The prevalence, characteristics and treatment of hemorrhoidal disease: results of an international web-based survey
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: This international study assessed the characteristics and treatment of individuals with hemorrhoids. Materials & methods: Online survey among nationally representative populations of adults from Brazil, Czech Republic, France, Hungary, Italy, Romania, Russia and Spain, that identified participants who self-reported having hemorrhoidal disease. Results: Hemorrhoid prevalence was 11% (1725/16015); most respondents had low-severity disease (71%). Compared with the general population, participants with hemorrhoidal disease had more comorbidities (mean 3.1 vs 1.3) and included more women who had been pregnant (81 vs 68%). Common initial signs/symptoms were pain (60%), bleeding (47%) and discomfort (43%). Hemorrhoid respondents who consulted a physician were more likely to undergo interventions and take medications. Conclusion: The prevalence of hemorrhoidal disease in the adult population is 11%, mostly low-severity disease.
Hemorrhoids are engorged venous cushions within the anal canal [1]. The most common symptom of hemorrhoidal disease is rectal bleeding, usually after defecation, characterized by the passage of small amounts of bright red fresh blood (the color is a result of direct arteriovenous communication present in the hemorrhoidal cushion) [1,2].
The severity of hemorrhoidal disease is usually graded by the Goligher classification system, which is based on the degree of prolapse through the anus [1,2]. According to this system, Grade 1 corresponds to a hemorrhoid that bleeds but does not prolapse; Grade 2: hemorrhoid may prolapse during straining but spontaneously reduces or reverts; Grade 3: hemorrhoid may prolapse during straining or exertion but can be manually pushed back into the anal canal and Grade 4: hemorrhoid is permanently prolapsed and cannot be reduced manually [1,2]. Notably, this system does not take into account patients’ symptoms. In addition to bleeding, patients may also experience rectal itching or swelling, a sensation of rectal fullness, fecal soiling and pain, particularly if the hemorrhoids are prolapsed [1,2]. Prolapsed hemorrhoids may become thrombosed or strangulated, resulting in severe anal pain [1].
Hemorrhoidal disease usually develops when the supporting connective tissue framework in the anorectal apparatus becomes weakened, due to age or raised intra-abdominal pressures [1,2]. Therefore, risk factors for hemorrhoidal disease are conditions associated with increased intra-abdominal pressures such as pregnancy, obesity, constipation and straining during defecation and sitting for a long time on the toilet seat, repeated use of the Valsalva maneuver (e.g., to relieve back pain in ankylosing spondylitis) and chronic cough [3–5].
Hemorrhoidal disease is one of the most common anorectal conditions seen in general practice [6], but the true prevalence in the general population is not well understood, partly because many patients do not seek treatment [6,7]. Two French studies reported a prevalence of hemorrhoidal disease of 4 and 7% among adult patients attending general practice clinics [6,7], whereas population-based surveys in the USA, Spain and Japan reported a prevalence of 4, 13 and 17%, respectively [8–10]. A higher prevalence is reported in specific groups, such as pregnant or postpartum women, in whom the prevalence of hemorrhoidal disease is between 12 and 41% [11,12]. Notably, in the French general practice studies, most of the patients with an anal condition were seeing the primary care physician for a different condition and only revealed the anal condition after primary care physician questioning [6,7]. This suggests that hemorrhoidal disease may be underdiagnosed and undertreated.
The current study was undertaken to evaluate the prevalence of hemorrhoidal disease in a representative sample of the general population across a number of countries, as well as to assess the characteristics of patients affected by hemorrhoidal disease and how the condition was treated.
Materials & methods
Survey design
This web-based, adaptive survey was conducted by Harris Interactive (Paris, France). The survey consisted of two parts: questions about demographics and hemorrhoid characteristics and questions about the hemorrhoid treatment pathway.
Participants were recruited from December 2017 to February 2018 via the Toluna Global Panel (an online platform of panelists willing to participate in surveys created and managed by the company Toluna). The investigators were blinded to the identity of the participants. Individuals aged ≥18 years who resided in Brazil, the Czech Republic, France, Hungary, Italy, Romania, Russia and Spain and could speak and read the local language, were eligible for inclusion in the study. A quota sampling method was used to ensure that the sample populations were nationally representative in terms of sex, age and geographical region, based on sources for national statistics such as the National Institute of Statistics and Economic studies (INSEE) in France. The target sample size was a minimum of 2000 individuals from each country, for a total of at least 16,000 individuals. This sample size was estimated on the basis of the expected prevalence of hemorrhoidal disease [8–10] and the percentage of responders to surveys of this kind. Within the general population, individuals were identified who had experienced hemorrhoidal disease at least twice in the past 12 months and who reported specific predefined symptoms of hemorrhoidal disease (bleeding, itching, swelling and pain).
Hemorrhoid severity was defined using a combination of symptoms and Goligher classification of the degree of prolapse. Low severity was defined as the presence of discomfort and/or pain and/or signs including bleeding, hemorrhoid protrusion on straining but without hemorrhoid prolapse or hemorrhoids visible on proctoscopy (if performed). Moderate severity was defined as the presence of symptoms such as discharge, swelling, oozing, pruritus/itching or pain and signs, such as bleeding, a prolapsed hemorrhoid that is visible at the anal margin during straining and during defecation or marked straining, but spontaneously returns or can be reinserted manually when straining ends. High severity was defined as the presence of discharge or pain symptoms, with permanent and irreducible prolapse. The web survey form provided these detailed descriptions of severity, allowing respondents to select the grade most applicable to their hemorrhoid severity. The frequency of hemorrhoid symptoms was defined as follows: rare (once per year), occasional (2–5-times per year), frequent (6–12-times per year), very frequent (>12-times per year) or constant.
Respondents were classified as having normal weight if their BMI was <25 kg/m2, overweight if their BMI was 25–29 kg/m2 and obese if their BMI was >30 kg/m2.
Hemorrhoid therapies were classified into three categories: nonpharmacological therapies and lifestyle changes, medicinal products and drugs and interventions. Nonpharmacological therapies and lifestyle changes included dietary changes (food/hydration, avoiding spicy food), increased physical activity, behavioral changes (improved posture and skin hygiene, avoiding carrying heavy objects) and hip baths, with or without the addition of ice cubes. Medicinal products and drugs included creams, ointments and gels, oral venoactive drugs (VADs; in the form of tablets, oral solutions, capsules or ampoules), food supplements, phytotherapy and homeopathy. Interventions included surgery, laser/radiofrequency ablation or office procedures like banding, sclerotherapy.
In the survey, respondents were asked to describe their treatment steps (between one and five) in a chronological manner from the time of their first symptoms, identifying them as step 1, step 2 and so on. Those who had experienced more than five treatment steps and who were currently receiving new treatment (i.e., different from the prior steps) were then directed to a question regarding only their most recent (i.e., current) treatment beyond step 5 (i.e., step 5+). In the series of questions where respondents retraced their treatment steps, participants were asked about where they sought information (online or from friends/relatives, a pharmacist or healthcare professional) and the resultant action taken (or not) or treatment initiated since the symptoms had appeared or reappeared (e.g., change/no change in lifestyle, use of nonpharmacologic remedies or medicines or undergoing a medical procedure [e.g., surgery, laser therapy]). Respondents were asked to describe the following for each treatment step: the nature of treatment (nonpharmacological remedies, medicines or medical procedures [e.g., surgery, laser therapy]), the duration of treatment (for completed episodes of treatment), their satisfaction with treatment and the status of each treatment (completed, in progress or undergoing change). Examples of ‘undergoing change’ included from self-treatment to a recommendation from a pharmacist or a prescription from a physician; a switch of product recommended or prescribed by the same or another physician/pharmacist; a switch in management from their general practitioner (GP) to a specialist.
Ethics
Participants provided informed consent prior to completing the survey. Participants’ data were used in a general and anonymized manner for the purposes of this study only and were not provided to any third party. As this was not an investigation of clinical outcomes with a particular intervention, neither Ethics Committee approval nor clinical trial registration was required.
