Increasing transparency in indirect treatment comparisons: is selecting effect modifiers the missing part of the puzzle? A review of methodological approaches and critical considerations
Publication: Journal of Comparative Effectiveness Research
Abstract
Failure to adjust for effect modifiers (EMs) in indirect treatment comparisons (ITCs) can produce biased and uncertain effect estimates. This is particularly important for health technology assessments (HTAs), where the availability of new treatments is based on comparative effectiveness results. Much emphasis has been placed on advancing ITC methods to adjust for EMs, yet whether EMs are appropriately identified for the conduct of ITCs in the first place is unclear. To understand the extent of guidance and requirements for the selection of EMs for ITCs currently available and if and how this guidance is applied in practice, a series of pragmatic reviews of guidance documents from HTA and non-payer organizations, primary published ITC analyses, and prior HTA submissions in two indications (non-small cell lung cancer and psoriasis) was conducted. The reviews showed that current ITC guidance mainly focused on developing analytical methods to adjust for EMs. Some organizations, such as HTA bodies in the UK, France and Germany, recommended the use of literature reviews, expert opinion and statistical methods to identify EMs. No detailed guidance on the selection process or the appropriate literature review approach was found. Similar trends were identified through the database search and review of prior HTA submissions; only few published ITCs and submissions included information on the EM selection process which was either based on findings from the literature, trial subgroup analyses, or clinical input. No reference to a systematic selection approach was found.
There is an urgent need to fill the guidance gap identified across the reviews by including a step in ITC guidelines on how EMs should be identified through systematic reviews, formal expert elicitation, and a quantitative assessment of the EM distribution. Researchers and manufacturers are also encouraged to improve transparent reporting and justification of their selection of EMs to allow for an independent review of the set of factors being considered for adjustment. Both will contribute toward reducing bias in the ITC results and ultimately increase confidence in decision-making.
Tweetable abstract
The lack of guidance on how to identify effect modifiers (EM) for indirect treatment comparisons (ITC) in health technology assessments (HTA) led to a considerable underreporting of the EM selection process in published ITCs and HTA submissions. Further HTA guidance is needed.
Plain language summary
Certain variables that can affect the outcomes of new therapies must be accounted for to avoid bias when comparing the effectiveness of new and existing treatments. This is especially important in indirect treatment comparisons that are included in submissions to agencies which recommend whether a medicine should be financed through the local healthcare system. Previous research has focused on how to adjust for these variables to create an unbiased evaluation, but little information exists on how to appropriately identify them in the first place. A review of guidance documents from reimbursement bodies and other relevant publications demonstrated that there was no detailed guidance on the selection process or a systematic approach to handle this issue. These findings highlight an urgent need to develop guidance that will reduce bias in indirect treatment comparisons and increase confidence in the evidence needed to make new therapies available to the public.
Producing unbiased comparative treatment effect estimates on the clinical performance of health technologies under assessment is the cornerstone of healthcare decision-making. The reimbursement assessment of a new technology is based on the appraisal of its value in terms of improving clinical (and cost-) effectiveness outcomes in comparison with other relevant treatments currently used in clinical practice.
When the clinical evidence base for a new health technology is obtained from randomized clinical trials, the direct comparisons to all available treatments reflecting clinical practice and thus relevant to the health technology assessment (HTA) decision problem are rarely available. Therefore, indirect treatment comparisons (ITCs) such as network meta-analyses (NMAs) and population-adjusted indirect comparison (PAIC) methods have been developed to establish the relative clinical effectiveness of new technologies using aggregated or individual patient data, respectively [1,2].
Central to the planning and execution of ITCs based on aggregated trial data is a deliberation whether effect-modifying variables (EMs) differ between studies. EMs (also known as predictive variables) are covariates that can alter the effect of treatment as measured on a given scale [2,3]. EMs are distinguished from prognostic variables (PV) although the terms are sometimes incorrectly used interchangeably [2,4]. For clarity, PVs are covariates that affect the outcome, irrespective of treatment, and therefore do not interfere with the relative treatment effect estimates as calculated in ITCs. Any evidence of effect modification or absence of trial data on known EMs may lead to biased or uncertain results in comparative treatment effects that can ultimately affect the confidence in decision-making [5,6]. Likewise, adjusting for factors that are not actually EMs for a specific outcome can unnecessarily increase uncertainty [2,7]. This is because the loss of effective sample size due to (over) adjustment for additional factors inherently reduces the precision around the results [8,9].
Against that background, it is important to employ a robust approach for identifying whether and which EMs are critical for inclusion in ITCs given their weight in the validity of analyses results. This review aimed to identify and categorize the methodological approaches of identifying EMs in ITCs both from an HTA requirement standpoint and their use in practice, by summarizing related evidence from three sources: existing guidance by HTA bodies and other organizations, primary research from published literature and HTA submissions in two specific disease areas.
Methods
A series of comprehensive (pragmatic) reviews was conducted to determine what guidance is available for the appropriate identification and selection of EMs when conducting ITCs and how this guidance has been applied in practice; the review included guidance documents from HTA bodies and non-payer organizations, published ITCs and prior HTA submissions in key representative indications. The review focused on how EMs are identified and was not intended to summarize the methodologies used to adjust for EMs. The reviews were restricted to articles in English; however, no geographic restrictions were otherwise applied. The searches of published ITCs and HTA submission documents were also restricted to those published since 2015 and 2017, respectively. This is because one of the key guidance documents in this area – the National Institute for Health and Care Excellence (NICE) Decision Support Unit (DSU) Document 18 – was first published in December 2016, highlighting the relatively recent focus on more advanced methods to adjust for EMs in the context of ITCs [2].
Searches were first conducted in November 2021 and updated in February 2023 across HTA bodies, non-payer organizations and literature databases (Embase and MEDLINE via Ovid SP; Supplementary Table 1) to describe the requirements for the selection of EMs for ITCs and how this was applied in ITCs subsequently published in peer-reviewed journals. Articles on NMA/ITCs identified through the database searches that did not explicitly refer to these concepts in title or abstract were not selected further. Conference abstracts, letters, editorials, or narrative reviews were excluded. Furthermore, pairwise meta-analyses or publications on statistical methods for the adjustment of EMs were not considered. Overview of reviews (also called umbrella reviews) were not considered as they typically do not provide the breadth of information to allow elaboration of issues around EM selection and we considered that any relevant primary ITCs would have already been identified by the literature searches.
The websites of NICE and the Canadian Agency for Drugs and Technologies in Health (CADTH) were reviewed for submissions in non-small cell lung cancer (NSCLC) and psoriasis – an oncology indication and a chronic disease with rapidly changing treatment landscapes – as example case studies to identify how EMs and PVs (given that these terms are frequently used interchangeably) were identified and selected in the context of ITCs for the reimbursement of pharmaceuticals. The search was restricted to NICE and CADTH as other HTA bodies usually only publish submission summaries, which did not provide sufficient information for the purpose of the current review (Supplementary Table 2). Only the latest version of each submission or re-submission was included. Terminated appraisals were not considered.
The reviews were supplemented by Google searches and a snowballing approach using the identified articles. Information on the search strategies is provided in the online appendix.
All screening was conducted by one researcher, with a second, more senior researcher conducting quality assurance checks. The final list of records informing this publication was agreed through discussions among the researchers. Information from the relevant documents was extracted into pre-defined data extraction sheets specifically designed for each review type. All extractions were validated by a second researcher.
Themes across these publications were summarized qualitatively with the aim to identify relevant topics in individual documents and provide a critical assessment of proposed selection approaches for EMs in the context of ITCs for healthcare decision-making.
Results
Guidance documents from HTA bodies & non-payer organizations
The searches identified 15 relevant guidance documents and methods manuals across six HTA bodies (NICE, CADTH, Institute for Quality and Efficiency in HealthCare [IQWiG]/Federal Joint Committee [G-BA], Haute Autorité de Santé [HAS], Pharmaceutical Benefits Advisory Committee [PBAC], and the Institute for Clinical and Economic Review [ICER]) and three non-payer organizations that referred to the role of EMs and their potential impact on the validity of ITC analysis results. Six documents (one each from the NICE DSU [10], IQWiG [11], CADTH, The Professional Society for Health Economics and Outcomes Research [ISPOR] [12], Cochrane [13] and ICER [14]) focused on statistical methods to address EMs when conducting ITCs but did not provide guidance on how these variables should be systematically and comprehensively identified. The remaining nine documents (six were published by four different HTA agencies including NICE [2,15,16], G-BA [17], HAS [18], and PBAC [19], and three were from the non-payer organizations ISPOR [20] and Preferred Reporting Items for Systematic Reviews and Meta-Analyses group [21,22]) provided some guidance on the topic of EM selection. A full description of individual documents is presented in Table 1.
