Comparison of intravenous versus topical tranexamic acid in primary total hip arthroplasty: a systematic review and meta-analysis of ten randomized trials
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The optimal management approach for tranexamic acid (TXA) in primary total hip arthroplasty (THA) is still controversial. This meta-analysis aimed to evaluate the efficacy and safety of intravenous versus topical TXA during THA. Materials & methods: PubMed, Google Scholar, Embase and the Cochrane library were searched for all randomized controlled trials comparing topical and intravenous TXA (iTXA) following primary THA. The primary outcome consisted of blood loss including total blood loss, intraoperative blood loss and hidden blood loss (HBL), hemoglobin (Hb) level of postoperative day 1, maximum Hb drop and transfusion incidence. The second outcome included drainage volume, complications and length of stay. Extracted data were statistically analyzed with the Stata11.0. Results: A total of ten randomized controlled trials containing 1295 patients were included in the study. A similar effect of transfusion rate, total blood loss, Hb level of postoperative day 1, drainage volume, deep vein thrombosis events and wound complications appeared in the two routes. Intraoperative blood loss (weighted mean difference [WMD] = -12.687, 95% CI: -22.291, -3.083; p = 0.010), HBL (WMD = 14.276, 95% CI: 9.936, 19.459; p < 0.001) and maximum Hb drop (WMD = -0.400, 95% CI: -0.577, -0.222; p < 0.001) were significantly reduced in the intravenous group compared with topical group. Conclusion: The present result indicated comparable safety and transfusion rate for intravenous and topical TXA in primary THA, while the intravenous approach demonstrated a smaller intraoperative blood loss, HBL and maximum Hb drop.
Total hip arthroplasty (THA) is currently recognized as the most successful surgical method to treat hip diseases such as end-stage inflammatory or degenerative arthritis, displaced fractured neck of the femur and end-stage avascular necrosis [1,2]. It was reported more than 1 million THAs were performed every year all over the world and the number in the USA alone was more than 500,000, while the number was steadily increasing with the aging of the population [3,4]. But perioperative blood loss and consequent anemia are common and serious complications for joint replacement surgery which increase systemic risks especially for elderly cases [5]. Although both autologous and allogeneic blood transfusion can rapidly and effectively supplement lost blood, the former only provides limited blood volumes and the re-infusion volumes of blood decrease with increasing age, while the latter might induce the risk of side effects such as surgical-site infections, virus infection, anaphylactic reactions and even increased mortality [6–8]. To decrease blood transfusion requirements, tranexamic acid (TXA) has been widely adopted in major orthopedic surgery with amazing efficacy and safety identified by various researches [7,9–11]. As an antifibrinolytic drug, TXA with intravenous injection exists a high risk of thrombotic events, such as deep vein thrombosis (DVT) and pulmonary embolism in theory and this has led to the emergence of other ‘safer’ routes of TXA administration including topical, oral and combined TXA, all of which demonstrated no statistical difference in controlling bleeding and risk of thrombosis compared with each other based on recent studies [12,13]. During the above-described routes, the intravenous and topical administration of TXA has been most often compared for their representative roles of efficiency and safety respectively [14–17]. A previous meta-analysis in 2014 concluded intravenous injection showed similar transfusion requirements and safety compared with topical TXA (tTXA) in total joint arthroplasty, while it seemed to be associated with the smaller maximum drop in hemoglobin (Hb) [14]. However, recent randomized controlled trials (RCTs) in 2019 reported topical application had superior therapeutic values compared with the intravenous application of TXA using same dose in THA [18]. Thus, the optimal administration route of TXA in THA has remained controversial. To obtain a comprehensive understanding of these two approaches, we performed this meta-analysis of RCTs to compare the efficacy and safety of intravenous versus topical administration of TXA during THA.
Materials & methods
This systematic review and meta-analysis was designed according to the Preferred Reporting Items for Systemic Reviews and Meta-Analysis (PRISMA) guidelines [19,20].
Literature search
We searched all the related RCTs that comparing the approaches of TXA use in the treatment of THA through electronic databases including PubMed, Google Scholar, Embase, the Cochrane library with a full text in English. The retrieval was up until January 2021. The keyword including ‘tranexamic acid or TXA’, ‘intravenous topical (ivTXA) or intra-articular or local’ and ‘THA or total hip replacement’ with the Boolean operators was adopted as a search strategy. Furthermore, we manually screened the bibliography cited in the included studies for the potential eligible trials.
Inclusion & exclusion
The inclusion criterion was RCTs comparing intravenous with topical or local or intra-articular TXA for patients undergoing THA. The included studies should at least report the efficacy and safety of TXA between different administration routes for THA.
We excluded studies that were of low quality or not following inclusion criteria. To obtain comprehensive literature, follow-up time, patients’ age and presurgery status were not set as exclusion criteria.
Data extraction
All data were extracted by two separate reviewers, a third author was necessary when different opinions appeared. The following information from the included studies was extracted: the first author’s name, nationality, year of publication, sample number, mean age, gender, dose and route of TXA intervention, preoperative Hb, general surgical information and outcome parameters. Primary end points consist of blood loss including total blood loss (TBL), intraoperative blood loss (IBL), and hidden blood loss (HBL), Hb level including postoperative day 1 and maximum Hb drop and transfusion incidence. Second end points include drainage volume, complications (wound complications and DVT events) and length of stay (LOS).
Quality assessment
We conducted a quality assessment of RCTs by using the Cochrane Collaboration’s tool [21] and prepared a ‘risk of bias’ table including the following main factors to assess the risk of bias of each included publication: random sequence generation, allocation concealment, blinding, incomplete outcome data, selective reporting and other sources of bias. Three independent reviewers provided a score of high, unclear or low risk of bias for each bias domain. When there were different opinions, another leading author was involved until disagreements were resolved by consensus.
Statistical analysis
The extracted data were statistically analyzed with the Stata11.0 (T Stata Corp LP, TX, USA). When I2>50%, p < 0.1, the data were considered to be significant heterogeneity according to the Cochran’s Q statistic the I2 statistics and random-effect model was conducted for meta-analysis. Otherwise, a fixed-effect model was performed. The results of dichotomous outcomes (transfusion rate, wound complication and DVT events) were expressed as relative risk with 95% CIs. For continuous various outcomes including blood loss, Hb level, drainage volume and LOS, weighted mean differences (WMD) with 95% CIs were applied for assessment. p < 0.05 was defined as the threshold of a statistically significant difference.
Results
Search results
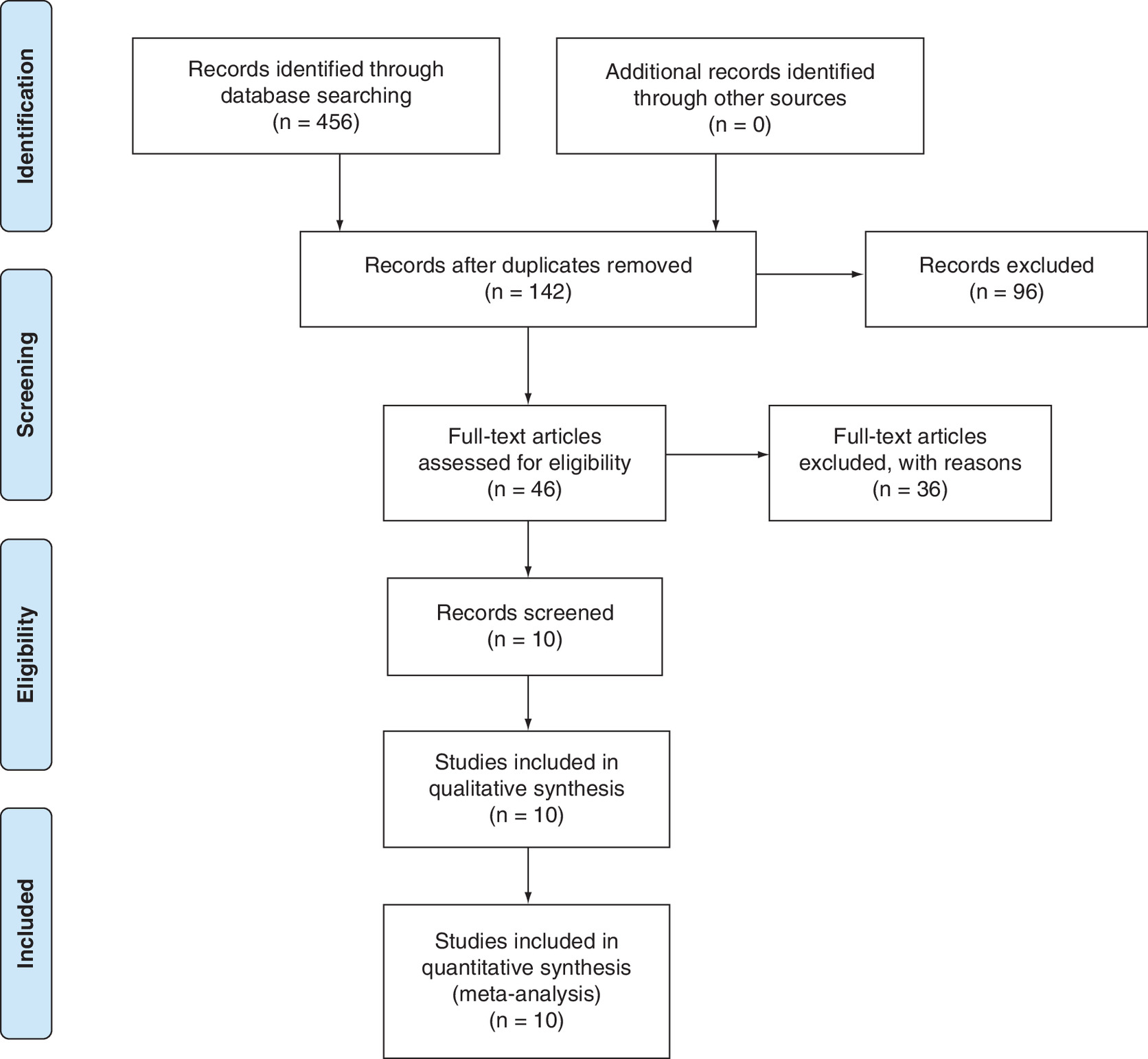
As shown in Figure 1, we preliminarily identified 456 pieces of literature in the four selected databases. First, 314 records were removed owing to duplication or irrelevant studies. Then, we scanned the title and abstract, 96 reports were excluded according to the eligibility criteria. The left 46 pieces of literature were read by the full text and 36 reports were removed for the lack of necessary data. Finally, ten RCTs were included for the data extraction and meta-analysis.
