Cost–effectiveness of brentuximab vedotin for the treatment of cutaneous T-cell lymphoma
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the cost–effectiveness of brentuximab vedotin (BV) versus physician’s choice (methotrexate or bexarotene) for treating advanced cutaneous T-cell lymphoma. Materials & methods: A partitioned-survival model was developed from the National Health Service perspective in England and Wales. Model inputs were informed by the ALCANZA trial, real-world UK data, published literature or clinical experts. Results: Over the modeled lifetime, BV dominated physician’s choice and provided an additional 1.58 life-years and 1.09 higher quality-adjusted life years with a net cost saving of £119,565. The net monetary benefit was £152,326 using a willingness-to-pay threshold of £30,000/quality-adjusted life year. Results were robust in sensitivity and scenario analyses. Conclusion: BV is a highly cost-effective treatment for advanced cutaneous T-cell lymphoma.
Cutaneous T-cell lymphoma (CTCL) is a rare, heterogeneous group of non-Hodgkin lymphomas affecting less than 2.2 in 10,000 people in Europe [1]. Variants of CTCL include: mycosis fungoides (MF; representing >50% of all CTCL cases), primary cutaneous anaplastic large-cell lymphoma (pcALCL) and Sézary syndrome (SS) [2–4]. Advanced CTCL includes those with MF stage IIB+, SS and pcALCL. While early localized disease is considered indolent, approximately 25% of patients progress to advanced disease during their life and 30% of patients present with advanced disease [5].
Patients with CTCL live with high symptom burden and require extensive symptom management which impacts daily functioning [6]. Physical CTCL symptoms, such as pain, pruritus, alopecia, odorous, disfiguring and weeping skin lesions, lead to substantial long-term burden of disease and can negatively impact patients’ psychological and social well-being [7–9]. Advanced MF (stage IIB–IVB) or SS is associated with poor prognosis with a median survival of 36 months [5] and is characterized by the development of aggressive and devastating lesions (e.g., painful disfiguring tumors, ulceration, erythroderma and eventual visceral spread) leading to higher burden of illness [10,11]. Patients with advanced disease require extensive healthcare resources and accrue greater costs compared with patients with early disease [12].
Commonly used systemic therapies, including bexarotene (BEX) or methotrexate (MTX), have low response rates of short duration [13–16]. Relapse is common and risk of progression is high, particularly among patients with advanced disease [11,17]. Relapse and disease progression lead to treatment cycling until patients exhaust all treatment options and move to symptom management. The burden of end-stage care is immense, with patients requiring intensive medical care and frequent specialized dressing changes for nonhealing wounds, which are characteristic of advanced CTCL [18].
Brentuximab vedotin (BV) is an anti-CD30 antibody-drug conjugate approved in Europe, the USA, Australia and other markets for the treatment of adults with CD30+ CTCL after at least one prior systemic therapy. Data from the Phase III, open-label, randomized controlled ALCANZA trial (NCT01578499) showed statistically significant improvement in both response rate and progression-free survival (PFS) with BV compared with physician’s choice (PC; MTX or BEX) in both the intention-to-treat (ITT) and advanced CTCL populations [16]. BV also demonstrated clinically meaningful reductions in symptom burden compared with PC as measured by Skindex-29, a dermatology-specific patient-reported outcome [19]. In clinical practice, BV has been used as a bridge to allogeneic stem cell transplant (alloSCT) for eligible patients [20,21]. AlloSCT is the only potentially curative treatment for CTCL [22]. The objective of this analysis was to assess the cost–effectiveness of BV versus PC for the treatment of CTCL.
Methods
Overview & structure
A partitioned-survival model with five health states was developed in accordance with the NICE guidance [23] to estimate the cost–effectiveness of BV versus PC among patients with CTCL from the perspective of the National Health Service in England and Wales. Results were presented over a lifetime horizon of 45-years with a maximum age of 100 years. The model used weekly cycles, and costs and quality-adjusted life years (QALYs) were discounted at 3.5% per year. The model was built using Microsoft Excel (Microsoft Corporation, WA, USA) with statistical analyses conducted in R (R Foundation; Vienna, Austria).
In line with local clinical guidelines [22], the base-case model considered the advanced CTCL population informed by ALCANZA; 95 patients had advanced CTCL (49 BV, 46 PC) with MF stage IIB+ or pcALCL (median follow-up of 33.9 months) [24]. Model results using the ITT population are reported in a scenario analysis.
Patients entered the model in the preprogression health state and received treatment with BV or PC. PC included MTX or BEX in accordance with the ALCANZA trial design [16]. Patients who received alloSCT followed the pathway depicted with red health states; the remaining followed the pathway depicted with blue health states (Figure 1). Eligibility for alloSCT was assessed at 18 weeks (i.e., equivalent to six cycles of BV), at which time a proportion of transplant-eligible patients without progression proceeded to the alloSCT health state. Patients underwent alloSCT following the Stanford Protocol [25]. After alloSCT, patients who relapsed moved to the alloSCT relapse health state. Patients without alloSCT who progressed moved from the preprogression health state to the non-alloSCT postprogression state. Patients could transition to death from any health state.
