Cost–effectiveness of an insertable cardiac monitor to detect atrial fibrillation in patients with cryptogenic stroke
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: We assessed cost–effectiveness of insertable cardiac monitors (ICMs) in a US cryptogenic stroke population. Materials & methods: We modelled lifetime costs and quality-adjusted life years for three monitoring strategies post cryptogenic stroke: ICM starting immediately, ICM starting after Holter monitoring (delayed ICM) and standard of care involving intermittent ECG and Holter monitoring. Patient characteristics and detection efficacy were based on the CRYSTAL-AF trial. AF detection altered the modelled anticoagulation therapy and subsequent stroke and bleed risks. Results & conclusion: Immediate ICM was found to be cost-effective versus standard of care and cost-saving versus delayed ICM. Results were robust to sensitivity analyses. ICMs are a cost-effective diagnostic tool for the prevention of recurrent stroke in a US cryptogenic stroke population.
Graphical abstract

Lay abstract
When patients have a stroke with no identifiable cause, there is a chance that it was caused by an abnormal heart rhythm called atrial fibrillation (AF). If a patient is found to have AF, their risk of having another stroke is much higher and their doctor will usually try to prescribe a blood thinner to prevent further strokes. Guidelines recommend that blood thinners are only prescribed after the presence of AF is confirmed. In the absence of AF they increase bleed risk without clear benefits.
The standard way to diagnose AF after a stroke, is to check the patient’s heart rhythm using an ECG and – sometimes but not always – to have the patient wear an external ECG monitor at home. Insertable cardiac monitors (ICMs) are a new alternative to this – they are inserted under the skin on the patient’s body by a minor surgical procedure – and record data on the heart continuously, for several years if required. ICMs are better at finding AF than standard methods and as a result they should help to prevent more strokes in the long run. They have a higher upfront cost because the devices and the minor operation must be paid for and there are also costs for the regular check-ups to review data from the ICM.
This project aimed to determine whether ICMs are a good investment for the US healthcare system to detect AF in patients who have had a stroke with no identifiable cause. We did this using an economic model that took into account all possible healthcare costs related to the care of this population and their condition and predict what might be expected to happen given the more complete AF detection that ICMs can provide.
The results of the model suggest that although ICMs cost more to administer than standard care without an ICM, they are likely to increase the length and quality of life that is preserved by preventing additional strokes. These benefits are highly valued within the US healthcare system, meaning ICMs are considered cost-effective.
Atrial fibrillation (AF) is associated with quality of life (QoL) impairment, an increase in the risk of stroke, cardiovascular morbidity and mortality and significant increases in the total cost of care [1,2]. Upon stroke occurrence, the underlying cause cannot be determined in 20–40% of cases, resulting in the classification by exclusion of cryptogenic stroke [3,4]. The risk of recurrent stroke in patients with AF can be significantly reduced by oral anticoagulation. Guidelines recommend a confirmed diagnosis of AF before initiation of anticoagulant therapy whereas in the absence of proven AF, antiplatelet therapy is usually recommended [5]. Several trials have demonstrated prophylactic anticoagulation in people without proven AF to be an ineffective strategy [6,7].
AF is often paroxysmal and asymptomatic. Consequently, it can remain undetected in many patients undergoing standard of care (SoC) cardiac monitoring [8,9]. Insertable cardiac monitors (ICMs) are capable of continuous monitoring of heart rhythm and are indicated across a range of conditions where this diagnostic information has value [10]. CRYSTAL-AF, a global randomized controlled trial, reported that use of ICMs in patients with cryptogenic stroke provided almost a ninefold higher AF detection rate compared with SoC, leading to a greater proportion of patients initiating oral anticoagulants [11]. Noninvasive cardiac rhythm monitoring has a lower diagnostic yield in patients with paroxysmal AF, even when longer duration and repeated monitoring is used [12,13]. A simulation study using CRYSTAL-AF data showed that the sensitivity of external monitors to detect AF relative to ICM-detected AF ranged from 1.3% (24-h monitor) to 22.8% (30-day monitor) [14].
The purpose of the current analysis is to assess if ICM use is cost-effective in cryptogenic stroke patients from a US payers’ perspective.
Materials & methods
We constructed a Markov model in Microsoft Excel® to estimate lifetime quality-adjusted life years (QALYs) and costs from a US payer perspective, discounted 3% annually as recommended in current guidelines for health economic evaluation [15]. Life-years gained and stroke events avoided were also modeled. The model considered a hypothetical cohort of patients with a recent cryptogenic stroke or transient ischemic attack, matching those of the CRYSTAL-AF study allocated to receive either: an immediate ICM; SoC (comprised of ECGs and intermittent Holter monitor use ranging from 24 h to 7 days, with the distribution of frequencies taken from the control arm of the CRYSTAL-AF study) [11] a strategy of delayed ICM, comprising a 7-day external Holter monitor, followed by an ICM in patients remaining undiagnosed with AF.
The effectiveness of these strategies to detect AF is based on the CRYSTAL-AF clinical trial [11] as well as a previously published simulation that used continuous monitoring data from ICMs to model the rate of AF detection with different external cardiac monitoring strategies in patients matching those in CRYSTAL-AF [14].
To ensure all relevant costs and health-related QoL (HRQoL) impairments are captured, a lifetime horizon is used. Outcomes are evaluated at fixed time increments (cycles) of 3 months, consistent with the scheduled patient follow-up intervals in the CRYSTAL-AF trial and models used in a previous Institute for Clinical and Economic Review assessment of AF treatment [16].
Model structure
Movement of patients through the model is shown in Figure 1. In each cycle, the cohort has a probability of having AF detected, or developing it without detection. If AF is detected, patients receive a nonvitamin-K oral anticoagulants (NOAC), as recommended by current clinical guidelines [17]. If AF is undetected, patients continue to receive only aspirin.

Figure 1. Model schematic.
Nonvitamin-K oral anticoagulants are administered in base case analysis, warfarin is substituted in sensitivity analysis.
AF: Atrial fibrillation; CRNM: Clinically relevant nonmajor; ECH: Extracranial hemorrhage; HS: Hemorrhagic stroke; ICH: Intracranial hemorrhage; IS: Ischemic stroke.
Secondary stroke and bleeding risks are based on the cohort’s cerebrovascular risk and the efficacy and safety of treatments received. Patients can experience up to two recurrent strokes within the model; first and second recurrent strokes each have an associated level of permanent disability as captured in distinct ‘post-stroke’ health states. AF detection and treatment change can still occur in these states, but the only transition patients can make following a second recurrent stroke is to death.
Monitoring in delayed ICM arm
Patients in the delayed ICM arm started by receiving a 7-day external Holter monitor. After 3 months (upon the beginning of the next model cycle), an ICM is implanted, if no AF has been detected and patients have not experienced a hemorrhagic stroke. If a patient has experienced a hemorrhagic stroke they are assumed to become ineligible for NOACs, so diagnosing AF does not provide the benefit of a change in treatment; thus these patients do not progress to an ICM and transition to SoC instead.
Input parameters
Event probabilities used in the model are shown in Table 1. Values were derived from published studies of baseline risks and calculated via application of drug treatment effects on those risks. Further details of model input parameters are given in Supplementary Figures 1–4 & Supplementary Tables 1–13.
| Annual risks and severity profile | Ref. | ||||
|---|---|---|---|---|---|
| AF free | AF undetected | AF detected | |||
| Treatment received | Aspirin | Aspirin | NOAC† | ||
| Risk of ischemic stroke‡ | 0.0528 | 0.0785 | 0.0319 | [18–20] | |
| Risks of major and minor bleeding§ | |||||
| ICH | 0.0055 | 0.0055 | 0.0056 | [21] | |
| GI bleed | 0.0115 | 0.0115 | 0.134 | [20,22] | |
| Clinically relevant nonmajor bleed | 0.0756 | 0.0756 | 0.0864 | [23–27] | |
| Distribution of major bleed type | All patients | ||||
| % of ICH that is hemorrhagic stroke | 59.7% | [23,28] | |||
| % of ECH that is GI bleed | 41.8% | [23,28] | |||
| Severity of first recurrent stroke event (%) | Mild | Moderate | Severe | Fatal | |
| Ischemic stroke | 42% | 26% | 10% | 22% | [23,28] |
| Hemorrhagic stroke | 28% | 23% | 12% | 37% | [23,28] |
†
NOAC was used as treatment in base case and warfarin was considered in sensitivity analysis.
