Risk of long-term care admissions among Medicare beneficiaries treated with pimavanserin or quetiapine for Parkinson's disease psychosis in USA: a retrospective administrative claims database analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Risk of long-term care (LTC) admission (LTCA) associated with atypical antipsychotic (AAP) use among patients with Parkinson's disease psychosis (PDP) is a major concern. However, no comparative studies have examined the differences in risk of LTC admissions between pimavanserin (PIM), the only FDA-approved AAP for PDP, and other off-label AAPs including quetiapine (QUE). Objective: To examine all-cause LTCA rates and risk among PDP patients treated with AAPs such as QUE or PIM. Methods: Analysis of Parts A, B and D claims (100% Medicare sample; 2013–2019) of Medicare beneficiaries with PDP that initiate ≥12-month continuous PIM or QUE monotherapy from 1 January 2014 to 31 December 2018 (i.e., index date) without any AAP use in the 12-month pre-index period was conducted. Outcome assessments among 1:1 propensity score-matched (31 variables – age, sex, race, region and 27 Elixhauser comorbidities) beneficiaries on PIM versus QUE included risk of all-cause skilled nursing facility stays (SNF-stays), LTC-stays, and overall LTCA (i.e., SNF-stays or LTC-stays). All-cause LTCA rates and LTCA risk were compared using logistic regression and cox proportional hazards models, respectively, controlling for demographics, comorbidities and co-existing-dementia or insomnia. Results: Of the matched sample (n = 842 for each group) from total sample (n = 9652), overall all-cause LTCA and SNF-stay rates were 23.2 and 20.2% for PIM versus 33.8 and 31.4% for QUE, respectively (p < 0.05, for each). Hazard ratio (95% CI) for risk of SNF-stay and overall LTCA was 0.78 (0.61, 0.98) and 0.80 (0.66, 0.97), respectively, for PIM versus QUE beneficiaries (p < 0.05, for each). Conclusion: The 20% lower risk of LTCA (i.e., greater delay) with PIM versus QUE in this analysis may suggest that PIM should be started early for the treatment of PDP.
Plain language summary
This study compared patients aged greater than or equal to 65 years old residing in the community setting and diagnosed with Parkinson’s disease psychosis (PDP) who were initiated on pimavanserin (PIM) or other atypical antipsychotics (AAPs). Currently, PIM, is the only FDA-approved AAP, however, other AAPs, such as quetiapine (QUE) are used off-label for PDP. In this study, patients were evaluated for their risk of long-term care admissions while being on PIM versus (i) other AAPs, and (ii) QUE.
A 100% US Medicare sample with Medical claims data (Part A and B) and Pharmacy claims data (Part D) between 2013–2019 was used to compare long-term care admission rates. The annual risk of skilled nursing facilities stays (SNF-stays), long-term care stays (LTC-stays), and overall LTC admission (LTCA) between those who are treated with PIM only or QUE only for at least 12 months were compared during 12 months of follow-up. To make the PIM only and QUE only groups comparable, researchers matched individuals based on 31 different factors such as age, sex, race, region and 27 comorbid health conditions that resulted in a total of 842 matched patients in each group. PIM patients had lower rates of all-cause LTC admissions (23.2% vs 33.8% and SNF-stays (20.2% vs 31.4%) compared to QUE patients. The hazard ratios indicated a 22% lower risk of SNF-stays (hazard ratio = 0.78) and 20% lower risk for overall LTCA (hazard ratio = 0.80) for PIM compared to QUE, suggesting that starting PIM early may delay as well as reduce LTCA among Medicare beneficiaries with PDP compared to QUE. The results for PIM vs other AAPs were shown to be similar as PIM vs QUE in these outcomes.
Parkinson's disease, the second most common neurodegenerative disease, is characterized by loss of dopaminergic neurons that results in motor and nonmotor symptoms affecting 1 million individuals in the USA [1–3]. Among PD patients, approximately 25–40% develop Parkinson's disease psychosis (PDP), characterized by symptoms of hallucinations and delusions, over the course of the disease [2,4]. As PDP severity increases, it can often increase caregiver burden and eventually increase nursing home stay and long-term care placement [4,5]. Studies examining the rate and predictors of nursing home placement among PD patients have also demonstrated that neuropsychiatric symptoms such as hallucinations, delusions and other cognitive problems contribute to institutionalization [4,6]. However, the presence of hallucinations is known to be the strongest predictor as patients with PDP-related hallucinations are 2.5-times more likely to be placed in nursing homes than those without PDP [4]. After nursing home placement, PDP patients are likely to remain there permanently and have a high rate of mortality [5,7,8]. Therefore, timely diagnosis and treatment of PDP is critical.
Over the last two decades, atypical antipsychotics (AAPs) have been used off-label to treat symptoms of psychosis despite the elevated risk of adverse events such as falls, fractures and stroke and a potential for exacerbating movement disorder related symptoms associated with them [9,10]. A study conducted on Veterans Affairs data reported that AAPs were prescribed among 50% of patients with PDP during 1 year of follow-up. Furthermore, quetiapine (QUE) was prescribed among 66% of patients who were prescribed antipsychotics [11].
In 2016, pimavanserin (PIM), a 5-HT2A receptor inverse agonist, became the first atypical antipsychotic to be approved by US FDA for the treatment of hallucinations and delusions associated with PDP [12,13]. In a 6-week placebo-control study, PIM has shown to significantly reduce the frequency and/or severity of hallucinations and delusions associated with PD psychosis compared with placebo, without impacting motor function. PIM has an established safety profile and in a recent retrospective analysis, PIM was associated with lower all-cause falls and fractures compared with other AAPs [10,14]. In a meta-analysis of 417 patients with PDP on PIM, a significant reduction in positive symptoms, hallucinations and delusion were observed [15].
While PIM's effect on healthcare resource utilization rates have been recently studied [16], effect of PIM versus QUE or other off-label AAPs on risk of long-term care (LTC) admission (LTCA) has not been previously assessed. As QUE is the most frequently used antipsychotic within the other-AAP cohort, the primary objective of this analysis was to examine the rates of LTCA, the time to LTCA, and the risk of LTC /nursing home (NH) stay among PDP Medicare beneficiaries treated with PIM versus QUE.
