Real-world direct healthcare costs of treating recurrent high-grade serous ovarian cancer with cytotoxic chemotherapy
This article has been corrected.
VIEW CORRECTIONPublication: Journal of Comparative Effectiveness Research
Abstract
Aim: To describe the direct healthcare costs associated with repeated cytotoxic chemotherapy treatments for recurrent high-grade serous cancer (HGSC) of the ovaries. Patients & methods: Retrospective review of 66 women with recurrent stage III/IV HGSC ovarian cancer treated with repeated lines of cytotoxic chemotherapy in a Canadian University Tertiary Center. Results: Mean cost of treatment of first relapse was CAD$52,227 increasing by 38% for two, and 86% for three or more relapses with median overall survival of 36.0, 50.7 and 42.8 months, respectively. In-hospital care accounted for 71% and chemotherapy drugs accounted for 17% of the total costs. Conclusion: After the third relapse of HGSC, cytotoxic chemotherapy did not prolong survival but was associated with substantially increased healthcare costs.
Ovarian cancer ranks within the top five as a cause of cancer-related mortality and healthcare expenditure in women [1,2]. 80% of deaths from ovarian cancer are due to its most common subtype, high-grade serous cancer (HGSC), which is characteristically diagnosed at stage III/IV, and despite treatment will recur in 80% of patients [3–5]. Once it recurs, unless amenable to complete resection, it is incurable and hence the goal of treatment is to alleviate symptoms and prolong good-quality life with chemotherapy [3,6]. However, emerging resistance makes the remissions achieved with cytotoxic chemotherapy only temporary, with shorter treatment-free intervals and cumulative toxicity with successive lines of treatment [7].
Advances in precision medicine now make available, targeted therapies that significantly delay recurrence with lower toxicity compared with cytotoxic chemotherapy [5,6]. For example, oral poly-ADP ribose polymerase inhibitors have produced clinically meaningful prolongation of good-quality life for women with germline or somatic breast cancer gene mutations and platinum-sensitive HGSC recurrence [8–11]. Despite benefits to patients, the high acquisition cost of these therapies limits their accessibility.
Unfortunately, the health economic assessment of newer treatments is hampered by the lack of comprehensive data on healthcare costs related to the treatment of disease recurrences with the current standard of care, specifically, multiple lines of chemotherapy [12,13]. This is because health economic assessments focus on drug acquisition costs, which represent only a fraction of the total financial burden of cancer care. Other costs, such as those related to emergency room visits, tests, interventions as well as hospital stays, are often not included or are underestimated in these assessments. This happens because fragmentation of healthcare provision, combined with lack of precision and granularity in administrative databases that group together various ovarian cancer subtypes and stages of disease, preclude obtaining accurate and specific healthcare utilization and cost estimates. As a result, the costs of treating cancer are underestimated. In addition, most cost–effectiveness evaluations of cancer treatments are based on Phase II/III randomized controlled trials [14], which have limited generalizability to the target population because neither treatment protocols, nor the participating patients are representative of the real-world setting [15]. For example, poor performance status and comorbidities, despite being common in patients with recurrent cancer, are exclusion criteria in Phase II/III randomized controlled trials [15]. It follows that accurate cost assessments derived from the real-world setting are essential for the assessment of new treatments and their comparison to conventional cytotoxic therapies.
The results of a study published by Doyle et al. almost 20 years ago, showed that increased lines of chemotherapy were associated with increased costs but not better outcome or survival. In this study, inpatient care, chemotherapy agents and outpatient care accounted for 62, 21 and 8% of the total healthcare costs. Of the total costs, 43% was attributable to chemotherapy and 43% to supportive care. However, since the publication of this study, cancer treatments have changed and most chemotherapy is now delivered in the outpatient setting [16]. Gordon et al. reported that in women with primary epithelial ovarian cancer, treatment costs increased with later stage at diagnosis and more than one lines of chemotherapy [17]. Similar results were reported by Delgado-Ortega et al. using Markov models to simulate cohorts of women with epithelial ovarian cancer in Spain [18]. Using health economic models, Rocconi et al. showed that the incremental cost–effectiveness ratio was not favorable after the second line of chemotherapy in patients with platinum resistant epithelial ovarian cancer [19]. Therefore, there is a need for contemporary real-world cost assessment of conventional chemotherapy regimens to provide a benchmark in the health economic evaluation of new emerging treatments [12,13,15].
The current study describes the direct healthcare cost of treating recurrent HGSC with standard-of-care cytotoxic chemotherapy in a Canadian Tertiary University Center.
Material & methods
Study design
This is a retrospective chart review of patients treated by the Gynecology Oncology Service at the McGill University Health Center (MUHC), a tertiary care academic hospital in Montreal (QB, Canada). The study was approved by the Research Ethics Board of the MUHC. Using the database of the Service, the oncology pharmacy-database and the institutional tumor registry, we identified all patients with recurrent stage III/IV HGSC treated at the MUHC between 2010 and 2014. In order to be included in the study, patients must have had their first recurrence between 2010 and 2014 and were exclusively treated at the MUHC from recurrence until transfer to palliative care services or death. Patients treated with targeted therapies, such as PARP-inhibitors and Bevacizumab, were excluded because during the study period, these therapies were not publicly funded and were used only as part of clinical trials.
Setting
The Canadian universal public health insurance covers all in-hospital medical services and medications. In Quebec, all residents have mandatory public or private outpatient drug insurance. Gynecologic cancer care in Quebec is largely provided by teams accredited by the government’s cancer agency. The MUHC Gynecology Oncology team has level IV accreditation (the highest).
Details of standard of care are provided in Box 1. At first recurrence, patients for whom repeat surgery is not possible are treated with chemotherapy that is delivered in a dedicated ambulatory Oncology Day Center. More specifically, the medical team consists of surgeons that perform all surgeries and medical oncologists who are responsible for the selection and administration of chemotherapy. The type of chemotherapy used depends on the platinum sensitivity of the disease and response to previous treatments and the treating physician’s judgment. Patient care is provided by a multidisciplinary team that is comprised of gynecologic oncologists, palliative care specialists, nurses, pharmacists and other healthcare professionals as needed. All treatments including administration of chemotherapy, transfusions, drainage of ascites or pleural effusions and management of adverse events are provided by the Gynecology Oncology Service. The Gynecologic Oncology Service consults and works with the Supportive and Palliative Care Service (SPCS) early in the trajectory of recurrent disease. When the projected life expectancy of a patient is thought to be less than 3 months and the patient is no longer on chemotherapy, she is eligible for increased home services under the jurisdiction of the SPCS, or for transfer to the SPCS inpatient facility at the MUHC or to a hospice in the community. All cost for patient management including chemotherapy is paid by the Provincial Health Insurance. The majority of Quebec residents have mandatory drug insurance that covers most of the prescription drug costs. Thus, all patients have equitable access to approved and funded interventions/drugs regardless of their financial status and ability to pay. The current study includes only the costs incurred while patients were under active chemotherapy treatment by the Gynecology Oncology Service.
•
Decisions about each patient’s management at recurrence are made at the interdisciplinary tumor-board. Patients with potentially resectable disease, in other words, oligo-metastases, are generally treated by repeat surgery. If the recurrent disease is deemed inoperable, patients are offered chemotherapy. As the goal of treatment is to prolong good-quality life, we delay starting chemotherapy in asymptomatic patients; however, we initiate it before tumor burden is high.
•
Patients with platinum-sensitive recurrence are retreated with combination chemotherapy of platinum with taxol or pegylated liposomal doxorubicin; platinum monotherapy is used in patients with poor performance status. Platinum-resistant recurrence is treated with pegylated liposomal doxorubicin. If the disease fails to respond, gemcitabine, weekly taxol, topotecan, alkylating agents, hormones are used as per the treating physician’s judgement. As the single-payer of the second most populous province in Canada, the Quebec Government negotiates drug prices and, when available, generic versions of drugs are used.
•
The interdisciplinary gynecologic oncology team includes a dedicated pivot nurse, a clinical nurse specialist and a liaison nurse, who help patients maximize the use of outpatient services and services in the community and reduce the need for inpatient care.
•
The gynecologic oncology service works closely with the Supportive and Palliative Care Service, which includes four subspecialized services: Cancer Pain Clinic, Cancer Nutrition and Rehabilitation, Psycho-social Oncology and the Supportive Care Clinic. Symptomatic patients are referred to this service to help manage physical and emotional symptoms alongside active chemotherapy treatment.
•
Intervention to prolong life or alleviate symptoms (gastrointestinal stents, double j-catheters/nephrostomy, drains for pleural effusion and ascites, intensity-modulated radiotherapy, radio ablation or surgical removal of isolated metastasis, nerve blocks) are used liberally.
•
In Quebec, physicians are not salaried and bill the provincial government using a complex system of basic and supplemental fees. Fees vary depending on whether the physician is on the subspecialist register, time of consultation (e.g., night, holidays), duration of consultation, whether academic teaching is involved, language barriers, reduced mobility, among others.
