Surfactant therapy for meconium aspiration syndrome in neonates: a systematic overview of systematic reviews and recent clinical trials
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To conduct a systematic overview of systematic reviews (SRs) and randomized clinical trials (RCTs) on surfactant therapy in neonatal meconium aspiration syndrome. Methods: We searched EMBASE, PROQUEST and PubMed to summarize the different effects of surfactant lung lavage and bolus surfactant therapies in neonates with meconium aspiration syndrome. Results: With a total of 1377 patients, three SRs and two RCTs were included in analysis. Surfactant effectiveness was concluded by low-quality SRs, with high risk of bias, which was contradicted by high-quality SRs, with low risk of bias. In SRs, the surfactant lung lavage reduced mortality, need for extracorporeal membrane oxygenation and hospitalization, while the bolus surfactant did not. In recent high-quality RCTs, however, the two modalities did not significantly differ. Conclusion: The evidence on surfactant effectiveness and its method of administration is sparse and inconsistent.
Background
Meconium aspiration syndrome (MAS) is defined as respiratory distress in a neonate born through a meconium-stained amniotic fluid, having characteristic radiological changes whose symptoms cannot be otherwise explained [1]. Although MAS is as yet a noteworthy cause of mortality and morbidity in developing countries [2], in a study conducted in an urban Pakistanis, 27.3% of neonatal mortality was estimated to have a history or evidence of meconium passage during delivery [3]. A study conducted in China found that among all neonates, MAS becomes a source for 10% of cases of respiratory failure and is associated with up to 39% of morbidity and high mortality [4]. The pathophysiology of this condition is characterized by acute airway obstruction, surfactant dysfunction or inactivation, chemical pneumonitis by aspirated meconium and pulmonary hypertension induced right-to-left extra-pulmonary shunting [5]. Treatment of MAS in neonates involves supportive care-oxygen therapy, assisted ventilation, inhaled nitric oxide and, if available, extracorporeal membrane oxygenation (ECMO) [6,7]. A Cochrane review assessed bolus surfactant (BS) therapy in MAS, which indicated that the surfactant therapy decreases progressive respiratory failure requiring ECMO [8]. A study with three case reports found that lung lavage with diluted surfactant appeared to improve the outcomes among infants with MAS [9]. Our literature suggested that there are several systematic reviews (SRs) published in the past decade, citing more than ten randomized controlled trials (RCTs) and observational studies. When evidence is depressed among multiple SRs on relevant aspects of a topic of interest, systematic overviews of SRs are offer a solution to the information overload in literature, enabling enhanced access to targeted information of interest. Within the context of guiding the decision making on the use of surfactants for MAS, there is a need to systematically bring together, assess and summarize overall evidence available so far, especially as there is no available robust and comprehensive evidence to support the effective surfactant modality. Here, in this review, we aimed to summarize all the existing SRs and the RCTs that were not part of SRs, and to assess their quality.
Methodology
This is a systematic overview that follows the preferred reporting items for systematic reviews and meta-analyses (PRISMA) checklist recommendations for reporting (Supplementary Material 1).
Identification & selection of SRs
We searched EMBASE, PROQUEST and PubMed databases with the variations of the key terms of ‘meconium’, ‘MAS’ and ‘surfactant’ since inception to January 2020 for identifications of literature on this topic. Search strategies can be seen in Supplementary Material 2. No restrictions were imposed on the search. In addition, to identify potentially missed relevant literature, we have searched Google Scholar and references of relevant reviews (grey literature).
Studies that were SRs or comparative clinical trials on neonates with MAS that were treated with surfactants and assessed for mortality and morbidity were considered for inclusion. Any included SR, identified as SR or meta-analysis, was one that systematically identified the evidence about using the surfactants; summarized the different outcomes from different sources and; synthesized summative evidence about each of the different outcomes. Included RCTs are the ones that were not included in any of the included SRs in the current study.
We have excluded studies such as expert opinions, previous SRs of current/updated ones, narrative reviews, conference abstracts and editorials.
Selection of studies
Two reviewers independently screened title/abstracts for inclusion and exclusion and then the eligible studies were subjected to the full-text screening based on the aforementioned definition of an SR. The same two reviewers conducted full-text screening and any discrepancies were resolved by consulting the senior author.
Data abstraction & scoring
Two authors independently extracted the data of interest from each included SR. The extracted data related to the study characteristics, literature search strategies, patient characteristics, intervention, comparator, outcome measures, duration of follow-up, effect estimates, surfactant type, formulation and the number of doses. In addition, we also extracted the relevant data from recently published RCTs that are not included in the most recent SR.
Quality & risk of bias assessment
Critical Appraisal Skills Programme checklist
Two reviewers independently did the scoring on each item of RCT critical appraisal skills programme tool [10] to evaluate the quality of each included RCT. Any disagreements were resolved by consensus. If consensus was unable to be reach regarding any item, a third reviewer was involved for adjudication.
