Economic burden of readmission due to postoperative cerebrospinal fluid leak in Chinese patients
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This real-world data study investigated the economic burden and associated factors of readmissions for cerebrospinal fluid leakage (CSFL) post-cranial, transsphenoidal, or spinal index surgeries. Methods: Costs of CSFL readmissions and index hospitalizations during 2014–2018 were collected. Readmission cost was measured as absolute cost and as percentage of index hospitalization cost. Factors associated with readmission cost were explored using generalized linear models. Results: Readmission cost averaged US$2407–6106, 35–94% of index hospitalization cost. Pharmacy costs were the leading contributor. Generalized linear models showed transsphenoidal index surgery and surgical treatment for CSFL were associated with higher readmission costs. Conclusion: CSFL readmissions are a significant economic burden in China. Factors associated with higher readmission cost should be monitored.
Cerebrospinal fluid leakage (CSFL) is a serious complication of cranial, spinal and transsphenoidal surgeries. The incidence rate of CSFL varies from 0.3 to 14.3%, depending on the types of the underlying neuro- and spinal surgery [1–6]. Postoperative CSFL may present as headaches, projectile vomiting, neck stiffness or other signs of meningeal irritation [7]. Serious sequelae, such as meningitis, seizures, hemorrhage, cerebral abscess or death have also been reported [7–9].
Postoperative CSFL may prolong hospital stay or lead to reoperation and increase healthcare costs [7,8,10–16]. Postoperative CSFLs were also reported as a common cause of readmission after neuro- and spinal surgeries [10]. Thirty-day readmission has been demonstrated as a major driver of total hospitalization expenditure growth [17–20]. Most of the aforementioned disease burden studies were conducted in the US or European countries [12,13,15,16]. These studies primarily focused on the burden of CSFLs during the same hospital stay as the initial neuro- or spinal surgery. Our literature review found only one study involving postoperative CSFL patients in China [11]. The healthcare system in China differs significantly from those in the US and Europe. It is difficult to estimate the economic burden of CSFLs in China based on the published results from developed countries.
As control of healthcare expenditure is a major policy priority in China, it is important to gain a better understanding of CSFL readmission costs. Cao et al. examined patients readmitted for CSFL after surgery for cerebellopontine angle tumors. They reported the average readmission costs of RMB 18,140 to 28,894 (approximately US$2800–4500) [11]. However, the study was a single-center study with limited representativeness. The published manuscript did not report any healthcare resource utilization details. To address the information needs for public health decision makers, we conducted this real-world data (RWD) study to investigate the detailed cost structure of CSFL readmissions within 30 days after cranial, transsphenoidal and spinal surgery. Statistical analysis was performed to identify potential influencing factors associated with readmission costs and length of stay (LOS).
Materials & methods
Study population & analysis set selection
This retrospective RWD study used data extracted from the electronic medical record and medical claim databases managed by the Shanghai Information Center for Health. The databases collect patient records from more than 450 public health institutions throughout Shanghai. During the study period of 2014–2018, the databases covered 6 million uniquely identifiable patients, with 10.5 million inpatient records. The database contains patient demographic information, hospitalization details (diagnosis, operations in the same hospitalization, date of visit, LOS and health insurance type) and categorized costs (such as surgery service costs, pharmacy costs, medical supply costs, etc.). The data used in this study were fully de-identified for patient privacy protection and were exempt from an institutional review board approval.
Two cohorts were analyzed in this study: a Readmission Group and a Benchmark Group. The Readmission Group included patients readmitted for CSFL after index surgery discharge during 2014–2018. The types of index surgeries involved in this study were cranial, spinal and transsphenoidal surgeries that were originally performed. The Benchmark Group included patients who underwent one of the index surgeries during 2014–2018. The attrition flows for both cohorts were shown in Figure 1.
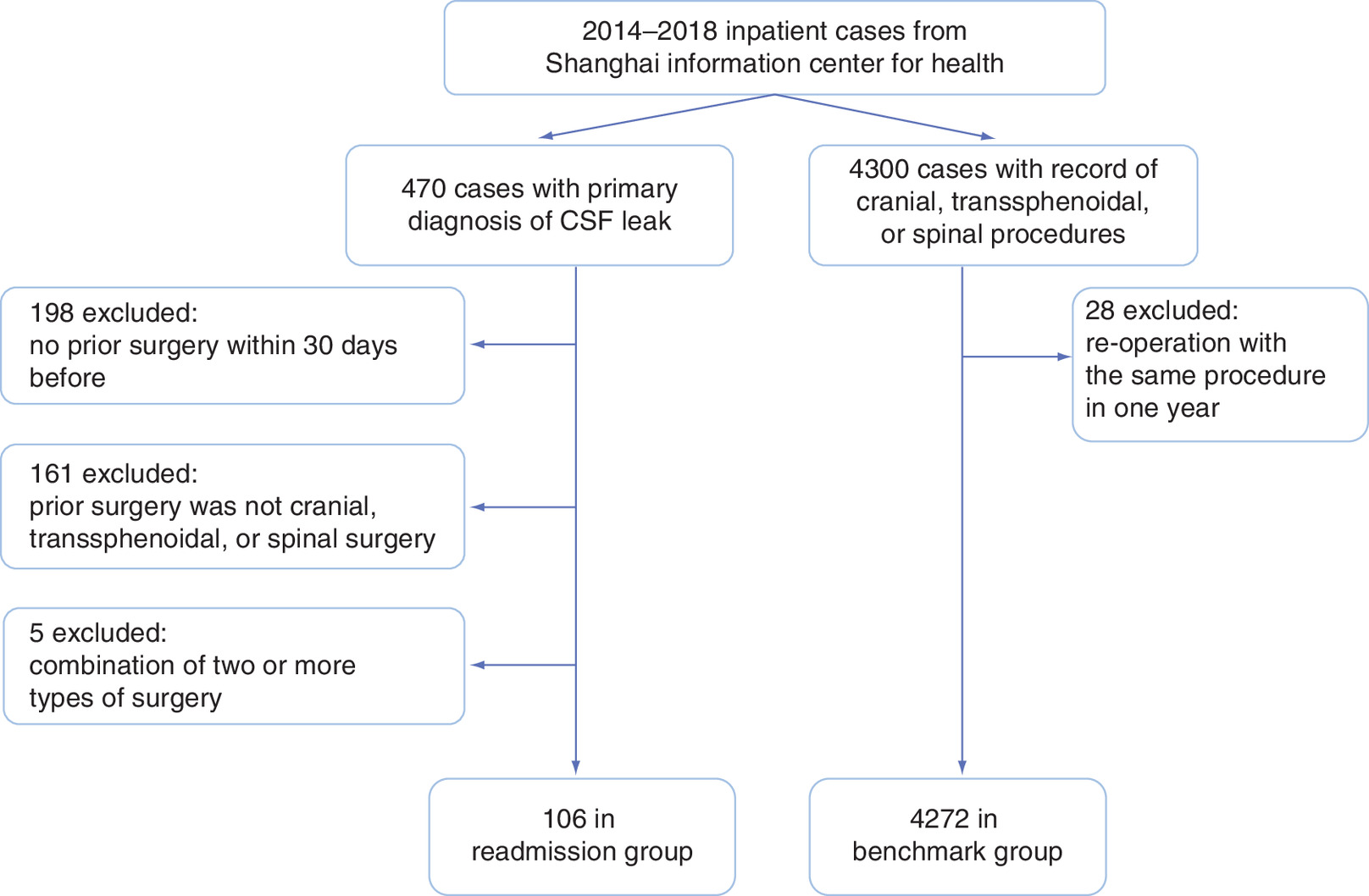
Figure 1. Attrition flow of Readmission Group and Benchmark Group patients.
