Are treatment effects consistent with hypothesized mechanisms of action proposed for postoperative delirium interventions? Reanalysis of systematic reviews
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Postoperative delirium (POD) is associated with increased morbidity and is poorly understood. The aim of this review was to identify putative mechanisms through re-analysis of randomized trials on treatment or prevention of POD. Materials & methods: A systematic review was performed to identify systematic reviews of treatments for POD. Constituent randomized controlled trials were identified, and interventions were grouped according to hypothesized mechanisms of action. Effects were meta-analyzed by hypothesized mechanism and timing of intervention. Results: A total of 116 randomized controlled trials described 47 individual interventions for POD, with nine mechanisms identified. The largest effects were observed for postoperative inflammation reduction, and preoperative reinforcement of sleep–wake cycle. Conclusion: This approach identifies treatments focused on mechanisms of action that may be front runners for future trials and interventions.
Postoperative delirium (POD) is an acute, fluctuating disturbance of consciousness with inattention, occurring in up to 61% patients shortly after surgical and anesthesia interventions [1]. It is associated with significantly increased morbidity and mortality rates up to 5 years after the event [2]. The etiology of POD is multifactorial, with general anesthesia, poor pain management and inadequate perioperative hydration all implicated [3]. Advanced age, pre-existing cognitive impairment and multiple pre-existing comorbidities are also thought to increase risk [4]. Therefore, it is plausible that different intervention strategies might be employed, each with varying effect depending on the etiology.
Current approaches to the prevention and management of POD are based on piecemeal evaluation of idiosyncratic interventions of unclear application [5]. The term POD covers different phenotypes (with potentially variable etiologies) [6], highlighting the need to explore mechanisms of action that are incompletely understood. Analysis of trial data at the level of specific drug type used might prove to be overly granular, especially when active interventions are compared. A more global view considering interventions according to their hypothesized mechanism of action (hMOA) might provide a useful balance between heterogeneity of effects and excessive granularity linked to use of a single intervention. Such an approach also has the potential to inform the development of multimodal interventions through establishing both efficacy and external validity [7].
The aim of this study was to review the literature to identify the hMOA for interventions evaluated in trials to treat or prevent POD. The secondary aim was to re-analyze randomized controlled trials (RCTs) grouped by hMOA and timing of intervention.
Materials & methods
Design
This review was conducted as a re-analysis of data from published systematic reviews. In keeping with previous reanalyzes of systematic reviews [8], this review was not eligible for registration and no risk-of-bias assessment was performed on the included studies, which have been critically appraised elsewhere.
Eligibility criteria
The sample for this re-analysis was RCTs, already critically appraised in systematic reviews, which evaluated interventions for the treatment or prevention of POD. Systematic reviews were part of the sample frame if they were complete, published and reported the incidence of POD as an outcome. Reviews were excluded if: they did not address POD in the perioperative setting; they did not report incidence of POD; they did not use systematic review methodology; or the full text could not be retrieved. RCTs from this sample frame were excluded if: they used active controls (may compare two interventions with actions through the same general mechanism); a full text article was unavailable; they were nonrandomized trials; incidence of POD was not reported clearly as an outcome.
Search strategy
The search strategy was devised through pearl growing (Supplementary Material 2) [9]. The final searches (Supplementary Materials 3 & 4) were conducted in Ovid MEDLINE on 30 September 2019, and on the Cochrane Library on 4 October 2019. The bibliographies of eligible articles were searched for completeness. No language restrictions were applied. An updated search of MEDLINE through PubMed was conducted in August 2021 to identify any systematic reviews published in the interim period.
Study selection
Emily Boxell and Dan Hind assessed systematic reviews for inclusion. At least two of Jeyinn Wong, Yuhaniz Malik and Min Hyung Lee, in discussion with Matthew Lee and Matthew Wilson assessed RCTs from the sample frame for eligibility in this review. Each study was included only once.
Data collection process
In Phase I, full-text versions of primary research articles were retrieved and the following data was tabulated: citation; specific intervention examined; timing of intervention compared with surgery (pre-, intra-, post- and perioperative); hMOA; and incidence of POD in each intervention arm and its definition.
In Phase II, a second round of extraction by two reviewers was performed. Studies were grouped by hMOA by both researchers. Data extracted included study population descriptors (cardiac/noncardiac surgery, age and sex), outcome definition and timing of measurement, the identified intervention and comparator and events and total numbers in each arm of the study.
Synthesis
Definition of hypothesized mechanisms of action
A conceptual system of mechanisms of action was developed with the support of healthcare professionals with expert knowledge in clinical pharmacy (Richard Bourne), anesthesia (Matthew Wilson/Iain McCullagh) and surgery (Matthew Lee). This conceptual framework was divided into three high level categories (pharmacological, individual-level nonpharmacological and policy-level interventions). Interventions were grouped by reference to these categories based upon agreed commonalities in the hMOA and were stratified according to timing of intervention relative to surgery. In this way, umbrella groupings of hMOA for interventions to treat or prevent POD were identified.
Meta-analysis
Studies comparing an intervention to placebo or standard care were eligible for inclusion in the meta-analysis (MA). Where authors attributed more than one mechanism of action to an intervention, a member of the research team (Matthew Wilson) was asked to adjudicate on the mechanism being assessed, without reference to the outcome data. To avoid double counting of participants, Matthew Wilson selected one of the intervention arms to include, again, without access to study findings.
Separate MA were performed based on the timing of intervention (pre-, intra-, post- or perioperative), using RevMan 5 (Cochrane Collaboration, Copenhagen, Denmark). Subgroup analyses were performed for each hMOA. To ensure claims of statistical significance were conservative, MA was conducted using the Mantel–Haenszel random effects model, to calculate risk ratio (RR) [10]. About 95% CI were also calculated (presented in brackets following RR). Between-study variation in observed effects not attributable to chance alone was estimated using I2. We hypothesized that the plausibility of mechanistic groupings would be supported by low I2 values.
Results
Study selection
A total of 130 systematic reviews were identified through MEDLINE, Cochrane library and hand searching. Eighty nine were excluded at screening. Of the remaining 39 reports, a further 21 reports were excluded due to; ineligible outcomes (n = 16), ineligible interventions (n = 2), insufficient systematic methodology (n = 1), did not reference primary data (n = 1) and one paper that was not retrievable by the close of the study (n = 1). This one inaccessible systematic review was therefore excluded, contained six RCTs. It was not possible to ascertain whether these RCTs were considered in any of the eligible systematic reviews. In total, 18 systematic reviews including 116 unique primary research articles, were identified. Data from one RCT could not be collected, as it was yet to be published and so was excluded from the mapping of mechanism review. See PRISMA chart (Figure 1) and Table 1 for further details.