Ascertainment of direct healthcare costs
We ascertained healthcare resource utilization from hospital medical records, in-hospital medication use from the hospital pharmacy database and outpatient prescriptions from the medical records. Costs for services were calculated using the unit costs provided by the Regie de l'assurance maladie du Quebec, the Quebec government’s health insurance agency, and the MUHC Finance Department.
Direct healthcare costs were ascertained for the following:
•
All prescription drugs, including chemotherapy;
•
Imaging;
•
Blood tests;
•
Surgery, radiotherapy and other interventions intended to palliate or cure recurrent disease;
•
Ambulatory care;
•
Emergency room visits;
•
Cost for inpatient hospital stays including medical interventions, nursing, support services, nutritional support, physiotherapy, palliative and occupational therapy. These are predominantly, but not exclusively, related to the costs of managing adverse events;
•
Outpatient costs which include the cost for administration of chemotherapy.
The following costs could not be ascertained and are not included in the analysis:
•
Physician fees;
•
Services provided by the Local Community Services Centers;
•
Cost incurred during admission to rehabilitation centers;
•
Home care services;
•
Palliative care services;
•
Primary care services.
Statistical analyses
Patients were classified into treatment groups according to the number of chemotherapy regimens (lines) received as none, one, two and three or more. Descriptive statistics were reported for the entire patient cohort and for groups according to the number of chemotherapy treatments received. Overall survival (OS) and progression-free survival (PFS) were estimated with the Kaplan–Meier Estimator. Healthcare costs were ascertained from the time of recurrence until transfer to the palliative care service or death. Costs are reported in 2016 Canadian dollars. Analyses were conducted on observed data. There were no imputations for missing data. Descriptive statistics for costs included the mean, median and interquartile range. Bivariate comparisons were conducted with the χ2 statistics for categorical variables, analysis of variance for continuous variables and the Jonckheere–Terpstra test for ordered alternatives for costs. Multivariate analysis of variance was used to determine the proportion of variance in the total costs attributed to each cost component and to adjust the between-group differences with respect total costs for patient demographics and profile. Generalized linear models with a gamma distribution and log as the link function was used to adjust the total healthcare costs for potential confounders. Multivariate linear regression was used to develop a predictive model for total direct healthcare costs. All analyses were conducted with Statistical Package for the Social Sciences (SPSS) version 24.
Results
Of the 120 patients with recurrent stage III/IV HGSC treated at the MUHC during the study period, 66 met the study inclusion criteria. There were no clinically important differences between the patients included in the analysis and those who were excluded (Table 1), demonstrating that the study cohort was representative of women with recurrent stage III/IV HGSC treated at the MUHC. Mean age (standard deviation [SD]) was 60.6 (8.6) years, and 48% of the women were Caucasian. At diagnosis, 68% had stage IIIC, and 25% had stage IV disease. The median (95% CI) PFS and OS of the 66 HGSC patients included in the analysis were 16.4 (12.9–21.4) and 40.3 (33.2–50.7) months, respectively. No patient in this series was admitted to the intensive care or high-dependency unit during follow-up. All had at least one consultation with the SPCS.
| Variable | Total cohort | Excluded from cohort | Excluded from analysis | Included in analysis | ||||
|---|---|---|---|---|---|---|---|---|
| N | 120 | Percentage | 54 | Percentage | 7 | Percentage | 59 | Percentage |
| Age: n, % | ||||||||
| – <55 | 33 | 27.5 | 16 | 29.6 | 1 | 14.3 | 16 | 27.1 |
| – 55–64 | 47 | 39.2 | 21 | 38.9 | 1 | 14.3 | 25 | 42.4 |
| – 65–74 | 30 | 25.0 | 12 | 22.2 | 4 | 57.1 | 14 | 23.7 |
| – 75+ | 10 | 8.3 | 5 | 9.3 | 1 | 14.3 | 4 | 6.8 |
| Age: mean (SD) | 60.3 (9.7) | 59.4 (10.4) | 65.3 (10.83) | 60.6 (8.61) | ||||
| Ethnicity: n % | ||||||||
| – Caucasian | 60 | 50.4 | 27 | 50.0 | 5 | 71.4 | 28 | 48.3 |
| – Other | 22 | 18.5 | 12 | 22.2 | 1 | 14.3 | 9 | 15.5 |
| – Unknown | 37 | 30.8 | 15 | 27.8 | 1 | 14.3 | 21 | 36.2 |
| History of breast cancer: n % | ||||||||
| – Yes | 13 | 10.8 | 5 | 9.3 | 8 | 13.6 | ||
| – No | 102 | 85.0 | 45 | 83.3 | 7 | 100.0 | 50 | 84.7 |
| – Unknown | 5 | 4.2 | 4 | 7.4 | 1 | 1.7 | ||
| BRCA status: n % | ||||||||
| – BRCA1/BRCA2 | 20 | 16.7 | 7 | 13.0 | 1 | 14.3 | 12 | 20.3 |
| – Wild type | 37 | 30.8 | 15 | 27.8 | 2 | 28.6 | 20 | 33.9 |
| – Unknown | 62 | 52.5 | 31 | 57.4 | 4 | 57.1 | 27 | 45.8 |
| Surgery outcome (residual): n % | ||||||||
| – No residual | 32 | 26.7 | 16 | 29.6 | 3 | 42.9 | 13 | 22.0 |
| – <1 cm residual | 52 | 43.3 | 22 | 40.7 | 2 | 28.6 | 28 | 47.5 |
| – 1+ cm residual | 31 | 25.8 | 13 | 24.1 | 2 | 28.6 | 16 | 27.1 |
| – Unknown | 5 | 4.2 | 2 | 3 | 2 | 3.4 | ||
| FIGO stage: n % | ||||||||
| – Stage 3A/3B | 10 | 8.3 | 4 | 6 | 4 | 6.8 | ||
| – Stage 3C | 85 | 70.8 | 46 | 69.7 | 6 | 85.7 | 40 | 67.8 |
| – Stage IV | 25 | 20.8 | 16 | 24.2 | 1 | 14.3 | 15 | 25.4 |
| Chemotherapy type: n % | ||||||||
| – Adjuvant | 62 | 51.7 | 31 | 47 | 2 | 28.6 | 29 | 49.2 |
| – Neo adjuvant | 58 | 48.3 | 35 | 53 | 5 | 71.4 | 30 | 50.8 |
There were 120 patients identified, of which 66 fulfilled the study inclusion and exclusion criteria. Of these 66, 7 were excluded from further analyses because they died before receiving the chemotherapy after the recurrence.
FIGO: International Federation of Gynecology and Obstetrics.
Seven patients (11%) with comorbidities and poor performance status died without receiving further chemotherapy postrecurrence and were not included in the cost analysis. Of the remaining 59 patients, 16 (24%) received one line, 21 (32%) received two and 22 (33%) received three or more lines of cytotoxic chemotherapy for recurrent disease. There were no statistically significant differences with respect to patient demographics and disease parameters between the patient groups.
The patients that received only one line of chemotherapy had a lower proportion of patients younger than 55 years old (18.8 vs 28.65 and 31.8%), lower proportion with history of breast cancer (6.3 vs 19.0 and 13.6%), lower proportion with wild-type BRCA (18.8 vs 28.6 and 50.0%) and higher proportion with no residual after surgery (31.3 vs 19.0 and 18.2%) when compared with those receiving two or more lines.
Patients that received two lines of chemotherapy postrecurrence had lower proportion with International Federation of Gynecology and Obstetrics (FIGO) stage IV (19.0 vs 31.3 and 27.3%), platinum resistant tumors (14.3 vs 26.7 and 31.8%) and treated with neoadjuvant chemotherapy (38.1 vs 62.5 and 54.5%) when compared with patients treated with one or more than three lines, respectively (Table 2).