CSF: Cerebrospinal fluid.
Index surgeries were selected using the standardized operation names in the database. We manually categorized the surgeries as cranial, transsphenoidal or spinal. Specifically, ‘resection of skull base tumor,’ ‘resection of sellar region tumor,’ ‘resection of meningioma,’ ‘decompression of optic nerve,’ ‘decompression of trigeminal nerve,’ ‘removal of intracranial hematoma,’ ‘removal of intracerebral hematoma,’ ‘craniotomy for decompression’ and ‘cranioplasty’ were classified as the cranial surgery subgroup; transsphenoidal hypophysectomy surgeries were classified as transsphenoidal surgery; “spinal fixation” was classified as spinal surgery. Patients who underwent more than one type of the index surgeries were excluded.
CSFL readmissions were first selected using International Classification of Diseases, tenth edition (ICD-10) codes [21]. The primary diagnosis codes for readmission must have had one of the codes under Cerebrospinal Fluid Leak [G96.0]. The initial hits were further filtered by excluding cases with multiple index surgery types, cases without any of the index surgery types and cases with CSFL hospitalization more than 30 days after previous discharge.
The index hospitalization was defined as the hospitalization in which one of the index surgeries occurred. In this study, index hospitalization costs were estimated using the Benchmark Group. This was because the total case count in the Readmission Group was relatively small. Estimation of index hospitalization costs using only Readmission Group would introduce large variation. Therefore, the Benchmark Group was created to leverage a much larger sample size for a more stable and accurate estimation of the index hospitalization costs.
Patients in both groups were classified into subgroups based on index surgery categories. To ensure that the subgroups in both cohorts were comparable, propensity score matching (PSM) was performed prior to statistical comparison.
Cost definition
The economic burden of readmission due to CSFL was defined as the direct medical cost of readmission, in other words, all itemized charges billed to patients and insurance by hospitals. Readmission costs were calculated from the Readmission Group data, while index hospitalization costs were calculated using the Benchmark Group data. All costs reported were converted to USD based on the currency exchange rate of RMB 6.8 to USD 1 on December 31, 2018. No inflation adjustment was applied to the costs in this study.
Study variables
The primary outcome was the total cost of readmission for CSFL. We further examined components of the total CSFL readmission cost, including pharmacy costs, supply costs and surgery service costs. LOS for CSFL readmission was also investigated.
Factors which might be predictive of readmission burden were analyzed using the Readmission Group exclusively. These included three major categories: patient characteristics, index surgery type and readmission characteristics. Patient characteristics included age, gender and comorbidities (diabetes and hypertension). Readmission characteristics included discharge-to-readmission days (number of days between readmission and index hospitalization discharge), CSFL treatment types (conservative care or surgical intervention) and number of surgical interventions for CSFL.
Statistical analysis
Descriptive statistics of patient characteristics were calculated for the Readmission Group and Benchmark Group; descriptive statistics of readmission characteristics were computed for the Readmission Group only. The mean and standard deviation (SD) were calculated for quantitative variables. The distributions for categorical variables were captured using proportions. Patient characteristics were compared between the two groups per index surgery type. Two-sided Welch's t-test was used for comparing quantitative variables since we did not assume equal variances between groups [22]. Pearson's chi-square test was used to compare gender composition between groups because there were no expected probabilities less than 5, and Fisher's exact test was used to compare comorbidity proportions (diabetes and hypertension) [22]. Matching was deemed necessary when the p-value between groups was less than 0.1. PSM was performed using the MatchIt package for R 3.5.1 [23]. Nearest neighbor matching was applied, with a matching ratio of 1 to 10.
In addition to the absolute values of readmission costs, relative costs were reported. For each index surgery type, the costs of CSFL readmission were compared with index hospitalization costs. For each readmission component cost, we report the relative magnitude as a percentage of corresponding index hospitalization component cost:
Within the Readmission Group, generalized linear models (GLMs) [24] were used to investigate the relationship of a selected group of factors with each healthcare resource utilization outcome separately. Utilization outcomes included total cost, total pharmacy costs, disposable medical supply costs and LOS.
The independent variables in the GLMs were patient age and gender, type of index surgery, time to readmission and CSFL treatment type.
