Cost–effectiveness analysis of Avance® allograft for the treatment of peripheral nerve injuries in the USA
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Peripheral nerve injury (PNI) is a debilitating condition with significant associated morbidity, and which places a substantial socioeconomic burden on healthcare systems worldwide. Recently, allograft has emerged as a viable surgical alternative to autograft for the treatment of PNI. This study evaluated the cost effectiveness of allograft (Avance® Nerve Graft) compared with autograft for the peripheral nerve repair, from a US payer perspective. Methods: A Markov cohort model was developed to consider the treatment pathways followed by a patient population undergoing a single transected nerve repair with either allograft, or autograft. The marginal difference in meaningful recovery (MR) (effectiveness), and costs, between the two groups were estimated over a lifetime horizon. Deterministic and probabilistic sensitivity analyses (PSA) were performed to consider the uncertainty surrounding the base-case input parameter values and their effect on the overall incremental cost–effectiveness ratio (ICER). Results: The base-case analysis indicates that there is a small difference in the average probability of MR between the two groups (75.15% vs 70.46%; +4.69% with allograft). Allograft also results in cost savings ($12,677 vs $14,023; -$-1346 with allograft) compared with autograft. Deterministic sensitivity analysis shows that the costs of the initial surgical procedures are the main drivers of incremental cost, but that the intervention is likely to be cost saving compared with autograft regardless of the parameter variations made. Conclusion: The use of allograft with the Avance Nerve Graft has the potential to be a cost-effective alternative to autograft for the surgical treatment of PNI in the USA.
Plain language summary
What is this article about?
This article is about finding the cost-effective way to treat peripheral nerve injuries (PNI). It looks at whether using donated nerve tissue (allograft) is a good option compared with using a patient's own nerve tissue (autograft) for treating these injuries in the United States.
What were the results?
The study revealed that employing allograft may present a marginally superior option. A greater proportion of individuals who underwent allograft treatment achieved improved recovery outcomes, and it also demonstrated a modest reduction in associated costs. Moreover, even when various scenarios were considered, the utilization of donated nerve tissue consistently appeared to be a favorable choice.
What do the results of the study mean?
The results suggest that in the US, using allograft like the Avance Nerve Graft for nerve injuries could be both cost-effective and beneficial for recovery.
About half a million people in the USA have traumatic peripheral nerve injuries (PNIs) on an annual basis [1]. Irrespective of the severity of the PNI, it is a debilitating condition for the affected patient that results in pain, as well as loss of sensory and motor function [2]. Treatment of the PNI is dependent on whether the nerve has been stretched, compressed or cut, and may range from non-invasive methods, including rest, physical therapy and medication, to surgical techniques for patients in whom the injury is not healing correctly [3]. Although peripheral nerve repair is not a life-saving surgery, it has been shown to be an effective intervention, with significant benefits for patient quality-of-life (QoL) [4]. Additionally, since most patients with PNIs can be categorized in the working-age population, peripheral nerve repair has substantial economic and societal benefits [5].
Effective surgical repair of a transected nerve requires tension-free coaptation of healthy nerve tissue. End-to-end repair is common, though tension free technique is not always possible [6]. When primary nerve repair cannot be performed without undue tension, surgeons use available bridging materials including nerve autografts, conduits or processed nerve allografts [7,8]. Surgeons typically use autologous nerve grafts taken from the patient's own body to bridge nerve gaps, which is a well-established method to manage nerve gap injuries [9]. However, tissue availability is limited and requires a healthy, functional nerve to be sacrificed in order to repair the damaged nerve. Moreover, nerve autografts require an additional surgical procedure to be performed, which increases costs and anesthesia time, as well as being associated with surgical and healing complications (e.g., scarring, pain, and neuromas) [2,10]. Ducic et al. showed that the probability of post-repair complications with autograft at the donor site is high; chronic pain (22.30%), infection (28.60%), and neuroma (20.00%) [11]. These complications are likely associated with additional costs, however no cost analysis for post-nerve repair complications has been performed to date.
To overcome the issue of donor site complications, artificial nerve graft conduits; hollow tubes made from various biological or synthetic materials, may be utilized [12]. However, the majority of the marketed and FDA-approved artificial nerve conduits are limited to a gap length of 3.00 cm, and are associated with highly variable and inconsistent outcomes [13].
In recent years, processed cadaveric nerve allografts (PNAs) have been increasingly used as a viable option in clinical practice, with promising results in nerve gaps up to 70 mm [14,15]. The only available decellularized allograft on the market is the Avance® Nerve Graft (Axogen, Inc., Alachua, FL, USA), which is pre-degenerated, sterilized extracellular matrix (ECM) processed from donated human peripheral nerve tissue that serves as a scaffold for nerve regeneration [7]. Decellularized allograft provides flexible, pliable, ECM that maintains the structure and laminin of the native nerve, allows for revascularization, and remodels into the patient's own tissue while supporting axonal growth across the nerve discontinuity [16].
A number of clinical studies have demonstrated the efficacy of the use of allograft to repair nerve gap injuries. The most recent, by Safa et al. [13], analyzed data from a multi-center observational registry (RANGER®), which is the largest peripheral nerve registry, including data on over 1600 nerve repairs. The analyses showed that overall, 82% meaningful recovery (MR) was achieved across sensory, mixed and motor nerve repairs up to gaps of 70 mm. Comparable MR results were reported in the literature for allograft versus autograft nerve repairs (nine allograft studies with 711 nerve repairs vs 21 autograft studies with 670 nerve repairs) in the study Lans et al. [17].
Despite available clinical evidence, the published literature on healthcare costs associated with allograft and autograft procedures is limited. Styron et al. assessed nerve graft procedure costs, comparing allograft and autograft in a Medicare population. This analysis found similar costs for allograft versus autograft repair in an outpatient setting ($13,143 and $12,635, respectively), and lower total costs of care for allograft versus autograft repair in the inpatient setting ($25,751 and $29,560 respectively) [18]. These findings were supported by an analysis by Foster et al. [19], and a recent cost analysis performed in a claim database analysis by Raizman et al. [20]. Despite the available procedure cost evidence, there remains gaps in the literature related to the long-term costs and effects of using allograft and autograft in the PNI patient population.
