One-year budget impact of InTandem™: a novel neurorehabilitation system for individuals with chronic stroke walking impairment
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Chronic stroke walking impairment is associated with high healthcare resource utilization (HCRU) costs. InTandem™ is a neurorehabilitation system that autonomously delivers a rhythmic auditory stimulation (RAS)-based intervention for the at-home rehabilitation of walking impairment in adults in the chronic phase of stroke recovery. This study was conducted to estimate the budget impact of InTandem in comparison with currently available intervention strategies for improvement of gait/ambulation in individuals with chronic stroke walking impairment. Methods & materials: A budget impact analysis (BIA) for InTandem was conducted based on a 1-million-member US third-party payer perspective over a 1-year time horizon. Key inputs for the budget impact model were: costs for each intervention strategy (InTandem, physical therapy, self-directed walking and no treatment), HCRU costs for persons with chronic stroke and anticipated HCRU cost offsets due to improvements in gait/ambulatory status as measured by self-selected comfortable walking speed (based on functional ability). In addition to the reference case analysis, a sensitivity analysis was conducted. Results: Based on the reference case, introduction of InTandem was projected to result in overall cost savings of $439,954 in one year. Reduction of HCRU costs (-$2,411,778) resulting from improved walking speeds with InTandem offset an increase in intervention costs (+$1,971,824). Demonstrations of cost savings associated with InTandem were robust and were consistently evident in nearly all scenarios evaluated in the sensitivity analysis (e.g., with increased/decreased patient shares, increased HCRU cost or increased InTandem rental duration). Conclusion: The InTandem system is demonstrated to improve walking and ambulation in adults in the chronic phase of stroke recovery after a five-week intervention period. The BIA predicts that introduction of InTandem will be associated with overall cost savings to the payer.
Shareable abstract
This evidence-based budget impact analysis predicted that the new rhythmic auditory stimulation-based neurorehabilitation system, InTandem, will provide overall cost savings upon introduction for treatment of walking impairment in individuals in the chronic phase of stroke recovery.
Stroke is a leading cause of death and chronic disability in the US and around the world [1,2]. Chronic stroke is typically defined as the phase ≥6 months after the initial stroke event [3,4]; an estimated 45% of individuals with chronic stroke have walking impairments that prevent them from fully participating in the daily activities of their lives [5]. Reduced mobility is experienced by more than half of stroke survivors aged ≥65 years [1], and stroke-related balance and gait deficits can contribute to the risk of falls and fall-related fractures [6]. In addition, the ability to ambulate around one's community is critical to one's ability to socialize and take advantage of resources available to them. As such, community ambulation categories based on comfortable walking speed can be helpful for characterizing someone's ability to functionally ambulate in their community, and one threshold for a ‘full community ambulator’ classification among individuals with chronic stroke is a self-selected comfortable walking speed of ≥0.80 m/s [7]. Walking impairments are associated with a wide range of negative effects beyond direct mobility, including greater caregiver burden [8], reduced ability to return to work [9], lower quality of life (QoL) [8], reduced social participation [10] and increased healthcare resource utilization (HCRU)-associated costs [11,12].
There is a need for more effective and accessible rehabilitation options for individuals with chronic stroke walking impairment [13]. Rhythmic auditory stimulation (RAS) is a standardized clinical intervention [14] and is included in US clinical practice guidelines to improve walking in survivors of stroke [15,16]. RAS accesses and influences auditory-motor neural networks to create fast, temporally precise and stable synchronization [17] between an external rhythm and motor movements to help establish new neural connections within the brain's motor region, leading to improved walking speed [18]. Outpatient use of RAS has generally been limited due, in part, to the relatively small number of clinicians trained in administering RAS and the use of RAS typically occurring only in select clinical settings. This places a burden on community-dwelling patients and their caregivers, whose health, daily responsibilities and access to transportation may further hinder access [16]. Barriers to access to stroke rehabilitation therapy can be addressed with InTandem (MedRhythms, ME, USA), an RAS-based, at-home autonomous neurorehabilitation system designed to improve walking and ambulation in adults with chronic stroke.
InTandem uses two shoe-worn sensors and software preinstalled on a locked touchscreen device (the system control unit), together with a headset to deliver the auditory stimulation [19,20]. A session begins with walking at a self-selected comfortable pace (based on functional ability) while the sensors collect baseline gait data. After baseline, music is introduced at a tempo that matches the individual's starting cadence. The sensors then continuously transmit gait data that are interpreted by the InTandem software algorithm. The InTandem software uses the sensor data to make a clinical decision and adapt the time-shifted music and auditory cues in an individualized manner [19,20]. To ensure patient safety, real-time assessments of gait quality (temporal variability and asymmetry) are employed in the InTandem algorithm [19,20].
Several studies with InTandem were conducted prior to the development of the budget impact model and informed the model. For instance, two feasibility and proof-of-concept studies provided signal of clinical impact of InTandem on gait and walking speed for individuals with chronic stroke walking impairment [21,22]. A summative usability study suggested that individuals in the chronic phase of stroke recovery could safely and successfully use InTandem in the intended environment, the home [23]. And, a pivotal, randomized, controlled clinical trial evaluating the efficacy and safety of InTandem (NCT04121754) [19] in adults with chronic stroke walking impairment was conducted. In the pivotal trial, people with baseline walking speeds of ≥0.5 m/s to <0.8 m/s and observable gait asymmetry were randomized to either InTandem or supervised, self-directed overground walking (as active comparator intervention). Participants in each arm completed 3 sessions per week of 30 min of walking per session for 5 weeks [19]. Individuals receiving InTandem experienced significantly greater improvement in comfortable walking speed (as assessed via the 10-meter walk test) versus the active comparator arm (mean change, +0.14 ± 0.03 m/s vs +0.06 ± 0.02 m/s, respectively; p = 0.013) [19]. Moreover, the proportion of individuals in the InTandem group who increased their walking speed beyond the established minimum clinically important difference of 0.16 m/s [24] and who had a post-intervention walking speed of ≥0.8 m/s was more than triple that observed in the active comparator arm (35.0% vs 9.4%; p = 0.01), suggesting that more participants who used InTandem showed clinically meaningful improvement in speed and could be classified as full community ambulators [19]. InTandem was also demonstrated to be a safe intervention, with adverse event rates comparable between InTandem and the active comparator arm [19]. The availability of InTandem for at-home gait rehabilitation has the potential to address efficacy and access needs that currently limit recovery of adults with chronic stroke walking impairment.