This consists of 11 questions, out of which the first three questions are screening questions and can be answered quickly. If the answers were ‘yes’, it is worth proceeding with the remaining questions. There is some degree of overlap between the questions, researchers are asked to record a ‘yes’, ‘no’ or ‘cannot tell’ to most of the questions. A number of italicized prompts are given after each question [10].
Measurement tool to assess SRs
AMSTAR-2 (a measurement tool to assess systematic reviews-2) is a 16-item instrument used to determine the methodological quality of SRs. This tool requires assessors to answer “yes”, “no”, “partial yes”, or “not applicable”; and AMSTAR-2 has a good agreement, reliability, construct validity and feasibility to assess the quality of SRs. The overall methodological quality of each SR was rated as, high, moderate, low and critically low according to the guidance document. We used the online AMSTAR-2 checklist for the purpose of this study (https://amstar.ca/Amstar_Checklist.php) [11].
Risk of bias in SRs
Two reviewers independently performed the risk of bias assessment of included SRs using the risk of bias in systematic reviews (ROBIS) tool [12] for all included SRs. Any disagreements between the reviewers were resolved by discussion. Reviewers were asked to read the ROBIS guidance document and understand the assessment procedure prior to employing this tool. This tool was completed in three phases: assess relevance (which is optional); identify concerns with the review process; judge risk of bias in the review. Phase II involves assessment of risk of bias in four domains, through 21 signalling questions (SQs), from which bias is likely to be introduced: study eligibility criteria; identification and selection of studies; data collection and study appraisal; and synthesis and findings. In Phase III, the overall quality of each SR was rated as ‘high risk of bias’, ‘unclear risk of bias’, or ‘low risk of bias’ depending upon the rating given for each signalling question in Phase II.
Data analysis
Data were reported descriptively and graphically using Microsoft Excel 2016. Ethical approval for this work was not required because the sample included published SRs, not humans or animals. Since there were less than ten SRs included in this study, we did not assess the association between publication year, impact factor and quality of the SR.
Results
Our literature search yielded 1797 studies from all databases. After the removal of duplicates (n = 591), we screened the titles and abstracts and removed the irrelevant articles (Figure 1). The relevant articles were subjected to full-text screening and finally, we identified three SRs [8,13,14] and two RCTs [15,16].

Figure 1. Flow of study selection.
RCT: Randomized clinical trials.
The main characteristics of the included SRs are presented in Table 1 and the recent RCTs are presented in Table 2. All three SRs included randomized trials that used accepted methods of randomization. However, the SR conducted by Choi et al. also included eight nonrandomized studies (NRSs) [13]. Studies in one SR [13] used surfactant lung lavage (SLL) and were not blinded, whereas three of the studies that were included in the Cochrane SR [8], which used BS, were blinded, except one RCT [17]. Three of the RCTs in the third SR [14], by Natarajan et al. were on antibiotic use in MAS [18–20]. The remaining studies in this SR, which studied the surfactant use, used both SLL and BS.
| Study | Year | Number of studies | Study designs | Type of participants | Condition | Interventions | Route of administration | Comparators | Outcomes | Duration of follow-up | AMSTAR-2 | Ref. | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| El Shahed et al. | 2014 | 4 | RCTs | Late preterm and term infants | MAS | Surfactant therapy (Intratracheal administration) four doses of 100–150 mg (6 ml)/kg beractant (Survanta) and porcine lung-derived surfactant (Curosurf) at 200 mg/kg, with repeated doses of 200, 100 and 100 mg/kg | Bolus | Air placebo, control group and standard care | Mortality (RR: 0.98; 95% CI: 0.41–2.39), treatment with ECMO (RR: 0.64; 95% CI: 0.46–0.91), pneumothorax, hospital stay (MD: 8 days; 95% CI: 14–3 days) | 4–28 days | Surfactants instillation may reduce the severity of respiratory illness and decrease the number of infants with progressive respiratory failure requiring support with ECMO | High quality | [8] |
| Choi et al. | 2012 | 10 | RCTs and non-RCTs | Infants | MAS | Lung lavage with diluted surfactant (Lucinactant 2.5–10 mg/ml, Beractant 5/10/5.3 mg/ml) | Intratracheal | Nonsurfactant control | Mortality (RR: 0.44; 95% CI: 0.13–1.50), need for ECMO (RR: 0.27; 95% CI: 0.04–2.08), pneumothorax (RR: 0.39; 95% CI: 0.08–1.95) | 1–28 days | Lung lavage with diluted surfactant found to improve the clinical outcomes | Low quality | [13] |
| Natarajan et al. | 2016 | 11 | RCTs | Term neonates | MAS | Lung lavage with surfactant (Survanta, 15 ml/kg aliquots and 150 mg/kg), Surfaxin (2.5 & 10 mg/ml), Bovine surfactant (70 mg/kg), Porcine surfactant (120/mg/kg), Curosurf (100–200 mg/kg) | Intratracheal and bolus | No lavage, supportive care, air placebo | In-hospital mortality (SLL; RR: 0.38; 95% CI: 0.09–1.57 vs BS: 0.80; 95% CI: 0.39–1.66); duration of hospital stay (MD: 4.68; 95% CI: 7.11– 2.24); duration of oxygen therapy (SLL; MD: 0.03; 95% CI: 1.36–1.42 vs BS; MD: 4.06; 95% CI: 10.8–2.7) | 1–7 days | Surfactant instillation in both routes was found to reduce the duration of mechanical ventilation and hospital stay. In addition, BS reduces the need for ECMO | Critically low | [14] |
AMSTAR 2: A measurement tool to assess systematic reviews; BS: Bolus surfactant; ECMO: Extracorporeal membrane oxygenation; MAS: Meconium aspiration syndrome; MD: Mean difference; RCT: Randomized controlled trial; RR: Risk ratio; SLL: Surfactant lung lavage.