GLMs were performed using the GLM function in base R 3.5.1 [25] and the glm.nb function in the MASS package [26]. Distributions of the dependent variables were shown in Supplementary Figure 1. GLMs were fitted with a gamma distribution and log link for cost outcomes [27–29], while a negative binomial distribution and log link were applied to LOS [30–32]. For ease of interpretation, we applied the natural exponential function to the coefficients for reporting.
For the independent variables, continuous variables were scaled by their standard deviations, with resulting standard deviations equal to 1. Centering was not applied as no interaction terms were used [33].
Results
The Readmission Group included a total of 106 patients, with 56 in the cranial surgery subgroup, 18 in the spinal surgery subgroup and 32 in the transsphenoidal surgery subgroup.
After PSM, the Benchmark Group included 3474 patients, with 2974, 180 and 320 in the cranial, spinal and transsphenoidal subgroups, respectively.
Descriptive statistics
Patient characteristics of both groups are shown in Table 1. according to index surgery subgroups. In the cranial surgery subgroup, patient characteristics were comparable between the Readmission and Benchmark Groups. Matching was applied to the transsphenoidal surgery and spinal surgery subgroups because of unmatched baseline characteristics. Overall, patient age ranged from 43 to 54 years. Patient gender was mostly balanced. Cases of diabetes and hypertension were few in both groups.
| Charactetistics | Readmission group | Benchmark group | p-value |
|---|---|---|---|
| Cranial surgery† | |||
| – N | 56 | 2974 | – |
| – Age (years, mean ± SD) | 46.6 ± 14.20 | 46.5 ± 20.05 | 0.944 |
| Gender (%) | |||
| – Male | 53.15 | 55.50 | 0.274 |
| – Female | 46.85 | 44.50 | |
| Comorbidities (%) | |||
| – Diabetes | 0.90 | 2.55 | 0.637 |
| – Hypertension | 6.31 | 8.82 | 0.169 |
| Spinal surgery (matched)‡ | |||
| – N | 18 | 180 | – |
| – Age (years, mean ± SD) | 52.9 ± 19.22 | 50.6 ± 12.37 | 0.625 |
| Gender (%) | |||
| – Male | 50.00 | 58.33 | 0.666 |
| – Female | 50.00 | 41.67 | |
| Comorbidities (%) | |||
| – Diabetes | 0 | 0 | 1 |
| – Hypertension | 1.67 | 6.11 | 0.121 |
| Transsphenoidal surgery (matched)‡ | |||
| – N | 32 | 320 | |
| Age (years, mean ± SD) | 53.7 ± 11.16 | 54.6 ± 11.35 | 0.676 |
| Gender (%) | |||
| – Male | 37.50 | 43.13 | 0.670 |
| – Female | 62.50 | 56.88 | |
| Comorbidities (%) | |||
| – Diabetes | 3.13 | 2.82 | 1 |
| – Hypertension | 6.25 | 5.00 | 0.673 |
†
The cranial surgery subgroup was balanced, and no matching was applied.
‡
The spinal and transsphenoidal surgery subgroups were matched using age, gender and comorbidities with a ratio of 10. The unmatched results are shown in Supplementary Table 1.
SD: Standard deviation.
Readmission characteristics of the Readmission Group are shown in Table 2. In all, 61% of spinal surgery patients received only conservative therapy, and 28 and 32% of cranial surgery and transsphenoidal surgery patients received conservative therapy, respectively. The average time from index hospitalization discharge to readmission was 15, 20 and 17 days in the subgroups of spinal surgery, transsphenoidal surgery and cranial surgery, respectively. Readmission LOS was similar between cranial and spinal surgery patients, with an average of 17 days, while transsphenoidal surgery patients had a slightly longer LOS, with an average of 19 days.
| Characterisics | Cranial (n = 56) | Spinal (n = 18) | Transsphenoidal (n = 32) |
|---|---|---|---|
| Type of therapy (%) | |||
| – Conservative therapy | 32% | 61% | 28% |
| – Surgical intervention | 68% | 39% | 72% |
| N surgical interventions (n, mean) | 0.89 | 0.50 | 0.91 |
| Duration before readmission (days, mean) | 17.25 | 15.44 | 20.34 |
| Length of stay (days, mean) | 17.5 | 17.9 | 19.2 |
Hospitalization costs
Readmission costs for CSFL after the three different types of index surgery are shown in Table 3. Patients who received transsphenoidal index surgery incurred the highest total readmission costs (US$6106/RMB 41,521), followed by cranial surgery (US$3753/RMB 25,520) and spinal surgery (US$2407/RMB 16,370). Compared with index hospitalization costs, the economic burden for CSFL was quite substantial. In particular, the readmission cost after transsphenoidal index surgery reached 94.14% of the index hospitalization cost. For spinal and cranial index surgeries, readmission costs reached 46.90% and 34.94% of index hospitalization costs, respectively. Notably, pharmacy costs for readmission after transsphenoidal index surgery were equivalent to 150.04% of pharmacy costs for the index hospitalization itself. Pharmacy costs for readmission after spinal surgery were also much higher compared with those of the index hospitalization, with an increase of 200.99%.
| Surgery type | Readmission group | Benchmark group | Δ% cost | ||
|---|---|---|---|---|---|
| N | CSFL readmission costs (mean ± SD) | N | Index hospitalization costs (mean ± SD) | ||
| Cranial surgery‡ | |||||
| – Total cost | 56 | 3753 ± 4678 | 2974 | 10,740 ± 6223 | 34.94 |
| – Surgery service cost | 427 ± 705 | 1472 ± 1687 | 29.02 | ||
| – Pharmacy cost | 1674 ± 2863 | 2725 ± 2892 | 61.43 | ||
| – Supply cost | 739 ± 1006 | 2999 ± 2594 | 24.63 | ||
| Spinal surgery (matched)§ | |||||
| – Total cost | 18 | 2407 ± 2805 | 180 | 5133 ± 5433 | 46.90 |
| – Surgery service cost | 112 ± 215 | 589 ± 378 | 19.07 | ||
| – Pharmacy cost | 1383 ± 2039 | 688 ± 646 | 200.99 | ||
| – Supply cost | 264 ± 291 | 3191 ± 3193 | 8.29 | ||
| Transsphenoidal surgery (matched)§ | |||||
| – Total cost | 32 | 6106 ± 4022 | 96 | 6486 ± 2012 | 94.14 |
| – Surgery service cost | 679 ± 812 | 1198 ± 654 | 56.68 | ||
| – Pharmacy cost | 2614 ± 2118 | 1742 ± 1064 | 150.04 | ||
| – Supply cost | 1155 ± 1019 | 3309 ± 3129 | 34.91 | ||
†
The costs reported as central values are shown in Supplementary Tables 2 & 3.
