Patient-related barriers to some virtual healthcare services among cancer patients in the USA: a population-based study
Publication: Journal of Comparative Effectiveness Research
Abstract
Objective: To assess the patient-related barriers to access of some virtual healthcare tools among cancer patients in the USA in a population-based cohort. Materials & methods: National Health Interview Survey datasets (2011–2018) were reviewed and adult participants (≥18 years old) with a history of cancer diagnosis and complete information about virtual healthcare utilization (defined by [a] filling a prescription on the internet in the past 12 months and/or [b] communicating with a healthcare provider through email in the past 12 months) were included. Information about video-conferenced phone calls and telephone calls are not available in the National Health Interview Survey datasets; and thus, they were not examined in this study. Multivariable logistic regression analysis was used to evaluate factors associated with the utilization of virtual care tools. Results: A total of 25,121 participants were included in the current analysis; including 4499 participants (17.9%) who utilized virtual care in the past 12 months and 20,622 participants (82.1%) who did not utilize virtual care in the past 12 months. The following factors were associated with less utilization of virtual healthcare tools in multivariable logistic regression: older age (continuous odds ratio [OR] with increasing age: 0.987; 95% CI: 0.984–0.990), African-American race (OR for African American vs white race: 0.608; 95% CI: 0.517–0.715), unmarried status (OR for unmarried compared with married status: 0.689; 95% CI: 0.642–0.739), lower level of education (OR for education ≤high school vs >high school: 0.284; 95% CI: 0.259–0.311), weaker English proficiency (OR for no proficiency vs very good proficiency: 0.224; 95% CI: 0.091–0.552) and lower yearly earnings (OR for earnings <$45,000 vs earnings >$45,000: 0.582; 95% CI: 0.523–0.647). Conclusion: Older patients, those with African-American race, lower education, lower earnings and weak English proficiency are less likely to access the above studied virtual healthcare tools. Further efforts are needed to tackle disparities in telemedicine access.
The traditional model of cancer care would indicate that patients need to visit cancer hospitals quite frequently to meet their treating team and to receive cancer treatments (like chemotherapy and radiation therapy) [1,2]. In the current peri-COVID-19 pandemic era, lots of discussions are ongoing within the oncology community regarding how to ensure continuity of care of cancer patients without jeopardizing their safety [3,4]. Cancer patients were found to have an, unfortunately, higher risk of severe COVID-19 infection and physical distancing has been recommended as the public health strategy of choice to minimize infection risk (particularly for high risk and vulnerable groups of the society) [5,6]. Virtual care has emerged as a possible solution to ensure continuity of care while mitigating infection risks as much as possible and many cancer centers around the world are currently implementing it [7–9]. Virtual care is a broad term that encompasses all the ways through which healthcare providers remotely interact with their patients. Simply put, the term virtual care is a way of talking about how patients and doctors can use digital tools to communicate in real-time [10,11]. Examples might include video-conferenced phone calls, telephone calls, email communications and online filling of prescriptions [12]. However, it is not well-known if access to virtual healthcare tools would be feasible for every cancer patient in North America or if some patient-related barriers would impair the delivery of this type of care certain subgroups of patients.
National Health Interview Survey (NHIS) is an annual survey that screens different aspects of healthcare delivery among the US population. It should thus provide an optimal tool to examine the current trends and possible patient-related barriers to the administration of select modes of virtual healthcare that are covered within this survey. The results of this analysis would be important for patients, providers and policymakers to identify potential gaps associated with virtual healthcare delivery that should be addressed while implementing these methods.
Objective
To assess the patient-related barriers to access some virtual healthcare tools among cancer patients in the USA, in a population-based cohort.
Materials & methods
Data sources
The current study is based on annual NHIS datasets (2011–2018) (as these datasets contain consistent information about the end points of interest in the current study). NHIS is one of the largest and most influential resources of healthcare status in the US. These surveys are designed, conducted and collected by the National Center for Health Statistics (part of the CDC). Further information about the history and methodology of NHIS is provided elsewhere [13].
Cohort definition
Adult participants (≥18 years old) with a history of cancer diagnosis and complete information about virtual healthcare access were included. Virtual healthcare access is indicated in the NHIS datasets by these two parameters: filling a prescription on the internet in the past 12 months and/or; communicating with a healthcare provider through email in the past 12 months. There is no other specific description within the NHIS datasets of virtual consults/appointments.