Statistical methods
Descriptive statistics (i.e., totals, percentages and means ± standard deviation) were calculated for demographic and disease data. The prevalence of hemorrhoidal disease was calculated as the proportion of the overall population with participant-reported symptoms of hemorrhoidal disease.
Statistical comparisons were undertaken between a number of different respondent groups, including between the hemorrhoid population and the general population in order to identify the main differences between both populations; between the global hemorrhoid population and national hemorrhoid populations and between the global hemorrhoid population and subgroups of the hemorrhoid population (e.g., those who consult a physician, those who seek information by themselves, subgroups based on treatment steps). These comparisons were made using a two-tailed (significantly superior or significantly inferior) z-test, with a significance threshold of p < 0.05, using Daisie software (ADN SAS, Paris, France; available at http://adn-soft.com/daisie/). Missing values were excluded from the statistics. Analyses were not conducted on groups with a sample size of <30 individuals. Data are available on request from Harris Interactive (Fabienne Goron and Ghislaine Salmat).
Results
Prevalence
A total of 16,015 individuals were recruited into the general population (Table 1). Of these, 1725 individuals (11%) had hemorrhoidal disease. The prevalence of hemorrhoidal disease ranged from 6 to 7% (in Brazil and France, respectively) to 16% in Italy and Russia. In most countries, the prevalence of hemorrhoidal disease was approximately 9–11%, reported in 9% of respondents in Czech Republic, 10% in Romania and Hungary and 11% in Spain. Characteristics of individuals with hemorrhoidal disease by country are detailed in Supplementary Table 1.
| Characteristics | General population (n = 16015), n (%) | Hemorrhoid population (n = 1725), n (%) | p-value† |
|---|---|---|---|
| Sex: | |||
| Male | 7714 (48) | 765 (44) | <0.05 |
| Female | 8301 (52) | 960 (56) | <0.05 |
| Age (years): | |||
| Mean ± SD | 44.9 ± 14.8 | 46.38 ± 12.3 | <0.05 |
| Median | 44.75 | 45.56 | |
| Age categories: | |||
| 18–40 years | 6562 (41) | 604 (35) | <0.05 |
| 41–60 years | 6770 (42) | 885 (51) | <0.05 |
| >60 years | 2683 (17) | 236 (14) | <0.05 |
| BMI categories: | |||
| Normal (<25 kg/m2) | 7675 (48) | 775 (45) | <0.05 |
| Overweight (25–29 kg/m2) | 5334 (33) | 588 (34) | NS |
| Obese (>30 kg/m2) | 3006 (19) | 362 (21) | NS |
| Comorbidities: | |||
| Crohn’s disease | 125 (1) | 32 (2) | <0.05 |
| Hematologic disease/blood cancer | 122 (1) | 33 (2) | <0.05 |
| Psoriasis | 840 (5) | 205 (12) | <0.05 |
| Asthma | 1114 (7) | 216 (13) | <0.05 |
| Heavy legs or varicose veins | 3905 (24) | 847 (49) | <0.05 |
| Varicose veins | 1522 (10) | 424 (25) | <0.05 |
| Heavy/tired/swollen legs problems | 3222 (20) | 700 (41) | <0.05 |
| Hemorrhoidal disease | 2407 (15) | 1725 (100) | <0.05 |
| Hypertension | 3948 (25) | 641 (37) | <0.05 |
| Cancer (of whatever organ) | 278 (2) | 39 (2) | NS |
| Depression | 2467 (15) | 498 (29) | <0.05 |
| Allergy | 3762 (23) | 671 (39) | <0.05 |
| Diabetes (Type I or II) | 1357 (8) | 223 (13) | <0.05 |
| None of the above | 5440 (34) | 0 | <0.05 |
| Number of comorbidities: | |||
| Mean ± SD | 1.3 ± 1.4 | 3.1 ± 1.8 | <0.05 |
| Median | 0.52 | 2.33 | |
| History of pregnancy‡ | 5660 (68) | 778 (81) | <0.05 |
| Physical activity: | |||
| Not regular§ | 10,746 (67) | 1178 (68) | NS |
| Regular¶ | 5269 (33) | 547 (32) | NS |
| Standing during the day: | |||
| Yes# | 6881 (43) | 736 (43) | NS |
| No†† | 9134 (57) | 989 (57) | NS |
| Income: | |||
| Low | 4118 (26) | 327 (19) | <0.05 |
| Medium | 6756 (42) | 744 (43) | NS |
| High | 5141 (32) | 654 (38) | <0.05 |
†
Student’s t-test for comparisons of percentages and z-test for comparisons of means.
‡
Of the number of women (8301 in the general population and 960 among the hemorrhoid population).
§
Respondents indicated that they did not undertake regular physical exercise or exercised once or twice a week.
¶
Respondents indicated that they exercised 3 or 4-times per week or did daily physical exercise.
#
Respondents indicated that they had a job that required them to be constantly, almost constantly or frequently standing.
††
Respondents indicated that they had a job that required them to be standing occasionally or rarely.
NS: Not significant; SD: Standard deviation.
Profile of individuals with hemorrhoidal disease
Compared with the general population, the cohort with hemorrhoidal disease included a slightly higher proportion of females (52 vs 56%) and obese people (19 vs 21%), had a higher mean age (44.9 vs 46.8 years), had more comorbidities on average (1.3 vs 3.1) and included more respondents in the high income bracket (32 vs 38%) and fewer in the low income bracket (26 vs 19%) (Table 1). A higher proportion of women in the hemorrhoid cohort had been pregnant (81%) compared with the general population (68%; Table 1); women with hemorrhoidal disease had had an average of 1.9 pregnancies. Similar proportions of respondents in the hemorrhoid group and the general population engaged in regular physical activity (32 and 33%, respectively) or had a job that required them to stand for most of the day (43% in both). Comorbidities that occurred at a higher prevalence in the hemorrhoid group than in the general population included psoriasis (12 vs 5%), asthma (13 vs 7%), varicose veins (25 vs 10%), heavy/tired/swollen leg problems (41 vs 20%), hypertension (37 vs 25%), depression (29 vs 15%), allergy (39 vs 23%) and diabetes (type unspecified; 13 vs 8%).
Disease characteristics
In most individuals with hemorrhoidal disease, the condition was perceived by respondents (according to their symptoms classified with Goligher grade) to be of low severity (71%); 15% of respondents had medium severity and 14% had high-severity hemorrhoidal disease. Overall, 64% of respondents had a family history of hemorrhoidal disease and 15% did not; the other 21% of respondents did not know their family history in relation to hemorrhoidal disease. Most survey participants had experienced hemorrhoidal disease for at least 1 year, with the duration of hemorrhoidal disease being <1 year in 15%, 1–<5 years in 41% and ≥5 years in 44%. Only 6% of participants with hemorrhoidal disease experienced constant symptoms; 31% reported having frequent or very frequent symptoms and 63% reported rare or occasional symptoms. Most respondents (63%) reported that the hemorrhoid episode lasted <1 week, while 25% had episodes lasting between 1 week and 1 month and 12% had episodes lasting ≥1 month. Symptoms were unrelated to the time of year in 71% of respondents and when they were seasonal, there was no particular season in which hemorrhoid symptoms were more likely to occur (reported in 9% of respondents in spring, 11% in summer or autumn and 13% in winter).