‡
The cranial surgery subgroup was balanced, and no matching was applied.
§
The spinal and transsphenoidal surgery subgroups were matched using age, gender and comorbidities with a ratio of 10.
Readmission Group and Benchmark Group cost comparison (US$).
CSFL: Cerebrospinal fluid leakage; SD: Standard deviation.
Factors associated with economic burden
Exponentially transformed coefficients of independent variables from GLM fitting are reported in Table 4. Compared with cranial index surgery, transsphenoidal index surgery was associated with significantly higher readmission total cost and pharmacy costs, but not supply costs. Surgical treatments in CSFL readmission was associated with significantly increased total cost, pharmacy costs, supply costs and LOS. Delayed readmission, which meant longer time from index hospitalization discharge to readmission, was associated with an increased pharmacy cost.
| Factor | Total cost | Pharmacy costs | Supply costs | Length of stay |
|---|---|---|---|---|
| Therapy for CSFL† | ||||
| – Conservative therapy‡ | 0.28*** | 0.26*** | 0.17*** | 0.55*** |
| Prior surgery | ||||
| – Spinal surgery§ | 0.95 | 1.59 | 0.82 | 1.17 |
| – Transsphenoidal surgery§ | 1.84** | 1.99* | 1.43 | 1.05 |
| Duration before readmission¶ | 1.14 | 1.30* | 1.05 | 1.06 |
| Gender | 0.91 | 0.87 | 1.14 | 0.95 |
| Age | 1.02 | 1.07 | 0.84 | 1.03 |
†
Therapy for CSFL during readmission.
‡
Compared with surgical intervention for CSFL treatment.
§
Compared with cranial surgery.
¶
Days between readmission and prior discharge (scaled).
Significance values: ***p < 0.001; **p < 0.01; *p < 0.05.
CSFL: Cerebrospinal fluid leakage.
Discussion
This RWD study demonstrated the economic burden of readmission for CSFLs after cranial surgery, transsphenoidal surgery or spinal surgery in China. The excess burden of readmission has been widely recognized in the US. Thirty-day readmission is used as a healthcare quality measures [17–20]. The characteristics of 30-day readmission costs for postoperative CSFL in China had not been extensively investigated thus far.
Total readmission costs for the treatment of postoperative CSFLs were high, and most of these increased costs came from pharmacy costs rather than surgery service or supply costs. Total CSFL readmission costs ranged from US$2407 (RMB 16,370) to US$6106 (RMB 41,521), equivalent to 35–94% of the index hospitalization cost. These results are in line with those reported by Cao and his colleagues [11], who reported that the total economic cost for readmission ranged from RMB 18,140 to 28,894 (equivalent to US$2668 and US$4248, respectively, using the exchange rate of 6.8 in this study), and the LOS ranged from 18.2 to 19.8 days.
The economic burden of postoperative CSFLs varied by index surgery type. We found that readmission cost for CSFLs after transsphenoidal index surgery was almost equal to the total index hospitalization cost. This means that CSFL readmission could double the economic burden of a transsphenoidal surgery. For cranial and spinal index surgeries, readmission costs were also substantial relative to the index hospitalization cost. These phenomena are also consistent with other studies [12,13].
The relatively higher costs of readmission for post-transsphenoidal surgery CSFL readmission may be related to the risk of surgical site infection or meningitis. Transsphenoidal surgery is a clean-contaminated surgery because this approach traverses the nasal cavity [34]. To prevent infection, surgeons tend to use antibiotics [35,36], specifically in transsphenoidal surgery [37–39]. This may suggest higher antibiotic usage also occurs in cases of CSFLs post-transsphenoidal surgery to prevent or treat infection. Our data also showed that transsphenoidal index surgery is associated with increased pharmacy costs (Tables 2 & 3).
Type of treatment used for CSFL was related to index surgery type, as shown in Table 1. The transsphenoidal index surgery subgroup had the highest rate of surgical intervention. Several studies reported the rates of surgical intervention for postoperative CSFL after spinal [42–45], transsphenoidal [46–50] and cranial surgery [51–53]. These studies also confirmed that surgery treatment for CSFL was used more frequently after transsphenoidal surgery. One potential explanation is that prompt surgery treatment of CSFL was deemed more appropriate clinically to reduce the risk of infection [48,54–57].
Selection of CSFL treatment was an important factor affecting total readmission costs. Some authors have recommended a step-wise approach [40,41], though this may not be suitable for all index surgery types, such as transsphenoidal surgery. In the stepwise approach, the first choice is usually conservative therapy, such as bed rest with a reversed Trendelenburg position, caffeine, antibiotic therapy, etc. Lumbar drainage or other types of drainage are recommended if conservative therapy fails. Patients will be treated by surgical intervention if CSFL persists [11]. Cao and his colleagues demonstrated that patients who underwent surgical repair for CSFL incurred higher total costs than those who underwent conservative methods [11]. Our study showed that surgical intervention was associated with significantly increased total costs, and pharmacy costs specifically. This result may be because surgical intervention could necessitate the use of higher antibiotic dosages and other medication. It may also be that more severe cases of CSFL undergo surgical repair, as well as patients that have failed conservative therapy. In addition, due to the high risk of meningitis and low cure rate of conservative therapy [46,48], surgical repair is generally the first option for CSFL after transsphenoidal surgery. Therefore, the clinical need of surgical repair may outweigh financial considerations.