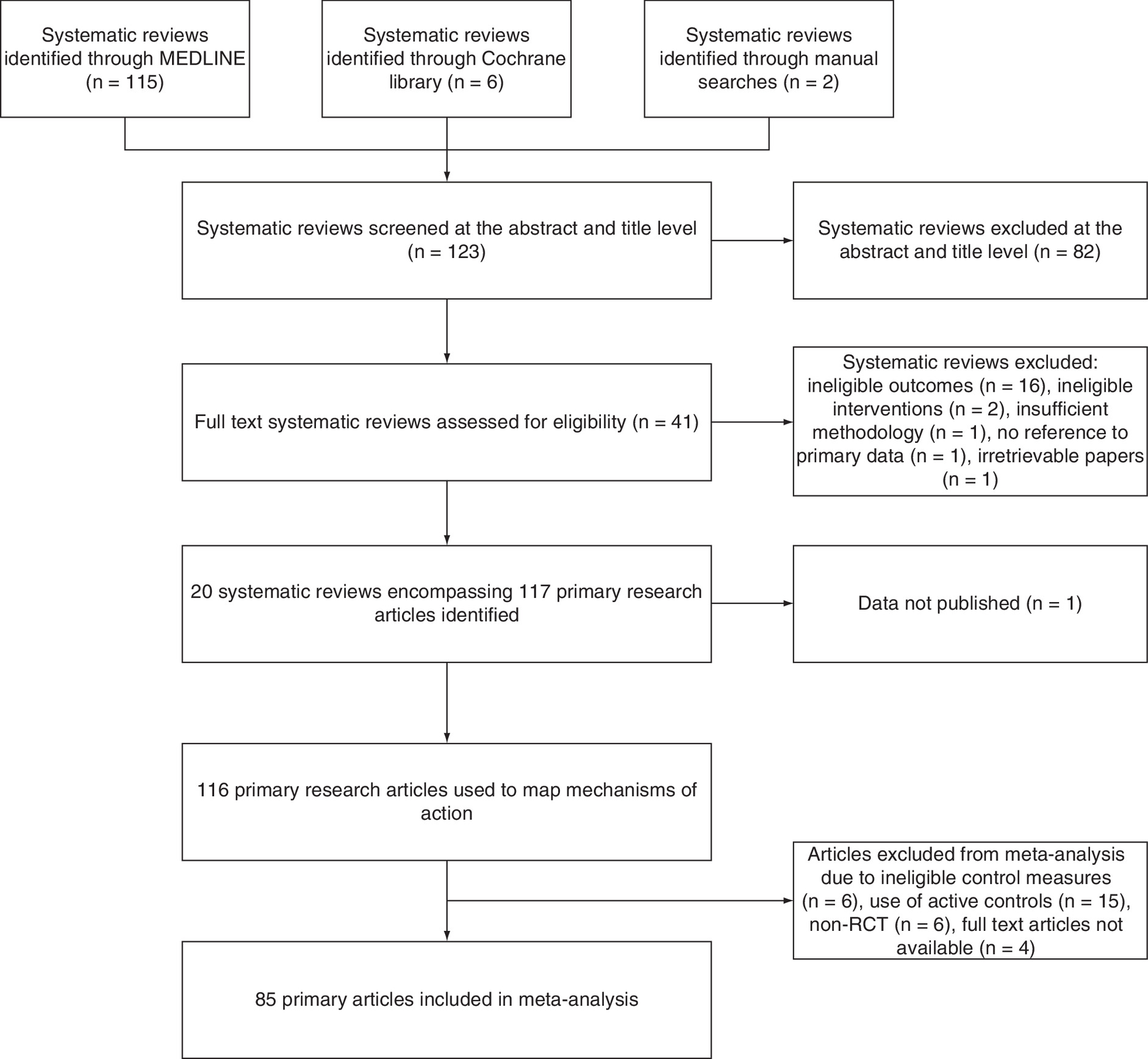
Figure 1. PRISMA flowchart.
RCT: Randomized controlled trial.
| Systematic review/meta-analysis | Primary research articles included (n) | Patients (n) | Type of surgery | Pharmacological, nonpharmacological or policy interventions | Ref. |
|---|---|---|---|---|---|
| Duan (2018) | 18 RCTs | 3309 | 9 Cardiac 6 Noncardiac 3 Orthopedic | Pharmacological | [11] |
| Fok (2015) | 6 RCTs | 1710 | 1 Cardiac 1 Noncardiac 3 Orthopedic 1 Gastrointestinal | Pharmacological | [12] |
| Gilmore (2013) | 5 RCTs | 1491 | 1 Cardiac 1 Noncardiac 2 Orthopedic 1 Gastrointestinal | Pharmacological | [13] |
| Haque (2019) | 3 RCTs | 282 | 1 Cardiac 1 Noncardiac 1 Orthopedic | Pharmacological | [14] |
| Igwe (2020) | 20 RCTs 2 before/after | 5075 | 3 Cardiac 11 Orthopedic 9 Noncardiac | 15 Pharmacological 7 Nonpharmacological | [15] |
| Janssen (2019) | 31 RCTs + 4 ‘before-and after’ studies | 9663 | 12 Orthopedic 11 Abdominal 1 Vascular 11 Combination | 22 Pharmacological 4 Nonpharmacological 9 Policy | [1] |
| Leigh (2019) | 3 RCTs | 205 | Cardiac | Pharmacological | [4] |
| Liu (2019) | 38 RCTs | 20302 | 15 Cardiac 3 Noncardiac 13 Orthopedic 1 Abdominal 6 Combination | Pharmacological | [16] |
| Lu (2019) | 13 RCTs | 2015 | 1 Cardiac 3 Noncardiac 3 Orthopedic 1 Oral 1 Abdominal 2 Esophageal 2 Combination | 9 Pharmacological 4 Nonpharmacological | [17] |
| Luo (2018) | 5 RCTs | 2868 | 3 Cardiac 2 Noncardiac | Pharmacological | [18] |
| Leon-Salas (2020) | 18 RCTs | 4381 | 1 Cardiac 9 Orthopedic 1 Colorectal 2 Gastrointestinal 3 Noncardiac | Pharmacological | [19] |
| Moyce (2014) | 29 RCTs | 7098 | 3 Noncardiac 14 Orthopedic 5 Abdominal 2 Esophageal 1 Laparoscopic 1 Ophthalmic 1 Combination 2 Not specified | 24 Pharmacological 2 Nonpharmacological 3 Policy | [20] |
| Mu (2015) | 13 RCTs | 5848 | Cardiac | Pharmacological | [21] |
| Pan (2019) | 11 RCTs | 2890 | 5 Orthopedic 1 Thoracic 1 Oral 4 Combination | Pharmacological | [22] |
| Shields (2017) | 4 RCTs | 973 | Orthopedic | Policy | [23] |
| Tao (2018) | 14 RCTs | 14139 | Cardiac | Pharmacological | [24] |
| Teslyar (2013) | 5 RCTs | 1491 | 1 Cardiac 1 Noncardiac 2 Orthopedic 1 Abdominal | Pharmacological | [25] |
| Wu (2018) | 10 RCTs | 1387 | Cardiac | Pharmacological | [26] |
| Zeng (2019) | 6 RCTs | 2102 | 6 Noncardiac | 6 Pharmacological | [27] |
| Zhang (2013) | 38 RCTs | 4667 | 9 Cardiac 2 Noncardiac 18 Orthopedic 6 Abdominal 2 Thoracic 1 Combination | 32 Pharmacological 4 Nonpharmacological 2 Policy | [28] |
Table includes information as to number of RCTs considered by each systematic review, number of patients involved, types of surgery and intervention type (pharmacological, nonpharmacological or policy level).
RCT: Randomized controlled trial.
The 116 primary research articles from the initial phase were further reviewed for inclusion in the MA. Of these, 31 were excluded due to ineligible outcome measures (n = 6), the use of active controls (n = 15), were not RCTs (n = 6) and full text articles were not available (n = 4). This left 85 articles for MA.
Study characteristics
Studies reported seven different preoperative interventions, 17 intraoperative interventions, 21 postoperative interventions and 25 perioperative interventions.
The types of operation undertaken in the primary research articles were cardiac (n = 29), noncardiac (n = 10), orthopedic (n = 41), thoracic (n = 1), abdominal (n = 10), vascular (n = 1), oral (n = 2), ENT (n = 2), esophageal (n = 2), cancer (n = 3), mixed (n = 5) and not specified (n = 9).