Study characteristics
Eleven RCTs published between 2014 and 2020 were included in this study, all of which compared the effect of intravenous versus topical administration of TXA in patients receiving THA. A total of 1295 patients were involved, during which 656 participated in the intravenous group and 639 in the topical group. Other demographic characteristics and details such as mean age, sex ratio, BMI were shown in Table 1. All the included trials provided details about the methods and doses of TXA, transfusion criteria and DVT events prophylaxis during THA. One RCT particularly recorded and analyzed the dynamic process of coagulation under the administration of TXA. Other surgical information was shown in Table 2.
| Study | Year | Country | Recruitment | Sample | Mean age (Y) | Gender (M/F) | BMI | Preoperative Hb (g/dl) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ivTXA | tTXA | ivTXA | tTXA | ivTXA | tTXA | ivTXA | tTXA | ivTXA | tTXA | ||||
| Zhou et al. | 2018 | China | 2014–2015 | 57 | 56 | 63.2 ± 10.0 | 65.8 ± 9.4 | 12/45 | 17/39 | 23.7 ± 3.2 | 23.2 ± 3.1 | 12.74 ± 1.4 | 12.96 ± 1.28 |
| Xu et al. | 2019 | China | 2016–2018 | 68 | 72 | 62.5 ± 6.6 | 61.9 ± 6.1 | 32/36 | 34/38 | 22.0 ± 2.3 | 22.3 ± 2.7 | – | – |
| Luo et al. | 2017 | China | 2016–2017 | 60 | 60 | 59.53 ± 11.50 | 62.24 ± 11.04 | 27/33 | 25/35 | 24.5 ± 3.87 | 25.27 ± 4.19 | 13.71 ± 0.75 | 14.07 ± 0.99 |
| Xie et al. | 2016 | China | 2014–2015 | 70 | 70 | 59.53 ± 11.50 | 62.24 ± 11.04 | 20/50 | 25/45 | 24.16 ± 3.08 | 24.47 ± 3.30 | 13.32 ± 1.26 | 13.22 ± 0.84 |
| Zhang et al. | 2020 | China | 2018–2019 | 36 | 36 | 66.98 ± 9.01 | 67.98 ± 8.87 | 15/21 | 16/20 | 23.4 ± 2.01 | 23.86 ± 2.38 | – | – |
| Wei et al. | 2014 | China | 2013–2014 | 101 | 102 | 63.6 ± 7.0 | 60.2 ± 6.5 | 39/62 | 35/67 | 24.2 ± 3.1 | 25.3 ± 3.0 | – | – |
| Vles et al. | 2020 | Belgium | 2014–2015 | 60 | 60 | 61.5 ± 11.8 | 64.0 ± 13.4 | 29/31 | 22/38 | 27.6 ± 4.4 | 26.3 ± 4.4 | 14.5 ± 1.23 | 13.9 ± 1.5 |
| Gómez-Aparicio et al. | 2020 | Spain | 2017–2019 | 110 | 85 | 63.94 ± 10.80 | 65.52 ± 10.92 | 48/62 | 45/40 | 28.43 ± 3.81 | 29.20 ± 5.26 | 14.21 ± 1.31 | 14.30 ± 2.21 |
| North et al. | 2015 | USA | 2013–2013 | 70 | 69 | 64.1 ± 12.0 | 65.7 ± 10.6 | 38/32 | 39/30 | 31.1 ± 5.4 | 31.1 ± 6.4 | 13.4 ± 1.3 | 13.2 ± 1.4 |
| Zhang et al. | 2016 | China | 2013–2014 | 25 | 25 | 44.5 ± 2.4 | 44.3 ± 3.7 | 14/11 | 13/12 | 24.3 ± 3.2 | 23.5 ± 3.4 | 126.5 ± 6.5 | 13.02 ± 0. 58 |
F: Female; Hb: Hemoglobin; ivTXA: Intravenous tranexamic acid; M: Male; TXA: Topical tranexamic acid.
| Study (year) | Surgical approach | Anesthesia | ivTXA | tTXA | Drainage | Transfusion criteria | VTE prophylaxis | Follow-up |
|---|---|---|---|---|---|---|---|---|
| Zhou et al. (2018) | Anterolateral approach | General anesthesia | First dose: 10 mg/kg 15 min before incision Second dose: 10 mg/kg 3 h after the first dose | 3.0 g/60 ml irrigated 3 min before closure | Clamped for 2 h Removed on the 48 h postoperative | Hb <80 g/l or <100 g/l with anemic complications | Rivaroxaban for 15 days | 6 weeks |
| Xu et al. (2019) | Posterolateral approach | Spinal anesthesia | Single dose: 20 mg/kg 5 min before incision | 2.0 g/50 ml irrigated before closure | Clamped for 2 h Removed on the 48 h postoperative | (Hb) level <70 g/l or >70 g/l with anemic complications | Rivaroxaban for 35 days | 6 months |
| Luo et al. (2017) | Posterolateral approach | General anesthesia | Single dose: 20 mg/kg 5 min before incision | 2.0 g/150 ml dilution 50 ml irrigated the acetabulum 50 ml irrigated the femoral 50 ml injected after closure | No drains | Hb <70 g/l or >70 g/l with anemic complications | LMWH until discharge Rivaroxaban for another 15 days | 3 months |
| Xie et al. (2016) | Posterolateral approach | General anesthesia | Single dose: 1.5 g 15 min before incision | 3.0 g/150 ml dilution 50 ml irrigated the acetabulum 50 ml irrigated the femoral 50 ml injected after closure | Clamped for 30 min Removed on the 24 h postoperative | Hb <70 g/l or >70 g/l with anemic complications | LMWH until discharge Rivaroxaban for another 30 days | 3 months |
| Zhang et al. (2020) | Posterolateral approach | General anesthesia | Single dose: 2.0 g/100 ml 30 min before incision | 2.0 g/100 ml injected after closure | Clamped for 2 h Removed on the 24 h postoperative | Hb <70 g/l or <70 g/l with anemic complications | LMWH until discharge Rivaroxaban for another 10 days | NA |
| Wei et al. (2014) | Posterolateral approach | NA | Single dose: 3.0 g 10 min before incision | 3.0 g/100 ml dilution 20 ml irrigated the acetabulum 20 ml irrigated the femoral 60 ml injected after closure | Clamped for 2 h Removed on the 24 h postoperative | Hb <90 g/l | LMWH | 3 months |
| Vles et al. (2020) | Direct anterior approach | Spinal anesthesia | Single dose: 1.5 g/100 ml before closure | 3.0 g/100 ml injected after closure | Clamped for 2 h | Hb <80 g/l or <85 g/l with anemic complications | LMWH until discharge Rivaroxaban for another 30 days | NA |
| Gómez-Aparicio et al. (2020) | NA | NA | Single dose: 15 mg/kg 15–20 min before incision | 2.0 g/100 ml injected after closure | Clamped for 2 h Removed on the 48 h postoperative | Hb <80 g/l or <100 g/l with anemic complications | LMWH for 30 days | NA |
| North et al. (2015) | NA | NA | First dose: 1.0 g/50 ml10 min before incision Second dose:1.0 g/50 ml before fascial closure | 2.0 g/100 ml irrigated before closure | No drains | Hb <70 g/l or <80 g/l with anemic complications | LMWH for 21 days or rivaroxaban for 35 days or aspirin for 21 days | NA |
| Zhang et al. (2016) | Anterior lateral approach | General or spinal anesthesia | Single dose: 1.0 g/250 ml 10 min before incision | 1.0 g/100 ml injected after closure | Clamped for 3 h Removed on the 45 h postoperative | Hb <70 g/l or >80 g/l with anemic complications | LMWH for 2 weeks | 1 year |
Hb: Hemoglobin; ivTXA: Intravenous tranexamic acid; LMWH: Low molecular weight heparin; NA: Not available; tTXA: Topical tranexamic acid.