In this study, we present a decision-analytic model developed to estimate the cost effectiveness of allograft (Avance Nerve Graft) compared with autograft in patients who are candidates for nerve reconstruction for the management of PNIs in the USA.
Methods
A Markov cohort model was developed to estimate the costs and clinical outcomes associated with allograft and autograft, respectively in repairing a single transected nerve. Effectiveness data from previously published systematic reviews were used to populate the model [21]. Total costs and clinical outcomes were assessed over a lifetime horizon (3-month time cycle), with a discount rate at rate of 3.0% applied [22].
Study setting & patient population
The analysis was performed from a US healthcare payer perspective. The model population consisted of patients with PNIs – severe axonotmesis and neurotmesis injuries - who required nerve grafting up to 70 mm. The age at onset of treatment was 42 years, in accordance with mean data derived from a large multicenter review of cases of PNIs performed by Safa et al. [13]. Based on the US Premier claims analysis by Raizman et al., the model was populated with a 60.11% proportion of male patients and the single nerve repairs which account for 83% of all graft repairs [20].
Model structure
Each patient who enters the model has the possibility of receiving allograft or autograft for the treatment of PNI, as well as receiving the additional care associated with each type of procedure. Following initial nerve repair surgery (NRS), patients move into the ‘regrowth period’ health state for a period of 18 months (based on expert clinical input) while they are still experiencing the symptoms of their initial nerve injury. At the end of this 18-month period in the ‘regrowth’ health state (6 cycles of 3 months each), patients either progress to a ‘successful’ or ‘unsuccessful’ health state, based on the success of the initial procedure. Those patients transitioning to the ‘successful’ heath state are assumed to experience improved QoL following a recovery in sensory and motor nerve functioning. Of the patients who do not experience sufficient improvement in nerve functionality to have had a successful recovery, a proportion are candidates to undergo secondary NRS due to technical failure of the initial procedure. These patients re-enter the ‘NRS’ health state, while the remaining patients who had an unsuccessful recovery transition to the ‘unsuccessful’ health state.
In the base-case analysis, the model assumes that ‘Unsuccessful’ patients who undergo a second surgical treatment following initial nerve grafting in both treatment arms will undergo allograft in the second round of NRS, as when the initial treatment is autograft there is no possibility of undergoing further NRS with autograft surgery as it may be unlikely to have an additional donor site from which to prepare the graft. However, the model also assesses the results of a scenario in which surgeons decided to use autograft in case of an unsuccessful initial allograft procedure. In this scenario, patients with unsuccessful primary grafts suffered from both repair and donor site complications.
For patients undergoing a second surgical treatment in either arm of the analysis, all unsuccessful secondary NRS patients proceed to the ‘unsuccessful’ health state after a second 18-month period in the ‘regrowth period’ health state and remain in that health state for the duration of the model. Alternatively, patients who undergo a successful secondary NRS proceed to the ‘Successful’ health state following the regrowth period.
Patients in the ‘Successful’ heath state experience better sensory and motor function, which may lead to an improvement in QoL, compared with those patients in the ‘NRS’, ‘regrowth’, or ‘unsuccessful’ health states, however their functionality would still not be at the level experienced among the general population. This is due to partially recovered nerve functionality, compared with full functionality with the healthy original nerve. A proportion of patients in both the ‘successful’ and ‘unsuccessful’ health states may suffer from long-term complications associated with nerve repair. In addition to the post-surgical complications that may be experienced in either treatment arm, patients undergoing an autologous nerve grafting procedure (autograft) may also suffer from procedure-related complications at the donor site; these complications will impact the costs and health outcomes incurred by individual patients. In each model cycle, there is a possibility of death due to age-specific background mortality; these rates are included in the model. Supplementary Figure 1 presents the patient pathway and the economic model structure.
Clinical inputs
The probability of achieving MR following NRS in the allograft and autograft arms of the analysis was based on a network meta-analysis [17]. This review of nine allograft nerve graft studies with 711 nerve repairs versus 21 autograft studies with 670 nerve repairs, showed MR rates of 81.9% for allograft sensory nerve repairs versus 71.8% for autograft, and 58.3% for allograft motor nerve repairs versus 56% for autograft. The probabilities of experiencing post-nerve repair complications at the repair site were considered in each arm of the analysis. The modeled complications included neuroma, infection and pain. Estimates were obtained from the studies by Ducic et al., and Safa et al., respectively [11,13]. Ducic et al. looked at post-surgical complications among 478 nerve repair surgeries [11], while Safa et al. reported results from a large, peripheral nerve registry study [13]. Complications rates were assumed to be identical for both approaches (allograft and autograft), with the following values included: 0.96% for neuroma, 1.06% infection and 0.14% for pain.
The post-operative complications at the donor site in the autograft arm of the model included chronic pain, infection and neuroma. These probabilities were based on data from Ducic et al., and an analysis by Martin et al. [11,23], and were estimated as follows: 22.90% for chronic pain, 01.40% for infection and 20.00% for neuroma.
Among patients who had an unsuccessful initial surgery, the probability of undergoing revision in the allograft arm of the analysis was estimated to be 6.32% (due to technical failure of the initial procedure), based on data from the study by Safa et al. [13]. In the base-case analysis, due to insufficient evidence to inform revision rates with autograft, it was assumed that the probability of undergoing revision was the same in the autograft arm of the analysis.
Costs
A weighted average of direct medical repair procedure costs in outpatient and inpatient settings of care were estimated for both allograft ($10,961) and autograft ($10,772), from the US healthcare payer perspective, based on a recent claim database analysis (Supplementary Table 2) [20]. This was a retrospective observational study utilizing the Premier Healthcare Database (PHD), and was conducted to describe the demographics, hospital characteristics, healthcare resource utilization and costs among patients undergoing nerve graft repair surgery (allograft or autograft). All data included in the analysis were statistically de-identified and compliant with the Health Insurance Portability and Accountability Act [24]. Surgery costs for allograft were based on Current Procedural Terminology (CPT) code 64912 ($910), and an average facility value of physician fee schedule, based on CPT codes 64885, 64886, 64890–64893, 64895–64898 ($1247) [25].