Of the 116 primary research articles, 112 were RCTs and four articles were ‘before and after’ studies, which were investigating policy-level interventions.
Synthesis
In total, 57 interventions were considered in the 116 studies (Supplementary Material 5). For six of the 116 included primary research articles, hMOA were obtained only from the abstracts as the full-texts were not accessible.
Categorizing mechanisms of action of intervention
Nine hypothesized mechanisms of action for reducing incidence of POD were identified from the individual studies. These hypothesized mechanisms of action are:
•
Reducing delirium-inducing medication.
•
Optimizing analgesia.
•
Targeted pharmacological therapy against dysregulation of neuronal activity.
•
Re-enforcing normality of sleep–wake cycle.
•
Reducing inflammatory response.
•
Optimized and personalized care (referring to a range of interventions which are intended to reduce risk of delirium related to baseline characteristics and physiological risk. This is typically a function of older persons medical care).
•
Minimizing hypoxemia.
•
Improving cerebral oxygen metabolism.
•
Anxiolysis (nonpharmacological).
Five of the hypothesized mechanisms of action of interventions encompassed both nonpharmacological and pharmacological interventions. Pharmacological interventions targeted eight mechanisms of action and nonpharmacological interventions targeted six different mechanisms of action, these are summarized in Figure 2. Further stratified information is presented in Supplementary Material 6.
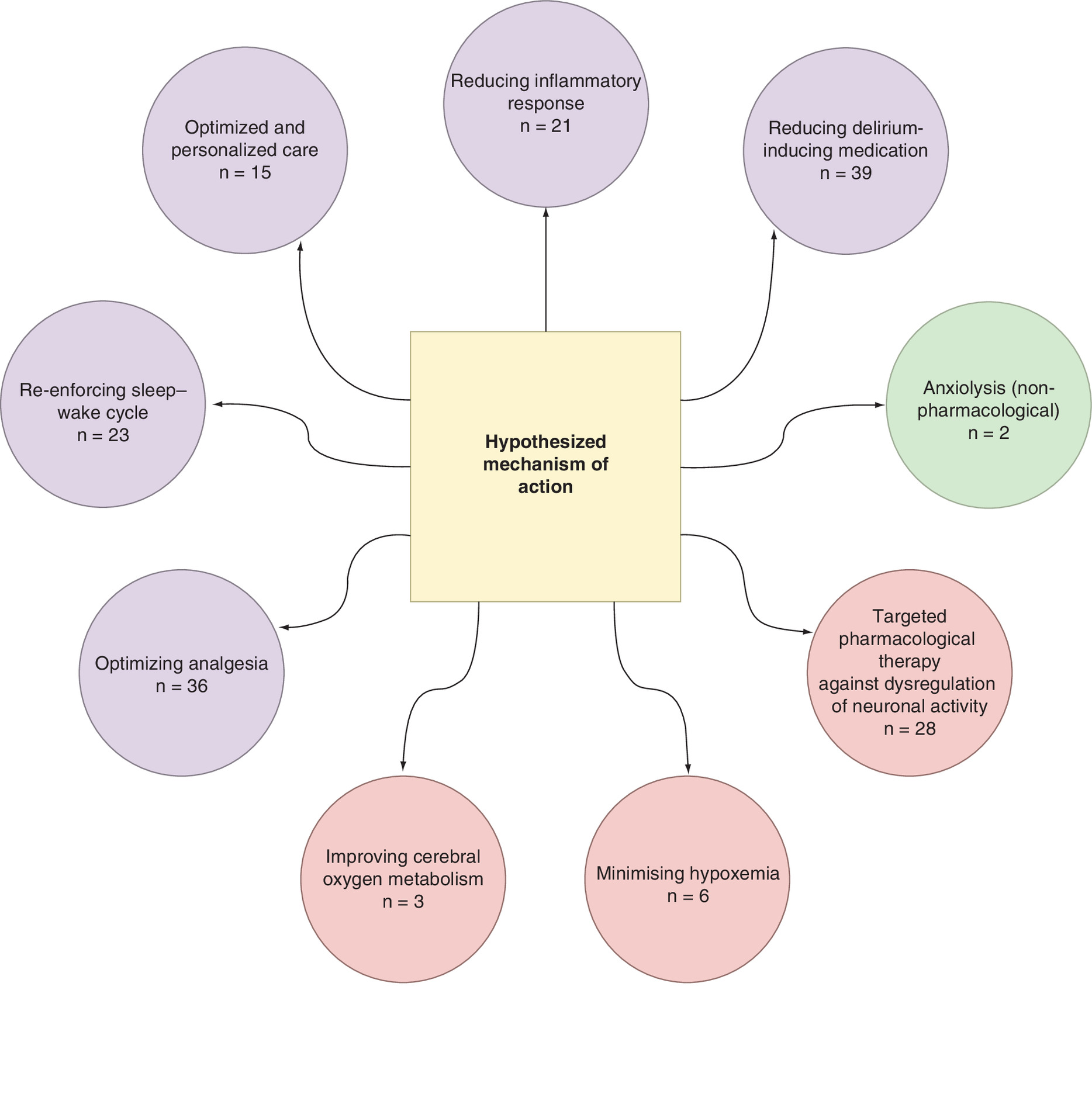
Figure 2. Summary of hypothesized mechanisms of action proposed in the 115 studies extracted.
Green color represents interventions that were solely nonpharmacological. Red color represents interventions that were solely pharmacological. Purple color represents both pharmacological and nonpharmacological interventions. Some interventions have multiple proposed hypothesized mechanisms of action and so are recorded in more than one circle.
n = number of studies, not the number of different interventions.
Mapping interventions to mechanisms
The most frequently investigated intervention was dexmedetomidine (n = 15 studies, 17.9% of total studies included), either alone or in combination with other drugs (ketamine). Dexmedetomidine intervention was tested intra- (n = 6), post- (n = 5) and perioperatively (n = 4). Dexmedetomidine also had the highest number of different proposed mechanisms of action, being included in seven of the nine proposed groups. Researchers hypothesized that dexmedetomidine potentially reduces incidence of POD by: reducing delirium-inducing medication; optimizing analgesia; acting as targeted pharmacological therapy against dysregulation of neuronal activity; re-enforcing sleep–wake cycle; reducing inflammatory response; minimizing hypoxemia; and, improving cerebral oxygen metabolism.
Regional (epidural) anesthesia intervention was associated with four out of the total nine different broad mechanisms of action. The five studies investigating this intervention theorized it had effect by reducing delirium-inducing medication (principally opioids); acting as targeted pharmacological therapy against dysregulation of neuronal activity; minimizing hypoxemia; and improving cerebral oxygen metabolism.
The intervention with the third highest accumulation of attributed mechanisms of action was postoperative bright light therapy, conducted in three separate studies. This was associated with three out of the total nine proposed mechanisms: re-enforcing sleep–wake cycle; reducing inflammatory response; and anxiolysis (nonpharmacological).
Meta-analysis
Studies identified in the identification of mechanism of action underwent secondary screening prior to inclusion in the MA.