A budget impact analysis (BIA) is an important part of a comprehensive economic evaluation that can provide guidance for healthcare plan budgeting and help estimate the economic impact associated with the adoption of and reimbursement for a new product or technology. To our knowledge, a BIA for a walking impairment intervention in individuals six or more months after a stroke has not yet been published. This BIA was conducted to estimate the 1-year budget impact of InTandem use in comparison with current intervention strategies (physical therapy, self-directed walking and no treatment) for improvement of gait and ambulation in individuals with chronic stroke walking impairment.
Methods
A budget impact model (BIM) was developed using Microsoft Excel® and the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) best practice guidelines [25]. The BIA incorporated intervention-related costs as well as estimated HCRU costs expected to result from changes in treatment practice patterns, using a 1-year time horizon and a 1-million-member US public payer perspective. A 1-year time horizon was selected for the reference case because it most accurately reflected the immediate value and cost offsets associated with the adoption of InTandem. Additional variables (e.g., chronic stroke incidence, prevalence and mean annual healthcare costs; HCRU cost reduction associated with increased walking speed; intervention strategies; patient shares; reimbursement amounts) are detailed in Table 1.
| General parameters | Value | |||
|---|---|---|---|---|
| Time horizon | 1 year | |||
| Payer plan size, n | 1,000,000 | |||
| Annual incidence of chronic stroke in the US | 0.2%† | |||
| Prevalence of chronic stroke in the US | 3.2%‡ | |||
| Mean annual healthcare costs for patients with chronic stroke | $11,214.66§ | |||
| Patients with chronic stroke walking impairment | 50.0%¶ | |||
| HCRU cost reduction for every 0.10-m/s walking speed increase | $2026.89# | |||
| Intervention strategy-specific parameters | InTandem | No treatment | Self-directed walking | Physical therapy |
| Patient shares: current scenario (without InTandem)†† | 0% | 56% | 8% | 36% |
| Patient shares: future scenario (with InTandem)†† | 5% | 51% | 8% | 36% |
| Intervention strategy cost | $1450.00†† (per 5-wk rental) | $0.00 | $0.00 | $75.00‡‡ (per 30-min session) |
| Intervention strategy frequency (per year) | 2 1-month rental periods | N/A | 15 sessions§§ | 24 sessions¶¶ |
| Reimbursement code | N/A | N/A | N/A | 97110## |
| Patient co-pay | 20%††† | N/A | N/A | 22%‡‡‡ |
| Reimbursement amount | $1160.00§§§ | N/A | N/A | $58.18# |
| Walking speed increase | 0.14 m/s§§ | 0.00 m/s | 0.06 m/s§§ | 0.07 m/s¶¶¶ |
| Patients converted to full community ambulators | 47.5%§§ | 0.00% | 25.0%§§ | 25.0%### |
| Reimbursement amount | $1160.00§§§ | N/A | N/A | $58.18## |
†
‡
All prevalent patients were assumed eligible in year 1 [28].
§
Based on Yousufuddin et al. (study reporting 3-year HCRU costs for survivors of stroke [excluding the index hospitalization cost]) [29].
¶
Based on Faria-Fortini et al. (study of adults with chronic stroke) [5].
#
Based on Purser et al. (study of elderly male veterans) [12].
††
Assumption based on MedRhythms data on file [30].
‡‡
Conservative estimate based on multiple online sources [31–34].
§§
Based on data from the MedRhythms pivotal trial [19].
##
Conservative assumption based on data from Centers for Medicare and Medicaid Services [37].
†††
Estimated based on anticipated coverage by a US public payer [38].
‡‡‡
Calculated percentage equal to the remaining cost after the reimbursement amount (associated with 97110) is deducted from the intervention strategy cost.
§§§
Calculated remaining cost after the patient co-pay is deducted from the intervention strategy cost.
¶¶¶
Sourced from States et al. (review reporting outcomes of overground walking training for patients with chronic stroke) [39].
###
Assumed equivalent to self-directed walking.
HCRU: Healthcare resource utilization; min: Minute; n: Number of patients; N/A: Not applicable; wk: Week.