Costs of complications at the repair site were assumed to be identical for both allograft and autograft procedures. These included the costs of neuroma, infection and short-term pain after surgery. The cost of neuroma ($2205) was estimated based on the 2022 Medicare rates for CPT codes for neuroma excision (64774, 64776, 64782, 64784 [average = $587]), implantation of nerve end into bone or muscle (64,787 [$284]), and the weighted average of level 1 and 2 nerve procedures in hospital-based outpatient departments (10%) and ambulatory surgery centers (90%), using CPT codes 25922, 64774, 64776, 64782, 64784, 64786, 64788, 64790, 64792 (average = $1334) [25]. The cost of pain management after surgery ($408) was based on data from a study by Guest et al. [26], performed in the UK setting. The cost of management of infection ($378) was estimated based on resource use data from Martin-Broekman et al. [23], including one GP visit ($171) [27], wound care appliance ($83) [26], anti-infectives ($43) [26], and topical treatments ($17) [26]. Costs derived from studies performed in the UK were inflated to a 2022 price year, and were then converted to US dollars using a purchasing power parity conversion rate of 1.443 in 2021 [28].
For post-surgical long-term complications at the donor site in the case of autograft, pain management costs were estimated based on a range of medical services used for long-term pain management as reported by the Washington Nerve Institute, based on a retrospective survey of 767 patients (Supplementary Table 3) [29]. These data were used as the source of resources for non-medication chronic pain management. To obtain the resource use associated with different types of medication (opioids and nonopioids), data from Gore et al. were utilized, which reported both prescription and over-the-counter medication use for painful diabetic peripheral neuropathy [30]. According to Gore et al., among those who used at least one prescription medicine, 54% and 100% of patients used any opioids, and other analgesic medications, respectively [30]. Based on clinical expert input, monthly unit costs for opioids were based on one monthly morphine equivalent does of 30 mg. For other analgesics, a weighted average of two paracetamol 500 mg ($0.27 for 61.88%), one naproxen 500 mg ($0.55 for 18.81%), one ibuprofen 800 mg ($0.44 for 36.14%) every six hours per day each, one gabapentin 300 mg ($0.96 for 23.91%), and two pregabalin 75 mg ($0.01 for 10.25%), was applied. The weights were obtained from Gore et al. [30], and the unit costs for medications were obtained from the 2022 Medicare rates [31]. Regarding other medical services for chronic pain management, the unit costs were based on various 2022 CPT codes rates [25]. These estimates were supported by clinical expert input. A complete overview of all cost parameters included in the economic model is presented in Supplementary Table 3.
Base-case analysis
Due to insufficient evidence on QoL among this patient population, disease-specific outcomes measures were assessed as the measure of effectiveness in this economic analysis. The primary health outcome measure in the model was the probability of experiencing MR. It reflects the restoration of motor and/or sensory functions lost due to PNI after nerve reconstruction surgery and is highly correlated with patient QoL [6]. Combined with the costs associated with the respective strategies, the model estimated the incremental cost–effectiveness ratio (ICER) of the intervention, i.e., cost per percentage of MR gained. The MR rates were based on the medical research council classification (MRCC) scale for sensory and motor functions [21]. Meaningful functional recovery was defined as being S3–S4 on the sensory scale, or M3–M5 on the motor function scale.
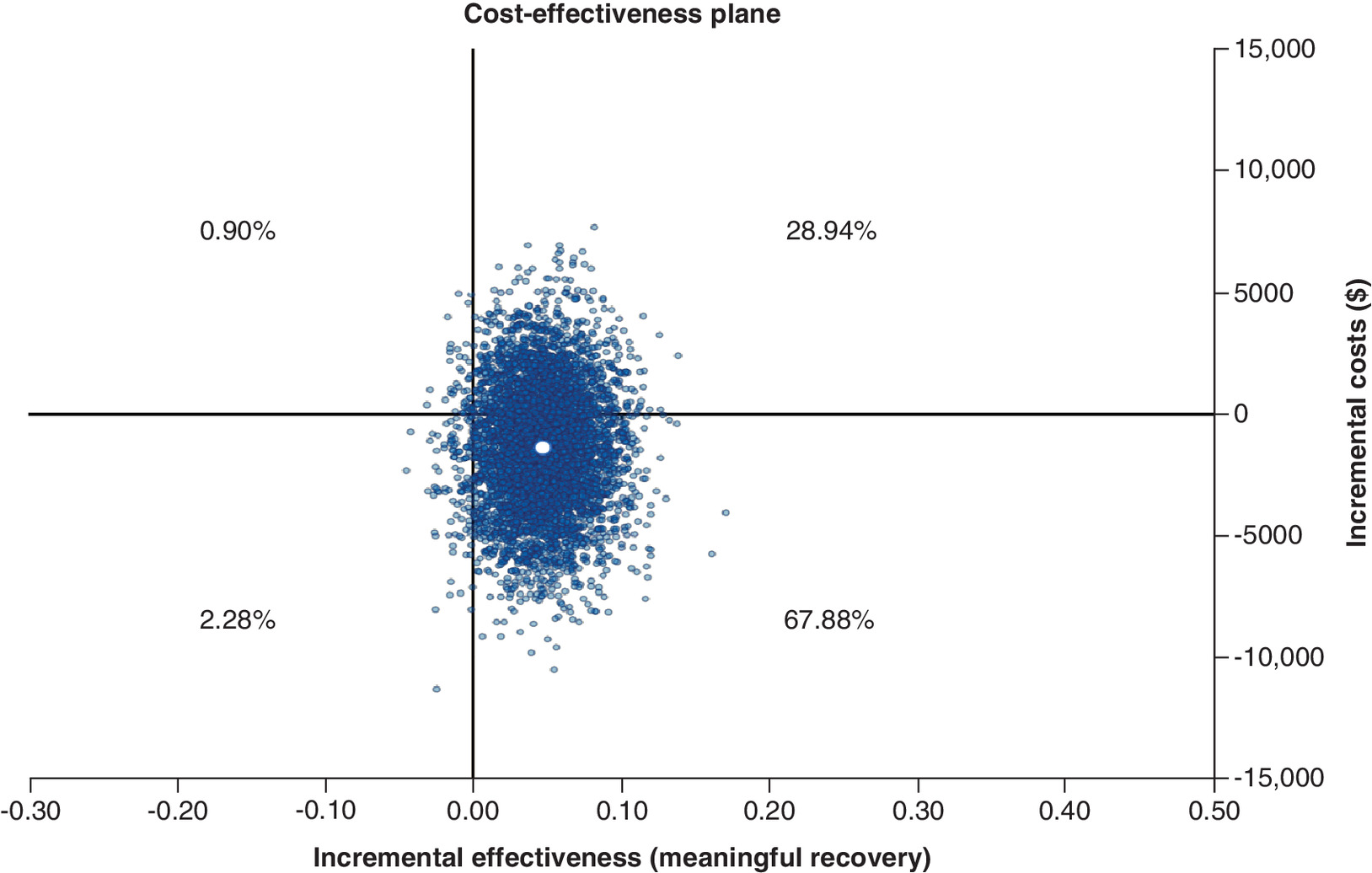
The base-case analysis was performed probabilistically – probabilistic sensitivity analysis (PSA) - in order to quantify the level of confidence in the overall output of the analysis [32]. Appropriate distributions, i.e., beta or gamma, were assigned to included model parameters. In the PSA, all input parameters were varied simultaneously to assess cost effectiveness in response to collective parameter uncertainty. A Monte Carlo simulation was performed, with 5000 model iterations, in order to vary parameter values stochastically to estimate the distribution of the model outputs [33]. cost–effectiveness outcomes were calculated for each iteration of random sampling, with appropriate probabilistic output produced, i.e., cost–effectiveness plane.