Compared with the overall population of individuals with hemorrhoidal disease, the proportion of respondents with low severity disease was significantly higher in Russia (76%) and the proportion with high severity disease was significantly higher in Romania (19%; Table 2). The mean number of pregnancies was significantly higher in Hungarian women (2.28) and significantly lower in Russian (1.77) and Romanian (1.74) women than in the overall cohort of women with hemorrhoidal disease (1.93). The proportion of respondents experiencing a high frequency of symptoms was significantly higher in Italy (47%) and Brazil (50%) and significantly lower in the Czech Republic (35%), than in the overall population (42%). A family history of hemorrhoidal disease was significantly more common in Italy (77%) and significantly less common in Romania (51%) and Czech Republic (46%).
| Characteristics | France (n = 139), n (%) | Italy (n = 327), n (%) | Spain (n = 227), n (%) | Brazil (n = 121), n (%) | Russia (n = 319), n (%) | Romania (n = 201), n (%) | Hungary (n = 204), n (%) | Czech Republic (n = 187) | Total (n = 1725), n (%) |
|---|---|---|---|---|---|---|---|---|---|
| Family history of hemorrhoidal disease: | |||||||||
| Yes | 84 (60) | 253 (77)† | 154 (68) | 77 (64) | 217 (68) | 102 (51)† | 136 (67) | 86 (46)† | 1109 (64) |
| No | 24 (17) | 36 (11)† | 35 (15) | 22 (18) | 32 (10)† | 38 (19) | 16 (8)† | 54 (29)† | 257 (15) |
| Do not know | 31 (22) | 38 (12)† | 38 (17) | 22 (18) | 70 (22) | 61 (30)† | 52 (25) | 47 (25) | 359 (21) |
| Disease severity: | |||||||||
| Low | 92 (66) | 219 (67) | 154 (68) | 89 (74) | 242 (76)† | 140 (70) | 143 (70) | 139 (74) | 1218 (71) |
| Medium | 30 (22) | 69 (21)† | 46 (20)† | 11 (9)† | 39 (12) | 22 (11)† | 34 (17) | 15 (8)† | 266 (15) |
| High | 17 (12) | 39 (12) | 27 (12) | 21 (17) | 38 (12) | 39 (19)† | 27 (13) | 23 (18) | 241 (14) |
| Number of pregnancies: | |||||||||
| Mean ± SD | 2.07 ± 0.9 | 1.88 ± 0.9 | 1.93 ± 0.8 | 2.16 ± 1.0 | 1.77† ± 0.8 | 1.74† ± 0.8 | 2.28† ± 1.2 | 1.93 ± 0.8 | 1.93 ± 0.9 |
| Median | 1.47 | 1.32 | 1.34 | 1.29 | 1.16 | 1.03 | 1.54 | 1.48 | 1.35 |
| Time to first hemorrhoid symptoms: | |||||||||
| <1 year | 14 (10)† | 41 (13) | 69 (30)† | 24 (20) | 32 (10) | 33 (16) | 19 (9)† | 31 (17) | 263 (15) |
| 1–<5 years | 75 (54)† | 137 (42) | 73 (32)† | 56 (46) | 133 (42) | 83 (41) | 72 (35) | 78 (42) | 707 (41) |
| ≥5 years | 50 (36)† | 149 (46) | 85 (37)† | 41 (34)† | 154 (48) | 85 (42) | 113 (55)† | 78 (42) | 755 (44) |
| Symptom frequency: | |||||||||
| Rarely or occasionally | 76 (55) | 152 (46) | 114 (50) | 49 (40)† | 166 (52) | 115 (57) | 102 (50) | 104 (56) | 878 (51) |
| Constantly | 9 (6) | 20 (6) | 16 (7) | 11 (9) | 21 (7) | 12 (6) | 23 (11) | 18 (10) | 130 (8) |
| Frequently or very frequently | 54 (39) | 155 (47)† | 97 (43) | 61 (50)† | 132 (41) | 74 (37) | 79 (39) | 65 (35)† | 717 (42) |
| Season when symptoms occur: | |||||||||
| Spring | 21 (15) | 39 (12) | 28 (12) | 11 (9) | 42 (13) | 24 (12) | 11 (5)† | 15 (8) | 191 (11) |
| Summer | 20 (14) | 57 (17)† | 47 (21)† | 31 (26)† | 25 (8)† | 24 (12) | 8 (4)† | 22 (12) | 234 (14) |
| Autumn | 26 (19) | 45 (14) | 30 (13) | 9 (7)† | 53 (17) | 23 (11) | 26 (13) | 31 (17) | 243 (14) |
| Winter | 22 (16) | 53 (16) | 27 (12) | 15 (12) | 37 (12)† | 29 (14) | 43 (21)† | 15 (19) | 261 (15) |
| Regardless of season | 98 (71) | 212 (65) | 146 (64) | 79 (65) | 237 (74)† | 138 (69) | 145 (71) | 125 (67) | 1180 (68) |
| Typical duration of episode: | |||||||||
| <1 week | 87 (63) | 192 (59) | 134 (59) | 75 (62) | 203 (64) | 146 (73)† | 134 (66) | 118 (63) | 1089 (63) |
| 1–4 weeks | 38 (27) | 101 (31)† | 70 (31)† | 28 (23) | 76 (24) | 38 (19)† | 44 (22) | 38 (20) | 433 (25) |
| >4 weeks | 14 (10) | 34 (10) | 23 (10) | 18 (15) | 40 (13) | 17 (8) | 26 (13) | 31 (17) | 203 (12) |
†
p < 0.05 vs total population.
SD: Standard deviation.
Treatment pathways
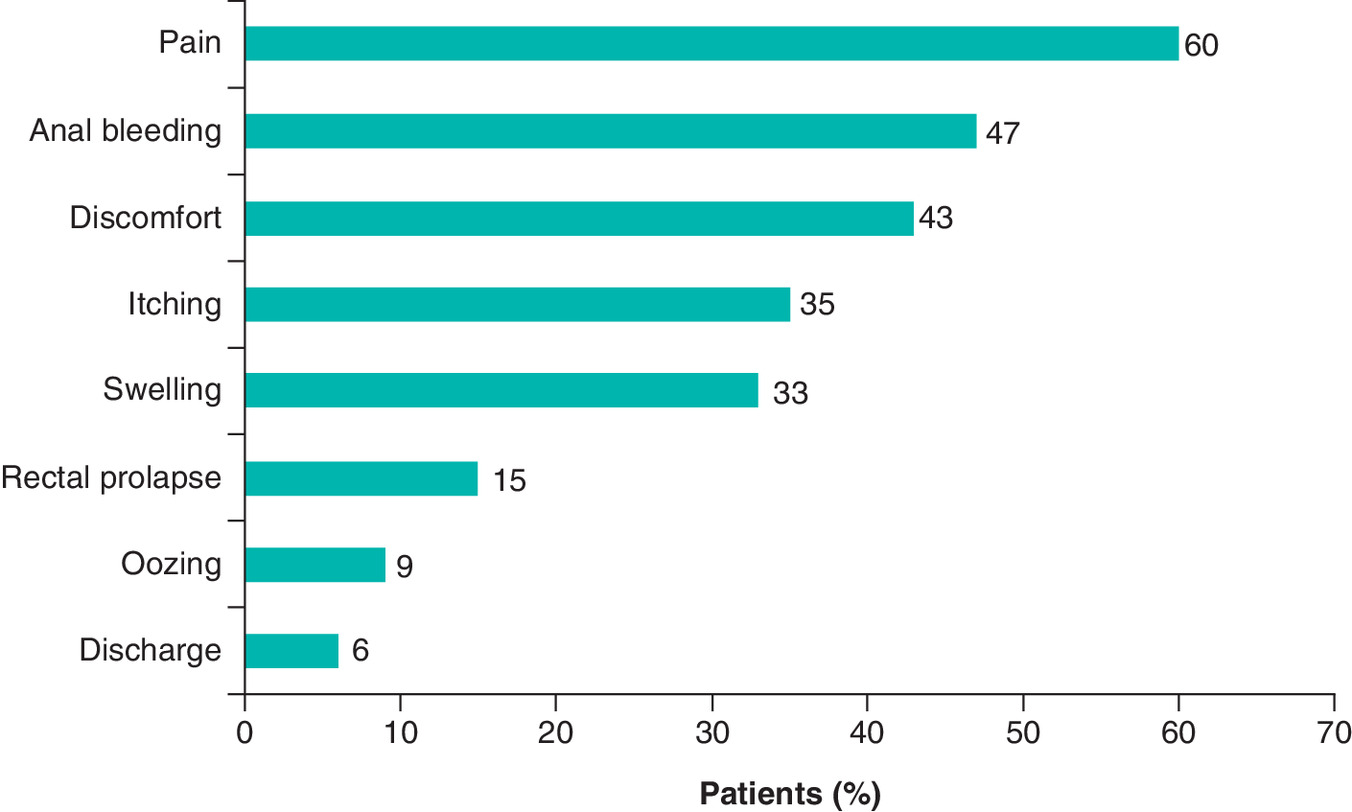
After enrichment of the study population, 3812 individuals with hemorrhoidal disease participated in the analysis of treatment pathways. The most common signs and symptoms experienced by these individuals before seeking treatment were pain (60%), anal bleeding (47%), discomfort (43%), itching (35%) and swelling (33%; Figure 1). Overall, 2961 respondents (77.7%) stated that their hemorrhoid diagnosis was confirmed by a general practitioner (GP) or family doctor in 38%, gastroenterologist or proctologist in 20%, retail pharmacist in 12%, unknown in 10%, surgeon in 7%, gynecologist in 4%, nurse in 3%, midwife in 2%, another physician in 2% and a physiotherapist in 1%).