Risk of bias
The risk of bias of the included study was evaluated separately by two reviewers. Random sequence generation was illustrated in six studies. Allocation concealment and blinding of participants and personnel were considered as with a low risk of bias in five studies. Six studies were revealed to have a low risk of bias on the blinding of outcome assessment. As shown in Table 3, all the ten RCTs did not make selective reports.
| Study (year) | Sequence generation | Allocation concealment | Blinding of outcome assessors | Incomplete outcome data | Selective outcome reporting | Others |
|---|---|---|---|---|---|---|
| Zhou et al. (2018) | Low | Low | Low | Low | Low | Low |
| Xu et al. (2019) | Low | Low | High | Low | Low | Unclear |
| Luo et al. (2017) | Low | Unclear | High | Low | Low | Low |
| Xie et al. (2016) | Unclear | Low | Low | Low | Low | Low |
| Zhang et al. (2020) | High | Unclear | High | Low | Low | Unclear |
| Wei et al. (2014) | Low | Low | Low | Low | Low | Low |
| Vles et al. (2020) | Low | Unclear | Low | Low | Low | Low |
| Gómez-Aparicio et al. (2020) | High | Unclear | Low | Low | Low | Unclear |
| North et al. (2015) | Unclear | Unclear | Low | Low | Low | Low |
| Zhang et al. (2016) | Low | Low | Unclear | Low | Low | Low |
ivTXA: Intravenous tranexamic acid; tTXA: Topical tranexamic acid.
Outcomes of the meta-analysis
The effects of intravenous versus topical administration of TXA during THA was assessed via the evaluation indicators including blood loss (TBL, IBL and HBL), Hb level (postoperative day 1 and maximum Hb drop), transfusion incidence, drainage volume, complications (wound complications and DVT events) and LOS.
Blood loss
For a full comparison of blood loss between intravenous versus topical administration of TXA, a subgroup analysis was conducted based on the type of blood loss (TBL, IBL and HBL). Seven RCTs including 1050 patients in total provided data on TBL, during which 536 cases were in the intravenous group and 514 in the topical group and the data from different studies did not reveal significant heterogeneity (p = 0.306; I2 = 16.2%). As shown in Figure 2, the effect of intravenous administration of TXA on TBL compared with the topical group during THA was not statistically significant (WMD = -40.665, 95% CI: -85.153, 3.823; p = 0.073). Four studies reported relevant data on IBL without statistical heterogeneity (I2 = 0.0; p = 0.763%,), and the comparison illustrated statistical significance in the two groups (WMD = -12.687, 95% CI: -22.291, -3.083; p = 0.010; Figure 3). The present meta-analysis demonstrated ivTXA with a lower intraoperative blood loss than tTXA during THA. We further analyzed HBL which was mentioned in three studies involving 216 cases in the intravenous group and 191 in the topical group. A random-effect model was used due to significant heterogeneity among the RCTs (I2 = 20.6%; p = 0.284) and the result was statistically significant differences on HBL between the two groups (WMD = 14.276, 95% CI: 9.936, 19.459; p < 0.001). The result demonstrated ivTXA with a lower HBL than tTXA.
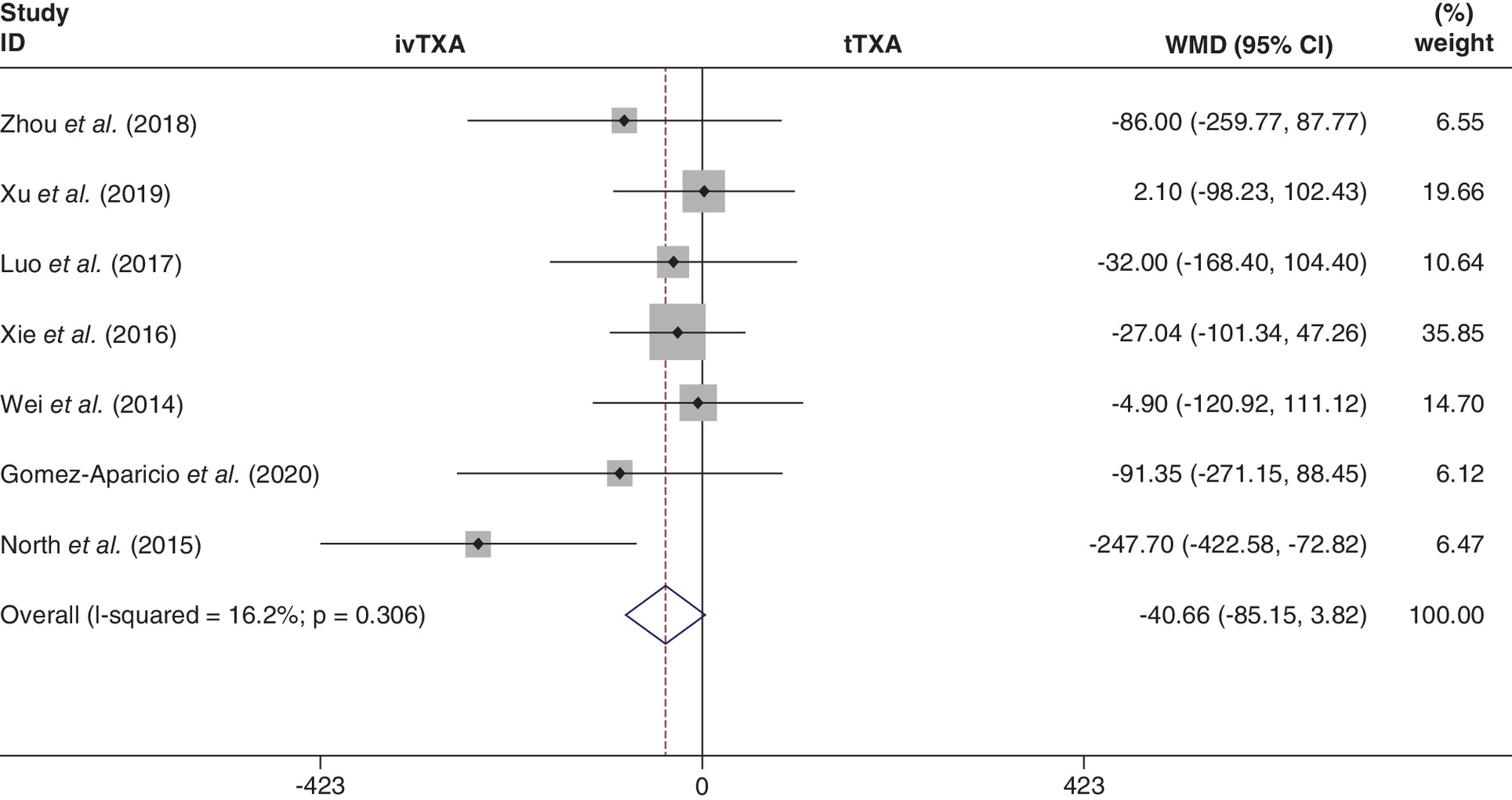
Figure 2. Forest plot diagram of the effect of intravenous versus tTXA on total blood loss.
ivTXA: Intravenous tranexamic acid; tTXA: Topical tranexamic acid; WMD: Weighted mean difference.