‡
Ischemic stroke risk was adjusted by a factor of 1.46 (95% CI: 0.8–2.16) per decade [29].
§
Bleeding risks were adjusted by a factor of 1.97 (95% CI: 1.79–2.16) per decade [30]. ECH, extracranial hemorrhage.
AF: Atrial fibrillation; ECH: Extracranial hemorrhage; GI: Gastrointestinal; ICH: Intracranial hemorrhage.
AF incidence & detection
The definition of AF considered in this analysis is the same as used in the CRYSTAL-AF trial (episodes >30 s) [11]. Data from the first 36 months of CRYSTAL-AF were used to model AF detection with an ICM (REVEAL® XT, Medtronic), a 7-day Holter and SoC. The relationship between ICM and SoC strategies was defined by the hazard ratio for AF detection observed in the trial: 8.8 (95% CI: 3.5–22.2) [11]. Detection probabilities vary between cycles; for the first cycle, they are 8% for ICM, 1% for the Holter in the delayed ICM arm and 0.9% for SoC. Since an ICM may not accurately identify all episodes of AF, we applied a 96.1% sensitivity rate to the device to estimate the true incidence of AF [31]. For patients in the delayed ICM arm who transition to ICM, the rate of detection following transition to ICM is assumed to catch up with the rate of detection in the immediate ICM arm within one cycle.
Ischemic stroke risk & severity
The risk of ischemic stroke in the model depends on AF status, CHADS2 score, treatment and age. Gage et al. [18] reported the annual risk of ischemic stroke among patients with diagnosed AF receiving aspirin divided by CHADS2 score. These data were used as baseline risks, with the effect of AF status, treatment and age applied using a range of sources [19,20,22,29,32]. The risks of a second recurrent stroke (either ischemic or hemorrhagic) and a first recurrent stroke are independent. This is a conservative assumption, made based on clinical expert opinion in the absence of empirical data.
A distribution of the severity for a secondary ischemic stroke was defined based on data from recent cost–effectiveness analyses [23,28] and was independent of treatment. Based on expert opinion, it was assumed that a second recurrent ischemic stroke will be at least as severe as the first recurrent ischemic stroke. The likely severity of a second recurrent stroke was modeled by redistributing the probable severity of a first recurrent stroke.
Bleeding risk
Bleeding risks were taken from several studies and were treatment- and age-related [24,30,32–34]. The breakdown of different major bleeding events, in terms of type and severity, was taken from two cost–effectiveness analyses [23,28] and was assumed to apply independently of treatment.
In the model, patients experiencing clinically relevant nonmajor bleeds are assumed to remain on treatment without discontinuation. Patients experiencing hemorrhagic stroke while on NOAC, discontinued and switched to aspirin. Hemorrhagic stroke patients on aspirin did not discontinue treatment following major bleeding events but were precluded from ever changing to NOAC, even if they were subsequently diagnosed with AF. The severity of a second recurrent hemorrhagic stroke was modeled using the same method as for ischemic stroke outlined in the previous section.
Among model patients on NOACs, a nonfatal extracranial hemorrhage or other intracranial hemorrhage would prompt 25 and 56%, respectively, to permanently switch to aspirin [35,36]. The remainder of the patients stopped NOAC temporarily, resuming after 6 weeks. The same percentages were precluded from subsequently receiving NOAC therapy if the bleeding event occurred while on aspirin.
Nonfatal extracranial hemorrhage, other intracranial hemorrhage and clinically relevant nonmajor bleeds carry temporary consequences lasting only the cycle in which the bleed occurred. The consequences of ischemic stroke and hemorrhagic strokes were assumed to be permanent, with the impact on costs, HRQoL and long-term mortality dependent on the severity of the stroke (Table 2).
| Event, intervention or health state | Cost mean (SE), US$ | Utility mean (SE) | Ref. |
|---|---|---|---|
| Stroke events† | |||
| Mild IS | 12,398 (1898) | 0.76 (0.05) | [18,37] |
| Moderate IS | 26,248 (4018) | 0.39 (0.02) | [18,37] |
| Severe IS | 60,811 (9308) | 0.11 (0.01) | [18,37] |
| Fatal IS | 29,709 (4547) | 0 | [37] |
| Mild HS | 11,975 (1833) | 0.76 (0.05) | [18,37] |
| Moderate HS | 29,101 (4454) | 0.39 (0.02) | [18,37] |
| Severe HS | 69,836 (10,689) | 0.11 (0.01) | [18,37] |
| Fatal HS | 34,955 (5350) | 0 | [37] |
| Disutility for all secondary stroke events (acute period)† | -0.15 (0.039) | [18] | |
| Other events | |||
| Other intracranial hemorrhage event | 34,955 (5350) | 0.7 (0.093) | [23,28,37–39] |
| Clinically relevant nonmajor bleed | 10,795 (1647) | -0.181 (0.014)‡ | [23,28,37] |
| Gastrointestinal bleed | 38,892 (6791) | -0.181 (0.014)§ | [23,28,37] |
| Other extracranial hemorrhage | 38,892 (5350) | -0.181 (0.014)§ | [23,28,37] |
| Health states before any event | |||
| Starting utility and No-AF | N/A | 0.774 (0.013) | |
| Disutility for presence of AF | N/A | -0.014 (0.019) | |
| Post-stroke health states (per cycle) | |||
| Annual post mild stroke (IS or HS) | 12,922 (1989) | 0.727 (0.012) | [37] |
| Annual post moderate stroke (IS or HS) | 24,752 (3789) | 0.582 (0.035) | [37] |
| Annual post severe stroke (IS or HS) | 61,876 (9471) | 0.397 (0.065) | [37] |
| Disutility for secondary stroke (post-acute period) | N/A | -0.068 (0.024) | [18] |
| One-time intervention costs | |||
| ICM acquisition and insertion | 7042.20 | N/A | [40] |
| ICM removal | 738.10 | N/A | [40] |
| Monitoring & follow-up (per cycle) | |||
| ICM | 118.61 | N/A | [40] |
| SoC (year 1) | 45.38 | N/A | [40] |
| SoC (year 2) | 23.22 | N/A | [40] |
| SoC (year 3 and beyond) | 17.38 | N/A | [40] |
| Drug costs (per cycle) | |||
| Aspirin | 54.16 | N/A | |
| OAC | 118.73 | N/A | |
†
Utility and cost values in the model are adjusted for a 3-month cycle length.
‡
Disutility from CRNM bleed assumed to last 2 days.
§
Disutility from extracranial hemorrhage assumed to last 2 weeks.
AF: Atrial fibrillation; CRNM: Clinically relevant nonmajor; HS: Hemorrhagic stroke; ICM: Insertable cardiac monitor; INR: International normalized ratio; IS: Ischemic stroke; OAC: Oral anticoagulation; SE: Standard error; SoC: Standard of care.
Mortality
Age-dependent mortality risks in the model were based on US life tables [41] and were adjusted, where applicable, to exclude deaths due to cerebrovascular events which were explicitly modeled [41,42]. Following a nonfatal stroke, an individual’s mortality risk increases depending on the stroke’s severity and their treatment.
Health-related quality of life
Calculating QALYs requires estimating patients’ utility, or HRQoL, over time on a scale between 1 (perfect health) and 0 (equivalent to death). We used evidence from the OXVASC study and Gage et al., to obtain HRQoL values for stroke events and from other published models for disutility values, or utility decrements, associated with bleeding (Table 2) [23,28,38,39]. These were applied to baseline utility estimates taken from the CRYSTAL-AF trial [11]. All utilities were adjusted to account for the age and sex of the population, using published formulae [43]. Further details are available in Supplementary Tables 14 & 15.