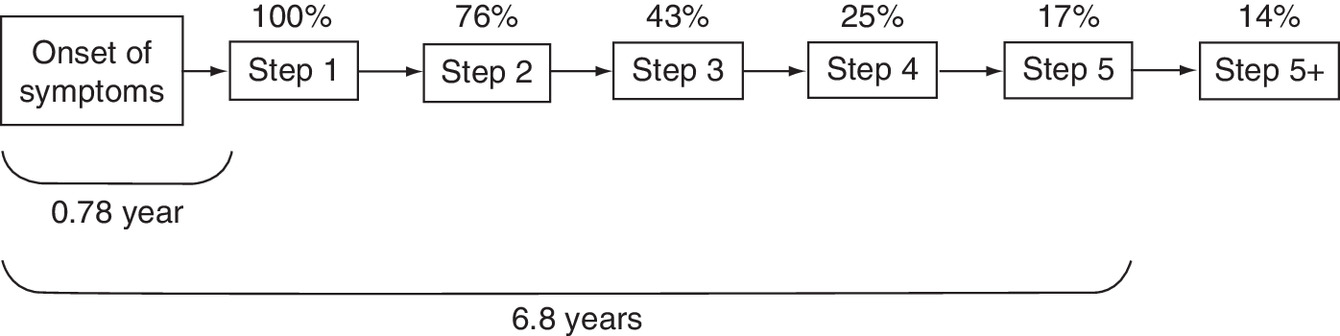
Of the 3812 individuals with hemorrhoidal disease, all had undertaken at least one step in the treatment pathway, with 76% having undertaken at least two steps. The proportion of respondents declined at each step, such that 17% had undertaken five steps and 14% had undertaken more than five (Figure 2). The mean number of steps was 2.4. The mean time from the onset of hemorrhoid symptoms to step 1 was 0.8 years and the mean time to step 5 was 6.8 years. The treatment pathway was stopped after step 3 in 75% of respondents.
Across all steps, healthcare professionals (mainly GPs or family doctors) were the most common source of information about hemorrhoidal disease (Figure 3). The first treatment step was to seek information or advice about treatment options and to do this, 41% of respondents consulted a physician, 22% sought information by themselves, 16% asked relatives, friends or colleagues, 13% consulted a retail pharmacist, 5% consulted a paramedical professional and 3% asked a consultant of a healthcare store or a seller in a specialized store for advice. Of the online sources of information, medical websites were the most commonly used (62%), followed by forums (36%), blogs, medically oriented publications and product websites (18% for all), pharmaceutical company websites (13%), Facebook (5%) and other (2%).
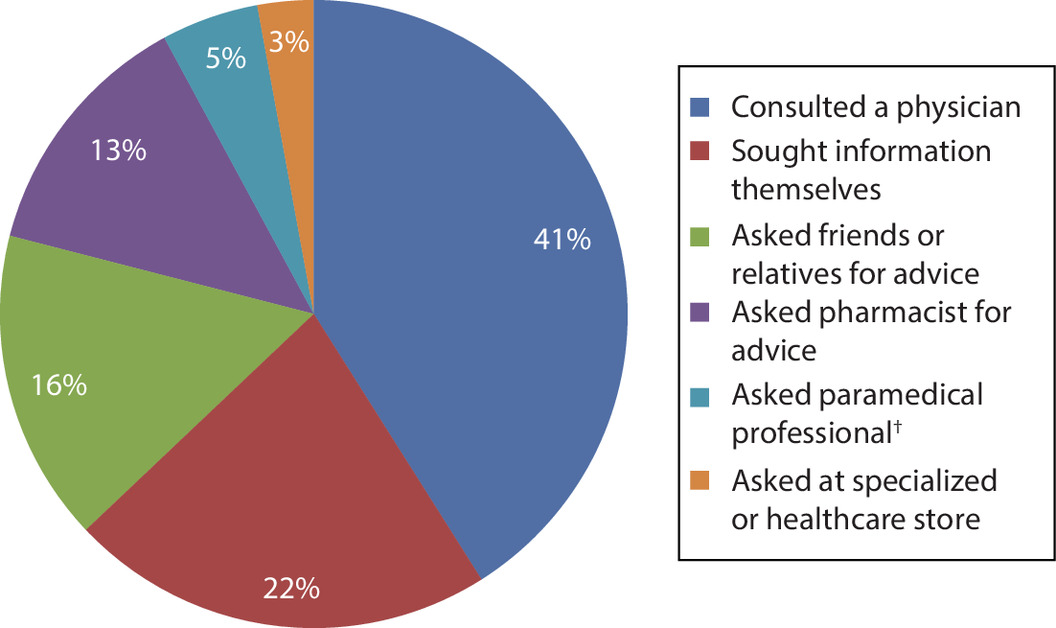
Figure 3. Sources of information used by respondents with hemorrhoidal disease at the first treatment step.
†Paramedical specialists included physiotherapists, nurses and midwives.
Between 69 and 75% of respondents with hemorrhoidal disease were advised to make lifestyle changes or use non-pharmacological approaches at each step in the treatment pathway. Among nonpharmacological therapies and lifestyle changes, the most frequently reported was a change in diet (food or hydration, no spicy food) in 48% (Table 3).
| Therapies | Step 1 (n = 2988), n (%) | Step 2 (n = 2087), n (%) | Step 3 (n = 1100), n (%) | Step 4 (n = 620), n (%) | Step 5 (n = 398), n (%) |
|---|---|---|---|---|---|
| Nonmedical treatments and lifestyle changes: | 2168 (73)† | 1437 (69)† | 760 (69) | 463 (75)† | 297 (75) |
| Diet (food, hydration, avoid spicy food) | 1502 (50)† | 947 (45)† | 508 (46) | 298 (48) | 182 (46) |
| Physical activity | 600 (20)† | 513 (25) | 295 (27)† | 192 (31)† | 138 (35)† |
| Behavior changes (posture, skin hygiene, avoid carrying heavy objects) | 636 (21)† | 473 (23) | 260 (24) | 167 (27)† | 106 (27) |
| Hip baths ± ice cubes | 643 (22)† | 355 (17)† | 193 (18) | 120 (19) | 83 (21) |
| Medicinal products and drugs: | 2705 (91)† | 1735 (83)† | 880 (80)† | 500 (81)† | 314 (79)† |
| Cream/ointment/gel | 2082 (70)† | 1158 (55)† | 585 (53)† | 306 (49)† | 192 (48)† |
| Oral venoactive drugs (tablet, oral solution, capsules, ampoules) | 536 (18)† | 419 (20) | 208 (19) | 126 (20) | 88 (22) |
| Venoactive drugs by suppository | 458 (15) | 275 (13)† | 164 (15) | 102 (16) | 76 (19)† |
| Food supplements | 309 (10)† | 254 (12) | 160 (15)† | 95 (15)† | 56 (14) |
| Other agents (e.g., analgesics) | 310 (10) | 227 (11) | 126 (11) | 81 (13) | 47 (12) |
| Nonvenoactive drugs by suppository | 297 (10) | 199 (10) | 113 (10) | 64 (10) | 39 (10) |
| Phytotherapy/homeopathy | 174 (6)† | 140 (7) | 89 (8) | 68 (11)† | 36 (9) |
| Interventions | 203 (7)† | 178 (9) | 112 (10)† | 64 (10) | 41 (10) |
†
p < 0.05 vs total hemorrhoid population (all steps combined).