Materials & methods
Study design
A retrospective cohort analysis of beneficiaries with PDP using Parts A, B and D claims data from January 2013 to December 2019 using the Centers for Medicare and Medicaid Services (CMS) 100% Medicare fee-for-service (FFS) sample was conducted. Beneficiaries with PDP that initiate PIM or QUE-only were identified from diagnostic claim for PD and concurrent psychosis from January 2013 to December 2018 to create the primary analysis cohorts. Similarly, a secondary cohort of beneficiaries initiating PIM compared with other-AAPs (quetiapine, risperidone, olanzapine, aripiprazole) was also examined as a secondary comparison. This analysis was conducted in accordance with HIPAA compliance after a New England Review Board ethics committee approval and CMS data use agreement.
Data source
The Medicare 100% sample was the data source used for this analysis. The 100% Medicare sample represents data from the federal health insurance program that provides health insurance coverage for all US residents ≥65 years, select individuals with disabilities aged <65 years, and individuals with end-stage renal disease. As of 2019, there were 63 million US Medicare beneficiaries, all of whom were represented in the 100% sample and contains claims for all inpatient, outpatient, and pharmacy services incurred by all the covered beneficiaries. The analysis dataset, therefore, represents all beneficiaries ≥65 year of age with Parkinson's disease psychosis during 2013–2019 in USA. It should be noted that Medicare Part A, B and D covers hospital insurance (i.e., inpatient hospitalizations, skilled nursing, hospice and home healthcare), medical insurance (i.e., doctor visits, outpatient care, preventive services and durable medical equipment) and pharmacy insurance (i.e., prescription medication coverage through private insurance plans). Medicare Fee-for-Service (FFS) refers to the traditional indemnity Medicare program, which includes Part A and Part B, where healthcare providers are paid on a fee schedule for each service provided to the beneficiary, and reimbursement is based on fees established by Medicare.
Patient population
Beneficiaries with at least one ICD-9 (332.0) or ICD-10 (G20) diagnostic claim for PD along with concurrent occurrence of one or more psychosis or psychotic disorder diagnostic claim (Supplementary Table 1) from January 2013 to December 2018 were selected. The study population comprised of treatment-naive beneficiaries with PDP who initiated continuous monotherapy for at least 12 months with: PIM versus QUE-only as a primary analysis and PIM versus other-AAP monotherapy (i.e., quetiapine, risperidone, olanzapine and aripiprazole) as a secondary analysis. Continuous monotherapy was defined as the use of only the index AAP for at least 12 months between January 2014 to December 2019 until discontinuation, augmentation/switch, or end of data period (31 December 2019), whichever occurred first.
Date of first prescription for PIM or QUE or other-AAPs formed the index date for the respective case and reference control cohorts. Only beneficiaries without prior use of any AAP for at least 12 months prior to index date were included. Beneficiaries with a pre-index diagnosis of psychosis, secondary parkinsonism, delirium, other psychotic disorders, alcohol/drug-induced psychosis, schizophrenia, paranoia, or personality disorders, were also excluded from the study population. List of diagnostic codes used to describe study population selection are listed in Supplementary Table 1. Details describing sample selection and sample disposition chart is provided in Figure 1.

Figure 1. Patient attrition.
*Only beneficiaries without prior use of any AAP for at least 12 months prior to index date were included. Beneficiaries with a pre-index diagnosis of psychosis, secondary parkinsonism, delirium, other psychotic disorders, alcohol/drug-induced psychosis, schizophrenia, paranoia, or personality disorders, were also excluded from the study population.
AAP: Atypical antipsychotic; PD: Parkinson's disease; PDP: Parkinson's disease psychosis; PIM: Pimavanserin; QUE: Quetiapine.
Study covariates
Baseline demographics, clinical comorbidities, concomitant movement disorder medication (i.e., levodopa, carbidopa, levodopa/carbidopa) use and co-existing insomnia or dementia were used to describe the sample characteristics. Baseline demographic characteristics such as age, sex, race or ethnicity, region and Elixhauser comorbidity index were described based on data on or prior to the index date. Comorbidities such as psychosis, HIV, alcohol abuse and substance abuse were excluded from PSM to avoid potential confounding [17–20]. Psychosis was not used for matching in PSM since beneficiaries with psychosis in the pre-index (i.e., baseline) were excluded in this analysis. Also, data for beneficiaries with HIV, alcohol abuse and substance use were suppressed by CMS to accommodate patient confidentiality and would not have allowed an appropriate method of matching. Additionally, breakdown of AAPs initiated on index date in the other-AAP group were described.
Propensity score matching
Beneficiaries initiating PIM or QUE were 1:1 propensity score matched (PSM) to create a balanced sample on measured characteristics. Propensity scores were calculated using multivariate logistic regression on patient age, sex, race, region and 27 of the Elixhauser comorbidity characteristics. The PSM algorithm utilized an 8:1 Digit Match®, a greedy nearest neighbor matching algorithm to first match PIM beneficiaries to QUE on 8 digits of the propensity score. Among the unmatched, PIM beneficiaries are then matched to QUE on 7 digits of the propensity score, sequentially proceeding to the lowest digit (1 digit) match on propensity score), until no other matches can be made [21]. Covariate balance were assessed using standardized mean differences (SMDs) value of <0.1 between PIM versus QUE. A similar matching procedure was conducted for the secondary analysis involving PIM versus other-AAP cohorts. All missing data were excluded pre-match and the final, matched sample had no missing data.
Follow-up
Follow-up commenced on the index date and continued for at least 12 months until discontinuation, augmentation/switch, or end of data period (31 December 2019), whichever occurred first. Censoring occurred 365 days after index date.
Study outcomes
All-cause annual rates of LTCA, (defined as a composite of skilled nursing facility stay (SNF-stay) or long-term care stay (LTC-stay) were analyzed for PIM versus QUE cohort based on 12-month follow-up. Additionally, time to SNF-stay, LTC-stay, and all-cause LTCA and 12-month risk of all-cause SNF-stay, LTC-stay, and LTCA were analyzed for both PIM and QUE cohort. It should be noted that in Medicare claims, both SNF-stay and LTC-stay are inpatient hospitalizations, which are defined based on provider type/facility characteristics. Three types of inpatient hospital admissions are defined in Medicare claims: short-term stay (ST-stay), LTC-stay and SNF-stay. LTC-stays are hospitalizations in certified long-term acute care hospitals, where beneficiaries may stay for more than 25 days on average. On the other hand, SNF-stays are hospitalizations that are longer than LTC-stays, where beneficiaries may stay up to 100 days. Since this analysis was focused on time to LTC/NH placement, only LTC-stay and SNF-stay variables were considered for analysis; ST-stay were not considered.