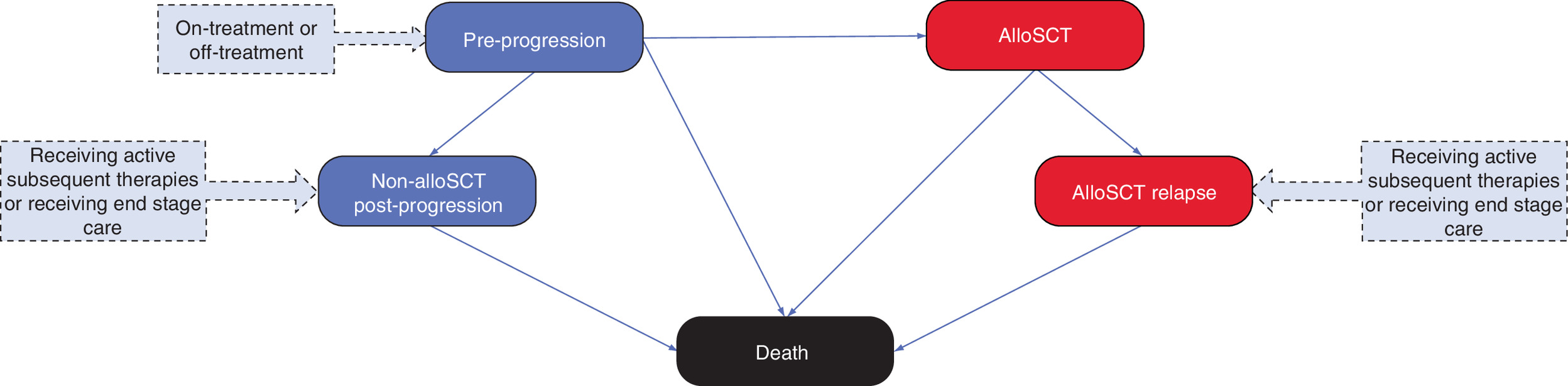
Figure 1. Model structure.
Blue health states indicate the pathway for a patient who has not met the eligibility criteria for an alloSCT. Red health states reflect the pathway for a patient meeting these criteria and receiving an alloSCT.
alloSCT: Allogeneic stem cell transplant.
Based on guidance from clinical experts (n = 10), patients who progressed received further systemic anticancer treatments until options were exhausted, followed by a prolonged period with end-stage symptom care. In line with the British Association of Dermatologists and UK Cutaneous Lymphoma Group guidelines [22], treatment options for patients postprogression, independent of alloSCT receipt, during ‘active treatment’ phase include: gemcitabine, CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone) and other mono-chemotherapy. Total skin electron beam therapy was an option for patients who had not received an alloSCT postprogression; it was assumed that all patients undergoing alloSCT received total skin electron beam therapy prior to transplant per the Stanford Protocol conditioning regimen [25]. Following exhaustion of therapies, patients in the postprogression states received end-stage care.
To model multiple lines of subsequent therapy, a ‘payoff approach’ was used [26]. The approach calculated the proportion of patients leaving the preprogression states in each model cycle and then applied the mean total costs and outcomes received in both the postprogression ‘active treatment’ phase and the ‘end-stage management’ phase. The model used a continuous discounting approach to ensure that future costs and outcomes were discounted appropriately.
Clinical inputs
Clinical inputs are provided in Supplementary Table 1. The model used data from ALCANZA to inform the PFS and overall survival (OS) for patients not receiving alloSCT [16,24] and real-world UK data to inform the post-alloSCT outcomes [27,28]. For non-alloSCT states, PFS was modeled using Weibull parametric curves fit independently for BV and PC. In ALCANZA, OS did not statistically differ between BV and PC. OS was neither a primary nor secondary end point in ALCANZA, and the OS data were limited by very few events (<30%) and confounding from high crossover from PC to BV (46%). Therefore, OS was assumed the same for BV and PC in this model, and the ALCANZA data were fit using a log-logistic model. For alloSCT, PFS was modeled with a Gompertz curve and OS with a log-normal curve using real-world UK data [27,28]; survival extrapolations incorporated background population mortality [29]. PFS and OS for non-alloSCT and alloSCT were validated by clinical experts and compared against published data [11,30]. Scenario analyses explored alternative parametric models (Supplementary Table 1).
Time on treatment with BV and PC was taken directly from the long-term follow-up from ALCANZA [24] with no extrapolation necessary as data were complete. Time on treatment for subsequent therapies was informed by the literature and clinical expert opinion [31–33].
Based on clinical expert guidance, it was assumed that 40% of patients with advanced CTCL who had sufficient disease control would be eligible for an alloSCT, considering: age, co-morbidities, likelihood of matching to a donor and patient choice. Based on clinical input, sufficient disease control was defined as achieving a partial or complete response (jointly defined as overall response rate, ORR, in ALCANZA) and was informed by ALCANZA (BV: 68.8%; PC: 17.8%) [16]. The ORR was multiplied by the 40% eligibility assumption which translated to 27.5% of patients who received an alloSCT in the BV arm and 7.1% in the PC arm. The timing of alloSCT and the proportion of responders eligible for alloSCT were explored in scenario analyses.
Cost inputs
Drug costs (Supplementary Table 2) were estimated based on average weight or body surface area using list prices from UK-specific sources. Duration of therapy in the non-alloSCT group was derived from ALCANZA and was assumed to be 18 weeks (i.e., six cycles) for the alloSCT group, based on clinical input. Administration costs were estimated from NHS Reference Costs 2016/17 (Supplementary Table 2). The base-case cost of alloSCT represented an average of the cost of haploidentical transplant and of transplant with unrelated donor including the procedure cost and 2 years of follow-up [34]. A scenario analysis used the NHS Reference Costs for alloSCT.
