The societal impact of a biologic treatment of ankylosing spondylitis: a case study based on secukinumab
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study estimates the societal benefits of using biologics like secukinumab (SEC) instead of nonsteroidal anti-inflammatory drugs for treating patients with ankylosing spondylitis in Germany. Materials & methods: A Markov and a population model were used to predict the functional impairment of German ankylosing spondylitis patients using SEC or nonsteroidal anti-inflammatory drugs. This was translated into avoided productivity losses, which were valued according to gross value added. Results: The productivity impairment of SEC users was predicted to decrease by 20 percentage points, corresponding to 12.8 and 32.7 million hours in paid and unpaid work and a monetary value of €1.6 billion from 2016 to 2030. Accounting for economic spillover effects increases the societal value to € 3.3 billion. Conclusion: The improvements in functional impairment due to biologics could lead to sizable productivity effects.
Ankylosing spondylitis (AS) is a progressive axial spondyloarthritis. It is characterized by enthesitis and chronic inflammation, predominantly of peripheral joints and the spine [1]. Clinical manifestations of AS are asymmetric peripheral oligoarthritis and inflammatory back pain [2]. Spinal mobility is increasingly reduced throughout the disease which leads to significant functional restrictions [3,4]. Disease onset is usually before the ages of 30 and 40 years with a higher incidence among males [5,6]. It is estimated that between 1.3 and 1.6 million people in Europe suffer from AS [7] with recent calculations claiming a prevalence of 0.37% in Germany [8]. AS patients suffer from significant impairments in activities of daily living [9] and reduced health-related quality of life [10]. Besides the considerable economic burden to the healthcare system [11], loss in productivity represents a substantial part of the societal burden of AS [12,13]. Productivity losses in the AS patient population, where many individuals are still in working age, could occur due to presenteeism, absenteeism, unemployment or early retirement [14].
Guidelines suggest the use of nonsteroidal anti-inflammatory drugs (NSAIDs) as first-line treatment of AS for symptom control [15–17]. However, these are unable to stop or reverse disease progression [18]. Biologic treatment with anti-TNF agents like infliximab, adalimumab, certolizumab or golimumab builds the last and most effective line of treatment of AS [16,19]. Secukinumab (SEC), a novel IL-17A inhibitor, provides a new mode of action for the treatment of active AS in adults and received European market approval in late 2015 for patients who have responded inadequately to conventional therapy [20]. As part of a new class of biologics, SEC aims to overcome the low persistence [21] and unfavorable adverse event risk profile of anti-TNFs [22]. The Phase III clinical trials of SEC, MEASURE 1 (CAIN457F2305) and MEASURE 2 (CAIN457F2310), provide evidence on its effectiveness and safety [23–25]. Follow-up studies show that improvements in disease activity and symptoms are sustained over a long-term period [26,27].
To our knowledge, no studies have assessed the societal impact of the use of biologics in the treatment of AS for Germany, the context of interest of our analysis. In an effort to overcome this gap in the literature, our study aims to assess the societal impact of the use of a biologic treatment, with SEC as an example, in terms of paid and unpaid work, compared with a non biologic treatment among AS patients in Germany. We opted for focusing on the effect of an introduction of a single treatment and not the full class of biologics, since results would be more informative for health technology assessment, or the related policy context, which mostly focus on single products. The choice to use SEC as case study was based on the product being one of the newest treatment options in this indication and, more pragmatically, that detailed (clinical) data, beneficial for the type of analysis we conducted, was available to us only for this treatment.
For the purpose of our analysis, we adopt an existing cost–effectiveness framework [28], and extrapolate the health effects to the expected SEC users in the German AS population from 2016 until 2030. In a second step, these health effects are translated into avoided productivity losses and monetized in terms of gross value added (GVA), a widely used metric to measure economic activity from a macroeconomic perspective. This monetized value of the patient’s potential for paid and unpaid work is then compared with the expected healthcare costs associated with the treatment.
Materials & methods
As a first step, we simulate the effects of SEC on the German social health insurance patients with active AS, aged 20 years and over, and who exhibited inadequate drug response to conventional care (CC) defined as NSAIDs. We compare two scenarios: patients continuously treated with SEC, and patients treated with NSAIDs, hereinafter called CC. Therefore, we estimate the societal value that is created through the use of biologics like SEC in comparison with non biologic treatments. We did not extend our analysis to compare SEC with anti-TNFs as a comparison within biologic treatment options was not relevant to the study objective. Further, such a comparison within biologics would be limited, as it would entail indirect treatment comparisons due to a lack of head-to-head studies.
The time period of our analysis is from 1 January 2016 to 31 December 2030. This period was chosen to reflect the approximate product life cycle of SEC. A longer time frame was not chosen as all future cohorts of our target population were simulated to capture the impact on the health and productivity of the AS population through the year 2030. This required a dynamic population approach, accounting for new cohorts entering the model every cycle, as well as for the possibility of discontinuing treatment or death.
Patient-level model
To capture these dynamics for the population, we simulated the corresponding events and disease severity for an average patient, adapting a newly developed cost–effectiveness framework [28]. This framework consists of a semi-Markov model with a 6-month treatment induction period, after which treatment response is assessed. In the SEC scenario, based on a positive response, patients proceed treatment with SEC. In the following 3-month model cycles, patients could transition to the following states: Discontinue SEC and return to CC, suffer from a severe adverse event (infection and malignancy), also leading to treatment discontinuation and additional treatment costs, or transition to the death state. In the CC scenario, patients are continuously treated with NSAIDs and cannot switch to other treatments. If SEC treatment is discontinued in the SEC scenario, patients are censored and no longer followed in the model. The reasoning behind this censoring was that we assumed no difference in disease severity and treatment cost between patients who newly entered CC due to treatment discontinuation and patients in the scenario that received CC from the beginning. This implies that the initial improvement in disease activity due to the use of SEC, and therefore the difference in benefits to the CC scenario, is lost again after treatment discontinuation. All patients in CC receive the same treatment (NSAIDs), as such there is no difference in treatment costs between the scenarios for patients discontinuing treatment. The model does not assume any natural progression of disease activity over time [28].
Clinical input data for our patient-level model, like baseline severity or effectiveness, are summarized in Table 1. They were predominantly calculated based on results from the MEASURE 1 and 2 trials (CAIN457F2305, CAIN457F2310), where 590 patients were randomized to receive subcutaneous maintenance injections of SEC or placebo. SEC achieved clinically meaningful improvements in disease severity compared with placebo [25].