Statistical analysis
Baseline demographic characteristics such as sex, race/ethnicity, Elixhauser comorbidity index, other comorbidity status (i.e., dementia or insomnia) and concomitant PD medication use were described using frequencies and proportions. Age was described using mean, median, and standard deviation. Rates of all-cause LTCA, LTC-stay and SNF-stay were estimated as proportions. Differences in all-cause admissions between the groups were assessed using chi-square or Fisher's exact tests for categorical variables, t-tests for continuous variables that are normally distributed, and Wilcoxon rank-sum test for continuous variables that are not normally distributed.
Adjusted all-cause LTCA, LTC-stay, and SNF-stay rates between (i) PIM versus QUE, and (ii) PIM versus other-AAP matched cohorts were also compared using logistic regression models controlling for coexisting dementia, insomnia, and demographic characteristics as well as two additional logistic regression models controlling for additional variables such as region and index year, respectively. Time to all-cause SNF-stays, LTC-stays, and LTCA was assessed using mean (SD) and median (IQR) and risk of LTCA, SNF-stays and LTC-stays were compared using cox proportional hazards models for PIM-only versus QUE-only cohort controlling for demographics, 27 Elixhauser comorbidities, co-existing dementia, and co-existing insomnia. Hazard ratios (HR) and 95% confidence intervals (CIs) were estimated. All analyses were conducted using SAS 9.4® Enterprise Server via the CMS Virtual Research Data Center.
Results
Of 9652 beneficiaries on continuous monotherapy, 842 beneficiaries on PIM were matched 1:1 with those on QUE (Figure 1). Before matching, mean age of the beneficiaries in PIM was statistically lower compared with QUE (77 vs 78, p < 0.05). PIM group also had a significantly lower average comorbidity score (4.5 vs 4.2, p < 0.05), dementia (71.3% vs 84.4%, p < 0.05) and insomnia (29.2% vs 37.0%, p < 0.05) compared with QUE. After matching, distribution of age, gender, race and comorbidity score were balanced between groups. However, PIM had a significantly lower rate of dementia (71.3% vs 84.4%, p < 0.05) and insomnia (29.2% vs 37.0%, p < 0.05) compared with QUE, after matching. During post-index follow-up period, median daily dose of PIM and QUE was 34 mg (interquartile range [IQR] 34, 34) and 38 mg (IQR: 25, 50), respectively. Details about the demographic and baseline comorbidities for PIM and QUE, before and after PS matching are described in Tables 1 and 2.
| Unmatched PIM (n = 842) | Unmatched QUE (n = 7116) | p-value | SMD | Matched PIM (n = 842; 50%) | Matched QUE (n = 842; 50%) | p-value | SMD | |
|---|---|---|---|---|---|---|---|---|
| Age (years) | ||||||||
| Mean (SD) | 77.36 (7.2) | 78.06 (7.66) | <0.05 | 0.093 | 77.36 (7.2) | 77.4 (7.05) | NS | 0.005 |
| Median (IQR) | 77 (73, 82) | 78 (73, 83) | 77 (73, 82) | 77 (73, 82) | ||||
| Minimum, Maximum | 53, 98 | 41, 106 | 53, 98 | 53, 96 | ||||
| <65, n (%) | 24 (2.85%) | 247 (3.47%) | 24 (2.85%) | 23 (2.73%) | ||||
| 65–70, n (%) | 124 (14.73%) | 859 (12.07%) | 124 (14.73%) | 121 (14.37%) | ||||
| 71–75, n (%) | 188 (22.33%) | 1491 (20.95%) | 188 (22.33%) | 189 (22.45%) | ||||
| 76–80, n (%) | 238 (28.27%) | 1831 (25.73%) | 238 (28.27%) | 241 (28.62%) | ||||
| >80, n (%) | 268 (31.83%) | 2688 (37.77%) | 268 (31.83%) | 268 (31.83%) | ||||
| Sex, n (%) | NS | 0.024 | NS | 0.060 | ||||
| Female | 396 (47.03%) | 3262 (45.84%) | 396 (47.03%) | 371 (44.06%) | ||||
| Male | 446 (52.97%) | 3854 (54.16%) | 446 (52.97%) | 471 (55.94%) | ||||
| Race, n (%) | ||||||||
| Unknown | 11 (1.31%) | 64 (0.90%) | NS | 0.039 | 11 (1.31%) | † | <0.05 | 0.122 |
| White | 758 (90.02%) | 6332 (88.98%) | NS | 0.034 | 758 (90.02%) | 765 (90.86%) | NS | 0.028 |
| Black | 28 (3.33%) | 297 (4.17%) | NS | 0.045 | 28 (3.33%) | 29 (3.44%) | NS | 0.007 |
| Other | 17 (2.02%) | 108 (1.52%) | NS | 0.038 | 17 (2.02%) | 14 (1.66%) | NS | 0.027 |
| Asian | 14 (1.66%) | 153 (2.15%) | NS | 0.036 | 14 (1.66%) | 13 (1.54%) | NS | 0.009 |
| Hispanic | † | 141 (1.98%) | NS | 0.075 | † | 15 (1.78%) | NS | 0.060 |
| American Native | † | 21 (0.30%) | NS | 0.045 | † | † | NS | 0.016 |
| Geographic region, n (%) | ||||||||
| Midwest | 193 (22.92%) | 1720 (24.17%) | NS | 0.029 | 193 (22.92%) | 112 (13.3%) | <0.05 | 0.252 |
| Northeast | 165 (19.16%) | 1464 (20.57%) | NS | 0.024 | 165 (19.16%) | 398 (47.27%) | <0.05 | 0.614 |
| South | 326 (38.72%) | 2773 (38.97%) | NS | 0.005 | 326 (38.72%) | 256 (30.4%) | <0.05 | 0.175 |
| West | 158 (18.76%) | 1159 (16.29%) | NS | 0.065 | 158 (18.76%) | 76 (9.03%) | <0.05 | 0.284 |
| Elixhauser comorbidity score | ||||||||
| Mean (SD) | 4.12 (2.47) | 4.54 (2.81) | <0.05 | 0.024 | 4.12 (2.47) | 4.18 (2.52) | NS | 0.037 |
| Median (IQR) | 4 (2, 6) | 4 (2, 6) | 4 (2, 6) | 4 (2, 6) | ||||
| 0 | 304 (36.1%) | 1430 (20.10%) | 304 (36.1%) | 291 (34.56%) | ||||
| 1 | 59 (7.01%) | 562 (7.90%) | 59 (7.01%) | 63 (7.48%) | ||||
| 2–4 | 285 (33.85%) | 2758 (38.76%) | 285 (33.85%) | 278 (33.02%) | ||||
| 4–9 | 175 (20.78%) | 2003 (28.15%) | 175 (20.78%) | 193 (22.92%) | ||||
| ≥9 | 19 (2.26%) | 363 (5.10%) | 19 (2.26%) | 17 (2.02%) | ||||
| Movement disorder medication, n (%) | ||||||||
| Carbidopa | † | 68 (0.10%) | NS | † | † | NS | ||
| Levodopa | 0 (0%) | 0 (0%) | NS | 0 (0%) | 0 (0%) | NS | ||
| Carbidopa/Levodopa | 741 (88.0%) | 5745 (80.7%) | <0.05 | 741 (88.0%) | 677 (80.4%) | <0.05 | ||
| Other comorbidities, n (%) | ||||||||
| Dementia | 600 (71.26%) | 6004 (84.37%) | <0.05 | 600 (71.26%) | 715 (84.92%) | <0.05 | ||
| Insomnia | 246 (29.21%) | 2635 (37.03%) | <0.05 | 246 (29.21%) | 296 (35.15%) | <0.05 | ||
†
Cells with sample size of <11 are suppressed per CMS requirements.