Due to the scarcity of published evidence on resource use among patients with advanced CTCL, particularly for end-stage management, semistructured interviews were conducted with clinical experts from all seven supraregional CTCL centers in England and Wales. The interviews covered pain, anxiety/depression, itch relief and skin care and wound management, including specialized dressings. The average for each measurement informed the base-case (Supplementary Table 2). The lower range informed a scenario analysis (Supplementary Table 3).
Grade ≥3 adverse events (AEs) for patients on treatment with BV or PC in the preprogression state were included in the model. The proportion of AEs treated and the treatment setting were informed by expert opinion.
Utility inputs
ALCANZA measured health-related quality of life (HRQOL) using the Skindex-29 and European Quality of Life 5-Dimension 3 Level (EQ-5D-3L) Version measures [16]. The Skindex-29 is a 30-item, dermatology-specific, self-reported questionnaire assessing symptoms, emotions and function, and has been extensively studied and validated in different patient populations, including CTCL [6,16,37]. The EQ-5D-3L is a generic instrument covering five domains of patient-reported HRQOL – mobility, self-care, usual activities, pain/discomfort and anxiety/depression – and is recommended for use in economic evaluations [23]. In the base-case analysis, the EQ-5D-3L responses from ALCANZA [16,19] were converted into utilities using the EQ-5D UK Tariff values (Supplementary Table 4) [38]. Health-state specific utilities were then estimated using mixed-effects regression models with progression included as a covariate.
Evidence from ALCANZA suggested that the EQ-5D-3L may be insensitive to the burden associated with CTCL (e.g., constant severe, intense itching causing insomnia) [19]. Therefore, HRQOL derived from the EQ-5D-3L may not capture the extent of the condition or fully reflect the change in patients’ HRQOL. The Skindex-29 is more sensitive to the CTCL burden and a recognized tool for HRQOL by experts in CTCL. However, no algorithms have been published to map Skindex-29 values into EQ-5D-3L utilities for use in economic evaluations. To explore this further, mixed-effects regression models controlling for Skindex-29 score and progression were used in a scenario analysis [19,39].
Utilities for other health states including alloSCT and end-stage care were obtained from the literature (Supplementary Table 4) [40,41]. In the base case, it was assumed that the HRQOL impact of AEs was reflected in the ALCANZA data. In a scenario analysis, disutilities for AEs were obtained from the literature.
Outcomes
Model outcomes included lifetime costs, life-years, QALYs, incremental cost–effectiveness ratio (incremental costs per QALY gained) as well as clinically relevant outcomes such as the time spent preprogression. When BV had higher QALYs and lower costs than PC, BV was ‘dominant’ and the incremental cost–effectiveness ratio was not expressed. To facilitate the interpretation of results, the net monetary benefit (NMB) was reported using a willingness-to-pay (WTP) threshold of £30,000 per QALY. NMB was calculated as NMB = ΔQALY * WTP - ΔCost, where Δ signifies the difference between BV and PC. A positive NMB implies that BV was cost-effective at the WTP threshold.
Sensitivity & scenario analyses
Extensive sensitivity analyses were conducted to explore parameter uncertainty, including probabilistic sensitivity analysis (PSA) and one-way sensitivity analyses (OWSA). The deterministic OWSA investigated the impact of varying each parameter in isolation between its lower and upper bound (i.e., 95% CI). A standard error of 10% of the mean was assumed in cases where bounds were unavailable. In the PSA, 5000 Monte Carlo simulations were performed, randomly sampling from each parameter’s assigned distribution simultaneously. Scenario analyses were conducted to explore the impact of structural assumptions (Supplementary Tables 1–4). An additional scenario analysis considered the ITT population from ALCANZA and used the ITT results for OS, PFS, ORR and time on treatment [16,24].
Results
Base case results for advanced CTCL population
Treatment with BV increased the time spent in the preprogression health states, where patients have higher utility and lower resource utilization, compared with PC (an estimated 1.33 vs 0.54 years). Over the modeled lifetime, BV dominated PC in the advanced CTCL population (Table 1, NMB: £152,326). BV provided an additional 1.58 life years and 1.09 QALYs with a net cost saving of £119,565 compared with PC.
| BV | PC | Incremental | |
|---|---|---|---|
| Costs | £504,619 | £624,184 | -£119,565 |
| QALYs | 4.33 | 3.24 | 1.09 |
| LYs | 8.93 | 7.36 | 1.5858 |
| ICER | – | – | BV dominates |
| NMB | – | – | £152,326 |
BV: Brentuximab vedotin; ICER: Incremental cost–effectiveness ratio; LY: Life year; NMB: Net monetary benefit; PC: Physician’s choice; QALY: Quality-adjusted life year.
Sensitivity analyses
In OWSA, BV remained dominant over PC in all analyses (i.e., lower costs and higher QALYs) with a positive NMB. The difference in total costs for BV compared with PC was most sensitive to the costs for CTCL-specific end-stage care and the proportion of patients eligible for alloSCT (Figure 2). Using the lower bound of £1684 for the cost of CTCL-specific end-stage care yielded the lowest NMB (£119,360) while using the upper bound of £2506 yielded the highest NMB (£185,292). The PSA indicated a 98.4% chance that BV was cost-effective at a WTP threshold of £30,000 per QALY (Supplementary Figure 1).