Data collection
The following data were collected from included participants (where available); age at survey completion, gender, race, educational status, yearly earnings (in US $), marital status, working status, self-reported health status, English language proficiency, type of insurance coverage (private, Medicare and/or Medicaid) and primary tumor site. Yearly earnings were reported in the NHIS datasets as a categorical variable (not as a continuous variable). The following healthcare services/interactions were collected as well: filling a prescription on the internet in the past 12 months, communicating with a healthcare provider through email in the past 12 months, looking up health information on the internet in the past 12 months and scheduling an appointment with healthcare providers through the internet in the past 12 months. For the sake of the statistical analysis of the current study, virtual healthcare access will mean only filling a prescription online and/or communicating with a healthcare provider through an email. Information about video-conferenced phone calls and telephone calls are not available in the NHIS datasets; and thus, they were not examined in this study.
Statistical analysis
The main hypothesis of the current study is that access to virtual healthcare is not homogenous among different socioeconomic groups of the cancer patients. In order to address this hypothesis, the following analyses were conducted:
•
Differences in baseline characteristics between individuals who utilized internet-delivered care tools were compared with individuals who did not utilize these tools. Chi-squared testing was used for this comparison.
•
Multivariable logistic regression analysis was then used to evaluate factors associated with the use of internet-delivered care tools (as defined above). This model included the following variables: age at survey completion, gender and race, marital status, working status, yearly earnings, self-reported health status, and English language proficiency. These variables were chosen because of their impact on the socioeconomic status of an individual and hence, their access to care.
Moreover, an additional analysis of the temporal trends in virtual healthcare access among cancer patients was done.
All statistical analyses were conducted through SPSS (version 26.0; IBM, NY, USA).
Results
Participants’ characteristics
A total of 25,121 participants were included in the current analysis; including 4499 participants (17.9%) who utilized virtual care in the past 12 months and 20,622 participants (82.1%) who did not utilize virtual care in the past 12 months. Comparing both groups together, individuals receiving virtual care were more likely to be younger (p < 0.001), males (p = 0.032), white (p < 0.001), married (p < 0.001), working (p < 0.001), better educated (p < 0.001), English-proficient (p < 0.001), with better self-reported health (p < 0.001) and having private health insurance (p < 0.001), but less likely to be enrolled in Medicare or Medicaid programs (p < 0.001 for each; Table 1).
| Parameter | Virtual care (4499 participants) | No virtual care (20,622 participants) | p-value |
|---|---|---|---|
| Age (mean; SD) | 61.57; 12.74 | 65.67; 13.87 | <0.001 |
| Gender – Male – Female | 1905 (42.3%) 2594 (57.7%) | 8374 (40.6%) 12,248 (59.4%) | 0.032 |
| Race – White – African-American – Asian – American-Indian – Others | 4110 (91.4%) 185 (4%) 102 (2.3%) 14 (0.3%) 88 (2%) | 17,901 (86.8%) 1783 (8.6%) 448 (2.2%) 130 (0.6%) 360 (1.8%) | <0.001 |
| Marital status – Married – Unmarried – Unknown | 2595 (57.7%) 1899 (42.2%) 5 (0.1%) | 9092 (44.1%) 11,497 (55.8%) 33 (0.1%) | <0.001 |
| Work – Working – Not working – Unknown | 2110 (46.9%) 2389 (53.1%) 0 | 6046 (29.3%) 14,567 (70.6%) 9 (<0.01%) | <0.001 |
| Education – ≤High school – >High school – Unknown | 669 (14.9%) 3825 (85%) 5 (0.1%) | 9113 (44.2%) 11,424 (55.4%) 85 (0.4%) | <0.001 |
| English proficiency – Very well – Well – Not well – Not at all – Unknown | 3623 (80.5%) 85 (1.9%) 17 (0.5%) 5 (0.1%) 769 (17.1%) | 14,306 (69.4%) 735 (3.6%) 295 (1.4%) 175 (0.8%) 5111 (24.8%) | <0.001 |
| Health status† – Excellent – Very good – Good – Fair – Poor – Unknown | 786 (17.5%) 1505 (33.5%) 1403 (31.2%) 603 (13.4%) 199 (4.4%) 3 (0.1%) | 2688 (13%) 5470 (26.5%) 6752 (32.7%) 4051 (19.6%) 1646 (8%) 15 (0.1%) | <0.001 |
| Yearly earnings – ≤$45,000 – >$45,000 – Unknown | 924 (20.5%) 1201 (26.7%) 2374 (52.8%) | 3790 (18.4%) 2191 (10.6%) 14,641 (71%) | <0.001 |
| Insurance coverage‡ – Private – Medicare – Medicaid | 3214 (71.4%) 2213 (49.2%) 185 (4.1%) | 11,620 (56.3%) 13,369 (64.8%) 2340 (11.3%) | <0.001 <0.001 <0.001 |
†
Self-reported.