| Study | Year | Design | Participants | Condition | Intervention | Comparator | outcomes | Duration | Conclusion | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|
| Bandiya et al. | 2019 | RCT | Infants | Patients with MAS who had moderate to severe respiratory distress (Downes score >4) | SLL (bovine surfactant [Survantant] diluted in normal saline to a phospholipid concentration of 5 mg/ml) | No lung lavage | Duration of respiratory support and tolerability | 1–2 days | Lung lavage is well tolerated but there was no change in overall duration of respiratory support | [16] |
| Arayici et al. | 2019 | RCT | Newborns | MAS | 30 ml/kg of diluted porcine surfactant | Porcine surfactant (100 mg/kg) as bolus | Duration of respiratory support (mechanical ventilation and nasal continuous positive airway pressure Mortality | 3–3.5 days | No significant difference found between both therapies for duration of respiratory support. However, incidence of pneumothorax and surfactant re-administration decreased nonsignificantly in lavage group | [15] |
MAS: Meconium aspiration syndrome; RCT: Randomized controlled trial; SLL: Surfactant lung lavage.
The identified SRs included 13 unique RCTs (1106 patients) and the eight NRSs [21–28] (178 patients). All these studies reported hospital admission outcomes.
Out of the ten RCTs on surfactant for MAS, four used SLL and the remaining studies tested BS [15,16,29–36]. Among the four RCTs that tested SLL, one tested a synthetic surfactant (Surfaxin), while the other studied bovine surfactant for lavage. In contrast, all BS studies evaluated only natural or animal surfactants that were made from either bovine or porcine.
Summary of outcomes of included SRs
An SR conducted in 2012 by Choi et al. [13] had included both RCTs and NRSs studies that assessed the effects of surfactant lavage therapy for MAS. This review included studies that were clinically heterogeneous in terms of the severity of the disease, method of surfactant lavage, initial intervention time and combined treatment modalities. Meta-analysis of two RCTs indicated that the surfactant lavage significantly decreased death or the need for ECMO (risk ratio [RR]: 0.34; 95% CI: 0.11–0.99) with no heterogeneity, however, no statistical significant difference was found for the pneumothorax outcome (RR: 0.39; 95% CI: 0.08–1.95).
This review also included eight NRSs and the meta-analysis of studies with available data indicated that the surfactant lavage had a significant effect on air leaks (RR: 0.52; 95% CI: 0.28–0.96; six studies), pneumothorax (RR: 0.45; 95% CI: 0.23–0.89; five studies) and death or the need for ECMO (RR: 0.35; 95% CI: 0.13–0.94; six studies). These results are inconsistent with those from RCTs. However, the allocation methods in these studies with concurrent control may be prone to selection bias.
A Cochrane review [8] was conducted to determine the efficacy of surfactant administration in the treatment of late preterm and term infants with MAS in RCTs. The meta-analysis of four trials (326 infants) showed no statistically significant effect on mortality (RR: 0.98; 95% CI: 0.41–2.39; typical risk difference: 0.00; 95% CI: 0.05–0.05) with no heterogeneity. There were no statistically significant reductions in the secondary outcomes of duration of assisted ventilation, supplemental oxygen, pneumothorax, air leaks, chronic lung disease and the need for oxygen at discharge, but not for the hospital stay (median duration: 8 days; 95% CI: 14–3) and need for ECMO (RR: 0.64; 95% CI: 0.46–0.91; typical risk difference: 0.17; 95% CI: 0.30–0.04; two RCTs).
A recent SR conducted by Natarajan et al. [14] studied surfactant therapy and antibiotics in neonates with MAS. Out of the 11 RCTs, eight studies assessed the effects of the use of surfactant and the other three were on the use of antibiotics. Both SLL and BS methods did not reduce the risk of mortality (RR: 0.38; 95% CI: 0.09–1.57; two studies; and RR: 0.80; 95% CI: 0.39–1.66; five studies, respectively), however, both methods reduced the duration of hospital stay (mean difference: 2.0; 95% CI: 3.66– −0.34; one study; and RR: 4.68; 95% CI: 7.11–2.24 days; four studies) and duration of mechanical ventilation (mean difference: 1.31; 95% CI: 1.91–0.72; two studies; and mean difference: 5.4; 95% CI: 9.76–1.03 days; five studies). There was no significant reduction with the use of antibiotics for MAS in the risk of mortality (RR: 1.72; 95% CI: 0.22–13.31; three studies), sepsis (RR: 1.31; 95% CI: 0.34–5.07; three studies) and duration of hospital stay and duration of oxygen therapy.