One-way sensitivity analysis
The influence of individual input parameters on the base-case results was examined in deterministic sensitivity analysis (DSA). The ranges in the parameter's values were determined based on either the literature, or following clinical expert input. Where a range of values could not be defined, i.e., 95% confidence interval (CI), parameters were increased/decreased by 30%. Based on expert clinical input, wide variation ranges of 0–22% and 0–20% were used for the likelihood of chronic pain and neuroma at the donor site, respectively, to explore uncertainties around the impact of these two parameters on the economic evaluation results. Results of the one-way sensitivity analyses were presented for both incremental cost, and incremental effectiveness.
Results
Base-case analysis
Over a lifetime horizon, there is a small difference (4.69%) in the average probability of MR between allograft (75.15%) and autograft (70.46%). Nerve repair with allograft also results in lower costs compared with autograft based on results of the base-case probabilistic analysis ($12,677 vs $14,023; -$1346 with allograft). Therefore, allograft is a less costly and more effective approach than autograft for the surgical repair of PNI.
Further results of the base-case probabilistic analysis are presented in the cost–effectiveness plane shown in Figure 1, which displays a scatterplot of the results of 5000 individual model iterations. Points to the right of the y-axis indicate that allograft is more effective than autograft, while points above the x-axis indicate that allograft results in greater costs than autograft. As shown in Figure 1, most of the points in the scatterplot are below the x-axis (67.88%), indicating a higher probability that allograft therapy will reduce costs compared with autograft. Additionally, most of the points are to the right of the y-axis, indicating that there is a higher probability that allograft is more effective compared with autograft.
One-way sensitivity analysis
One-way sensitivity analyses highlighted the input parameters with the greatest impact on the base-case cost and effectiveness results. Figure 2 shows that the most impactful parameters on the incremental cost of the intervention were the costs of nerve repair associated with both procedures (upper limit value for autograft results in an incremental cost of -$7446 for the intervention, while the lower limit value for allograft results in an incremental cost of -$7402 for the intervention). The probability of experiencing chronic pain at the donor site after repair with autograft and unit costs of non-opioid analgesics also had a large impact on the results of this analysis. Regardless of the one-way parameter variations made, allograft remained a cost-saving intervention.
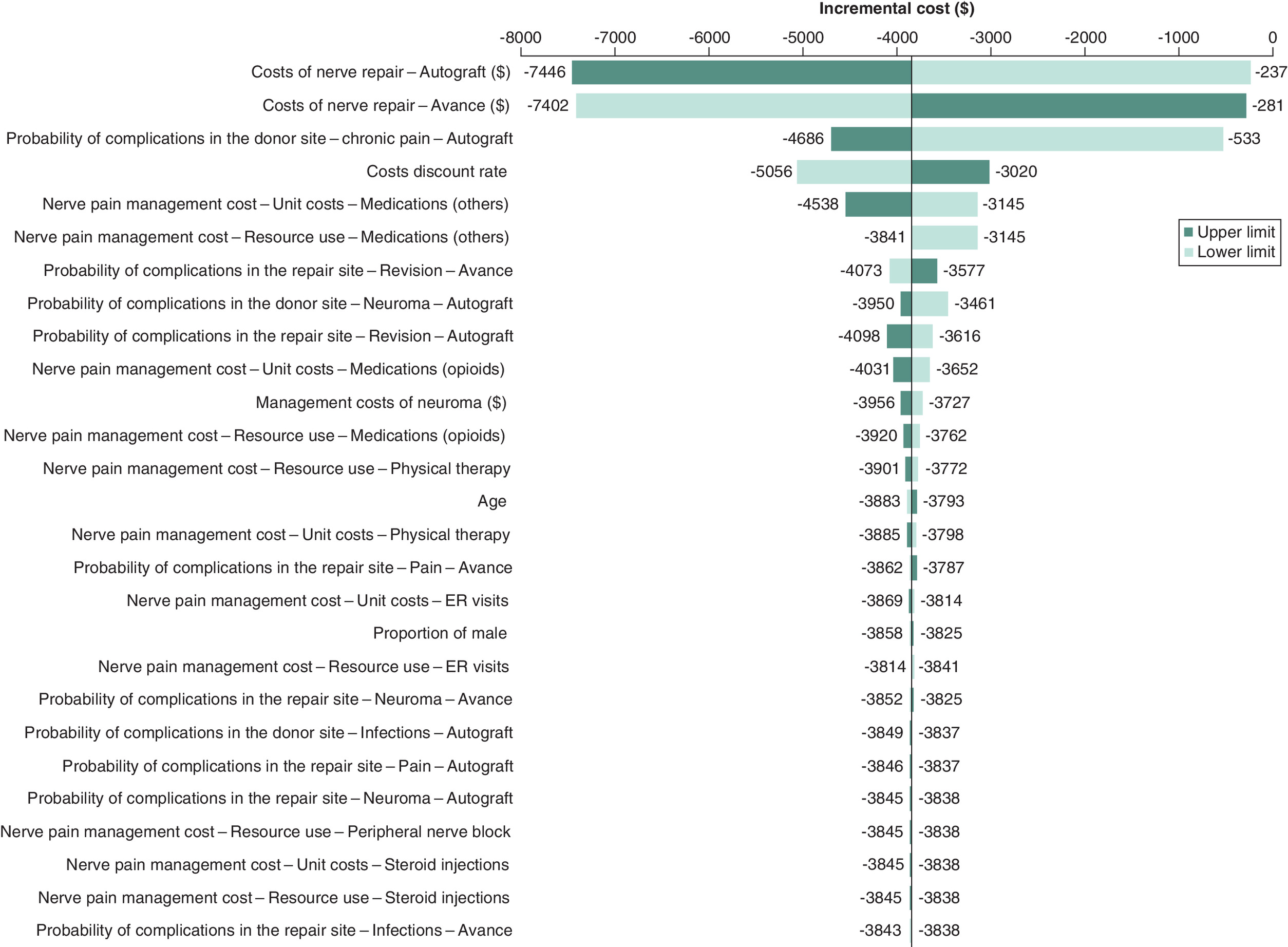
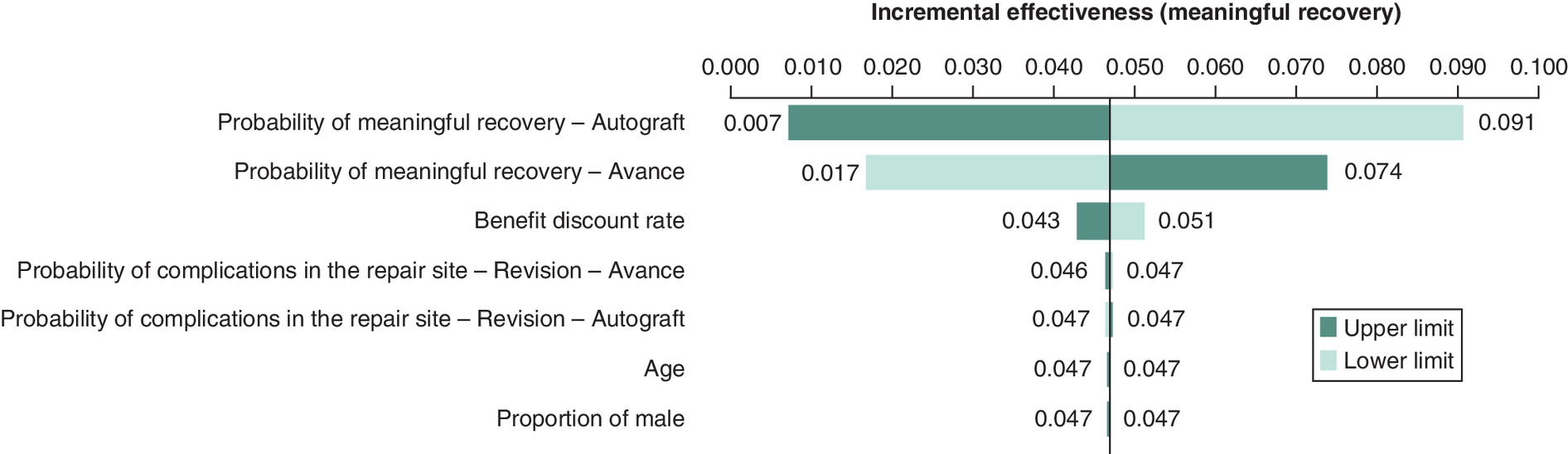
Figure 3 presents results of the one-way sensitivity analyses focused on incremental effectiveness (MR). The majority of parameters included in the analysis had no impact on the effectiveness results. The probabilities of achieving MR in the autograft and allograft arms of the analysis were the most impactful parameters on incremental effectiveness. As in the analysis of incremental cost, allograft remained more effective than the comparator regardless of the parameter variations made.
Scenario analysis