| Organization | Title of guidance document | Year of publication | Specific guidance on how to identify EM? | Key findings | Ref. |
|---|---|---|---|---|---|
| HTA body | |||||
| NICE DSU | TSD 18: Methods for population-adjusted indirect comparisons in submissions to NICE | 2016 | Yes | Reference to the manual of health technology evaluations, which states that a thorough review of the subject area or discussion with clinical experts is needed. | [2] |
| NICE DSU | TSD 7: Evidence synthesis of treatment efficacy in decision making: a reviewer's checklist | 2012 | Yes | Checklist for evidence synthesis of treatment efficacy (question on whether EMs were identified through a literature review, and whether differences in patient populations were accounted for). | [15] |
| NICE DSU | TSD 3: Heterogeneity: subgroups, meta-regression, bias and bias-adjustment | 2012 | No (guidance on how to address the presence of EMs) | Guidance focuses on the adjustment for EMs. No information on how EMs should be identified or selected. | [10] |
| NICE | NICE health technology evaluations: the manual | 2022 | Yes | Potential EMs should be identified before data analysis through a review of the subject area or discussion with experts in the clinical discipline. | [16] |
| G-BA | Dossier zur Nutzenbewertung gemäß § 35a SGB V (dossier for benefit assessment) | 2019 | Yes | Potential EMs should be investigated through homogeneity or interaction tests based on regression analyses. Subgroup analyses using IPD are preferred. If clinically plausible, the following factors should be investigated: sex, age, disease severity or stage, geography, single- vs multi-centre studies. All a priori-defined subgroup analyses should also be considered. No further information on how EMs should be selected. | [17] |
| HAS | Indirect comparisons methods and validity | 2009 | Yes | Interaction covariables should be identified through subgroup analyses conducted in the relevant clinical trials and interaction tests. | [18] |
| PBAC | Guidelines for preparing a submission to the Pharmaceutical Benefits Advisory Committee (v5) | 2016 | Yes | Differences in factors violating the transitivity assumption should be investigated qualitatively and quantitatively. No guidance on how these factors should be (systematically) identified. | [19] |
| ICER | 2020–2023 Value Assessment Framework | 2020 | No (guidance on how to address the presence of EMs) | The document states that in some cases, factors are known to account for EMs. The framework also states that ICER will consider EMs in the discussion. No formal guidance on how EMs should be identified is given. | [14] |
| IQWiG | General methods (v6.1) | 2022 | No (guidance on how to address the presence of EMs) | No guidance on how EMs should be systematically identified. Guidance given on how subgroup analyses should be conducted, especially in the presence of multiple EMs. | [11] |
| CADTH | Procedures for CADTH Reimbursement Reviews [Sponsor Summary of Clinical Evidence Template] | 2023 | No (only top-level guidance available) | Potential EMs should be identified before data analysis. No clear guidance on how EMs should be identified. | [45] |
| Non-payer organizations | |||||
| ISPOR Task Force | Interpreting Indirect Treatment Comparisons and Network Meta-Analysis for HealthCare Decision Making: Report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: Part 1 | 2011 | Yes | Simplified checklist to assist decision-makers in evaluating a reported NMA. The NMA publication should include a table or list of studies with information regarding study design and patient characteristics that might act as EMs. | [20] |
| ISPOR Task Force | Conducting Indirect-Treatment-Comparison and Network-Meta-Analysis Studies: Report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: Part 2 | 2011 | No (guidance on how to address the presence of EMs) | No guidance on how EMs should be identified. | [12] |
| PRISMA group | Preferred Reporting Items for a Systematic Review and Meta-analysis of Individual Participant Data: The PRISMA-IPD Statement | 2015 | Yes | Checklist for SLRs and MAs of IPD that includes an item on the identification of potential EMs. | [22] |
| PRISMA group | The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-analyses of HealthCare Interventions: Checklist and Explanations | 2015 | Yes | Guidance document on how NMAs should be reported. Recommendations across various items to report collected data on EMs (including from additional sources). No clear guidance on how EMs should be identified. | [21] |
| Cochrane group | Cochrane Handbook for Systematic Reviews of Interventions | 2022 (access date) | No (guidance on how to address the presence of EMs) | Characteristics used for subgroup analyses or meta-regression should be pre-specified in the protocol. No clear guidance on how EMs should be identified. | [13] |
CADTH: Canadian Agency for Drugs and Technologies in Health; DSU: Decision Support Unit; EM: Effect modifier; G-BA: Gemeinsamer Bundesausschuss (Federal Joint Committee); HAS: Haute Autorité de Santé; HTA: Health technology assessment; ICER: Institute for Clinical and Economic Review; IPD: Individual patient data; IQWiG: Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen (Institute for Quality and Efficiency in HealthCare); ISPOR: The Professional Society for Health Economics and Outcomes Research; MA: Meta-analysis; NICE: National Institute for Health and Care Excellence; NMA: Network meta-analysis; PBAC: Pharmaceutical Benefits Advisory Committee; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SGB: Sozialgesetzbuch (social code); SLR: Systematic literature review; TSD: Technical support document.
Across the HTA guidance documents, two main themes were identified regarding the identification of EMs for ITCs (Figure 1).
•
•
An assessment is needed whether pre-selected factors are acting as EMs in specific ITC scenarios using quantitative methods such as homogeneity or interaction tests (G-BA [17] and HAS [18]), subgroup analyses of relevant clinical trials (HAS [18] and NICE [2]), or quantitative or qualitative assessments of the transitivity assumption, that is, there are no considerable differences in the distribution of EMs across trials (PBAC [19]).
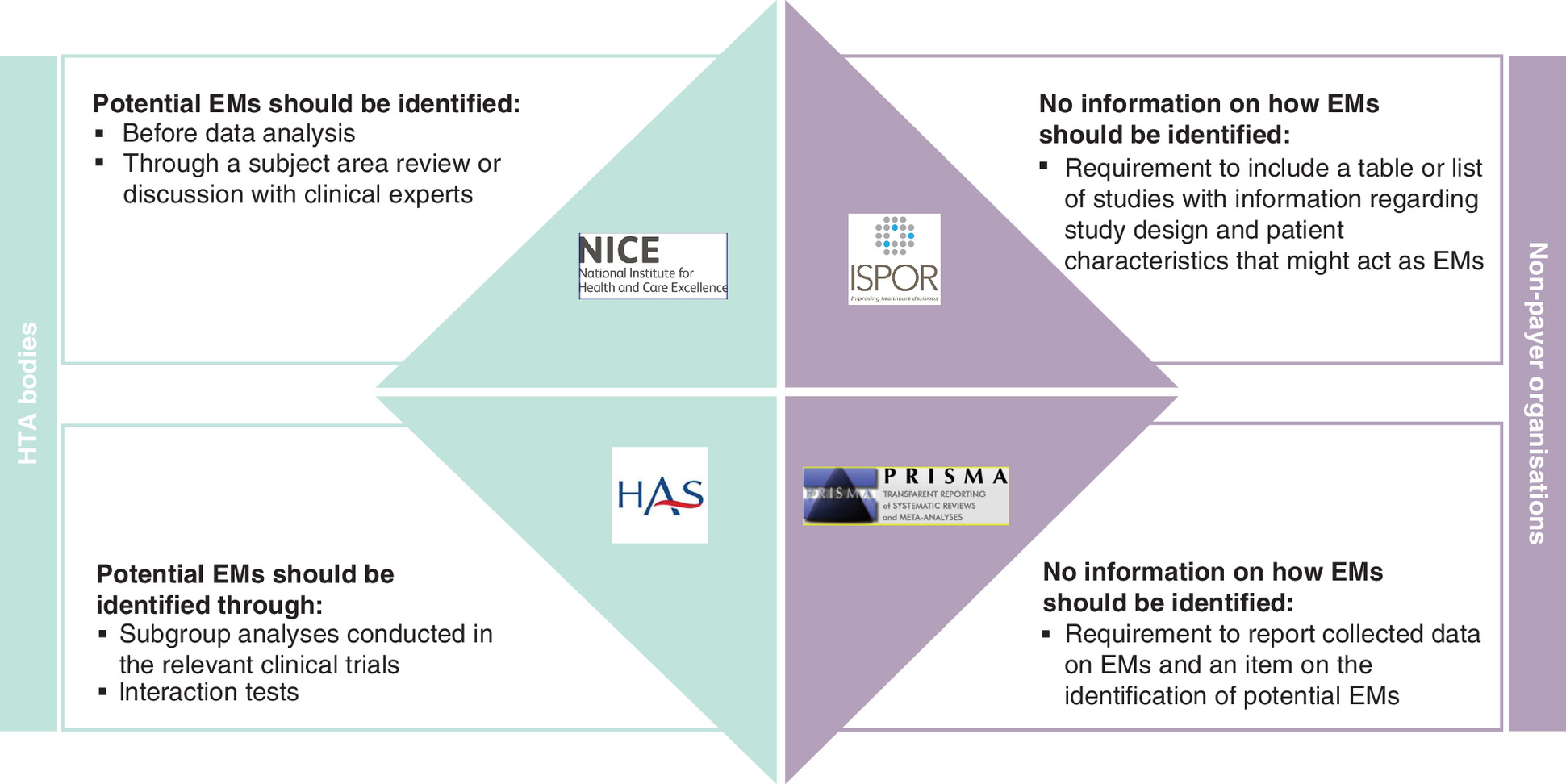
Figure 1. Summary of themes identified in payer and non-payer guidance documents.
EM: Effect modifier; HTA: Health technology assessment.
From non-HTA bodies, guidance was restricted to adequate reporting of EM selection. However, it was outside the scope of these checklists to provide specific guidance on the EM selection method [20–22].
Application of guidance in the literature & prior HTA submissions
Pragmatic review of ITCs published in peer-reviewed journals
Of the 511 unique articles identified through the Embase and MEDLINE search, 17 mentioned a selection process for interfering variables, such as EMs and PVs (Figure 2 and Supplementary Table 3 ). Eleven publications reported on ITCs across specific clinical indications [23–33]. Two publications concerned reviews of ITCs irrespective of the indication: a review of population-adjusted analyses across published NICE submissions [7] and a review of previously published NMAs to assess the level of EM reporting [34]. The remaining four publications were protocols of NMAs in Type 1 diabetes [35] and depressive disorder [36–38].
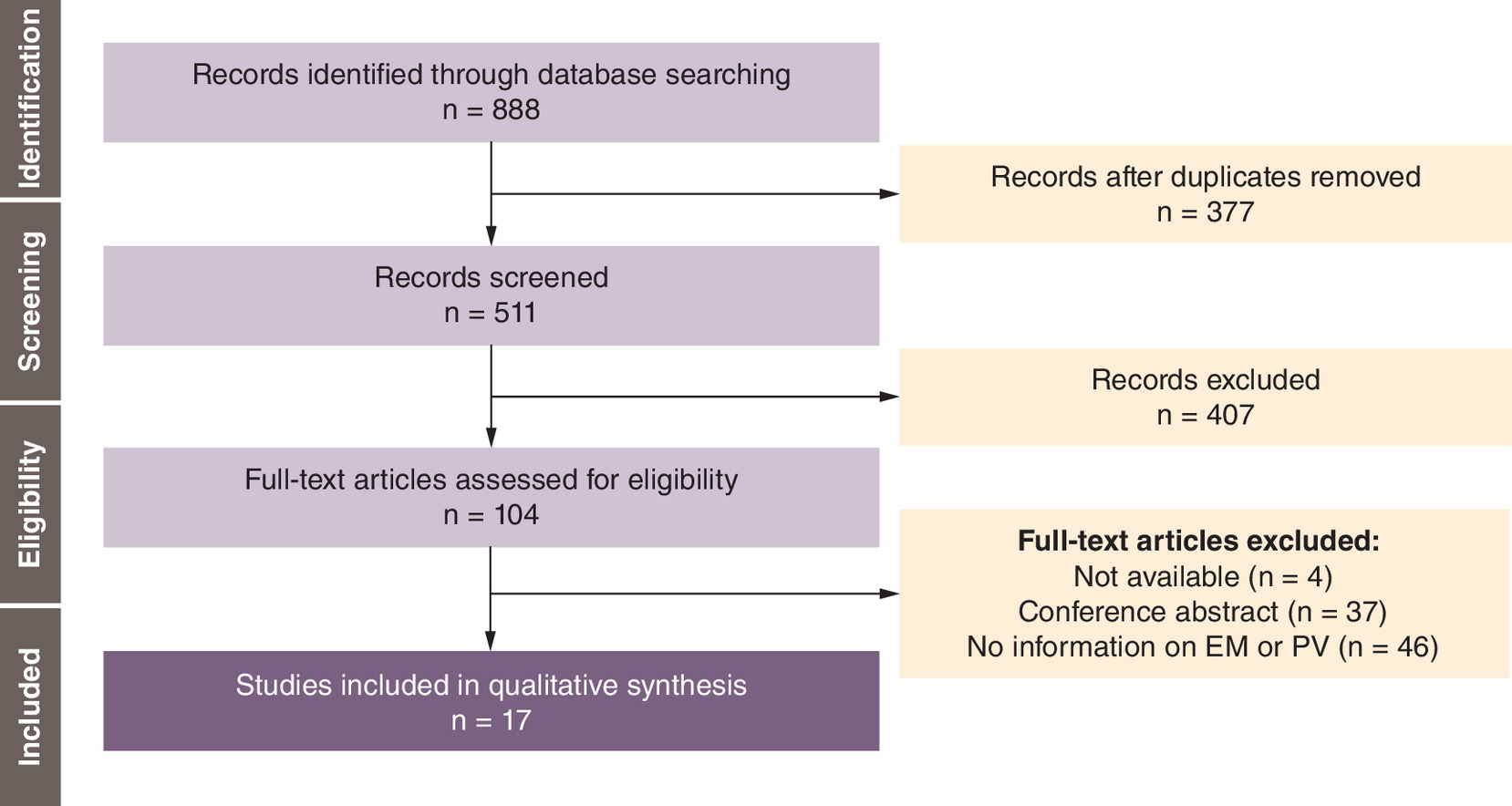
Figure 2. PRISMA flow chart for the review of published indirect treatment comparisons.