Among the studies included in these SRs, only the Chinese Study Group 2005 [17] and Lotze et al. (1998) [32] studied incidence of complications, which indicated no significant difference between the studied groups. The complications monitored were technical, neurologic, pulmonary, hemorrhagic, cardiac complications and proven sepsis.
Review of recent RCTs
An RCT [15] conducted in Turkey included newborns with MAS (diagnosed according to the criteria of: evidence of meconium passage at or before delivery, presence of respiratory distress after <2 h birth, chest radiography typically suggesting aspiration of meconium). Patients in lavage group (n = 17) received 30 ml/kg of diluted porcine surfactant and bolus group (n = 16) received porcine surfactant (100 mg/kg) in repetitive dose endotracheally. Lung lavage did not show any advantage over bolus therapy on duration of respiratory support, high-frequency ventilation or inhaled nitric oxide requirement. A total of three deaths occurred (two in lavage and one in bolus group). The quality score of this RCT based on the critical appraisal skills programme checklist was 9/11.
Another RCT [16] conducted in India included term infants with MAS who had moderate to severe respiratory distress (Downes score >4) and were randomized to bovine surfactant (Survanta), diluted using normal saline to a phospholipid concentration of 20 ml/kg (n = 31), or to no lung lavage (NLL) (n = 29). The median duration of respiratory support was 34 h in SLL group and 44 h in NLL group. The duration of oxygen therapy post-respiratory support decreased by 78% in SLL as compared with NLL group. There was no significant difference between both groups for duration of hospital stay and oxygen therapy, death, ECMO, incidence of clinical sepsis, pneumothorax, persistent pulmonary hypertension, discharge and death. The quality score of this RCT based on critical appraisal skills programme checklist was 9/11.
Methodological quality of SRs
The three SRs were found to be of high, low and critically low quality (Table 1). Out of the seven critical items, only item ten was satisfied by all three SRs and protocol registration before the commencement of SR and the reporting of list of excluded studies with justification were not satisfied by two SRs. The majority of the SRs satisfied the remaining noncritical domains, which were; items 1, 3, 6, 8 and 16 (n = 3), items 5, 12 and 15 (n = 2), and none of the SR satisfied the item 10 (funding for the included studies).
Risk of bias in SRs
SRs were found to be of high [14], unclear [13] and low [8] risk of bias on the assessment of ROBIS. The sequence of domains that contributed to high risk of bias in the Natarajan et al. SRs were: domain 3 and domain 4. For unclear risk of bias in the Choi et al. SRs, the contributing domain was number 2. The major SQs that were contributing to the rating of high risk of bias were in domain 3 (3.4, 3.5) and domain 4 (4.5 & 4.6). The major SQs that were contributing to rating the unclear risk of bias were in domain 2 (2.3, 2.5; Figure 2).
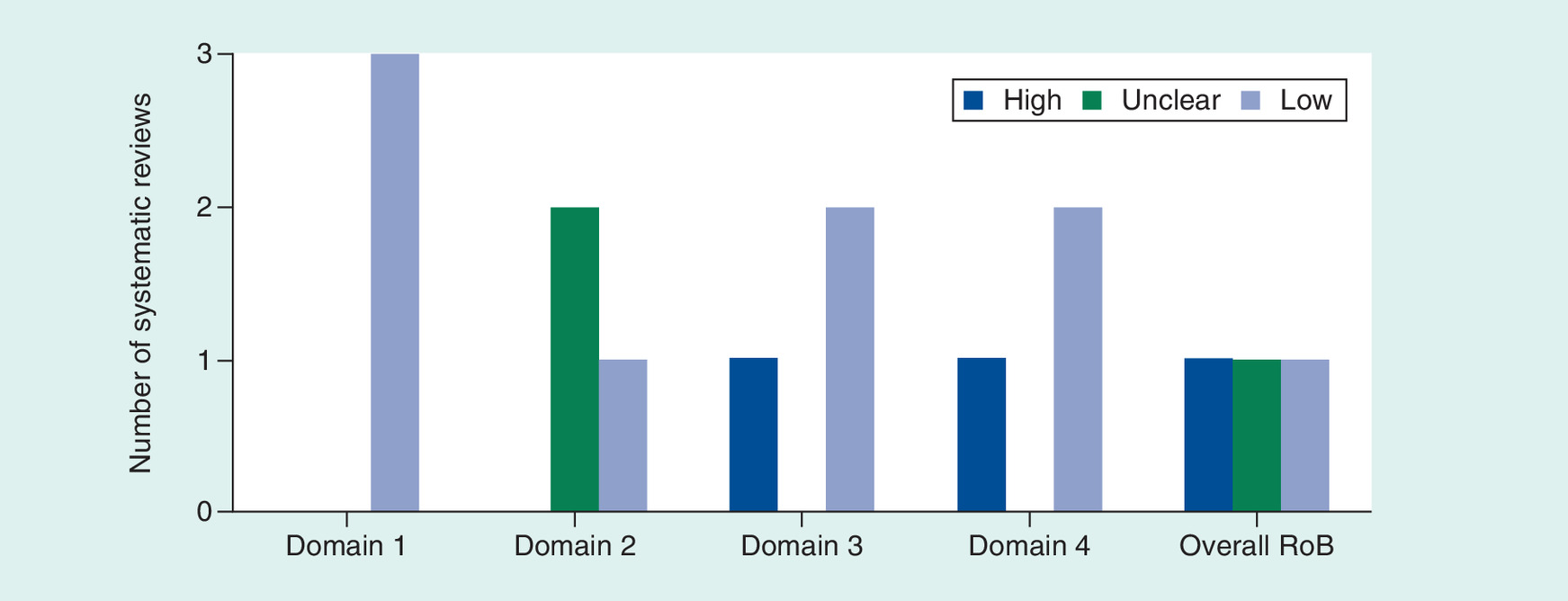
Figure 2. Extent of risk of bias in included systematic reviews.