‡
Some patients might have more than one form of insurance coverage.
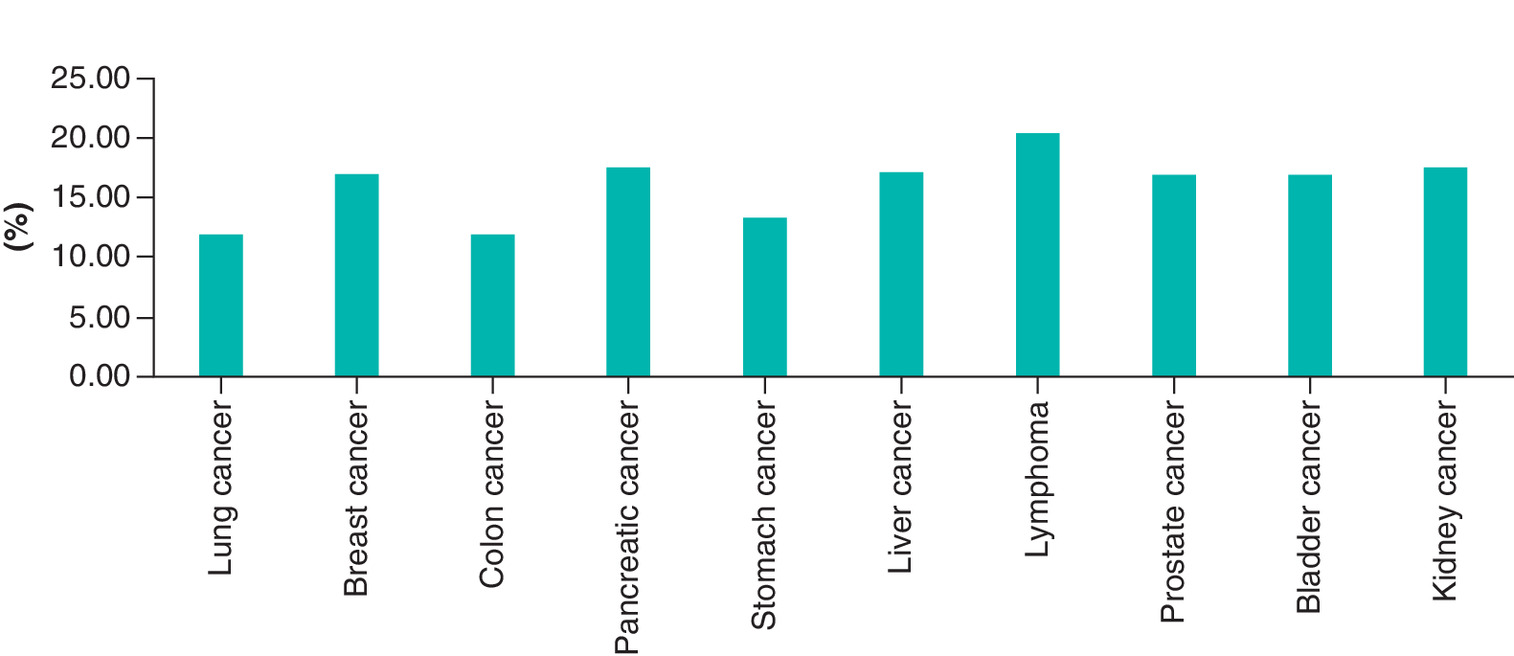
Figure 1 provides a detailed analysis of the use of internet-delivered care tools among individuals with the most common primary cancers in the USA (lung, breast, colon, stomach, pancreas, liver, lymphoma, prostate and bladder and kidney cancers). The highest reported uptake was for individuals with history of lymphoma (20.4%); while the lowest reported uptake was for individuals with lung cancer and colon cancer (11.9% each).