EM: Effect modifier; PV: Prognostic variable.
Of the 17 publications, six were on traditional NMAs [24,25,30,31,33,38], three on NMAs using individual patient data (IPD) [35–37], one each on a matching-adjusted indirect comparison (MAIC) [23] and both an NMA and simulated treatment comparison [32], and six publications concerned reviews of NMAs and other forms of ITCs [7,26–29,34].
Only few published ITCs included information on the selection process for EMs which was either based on evidence previously highlighted in the literature, input from clinical experts or findings from prior trial subgroup analyses. No reference to a systematic identification of EMs through literature reviews was found (Figure 3).
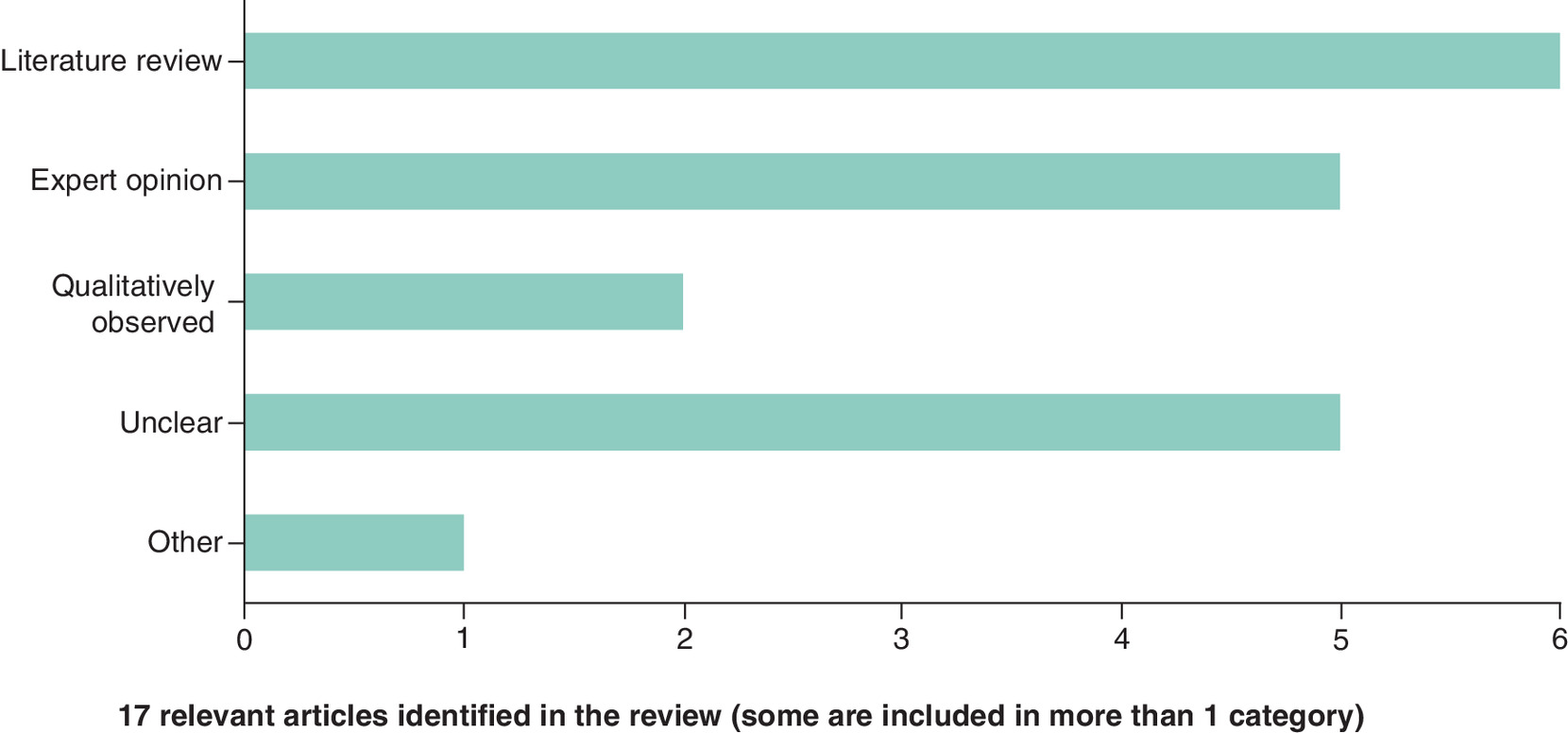
Two protocols for an IPD-NMA [36,37] of various interventions for depressive disorder included a list of EMs based on the literature, with both protocols citing the same previously published literature review. Factors to be investigated included age, sex, socioeconomic status, disease history, current symptoms and study characteristics. However, the protocols did not describe whether these factors had been identified through a systematic literature search of EMs. The protocols further stated that the final list of EMs would ultimately depend on the availability of these factors in the identified trials. Similarly, four published NMAs [30–33] provided a list of potential EMs based on information derived from the literature. However, no further information on the literature review approach was provided.
In five articles (two published NMAs [30,32] and three reviews of NMAs and ITCs [7,27,29]), the selection of EMs was based on expert opinion. No further details were provided on whether the discussion with subject matter experts was based on a formal elicitation exercise to justify their inclusion.
Two systematic literature reviews (SLRs) of NMAs [26,34] highlighted issues frequently encountered in the selection of EMs in the context of NMAs/ITCs. In these cases, EMs were mainly identified qualitatively through a comparison of patient baseline characteristics or subgroup results across the trials included in the analyses.
One publication mentioned the application of IPD analyses to identify EMs [35], and the remaining five publications did not provide a clear description of how EMs had been identified [23–25,28,38].
Most publications did not specifically state the timing of EM identification, i.e., whether this exercise was done prior, during or after conducting the analysis. In four cases, EMs were identified at the protocol or statistical analysis plan stage [31,35–37]. For a further nine publications, it was assumed that EMs had been identified prior to conducting the analysis given descriptions of the selection process in the methods. One review of published NMAs reported that of the 11 included studies, seven identified EMs before the conduct of the ITC, one after assessing inconsistency in the network, and three before and after [26]. The remaining three publications did not provide sufficient information on the timing of the EM selection processes [27,28,34].
Pragmatic review of prior HTA submissions
The review identified 51 relevant submissions with an ITC and information on EM/PVs, including 28 standard NMAs, three fractional-polynomial NMAs, five Bucher ITCs, 14 MAICs, and six propensity score weighting analyses, with some submissions including more than one analysis type (Figure 4).
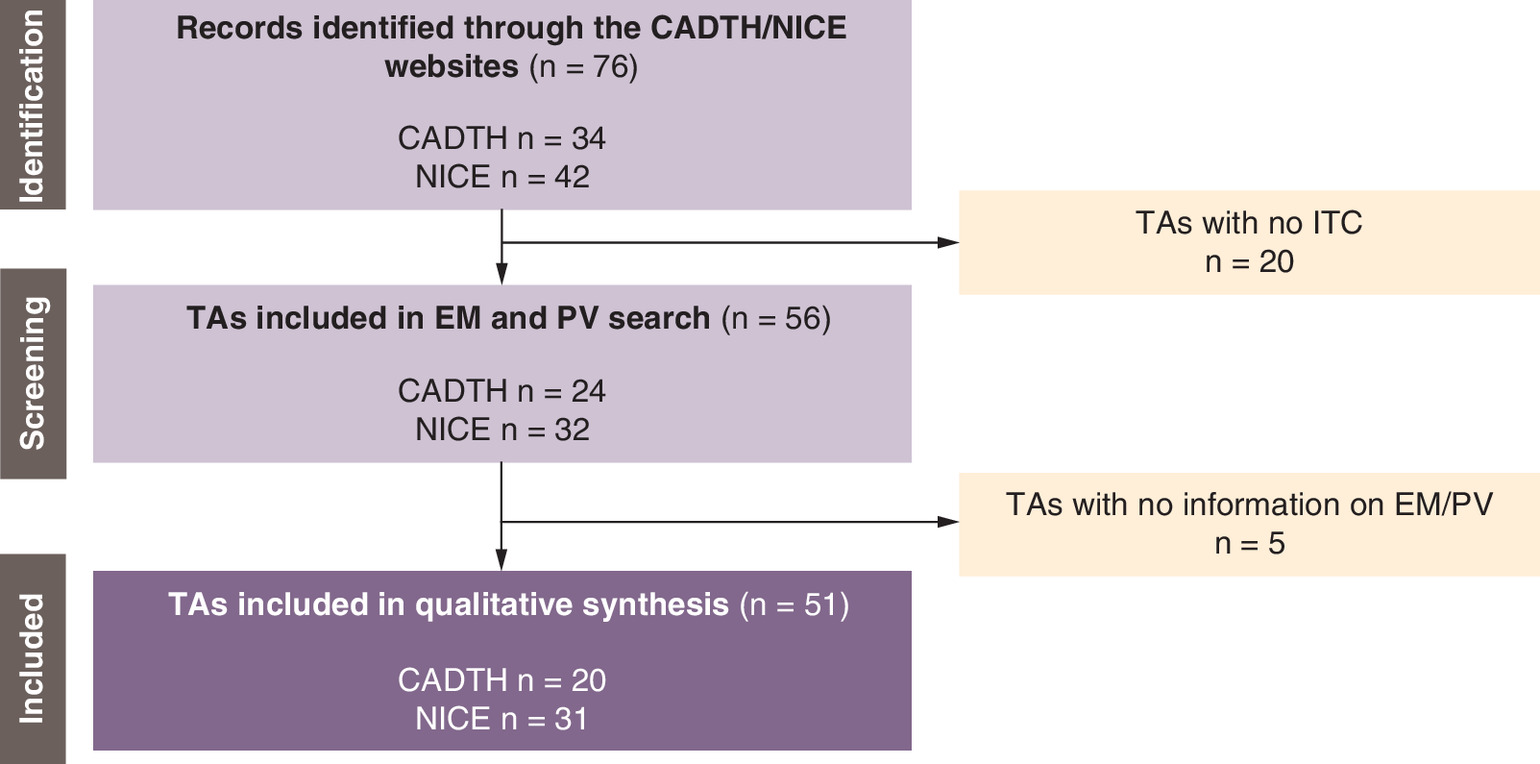
Figure 4. PRISMA flow chart for the review of published Canadian Agency for Drugs and Technologies in Health and national Institute for Health and Care Excellence technology assessments.