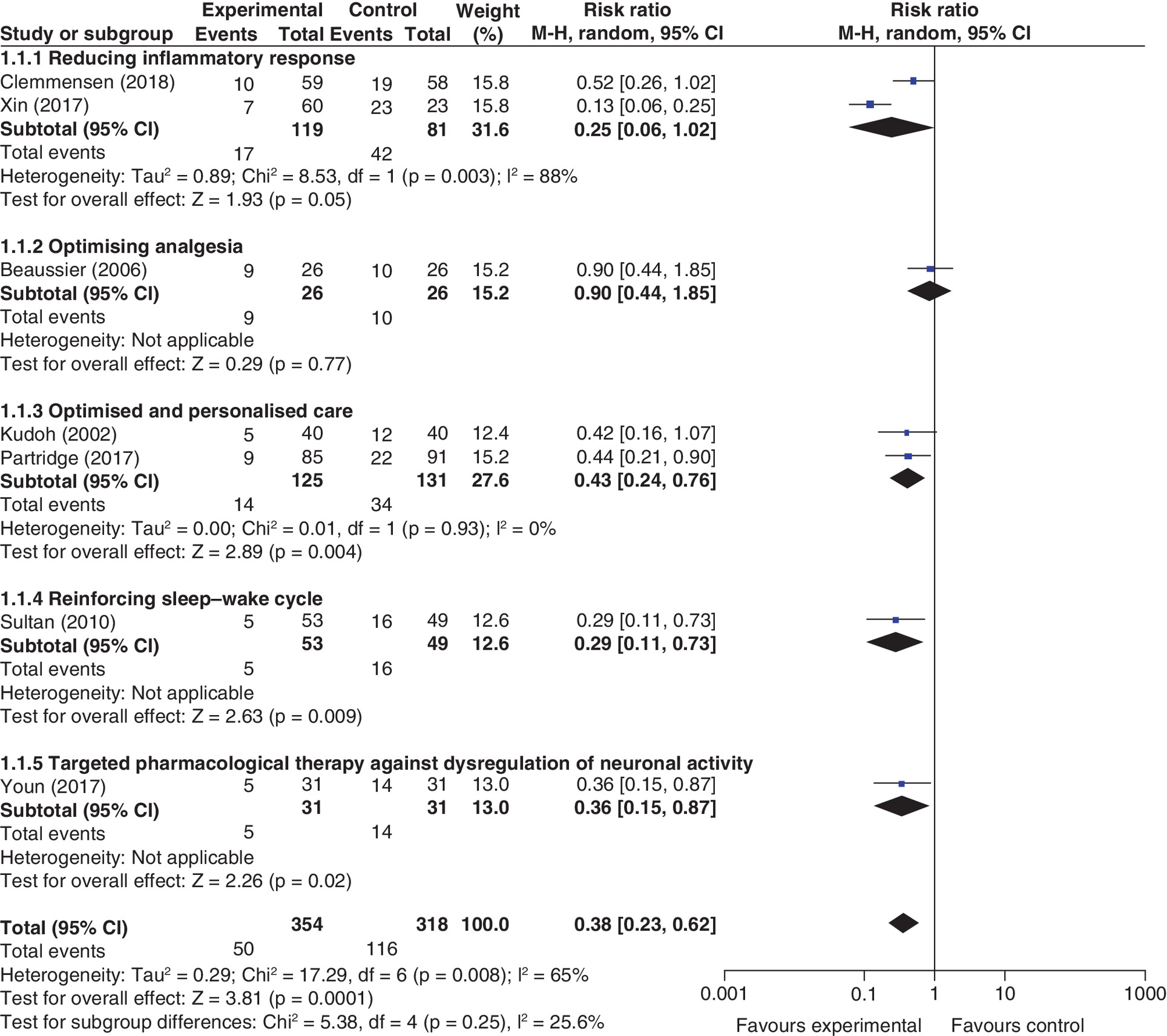
Preoperative
Seven studies were included in the preoperative MA (Figure 3). The pooled effect of preoperative interventions showed a benefit in POD reduction (RR: 0.38 [0.23–0.62], I2 = 71%). MA of preoperative interventions was limited as only two of the five subgroups had more than one study. Reduction of inflammatory response did not reduce POD (RR: 0.25 [0.26–1.02], I2 = 88%). Optimized and personalized care reduced POD (RR: 0.43 [0.24–0.76], I2 = 0%).
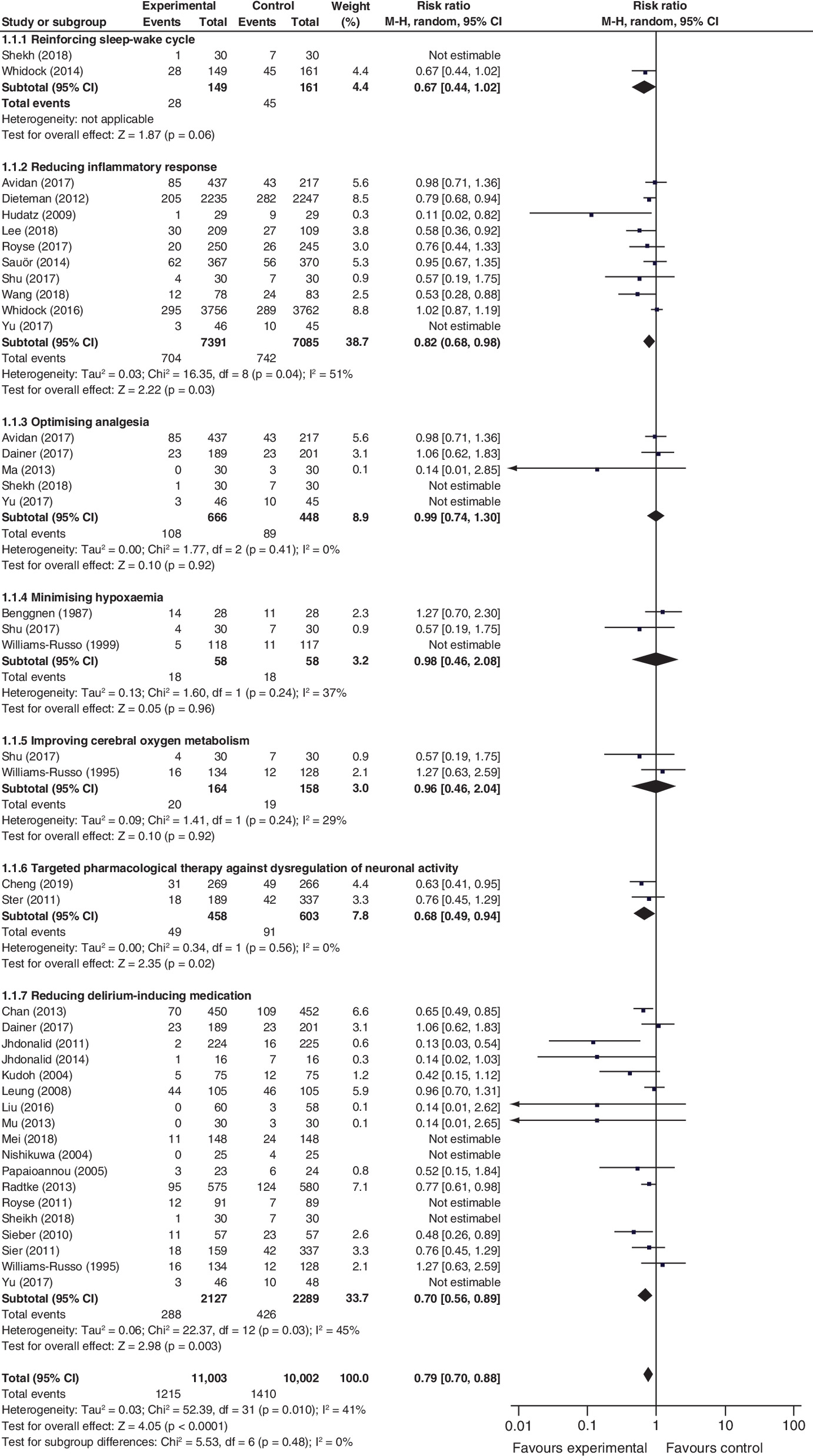
Intraoperative
Twenty-five studies were included in the intraoperative MA (Figure 4). The pooled effect of intraoperative interventions showed a benefit in POD reduction (RR: 0.79 [0.70–0.88]; I2 = 41%). Six of the seven subgroups in the intraoperative setting had more than one study for comparison. Reducing inflammatory response led to lower rates of POD (RR: 0.82 [0.68–0.98]; I2 = 51%). Optimizing analgesia did not reduce POD (RR: 0.99 [0.74–1.30], I2 = 0%), neither did minimization of hypoxemia (RR: 0.98 [0.46–2.08], I2 = 37%), nor strategies to improve cerebral oxygen metabolism (RR: 0.96 [0.46–2.04]; I2 = 29%). Targeted pharmacological therapy against dysregulation of neuronal activity (RR: 0.68 [0.68–0.94], I2 = 0%), and reducing delirium inducing medication did reduce POD (RR: 0.70 [0.56–0.89]; I2 = 45%).