The results of the scenario analysis in which autograft was assumed to be performed in case of an unsuccessful allograft, showed slightly less cost-savings (-$1230) compared with the base-case analysis. This was due to more costly complications at the autograft donor site ($308 donor site complication costs incurred in the allograft arm when autograft was used after an unsuccessful allograft procedure). Moreover, the model results showed that the probability of MR in the allograft arm was reduced to 74.76%, leading to an incremental MR of 4.28% compared with autograft.
Discussion
The impact of PNIs on patient morbidity and overall economic burden, is significant, with a high associated complication rate [19]. While treatment options including medication, immobilization, and physical therapy may be sufficient depending on the severity of the condition, surgical repair is the only treatment option that can restore function of a transected nerve [34]. Although nerve autografts are the historical gold standard for the nerve graft repair of PNIs, their use is restricted due to limited self-donor graft tissue [35]. Additionally, the requirement to perform an additional procedure during the surgery to harvest the autograft, as well as donor site morbidity and potential loss of function, necessitates the need to seek alternative surgical options for the treatment of PNIs [13]. Pooled evidence has shown that allograft surgery for peripheral nerve reconstruction is a viable alternative, with comparable effectiveness to autograft [28,29]. This study involved the development of a US-based economic model to compare the costs and health outcomes associated with these two alternative surgical treatment options, over a lifetime horizon.
The base-case results indicated that allograft leads to improved MR compared with autograft, which supports the comparable effectiveness data in the literature [12,16]. While there is a slight difference between the upfront costs associated with the respective surgery types during initial nerve repair (Supplementary Table 3 presents the initial cost savings associated with utilizing allograft), allograft was cost-saving even in the first year after surgery, when procedure complication costs were considered. This study also explored the long-term cost savings associated with allograft, which have been demonstrated through the economic modeling. The base-case results indicated that the intervention leads to cost savings over a lifetime horizon, when the effect on subsequent complication rates is also considered. Significant costs are associated with donor-site complications, including chronic pain management costs, which are not incurred when patients undergo an allograft procedure. These donor-site complications are an important clinical limitation of the autograft procedure that should be considered when deciding on the most appropriate method of surgical repair [30,31], and their economic implications have been demonstrated in the analysis presented here. Indeed, with the cost of neuroma excision exceeding $2200 upon occurrence, the increased complication rate associated with autograft, and the fact that donor-site complications are not incurred with allograft, is a strong determinant of the overall cost–effectiveness results. Probabilistic results highlighted the likelihood that allograft would represent a cost-saving and more effective surgical alternative to autograft.