CADTH: Canadian Agency for Drugs and Technologies in Health; EM: Effect modifier; ITC: Indirect treatment comparison; NICE: National Institute for Health and Care Excellence; PV: Prognostic variable; TA: Technology appraisal.
The review of prior CADTH and NICE submissions of treatments for NSCLC (Table 2) and psoriasis (Table 3) confirmed the direction of the trend identified by the review of peer-reviewed, published ITCs in that detailed information on the identification and section of EMs and PVs was rarely available.
| Submission ID | Date of Guidance | Intervention (LoT) | Type of ITC | EM Identification | PV Identification | Timing of EM/PV Identification | Ref. |
|---|---|---|---|---|---|---|---|
| NICE | |||||||
| TA428 | 11 January 2017 | Pembrolizumab (2L+) | NMA | – | Based on subgroup analysis | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on trial subgroup analyses | [46] |
| TA500 | 24 January 2018 | Ceritinib (1L) | MAIC | No information on selection process provided | Based on literature | Timing of EM/PV identification is unclear | [47] |
| TA520 | 16 May 2018 | Atezolizumab (2L+) | NMA | – | The consistency of overall survival results was examined across subgroups based on important prognostic characteristic (no information on how these were selected) | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on trial subgroup analyses | [48] |
| TA571 | 20 March 2019 | Brigatinib (2L+) | MAIC | Based on clinical advice | Based on clinical advice | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the MAIC given the focus on expert elicitation exercises | [49] |
| TA584 | 5 June 2019 | Atezolizumab (1L) | NMA | – | • Based on literature and clinical advice • Additional PVs identified by ERG | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on expert elicitation exercises to identify factors for the NMA; additional PVs identified by the ERG after the conduct of the original NMA | [50] |
| TA595 | 14 August 2019 | Dacomitinib (1L) | FP-NMA | Based on literature and clinical advice | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on expert elicitation exercises and literature reviews | [51] |
| TA628 | 13 May 2020 | Lorlatinib (2L+) | MAIC | Based on literature, clinical advice and trial IPD analysis | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the MAIC given the focus on expert elicitation exercises, literature review and analysis of trial IPD | [52] |
| TA643 | 12 August 2020 | Entrectinib (1L+) | MAIC | • Based on clinical advice • ERG suggested additional EMs following the clinical advice | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the MAIC given the focus on expert elicitation exercises to identify factors for the MAIC; additional PVs identified by the ERG after the conduct of the original MAIC | [53] |
| TA653 | 14 October 2020 | Osimertinib (2L) | MAIC | – | • Based on literature • ERG suggested additional EMs following the clinical advice | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the MAIC given the focus on literature reviews to identify factors for the MAIC; additional PVs identified by the ERG after the conduct of the original MAIC | [54] |
| TA654 | 12 October 2020 | Osimertinib (1L) | Bucher ITC | – | – | No information on EM/PV given | [55] |
| TA670 | 27 January 2021 | Brigatinib (1L) | MAIC | No information on selection process provided | No information on selection process provided | Insufficient information provided to conclude on the timing of identification | [56] |
| TA683 | 10 March 2021 | Pembrolizumab (1L) | NMA; Bucher ITC | No information on selection process provided | – | Insufficient information provided to conclude on the timing of identification | [57] |
| TA705 | 2 June 2021 | Atezolizumab (1L) | NMA; FP-NMA | – | No information on selection process provided | Insufficient information provided to conclude on the timing of identification | [58] |
| TA724 | 8 September 2021 | Nivolumab (1L) | FP-NMA | Based on literature and subgroup analysis | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on subgroup analysis and literature reviews | [59] |
| TA760 | 12 January 2022 | Selpercatinib (2L+) | NMA | – | Based on literature and clinical advice | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on expert elicitation exercises and literature reviews | [60] |
| TA770 | 9 February 2022 | Pembrolizumab (1L) | Bucher ITC | Based on sensitivity analyses and clinical advice | – | EM/PV likely identified during or after the conduct of the Bucher ITC given the focus on sensitivity analyses | [61] |
| TA781 | 30 March 2022 | Sotorasib (2L+) | MAIC; PSWA | Based on literature review and clinical advice | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the MAIC given the focus on literature reviews | [62] |
| TA789 | 18 May 2022 | Tepotinib (1L+) | MAIC | – | • Based on literature (unclear how results were used) • Based on clinical advice | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the MAIC given the focus on literature reviews and expert elicitation exercises | [63] |
| TA812 | 3 August 2022 | Pralsetinib (1L+) | PSWA | – | No information on selection process provided | Insufficient information provided to conclude on the timing of identification | [64] |
| TA850 | 14 December 2022 | Amivantamab (2L+) | IPTW | Based on literature review and clinical advice | – | EM/PV identification prior to the conduct of the MAIC | [39] |
| TA855 | 4 January 2023 | Mobocertinib (2L+) | IPTW | Based on literature review and clinical advice | Based on literature review and clinical advice | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the IPTW given the focus on literature reviews and expert elicitation exercises | [65] |
| CADTH | |||||||
| PC0106-000 | 2 November 2017 | Dabrafenib + trametinib (2L+) | NMA; MAIC | • Pivotal trial in NSCLC BRAF V600 mutation, with that specific mutation a-priori considered an EM by pERC • pERC noted that not all EMs had been considered | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA and MAIC given the description of differences in patient characteristics across the included trials | [66] |
| PC0114-000 | 29 March 2018 | Alectinib (2L+) | NMA | • No information on selection process provided • pERC noted that not all EMs had been considered | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA and MAIC given the description of differences in patient characteristics across the included trials | [67] |
| PC0115-000 | 20 June 2018 | Atezolizumab (2L+) | NMA | Patient characteristics from studies included in the NMA were investigated to detect potential EMs | – | Timing of EM/PV identification is unclear; but likely to have occurred during the conduct of the NMA given the use of interaction tests to identify potential EMs | [68] |
| PC0129-000 | 31 May 2019 | Dacomitinib (1L) | NMA | – | No information on selection process provided | Insufficient information provided to conclude on the timing of identification | [69] |
| PC0137-000 | 4 January 2019 | Osimertinib (1L) | Bucher ITC | Based on observed differences | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the ITC given the description of differences in patient characteristics across the included trials | [70] |
| PC0153-000 | 31 May 2019 | Pembrolizumab (1L) | Bucher ITC | Patient characteristics from studies included in the NMA were investigated to detect potential EMs | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the ITC given the description of differences in patient characteristics across the included trials | [71] |
| PC0155-000 | 3 July 2020 | Atezolizumab + bevacizumab (2L+) | NMA; MAIC | Based on observed differences | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA and MAIC given the description of differences in patient characteristics across the included trials | [72] |
| PC0167-000 | 1 August 2019 | Brigatinib (2L+) | NMA; MAIC | – | Logistic regression models using trial data were used to identify PVs affecting overall response rate | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA and MAIC given the description of differences in patient characteristics across the included trials | [73] |
| PC0176-000 | 3 January 2020 | Pembrolizumab (1L) | NMA | Based on observed differences | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the description of differences in patient characteristics across the included trials | [74] |
| PC0183-000 | 30 January 2020 | Lorlatinib (2L+) | MAIC | – | • Potentially based on literature review • pERC commented that not all relevant variables were included in the analysis | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the MAIC given the focus on literature reviews | [75] |
| PC0206-000 | 27 January 2021 | Entrectinib (1L) | MAIC | Based on literature | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the MAIC given the focus on literature reviews | [76] |
| PC0218-000 | 4 March 2021 | Nivolumab + ipilimumab (1L) | Bucher ITC | Based on subgroup analysis | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the ITC given the focus on subgroup analysis comparisons | [77] |
| PC0226-000 | 28 May 2021 | Dabrafenib + trametinib (1L) | PSWA | – | Based on observed differences | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the PSWA given the description of differences in patient characteristics across the included trials | [78] |
| PC0230-000 | 21 April 2021 | Brigatinib (1L) | MAIC | • Based on previous submissions • Based on interaction tests • pERC noted that not all EMs had been considered | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the MAIC given the focus on interaction tests and use of prior submissions to inform selection | [79] |
| PC0249-000 | 17 March 2022 | Lorlatinib (1L) | NMA | • Based on literature and subgroup analysis | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus literature reviews and subgroup analyses of included trials | [80] |
| PC0255-000 | 24 August 2022 | Tepotinib (1L+) | MAIC; PSWA | – | – | No information on EM/PV given | [81] |
| PC-0261-000 | 28 April 2022 | Selpercatinib (1L) | NMA | – | Based on real-world data | Insufficient information provided to conclude on the timing of identification | [82] |
| PC-0283-000 | 29 September 2022 | Pralsetinib (1L+) | PSWA | – | • Based on clinical advice • pERC noted that not all PVs had been considered | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus expert elicitation exercises | [83] |
1L: First line; 2L+: Second line or later; CADTH: Canadian Agency for Drugs and Technologies in Health; EM: Effect modifier; ERG: Evidence review group; FP: Fractional polynomial; ID: Identification; IPD: Individual patient data; ITC: Indirect treatment comparison; LoT: Line of treatment; MAIC: Matching-adjusted indirect comparison; NICE: National Institute for Health and Care Excellence; NMA: Network meta-analysis; NSCLC: Non-small cell lung cancer; pERC: Pan-Canadian Oncology Drug Review Expert Review Committee; PSWA: Propensity score weighting analysis; PV: Prognostic variable; TA: Technology appraisal.
