healthcare providers to better understand the practical implications of conservative treatments for hemorrhoids, optimize treatment strategies and ultimately improve patient outcomes.
To the best of our knowledge, this is the first prospective observational study of large scale that was designed with follow-up visits to assess the effectiveness of conservative treatments for acute HD that also assessed both patients' and physicians' perspectives. The end points focused on patient-reported outcomes evaluating the severity of HD symptoms, the impact on daily activities and satisfaction with treatment, collected directly from the patient without interpretation by a healthcare professional. In addition, physicians reported the observed clinical signs over the study as well as their satisfaction with the treatment prescribed.
Conclusion
In this prospective, large scale, real-world study conducted in patients with acute HD, treatment with conservative therapy mainly based on VADs was associated with improvements in the clinical signs and symptoms of the disease as well as in quality of life. This study provides additional evidence base of the clinical advantages associated with the utilization of VADs, mostly MPFF, for effectively managing acute hemorrhoidal disease. Further research is required to confirm these findings.
Summary points
•
Hemorrhoid disease is a common anorectal condition, but its prevalence is thought to be underestimated partly due to patients feeling embarrassed or uncomfortable discussing symptoms related to the condition with healthcare providers.
•
Data regarding the effectiveness of conservative treatments in patients with hemorrhoid disease from real-life settings are limited.
•
This prospective observational study was conducted in 9 countries to assess the effectiveness of conservative treatments on symptoms and quality of life in 3592 patients experiencing the symptomatic acute phase of hemorrhoid disease.
•
Study investigators confirmed the diagnosis and graded disease severity, with the majority of patients having grade I or II disease (72%) and almost 50% having a prior history of hemorrhoidal disease.
•
The most common symptoms were pain and discomfort (in 89% and 95% of individuals, respectively).
•
Hemorrhoidal disease had a mild-to-moderate impact on patient quality of life, with patients with more severe disease experiencing worse quality of life.
•
Most participants were prescribed venoactive drugs (VADs; 91%), of which the most common was micronized purified flavonoid fraction (MPFF; 74%). Lifestyle modifications and fiber intake were also common conservative therapeutic strategies recommended to patients.
•
VAD treatment resulted in improvements in symptoms and on quality of life in the majority of patients, with particular benefits observed in MPFF versus diosmin recipients.
Author contributions
All authors were involved in the study design. P Godeberge, Z Csiki, M Zakharash, EN Opot, YA Shelygin, TT Nguyen, A Amir, I Konaté, M Momoh and R Donglin enrolled patients in the study. J Chirol and V Blanc-Guillemaud performed the data analyses, and all authors had access to the data. All authors read and revised the drafts, and approved the final version. M Cheeseman and N Ryan wrote the outline and first draft of this manuscript, respectively, on behalf of Springer Healthcare.
Financial disclosure
The study and journal article processing charge were funded by Servier Global Medical and Patient Affairs. J Chirol and V Blanc-Guillemaud are employees of Servier. P Godeberge has received fees or grants from Laboratoire Servier; fees from Ethicon; and facilities from Norgine SAS and Mayoly Spindler. All authors received research fees associated with the study from Servier. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
This medical writing assistance was funded by Servier.
Ethical conduct of research
The protocol for this study followed the ethical guidelines of the Declaration of Helsinki. The study protocol received ethical approval in each country where participants were enrolled, and, when applicable, at each study center. All participants provided written informed consent.
Data sharing statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Lohsiriwat V. Hemorrhoids: from basic pathophysiology to clinical management. World J. Gastroenterol. 18(17), 2009–2017 (2012).
2.
Johanson JF, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology 98(2), 380–386 (1990).
3.
Tournu G, Abramowitz L, Couffignal C et al. Prevalence of anal symptoms in general practice: a prospective study. BMC Fam. Pract. 18(1), 78 (2017).
4.
Abramowitz L, Benabderrahmane M, Pospait D, Philip J, Laouenan C. The prevalence of proctological symptoms amongst patients who see general practitioners in France. Eur. J. Gen. Pract. 20(4), 301–306 (2014).
5.
Violán C, Foguet-Boreu Q, Hermosilla-Pérez E et al. Comparison of the information provided by electronic health records data and a population health survey to estimate prevalence of selected health conditions and multimorbidity. BMC Public Health. 13(1), 251 (2013).
6.
Asakura K, Nakano M, Omae K. Relationship between bidet toilet use and haemorrhoids and urogenital infections: a 3-year follow-up web survey. Epidemiol. Infect. 146(6), 763–770 (2018).