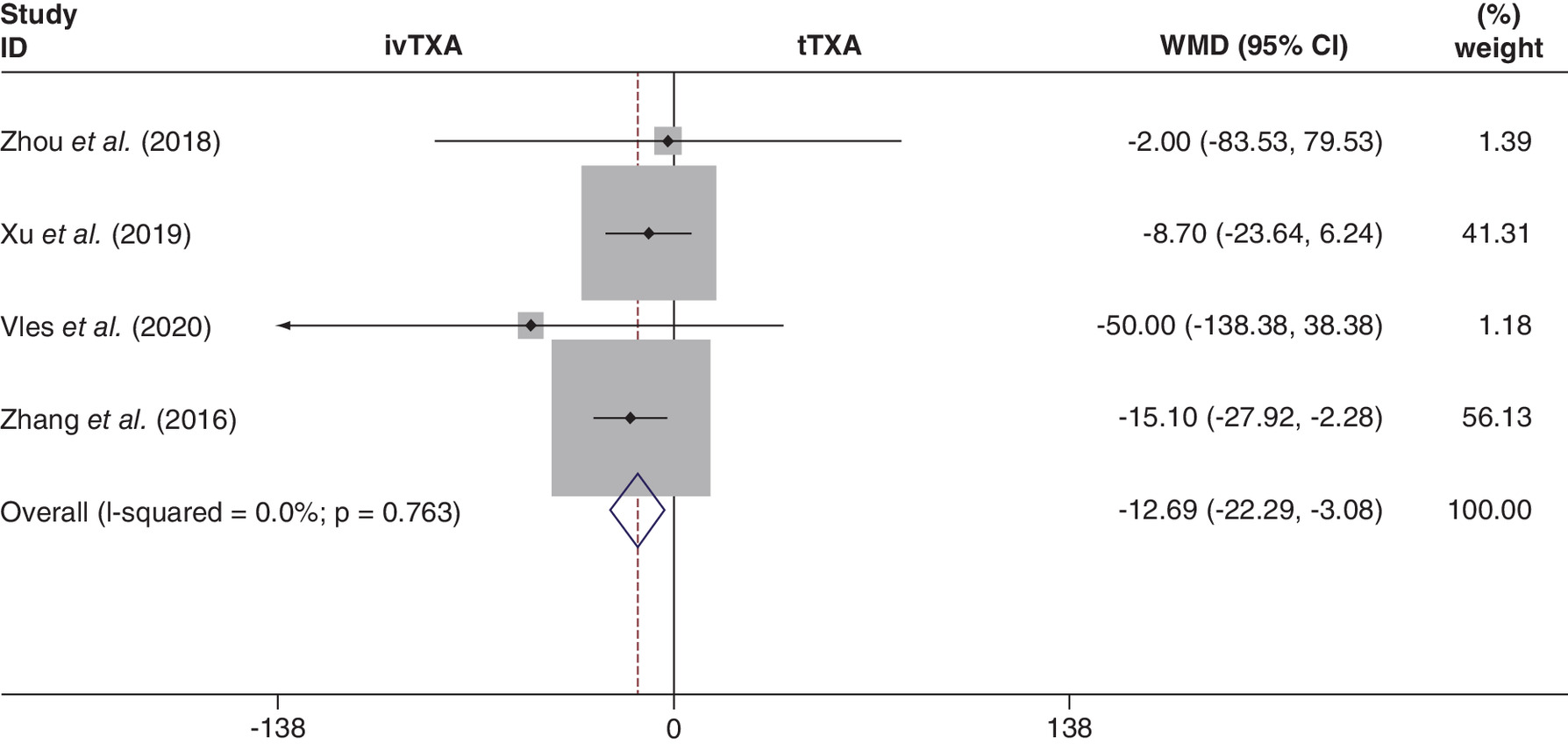
Figure 3. Forest plot diagram of the effect of intravenous versus tTXA on intraoperative blood loss.
ivTXA: Intravenous tranexamic acid; tTXA: Topical tranexamic acid; WMD: Weighted mean difference.
Hb level
Hb level was analyzed based on postoperative day 1 Hb (six studies) and maximum Hb drop (four studies). A random-effect model was adopted for these two indicators owing to the significant heterogeneity was illustrated among the studies (I2 >50%; p < 0.1). There was no significant difference on postoperative day 1 Hb (WMD = -1.803, 95% CI: -5.269, 1.663; p = 0.308) between the two groups based on the results of the pooled analysis while the results demonstrated that ivTXA was related to a significantly smaller maximum Hb drop during THA (WMD = -0.400, 95% CI: -0.577, -0.222; p < 0.001; Figure 4).
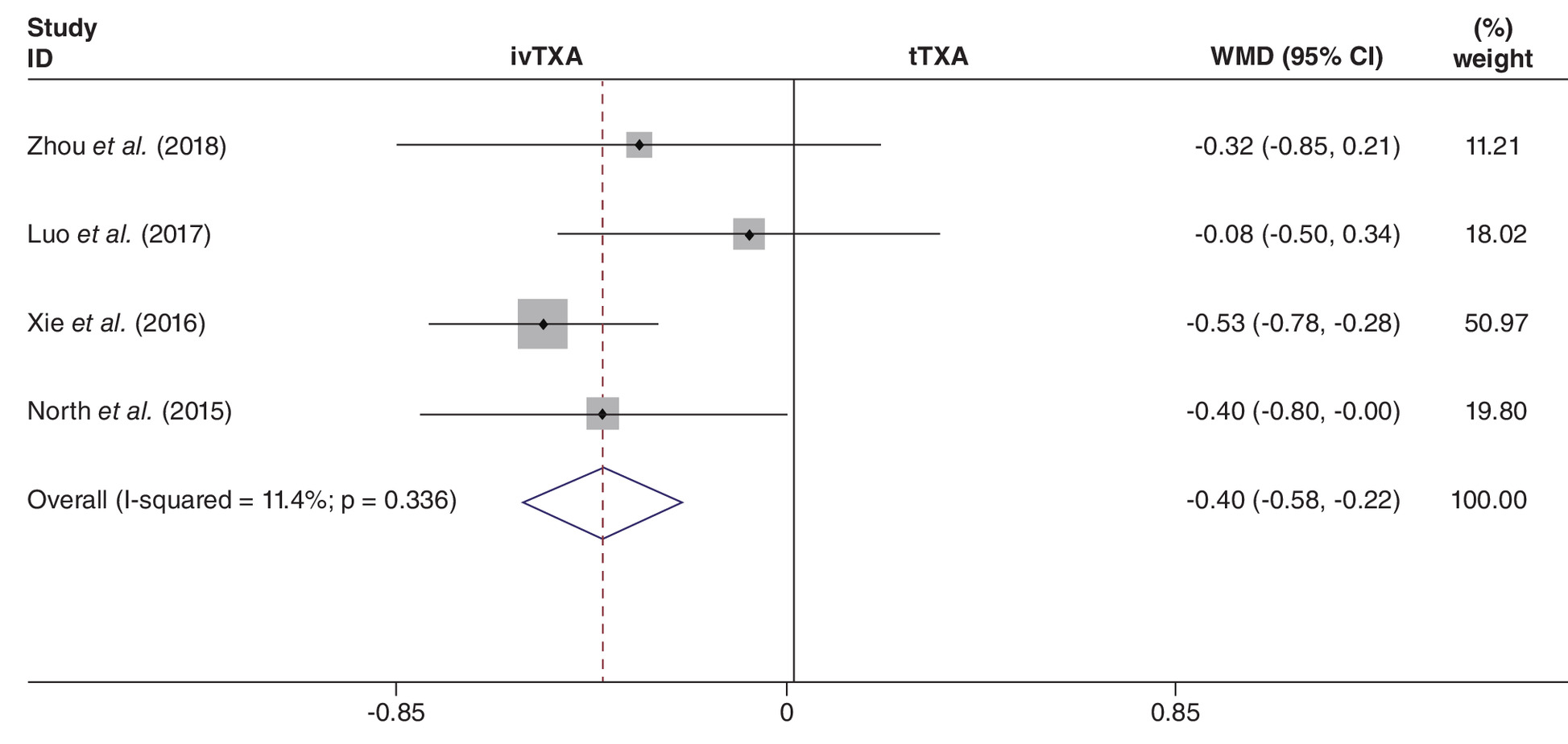
Figure 4. Forest plot diagram of the effect of intravenous versus tTXA on maximum hemoglobin drop.
ivTXA: Intravenous tranexamic acid; tTXA: Topical tranexamic acid; WMD: Weighted mean difference.
Transfusion rate
All the ten RCTs reported direct information on the blood transfusion rate. Transfusions were needed in 63 of 639 cases (9.9%) in the topical group, compared with 79 of 656 cases (12.0%) in the intravenous group. Significant heterogeneity was not revealed (I2 = 0.0%; p = 0.442), so a fixed-effect model was adopted. The results showed that there was no significant difference between the two groups (OR: 1.274; 95% CI: 0.885, 1.835; p = 0.193; Figure 5).
