Factors impacting self-management ability in patients with chronic diseases in the United Arab Emirates, 2019
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Poor adherence to chronic disease therapy is a critical global problem that negatively effects the long-term therapy for chronic diseases, resulting in negative population health and economic effects. The WHO multidimensional model proposed a systems-based approach for improving adherence to chronic disease therapy. Patients & methods: In the current study, the WHO five-dimension framework was used to evaluate factors among, chronic-disease patients in the United Arab Emirates. Results: We show that patient’s understanding of disease, involvement in treatment decision, age more than 40 years, time spent with physician and fear of how patients were perceived by others were the most predictive factors associated with a high ability to self-manage a chronic disease. Conclusion: Sociocultural factors have an indirect impact on disease self-management.
Poor adherence to chronic disease therapy is a significant public health problem, with adherence averaging only 50% in developed countries and lower in developing countries [1]. This poor adherence negatively effects the outcomes of long-term therapy for chronic diseases, resulting in significant negative population health and economic effects [1]. Since 1990, the number of disability-adjust life years (DALYs) due to chronic diseases, such as ischemic heart disease, stroke, chronic obstructive pulmonary disease (COPD), diabetes, chronic low back pain, depressive and anxiety disorders, and chronic kidney disease, have increased, and these conditions accounted for nine of the top 25 causes of DALYs in 2019 [2]. As the global burden of chronic diseases increases, the need to improve adherence to chronic disease therapy becomes crucial as a critical strategy to ensure quality of care for patients, minimize the impacts of these diseases, preventing further complications and disability and reducing costs for health systems and individual patients.
Despite the urgent need, improving adherence to chronic disease therapy is hindered by the multiple and myriad interactions among diverse factors that impact the extent to which patients can follow their healthcare providers’ recommendations – with respect to both medication and lifestyle changes. In 2003, the WHO put forth a multidimensional model that moved away from ‘blaming’ patients or healthcare providers and instead proposed a systems-based approach for improving adherence to chronic disease therapy. This multidimensional model is based on five broad categories of factors/interventions: social- and economic-related; health system- and healthcare team-related; therapy-related; condition-related; and patient-related. While this model is an important framework for understanding and developing strategies to overcome the barriers to chronic disease therapy adherence, the role of the individual factors in adherence have not been comprehensively evaluated. Additionally, many of these factors require consistent and persistent actions on the part of the patient, making patients’ self-management of their chronic diseases an essential component to improving adherence to long-term therapy [1,3].
Improving self-management among patients with chronic diseases requires defining what self-management means in the context of chronic illness as well is identifying the processes that contribute to self-management. Self-management in the context of chronic disease has previously been defined as ‘the ability to manage symptoms, treatments, lifestyle changes and psychosocial, cultural and spiritual consequences of health conditions’ [3]. This definition requires that patients are willing and able to monitor their illness and to employ effective cognitive, behavioral and emotional strategies to maintain a satisfactory quality of life [3,4].
A qualitative metasynthesis of published studies identified three categories self-management processes: focusing on illness needs, activating resources and living with a chronic disease [3]. Tasks that contribute to self-management processes have also been organized into medical, behavioral and emotional groups, which comprise activities such as taking medication and attending medical appointments, making lifestyle changes and managing the emotional impacts of a living with a chronic disease [5]. Tasks involved with decision-making, changing behaviors and taking daily actions that allow patients to live well with a chronic disease are also important for effective self-management [6,7].
The ability to identify and leverage these factors to improve management and outcomes for patients with chronic diseases in the United Arab Emirates (UAE) is of growing urgency given the increasing impact and burden of these diseases in the country and in neighboring countries of the Gulf Cooperation Council (GCC) [8]. A synthesis of 11 systematic reviews on the prevalence of cardiovascular disease risk factors in the GCC countries found high rates of female obesity (ranging from 29–45.7%), physical inactivity (50.7–98.7%), hypertension (21–50%), metabolic syndrome (23–45.9%) and diabetes (average 21%) [8]. Another study found rates of diabetes ranging from 8.5 to 15.3% in four GCC countries, with more than half of diabetics in these countries reported to have another chronic disease [9]. Results from a study of factors impacting asthma control among patients in the GCC countries emphasize the need for a multidisciplinary approach to asthma management, for which self-management strategies may play an important role [10]. To mitigate the potential negative impact of copay requirements on adherence participants in the current study did not make a copay for their chronic disease medication [11,12].
There are limited data in the literature describing the factors that enable patients with chronic disease to engage in these self-management tasks, both broadly and as a function of geographic demographic, cultural, socioeconomic, educational and disease-status factors. Although a metasynthesis study of published literature identified the individual, family, environment and healthcare system dimensions as factors that influence self-management.
In the current study, we used the WHO five-dimension framework to evaluate factors among chronic-disease patients in the UAE, with the goal of identifying predictive factors associated with self-management ability.
Patients & methods
Setting & study design
In 2019, Axios International implemented an adherence program for chronic diseases with the aim to educate patients on their disease and treatment, support them in their medication adherence and other relevant procedures throughout their treatment journey, including regular follow-up.
The program uses a personalized approach adapted to the needs of patients who are newly diagnosed with a chronic disease, based on an initial assessment of patients’ needs to improve self-management abilities ‘Patient Needs Assessment Tool (PNAT).’ The PNAT uses 28 variables to evaluate patients’ needs based on the WHO’s five dimensions of adherence and is designed to enable the development of personalized and comprehensive support plans for individual patients that aim to improve adherence to therapy. The PNAT is administered by a health worker. The adherence program resulting from use of the PNAT comprises three objectives: to develop a personalized action plan in which patients’ needs for adherence are addressed; to provide educational, emotional and psychological support that help patients understand how to manage their disease; and to provide educational support to improve patients’ understanding of the mode of action and route of administration of their chronic disease medications. Information gained through the PNAT are used to develop a personalized adherence support plan and patients in the program receive comprehensive support from a wider, multidisciplinary team including medical doctors, nurses, dieticians and social workers.
In the context of implementing the adherence program, the PNAT was used in a cross-sectional study conducted in 2019 in a total of 50 hospitals, which had previously adopted and used the PNAT tool developed by Axios international. These 50 hospitals represented 47.6% of the total hospitals in the UAE and included ten government hospitals (30.3% of all government hospitals) and 40 private hospitals (55.5% of all private hospitals).
Study population
The study population included UAE citizens as well as noncitizen residents. Patients aged 18 years or older who were newly diagnosed with one of the following diagnosis: ankylosing spondylitis, heart failure, multiple sclerosis, psoriasis or asthma and had been prescribed long-term (≥1 year) medication were considered eligible for inclusion in the study. Patients were enrolled from the public and private sectors to reflect, as well as possible, the representative distribution of treatment patterns in the general population. Participating patients received medication and care at multiple public and private hospitals and health facilities in the UAE.