| Submission ID | Date of Guidance | Intervention (LoT) | Type of ITC | EM Identification | PV Identification | Timing of EM/PV Identification | Ref. |
|---|---|---|---|---|---|---|---|
| NICE | |||||||
| TA442 | 26 April 2017 | Ixekizumab Retreatment (unresponsive/ intolerance) | NMA | No information on selection process provided | – | Insufficient information provided to conclude on the timing of identification | [84] |
| TA455 | 12 July 2017 | Adalimumab, etanercept, ustekinumab Retreatment (unresponsive/ intolerance) | NMA | Based on literature and subgroup analysis | Based on literature and subgroup analysis | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on literature reviews and trial subgroup analyses | [85] |
| TA475 | 6 September 2017 | Dimethyl fumarate Retreatment (unresponsive/ intolerance) | NMA | Based on subgroup analysis | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on trial subgroup analyses | [86] |
| TA511 | 21 March 2018 | Brodalumab Retreatment (unresponsive/ intolerance) | NMA | • Based on literature • ERG noted that not all EMs had been identified | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on literature reviews | [87] |
| TA521 | 13 June 2018 | Guselkumab Retreatment (unresponsive/ intolerance) | NMA | Based on subgroup analysis | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on trial subgroup analyses | [88] |
| TA574 | 17 April 2019 | Certolizumab pegol Retreatment (unresponsive/ intolerance) | NMA | – | The submission stated that studies included in the ITC were similar in terms of PVs. Manufacturer also provided (pre-planned) subgroup analysis, but it is not clear how these subgroups had been selected. | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on subgroup analyses | [89] |
| TA575 | 17 April 2019 | Tildrakizumab Retreatment (unresponsive/ intolerance) | NMA | – | Based on observed differences across trials and subgroup analysis | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on subgroup analyses and observed differences (part of a feasibility assessment) | [90] |
| TA596 | 21 August 2019 | Risankizumab Retreatment (unresponsive/ intolerance) | NMA | Information on EMs given in the appendix only (not publicly available) | – | Timing of EM/PV identification is unclear | [91] |
| TA723 | 1 September 2021 | Bimekizumab Retreatment (unresponsive/ intolerance) | NMA | The manufacturer suggested that no EMs had been clearly established in this disease area | – | Timing of EM/PV identification is unclear | [40] |
| TA734 | 7 October 2021 | Secukinumab Retreatment (unresponsive/ intolerance) | NMA | Based on observed differences across trials | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on observed differences (part of a feasibility assessment) | [92] |
| CADTH | |||||||
| SR0530-000 | 21 February 2018 | Guselkumab Retreatment (unresponsive/ intolerance) | NMA | • No mention of EMs in the company submission • EMs suggested by clinical experts as part of the committee discussions | – | Insufficient information provided to conclude on the timing of identification | [93] |
| SR0547-000 | 20 June 2018 | Brodalumab Retreatment (unresponsive/ intolerance) | ITC | – | – | No information on EM/PV given | [41] |
| SR0583-000 | 28 May 2019 | Risankizumab Retreatment (unresponsive/ intolerance) | NMA | – | – | No information on EM/PV given | [94] |
| SR0624-000 | 21 June 2021 | Tildrakizumab Retreatment (unresponsive/ intolerance) | NMA | Based on subgroup analysis | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to or during the conduct of the NMA given the use of subgroup analyses to identify EMs | [95] |
| SR0638-000 | 28 October 2020 | Halobetasol propionate, tazarotene Retreatment (unresponsive/ intolerance) | NMA | – | – | No information on EM/PV given | [96] |
| SR-0698-000 | 30 March 2022 | Bimekizumab | NMA | Based on literature and clinical advice | – | Timing of EM/PV identification is unclear; but likely to have occurred prior to the conduct of the NMA given the focus on literature reviews and expert elicitation exercises | [97] |
CADTH: Canadian Agency for Drugs and Technologies in Health; EM: Effect modifier; ERG: Evidence review group; ID: Identification; ITC: Indirect treatment comparison; LoT: Line of treatment; NICE: National Institute for Health and Care Excellence; NMA: Network meta-analysis; PV: Prognostic variable; TA: Technology appraisal.
Across the manufacturer submissions, specific patient characteristics (e.g., genetic mutations or exposure to prior treatment) of the target populations were most commonly cited as factors that might impact treatment effects or clinical outcomes. In many instances, between-group differences were highlighted with regard to the validity of ITC results, suggesting that differences in patient baseline characteristics were investigated as part of the feasibility assessment. However, no clear information was presented as to whether the differences in baseline characteristics accounted for EMs or PVs. In some cases, the manufacturer submissions also referred to prior submissions as a source for potential EMs.
In CADTH submissions, observed between-group differences in patient characteristics were the most common source of justifying the selection of potential EM/PVs, followed by published evidence and subgroup analyses of the included trials. In contrast, manufacturer submissions to NICE most commonly mentioned clinical advice and information retrieved from the literature as sources for potential EMs and PVs. Only one company submissions (technology appraisal [TA]850 [39] on amivantamab as second- or later-line treatment for NSCLC) specifically stated that relevant EMs (interfering factors) had been identified prior to the conduct of the ITC. Based on the limited information provided in the other submissions, it was assumed that factors had been selected either prior to or when conducting the ITC. Although literature sources were commonly cited as sources for the selection of EMs and PVs, lack of information around the sources and the identification of such evidence makes a systematic approach highly unlikely to have been conducted. Prior knowledge about the natural history of disease and research on EMs and PVs have been stated as reasons for the limited information regarding the EM selection included in the ITCs [40,41].
Across the submissions, the assessment groups generally criticised that not all interfering variables had been accounted for in the ITCs, which ultimately resulted in considerable limitations in the analysis and confidence in the ITC results. For example, in many NICE submissions, the ERG criticised that manufacturers had either not fully addressed all known factors (clinical input sought from the ERG highlighted additional EMs and PVs to consider for adjustment), not designed their efforts to identify interfering variables in a way that could establish whether such a variable is indeed an EM or PV, or not provided sufficient detail and justification for a subset of potential interfering variables being chosen for adjustment among a longer list of potential factors being considered. On the contrary, in many CADTH submissions for psoriasis, the ERG attributed the lack of EM/PV consideration to data not being available for all factors across studies. As such, addressing these limitations might not have been possible even if additional efforts to identify EMs and PVs (e.g., through additional literature review sources or expert opinion) had been undertaken.
Discussion
Comparative treatment effects for novel health technologies commonly rely on the use of indirect comparisons in the absence of head-to-head trials, based on the assumption that the distribution of EMs is similar across the study populations. While imbalance in this EM distribution can considerably bias the validity of analysis results, issues can also arise if PVs are considered interchangeable with EMs, also introducing uncertainty in the decision-making [2,7]. Yet, no clear guidance exists from HTA bodies on the “appropriate” method for identification and selection of EMs.
The current series of pragmatic reviews showed that published guidance, across different organisations and settings, on this topic was generally scarce. This is surprising given the importance of EMs in ITC methods and analysis.
The most explicit guidance was from NICE which recommended a review of the literature or structured discussions with clinical experts to inform this selection [16]. However, the guidance falls short of providing clarity on how literature reviews should be designed; for example, which type of evidence should be considered, which criteria should be applied to define the transferability of findings on EMs and PVs from other sources to the current trial and trial population, and whether a hierarchical approach to the final selection of EMs and PVs to be considered and adjusted for should be applied. Documents from HAS, PBAC and the G-BA referred to qualitative and quantitative methods to test for EMs without providing further details on the exact methods to be employed (the 2009 HAS guidance was the most recent English version that could be identified) [17–19]. Non-payer organisations mainly provided checklists for reporting ITC methods and results. Although many included specific reporting items for the EM selection process, it was not the remit of these checklists to provide clear guidance on how the selection should be conducted in practice.
In line with the lack of clear guidance by payers and non-payer organisations, this trend also continued in practice (published literature). Authors rarely provided justification for the selection of EMs in the published NMAs/ITCs. Some publications listed a-priori selected factors but did not provide additional details on how these lists had been compiled. Six published ITCs noted that the selection of EMs was based on results from a literature review whereas five articles mentioned that experts had been consulted. However, none of these reported whether a systematic approach had been applied for the identification of these factors. It is also unclear to what extent word limits by scientific journals may have contributed to the omission of such information. Despite the short timeframe of the review of published NMAs and ITCs, an early trend suggested increasing awareness of the need to provide more information on the EM selection process, with an increasing number of relevant articles identified year-on-year.
The findings from these reviews were supported by the results of reviewing previous NICE and CADTH submissions for NSCLC and psoriasis—two indications with a rapidly changing treatment landscape. In many instances, EMs appeared to have been defined a-priori (based on prior submissions on the same disease) or the selection was informed by subgroup analyses of clinical trials considered for the analysis. Clinical experts were often involved in validating these assumptions in many submissions, in line with general requirements from HTA bodies, although this was more often explicitly stated in NICE than in CADTH submissions. Clear descriptions of a systematic identification of EMs, an important aspect in providing confidence in the ITC results, were lacking across the identified submissions.
Against this background, further research is needed to address key aspects for building an evidence base with an eye toward supporting regulatory as well as reimbursement submissions (Figure 5). SLRs may need to be tailored accordingly so that a systematic approach to the identification and selection of EMs can be applied. For example, a broad scope SLR of clinical data (both from clinical trials and real-world evidence) can be conducted to identify (1) factors previously described in the literature and prior HTA submissions, and (2) subgroup analyses from both the index trial, previously conducted trials, and published NMAs/ITCs.