| Model input | Input value; description | Ref. |
|---|---|---|
| ASAS20 response rate: | ||
| – 6 months | 69.7% (95% CI: 58.9–82.0); MEASURE 2 for patients receiving 150 mg dosage of SEC | [29] |
| Baseline severity (SD): | ||
| – BASDAI total | 6.59 (1.47); MEASURE 2 baseline for patients receiving 150 mg dosage of SEC | [29] |
| – BASDAI given ASAS20 response | 6.90; Calculated based on MEASURE 1 & 2 trial data (not reported in trial results publication) | |
| – BASDAI no ASAS20 response | 6.13; Calculated based on MEASURE 1 & 2 trial data (not reported in trial results publication) | |
| Change in BASDAI with SEC150 (6 months) (SD): | ||
| – ASAS20 Responders | -3.70 (1.86); Calculated based on MEASURE 1 & 2 trial data (not reported in trial results publication) | |
| – ASAS20 Non-responders | -1.42; Calculated based on MEASURE 1 & 2 trial data (not reported in trial results publication) | |
| BASDAI change in CC | Assuming no improvement or deterioration for patients with conventional care | Assumption and CE-Model [28] |
| Annual drop-out-rate SEC: | ||
| – Year 1 | 15.3% | [27] |
| – Years 2+ | 2.3%; 2- and 3-year results MEASURE 2 | [27] |
| Exposure to biologics | Model uses weighted average of effectiveness of SEC for biologic experienced and naive patients | Assumption and CE-Model [28] |
| BASDAI with continuing SEC treatment | 3.2; Baseline BASDAI given response – Change in BASDAI given response | Own calculations and [27] |
| Adverse events: | ||
| – Serious infections per 3-month cycle | 0.24%; 10% of which tuberculosis | [29] |
| – Malignancy | 0.0015% | [29] |
| Relative mortality risk vs general population: | ||
| – Male | 1.63; General population mortality was extracted from German statistical office Destatis | [30,31] |
| – Female | 1.38 | [30] |
| Age and gender distribution (female/male), %: | ||
| – 20–29 years | 2.28/3.15 | |
| – 30–39 years | 5.35/7.11 | |
| – 40–49 years | 6.82/9.77 | |
| – 50–59 years | 9.05/12.24 | |
| – 60–69 years | 8.40/14.09 | |
| – 70+ years | 6.64/15.10 | |
| Employment rate (female/male), %: | [32–34] | |
| – 20–29 years | 50.59/50.44 | |
| – 30–39 years | 70.35/73.93 | |
| – 40–49 years | 71.02/75.66 | |
| – 50–59 years | 58.74/58.37 | |
| – 60–69 years | 10.30/15.55 | |
| – 70+ years | 0.81/1.92 | |
ASAS20: Assessment of spondyloarthritis 20 criteria; BASDAI: Bath AS disease activity index; CC: Conventional care; SEC: Secukinumab.
Main parameters are the SEC treatment response at 6 months measured via the assessment of spondyloarthritis 20 (ASAS20) criteria and the change in disease activity measured via the Bath AS disease activity index (BASDAI) [35,36]. The former is a widely used criterion to show whether a patient benefits from treatment and should continue with the regimen. The BASDAI is a measure of disease activity scaled from 0 to 10 with higher values indicating worse health. The central assumption of the model is that there is no change in BASDAI in the CC scenario. This follows from the definition of the patient population, which previously exhibited inadequate drug response to NSAIDs. The model assumes that the improvement in BASDAI given ASAS20 response can be sustained over the modeled time period. 3-year results from the MEASURE trials do indicate that this is not an unrealistic assumption [26,27].
We ran separate models for gender and age groups (20–29, 30–39, 40–49, 50–59, 60–69 and 70+ years) to account for the differences in mortality, imputing the midpoint of the age intervals into the patient-level model (75 for 70+ years). These age groups were selected to be congruent with age categories most frequently used in official statistics relevant to our analysis (see below).
Population model
In a separate model, we combined health state probabilities, and disease activity (BASDAI) from these lifetime patient-level simulations with the number of AS patients expected to initiate treatment with SEC in the respective 3-month cycle until 2030 in the respective age/gender group.
Individuals initiating treatment with SEC are either patients with no prior adequate response to NSAIDs or patients switching from other biologics. In the benefit dossier submitted to the federal joint committee (G-BA), this population is estimated to be in between 22,031 and 98,294 social health insurance patients [8]. This range is based on an AS prevalence of 0.37% and a share of patients receiving biologics or potentially eligible for biologic treatment – active AS without adequate response to CC – of 10.3 and 45.7% [8]. Applying a moderate market share among biologics, the estimated number of patients initiating treatment with SEC and entering the model is 1344 in 2016. We assume an increase in the proportion of AS patients receiving biologics due to higher acceptability and tolerability of biologics and an increasing market share for SEC until 2021. Using a logarithmic extrapolation, we assume that the entry cohort sizes decrease after 2021 and conservatively drop to zero in 2028 due to potential new market entries and displacement of SEC. Appendix A plots the development of the expected cohort sizes until 2030. Yearly cohorts are evenly distributed to 3-month cycles in our model.
Patients are distributed across gender and age groups according to data from the benefit dossier submitted to the federal joint committee (Table 1). The main assumptions of the long-term population-level model are the following: Drop-out rates (besides mortality) and sustained effectiveness are independent of age and gender; all input parameters of the patient-level model (Table 1), as well as the age and gender distribution of the newly entering cohorts of AS SEC users, stay constant over the full-time horizon of our analysis. While these are strong assumptions, they constitute logical choices in light of lacking valid prospective data on these parameters. All of the above described patient cohorts are followed until 31 December 2030. The population model provides information on the number of patients in each model cycle with continuous SEC treatment, who are assumed to sustain their initial average BASDAI improvement (Table 1). Patients discontinuing treatment (e.g., adverse event, lack of efficacy, adherence and death) drop out of the model.
Linking clinical outcome to productivity & monetary valuation
To estimate the societal benefits associated with sustained improvements in disease activity (BASDAI), we had to quantify the relationship between BASDAI scores and some type of productivity measure. Previous research used the work productivity and activity impairment questionnaire (WPAI) for that purpose [37]. The WPAI is a reliable and valid patient-reported instrument quantifying the percentage of work and activity impairment due to (bad) health [38,39]. We utilized patient-level longitudinal data from the MEASURE 1 and MEASURE 2 trials to estimate the relationship between BASDAI and the work productivity loss and activity impairment dimensions of the WPAI general health questionnaire. The calculations included patients randomized to either a 150 mg dosage of SEC or placebo using observations at baseline and weeks 16, 24 and 52. A linear mixed model with log link and gamma distribution was used to fit WPAI scores as response variables and BASDAI score as a predictor, controlling for gender and age. To account for the within-subject correlation of assessments across time, we used subject as random effects. The results of these calculations allow us to quantify the percentage work and activity impairment of our SEC model population and compare it with the CC population.
Estimating amount of gained productive time
Figure 1 outlines our approach to estimating the societal impact induced by the improvement in work and activity impairment. Besides productivity related to paid work, we also quantify the impact on unpaid work using the estimated difference in activity impairment. Following the ‘third-person criteria’, unpaid work activities are productive activities with no direct remuneration, which are replaceable by others [40]. This is, for example, the case for unpaid household production and volunteering. Unpaid work is an important contributor to societal welfare [41] and therefore should not be neglected in this type of analysis. The differences in average percentage work and activity impairment in AS patients between our treatment scenario with SEC and the CC scenario are then multiplied by a baseline.