Data collection
After receiving the prescription and the information about the disease and treatment from the healthcare professional (HCP), participant information was collected using a structured interview conducted by a bilingual investigator (English–Arabic). Both citizens and noncitizens of the UAE were included in the study. The PNAT tool, which was validated prior to its use to collect data in this study, was implemented in both Arabic, the national language of the UAE, and in English, which is widely spoken in the UAE. The PNAT has previously been validated as a data collection tool in English. The investigator had previously received interview-technique training, and the collected data were anonymously coded to protect participants’ confidentiality. The Ethical Committee of Rouen University Hospital (CERDE-HLJ) approved the research. All the participants provided informed consent.
Multiple variables organized within the WHO’s five-dimension framework [1] and evaluated on 5-point Likert scales were collected as follows.
Variables for healthcare team and system-related factors: Quality of information provided, confidence in medical doctor (MD) explanations, confidence in MD prescription, confidence in hospital care, support of HCP to join other patients (i.e., in associations of patients) with a chronic disease, availability of HCP, satisfaction with HCP explanations and responses, satisfaction with time spent in consultation with the MD and patient involvement in treatment decision.
Variables for treatment-related factors: Ability of disease management (see below), fear of treatment inefficiency, long-time treatment, adverse events and interactions of treatment with living habits.
Variables for patient-related factors: Disease understanding, medication dosing strategy, impact of age on disease management, fear to become dependent on others and fear of others’ perception.
Variables for socioeconomic factors: Supporting role of community, interference between living conditions and treatment, and the roles of spiritual beliefs, family and cultural habits.
Variables for condition-related factors: Memory difficulties, impaired work performance due to the disease and/or treatment, risk of forgetting to take medication, anxiety and stress, burden of treatment cost.
Additionally, gender, age, the highest level of education (secondary school or lower, undergraduate and graduate studies), employment (yes, no), living status (living with wife or husband, living with parents or family, and living alone) and health insurance information were collected. Patient-provider communication, perceived quality of healthcare delivery and level of treatment information received were evaluated on a 5-point Likert scale [13,14] (strongly disagree = 1, disagree = 2, neither agree nor disagree = 3, agree = 4, strongly agree = 5). Scores above ‘3’ were used to categorize respondents as having good communication with their provider, perceiving good quality of healthcare delivery and receiving complete treatment information for each item, respectively.
Primary end point
Each participant’s perceived ability to self-manage his or her chronic disease following the information received from HCP was determined as the main measure for the present study, with a standardized question: ‘How do you estimate your self-ability to manage your disease.’ A 5-point Likert scale (‘strongly unable’ coded [1], ‘unable’ [2], ‘moderately able’ [3], ‘able’ [4] and ‘strongly able’ [5]) was used to assess the participant’s ability to manage the chronic disease [13,14]. Responses to this question were used to categorize participants according to the median value into a ‘high ability’ group (Likert scale at 5) and ‘low-to-moderate ability’ group (Likert scale from 1 to 4).
Statistical analysis
Descriptive statistics were computed for the characteristics of patients included in the program and were calculated as means and their standard deviations (SD) and median (M) values for quantitative variables and percentages for qualitative variables. Chi-square test was used for qualitative data comparisons; Student’s t test for quantitative comparisons. No sample size was calculated.
For the primary end point analysis, variables with p < 0.20 from the univariate analysis were fitted into the multivariate logistic regression in order to identify independent factors associated with high self-management ability. Adjusted odds ratio (AOR) and 95% CI were calculated.
A complementary analysis was performed to allow a better characterization of the patients’ profiles in terms of responses to the WHO’s five-dimension framework (1), by applying unsupervised (without a priori knowledge) clustering analysis. Clustering analysis relied on self-organizing maps (SOMs), a nonparametric neural network clustering technique that allows the visual identification of homogenous groups (clusters) in 2D maps. Patients sharing similar characteristics in terms of responses to the questionnaire are displayed in close proximity on the SOMs, whereas patients with opposite features are mapped in areas distant from one another [15]. A circular implementation applying the ‘Numero’ statistical framework was used to build the SOMs and to define clusters boundaries, by constructing the SOMs with statistical verification of the robustness of the contrasts observed through permutation tests and determining suitable groupings of patients based on the visual identification of key data patterns [16].
For illustrative purposes, Gabriel’s biplots were plotted to project the patients along the principal components axes from principal component analysis according to their individual characteristics, coloring patients according to their final clustering diagnosis or cluster and thus allowing for direct visual assessment of the discriminative ability of each subgrouping.
Results were considered statistically significant when two-sided p-values were ≤0.05. Statistical analyses were performed using Excel Stat (Addinsoft) for descriptive analyses between-group comparisons and regression models, and R 4.0.2 (R Foundation, Vienna, Austria; pca2d, PCAMix, Numero, mclust and NbClust packages) for clustering analyses and visualizations.
Results
A total of 106 patients with ankylosing spondylitis (n = 10), heart failure (n = 13), multiple sclerosis (n = 38), psoriasis (n = 40) and asthma (n = 5) in the UAE were included in this study. Five patients (4.7%) declined to be included in the study. Baseline characteristics of these patients are summarized in Table 1. The sex-ratio (male:female) was 0.80 and mean age was 41.1 (SD = 13, M = 39.4).
| n (%) | |
|---|---|
| Sex ratio (male:female) | 0.80 |
| Age (years), mean (standard deviation) | 41.1 (13.0 ± 39.4) |
| Educational level None, primary and secondary school Undergraduate studies Graduate studies | 17.3 53.1 29.6 |
| Working employment | |
| Yes | 56.0 |
| No | 44.0 |
| Living status | |
| Married | 71.4 |
| Living with parents or family | 5.7 |
| Living alone | 22.9 |
| Health insurance | |
| Yes | 51.9 |
| No | 48.1 |
| Disease | |
| Ankylosing spondylitis | 9.4 |
| Heart failure | 12.3 |
| Multiple sclerosis | 35.8 |
| Psoriasis | 37.8 |
| Asthma | 4.7 |
| Treatment administration | |
| Oral | 47.2 |
| Injection | 52.8 |
| At least one treatment taken for other chronic disease Yes No | 40.6 59.4 |
| Hospital status | |
| Public | 23.8 |
| Private | 76.2 |
The mean value of Likert scale responses regarding patients’ perception of their ability to self-manage their chronic disease after completing the adherence program was 4.17 (SD = 0.82, M = 4.0). Based on the Likert scale responses, 42 patients (39.6%) were classified as low ability and 64 patients (60.4%) were classified as high ability with respect to self-managing their chronic disease. The sociodemographic characteristics of patients with low compared with high self-ability to manage the disease group are shown in Table 2. There was no significant difference between the two groups, except for hospital status, in which the high-ability group had a greater proportion of patients receiving care in a private hospital (81%) compared with the low-ability group (73%) (p = 0.05).