Postoperative
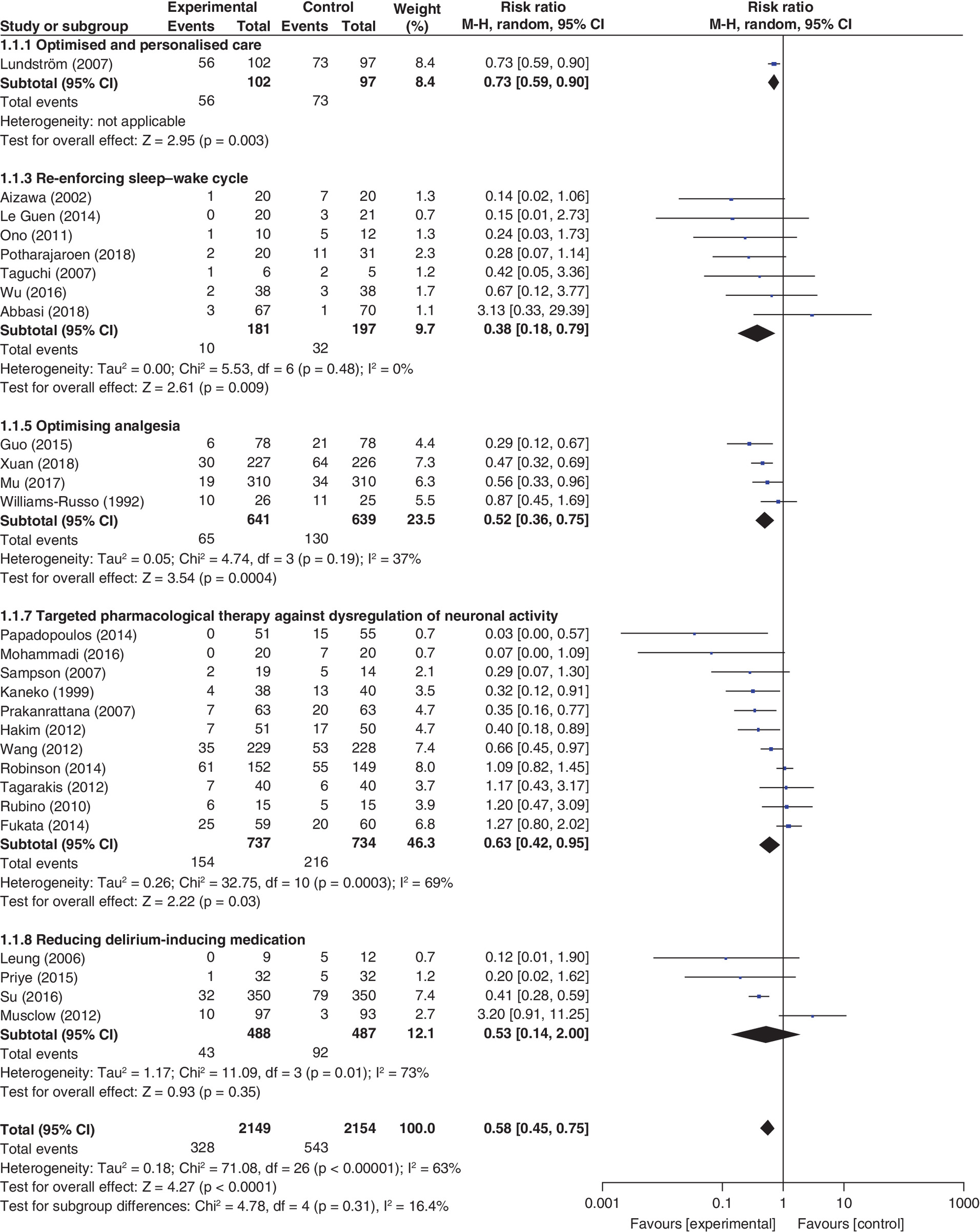
Twenty-seven studies were included in the postoperative intervention MA (Figure 5). The pooled effect of postoperative interventions showed a benefit in POD reduction (RR: 0.56 [0.44–0.72], I2 = 63%). Of the six mechanistic subgroups, four had more than one study. Strategies to reinforce sleep–wake cycle were associated with a RR of 0.38 (0.18–0.79). Heterogeneity was low (I2 = 0%). Optimizing analgesia was associated with a RR of 0.52 (0.36–0.75, I2 = 37%). Pharmacological interventions against the dysregulation of neuronal activity reduced POD with a RR of 0.63 (0.42–0.95), with high levels of heterogeneity (I2 = 69%). Reduction of delirium-inducing medication did not lead to reduced POD in this setting (RR: 0.53 [0.14–2.00], I2 = 73%).