Resource use & costs
SoC arm
The frequency and number of tests for SoC were based on those observed in the control arm of the CRYSTAL-AF trial [11]. We separated first-, second- and third-year tests performed on patients (Supplementary Table 16) and assumed that third year clinical care would be typical of long-term follow-up. Tests include infrequent use of electrocardiograms, 24-h, 48-h and 7-day Holter monitors. The frequency of unscheduled office visits was obtained from an unpublished post-hoc analysis of CRYSTAL-AF data. The unit cost for diagnostic tests and office visits were based on national average Medicare payments [44]. A mark-up of 25% was applied to Medicare payments to estimate commercial payer payments. Final blended model costs were calculated by applying commercial rates to the proportion of cryptogenic stroke patients in the US with commercial plans (40%) and those (60%) reimbursed by Medicare.
ICM arm
There are one-time costs associated with ICM insertion and subsequent removal. A per-cycle cost associated with follow-up of an ICM patient includes the cost of visiting a healthcare provider if AF was detected and regular remote and in-person interrogation of the ICM. The frequency of in-person visits was obtained from an unpublished post-hoc analysis of the Reveal LINQ Registry [37,40]. The ICM battery life is 3 years, at which point the model assumed it was removed. Following removal, patients yet undiagnosed with AF continued to receive SoC monitoring. The annual risk of unplanned ICM removal before 3 years is 3%, which comprises clinical, technical and personal reasons [11].
Delayed ICM arm
For delayed ICM, there is an initial visit, a cost for the Holter monitor and the subsequent ICM-related costs in patients who go on to receive an ICM.
Per cycle costs for drug treatment and health states, as well as one-time event costs were obtained from various sources (Table 2). The cost of oral anticoagulation therapy was estimated by averaging across all NOACs (Supplementary Table 17).
Analysis
The cost–effectiveness of ICM compared with delayed ICM and SoC was estimated with the incremental cost–effectiveness ratio (ICER), which synthesizes QALYs and healthcare costs accrued over the cohort's lifetime. We use the US payers’ willingness-to-pay thresholds of $50,000, 100,000 and 150,000 per added QALY [45,46]. The base–case analysis was based on CRYSTAL-AF patient characteristics [11] and patients diagnosed with AF were switched to a NOAC. We also performed subgroup analyses by CHADS2 score [11]. A deterministic one-way sensitivity analysis was performed on all model parameters: baseline characteristics, diagnostic accuracy, treatment efficacy and safety, utility and cost values. A scenario was tested in which the battery life of an ICM is increased to 4.5 years, by extrapolating AF detection rates via two methods: assuming a linear increase in AF detection at the end of the trial and assuming 50% of the linear rate. Probabilities of treatment discontinuation for reasons other than bleeding were also considered. A range of different Holter lengths were considered as part of the delayed ICM strategy, as was lower Holter compliance and dropout of patients being lost to follow-up before progressing to an ICM (Table 4). Use of warfarin instead of NOACs was considered, with additional results presented in the Data Supplement. A probabilistic sensitivity analysis was also performed (1,000 samples) and appropriate distributions were fitted to all model variables (Supplementary Table 18).
| Analysis | SoC | Immediate ICM | Delayed ICM | Immediate ICM vs SoC |
|---|---|---|---|---|
| Deterministic results | ||||
| Total costs (US$) | 95,877 | 102,088 | 102,223 | 6211 |
| Total ischemic strokes | 0.6393 | 0.5794 | 0.5795 | -0.0599 |
| QALYs | 6.786 | 6.985 | 6.983 | 0.198 |
| LYS | 10.037 | 10.264 | 10.263 | 0.226 |
| ICER vs SoC, US$/QALY | Reference | 31,345 | 32,200 | – |
| ICER vs SoC, US$/LY | Reference | 27,438 | 28,160 | – |
| Probabilistic results | ||||
| Total costs (95% CI), US$ | 96,859 (82,159 to 114,475) | 103,069 (88,294–120,478) | 103,217 (88,460–120,608) | 6210 |
| Total ischemic strokes (95% CI) | 0.638 (0.493 to 0.79) | 0.575 (0.431–0.732) | 0.575 (0.431–0.732) | -0.063 |
| QALYs (95% CI) | 6.795 (6.162–7.407) | 6.998 (6.34–7.646) | 6.997 (6.339–7.644) | 0.203 |
| LYs (95% CI) | 10.05 (9.379–10.6) | 10.282 (9.639–10.821) | 10.281 (9.638–10.82) | 0.232 |
| ICER vs SoC, US$/QALY | Reference | 30,613 | 31,499 | – |
| ICER vs SoC, US$/LY | Reference | 26,798 | 27,548 | – |
| Probability of being the most cost–effective | ||||
| WTP of US$50k/QALY | 14.7% | 85.3% | 0% | – |
| WTP of US$100k/QALY | 1.9% | 98.1% | 0% | – |
| WTP of US$150k/QALY | 1.0% | 99.0% | 0% | – |
ICER: Incremental cost–effectiveness ratio; SoC: Standard of care; QALY: Quality-adjusted life year; WTP: Willingness to pay.
| Scenario | Immediate ICM vs delayed ICM | ICER | |
|---|---|---|---|
| Incremental costs (US$) | Incremental QALYs | ||
| Results of alternative delayed one-off ICM strategies | |||
| 7-Day Holter (base case) | -135 | 0.001 | Immediate ICM dominates |
| 24-hour Holter | -153 | 0.001 | |
| 48-hour Holter | -140 | 0.001 | |
| 21-day Holter | -75 | 0.001 | |
| 30-day monitor | -221 | 0.001 | |
| Results of alternative delayed quarterly ICM strategies | |||
| 24-hour Holter quarterly | -211 | 0.008 | Immediate ICM dominates |
| 48-hour Holter quarterly | -178 | 0.008 | |
| 7-day Holter quarterly | -177 | 0.006 | |
| Scenario analyses (compared with base case 7-day Holter) | |||
| 50% Holter compliance | -173 | 0.001 | Immediate ICM dominates |
| 15% dropout rate | 679 | 0.03 | Immediate ICM extendedly dominates |
One-off strategies are use of a Holter once, before transitioning to an ICM after 3 months. Quarterly strategies are the quarterly use of a Holter for a year, before transitioning to an ICM. A strategy is described as economically dominant if it is cost saving and leads to better health outcomes. The 15% dropout scenario assumes that 15% of the patients eligible for an ICM in the delayed ICM arm, are lost to follow-up before they receive it.
ICER: Incremental cost–effectiveness ratio; ICM: Insertable cardiac monitor.
Results
Base–case analysis for patients using NOAC therapy
The deterministic analysis comparing the immediate ICM versus SoC strategies over the patient’s lifetime showed an incremental benefit of 0.198 QALYs and 0.226 life years, a reduction of 60 strokes per 1,000 patients and an incremental cost of US$6,211 (Table 3). These benefits were driven by the 3 years of ICM monitoring. The immediate ICM strategy was associated with higher initial costs for the technology and its use and higher bleed-related costs compared with SoC. It was also associated with lower stroke event costs and lower long-term health related costs. Based on these deterministic results, the comparison of the immediate ICM and SoC strategies showed an estimated ICER of $31,345 per QALY and US$27,438 per life year gained, making the ICM a cost-effective intervention in the US setting.
Compared with delayed ICM, the immediate ICM strategy was associated with 0.001 additional QALYs and US$135 lower costs on average over a patient’s lifetime. This means that an immediate ICM strategy had comparable effectiveness yet was cost-saving compared with delayed ICM. In the delayed ICM strategy, 7-day monitor costs totaled US$233,300 per 1,000 patients but captured only 3% of patients ultimately diagnosed with AF (the remaining 97% were detected via ICM).
A detailed breakdown of the results is available in Supplementary Tables 19–27.
Sub-group analysis by CHADS2 score
Relative to the base–case analysis, the ICER increased when we considered patients with CHADS2 scores of 2 and 3 (US$53,492 and 38,415 vs 31,345, respectively). When we considered a higher risk population (CHADS2 scores 4–6), the ICER decreased to US$19,514 per QALY gained.