| Low ability (n = 64) | High ability (n = 42) | p-value | |
|---|---|---|---|
| Sex ratio | 0.83 | 0.75 | 0.80 |
| Age (years), mean (SD) | 42.5 (13.7) | 39.7 (12.3) | 0.28 |
| Education level (%) None, primary and secondary school Undergraduate studies Graduate studies | 32.2 49.2 18.6 | 25.6 59.0 15.4 | 0.63 |
| Working employment (%) Employed Unemployed | 45.0 55.0 | 42.5 57.5 | 0.80 |
| Living status (%) Married Living with parents or family Living alone | 66.7 6.3 27.0 | 78.6 4.7 16.7 | 0.41 |
| Health insurance (%) Yes No | 45.3 54.7 | 47.6 52.1 | 0.47 |
| Disease % Ankylosing spondylitis Heart failure Multiple sclerosis Psoriasis Asthma | 12.5 15.6 28.1 39.1 4.7 | 4.8 7.1 47.6 35.7 4.8 | 0.21 |
| Treatment administration (%) Oral Injection | 43.7 56.3 | 47.6 52.4 | 0.38 |
| Other treatment taken for chronic disease Yes No | 42.2 57.8 | 61.9 38.1 | 0.17 |
| Hospital status | |||
| Public Private | 27.0 73.0 | 19.0 81.0 | 0.05 |
SD: Standard deviation.
Table 3 compares adherence variables, organized according to the WHO five-dimension framework, between the low- and high-ability self-management groups. With respect to the 28 variables assessed within the five dimensions, the highest mean difference in scores between the low- and high-ability groups were found for medication dosing strategy (difference = 1.37, p < 10-4), burden of treatment cost (-0.86, p = 0.004) and patient involvement in treatment decision (0.85, p = 0.004).
| Mean score on a total of 5 (SD) | ||||
|---|---|---|---|---|
| Low ability (n = 64) | High ability (n = 42) | Mean diff. (high–low) | p-value | |
| Healthcare system-related factors | 3.85 (0.50) | 4.17 (0.53) | 0.32 | 0.002 |
| Quality of information provided | 4.25 (0.64) | 4.64 (0.61) | 0.39 | 0.002 |
| Confidence with MD explanations | 3.94 (0.85) | 4.00 (0.96) | -0.06 | 0.72 |
| Confidence with MD prescription | 4.44 (0.50) | 4.74 (0.50) | 0.37 | 0.006 |
| Confidence in hospital care | 4.14 (0.89) | 4.12 (0.99) | 0.02 | 0.91 |
| Support of HCP to join other patients | 3.25 (1.32) | 3.69 (1.49) | 0.44 | 0.11 |
| HCP availability | 3.97 (1.05) | 4.19 (0.99) | 0.22 | 0.28 |
| Satisfaction with HCP responses | 4.13 (0.70) | 4.29 (0.86) | 0.16 | 0.29 |
| Satisfaction by time spent with MD | 3.92 (0.97) | 4.43 (0.89) | 0.51 | 0.007 |
| Involved in treatment decisions | 2.62 (1.35) | 3.47 (1.58) | 0.85 | 0.004 |
| Treatment-related factors | 3.02 (0.48) | 3.32 (0.53) | 0.30 | 0.004 |
| Fear of treatment inefficiency | 2.94 (1.15) | 3.19 (1.06) | 0.25 | 0.26 |
| Fear of long-time treatment | 2.55 (1.17) | 3.17 (1.15) | 0.62 | 0.008 |
| Fear of adverse events | 2.56 (1.17) | 2.11 (1.13) | -0.44 | 0.05 |
| Fear of treatment interactions with life | 4.03 (1.27) | 4.79 (0.75) | 0.70 | 0.001 |
| Patient-related factors | 3.48 (0.50) | 3.76 (0.35) | 0.28 | 0.002 |
| Disease understanding | 4.05 (0.72) | 4.76 (0.48) | 0.72 | <10-4 |
| Medication dosing strategy | 3.62 (0.60) | 5.00 (0) | 1.37 | <10-4 |
| Impact of age on disease management | 3.27 (1.01) | 2.50 (1.09) | -0.77 | 0.0001 |
| Fear to be dependent | 4.77 (1.18) | 4.33 (1.12) | -0.59 | 0.03 |
| Fear of look of others | 2.69 (1.33) | 2.21 (1.24) | -0.65 | 0.07 |
| Socioeconomic factors | 2.52 (0.55) | 2.37 (0.60) | -0.15 | 0.19 |
| Role of community | 2.12 (1.21) | 2.26 (1.40) | -0.14 | 0.59 |
| Interferences between life and treatment | 1.98 (0.98) | 1.69 (0.92) | -0.29 | 0.05 |
| Role of cultural habits | 1.89 (0.96) | 1.71 (0.97) | -0.17 | 0.36 |
| Role of spiritual beliefs | 2.36 (1.53) | 2.02 (1.47) | -0.34 | 0.26 |
| Role of family and friends | 4.23 (0.68) | 4.17(1.15) | 0.06 | 0.70 |
| Conditions-related factors | 3.30 (0.64) | 3.17 (0.64) | -0.12 | 0.33 |
| Memory difficulties | 3.91 (1.17) | 3.95 (1.23) | -0.04 | 0.85 |
| Impaired work performance | 2.46 (1.36) | 2.44 (1.46) | -0.02 | 0.95 |
| Risk of treatment forget | 4.12 (1.12) | 4.19 (1.09) | 0.07 | 0.77 |
| Anxiety and stress level | 2.81 (1.44) | 2.67 (1.37) | -0.14 | 0.60 |
| Burden of treatment cost | 3.81 (1.31) | 2.95 (1.70) | -0.86 | 0.004 |
HCP: Healthcare professional; MD: Medical doctor; SD: Standard deviation.
As shown in Table 4, logistic regression analysis found a significant association between a patient’s ability to self-manage his or her chronic disease and the following independent variables: disease understanding by the patient (AOR = 12.25; 95% CI = 4.51–18.76; p < 10-4), patient involved in the treatment decision (AOR = 6.29; 95% CI = 1.12–15.78; p = 0.01), fear of how they are perceived by others (AOR = 0.15; 95% CI = 0.07–0.92; p = 0,04), satisfaction with time spent with the physician (AOR = 0.11; 95% CI = 0.04–0.87; p = 0,04) and age (>40 years) (AOR = 11.62; 95% CI = 2.49–23.89; p = 0.02).