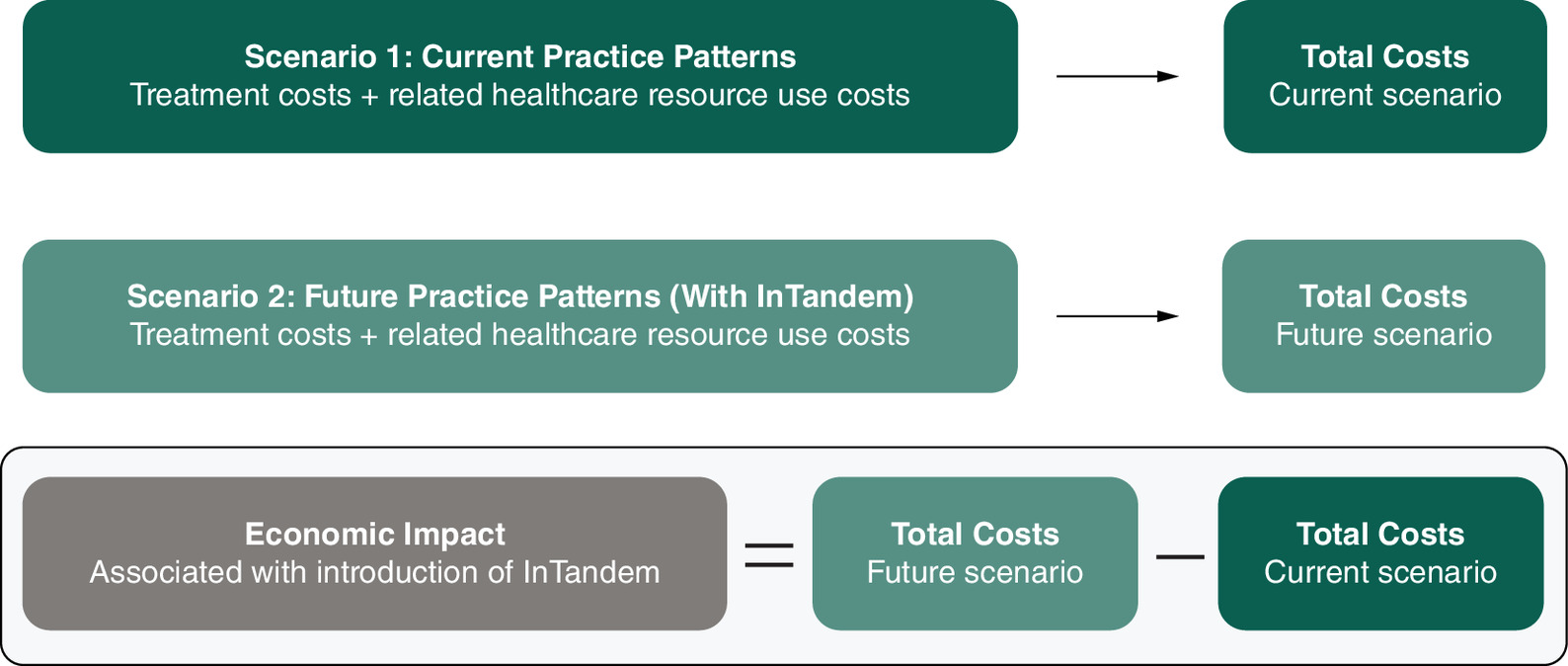
The BIM was used to calculate economic outcomes in current (without InTandem) and future (with InTandem) scenarios (Figure 1). The incremental costs, defined as the difference in overall costs between the current and future scenarios for the total plan, were calculated per member per month (PMPM) and per indicated member per month (PIMPM). The incremental PMPM and PIMPM costs were calculated by dividing the total plan budget impact results by the plan population size or indicated population size, respectively, and further dividing by 12 months. The incremental number of patients who were estimated to convert to community ambulators (end point walking speed ≥0.80 m/s) was also reported.
Population
The patient population included adults with chronic stroke walking impairment. Published US epidemiological estimates were used to determine the eligible (indicated) patient population; epidemiological inputs included the annual incidence of stroke, the stroke survival rate, the prevalence of stroke and the proportion of patients with chronic stroke walking impairment (Table 1) [5,12,26–29]. The annual incidence of stroke and the stroke mortality rate were used together to estimate the number of eligible incident patients (Table 1) [26,27]. Because a 1-year time horizon was selected for this analysis, all prevalent patients were assumed to be eligible for treatment in year 1. Additionally, it was assumed that the distribution of patients with stroke in the general population was equal to that covered by a payer plan.
Intervention strategies & patient shares
The following intervention strategies were considered in this analysis: InTandem, self-directed walking, physical therapy and no treatment. For the model, it was assumed that these intervention strategies were administered independently of one another and not at the same time. The ‘InTandem’ group was defined as patients treated solely with InTandem three-times per week (30 min per session) for 5 weeks, consistent with the design of the InTandem pivotal trial [19]. The ‘active comparator group’ in the pivotal trial was used as a proxy for a self-directed walking group with the same frequency and duration [19]. The ‘physical therapy’ group represented patients attending a total of 24 physical therapy sessions per year that were specifically related to walking rehabilitation (at an assumed 30 min per session), in alignment with clinical practice guidelines [16]. The ‘no treatment group’ represented patients with chronic stroke who continued their usual care and received no treatment for walking impairment. The model included 2 InTandem rental periods of 1-month each, equaling a total rental duration of 2 months.
The percentage of patients expected to be treated with a given intervention strategy (i.e., patient shares) in the current and future scenarios was based on conservative forecasting assumptions (Table 1) [30]. It was assumed that many patients in the chronic phase of stroke recovery did not receive treatment for walking [13]. In the future scenario, patient shares for the InTandem group were conservatively assumed to be 5% and taken from only the no treatment group (Table 1) [30].
Intervention strategy costs & reimbursement amounts
The cost of InTandem in the model was $1450.00 per 5-week rental, based on an estimated wholesale acquisition cost [30]. The cost of physical therapy was conservatively estimated at $75.00 per 30-minute session; the typical range without insurance is $75 to $150 per 30- to 90-minute session (Table 1) [31–34]. The self-directed walking and no treatment intervention strategies were assumed to have no associated cost to patients or payers. The reimbursement amount for InTandem was estimated assuming a 20% patient co-pay, emulating anticipated coverage by a US public payer [38]. The reimbursement amount for physical therapy was based on code 97110 (therapeutic exercises to develop strength and endurance, range of motion and flexibility) per the Medicare fee schedule [37]. Code 97110 was selected because it is commonly used for physical therapy sessions and therefore relevant for real-world applicability (Table 1) [30]. It is also associated with the same reimbursement amount as some of the other relevant codes (e.g., 97116 [gait training including stair climbing]).
Efficacy
Efficacy values used to calculate patient outcomes and costs are presented in Table 1. Improvements in walking speed for the InTandem and self-directed walking groups were defined as 0.14 and 0.06 m/s, respectively, and derived from the walking speed improvements observed across the InTandem and active comparator groups in the pivotal trial [19]. The improvement in walking speed for physical therapy was defined as 0.07 m/s, based on a systematic review reporting outcomes of gait training for patients with chronic stroke [39]. Patients in the no treatment group were assumed to have no change in walking speed [12,40].