Sensitivity analysis
We used deterministic sensitivity analysis to test the importance of several input parameters (Figure 2). The most important driver of cost–effectiveness was the efficacy of NOACs versus aspirin, followed by total utility estimates. Increasing the hazard ratio for ischemic strokes on NOACs versus aspirin to its upper confidence interval limit (0.49), increased the ICER to $60,767 (compared with US$20,299 at the lower bound of 0.22). An increase in utilities of 20% led to an ICER of $26,120, compared with US$39,181 for a 20% decrease. Varying the cost of ICM device and insertion cost yielded a range of ICERS from $28,114 to 36,191. The rate of NOAC discontinuation for reasons other than bleeding was varied from 0 to 3.2%, leading to modest changes in the ICER (US$30,249, 32,458). Varying the hazard ratio for ischemic stroke rate with and without AF, also led to modest changes in the ICER ($30,444, 32,584).
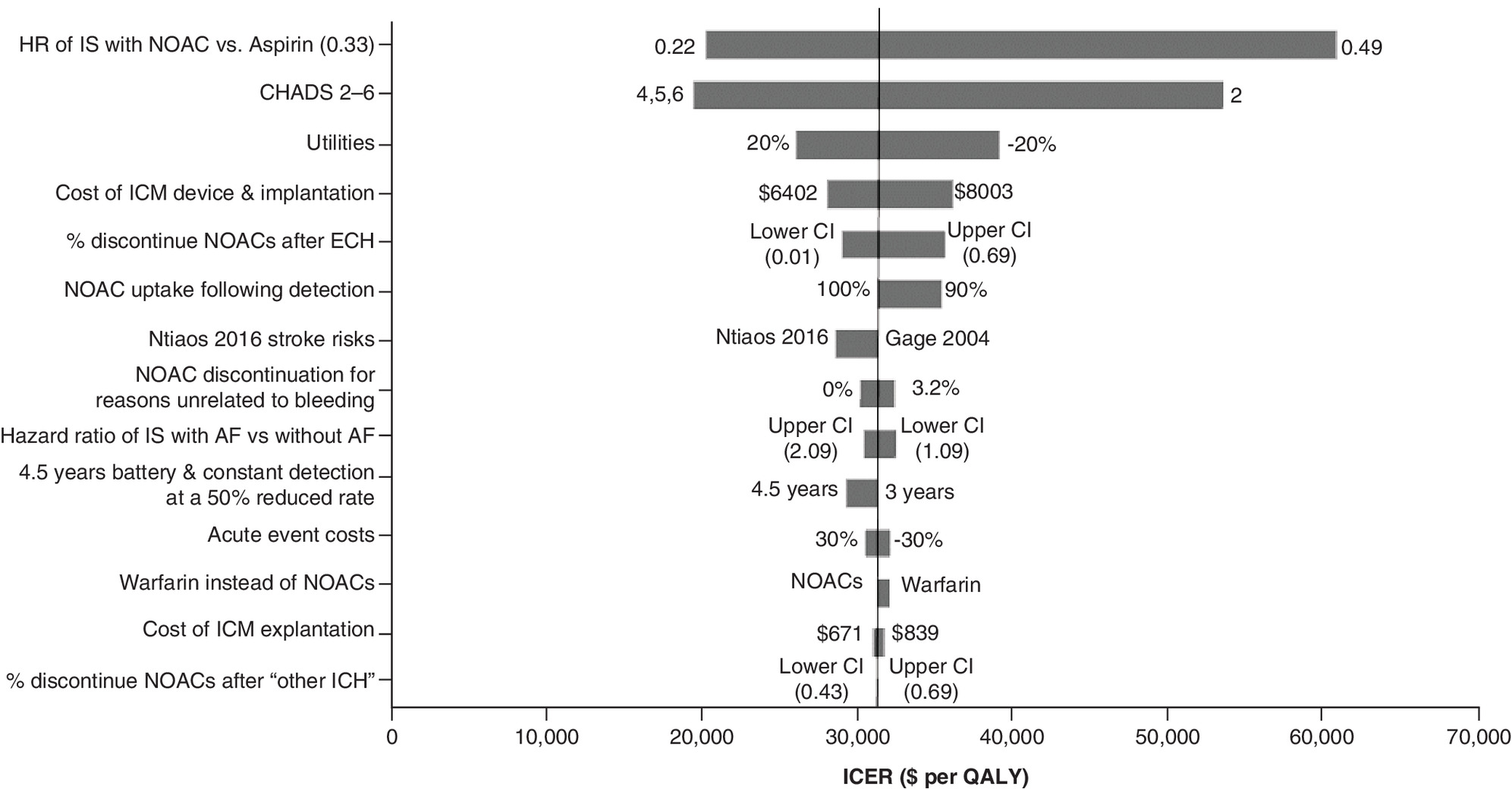
Figure 2. Immediate insertable cardiac monitor versus standard of care incremental cost–effectiveness ratio: tornado diagram.
Vertical line represents the base case ICM of US$31,345.
ECH: Extra-cranial hemorrhage; HR: Hazard ratio; ICER: Incremental cost–effectiveness ratio; ICH: Intracranial hemorrhage; ICM: Insertable cardiac monitor; IS: Ischemic stroke; NOAC; Nonvitamin-K oral anticoagulant; QALY: Quality-adjusted life-year.
We tested a number of relevant scenarios. One with a significant impact was the ICM battery life. Increasing the ICM battery life from 3 to 4.5 years and assuming a linear extrapolation of AF detection after the 3-year trial data, yielded an ICER of US$26,717. If the linear increase is reduced by 50%, the ICER increases to US$29,304, though is still improved from the base case. Another important parameter was the rate of uptake of NOACs following AF detection. Reducing this from 100 to 90% increased the ICER to US$35,508. One scenario tested the situation in which patients received warfarin instead of NOACs. This increased the ICER to US$32,183 because although the acquisition cost of warfarin is lower, it is counterbalanced by additional INR monitoring costs and higher bleeding risks.
The length of external Holter monitoring used as part of the delayed ICM strategy was also varied. For one-time monitors ranging from 24 h to 30 days, the immediate ICM strategy remains cost-saving, with a range of US$75–221 average cost savings per patient. For all quarterly monitoring scenarios tested, immediate ICM extendedly dominates delayed ICM, meaning that immediate ICM is more effective than delayed ICM and has a lower ICER versus SoC.
Table 3 shows results from the probabilistic sensitivity analysis. The probabilities that the ICM strategy would be cost-effective under willingness-to-pay thresholds of US$50,000, 100,000 and 150,000 per QALY were 85.3, 98.1 and 99.0%, respectively. SoC was more effective and less costly than immediate ICM in only 3% of samples. Delayed ICM was never found to be more cost-effective than immediate ICM. A cost–effectiveness acceptability curve is shown in Figure 3.