| Variable | Total lines of chemotherapy postrecurrence | p-value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | >= 3 | Total | |||||||
| N | Percentage | N | Percentage | N | Percentage | N | Percentage | |||
| N | 16 | 21 | 22 | 59 | ||||||
| Age group | <55 | 3 | 18.8 | 6 | 28.6 | 7 | 31.8 | 16 | 27.1 | 0.060 |
| 55–64 | 8 | 50.0 | 5 | 23.8 | 12 | 54.5 | 25 | 42.4 | ||
| 65–74 | 5 | 31.3 | 6 | 28.6 | 3 | 13.6 | 14 | 23.7 | ||
| >= 75 | 4 | 19.0 | 4 | 6.8 | ||||||
| Age (years): mean (SD) | 61.1 (6.6) | 62.8 (11.12) | 58.3 (6.72) | 60.6 (8.61) | 0.227 | |||||
| Race | Caucasian | 8 | 50.0 | 8 | 40.0 | 12 | 54.5 | 28 | 48.3 | 0.422 |
| Other | 1 | 6.3 | 3 | 15.0 | 5 | 22.7 | 9 | 15.5 | ||
| Unknown | 7 | 43.8 | 9 | 45.0 | 5 | 22.7 | 21 | 36.2 | ||
| History of breast cancer | Yes | 1 | 6.3 | 4 | 19.0 | 3 | 13.6 | 8 | 13.6 | 0.560 |
| No | 15 | 93.8 | 17 | 81.0 | 18 | 81.8 | 50 | 84.7 | ||
| Unknown | 1 | 4.5 | 1 | 1.7 | ||||||
| BRA | BRCA1/BRCA2 | 4 | 25.0 | 5 | 23.8 | 3 | 13.6 | 12 | 20.3 | 0.337 |
| Wild type | 3 | 18.8 | 6 | 28.6 | 11 | 50.0 | 20 | 33.9 | ||
| Unknown | 9 | 56.3 | 10 | 47.6 | 8 | 36.4 | 27 | 45.8 | ||
| Surgery outcome (residual) | None | 5 | 31.3 | 4 | 19.0 | 4 | 18.2 | 13 | 22.0 | 0.565 |
| <1 cm | 7 | 43.8 | 10 | 47.6 | 11 | 50.0 | 28 | 47.5 | ||
| >= 1 cm | 4 | 25.0 | 5 | 23.8 | 7 | 31.8 | 16 | 27.1 | ||
| Unknown | 2 | 9.5 | 2 | 3.4 | ||||||
| FIGO stage | IIIA/IIIB | 1 | 6.3 | 3 | 14.3 | 4 | 6.8 | 0.410 | ||
| IIIC | 10 | 62.5 | 14 | 66.7 | 16 | 72.7 | 40 | 67.8 | ||
| IV | 5 | 31.3 | 4 | 19.0 | 6 | 27.3 | 15 | 25.4 | ||
| Platinum sensitive† | Yes | 11 | 73.3 | 18 | 85.7 | 15 | 68.2 | 50 | 76.9 | 0.517 |
| No | 4 | 26.7 | 3 | 14.3 | 7 | 31.8 | 15 | 23.1 | ||
| Chemotherapy type | Adjuvant | 6 | 37.5 | 13 | 61.9 | 10 | 45.5 | 29 | 49.2 | 0.308 |
| Neoadjuvant | 10 | 62.5 | 8 | 38.1 | 12 | 54.5 | 30 | 50.8 | ||
The p-value based on χ2 test and analysis of variance for mean age.
†
Platinum sensitivity was not know for one patient with I line of chemotherapy.
FIGO: International Federation of Gynecology and Obstetrics.
The median OS from first diagnosis for patients with one, two and three or more chemotherapy lines postrecurrence was 36.7, 50.7 and 42.8 months, respectively (p = 0.941; Figure 1); median PFS was 13.3, 13.6 and 14.7 months, respectively (p = 0.161; Figure 2). Median OS for the entire cohort from first recurrence was 21.0 months (95% CI: 17.25, 24.7) and from initiation of chemotherapy for the third relapse it was 7.9 months (95% CI: 3.6, 11.74).
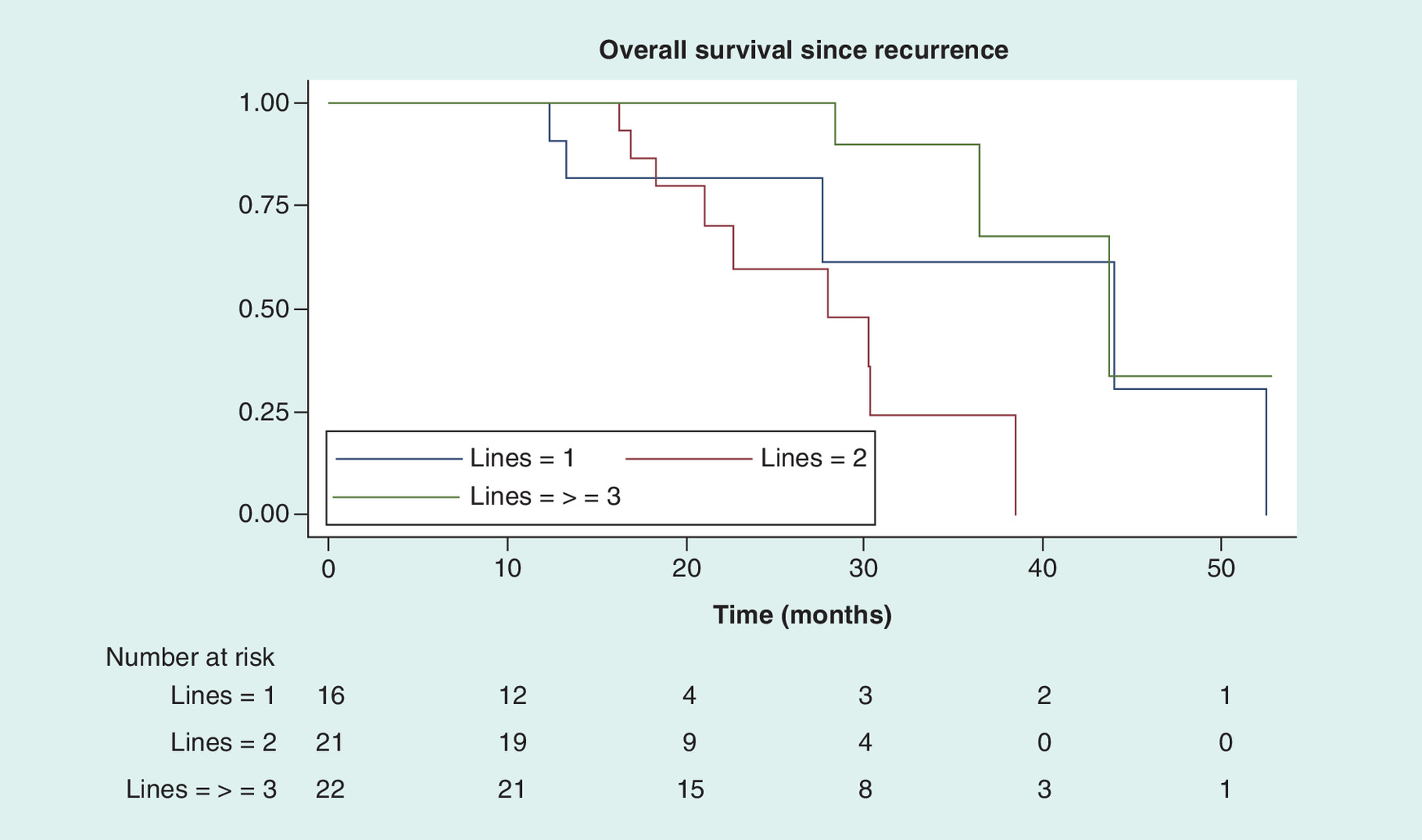
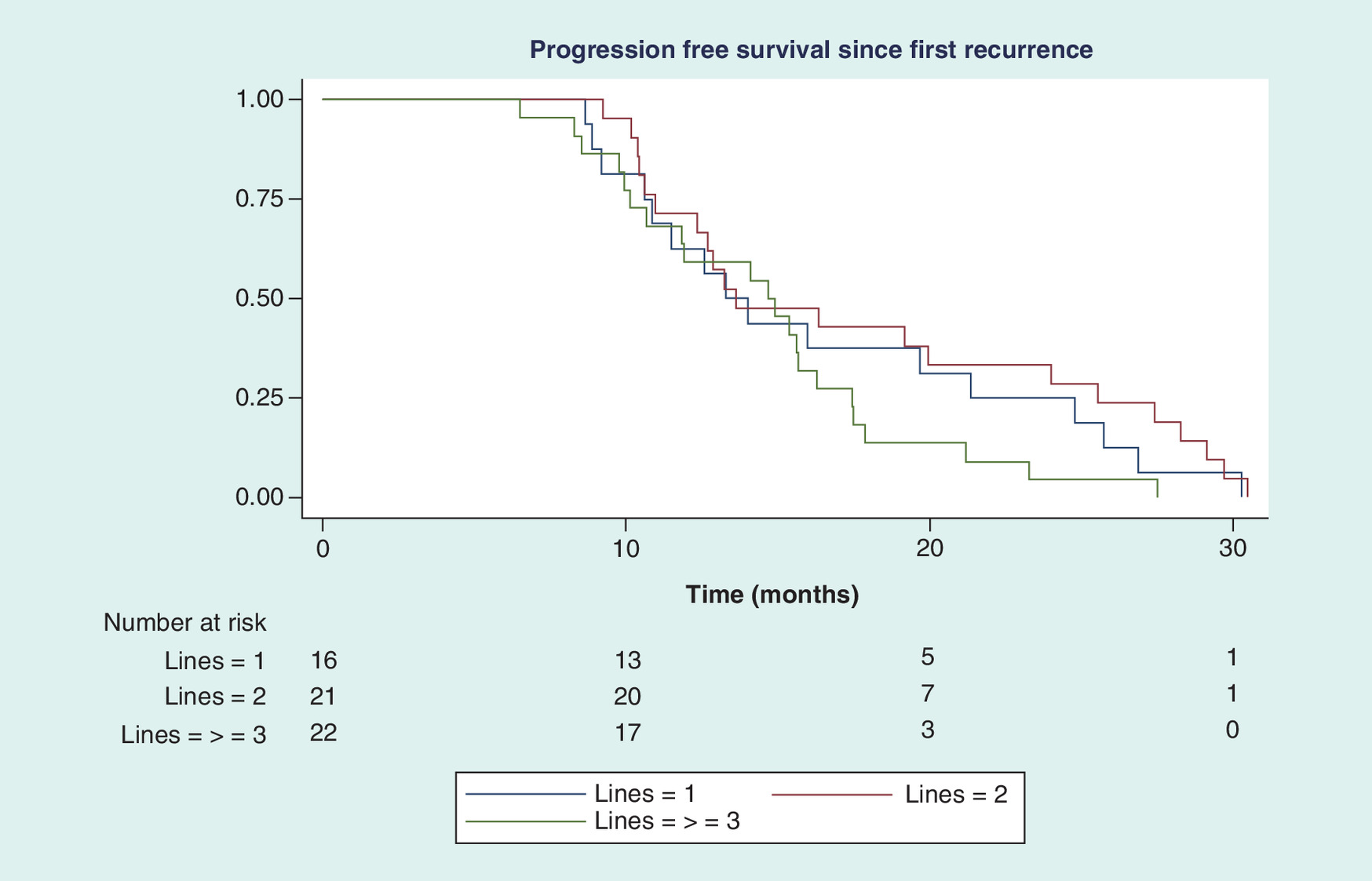
Table 3 shows that compared with the mean healthcare costs incurred for patients receiving one line of chemotherapy (CAD$52,227) for relapsed disease, the mean total costs were 38% ($72,374) and 86% ($97,243) higher, respectively, for those treated with two or three and more lines of chemotherapy. The mean for all cost components increased with the number of chemotherapy lines used. In-hospital stay was the largest contributor to healthcare costs for all groups, accounting for 71% of the direct costs (Figure 3). The cost of all prescription medications, including chemotherapy, accounted for 17% of the total direct healthcare costs across all treatment groups.
