The health-related quality of life of patients with a benign gynecological condition: a 2-year follow-up
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess health-related quality of life (HRQoL) of patients with benign gynecological disorders. Materials & methods: Prospective 2-year follow-up with the 15D HRQoL-instrument of 311 women treated in Helsinki-area hospitals in 2012–2013. Results: The initially impaired HRQoL regarding excretion, discomfort and symptoms, and vitality and sexual activity improved after treatment. However, only sexual activity reached similar levels as in the general population. Treatment of endometriosis, fibroids and polyps resulted in best and that of unspecific pelvic pain and bleeding disorders in worst HRQoL scores. Results were independent of hospital size. Conclusion: The impaired HRQoL dimensions were improved by treatment but HRQoL still remained poorer than in the general female population. Treatment of unspecific pelvic pain and bleeding disorders needs further evaluation.
The impact of seemingly simple common benign gynecological conditions on the quality of life (QoL) of women [1] and on the costs for the society is high [2,3]. Half of fertile aged women suffer from a benign gynecological condition [4]. Nearly 80% of these women see a doctor annually and a third spends one or more days in bed every year due to their condition [1]. Physical, sexual and mental well-being is impaired in these women [1,5,6]. Women with chronic pelvic pain and conditions associated with it (endometriosis) have been reported to have worse health-related QoL (HRQoL) than women with other benign gynecological conditions [1]. However, it is not only the endometriosis and pelvic pain patients that suffer from diminished HRQoL as for example two-thirds of uterine fibroid patients report moderate to severe symptoms and diminished HRQoL [7]. Even more concerning than this is the fact that, for example, only a third of women treated for a gynecological bleeding disorder where satisfied with the treatment regarding symptoms and HRQoL 1 year after treatment [8]. Nevertheless, limited data on patient reported outcomes have hindered the establishment of new, better patient satisfaction yielding treatment protocols [9]. Another challenge in the field of benign gynecology is how to assess whether surgery yields more benefit than conservative treatment and whether this benefit will last. For example, studies have not been able to answer whether surgical treatment of pelvic organ prolapse improves HRQoL at all, and if it does, will the benefit last in the long term [10–12].
During the recent years, there has been a shift among healthcare professionals toward a more patient-centered healthcare system. Patient-reported outcomes have gained importance when assessing treatments and can now-a-days even outweigh clinical and caregiver-reported outcomes during therapy selection [13]. In order to assess the HRQoL results of treatment, various generic instruments (such as EQ-5D, 15D, SF-36 or HUI-3) can be used.
The aim of this study is to provide new, original, and short- and long-term data on the HRQoL of patients with a common benign gynecological condition. The study perspective is that of patients in a typical outpatient gynecological clinic in a real-world setting. The long-term follow-up enables better recognition of patient groups whose treatment protocols need further development.
Materials & methods
A prospective observational HRQoL and cost study was conducted in the Department of Obstetrics and Gynecology in the hospitals of the Helsinki and Uusimaa Hospital District: the Helsinki University Hospital (comprising the Women’s Hospital, the Kätilöopisto Maternity Hospital and the Jorvi Hospital in the Helsinki metropolitan area) and four smaller community hospitals (Hyvinkää Hospital, Lohja Hospital, Porvoo Hospital and Raasepori Hospital [former Länsi-Uusimaa Hospital] outside of the Helsinki metropolitan area). The cost data will be reported separately. All women treated for a benign gynecological condition in the general gynecological outpatient department in these hospitals between 1 June 2012 and 31 August 2013 were invited to participate in the study. Patients with uterine fibroids or other benign uterine neoplasm, endometriosis, adenomyosis, a uterine prolapse, endometrial or cervical polyps, a gynecological bleeding disorder, dysmenorrhea or lower abdominal/pelvic pain, or some other benign uterine finding were included in the study. No other inclusion or exclusion criteria were used apart from the above-mentioned diagnosis groups. The ICD-10 classification codes were used to group the patients according to the clinician’s assessment. If a specific reason for the condition was found (for example a uterine fibroid or a uterine polyp causing abnormal uterine bleeding), this specific disease was the primary diagnosis and the patient fell into that patient group. If no apparent reason for the condition was found, the patient was categorized into the group reflecting the symptom (for example, idiopathic menorrhagia in the bleeding disorder group).
Patients were treated according to typical clinical practice. They filled in the 15D HRQoL questionnaire before treatment (before/when attending the first outpatient clinic appointment and baseline) and 6 months and 2 years after treatment initiation. If no answer to the follow-up survey was received in 3 weeks, one reminder was sent. The results were compared with the HRQoL of age-standardized general female population of the same geographical area (urban Southern Finland). The population data came from the Health 2011 Health Examination Survey which covers a representative sample of the general Finnish population [14].
The 15D is a standardized, generic and self-administered HRQoL instrument validated in the Finnish population that provides a HRQoL profile and a single index score. The patient is asked to evaluate its 15 dimensions (mobility, vision, hearing, breathing, sleeping, eating, speech, excretion, usual activities, mental function, discomfort and symptoms, depression, distress, vitality, and sexual activity) on a scale of 1–5 (1 = no problems and 5 = worst possible state). Population-based preference weights are used to calculate dimension level values and the single index score representing overall HRQoL (the 15D score) on a 0–1 scale (1 = full health and 0 = being dead). Thus, the higher the score is, the better the QoL of the patient is. Up to three missing answers can be imputed by predictions from linear regression analysis based on the other dimensions, with age and gender as independent variables [15,16]. The minimum clinically important change or difference in the 15D score has been established to be ± 0.015 [17].
Paired samples t-test was used to test the statistical significance of the change in HRQoL during follow-up. Statistical significance of the differences in means between groups was tested using Student’s t-test. A two-way p-value of <0.05 was considered statistically significant. All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (Ethics Committee of the Helsinki University Central Hospital, registration number 538/E0/02) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed written consent was obtained from all individual study participants. This included consent to include material pertaining to themselves and an acknowledgement that patients cannot be identified via the published article.