For the percentage of patients that converted to full community ambulators, the inputs for InTandem and self-directed walking were also based on the InTandem pivotal study results [19], and the value for physical therapy was assumed to be equivalent to the self-directed walking percentage as a simplifying assumption (Table 1). It was also assumed that conversion to full community ambulator status would not occur for patients in the no treatment group, but that no declines in walking speed would occur with no treatment, both of which were conservative assumptions. Additional simplifying assumptions included that patients treated with InTandem, physical therapy, or self-directed walking complied fully with their treatment regimens (i.e., had an adherence rate of 100%) and that no included patient died across the 1-year time horizon.
Healthcare resource utilization costs
To derive the HCRU cost reduction from improvement in walking speed, it was estimated that every 0.10-m/s increase in walking speed would result in a HCRU cost reduction of $2026.89 [12]. The aggregate mean annual HCRU costs excluded the index hospitalization cost to avoid inclusion of costs associated with acute stroke management. Inputs were sourced from a US-based study reporting 3-year HCRU costs for adult survivors of stroke and included costs associated with home care, lost productivity and inpatient stroke rehabilitation (Table 1) [29]. Costs were inflated to 2023 US dollars using the US Medical Care Consumer Price Index [40].
Sensitivity analysis
A sensitivity analysis was performed to evaluate the impact of parameter uncertainties in the BIA, including incorporating recurrent stroke hospitalization costs and long-term care (LTC) costs, increasing or decreasing share of patients receiving InTandem with a corresponding change in patient shares for no treatment, increasing the aggregate HCRU costs to include the cost of index hospitalization [29], increasing the InTandem patient co-pay from 20 to 50%, increasing the combination of InTandem rental duration (from 2 to 3 months) and associated efficacy (i.e., increasing walking speed), varying the change in HCRU reduction by ±20% per 0.10-m/s increase in walking speed and varying the percentage of patients with chronic stroke walking impairment by ±20%. The model inputs used in the sensitivity analysis are listed in Supplementary Table 1. Additional methodologic details for the recurrent stroke hospitalization cost and LTC cost-related sensitivity analysis are provided in Supplementary Table 2.
Results
Reference case analysis
Over the 1-year time horizon, for an estimated eligible patient population of 16,998 in the 1-million-member plan, the future scenario with InTandem was associated with an estimated total cost savings of $439,954, which included HCRU cost savings of $2,411,778 (Table 2). A rise in intervention costs in the future scenario was offset by a greater reduction in HCRU costs. The total projected annual HCRU cost per patient was lowest for InTandem ($8377) relative to that for the comparator intervention strategies, which ranged from $9796 to $11,215 (Table 3). Compared with the current scenario without InTandem, more patients in the future scenario with InTandem were expected to improve ambulation status to full community ambulators (Supplementary Tables 1 & 2). Introduction of InTandem was associated with total incremental cost savings of $0.04 PMPM and $2.16 PIMPM (Table 2).
| Outcomes | Current scenario (without InTandem) | Future scenario (with InTandem) | Incremental | |
|---|---|---|---|---|
| Patients | Total patients with chronic stroke walking impairment, n | 16,998 | 16,998 | 0 |
| Treated with InTandem, % | 0 | 5 | 5 | |
| Treated with InTandem, n | 0 | 850 | 850 | |
| Total costs for cohort | Intervention strategy costs to payer | $8,544,716 | $10,516,540 | $1,971,824 |
| HCRU costs | $180,295,978 | $177,884,200 | -$2,411,778 | |
| Total budget impact to payers | $188,840,694 | $188,400,739 | -$439,954 | |
| Costs PMPM | Intervention strategy costs to payer | $0.71 | $0.88 | $0.16 |
| HCRU costs | $15.02 | $14.82 | -$0.20 | |
| Total | $15.74 | $15.70 | -$0.04 | |
| Costs PIMPM | Intervention strategy costs to payer | $41.89 | $51.56 | $9.67 |
| HCRU costs | $883.88 | $872.06 | -$11.82 | |
| Total | $925.77 | $923.62 | -$2.16 |
HCRU: Healthcare resource utilization; n: Number of patient; PIMPM: Per indicated member per month; PMPM: Per member per month.
| Outcome | InTandem | No treatment | Self-directed walking | Physical therapy |
|---|---|---|---|---|
| Total intervention strategy costs per patient | $2320.00 | $ 0.00 | $ 0.00 | $1396.32 |
| Total HCRU cost per patient† | $8377.02 | $11,214.66 | $9998.53 | $9795.84 |
†
Total HCRU cost per patient includes the annual healthcare resource utilization cost to treat patients with chronic stroke minus the reduction in the annual healthcare resource utilization cost associated with an increase in walking speed.
HCRU: Healthcare resource utilization.
Sensitivity analysis
Results of the sensitivity analysis are summarized in Table 4. The inclusion of both recurrent stroke hospitalization costs and LTC costs was associated with the largest change from the reference case, with cost savings of $1,409,048. All scenarios except 1 demonstrated cost savings to payers regardless of how the specific parameters were modified in the analysis. The only scenario in which a cost savings to payers was lost relative to the reference case was when the value for HCRU cost reduction associated with improved walking speed was reduced by 20% relative to the reference case. Relative to the model reference case, cost savings were consistently observed with an increase in InTandem co-pay, HCRU cost reduction and InTandem rental duration resulting in additional improvement in walking speed were increased relative to the model reference case.