| Cost component | Total lines of chemotherapy postrecurrence | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | ≥3 | Total | ||||||||||
| Mean | Median | IQR | Mean | Median | IQR | Mean | Median | IQR | p-value† | Mean | Median | IQR | |
| Drugs | $10,380 | $2670 | $4078 | $9646 | $6450 | $8366 | $18,442 | $16,237 | $12,549 | 0.001 | $13,126 | $8942 | $12,094 |
| ER visits | $875 | $467 | $1167 | $1267 | $934 | $1400 | $1507 | $1400 | $1400 | NS | $1250 | $934 | $1400 |
| Drains/materials | $874 | $290 | $1210 | $900 | $540 | $1133 | $2039 | $828 | $2097 | NS | $1318 | $540 | $2398 |
| Transfusion | $570 | $454 | $454 | $974 | $905 | $551 | $1343 | $1455 | $810 | <0.001 | $1002 | $908 | $1103 |
| Imaging | $2695 | $2966 | $3190 | $2851 | $2516 | $1406 | $3287 | $3371 | $1784 | NS | $2972 | $3213 | $1640 |
| Surgery/radiotherapy | $3581 | $3505 | $1400 | $4007 | $4616 | $4708 | $3753 | $4028 | $1870 | NS | $3838 | $4028 | $3523 |
| Outpatient visits | $1232 | $1034 | $1334 | $1753 | $1698 | $977 | $2237 | $2184 | $1241 | 0.004 | $1792 | $1716 | $2002 |
| Inpatient stay | $34,092 | $16,373 | $45,431 | $53,281 | $55,392 | $59,886 | $66,473 | $65,690 | $67,105 | 0.036 | $52,997 | $46,033 | $52,930 |
| Total costs: | |||||||||||||
| Entire cohort | $52,277 | $43,139 | $57,507 | $72,374 | $79,001 | $61,146 | $97,243 | $93,089 | $64,196 | 0.010 | $76,197 | $74,017 | $62,892 |
| Platinum sensitive | $50,898 | $28,296 | $65,386 | $67,886 | $55,023 | $54,435 | $91,622 | $91,859 | $65,435 | 0.014 | $71,730 | $63,633 | $73,655 |
| Platinum resistant | $50,652 | $44,021 | $81,840 | $96,744 | $104,707 | – | $105,957 | $101,664 | $60,086 | 0.207 | $88,182 | $98,437 | $63,367 |
| p-value‡ | 0.794 | 0.269 | 0.860 | 0.364 | |||||||||
p-values are based on the Jonckheere–Terpstra test for ordered alternatives.
†
Between number of treatment lines;
‡
Platinum sensitive versus resistant.
IQR: Interquartile range.
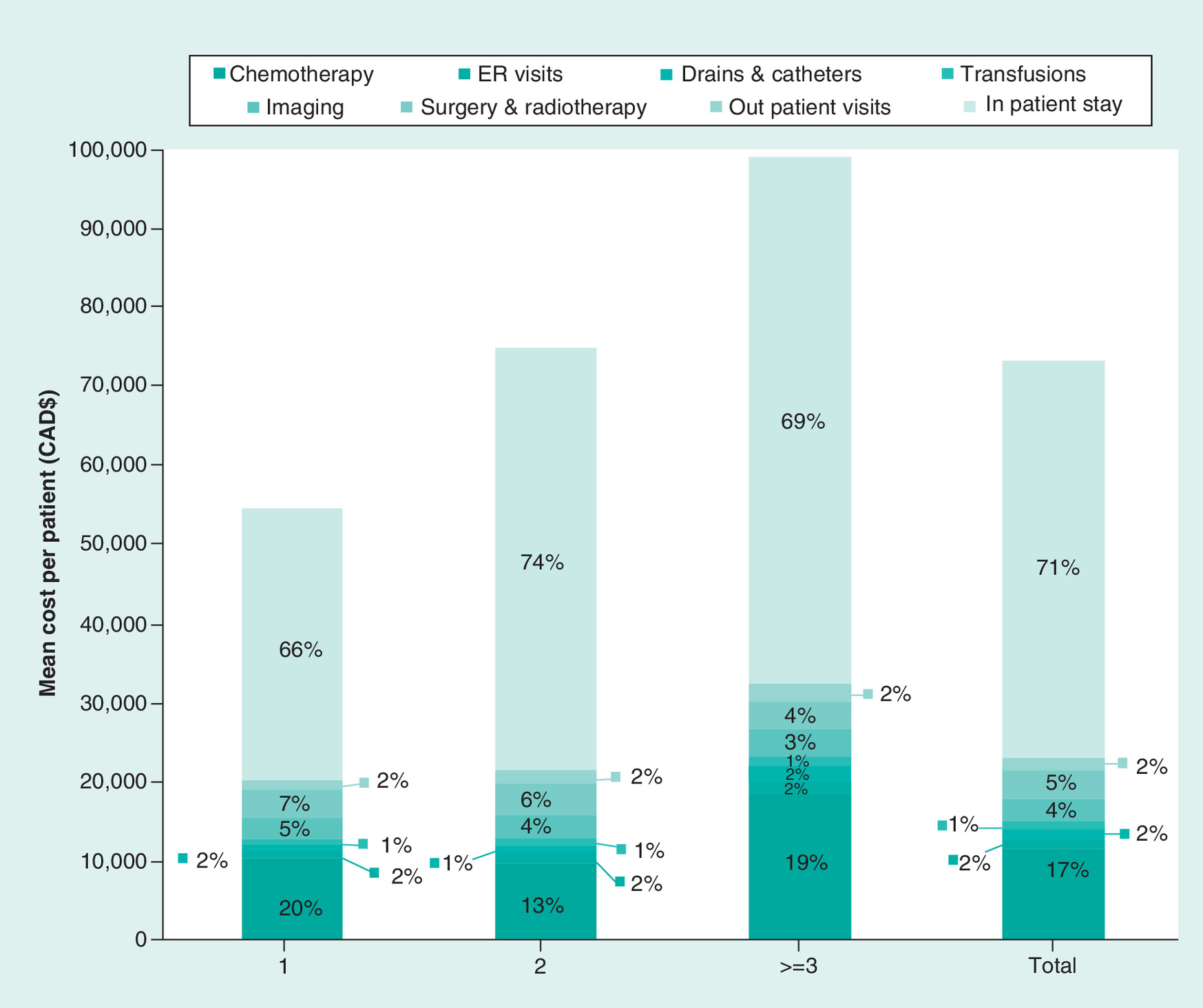
Figure 3. Total direct healthcare cost by number of postrecurrence chemotherapy treatments.