Results
Of the 1173 women who were invited to participate in the study, 543 women answered the baseline questionnaire. Of them 389 (71.6% of the women who decided to participate in the study) women fulfilling the inclusion criteria (concerning the reason of treatment and had answered at least 12 of the 15D dimensions in all three follow-up questionnaires) answered the 6-month follow-up and 311 (57.3%) women the 2-year follow-up. The mean age of the included patients at baseline was 49.6 years (standard deviation [SD] ± 12.8, range 19–98). Of them 178 (57.2%) were treated in a university hospital and 133 (42.8%) in a community hospital. Patients were treated due to bleeding disorders (n = 94), uterine fibroids (n = 79), polyps (n = 68), dysmenorrhea/pelvic pain (n = 24), endometriosis (n = 23), uterine prolapse (n = 7) or some other benign uterine disorder (n = 16). The mean long-term follow-up time was 24 months 11 days (SD ± 12 days).
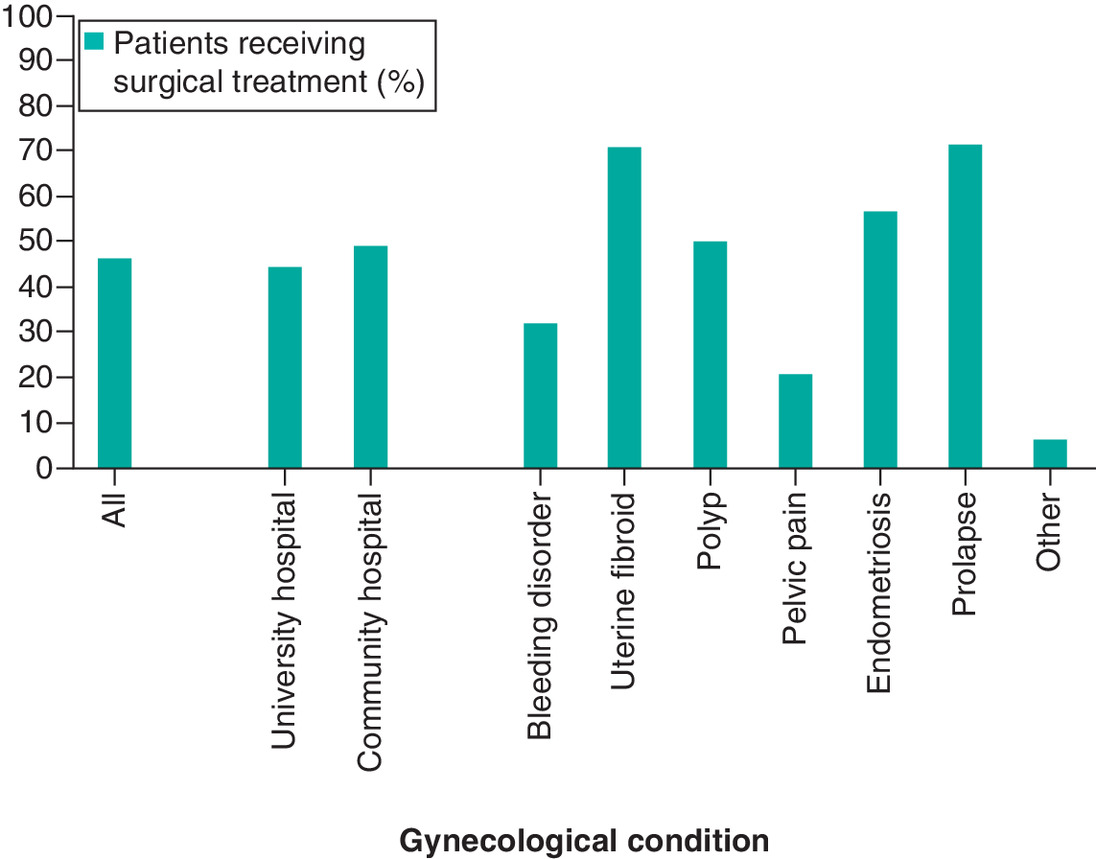
Of all patients 167 (46.3%) were treated operatively: 44.4% (n = 79) of university hospital patients and 48.9% (n = 65) of community hospital patients. The percentage of patients operated on varied depending on the patient’s disorder (Figure 1). The only statistically significant difference in operative treatment between university hospitals and community hospitals was the higher frequency of polyp treatment in the surgical theatre in community hospitals (66.7 vs 36.8%, p < 0.05).
HRQoL
The total HRQoL score improved in a clinically important manner (15D score change of ≥0.015) in 41.5% (n = 129) of the study patients by the 6-month follow-up and 46.3% (n = 144) by the 2-year follow-up. The mean 15D score had improved statistically significantly compared with baseline (mean 0.901, SD ± 0.084) at the 6-month (0.909, SD ± 0.092, p < 0.05) and the 2-year follow-ups (0.909, SD ± 0.087, p < 0.05) but it did not improve statistically significantly between the 6-month and 2-year measurement points. The dimensions of excretion, discomfort and symptoms, and vitality and sexual activity improved statistically significantly (p < 0.05) in the whole study group from baseline compared with both the 6-month and the 2-year follow-up. Of these dimensions, only sexual activity improved statistically significantly also between the 6-month and the 2-year follow-up. No dimensions deteriorated during the follow-up.
When compared with the age-standardized general female population of the same geographical area, patients in our study had poorer mean 15D scores both at baseline (0.901, SD ± 0.084 vs 0.927, SD ± 0.020) and at the follow-up points (0.909, SD ± 0.092 vs 0.927, SD ± 0.020 and 0.909, SD ± 0.087 vs 0.924, SD ± 0.024). The differences were both statistically significant (p < 0.05) and clinically important (≥0.015). At baseline, the study patients were statistically significantly worse off on the dimensions of vision, sleeping, excretion, usual activities, discomfort and symptoms, distress, and vitality and sexual activity than the general female population. Of the dimensions impaired at baseline, treatment effectively improved only sexual activity to a similar level as observed in the general population during the 2-year follow-up. All other dimensions impaired at baseline remained impaired during the whole follow-up (Figure 2).