PIM: Pimavanserin, QUE: Quetiapine, SD: Standard deviation; IQR: Inter-quartile range; SMD: Standardized mean difference; NS: Not significant.
| PIM (n = 842; %) | Unmatched QUE, (n = 7116; %) | SMD‡ | Matched QUE, (n = 842; %) | SMD§ | |
|---|---|---|---|---|---|
| Congestive heart failure | 59 (7.01%) | 805 (11.31%) | 0.15 | 69 (8.19%) | 0.045 |
| Cardiac arrhythmia | 114 (13.54%) | 1481 (20.81%) | 0.194 | 136 (16.15%) | 0.074 |
| Valvular disease | 50 (5.94%) | 569 (8%) | 0.081 | 61 (7.24%) | 0.053 |
| Pulmonary circulation disorder | 17 (2.02%) | 218 (3.06%) | 0.066 | 15 (1.78%) | 0.017 |
| Peripheral vascular disease | 116 (13.78%) | 1174 (16.5%) | 0.076 | 108 (12.83%) | 0.028 |
| Hypertension uncomplicated | 350 (41.57%) | 3969 (55.78%) | 0.287 | 355 (42.16%) | 0.012 |
| Hypertension complicated | 70 (8.31%) | 775 (10.89%) | 0.088 | 58 (6.89%) | 0.054 |
| Paralysis | † | 120 (1.69%) | 0.103 | 17 (2.02%) | 0.126 |
| Other neurological sisorders | 534 (63.42%) | 5301 (74.49%) | 0.241 | 531 (63.06%) | 0.007 |
| Chronic pulmonary sisease | 53 (6.29%) | 909 (12.77%) | 0.222 | 47 (5.58%) | 0.030 |
| Diabetes uncomplicated | 108 (12.83%) | 1348 (18.94%) | 0.168 | 128 (15.20%) | 0.068 |
| Diabetes complicated | 71 (8.43%) | 693 (9.74%) | 0.045 | 53 (6.29%) | 0.082 |
| Hypothyroidism | 102 (12.11%) | 1224 (17.20%) | 0.144 | 113 (13.42%) | 0.039 |
| Renal failure | 68 (8.08%) | 822 (11.55%) | 0.117 | 60 (7.13%) | 0.036 |
| Liver disease | † | 108 (1.52%) | 0.121 | † | 0.000 |
| Peptic ulcer disease excluding bleeding | † | 61 (0.86%) | 0.065 | † | 0.049 |
| Lymphoma | † | 59 (0.83%) | 0.013 | † | 0.000 |
| Metastatic cancer | † | 45 (0.63%) | 0.005 | † | 0.055 |
| Solid tumors without metastasis | 37 (4.39%) | 533 (7.49%) | 0.131 | 38 (4.51%) | 0.006 |
| Rheumatoid arthritis | 16 (1.90%) | 311 (4.37%) | 0.142 | 15 (1.78%) | 0.009 |
| Coagulopathy | 27 (3.21%) | 250 (3.51%) | 0.017 | 24 (2.85%) | 0.021 |
| Obesity | 26 (3.09%) | 344 (4.83%) | 0.09 | 37 (4.39%) | 0.069 |
| Weight loss | 41 (4.87%) | 578 (8.12%) | 0.132 | 59 (7.01%) | 0.091 |
| Fluid and electrolyte disorders | 102 (12.11%) | 1279 (17.97%) | 0.164 | 105 (12.47%) | 0.011 |
| Blood loss anemia | † | 83 (1.17%) | 0.061 | † | 0.052 |
| Deficiency anemia | 42 (4.99%) | 523 (7.35%) | 0.098 | 53 (6.29%) | 0.057 |
| Depression | 187 (22.21%) | 2258 (31.73%) | 0.216 | 196 (23.28%) | 0.026 |
†
Cells with sample size of <11 are suppressed per Centers for Medicare and Medicaid Services requirements.
‡
Compares QUE unmatched to PIM.
§
Compares matched QUE to matched PIM.
PIM: Pimavanserin; QUE: Quetiapine; SMD: Standardized mean difference.