As highlighted, the likelihood of experiencing complications at the donor site following an autograft procedure were also shown to be strong drivers of incremental cost. Additionally, as demonstrated in one-way sensitivity analyses of incremental effectiveness, allograft is more effective compared with autograft (increment of 4.9% in MR), even when the lower parameter value for the probability of MR with allograft or the higher parameter value of the probability of MR with autograft, are assumed.
While considerable research has been performed exploring the clinical outcomes associated with both allograft and autograft in nerve reconstruction surgeries as demonstrated in a 5-year bibliometric analysis performed by Gao et al. [35], evidence on their respective, and comparable, costs is more limited. The work by Lans et al., which presents details of a systematic literature review, highlights the comparable effectiveness of allograft and autograft nerve repairs in relation to MR in both sensory and motor function, and the improved effectiveness of both compared with conduit [17]. Their work also highlights the reduced costs associated with allograft in the inpatient setting following a Medicare claims cost analysis, and their comparable costs in the outpatient setting, although details of the methodology of this analysis are sparse. Our work, therefore, adds considerably to the existing economic evidence base.
Although cost analyses of the individual surgical techniques are limited, previous work has been performed to examine the economic burden, and socioeconomic effects, of PNI overall. A European-based study by Bergmeister et al. analyzed data from 250 patients with 286 work-related upper extremity nerve injuries in Germany [36]. Their work showed that single median nerve injuries averaged 7 ± 5 days in the hospital and costs of €3570 ± €3570. Comparably, combined nerve injuries were significantly (p > 0.01) more expensive at €7962 ± €6896, with cost increasing further if nerve injuries were combined with tendon or vascular injury. Their analysis, based on a German patient sample, indicated that nerve injury has a major impact on function and employment, resulting in significant healthcare costs, while both proximal and distal nerve injuries lead to long-term disability, subsequent sick-leave and to permanent disability pension among 30% of patients [36]. Studies such as this, which highlight the significant economic burden associated with this condition, reinforce the need to ensure that treatment choices for PNI are both clinically effective and represent value for money. The cost–effectiveness model presented in this study may be utilized by decision-makers to make optimal choices in relation to surgical therapy.
While a robust economic analysis has been performed, there are some limitations that should be considered. Firstly, the effect estimates used in the model were based on pooled retrospective studies rather than clinical trials, and thus are subject to biases and confounding factors that may impact the model results [11,13]. Secondly, due to data limitations in this clinical area, it was not possible to include utility weights in the economic analysis and therefore, the impact of the intervention on quality-adjusted life-years (QALYs) gained compared with autograft could not be estimated. As a result, MR was included as an alternative measure of effectiveness, which provides a strong correlation with improvements in QoL [5]. Additionally, for the sake of comparability, we limited our analysis to single nerve repair cases. From a cost perspective, autografts may be favored if there is an adequate donor nerve available to repair multiple nerves in the subgroup of patients with multiple nerve injuries. Furthermore, considering that allografts are only available up to 70 mm, allografts would not be a suitable option for nerve gaps longer than 70 mm. Consequently, the findings of this study may not be generalizable to cases with nerve gaps beyond that threshold. Lastly, in the absence of long-term data on complications associated with the alternative strategies, expert opinion was used to populate the model. Uncertainties in the clinical data included in the model were assessed through rigorous one-way sensitivity analyses, and with the performance of a PSA to consider the uncertainty present in individual model parameters. The allograft nerve reconstruction intervention remained a cost saving, and cost-effective, option regardless of the parameter variations made.
Conclusion
This study presents a cost–effectiveness analysis of allograft surgery (Avance Nerve Graft) compared with autograft for the treatment of peripheral nerve injury. Results indicate that allograft has a high probability of being cost saving, and more effective, over a lifetime horizon, from a US healthcare payer perspective. Future analyses may consider the inclusion of utility data, and robust data on long-term consequences of treatment strategies, to allow decision-makers to consider the full range of benefits associated with allograft procedures, including impact on patient quality-of-life.
Summary points
•
An economic model has been developed to consider the lifetime costs and health outcomes associated with allograft using the Avance Nerve Graft, compared with autograft, from a US healthcare payer perspective.
•
Economic modeling results indicate that allograft has a high probability of being cost saving (67.88%), while base-case findings demonstrate both cost savings (-$1346) and improved effectiveness (+5% average probability of meaningful recovery) with the intervention.
•
A robust economic model has been developed, and may be utilized by decision-makers, to inform optimal surgical treatment choices in a clinical area that is currently hindered by a lack of reliable economic evidence.
Author contributions
AA was responsible for designing and developing the economic model, performing the economic analysis, interpreting the results and drafting the manuscript. MJ designed the study and interpreted the results. JFS was responsible for the clinical validity of the analysis, interpreting the results and critically reviewing the manuscript, and AT was responsible for interpreting the results and critically reviewing the manuscript. All authors reviewed and approved the final version of the manuscript.
Acknowledgments
Authors express their deep gratitude to clinical expert Dr Ivica Ducic, who reviewed all modeling assumptions and supported the research team in filling the knowledge gaps.
Financial disclosure
This research was funded by Axogen, Inc., Alachua, Florida. The views expressed in this publication are those of the author(s) and not necessarily those of the company. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
A Ansairpiour and M Javanbakht are employees of Optimax Access Ltd., which has received research grants from Axogen, Inc via Device Access UK Ltd. A Thompson is an employee of Axogen, Inc, who funded this study. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Data sharing statement
The information reported in this manuscript is sufficient to replicate the results of the study.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 124.92 KB
References
Papers of special note have been highlighted as: • of interest
1.
Cairns C, Kang K. National hospital ambulatory medical care survey: 2019 emergency department summary tables [Internet]. National Center for Health Statistics (U.S.) (2022). https://stacks.cdc.gov/view/cdc/115748
2.