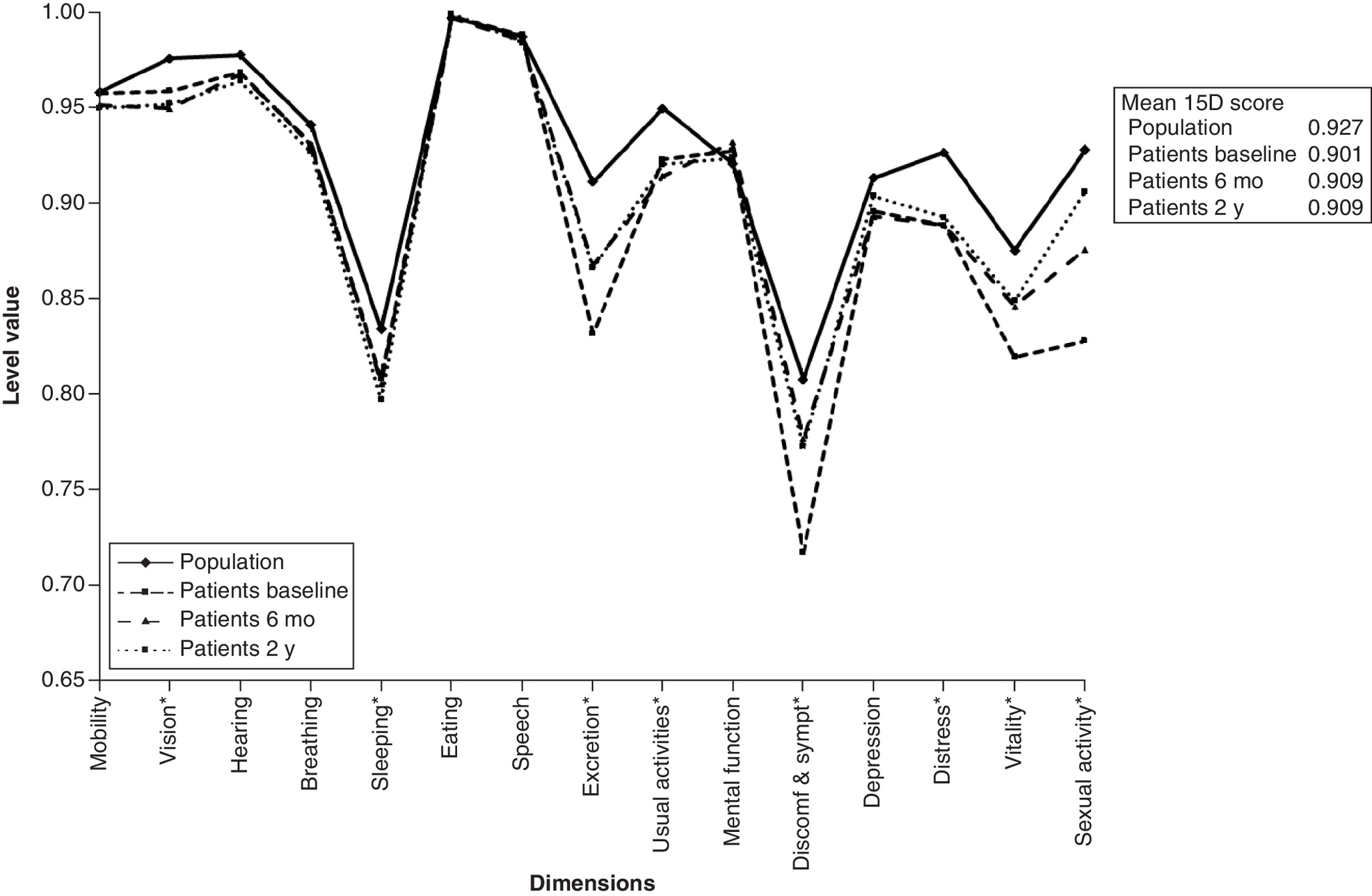
Figure 2. Health-related quality of life profile & 15D scores of age-standardized general female population compared with study patients at baseline, 6 months & 2 years.
*Statistically significant difference when comparing study patients and the general female population.
Both at baseline and at the short-term follow-up, patients with a uterine fibroid or polyp were better off regarding total HRQoL than those with pelvic pain (p < 0.05). At the 2-year follow-up the only significant difference in total HRQoL was seen between patients with fibroids and bleeding disorders in favor of the fibroid patient group. The total HRQoL score did not differ significantly when comparing the other patient groups to each other at the different follow-up points (Table 1).
| 15D baseline | 15D 6 months | 15D 2 years | |
|---|---|---|---|
| All | 0.901 (SD ± 0.08)† | 0.909 (SD ± 0.09)† | 0.909 (SD ± 0.09)† |
| University hospitals | 0.898 (SD ± 0.09) | 0.905 (SD ± 0.09) | 0.902 (SD ± 0.09) |
| Community hospitals | 0.905 (SD ± 0.08) | 0.914 (SD ± 0.09) | 0.919 (SD ± 0.08) |
| Bleeding disorder | 0.895 (SD ± 0.10) | 0.900 (SD ± 0.10) | 0.898 (SD ± 0.10) |
| Fibroid | 0.911 (SD ± 0.07)† | 0.917 (SD ± 0.09) | 0.926 (SD ± 0.07)† |
| Polyp | 0.910 (SD ± 0.08) | 0.921 (SD ± 0.08) | 0.915 (SD ± 0.08) |
| Pelvic pain/dysmenorrhea | 0.872 (SD ± 0.10) | 0.875 (SD ± 0.10) | 0.881 (SD ± 0.10) |
| Endometriosis | 0.894 (SD ± 0.07) | 0.914 (SD ± 0.09) | 0.906 (SD ± 0.09) |
| Prolapse | 0.883 (SD ± 0.09) | 0.911 (SD ± 0.12) | 0.886 (SD ± 0.15) |
| Other | 0.915 (SD ± 0.08) | 0.919 (SD ± 0.07) | 0.921 (SD ± 0.04) |
| All – oper | 0.915 (SD ± 0.06)† | 0.926 (SD ± 0.08)† | 0.927 (SD ± 0.07)† |
| All – nonoper | 0.889 (SD ± 0.10)† | 0.895 (SD ± 0.10)† | 0.894 (SD ± 0.09)† |
| Bleeding disorder – oper | 0.877 (SD ± 0.19) | 0.923 (SD ± 0.19) | 0.914 (SD ± 0.08) |
| Bleeding disorder – nonoper | 0.888 (SD ± 0.11) | 0.888 (SD ± 0.11) | 0.891 (SD ± 0.10) |
| Fibroid – oper | 0.925 (SD ± 0.05)† | 0.925 (SD ± 0.09) | 0.944 (SD ± 0.05)† |
| Fibroid – nonoper | 0.876 (SD ± 0.10)† | 0.898 (SD ± 0.08) | 0.880 (SD ± 0.09)† |
| Polyp –oper | 0.920 (SD ± 0.06) | 0.938 (SD ± 0.06) | 0.925 (SD ± 0.07) |
| Polyp – nonoper | 0.899 (SD ± 0.09) | 0.903 (SD ± 0.10) | 0.905 (SD ± 0.08) |
| Pelvic pain – oper | 0.913 (SD ± 0.08) | 0.894 (SD ± 0.09) | 0.889 (SD ± 0.15) |
| Pelvic pain – nonoper | 0.861 (SD ± 0.10) | 0.870 (SD ± 0.10) | 0.879 (SD ± 0.09) |
| Endometriosis – oper | 0.872 (SD ± 0.07) | 0.894 (SD ± 0.10) | 0.894 (SD ± 0.10) |
| Endometriosis – nonoper | 0.923 (SD ± 0.06) | 0.940 (SD ± 0.06) | 0.921 (SD ± 0.08) |
| Prolapse – oper | 0.908 (SD ± 0.04) | 0.976 (SD ± 0.03)† | 0.954 (SD ± 0.03)† |
| Prolapse – nonoper | 0.822 (SD ± 0.14) | 0.750 (SD ± 0.12)† | 0.715 (SD ± 0.21)† |
| Other – oper (n = 1) | 0.917 (−) | 0.879 (−) | 0.876 (−) |
| Other – nonoper | 0.915 (SD ± 0.08) | 0.922 (SD ± 0.07) | 0.924 (SD ± 0.04) |
†
Significant differences (p < 0.05).