There were fewer overall LTCA (23.2% vs 33.8%, p < 0.05) and SNF-stays (20.2% vs 31.4%, p < 0.05) for PIM versus QUE, respectively (Table 3). Time to overall LTCA was significantly greater for PIM versus QUE beneficiaries (149 days [IQR: 49–267] versus 105 days [IQR: 35–213], p < 0.05; hazard ratio [HR]: 0.80 [95% CI 0.66–0.97]) (Figure 2a). Median time to first SNF-stay was greater for PIM than QUE beneficiaries (142 days [IQR: 54–28] versus 99 days [IQR: 32–208], p < 0.05; HR: 0.78 [95% CI: 0.61–0.98]) (Figure 2c). Median time to LTC-stay for PIM was longer compared with QUE beneficiaries [130 days (IQR 49–266) vs 115 days (IQR: 54–230)], however, there was no statistical difference between the two groups (Table 3). Adjusted odds ratios from the logistic analyses for PIM versus QUE comparison, can be found in Table 4. Additionally, we conducted two post hoc sensitivity analyses controlling for region, insomnia and dementia and found odds ratios did not change much with the addition of region (odds ratio for overall LTCA [OR]: 0.71 [95% CI: 0.56–0.89]) and SNF-stay: 0.66 (95% CI: 0.52–0.84). Similarly, sensitivity analyses limiting the matched cohort to those with index year 1 January 2016 and onwards, adjusting region, index year, dementia and insomnia yielded lower OR estimates for PIM compared with QUE.
| PIM (n = 842) | QUE (n = 842) | p-value | |
|---|---|---|---|
| LTC admission | |||
| n (%) | 196 (23.2%) | 285 (33.8%) | <0.05 |
| Time to first admission | |||
| Mean days (SD) | 161 (113) | 141 (111) | |
| Median days (IQR) | 149 (49, 267) | 105 (35, 213) | <0.05 |
| LTC-stay | |||
| n (%) | 52 (6.2%) | 47 (5.6%) | NS |
| Time to first admission | |||
| Mean days (SD) | 157 (111) | 143 (102) | |
| Median days (IQR) | 130 (49, 266) | 115 (54, 230) | NS |
| SNF | |||
| n (%) | 170 (20.2%) | 265 (31.4%) | <0.05 |
| Time to first admission | |||
| Mean days (SD) | 165 (113) | 140 (111) | |
| Median days (IQR) | 142 (54, 248) | 99 (32, 208) | <0.05 |
PIM: Pimavanserin, QUE: Quetiapine, SD: Standard deviation; IQR: Inter-quartile range; SNF: Skilled nursing facility; LTC: Long-term care; NS: Not significant.
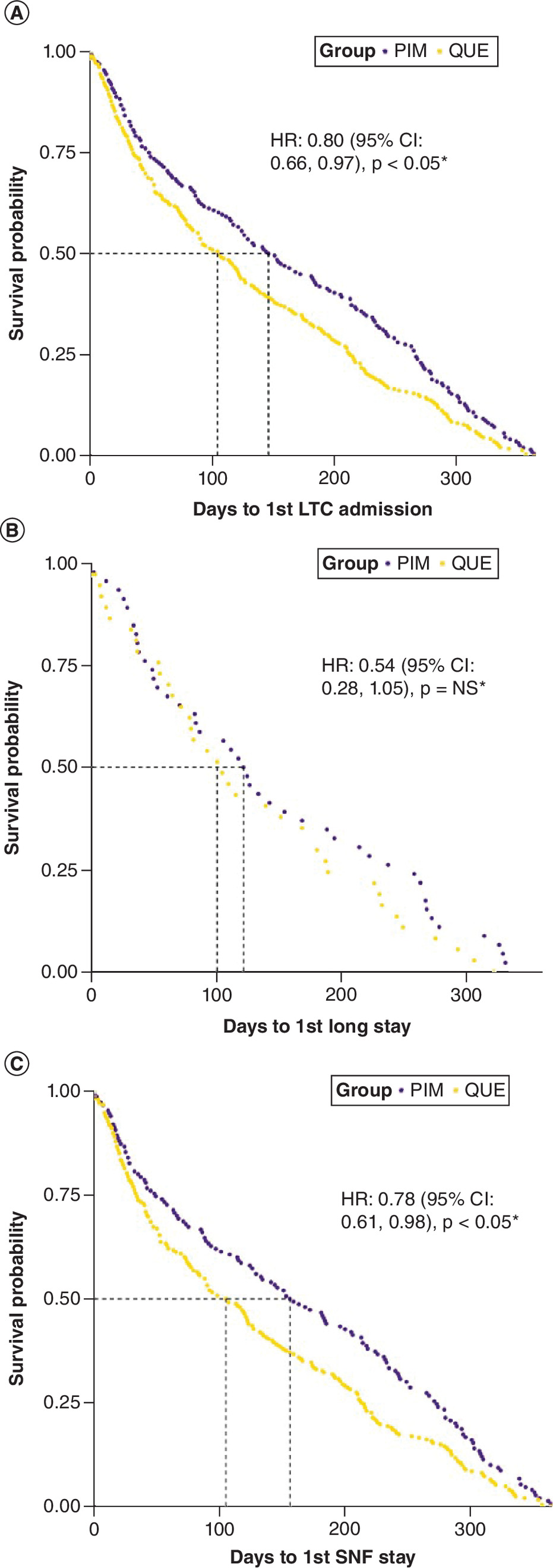
Figure 2. Kaplan–Meier survivor curves.
(A) Kaplan–Meier survivor curve of time to overall LTC admission for PIM vs QUE patients. (B) Kaplan–Meier survivor curve of time to Long-term stay for PIM vs QUE patients. (C) Kaplan–Meier survivor curve of time to SNF stay for PIM vs QUE patients.
CI: Confidence interval; HR: Hazard ratio; LTC: Long-term care; PIM: Pimavanserin; QUE: Quetiapine; SNF: Skilled nursing facility.
| OR (95% Cl)‡ | p-value | OR (95% Cl)§ | p-value | OR (95% Cl)¶ | p-value | |
|---|---|---|---|---|---|---|
| LTC Admission | 0.65 (0.53, 0.81) | <0.05 | 0.71 (0.56, 0.89) | <0.05 | 0.61 (0.46, 0.8) | <0.05 |
| LTC-Stay | 1.14 (0.76, 1.73) | NS | 1.10 (0.71, 1.69) | NS | 1.14 (0.67, 1.94) | NS |
| SNF | 0.61 (0.49, 0.77) | <0.05 | 0.66 (0.52, 0.84) | <0.05 | 0.57 (0.43, 0.75) | <0.05 |
†
Reference is Quetiapine.
‡
Model is adjusted for dementia and insomnia.
§
Model is adjusted for dementia, insomnia, and region.