In-hospital stay was the largest contributor to healthcare costs, accounting for 71% of the total direct healthcare costs, while the cost of medications accounted for 17% of the costs.
Figure 4 shows the quintile distributions of the total costs by the number of postrecurrence lines of chemotherapy. The respective distribution of total healthcare costs for patients receiving one, two and three or more lines of chemotherapy were below $79,900 in 57, 38 and 18% between $79,900 and $109,854 in 6, 33 and 18% and above $109 854 for 13, 14 and 41%, respectively, for each group.
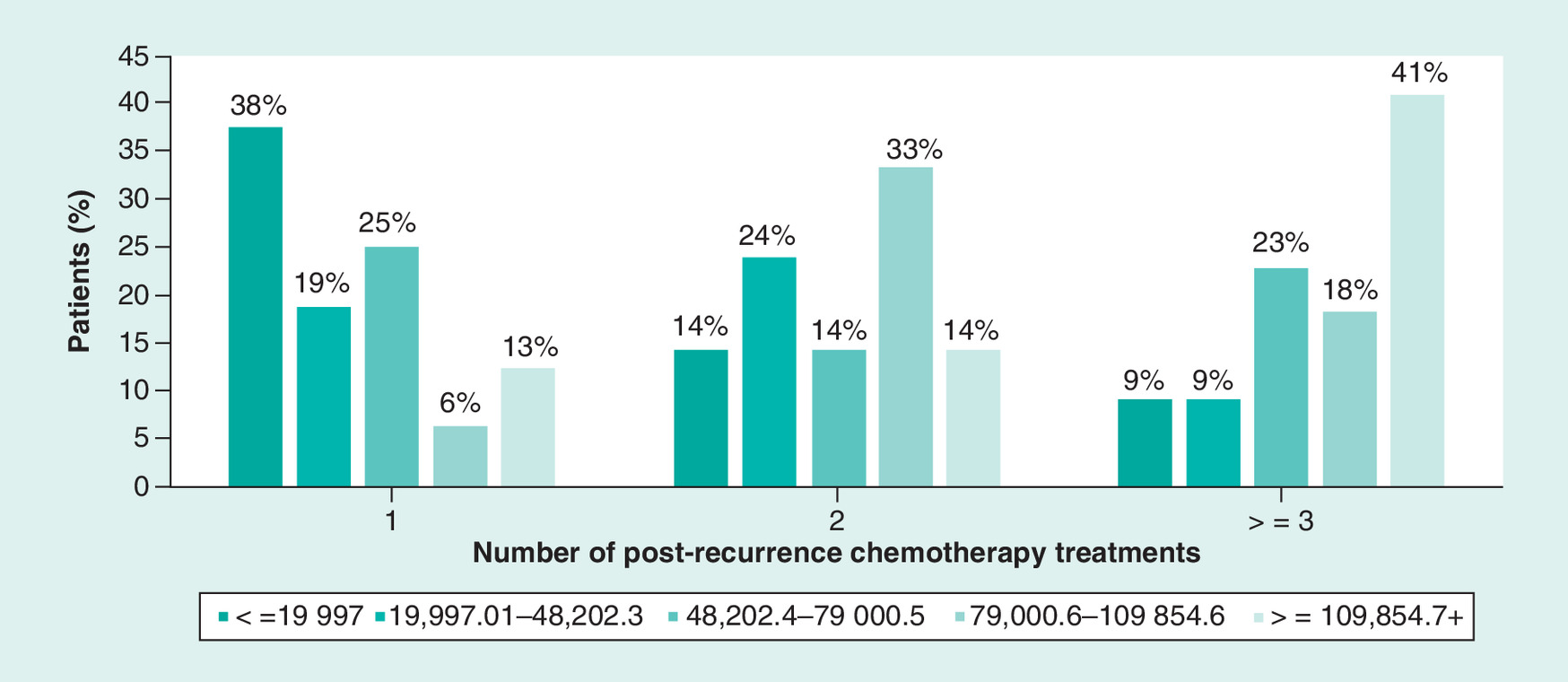
Figure 4. Distribution of total direct healthcare costs by number of postrecurrence chemotherapy treatments.
With increasing number of chemotherapy treatments, the proportion of patients in whom costs exceeded CAD$109,854 increased from 13 to 41%.
The total direct healthcare costs for patients with platinum resistance disease were higher when compared with those with platinum sensitive tumors, although the differences were not statistically significant (p = 0.364). The increase in total direct healthcare costs with higher number of lines of chemotherapy treatment was similar for platinum sensitive and resistant disease. Furthermore, chemotherapy accounted for 14.8 and 24.5%, and inpatient cost accounted for 71.5 and 66.4% of the total direct healthcare costs for patients with platinum sensitive and resistant disease respectively (Figure 5).
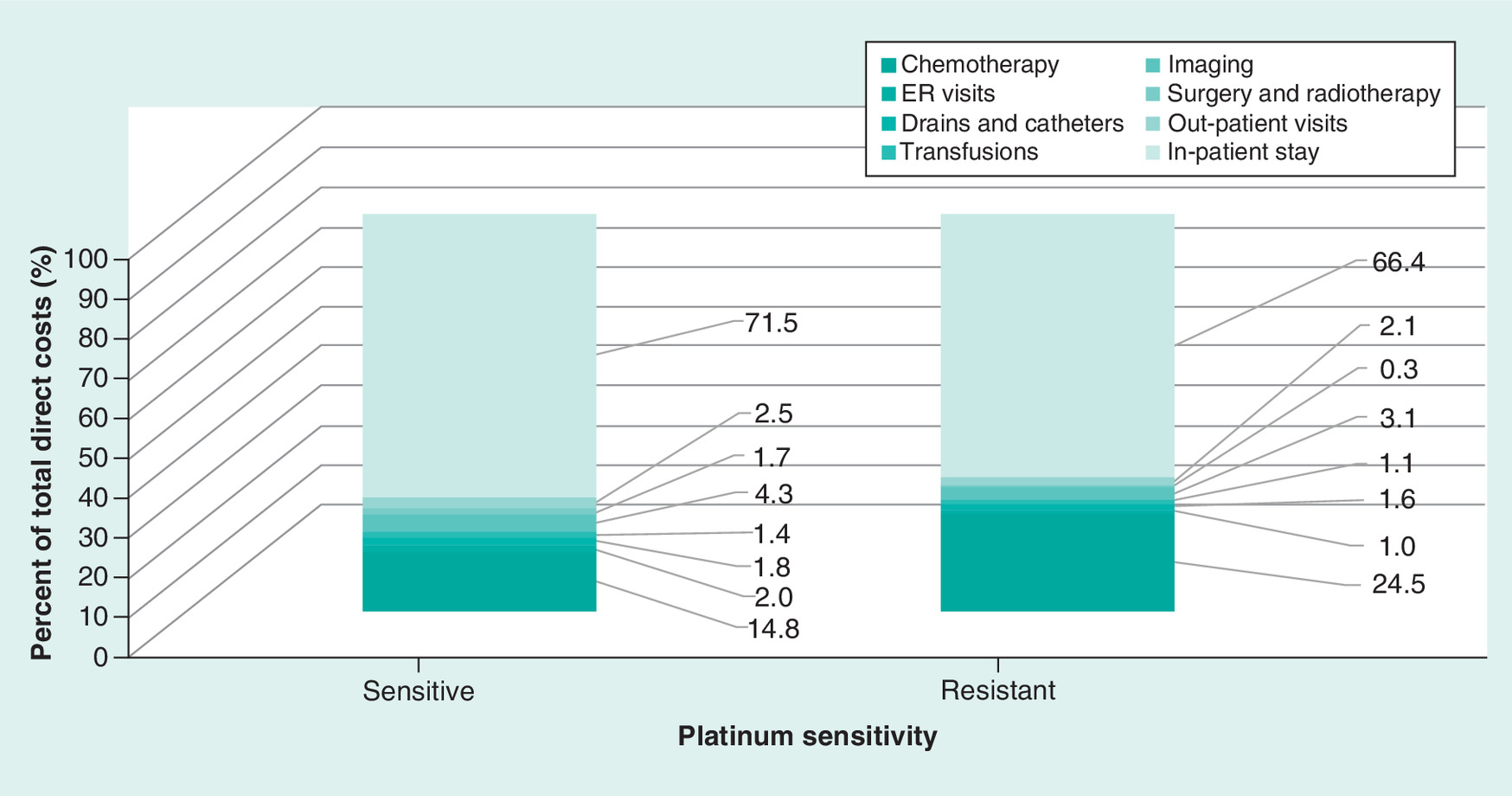
Figure 5. Distribution of total direct healthcare costs by platinum sensitivity of the disease.