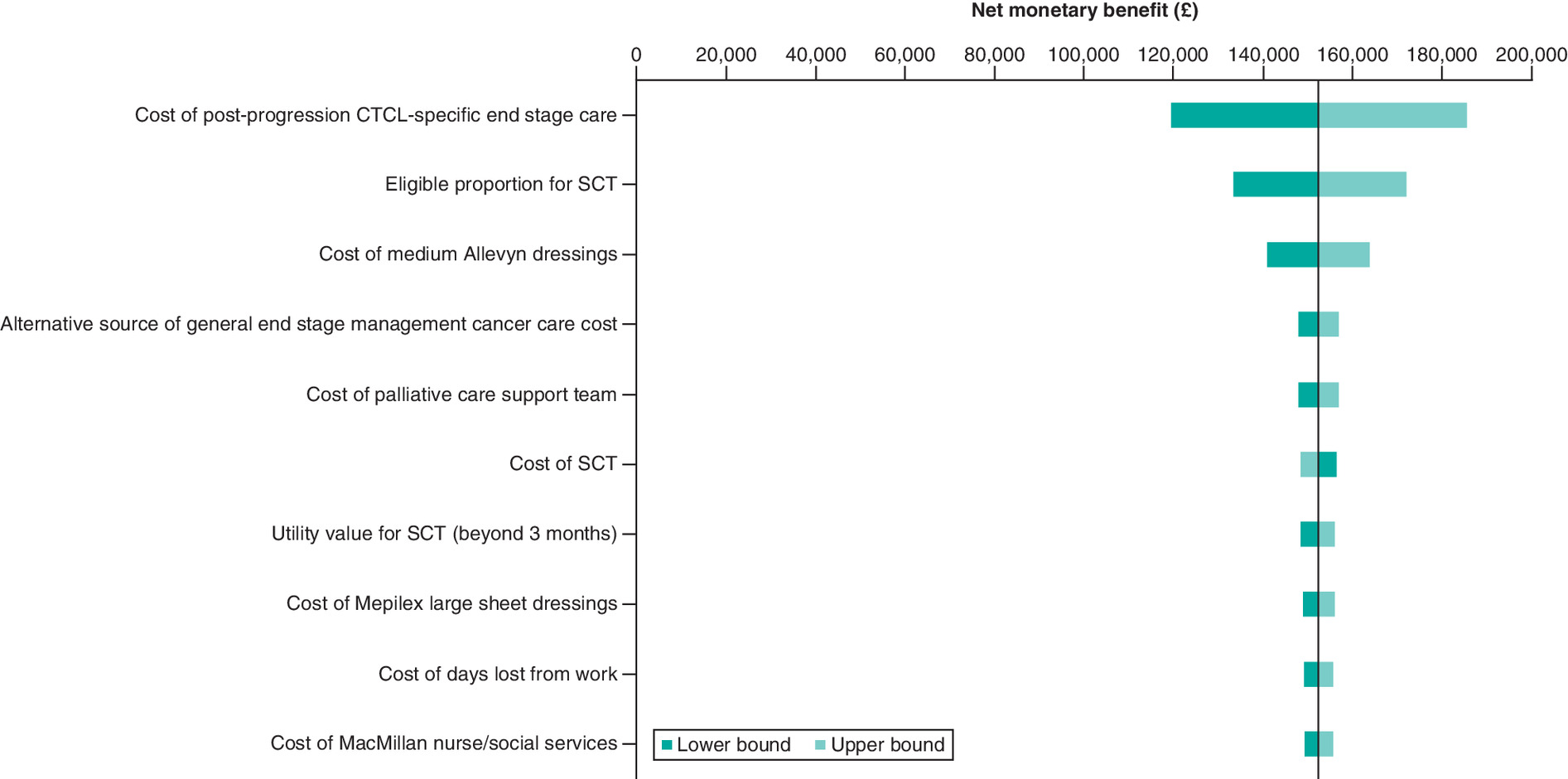
Figure 2. One-way sensitivity analysis applied to the economic model base case (top 10 most influential parameters).
CTCL: Cutaneous T-cell lymphoma; SCT: Stem cell transplant.
Scenario analyses
In scenario analyses (Table 2), BV was dominant over PC (NMB: £94,822 to £172,027). Two scenarios resulted in an NMB less than £100,000: the scenario utilizing lower resource use postprogression (NMB: £98,736) and the scenario considering an extreme upper bound for OS benefit (9.5 months) of BV relative to PC (NMB: £94,822).