| AOR | 95% CI | p-value | |
|---|---|---|---|
| Age (in years) <32 32–40 >40 | 1.0 6.81 11.62 | – 0.85–20.56 2.49–23.89 | 0.09 0.02 |
| Hospital status Public Private | 1.0 1.17 | – 0.25–7.67 | 0.88 |
| Treatment for other chronic disease No | 1.0 | ||
| Yes | 1.34 | 0.26–7.89 | 0.70 |
| Health system-related factors | |||
| Quality of information provided Low score High score | 1.0 1.87 | – 0.28–9.40 | 0.52 |
| Support of HCP to join other patients Low score High score | 1.0 4.79 | – 0.97–9.87 | 0.07 |
| Confidence with MD prescription Low score High score | 1.0 5.41 | – 0.78–9.78 | 0.07 |
| Satisfaction by time spent with MD Low score High score | 1.0 0.11 | – 0.04–0.87 | 0.04 |
| Involved in treatment decision Low score High score | 1.0 6.29 | – 1.12–15.78 | 0.01 |
| Treatment-related factors | |||
| Fear of treatment interactions with life Low score High score | 1.0 1.71 | – 0.3–8.88 | 0.52 |
| Fear of long-time treatment Low score High score | 1.0 2.51 | – 0.43–12.32 | 0.30 |
| Fear of adverse events Low score High score | 1.0 0.37 | – 0.09–1.80 | 0.22 |
| Patient-related factors | |||
| Disease understanding Low score High score | 1.0 12.25 | – 4.51–18.76 | <10-4 |
| Impact of age on disease management Low score High score | 1.0 0.20 | – 0.05–1.35 | 0.10 |
| Fear of look of others Low score High score | 1.0 0.15 | – 0.07–0.92 | 0.04 |
| Socioeconomic factors | |||
| Interferences between living conditions and treatment Low score High score | 1.0 0.32 | – 0.05–2.26 | 0.24 |
| Burden of treatment cost | |||
| Low score | 1.0 | – | |
| High score | 0.40 | 0.04–3.93 | 0.43 |
†
Weighted on disease.
AOR: Adjusted odds ratio; HCP: Healthcare professional; MD: Medical doctor.
Figure 1 shows the clustering analysis using the SOM methodology, displaying polarized distributions of patient characteristics across the maps, as evidenced by the contrasting colorings from blue (the lowest values) to red (the highest values). Patients identified as globally similar with respect to answers to the WHO’s five-dimension framework questionnaire are grouped in districts represented as polygons placed at fixed positions on the map. The more those specific patient subgroups resemble each other, the closer they are on the map and, conversely, subgroups with fewer commonalities are further apart. For illustrative purpose, a selection of average district values is shown for representative districts in each SOM. After visual analysis of the SOMs, four clusters of patients with homogenous phenotypes were built. Cluster boundaries are shown at the top left of Figure 1 and as solid black lines across the maps, with detailed characteristics presented in Table 5.
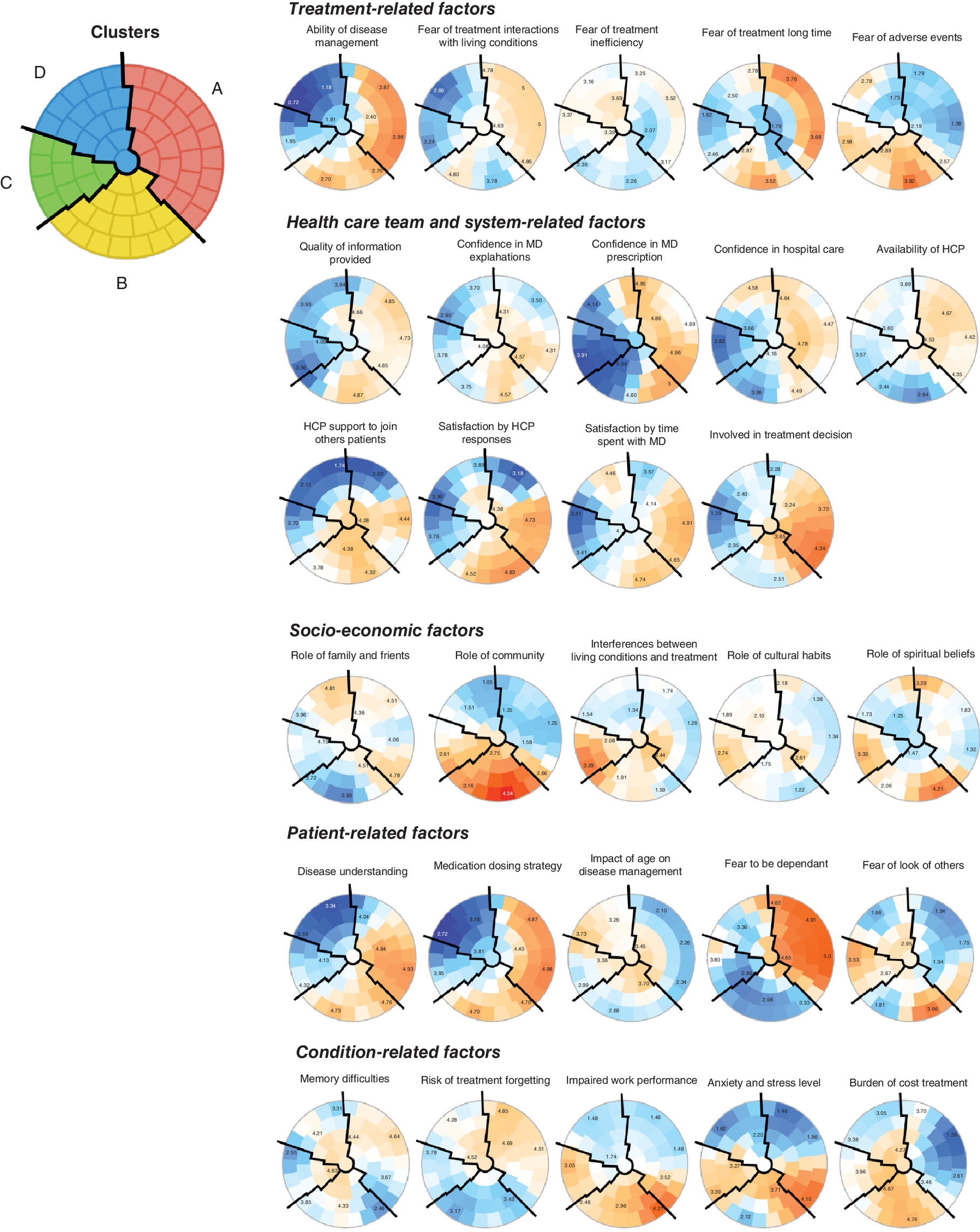
Figure 1. Results from the clustering analysis by self-organized maps.
(Left) Based on expert-driven visual identification of key patterns in the SOMs on the right, close districts were combined to provide four suitable clusters of patients. Cluster boundaries are delimited by solid black lines. (Right) Unsupervised analysis by SOMs placed all patients identified as globally similar for responses to PNAT questionnaire in one of 66 small groupings (‘districts’) throughout the map. The more patients were similar in terms of responses, the closer they are placed on the map. Each individual map shows the mean values or proportions per district for each characteristic; blue indicates the lowest average values and red the highest, with detailed numbers shown for a selection of representative districts in each SOM.