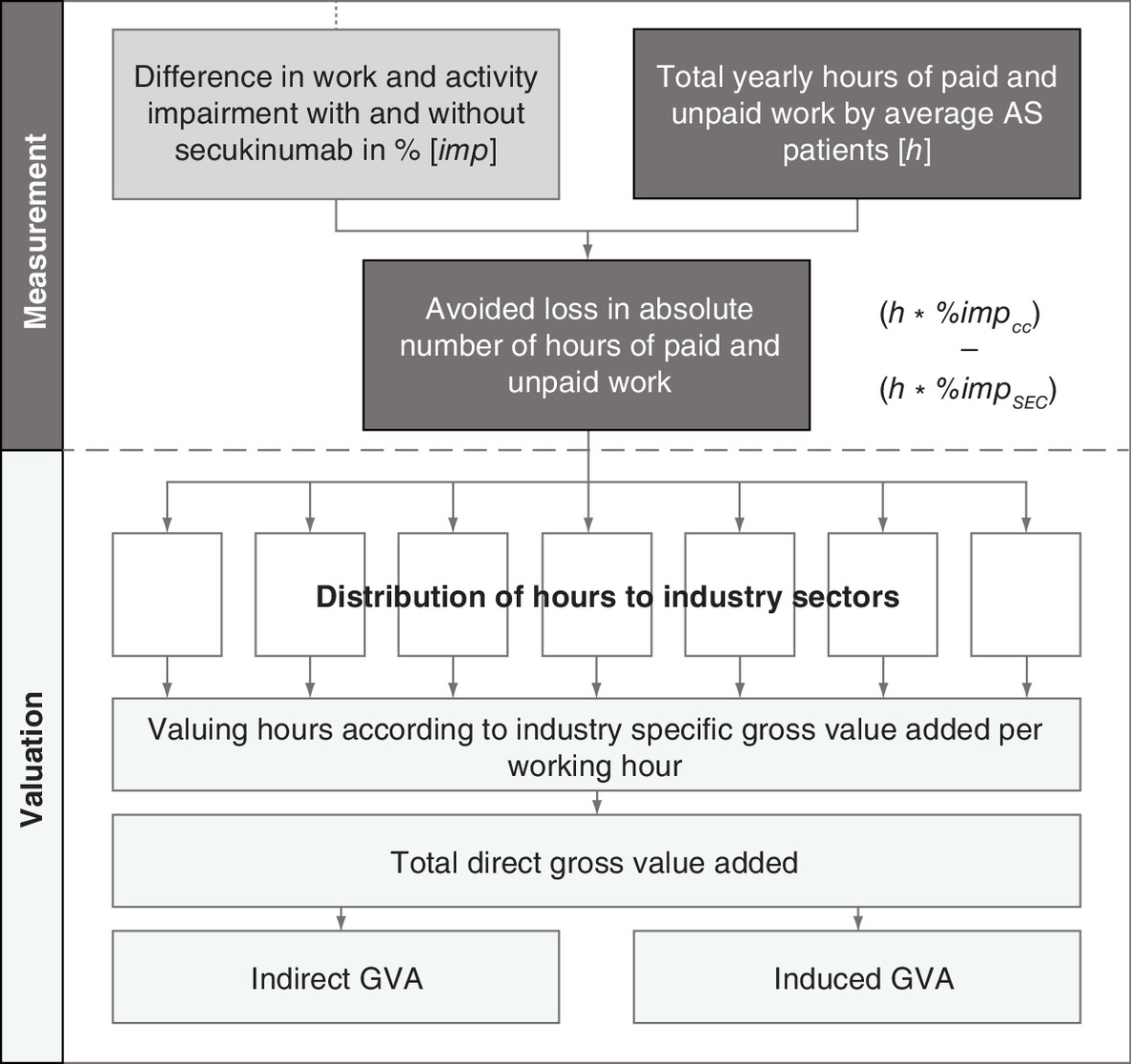
Figure 1. Stylized depiction of estimating productive time and monetary value based on differences in work and activity impairment.
AS: Ankylosing spondylitis; CC: Conventional care; GVA: Gross value added; IAB: Institut fürArbeitsmarkt-und Berufsforschung; SEC: Secukinumab.
To establish a baseline of hours worked in gainful employment in our model population, the following steps were necessary: first, we utilized age- and gender-specific employment rates of AS patients from a study analyzing employment of AS and rheumatoid arthritis patients in Germany to estimate the share of employed patients [32]. We aggregated the information on 5-year age groups into 10-year groups to fit our model purposes and then extrapolated a reduced employment rate for individuals older than 64 years (Table 1). Second, working time calculation data from the federal labour office and information from the German national accounts and statistical offices were used to calculate the average working hours per age and gender cell allocated to each industry sector [42–44].
The baseline number of hours spent on unpaid work for all relevant age- and gender cells was extracted from data from the German time use survey [45,46]. The following activities collected by the time use survey are subsequently assigned to the industry sector of their closest market substitute, following the proxy good approach (also known as market replacement cost approach) for monetary valuation: Gardening, improvements and home repair, preparation of meals, maintenance of dwelling, manufacturing and care of textile fabrics, purchases and procurement, planning and organization, informal care, child care, other care and voluntary work [41]. Other activities are not captured. By definition, a monetary compensation of unpaid work cannot be observed. Therefore, in the following, we refer to ‘equivalents’ to highlight that the monetary value of unpaid work is hypothetical.
Monetary valuation of paid & unpaid work
The avoided loss in productive time per industry sector for paid and unpaid work is then valued according to industry-specific GVA per working hour. GVA is an indicator, measuring the value of economic activity as economic output exclusive of intermediate consumption. One of the most widely used measures for economic performance, it constitutes the contribution of an economic subject to the gross domestic product [47]. Industry-specific GVA per working hour is extracted from the German national accounts [43]. Hourly productivity is assumed to remain constant throughout our analysis.
So far, we have estimated the direct GVA equivalent value corresponding to avoided losses in paid and unpaid work. GVA effects are synonymous to additional goods and services being produced. The production of goods and services initiates further economic activity. To estimate these spillovers, we employ industry-specific Leontief multipliers for indirect and induced economic effects using the input-output tables from the German national accounts [48]. Indirect effects represent the intermediate consumption of goods and services and suppliers. Induced effects capture the impact of spending by households receiving income based on direct and indirect effects. While the reasoning behind indirect and induced effects is more comprehensible for paid market activities, the production of unpaid work activities is assumed to generate indirect and induced GVA effects as well, as these still require certain goods and services.
Estimating costs of treatment
In addition to estimating the benefits associated with biologic treatment, we calculated the cost or investment necessary to achieve the outlined improvements in health and productivity impairment up to 2030. Patient-level and population models were used to estimate the overall drug costs for SEC, costs for initial administration and monitoring, as well as costs caused by adverse events like infection and malignancy. Resource use and cost input data can be found in Appendix B.
Sensitivity analysis
Univariate sensitivity analysis was conducted to provide information about the impact of the uncertainty around our main input parameter using their 95% CIs (if available, see Table 1). The interval for BASDAI change after 6 months had to be calculated based on its standard deviation. As information on the uncertainty around the gender- and age-specific employment rates was not available, those were varied by 10%. The structure of our model with two sequential models (patient-level and population), and the limitations of Microsoft Excel, did not allow us to conduct probabilistic sensitivity analysis.
We did not discount future incurred costs and generated societal value in our base case estimates but provide discounted overall benefit and cost estimates based on a 3% discount rate as common in cost–effectiveness analysis. Not discounting is in line with guidance for budget impact analysis [49], which we consider more closely related to our analysis, compared with cost–effectiveness analysis, where net present values are required. The quantification of the relationship between BASDAI and WPAI was conducted using SAS version 9.4 (SAS Institute, NC, USA). Microsoft Excel 2013 (Microsoft Corporation, WA, USA) was used for all other calculations.
Results
Population size, disease severity & activity impairments
The patient-level and population model predicted the number of AS patients with continuous use of SEC and the number of patients discontinuing treatment, less the number of patients dying throughout the modeled period. As outlined in section 2, we are merely interested in patients with continuous SEC use and assume a sustained improvement in disease activity in these patients. This corresponds to a constant BASDAI score of 3.2. In the comparator scenario, where patients are assumed not to profit from CC, the BASDAI score remains at the baseline of 6.59 (Table 1).