Patient-related factors associated with virtual healthcare access
Through multivariable logistic regression analysis, the following factors were associated with less utilization of virtual healthcare tools (filling a prescription online and/or communicating with an individual through an email): older age (continuous OR with increasing age: 0.987; 95% CI: 0.984–0.990), African American race (OR for African American race vs white race: 0.608; 95% CI: 0.517–0.715), unmarried status (OR for unmarried compared with married status: 0.689; 95% CI: 0.642–0.739), lower level of education (OR for education ≤high school vs >high school: 0.284; 95% CI: 0.259–0.311), weaker English proficiency (OR for no proficiency vs very good proficiency: 0.224; 95% CI: 0.091–0.552) and lower yearly earnings (OR for earnings <$45,000 vs earnings >$45,000: 0.582; 95% CI: 0.523–0.647; Table 2).
| Parameter | OR (95% CI) | p-value |
|---|---|---|
| Age (mean; SD) | 0.987 (0.984–0.990) | <0.001 |
| Gender – Male – Female | Reference 1.006 (0.937–1.081) | 0.861 |
| Race – White – African American – Asian – American Indian – Others | Reference 0.608 (0.517–0.715) 1.069 (0.845–1.352) 0.493 (0.279–0.871) 1.108 (0.864–1.420) | <0.001 0.578 0.015 0.418 |
| Marital status† – Married – Unmarried | Reference 0.689 (0.642–0.739) | <0.001 |
| Work† – Working – Not working | Reference 0.983 (0.883–1.094) | 0.754 |
| Education† – >High school – ≤High school | Reference 0.284 (0.259–0.311) | <0.001 |
| English proficiency† – Very well – Well – Not well – Not at all | Reference 0.618 (0.486–786) 0.345 (0.209–0.569) 0.224 (0.091–0.552) | <0.001 <0.001 0.001 |
| Health status† – Excellent – Very good – Good – Fair – Poor | Reference 1.095 (0.987–1.214) 1.058 (0.952–1.175) 0.957 (0.843–1.087) 0.880 (0.735–1.054) | 0.085 0.294 0.502 0.165 |
| Yearly earnings† – >$45,000 – ≤$45,000 | Reference 0.582 (0.523–0.647) | <0.001 |
†
Patients with unknown status were included but not reported in this table.
SD: Standard deviation.
Temporal trends in virtual healthcare access among cancer patients
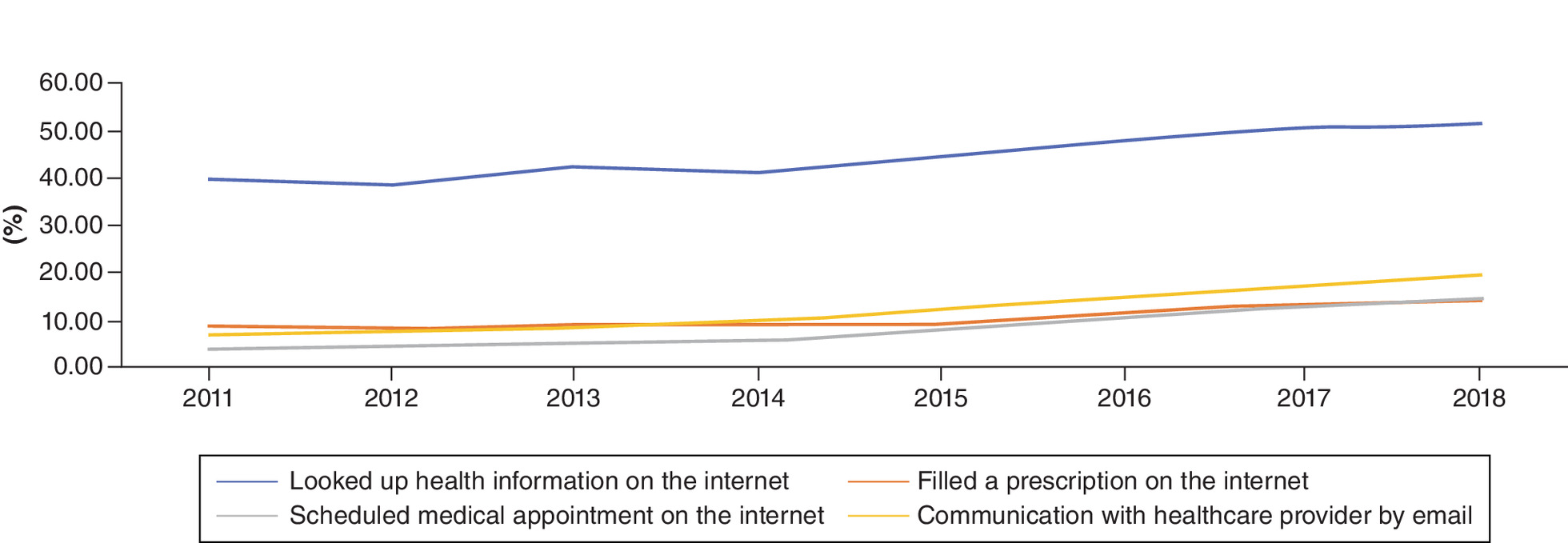
Figure 2 describes the temporal trends (2011–2018) in filling a prescription on the internet, communicating with a healthcare provider through email, looking up health information on the internet and scheduling an appointment with healthcare providers through the internet. There is evidence of increasing uptake of each of these aspects; including looking up health information on the internet (rate in 2018: 51.8% vs rate in 2011: 40%), rate of filling a prescription on the internet was 14.3% in 2018 versus 8.8% in 2011, rate of communicating with healthcare provider through email was 51.8% in 2018 versus 40% in 2011, and rate of scheduling an appointment with healthcare providers over the internet was 19.9% in 2018 versus 6.8% in 2011.