PNAT: Patient needs assessment tool; SOM: Self-organized map.
| Cluster A (n = 40) | Cluster B (n = 26) | Cluster C (n = 18) | Cluster D (n = 22) | |||
|---|---|---|---|---|---|---|
| Age | 40.7 (±12.7) | 39.5 (±10.3) | 41.7 (±10.8) | 43.1 (±17.8) | 0.811 | |
| Gender | Men | 19 (47.5%) | 9 (34.6%) | 8 (44.4%) | 11 (50.0%) | 0.695 |
| Women | 21 (52.5%) | 17 (65.4%) | 10 (55.6%) | 11 (50.0%) | ||
| Disease | Ankylosing spondylitis | 2 (5.0%) | 4 (15.4%) | 2 (11.1%) | 2 (9.1%) | 0.003† |
| Heart failure | 3 (7.5%) | 1 (3.8%) | 0 (0.0%) | 9 (40.9%) | ||
| Multiple sclerosis | 17 (42.5%) | 8 (30.8%) | 6 (33.3%) | 7 (31.8%) | ||
| Psoriasis | 15 (37.5%) | 13 (50.0%) | 8 (44.4%) | 4 (18.2%) | ||
| Severe eosinophilic asthma | 3 (7.5%) | 0 (0.0%) | 2 (11.1%) | 0 (0.0%) | ||
| Employed | No | 13 (33.3%) | 13 (54.2%) | 6 (35.3%) | 12 (60.0%) | 0.144 |
| Yes | 26 (66.7%) | 11 (45.8%) | 11 (64.7%) | 8 (40.0%) | ||
| Insurance | No | 19 (47.5%) | 14 (53.8%) | 9 (50.0%) | 9 (40.9%) | 0.842 |
| Yes | 21 (52.5%) | 12 (46.2%) | 9 (50.0%) | 13 (59.1%) | ||
| Education level | 1 | 3 (7.9%) | 4 (16.7%) | 4 (25.0%) | 6 (30.0%) | 0.305 |
| 2 | 25 (65.8%) | 11 (45.8%) | 8 (50.0%) | 8 (40.0%) | ||
| 3 | 10 (26.3%) | 9 (37.5%) | 4 (25.0%) | 6 (30.0%) |
†
p < 0.05. Results are means (± standard deviation) or n (%).
On the right part of the maps, cluster A (n = 40, 38%) was characterized by the highest levels of self-management ability. Confirming previous results from the main analysis on independent determinants of self-management, this cluster was also marked by high values in disease understanding by the patient, patient involvement in the treatment decision, satisfaction with time spent with the physician and low values in fear of how they are perceived by others. Interestingly, clustering analysis further revealed another group of patients with higher values in self-management ability (cluster B, n = 26, 25%), but with contrasted associated characteristics, notably including higher values in items regarding the role of community, impaired work performance, anxiety and stress level and, conversely to cluster A, higher values in the fear of how they were perceived by others.
Clusters C (n = 18, 17%) and D (n = 22, 21%) were marked by the lowest values in self-management ability, associated with low values in satisfaction by time spent with the physician, patients involved in treatment decision, fear of long-time treatment and interactions with living conditions (clusters C and D). These two clusters also differed with respect to the role of spiritual beliefs, interference between living conditions and treatment, anxiety and fear of adverse events (high in C while low in D). Key differences between patients as a function of the cluster to which they belong, and the clear separation between the different clusters are illustrated in the 2D biplot in Figure 2.
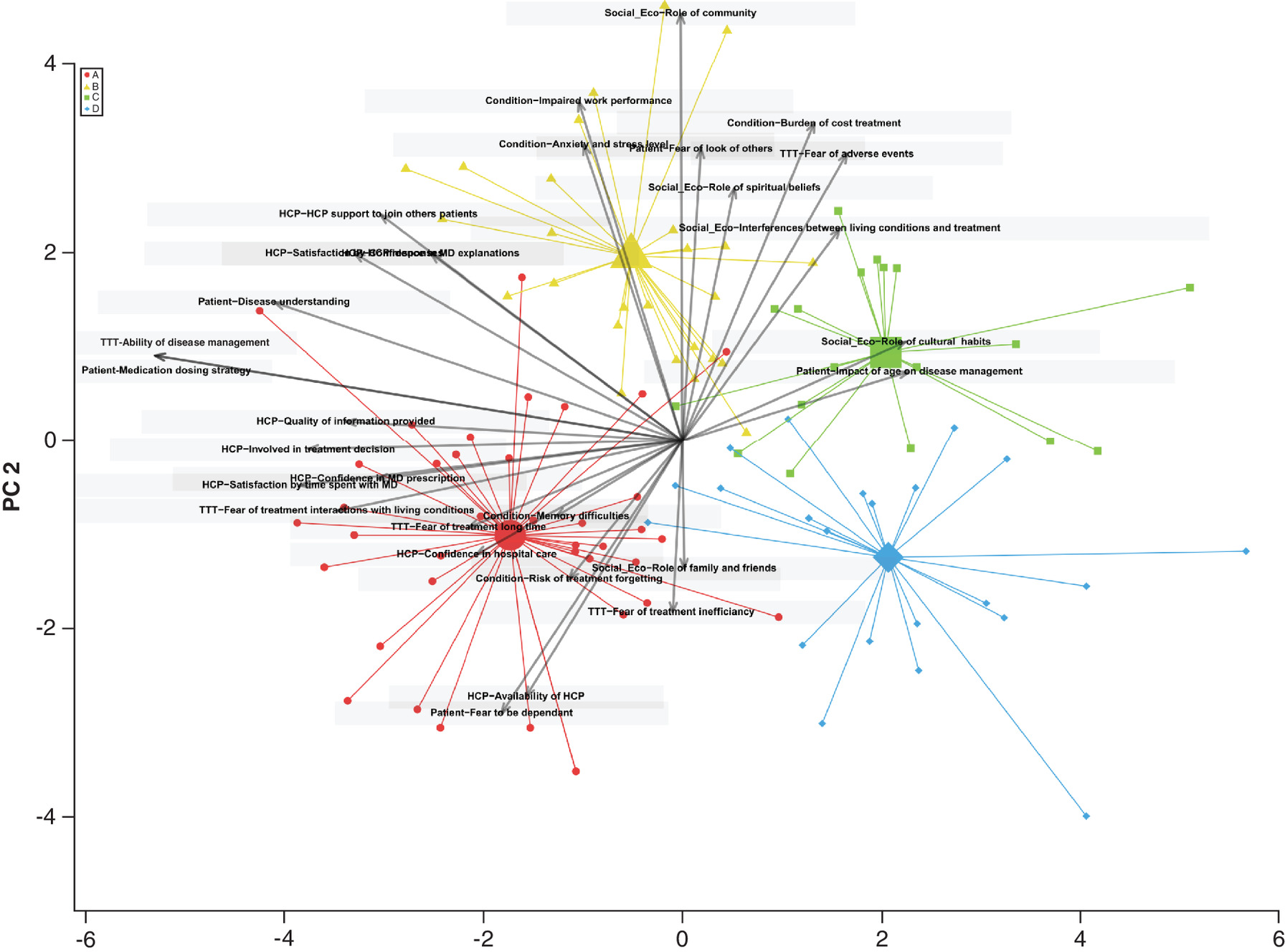
Figure 2. Two-dimensional biplot representations of patients’ responses to patient needs assessment tool questionnaire by clusters identified by self-organized map.