The linear mixed model estimating the relationship of BASDAI and WPAI score calculated that BASDAI is a significant predictor of work and activity impairment (p < 0.0001). Age and gender, however, seem not to influence work productivity in AS patients, while age is a significant predictor of activity impairment. The results of these calculations are shown in Table 2.
| Variable | Estimate (SE) | 95% CI | p-value |
|---|---|---|---|
| Work productivity loss | |||
| Intercept | 2.9993 (0.1092) | 2.7843–3.2144 | <0.0001 |
| BASDAI total score | 0.1489 (0.0077) | 0.1338–0.1640 | <0.0001 |
| Age (years) | 0.0006 (0.0023) | -0.0039–0.0051 | 0.7879 |
| Male | -0.0036 (0.0519) | -0.1055–0.0983 | 0.9450 |
| n | 778 | ||
| Activity impairment | |||
| Intercept | 2.8088 (0.0704) | 2.6703–2.9473 | <0.0001 |
| BASDAI total score | 0.1657 (0.0050) | 0.1560–0.1755 | <0.0001 |
| Age (years) | 0.0035 (0.0013) | 0.0009–0.0061 | 0.0079 |
| Male | -0.0338 (0.0347) | -0.1019–0.0343 | 0.3300 |
| n | 1319 |
Own calculations based on linear mixed model with log link and MEASURE 1 and 2 trial data.
BASDAI: Bath AS disease activity index; SE: Standard error; WPAI: Score based on the work productivity and activity impairment questionnaire.
Age- and gender-specific work and activity impairment in the population per model cycle were predicted using the estimated coefficients according to Equations (1 & 2):
(Eq. 1)
(Eq. 2)
We used the midpoints of the age categories as age inputs for the calculations (and 75 for 70+ years). The corresponding calculations resulted in average percentage work productivity loss and activity impairment of 33.4 and 33.8% in SEC users. For CC users, remaining on the BASDAI baseline of 6.59, the corresponding work productivity loss and activity impairment was 55.3 and 59.3%.
These differences in productivity and activity impairment correspond to 45.5 million hours of productive time that could be avoided in the German AS population treated with a biologic like SEC from 2016 to 2030. Out of these 45.5 million hours lost, 32.7 million hours (72%) are attributed to unpaid activities such as household production or volunteering while the remainder is attributed to paid work (12.8 million hours). On patient level, these numbers equal to a potential of 116 h in paid work and 299 h in unpaid work per patient per year. This result highlights the importance of including unpaid activities in such type of analyses.
Societal value & costs
Valuing the aggregated benefit in paid work in terms of GVA corresponds to a monetary impact of €611.6 million. The benefit in unpaid work corresponds to a GVA equivalent of €975.8 million. Using Leontief multipliers to account for the indirect and induced economic activity results in a societal value of healthier patients, or social impact, of €3.3 billion (Table 3). Applying a 3% discount rate to streams from 2017 to 2030 yields a total value of €2.54 billion.
| Aggregated results | |
|---|---|
| Person-years in model for secukinumab users | 109,685 |
| Gained hours of productivity until 2030: | |
| – Paid work | 12,754,128 |
| – Unpaid work | 32,743,704 |
| Value of hours gained until 2030 in terms of gross value added (undiscounted): | |
| – Paid work | Direct: €611,554,551 Indirect: €446,999,365 Induced: €273,394,382 |
| – Unpaid work | Direct: €975,817,109 Indirect: €578,577,097 Induced: €372,194,820 |
| Total social impact | €3,258,537,324 |
| Social impact per patient per year | €29,708 |
The corresponding costs of treatment, on the other hand, are estimated to be € 1.30 bn. This amount is inclusive of drug costs (99.46%), initial and monitoring costs (0.25%) and adverse event costs (0.29%). Using a 3% discount rate decrease, the total costs to € 1.01 bn. The yearly projected social impact and costs occurring from 2016 to 2030 are presented in Figure 2.
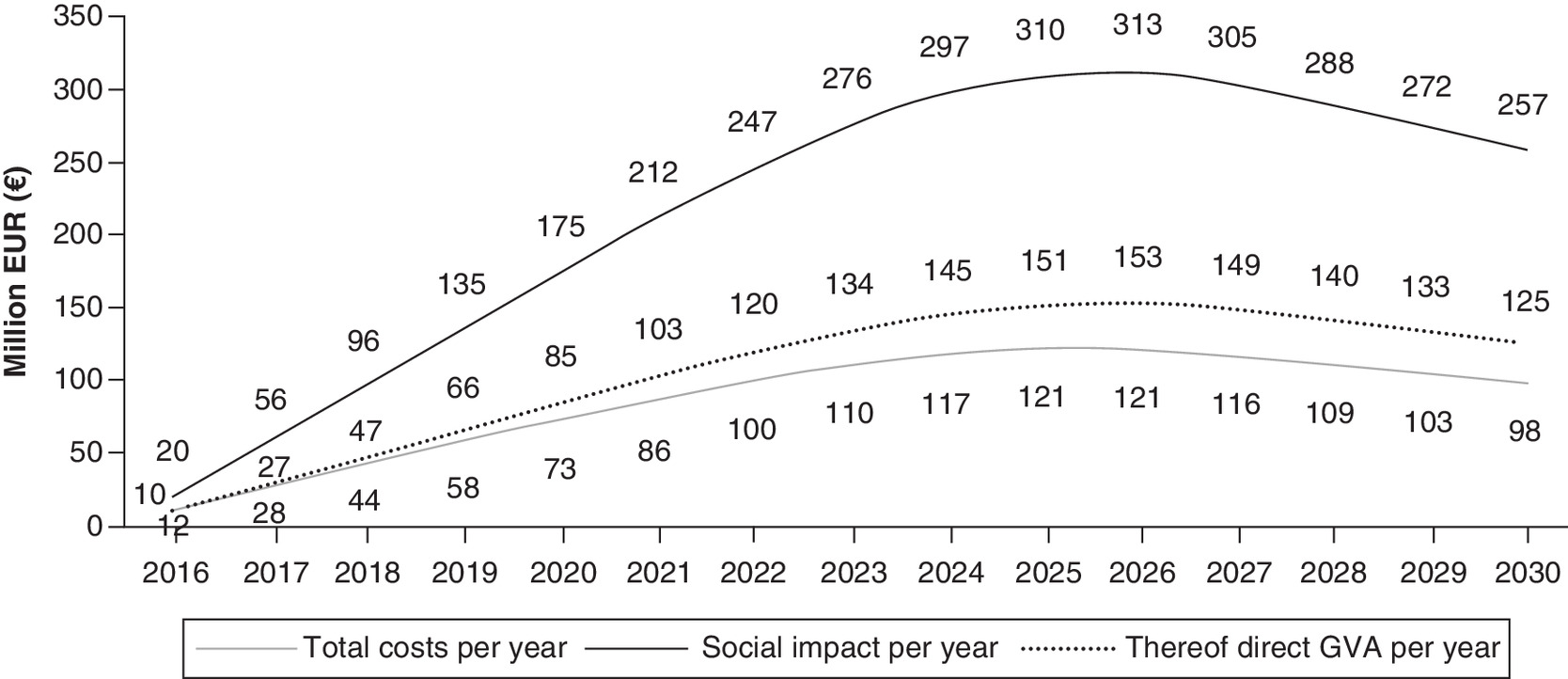
Figure 2. Projected social impact and costs generated by secukinumab until 2030.
GVA: Gross value added equivalent.
Sensitivity analysis
The sensitivity of the societal impact of biologic treatment concerning the uncertainty around our main input parameters is depicted in Figure 3, using the 95% CIs as the upper and lower bounds of the parameters (where available). The figure illustrates that transforming BASDAI-scores into percentage productivity impairment, based on BASDAI coefficient estimates from Table 2, introduces the highest level of uncertainty in our model. The results are more stable to changes in the clinical input parameters or the employment rate.