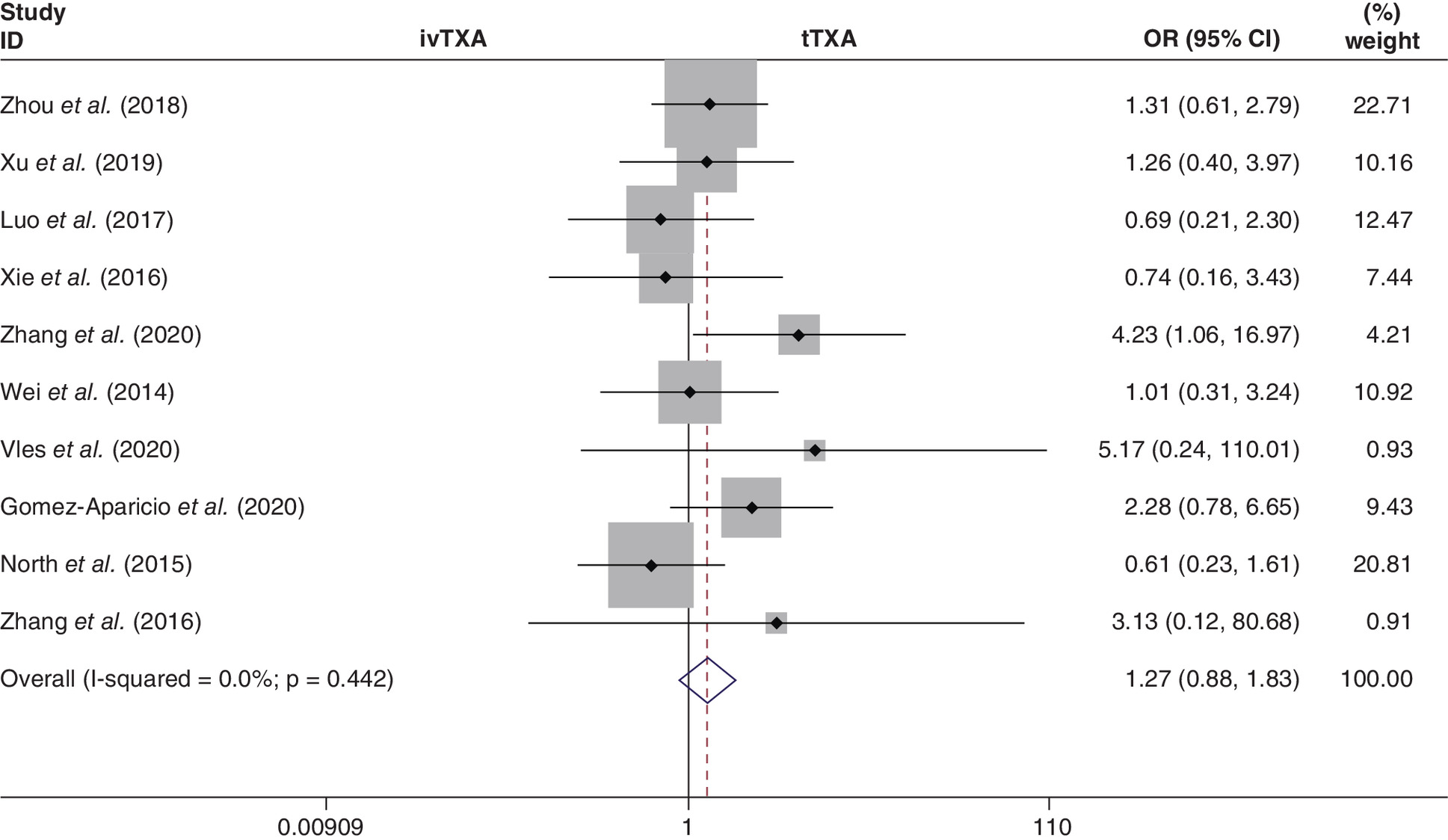
Figure 5. Forest plot diagram of the effect of intravenous versus tTXA on transfusion rate.
ivTXA: Intravenous tranexamic acid; tTXA: Topical tranexamic acid; WMD: Weighted mean difference.
A subgroup analysis was performed based on topical dose (≥2 g) or intravenous dose (single). Among the whole ten RCTs, nine studies (1247 patients) provided data on topical dose ≥2 g and eight studies (1043 patients) provided data on a single intravenous dose. The fixed-effect model was adopted because significant heterogeneity was not found among the studies (I2 <50%; p > 0.1). The subgroup analysis demonstrated that there was no significant difference observed in the transfusion rate between the topical route (dose ≥2 g) and the intravenous route (OR: 1.257; 95% CI: 0.870; 1.815; p = 0.222). Similarly, ivTXA in a single dose showed no significant difference in transfusion rate compared with the topical route (OR: 1.504; 95% CI: 0.942, 2.401; p = 0.088; Figure 6).
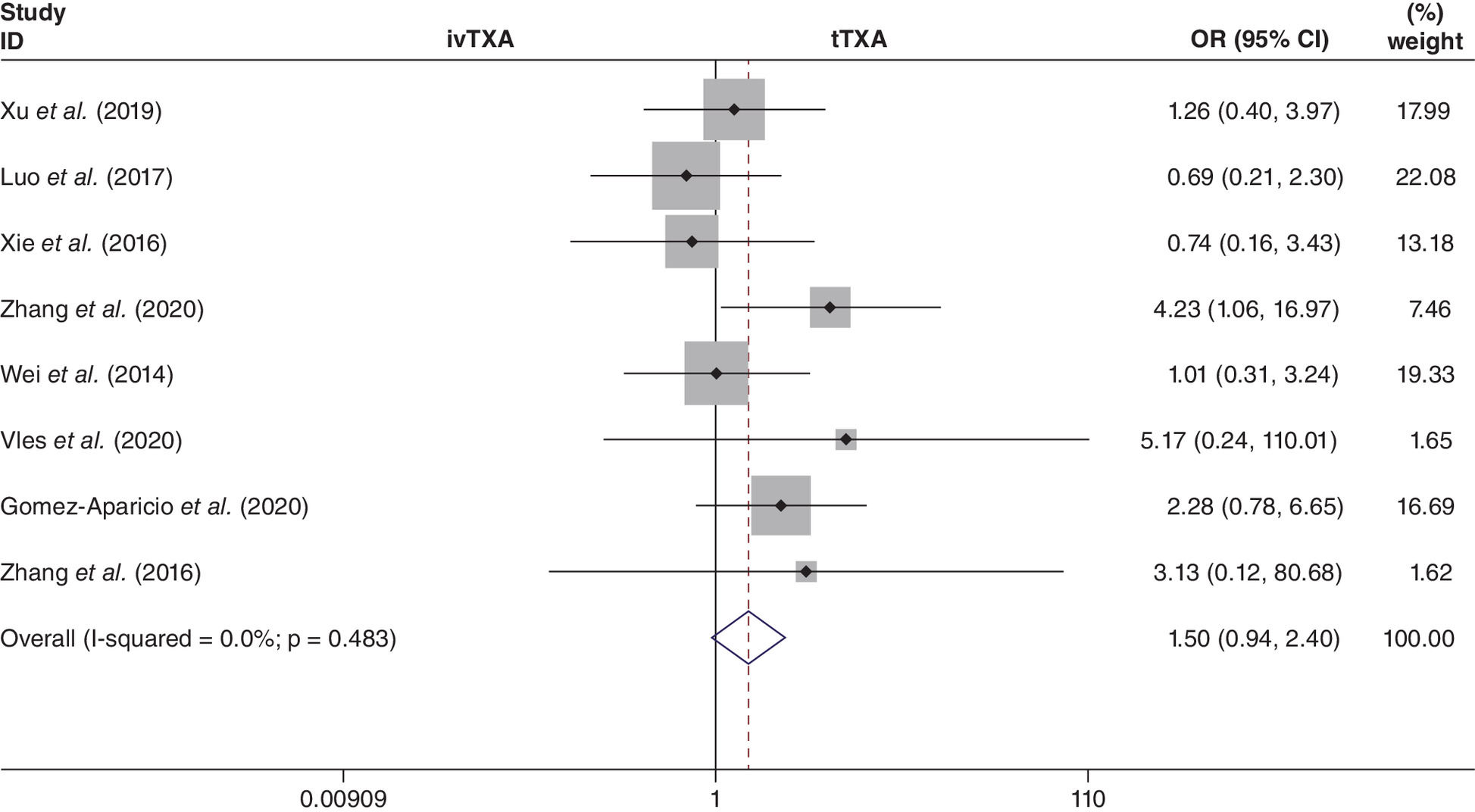
Figure 6. Forest plot diagram of the effect of the single-dose intravenous versus tTXA on transfusion rate.
ivTXA: Intravenous tranexamic acid; tTXA: Topical tranexamic acid.
Drainage volume
Four studies (568 patients) mentioned the data of drainage volume, and a random-effect model was used owing to significant heterogeneity among the studies (I2 = 96.3%; p < 0.001). The result showed there was no significant difference in drainage volume between the two groups (WMD = 44.152, 95% CI: -84.118, 172.422; p = 0.500). More details were shown in Table 4.
| Outcomes | Studies numbers | Groups size | Overall effect | Heterogeneity | ||||
|---|---|---|---|---|---|---|---|---|
| ivTXA | tTXA | Effect estimate | 95% CI | p-value | I2(%) | p-value | ||
| Transfusion rate | 10 | 656 | 639 | OR, 1.274 | 0.885, 1.835 | 0.193 | 0.0% | 0.442 |
| tTXA dose ≥2 g | 9 | 632 | 615 | OR, 1.257 | 0.870, 1.815 | 0.222 | 7.3% | 0.374 |
| ivTXA dose = single | 8 | 529 | 514 | OR, 1.504 | 0.942, 2.401 | 0.088 | 0.0% | 0.483 |
| Total blood loss | 7 | 536 | 514 | WMD, -40.665 | -85.153, 3.823 | 0.073 | 16.2% | 0.306 |
| Intraoperative blood loss | 4 | 210 | 213 | WMD, -12.687 | -22.291, -3.083 | 0.010 | 0.0% | 0.763 |
| Hidden blood loss | 3 | 216 | 191 | WMD, 14.276 | 9.936, 19.459 | <0.001 | 20.6% | 0.284 |
| Postoperative 1st Hb | 6 | 346 | 321 | WMD, -1.803 | -5.269, 1.663 | 0.308 | 74.3% | 0.002 |
| Drainage volume | 4 | 295 | 273 | WMD, 44.152 | -84.118, 172.422 | 0.500 | 96.3% | 0.000 |
| Maximum Hb drop | 4 | 257 | 255 | WMD, -0.400 | -0.577, -0.222 | <0.001 | 11.4% | 0.336 |
| DVT | 9 | 545 | 549 | RD, 0.000 | -0.014, 0.014 | 0.992 | 0.0% | 0.906 |
| Wound complications | 5 | 409 | 389 | RD, -0.003 | -0.028, 0.022 | 0.816 | 0.0% | 0.920 |
| Length of stay | 6 | 437 | 413 | WMD, 0.283 | -0.152, 0.718 | 0.202 | 88.0% | 0.000 |
DVT: Deep vein thrombosis; Hb: Hemoglobin; ivTXA: Intravenous tranexamic acid; OR: Odds ratio; RD: Rate difference; tTXA: Topical tranexamic acid; WMD: Weighted mean difference.