Medicinal product use was reported in 79–91% of respondents at each treatment step, but most commonly at step 1. Among medicinal products and drugs, creams, ointments and gels were used by 60% of respondents at any step in the treatment, but 70% used these agents at step 1 and use of topical agents declined in subsequent steps to 55% at step 2, 53% at step 3, 49% at step 4 and 48% at step 5 (Figure 4). Oral VADs were used by 19% of respondents and VAD suppositories by 15% at any step (Figure 4).
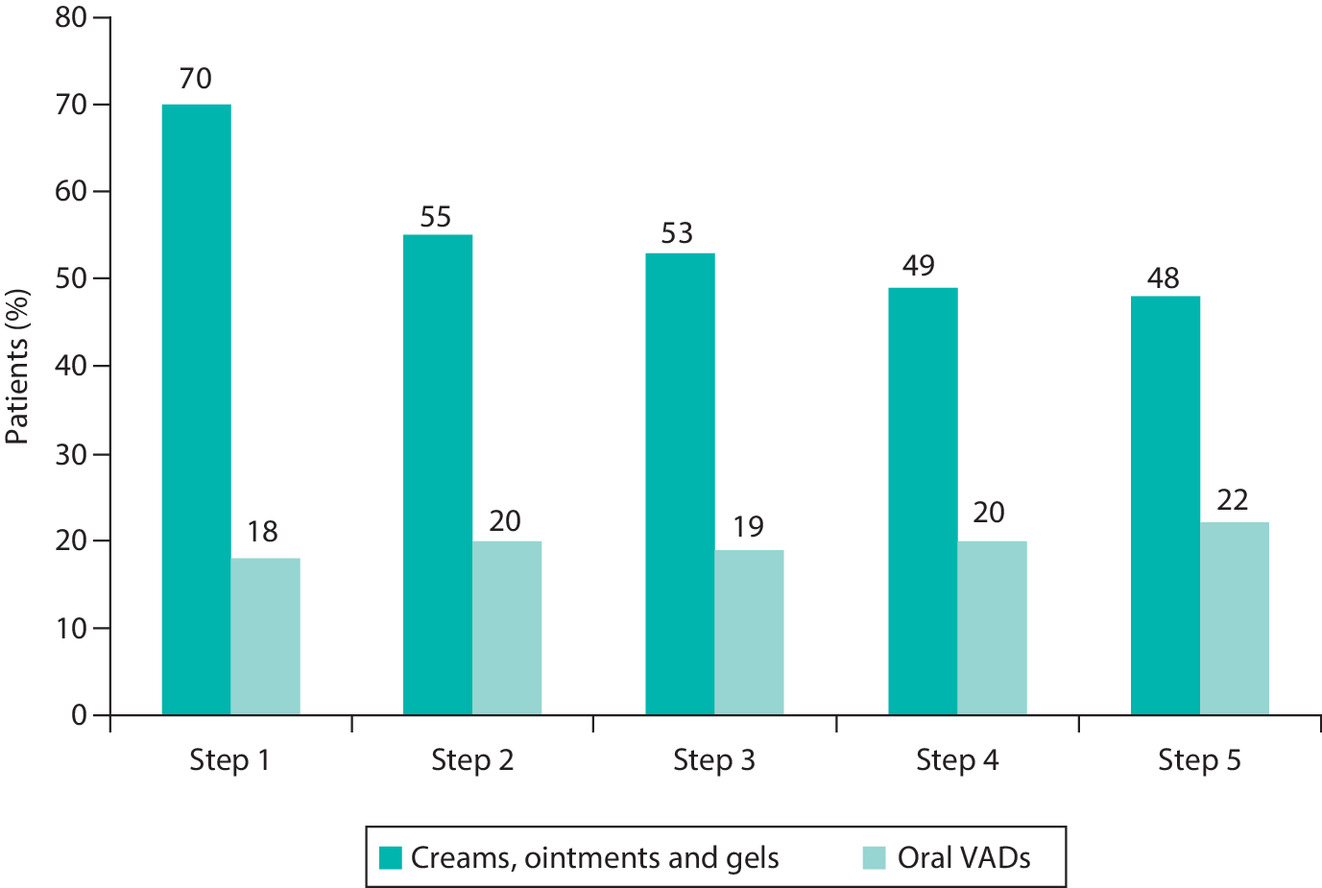
Figure 4. Proportion of respondents who used topical medicinal products and oral venoactive drugs.
VAD: Venoactive drug.
Throughout steps 1–5, the median treatment durations were longer with oral VADs (2.76 weeks) than with creams (1.85 weeks) but shorter than with food supplements (3.43 weeks). Use of creams was more frequent during the earlier treatment steps and decreased over time, whereas the use of VADs and food supplements was lower than creams but relatively constant up to step 4. Approximately a third of participants who used creams also used oral VADs (29%). Over half of participants who used oral VADs also used creams (55%). Of the participants who used food supplements, 63% also used creams and 55% used oral VADs.
Of the 3812 individuals with hemorrhoidal disease in this analysis, 30% had undergone colonoscopy. The proportion of respondents who had a colonoscopy was significantly higher than 30% in France and the Czech Republic, where 41 and 44% of respondents, respectively, had colonoscopy and significantly lower in Romania, where 19% had colonoscopy.
Four common treatment pathways were identified based on the person from whom respondents first sought help with their condition (Table 4); the characteristics of respondents differed between treatment pathways. Compared with the overall population of individuals with hemorrhoidal disease, respondents who sought help from a physician were significantly older and were more likely to undergo intervention for hemorrhoidal disease. On the other hand, respondents who sought information themselves or asked friends, relatives or colleagues for help included a higher proportion of young respondents (aged 18–40 years), had fewer comorbidities on average and were less likely to take medication or undergo interventions compared with the overall population. Those who sought information from a retail pharmacist were more likely to take medicinal products compared with the overall group of individuals with hemorrhoidal disease.