| ICER | NMB | |
|---|---|---|
| Advanced population | ||
| Base case | BV dominates | £152,326 |
| Scenario 1a: Survival benefit for BV: 2 months | BV dominates | £139,901 |
| Scenario 1a: Survival benefit for BV: 4 months | BV dominates | £128,262 |
| Scenario 1a: Survival benefit for BV: 9.5 months | BV dominates | £94,822 |
| Scenario 2: Alternative OS curve for PC (log-normal) | BV dominates | £151,468 |
| Scenario 3: Alternative OS curve for alloSCT (Weibull) | BV dominates | £152,321 |
| Scenario 4: Alternative PFS curves for BV and PC (exponential) | BV dominates | £172,027 |
| Scenario 5a: Duration of treatment prior to alloSCT: 12 weeks | BV dominates | £155,600 |
| Scenario 5a: Duration of treatment prior to alloSCT: 24 weeks | BV dominates | £149,136 |
| Scenario 6: 20% of responders eligible for alloSCT | BV dominates | £102,859 |
| Scenario 7: Lower cost of alloSCT (£64,125) | BV dominates | £159,015 |
| Scenario 8: Lower resource use postprogression | BV dominates | £98,736 |
| Scenario 9: Predicted utility values for BV and PC arms and progressive disease | BV dominates | £152,959 |
| Scenario 10: Include AE-related treatment disutilities | BV dominates | £151,987 |
| ITT population | ||
| Scenario 11: ITT population | BV Dominates | £193,279 |
AE: Adverse event; BV: Brentuximab vedotin; ICER: Incremental cost–effectiveness ratio; ITT: Intent-to-treat; NMB: Net monetary benefit; OS: Overall survival; PC: Physician’s choice; PFS: Progression-free survival; QALY: Quality-adjusted life year.
In an analysis of the ITT population from ALCANZA, BV also dominated PC (NMB: £193,279). BV provided an additional 0.68 LYs and 0.78 QALYs with a net cost saving of £169,984 compared with PC.
Discussion
The results of this cost–effectiveness analysis demonstrate the clinical and economic value of BV for the treatment of CTCL in the UK. BV improves disease control and does so for a longer duration compared with PC, such that over the modeled lifetime, patients receiving BV experience gains in life expectancy and QALYs with lower total costs. Results are robust to differing model inputs and assumptions explored in sensitivity and scenario analyses.
Delaying CTCL progression reduces time spent in a more severe and costly postprogression health state. In ALCANZA, BV demonstrated superior clinical efficacy versus PC in the advanced CTCL population in terms of complete or partial response (BV 69%; PC 18%) and delayed progression (median PFS: 16.4 months for BV and 3.5 months for PC) [16]. Real-world data support the response rate (ORR: 75%) and tolerability of BV [20]. An ORR over 70% is unusual in anti-CTCL therapy, where systemic treatments in advanced disease tend to have response rates between 30 and 40% which are often partial and of short duration [22,42]. Postprogression, patients exhaust the limited anticancer treatment options quickly and subsequently receive resource-intense end-stage care focused on symptom management until they succumb to the disease. Due to the chronic nature of CTCL and the prolonged time spent in end-stage management, the costs accrued in end-stage management are high. In the base-case model, end-stage management costs accounted for over half of the total costs. Although the difference in lifetime costs between BV and PC was most sensitive to the cost of end-stage management, results continued to favor BV when using the lower range of resource utilization. As BV is administered over a 3-week cycle with few cycles needed, these results suggest that the lifetime cost-savings from reduced time in end-stage management offset the upfront drug costs of BV.
In addition to improving clinical response and delaying progression, it is important for treatment to reduce the symptom burden of CTCL, including chronic severe pain and itching, in order to improve patients’ HRQOL. In ALCANZA, BV demonstrated a clinically meaningful and statistically significant improvement in Skindex-29 symptom burden compared with PC (mean change of -27.96 vs -8.62; p < 0.001) [19]. The EQ-5D-3L, a generic measure of HRQOL, may be insensitive to changes in symptom burden; previous analyses have shown poor correlation between the EQ-5D-3L and the Skindex-29 [39]. Scenario analyses attempted to control for Skindex-29 in the EQ-5D-3L utility estimation; these results remain limited by the sensitivity of the EQ-5D-3L. While further research into a CTCL-specific, preference-based measure is needed, cost–effectiveness results appear insensitive to alternative utility estimates.
Current survival data from ALCANZA are immature and do not suggest an OS benefit with BV versus PC. In the base-case analysis, the OS for BV was assumed to be equivalent to that of PC. The observed gains in life-years with BV over the modeled lifetime arise from the improved response rates with BV, which allows for a greater proportion of patients to be eligible for a potentially curative transplant. This is supported by findings from a real-world setting, where BV was successfully used to bridge to transplant in five of 17 patients with advanced CTCL [21]. Scenario analyses explored the impact of varying the proportion of responders eligible for alloSCT (20%, an extreme lower bound) and varying BV’s impact on OS (up to 9.5 months, an extreme upper bound). The results from these analyses suggest that BV remains a cost-effective treatment option even at extreme bounds.
This study has several limitations. As discussed above, the full benefits of BV may not be captured in the model. OS data remain immature, the OS treatment effect is confounded by crossover from PC to BV, and HRQOL measures may not capture all skin-related and physiological impacts of CTCL. The latter limitation was acknowledged by a NICE appraisal committee, which concluded that the full impact of BV on patients’ HRQOL may not be fully captured [43]. Further work is needed on capturing the HRQOL impact of CTCL and understanding what aspects of CTCL are not sufficiently captured by the EQ-5D-3L. There is a scarcity of evidence pertaining to resource use relevant to patients with advanced CTCL, particularly for end-stage management. In this analysis, estimates of end-stage resource use were informed by clinical experts across all supraregional centers in the UK [44,45]. Further research based on patient-level data could provide more robust evidence-based estimates of CTCL resource use including the variability between patients. The results of this study may not be generalizable to other countries given the differences in healthcare resource use and costs between countries. Finally, the treatment pathway for patients with CTCL is complex particularly postprogression, and this model, like all models, makes simplifying assumptions. Here, a ‘payoff’ approach was employed to retain a simple structure while incorporating complex postprogression treatment pathways. While this approach allows sufficient flexibility to investigate key uncertainties and assumptions, a level of granularity is lost.