| Scenario | Intervention strategy costs† | HCRU costs† | Total costs† | PMPM | PIMPM |
|---|---|---|---|---|---|
| Reference case | $1,971,824 | -$2,411,778 | -$439,954 | -$0.04 | -$2.16 |
| Include recurrent stroke hospitalization costs and LTC costs | $1,971,824 | -$3,380,871 | -$1,409,048 | -$0.12 | -$6.91 |
| Increase InTandem patient co-pay | $1,232,390 | -$2,411,778 | -$1,179,388 | -$0.10 | -$5.78 |
| Increase HCRU reduction per 0.10-m/s increase in walking speed | $1,971,824 | -$2,894,143 | -$922,319 | -$0.08 | -$4.52 |
| Decrease HCRU reduction per 0.10-m/s increase in walking speed | $1,971,824 | -$1,929,425 | $42,399 | $0.00 | $0.21 |
| Increase patient shares for InTandem | $3,943,648 | -$4,823,556 | -$879,909 | -$0.07 | -$4.31 |
| Decrease patient shares for InTandem | $985,912 | -$1,205,889 | -$219,977 | -$0.02 | -$1.08 |
| Increase patients with chronic walking impairment | $2,760,554 | -$3,376,490 | -$615,936 | -$0.05 | -$2.16 |
| Decrease patients with chronic walking impairment | $1,183,094 | -$1,447,067 | -$263,973 | -$0.02 | -$2.16 |
| Increase HCRU cost | $1,971,824 | -$2,411,778 | -$439,954 | -$0.04 | -$2.16 |
| Increase InTandem rental duration and improvement in walking speed | $2,957,736 | -$3,100,858 | -$143,122 | -$0.01 | -$0.70 |
†
Costs to payer.
HCRU: Healthcare resource utilization; LTC: Long-term care; m/s: Meters per second; PIMPM: Per indicated member per month; PMPM: Per member per month.
Discussion
This BIA projected that, based on a 1-million-member US third-party payer perspective, a 5% InTandem patient share among adults with chronic stroke walking impairment would lead to a conservatively estimated cost savings of $439,954 over 1 year. This finding was supported by the sensitivity analysis that evaluated several alternate scenarios, such as recurrent stroke hospitalization and LTC costs, increased InTandem co-pay, increased duration of InTandem rental and increased HCRU costs. Payers may realize greater cost savings with real-world use of InTandem than is reflected in this budget impact estimate, because the selected model inputs and assumptions were conservative (see Limitations section), a short time horizon of 1 year was evaluated and the model did not include other indirect health benefits that may be expected from increased mobility, such as increased social engagement [41,42], quality of life [43] and fewer depressive symptoms [44].
The introduction of InTandem was associated with a projected reduction in HCRU costs of $2,411,778, resulting from gait/ambulation improvement, which offset the expected increase in intervention costs of $1,971,824. Further, despite having a higher intervention cost relative to the comparator intervention strategies, use of InTandem was associated with the lowest total HCRU cost per patient. The reduction in HCRU costs as a result of improved walking speed was expected, as this inverse relationship has been well documented [12,29,39].
Importantly, demonstrations of cost savings associated with InTandem were robust, with savings consistently evident across nearly all scenarios assessed in the sensitivity analysis. The model was sensitive to ±20% changes in HCRU in terms of cost reduction due to an increase in walking speed, representing a range of HCRU cost reductions that may be experienced due to increases in walking speed. A notably large difference was found in PIMPM costs between the +20% and -20% scenarios (-$4.52 vs $0.21, respectively). This was expected given that changes in walking speed of 0.10 m/s can result in large changes in HCRU costs (i.e., $2026.89 per 0.10 m/s) [12]. In contrast, the model was less sensitive to 20% changes in the number of indicated patients included (PIMPM was equivalent in +20% and -20% scenarios). This could be due to the fact that the model estimates were based on a fixed percentage of patients across treatment options included in the model, so that an increase or decrease in the number of patients indicated for treatment would affect all treatment options at the same rate as the reference case. Thus, these findings suggest that cost savings may possibly be observed in a similar fashion across payer plans of varying numbers of covered lives. Additionally, the scenario examining recurrent stroke hospitalization and LTC costs resulted in markedly greater cost savings to the payer than the reference case. In this scenario, it was assumed that risk of recurrent stroke would decrease equally for all intervention strategies except no treatment, given that the risk of recurrent stroke is inversely related to physical activity [45].
As noted previously, a conservative 5% InTandem patient share was assumed in the reference case, and real-world patient shares may be larger because of the unmet need and thus associated with greater cost savings. The sensitivity analysis examining the increasing or decreasing of InTandem patient shares led to respective increases or decreases in the estimated cost savings relative to the reference case, as expected; however, even reduction in InTandem patient shares from 5% to 2.5% demonstrated cost savings compared with a scenario without InTandem. Including the cost of index hospitalization in the HCRU costs did not change the incremental budget impact because increasing the total aggregate HCRU cost affected the current and future economic scenarios equally. Conversely, the scenario increasing the InTandem patient co-pay from 20% to 50% resulted in incremental cost savings of $1,179,388 to the payer because patients would bear more of the InTandem rental cost. A scenario examining a 3-month rental duration of InTandem (versus a 2-month duration in the reference case) with an assumed 30% increase in walking speed (0.14 to 0.18 m/s) was examined in anticipation of the potential for prolonged treatment to lead to additional efficacy gains. In practice, patients may realize greater improvements with longer durations of rehabilitation treatment.
Strengths of this preliminary BIA include following ISPOR BIA best practices [25] and the use of best available data sources to inform inputs, such as the InTandem pivotal study data [19] and other relevant peer-reviewed published studies. Furthermore, the eligible patient population was determined using published epidemiological data on stroke and chronic stroke walking impairment [5,26,28] and, as such, is highly representative of the patient population for whom InTandem would be indicated and would most benefit from this treatment. To our knowledge, this is the first BIA focused on an intervention strategy for chronic stroke walking impairment. It is notable that, with the introduction of the InTandem neurorehabilitation system, payers can expect cost savings at year 1, which was demonstrated consistently in the sensitivity analysis.