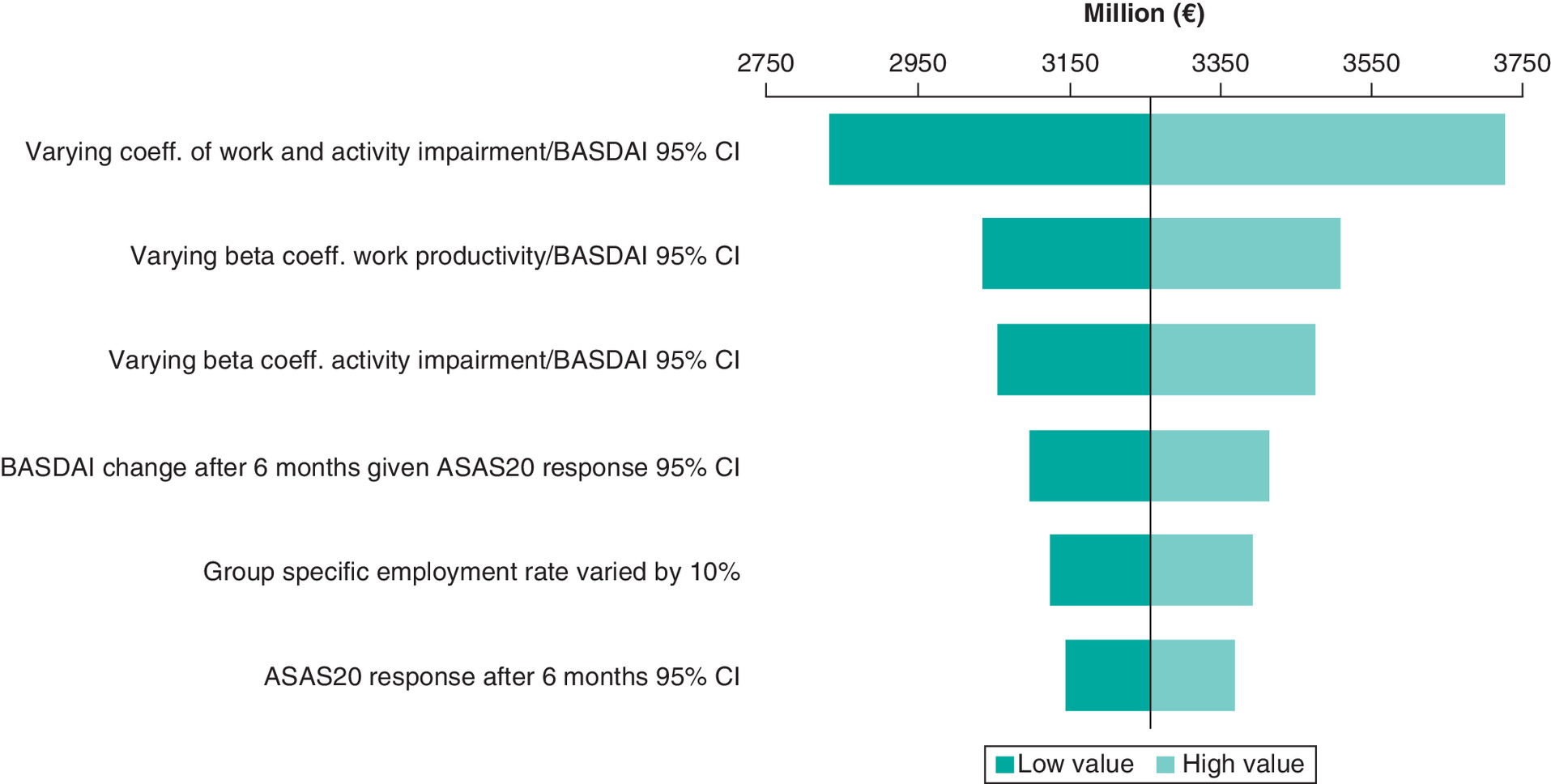
Figure 3. Robustness of calculated societal impact (including indirect and induced effects) to changes in main input parameters.
Input parameters were varied according to lower and upper bound of 95% CIs (where available).
ASAS20: Assessment of spondyloarthritis 20 criteria; BASDAI: Bath AS disease activity index.
Discussion
Using an extended approach, we quantified the societal value created by biologic treatment like SEC among AS patients in Germany compared with a non biologic treatment by extrapolating results from the MEASURE trials. The use of biologic treatment can lead to sustained improvements in disease activity in the eligible German AS population due to non response to CC defined as NSAIDs. This improvement has the potential to enable considerable productivity effects for both paid and unpaid work. Monetizing these in terms of GVA leads to an estimated direct value of € 1.6 bn up to 2030. By including the potential to stimulate indirect and induced effects, the total societal value is estimated at € 3.3 bn. Our estimates display a comprehensive economic valuation of avoided losses of productive time in order to approximate the productivity-related welfare gain due to better health. It is important to note, however, that we do not claim the estimated effect to correspond to the real expected gross domestic product impact.
A novelty of our study lies in the chosen approach for quantifying a monetary value of health-related productivity effects: Valuing avoided losses of productive time in terms of GVA based on the national accounts and taking into account possible indirect and induced economic effects present new ways of estimating productivity effects. By also including unpaid work, which has been applied and discussed before [50], we are providing a more comprehensive picture of the societal impact of improvements in productivity impairment.
Related literature
By including unpaid work, and valuing productive time according to GVA, which enabled the calculations of economic spillover effects, our study provides a broader analysis of the societal impact of a specific medication for AS, than the previous literature. Due to vast differences in the methodological choices between studies, directly comparing our monetary estimates of the economic burden of AS or its improvement to existing literature is difficult [51]. For example, one analysis, which considered unpaid work in this context, uses self-reported time needing help as a proxy for activities that the patient was unable to perform [52]. This methodology is hardly comparable with our estimation approach.
A related study from the Netherlands estimated annual decreases of productivity costs as a result of the introduction of the class of anti-TNFs of €12.58–31.21 million [53]. Taking the midpoint of their estimate, the time frame of our study (15 years) and a difference in size of population between Germany and the Netherlands (factor of four; in their study, the prevalence of AS for the Netherlands was assumed to be 0.4%, with an estimate of 0.36% used in our study) roughly translates to productivity improvements of € 1.2 bn. However, measurement and valuation of productivity effects differed significantly compared with our study.
An analysis, which used a comparable approach, estimated the societal impact of SEC in comparison with the non biologic csDMARDs in the German psoriatic arthritis population [54]. The societal impact of SEC up to 2030 in this patient population was estimated to be € 2.7 bn overall and € 17,953 per patient per year. Our disaggregated estimate of € 29,708 per patient per year is considerably larger. The larger effect is plausible as there is a larger difference in work and activity impairment (avg. 13.6 and 12.1% vs 21.9 and 25.5%) and relates to a younger patient population.
The only analysis in Germany, which estimated productivity costs due to AS in general, is an analysis by Huscher et al. [12]. They include absenteeism and permanent work disability, and value productivity losses according to the average daily German wage. We, on the other hand, do not include work disability but account for presenteeism and unpaid work, and value avoided productivity losses in terms of the hourly GVA, while also including indirect and induced economic effects. Applying the human capital approach, the annual loss of productivity per patient for paid work with functional impairment above 50% was estimated to be € 30,557 (inflation-adjusted 2015 values) [12]. This level of impairment corresponds to the level in our CC scenario. The calculated direct benefit of biologic treatment in paid work in our analysis, which is the estimate most closely related to Huscher et al., is € 5576 per patient per year. Although we refrain from a direct comparison given the methodological differences, this shows that our estimated value of an average work productivity improvement of 21.9% points is not unrealistic, at least for the direct impact on paid work.