Perioperative
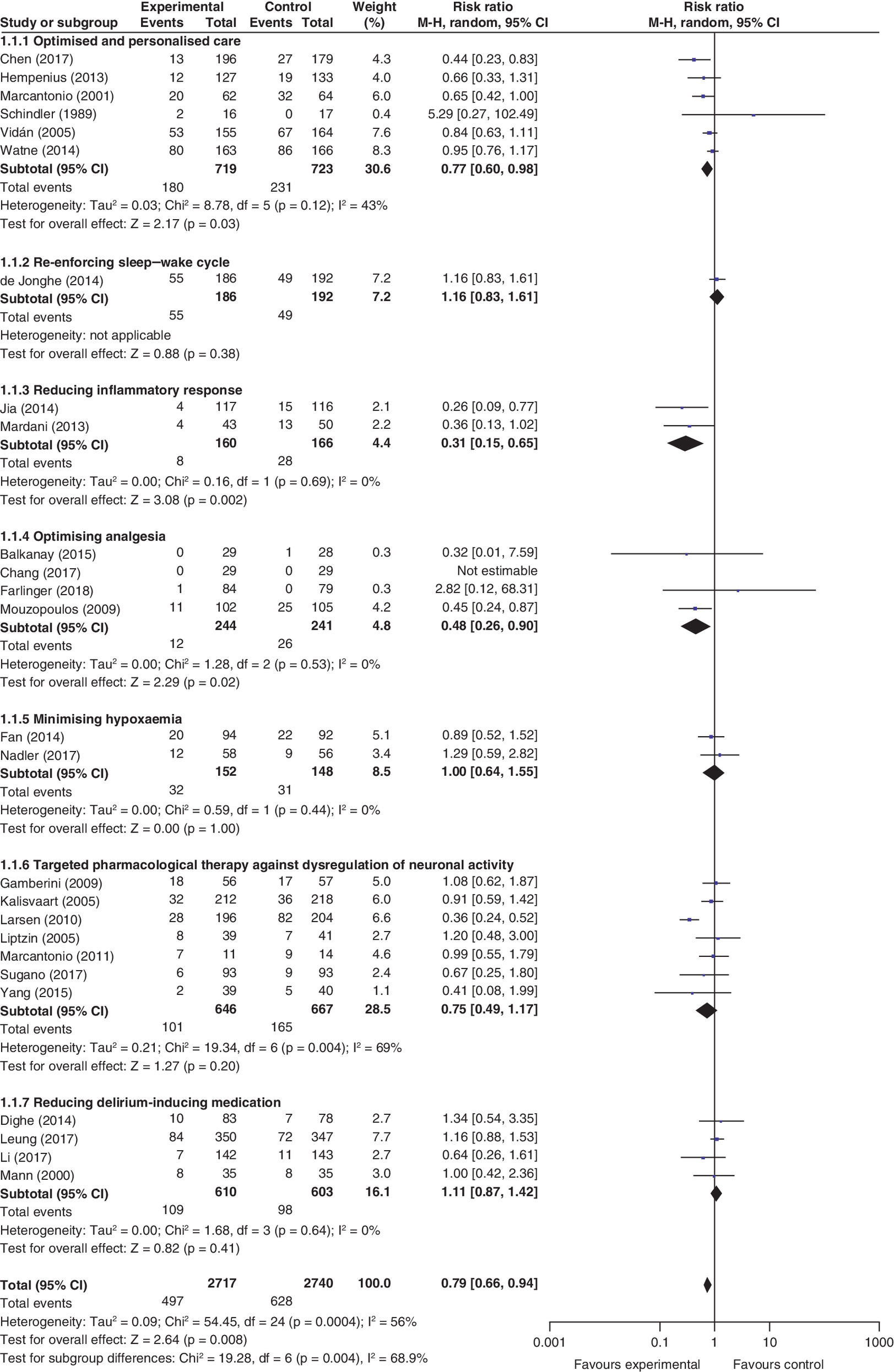
Twenty-six studies were included in the perioperative intervention MA (Figure 6). The pooled effect of perioperative interventions showed a benefit in POD reduction (RR: 0.79 [0.66–0.94]; I2 = 56%). Six mechanistic subgroups contained more than one study. Optimized and personalized care reduced POD (RR: 0.77 [0.60–0.98], I2 = 43%). Reduction of inflammatory response led to reduced POD (RR: 0.31 [0.15–0.65], I2 = 0%), as did optimizing analgesia (RR: 0.48 [0.26–0.90], I2 = 0%). Neither reduction of delirium-inducing medication (RR: 1.11 [0.87–1.42], I2 = 69%), nor minimizing of hypoxemia showed a benefit (RR: 1.00 [0.64–1.55], I2 = 0%).
Consistency of re-analysis by hMOA
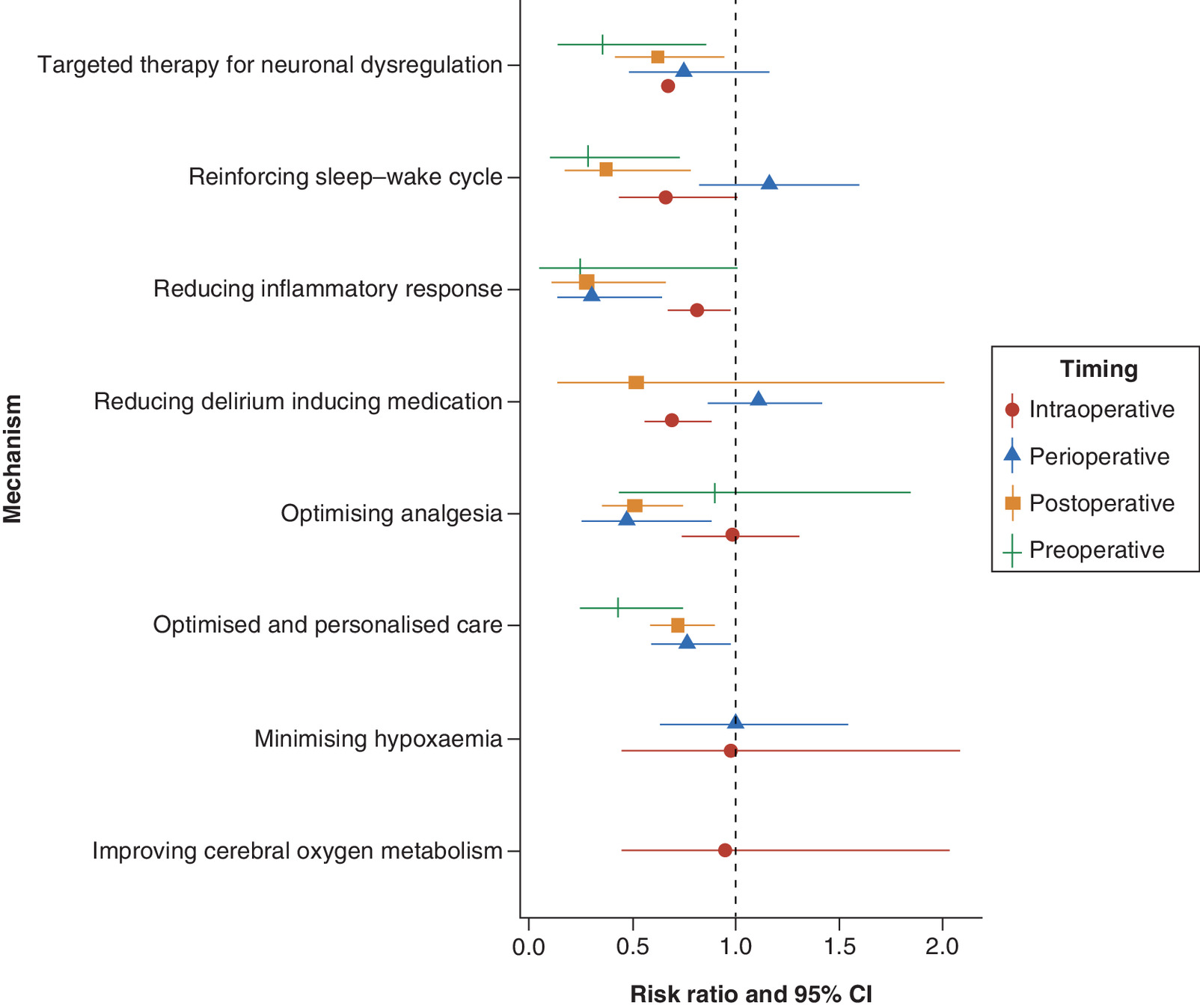
Inspection of plots according to mechanism of action and timing of intervention demonstrated relative consistency in the estimated RR for targeted therapy for neuronal dysregulation and reducing inflammatory response. It showed a split in optimization of analgesia, with post and perioperative interventions having a greater effect than preoperative interventions. Two out of three ‘personalized and optimized care’ interventions overlapped and there was consistency between the closely related mechanisms of avoiding hypoxemia and improving cerebral oxygen metabolism (Figure 7).
Inspection of the related I2 plots showed varying results (Supplementary Material 7). Heterogeneity was low in comparisons where inflammatory response was attenuated in the post- and perioperative settings. It was high in other settings. Low heterogeneity was seen for minimization of hypoxemia in the perioperative setting, optimized and personalized care in the preoperative setting, optimizing analgesia in the peri- and intraoperative settings, reducing of delirium-inducing medications in the perioperative settings and reinforcing the sleep–wake cycle in the postoperative setting.