The burdens associated with the required surgical repairs for some cases of CSFL highlight the need for CSFL prevention. This is especially important for transsphenoidal surgery, as the data showed that transsphenoidal index surgery had the highest readmission costs among the three types of index surgeries. Closure of the surgical defect is the key to preventing postoperative CSFLs. Various closure techniques have been reported. Small dural tears may be repaired by watertight sutures, along with hemostyptic or hemostatic agents [40,58,59]. Where dural sutures are not sufficient or feasible, more sophisticated techniques can be applied. These techniques usually involve sealing the dura with suitable materials and supporting these materials with a buttress [14]. Autologous tissue, such as abdominal fat, thigh fat or nasoseptal flaps, can be used along with fibrin sealant or synthetic materials, including collagen sponges, gelfoam, dural substitutes or resorbable meshes [8,14,15,60].
In the US., researchers have also recognized CSFL as a concern for surgeons, particularly because of potential sequelae [8,10,16,52,54,61–64]. Multiple US studies documented CSFL incidence rates of 6.2–17.2% in cranial surgeries [52,54], 7.4–11.7% in spinal surgeries [61–63] and 3.9–13.5% in transsphenoidal surgeries [8,16,64,66]. Cote et al. reported that CSFL was the most common reason for reoperation after transsphenoidal surgery (63.6%), and the second most common reason for readmission (16.0%) [10].
The mean costs for treating CSFL during the index hospitalization were reported as US$46,026 after transsphenoidal surgery, about 86% of the index surgery itself [65]. CSFL were also linked to prolonged LOS of the index hospitalization, by 2.8–4 days on average, after transsphenoidal surgery. Chern et al. reported the median cost of CSFL repair to be US$50,401 after cranial surgery, including treatment during the index hospitalization and outpatient visits [15]. Studies from Germany reported an increase of EUR 10,350 and 10,643 (or US$9079 and 9336, based on the exchange rate of EUR 1 to US$1.14 on December 31, 2018) in DRG reimbursement after spinal and cranial surgery, respectively [12,13].
Our study suggested that the economic burdens of CSFL readmission are substantial relative to the index surgery. While healthcare systems vary between countries, this finding is consistent with similar studies in other countries. The financial consequences of CSFL readmission warrant serious consideration for healthcare systems globally. The association between index surgery type and CSFL readmission cost may be of interest for further investigations. Our results showed that the cost of CSFL readmission following transsphenoidal surgery was the highest among the three types of index surgeries. Marchiano et al. also reported that surgical repair for CSF rhinorrhea significantly increased costs of CSFL treatment [67]. As surgical repair for CSFL after transsphenoidal surgery is generally more common compared with other index surgeries, CSFL readmission following transsphenoidal surgery may also lead to significant increase in cost in other healthcare systems.
Limitations
Our study had several limitations. We focused on CSFLs readmissions and did not cover CSFLs which occurred in the same hospitalization period as the index surgery. In addition, our study excluded patients when CSFL was not their primary diagnosis for hospitalization. This may have biased the sample toward patients with more serious CSFL symptoms.
Conclusion
The economic burden of readmission due to CSFL readmission is substantial in China. Prevention measures of CSFL must be emphasized to reduce the economic burden caused by readmission. This is especially important for transsphenoidal surgery.
•
Postoperative cerebrospinal fluid leakage (CSFL) is a serious neuro- and spinal surgery complication that may lead to readmission.
•
Medical records of 30-day readmissions for CSFL during 2014–2018, as well as those of cranial, spinal and transsphenoidal index surgeries, were collected from a Shanghai municipal platform for hospital management.
•
The average total costs of the Readmission Group (n = 106) after cranial, transsphenoidal and spinal index surgeries were RMB 25,520 (US$3753), RMB 41,521 (US$6106), and RMB 16,370 (US$2407), respectively.
•
Compared with the Benchmark Group, these costs mean that readmission for CSFL increased the economic burden by 35, 94 and 47% for patients who underwent cranial, transsphenoidal and spinal index surgeries, respectively.
•
Across all three types of index surgery, pharmacy costs were the main contributors to CSFL readmission costs.
•
CSFL caused by transsphenoidal surgery was associated with increased total and pharmacy costs during readmission.
•
Surgical repair for CSFL was also associated with increased costs, however surgery may be clinically required.
•
Aside from controlling readmission costs, reduction of readmissions by taking preventive measures should also be emphasized.
Author contributions
Y Han and Y Wu were responsible for study conception and design; X Cui, S Zhang, W Tian and J Liu were responsible for data acquisition and management; S Wu was responsible for data analysis; S Wu, X Cui, Y Wu, M Wu and Y Han were responsible for drafting and revision of the manuscript.
Financial & competing interests disclosure
The study was funded by Johnson & Johnson Medical Company. M Wu and Y Wu are employees of Johnson & Johnson Medical Company. S Wu is an employee of WPP Health Practice (Shanghai), which received funding to conduct this study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
American Journal Experts (AJE) and Editage provided paid language editing services for this manuscript.
Supplementary Material
File (suppl_file.docx)
- Download
- 122.81 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Daming C, Yiwen S, Bin Z et al. Large vestibular schwannoma resection through the suboccipital retrosigmoid keyhole approach. J. Craniofac. Surg. 25(2), 463–468 (2014).
2.
Liu G, Huang L. Jizhu shoushu hou naojiye lou de zhenzhi jinzhan [Diagnosis and treatment of cerebrospinal fluid leakage in spinal surgery]. Jingyaotong Zazhi. 37(2), 150–153 (2016).
3.
Zhang G, Li W, Chen L. Xiong yaozhui houlu shoushu fasheng naojiye lou de xiangguan yuanyin ji chuli [The reasons and managements of cerebrospinal fluid leakage secondary to posterior thoracic and lumbar spinal surgery]. Zhongguo Shiyong Shenjing Jibing Zazhi 19(3), 15–17 (2016).