A study from the UK investigated work productivity loss in terms of both presenteeism and absenteeism in AS patients following the human capital approach [55]. Their estimate for the overall work impairment per patient per year amounts to £ 3836 (€ 5467 in 2015 values). This number is considerably lower than our baseline productivity loss due to two factors: first, we value productivity losses in terms of GVA, while Cooksey et al. use average daily wages [55]. Second, our analysis only includes AS patients, who are eligible for biologic treatments and did not adequately respond to non biologic treatments, while the only inclusion criteria in Cooksey et al. is a confirmed AS diagnosis [56]. Therefore, disease severity and work impairment vary considerably between the two analyses. The estimated average work impairment was 26.1% in Cooksey et al., while the average work productivity improvement due to the use of SEC was estimated to be 21.9% points in our analysis. Although the baseline work impairment is widely different, the valuation of these two similar numbers lies within a reasonable range (€ 5467 vs € 5576).
Limitations
Our results have to be interpreted in acknowledgment of several limitations. First and foremost, our simulation solely focuses on a comparison of a biologic treatment using SEC as example with a non biologic treatment. This treatment was assumed to be not effective as the modeled population did not adequately respond to a treatment with NSAIDs before. The estimated effects therefore do not represent the added benefit of SEC on top of the existing biologic treatments. They should be interpreted as the societal impact of SEC as member of this class of drugs compared with a scenario where these effective treatments are not available.
Another main limitation of the simulation is the uncertainty concerning the expected number of patients, which take up treatment with SEC from 2016 through the year 2030. Therefore, we decided to make a conservative assumption about the number of patients initiating treatment with SEC in the later years of the simulation (Appendix A), where competitors, biosimilar treatments or other innovations in treating AS may displace SEC.
Although our analysis goes further in including all relevant societal benefits than previous analysis, the picture is not yet complete. For instance, we did not account for possible changes in the caregiver burden due to a more effective treatment. One analysis estimated that on average, an AS patient requires 52 h of caregiver’s time per 3-month period [55]. Furthermore, individuals taking care of relatives/friends with chronic diseases, like AS, themselves potentially are negatively affected by the care they are giving. These negative consequences could also include health deterioration [56,57]. Furthermore, our analysis also does not include activities like leisure, which undoubtedly have value to individuals as well as economic relevance.
The sensitivity analysis revealed that the transformation of BASDAI into productivity has a considerable impact on our results and shows that this type of mapping approach is invariably the second-best approach if long-term observations of productivity measures are not available. Therefore, it might be worthwhile in the future to include a measurement like the WPAI also in the long-term follow-up of a study. Although 3-year effectiveness data show that the improvement in disease activity can be sustained, it is unclear whether this would also be the case for the improvements in work productivity and activity impairment [26].
Labor market participation of AS patients in our model had to be estimated based on data from 2007 to 2011 due to the lack of more current information [32]. Employment rates were assumed to be equal between SEC and CC. Therefore, we did not account for possible differences in early retirement due to AS, although this relationship does exist [58].
Apart from the degree of labor market participation and the estimated work and activity impairment, we assumed that the potential for paid and unpaid work of the modeled AS patients does not differ from the general German population. Although using GVA to value productive time goes beyond what has been done before, we could not account for wage differences between men and women as well as between the more/less experienced employees. We furthermore did not consider compensation mechanisms or multiplier effects (e.g., by co-workers) [59].
Our analysis does not only provide an estimation of paid and unpaid work productivity, it also includes an assessment of the healthcare costs associated with the use of a biologic like SEC over the modeled time period. However, for interpreting the results of this type of analysis, it is important to acknowledge that the estimated effects do not constitute a net benefit to society. It is possible that resources allocated to biologic treatment could alternatively be spent on other drugs or interventions, which generate larger effects with similar or lower costs. Within AS treatments, this is, however, not necessarily the case, considering the favorable cost–effectiveness results of SEC [28].
Conclusion
This study shows the extent to which a reduction of the health burden of AS patients in Germany can bring about societal benefits in terms of avoided productivity losses/gains in productivity potential. It emphasizes that the impact of AS is not limited to the detrimental health of patients or the associated healthcare resource use, but also includes considerable productivity effects. It also explores the relevance of an effective treatment of AS from a societal perspective.
The explicit consideration of unpaid work in our study adds to the existing literature by including a broader perspective on productivity to inform decision-making. The results suggest that unpaid work is a non-negligible aspect when determining the burden of a disease and should be included in all future analyses of this type. A precondition for this is, however, that the necessary information on unpaid work capability is collected more frequently and in a more comprehensive manner than in the past.
Our estimates indicate that avoided losses in paid and unpaid work outweigh the healthcare costs related to the treatment with a biologic using SEC as example. This is still the case if potential economic spillover effects are disregarded. We thereby show that the societal investment in effective treatments for AS, or medical interventions in general, do have the potential to be compensated by the value it is creating within society by merely looking at productivity effects. However, productivity should only ever be one component in the assessment of the relevance of a particular disease or a medical intervention. Other aspects, like equity and health equity, must not be disregarded in decision-making.
•
The use of secukinumab in ankylosing spondylitis (AS) patients who did not adequately respond to NSAIDs is simulated to considerably decrease disease activity as measured via the BASDAI compared with a conventional, non biologic treatment.
•
Reductions in disease activity in patients with AS are estimated to lead to sizable decreases of productivity impairment on an individual level.
•
Aggregating these productivity effects to the German AS population, expected to receive a biologic like secukinumab, amounts to 12.8 million productive hours for paid work from 2016 to 2030.
•
The corresponding avoided loss in unpaid work is 32.7 million hours, highlighting the importance of including unpaid work in productivity (cost) calculations.
•
Productive time was valued according to gross value added (GVA) per working hour, leading to a direct GVA equivalent monetary estimate of € 1.59 bn.
•
By using GVA, further indirect and induced economic effects can be calculated to provide a more complete picture of the productivity effect. This leads to a total monetary estimate of € 3.26 bn.
Author contributions
S Himmler and JC Branner conducted the analysis and drafted the manuscript under supervision and guidance from DA Ostwald. The idea for the study originated from DA Ostwald.
Acknowledgments
We thank B Sherif (RTI Health Solutions) for calculating the relationship between WPAI and BASDAI, as well as conducting additional analysis on MEASURE 1 and MEASURE 2 trial data.
Financial & competing interests disclosure
This work was supported by Novartis Pharma GmbH. S Himmler and JC Branner worked on this study as employees of WifOR Institute. DA Ostwald is CEO and founder of WifOR Institute and has an academic relationship with Novartis. As a result, he received speaker fees from the company. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data conducted by RTI Health Solutions, which have been shared with them, and that the use of this shared data is in accordance with the terms agreed upon their receipt. The source of this data is: Novartis Pharma AG / MEASURE 1 trial (CAIN457F2305/NCT01358175), and MEASURE 2 trial (CAIN457F2310/NCT01649375).
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Taurog J. The Spondyloarthritides. In: Harrison's Rheumatology. 16th Ed. McGraw-Hill, Fauci A, Langford C (Eds). NY, USA (2006).
2.
Braun J, Sieper J. Ankylosing spondylitis. Lancet 369(9570), 1379–1390 (2007).
3.
Baraliakos X, Listing J, Rudwaleit M et al. Progression of radiographic damage in patients with ankylosing spondylitis: defining the central role of syndesmophytes. Ann. Rheum. Dis. 66(7), 910–915 (2007).
4.
Rudwaleit M, Haibel H, Baraliakos X et al. The early disease stage in axial spondylarthritis: results from the german spondyloarthritis inception cohort. Arthritis Rheum. 60(3), 717–727 (2009).
5.