Discussion
This review identified 47 interventions for prevention or treatment of POD that we have categorized into nine broad hMOAs. Several interventions were hypothesized to exert their effect through more than one mechanism, reflecting a varied understanding of the multifactorial etiology of POD [3,4].
MA by mechanistic subgroups indicated that some mechanisms of action (minimizing hypoxia/increasing cerebral oxygenation) did not confer statistically significant treatment effects at any time point in the patient pathway. Some mechanisms provided point estimates of effect which were relatively consistent across timing of intervention. For example, studies in the intra- or postoperative phase, which reduced delirium-inducing medication, had point estimates of 0.66 and 0.53 respectively. Others (e.g., optimizing analgesia) were associated with statistically significant reductions in POD at some, but not all, time points. In some cases, the findings from perioperative mechanistic subgroups were at odds with those seen for individual time periods in other forest plots. This may reflect increasing complexity of interventions, constraining our ability to achieve precision [29]. Furthermore, the effects of some interventions may be time dependent. Therefore, assessment of interventions through the entire perioperative period conceivably introduces heterogeneity in effect and loss of signal.
This review takes a high-level mechanism-based approach to provide a broad overview of this rapidly expanding, complex field. However, the use of textual data in quantitative studies to identify hMOA [30] and of systematic review methods to summarize them [31], are not novel. Our classification system is an intuitive partitioning of mechanistic claims from trial reports, informed by the intended end users of this review; surgeons, anesthetists and pharmacists. The proposed groupings seem to match broad mechanistic headings seen in other parts of the literature [32,33]. The low levels of statistical heterogeneity in most subgroup analyses suggest that categories were at an appropriate level of granularity to inform the design of future POD multimodal intervention studies.
Between-trial variation – high I2 values – observed in some subgroups may indicate that narrower categories – at the level of individual interventions – are warranted in future research on those areas. Furthermore, problematic application of animal models [34], poor quality preclinical studies [35], within-person variation in treatment effects [36] and inconsistencies between the reported contraindications of identical medications [37] all indicate the fragility of many assumed mechanisms of action.
This review has many strengths. Sensitive and comprehensive searches were carried out on two different databases, augmented by screening citations of included studies. The review included non-English language papers, adopted a broad definition of POD, considered all surgery types at all time points, maximizing the generalizability of the work. hMOA were reviewed by a multidisciplinary team. The truncation of the initial review on 21 October 2019, meant one potentially eligible systematic review containing six RCTs was omitted. Six other RCTs were omitted due to the unavailability of the full text or English translations. We addressed this by extracting data from accessible English-language abstracts and the hMOA from those studies have been covered elsewhere. Potential heterogeneity might arise from the nature of underlying surgery, the range of years included in the review and the definition of POD used in constituent studies.
Broad, complex areas of study require triangulation of multiple lines of evidence. For areas such as targeted pharmacological therapy against dysregulation of neuronal activity or reducing inflammatory response, greater granularity may be required for practitioners to have confidence in the evidence. Nevertheless, there is a sound basis for inclusion of these therapies in future studies of multimodal interventions in the prevention and treatment of POD.
The assessment of the effectiveness and cost–effectiveness of multimodal strategies for the prevention and treatment of POD remains a research priority [5]. As more major surgical procedures are performed in a population of advancing age are performed, the relevance of determining and targeting mechanisms of POD becomes ever more pressing. To reach the point where stratified care trials are possible, a better understanding of the key prognostic factors is required [38]. This data might support an adaptive trial design where treatment allocation is based upon hMOA, rather than a specific agent. This might allow the identification of a clear front running mechanism in the trial, and allow expansion of this arm to compare the relative effect of individual agents within this grouping. In the meantime, this review suggests that interventions targeting neuronal dysregulation, reinforcing sleep–wake cycle and limiting the inflammatory response, along with tailored reviews of multimorbid patients, might prevent or reduce the rate of POD.
Conclusion
Research into the treatment and prevention of POD targets nine broad mechanisms of action, reflecting the multifactorial etiology of POD. This evidence map provides a basis for future investigations into the prevention and treatment of POD.
•
Postoperative delirium is a major problem for both clinicians and patients. It is associated with significant morbidity and mortality following surgery.
•
There is currently no front running intervention to prevent this.
•
This paper re-analyses randomized trials included in previously published systematic reviews.
•
The re-analysis groups treatments by their proposed mechanism of action, rather than the specific drug or intervention. We also compared effectiveness across timing of intervention delivery, as this might impact its effect.
•
We identified nine hypothesized mechanisms of action in 85 randomized trials.
•
Postoperative reduction of inflammation and preoperative reinforcement of sleep–wake cycle appear to be effective strategies.
•
This approach suggests that grouping interventions by hypothesized mechanism of action might be a useful approach to identify the best interventions for this group. Future studies might first identify front running mechanism groups, and then identify the most effective agent within each category.
Author contributions
Study concept: MJ Lee, RS Bourne, IJ McCullagh, MJ Wilson, D Hind. Study design: E Boxell, Y Malik, J Wong, MH Lee, HM Berntsson, MJ Lee, RS Bourne, IM, MJ Wilson, D Hind. Data collection and analysis: E Boxell, Y Malik, J Wong, MH Lee, HM Berntsson, MJ Lee, RS Bourne, IJ McCullagh, MJ Wilson, D Hind. Manuscript preparation and critical review: E Boxell, Y Malik, J Wong, MH Lee, HM Berntsson, MJ Lee, RS Bourne, IJ McCullagh, MJ Wilson, D Hind.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Data sharing statement
No primary data is held for this study; all data extracted can be retrieved from published studies. Data tables will not be shared.
Open access
This work is licensed under the Creative Commons Attribution 4.0 License. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 366.18 KB
References
1.
Janssen TL, Alberts AR, Hooft L, Mattace-Raso F, Mosk CA, van der Laan L. Prevention of postoperative delirium in elderly patients planned for elective surgery: systematic review and meta-analysis. Clin. Interv. Aging 14, 1095–1117 (2019).
2.
Moskowitz EE, Overbey DM, Jones TS et al. Post-operative delirium is associated with increased 5-year mortality. Am. J. Surg. 214(6), 1036–1038 (2017).
3.
Orena EF, King AB, Hughes CG. The role of anesthesia in the prevention of postoperative delirium: a systematic review. Minerva Anestesiol. 82(6), 669–683 (2016).
4.
Leigh V, Stern C, Elliott R, Tufanaru C. Effectiveness and harms of pharmacological interventions for the treatment of delirium in adults in intensive care units after cardiac surgery: a systematic review. JBI Database Syst. Rev. Implement. Rep. 17(10), 2020–2074 (2019).
5.
Hughes CG, Boncyk CS, Culley DJ et al. American society for enhanced recovery and perioperative quality initiative joint consensus statement on postoperative delirium prevention. Anesth. Analg. 130(6), 1572–1590 (2020).
6.
Girard TD, Thompson JL, Pandharipande PP et al. Clinical phenotypes of delirium during critical illness and severity of subsequent long-term cognitive impairment: a prospective cohort study. Lancet Respir. Med. 6(3), 213–222 (2018).
7.
Parkkinen V-P, Wallmann C, Wilde M et al. Chapter 3: How to Consider Evidence of Mechanisms: An Overview. In: Evaluating Evidence of Mechanisms in Medicine. Springer International Publishing, Cham, Switzerland (2018).
8.