The distribution of sources of cost was similar for patients with platinum sensitive and resistant disease with the majority of the costs being due to in-hospital stay.
ER: Emergency room.
After adjusting for patient’s age, race, BRCA type, use of adjuvant chemotherapy, history of breast cancer, FIGO status and platinum sensitivity, the mean (95% CI) total direct health costs for 1, 2 and >= 3 lines of postrecurrence chemotherapy were $68,805 ($39,238–$98,374), $84,482 ($56,723–$112,242) and $107,202 ($81,396–$133,008; Figure 6).
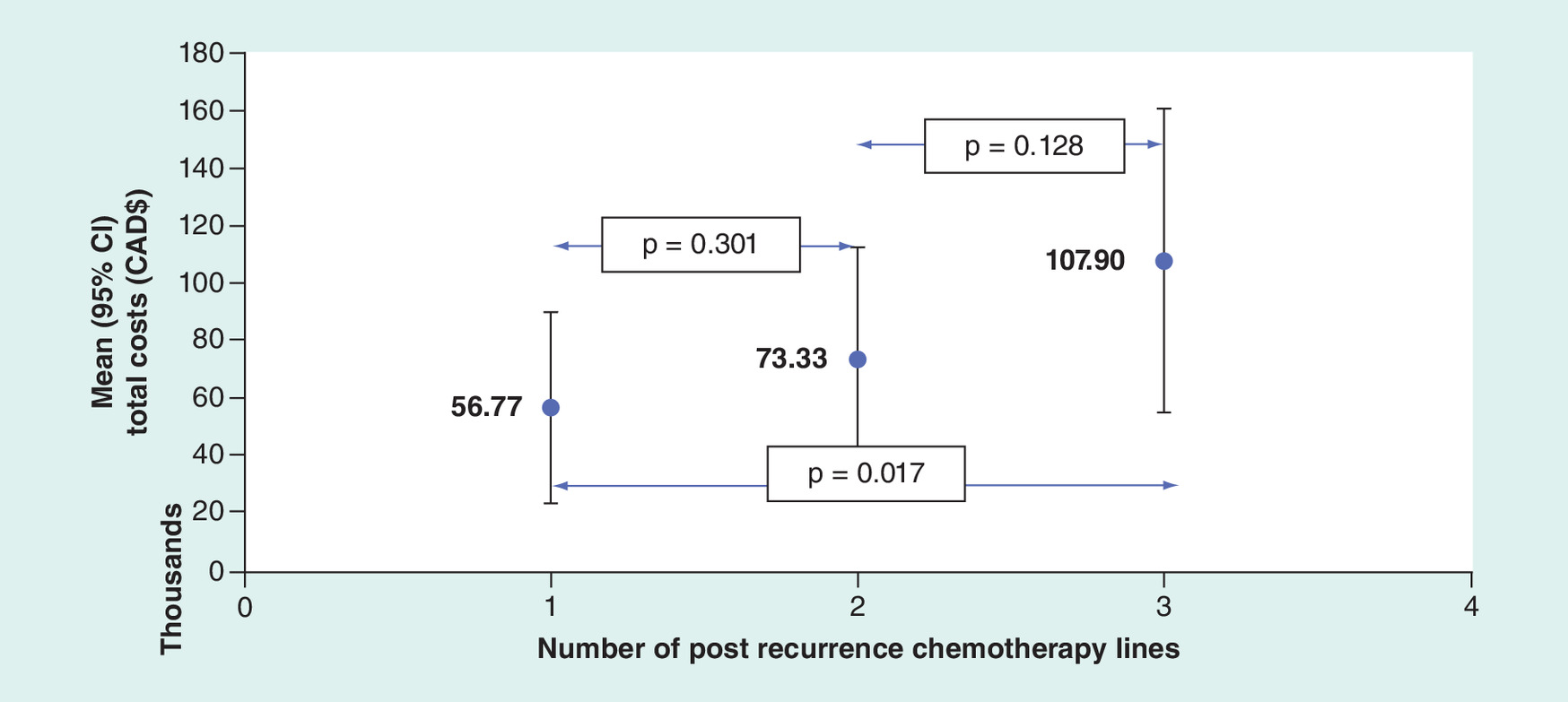
Figure 6. Total direct healthcare costs by number of chemotherapy lines postrecurrence.
Least square means adjusted for race, history of breast cancer, BRCA, chemotherapy type (adjuvant vs neoadjuvant), FIGO status, platinum sensitivity.
Inpatient stay was the major driver of the between-group differences in adjusted direct health costs, contributing 80.8% of the cost variance, with chemotherapy accounting for 8.1% (Table 4).
| Independent variable | Cost variance (%)† |
|---|---|
| Inpatient stay | 80.84 |
| Chemotherapy | 8.09 |
| Imaging | 3.31 |
| Surgery and radiotherapy | 2.33 |
| Outpatient visits | 0.87 |
| ER visits | 0.46 |
| Drains and catheters | 0.20 |
| Transfusions | 0.01 |
| Patient and disease parameters‡ | 3.89 |
†
Proportion of variance in direct healthcare costs explained by each variable in multivariate analysis of variance model.
‡
Number of postrecurrence chemotherapy lines, race, history of breast cancer, BRCA, chemotherapy type (adjuvant vs neoadjuvant), International Federation of Gynecology and Obstetrics status, platinum sensitivity.
ER: Emergency room.
The results of the multivariate linear regression analysis showed that after adjusting for the same covariates listed above, each additional line of chemotherapy postrecurrence increased the total direct healthcare costs by $10,620 (p = 0.067; Table 5). This analysis also showed that the effect of history of breast cancer (p = 0.109), BRCA type (p = 0.113) and FIGO stage (p = 0.116) on total direct healthcare costs approached statistical significance.
| Independent/predictor variable | Parameter estimate (β) | SE (β) | p-value |
|---|---|---|---|
| Constant | 24437.74 | 35361.93 | 0.493 |
| Number of post recurrence chemotherapy lines | 10619.53 | 5677.61 | 0.067 |
| Race (caucasian vs other) | -13644.45 | 14032.37 | 0.336 |
| History of breast cancer (yes vs no) | 37394.65 | 22912.20 | 0.109 |
| BCRA-1/2 vs wild type/unknown | -29760.88 | 18449.52 | 0.113 |
| Chemotherapy (adjuvant vs neoadjuvant) | -12931.55 | 15387.37 | 0.405 |
| FIGO 3C vs 3A/3B | 29337.85 | 30940.66 | 0.348 |
| FIGO IV vs 3A/3C | 53175.68 | 33245.24 | 0.116 |
| Platinum sensitive vs resistant | -4364.59 | 17585.44 | 0.805 |
Dependent variable = total direct healthcare costs.
FIGO: International Federation of Gynecology and Obstetrics.
Discussion
In the current study of patients with recurrent ovarian HGSC, continued chemotherapy after the third recurrence did not improve OS or PFS. This is similar to the results reported by Boyle [16] and suggests that when all patients with this disease receive a uniformly high standard of care, patient outcomes are most likely determined by patient characteristics and the biology of the disease, rather than the number of lines of chemotherapy. However, with each recurrence and associated treatment, the direct healthcare costs increased substantially. The proportion of patients in whom costs exceeded $109,854 (the fifth quintile) increased from 13% in those treated with one line of chemotherapy to 41% in those treated with three or more lines for repeated relapses. After adjusting for patient and disease parameters, the major driver of healthcare costs in this cohort of patients was inpatient hospital services accounting for 81%, while drug acquisition costs accounted for only 8% of the total.
The pooled results of three large Phase III randomized control trials including 1620 patients showed that the median survival was 8.9, 6.2 and 5.0 months respectively, after treatment of the third, fourth and fifth relapse [7]; the authors suggested that, after three relapses, additional chemotherapy treatments did not appear to be clinically worthwhile. Although patients recruited into randomized control trials are generally selected for better baseline health, in our unselected cohort of patients treated with three or more regimens of chemotherapy for relapse, the median OS of 7.9 months (95% CI: 3.6, 11.7), from the third relapse, was comparable to that of the above study.
The main strength of this study is that it reflects real-world practice. Additional strengths include near complete ascertainment of direct healthcare costs, the granularity of the data, and the homogeneous study population focusing on only stage-III/IV patients with recurrent HGSC. Furthermore, patients were treated by an accredited interdisciplinary team, benefited from the best available treatment regardless of their financial situation, and had access to supportive and palliative care services early in the trajectory of recurrent disease. The lack of improved survival with repeated cytotoxic chemotherapy after the third relapse, even in these near optimal conditions, reveals a major treatment gap for these patients, one that warrants careful consideration for investment in targeted treatments instead of cytotoxic chemotherapy. This study provides useful benchmark cost data for analyses comparing new treatments to conventional cytotoxic chemotherapy. In addition, the current study provides data that can be used to model the effect of additional lines of post recurrence chemotherapy in the real-world setting.