All: baseline vs 6 months, baseline vs 2 years
Fibroid: baseline vs 2 years
All oper vs all nonoper: baseline, 6 months, 2 years
Fibroid oper vs fibroid nonoper: baseline, 2 years
Prolapse oper vs prolapse nonoper: 6 months, 2 years
Non-oper: Non-operative treatment; Oper: Operative treatment; SD: Standard deviation.
The percentage of patients who had a clinically important improvement (≥0.015) in the 15D score was largest in endometriosis patients at the long-term follow-up (65.2%) and in endometriosis and prolapse patients at the short-term follow-up (56.5 and 57.1%, respectively). Only 33.0% of patients suffering from bleeding disorders and 37.5% of those with pelvic pain received clinically important symptom alleviation by 6 months. HRQoL improvement remained poor for pelvic pain patients even at the 2-year follow-up, as only 33.3% of patients showed a clinically important improvement. Some of the bleeding disorder patients, however, benefited from treatment later on as by the long-term follow-up 43.6% of patients had clinically important improvement in HRQoL, more in line with the other diagnosis groups (Table 2).
| Patient groups | Change in HRQoL from baseline to 6 months | Change in HRQoL from baseline to 2 years | ||
|---|---|---|---|---|
| HRQoL improved | HRQoL deteriorated | HRQoL improved | HRQoL deteriorated | |
| All | 41.5 | 26.4 | 46.3 | 28.0 |
| Bleeding disorder | 33.0 | 31.9 | 43.6 | 27.7 |
| Fibroid | 44.3 | 21.5 | 54.4 | 25.3 |
| Polyp | 48.5 | 20.6 | 44.1 | 27.9 |
| Pelvic pain | 37.5 | 33.3 | 33.3 | 37.5 |
| Endometriosis | 56.5 | 21.7 | 65.2 | 17.4 |
| Prolapse | 57.1 | 42.9 | 42.9 | 42.9 |
| Other | 25.0 | 31.2 | 25.0 | 37.5 |
| University hospitals | 42.1 | 29.2 | 43.3 | 32.6 |
| Community hospitals | 40.6 | 22.6 | 50.4 | 21.8 |
HRQoL: Health-related quality of life.
Prolapse patients seemed to benefit from operative treatment as the percentage of patients with improved HRQoL at the 6-month follow-up was higher in those treated operatively than in those treated conservatively (p ≤ 0.0005). Also the mean HRQoL scores at the 6-month and 2-year follow-ups were higher in operatively treated patients. Also patients with uterine fibroids reported significantly higher mean 2-year HRQoL scores in the patient group treated surgically.
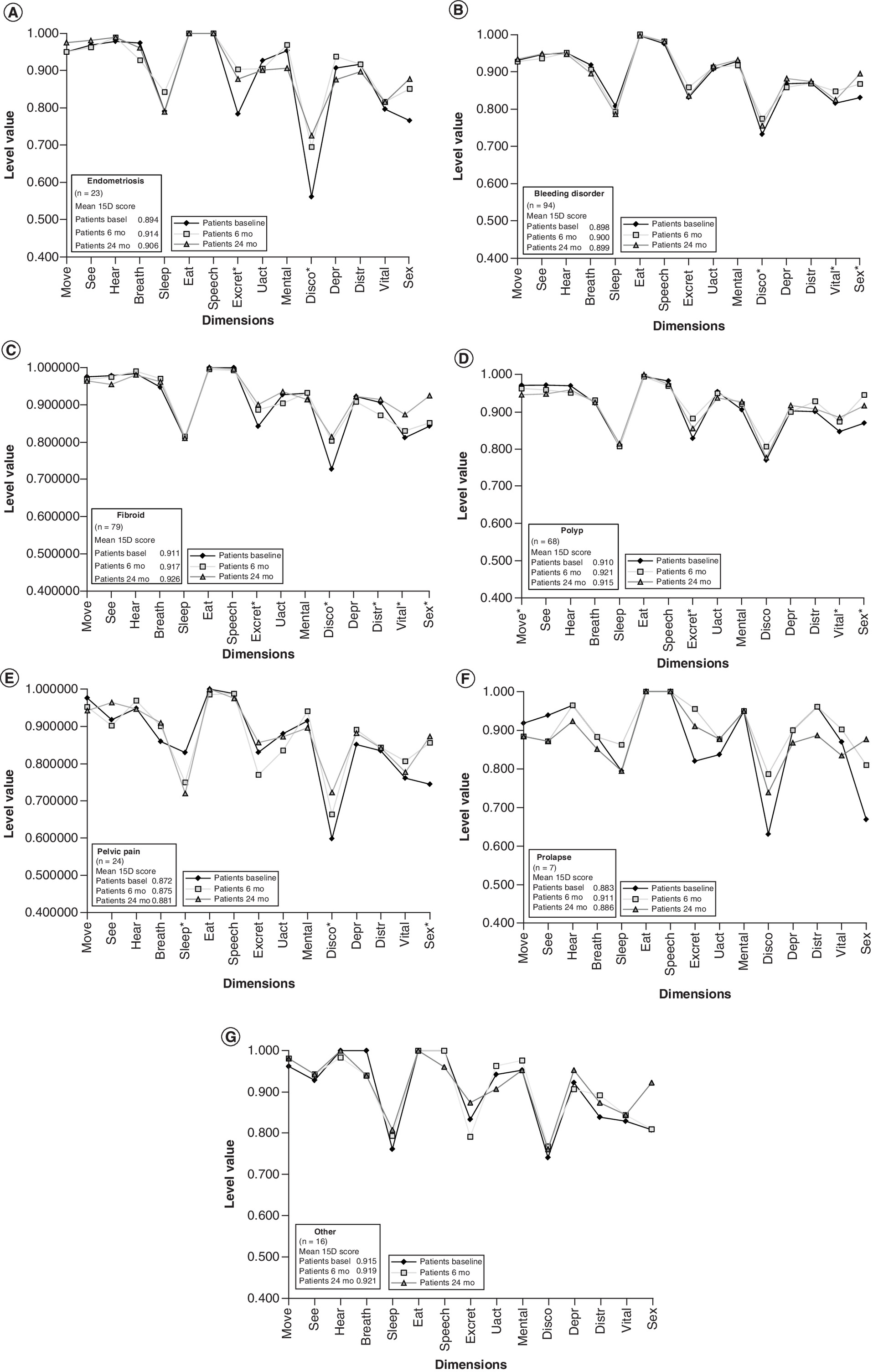
The only statistically significant and clinically important change in the mean HRQoL score in the different diagnosis groups during the whole follow-up was seen in fibroid patients as their score improved from the baseline 0.911 to 0.926 at 2 years (p < 0.05). Treatment had a significant impact most often on the sexual activity of the study patients. Also the dimensions of discomfort and symptoms, excretion and vitality improved statistically significantly (p < 0.05) in more than one of the diagnosis groups (Table 3). When comparing the different dimensions along the follow-up between the different disorder groups it was noted that as a whole, patients with pelvic pain or bleeding disorders seemed to have more HRQoL concerns than patients with polyps or fibroids (Figure 3).
| From baseline to 6 months | From baseline to 2 years | From 6 months to 2 years | |||
|---|---|---|---|---|---|
| Improvement | Deterioration | Improvement | Deterioration | Improvement deterioration | |
| All | Discomfort and symptoms | – | Discomfort and symptoms | – | Sexual activity |
| Excretion | Excretion | ||||
| Vitality | Vitality | ||||
| Sexual activity | Sexual activity | ||||
| Bleeding disorder | Discomfort and symptoms | – | Sexual activity | – | – |
| Vitality | |||||
| Uterine fibroid | Discomfort and symptoms | – | Discomfort and symptoms | – | Discomfort and symptoms |
| Excretion | Vitality | ||||
| Vitality | Sexual activity | ||||
| Sexual activity | |||||