4.
Cong Z, Liu K, Wen G, Qiao L, Wang H, Ma C. Universal sellar anatomical reconstruction using the sellar floor flap after endoscopic pituitary adenoma surgery. Otolaryngol. Head. Neck. Surg. 158(4), 774–776 (2018).
5.
Yu J, Zhao Y, Wang Y, Zhang G, Gao D, Zheng X. Juda chuitixianliu jingdie shoushu hou fasheng najiye bilou de weixian yinsu fenxi [Analysis of risk factors on cerebrospinal fluid rhinorrhea after the treatment of giant pituitary adenomas by transsphenoidal surgery]. Xiandai Shengwu Yixue Jinzhan 14, 1128–1130 (2014).
6.
Fengbin Y, Xinyuan L, Xiaowei L, Xinwei W, Deyu C. Management and Outcomes of Cerebrospinal Fluid Leak Associated With Anterior Decompression for Cervical Ossification of the Posterior Longitudinal Ligament With or Without Dural Ossification. J. Spinal. Disord. Tech. 28(10), 389–393 (2015).
7.
Massoud VA, Fay A, Yoon MK. Cerebrospinal fluid leak as a complication of oculoplastic surgery. Semin. Ophthalmol. 29(5-6), 440–449 (2014).
8.
Ivan ME, Iorgulescu JB, El-Sayed I et al. Risk factors for postoperative cerebrospinal fluid leak and meningitis after expanded endoscopic endonasal surgery. J. Clin. Neurosci. 22(1), 48–54 (2015).
9.
Balasubramaniam C, Rao SM, Subramaniam K. Management of CSF leak following spinal surgery. Childs. Nerv. Syst. 30(9), 1543–1547 (2014).
10.
Cote DJ, Dasenbrock HH, Muskens IS et al. Readmission and other adverse events after transsphenoidal surgery: prevalence, timing, and predictive factors. J. Am. Coll. Surg. 224(5), 971–979 (2017).
11.
Cao W, Xin T, Liu W, Zhang Y. Qiaoxiaonao jiaoqu zhongliu shuhou yinnixing naojiye lou linchuang fenxi [Clinical analysis of latent cerebrospinal fluid leakage after cerebellopontine angle tumor surgery]. Shangdong Daxue Xuebao. 51(12), 78–81 (2013).
•• Examines costs of readmission for cerebrospinal fluid leakage (CSFL) after surgery for cerebellopontine angle tumors with follow-up periods varying from 6 to 35 months.
12.
Piek J, Weber C, Kundt G et al. Pharmacoeconomical consequences of postoperative CSF leaks after intracranial surgery–a prospective analysis. J. Neurol. Surg. A. Cent. Eur. Neurosurg. 73(1), 25–28 (2012).
• This study from Germany examined the economic aspects of postoperative CSFLs that occurred during the same stay as the initial intracranial surgery.
13.
Weber C, Piek J, Gunawan D. Health care costs of incidental durotomies and postoperative cerebrospinal fluid leaks after elective spinal surgery. Eur. Spine. J. 24(9), 2065–2068 (2015).
• Investigates the additional health care costs of postoperative CSFLs after spinal surgery in Europe.
14.
Zhou Q, Yang Z, Wang X et al. Risk factors and management of intraoperative cerebrospinal fluid leaks in endoscopic treatment of pituitary adenoma: analysis of 492 patients. World Neurosurg. 101, 390–395 (2017).
15.
Chern A, Hunter JB, Bennett ML. Cost analysis of cerebrospinal fluid leaks and cerebrospinal fluid leak prevention in patients undergoing cerebellopontine angle surgery. Otol. Neurotol. 38(1), 147–151 (2017).
• This study from the US conducted an economic evaluation of a surgical intervention technique for CSFL after a type of cranial surgery.
16.
Asemota AO, Ishii M, Brem H, Gallia GL. Comparison of complications, trends, and costs in endoscopic vs microscopic pituitary surgery: analysis from a US Health Claims Database. Neurosurgery 81(3), 458–472 (2017).
• This study from the US investigated the additional costs and length of stay of a number of complications after a type of cranial surgery, including CSFL.
17.
Kind AJH, Jencks S, Brock J et al. Neighborhood socioeconomic disadvantage and 30-day rehospitalization: a retrospective cohort study. Ann. Intern. Med. 161(11), 765–774 (2014).
18.
Mahmoudi E, Lu Y, Chang S-C et al. The Associations of Hospital Volume, Surgeon Volume, and Surgeon Experience with Complications and 30-Day Rehospitalization after Free Tissue Transfer: A National Population Study. Plast. Reconstr. Surg. 140(2), 403–411 (2017).
19.
Berenson RA, Paulus RA, Kalman NS. Medicare's readmissions-reduction program – a positive alternative. N. Engl. J. Med. 366(15), 1364–1366 (2012).
20.
Moschini M, Gandaglia G, Fossati N et al. Incidence and predictors of 30-day readmission after robot-assisted radical prostatectomy. Clin. Genitourin. Cancer 15(1), 67–71 (2017).
21.
Brämer GR. International statistical classification of diseases and related health problems. Tenth revision. World Health Stat Q. 41(1), 32–36 (1988).
22.
Sheskin DJ. Handbook of Parametric and Nonparametric Statistical Procedures (3rd Edition). CRC Press, FL, USA (2003).
23.
Ho DE, Imai K, King G, Stuart EA. MatchIt: nonparametric preprocessing for parametric causal inference. J. Stat. Soft. 42(8), (2011).
24.
McCullagh P. Generalized linear models. Eur. J. Oper. Res. 16(3), 285–292 (1984).
25.
R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria (2017).
26.
Venables WN, Ripley BD. Modern Applied Statistics with S (4th Edition). [Nachdr.]. Springer, NY, USA (2002).
27.
Silver SA, Long J, Zheng Y, Chertow GM. Cost of acute kidney injury in hospitalized patients. J. Hosp. Med. 12(2), 70–76 (2017).
28.