7.
Kibret AA, Oumer M, Moges AM. Prevalence and associated factors of hemorrhoids among adult patients visiting the surgical outpatient department in the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. PLOS ONE. 16(4), e0249736 (2021).
8.
Riss S, Weiser FA, Schwameis K et al. The prevalence of hemorrhoids in adults. Int. J. Colorectal Dis. 27(2), 215–220 (2012).
9.
Sheikh P, Régnier C, Goron F, Salmat G. The prevalence, characteristics and treatment of hemorrhoidal disease: results of an international web-based survey. J. Comp. Eff. Res. 9(17), 1219–1232 (2020).
•• A web-based large-scale survey conducted in Brazil, the Czech Republic, France, Hungary, Italy, Romania, Russia and Spain, describing the prevalence of hemorrhoid disease in adults (11%), and characteristics of patients with hemorrhoid disease.
10.
Sun Z, Migaly J. Review of hemorrhoid disease: presentation and management. Clin. Colon Rectal Surg. 29(1), 22–29 (2016).
11.
Morgado PJ, Suárez JA, Gómez LG, Morgado PJ Jr. Histoclinical basis for a new classification of hemorrhoidal disease. Dis. Colon Rectum 31(6), 474–480 (1988).
12.
Aigner F, Bodner G, Gruber H et al. The vascular nature of hemorrhoids. J. Gastrointest. Surg. 10(7), 1044–1050 (2006).
13.
Gallo G, Martellucci J, Sturiale A et al. Consensus statement of the Italian Society of Colorectal Surgery (SICCR): management and treatment of hemorrhoidal disease. Tech. Coloproctol. 24(2), 145–164 (2020).
14.
Singh G, Lingala V, Wang H et al. Use of health care resources and cost of care for adults with constipation. Clin. Gastroenterol. Hepatol. 5(9), 1053–1058 (2007).
15.
De Marco S, Tiso D. Lifestyle and risk factors in hemorrhoidal disease. Front. Surg. 8, 729166 (2021).
16.
Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the management of hemorrhoids. Dis. Colon Rectum 61(3), 284–292 (2018).
• American clinical practice guidelines for the diagnosis and treatment of hemorrhoid disease.
17.
Van Tol RR, Kleijnen J, Watson AJM et al. European Society of ColoProctology: guideline for haemorrhoidal disease. Colorectal Dis. 22(6), 650–662 (2020).
• European clinical practice guidelines for the diagnosis and treatment of hemorrhoid disease.
18.
Godeberge P, Sheikh P, Zagriadskiĭ E et al. Hemorrhoidal disease and chronic venous insufficiency: concomitance or coincidence; results of the CHORUS study (Chronic venous and HemORrhoidal diseases evalUation and Scientific research). J. Gastroenterol. Hepatol. 35(4), 577–585 (2020).
•• The international CHORUS study in 5617 patients with hemorrhoid disease provides information on symptom prevalence, risk factors, presence of concomitant chronic venous disease and common treatments.
19.
Abramowitz L, Bouchard D, Siproudhis L et al. Psychometric properties of a questionnaire (HEMO-FISS-QoL) to evaluate the burden associated with haemorrhoidal disease and anal fissures. Colorectal Dis. 21(1), 48–58 (2019).
20.
Goligher JC. Haemorrhoids or piles. In: Surgery of the anus, rectum and colon. Goligher JC (Ed.). Baillière Tindall London, UK (1980).
21.
Sanchez C, Chinn BT. Hemorrhoids. Clin. Colon Rectal Surg. 24(1), 5–13 (2011).
22.
Johanson JF, Sonnenberg A. Constipation is not a risk factor for hemorrhoids: a case-control study of potential etiological agents. Am. J. Gastroenterol. 89(11), 1981–1986 (1994).
23.
Dekker L, Han-Geurts IJM, Grossi U, Gallo G, Veldkamp R. Is the Goligher classification a valid tool in clinical practice and research for hemorrhoidal disease? Tech. Coloproctol. 26(5), 387–392 (2022).
24.
Rørvik HD, Davidsen M, Gierløff MC, Brandstrup B, Olaison G. Quality of life in patients with hemorrhoidal disease. Surg. Open Sci. 12, 22–28 (2023).
•• A valuable study that investigated in detail the impact of hemorrhoid disease on patient quality of life in 257 patients, comparing results with the general population.
25.