| Consulted a physician, n (%) | Sought information on his/her own, n (%) | Asked relatives/friends/ colleagues for advice, n (%) | Consulted a retail pharmacist, n (%) | Total, n (%) | |
|---|---|---|---|---|---|
| Characteristics | n = 1553 | n = 846 | n = 609 | n = 499 | n = 3812 |
| Country: | |||||
| France | 230 (15)‡ | 100 (12) | 47 (8)‡ | 66 (13) | 475 (12) |
| Italy | 548 (35)‡ | 158 (19)‡ | 172 (28) | 197 (39)‡ | 1159 (30) |
| Spain | 274 (18) | 110 (13)‡ | 155(25)‡ | 89 (18) | 705 (18) |
| Brazil | 180 (12) | 102 (12) | 65 (11) | 26 (5)‡ | 401 (11) |
| Russia | 121 (8)‡ | 180 (21)‡ | 89 (15) | 31 (6)‡ | 461 (12) |
| Romania | 64 (4)‡ | 72 (9)‡ | 16 (3)‡ | 46 (9)‡ | 215 (6) |
| Hungary | 73 (5) | 64 (8)‡ | 34 (6) | 21 (4) | 204 (5) |
| Czech Republic | 63 (4)‡ | 60 (7)‡ | 31 (5) | 23 (5) | 192 (5) |
| Mean age (years) | 46.07‡ | 42.83‡ | 40.22‡ | 44.32 | 43.67 |
| Age categories: | |||||
| 18–40 years | 571 (37)‡ | 400 (47)‡ | 332 (55)‡ | 210 (42) | 1686 (44) |
| 41–60 years | 754 (49)‡ | 366 (43) | 246 (40)‡ | 237 (47) | 1720 (45) |
| >60 years | 228 (15)‡ | 80 (9)‡ | 31 (5)‡ | 52 (10) | 406 (11) |
| BMI categories: | |||||
| Normal (<25 kg/m2) | 759 (49) | 410 (48) | 316 (52) | 258 (52) | 1909 (50) |
| Overweight (25–29 kg/m2) | 515 (33) | 276 (33) | 192 (32) | 146 (29) | 1224 (32) |
| Obese (>30 kg/m2) | 279 (18) | 160 (19) | 101(17) | 95 (19) | 679 (18) |
| Comorbidities: | |||||
| Hypertension | 503 (32) | 249 (29) | 164 (27)‡ | 150 (30) | 1157 (30) |
| Depression | 420 (27)‡ | 238 (28) | 168 (28) | 118 (24) | 1032 (27) |
| Diabetes (Type I or II) | 207 (13)‡ | 77 (9)‡ | 59 (10) | 52 (10) | 440 (12) |
| Mean number of comorbidities | 3.07 | 2.90‡ | 2.88‡ | 2.94 | 3.01 |
| Treatments | n = 3087† | n = 1333† | n = 1137† | n = 977† | n = 7193† |
| Hemorrhoid therapy: | |||||
| Nonmedical treatments and lifestyle changes | 2244 (73)‡ | 928 (70) | 793 (70) | 654 (67)‡ | 5125 (71) |
| Medicinal products and drugs | 2656 (86) | 1110 (83)‡ | 935 (82)‡ | 864 (88)‡ | 6134 (85) |
| Interventions | 344 (11)‡ | 72 (5)‡ | 52 (5)‡ | 57 (6)‡ | 598 (8) |
†
N-value refers to the number of individuals who reported this step at any time during their treatment pathway, for example, all respondents who consulted a physician during first, second, third or later step in the treatment pathway.
‡
p < 0.05 vs total hemorrhoid population.
SD: Standard deviation.
Discussion
In this international online survey study, the prevalence of hemorrhoidal disease in the general population was 11%. Individuals with hemorrhoidal disease were generally middle-aged (average 46 years) and had a family history of this condition. Women were slightly over-represented in the hemorrhoid population compared with men (56 vs 44%), and most women (81%) affected by hemorrhoidal disease had a history of pregnancy (average of 1.9 pregnancies each). In most respondents (71%), hemorrhoidal disease were of mild severity with no prolapse (Grade 1), while 14% of respondents had permanent and irreducible prolapse (Grade 4). Hemorrhoidal disease generally occurred periodically, with no seasonal pattern and most episodes (63%) lasted <1 week. Only 6% of respondents had constant symptoms of hemorrhoidal disease. However, 85% of respondents had been experiencing hemorrhoidal episodes for >1 year and 44% had been experiencing them for ≥5 years.
The prevalence of hemorrhoidal disease reported in this multinational survey is within the range (4–17%) reported in other studies conducted in the general populations of the USA, Spain and Japan [8–10].
Although hemorrhoidal disease is common in clinical practice, published data on symptom and treatment patterns are limited. One of the few studies presenting such data is a natural history study by Jensen and colleagues (1989) describing hemorrhoid presentation in 189 patients with grade 2 hemorrhoidal disease [13]. The mean age of patients in that study (46–50 years) was very similar to the present study [13], and consistent with data showing that the peak age for hemorrhoid development is between 45 and 65 years [8]. Jensen and colleagues found a slight predominance of men in their hemorrhoid population (54%) [13], whereas we found a slight preponderance of women. Other epidemiological analyses suggest that neither sex is at greater risk of developing hemorrhoidal disease than the other [8]. Analysis of the hemorrhoid treatment pathway showed that pain, anal bleeding and discomfort were the most common first symptoms leading patients to seek treatment, and most patients sought treatment within the first 12 months of experiencing symptoms. The high incidence of pain (60%) reported by individuals with hemorrhoidal disease, in our study, is somewhat surprising since the earlier study of the natural history of hemorrhoidal disease by Jensen and colleagues suggests that only approximately 30% of patients with grade 2 hemorrhoidal disease experience pain [13]. Bleeding is the most commonly reported symptom of hemorrhoidal disease in most publications. The previously described natural history study reported anal bleeding in approximately 90% of patients with grade 2 disease [13] and a retrospective analysis of US patients with hemorrhoidal disease noted that 60% reported bleeding at diagnosis [14]. In contrast, bleeding was reported by fewer than half of the respondents in our survey. On the other hand, itching was reported by 35% of participants in our study, whereas only 19% of patients in the natural history study reported itching [13]. Consistent with previous studies [13], our data show that discharge is an uncommon symptom of hemorrhoidal disease, occurring in <10% of respondents.
The difference in the symptom reporting rate between our study and earlier ones may be related to a number of issues. First, the current survey included individuals with hemorrhoidal disease of any severity and 29% of respondents had a prolapse of some kind and 14% had permanent prolapse (Grade 4 disease). In contrast, the natural history study by Jensen and colleagues was limited to patients with grade 2 hemorrhoidal disease in whom prolapse spontaneously and immediately reverted [13]. Therefore, our survey included individuals who had more severe hemorrhoidal disease and, as a result, were more likely to experience pain. Second, our survey used a multiple-choice format to ask participants about their symptoms, which may have prompted them to report pain, thus leading to a higher incidence. Analyses of methods to elicit adverse event information suggest that questioning patients about specific events or symptoms usually results in higher rates of reporting than open-ended questions that rely on patients spontaneously reporting that event [15,16]. A similar effect may be at play in surveys using multiple-choice questions to elicit symptom information.
Our data show that, although more individuals with hemorrhoidal disease will seek information from a doctor than from other sources, only about 40% of them seek help from a medical practitioner as their first step in the treatment pathway. This is consistent with previous data showing that many patients with hemorrhoidal disease will not necessarily disclose this information to their family doctor [6,7]. The reasons for this are unclear, but patient embarrassment or concerns that nothing can be done to relieve hemorrhoidal disease may contribute to patients’ reluctance to consult a health professional.
There were differences in treatment patterns for hemorrhoidal disease between countries; for example, respondents in eastern Europe were generally less likely to consult a physician at step 1 in the treatment pathway, and more likely to seek information on their own. In Russia, this treatment pathway may be explained by the high proportion of respondents with low-severity disease, but is somewhat surprising in Romania and the Czech Republic, which had the lowest proportion of respondents with low-severity disease. Survey participants in Italy and Romania were significantly more likely to consult a retail pharmacist for advice as their first treatment step.
The types of treatments respondents received were largely consistent with current guidelines for low- to moderate-severity disease [17–21]. These guidelines recommend dietary intervention (increased fiber and fluid intake) as the first key step in the management of symptomatic grade 1 or 2 hemorrhoidal disease [17–21]. While a high proportion of participants in our survey used nonmedicinal treatments and lifestyle changes at all steps in the treatment pathway, only half undertook dietary changes. VADs are also recommended in guidelines for the relief of symptoms, regardless of disease severity; surgical interventions are recommended only in patients with grade 3 or 4 hemorrhoidal disease or those with lower grade disease who are unable to achieve adequate symptom relief with medication and lifestyle changes and who do not respond to office-based procedures such as rubber band ligation [17–21]. Consistent with these recommendations, topical preparations and VADs, administered orally or by suppository, were the most common form of medical treatment undertaken by respondents in our survey. The frequent use of topical therapy in our study was consistent with previous data from France showing that topical treatment is the most commonly prescribed treatment for hemorrhoidal disease in primary care [7]. This is despite the fact that topical therapy has a limited role in hemorrhoid treatment, according to most guidelines, although topical agents can help to relieve skin irritation around the anus in patients with mild hemorrhoidal disease [17,19].
The strengths of the present study include the fact that it was conducted in a large and representative sample of the general population and that it examined multiple demographic and clinical characteristics relevant to hemorrhoidal disease across a range of countries. We used random sampling to limit the potential for responder/nonresponder bias.