¶
Model is adjusted for dementia, insomnia, region, and index year (Sample is limited to those with index year after Jan 1, 2016; N = 1317).
PIM: Pimavanserin, QUE: Quetiapine; SNF: Skilled nursing facility; LTC: Long-term care; NS: Not significant; CI: Confidence Interval; OR: Odds Ratio.
A secondary analysis for differential risks of long-term care admissions comparing PIM to other-AAPs was also conducted. In a cohort of 842 beneficiaries on PIM were matched 1:1 with those treated with other-AAPs. All-cause SNF-stay (20.2% vs 31.7%, p < 0.05) and overall LTCA rates (23.2% vs 34.6%, p < 0.05) were statistically lower for beneficiaries on PIM compared with other-AAPs. However, there was no statistical difference in time to LTC-stay, SNF-stay, or overall LTCA for PIM compared with other-AAP beneficiaries (Supplemental Table 2).
Discussion
This analysis examined the differential 12-month risk of all-cause long-term care admissions (LTCA), defined as either LTC-stay or SNF-stay, among beneficiaries with PDP treated with either PIM or QUE. In particular, the study examined the rates of LTCA and time to LTCA. Results suggest that PIM beneficiaries had lower rates of LTCA compared with QUE beneficiaries. Specifically, PIM beneficiaries had significantly lower SNF-stays compared with QUE. Median time to LTCA for PIM beneficiaries was also 44 days longer as compared with QUE. Additionally, a secondary analysis examining these differences between PIM versus other-AAPs also showed fewer SNF-stays among beneficiaries treated with PIM. It is unclear why beneficiaries treated with PIM have significantly fewer SNF-stays and lower overall LTC-admissions compared with QUE beneficiaries or those treated with other-AAPs including QUE. Future research is needed to examine the predictors of LTCA, SNF-stay, and LTC-stays and the potential association between incidence of falls and fractures and subsequent NH/LTC placement among beneficiaries treated with PIM versus QUE-only or other-AAPs. While no head-to-head comparative clinical trials of PIM versus QUE or other-AAPs exist, systematic reviews from indirect comparisons of PIM versus QUE from the literature suggest that PIM may be associated with greater degree of reduction in hallucinations and delusions [22,23]. Evidence from a recently published systematic review and network meta-analysis of atypical antipsychotics used to treat beneficiaries with PDP also showed that PIM and clozapine significantly improved symptoms without affecting motor function compared with other AAPs [24]. While these results are not intended to establish causation, they lend support to the American Geriatrics Society (AGS) and the Movement Disorder Society (MDS) expert panel recommendations to use PIM for the treatment of PDP symptoms [25,26]. It should be noted that, to date, PIM remains the only FDA-approved AAP for the treatment of hallucinations and delusions related to PDP.
Since beneficiaries with PDP that are treated with AAPs compared with PIM may have higher mortality rates, the study aimed toward removing the bias of competing mortality risk that may favor PIM. It should be noted that potentially biased reports from consumer watchdogs (e.g., Institute for Safe Medical Practices) and the popular press, as well as a study comparing 1-yr mortality rates among beneficiaries on PIM versus no treatment for PD psychosis reported increased rates for death [27,28]. However, recent publications have consistently reported lower risk of mortality with PIM versus QUE or other-AAPs [29–31]. Therefore, to avoid any systematic bias that can favor PIM due to its potential lower mortality risk, all eligible beneficiaries in the cohorts were required to have 12 months of continuous monotherapy treatment to eliminate the competing risk of mortality among these beneficiaries.
Rates of LTC-stay were numerically lower in PIM versus QUE or other-AAP cohorts; with overall LTC-stay rates being low in general for all cohorts compared with SNF-stay rates. These results suggest that PDP beneficiaries in general may have greater number of SNF-stays (i.e., stays as high as 100 days) compared with LTC-stays that last fewer than 25 days. The study has limitations that are common to all administrative claims database analyses. Any secondary data, including administrative claims data, may contain coding errors, missed claims, bias introduced by omission of variables, and these should be considered as limitations to these data. Identification of psychosis was based on a diagnosis of psychosis-related hallucinations and delusions, as no diagnostic code for PDP exists. Accordingly, it is likely that PDP diagnosis is underestimated. While the study addressed potential confounding issues through appropriate matching and covariate adjustment, residual confounding may exist.
Conclusion
In this analysis, PDP beneficiaries initiated on PIM monotherapy had 10% lower LTC-admission rates as compared with QUE cohort. SNF-stays were 11% lower for PIM beneficiaries as compared with QUE beneficiaries. Beneficiaries receiving PIM monotherapy also had a 20% lower LTC-admission risk than QUE. Published research suggests that odds of LTC/NH admission may be 16-times higher among PDP beneficiaries compared with PD-only beneficiaries [5]. These results, while not causal in nature, may provide early insights about a potential association between PIM use and lowered risk of LTC/NH placements among PDP beneficiaries in real world community settings.
Since LTC/NH placement are often known to increase the rates of stroke, falls, fractures and premature deaths, it is expected that delaying nursing home placement can improve the healthcare quality of patients [5,7–10,28–31]. Additionally, LTC/NH placement also imposes significant informal cost burden due to increased caregiving burden among family and friends, as well as the burden on NH/LTC staff members. Furthermore, NH placement may significantly increase the economic burden of an already costly condition such as PDP, potential cost savings of delayed LTC/NH stays and associated rehabilitation and residential care costs among patients may be significant. Given that patients with PDP have a higher risk of LTC/NH placement. Given that PIM delays LTC/NH placement among Medicare beneficiaries in this analysis, it may play an important public health role in improving healthcare quality of PDP patients while lowering costs of care.
Summary points
•
A major concern among patients with Parkinson's disease psychosis (PDP) is risk of long-term care (LTC) admission (LTCA) when prescribing off-label atypical antipsychotics.
•
We analysed Parts A, B and D claims (100% Medicare sample; 2013–2019) of PDP patients initiating continuous pimavanserin or quetiapine monotherapy.
•
Outcome assessments included risk of all-cause skilled nursing facility stays (SNF-stays), LTC-stays, and overall LTCA (i.e., SNF-stays or LTC-stays).
•
Of the matched pimavanserin versus quetiapine (n = 842 for each group) patients from total sample (n = 9652) formed the cohort.
•
Overall, all-cause LTCA rates were 23.2% for patients with pimavanserin and 33.88% for patients with quetiapine which is statistically significant.