| Polyp | Excretion | – | Vitality | Mobility | – |
| Sexual activity | Sexual activity | ||||
| Pelvic pain | Sexual activity | – | Discomfort and symptoms | Sleep | – |
| Sexual activity | |||||
| Endometriosis | Discomfort and symptoms | – | Discomfort and symptoms | – | – |
| Excretion | Excretion | ||||
| Prolapse | – | – | – | – | – |
| Other | – | – | – | – | – |
There were no statistically significant differences on either follow-up point and in any of the diagnosis groups in the mean 15D scores between patients treated in university hospitals and those treated in community hospitals. A total of 42.1 and 43.3% of patients treated in a university hospital, and 40.6 and 50.4% of patients treated in community hospitals showed a clinically important improvement (≥0.015) in the mean 15D score at the 6-month and 2-year follow-ups, respectively.
As only 57.3% of the 542 women, who answered the baseline questionnaire in the end, met the inclusion criteria concerning diagnosis and answered all of the follow-up questionnaires, we analyzed the HRQoL results of those lost-to-follow-ups as well. One could suppose that patients with more distress caused by the condition at hand would more eagerly answer study questionnaires. However, when comparing the baseline mean HRQoL score of the patients, who did not answer the follow-up questionnaires to those who did, it turned out that the mean baseline 15D score was higher in those who continued to participate in the study (0.901 [SD ± 0.084] vs 0.872 [SD ± 0.123], p < 0.001). It remains out of reach of this study to determine whether the HRQoL of these patients improved so well due to treatment that they did not feel inclined to answer the follow-up questionnaires, or whether these patients were already so tired of their symptoms that answering the study questionnaires did not seem relevant.
Discussion
Even though the impact of benign gynecological conditions on the HRQoL of women is significant, relatively little has been published on HRQoL results of typical treatment protocols in an every-day clinical environment [1,3]. As a whole, our study revealed that the present clinical practice of treatment of benign uterine disorders yields mostly rather good HRQoL results. However, HRQoL remains inferior compared with the general female population and the degree of improvement after treatment varies from one condition to another.
As nearly 80% of women suffering from a benign gynecological disorder see a doctor annually [4] and up to two-thirds of patients may report moderate to severe impact on QoL [7], the HRQoL results in our study were surprisingly good already at baseline. However, the significance of these seemingly minor common disorders is evident also in our study as HRQoL of the women suffering from them does not reach the level of that of the general female population even after treatment. A wide spectrum of HRQoL dimensions is impaired but it is noteworthy that treatment allows women to regain sexual activity over time.
It has been reported previously that the impaired physical, sexual and also mental well-being in women with a benign gynecological condition improves after treatment [1,5–7,18–21]. Our study showed that the benefits of treatment appear fairly rapidly and were evident already at the short-term follow-up in the whole study group and in most of the specific diagnosis groups. The benefits were also relatively well sustained throughout the long-term follow-up. The physical QoL (dimensions of excretion, discomfort and symptoms, andvitality) and the mean 15D score improved statistically significantly from the baseline to the 6-month follow-up and remained at the improved level also at the 2-year follow-up. Sexual activity kept improving significantly throughout the study period, even from the 6-month follow-up to the 2-year follow-up.