Berkowitz SA, Seligman HK, Rigdon J, Meigs JB, Basu S. Supplemental Nutrition Assistance Program (SNAP) participation and health care expenditures among low-income adults. JAMA Intern. Med. 177(11), 1642–1649 (2017).
29.
Aslam MV, Owusu-Edusei K, Marks SM et al. Number and cost of hospitalizations with principal and secondary diagnoses of tuberculosis, United States. Int. J. Tuberc. Lung Dis. 22(12), 1495–1504 (2018).
30.
Inabnit LS, Blanchette C, Ruban C. Comorbidities and length of stay in chronic obstructive pulmonary disease patients. COPD 15(4), 355–360 (2018).
31.
Ryan M, Donato BMK, Irish W, Gasteyger C, L'Italien G, Laurence J. Economic impact of early-in-hospital diagnosis and initiation of eculizumab in atypical haemolytic uraemic syndrome. Pharmacoeconomics 38(3), 307–313 (2020).
32.
Rowell-Cunsolo TL, Liu J, Shen Y, Britton A, Larson E. The impact of HIV diagnosis on length of hospital stay in New York City, NY, USA. AIDS Care 30(5), 591–595 (2018).
33.
Yi Y. On the evaluation of main effects in multiplicative regression models. J. Market Res. Soc. 31(1), 133–138 (1989).
34.
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Am. J. Infect. Control. 27(2), 97–132; quiz 133–134; discussion 96 (1999).
35.
Berríos-Torres SI, Umscheid CA, Bratzler DW et al. Centers for Disease Control and Prevention Guideline for the prevention of surgical site infection, 2017. JAMA Surg. 152(8), 784–791 (2017).
36.
Vila PM, Zenga J, Jackson RS. Antibiotic prophylaxis in clean-contaminated head and neck surgery: a systematic review and meta-analysis. Otolaryngol. Head. Neck. Surg. 157(4), 580–588 (2017).
37.
Little AS, White WL. Prophylactic antibiotic trends in transsphenoidal surgery for pituitary lesions. Pituitary 14(2), 99–104 (2011).
38.
Moldovan ID, Agbi C, Kilty S, Alkherayf F. A systematic review of prophylactic antibiotic use in endoscopic endonasal transsphenoidal surgery for pituitary lesions. World Neurosurg. 128, 408–414 (2019).
39.
Somma T, Maraolo AE, Esposito F et al. Efficacy of ultra-short single agent regimen antibiotic chemo-prophylaxis in reducing the risk of meningitis in patients undergoing endoscopic endonasal transsphenoidal surgery. Clin. Neurol. Neurosurg. 139, 206–209 (2015).
40.
Fang Z, Tian R, Jia Y-T, Xu T-T, Liu Y. Treatment of cerebrospinal fluid leak after spine surgery. Chin. J. Traumatol. 20(2), 81–83 (2017).
41.
Sang D, Shi W, Chen J. Waishangxing naojiye lou 50 li linchuang zhiliao jingyan fenxi [Analysis of 50 cases of traumatic cerebrospinal fluid leakage]. Zhongguo Chufang Yao 12, 92–93 (2014).
42.
Khazim R, Dannawi Z, Spacey K et al. Incidence and treatment of delayed symptoms of CSF leak following lumbar spinal surgery. Eur. Spine J. 24(9), 2069–2076 (2015).
43.
Barbanti Bròdano G, Serchi E, Babbi L et al. Is lumbar drainage of postoperative cerebrospinal fluid fistula after spine surgery effective? J. Neurosurg. Sci. 58(1), 23–27 (2014).
44.
Tosun B, Ilbay K, Kim MSM, Selek O. Management of persistent cerebrospinal fluid leakage following thoraco-lumbar surgery. Asian. Spine J. 6(3), 157–162 (2012).
45.
Fourney DR, Abi-Said D, Rhines LD et al. Simultaneous anterior-posterior approach to the thoracic and lumbar spine for the radical resection of tumors followed by reconstruction and stabilization. J. Neurosurg. 94(Suppl. 2), 232–244 (2001).
46.
Fan S, Chen Y, Cao Y et al. The effectiveness of lumbar drainage in the management of delayed or recurrent cerebrospinal fluid leaks: a retrospective case series in a single center. World Neurosurg. 129, e845–e850 (2019).
47.
Lee JJ, Kim HY, Dhong H-J et al. Delayed cerebrospinal fluid leakage after treatment of skull base tumors: case series of 9 patients. World Neurosurg. 132, e591–e598 (2019).
48.
Caggiano C, Penn DL, Laws ER. The role of the lumbar drain in endoscopic endonasal skull base surgery: a retrospective analysis of 811 cases. World Neurosurg. 117, e575–e579 (2018).
• This study found that a substantial proportion of patients with postoperative CSFL did not recover after lumbar drainage, and surgical repair was required.
49.
Zhang C, Ding X, Lu Y, Hu L, Hu G. Cerebrospinal fluid rhinorrhoea following transsphenoidal surgery for pituitary adenoma: experience in a Chinese centre. Acta Otorhinolaryngol. Ital. 37(4), 303–307 (2017).
50.
Zhan R, Chen S, Xu S, Liu JK, Li X. Postoperative low-flow cerebrospinal fluid leak of endoscopic endonasal transsphenoidal surgery for pituitary adenoma–wait and see, or lumbar drain? J. Craniofac. Surg. 26(4), 1261–1264 (2015).
51.
Jito J, Nitta N, Nozaki K. Delayed cerebrospinal fluid leak after watertight dural closure with a polyethylene glycol hydrogel dural sealant in posterior fossa surgery: case report. Neurol. Med. Chir. (Tokyo) 54(8), 634–639 (2014).
52.
Hutter G, von Felten S, Sailer MH, Schulz M, Mariani L. Risk factors for postoperative CSF leakage after elective craniotomy and the efficacy of fleece-bound tissue sealing against dural suturing alone: a randomized controlled trial. J. Neurosurg. 121(3), 735–744 (2014).
53.