•
SNF-stay rates for pimavanserin patients were 20.2% whereas, 31.4% were reported by patients who were on quetiapine which is statistically significant.
•
Hazard ratio (95% CI) for risk of SNF-stay and overall LTCA was 0.78 (0.61, 0.98) and 0.80 (0.66, 0.97), respectively, for pimavanserin versus quetiapine patients (p < 0.05).
•
In conclusion, pimavanserin patients had 10% lower all-cause LTCA and 20% lower risk of LTCA than patients with quetiapine.
Author contributions
K Rajagopalan, N Rashid and D Doshi were responsible for study conception and design; K Rajagopalan was responsible for acquisition of data; K Rajagopalan, N Rashid and D Doshi were responsible for data analysis, and drafting and revision of the manuscript.
Acknowledgments
D Gopal, an employee of Anlitiks Inc., conducted parts of the analysis and provided medical writing and editorial support for the manuscript. SS Syed, an employee of Anlitiks Inc., provided editorial support for the manuscript.
Financial disclosure
This study was financially sponsored by Acadia Pharmaceuticals. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
K Rajagopalan is a current employee of Anlitiks Inc., a company that received funding from Acadia Pharmaceuticals to conduct this study. N Rashid and D Doshi are employees of Acadia Pharmaceuticals. The authors have no other competing interests or relevant affiliations with any organization/entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 466.21 KB
References
Papers of special note have been highlighted as: • of interest
1.
Willis AW, Roberts E, Beck JC et al. Incidence of Parkinson disease in North America. NPJ Parkinsons Dis. 8(1), 170 (2022).
2.
Factor SA, Scullin MK, Sollinger AB et al. Cognitive correlates of hallucinations and delusions in Parkinson's disease. J. Neurol. Sci. 347(1–2), 316–321 (2014).
3.
Marras C, Beck JC, Bower JH et al. Prevalence of Parkinson's disease across North America. NPJ Parkinsons Dis. 4, 21 (2018).
4.
Aarsland D, Larsen JP, Tandberg E, Laake K. Predictors of nursing home placement in Parkinson's disease: a population-based, prospective study. J. Am. Geriatr. Soc. 48(8), 938–942 (2000).
• In this prospective study, researchers investigated the factors contributing to institutionalization in patients with Parkinson's disease. They found that both motor and neuropsychiatric symptoms played a role in the need for institutionalization, however, presence of hallucinations emerged as the most influential predictor. These findings indicate treating hallucinations may potentially decrease the likelihood of institutionalization in individuals with Parkinson's disease.
5.
Goetz CG, Stebbins GT. Risk factors for nursing home placement in advanced Parkinson's disease. Neurology 43(11), 2227–2229 (1993).
6.
Safarpour D, Thibault DP, DeSanto CL et al. Nursing home and end-of-life care in Parkinson disease. Neurology 85(5), 413–419 (2015).
7.
Akbar U, Friedman JH. Long-term outcomes with pimavanserin for psychosis in clinical practice. Clin. Park. Relat. Disord. 6, 100143 (2022).
8.
Hermanowicz N, Edwards K. Parkinson's disease psychosis: symptoms, management, and economic burden. Am. J. Manag. Care. 21(Suppl. 10), S199–S206 (2015).
• In this review article, authors talk about Parkinson's disease psychosis (PDP) as a costly and debilitating condition that often develops several years after the initial diagnosis of Parkinson's disease (PD). Patients with PDP experience higher healthcare expenditures, particularly in long-term care, skilled nursing facilities, and inpatient settings, compared to patients with PD without psychosis.
9.
Ballard C, Cream J. Drugs used to relieve behavioral symptoms in people with dementia or an unacceptable chemical cosh? Argument. Int. Psychogeriatr. 17(1), 4–29 (2005).
10.
Layton JB, Forns J, Turner ME et al. Falls and fractures in patients with Parkinson's disease-related psychosis treated with pimavanserin vs atypical antipsychotics: a cohort study. Drugs Real World Outcomes. 9(1), 9–22 (2022).
• This study focused on a cohort of patients with Parkinson's disease-related psychosis (PDP) and aimed to evaluate the risk of falls and fractures associated with the use of pimavanserin compared to other antipsychotics. The results indicate that there is no evidence suggesting an increased risk of falls or fractures with pimavanserin use in PDP patients, sensitivity analyses even suggest a decreased risk.
11.
Weintraub D, Chiang C, Kim HM et al. Association of antipsychotic use with mortality risk in patients with Parkinson disease. JAMA Neurol. 73(5), 535–541 (2016).
12.
Acadia Pharmaceuticals. Nuplazid® (Pimavanserin) Prescribing Information. Acadia Pharmaceuticals Inc, CA, USA (2018).
13.
Markham A. Pimavanserin: first global approval. Drugs 76(10), 1053–1057 (2016).
14.
Cummings J, Isaacson S, Mills R et al. Pimavanserin for patients with Parkinson's disease psychosis: a randomized, placebo-controlled Phase 3 trial [published correction appears in Lancet 384(9937), 28 (2014)]. Lancet. 383(9916), 533–540 (2014).
15.
Mansuri Z, Reddy A, Vadukapuram R, Trivedi C, Amara A. Pimavanserin in the treatment of Parkinson's disease psychosis: meta-analysis and meta-regression of randomized clinical trials. Innov. Clin. Neurosci. 19(1–3), 46–51 (2022).
• In this meta-analysis revealed that patients with Parkinson's disease (PD) experienced a notable enhancement in psychosis symptoms when treated with pimavanserin. Additionally, pimavanserin demonstrated a protective effect against orthostatic hypotension in PD patients.
16.
Rajagopalan K, Rashid N, Kumar S, Doshi D. Health care resource utilization patterns among patients with Parkinson's disease psychosis: analysis of Medicare beneficiaries treated with pimavanserin or other-atypical antipsychotics. J. Med. Econ. 26(1), 34–42 (2023).
17.
Sewell DD, Jeste DV, Atkinson JH et al. HIV-associated psychosis: a study of 20 cases. Am. J. Psychiatry 151(2), 237–242 (1994).
18.
Beckett MK, Collins RL, Burnam MA et al. Mental health and substance abuse issues among people with HIV. Lessons from HCSUS www.rand.org/pubs/research_briefs/RB9300.html (2007).