Only a third of the bleeding disorder patients reported improved HRQoL during 6 months after treatment initiation. However, some of these patients benefited from treatment later on, as by the 2-year follow-up 43.6% of patients had improved HRQoL compared with baseline, quite well in line with the other diagnosis groups. The mean total HRQoL score did not improve and patients with bleeding disorders had more concerns in the different areas of QoL when compared with several other diagnosis groups. Thus, it seems that bleeding disorders affect the QoL of women suffering from them and treatment is not always easy. Hysterectomy has traditionally been thought to be the most effective treatment strategy of heavy menstrual bleeding [22–27]. However, literature has more recently also shown HRQoL results to be similar after less invasive treatments such as endometrial ablation and levonorgestrel-releasing intrauterine system (IUS) [23–27]. Furthermore, the IUS has been found to be the most cost-effective treatment [28,29] even though nearly 50% of patients initially treated with IUS may need to undergo hysterectomy later on [28]. Our study showed no difference in total HRQoL independent of whether bleeding disorder patients were treated conservatively or operatively. However, the 6-month results were not encouraging which could be due to conservative treatment failing in some patients. A larger proportion of patients had received symptom alleviation by the 2-year follow-up. In order to improve HRQoL of patients with bleeding disorders, a possibility for a second assessment of symptoms after 6 months of primary treatment should be maintained to be able to intervene if burdensome symptoms persist.
Like the systematic review of Jones et al., our study also found dysmenorrhea and pelvic pain patients to have impaired HRQoL. However, opposed to findings of the systematic review, virtually no improvement was seen in the HRQoL of our study patients during the 6-month or the 2-year follow-up [1]. Thus, our study suggests that the treatment conventions of pelvic pain and dysmenorrhea patients should be re-evaluated as healthcare resources are used for very little HRQoL benefit.
The QoL of endometriosis patients has been reported to affect all areas of QoL [30]. However, in our patient material, endometriosis patients were not significantly worse off at baseline than the other patient groups, but the patients with diagnosed endometriosis stood out from the other diagnostic groups with the biggest proportion of patients benefiting from treatment. Compared with treatment of other benign indications, hysterectomy has been found to be especially cost-effective in the treatment of endometriosis [2]. However, as a primary treatment of endometriosis drug treatment has been reported to be more cost-effective than surgery [31,32]. Even though laparoscopic excision of endometriosis has been shown to improve all domains (pain, control and powerlessness, emotional well-being, social support, and self-image) of QoL [33], our study patients with endometriosis had similar mean 15D scores irrespective of whether surgery or conservative treatment was used. This could, however, also be an indication of successful selection of the treatment modality for the patients at hand.
Treatment in the operation theatre is associated with high healthcare resource use and often places the patient under a higher complication risk. Thus, decisions for surgical treatment should always be justifiable. A study setting of comparison of the subjective patient outcome between operative and conservative treatment of a certain gynecological condition is rare. In our study, patients with uterine fibroids and prolapses benefited from operative treatment with better HRQoL results after surgery than after conservative treatment. Patients treated for polyps with an operational hysteroscopic polypectomy or in an outpatient setting did not differ regarding HRQoL results suggesting that outpatient hysteroscopic polypectomy should be preferred, as resource use in an outpatient setting tends to be smaller. Similar results concerning polypectomy have been reported earlier but the accessibility of outpatient polypectomies has been thought to be a restricting factor [34,35].
Strengths & limitations
HRQoL data of the variety of common benign gynecological disorders in usual clinical practice in a real-life setting are rare. The aim of this study was to produce such data on the HRQoL and treatment results of the whole entity of gynecological patients treated in a typical public outpatient clinic. A consequence was a fairly heterogeneous patient material with many different conditions. Yet, the patient material of a typical gynecological outpatient clinic is broad and the precise aim of the study was to reflect the actual real-life situation of gynecological patients. This heterogeneity of the patient material can be regarded as strength of the study but at the same time also as a limitation as some of the diagnosis groups were rather small. In a real-life setting some overlapping of diagnoses may always exist. Therefore, the HRQoL may have been reported by some women while suffering from two separate medical conditions simultaneously. In this study they have, however, been grouped to only one group according to their primary diagnoses. Even though this might disturb the HRQoL comparisons between groups, the authors find this to be acceptable when gaining knowledge from a real-life setting. The authors consider this is strength of the study. Even though the study cohort is from a few years back, the patient material in outpatient gynecological clinics has remained the same and treatment protocols have not changed since the IUS gained ground before the study time period. Millions of women worldwide suffer from these common gynecological conditions. Thus our study setting and cohort is valid and still timely.
Conclusion
As a whole, the HRQoL of patients with benign gynecological disorders is good but still inferior to that of the general female population. The treatment improved especially the patients’ excretion functions, decreased discomfort and symptoms, and enhanced vitality and sexual activity. However, of these dimensions only sexual activity did not deviate statistically significantly from that in the general population at 2 years. Treatment of endometriosis, fibroids and polyps resulted in best HRQoL scores but the treatment protocols of unspecific pelvic pain and bleeding disorders need further evaluation. No differences in the HRQoL results were seen between smaller community hospitals and university hospitals.
Future perspective
Millions of women worldwide suffer from common gynecological conditions. These conditions have a marked effect on the HRQoL of the women affected by them. Thus, the impact of these seemingly minor disorders, without clear objective parameters to follow in healthcare, is vast on our population. In healthcare, more weight has generally started to be placed on subjective patient reported outcomes. In the future, especially in the field of common benign gynecological disorders, it is important to evaluate the outcome of treatment, the need for further treatment and the appropriate allocation of healthcare funds according to patient reported outcomes. Based on the research trend of recent years, we suspect that clinical practice could very well be evolving toward this direction in the upcoming years.
•
Health-related quality of life (HRQoL) data on the variety of common benign gynecological disorders in real-life clinical practice are rare.
•
The impact of benign gynecological conditions on the HRQoL of women is significant.
•
The impaired HRQoL of women with gynecological disorders is improved by treatment but still remains poorer than in the age-standardized general female population.
•
Treatment especially improved the patients’ excretion functions, decreased discomfort and symptoms, and enhanced vitality and sexual activity.
•
Treatment of endometriosis, fibroids and polyps resulted in best HRQoL scores, but the treatment conventions of unspecific pelvic pain and bleeding disorders need further evaluation.