Discussion
The current study evaluates patient-related barriers to access of some virtual healthcare tools among cancer patients in a population-based setting in the USA. It suggested that although the use of virtual care tools has increased in the last decade, certain socioeconomic subgroups are still under-utilizing them. Specifically, older patients, those with African American race, lower education, lower earnings and weak English proficiency are less likely to utilize these tools. Further steps need to be made to increase access to virtual care services to these socioeconomic strata of the society.
The current study has also shown that individuals with private insurance coverage were more likely to utilize these tools; while individuals with Medicare or Medicaid coverage were less likely to utilize these tools. This is consistent with the other findings of the study given that individuals with private insurance are more likely to have higher earnings; while individuals with Medicare coverage are older and individuals with Medicaid coverage have fewer earnings. This observation seems to be more a marker of wealth and age rather than any intrinsic feature of the insurance; thus, we need to be concerned that socioeconomic disparities have a great potential to limit the expansion of virtual care to underserved communities. The noted socioeconomic disparities in the current study add to the growing body of evidence highlighting the role played by socioeconomic variables in determining outcomes and utilization of health services among cancer patients. Previous studies have suggested that cancer patients in the lower socioeconomic strata of the society are more likely to die of cancer as well as die of noncancer reasons (like suicide) [14–16].
The observation that older patients were less likely to utilize virtual care tools is concerning (albeit expected). This could be both fear of technology but also, they are a generation used to the model of coming in physically to see their physicians in person and they might feel that much would be lost with virtual visits. This needs to be studied further.
Cancer is more likely to occur among older individuals and older individuals are also more likely to experience severe COVID-19 infection [17]. Further efforts to create ‘elderly-friendly’ virtual care technology are needed. The current study has also shown the crucial role played by language barriers in affecting the outcomes of cancer patients. While individuals with less English proficiency may be more likely to have weaker financial status and suboptimal insurance coverage (and thus less access to virtual healthcare tools); it is also possible that the language barrier itself works as a deterrent for those individuals with cancer to seek services virtually. Healthcare facilities need to do better to remove these language barriers for those individuals and to increase their awareness of the different options available to them. Licensed translation services should be made available not only for patients attending cancer hospitals in person but also for individuals communicating virtually with healthcare providers [18].
Expanding virtual healthcare tools within cancer hospitals will not only protect vulnerable cancer patients from undue exposure to potential infections in their physical journey to the cancer hospital; but also increase the capacity of cancer hospitals to accept and review more patients and thus shorten waiting lists for cancer treatments and hopefully improve patients’ outcomes [19].
Virtual care delivery to cancer patients is not, however, without its problems. First, the breach of privacy that might be associated with the online transfer of sensitive patient information is a big concern. Healthcare systems working on virtual delivery methods need to pay extra attention to protecting patient privacy, particularly in the age of increasing cyber threats to online information content. Data security and privacy are governed by different data protection acts in different countries [20]. Also, healthcare providers involved in virtual care delivery need to appreciate medico-legal issues that might be associated with the utilization of virtual care tools [21,22]. Second, within oncology practice, clinical in-person assessment is fundamental in the context of dictating possible treatment strategies. Moreover, and from the perspective of patient satisfaction and psychology, the delivery of sensitive cancer-related news virtually is not the optimal method for many patients [23]. A SPIKES model tailored after the new realities of virtual care has been proposed recently [24]. Thus, while virtual delivery of care might be the reasonable thing today in many vignettes, it cannot completely replace in-person doctor-patient relationship in cancer care. Third, the establishment of a successful telemedicine program in cancer care would need significant time and financial investments on the side of the healthcare systems; this might be an issue in the era of soaring healthcare costs and particularly in the context of the struggling world economy post-COVID-19 pandemic.