RoB: Risk of bias.
Discussion
In this overview of SRs, we examined three SRs and two RCTs that were published recently and not included in any SR. All these included SLL and BS methods using natural and synthetic products for MAS treatment.
To add to the comprehensive reporting of the top sources of evidence in literature that assessed surfactant therapy (bolus and lavage) in MAS, we went beyond the published SRs and included recently published RCTs that are not included in any SRs. Each meta-analysis outcomes in SRs were summarized separately, including in a structured table, which can help readers realize or review interesting outcomes easily.
There is a clear inconsistency in the reported outcomes of SRs, which disable a straightforward interpretation about the usefulness of surfactants for MAS. A meta-analysis of RCTs of SLL in the low-quality SR, by Choi et al. [13], concluded surfactant effectiveness against death and ECMO use, but not against the pneumothorax as a result of MAS. In the same SR, a meta-analysis of NRSs concluded effectiveness against all the aforementioned, including the pneumothorax and air leaks outcome. This, however, was all contradicted by a high-quality Cochrane meta-analysis [14] on the use of BS. This Cochrane review suggested decreased progressive respiratory failure requiring ECMO. It, however, concluded no effect against death, pneumothorax, air leaks, and MV duration. With the critically low-quality meta-analysis that looked at both SLL and BS together [8], an effectiveness was not concluded against death, but only against the need for ECMO and the hospital stay.
To add to the inconclusively of surfactant effectiveness, based on the results of Choi et al. and El Shahed et al. meta-analyses, one might conclude that SLL are more effective than the BS. This, however, is negated by the two high-quality and most recent RCTs that conclude no difference between SLL and BS in effectiveness [15,16].
An important safety concern is that the instillation of large volume of fluid into a newborn’s lung might be a burden, especially in cases of severe MAS, which leads to mortality [37]. The El Shahed et al. Cochrane review assessed the efficacy of BS and indicated no improvement on morbidity or mortality [8]. Nevertheless, while two RCTs [38,39] assessed a surfactant made of porcine administered in small lavage quantity to eight infants and showed improvements in oxygenation, those effects were improved with large volume of diluted porcine surfactant in a recently published RCT [15].
In vivo studies indicated that there was more release of proinflammatory cytokines that occurred in male fetuses when stimulated with lipopolysaccharide stimulation compared with female fetuses [40,41]. A recent study (n = 95), conducted in Japan, found that male neonates were at a higher risk of developing MAS than female neonates. However, further studies are needed to confirm the role of sex on MAS development [42].
The quality assessment of SRs indicated that none of the SR reported funding source and the two other non-Cochrane reviews did not have prior protocol and did not provide excluded studies list. Hence, based on AMSTAR-2 assessment, the quality of included SRs were rated as high [8], low [13] and critically low quality [14]. In addition to that, we have found a similar pattern in risk of bias assessment results based on the ROBIS tool. Among three reviews, only the Cochrane review was found to be of low risk of bias.
The overview has some limitations. The restriction to English language might have excluded some studies published in other languages. The authors in the current study however do not have the resources to translate the non-English research literature that may generate from a non-restricted search. Furthermore, searching additional index terms to those in the study or additional combinations of them is always possible and may generate additional studies. In addition, the fact that a primary article could have been included in more than an SR may contribute to double counting of data within reported meta-analyses. Not exploration of such overlaps tool place in this study.