Responses to the PNAT questionnaire were used as characteristic parameters, allowing for visualization of the relations between variables used for building clusters (arrows), while simultaneously displaying the patients (dots), based on their individual characteristics. Results are projected onto the two first dimensions (PC1, PC2) generated by principal component analysis. Colors for observations correspond to the four-cluster solution from the cluster analysis in Figure 1, illustrating the excellent separation between the clusters achieved by the SOM analysis.
PNAT: Patient needs assessment tool; SOM: Self-organized map.
Discussion
To our knowledge, this is the first study undertaken in a GCC country to evaluate factors associated with the ability to self-manage chronic disease based on the WHO multidimensional framework. Although a prior study undertook a similar evaluation in Spain [17], we did not find additional studies that evaluated chronic disease self-management based on the WHO multidimensional framework. The key findings of this analysis are that a patient’s understanding of disease, involvement in treatment decision, age more than 40 years, the time spent with physician and fear of how patients were perceived by others were the most predictive factors associated with a high ability to self-manage a chronic disease. Knowledge about disease has also been identified as an important factor for self-management of chronic disease in a large metasynthesis analysis [7]. A cross-sectional study conducted in patients prescribed medication for at least two chronic conditions in two community health centers in the United States found that patients who did not receive information about their medication had higher adjusted odds of nonadherence [18]. Receiving complete information about treatment and having adequate knowledge about medication regimen were also identified as independent factors associated with adherence in a cross-sectional study conducted in adult patients prescribed medication for at least one chronic disease in Spain [17]. Additionally, a meta-analysis of observational studies that utilized the Necessity-Concerns Framework found that there was a significant relationship between necessity beliefs and adherence [19]. Taken together, these prior findings suggest that the correlation in our study between understanding of disease and high ability for disease self-management may result from patients’ increased belief in the necessity of treatment based on their understanding the disease.
The metasynthesis of Schulman-Green also identified prior self-management experience, the ability to create a self-management routine and life transitions as factors that positively influenced self-management of chronic disease [7]. This could account for the finding in our study that age over 40 years was predictive of a high ability to self-manage, as patients in this age group would have had more opportunities to engage in self-management in other aspects of their lives and with life transitions than people younger than 40 years. Age was also identified as independent significant factor associated with adherence in the Spanish cross-sectional study [17].
Interestingly, while our analysis found that sociocultural factors were not directly associated with patients’ ability to self-manage a chronic disease, there appears to be a relationship between some sociocultural factors and others factors that are directly associated with self-management ability. For example, clusters B and C had a higher proportion of patients with psoriasis – a disease that has visible symptoms – compared with the clusters A and D and had higher scores for fear of how other would look of them. Similarly, while role of spiritual beliefs was not a significant predictive factor, comparison of clusters C and D demonstrates a relationship between this sociocultural factor and the predictive factor of anxiety and stress levels. This could suggest that spiritual belief may reduce anxiety and demonstrates the relationship between some sociocultural factors and some predictive factors.
Result of prior studies are also heterogeneous with respect to their conclusions about the role of sociocultural factors and patients’ ability to self-manage chronic disease. A meta-analysis of patient-related determinants of glycemic control in patients with type 2 diabetes (T2D) in the GCC, which found that poor self-management was associated with poor glycemic control, also found that sociocultural factors did not impact directly glycemic control, suggesting that such factors may not have a significant impact across a broad range of chronic diseases in the GCC [20]. However, a study of diabetes medication adherence in the UAE found a statistically significant association between comporting with traditional Arab dress codes and nonadherence suggesting that sociocultural factors may in fact have an impact on medication adherence, which is a critical component of chronic disease self-management [21].
A systematic review that was not geographically restricted found that family support is associated with reduction in HbA1c [21], and a study conducted in Turkish immigrants in The Netherlands with multiple co-morbidities (average of 2.68 chronic diseases) found that there was a slightly stronger relationship between disease self-management and attachment to Dutch culture than between disease self-management and attachment to Turkish culture [21,22 ]. Another metasynthesis of factors affecting self-management of chronic illness also found that cultural beliefs could negatively impact disease self-management when such beliefs were not congruent with recommended self-management strategies [7]. This was exemplified by challenges in following nutrition and diet recommendations when this required food choices that were not part of traditional cultural diets.
Taken as a whole, these studies and the data reported here suggest that the role of sociocultural factors in patients’ ability to self-manage chronic disease may be a function of their specific cultural environments or the congruence (or lack thereof) between their cultural beliefs and self-management strategies. The cluster analysis we performed showed that some sociocultural factors were linked with other dimensions, particularly those dimensions related to health and chronic disease therapy. Clusters of patients who demonstrate specific patterns with regard to some sociocultural factors also demonstrated similar trends in therapy or healthcare provider-related dimensions. This suggests that some sociocultural factors indirectly impact adherence through their interaction with and effects on direct determinants of adherence. Such relationships may be difficult to discern from a single interview for question. For example, an individual may indicate a fear of developing an adverse event, but this response does not provide insight into whether this fear is based on the individual’s internal thinking or if it results from hearing about adverse events that others in the family or community may have experienced. This underscores the importance of understanding each patient’s individual sociocultural beliefs and priorities and suggests that there is no ‘one-size-fits-all’ approach to providing support that will enhance self-management ability. The varied findings among these different analyses are also likely indicative of a dearth of robust data on the role that sociocultural factors play in patient self-management across a variety of chronic diseases and cultures.
Another potential reason that sociocultural factors were not directly predictive of disease self-management in our study may be that it was conducted in a population of patients newly diagnosed with a chronic disease. However, the self-management behaviors of patients with chronic diseases have been shown to comprise four different developmental patterns that change over time and appear to be a function of whether patients consider their chronic disease to be stable, episodic or progressively deteriorating [23,24]. One study found that patients who considered their disease to be episodic or progressively deteriorating had higher self-management support needs, and that patients’ perceptions of their disease course and changes in how patients rate their own health are predictive of self-management support needs [24]. Consequently, it is possible that patients in our study, who are earlier in their disease journey, have not yet adopted disease perceptions or self-management behaviors for which sociocultural factors might play a more significant role as patients adapt to living with and managing a long-term illness. This may have important implications for clinical practice, as it suggests that self-management support needs may evolve over time and should be revisited on a periodic basis, and that healthcare providers should monitor patients’ perception of their disease course and health status in order to identify and address evolving support needs.
Time spent with the physician was also identified as a predictive factor for high ability to self-manage a chronic disease in multivariate analysis in our study and was also found to positively facilitate self-management in a metasynthesis analysis [7]. A longitudinal study in patients participating in 18 Dutch disease management programs also found that productive interactions between patients and physicians strongly predicted patients’ self-management abilities [25]. A study of factors impacting adherence to diabetes medication in the UAE found that adjusting these medications during Ramadan under a physician’s supervision was significantly associated with increased adherence [26]. These findings underscore the importance of creating healthcare environments and practices that foster constructive interactions between patients and physicians.