Taken together, although rates of different aspects of virtual care tools described in the current study have increased throughout the course of the study, they are still below expectations with almost one in ten individuals with cancer who are able to schedule an appointment over the internet or filling a prescription online. This indicates the need for coordinated efforts to improve the experience of cancer patients with internet-delivered medical services.
The current study has several weaknesses and strengths that need to be acknowledged. First, the NHIS data collection strategy is based on self-reporting by participants; thus, some individuals may have missed or mischaracterized their interactions with the healthcare system while answering these survey questions. Second, although NHIS covered important aspects of virtual care (like online communications or prescription filling), other aspects of virtual care might have been overlooked and not covered by NHIS questions. Specifically, although the above-described aspects of care are important, they cannot be equated with actual virtual visits which many oncologists have shifted to in the post-COVID-19 era. These actual virtual visits are not unfortunately addressed within the NHIS datasets. Third, although NHIS provided information about cancer diagnosis and primary tumor site, it did not provide any additional relevant oncological information (e.g., stage of cancer diagnosis, treatment received, etc.). Fourth, NHIS did not provide information about patient satisfaction or preference. Thus, although – from a health system perspective-virtual care might be a safe and effective method of delivering care, we do not know if patients are happier with that method of care. A recent systematic review evaluates patient and caregivers’ satisfaction with telehealth videoconferencing (that was not specific to oncology patients). It found that people living in remote areas are generally satisfied with this modality as it could improve access to healthcare without the associated travel inconvenience [25]. Fifth, this study is based on a US community health survey; whether the results apply to other jurisdictions in Western Europe, Canada or elsewhere in the world is not known. Sixth, this study focused on patient-related factors associated with the use of virtual care tools. It is possible that many provider-related or system-related factors also determine the rate of utilization of virtual care tools; but unfortunately, this cannot be assessed from the NHIS datasets. NHIS data cannot measure if the clinic where the patient was seeking treatment even offered virtual visits. In fact, many US centers in smaller communities delayed or even failed to bring in electronic medical records, and thus, the ability of patients to communicate with the office through the patient portals of the electronic medical records; moreover, many academic centers that potentially had the capabilities to expand virtual care tools did not do so until the COVID-19 pandemic. The above weaknesses need to be weighed against the strengths of the study, notably the large sample size and the contemporaneous nature of the study. Collectively, the results of the current analysis would indicate association rather than causation and further studies are needed to dissect the factors underlying better or worse virtual delivery of care and to improve it.
Conclusion
Although the use of the above-studied virtual care tools has increased in the last decade, certain socioeconomic subgroups are still under-accessing them. Specifically, older patients, those with African American race, lower education, lower earnings and weak English proficiency are less likely to access these tools. Although these results reflect patterns of care in the pre-COVID-19 era, this work may be foundational in morphing these results with post-COVID-19 data and comparing both sets of data together.
•
The traditional model of cancer care would indicate that patients need to visit cancer hospitals quite frequently to meet their treating team and to receive cancer treatments (like chemotherapy and radiation therapy).
•
In the current peri-COVID-19 pandemic era, lots of discussions are ongoing within the oncology community regarding how to ensure continuity of care of cancer patients without jeopardizing their safety.
•
National Health Interview Survey datasets (2011–2018) were reviewed.
•
Adult participants (≥18 years old) with a history of cancer diagnosis and complete information about virtual healthcare utilization (defined by [a] filling a prescription on the internet in the past 12 months and/or [b] communicating with a healthcare provider through email in the past 12 months) were included.
•
Multivariable logistic regression analysis was used to evaluate factors associated with the utilization of virtual care tools.
•
A total of 25,121 participants were included in the current analysis; including 4499 participants (17.9%) who utilized virtual care in the past 12 months and 20,622 participants (82.1%) who did not utilize virtual care in the past 12 months.
•
The following factors were associated with less utilization of virtual healthcare tools in multivariable logistic regression: older age, African American race, Unmarried status, lower level of education, weaker English proficiency and lower yearly earnings.
•
Further efforts are needed to tackle disparities in telemedicine access.
Acknowledgments
This work is based on the National Health Interview Survey annual datasets (2011–2018).
Financial & competing interests disclosure
The author has no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
Because this study was based on publicly available anonymized dataset, ethical approval was not required. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. All included National Health Interview Survey participants have signed informed consent as dictated by Statistics Canada policies.
References
Papers of special note have been highlighted as: • of interest
1.