Conclusion
Overall, our overview of SRs and recent RCTs considered all the available literature to summarize and critically appraise the evidence using the available tools. However, while limited evidence of effectiveness against death, ECMO, pneumothorax, air leaks and MV duration was reported in literature, this was provided via critically low quality, with high risk of bias, reviews. Higher quality SRs, with low risk of bias, concluded a lack of surfactant effectiveness. A similar lack of clarity trend is observed when one tries to draw overall conclusion about how different surfactant modalities compare. Larger trials are needed to determine the effectiveness of BS administration and/or SLL to treat MAS effectively and safely.
•
There are three systematic reviews (SRs) in the literature that analyzed the effectiveness of surfactant in meconium aspiration syndrome (MAS).
•
One SR focused on surfactant lung lavage (SLL) and concluded that surfactant therapy is effective against MAS. This was of critically low quality methods and had high risk for bias. This concluded that the surfactant reduces death, extracorporeal membrane oxygenation, pneumothorax, air leaks, and MV duration.
•
One SR focused on SLL and bolus surfactant (BS) and concluded that surfactant therapy is effective against MAS in reducing hospital stay and need for mechanical ventilation, but not mortality. This was of low quality methods and had unclear risk for bias.
•
One SR was a Cochrane SR that focused on BS and concluded that the surfactant therapy does not have any significant effect against primary outcomes in MAS. This was of high quality methods and had low risk for bias.
•
There are two recent randomized clinical trials in the literature that were not included in SRs of the effectiveness of surfactant in MAS.
•
Based on SRs, SLL performed better than BS in overall. Based on recent randomized clinical trials, SLL and BS are equivalent in effectiveness.
•
Among studies in the SRs, only two studies focused on the complications of surfactants. No significant differences among groups were reported.
•
Overall, there is limited and inconsistent evidence of the effectiveness of surfactant in MAS. There is a need for large clinical studies that are of high quality to improve on the available evidence about surfactant effectiveness.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Author contributions
D Al-Badriyeh conceived and designed the study. All authors contributed equally in data collection and analysis, result interpretation and revising the manuscript. M A Abdelaal wrote the first manuscript draft. All authors read and approved the final manuscript.
Financial & competing interests disclosure
This research was funded by a Qatar University grant number: QUST-1-CPH-2019-15. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
References
Papers of special note have been highlighted as: • of interest
1.
Wiswell TE, Tuggle JM, Turner BS. Meconium aspiration syndrome: have we made a difference? Pediatrics 85, 715–721 (1990).
2.
Velaphi S, Van Kwawegen A. Meconium aspiration syndrome requiring assisted ventilation: perspective in a setting with limited resources. J. Perinatol. 28(3), 36–42 (2008).
3.
Jehan I, Harris H, Salat S et al. Neonatal mortality, risk factors and causes: a prospective population-based cohort study in urban Pakistan. Bull World Health Organ. 87, 130–138 (2009).
4.
Qian L, Liu C, Zhuang W et al. Neonatal respiratory failure: a 12-month clinical epidemiologic study from 2004 to 2005 in China. Pediatrics 121, e1115–e1124 (2008).
5.
Swarnam K, Soraisham AS, Sivanandan S. Advances in the management of meconium aspiration syndrome. Int. J. Pediatr. 359571 (2012).
6.
Cleary GM, Wiswell TE. Meconium-stained amniotic fluid and the meconium aspiration syndrome: an update. Pediatric Clin. North Am. 45(3), 511–529 (1998).
7.
Wiswell T. Advances in the treatment of the meconium aspiration syndrome. Acta Paediatr. 90, 28–30 (2001).
8.
El Shahed AI, Dargaville PA, Ohlsson A, Soll R. Surfactant for meconium aspiration syndrome in term and late preterm infants. Cochrane Database Syst. Rev. 12, Cd002054 (2014).
• A high quality, with low risk of bias, systematic review (SR) for summarizing the evidence about the bolus surfactant (BS) therapy in meconium aspiration syndrome (MAS). This included four randomized controlled trials.
9.
Lo CW, Jeng MJ, Chang FY et al. Therapeutic lung lavage with diluted surfactant in neonates with severe meconium aspiration syndrome. J. Chin. Med. Assoc. 71, 103–109 (2008).
10.
Critical Appraisal Skills Programme (CASP). Randomised controlled trials checklist (2018). https://casp-uk.net/casp-tools-checklists/
11.
Shea BJ, Reeves BC, Wells G et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 358, j4008 (2017).
12.
Whiting P, Savovic J, Higgins JP et al. ROBIS: a new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 69, 225–234 (2016).
13.
Choi HJ, Hahn S, Lee J et al. Surfactant lavage therapy for meconium aspiration syndrome: a systematic review and meta-analysis. Neonatology 101, 183–191 (2012).
• A critically low quality, with high risk of bias, SR for summarizing the evidence about the surfactant lung lavage (SLL) therapy in MAS. This included 11 randomized controlled trials and nonrandomized clinical studies.
14.
Natarajan CK, Sankar MJ, Jain K, Agarwal R, Paul VK. Surfactant therapy and antibiotics in neonates with meconium aspiration syndrome: a systematic review and meta-analysis. J. Perinatol. 36, S48–S53 (2016).