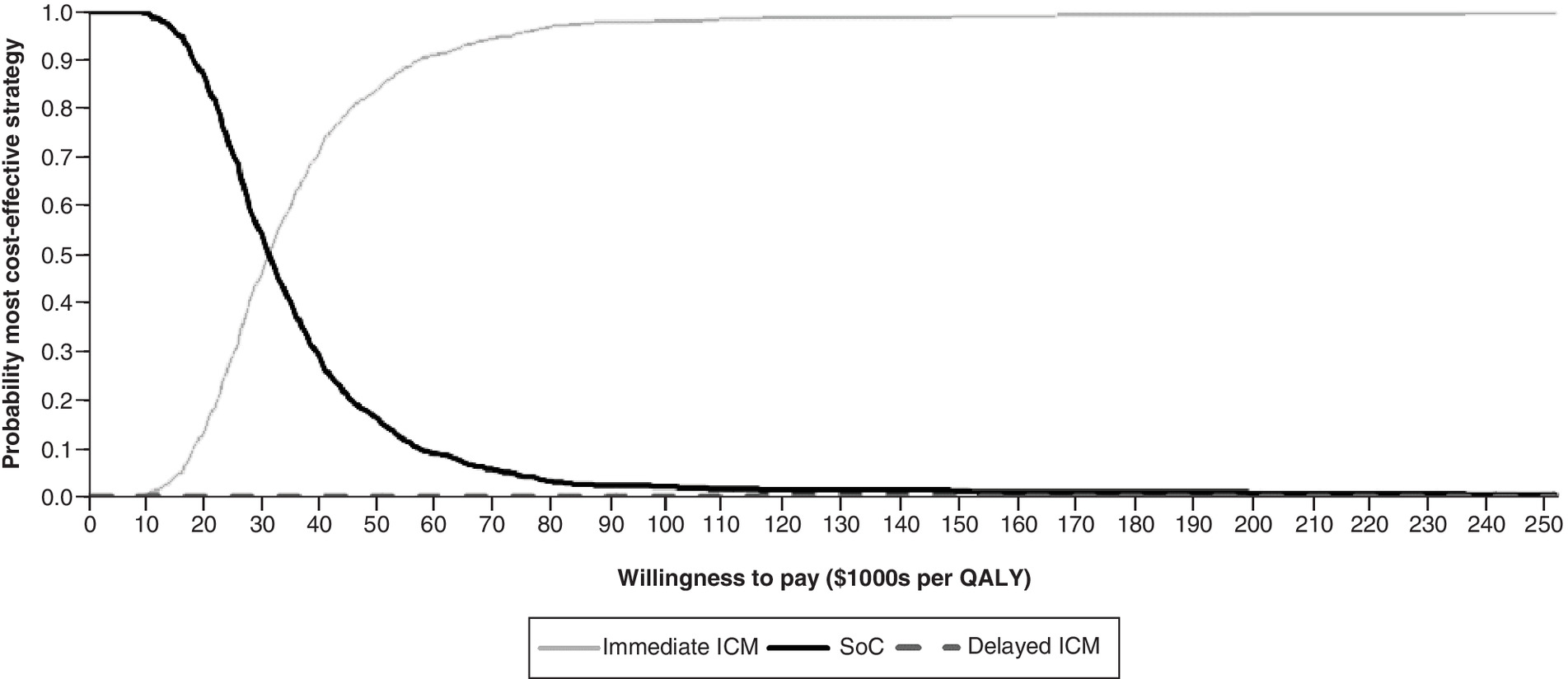
Figure 3. Cost–effectiveness acceptability curve.
Costs are in US$.
ICM: Insertable cardiac monitor; QALY: Quality-adjusted life-year; SoC: Standard of care.
Discussion
The cost–effectiveness of a diagnostic strategy is determined by the performance of the diagnostic tool and by the impact that an accurate and timely diagnosis can have on treatment and subsequent health events. ICM is associated with an almost ninefold higher rate of AF detection, compared with SoC [11], which leads to significantly more patients switching to oral anticoagulation. In the model, this resulted in fewer strokes and therefore lower costs associated with secondary stroke events, as well as increased life expectancy and more QALYs compared with SoC. Costs associated with bleeding events were higher in the immediate ICM arm (due to increased oral anticoagulant usage), as were the upfront diagnostic costs associated with the device, but these were partially offset by the savings associated with a reduction in recurrent stroke events. The ratio of the additional costs to the QALY gains of immediate ICM was found to be consistently cost-effective compared with SoC. An ICER of US$31,345 per QALY gained was estimated versus SoC which is below the willingness-to-pay thresholds (US$50,000–150,000 per QALY gained) typically considered in the US payer setting [45–47].
Compared with delayed ICM, immediate ICM was associated with a lower rate of ischemic strokes. The model shows that few patients with AF are detected by short term Holter monitoring such that the majority will eventually receive an ICM. The delay to ICM of 3 months (after a one-time Holter monitor) to a year (after four quarterly Holter monitors), means that a substantial percentage of patients with AF are delayed from receiving the appropriate treatment while all patients accrue the costs of Holter monitoring and are exposed to the risk of undetected AF. This assumption follows real world evidence from the Optum US electronic health record database, showing an average of 101 days between patients receiving a negative Holter reading and receiving an ICM [48]. Compared with delayed ICM, immediate ICM was consistently cost saving, with comparable clinical effectiveness.
This study used a range of scenario analyses, to examine the impact of key assumptions. Results were estimated for different CHADS2 subgroups (2, 3 and 4–6) demonstrating the combined effect of AF prevalence in the population, the relative accuracy of ICM versus SoC and stroke risk on the cost–effectiveness of ICMs. Results showed that ICMs are most cost-effective in the highest risk group, but still good value in those with lower CHADS2 score.
ICMs are cost-effective in so far as they enable patients with AF to be diagnosed and then anticoagulated. Anything that negatively impacts this relationship will reduce cost–effectiveness of ICMs. For example, the rate of uptake of NOACs following AF diagnosis is a key driver. The model assumed all patients would initiate NOAC at the time of AF detection, but in practice this might vary. Real-world observational datasets describe the uptake rate following cryptogenic stroke to be consistently >90%, supporting our assumptions [11,49,50]. At a level of 90%, ICMs remain cost-effective and uptake would need to reduce to below 67% for ICMs to no be considered cost-effective at the US$50k threshold. Likewise, high rates of NOAC discontinuation will reduce the value of ICM as a strategy to prevent recurrent strokes. The annual rate of discontinuation for reasons unrelated to bleeding would need to be more than 10% for the ICER of ICM to exceed US$50,000 per QALY gained.
Over time, ICM devices are expected to evolve and battery longevity will increase. Our results suggest that lengthening the battery life from 3 to 4.5 years would improve the cost–effectiveness of ICMs, though the magnitude of the improvement depends on the rate of detection after the 3 years of observation from the CRYSTAL-AF trial.
Across deterministic and probabilistic sensitivity analyses, ICM was consistently found to be cost-effective, a finding which demonstrates the robustness of the base–case conclusions. In deterministic sensitivity analysis, only varying the comparative effectiveness of NOACs and aspirin pushed the ICER above the US$50,000 threshold for immediate ICM compared with SoC. In probabilistic sensitivity analysis, immediate ICM was cost-effective in 85% of simulations at the US$50,000 threshold and delayed ICM was never the most cost-effective option. Delayed ICM was essentially a less cost-effective variant of the immediate ICM strategy, meaning that their cost–effectiveness varies in tandem within probabilistic analysis.
The model used for this analysis builds on a previous economic evaluation of ICM in a cryptogenic stroke population within the UK National Health Service (NHS) setting [51]. In contrast to the previous model which only allowed for one recurrent stroke, this new analysis incorporates the risks and consequences of up to two recurrent strokes, which gives a fuller account of health consequences of ICMs. It also includes an additional comparator, delayed ICM, which is highly relevant to clinical decision-making given the widespread use of Holter monitors and the existence of coverage policies held by some third-party payers requiring negative Holter monitoring prior to ICM. It has the added advantage of drawing on registry data, which gives an accurate account of real-world clinical practice.
ICMs were recently the subject of a health technology appraisal by the National Institute of Health and Care Excellence (NICE) in the UK [52]. On the basis of its clinical and cost–effectiveness, guidance from the Institute recommends the routine adoption of the Reveal LINQ ICM to detect AF following a cryptogenic stroke. A recent literature review by Chew et al. identified eight cost–effectiveness analyses of extended monitoring in a cryptogenic stroke population [53,54]. Strategies included 7–10-day ECG monitoring, 30-day ECG monitoring and prolonged monitoring with ICMs. They found that most studies reported ICERs within the traditionally accepted cost–effectiveness range for high income European countries, Canada, the USA and Australia. A new cost–effectiveness analysis, published after Chew et al. literature review, found ICM to be a cost-effective monitoring strategy in the US healthcare setting [55]. The present analysis further substantiates these previous findings that ICM monitoring in cryptogenic stroke patients is cost-effective, specifically in the USA. STROKE AF is an ongoing study examining the effectiveness of ICMs in patients with ischemic strokes of presumed known origin [56]. It will enable future cost–effectiveness analysis of ICMs to include this population.
Limitations
Model input data were derived from a clinical trial which, although providing the best available evidence for a cryptogenic stroke population, had patient selection criteria and treatment pathways that may not reflect current US clinical practice. However, the ICER for immediate ICM was consistently below US$50,000 per QALY gained even after adjusting for variations expected within US practice, such as stroke risks and treatment costs. If AF detection rates are higher in real-world use than in CRYSTAL-AF, as reported by Ziegler et al. then the cost–effectiveness of ICMs is likely to be even better [57].