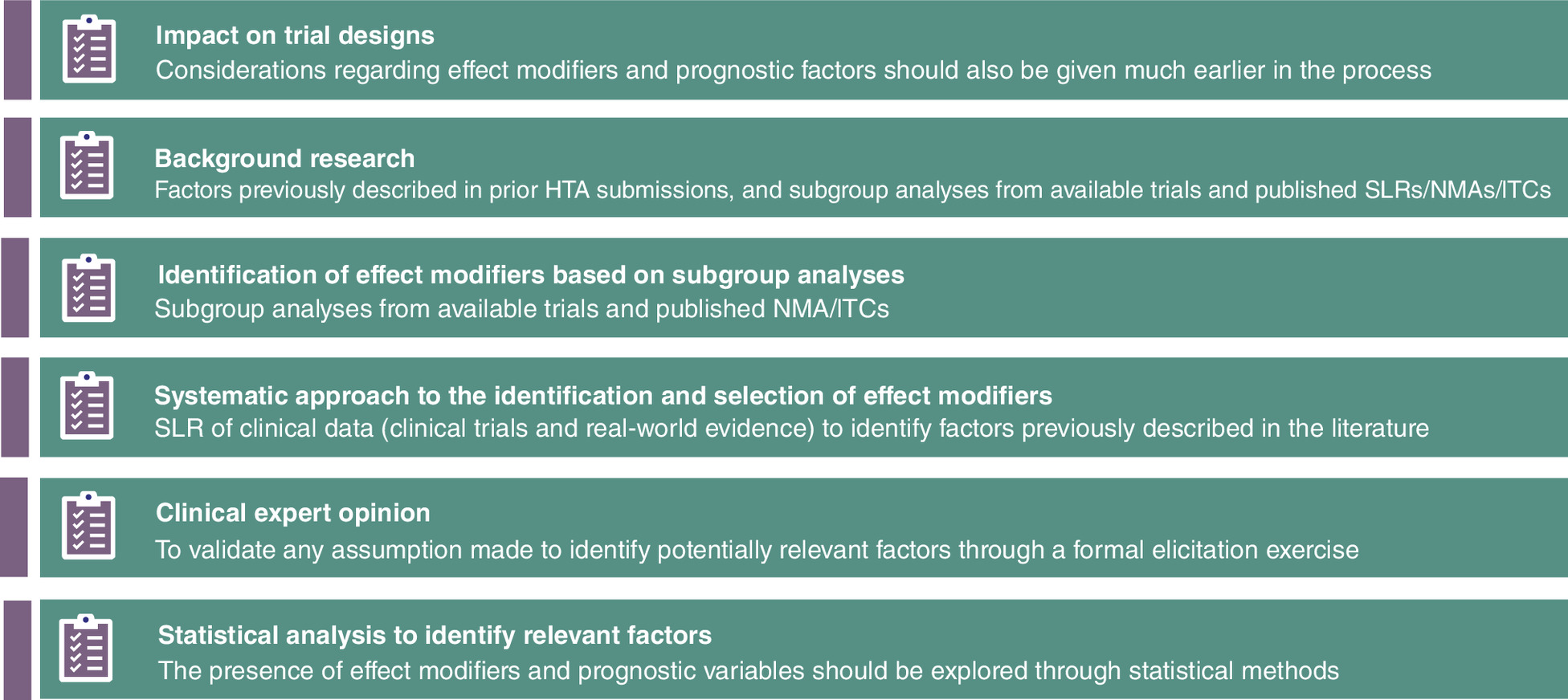
Figure 5. Recommended approaches for ensuring an unbiased identification and selection of effect modifiers.
HTA: Health technology assessment; ITC: Indirect treatment comparison; NMA: Network meta-analysis; SLR: Systematic literature review.
A key component in HTA submissions is the integration of expert opinion to describe uncertainties associated with the clinical and cost-effectiveness of competing interventions; structured elicitation exercises have a critical role in validating some of the assumptions in the use of PVs during ITC feasibility studies but a clear documentation of the processes and its results is needed to ensure unbiased conclusions [42–44]. Another component of paramount importance to the study design is the inclusion of clinical experts to validate assumptions made during the feasibility assessment or to identify potentially relevant factors through a formal elicitation exercise. The distinction between EMs and PVs can be challenging when based solely on clinical practice experience, underscoring the need for providing experts with detailed methodological a-priori training to separate the meaning between the two definitions.
The key strength of this research is the combination and comprehensiveness of review activities (guidance frameworks, HTA submissions based on these frameworks, and published ITCs in a real-world setting) to answer the research question. Despite the relatively short timeframe for the reviews of HTA submissions and published ITCs, it is unlikely that more comprehensive information on the EM selection process is available from older publications given the clear recommendation by the NICE DSU published only in 2016 [2].
This research was limited by several factors. First, the literature searches for published ITCs were restricted by terms for EMs and PVs for practical reasons. However, this was deemed unlikely to have biased the trend around the underreporting. Given the importance of addressing interfering variables in ITCs, abstracts were considered to commonly include whether an extensive exercise to identify these factors had been conducted. Second, a pragmatic decision was made to restrict the review of HTA submissions to two representative indications both of which are associated with a rapidly evolving treatment landscape: one chronic disease and one oncology indication. EMs are relatively well established for NSCLC; however, this is not true for psoriasis. This may partially explain the lack of information on interfering factors in many of the HTA submissions for psoriasis. It should be noted that in cases where data are not sufficiently available on interfering variables, additional (systematic) efforts to identify EMs and PVs are unlikely to result in a more comprehensive list of factors to be considered. Third, commercially sensitive information in HTA submissions is often redacted from published documents. In many CADTH submissions, the ITC relevant sections were heavily redacted, providing limited information on the analysis and any EMs and PVs considered relevant for. Some CADTH submissions had to be excluded from the review because even the analysis type was considered commercially sensitive. Finally, the lack of clear information in NICE appraisals on how interfering variables were identified may partially be due to the structure of the NICE submission template. Most NMA/ITC details are included in the appendices which are not immediately publicly available.
Conclusion
Given the evidence-based commitment by HTA bodies for using high-quality, fit-for-purpose evidence, there is a gap in guidance on how to appropriately identify EMs for inclusion in ITCs supporting HTA submissions. Adjusting for the “right” factors should be considered equally as important as choosing the appropriate ITC method. This guidance gap continues as a trend of underreporting of the identification and selection of EMs and PVs in published ITCs and company submissions for reimbursement. More explicit guidance is therefore needed on the wide range of evidence and sources needed to comprehensively identify EMs, including how to conduct SLRs on EMs and validation through formal expert elicitation. Similarly, a transparent reporting of the EM and PV selection process is required when conducting NMAs and ITCs to allow for an independent review and critique of the set of variables included for adjustment.
Executive summary
•
Indirect treatment comparisons (ITC) are frequently used in health technology assessments (HTA) to evaluate the value of new treatment in absence of sufficient head-to-head evidence.
•
The validity of ITCs can be impacted by differences in effect modifiers (EM) or prognostic variables (PV) across the included trials.
•
ITC methodological discussions have so far been centred around the statistical properties of these methods including the assumptions around EMs and their validity, yet very little attention has been paid to how EMs are identified in the first place.
•
This series of pragmatic reviews aimed to describe requirements for the appropriate selection of EMs (based on guidance documents from HTA and non-payer organisations) and how these are applied in practice (based on published ITCs and prior HTA submissions in non-small cell lung cancer and psoriasis).
•
Lack of detailed guidance on how to systematically identify EMs for ITCs in the context of HTA decision-making.
•
Only 17 of 511 (3.3%) reviewed ITCs included a description of the selection process for EMs and PVs; literature reviews and expert opinion were the most commonly cited sources.
•
A similar trend was found across prior HTA submissions; many EMs were defined a-priori based on information from prior submissions and trial subgroup analyses and validated by clinical input.
•
Providing clear guidance on the identification and selection of EMs must be considered a key research area by HTA bodies.
Author contributions
A Freitag, L Gurskyte and G Sarri were responsible for study conception and design; all authors contributed equally to the literature review, and drafting and revision of the manuscript.
Acknowledgments
The authors thank Maria Rizzo for valuable input in the design of the review, and Colleen Dumont for reviewing the manuscript and providing comprehensive editorial assistance.
Financial & competing interests disclosure
All authors are employed by Cytel. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 61.14 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Dias S, Welton NJ, Sutton AJ, Ades A. Evidence synthesis for decision making 1: introduction. Med. Decis. Making 33(5), 597–606 (2013).
2.
Phillippo D, Ades T, Dias S, Palmer S, Abrams KR, Welton N. NICE DSU Technical Support Document 18: Methods for population-adjusted indirect comparisons in submissions to NICE. (Technical Support Documents). NICE Decision Support Unit, UK (2016). http://www.nicedsu.org.uk/Populationadjusted-ICs-TSD(3026862).htm
• Provides guidance on the methods and appropriate use of population-adjusted analyses when differences in patient characteristics exist that will impact the comparability of trials.
3.
Hingorani AD, van der Windt DA, Riley RD et al. Prognosis research strategy (PROGRESS) 4: stratified medicine research. BMJ 346, e5793 (2013).
4.
Kapetanakis V, Prawitz T, Schlichting M et al. How assessment-schedule matching limits bias when comparing progression-free survival in single-arm studies: an application in second-line urothelial carcinoma treatments. Value Health 24(8), 1137–1144 (2021).
5.
Salanti G. Indirect and mixed-treatment comparison, network, or multiple-treatments meta-analysis: many names, many benefits, many concerns for the next generation evidence synthesis tool. Res. Synth. Methods 3(2), 80–97 (2012).
6.
Hancock M, Herbert RD, Maher CG. A guide to interpretation of studies investigating subgroups of responders to physical therapy interventions. Phys. Ther. 89(7), 698–704 (2009).
7.
Phillippo DM, Dias S, Elsada A, Ades A, Welton NJ. Population adjustment methods for indirect comparisons: a review of national institute for health and care excellence technology appraisals. Int. J. Tech. Assess. Health Care 35(3), 221–228 (2019).
8.
Groff M, Tremblay G, Faulkner M. MSR131 Characterizing the impact of the shared-effect modification assumption on population-adjusted indirect comparisons. Value Health 25(12), S375 (2022).
•• This ISPOR poster describes the potential impact of imbalances in effect modifiers on analysis results.
9.
Remiro-Azócar A, Heath A, Baio G. Methods for population adjustment with limited access to individual patient data: a review and simulation study. Res. Synth. Methods 12(6), 750–775 (2021).
10.
Dias S, Sutton AJ, Welton NJ, Ades A. NICE DSU technical support document 3: Heterogeneity: subgroups, meta-regression, bias and bias-adjustment. NICE Decision Support Unit, UK (2011). https://www.ncbi.nlm.nih.gov/books/NBK395886/pdf/Bookshelf_NBK395886.pdf
11.
Institute for Quality and Efficiency in Health Care. General methods (v6.1) (2022). https://www.iqwig.de/en/about-us/methods/methods-paper/
12.
Hoaglin DC, Hawkins N, Jansen JP et al. Conducting indirect-treatment-comparison and network-meta-analysis studies: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: part 2. Value Health 14(4), 429–437 (2011).
13.
Higgins JPT, Thomas J, Chandler J et al. Cochrane Handbook for Systematic Reviews of Interventions, Version 6.3 (2022). http://www.training.cochrane.org/handbook
14.
Institute for Clinical and Economic Review. 2020-2023 Value Assessment Framework 2020. https://icer.org/wp-content/uploads/2020/10/ICER_2020_2023_VAF_102220.pdf
15.
Ades A, Caldwell DM, Reken S, Welton NJ, Sutton AJ, Dias S. NICE DSU Technical Support Document 7: Evidence synthesis of treatment efficacy in decision making: a reviewer's checklist. NICE Decision Support Unit, UK (2012). https://www.ncbi.nlm.nih.gov/books/NBK395872/
16.
National Institute for Health and Care Excellence. NICE health technology evaluations: the manual (2022). https://www.nice.org.uk/process/pmg36/chapter/introduction-to-health-technology-evaluation
•• NICE methods manual for health technology assessments, which accounts for one of the key methods documents for reimbursement submissions
17.
Federal Joint Committee. Dossier zur Nutzenbewertung gemäß § 35a SGB V (dossier for benefit assessment) (2019). https://www.g-ba.de/english/benefitassessment/
18.