Author contributions
All the authors participated in planning the study. K Pynnä gathered the data. K Pynnä and H Sintonen were responsible for data analysis and K Pynnä for most of the interpretation of the data and for drafting the manuscript. P Räsänen, H Sintonen, RP Roine and P Vuorela acted as senior authors and consultants throughout the writing process and were responsible for revising the manuscript. All authors have approved the final version to be published.
Acknowledgments
R Kekkonen and R Hurskainen are thanked for helping to plan the study. Clinicians K Palva, H Hieta-Heikurainen, A Vallasto, P Härkki, M Pöyhönen-Alho, P Lehtovirta, O Kilpiö and J Tapper are gratefully acknowledged for enabling the study execution in the different hospitals. H Sarpila is warmly thanked for help in filing patient data.
Financial & competing interests disclosure
H Sintonen is the developer of the 15D and receives royalties from its electronic versions. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The study protocol was approved by the Ethics Committee of the Helsinki University Central Hospital (registration number 538/E0/02) and, thus, the study was performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed written consent was obtained from all individual study participants. This included consent to include material pertaining to themselves, an acknowledgement that patients cannot be identified via the paper and that full anonymization was performed.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. Individual, de-identified participant data that underlie the results reported in this article (text, tables, figures and appendices) are available from the corresponding author following publication if needed.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Jones GL, Kennedy SH, Jenkinson C. Health-related quality of life measurement in women with common benign gynecologic conditions: a systematic review. Am. J. Obstet. Gynecol. 187(2), 501–511 (2002).
•• A systematic review on the health-related quality of life (HRQoL) of women with common gynecological conditions.
2.
Taipale K, Leminen A, Räsänen P et al. Costs and health-related quality of life effects of hysterectomy in patients with benign uterine disorders. Acta Obstet. Gynecol. Scand. 88(12), 1402–1410 (2009).
•• Analysis of the effect of operative treatment on the HRQoL of patients with common gynecological disorders in a real-world setting.
3.
Pynnä K, Vuorela P, Lodenius L, Paavonen J, Roine RP, Räsänen P. Cost–effectiveness of hysterectomy for benign gynecological conditions: a systematic review. Acta Obstet. Gynecol. Scand. 93(3), 225–232 (2013).
4.
Kjerulff KH, Erickson BA, Langenberg PW. Chronic gynecological conditions reported by US women: findings from the National Health Interview Survey, 1984 to 1992. Am. J. Public Health 86(2), 195–199 (1996).
5.
Liu Z, Doan QV, Blumenthal P, Dubois RW. A systematic review evaluating health-related quality of life, work impairment and health-care costs and utilization in abnormal uterine bleeding. Value Health 10(3), 183–194 (2007).
• A systematic review on the burden of the common gynecological disorder of abnormal bleeding.
6.
Jia SZ, Leng JH, Shi JH, Sun PR, Lang JH. Health-related quality of life in women with endometriosis: a systematic review. J. Ovarian Res. 5(1), 29 (2012).
•• A systematic review on the HRQoL of women with endometriosis.
7.
Hervé F, Katty A, Isabelle Q, Céline S. Impact of uterine fibroids on quality of life: a national cross-sectional survey. Eur. J. Obstet. Gynecol. Reprod. Biol. 229, 32–37 (2018).
• A national cross-sectional survey on the impact of uterine fibroids on HRQoL.
8.
Whitaker L, Critchley HO. Abnormal uterine bleeding. Best Pract. Res. Clin. Obstet. Gynaecol. 34, 54–65 (2016).
9.
Matteson KA, Rahn DD, Wheeler TL et al. Nonsurgical management of heavy menstrual bleeding: a systematic review. Obstet. Gynecol. 121(3), 632–643 (2013).
10.
Mattsson NK, Karjalainen PK, Tolppanen AM et al. Pelvic organ prolapse surgery and quality of life-a nationwide cohort study. Am. J. Obstet. Gynecol. 222(6), 588.e1–588.e10 (2020).
11.
Doaee M, Moradi-Lakeh M, Nourmohammadi A, Razavi-Ratki SK, Nojomi M. Management of pelvic organ prolapse and quality of life: a systematic review and meta-analysis. Int. Urogynecol. J. 25(2), 153–163 (2014).
12.
Mäkelä-Kaikkonen J, Rautio T, Ohinmaa A et al. Cost-analysis and quality of life after laparoscopic and robotic ventral mesh rectopexy for posterior compartment prolapse: a randomized trial. Tech. Coloproctol. 23(5), 461–470 (2019).
13.
Deshpande PR, Rajan S, Sudeepthi BL, Abdul Nazir CP. Patient-reported outcomes: a new era in clinical research. Perspect. Clin. Res. 2(4), 137–144 (2011).
14.
National Institute for Health and Welfare (THL). Health, Functional Capacity and Welfare in Finland in 2011. Koskinen S, Lundqvist A, Ristoluoma N (Eds). Helsinki, Finland (2012).
15.
Sintonen H. The 15D instrument of health-related quality of life: properties and applications. Ann. Med. 33, 328–336 (2001).
16.
The 15D health-related quality of life (HRQoL) instrument home page. http://www.15d-instrument.net/15D
17.
Alanne S, Roine RP, Räsänen P, Vainiola T, Sintonen H. Estimating the minimum important change in the 15D scores. Qual. Life Res. 24(3), 599–606 (2015).
18.
Gallagher JS, DiVasta AD, Vitonis AF, Sarda V, Laufer MR, Missmer SA. The impact of endometriosis on quality of life in adolescents. J. Adolesc. Health 63(6), 766–772 (2018).
19.
Fritzer N, Hudelist G. Love is a pain? Quality of sex life after surgical resection of endometriosis: a review. Eur. J. Obstet. Gynecol. Reprod. Biol. 209, 72–76 (2017).
20.
Setälä M, Härkki P, Matomäki J, Mäkinen J, Kössi J. Sexual functioning, quality of life and pelvic pain 12 months after endometriosis surgery including vaginal resection. Acta Obstet. Gynecol. Scand. 91, 692–698 (2012).
• A 1 year follow-up of the HRQoL of operatively treated endometriosis patients.
21.
Cozza G, Pinto A, Giovanale V et al. Comparative effectiveness and impact on health-related quality of life of hysterectomy vs. levonorgestrel intra-uterine system for abnormal uterine bleeding. Eur. Rev. Med. Pharmacol. Sci. 21(9), 2255–2260 (2017).
22.