The delayed ICM strategy represents a scenario in which clinicians attempt to detect AF without immediately resorting to internal monitor placement and thus is likely to be highly relevant. The detection efficacy of a delayed approach is unknown. In the model, it is conservatively assumed that cumulative detection under delayed ICM catches up with the immediate ICM arm in the same cycle that ICM is inserted. No data are available to inform alternative assumptions, but it is likely that this represents the highest possible detection efficacy that could be expected in a delayed ICM strategy. Further, it is assumed that 100% of eligible patients receive an ICM, whereas in reality a portion of patients might opt out or be lost to follow-up. If fewer patients receive an ICM after short-term monitoring, the delayed ICM strategy becomes less expensive, but also less effective. The costs saved in this scenario are not worth the health benefits forgone and immediate ICM remains the more cost-effective strategy.
CHA2DS2-VASc has been introduced as an updated alternative to CHADS2. Although this score was not directly captured in the CRYSTAL-AF trial, a future model could assess the impact of mapping and modeling the new risk score.
This analysis included a number of subgroups, but future analyses could further explore subgroups defined according to different clinical criteria that might affect their likelihood of having AF or their stroke risk, for example, age and atrial size. There has been discussion about the length of AF that must be detected to consider it clinically meaningful [58]. The CRYSTAL-AF study used a 30-s threshold, although the ICM was automatically limited to detect only AF episodes >2 min, while the SoC arm included episodes of 30 s or more, which is a conservative assumption. Different definitions could be tested within further research. A subgroup analysis of CRYSTAL-AF found 95% of patients in the ICM arm who were diagnosed with AF experienced an episode >6 min [59]. This suggests that results would be robust to assuming a higher AF threshold [59].
In US clinical practice, decisions can vary about whether and when to discontinue NOACs after patients experience different types of major bleeds, including hemorrhagic stroke. In our model, we took a conservative approach in which hemorrhagic stroke leads to immediate and permanent discontinuation of NOACs with no exceptions. A future analysis could investigate the effect of allowing a proportion of patients to resume NOACs after a hemorrhagic stroke or take up a NOAC at the point of AF diagnosis despite a history of hemorrhagic stroke on ICM’s cost–effectiveness.
Finally, use of a payer perspective means that our model does not capture the societal costs of ischemic strokes in a relatively young population, many of whom might be employed. Although the ICER was highest in the younger subgroup of patients with CHADS2 score of 2, the societal costs may be greater. Future evaluations taking a societal costing perspective might show a reduced ICER in this subgroup and overall.
Conclusion
Our analysis shows that by identifying AF patients who will benefit from anticoagulation therapy accurately and in a timely manner, ICMs are a cost-effective diagnostic tool for the prevention of recurrent stroke in cryptogenic stroke patients in the USA. Results were most sensitive to the cerebrovascular risk in the population, uptake and adherence to anticoagulant therapy and the time over which ICMs can detect patients with AF. ICMs were most cost-effective when the risk in the population is high and where AF detection leads to improved management in the long term. Compared with delayed ICM, immediate ICM was consistently cost saving, accompanied by a marginal gain in clinical effectiveness. These results have relevance for the USA and other value-based healthcare systems that assess costs relative to outcomes.
Future perspective
ICM technology is constantly evolving in ways that may improve the cost–effectiveness of ICM devices in future, assuming their pricing remains relatively similar. Engineering advances have resulted in smaller devices with longer battery life and improved data transmission. It is likely that battery longevity will continue to increase in future. Computational upgrades continue to provide more efficient and intelligent analysis of the raw monitoring data reducing analytical burden on doctors and improving the chance of AF detection. Furthermore, as safer and more effective anticoagulants come to market, the benefit of early and accurate detection of AF increases. These improvements may be accompanied by increased costs.
STROKE AF is examining the effectiveness of ICMs in patients with ischemic strokes of presumed known origin. The findings from this study may support expanding the use of ICMs to patients who have experienced strokes that were not cryptogenic. Given the speed of change in this field, it is important to understand how evolving technology and costs impact the value of ICM monitoring within the US healthcare system.
•
The purpose of the current analysis is to assess if insertable cardiac monitor (ICM) use to detect atrial fibrillation (AF) is cost-effective in cryptogenic stroke patients from a US payers’ perspective.
•
A Markov model was constructed to estimate lifetime quality-adjusted life years (QALYs) and costs for three monitoring strategies: immediate ICM, delayed ICM and standard of care involving ECGs and intermittent Holter monitoring. AF detection efficacy was based on the CRYSTAL-AF study. Other efficacy estimates and inputs were based on previously published analyses or registry data.
•
Immediate ICM was associated with a QALY gain of 0.198 and life year gain of 0.226 versus standard of care, at an incremental cost of US$6211. This yielded a cost-effective ICER of US$31,345 per QALY gained.
•
Compared with delayed ICM, the immediate ICM strategy delivered similar QALY benefit, but was cost-saving.
•
Benefits were driven by 3 years of ICM monitoring, during which time the improved AF detection resulted in more cryptogenic stroke patients being given preventive anticoagulation therapy and thus avoiding a recurrent stroke.
•
Findings were robust to sensitivity analyses and suggest that ICM is a cost-effective strategy for the monitoring of AF in cryptogenic stroke patients within the US healthcare setting.
Author contributions
All authors contributed to the conception and design of the study, collection and analysis of data and interpretation of results. L Sawyer, F Grimsey Jones, S Rosemas, P Ziegler and R Kaplon were responsible for data collection; L Sawyer and F Grimsey Jones carried out the health economic analysis; K Witte, M Reynolds, S Yaghi and S Mittal provided advice on clinical validation of assumptions and data sources. All authors reviewed, edited and approved the manuscript and are responsible for its content.
Acknowledgments
The authors would like to thank J Tillotson for editorial support with this manuscript.
Financial & competing interests disclosure
The project was commissioned and sponsored by Medtronic, Inc. L Sawyer and F Grimsey Jones are employees of Symmetron and consultants to Medtronic for this study; S Rosemas, P Ziegler and R Kaplon are Medtronic employees. K Witte was an NIHR Clinician Scientist when the initial UK-based analyses took place and has received unconditional research funding from Medtronic to the University of Leeds for a PhD Fellowship program and consultancy or speaker fees from Medtronic, Novartis, AstraZeneca, Pfizer, Napp, Abbott, Cardiac Dimensions, Microport. M Reynolds, S Mittal and S Yaghi are consultants to Medtronic. S Yaghi has also received funding from Mediasphere, Massachusetts General Hospital, Medlink and Medscape. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The manuscript was prepared by Symmetron Limited, via funding from Medtronic Inc.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 233.17 KB
References
Papers of special note have been highlighted as: • of interest
1.
Stewart S, Hart CL, Hole DJ, Mcmurray JJ. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am. J. Med. 113(5), 359–364 (2002).
2.
Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 22(8), 983–988 (1991).
3.
Grau AJ, Weimar C, Buggle F et al. Risk factors, outcome and treatment in subtypes of ischemic stroke: the German stroke data bank. Stroke 32(11), 2559–2566 (2001).
4.
Adams HP Jr, Bendixen BH, Kappelle LJ et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 24(1), 35–41 (1993).
5.
Jauch EC, Saver JL, Adams HP Jr et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 44(3), 870–947 (2013).
6.
Hart RG, Sharma M, Mundl H et al. Rivaroxaban for stroke prevention after embolic stroke of undetermined source. N. Engl. J. Med. 378(23), 2191–2201 (2018).
7.
Diener H-C, Sacco RL, Easton JD et al. Dabigatran for prevention of stroke after embolic stroke of undetermined source. N. Engl. J. Med. 380(20), 1906–1917 (2019).
8.
Healey JS, Connolly SJ, Gold MR et al. Subclinical atrial fibrillation and the risk of stroke. N. Engl. J. Med. 366(2), 120–129 (2012).
9.
Camm AJ, Corbucci G, Padeletti L. Usefulness of continuous electrocardiographic monitoring for atrial fibrillation. Am. J. Cardiol. 110(2), 270–276 (2012).
10.