Haute Autorité de Santé. Indirect comparisons: methods and validity (2009). https://www.has-sante.fr/upload/docs/application/pdf/2011-02/summary_report__indirect_comparisons_methods_and_validity_january_2011_2.pdf
19.
Pharmaceutical Benefits Advisory Committee. Guidelines for preparing submissions to the Pharmaceutical Benefits Advisory Committee, Version 5.0 (2016). https://pbac.pbs.gov.au/
20.
Jansen JP, Fleurence R, Devine B et al. Interpreting indirect treatment comparisons and network meta-analysis for health-care decision making: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: part 1. Value Health 14(4), 417–428 (2011).
21.
Hutton B, Salanti G, Caldwell DM et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann. Intern. Med. 162(11), 777–784 (2015).
22.
Stewart LA, Clarke M, Rovers M et al. Preferred reporting items for a systematic review and meta-analysis of individual participant data: the PRISMA-IPD statement. JAMA 313(16), 1657–1665 (2015).
23.
Bourdin A, Husereau D, Molinari N et al. Matching-adjusted indirect comparison of benralizumab versus interleukin-5 inhibitors for the treatment of severe asthma: a systematic review. Eur. Respir. J. 52(5), 1801393 (2018).
24.
McGirr A, Iqbal SM, Izurieta P et al. A systematic literature review and network meta-analysis feasibility study to assess the comparative efficacy and comparative effectiveness of pneumococcal conjugate vaccines. Hum. Vaccin. Immunother. 15(11), 2713–2724 (2019).
25.
Al-Moraissi E, Alkhutari A, Abotaleb B, Altairi N, Del Fabbro M. Do osteoconductive bone substitutes result in similar bone regeneration for maxillary sinus augmentation when compared to osteogenic and osteoinductive bone grafts? A systematic review and frequentist network meta-analysis. Int. J. Oral Maxillofac. Surg. 49(1), 107–120 (2020).
26.
Cope S, Clemens A, Hammes F, Noack H, Jansen JP. Critical appraisal of network meta-analyses evaluating the efficacy and safety of new oral anticoagulants in atrial fibrillation stroke prevention trials. Value Health 18(2), 234–249 (2015).
• Previously published review of indirect treatment comparisons highlighting issues in the selection of effect modifiers.
27.
Cope S, Toor K, Popoff E et al. Critical appraisal of published indirect comparisons and network meta-analyses of competing interventions for multiple myeloma. Value Health 23(4), 441–450 (2020).
28.
Wright E, Yasmeen N, Malottki K et al. Assessing the quality and coherence of network meta-analyses of biologics in plaque psoriasis: what does all this evidence synthesis tell us? Dermatol. Ther. 11(1), 181–220 (2021).
29.
Wade R, Sharif-Hurst S, Dias S. Patient characteristics as effect modifiers for psoriasis biologic treatment response: an assessment using network meta-analysis subgroups. Syst. Rev. 9(1), 1–15 (2020).
30.
Rose CJ, Ohm IK, Giske L, Næss GE, Fretheim A. Effect modification in network meta-analyses of treatments for relapsing refractory multiple myeloma (RRMM): systematic review, meta-analysis, and simulation. https://www.medrxiv.org/content/10.1101/2022.05.13.22275047v2
31.
Kanters S, Renaud F, Rangaraj A et al. Evidence synthesis evaluating body weight gain among people treating HIV with antiretroviral therapy-a systematic literature review and network meta-analysis. Eclinicalmedicine 48, 101412 (2022).
32.
Menzies-Gow A, Steenkamp J, Singh S et al. Tezepelumab compared with other biologics for the treatment of severe asthma: a systematic review and indirect treatment comparison. J. Med. Econ. 25(1), 679–690 (2022).
33.
Saramago P, Gega L, Marshall D et al. Digital interventions for generalized anxiety disorder (GAD): systematic review and network meta-analysis. Front. Psych. 12, 726222 (2021).
34.
Kovic B, Zoratti MJ, Michalopoulos S, Silvestre C, Thorlund K, Thabane L. Deficiencies in addressing effect modification in network meta-analyses: a meta-epidemiological survey. J. Clin. Epidemiol. 88, 47–56 (2017).
•• Previously published review of indirect treatment comparisons highlighting issues in the selection of effect modifiers.
35.
Veroniki AA, Straus SE, Ashoor HM, Hamid JS, Yu C, Tricco AC. Safety and effectiveness of long-acting versus intermediate-acting insulin for patients with type 1 diabetes: protocol for a systematic review and individual patient data network meta-analysis. BMJ Open 5(12), e010160 (2015).
36.
Furukawa TA, Karyotaki E, Suganuma A et al. Dismantling, personalising and optimising internet cognitive–behavioural therapy for depression: a study protocol for individual participant data component network meta-analysis. BMJ Open 8(11), e026137 (2018).
37.
Furukawa TA, Schramm E, Weitz ES et al. Cognitive-behavioural analysis system of psychotherapy (CBASP), a drug, or their combination: differential therapeutics for persistent depressive disorder: a study protocol of an individual participant data network meta-analysis. BMJ Open 6(5), e011769 (2016).
38.
Nikolin S, Owens K, Francis-Taylor R et al. Comparative efficacy, cognitive effects and acceptability of electroconvulsive therapies for the treatment of depression: protocol for a systematic review and network meta-analysis. BMJ Open 12(12), e068313 (2022).
39.
National Institute for Health and Care Excellence. Amivantamab for treating EGFR exon 20 insertion mutation-positive advanced non-small-cell lung cancer after platinum-based chemotherapy (TA850) (2022). https://www.nice.org.uk/guidance/ta850
40.
National Institute for Health and Care Excellence. Bimekizumab for treating moderate to severe plaque psoriasis (TA723) (2021). https://www.nice.org.uk/guidance/ta723
41.
Canadian Agency for Drugs and Technologies in Health. Brodalumab (SR0547-000) (2018). https://www.cadth.ca/brodalumab
42.
Bojke L, Soares M, Claxton K et al. Developing a reference protocol for structured expert elicitation in health-care decision-making: a mixed-methods study. Health Technol. Assess. 25(37), 1–124 (2021).
•• Describes a protocol for structured expert elicitation exercises, which are a key component of systematically and appropriately identifying effect modifier in the context of health technology assessments.
43.
University of York – Centre for Health Economics. Eliciting experts judgements in HTA. Report commissioned for NICE methods update (2020). https://www.york.ac.uk/media/che/documents/Elicitation-NICE-final-report-York_01042020.pdf
44.
Peel A, Jenks M, Choudhury M et al. Use of expert judgement across NICE guidance-making programmes: a review of current processes and suitability of existing tools to support the use of expert elicitation. Appl. Health Econ. Health Policy 16, 819–836 (2018).
45.
Canadian Agency for Drugs and Technologies in Health. Sponsor summary of clinical evidence template (2020). https://www.cadth.ca/cadth-procedures-reimbursement-reviews
46.
National Institute for Health and Care Excellence. Pembrolizumab for treating PD-L1-positive non-small-cell lung cancer after chemotherapy (TA428) (2017). https://www.nice.org.uk/guidance/ta428
47.
National Institute for Health and Care Excellence. Ceritinib for untreated ALK-positive non-small-cell lung cancer (TA500) (2018). https://www.nice.org.uk/guidance/ta500
48.
National Institute for Health and Care Excellence. Atezolizumab for treating locally advanced or metastatic non-small-cell lung cancer after chemotherapy (TA520) (2018). https://www.nice.org.uk/guidance/ta520
49.
National Institute for Health and Care Excellence. Brigatinib for treating ALK-positive advanced non-small-cell lung cancer after crizotinib (TA571) (2019). https://www.nice.org.uk/guidance/ta571
50.
National Institute for Health and Care Excellence. Atezolizumab in combination for treating metastatic non-squamous non-small-cell lung cancer (TA584) (2019). https://www.nice.org.uk/guidance/ta584
51.
National Institute for Health and Care Excellence. Dacomitinib for untreated EGFR mutation-positive non-small-cell lung cancer (TA595) (2019). https://www.nice.org.uk/guidance/ta595
52.
National Institute for Health and Care Excellence. Lorlatinib for previously treated ALK-positive advanced non-small-cell lung cancer (TA628) (2020). https://www.nice.org.uk/guidance/ta628
53.
National Institute for Health and Care Excellence. Entrectinib for treating ROS1-positive advanced non-small-cell lung cancer (TA643) (2020). https://www.nice.org.uk/guidance/ta643
54.
National Institute for Health and Care Excellence. Osimertinib for treating EGFR T790M mutation-positive advanced non-small-cell lung cancer (TA653) (2020). https://www.nice.org.uk/guidance/ta653
55.
National Institute for Health and Care Excellence. Osimertinib for untreated EGFR mutation-positive non-small-cell lung cancer (TA654) (2020). https://www.nice.org.uk/guidance/ta654
56.
National Institute for Health and Care Excellence. Brigatinib for ALK-positive advanced non-small-cell lung cancer that has not been previously treated with an ALK inhibitor (TA670) (2021). https://www.nice.org.uk/guidance/ta670
57.
National Institute for Health and Care Excellence. Pembrolizumab with pemetrexed and platinum chemotherapy for untreated, metastatic, non-squamous non-small-cell lung cancer (TA683) (2021). https://www.nice.org.uk/guidance/ta683
58.
National Institute for Health and Care Excellence. Atezolizumab monotherapy for untreated advanced non-small-cell lung cancer (TA705) (2021). https://www.nice.org.uk/guidance/ta705
59.
National Institute for Health and Care Excellence. Nivolumab with ipilimumab and chemotherapy for untreated metastatic non-small-cell lung cancer (TA724) (2021). https://www.nice.org.uk/guidance/ta724
60.
National Institute for Health and Care Excellence. Selpercatinib for previously treated RET fusion-positive advanced non-small-cell lung cancer (TA760) (2022). https://www.nice.org.uk/guidance/ta760
61.
National Institute for Health and Care Excellence. Pembrolizumab with carboplatin and paclitaxel for untreated metastatic squamous non-small-cell lung cancer (TA770) (2022). https://www.nice.org.uk/guidance/ta770
62.
National Institute for Health and Care Excellence. Sotorasib for previously treated KRAS G12C mutation-positive advanced non-small-cell lung cancer (TA781) (2022). https://www.nice.org.uk/guidance/ta781
63.
National Institute for Health and Care Excellence. Tepotinib for treating advanced non-small-cell lung cancer with MET gene alterations (TA789) (2022). https://www.nice.org.uk/guidance/ta789
64.
National Institute for Health and Care Excellence. Pralsetinib for treating RET fusion-positive advanced non-small-cell lung cancer (TA812) (2022). https://www.nice.org.uk/guidance/ta812
65.