19.
Substance Abuse and Mental Health Services Administration. Co-occurring disorders and other health conditions. www.samhsa.gov/medication-assisted-treatment/medications-counseling-related-conditions/co-occurring-disorders (2022).
20.
Sterling S, Chi F, Hinman A. Integrating care for people with co-occurring alcohol and other drug, medical, and mental health conditions. Alcohol Res. Health. 33(4), 338–349 (2011).
21.
Performing a 1: N case-control match on propensity score [computer program]. SAS Institute, Montreal, Canada (2004).
22.
Zhang H, Wang L, Fan Y et al. Atypical antipsychotics for Parkinson's disease psychosis: a systematic review and meta-analysis. Neuropsychiatr. Dis. Treat. 15, 2137–2149 (2019).
• In this systematic review and Meta-analysis, Pimavanserin has been found to be effective in treating Parkinson's disease-related psychosis (PDP). While clozapine is also recommended for PDP treatment, caution is advised due to its associated side effects, and further well-designed randomized controlled trials are needed to confirm and update the findings.
23.
Yunusa I, Rashid N, Demos GN, Mahadik BS, Abler VC, Rajagopalan K. Comparative outcomes of commonly used off-label atypical antipsychotics in the treatment of dementia-related psychosis: a network meta-analysis. Adv. Ther. 39(5), 1993–2008 (2022).
24.
Yunusa I, Rashid N, Seyedin R, Paratane D, Rajagopalan K. Comparative efficacy, safety, and acceptability of pimavanserin and other atypical antipsychotics for Parkinson's disease psychosis: systematic review and network meta-analysis. J. Geriatr. Psychiatry Neurol. 36(5), 417–432 (2023).
25.
American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American Geriatrics Society 2015 updated Beers criteria for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 63(11), 2227–2246 (2015).
26.
Seppi K, Ray Chaudhuri K, Coelho M et al. Update on treatments for nonmotor symptoms of Parkinson's disease-an evidence-based medicine review [published correction appears in Mov. Disord. 34(5), 765 (2019)]. Mov. Disord. 34(2), 180–198 (2019).
27.
Schneider LS. The safety of pimavanserin for Parkinson's disease and efforts to reduce antipsychotics for people with dementia. Am. J. Psychiatry 179(8), 519–521 (2022).
28.
Hwang YJ, Alexander GC, An H, Moore TJ, Mehta HB. Risk of hospitalization and death associated with pimavanserin use in older adults with Parkinson disease. Neurology 97(13), e1266–e1275 (2021).
29.
Mosholder AD, Ma Y, Akhtar S et al. Mortality among Parkinson's disease patients treated with pimavanserin or atypical antipsychotics: an observational study in Medicare beneficiaries. Am. J. Psychiatry 179(8), 553–561 (2022).
• This is a retrospective cohort study of Medicare recipients, where researchers found Pimavanserin was linked to lower mortality rates compared to the use of atypical antipsychotics within the initial 180 days of treatment. However, this association was observed only in patients living in the community and not among those residing in nursing homes.
30.
Brown JD, Cicali B, Henriksen C, Malaty I, Okun MS, Armstrong MJ. Comparative pharmacovigilance assessment of mortality with pimavanserin in Parkinson disease-related psychosis. J. Manag. Care Spec. Pharm. 27(6), 785–790 (2021).
31.
Rissardo JP, Durante Í, Sharon I, Fornari Caprara AL. Pimavanserin and Parkinson's disease psychosis: a narrative review. Brain Sci. 12(10), 1286 (2022).
Information & Authors
Information
Published In
Copyright
© 2023 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 6 July 2023
Accepted: 22 November 2023
Published online: 15 December 2023
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Risk of long-term care admissions among Medicare beneficiaries treated with pimavanserin or quetiapine for Parkinson's disease psychosis in USA: a retrospective administrative claims database analysis. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0114
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Nazia Rashid, Krithka Rajagopalan, Daksha Gopal, Lambros Chrones, Dilesh Doshi, mpact of Early Treatment with Pimavanserin on Healthcare Resource Utilization Among Newly Diagnosed Patients with Parkinson’s Disease Psychosis: A Pre-Post Medicare Claims Database Analysis, Journal of Health Economics and Outcomes Research, 10.36469/jheor.2026.154805, (1-9), (2026).
- Nazia Rashid, Krithika Rajagopalan, Daksha Gopal, Lambros Chrones, Dilesh Doshi, Impact of Early Treatment with Pimavanserin on Healthcare Resource Utilization Among Newly Diagnosed Patients with Parkinson’s Disease Psychosis: A Pre-Post Medicare Claims Database Analysis, Journal of Health Economics and Outcomes Research, 10.36469/001c.154805, 13, 1, (2026).
- Nazia Rashid, Ismaeel Yunusa, Dilesh Doshi, Vinod Yakkala, Daksha Gopal, Victor Abler, Krithika Rajagopalan, Real-world evidence of pimavanserin utilization among patients with Parkinson’s disease psychosis: a review of real-world data that augments data from randomized controlled trials, Journal of Comparative Effectiveness Research, 10.57264/cer-2025-0129, 14, 12, (2025).
- Krithika Rajagopalan, Daksha Gopal, Lambros Chrones, Dilesh Doshi, Nazia Rashid, Healthcare resource utilization patterns among patients with Parkinson’s disease psychosis and dementia: analysis of US Medicare beneficiaries treated with pimavanserin versus other-atypical antipsychotics or versus quetiapine, Journal of Medical Economics, 10.1080/13696998.2025.2487358, 28, 1, (556-566), (2025).
- Stuart H. Isaacson, Henry Nasrallah, Rajesh Pahwa, Gustavo Alva, Daniel Kremens, Stephen M. Stahl, Management of Parkinson’s disease psychosis: first-line antipsychotic selection and rationale for continuing, combining, or switching, Expert Opinion on Pharmacotherapy, 10.1080/14656566.2025.2481205, 26, 6, (707-717), (2025).
- Jianhong Wu, Xin Jin, Weiming Xie, Liang Liu, Fei Wang, Ling Zhu, Yuan Shen, Linghe Qiu, Global research trends and hotspots in Parkinson’s disease psychosis: a 25-year bibliometric and visual analysis, Frontiers in Aging Neuroscience, 10.3389/fnagi.2024.1480234, 16, (2024).