A limitation of the present study was the fact that, as a survey, it relied on participant self-report, which by its nature relied on the respondents’ subjective interpretation of terms, for example, of the term ‘discomfort’ and in addition, self-report may be subject to response bias (tailoring responses according to expectations or social desirability of responses) and recall bias [22]. By providing responders with multiple choice answers, the survey format ran the risk of them over-reporting symptoms (e.g., pain) compared with research that relies on spontaneous self-report. Our survey did not confirm the hemorrhoid diagnosis against responders’ medical records, so there is a potential for overestimation of the prevalence because patients are prone to attribute any anal symptoms to hemorrhoidal disease [18,23]. However, we consider this to be unlikely since the survey provided detailed definitions of hemorrhoid severity, in terms of both specific symptoms and signs, including the presence and reducibility of prolapse. In addition, the fact that the prevalence of hemorrhoidal disease in our study, both in the overall population and in each individual country, lies completely within the range reported in the published literature suggests that overestimation, if present, was not marked. However, another limitation is that, because we did not have access to the patients’ medical records, we cannot determine whether the high incidence of pain was related to coexisting painful conditions, such as anal fissure.
Conclusion
In this online survey study, the prevalence of hemorrhoidal disease in the adults was 11%, but most respondents had low severity episodic disease. Only about 40% of respondents with hemorrhoidal disease sought help from a medical practitioner as the first step in the treatment pathway, highlighting a pattern of under diagnosis and under treatment, as well as the need for respondents to be able to access reliable and accurate health information from other sources. These findings highlight the need for greater education of individuals with hemorrhoidal disease to seek medical advice for early diagnosis and treatment, as well as education for family practitioners to thoroughly investigate hemorrhoidal symptoms. Patient education should include reducing the taboo around rectal conditions, so that reluctance and embarrassment do not delay medical assessment. Any rectal bleeding, which patients are likely to attribute to hemorrhoidal disease [18], needs to be promptly investigated to exclude other more serious conditions, such as inflammatory bowel disease or cancer [17]. Therefore, prompt assessment at the first signs of hemorrhoidal disease will not only provide early symptom relief for patients but may also assist in early colorectal cancer detection. GPs should also receive education on guideline-recommended treatments, so that patients receive the most effective protocol available rather than relying on empirical treatment with poorly effective therapies.
•
Hemorrhoidal disease is one of the most common anorectal conditions seen in general practice, but the true prevalence in the general population is not well understood, partly because many patients do not seek treatment.
•
A large international web-based survey was undertaken of 16,015 adults in Brazil, Czech Republic, France, Hungary, Italy, Romania, Russia and Spain.
•
Based on self-reported signs and symptoms, the estimated prevalence of hemorrhoidal disease was 11%.
•
Compared with the general population, individuals with hemorrhoidal disease were generally older and had more comorbidities, and included a higher proportion of females, including women who had been pregnant.
•
Hemorrhoidal disease was mostly mild or moderate in severity and of >1 year’s duration.
•
The most common signs and symptoms before seeking treatment were pain, anal bleeding, discomfort, itching and swelling.
•
Symptoms were mostly sporadic (only 6% had constant symptoms), with most episodes lasting <1 week.
•
Consulting a physician was the most popular initial option, but most respondents also sought information elsewhere.
•
Lifestyle modifications and medicinal products were the most frequent management approaches; the most common types of medicinal products used were creams, ointments and gels.
•
Participant characteristics and treatment patterns varied across countries.
Author contributions
G Salmat was involved in the data processing of the study, statistical calculations, checking the accuracy of the data and review and approval of manuscript drafts on statistical topics. F Goron was involved in the conception and study design, participant enrolment, data analysis, report writing, review and approval of manuscript drafts, including checking the accuracy of the data. C Regnier was involved in the conception and design of the study, reading and revising the manuscript drafts and approval of the final manuscript. P Sheikh was involved in reviewing the study results, reading and revising the manuscript drafts and approval of the final manuscript.
Acknowledgments
We would like to thank C Rees, G Filatov and T Harrison of Springer Healthcare Communications who wrote the outline, first draft and provided editorial assistance on postsubmission revisions of this manuscript, respectively.
Financial & competing interests disclosure
P Sheikh has received lecture fees from Servier. F Goron and G Salmat are employees of Harris Interactive (France). C Regnier is an employee of Servier International. The study was funded by Servier. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing assistance was funded by Servier.
Ethical conduct of research
Participants provided informed consent prior to completing the survey. As this was not an investigation of clinical outcomes with any particular intervention, neither Ethics Committee approval nor clinical trial registration was required. Harris Interactive Europe is a full service, consultative custom market research agency. We comply with the Quality and Professional Code of Ethics published by Syntec Etudes and the ICC/ESOMAR International Code on Market, Opinion and Social Research and Data Analytics and other applicable guidelines and codes of conduct on market research. Harris Interactive uses market research industry standards, techniques and methodologies to ensure that respondents to market research studies are kept anonymous and the results are provided on an aggregated basis. Harris Interactive, its hosting and backup services and any third-party suppliers are fully compliant with the General Data Protection Regulation 2016/679 (GDPR). Harris Interactive only accepts personal data via secure encrypted transfer protocols such as sFTP sites. Data will only be processed for the purposes for which they were provided and for no other reason. Access to the data is restricted to predefined and tightly controlled groups of employees on a ‘need to know’ basis only. The healthcare department is also member of ASOCS and follows the EPHMRA regulation (without being member). All data are located on a single secure server (never transferred) and none of the data can be personally identifiable. This includes personal socio-demographic data (gender, age, geography defined in zones and not at a finer level) which the respondent gave his/her consent for use in a conglomerate and anonymized manner. All people completing surveys on health-related matters are asked a health consent question to make sure that the person knows that health questions will be asked and that they accept this condition before completing the questionnaire. These data are always collected on an anonymized basis. No information that can precisely identify the person is possible. The data are available to the sponsor for a maximum of 2 to 3 years after the end of the study for possible additional research requests or realization of barometric monitoring. At the end of this time, the database undergoes automatic destruction.
Data sharing statement
Data are available on request from Harris interactive (F Goron and G Salmat).
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 59.99 KB
References
Papers of special note have been highlighted as: • of interest
1.
Acheson AG, Scholefield JH. Management of haemorrhoids. BMJ 336(7640), 380–383 (2008).
• Provides a review of the literature on the management of hemorrhoids.
2.
Lohsiriwat V. Hemorrhoids: from basic pathophysiology to clinical management. World J. Gastroenterol. 18(17), 2009–2017 (2012).
3.
Caglayan M, Turkoglu A, Oktayoglu P et al. Evaluation of the incidence of haemorrhoidal disease in patients with ankylosing spondylitis. Clin. Rheumatol. 34(3), 511–514 (2015).
4.
Negri E, Pagano R, Decarli A, La Vecchia C. Body weight and the prevalence of chronic diseases. J. Epidemiol. Community Health 42(1), 24–29 (1988).
5.
Ravindranath GG, Rahul BG. Prevalence and risk factors of hemorrhoids: a study in a semi-urban centre. Int. J. Surg. 5(2), 496–499 (2018).
6.
Tournu G, Abramowitz L, Couffignal C et al. Prevalence of anal symptoms in general practice: a prospective study. BMC Fam. Pract. 18(1), 78 (2017).
7.
Abramowitz L, Benabderrahmane M, Pospait D, Philip J, Laouenan C. The prevalence of proctological symptoms amongst patients who see general practitioners in France. Eur. J. Gen. Pract. 20(4), 301–306 (2014).
8.
Johanson JF, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology 98(2), 380–386 (1990).
9.
Violan C, Foguet-Boreu Q, Hermosilla-Perez E et al. Comparison of the information provided by electronic health records data and a population health survey to estimate prevalence of selected health conditions and multimorbidity. BMC Public Health 13, 251 (2013).
10.