Limitations of this study are inherent to retrospective chart reviews and hospital health record databases. One of the main limitations of retrospective studies is that certain costs may not be ascertained and hence the overall costs would be underestimated. We could only ascertain costs that were documented in medical charts and hospital databases. Costs for physician fees, community clinics, rehabilitation, palliative services and home care as well as indirect healthcare and intangible costs were not included. Physician fees, being the most important of the nonincluded costs, could not be accurately ascertained, as the Quebec supplemental fee system would render estimates unreliable. Data from the literature on direct healthcare costs for ovarian cancer treatment indicate that physician fees account for 13–20% when chemotherapy administration is included as a physician service [20,21]. Thus, the impact of not including physician-fees on the validity of the results is unlikely to be material but would most likely increase with repeated lines of chemotherapy and further dilute the impact of drug acquisition costs on the total.
Another potential limitation of the study is that the data were derived from a single Canadian University Health Center and that this can affect the generalizability of the results to the target populations of patients with recurrent high-grade serous ovarian cancer that are treated in other provinces of Canada or in other countries.
The MUHC is one of the two University Tertiary Centers in Quebec and one of the few institutions where advanced cancer care is provided in the province. Based on the above, we can consider the sample of patients treated in the MUHC to be an unbiased, and random and hence a valid representative of the Quebec population of women with advanced ovarian cancer.
The age adjusted and overall incidence rates of ovarian cancer is not different between Canadian provinces [22]. Furthermore, the profile, treatment protocols and outcomes of patients with high-grade recurrent serous ovarian cancer will not be different between Canadian provinces and most likely between different developed countries. We can therefore accept that the sample of patients with high-grade recurrent serous ovarian cancer in our study is a reasonable representation of the target population in Canada and developed countries.
With respect to the absolute cost for treatment the recurrences with sequential cytotoxic chemotherapy, there may be differences between provinces and certainly between countries. However, the focus of the study results and the message conveyed, is not with respect to the absolute costs but the relative costs, and specifically the increase in costs with sequential cytotoxic chemotherapies and the proportional contribution of each service component to the overall hospital costs. We can, therefore, accept that while generalization of the absolute cost results in our study to other time periods or provinces may be somewhat limited, the inference to the target population with respect to the impact of repeated sequential chemotherapies and the relative contribution of the different service components to the total costs is reasonable.
Generalization of results in the Universal Canadian healthcare system to other jurisdictions without universal healthcare, with respect to absolute and even relative costs, may be limited. Nonetheless, the results of studies from the Canadian Universal healthcare system, provide valuable benchmark estimates of the absolute costs and relative increases in costs in a setting where access to care is universal. In other words, these studies allow us to conduct health economic assessments under ideal conditions where all patients have access to the same high-quality care.
We could not discern from the clinical notes which of the various factors associated with advanced cancer namely, disease burden, drug toxicity or physical deterioration dictated the need for more inpatient treatment, as these were intertwined. Patients with advanced, recurrent on cytotoxic chemotherapy require frequent admissions to resource-intensive, inpatient units, because any adverse event in a patient on chemotherapy treatment warrants investigations/interventions due to the possibility that it is chemotherapy related and therefore potentially reversible. However, with repeated relapses, bowel-obstruction, increasing pleural effusion and ascites is a function of disease progression for which cytotoxic chemotherapy rarely helps [23].
Our results show that while continuing treatment with more than three lines of chemotherapy does not improve survival, the need for inpatient care reflecting deterioration of functioning was associated with substantially higher costs. This finding is comparable with the data reported by others. Lewin et al. found no improvement in survival in patients treated with chemotherapy compared with those receiving palliative care during the end-of-life period; however, there was a significant cost difference [24].
The results of this study and the others attesting to downstream human and financial consequences of using repeated regimens of cytotoxic chemotherapy for HGSC recurrences calls for reappraisal of the current paradigm for treating this disease. Increasingly, new therapies/interventions that are more effective in prolonging life with lower toxicity are becoming available but are much more expensive. When considering the value of these treatments, it would be necessary to compare drug acquisition costs along with downstream healthcare costs associated with these treatments.
Future perspective
The incorporation of newer treatments for cancer that will include targeted therapies, immunotherapies and personalized medicine will be challenged by higher acquisition costs in comparison to currently used cytotoxic chemotherapy-based regimens. Comparative cost–effectiveness studies will be required to assess the societal benefits of these advanced treatments and to appropriately allocate healthcare resources and funding. Real-world ascertainment of the direct healthcare costs associated with conventional cytotoxic chemotherapy treatment will be essential in these evaluations that must consider not only acquisition costs, but all direct healthcare costs related to the management of cancer patients. The current study provides real-world estimates of costs for repeated cytotoxic therapies in patients with recurrent high-grade serum ovarian cancer as well as parameters that can be used in the development of health economic models for the treatment of this disease.
•
Recurrent high-grade serous cancer (HGSC) of the ovaries is largely incurable.
•
The goal of treatment is palliation but repeated treatments with cytotoxic chemotherapy have limited efficacy and high toxicity.
•
Precision therapies delay recurrence with lower toxicity, but drug acquisition costs are high.
•
This study ascertains the real-world healthcare costs of treating recurrent HGSC with successive regimens of standard-of-care chemotherapy.
•
We ascertained the total direct healthcare costs for the treatment of 66 women with stage III/IV HGSC with sequential lines of chemotherapy for their recurrences.
•
Healthcare costs ascertained were comprised of costs for prescription medications including chemotherapy, imaging, blood tests, surgical and medical interventions, nursing, and auxiliary healthcare provided in the ambulatory, emergency department and inpatient settings.
•
Patients received a median of two lines of chemotherapy for recurrent disease; 33% received three or more lines.
•
Median overall survival (from diagnosis to death) was 36.0, 50.7 and 42.8 months, respectively, for patients receiving one, two, and three or more lines of chemotherapy postrecurrence (p = 0.941).
•
Mean cost of treatment of first relapse was CAD$52,227, and increased by 38% for two, and 86% for three or more relapses.
•
In-hospital care was the major driver of healthcare costs, accounting for 71% of the total, while drugs accounted for 17%.
•
After the third relapse of HGSC, cytotoxic chemotherapy did not prolong survival but was associated with substantially increased healthcare costs, largely due to the need for in hospital care.
•
Downstream real-world costs, including the need for inpatient support associated with repeated cytotoxic therapy should be considered in addition to drug acquisition costs when conducting health economic comparisons of novel precision targeted therapies versus standard of care cytotoxic chemotherapies.
Author contributions
MC Festa, L Shbat, MA Alsoud and C Martins collected data and contributed to interpretation of the results and literature searches. AV Ramanakumar and J Sampalis were responsible for data analysis and interpretation of the results. L Gilbert, M Wolfson and O Basso contributed to interpretation of results. L Gilbert, K Jardon, X Zeng and M Borod cared for the patients who were the subject of the study, supervised data acquisition and interpretation. L Gilbert conceived, designed and planned the study, obtained funding, and drafted the manuscript with the help of O Basso and J Sampalis. All authors contributed to critically reviewing iterations of the manuscript and approved the final version for submission.
Acknowledgments
The views expressed in this publication are those of the authors and not those of the funders.
Financial & competing interests disclosure
The authors gratefully acknowledge generous funding in the form of an unrestricted grant from AstraZeneca. They are grateful for the invaluable help provided by R Walton, MPH, of AstraZeneca with procuring the start-up funds, for the initial literature search, and for helpful and insightful suggestions. The authors are grateful to J Quennville of the Royal Victoria Hospital Foundation and J Shamie of The Cedars Cancer Institute for timely support with procuring critical funds to continue and complete the project. L Gilbert reports grants from AstraZeneca during the conduct of the study and has received lecture honoraria and consultation fees from Roche, AstraZeneca, Pfizer, consultation fees from Wyeth, and research funding from Canadian Institutes of Health Research, National Institutes of Health, US Department of Defense, Rossy Cancer Network, Royal Victoria Hospital Foundation, The Doggone foundation, Cedars Cancer Institute, Montreal General Hospital Foundation, Carole Epstein Foundation, McGill Collaborative Research Development Fund, Tesaro Inc, Pfizer Inc., ImmunoGen Inc., AstraZeneca, Merck Canada Inc., Endocyte Inc., Aeterna Zentaris, Boehringer Ingelheim, Biogen Idec, Aventis Pharma Inc., Wyeth Canada and Merck Frosst Canada Inc. outside the submitted work. K Jardon and X Zeng have received research funding from Tesaro Inc., Pfizer Inc., ImmunoGen Inc., AstraZeneca and Aeterna Zentaris, outside the submitted work. J Sampalis has received honoraria as a consultant for several pharmaceutical companies including Roche, Pfizer, Novartis, AbbVie, GSK, BMS, Janssen, Celgene, Amgen, Merck, Oncozyme, Oncolytics, Ethicon Endosurgery, Forrest, Genzyme, Lundbeck, IMS, Novo Nordisk, Otsuka, Servier, Shire, Theratechnologies, Valeant and others, outside the submitted work. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Dedication
Dedicated to the loving memory of Dr T Sampalis MD, PhD, innovator of microinvasive breast cancer surgery, who beat ovarian cancer but lost the battle to the toxic effects of chemotherapy.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J. Clin. 67(1), 7–30 (2017).