Educating patients about the importance of adhering to medication – whether conducted in person or using online/telemedicine platforms may also be important for improving patients’ ability to self-mange chronic diseases, as a study conducted in the UAE found that a 30-min educational session on the importance of medication adherence was associated with a statistically significant change in adherence to diabetes medication [26]. Patient education was also consistently identified as effective intervention for improving medication adherence in a systematic overview of 25 reviews of interventions designed to address non-adherence to medication [27].
The high and increasing prevalence of chronic diseases in GCC countries [8–10], which one author referred to as a “ticking time bomb” that requires urgent attention [8] underscores the need to develop multiple strategies that can both reduce disease incidence, improve detection and diagnosis, and enable improved outcomes for patients living with these diseases. Our results provide an important foundation for the development of effective self-management strategies for chronic disease patients in the UAE and, potentially, in other GCC countries.
This study reported here has several limitations. Self-management abilities were not measured by a validated scale, such as the Self-Management Ability Scale used in other studies [25]. However, we believe that the use of the patient perception of his or her self-management skill as a proxy is appropriate and robust for assessing ability. This approach provides a robust and conservative estimate of self-management ability and is a consistent indicator across all groups. While the PNAT has been validated in English, a potential limitation in this study is the use of an Arabic version of the PNAT, which has not been validated. The lack of a control group is another limitation and is a consequence of having all patients in the study participate in the adherence program for at least 1 year. Future studies should help to assess the added value of self-management abilities program and further identify factors that are predictive of high-ability self-management. Additionally, the current study was a cross-sectional design and thus cannot prospectively investigate longitudinal associations between management self-efficacy and determinants. A prospectively follow-up study of these patients, which is currently ongoing, will provide useful data for analyzing the importance of adherence to treatment as well as predictive factors associated to adherence.
A key strength of this study is that it investigated a large variety of factors, such as patients’ socioeconomic characteristics, factors related to patients and hospital care on patients’ self-management ability. Importantly, our study evaluated predictors of self-management in five diverse chronic diseases with different treatment paradigms, disease courses and self-management needs. Additionally, it is, to our knowledge, one of the first studies to evaluate self-management ability in a GCC.
Conclusion & recommendations
Conclusion
Adherence to long-term treatments for chronic diseases remains a challenging issue. The PNAT for self-management has interesting potential as a tool for developing personalized strategies to improve chronic disease self-management. Considerable attention should be given to multidimensional factors, such understanding of disease, involvement in treatment decision, age more than 40, fear of other people’s perceptions and discussion time spent with physician, as predictive factors for a high self-management ability. In frequently saturated and sometimes overcrowded healthcare facilities, HCPs are unlikely to have enough time to address all these issues (e.g., COVID-19 pandemic). Our findings also suggest that sociocultural factors may indirectly impact disease self-management ability through interactions with factors that are significant predictors of high self-management ability. These results provide important insights to support the development of specific new approaches designed to enhance adherence. Ongoing follow-up will provide additional insight into factors that predict high self-management ability and the impact of such ability on adherence to chronic disease treatments.
Recommendations
These findings suggest several actions that health authorities, clinicians and patient support organizations in the UAE may consider to improve adherence to long-term therapy for chronic diseases. First, more emphasis should be placed on meeting patients’ information needs, involving the patient in decisions about his or her treatment, and allocating sufficient time during patient visits for patients to ask and receive answers to disease and treatment-related decisions. Second, adherence programs in the UAE should be designed to provide additional resources and educational materials that patients can access on their own outside of a physician visit or formal health facility in order to more fully understand and be involved with decisions regarding their treatment. Third, health-focused entities within the UAE can leverage these findings and the availability of the PNAT to develop new approaches to improving medication adherence among patients with chronic diseases, and to conduct additional studies designed to identify other factors predictive of high self-management ability and the impact of such ability on adherence to chronic disease treatments.
•
The Patient Needs Assessment Tool (PNAT) for self-management has interesting potential as a tool for developing personalized strategies to improve chronic disease self-management.
•
In this study, the PNAT identified patients’ understanding of disease, involvement in treatment decision, age more than 40 years, the time spent with physician and fear of how patients were perceived by others as the most predictive factors associated with a high ability to self-manage a chronic disease.
•
Sociocultural factors have an indirect impact on disease self-management and may be a function of their specific cultural environments or the congruence (or lack thereof) between their cultural beliefs and self-management strategies.
•
Self-management support needs may evolve over time and should be revisited on a periodic basis, and that healthcare providers should monitor patients’ perception of their disease course and health status in order to identify and address evolving support needs.
•
Supporting patients with chronic diseases throughout the course of treatment – inside as well as outside the healthcare facility – significantly improves their ability to manage their disease, their adherence to treatment and hence the treatment outcome.
Acknowledgments
The authors thanks all patients who participated in the study. Special thanks to Stephanie Seiler for editing and revision of the manuscript.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing assistance has been used for the editing and revision of the manuscript and funded by Axios International.
Ethical conduct of research
An informed and signed consent has been obtained from all participants for data collection and treatment. All analyses were performed based on anonymized information.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
Sabate E. Adherence to Long Term Therapies: Evidence for Action. World Health Organization, Switzerland (2003).
2.
GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396, 1204–1222 (2020).
3.
Schulman-Green D, Jaser S, Martin F et al. Process of self-management in chronic illness. J. Nurs. Scholarsh. 44(20), 136–144 (2012).
4.
Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ. Couns. 48(2), 177–187 (2002).
5.
Corbin JM, Strauss AL. Unending Work and Care. Managing Chronic Illness at Home. Jossey-Bass Publisher, CA, USA (1988).
6.
Packer T, Kephart G, Audulv A et al. Protocol for development, calibration and validation of the Patient-Reported Inventory of Self-Management of Chronic Conditions (PRISM-CC). BMJ Open 10(9), e036776 (2020).
7.
Schulman-Green D, Jaser SS, Park C, Whittemore R. A metasynthesis of factors affecting self-management of chronic illness. J. Adv. Nurs. 72(7), 1469–1489 (2016).
8.
Alshaikh MK, Filippidis FT, Al-Omar HA, Rawaf S, Majeed A, Salmasi A-M. The ticking time bomb in lifestyle-related diseases among women in the Gulf Cooperation Council countries; review of systematic reviews. BMC Public Health 17, 536 (2017).
9.
Morgan SA, Ali MM, Channon AA et al. Prevalence and correlates of diabetes and its comorbidities in four Gulf Cooperation Council countries: evidence from the World Health Survey Plus. J. Epidemiol. Commun. Health 73(7), 630–636 (2019).
10.
Noibi S, Mohy A, Gouhar R, Shaker F, Lukic T, Al-Jahdali H. Asthma control factors in the Gulf Cooperation Council (GCC) countries and the effectiveness of ICS/LABA fixed dose combinations: a dual rapid literature review. BMC Public Health 20(1), 1211 (2020).