Bolland M, Grey A, Avenell A, Gamble G, Reid I. Calcium supplements with or without vitamin D and risk of cardiovascular events: reanalysis of the women's health initiative limited access dataset and meta-analysis. BMJ 342, d2040 (2011).
9.
Schlosser RW, Wendt O, Bhavnani S, Nail-Chiwetalu B. Use of information-seeking strategies for developing systematic reviews and engaging in evidence-based practice: the application of traditional and comprehensive pearl growing. A review. Int. J. Lang. Commun. Disord. 41(5), 567–582 (2006).
10.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control. Clin. Trials 7(3), 177–188 (1986).
11.
Duan X, Coburn M, Rossaint R, Sanders RD, Waesberghe JV, Kowark A. Efficacy of perioperative dexmedetomidine on postoperative delirium: systematic review and meta-analysis with trial sequential analysis of randomised controlled trials. Br. J. Anaesth. 121(2), 384–397 (2018).
12.
Fok MC, Sepehry AA, Frisch L et al. Do antipsychotics prevent postoperative delirium? A systematic review and meta-analysis. Int. J. Geriatr. Psychiatry 30(4), 333–344 (2015).
13.
Gilmore ML, Wolfe DJ. Antipsychotic prophylaxis in surgical patients modestly decreases delirium incidence--but not duration--in high-incidence samples: a meta-analysis. Gen. Hosp. Psychiatry 35(4), 370–375 (2013).
14.
Haque N, Naqvi RM, Dasgupta M. Efficacy of ondansetron in the prevention or treatment of post-operative delirium-a systematic review. Can. Geriatr. J. 22(1), 1–6 (2019).
15.
Igwe EO, Nealon J, Mohammed M et al. Multi-disciplinary and pharmacological interventions to reduce post-operative delirium in elderly patients: a systematic review and meta-analysis. J. Clin. Anesth. 67, 110004 (2020).
16.
Liu Y, Li X-J, Liang Y, Kang Y. Pharmacological prevention of postoperative delirium: a systematic review and meta-analysis of randomized controlled trials. Evid. Based Complement. Alternat. Med. 2019, 9607129 (2019).
17.
Lu Y, Li Y-W, Wang L et al. Promoting sleep and circadian health may prevent postoperative delirium: a systematic review and meta-analysis of randomized clinical trials. Sleep Med. Rev. 48, 101207 (2019).
18.
Luo C, Zou W. Cerebral monitoring of anaesthesia on reducing cognitive dysfunction and postoperative delirium: a systematic review. J. Int. Med. Res. 46(10), 4100–4110 (2018).
19.
León-Salas B, Trujillo-Martín MM, Del Castillo LPM et al. Pharmacologic interventions for prevention of delirium in hospitalized older people: a meta-analysis. Arch. Gerontol. Geriatr. 90, 104171 (2020).
20.
Moyce Z, Rodseth RN, Biccard BM. The efficacy of peri-operative interventions to decrease postoperative delirium in non-cardiac surgery: a systematic review and meta-analysis. Anaesthesia 69(3), 259–269 (2014).
21.
Mu JL, Lee A, Joynt GM. Pharmacologic agents for the prevention and treatment of delirium in patients undergoing cardiac surgery: systematic review and metaanalysis. Crit. Care Med. 43(1), 194–204 (2015).
22.
Pan H, Liu C, Ma X, Xu Y, Zhang M, Wang Y. Perioperative dexmedetomidine reduces delirium in elderly patients after non-cardiac surgery: a systematic review and meta-analysis of randomized-controlled trials. Can J Anaesth. 66(12), 1489–1500 (2019).
23.
Shields L, Henderson V, Caslake R. Comprehensive geriatric assessment for prevention of delirium after hip fracture: a systematic review of randomized controlled trials. J. Am. Geriatr. Soc. 65(7), 1559–1565 (2017).
24.
Tao R, Wang X-W, Pang L-J et al. Pharmacologic prevention of postoperative delirium after on-pump cardiac surgery: a meta-analysis of randomized trials. Medicine (Baltimore). 97(43), e12771 (2018).
25.
Teslyar P, Stock VM, Wilk CM, Camsari U, Ehrenreich MJ, Himelhoch S. Prophylaxis with antipsychotic medication reduces the risk of post-operative delirium in elderly patients: a meta-analysis. Psychosomatics 54(2), 124–131 (2013).
26.
Wu M, Liang Y, Dai Z, Wang S. Perioperative dexmedetomidine reduces delirium after cardiac surgery: a meta-analysis of randomized controlled trials. J. Clin. Anesth. 50, 33–42 (2018).
27.
Zeng H, Li Z, He J, Fu W. Dexmedetomidine for the prevention of postoperative delirium in elderly patients undergoing noncardiac surgery: a meta-analysis of randomized controlled trials. PLoS ONE 14(8), e0218088 (2019).
28.
Wang L, Zhang H, Xu F-Y et al. Strategies for prevention of postoperative delirium: a systematic review and meta-analysis of randomized trials. Crit. Care 17(2), R47 (2013).
29.
Aron DC. Precision medicine in an imprecise and complex world: magic bullets, hype, and the fuzzy line between health and disease. J. Eval. Clin. Pract. 26(5), 1534–1538 (2019).
30.
Drey N, Gould D, Purssell E et al. Applying thematic synthesis to interpretation and commentary in epidemiological studies: identifying what contributes to successful interventions to promote hand hygiene in patient care. BMJ Qual. Saf. 29(9), 756–763 (2020).
31.
Georgiou M, Papathanassoglou E, Xanthos T. Systematic review of the mechanisms driving effective blood flow during adult CPR. Resuscitation 85(11), 1586–1593 (2014).
32.
Van Den Boogaard M, Slooter AJC. Delirium in critically ill patients: current knowledge and future perspectives. BJA Educ. 19(12), 398–404 (2019).
33.
Jin Z, Hu J, Ma D. Postoperative delirium: perioperative assessment, risk reduction, and management. Br. J. Anaesth. 125(4), 492–504 (2020).
34.
Jansen K, Pou Casellas C, Groenink L, Wever KE, Masereeuw R. Humans are animals, but are animals human enough? A systematic review and meta-analysis on interspecies differences in renal drug clearance. Drug Discov. Today 25(4), 706–717 (2020).
35.
Kilkenny C, Browne WJ, Cuthill IC, Emerson M, Altman DG. Improving bioscience research reporting: the ARRIVE guidelines for reporting animal research. PLoS Biol. 8(6), e1000412 (2010).
36.
Senn S. Statistical pitfalls of personalized medicine. Nature 563(7733), 619–621 (2018).
37.
Gahr M, Freudenmann RW, Connemann BJ et al. Unterschiedliche Anzahl von Kontraindikationen zwischen Fachinformationen wirkstoffgleicher Arzneimittel – eine Analyse von Daten aus Fachinformationen von neuropsychiatrischen Arzneimitteln. Fortschr. Neurol. Psychiatr. 88(03), 152–169 (2020).
38.
Hemingway H, Croft P, Perel P et al. Prognosis research strategy (PROGRESS) 1: a framework for researching clinical outcomes. BMJ 346(e5595), 1–11 (2013).
Information & Authors
Information
Published In
Pages: 1301 - 1315
PubMed: 34585622
Copyright
© 2021 The Authors. This work is licensed under the Creative Commons Attribution 4.0 License
History
Received: 2 July 2021
Accepted: 23 August 2021
Published online: 29 September 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Are treatment effects consistent with hypothesized mechanisms of action proposed for postoperative delirium interventions? Reanalysis of systematic reviews. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0161
Export citation
Select the citation format you wish to export for this article or chapter.