Conclusion
BV has demonstrated significantly improved response, delayed progression and improved symptom burden compared with PC for the treatment of CTCL [16,19]. Based on these data, the results from the current economic model demonstrated that patients treated with BV spent more time preprogression, had a longer life expectancy and accrued more QALYs over a lifetime. These results indicate that BV is a highly cost-effective treatment option for patients with advanced CTCL.
•
In a Phase III, open-label, randomized controlled trial (ALCANZA, NCT01578499), brentuximab vedotin (BV) demonstrated statistically significant improvement in response rate, progression-free survival and symptom burden compared with physician’s choice (PC) of methotrexate or bexarotene, among patients with cutaneous T-cell lymphoma (CTCL) who have had at least one prior therapy.
•
The current study evaluated the cost–effectiveness of BV versus PC for treating advanced CTCL from the perspective of the NHS in England and Wales.
•
A partitioned-survival model was developed with model inputs informed by the ALCANZA trial, real-world UK data, published literature and clinical experts.
•
Over the modeled lifetime, BV dominated PC and provided an additional 1.58 life-years and 1.09 higher quality-adjusted life years with a net cost saving of £119,565.
•
The net monetary benefit was £152,326 using a willingness-to-pay threshold of £30,000/quality-adjusted life year.
•
Results were robust to differing model inputs and assumptions explored in the sensitivity and scenario analyses.
•
BV is a highly cost-effective treatment option for patients with advanced CTCL.
•
The economic value is attributed to the improvements in health-related quality of life and reductions in costs associated with delaying disease progression and reducing time spent in costly end-stage management characterized by low health-related quality of life.
Author contributions
T Podkonjak, H Cranmer and L-I Cheng contributed to the conceptualization, methodology, data curation, formal analysis, data interpretation, writing and revising manuscript. J Scarisbrick contributed to the data interpretation, writing and revising manuscript. G McCarthy and C Lilley was responsible for the conceptualization, methodology, formal analysis, data interpretation, writing and revising manuscript.
Acknowledgments
The authors acknowledge Fiona Fields, Medical Manager, Takeda UK for conduct of interviews that are cited in this work.
Financial & competing interests disclosure
This study was funded by Takeda Pharmaceuticals International Co. T Podkonjak, H Cranmer and L-I Cheng are employees of Takeda. G McCarthy and C Lilley are employees of BresMed, which received consulting fees for conducting this work. J Scarisbrick has provided consultancy services to Takeda, Helsinn, Recordati, Mallinkcrodt, Kyowa and Miragen. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The authors also kindly acknowledge Alexandra Ellis from Stratevi, LLC for her medical writing contributions in preparing this manuscript.
Ethical conduct of research
Authors confirm that all the research meets the ethical guidelines, including adherence to the legal requirements of the study country.
Data-sharing statement
The input data included in the economic model are available in the Appendix.
Supplementary Material
File (supplementary materials.docx)
- Download
- 234.73 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
European Medicines Agency. Public summary of opinion on orphan designation: brentuximab vedotin for the treatment of cutaneous T-cell lymphoma (EMA/COMP/923105/2011 Rev.2). https://www.ema.europa.eu/en/documents/orphan-designation/eu/3/11/939-public-summary-positive-opinion-orphan-designation-brentuximab-vedotin-treatment-cutaneous-t_en.pdf
2.
Zinzani PL, Bonthapally V, Huebner D, Lutes R, Chi A, Pileri S. Panoptic clinical review of the current and future treatment of relapsed/refractory T-cell lymphomas: cutaneous T-cell lymphomas. Crit. Rev. Oncol. Hematol. 99, 228–240 (2016).
3.
Wilcox RA. Cutaneous T-cell lymphoma: 2016 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 91(1), 151–165 (2016).
4.
Bekkenk MW, Geelen FA, van Voorst Vader PC et al. Primary and secondary cutaneous CD30(+) lymphoproliferative disorders: a report from the Dutch Cutaneous Lymphoma Group on the long-term follow-up data of 219 patients and guidelines for diagnosis and treatment. Blood 95(12), 3653–3661 (2000).
5.
Scarisbrick JJ, Prince HM, Vermeer MH et al. Cutaneous Lymphoma International Consortium study of outcome in advanced stages of mycosis fungoides and Sezary syndrome: effect of specific prognostic markers on survival and development of a prognostic model. J. Clin. Oncol. 33(32), 3766–3773 (2015).
6.
Demierre MF, Tien A, Miller D. Health-related quality-of-life assessment in patients with cutaneous T-cell lymphoma. Arch. Dermatol. 141(3), 325–330 (2005).
7.
Jonak C, Porkert S, Oerlemans S et al. Health-related quality of life in cutaneous lymphomas: past, present and future. Acta Derm. Venereol. 99(7), 640–646 (2019).
8.
Molloy K, Jonak C, Woei AJF et al. Characteristics associated with significantly worse quality of life in mycosis fungoides/Sezary syndrome from the Prospective Cutaneous Lymphoma International Prognostic Index (PROCLIPI) study. Br. J. Dermatol. 182(3), 770–779 (2020).
9.
Selman LE, Beynon T, Radcliffe E et al. ‘We’re all carrying a burden that we’re not sharing’: a qualitative study of the impact of cutaneous T-cell lymphoma on the family. Br. J. Dermatol. 172(6), 1581–1592 (2015).