11.
Simoens S, Sinnaeve PR. Patient co-payment and adherence to statins: a review and case studies. Cardiovasc. Drugs Ther. 28, 99–109 (2014).
12.
Lewey J, Shrank WH, Avorn J, Liu J, Choudhry NK. Medication adherence and healthcare disparities: impact of statin co-payment reduction. Am. J. Manag. Care 21, 696–704 (2015).
13.
Likert R. A technique for the measurement of attitudes. Arch. Psychol. 22(140), 55 (1932).
14.
Sullivan GM, Artino AR. Analyzing and interpreting data from Likert-Type scales. J. Grad. Med. Educ. 5, 541–542 (2013).
15.
Self-organizing maps. In: Springer Series in Information Sciences (3rd Edition). Kohonen T, Huang ST, Schroeder RM (Eds). Springer, NY, USA (2001).
16.
Gao S, Mutter S, Casey A, Makinen VP. Numero: a statistical framework to define multivariable subgroups in complex population-based datasets. Int. J. Epidemiol. 48(2), 369–374 (2019).
17.
Fernandez-Lazaro CI, Garcia-Gonzalez JM, Adams DP et al. Adherence to treatment and related factors among patients with chronic conditions in primary care: a cross-sectional study. BMC Family Pract. 20, 132 (2019).
18.
Fernandez-Lazaro CI, Adams DP, Fernandez-Lazaro D, Garcia-Gonzalez JM, Garcia-Caballero A, Miron-Canelo JA. Medication adherence and barriers among low-income, uninsured patients with multiple chronic conditions. Res. Soc. Admin. Pharm. 15, 744–753 (2019).
19.
Horne R, Chapman SCE, Parham R, Freemantle N, Forbes S, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the necessity-concerns framework. PLoS ONE 8(12), e80633 (2013).
20.
Al-Haj Mohd MMM, Phung H, Sun J, Morisky DE. The predictors to medication adherence among adults with diabetes in the United Arab Emirates. J. Diabetes Metabol. Disord. 15, 30 (2016).
21.
Stopford R, Winkley K, Ismail K. Social support and glycemic control in type 2 diabetes: a systematic review of observational studies. Patient Educ. Couns. 93(3), 549–558 (2013).
22.
Cramm JM, Nieboer AP. Acculturation is associated with older Turkish immigrants’ self-management abilities. BMC Public Health 19, 1228 (2019).
23.
Audulv A. The overtime development of chronic illness self-management patterns: a longitudinal qualitative study. BMC Public Health 13, 452 (2013).
24.
Van Houtum L, Rijken M, Heijmans M, Groenewegen P. Self-management support needs of patients with chronic illness: do needs for support differ according to the course of illness? Patient Educ. Couns. 93, 626–632 (2013).
25.
Cramm JM, Nieboer AP. Chronically ill patients’ self-management abilities to maintain overall well-being: what is needed to take the next step in the primary care setting? BMC Family Pract. 16, 123 (2015).
26.
Al-Haj Mohd MMM, Phung H, Sun J, Morisky DE. Improving adherence to medication in adults with diabetes in the United Arab Emirates. BMC Public Health 16, 857 (2016).
27.
Anderson LJ, Nuckols TK, Coles C et al. A systematic overview of systematic reviews evaluating medication adherence interventions. Am. J. Health Syst. Pharm. 77, 138–147 (2020).
Information & Authors
Information
Published In
Pages: 179 - 192
PubMed: 34806911
Copyright
© 2021 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 22 July 2021
Accepted: 1 November 2021
Published online: 22 November 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Factors impacting self-management ability in patients with chronic diseases in the United Arab Emirates, 2019. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0177
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Laura Hesters, Sofie Compernolle, Dominique Van de Velde Van de Velde, Katrien De Cocker, More Than Just Talk: The Role of Therapist Interactions in Patient Adherence, Patient Preference and Adherence, 10.2147/PPA.S604401, Volume 20, (1-18), (2026).
- Ingrid Olsson, George Kephart, Tanya Packer, Sabine Björk, Ulf Isaksson, Anna Nordström, Åsa Audulv, The Patient Reported Inventory of Self-Management of Chronic Conditions (PRISM-CC): testing for bias across patient characteristics and languages, Quality of Life Research, 10.1007/s11136-025-04124-5, 35, 1, (2026).
- Hesters Laura, Compernolle Sofie, De Craemer Marieke, De Cocker Katrien, Effectiveness of a self-determination theory-based module to improve interaction styles of physiotherapy students: a quasi-experimental study, BMC Medical Education, 10.1186/s12909-025-07805-4, 25, 1, (2025).
- Joel Ladner, Alshurafa Sawsan, Anas Nofal, Mohamed Rana, Malak Ammar, Joseph Saba, Etienne Audureau, Factors impacting chronic disease medication adherence in the UAE: a prospective cohort study, 2021–2022, Journal of Comparative Effectiveness Research, 10.57264/cer-2025-0020, 14, 6, (2025).
- Leila Rafiee-Vardanjani, Narges Arsalani, Farahnaz Mohammadi-Shahbolaghi, Kian Norouzi Tabrizi, Self-Management in Hemodialysis Patients: A Concept Analysis, Journal of Nursing and Midwifery Sciences, 10.5812/jnms-158696, 12, 2, (2025).
- Karina Toro-Aguirre, Alfonso Urzúa, Factores vinculados al automanejo de la enfermedad crónica: Una revisión sistemática, Universitas Psychologica, 10.11144/Javeriana.upsy23.fvae, 23, (1-14), (2025).
- Laura Hesters, Sofie Compernolle, Marieke De Craemer, Veerle Duprez, Ann Van Hecke, Katrien De Cocker, Understanding (de)motivating interaction styles of healthcare professionals in training: a profile approach, Advances in Health Sciences Education, 10.1007/s10459-025-10414-x, 30, 5, (1425-1451), (2025).
- Girma Yadesa, Abebe Abera, Shamsedin Amme, Getahun Fetensa, Diriba Mulisa, Getachew Alemu, Self-management practice and associated factors among asthmatic patients on follow-up care at public tertiary hospitals, south west, Ethiopia, 2022, PLOS ONE, 10.1371/journal.pone.0300589, 19, 8, (e0300589), (2024).
- Ambreen Tharani, Ann Van Hecke, Tazeen Saeed Ali, Veerle Duprez, Perspectives on self‐management of individuals living with chronic illnesses: A qualitative study in the Asian context, Research in Nursing & Health, 10.1002/nur.22339, 46, 6, (591-602), (2023).
- Joël Ladner, Farah Madi, Roshel Jayasundera, Joseph Saba, Etienne Audureau, Phone contacts and treatment discontinuation predict survival cancer patients in a subsidized drug access program, Journal of Comparative Effectiveness Research, 10.57264/cer-2022-0210, 12, 7, (2023).