• A low quality, with unclear risk of bias, SR for summarizing the evidence about SLL and BS therapies in MAS. This included ten randomized controlled trials.
15.
Arayici S, Sari FN, Kadioglu Simsek G et al. Lung lavage with dilute surfactant vs. bolus surfactant for meconium aspiration syndrome. J. Trop. Pediatr. 65, 491–497 (2019).
• A Turkey-based randomized clinical trial that was not included into any SR, and it has a high quality of methods. This concluded that SLL did not show any advantage over bolus therapy.
16.
Bandiya P, Nangia S, Saili A. Surfactant lung lavage vs. standard care in the treatment of meconium aspiration syndrome – a randomized trial. J. Trop. Pediatr. 65, 114–121 (2019).
• An India-based randomized clinical trial that was not included into any SR, and it has a high quality of methods. This concluded that SLL did not show any advantages over BS.
17.
Sun B. Treatment of severe meconium aspiration syndrome with porcine surfactant: a multicentre, randomized, controlled trial. Acta Paediatr. 94, 896–902 (2005).
18.
Basu S, Kumar A, Bhatia B. Role of antibiotics in meconium aspiration syndrome. Ann. Trop. Paediatr. 27, 107–113 (2007).
19.
Shankar V, Paul VK, Deorari AK, Singh M. Do neonates with meconium aspiration syndrome require antibiotics? Indian J. Pediatr. 62, 327–331 (1995).
20.
Lin H-C, Su B-H, Tsai C-H, Lin T-W, Yeh T-F. Role of antibiotics in management of non-ventilated cases of meconium aspiration syndrome without risk factors for infection. Neonatology 87, 51–55 (2005).
21.
Lam BCC, Yeung CY. Surfactant lavage for meconium aspiration syndrome: a pilot study. Pediatrics 103, 1014–1018 (1999).
22.
Chang HY, Hsu CH, Kao HA et al. Treatment of severe meconium aspiration syndrome with dilute surfactant lavage. J. Formos Med. Assoc. 102, 326–330 (2003).
23.
Salvia-Roiges MD, Carbonell-Estrany X, Figueras-Aloy J, Rodriguez-Miguelez JM. Efficacy of three treatment schedules in severe meconium aspiration syndrome. Acta Paediatr. 93, 60–65 (2004).
24.
Lee SM, Kim HM, Jeon JH et al. Effect of surfactant lavage in severe meconium aspiration syndrome. Korean J. Pediatr. 51, 367–371 (2008).
25.
Dargaville PA, Mills JF, Copnell B, Loughnan PM, McDougall PN, Morley CJ. Therapeutic lung lavage in meconium aspiration syndrome: a preliminary report. J. Paediatr. Child Health 43, 539–545 (2007).
26.
Schlössser R, Veldman A, Fischer D, Allendorf A, Von Loewenich V. Lavage mit exogenem surfactant bei neonataler Mekoniumaspiration. Zeitschrift für Geburtshilfe und Neonatologie. 206, 15–18 (2002).
27.
Kowalska K, Szymankiewicz M, Gadzinowski J. An effectiveness of surfactant lung lavage (SLL) in meconium aspiration syndrome (MAS). Przeglad lek. 59, 21–24 (2002).
28.
Kawano T. Effect of surfactant lavage to the babies with meconium aspiration syndrome. Acta Neonatol. Jpn. 35, 32–40 (1999).
29.
Wiswell TE, Knight GR, Finer NN et al. A multicenter, randomized, controlled trial comparing surfaxin (lucinactant) lavage with standard care for treatment of meconium aspiration syndrome. Pediatrics 109, 1081–1087 (2002).
30.
Dargaville PA, Copnell B, Mills JF et al. Randomized controlled trial of lung lavage with dilute surfactant for meconium aspiration syndrome. J. Pediatr. 158, 383–389 e2 (2011).
31.
Findlay RD, Taeusch HW, Walther FJ. Surfactant replacement therapy for meconium aspiration syndrome. Pediatrics 97, 48–52 (1996).
32.
Lotze A, Mitchell BR, Bulas DI, Zola EM, Shalwitz RA, Gunkel JH. Multicenter study of surfactant (beractant) use in the treatment of term infants with severe respiratory failure. Survanta in Term Infants Study Group. J. Pediatr. 132, 40–47 (1998).
33.
Maturana A, Torres‐Pereyra J, Salinas R, Astudillo P, Moya FR The Chile Surf Group. A randomized trial of natural surfactant for moderate to severe meconium aspiration syndrome. Pediatr. Acad. Soc. 57, 1545 (2005).
34.
Chinese Collaborative Study Group for Neonatal Respiratory Diseases. Treatment of severe meconium aspiration syndrome with porcine surfactant: a multicentre, randomized, controlled trial. Acta Paediatr. 94, 896–902 (2005).
35.