10.
Willemze R, Jaffe ES, Burg G et al. WHO-EORTC classification for cutaneous lymphomas. Blood 105(10), 3768–3785 (2005).
11.
Agar NS, Wedgeworth E, Crichton S et al. Survival outcomes and prognostic factors in mycosis fungoides/Sezary syndrome: validation of the revised International Society for Cutaneous Lymphomas/European Organisation for Research and Treatment of Cancer staging proposal. J. Clin. Oncol. 28(31), 4730–4739 (2010).
12.
Gu T, Raspa S, Tsang Y, Drake W. The burden of illness of mycosis fungoides cutaneous T-cell lymphoma: a retrospective cohort study of a commercially insured population in the U.S. Value Health 19(7), A608 (2016).
13.
Zackheim HS, Kashani-Sabet M, McMillan A. Low-dose methotrexate to treat mycosis fungoides: a retrospective study in 69 patients. J. Am. Acad. Dermatol. 49(5), 873–878 (2003).
14.
Duvic M, Martin AG, Kim Y et al. Phase 2 and 3 clinical trial of oral bexarotene (Targretin capsules) for the treatment of refractory or persistent early-stage cutaneous T-cell lymphoma. Arch. Dermatol. 137(5), 581–593 (2001).
15.
Duvic M, Hymes K, Heald P et al. Bexarotene is effective and safe for treatment of refractory advanced-stage cutaneous T-cell lymphoma: multinational Phase II–III trial results. J. Clin. Oncol. 19(9), 2456–2471 (2001).
16.
Prince HM, Kim YH, Horwitz SM et al. Brentuximab vedotin or physician’s choice in CD30-positive cutaneous T-cell lymphoma (ALCANZA): an international, open-label, randomised, Phase III, multicentre trial. Lancet 390(10094), 555–566 (2017).
•• This original article reports the results from the pivotal clinical trial ALCANZA.
17.
Hughes CF, Khot A, McCormack C et al. Lack of durable disease control with chemotherapy for mycosis fungoides and Sezary syndrome: a comparative study of systemic therapy. Blood 125(1), 71–81 (2015).
18.
Orlowska D, Selman LE, Beynon T et al. ‘It’s a traumatic illness, traumatic to witness’: a qualitative study of the experiences of bereaved family caregivers of patients with cutaneous T-cell lymphoma. Br. J. Dermatol. 179(4), 882–888 (2018).
19.
Dummer R, Prince HM, Whittaker S et al. Patient-reported quality of life in patients with relapsed/refractory cutaneous T-cell lymphoma: results from the randomised Phase III ALCANZA study. Eur. J. Cancer 133, 120–130 (2020).
•• This original article reports the patient reported quality of life results from the pivotal clinical trial ALCANZA.
20.
Engelina S, Saggu M, Yoo J et al. Brentuximab a novel antibody therapy: real-world use confirms efficacy and tolerability for CD30-positive cutaneous lymphoma. Br. J. Dermatol. 182(3), 799–800 (2020).
21.
Ritchie S, Qureshi I, Molloy K et al. Evaluation of haematopoietic stem cell transplantation in patients diagnosed with cutaneous T-cell lymphoma at a tertiary care centre: should we avoid chemotherapy in conditioning regimes? Br. J. Dermatol. 182(3), 807–809 (2020).
22.
Gilson D, Whittaker SJ, Child FJ et al. British Association of Dermatologists and UK Cutaneous Lymphoma Group guidelines for the management of primary cutaneous lymphomas 2018. Br. J. Dermatol. 180(3), 496–526 (2019).
• Describes the UK clinical guidelines for the management of primary cutaneous lymphomas, including cutaneous T-cell lymphoma.
23.
National Institute for Health and Care Excellence (NICE). Guide to the methods of technology appraisal 2013 (PMG9). London, UK (2013). https://www.nice.org.uk/process/pmg9/chapter/foreword
24.
Horwitz SM, Scarisbrick JJ, Dummer R et al. Updated analyses of the international, open-label, randomized, Phase 3 Alcanza study: longer-term evidence for superiority of brentuximab vedotin versus methotrexate or bexarotene for CD30-positive cutaneous T-cell lymphoma (CTCL). Blood 130(Suppl. 1), 1509 (2017).
25.
Lowsky R, Takahashi T, Liu YP et al. Protective conditioning for acute graft-versus-host disease. N. Engl. J. Med. 353(13), 1321–1331 (2005).
26.
Woods B, Eleftherios S, Palmer S, Latimer N, Soares M. NICE DSU Technical Support Document 19: partitioned survival analysis for decision modelling in health care: a critical review (2017). http://nicedsu.org.uk/wp-content/uploads/2017/06/Partitioned-Survival-Analysis-final-report.pdf
27.
Morris S, Scarisbrick J, Kanfer E et al. Reduced intensity allogeneic stem cell transplantation for advanced stage mycosis fungoides and Sezary syndrome. a series of 53 patients from the UK. Eur. J. Cancer 101, S36 (2018).
• This original article reports real-world data from the UK informing the post allogeneic transplant outcomes in the economic model.
28.
Palanicawandar R, Morris S, Lozano-Cerrada S et al. Allogeneic stem cell transplantation for advanced cutaneous T-cell lymphoma with minimal-intensity conditioning. In: European Organisation for Research and Treatment of Cancer. London, UK (2017). https://www.eortc.org/event/8587/
• This original article reports real-world data from the UK informing the post allogeneic transplant outcomes in the economic model.