Asakura K, Nakano M, Omae K. Relationship between bidet toilet use and haemorrhoids and urogenital infections: a 3-year follow-up web survey. Epidemiol. Infect. 146(6), 763–770 (2018).
11.
Mao L, Ma L, Liu N et al. Self-reported health problems related to traditional dietary practices in postpartum women from urban, suburban and rural areas of Hubei province, China: the ‘zuo yuezi’. Asia Pac. J. Clin. Nutr. 25(1), 158–164 (2016).
12.
Poskus T, Buzinskiene D, Drasutiene G et al. Haemorrhoids and anal fissures during pregnancy and after childbirth: a prospective cohort study. BJOG 121(13), 1666–1671 (2014).
13.
Jensen SL, Harling H, Arseth-Hansen P, Tange G. The natural history of symptomatic haemorrhoids. Int. J. Colorectal Dis. 4(1), 41–44 (1989).
14.
Trilling JS, Robbins A, Meltzer D, Steinbardt S. Hemorrhoids: associated pathologic conditions in a family practice population. J. Am. Board Fam. Pract. 4(6), 389–394 (1991).
15.
Allen EN, Chandler CI, Mandimika N, Leisegang C, Barnes K. Eliciting adverse effects data from participants in clinical trials. Cochrane Database Syst. Rev. 1, MR000039 (2018).
• This is a Cochrane systematic review of studies that compared various methods (open questions, checklist, interview) of eliciting adverse event information from clinical trial participants.
16.
Chrysant SG. Proactive compared with passive adverse event recognition: calcium channel blocker-associated edema. J. Clin. Hypertens. (Greenwich) 10(9), 716–722 (2008).
17.
Clinical Practice Committee, American Gastroenterological Association. American Gastroenterological Association medical position statement: diagnosis and treatment of hemorrhoids. Gastroenterology 126(5), 1461–1462 (2004).
• Position statement of the American Gastroenterological Association on the diagnosis and treatment of hemorrhoidal disease.
18.
Altomare DF, Roveran A, Pecorella G, Gaj F, Stortini E. The treatment of hemorrhoids: guidelines of the Italian Society of Colorectal Surgery. Tech. Coloproctol. 10(3), 181–186 (2006).
• Guidelines on the treatment of hemorrhoidal disease from the Italian Society of Colorectal Surgery.
19.
Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis. Colon Rectum 61(3), 284–292 (2018).
• Guidelines on the management of hemorrhoidal disease from the American Society of Colon and Rectal Surgeons.
20.
Rivadeneira DE, Steele SR, Ternent C, Chalasani S, Buie WD, Rafferty JL. Practice parameters for the management of hemorrhoids (revised 2010). Dis. Colon Rectum 54(9), 1059–1064 (2011).
21.
Van Tol RR, Kleijnen J, Watson AJM et al. European Society of ColoProctology: guideline for haemorrhoidal disease. Colorectal Dis. 22(6), 650–662 (2020).
• Clinical practice guidelines from the European Society of ColoProctology on the diagnosis and treatment of hemorrhoidal disease.
22.
Choi BC, Pak AW. A catalog of biases in questionnaires. Prev. Chronic Dis. 2(1), A13 (2005).
23.
Villalba H, Abbas MA. Hemorrhoids: modern remedies for an ancient disease. Perm. J. 11(2), 74–76 (2007).

Information & Authors
Information
Published In
Pages: 1219 - 1232
PubMed: 33079605
Copyright
© 2020 Parvez Sheikh. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 28 July 2020
Accepted: 11 September 2020
Published online: 20 October 2020
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The prevalence, characteristics and treatment of hemorrhoidal disease: results of an international web-based survey. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0159
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Gaetano Gallo, Antonella Salvatore, Giovanni Tomasicchio, Alberto Realis Luc, Arcangelo Picciariello, Angelo Di Vittori, Mario Trompetto, Marcella Rinaldi, Use of mesoglycan in the acute phase of hemorrhoidal disease, the aCute HaemORrhoidal MEsoglycan Study (CHORMES): A double-blind, randomized controlled trial, Surgery, 10.1016/j.surg.2026.110402, 198, (110402), (2026).
- Mohammad Dehbozorgi, Hooman Rezaei, Maryam Shahbazi, Kimia Falamarzi, Evaluating the role of preemptive intravenous ketorolac in preventing post-operative pain in patients undergoing hemorrhoidectomy: A randomized clinical trial, The Surgeon, 10.1016/j.surge.2025.11.008, 24, 4, (267-270), (2026).
- Eremeev Spiridon, Cristian Ichim, Paula Anderco, Ciprian Tanasescu, Radiofrequency Ablation for Hemorrhoidal Disease, Life, 10.3390/life16061025, 16, 6, (1025), (2026).
- Wei Zhang, Zhengfei Han, Qiang Lu, Effects of Transcutaneous Electrical Acupoint Stimulation Combined With Propofol–Sufentanil Intravenous Anesthesia on Perioperative Analgesia and Stress Response in Patients Undergoing Mixed Hemorrhoid Surgery, Acupuncture & Electro-Therapeutics Research: International Journal of Integrated Medicine, 10.1177/03601293261461851, (2026).
- Ankit Saha, Sk Monsur Alam, Rajat Kumar Pal, Subhranil Saha, Munmun Koley, Shubhamoy Ghosh, Sangita Saha, Soumya Bhattacharyya, Sagarika Muduli, Indrani Halder, Mousumi Koley, Amit Gunin, Suhisna Das, Doly Chakraborty, Abdur Rahaman Shaikh, Priyanka Ghosh, Satarupa Sadhukhan, Shyamal Kumar Mukherjee, Treatment of Hemorrhoids with Individualized Homeopathic Medicinal Products: A Double-Blind, Randomized, Placebo-Controlled Trial, Journal of Integrative and Complementary Medicine, 10.1177/27683605261435779, (2026).
- K Satanova, A Fursov, R Fursov, A Kaipova, A Talassov, RISKS OF COMPLICATIONS AND STATISTICAL CRITERION OF “ODDS RATIO” (OR) AS INDICATORS OF THE EFFECTIVENESS OF LASER VAPORIZATION OF HEMORRHOIDAL VESSELS, BULLETIN OF SURGERY OF KAZAKHSTAN, 10.35805/BSK2026I009, 22, 1, (58), (2026).
- Chris M Prince, Adhya M Tom, Sofia Ali, Jagat S Gopinath, Ashish Enos, Anusha Sreejith, Spectrum and Management of Anorectal Disorders: A Retrospective Analysis From the United Arab Emirates, Cureus, 10.7759/cureus.104155, (2026).
- Fabrício Doin Paz de Oliveira, Bruno Lorenzo Scolaro, Ana Carolina Buffara Blitzkow, Sonia Cristina Cordero Time, Alline Maciel Pinheiro Borges, Thais Alencar Pinto dos Santos, Alfadl Abdulfattah, Elisa Treptow Marques Lemos, Glicia Estevam de Abreu, Laser Hemorrhoidoplasty for Grade III Hemorrhoidal Disease: Safety and Efficacy in a Brazilian Multicenter Retrospective Cohort Study, Photobiomodulation, Photomedicine, and Laser Surgery, 10.1177/25785478251386982, (2026).
- Muhammad Usama Talib, Faiza Hameed, Qambar A Laghari, Zameer Hussain Laghari, Aijaz Ahmed Shaikh, Renad Al Mefleh, Comparative Study of Blood Loss and Hemostasis in Doppler-Guided Hemorrhoidal Artery Ligation Versus Open Hemorrhoidectomy, Cureus, 10.7759/cureus.102186, (2026).
- Mohammad Hossein Golezar, Hamed Ghorani, Fakhroddin Alemi, Farzad Fayedeh, Maryam Yeganegi, Samaneh Toutounchian, Hanieh Amani, Hadi Rokni Yazdi, Arterial Embolization for the Internal Hemorrhoids Management: A Systematic Review, Health Science Reports, 10.1002/hsr2.71577, 9, 1, (2026).
- See more