Bunnell CA, Weingart SN, Swanson S, Mamon HJ, Shulman LN. Models of multidisciplinary cancer care: physician and patient perceptions in a comprehensive cancer center. J. Oncol. Pract. 6(6), 283–288 (2010).
2.
Whear R, Thompson-Coon J, Rogers M et al. Patient-initiated appointment systems for adults with chronic conditions in secondary care. Cochrane Database Syst. Rev. 4, Cd010763 (2020).
3.
Lambertini M, Toss A, Passaro A et al. Cancer care during the spread of coronavirus disease 2019 (COVID-19) in Italy: young oncologists' perspective. ESMO Open 5(2), e000759 (2020).
4.
Shankar A, Saini D, Roy S et al. Cancer care delivery challenges amidst coronavirus disease-19 (COVID-19) outbreak: specific precautions for cancer patients and cancer care providers to prevent spread. Asian Pac. J. Cancer Prev. 21(3), 569–573 (2020).
5.
Liang W, Guan W, Chen R et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol. 21(3), 335–337 (2020).
6.
Bai Y, Yao L, Wei T et al. Presumed asymptomatic carrier transmission of COVID-19. JAMA 323(14), 1406–1407 (2020).
7.
Hollander JE, Carr BG. Virtually perfect? Telemedicine for Covid-19. N. Engl. J. Med. 382(18), 1679–1681 (2020).
• Reviews current telemedicine practices in the context of COVID-19.
8.
Gadzinski AJ, Ellimoottil C, Odisho AY, Watts KL, Gore JL. Implementing telemedicine in response to the 2020 COVID-19 pandemic. J. Urol. 204(1), 14–16 (2020).
9.
Ohannessian R, Duong TA, Odone A. Global telemedicine implementation and integration within health systems to fight the COVID-19 pandemic: a call to action. JMIR Public Health Surveill. 6(2), e18810 (2020).
10.
Karacin C, Bilgetekin I, Basal FB, Oksuzoglu OB. How does COVID-19 fear and anxiety affect chemotherapy adherence in patients with cancer. Future Oncol. 16(29), 2283–2293 (2020).
11.
Royce TJ, Sanoff HK, Rewari A. Telemedicine for cancer care in the time of COVID-19. JAMA Oncol. 16(18), 1225–1227 (2020).
12.
Ownsworth T, Chan RJ, Jones S, Robertson J, Pinkham MB. Use of telehealth platforms for delivering supportive care to adults with primary brain tumors and their family caregivers: a systematic review. Psychooncology (2020) (Epub ahead of print).
13.
National Health Interview Survey (2020). www.cdc.gov/nchs/nhis/about_nhis.htm
14.
Abdel-Rahman O. Socioeconomic predictors of suicide risk among cancer patients in the United States: a population-based study. Cancer Epidemiol. 63, 101601 (2019).
15.
Abdel-Rahman O. Outcomes of non-metastatic colon cancer patients in relationship to socioeconomic status: an analysis of SEER census tract-level socioeconomic database. Int. J. Clin. Oncol. 24(12), 1582–1587 (2019).
16.
Abdel-Rahman O. Impact of NCI socioeconomic index on the outcomes of nonmetastatic breast cancer patients: analysis of SEER census tract-level socioeconomic database. Clin. Breast Cancer 19(6), e717–e722 (2019).
17.
Li Q, Guan X, Wu P et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 382(13), 1199–1207 (2020).
18.
Granhagen Jungner J, Tiselius E, Blomgren K, Lutzen K, Pergert P. Language barriers and the use of professional interpreters: a national multisite cross-sectional survey in pediatric oncology care. Acta Oncol. 58(7), 1015–1020 (2019).
19.
Adler E, Alexis C, Ali Z et al. Bridging the distance in the Caribbean: telemedicine as a means to build capacity for care in paediatric cancer and blood disorders. Stud. Health Technol. Inform. 209, 1–8 (2015).
20.
Brous E. Legal considerations in telehealth and telemedicine. Am. J. Nurs. 116(9), 64–67 (2016).
21.
Becker CD, Dandy K, Gaujean M, Fusaro M, Scurlock C. Legal perspectives on telemedicine part 1: legal and regulatory issues. Perm. J. 23, 18–293 (2019).
22.
Becker CD, Dandy K, Gaujean M, Fusaro M, Scurlock C. Legal perspectives on telemedicine part 2: telemedicine in the intensive care unit and medicolegal risk. Perm. J. 23, 18–294 (2019).
23.
Ngo-Metzger Q. Breaking bad news over the phone. Am. Fam. Physician 80(5), 520 (2009).
24.