Yang JY, Peery AF, Lund JL, Pate V, Sandler RS. Burden and cost of outpatient hemorrhoids in the United States employer-insured population, 2014. Am. J. Gastroenterol. 114(5), 798–803 (2019).
26.
Godeberge P, Sheikh P, Lohsiriwat V, Jalife A, Shelygin Y. Micronized purified flavonoid fraction in the treatment of hemorrhoidal disease. J. Comp. Eff. Res. 10(10), 801–813 (2021).
27.
Sheikh P, Lohsiriwat V, Shelygin Y. Micronized purified flavonoid fraction in hemorrhoid disease: a systematic review and meta-analysis. Adv. Ther. 37(6), 2792–2812 (2020).
•• A systematic review of 11 studies, and meta-analysis of 4 studies, on MPFF showing significant improvements in symptoms (bleeding, discharge/leakage) and overall (according to patients and physicians).
28.
Lohsiriwat V, Sheikh P, Bandolon R et al. Recurrence rates and pharmacological treatment for hemorrhoidal disease: a systematic review. Adv. Ther. 40(1), 117–132 (2023).
•• This systematic review of the pharmacological management of hemorrhoidal disease included 44 publications, and summarized evidence regarding recurrence following surgical or pharmacological treatment, risk factors and the efficacy of conservative treatments.
29.
Corsale I, Carrieri P, Martellucci J et al. Flavonoid mixture (diosmin, troxerutin, rutin, hesperidin, quercetin) in the treatment of I-III degree hemorroidal disease: a double-blind multicenter prospective comparative study. Int. J. Colorectal Dis. 33(11), 1595–1600 (2018).
30.
Mokhtare M, Pakravan R, Rafieemanesh M et al. The efficacy of adding Daflon to the conventional treatment on the improvement of symptoms and health related quality of life in patients with acute hemorrhoids: a randomized clinical trial. EC Gastroenterol. Dig. Syst. 6, 44–51 (2019).
31.
Katsenis K. Micronized purified flavonoid fraction (MPFF): a review of its pharmacological effects, therapeutic efficacy and benefits in the management of chronic venous insufficiency. Curr. Vasc. Pharmacol. 3(1), 1–9 (2005).
32.
Bergan JJ, Schmid-Schönbein GW, Takase S. Therapeutic approach to chronic venous insufficiency and its complications: place of Daflon 500 mg. Angiology 52(Suppl. 1), S43–S47 (2001).
33.
Mansilha A, Sousa J. Pathophysiological mechanisms of chronic venous disease and implications for venoactive drug therapy. Int. J. Mol. Sci. 19(6), 1669 (2018).
Information & Authors
Information
Published In
Copyright
© 2024 Servier. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 25 April 2024
Accepted: 26 July 2024
Published online: 12 August 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
An international observational study assessing conservative management in hemorrhoidal disease: results of CHORALIS (aCute HemORrhoidal disease evALuation International Study). (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0070
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Lucija Brkic, Ivan Romic, Karmen Jericevic, Ante-Zvonimir Golem, Juraj Kolak, Branko Bogdanic, Are we missing out on free data? Utilizing Google Trends for establishing hemorrhoidal disease diurnality in Europe: Retrospective snapshot study, Current Problems in Surgery, 10.1016/j.cpsurg.2025.101967, 75, (101967), (2026).
- Michele Schiano di Visconte, Comparative efficacy of lidocaine- and nifedipine-based conservative therapies in acute hemorrhoidal disease: A retrospective cohort study, The Surgeon, 10.1016/j.surge.2025.06.002, 23, 6, (406-411), (2025).
- Nguyen Trung Tin, Tran Ngoc Dung, Nguyen Ngoc Anh, Nguyen Cong Long, Chung Hoang Phuong, Nguyen Thanh Binh, Ngo Minh Thu, The aCute HemORrhoidal disease evALuation International Study (CHORALIS): Subanalysis of the effectiveness of conservative treatment during the acute phase of hemorrhoidal disease in Vietnam, Journal of International Medical Research, 10.1177/03000605251397889, 53, 11, (2025).
- Wanliang Wang, Yong Yang, Lanlan Hou, Shuimei Wu, Comparative effectiveness and recurrence rates of endoscopic sclerotherapy, ligation, and combined therapy for grades I-III internal hemorrhoids, BMC Surgery, 10.1186/s12893-025-03289-7, 25, 1, (2025).
- Jean H. Ashburn, Hemorrhoidal Disease, JAMA, 10.1001/jama.2025.13083, 334, 17, (1541), (2025).