29.
Office for National Statistics. National life tables, UK: 2014 to 2016. Statistical Bulletin (2017). https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/bulletins/nationallifetablesunitedkingdom/2014to2016
30.
Kim YH, Liu HL, Mraz-Gernhard S, Varghese A, Hoppe RT. Long-term outcome of 525 patients with mycosis fungoides and Sezary syndrome: clinical prognostic factors and risk for disease progression. Arch. Dermatol. 139(7), 857–866 (2003).
31.
Dummer R, Quaglino P, Becker JC et al. Prospective international multicenter Phase II trial of intravenous pegylated liposomal doxorubicin monochemotherapy in patients with stage IIB, IVA, or IVB advanced mycosis fungoides: final results from EORTC 21012. J. Clin. Oncol. 30(33), 4091–4097 (2012).
32.
Duvic M, Tetzlaff MT, Gangar P, Clos AL, Sui D, Talpur R. Results of a Phase II trial of brentuximab vedotin for CD30+ cutaneous T-cell lymphoma and lymphomatoid papulosis. J. Clin. Oncol. 33(32), 3759–3765 (2015).
33.
Morris S, Scarisbrick J, Frew J et al. The results of low-dose total skin electron beam radiation therapy (TSEB) in patients with mycosis fungoides from the UK Cutaneous Lymphoma Group. Int. J. Radiat. Oncol. Biol. Phys. 99(3), 627–633 (2017).
34.
Debals-Gonthier M, Siani C, Faucher C et al. Cost-effectiveness analysis of haploidentical vs matched unrelated allogeneic hematopoietic stem cells transplantation in patients older than 55 years. Bone Marrow Transplant. 53(9), 1096–1104 (2018).
35.
Curtis L, Burns A. Unit costs of health and social care 2017 (2017). https://www.pssru.ac.uk/project-pages/unit-costs/unit-costs-2017/
36.
Statista. Euro (EUR) to British pound sterling (GBP) average annual exchange rate from 1999 to 2019 (2020).https://www.statista.com/statistics/412806/euro-to-gbp-average-annual-exchange-rate/
37.
Wright A, Wijeratne A, Hung T et al. Prevalence and severity of pruritus and quality of life in patients with cutaneous T-cell lymphoma. J. Pain Symptom Manage. 45(1), 114–119 (2013).
38.
Dolan P. Modeling valuations for EuroQol health states. Med. Care 35(11), 1095–1108 (1997).
39.
Podkonjak T, McCarthy G, Cranmer H, Birnie R. PCN472: patient reported health state utilities in cutaneous T-cell lymphoma (CTCL) - an analysis of EQ-5D and SKINDEX-29 data collected from the ALCANZA trial. Value Health 22(Suppl. 3), S528 (2019).
40.
van Agthoven M, Vellenga E, Fibbe WE, Kingma T, Uyl-de Groot CA. Cost analysis and quality of life assessment comparing patients undergoing autologous peripheral blood stem cell transplantation or autologous bone marrow transplantation for refractory or relapsed non-Hodgkin’s lymphoma or Hodgkin’s disease: a prospective randomised trial. Eur. J. Cancer 37(14), 1781–1789 (2001).
41.
Swinburn P, Shingler S, Acaster S, Lloyd A, Bonthapally V. Health utilities in relation to treatment response and adverse events in relapsed/refractory Hodgkin lymphoma and systemic anaplastic large cell lymphoma. Leuk. Lymphoma 56(6), 1839–1845 (2015).
42.
Scarisbrick JJ, Bagot M, Ortiz-Romero PL. The changing therapeutic landscape, burden of disease, and unmet needs in patients with cutaneous T-cell lymphoma. Br. J. Haematol. 192 (4), 683–696 (2020).
43.
National Institute for Health and Care Excellence (NICE). Brentuximab vedotin for treating CD30-positive cutaneous T-cell lymphoma. Technology appraisal guidance [TA577] (2019). https://www.nice.org.uk/guidance/ta577
• This is the final appraisal document from NICE that details the committee’s recommendations and rationale regarding brentuximab vedotin.
44.
Takeda Pharmaceutical Company. Clinicial expert questionnaires – Resource use and palliative care associated with CTCL. (2018).
45.
Takeda Pharmaceutical Company. Clinicial expert clinical consultation – Dr Whitaker. (2018).
Information & Authors
Information
Published In
Pages: 193 - 202
PubMed: 34879742
Copyright
© 2021 Future Medicine Ltd.
History
Received: 19 August 2021
Accepted: 28 October 2021
Published online: 9 December 2021
Keywords:
Topics
Authors
Funding Information
Takeda Pharmaceuticals International Co
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of brentuximab vedotin for the treatment of cutaneous T-cell lymphoma. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0201
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- YiRan Wang, YiQin Shu, Hao Wu, Advances in Drug Research Targeting Neutrophils for the Treatment of Rheumatoid Arthritis, Current Rheumatology Reports, 10.1007/s11926-025-01201-z, 27, 1, (2025).
- Charles Dumontet, Janice M. Reichert, Peter D. Senter, John M. Lambert, Alain Beck, Antibody–drug conjugates come of age in oncology, Nature Reviews Drug Discovery, 10.1038/s41573-023-00709-2, 22, 8, (641-661), (2023).