Complications
A total of nine publications provided the patient’s numbers of DVT events after THA and there was no significant heterogeneity (I2 = 0.0%; p = 0.906). Compared 545 patients treated with ivTXA to 549 patients treated with tTXA during THA, there was no statistical difference in DVT between the two groups (RD = 0.000; 95% CI: -0.014–0.014; p = 0.992, Figure 7). As for the wound complications, five studies reported related information without significant heterogeneity (I2 = 0.0%; p = 0.920) and no statistical difference was revealed between the two groups (OR: -0.003; 95% CI: -0.028, 0.022; p = 0.816).
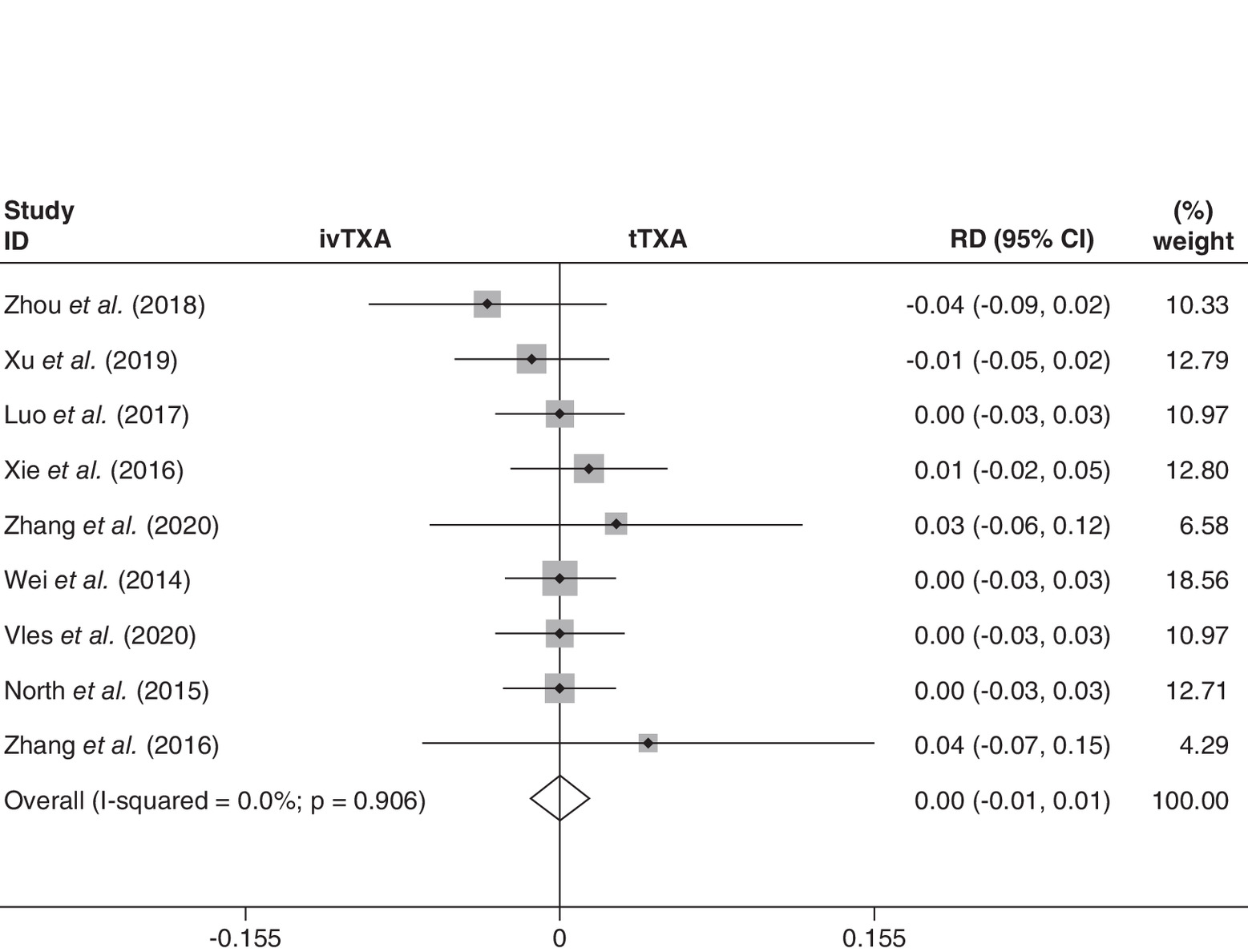
Figure 7. Forest plot diagram of the effect of intravenous versus topical tranexamic acid on deep vein thrombosis events.
ivTXA: Intravenous tranexamic acid; RD: Rate difference; tTXA: Topical tranexamic acid.
Length of stay
Six studies (850 patients) in total reported the LOS. We adopted the random-effect model due to the significant heterogeneity (I2 = 88.0%; p = 0.000). Pooled results revealed no statistical difference in the two groups (OR: 0.283; 95% CI: -0.152, 0.718; p = 0.202).
Discussion
Perioperative blood-sparing management is an important component of enhanced recovery after surgery [22]. As an antifibrinolytic agent, TXA administrated in different routes including oral, intravenous, topical and combined routes have been adopted in the clinic to reduce perioperative blood loss and transfusion rate during total joint arthroplasty for decades with reliable efficiency and safety [12,13,23]. During the above management routes, intravenous and tTXA have been most commonly compared for a long-running controversy, simply, ivTXA might lead to a higher risk of thromboembolic events but a better hemostatic effect in theory, while the topical approach is just the opposite. Although, the previous meta-analysis has revealed no statistical differences between these two routes during total joint arthroplasty, optimal administration of TXA is elusive especially for THA because most clinical research focused on total knee arthroplasty (TKA) and only limited RCTs did that for THA up to date [12–17,24]. For example, the latest meta-analysis in 2019 compared intravenous and tTXA in total knee and hip arthroplasty based on 20 RCTs, during which only five studies adopted TXA in THA [13]. As far as we know, our study is the most comprehensive systematic review and meta-analysis including ten RCTs in total comparing the efficacy and safety of intravenous versus tTXA during THA, which would avoid the heterogeneity caused by totally different surgical management between THA and TKA [18,25–34].
In this study, we firstly analyzed blood loss-related items during THA. Although the results showed no statistical differences between the two routes on the TBL, which is consistent with the previous report [13,17], the average TBL in the intravenous group was smaller than the topical group. Similarly, in one meta-analysis, it was also concluded that ivTXA can lead to smaller TBL and the possible explanation is that intravenous administration of TXA might take effect earlier than the topical method whose hemostatic effect is restricted to postoperative bleeding [14]. Our result may support this view because IBL was significantly smaller in patients treated with ivTXA compared with the topical approach. Meanwhile, we further analyzed HBL which was reported to occupy approximately 50% of TBL and thus a key parameter to be considered [35]. A total of three RCTs indicated that averaged HBL was lower in the intravenous group, and the result was statistically significant. What’s more, the result of lower HBL in the intravenous group was consistent with the previous report [14].
Hb level is the most important indicator to decide transfusion or not after surgery. A total of seven RCTs reported the Hb level of postoperative day 1, which demonstrated no statistical difference between the two routes in this study. However, the maximum Hb drop always appears on postoperative days 3–4 owing to HBL [36]. As a result, the maximum Hb drop was smaller in patients treated with ivTXA and this difference was statistically significant according to four RCTs. This lower maximum Hb drop induced by ivTXA may be especially significant for the rapid recovery of elderly patients receiving THA.
Although ivTXA is much more effective to reduce IBL, HBL and received less maximum Hb drop, the transfusion rate is similar in the present study, which may result from the similar TBL and different administrative doses of TXA among the included RCTs. Furthermore, the difference in maximum Hb drop may be compromised by different transfusion standards. To avoid the effects of different doses, we did a subgroup analysis for the ivTXA with a single dose and tTXA with a dose ≥2 g. Two doses of ivTXA will normally reduce the first dose of TXA, which in turn affecting the first-dose effect. At the same time, the fibrinolytic process might be repressed by the body and even be replaced by an antifibrinolytic reaction after surgery, which leads to less efficiency of the second dose of ivTXA in reducing blood loss [37]. The pooled result indicated ivTXA administrated in a single dose did not reduce transfusion rate compared with the topical route. The possible explanation is that although single-dose ivTXA enhances coagulation functions compared with tTXA during THA according to thrombosis-related parameters recorded by thromboelastography [32], the tTXA administration could reach a maximum and local dose in the shortest time at the surgical bleeding areas and; therefore, inhibit fibrinolytic and result in effective local microvascular hemostasis [38]. More importantly, the previous meta-analysis have reported the same effect on transfusion rate in the two routes during either THA or TKA [13,14,24].