2.
Mariotto AB, Yabroff KR, Shao YW, Feuer EJ, Brown ML. Projections of the cost of cancer care in the United States: 2010–2020. JNCI-J. Natl Cancer Inst. 103(2), 117–28 (2011).
3.
Pignata S, Cecere SC, Du Bois A, Harter P, Heitz F. Treatment of recurrent ovarian cancer. Ann. Oncol. 28, 51–6 (2017).
4.
Narod S. Can advanced-stage ovarian cancer be cured? Nature reviews. Clin. Oncol. 13(4), 255–61 (2016).
5.
Herzog TJ, Monk BJ. Bringing new medicines to women with epithelial ovarian cancer: what is the unmet medical need? Gynecol. Oncol. Res. Pract. 4, 13 (2017).
• Advanced and recurrent ovarian cancer is rarely cured, as multiple lines of platinum combinations or nonplatinum chemotherapeutics fail to achieve clinical benefit. Therefore, other active systemic therapies are needed. Recent advances have led to novel targeted treatments for recurrent ovarian cancer.
6.
Elit L, Hirte H. Palliative systemic therapy for women with recurrent epithelial ovarian cancer: current options. Onco Targets Ther. 6, 107–118 (2013).
• Although combination platinum-based chemotherapy has shown benefits for women with platinum-sensitive recurrent ovarian cancer, the optimal treatment strategy for those with platinum-resistant or platinum-refractory disease is not clear. Molecular and genetic targeted therapies may provide opportunities for those women with tumor profiles that show sensitivity for specific agents.
7.
Hanker LC, Loibl S, Burchardi N et al. The impact of second to sixth line therapy on survival of relapsed ovarian cancer after primary taxane/platinum-based therapy. Ann. Oncol. 23(10), 2605–2612 (2012).
• A maximum of three lines of subsequent relapse treatment seems to be beneficial for patients with recurrent ovarian cancer. Optimal primary tumor debulking and platinum sensitivity remain independent prognostic factors even after more frequent relapses.
8.
Ledermann J, Harter P, Gourley C et al. Olaparib maintenance therapy in patients with platinum-sensitive relapsed serous ovarian cancer: a preplanned retrospective analysis of outcomes by BRCA status in a randomised Phase 2 trial. Lancet Oncol. 15(8), 852–861 (2014).
9.
Mirza MR, Monk BJ, Herrstedt J et al. Niraparib maintenance therapy in platinum-sensitive, recurrent ovarian cancer. N. Engl. J. Med. 375(22), 2154–2164 (2016).
10.
Coleman RL, Oza AM, Lorusso D et al. Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): a randomised, double-blind, placebo-controlled, Phase 3 trial. Lancet 390(10106), 1949–1961 (2017).
11.
Pujade-Lauraine E, Ledermann JA, Selle F et al. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): a double-blind, randomised, placebo-controlled, Phase 3 trial. Lancet Oncol. 18(9), 1274–1284 (2017).
12.
Peppercorn J, Zafar SY, Houck K, Ubel P, Meropol NJ. Does comparative effectiveness research promote rationing of cancer care? Lancet Oncol. 15(3), 132–138 (2014).
13.
Poonawalla IB, Parikh RC, Du XLL, VonVille HM, Lairson DR. Cost–effectiveness of chemotherapeutic agents and targeted biologics in ovarian cancer: a systematic review. Pharmacoeconomics 33(11), 1155–1185 (2015).
14.
Giuliani J, Bonetti A. The pharmacological costs of second-line treatments for recurrent ovarian cancer. Int. J. Gynecol. Cancer 27(9), 1872–1876 (2017).
15.
Chrischilles EA, Friedman S, Ritzwoller DP, Selby JV. Patients, data, and progress in cancer care. Lancet Oncol. 18(11), E624–E625 (2017).
16.
Doyle C, Stockler M, Pintilie M et al. Resource implications of palliative chemotherapy for ovarian cancer. J. Clin. Oncol. 15(3), 1000–1007 (1997).
• There is potential to improve cost-efficiency by improving resource management, for example, by shifting from inpatient to outpatient chemotherapy, everything else being equal.
17.
Gordon LG, Scuffham PA, Beesley VL et al. Medical costs and outcomes for Australian women with ovarian cancer: a patient-level analysis over 2.5 years. Int. J. Gynecol. Cancer 20(5), 757–765 (2010).
18.
Delgado-Ortega L, Gonzalez-Dominguez A, Borras JM et al. The economic burden of disease of epithelian ovarian cancer in Spain: the OvarCost study. Eur. J. Health Econ. 20, 135–147 (2019).
19.
Rocconi RP, Case AS, Straughn JM Jr, Estes JM, Partridge EE. Role of chemotherapy for patients with recurrent platinum-resistant advanced epitelial ovarian cancer: a cost–effectiveness analysis. Cancer 107, 536–543 (2006).
20.
Cooper AL, Nelson DF, Doran S et al. Long-term survival and cost of treatment in patients with stage IIIC epithelial ovarian cancer. Curr. Womens Health Rev. 5(1), 44–50 (2009).
21.
Yawn BP, Wollan P, Klee M, Barrette B. Ovarian carcinoma: care and survival in a community-based population. Clin. Ther. 23(1), 146–159 (2001).
22.
Government of Canada. Cancer incidence in Canada: trends and projections (1983–2032)- ovarian cancer-HPCDP. 35(Suppl. 1), Chapter 4 (2015). www.canada.ca/en/public-health/services/reports-publications/health-promotion-chronic-disease-prevention-canada-research-policy-practice/vol-35-no-1-2015/supplement/page-06.html
23.
von Gruenigen VE, Huang HQ, Beumer JH et al. Chemotherapy completion in elderly women with ovarian, primary peritoneal or fallopian tube cancer – an NRG oncology/Gynecologic Oncology Group study. Gynecol. Oncol. 144(3), 459–467 (2017).
24.
Lewin SN, Buttin BM, Powell MA et al. Resource utilization for ovarian cancer patients at the end of life: how much is too much? Gynecol. Oncol. 99(2), 261–266 (2005).
• The findings demonstrate that there is a significant cost difference with no appreciable improvement in survival between ovarian cancer patients treated aggressively versus those enrolled in hospice at the end of life.
Information & Authors
Information
Published In
Pages: 537 - 551
PubMed: 32223298
Copyright
© 2020 John S Sampalis. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 14 February 2020
Accepted: 6 March 2020
Published online: 30 March 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-world direct healthcare costs of treating recurrent high-grade serous ovarian cancer with cytotoxic chemotherapy. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0032
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Matthew J. Monberg, Steve Keefe, Vassiliki Karantza, Konstantinos Tryfonidis, Sarper Toker, Jaime Mejia, Robert Orlowski, Amin Haiderali, Vimalanand S. Prabhu, Gursel Aktan, A Narrative Review of the Clinical, Humanistic, and Economic Value of Pembrolizumab-Based Immunotherapy for the Treatment of Breast and Gynecologic Cancers, Oncology and Therapy, 10.1007/s40487-024-00308-0, 12, 4, (701-734), (2024).
- Heather K. Barr, Andrea M. Guggenbickler, Jeffrey S. Hoch, Carolyn S. Dewa, Real-World Cost-Effectiveness Analysis: How Much Uncertainty Is in the Results?, Current Oncology, 10.3390/curroncol30040310, 30, 4, (4078-4093), (2023).
- Andrea M. Guggenbickler, Heather K. Barr, Jeffrey S. Hoch, Carolyn S. Dewa, Rapid Review of Real-World Cost-Effectiveness Analyses of Cancer Interventions in Canada, Current Oncology, 10.3390/curroncol29100574, 29, 10, (7285-7304), (2022).
- Manjusha Hurry, Shazia Hassan, Soo Jin Seung, Ryan Walton, Ashlie Elnoursi, Jacob McGee, Real-World Treatment Patterns, Survival, and Costs for Ovarian Cancer in Canada: A Retrospective Cohort Study Using Provincial Administrative Data, Journal of Health Economics and Outcomes Research, 10.36469/jheor.2021.29145, (114-121), (2021).
- Cytotoxic chemotherapy increases costs but not survival in recurrent ovarian cancer in Canada, PharmacoEconomics & Outcomes News, 10.1007/s40274-020-6741-5, 851, 1, (18-18), (2020).