Sakhi R, Theuns DaMJ, Szili-Torok T, Yap S-C. Insertable cardiac monitors: current indications and devices. Expert Rev. Med. Dev. 16(1), 45–55 (2019).
11.
Sanna T, Diener HC, Passman RS et al. Cryptogenic stroke and underlying atrial fibrillation. N. Engl. J. Med. 370(26), 2478–2486 (2014).
• Presents findings from the CRYSTAL atrial fibrillation (AF) study, which was used to model the quantity of AF diagnosed by insertable cardiac monitors (ICMs) in this study.
12.
Bang OY, Ovbiagele B, Kim JS. Evaluation of cryptogenic stroke with advanced diagnostic techniques. Stroke 45(4), 1186–1194 (2014).
13.
Gladstone DJ, Spring M, Dorian P et al. Atrial fibrillation in patients with cryptogenic stroke. N. Engl. J. Med. 370(26), 2467–2477 (2014).
14.
Choe WC, Passman RS, Brachmann J et al. A comparison of atrial fibrillation monitoring strategies after cryptogenic stroke (from the Cryptogenic Stroke and Underlying AF Trial). Am. J. Cardiol. 116(6), 889–893 (2015).
• Was used to estimate the efficacy of short-to-long term monitoring, when used as part of the delayed ICM strategy.
15.
ICER. ICER's reference case for economic evaluations: principles and rationale (2018). https://icer-review.org/wp-content/uploads/2018/07/ICER_Reference_Case_July-2018.pdf
16.
ICER. Rhythm control and stroke prevention strategies for patients with atrial fibrillation (2010). https://icer-review.org/wp-content/uploads/2016/02/Atrial-Fibrillation-Final-09-24-10.pdf
17.
January Craig T, Wann LS, Calkins H et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation. J. Am. Coll. Cardiol. 74(1), 104–132 (2019).
18.
Gage BF, Van Walraven C, Pearce L et al. Selecting patients with atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirin. Circulation 110(16), 2287–2292 (2004).
• Was used as the baseline risk of ischemic stroke, for patients with AF receiving aspirin.
19.
Mohan KM, Crichton SL, Grieve AP, Rudd AG, Wolfe CD, Heuschmann PU. Frequency and predictors for the risk of stroke recurrence up to 10 years after stroke: the South London Stroke Register. J. Neurol. Neurosurg. Psych. 80(9), 1012–1018 (2009).
• Was used to estimate the effect that risk factors for ischemic stroke have on the baseline risk of ischemic stroke.
20.
Ntaios G, Papavasileiou V, Diener HC, Makaritsis K, Michel P. Nonvitamin-K-antagonist oral anticoagulants in patients with atrial fibrillation and previous stroke or transient ischemic attack: a systematic review and meta-analysis of randomized controlled trials. Stroke 43(12), 3298–3304 (2012).
21.
Tawfik A, Bielecki JM, Krahn M et al. Systematic review and network meta-analysis of stroke prevention treatments in patients with atrial fibrillation. Clin. Pharmacol. 8, 93–107 (2016).
22.
Diener HC, Eikelboom J, Connolly SJ et al. Apixaban versus aspirin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a predefined subgroup analysis from AVERROES, a randomised trial. Lancet Neurol. 11(3), 225–231 (2012).
23.
Dorian P, Kongnakorn T, Phatak H et al. cost–effectiveness of apixaban vs. current standard of care for stroke prevention in patients with atrial fibrillation. Eur. Heart J. 35(28), 1897–1906 (2014).
24.
Connolly SJ, Ezekowitz MD, Yusuf S et al. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 361(12), 1139–1151 (2009).
25.
Patel MR, Mahaffey KW, Garg J et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 365(10), 883–891 (2011).
26.
Giugliano RP, Ruff CT, Braunwald E et al. Edoxaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 369(22), 2093–2104 (2013).
27.
Connolly SJ, Eikelboom J, Joyner C et al. Apixaban in patients with atrial fibrillation. N. Engl. J. Med. 364(9), 806–817 (2011).
28.
Lip GY, Kongnakorn T, Phatak H et al. cost–effectiveness of apixaban versus other new oral anticoagulants for stroke prevention in atrial fibrillation. Clin. Ther. 36(2), 192–210 e120 (2014).
29.
Pisters R, Lane DA, Marin F, Camm AJ, Lip GY. Stroke and thromboembolism in atrial fibrillation. Circ. J. 76(10), 2289–2304 (2012).
30.
Ariesen MJ, Claus SP, Rinkel GJ, Algra A. Risk factors for intracerebral hemorrhage in the general population: a systematic review. Stroke 34(8), 2060–2065 (2003).
31.
Hindricks G, Pokushalov E, Urban L et al. Performance of a new leadless implantable cardiac monitor in detecting and quantifying atrial fibrillation: results of the XPECT trial. Circ. Arrhythm Electrophysiol. 3(2), 141–147 (2010).
32.
Easton JD, Lopes RD, Bahit MC et al. Apixaban compared with warfarin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a subgroup analysis of the ARISTOTLE trial. Lancet Neurol. 11(6), 503–511 (2012).
33.
Granger CB, Alexander JH, Mcmurray JJ et al. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 365(11), 981–992 (2011).
34.
Hankey GJ, Patel MR, Stevens SR et al. Rivaroxaban compared with warfarin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a subgroup analysis of ROCKET AF. Lancet Neurol. 11(4), 315–322 (2012).
35.
Claassen DO, Kazemi N, Zubkov AY, Wijdicks EF, Rabinstein AA. Restarting anticoagulation therapy after warfarin-associated intracerebral hemorrhage. Arch. Neurol. 65(10), 1313–1318 (2008).
36.
Sorensen SV, Dewilde S, Singer DE, Goldhaber SZ, Monz BU, Plumb JM. Cost–effectiveness of warfarin: trial versus “real-world” stroke prevention in atrial fibrillation. Am. Heart J. 157(6), 1064–1073 (2009).
37.
Shireman TI, Wang K, SWIFT-PRIME Investigators et al . Cost–effectiveness of Solitaire stent retriever thrombectomy for acute ischemic stroke: results from the SWIFT-PRIME trial (Solitaire With the Intention for Thrombectomy as Primary Endovascular Treatment for Acute Ischemic Stroke). Stroke 48(2), 379–387 (2017).
38.
Luengo-Fernandez R, Paul NL, Gray AM et al. Population-based study of disability and institutionalization after transient ischemic attack and stroke: 10-year results of the Oxford Vascular Study. Stroke 44(10), 2854–2861 (2013).
39.
Luengo-Fernandez R, Gray AM, Bull L et al. Quality of life after TIA and stroke: ten-year results of the Oxford Vascular Study. Neurology 81(18), 1588–1595 (2013).
40.
Reveal LINQ Registry. https://clinicaltrials.gov/ct2/show/NCT02746471
41.
Centers for Disease Control (CDC). Deaths: final data for 2017 (2017). https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_09-508.pdf
42.
United States mortality database (2019). https://usa.mortality.org/
43.
Sullivan PW, Lawrence WF, Ghushchyan V. A national catalog of preference-based scores for chronic conditions in the United States. Med. Care 43(7), 736–749 (2005).
44.
Centers for Medicare & Medicaid Services. Physician fee schedule. https://www.cms.gov/apps/physician-fee-schedule/license-agreement.aspx
45.
ICER. ICER's reference case for economic evaluations: principles and rationale (2018). https://icer-review.org/methodology/icers-methods/icer_reference_case_july-2018/
46.
Anderson JL, Heidenreich PA, Barnett PG et al. ACC/AHA statement on cost/value methodology in clinical practice guidelines and performance measures: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures and Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 63(21), 2304–2322 (2014).
47.
ICER. Overview of the ICER value assessment framework and update for 2017–2019 (2018). https://icer-review.org/wp-content/uploads/2018/03/ICER-value-assessment-framework-update-FINAL-062217.pdf
48.
Optum. Electronic Health Record de-identified database (2007–2017). https://www.optum.com/business/solutions/government/federal/data-analytics-federal/clinical-data.html
49.
Ricci B, Chang AD, Hemendinger M et al. A simple score that predicts paroxysmal atrial fibrillation on outpatient cardiac monitoring after embolic stroke of unknown source. J. Stroke Cerebrovasc. Dis. 27(6), 1692–1696 (2018).