Drainage volume after THA was similar in the study. Theoretically, tTXA will affect drainage volume because most of the fluid that dilutes TXA left in the joint will flow into the drainage pack in the end. Meanwhile, the time to clamp the drainage tube and remove the drainage tube can inevitably interfere with the final drainage volume [39]. Although TXA is always with a certain risk of thrombosis, this has not been reported before [40]. Some studies even reported a potential protective role of TXA on thrombogenesis [41]. Similarly, our meta-analysis found no statistical difference between these two routes. Routine postoperative anticoagulation measures such as low molecular weight heparin, rivaroxaban and intermittent pneumatic compression devices could have reduced the real difference of thrombotic events caused by different routes of TXA. Besides, differentiated anticoagulation management as shown in Table 2 might also affect the reliability of results. Wound infection leads to delayed wound healing and even revision surgery [42]. The result showed no significant difference between intravenous and tTXA. Although it was reported that topical irrigation with TXA increased wound tension which in turn increase the risk of wound complication, this most commonly occurs in the knee joint instead of the hip joint owing to different anatomical conditions [43].
There are some strengths in this study compared with the previous meta-analysis. First, we only included RCTs which increased the reliability of results. Meanwhile, the most comprehensive RCTs on the ‘head-to-head’ comparison of topical and intravenous routes during THA were included in the study. In addition, considering the different anatomy and surgical administration in the knee and hip, only THA was selected for our research. At the same time, this study also has several limitations. First of all, significant heterogeneity exists among the included trials because of differentiation in perioperative management. Additionally, methodological deficits appeared in several trials, and insufficient details affect quality assessment in trials. Moreover, the lack of effective long-term follow-up details inevitably results in the underestimation of postoperative complications.
Conclusion
This systematic review and meta-analysis indicated the comparable effect of intravenous administration of TXA on transfusion rate, TBL, Hb of postoperative day 1, drainage volume, DVT events and wound complications compared with the topical route. There were statistically significant differences in IBL, HBL and maximum Hb drop between the two routes. However, the heterogeneity between studies is higher than 50% with respect to Hb of postoperative day 1, drainage volume and LOS, which could influence the results. Given the amount of included RCTs is limited and differentiated perioperative management, the generality of our conclusions is relatively restricted. Therefore, more high-quality RCTs are essential to determine the optimal TXA administration method in the future to support the existing conclusion.
•
The optimal management approach for tranexamic acid (TXA) in primary total hip arthroplasty (THA) is still controversial.
•
This meta-analysis aimed to evaluate the efficacy and safety of intravenous versus topical TXA (tTXA) during THA.
•
The most comprehensive randomized controlled trials (RCTs) on the ‘head-to-head’ comparison of topical and intravenous routes during THA were included in the study.
•
The present result indicated comparable safety and transfusion rate for intravenous and tTXA in primary THA.
•
The intravenous TXA demonstrated a smaller intraoperative blood loss hidden blood loss and maximum hemoglobin drop compared with tTXA.
•
Given the amount of included RCTs is limited, the generality of our conclusions is relatively restricted.
•
More high-quality RCTs are essential to determine the optimal TXA administration method in the future to support the existing conclusion.
•
This study is of great significance for the clinical management of TXA during THA.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Data sharing statement
The datasets used and/or analyzed during this study are available from the corresponding author upon reasonable request.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Malik AT, Jain N, Scharschmidt TJ, Li M, Glassman AH, Khan SN. Does surgeon volume affect outcomes following primary total hip arthroplasty? A systematic review. J. Arthroplasty 33(10), 3329–3342 (2018).
2.
Klug A, Gramlich Y, Hoffmann R, Pfeil J, Drees P, Kutzner KP. Trends in total hip arthroplasty in Germany from 2007 to 2016: what has changed and where are we now? Z. Für Orthop. Unfallchirurgie 3(3), 1–8 (2019).
3.
Singh JA, Yu S, Chen L, Cleveland JD. Rates of total joint replacement in the United States: future projections to 2020–2040 using the National Inpatient Sample. J. Rheumatol. 46(9), 1134–1140 (2019).
• Demonstrates that significant increase in the use of total hip arthroplasty and total knee arthroplasty are expected in the USA in the future if the current trend continues.
4.
Ferguson RJ, Palmer AJ, Taylor A, Porter ML, Malchau H, Glyn-Jones S. Hip replacement. Lancet Lond. Engl. 392(10158), 1662–1671 (2018).
5.
Gustafsson UO, Scott MJ, Hubner M et al. Guidelines for perioperative care in elective colorectal surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018. World J. Surg. 43(3), 659–695 (2019).
6.
Palmer AJR, Lloyd TD, Gibbs VN et al. The role of intraoperative cell salvage in patient blood management for revision hip arthroplasty: a prospective cohort study. Anesthesia 75(4), 479–486 (2020).
7.
Fowler AJ, Ahmad T, Phull MK, Allard S, Gillies MA, Pearse RM. Meta-analysis of the association between preoperative anemia and mortality after surgery. Br. J. Surg. 102(11), 1314–1324 (2015).
• This systematic review and meta-analysis of observational studies explores associations between preoperative anemia and postoperative outcomes and demonstrates that preoperative anemia is associated with poor outcomes after surgery.
8.
Kim JL, Park J-H, Han S-B, Cho IY, Jang K-M. Allogeneic blood transfusion is a significant risk factor for surgical-site infection following total hip and knee arthroplasty: a meta-analysis. J. Arthroplasty 32(1), 320–325 (2017).
9.
Lopez-Picado A, Barrachina B, Remón M, Errea M. Cost-benefit analysis of the use of tranexamic acid in total replacement hip surgery. J. Clin. Anesth. 57(1), 124–128 (2019).
• Demonstrates that the administration of tranexamic acid (TXA) is cost-effective, especially in total replacement hip surgery.
10.
Fillingham YA, Ramkumar DB, Jevsevar DS et al. The safety of tranexamic acid in total joint arthroplasty: a direct meta-analysis. J. Arthroplasty 33(10), 3070–3082 (2018).
• Demonstrates that the benefits of using TXA appear to outweigh the potential risks of thromboembolic events even in patients with higher comorbidity during total joint arthroplasty.
11.
Hunt BJ. The current place of tranexamic acid in the management of bleeding. Anesthesia 70, 50–53 (2015).
12.
Xu S, Chen JY, Zheng Q et al. The safest and most efficacious route of tranexamic acid administration in total joint arthroplasty: a systematic review and network meta-analysis. Thromb. Res. 176(1), 61–66 (2019).
13.
Sun Q, Li J, Chen J, Zheng C, Liu C, Jia Y. Comparison of intravenous, topical or combined routes of tranexamic acid administration in patients undergoing total knee and hip arthroplasty: a meta-analysis of randomized controlled trials. BMJ Open 9(1), 1–14 (2019).
14.
Xie J, Hu Q, Huang Q, Ma J, Lei Y, Pei F. Comparison of intravenous versus topical tranexamic acid in primary total hip and knee arthroplasty: an updated meta-analysis. Thromb. Res. 153(1), 28–36 (2017).
15.
Zhang P, Liang Y, Chen P, Fang Y, He J, Wang J. Intravenous versus topical tranexamic acid in primary total hip replacement. Medicine (Baltimore) 95(50), 1–7 (2016).
16.
Li J, Zhang Z, Chen J. Comparison of efficacy and safety of topical versus intravenous tranexamic acid in total hip arthroplasty. Medicine (Baltimore) 95(36), 1–8 (2016).
17.
Sun X, Dong Q, Zhang Y. Intravenous versus topical tranexamic acid in primary total hip replacement: a systemic review and meta-analysis. Int. J. Surg. 32(1), 10–18 (2016).
18.
Zhang X, Ma D, Wen L, Pan J. Better treatment values in local application of tranexamic acid (TXA) than intravenous application with the same dose in total hip arthroplasty. Adv. Ther. 37(10), 4346–4355 (2020).
19.
Page MJ, McKenzie JE, Bossuyt PM et al. Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. J. Clin. Epidemiol. 1(1), 1–22 (2021).
•• Summarizes decisions made at the PRISMA 2020 update meeting, describe and justify changes made to the guideline, which will enhance the acceptance and uptake of the guideline and assist those developing and updating future reporting guidelines.
20.
Shamseer L, Moher D, Clarke M et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ 350(2), 1–25 (2015).
21.
Higgins JPT, Altman DG, Gøtzsche PC et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343(1), 1–9 (2011).
22.
Joliat G-R, Ljungqvist O, Wasylak T, Peters O, Demartines N. Beyond surgery: clinical and economic impact of Enhanced Recovery After Surgery programs. BMC Health Serv. Res. 18(1), 1–4 (2018).
23.
Fillingham YA, Ramkumar DB, Jevsevar DS et al. The safety of tranexamic acid in total joint arthroplasty: a direct meta-analysis. J. Arthroplasty 33(10), 3070–3082 (2018).
24.