Jadon DR, Ramanan AV, Sengupta R. Juvenile versus adult-onset ankylosing spondylitis -- clinical, radiographic, and social outcomes. a systematic review. J. Rheumatol. 40(11), 1797–1805 (2013).
6.
Brunner R, Kissling RO, Auckenthaler C, Fortin J. Clinical evaluation of ankylosing spondylitis in Switzerland. Pain Physician 5(1), 49–56 (2002).
7.
Dean LE, Jones GT, MacDonald AG, Downham C, Sturrock RD, Macfarlane GJ. Global prevalence of ankylosing spondylitis. Rheumatology 53(4), 650–657 (2014).
8.
G-BA. Dossier Zur Nutzenbewertung Gemäß § 35a SGB V. Secukinumab (Cosentyx). Modul 3C. Aktive AS. Berlin (2015). [cited 2019 Aug 1]. https://www.g-ba.de/downloads/92-975-1271/2015-12-11_Modul3C_Secukinumab.pdf
9.
Giacomelli R, Gorla R, Trotta F et al. Quality of life and unmet needs in patients with inflammatory arthropathies: results from the multicentre, observational RAPSODIA study. Rheumatology 54(5), 792–797 (2015).
10.
Kotsis K, Voulgari PV, Drosos AA, Carvalho AF, Hyphantis T. Health-related quality of life in patients with ankylosing spondylitis: a comprehensive review. Expert Rev. Pharmacoecon. Outcomes Res. 14(6), 857–872 (2014).
11.
Krüger K, von Hinüber U, Meier F et al. Ankylosing spondylitis causes high burden to patients and the healthcare system: results from a German claims database analysis. Rheumatol. Int. 38(11), 2121–2131 (2018).
12.
Huscher D, Merkesdal S, Thiele K, Zeidler H, Schneider M, Zink A. Cost of illness in rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis and systemic lupus erythematosus in Germany. Ann. Rheum. Dis. 65(9), 1175–1183 (2006).
13.
Boonen A, Mau W. The economic burden of disease: comparison between rheumatoid arthritis and ankylosing spondylitis. Clin. Exp. Rheumatol. 27(55 Suppl. 4), S112–S117 (2009).
14.
Healey E, Haywood K, Jordan K, Garratt A, Packham J. Impact of ankylosing spondylitis on work in patients across the UK. Scand. J. Rheumatol. 40(1), 34–40 (2011).
15.
Ward MM, Deodhar A, Akl EA et al. American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network 2015 recommendations for the treatment of ankylosing spondylitis and nonradiographic axial spondyloarthritis. Arthritis Rheumatol. 68(2), 282–298 (2016).
16.
van der Heijde D, Ramiro S, Landewé R et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann. Rheum. Dis. 76(6), 978–991 (2017).
17.
NICE. TNF-alpha inhibitors for ankylosing spondylitis and non-radiographic axial spondyloarthritis. Technology Appraisal Guidance [TA383]. (2016). [cited 2019 Apr 30]. https://www.nice.org.uk/guidance/ta383
18.
Palazzi C, D'Angelo S, Gilio M, Leccese P, Padula A, Olivieri I. Pharmacological therapy of spondyloarthritis. Expert Opin. Pharmacother. 16(10), 1495–1504 (2015).
19.
Coates LC, Cawkwell LS, Ng NWF et al. Real life experience confirms sustained response to long-term biologics and switching in ankylosing spondylitis. Rheumatology 47(6), 897–900 (2008).
20.
European Medicines Agency. Cosentyx: EPAR - product information. (2018). [cited 2019 Aug 1]. https://www.ema.europa.eu/en/documents/product-information/cosentyx-epar-product-information_en.pdf
21.
Lyu R, Govoni M, Ding Q et al. Treatment persistence among patients with rheumatoid disease (RA, AS, PsA) treated with subcutaneous biologics in Germany. Rheumatol. Int. 36(1), 143–153 (2016).
22.
Singh JA, Wells GA, Christensen R et al. Adverse effects of biologics: a network meta-analysis and Cochrane overview. Cochrane Database Syst. Rev. 2011(2), CD008794 (2011).
23.
Deodhar AA, Dougados M, Baeten DL et al. Effect of Secukinumab on patient-reported outcomes in patients with active ankylosing spondylitis: a Phase III randomized trial (MEASURE 1). Arthritis Rheumatol. 68(12), 2901–2910 (2016).
• Summary of results of one of the underlying clinical trials.
24.
Sieper J, Deodhar A, Marzo-Ortega H et al. Secukinumab efficacy in anti-TNF-naive and anti-TNF-experienced subjects with active ankylosing spondylitis: results from the MEASURE 2 Study. Ann. Rheum. Dis. 76(3), 571–592 (2017).
• Summary of results of one of the underlying clinical trials.
25.
Baeten D, Sieper J, Braun J et al. Secukinumab, an interleukin-17a inhibitor, in ankylosing spondylitis. N. Engl. J. Med. 373(26), 2534–2548 (2015).
• Summary of results of the underlying clinical trials.
26.
Baraliakos X, Kivitz AJ, Deodhar AA et al. Long-term effects of interleukin-17A inhibition with secukinumab in active ankylosing spondylitis: 3-year efficacy and safety results from an extension of the Phase III MEASURE 1 trial. Clin. Exp. Rheumatol. 36(1), 50–55 (2018).
27.
Marzo-Ortega H, Sieper J, Kivitz A et al. Secukinumab provides sustained improvements in the signs and symptoms of active ankylosing spondylitis with high retention rate: 3-year results from the Phase III trial, MEASURE 2. RMD Open 3(2), e000592 (2017).
28.
Emery P, Van Keep M, Beard S et al. Cost effectiveness of secukinumab for the treatment of active ankylosing spondylitis in the UK. Pharmacoeconomics 36(8), 1015–1027 (2018).
•• Provides detailed description of the adopted cost–effectiveness model.
29.
Novartis. Clinical study report- Week 52 analysis of Phase III trial CAIN457F2310. (2014). [Data on file].
30.
Bakland G, Gran JT, Nossent JC. Increased mortality in ankylosing spondylitis is related to disease activity. Ann. Rheum. Dis. 70(11), 1921–1925 (2011).
31.
Destatis. Allgemeine Sterbetafel 2010/12. Statistisches Bundesamt, Wiesbaden, Germany (2015).
32.
Mau W, Thiele K, Lamprecht J. Trends der Erwerbstätigkeit von Rheumakranken: Ergebnisse aus Sozialversicherungsdaten und Kerndokumentation der Rheumazentren in Deutschland. Z. Rheumatol. 73(1), 11–19 (2014).
• Contains information used for estimating employment rate of modelled patient population.
33.
Destatis. Bevölkerung, Erwerbstätige, Erwerbslose: Deutschland, Jahre, Geschlecht, Altersgruppen. Genesis-Online (Table 12211-0003). Statistisches Bundesamt, Wiesbaden, Germany (2019). https://www-genesis.destatis.de/genesis/online
34.
Eurostat. Annual population by sex, age, degree of urbanisation and labour status (1 000). (2019). [cited 2019 Apr 12]. https://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=lfsa_pgauws&lang=en
35.
Anderson JJ, Baron G, Van Der Heijde D, Felson DT, Dougados M. Ankylosing spondylitis assessment group preliminary definition of short-term improvement in ankylosing spondylitis. Arthritis Rheum. 44(8), 1876–1886 (2001).
36.
Garrett S, Jenkinson T, Kennedy LG, Whitelock H, Gaisford P, Calin A. A new approach to defining disease status in ankylosing spondylitis: the Bath Ankylosing Spondylitis Disease Activity Index. J. Rheumatol. 21(12), 2286–2291 (1994).