National Institute for Health and Care Excellence. Mobocertinib for treating EGFR exon 20 insertion mutation-positive advanced non-small-cell lung cancer after platinum-based chemotherapy (TA855) (2023). https://www.nice.org.uk/guidance/ta855
66.
Canadian Agency for Drugs and Technologies in Health. Tafinlar & Mekinist in combo for non-small cell lung cancer (PC0106-000) (2017). https://www.cadth.ca/tafinlar-mekinist-combo-non-small-cell-lung-cancer-details
67.
Canadian Agency for Drugs and Technologies in Health. Alecensaro for locally advanced or metastatic non-small cell lung cancer (second line) (PC0114-000) (2018). https://www.cadth.ca/alecensaro-locally-advanced-or-metastatic-non-small-cell-lung-cancer-second-line-details
68.
Canadian Agency for Drugs and Technologies in Health. Tecentriq for non-small cell lung cancer (PC0115-000) (2018). https://www.cadth.ca/tecentriq-non-small-cell-lung-cancer-details
69.
Canadian Agency for Drugs and Technologies in Health. Vizimpro for non-small cell lung cancer (PC0129-000) (2019). https://www.cadth.ca/vizimpro-non-small-cell-lung-cancer-details
70.
Canadian Agency for Drugs and Technologies in Health. Tagrisso for non-small cell lung cancer (first line) (PC0137-000) (2019). https://www.cadth.ca/tagrisso-non-small-cell-lung-cancer-first-line-details
71.
Canadian Agency for Drugs and Technologies in Health. Keytruda for non-squamous NSCLC (PC0153-000) (2019). https://www.cadth.ca/keytruda-non-squamous-nsclc-details
72.
Canadian Agency for Drugs and Technologies in Health. Tecentriq & avastin non-squamous non-small cell lung cancer – details (PC0155-000) (2020). https://www.cadth.ca/tecentriq-avastin-non-squamous-non-small-cell-lung-cancer-details
73.
Canadian Agency for Drugs and Technologies in Health. Brigatinib (Alunbrig) for non-small cell lung cancer (NSCLC) (PC0167-000) (2019). https://www.cadth.ca/brigatinib-alunbrig-non-small-cell-lung-cancer-nsclc-details
74.
Canadian Agency for Drugs and Technologies in Health. Keytruda for squamous NSCLC (PC0176-000) (2020). https://www.cadth.ca/keytruda-squamous-nsclc-details
75.
Canadian Agency for Drugs and Technologies in Health. Lorlatinib (Lorbrena) for non-small cell lung cancer (PC0183-000) (2020). https://www.cadth.ca/lorlatinib-lorbrena-non-small-cell-lung-cancer-details
76.
Canadian Agency for Drugs and Technologies in Health. Entrectinib (Rozlytrek) for ROS1-positive non-small cell lung cancer (PC0206-000) (2021). https://www.cadth.ca/entrectinib-rozlytrek-ros1-positive-non-small-cell-lung-cancer
77.
Canadian Agency for Drugs and Technologies in Health. Nivolumab-ipilimumab for non-small cell lung cancer (PC0218-000) (2021). https://www.cadth.ca/nivolumab-ipilimumab-non-small-cell-lung-cancer-details
78.
Canadian Agency for Drugs and Technologies in Health. Dabrafenib and trametinib for non-small cell lung cancer BRAF V600 mutation (PC0226-000) (2021). https://www.cadth.ca/dabrafenib-and-trametinib-non-small-cell-lung-cancer-braf-v600-mutation
79.
Canadian Agency for Drugs and Technologies in Health. Brigatinib (Alunbrig) for anaplastic lymphoma kinase positive non-small cell lung cancer (PC0230-000) (2021). https://www.cadth.ca/brigatinib-alunbrig-anaplastic-lymphoma-kinase-positive-non-small-cell-lung-cancer-details
80.
Canadian Agency for Drugs and Technologies in Health. Lorlatinib (PC0249-000) (2022). https://www.cadth.ca/lorlatinib
81.
Canadian Agency for Drugs and Technologies in Health. Tepotinib (PC0255-000) (2022). https://www.cadth.ca/tepotinib
82.
Canadian Agency for Drugs and Technologies in Health. Selpercatinib (PC0261-000) (2022). https://www.cadth.ca/selpercatinib
83.
Canadian Agency for Drugs and Technologies in Health. Pralsetinib (PC0283-000) (2022). https://www.cadth.ca/pralsetinib
84.
National Institute for Health and Care Excellence. Ixekizumab for treating moderate to severe plaque psoriasis (TA442) (2017). https://www.nice.org.uk/guidance/ta442
85.
National Institute for Health and Care Excellence. Adalimumab, etanercept and ustekinumab for treating plaque psoriasis in children and young people (TA455) (2017). https://www.nice.org.uk/guidance/ta455
86.
National Institute for Health and Care Excellence. Dimethyl fumarate for treating moderate to severe plaque psoriasis (TA475) (2017). https://www.nice.org.uk/guidance/ta475
87.
National Institute for Health and Care Excellence. Brodalumab for treating moderate to severe plaque psoriasis (TA511) (2018). https://www.nice.org.uk/guidance/ta511
88.
National Institute for Health and Care Excellence. Guselkumab for treating moderate to severe plaque psoriasis (TA521) (2018). https://www.nice.org.uk/guidance/ta521
89.
National Institute for Health and Care Excellence. Certolizumab pegol for treating moderate to severe plaque psoriasis (TA574) (2019). https://www.nice.org.uk/guidance/ta574
90.
National Institute for Health and Care Excellence. Tildrakizumab for treating moderate to severe plaque psoriasis (TA575) (2019). https://www.nice.org.uk/guidance/ta575
91.
National Institute for Health and Care Excellence. Risankizumab for treating moderate to severe plaque psoriasis (TA596) (2019). https://www.nice.org.uk/guidance/ta596
92.
National Institute for Health and Care Excellence. Secukinumab for treating moderate to severe plaque psoriasis in children and young people (TA734) (2021). https://www.nice.org.uk/guidance/ta734
93.
Canadian Agency for Drugs and Technologies in Health. Guselkumab (SR0530-000) (2018). https://www.cadth.ca/guselkumab
94.
Canadian Agency for Drugs and Technologies in Health. Risankizumab (SR0583-000) (2019). https://www.cadth.ca/risankizumab
95.
Canadian Agency for Drugs and Technologies in Health. Tildrakizumab (SR0624-000) (2021). https://www.cadth.ca/tildrakizumab
96.
Canadian Agency for Drugs and Technologies in Health. Halobetasol propionate and tazarotene (SR0638-000) (2020). https://www.cadth.ca/halobetasol-propionate-and-tazarotene-0
97.
Canadian Agency for Drugs and Technologies in Health. Bimekizumab (SR0698-000) (2022). https://www.cadth.ca/bimekizumab
Information & Authors
Information
Published In
Copyright
© 2023 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 30 March 2023
Accepted: 4 August 2023
Published online: 21 August 2023
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Increasing transparency in indirect treatment comparisons: is selecting effect modifiers the missing part of the puzzle? A review of methodological approaches and critical considerations. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0046
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Alberto de la Cuadra-Grande, María Arruñada, Alejandro García-Solís, Ana Rossignoli-Montero, Miguel Ángel Casado, Evidence Synthesis via Indirect Treatment Comparisons in the European Framework of Joint Clinical Assessment, Epidemiologia, 10.3390/epidemiologia7030064, 7, 3, (64), (2026).
- Lotte Delemarre, Isabelle Huys, Walter Van Dyck, Steven Simoens, Addressing clinical uncertainties in ATMP reimbursement: a review of methodological guidelines and European practice, Frontiers in Pharmacology, 10.3389/fphar.2026.1749386, 17, (2026).
- Jianming He, Karen Chiang, Xiwu Lin, Winghan Jacqueline Kwong, John Maringwa, Lingfeng Yang, Sandhya Nair, Mahmoud Hashim, Mi Jun Keng, Imtiaz A Samjoo, Identification of treatment effect modifiers and prognostic factors in newly diagnosed and relapsed or refractory multiple myeloma, Journal of Comparative Effectiveness Research, 10.57264/cer-2024-0180, 14, 10, (2025).
- Nils Erik Gilhus, Saiju Jacob, Mahmoud Hashim, Suzy Van Sanden, Christopher Drudge, Anna Nero, Sumeet Singh, Kavita Gandhi, Brian Hutton, Network connectivity, between-study heterogeneity and timepoint challenges in generalized myasthenia gravis: a feasibility assessment of indirect treatment comparisons, Journal of Comparative Effectiveness Research, 10.57264/cer-2025-0009, 14, 6, (2025).
- K. Jack Ishak, Conor Chandler, Fei Fei Liu, Sven Klijn, A Framework for Reliable, Transparent, and Reproducible Population-Adjusted Indirect Comparisons, PharmacoEconomics, 10.1007/s40273-025-01503-1, 43, 7, (691-710), (2025).
- Jennifer D Guo, Adel Gehchan, Abraham Hartzema, Selection of indirect treatment comparisons for health technology assessments: a practical guide for health economics and outcomes research scientists and clinicians, BMJ Open, 10.1136/bmjopen-2024-091961, 15, 3, (e091961), (2025).
- Maria De Santis, Sara Martínez Breijo, Paul Robinson, Camille Capone, Katie Pascoe, Suzy Van Sanden, Mahmoud Hashim, Marco Trevisan, Caitlin Daly, Friso Reitsma, Sophie van Beekhuizen, Haoyao Ruan, Bart Heeg, Elena Verzoni, Feasibility of Indirect Treatment Comparisons Between Niraparib Plus Abiraterone Acetate and Other First-Line Poly ADP-Ribose Polymerase Inhibitor Treatment Regimens for Patients with BRCA1/2 Mutation-Positive Metastatic Castration-Resistant Prostate Cancer, Advances in Therapy, 10.1007/s12325-024-02918-6, 41, 8, (3039-3058), (2024).
- Mazyar Shadman, Alessandra Tedeschi, Leyla Mohseninejad, Keri Yang, Nicole Lamanna, Sheng Xu, Aileen Cohen, Swetha Challagulla, Mei Xue, Rhys Williams, Susan M. O’Brien, Jennifer R. Brown, Constantine Tam, Similar efficacy of ibrutinib arms across ALPINE and ELEVATE-RR trials in relapsed/refractory chronic lymphocytic leukemia: a matching-adjusted indirect comparison, Blood Cancer Journal, 10.1038/s41408-024-01044-4, 14, 1, (2024).
- Bérengère Macabeo, Arthur Quenéchdu, Samuel Aballéa, Clément François, Laurent Boyer, Philippe Laramée, Methods for Indirect Treatment Comparison: Results from a Systematic Literature Review, Journal of Market Access & Health Policy, 10.3390/jmahp12020006, 12, 2, (58-80), (2024).