Limitations
As with all modeling studies, this BIA was limited by assumptions related to model inputs. The current model has inherent assumptions related to patient shares, treatment patterns and intervention adherence rates. To mitigate uncertainty related to patient share estimates, a conservative patient share of 5% (based on internal forecasting assumptions [30]) was used in the reference case with shares taken only from the no treatment group. Concurrent use of interventions (e.g., physical therapy + InTandem; physical therapy + self-directed walking) was not included in this BIA owing to a lack of available efficacy data and to align with inclusion criteria (and therefore, the associated efficacy data) from the InTandem pivotal study [19]. However, in a real-world setting, it is possible that some patients would receive interventions concurrently. Another consideration is that the model assumed no change in walking speed in the no treatment group; this was a conservative estimate because it is likely that some patients in this group would experience a decline in walking speed [46] with an associated increase in HCRU costs; thus, there could be even greater relative cost savings potential with the implementation of InTandem. Further, adherence rates for each of the active interventions in the current model were assumed to be 100%, which may not represent reality given that adherence to physical therapy and self-directed walking programs would likely be less than 100% and would negatively impact estimated clinical outcomes for those intervention strategies [47]. Lastly, although the sensitivity analysis included a scenario with increased InTandem co-pay to estimate budget impact, variability in reimbursement rates across different payers for InTandem, as well as other interventions, may affect the generalizability of the results of this BIA and cost savings in the real world.
In the sensitivity analysis examining recurrent stroke hospitalization and LTC costs, the inclusion of recurrent stroke hospitalization may have resulted in double-counting the overall HCRU costs, as the source publication for HCRU in the reference case [29] included hospitalizations but did not specify cause, and therefore, some recurrent stroke hospitalization costs may have been included. Additionally, although a higher risk of LTC admissions have been reported in slow versus fast walkers [48], LTC-related costs may not be applicable to all payer types [49], and thus inclusion of LTC costs in the sensitivity analysis may have overestimated payer cost savings. Nonetheless, multiple scenarios evaluated in the sensitivity analysis consistently demonstrated plausible additional cost savings to payers and additional benefits for patients receiving treatment with InTandem. The sensitivity analysis did not include scenarios exploring the potential impact of adherence rates, which is an important area for future investigation since, as noted above, real-world adherence rates are likely to be less than 100% and could impact clinical improvement. Budget impact of InTandem beyond 1 year is also a valuable topic for evaluation in future studies.
Potential economic benefits to patients and caregivers that may be associated with improvement in walking speed for patients with chronic stroke walking impairment and home-based rehabilitation (and elimination of the burden of clinic visits) were not included in this preliminary BIA (in either the reference case or sensitivity analysis), as the focus was on costs to payers. However, InTandem is anticipated to improve adherence to prescribed rehabilitation because it provides an accessible option for at-home rehabilitation training for patients with chronic stroke walking impairment [47]. Although beyond the scope of this BIA, future work may explore the effects of InTandem use on patient and caregiver QoL.
Conclusion
InTandem is a neurorehabilitation system that offers adults with chronic stroke walking impairment – a historically underserved population with limited rehabilitation options – an effective and safe at-home rehabilitation option [19,22]. This preliminary BIA employed a conservative approach to estimate the budget impact associated with the introduction of InTandem and found that the intervention costs associated with adoption of InTandem are offset by a reduction in HCRU cost, leading to overall cost savings for payers.
Summary points
•
Chronic stroke walking impairment prevents individuals from fully participating in activities of daily living and contributes to increased morbidity and decreased quality of life as well as increased healthcare resource utilization (HCRU).
•
There is a need for more effective and accessible rehabilitation options for individuals with chronic stroke walking impairment.
•
InTandem™ is a prescription neurorehabilitation system that uses rhythmic auditory stimulation that can be used in the home to improve walking and ambulation in adults with chronic stroke.
•
This budget impact analysis was conducted based on a 1-million-member, third-party payer perspective over a 1-year time horizon and employed a conservative approach.
•
Key inputs for the budget impact model included costs for InTandem and other currently available intervention strategies, HCRU costs for individuals with chronic stroke and anticipated HCRU cost offsets due to improvements in gait/ambulatory status.
•
A 5% patient share for InTandem was projected to result in cost savings of $439,954 in 1 year, with a substantial reduction of HCRU costs that exceeded the anticipated increase in intervention costs.
•
The total projected annual HCRU cost per patient was $8377 for InTandem and ranged from $9796 to $11,215 for comparator strategies (physical therapy, self-directed walking, or no treatment).
•
Projected cost savings due to introduction of InTandem were consistently evident across a variety of scenarios (e.g., including costs related to recurrent stroke hospitalization and long-term care, increasing InTandem co-pay, reducing HCRU input costs and decreasing patient shares, among others).
•
InTandem represents an accessible and cost-saving rehabilitation option for individuals with chronic stroke walking impairment.
Author contributions
KE Smayda, J Lavanture, H Roberts and B Heikens were responsible for study conception; M Bourque, N Jayawardena and S Kane were responsible for study design and data acquisition; KE Smayda, J Lavanture, M Bourque, N Jayawardena, S Kane, H Roberts and B Heikens were responsible for data analysis and/or interpretation and drafting and revision of the manuscript.
Financial disclosure
This study was funded by MedRhythms, Inc. (ME, USA). Eversana (Burlington, Canada) was contracted by MedRhythms to design and conduct the economic modeling analyses. MedRhythms and Eversana were involved in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication. Eversana was involved in the design and build of the economic model. KE Smayda, J Lavanture and B Heikens are employees of and hold equity in MedRhythms. M Bourque, N Jayawardena and S Kane are employees of Eversana. H Roberts was an independent contractor for MedRhythms. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with anyorganization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
Medical writing assistance was provided by Kulvinder (Katie) Singh for The Curry Rockefeller Group, LLC (Tarrytown, NY, USA), and was funded by MedRhythms (Portland, ME, USA).