Wolf I, Waissengrin B, Pelles S. Breaking bad news via telemedicine: a new challenge at times of an epidemic. Oncologist 25(6), e879–e880 (2020).
25.
Orlando JF, Beard M, Kumar S. Systematic review of patient and caregivers' satisfaction with telehealth videoconferencing as a mode of service delivery in managing patients' health. PLoS ONE 14(8), e0221848 (2019).
Information & Authors
Information
Published In
Pages: 119 - 126
PubMed: 33448874
Copyright
© 2021 Future Medicine Ltd.
History
Received: 27 August 2020
Accepted: 27 October 2020
Published online: 15 January 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Patient-related barriers to some virtual healthcare services among cancer patients in the USA: a population-based study. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0187
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Victor M. Gallegos-Rejas, Jaimon T. Kelly, Ling Zhang, Nicole Marinucci, Karen Payne, Xiaoyun Zhou, Yiran Lu, Anthony C. Smith, Emma E. Thomas, Understanding the telehealth access through an intersectional lens: Experience of Mandarin-speaking consumers accessing health services from a tertiary hospital in Australia, DIGITAL HEALTH, 10.1177/20552076261415915, 12, (2026).
- Ramya Walsan, Reema Harrison, Johanna Westbrook, Ashfaq Chauhan, Michelle Moscova, Anita Vandyke, Elizabeth Manias, Tracey Webster, Natalie Taylor, Prince Peprah, Rebecca Mitchell, Characteristics of Patients Accessing Outpatient Oncology Services Virtually and Predictors of Subsequent Unplanned Emergency Department Presentations: A Retrospective Cohort Study of 78,323 Adults in Australia (Preprint), Journal of Medical Internet Research, 10.2196/87694, (2025).
- Jessica Faiz, Joy Toyama, Anita H. Yuan, Nicholas Jackson, Neil Patel, Lisa Zhao, Anita A. Vashi, Patricia Fermin, Donna L. Washington, Kristina M. Cordasco, Assessing Racial and Ethnic Disparities in Receipt of Tele-Emergency Care, Medical Care, 10.1097/MLR.0000000000002207, 63, 11, (866-874), (2025).
- Kristin L. Rising, Amanda Guth, Alexzandra T. Gentsch, Karla Martin Gonzalez, Richard Hass, Lindsey Shughart, Serena Gelfer, Megan McVane, Brooke Worster, Amy E. Leader, Development and Preliminary Validation of a Screener for Digital Health Readiness, JAMA Network Open, 10.1001/jamanetworkopen.2024.32718, 7, 9, (e2432718), (2024).
- Neal Malik, Kassandra L. Harding, Andres Garcia, The influence of COVID-19 on health seeking behaviors among students attending a minority-serving institution in the U.S, Journal of American College Health, 10.1080/07448481.2024.2334076, 73, 4, (1587-1593), (2024).
- John A. Iasiello, Arvind Rajan, Emmanuel Zervos, Alexander A. Parikh, Rebecca A. Snyder, Racial Differences in Patient-Reported Access to Telehealth: An Important and Unmeasured Social Determinant of Health, JCO Oncology Practice, 10.1200/OP.23.00006, 19, 12, (1215-1223), (2023).
- Omar Abdel-Rahman, Geographic Disparities in Access to Cancer Clinical Trials in Canada, American Journal of Clinical Oncology, 10.1097/COC.0000000000001039, 46, 11, (512-516), (2023).
- Janette Brual, Cherry Chu, Jiming Fang, Cathleen Fleury, Vess Stamenova, Onil Bhattacharyya, Mina Tadrous, Virtual care use among older immigrant adults in Ontario, Canada during the COVID-19 pandemic: A repeated cross-sectional analysis, PLOS Digital Health, 10.1371/journal.pdig.0000092, 2, 8, (e0000092), (2023).
- W. Nicholas Jungbauer, Rachana Gudipudi, Emily Brennan, Cathy L. Melvin, Phayvanh P. Pecha, The Cost Impact of Telehealth Interventions in Pediatric Surgical Specialties: A Systematic Review, Journal of Pediatric Surgery, 10.1016/j.jpedsurg.2022.10.008, 58, 8, (1527-1533), (2023).
- Massimo Pighin, Aldo Alvarez-Risco, Shyla Del-Aguila-Arcentales, Mercedes Rojas-Osorio, Jaime A. Yáñez, Factors of the Revisit Intention of Patients in the Primary Health Care System in Argentina, Sustainability, 10.3390/su142013021, 14, 20, (13021), (2022).