Alshryda S, Sukeik M, Sarda P, Blenkinsopp J, Haddad FS, Mason JM. A systematic review and meta-analysis of the topical administration of tranexamic acid in total hip and knee replacement. Bone Jt J. 96(8), 1005–1015 (2014).
25.
Aglietti P, Baldini A, Vena LM, Abbate R, Fedi S, Falciani M. Effect of tourniquet use on activation of coagulation in total knee replacement. Clin. Orthop. 6(371), 169–177 (2000).
26.
Wei W, Wei B. Comparison of topical and intravenous tranexamic acid on blood loss and transfusion rates in total hip arthroplasty. J. Arthroplasty 29(11), 2113–2116 (2014).
27.
Xie J, Ma J, Yue C, Kang P, Pei F. Combined use of intravenous and topical tranexamic acid following cementless total hip arthroplasty: a randomised clinical trial. Hip Int. 26(1), 36–42 (2016).
28.
North WT, Mehran N, Davis JJ, Silverton CD, Weir RM, Laker MW. Topical vs intravenous tranexamic acid in primary total hip arthroplasty: a double-blind, randomized controlled trial. J. Arthroplasty 31(5), 1022–1026 (2016).
29.
Zhang Y, Zhang L, Ma X et al. What is the optimal approach for tranexamic acid application in patients with unilateral total hip arthroplasty? Orthopade 45(7), 616–621 (2016).
30.
Zhou K, Wang H-Y, Wang Y, Liu Z-H, He C, Feng J-M. Is topical or intravenous tranexamic acid preferred in total hip arthroplasty? A randomized, controlled, noninferiority clinical trial. PLoS ONE 13(10), 1–13 (2018).
31.
Gómez Barbero P, Gómez Aparicio MS, Blas Dobón JA, Pelayo de Tomás JM, Morales Suárez-Varela M, Rodrigo Pérez JL. Which route of administration of acid tranexamic, intravenous or intra-articular, is more effective in the control of post-surgical bleeding after a total hip arthroplasty? A prospective, controlled and randomized study. Rev. Espanola Cirugia Ortop. Traumatol. 63(2), 138–145 (2019).
32.
Xu X, Jiang J, Liu W, Li X, Lu H. Application of thromboelastography to evaluate the effect of different routes administration of tranexamic acid on coagulation function in total hip arthroplasty. J. Orthop. Surg. 14(1), 1–8 (2019).
33.
Vles GF, Corten K, Driesen R, van Elst C, Ghijselings SG. Hidden blood loss in direct anterior total hip arthroplasty: a prospective, double blind, randomized controlled trial on topical versus intravenous tranexamic acid. Musculoskelet. Surg. 3(1), 1–7 (2020).
•• Provides detailed insights into the intra- and postoperative blood loss in total hip arthroplasty and shows that topical and intravenous TXA have similar effects on hidden blood loss.
34.
María del Sol Gómez-Aparicio, Patricia Gómez-Barbero, José Antonio Blas-Dobón, Alfredo Villar-Blanco, María Morales-Suárez-Varela, José Luís Rodrigo-Pérez. Results after the application of tranexamic acid intravenous or intra-articular in the control of postsurgical bleeding after total hip arthroplasty: a randomized controlled trial. Eur. J. Orthop. Surg. Traumatol. Orthop. Traumatol. 30(7), 1221–1230 (2020).
35.
Good L, Peterson E, Lisander B. Tranexamic acid decreases external blood loss but not hidden blood loss in total knee replacement. Br. J. Anaesth. 90(5), 596–599 (2003).
36.
Zhou Q, Zhou Y, Wu H et al. Changes of hemoglobin and hematocrit in elderly patients receiving lower joint arthroplasty without allogeneic blood transfusion. Chin. Med. J. (Engl.) 128(1), 75–78 (2015).
37.
Blanié A, Bellamy L, Rhayem Y et al. Duration of postoperative fibrinolysis after total hip or knee replacement: a laboratory follow-up study. Thromb. Res. 131(1), 6–11 (2013).
38.
Alshryda S, Sukeik M, Sarda P, Blenkinsopp J, Haddad FS, Mason JM. A systematic review and meta-analysis of the topical administration of tranexamic acid in total hip and knee replacement. Bone Jt J. 96(8), 1005–1015 (2014).
39.
Chareancholvanich K, Siriwattanasakul P, Narkbunnam R, Pornrattanamaneewong C. Temporary clamping of drain combined with tranexamic acid reduce blood loss after total knee arthroplasty: a prospective randomized controlled trial. BMC Musculoskelet. Disord. 13(124), 1–6 (2012).
40.
Poeran J, Rasul R, Suzuki S et al. Tranexamic acid use and postoperative outcomes in patients undergoing total hip or knee arthroplasty in the United States: retrospective analysis of effectiveness and safety. BMJ 349(4829), 1–10 (2014).
41.
Godier A, Roberts I, Hunt BJ. Tranexamic acid: less bleeding and less thrombosis? Crit. Care 16(3), 135 (2012).
42.
Pincus D, Jenkinson R, Paterson M, Leroux T, Ravi B. Association between surgical approach and major surgical complications in patients undergoing total hip arthroplasty. JAMA 323(11), 1070–1076 (2020).
43.
Sarzaeem MM, Razi M, Kazemian G, Moghaddam ME, Rasi AM, Karimi M. Comparing efficacy of three methods of tranexamic acid administration in reducing hemoglobin drop following total knee arthroplasty. J. Arthroplasty 29(8), 1521–1524 (2014).
Information & Authors
Information
Published In
Pages: 1089 - 1102
PubMed: 34406022
Copyright
© 2021 Future Medicine Ltd.
History
Received: 24 March 2021
Accepted: 25 July 2021
Published online: 18 August 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparison of intravenous versus topical tranexamic acid in primary total hip arthroplasty: a systematic review and meta-analysis of ten randomized trials. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0084
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Lin Zhao, Jinli Xie, Chong Wu, Topical, Local Injection, and Intravenous Tranexamic Acid for Postoperative Recovery in Implant-Based Rhinoplasty, Journal of Craniofacial Surgery, 10.1097/SCS.0000000000012605, (2026).
- İsmail Güzel, İbrahim Ulusoy, Mehmet Yılmaz, Mehmet Fırat Tantekin, Aybars Kıvrak, Comparison of Intravenous, Topical, and Control Groups in Blood Management During Total Hip Arthroplasty: A Retrospective Analysis, Advances in Orthopedics, 10.1155/aort/2709548, 2026, 1, (2026).
- Ankush Vinay Mohabey, Tranexamic acid in total hip arthroplasty—Differential efficacy in inflammatory versus degenerative arthritis, Current Rheumatology Research, 10.46439/rheumatology.5.031, 5, 1, (22), (2025).
- Amelia K. Stoner, Lynn M. Pezzanite, Steven W. Dow, Nicholas A. Alfonso, Kirk C. McGilvray, An In Vitro Assessment of a Biopolymer-Based Medical Foam for Enhanced Antifibrinolytic and Infection Prophylaxis for Acute Wound Management , ACS Applied Bio Materials, 10.1021/acsabm.5c01584, 8, 12, (10878-10889), (2025).
- Alessandro V. Oliveira, Ana Luiza N. Sampaio, Glicia A. Freitas, Dangilla R. Santos, Manoela C. Souza, Yuri C. Silva, Rui W. Mascarenhas, Luis Otávio A. D. Pinto, Tranexamic Acid in Men Undergoing Transurethral Resection of Prostate: An Updated Systematic Review and Meta‐Analysis, The Prostate, 10.1002/pros.70095, 86, 3, (279-290), (2025).
- Maude Boucher, Juliette Tremblay, Théo Pelet, Julien Dartus, Etienne L. Belzile, Stéphane Pelet, Topical Versus Systemic Tranexamic Acid to Reduce Blood Loss After Total Knee and Total Hip Arthroplasty, Journal of Bone and Joint Surgery, 10.2106/JBJS.24.01511, 107, 20, (2300-2309), (2025).
- Chengxin Xie, Liwei Zhang, Guoping Cai, Yongwei Su, Peng Wang, Hua Luo, Efficacy and safety of topical versus intravenous tranexamic acid in spinal surgery: a systematic review and meta-analysis, BMC Surgery, 10.1186/s12893-024-02743-2, 25, 1, (2025).
- Jun Wakasa, Kentaro Iwakiri, Yoichi Ohta, Yukihide Minoda, Akio Kobayashi, Hiroaki Nakamura, Perioperative bleeding control in total hip arthroplasty: hemostatic powder vs. tranexamic acid-a prospective randomized controlled trial, Archives of Orthopaedic and Trauma Surgery, 10.1007/s00402-024-05475-3, 144, 8, (3797-3805), (2024).
- Didier Mainard, Drainage in primary and revision hip and knee arthroplasty, Orthopaedics & Traumatology: Surgery & Research, 10.1016/j.otsr.2023.103764, 110, 1, (103764), (2024).
- Didier Mainard, Le drainage dans les prothèses et révisions de prothèses de hanche et de genou, Revue de Chirurgie Orthopédique et Traumatologique, 10.1016/j.rcot.2023.07.004, 109, 6, (S142-S147), (2023).