Sculpher M. A cost-utility analysis of abdominal hysterectomy versus transcervical endometrial resection for the surgical treatment of menorrhagia. Int. J. Technol. Assess. Health Care 14(2), 302–319 (1998).
23.
Bhattacharya S, Middleton LJ, Tsourapas A et al. Hysterectomy, endometrial ablation and Mirena (REGISTERED) for heavy menstrual bleeding: a systematic review of clinical effectiveness and cost–effectiveness analysis. Health Technol. Assess. 15(19), iii–xvi 1–252 (2011).
24.
Garside R, Stein K, Wyatt K, Round A, Price A. The effectiveness and cost–effectiveness of microwave and thermal balloon endometrial ablation for heavy menstrual bleeding: a systematic review and economic modelling. Health Technol. Assess. 8(3), iii, 1–155 (2004).
25.
Roberts TE, Tsourapas A, Middleton LJ et al. Hysterectomy, endometrial ablation, and levonorgestrel releasing intrauterine system (Mirena) for treatment of heavy menstrual bleeding: cost–effectiveness analysis. BMJ 342, d2202 (2011).
26.
You JH, Sahota DS, MoYuen P. A cost-utility analysis of hysterectomy, endometrial resection and ablation and medical therapy for menorrhagia. Hum. Reprod. 21(7), 1878–1883 (2006).
27.
Clegg JP, Guest JF, Hurskainen R. Cost-utility of levonorgestrel intrauterine system compared with hysterectomy and second generation endometrial ablative techniques in managing patients with menorrhagia in the UK. Curr. Med. Res. Opin. 23(7), 1637–1648 (2007).
28.
Heliovaara-Peippo S, Hurskainen R, Teperi J et al. Quality of life and costs of levonorgestrel-releasing intrauterine system or hysterectomy in the treatment of menorrhagia: a 10-year randomized controlled trial. Am. J. Obstet. Gynecol. 209(6), 535.e1–535.e14 (2013).
29.
Ganz ML, Shah D, Gidwani R et al. The cost–effectiveness of the levonorgestrel-releasing intrauterine system for the treatment of idiopathic heavy menstrual bleeding in the United States. Value Health 16(2), 325–333 (2013).
30.
Marinho MCP, Magalhaes TF, Fernandes LFC, Augusto KL, Brilhante AVM, Bezerra LRPS. Quality of life in women with endometriosis: an integrative review. J. Womens Health 27(3), 399–408 (2018).
31.
Winkel CA. A cost-effective approach to the management of endometriosis. Curr. Opin. Obstet. Gynecol. 12(4), 317–320 (2000).
32.
Schroder AK, Diedrich K, Ludwig M. Medical management of endometriosis: a systematic review. IDrugs 7(5), 451–463 (2004).
33.
Rindos NB, Fulcher IR, Donnellan NM. Pain and quality of life after laparoscopic excision of endometriosis. J. Minim. Invasive Gynecol. 27(7), 1610–1617 (2020).
34.
Cooper NA, Middleton L, Smith P et al. OPT trial collaborative group. A patient-preference cohort study of office versus inpatient uterine polyp treatment for abnormal uterine bleeding. Gynecol. Surg. 13(4), 313–322 (2016).
35.
Clark TJ, Middleton LJ, Cooper NA et al. A randomised controlled trial of outpatient versus inpatient polyp treatment (OPT) for abnormal uterine bleeding. Health Technol. Assess. 19(61), 1–194 (2015).
Information & Authors
Information
Published In
Pages: 685 - 695
PubMed: 33880938
Copyright
© 2021 Future Medicine Ltd.
History
Received: 6 November 2020
Accepted: 26 March 2021
Published online: 21 April 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The health-related quality of life of patients with a benign gynecological condition: a 2-year follow-up. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0243
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Runguo Wu, Kirsten D. Arendse, Tooba Hamdani, Fiona M. Walter, Emma J. Crosbie, Borislava Mihaylova, Garth Funston, Cost-effectiveness of CA125- and age-informed risk-based triage for ovarian cancer detection in primary care, British Journal of Cancer, 10.1038/s41416-025-03166-3, 133, 10, (1492-1500), (2025).
- Saara Vuontisjärvi, Henna-Riikka Rossi, Tanja Nordström, Salla Karjula, Anna Terho, Laure Morin-Papunen, Sari Koivurova, Terhi T Piltonen, Women with endometriosis have decreased health-related quality of life until late fertile age: a population-based cohort analysis at ages 31 and 46 years, Human Reproduction, 10.1093/humrep/deaf154, 40, 10, (1909-1918), (2025).
- Ulla‐Maija Haltia, Saku Torvinen, Saara Bryk, Harri Sintonen, Johanna Tapper, Health‐related quality of life in adult‐type ovarian granulosa cell tumor survivors, Acta Obstetricia et Gynecologica Scandinavica, 10.1111/aogs.15144, 104, 7, (1382-1389), (2025).
- Marta Włodarczyk, Michał Ciebiera, Grażyna Nowicka, Tomasz Łoziński, Mohamed Ali, Ayman Al-Hendy, Epigallocatechin Gallate for the Treatment of Benign and Malignant Gynecological Diseases—Focus on Epigenetic Mechanisms, Nutrients, 10.3390/nu16040559, 16, 4, (559), (2024).
- Marion Pinsard, Nicolas Mouchet, Ludivine Dion, Thomas Bessede, Martin Bertrand, Emile Darai, Pascale Bellaud, Philippe Loget, Séverine Mazaud-Guittot, Xavier Morandi, Jean Leveque, Vincent Lavoué, Martha Duraes, Krystel Nyangoh Timoh, Anatomic and functional mapping of human uterine innervation, Fertility and Sterility, 10.1016/j.fertnstert.2022.02.013, 117, 6, (1279-1288), (2022).
- Salvatore Giovanni Vitale, Rafał Watrowski, Fabio Barra, Maurizio Nicola D’Alterio, Jose Carugno, Thozhukat Sathyapalan, Ilker Kahramanoglu, Enrique Reyes-Muñoz, Li-Te Lin, Bulent Urman, Simone Ferrero, Stefano Angioni, Abnormal Uterine Bleeding in Perimenopausal Women: The Role of Hysteroscopy and Its Impact on Quality of Life and Sexuality, Diagnostics, 10.3390/diagnostics12051176, 12, 5, (1176), (2022).