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Centers for Disease Control and Prevention. Stroke facts (2023). https://www.cdc.gov/stroke/facts.htm (Accessed July 14, 2023).
2.
Xu J, Murphy SL, Kochanek KD, Arias E. Mortality in the United States, 2021. NCHS Data Brief., (456), 1–8 (2022).
3.
Bernhardt J, Hayward KS, Kwakkel G et al. Agreed definitions and a shared vision for new standards in stroke recovery research: The Stroke Recovery and Rehabilitation Roundtable taskforce. Int. J. Stroke 12(5), 444–450 (2017).
4.
Moore SA, Boyne P, Fulk G, Verheyden G, Fini NA. Walk the talk: current evidence for walking recovery after stroke, future pathways and a mission for research and clinical practice. Stroke 53(11), 3494–3505 (2022).
•• Provides a comprehensive overview of post-stroke walking recovery interventions and a proposed evidence-based model that integrates current knowledge, emerging innovations and approaches for implementation.
5.
Faria-Fortini I, Polese JC, Faria C, Teixeira-Salmela LF. Associations between walking speed and participation, according to walking status in individuals with chronic stroke. NeuroRehabilitation 45(3), 341–348 (2019).
6.
Ramnemark A, Nilsson M, Borssen B, Gustafson Y. Stroke, a major and increasing risk factor for femoral neck fracture. Stroke 31(7), 1572–1577 (2000).
7.
Middleton A, Fritz SL, Lusardi M. Walking speed: the functional vital sign. J. Aging Phys. Act. 23(2), 314–322 (2015).
• Summarizes updated testing protocols and evidence demonstrating the importance of walking speed, an indicator of current functional status and predicted health outcomes, in clinical decision-making.
8.
Cohen JT. Walking speed and economic outcomes for walking-impaired patients with multiple sclerosis. Expert Rev. Pharmacoecon. Outcomes Res. 10(5), 595–603 (2010).
9.
Jarvis HL, Brown SJ, Price M et al. Return to employment after stroke in young adults: how important is the speed and energy cost of walking? Stroke 50(11), 3198–3204 (2019).
10.
Avelino PR, Nascimento LR, Menezes KKP et al. Walking confidence and perceived locomotion ability explain participation after stroke: a cross-sectional experimental study. Acta Neurol. Scand. 146(5), 573–577 (2022).
11.
Dohl O, Halsteinli V, Askim T et al. Factors contributing to post-stroke health care utilization and costs, secondary results from the life after stroke (LAST) study. BMC Health Serv. Res. 20(1), 288 (2020).
12.
Purser JL, Weinberger M, Cohen HJ et al. Walking speed predicts health status and hospital costs for frail elderly male veterans. J. Rehabil. Res. Dev. 42(4), 535–546 (2005).
13.
Kim KT, Chang WK, Jung YS et al. Unmet needs for rehabilitative management in common health-related problems negatively impact the quality of life of community-dwelling stroke survivors. Front Neurol. 12, 758536 (2021).
14.
Wang L, Peng JL, Xiang W, Huang YJ, Chen AL. Effects of rhythmic auditory stimulation on motor function and balance ability in stroke: a systematic review and meta-analysis of clinical randomized controlled studies. Front Neurosci. 16, 1043575 (2022).
15.
Sall J, Eapen BC, Tran JE, Bowles AO, Bursaw A, Rodgers ME. The management of stroke rehabilitation: a synopsis of the 2019 U.S. Department of Veterans Affairs and U.S. Department of Defense clinical practice guideline. Ann. Intern. Med. 171(12), 916–924 (2019).
16.
Winstein CJ, Stein J, Arena R et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 47(6), e98–e169 (2016).
•• Highlights the need to prioritize comprehensive programs supporting sustained post-acute rehabilitation that balance cost considerations with impact on clinical outcomes and downstream medical morbidity.
17.
Damm L, Varoqui D, De Cock VC, Dalla Bella S, Bardy B. Why do we move to the beat? A multi-scale approach, from physical principles to brain dynamics. Neurosci. Biobehav. Rev. 112, 553–584 (2020).
• This comprehensive review describes the neurologic basis for rhythmic auditory stimulation and entrainment in gait rehabilitation.
18.
Yoo GE, Kim SJ. Rhythmic auditory cueing in motor rehabilitation for stroke patients: systematic review and meta-analysis. J. Music Ther. 53(2), 149–177 (2016).
19.
Awad LN, Jayaraman A, Nolan KJ et al. Efficacy and safety of using auditory-motor entrainment to improve walking after stroke: a multi-site randomized controlled trial of InTandem(TM). Nat Commun. 15(1), 1081 (2024).
•• Presents results of the pivotal clinical study of the rhythmic auditory stimulation-based neurorehabilitation system that is the subject of this budget impact analysis.
20.
MedRhythms. Technology: robust clinical algorithms paired with a seamless user experience (2023). https://medrhythms.com/technology/ (Accessed August 8, 2023).
21.
Collimore AN, Roto Cataldo AV, Aiello AJ et al. Autonomous control of music to retrain walking after stroke. Neurorehabil. Neural Repair. 37(5), 255–265 (2023).
22.
Hutchinson K, Sloutsky R, Collimore A et al. A music-based digital therapeutic: proof-of-concept automation of a progressive and individualized rhythm-based walking training program after stroke. Neurorehabil. Neural Repair. 34(11), 986–996 (2020).
23.
Smayda KE, Cooper SH, Leyden K, Ulaszek J, Ferko N, Dobrin A. Validating the safe and effective use of a neurorehabilitation system (InTandem) to improve walking in the chronic stroke population: usability study. JMIR Rehabil Assist Technol. 10, e50438 (2023).
24.
Tilson JK, Sullivan KJ, Cen SY et al. Meaningful gait speed improvement during the first 60 days poststroke: minimal clinically important difference. Phys. Ther. 90(2), 196–208 (2010).
25.