Kornfeld T, Vogt PM, Radtke C. Nerve grafting for peripheral nerve injuries with extended defect sizes. Wien. Med. Wochenschr. 169, 240–251 (2019).
3.
Mayo Clinic. Peripheral nerve injuries – diagnosis and treatment. (2022).
4.
Carvalho CR, Oliveira JM, Reis RL. Modern trends for peripheral nerve repair and regeneration: beyond the hollow nerve guidance conduit. Front. Bioeng. Biotechnol. 7, 337 (2019).
5.
Wojtkiewicz DM, Saunders J, Domeshek L, Novak CB, Kaskutas V, Mackinnon SE. Social impact of peripheral nerve injuries. HAND. 10(2), 161–167 (2015).
6.
Griffin MF, Malahias M, Hindocha S, Khan WS. Peripheral nerve injury: principles for repair and regeneration. Open Orthop J. 8, 199–203 (2014).
7.
Siemionow M, Brzezicki G. Current techniques and concepts in peripheral nerve repair. Int. Rev. Neurobiol. 87, 141–172 (2009).
8.
Grinsell D, Keating CP. Peripheral nerve reconstruction after injury: a review of clinical and experimental therapies. Biomed Res Int. 2014, 2014 (2014).
9.
Kornfeld T, Borger A, Radtke C. Reconstruction of critical nerve defects using allogenic nerve tissue: a review of current approaches. Int. J. Mol. Sci. 22(7), 3515 (2021).
10.
Siemionow M, Sonmez E. Nerve allograft transplantation: a review. J. Reconstr. Microsurg. 23(08), 511–520 (2007).
11.
Ducic I, Yoon J, Buncke G. Chronic postoperative complications and donor site morbidity after sural nerve autograft harvest or biopsy. Microsurgery 40(6), 710–716 (2020).
• This study reports nerve repair complication rate among 478 sural nerve procedures.
12.
Szynkaruk M, Kemp SWP, Wood MD, Gordon T, Borschel GH. Experimental and clinical evidence for use of decellularized nerve allografts in peripheral nerve gap reconstruction. Tissue Eng. Part B Rev. 19(1), 83–96 (2013).
13.
Safa B, Jain S, Desai MJ, Greenberg JA, Niacaris TR, Nydick JA et al. Peripheral nerve repair throughout the body with processed nerve allografts: results from a large multicenter study. Microsurgery 40(5), 527–537 (2020).
• Reports meaningful recovery rates to examine the continued use of processed nerve allograft up to 70 mm in sensory, mixed and motor nerve repair throughout the body and across a broad patient
14.
Leckenby JI, Furrer C, Haug L, Personeni BJ, Vögelin E. A retrospective case series reporting the outcomes of Avance nerve allografts in the treatment of peripheral nerve injuries. Plast. Reconstr. Surg. 145(2), 368e–381e (2020).
15.
Means KR, Rinker BD, Higgins JP, Payne SH, Merrell GA, Wilgis EFS. A multicenter, prospective, randomized, pilot study of outcomes for digital nerve repair in the hand using hollow conduit compared with processed allograft nerve. HAND. 11(2), 144–151 (2016).
16.
Karabekmez FE, Duymaz A, Moran SL. Early clinical outcomes with the use of decellularized nerve allograft for repair of sensory defects within the hand. HAND. 4(3), 245–249 (2009).
17.
Lans J, Eberlin KR, Evans PJ, Mercer D, Greenberg JA, Styron JF. A systematic review and meta-analysis of nerve gap repair: comparative effectiveness of allografts, autografts, and conduits. Plast. Reconstr. Surg. 151(5), 814e–827e (2023).
• Sought to conduct a systematic literature review and meta-analysis in order to compare recovery rates and postoperative complications among autograft, allograft, conduit repairs in nerve gaps of 5 mm to 70 mm in length.
18.
Styron J, Thompson A, Park L, Watson G. Nerve repair hospital index procedure costs – allograft vs. Autograft repair type. Presented at: The 75th annual meeting of the ASSH. TX, USA (2020).
19.
Foster CH, Karsy M, Jensen MR, Guan J, Eli I, Mahan MA. Trends and cost-analysis of lower extremity nerve injury using the national inpatient sample. Neurosurgery 85(2), 250–256 (2019).
20.
Raizman NM, Endress RD, Styron JF et al. Procedure costs of peripheral nerve graft reconstruction. Plas. Reconstr. Surg. Global Open. 11(4), e4908 (2023).
• Provides a retrospective cross-sectional observational study (n = 1363) using the US all-payer PINC AI Healthcare Database examined facility procedure costs and cost drivers in patients undergoing allograft or autograft repair
21.
The National Institute for Health and Care Excellence. Overview | Processed nerve allografts to repair peripheral nerve discontinuities | Guidance (2022). www.nice.org.uk/guidance/IPG597
22.
Neumann PJ, Sanders GD, Russell LB, Siegel JE, Ganiats TG. cost–effectiveness in Health and Medicine. Oxford University Press, NY, USA (2016).
23.
Martin E, Muskens IS, Senders JT, Cote DJ, Smith TR, Broekman MLD. A nationwide analysis of 30-day adverse events, unplanned readmission, and length of hospital stay after peripheral nerve surgery in extremities and the brachial plexus. Microsurgery 39(2), 115–123 (2019).
24.
Centers for Disease Control and Prevention. Health Insurance Portability and Accountability Act of 1996 (HIPAA) (2022). www.cdc.gov/phlp/publications/topic/hipaa.html
25.
The U.S. Centers for Medicare & Medicaid Services. List of CPT/HCPCS Codes | CMS [Internet] (2022). www.cms.gov/Medicare/Fraud-and-Abuse/PhysicianSelfReferral
26.
Guest JF, Fuller GW, Vowden P. Costs and outcomes in evaluating management of unhealed surgical wounds in the community in clinical practice in the UK: a cohort study. BMJ Open. 8(12), e022591 (2018).
27.
MD L deGraft-Johnson. How Much Does a Primary Care Visit Cost in 2022? [Internet]. K Health (2022). https://khealth.com/learn/healthcare/primary-care-visit-cost/
28.