50.
Wachter R, Gröschel K, Gelbrich G et al ; Find-AF (randomised) Investigators and Coordinators. Holter-electrocardiogram-monitoring in patients with acute ischaemic stroke (Find-AFRANDOMISED): an open-label randomised controlled trial. Lancet Neurol. 16(4), 282–290 (2017).
51.
Rinciog CI, Sawyer LM, Diamantopoulos A et al. Cost–effectiveness of an insertable cardiac monitor in a high-risk population in the UK. Open Heart 6(1), e001037 (2019).
• Modelled the cost–effectiveness of ICMs in a population at high risk of AF, in a UK setting.
52.
National Institute for Healthcare Excellence. Implantable cardiac monitors to detect atrial fibrillation after cryptogenic stroke (2020). https://www.nice.org.uk/guidance/dg41
• Was a contemporary health technology assessment of insertable cardiac monitors in a cryptogenic stroke population
53.
Chew D, Rennert-May E, Quinn FR, Spackman E, Manns B, Exner D. Cost–effectiveness of extended ECG monitoring for detection of occult atrial fibrillation in patients with cryptogenic stroke. J. Am. Coll. Cardiol. 75(1 Suppl. 11), 315 (2020).
54.
Chew Derek S, Rennert-May E, Spackman E, Mark Daniel B, Exner Derek V. Cost–effectiveness of extended electrocardiogram monitoring for atrial fibrillation after stroke. Stroke 51(7), 2244–2248 (2020).
• Was a systematic literature review of economic evaluations of ICMs.
55.
Maervoet J, Bossers N, Borge RP, Hilpert ST, Van Engen A, Smala A. Use of insertable cardiac monitors for the detection of atrial fibrillation in patients with cryptogenic stroke in the United States is cost-effective. J. Med. Econ. 22(11), 1221–1234 (2019).
56.
ClinicalTrials.gov Identifier: NCT02700945. Rate of Atrial Fibrillation Through 12 Months in Patients with Recent Ischemic Stroke of Presumed Known Origin. https://clinicaltrials.gov/ct2/show/NCT02700945
57.
Ziegler PD, Rogers JD, Ferreira SW et al. Real-world experience with insertable cardiac monitors to find atrial fibrillation in cryptogenic stroke. Cerebrovasc. Dis. 40(3–4), 175–181 (2015).
58.
Steinberg JS, O'connell H, Li S, Ziegler PD. Thirty-second gold standard definition of atrial fibrillation and its relationship with subsequent arrhythmia patterns: analysis of a large prospective device database. Circ. Arrhythm Electrophysiol. 11(7), e006274 (2018).
59.
Brachmann J, Morillo CA, Sanna T et al. Uncovering atrial fibrillation beyond short-term monitoring in cryptogenic stroke patients: three-year results from the Cryptogenic Stroke and Underlying Atrial Fibrillation Trial. Circ. Arrhythm Electrophysiol. 9(1), e003333 (2016).
Information & Authors
Information
Published In
Pages: 127 - 141
PubMed: 33300381
Copyright
© 2020 Laura Sawyer. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 16 October 2020
Accepted: 20 November 2020
Published online: 10 December 2020
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of an insertable cardiac monitor to detect atrial fibrillation in patients with cryptogenic stroke. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0224
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Jian Ye, Youqi Fan, Ye Wang, Yifei Jian, Yue Gao, Shuting Chen, Jianwei Xuan, Hesheng Hu, Health economic analysis of pulsed field ablation compared to conventional thermal ablation for patients with paroxysmal atrial fibrillation in China, Journal of Comparative Effectiveness Research, 10.57264/cer-2025-0153, 15, 5, (2026).
- Matthew R Reynolds, Vicki Pollit, Lee Schwamm, Klaus K Witte, Shadi Yaghi, David Z Rose, Sarah Cudworth, Julius Carpenter, Sarah C Rosemas, Paul D Ziegler, Karah Neisen, Noreli C Franco, Richard A Bernstein, Cost-effectiveness of an insertable cardiac monitor to detect atrial fibrillation in large- or small-vessel disease ischaemic stroke in the USA, BMJ Open, 10.1136/bmjopen-2025-103766, 16, 4, (e103766), (2026).
- Klaus K. Witte, Cho-Hsuan Lee, Sarah C. Rosemas, Jonas Villinger, Economic and clinical impact of diagnostic sensitivity for the use of insertable cardiac monitors to detect atrial fibrillation in cryptogenic stroke patients in the United Kingdom, BMC Cardiovascular Disorders, 10.1186/s12872-026-05871-0, 26, 1, (2026).
- Nadja Korajkic, Vincent Thijs, From Detection to Decision: Managing Device-Detected Atrial Fibrillation After Stroke, Current Neurology and Neuroscience Reports, 10.1007/s11910-025-01473-z, 26, 1, (2025).
- Amit K. Kishore, Crystal Sing Chiek Teoh, Kunal Sareen, Bibhu D. Mohanty, Marla Hairston, Mirko De Melis, Roberto Carta, Noreli C. Franco, Karah B. Neisen, David Z. Rose, Heterogeneity in Ischaemic Stroke Diagnostic Classification and Cardiac Monitoring between the UK and the USA: The DiVERT Stroke Sub-Study, Cerebrovascular Diseases, 10.1159/000548286, 55, 5, (564-570), (2025).
- William V. Padula, Alexandra Paffrath, Caroline M. Jacobsen, Benjamin G. Cohen, Rachel Nadboy, Brad S. Sutton, Edward P. Gerstenfeld, Moussa Mansour, Vivek Y. Reddy, Comparing pulsed field ablation and thermal energy catheter ablation for paroxysmal atrial fibrillation: a cost-effectiveness analysis of the ADVENT trial, Journal of Medical Economics, 10.1080/13696998.2024.2441071, 28, 1, (127-136), (2025).
- Satoshi Suzuki, Eriko Sugawara, Genpei Yamaura, Mutsumi Yokoyama, Hideto Joki, Yosuke Miyaji, Yuichi Higashiyama, Takayuki Momoo, Hiroshi Doi, Fumiaki Tanaka, Early Prediction of Paroxysmal Atrial Fibrillation in Patients With Acute Stroke Using the BANQMR Score, Journal of Clinical Neurology, 10.3988/jcn.2025.0103, 21, 6, (527), (2025).
- Vasily Lukyanov, Purvee Parikh, Manish Wadhwa, Alexandria Dunn, Roderick van Leerdam, Johan Engdahl, Goran Medic, Cost-Minimization Model in Cryptogenic Stroke: ePatch vs Implantable Loop Recorder in Patients from the UK, Netherlands, and Sweden, Medical Devices: Evidence and Research, 10.2147/MDER.S492389, Volume 17, (471-490), (2024).
- Nabeel A. Herial, Daniel R. Frisch, Elan Miller, Priyadarshee Patel, Alfredo Munoz, Melissa Warren, Jane Khalife, Shyam Majmundar, Nathan Farkas, Shaista Alam, Robin Dharia, Diana Tzeng, Behzad B. Pavri, Reginald T. Ho, Arnold Greenspon, Rodney Bell, Pascal Jabbour, Robert Rosenwasser, Reimagining Cryptogenic Stroke Care: Collaborative Care and Inpatient Insertable Cardiac Monitors for Detection of Atrial Fibrillation, Stroke: Vascular and Interventional Neurology, 10.1161/SVIN.124.001469, 4, 6, (2024).
- Morten Lock Hansen, Joe W. E. Moss, Jacob Tønnesen, Mette Lundsby Johansen, Malte Kuniss, Eleni Ismyrloglou, Jason Andrade, Oussama Wazni, Stuart Mealing, Alicia Sale, Daniela Afonso, Tom Bromilow, Emily Lane, Gian Battista Chierchia, A danish healthcare-focused economic evaluation of first-line cryoballoon ablation versus antiarrhythmic drug therapy for the treatment of paroxysmal atrial fibrillation, BMC Cardiovascular Disorders, 10.1186/s12872-024-04024-5, 24, 1, (2024).
- See more