Chang Z-x, Liu C-q, Ma H-Y. Neonatalogy Department of Hebei Province Children Hospital, Shijiazhuang 050031, China. The influence of exogenous pulmonary surfactant on pulmonary surfactant-associated proteins in infants with meconium aspiration syndrome. Chinese J. Neonatol. 5 (2009).
36.
Wanying H. Early application of pulmonary surfactant in the neonatal meconium aspiration syndrome. Guangdong Med. J. 30, 1151–1153 (2009).
37.
Kinsella JP. Meconium aspiration syndrome: is surfactant lavage the answer? Am. J. Respir. Crit. Care Med. 168, 413–414 (2003).
38.
Lista G, Bianchi S, Castoldi F, Fontana P, Cavigioli F. Bronchoalveolar lavage with diluted porcine surfactant in mechanically ventilated term infants with meconium aspiration syndrome. Clin. Drug Investig. 26, 13–19 (2006).
39.
Lejeune T, Pfister RE. Surfactant lavage for extracorporeal membrane oxygenation-requiring meconium aspiration syndrome – a cheap alternative. Eur. J. Pediatr. 164, 331–333 (2005).
40.
Kim-Fine S, Regnault TR, Lee JS et al. Male gender promotes an increased inflammatory response to lipopolysaccharide in umbilical vein blood. J. Matern. Fetal Neonatal. Med. 25, 2470–2474 (2012).
41.
Koch FR, Wagner CL, Jenkins DD et al. Sex differences in cerebral blood flow following chorioamnionitis in healthy term infants. J. Perinatol. 34, 197–202 (2014).
42.
Yokoi K, Iwata O, Kobayashi S, Muramatsu K, Goto H. Influence of foetal inflammation on the development of meconium aspiration syndrome in term neonates with meconium-stained amniotic fluid. PeerJ. 7, e7049 (2019).
Information & Authors
Information
Published In
Pages: 527 - 536
PubMed: 32394731
Copyright
© 2020 Future Medicine Ltd.
History
Received: 1 February 2020
Accepted: 2 March 2020
Published online: 12 May 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Surfactant therapy for meconium aspiration syndrome in neonates: a systematic overview of systematic reviews and recent clinical trials. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0018
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Özmert M.a. Özdemir, Surfactant treatment in newborns other than respiratory distress syndrome, Pamukkale Medical Journal, 10.31362/patd.1745105, Advanced Online Publication, (1-1), (2025).
- Vedeesh Sombattina, Sushma Nangia, Gunjana Kumar, Tapas Bandyopadhyay, Early (≤ 2 h) Bolus Surfactant Replacement Therapy Versus Standard Care in Term (≥ 37 Weeks) Neonates With Meconium Aspiration Syndrome: An Open‐Label Randomized Controlled Trial, Pediatric Pulmonology, 10.1002/ppul.71292, 60, 9, (2025).
- Arun Prasath, Etze Chotzoglou, Asmahan Ahmad, Efren Diaz, Patti Burchfield, L. Steven Brown, David B Nelson, Katherine Stumpf, Venkatakrishna Kakkilaya, Less invasive surfactant administration for meconium aspiration syndrome, BMJ Paediatrics Open, 10.1136/bmjpo-2025-003317, 9, 1, (e003317), (2025).
- Arifa Mustaqeem, Anita Yadav, Jogender Kumar, Pradeep Debata, Continuous positive airway pressure versus conventional oxygen therapy in meconium aspiration syndrome: a randomized controlled trial, Journal of Tropical Pediatrics, 10.1093/tropej/fmaf002, 71, 2, (2025).
- Hueng-Chuen Fan, Chuan-Mu Chen, Meconium aspiration syndrome: An overview of the literature, Tungs' Medical Journal, 10.4103/ETMJ.ETMJ-D-23-00025, 18, 1, (4-11), (2024).
- Ahmed Osman, Cecilie Halling, Mary Crume, Hayat Al Tabosh, Namrita Odackal, Molly K. Ball, Meconium aspiration syndrome: a comprehensive review, Journal of Perinatology, 10.1038/s41372-023-01708-2, 43, 10, (1211-1221), (2023).
- Hetal Pramod Budh, Somashekhar Nimbalkar, Surfactant Replacement Therapy: What’s the New Future?, Journal of Neonatology, 10.1177/09732179221136963, 36, 4, (331-347), (2022).
- Fernando Moya, Manuel Sánchez Luna, Surfactant Replacement Therapy, Manual of Neonatal Respiratory Care, 10.1007/978-3-030-93997-7_58, (557-569), (2022).
- Samaher Al-Shaibi, Dina Abushanab, Eilan Alhersh, Rasha Kaddoura, Abdul Rouf Pallivalappila, Daoud Al-Badriyeh, Use of ibuprofen for the closure of patent ductus arteriosus in preterm infants: a systematic review of meta-analyses, Journal of Comparative Effectiveness Research, 10.2217/cer-2020-0235, 10, 7, (549-568), (2021).