Arlt F, Trantakis C, Krupp W et al. Cerebrospinal fluid leak after microsurgical surgery in vestibular schwannomas via retrosigmoidal craniotomy. Neurol. Res. 33(9), 947–952 (2011).
54.
Ransom ER, Palmer JN, Kennedy DW, Chiu AG. Assessing risk/benefit of lumbar drain use for endoscopic skull-base surgery. Int. Forum. Allergy. Rhinol. 1(3), 173–177 (2011).
55.
Presutti L, Mattioli F, Villari D, Marchioni D, Alicandri-Ciufelli M. Transnasal endoscopic treatment of cerebrospinal fluid leak: 17 years’ experience. Acta Otorhinolaryngol. Ital. 29(4), 191–196 (2009).
56.
Scholsem M, Scholtes F, Collignon F et al. Surgical management of anterior cranial base fractures with cerebrospinal fluid fistulae: a single-institution experience. Neurosurgery 62(2), 463–469; discussion 469–471 (2008).
57.
Shiley SG, Limonadi F, Delashaw JB et al. Incidence, etiology, and management of cerebrospinal fluid leaks following trans-sphenoidal surgery. Laryngoscope 113(8), 1283–1288 (2003).
58.
Li J, Liao Y, Cao G, Zhou Y, Zhou M. Lunao shoushu hou qiekou naojiye lou zhiliao tihui [Experience on treatment of cerebrospinal fluid leakage after craniocerebral operation]. Zhonghua Shenjing Chuangshang Waike Dianzi Zazhi 1(6), 334–336 (2015).
59.
Li Z, Qu W, Ding J. Jingzhui qianlu shoushu bingfa naojiye lou de zhiliao [Therapy of cerebrospinal fluid leakage in anterior approach cervical surgery]. Shengwu Guke Cailiao Yu Linchuang Yanjiu 11, 21–23 (2014).
60.
Nakamura H, Matsuyama Y, Yoshihara H et al. The effect of autologous fibrin tissue adhesive on postoperative cerebrospinal fluid leak in spinal cord surgery: A randomized controlled trial. Spine 30(13), E347–E351 (2005).
61.
Sciubba DM, De la Garza Ramos R, Goodwin CR et al. Clinical, surgical, and molecular prognostic factors for survival after spinal sarcoma resection. Neurosurg. Focus 41(2), E9 (2016).
62.
Wong AP, Shih P, Smith TR et al. Comparison of symptomatic cerebral spinal fluid leak between patients undergoing minimally invasive versus open lumbar foraminotomy, discectomy, or laminectomy. World Neurosurg. 81(3-4), 634–640 (2014).
63.
Jankowitz BT, Atteberry DS, Gerszten PC et al. Effect of fibrin glue on the prevention of persistent cerebral spinal fluid leakage after incidental durotomy during lumbar spinal surgery. Eur. Spine J. 18(8), 1169–1174 (2009).
64.
Patel PN, Stafford AM, Patrinely JR et al. Risk factors for intraoperative and postoperative cerebrospinal fluid leaks in endoscopic transsphenoidal sellar surgery. Otolaryngol. Head. Neck. Surg. 158(5), 952–960 (2018).
65.
Parikh A, Adapa A, Sullivan SE, McKean EL. Predictive factors, 30-day clinical outcomes, and costs associated with cerebrospinal fluid leak in pituitary adenoma resection. J. Neurol. Surg. B. Skull. Base. 81(1), 43–55 (2020).
66.
Dlouhy BJ, Madhavan K, Clinger JD et al. Elevated body mass index and risk of postoperative CSF leak following transsphenoidal surgery. J. Neurosurg. 116(6), 1311–1317 (2012).
67.
Marchiano E, Carniol ET, Guzman DE, Raikundalia MD, Baredes S, Eloy JA. An analysis of patients treated for cerebrospinal fluid rhinorrhea in the United States from 2002 to 2010. J. Neurol. Surg. B. Skull. Base 78(1), 18–23 (2017).
Information & Authors
Information
Published In
Pages: 1105 - 1115
PubMed: 33112181
Copyright
© 2020 Future Medicine Ltd.
History
Received: 30 April 2020
Accepted: 30 April 2020
Published online: 28 October 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Economic burden of readmission due to postoperative cerebrospinal fluid leak in Chinese patients. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0067
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Hongwei Wang, Hong Yuan, Bin Zheng, Xiaoying Wang, Yan Gao, Xiaoyu Wang, Huan Zhang, Xinyuan Zhao, Zhihao Zhang, Hailong Yu, Risk factors of cerebrospinal fluid leakage following posterior lumbar interbody fusion for lumbar degenerative disease: A retrospective observational study of 684 patients, Medicine, 10.1097/MD.0000000000049901, 105, 30, (e49901), (2026).
- Jie Wang, Zhuoyuan Li, Yunfeng Wang, Zheng Peng, Xiaojian Li, Chunlei Chen, Huiying Yan, Wei Jin, Fang Wang, Lu Chen, Chunhua Hang, Wei Li, Analysis of Risk Factors and Development of a Prediction Model for Intraoperative Cerebrospinal Fluid Leakage During Transsphenoidal Pituitary Adenoma Surgery, Journal of Evidence-Based Medicine, 10.1111/jebm.70013, 18, 1, (2025).
- Ji-Yan Jin, Miao Yu, Rui-Feng Xu, Yu Sun, Bao-Hua Li, Fei-Fei Zhou, Risk Factors for Cerebrospinal Fluid Leakage After Extradural Spine Surgery: A Meta-Analysis and Systematic Review, World Neurosurgery, 10.1016/j.wneu.2023.08.075, 179, (e269-e280), (2023).
- Wenpei Ding, Yue Ma, Chao Ma, Daniel C Malone, Aixia Ma, Wenxi Tang, Lei Si, The lifetime cost estimation of human papillomavirus-related diseases in China: a modeling study, Journal of Translational Internal Medicine, 10.2478/jtim-2021-0039, 9, 3, (200-211), (2021).