37.
de Hooge M, Ramonda R, Lorenzin M et al. Work productivity is associated with disease activity and functional ability in Italian patients with early axial spondyloarthritis: an observational study from the SPACE cohort. Arthritis Res. Ther. 18(1), 265 (2016).
38.
Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics 4(5), 353–365 (1993).
39.
Tang K. Estimating productivity costs in health economic evaluations: a review of instruments and psychometric evidence. Pharmacoeconomics 33(1), 31–48 (2015).
40.
Reid M. Economics of Household Production. John Wiley and Sons Incorporated, NY, USA (1935).
41.
Hofmann S. Einfluss nicht-marktlicher Tätigkeiten auf den materiellen Wohlstand und die Einkommensverteilung in Deutschland. Sozioökonomische Schriften 50, (2015).
42.
Institut für Arbeitsmarkt- und Berufsforschung (IAB). Sonderauswertung der IAB Arbeitszeitrechnung. Arbeitszeit und Arbeitsvolumen nach Geschlecht und Altersgruppen (Inland, abgestimmt auf VGR-Eckwerte). Institut für Arbeitsmarkt- und Berufsforschung (IAB), Nürnberg, Germany (2017).
43.
Destatis. Volkswirtschaftliche Gesamtrechnungen, Inlandsproduktberechnung, detaillierte Jahresergebnisse 2016, Fachserie 18 Reihe 1.4. Statistisches Bundesamt, Wiesbaden, Germany (2017).
44.
Statistische Ämter des Bundes und der Länder. Erwerbstätige Bevölkerung Nach Geschlecht, Alter (10-Er Jahresgruppen) Und Wirtschaftszweig Abschnitte. Kombinierte Registerauszählung Und Hochrechnung Aus Der Haushaltsstichprobe. Zensus 2011. (2014).
45.
Destatis. Zeitverwendungserhebung - Aktivitäten in Stunden Und Minuten Für Ausgewählte Personengruppen 2012/13. Statistisches Bundesamt, Wiesbaden, Germany (2015).
46.
Destatis. Sonderauswertung auf Basis von Daten der Zeitverwendungserhebung 2012/13. Durchschnittliche Zeitverwendung von Personen je Tag nach Ausgewählten Aktivitäten, Personenmerkmalen und Altersgruppen [Special Analysis Based on Data of the Time Use Survey 2012/13. Statistisches Bundesamt, Wiesbaden, Germany (2017).
47.
Destatis. Volkswirtschaftliche Gesamtrechnungen: Wichtige Zusammenhänge Im Überblick. Statistisches Bundesamt, Wiesbaden, Germany (2017).
48.
Destatis. Volkswirtschaftliche Gesamtrechnungen, Input-Output-Rechnung 2014. Fachserie 18 Reihe 1.4 (revision 2014, as of August 2017). Statistisches Bundesamt, Wiesbaden, Germany (2018).
49.
Sullivan SD, Mauskopf JA, Augustovski F et al. Budget impact analysis-principles of good practice: report of the ISPOR 2012 Budget Impact Analysis Good Practice II Task Force. Value Health. 17(1), 5–14 (2014).
50.
Krol M, Brouwer W. Unpaid work in health economic evaluations. Soc. Sci. Med. 144, 127–137 (2015).
51.
Malinowski KP, Kawalec P. The indirect costs of ankylosing spondylitis: a systematic review and meta-analysis. Expert Rev. Pharmacoeconomics Outcomes Res. 15(2), 285–300 (2015).
52.
Boonen A, Brinkhuizen T, Landewé R, Van Der Heijde D, Severens JL. Impact of ankylosing spondylitis on sick leave, presenteeism and unpaid productivity, and estimation of the societal cost. Ann. Rheum. Dis. 69(6), 1123–1128 (2010).
53.
Tran-Duy A, Boonen A, Van de Laar MAFJ, Severens JL. Impact on total population health and societal cost, and the implication on the actual cost-effectiveness of including tumour necrosis factor-α antagonists in management of ankylosing spondylitis: a dynamic population modelling study. Cost Eff. Resour. Alloc. 13(1), 1–12 (2015).
54.
Himmler S, Müller M, Bintu S, Ostwald D. A case study applying a novel approach to estimate the social impact of a medical innovation - the use of secukinumab for psoriatic arthritis in Germany. Expert Rev. Pharmacoecon. Outcomes Res. 20(4), 369–378 (2020).
55.
Cooksey R, Husain MJ, Brophy S et al. The cost of ankylosing spondylitis in the UK using linked routine and patient-reported survey data. PLoS ONE 10(7), 1–17 (2015).
56.
Uludag M, Unalan H, Tuzun S et al. Assessment of quality of life and depression in spouses of patients with ankylosing spondylitis. Rheumatol. Int. 32(11), 3511–3516 (2012).
57.
Brouwer WBF, van Exel NJA, van de Berg B, Dinant HJ, Koopmanschap MA, van den Bos GAM. Burden of caregiving: evidence of objective burden, subjective burden, and quality of life impacts on informal caregivers of patients with rheumatoid arthritis. Arthritis Care Res. (Hoboken). 51(4), 570–577 (2004).
58.
Rafia R, Ara R, Packham J, Haywood K, Healey E. Healthcare costs and productivity losses directly attributable to ankylosing spondylitis. Clin. Exp. Rheumatol. 30(2), 246–253 (2012).
59.
Krol M, Brouwer WBF, Severens JL, Kaper J, Evers Silvia MAA. Productivity cost calculations in health economic evaluations: correcting for compensation mechanisms and multiplier effects. Soc. Sci. Med. 75(11), 1981–1988 (2012).
Information & Authors
Information
Published In
Pages: 143 - 155
PubMed: 33252266
Copyright
© 2020 Future Medicine Ltd.
History
Received: 11 May 2020
Accepted: 29 October 2020
Published online: 30 November 2020
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The societal impact of a biologic treatment of ankylosing spondylitis: a case study based on secukinumab. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0077
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Foteini Tsotra, Kyle Dunton, Mats Rosenlund, Lena Steinbeck, Sukhvinder Johal, Estimating the societal impact of medical interventions: a case study in metastatic breast cancer, Journal of Comparative Effectiveness Research, 10.57264/cer-2026-0005, 15, 6, (2026).
- Dennis A. Ostwald, Maike Schmitt, Platon Peristeris, Tim Gerritzen, Adeline Durand, The Societal Impact of Inclisiran in England: Evidence From a Population Health Approach, Value in Health, 10.1016/j.jval.2023.05.002, 26, 9, (1353-1362), (2023).
- Foteini Tsotra, Mathias Kappel, Platon Peristeris, Giovanni Bader, Eva Levi, Nicola Lister, Ankur Malhotra, Dennis A Ostwald, The societal impact of early intensified treatment in patients with type 2 diabetes mellitus, Journal of Comparative Effectiveness Research, 10.2217/cer-2022-0110, 11, 16, (1185-1199), (2022).
- Ahmed H. Seddik, Nima Melzer, Foteini Tsotra, Dennis A. Ostwald, The Societal Economic Impact of Secukinumab in First-Line Treatment of Moderate to Severe Plaque Psoriasis in Germany: An Open-Cohort Simulation, PharmacoEconomics - Open, 10.1007/s41669-021-00305-3, 6, 2, (265-275), (2021).
- Ahmed H. Seddik, Claudio Schiener, Dennis A. Ostwald, Sara Schramm, Jasper Huels, Zaza Katsarava, Social Impact of Prophylactic Migraine Treatments in Germany: A State-Transition and Open Cohort Approach, Value in Health, 10.1016/j.jval.2021.04.1281, 24, 10, (1446-1453), (2021).