Sullivan SD, Mauskopf JA, Augustovski F et al. Budget impact analysis-principles of good practice: report of the ISPOR 2012 Budget Impact Analysis Good Practice II Task Force. Value Health 17(1), 5–14 (2014).
26.
Tsao CW, Aday AW, Almarzooq ZI et al. Heart Disease and stroke statistics-2022 update: a report from the American Heart Association. Circulation 145(8), e153–e639 (2022).
27.
National Institute of Child Health and Human Development. How many people are affected by/at risk for stroke? (2023). https://www.nichd.nih.gov/health/topics/stroke/conditioninfo (Accessed August 8, 2023).
28.
Ovbiagele B, Nguyen-Huynh MN. Stroke epidemiology: advancing our understanding of disease mechanism and therapy. Neurotherapeutics. 8(3), 319–329 (2011).
29.
Yousufuddin M, Moriarty JP, Lackore KA et al. Initial and subsequent 3-year cost after hospitalization for first acute ischemic stroke and intracerebral hemorrhage. J. Neurol. Sci. 419, 117181 (2020).
30.
MedRhythms. Data on file. MedRhythms, ME, USA (2023).
31.
InMotion OC. How much does physical therapy cost? An In-depth Guide, (2023). https://www.inmotionoc.com/how-much-does-physical-therapy-cost/#how-much-does-physical-therapy-cost-3 (Accessed August 8, 2023).
32.
Miracle Rehab Clinic. How much physical therapy costs without insurance in 2023 (2023). https://www.miraclerehabclinic.com/blog/physical-therapy-cost-without-insurance (Accessed August 8, 2023).
33.
OrthoBethesda. How much does physical therapy cost? (2023). https://www.orthobethesda.com/blog/how-much-does-physical-therapy-cost/ (Accessed August 8, 2023).
34.
Thervo. How much does physical therapy cost? (2023). https://thervo.com/costs/physical-therapy-cost (Accessed August 8, 2023).
35.
MacKay-Lyons M, Billinger SA, Eng JJ et al. Aerobic exercise recommendations to optimize best practices in care after stroke: AEROBICS 2019 update. Phys. Ther. 100(1), 149–156 (2020).
36.
Teasell R, Salbach NM, Foley N et al. Canadian stroke best practice recommendations: rehabilitation, recovery, and community participation following stroke. Part one: rehabilitation and recovery following stroke; 6th edition update 2019. Int. J. Stroke 15(7), 763–788 (2020).
37.
CMS.gov. Physician fee schedule (2023). https://www.cms.gov/medicare/medicare-fee-for-service-payment/physicianfeesched (Accessed August 8, 2023).
38.
Medicare.gov. Physical therapy services (2023). https://www.medicare.gov/coverage/physical-therapy-services (Accessed August 8, 2023).
39.
States RA, Pappas E, Salem Y. Overground physical therapy gait training for chronic stroke patients with mobility deficits. Cochrane Database Syst. Rev. 2009(3), CD006075 (2009).
40.
BLS.gov. CPI for all urban consumers (2023). https://data.bls.gov/cgi-bin/surveymost?cu (Accessed August 8, 2023).
41.
Grant G, Machaczek K, Pollard N, Allmark P. Walking, sustainability and health: findings from a study of a Walking for Health group. Health Soc Care Community 25(3), 1218–1226 (2017).
42.
Van Cauwenberg J, De Donder L, Clarys P et al. Relationships between the perceived neighborhood social environment and walking for transportation among older adults. Soc. Sci. Med. 104, 23–30 (2014).
43.
Montero-Odasso M, Schapira M, Soriano ER et al. Gait velocity as a single predictor of adverse events in healthy seniors aged 75 years and older. J. Gerontol. A Biol. Sci. Med. Sci. 60(10), 1304–1309 (2005).
44.
Robertson R, Robertson A, Jepson R, Maxwell M. Walking for depression or depressive symptoms: a systematic review and meta-analysis. Mental Health and Physical Activity 5(1), 66–75 (2012).
45.
Hou L, Li M, Wang J et al. Association between physical exercise and stroke recurrence among first-ever ischemic stroke survivors. Sci. Rep. 11(1), 13372 (2021).
46.
van de Port IG, Kwakkel G, van Wijk I, Lindeman E. Susceptibility to deterioration of mobility long-term after stroke: a prospective cohort study. Stroke 37(1), 167–171 (2006).
• Presents data on prevalence and predictors of mobility decline in individuals with chronic stroke and implications for quality of life and participation in activities of daily living.
47.
Tack C, Grodon J, Shorthouse F, Spahr N. “Physio anywhere”: digitally-enhanced outpatient care as a legacy of coronavirus 2020. Physiotherapy 110, A26–A28 (2021).
48.
Lyons JG, Ensrud KE, Schousboe JT et al. Slow gait speed and risk of long-term nursing home residence in older women, adjusting for competing risk of mortality: results from the study of osteoporotic fractures. J. Am. Geriatr. Soc. 64(12), 2522–2527 (2016).
49.
National Institute on Aging. Paying for long-term care (2023). https://www.nia.nih.gov/health/paying-long-term-care (Accessed August 8, 2023).
Information & Authors
Information
Published In
Copyright
© 2024 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 26 January 2024
Accepted: 13 August 2024
Published online: 3 September 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
One-year budget impact of InTandem™: a novel neurorehabilitation system for individuals with chronic stroke walking impairment. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0010
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Sabrina R. Taylor, Lou N. Awad, Cecilia A. Carlowicz, Yuri A. Maricich, Seth P. Finklestein, Erika H. Riley, Brian A. Harris, Ryan T. Pohlig, Francois A. Bethoux, Outcomes and Health Economics of Stroke using Rhythmic Auditory Stimulation (OrcHESTRAS): a protocol for a pragmatic, decentralized, longitudinal, multi-phase, withdrawal with randomized re-treatment trial of MR-001 in chronic stroke, Trials, 10.1186/s13063-025-09415-3, 27, 1, (2026).