Organisation for Economic Co-operation and Development. Conversion rates – purchasing power parities (PPP) (2022). http://data.oecd.org/conversion/purchasing-power-parities-ppp.htm
29.
Unpublished data provided by Dr Ivica Ducic - Washington Nerve Institute study (Unpublished).
30.
Gore M, Brandenburg NA, Hoffman DL, Tai KS, Stacey B. Burden of illness in painful diabetic peripheral neuropathy: the patients' perspectives. J Pain. 7(12), 892–900 (2006).
31.
The U.S. Centers for Medicare & Medicaid Services. 2022 ASP Drug Pricing Files (2022). www.cms.gov/medicare/medicare-part-b-drug-average-sales-price/2022-asp-drug-pricing-files
32.
York Health Economics Consortium (YHEC). Probabilistic/Stochastic Sensitivity Analysis (2022). http://yhec.co.uk/glossary/probabilistic-stochastic-sensitivity-analysis/
33.
York Health Economics Consortium (YHEC). Monte-Carlo Simulation (2022). http://yhec.co.uk/glossary/monte-carlo-simulation/
34.
Stanford Health Care. Treatments (2022). https://stanfordhealthcare.org/medical-conditions/brain-and-nerves/peripheral-nerve-injury/treatments.html
35.
Gao Y, Wang YL, Kong D et al. Nerve autografts and tissue-engineered materials for the repair of peripheral nerve injuries: a 5-year bibliometric analysis. Neural Regen. Res. 10(6), 1003–1008 (2015).
36.
Bergmeister KD, Große-Hartlage L, Daeschler SC et al. Acute and long-term costs of 268 peripheral nerve injuries in the upper extremity. PLOS One. 15(4), e0229530 (2020).
Information & Authors
Information
Published In
Copyright
© 2023 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 2 July 2023
Accepted: 31 October 2023
Published online: 30 November 2023
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness analysis of Avance® allograft for the treatment of peripheral nerve injuries in the USA. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0113
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Aneeq S. Chaudhry, Daniel A. Rabin, Erin Kelley, Katherine Kozlowski, William Tian, Tarifa H. Adam, Jason H. Ko, Chad M. Teven, Marco F. Ellis, Robert D. Galiano, Safety of Breast Neurotization Using Nerve Allografts in Implant-Based Breast Reconstruction, Annals of Plastic Surgery, 10.1097/SAP.0000000000004779, 97, 2, (135-141), (2026).
- Wendy Ghanem, Hady Ezzeddine, Joseph Najjar, Antoine Saber, Rita Saad, Elyssa Kiwan, Georges Sakhat, Ali Ghosn, Johnny Saadeh, Fouad Assaf, Hicham AbdelNour, Mohamad Badra, Ramzi Moucharafieh, Vascularized Nerve Grafts: Current Concepts, Indications, and Future Perspectives, Orthopedic Reviews, 10.52965/001c.156463, 18, (2026).
- Caijun Jin, Xinrui Zhang, Yongxun Jin, Pham Ngoc Chien, Chan Yeong Heo, Acellular Extracellular Matrix Scaffolds in Regenerative Medicine: Advances in Decellularization and Clinical Applications, Journal of Functional Biomaterials, 10.3390/jfb16100383, 16, 10, (383), (2025).
- Dinesh Kumar, Sonia Gupta, Vrinda Gupta, Rajni Tanwar, Pooja Rani, Vikas Bansal, Stem Cells to Organoids: Pioneering the Future of Regenerative Therapies, Stem Cell Reviews and Reports, 10.1007/s12015-025-10985-7, 22, 1, (118-143), (2025).
- Stefanie Deininger, Andreas Knoll, Nadja Grübel, Andrej Pala, Ralph König, Christian Rainer Wirtz, Maria Teresa Pedro, Novelties and limitations of tissue-engineered materials in treating traumatic nerve injuries: a mini review, Frontiers in Cell and Developmental Biology, 10.3389/fcell.2025.1603678, 13, (2025).
- Marco Govoni, Leonardo Vivarelli, Nicola Fazio, Federico Bolognesi, Viscardo Paolo Fabbri, Alessandra Maso, Elisa Storni, Giulia Querzoli, Deyanira Contartese, Stefania Pagani, Luca Cavazza, Marta Pluchino, Lucia De Franceschi, Gianluca Giavaresi, Dante Dallari, Peripheral Nerve Decellularisation Protocol for Allogeneic Transplantation: From Tissue Procurement to Banking, International Journal of Molecular Sciences, 10.3390/ijms26167937, 26, 16, (7937), (2025).
- Nidhi Puranik, Shraddha Tiwari, Meenakshi Kumari, Shiv Kumar Yadav, Thakur Dhakal, Minseok Song, Advanced Bioactive Polymers and Materials for Nerve Repair: Strategies and Mechanistic Insights, Journal of Functional Biomaterials, 10.3390/jfb16070255, 16, 7, (255), (2025).
- Zhifa Xue, Yuye Huang, De Bi, Kai Ye, Hangyu Zhou, Lizhe He, Peng Wei, Yangjian Wang, Composite poly(lactic-co-glycolic acid) and a decellularized extracellular matrix conduit with Schwann cells for enhanced nerve regeneration, Bio-Design and Manufacturing, 10.1631/bdm.2400334, 8, 3, (359-374), (2025).
- Ashley Zhang, Sophia Salingaros, Sophia Arbuiso, Grant G. Black, Marcos Lu Wang, Hao Huang, David Otterburn, Comparing Primary Coaptation and Allograft in Deep Inferior Epigastric Perforator Flap Breast Reconstruction, Annals of Plastic Surgery, 10.1097/SAP.0000000000004266, 94, 4S, (S291-S296), (2025).
- Yu Hwa Nam, Ji-Sup Kim, Yoonji Yum, Juhee Yoon, Hyeryung Song, Ho-Jin Kim, Jaeseung Lim, Saeyoung Park, Sung-Chul Jung, Application of Mesenchymal Stem Cell-Derived Schwann Cell-like Cells Spared Neuromuscular Junctions and Enhanced Functional Recovery After Peripheral Nerve Injury, Cells, 10.3390/cells13242137, 13, 24, (2137), (2024).
- See more