Effectiveness of durvalumab versus chemotherapy in metastatic urothelial cancer: an observational, indirect comparison
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare the overall survival of patients with metastatic urothelial carcinoma (mUC) who failed platinum-based chemotherapy and received durvalumab or chemotherapy. Patients & methods: In an indirect comparison of patients with mUC who failed platinum-based chemotherapy, those who received durvalumab in a single-arm study were matched to patients from the Flatiron oncology electronic medical record database who received chemotherapy (n = 158 for each cohort). Matching was based on propensity scores. Kaplan–Meier methods and Cox regression models were utilized. Results: Median overall survival was 11.2 months (95% CI: 7.2–16.9) for durvalumab versus 8.2 months (95% CI: 6.7–9.8) for chemotherapy (hazard ratio: 0.63; 95% CI: 0.48–0.84). Conclusion: As a second-line therapy for mUC, durvalumab was associated with longer overall survival than chemotherapy.
Urothelial carcinoma (UC), which accounts for greater than 90% of all bladder cancers [1], is one of the ten predominant malignancies worldwide [2]. Systemic, platinum-based chemotherapy, introduced nearly 30 years ago, remains the standard of care for untreated patients with locally advanced or metastatic UC; this treatment is associated with a median overall survival (OS) of 13–15 months and a 5-year survival rate of approximately 15% [3–7]. The prognosis for patients who fail standard, platinum-based chemotherapy was historically dismal (median OS ranging from 5 to 7 months [4]), with a lack of effective second-line treatments [8].
The treatment landscape has changed since 2016, however, with the approval of five immuno-oncology (IO) agents by the US FDA: two anti-PD-1 antibodies, nivolumab and pembrolizumab, and three anti-PD-L1 antibodies, atezolizumab, avelumab and durvalumab [9]. Current National Comprehensive Cancer Network guideline recommendations include pembrolizumab as the preferred regimen, and nivolumab, atezolizumab, avelumab and durvalumab as alternative preferred regimens in the post-platinum setting [10].
Durvalumab was granted accelerated approval in May 2017 by the US FDA for the treatment of patients with locally advanced or metastatic UC whose disease progressed during or after one standard, platinum-based regimen or who had disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy. Efficacy evidence for durvalumab to support the claim in the proposed indication is based on an analysis of 182 patients treated with durvalumab 10 mg/kg every 2 weeks for up to 12 months or until progression in a single-arm, Phase I/II, open-label study (Study 1108, NCT01693562) [11]. The primary efficacy end point was objective response rate (ORR); results demonstrated an ORR of 17.0% for all evaluable patients (95% confidence interval [CI]: 11.9–23.3 [12]).
Since Study 1108 employed a single-arm design, there is a need to demonstrate effectiveness, especially with respect to OS, of comparator therapeutic agents. The purpose of this study was to provide an indirect treatment comparison to the second-line chemotherapy regimens utilized for this patient population within the real-world database provided by Flatiron Health [13], an electronic medical record database containing patient data from oncology clinics.
Methods
Study design & data sources
This was a retrospective indirect treatment comparison of OS between patients in the Flatiron database with advanced or metastatic UC who failed at least one platinum-based therapy prior to starting second-line chemotherapy (Flatiron group) and advanced/metastatic UC patients from Study 1108 who received durvalumab monotherapy as second-line treatment (durvalumab group) to estimate the treatment effect of durvalumab.
Study 1108 was a Phase I/II, open-label, single-arm trial designed to provide evidence on the clinical benefit of durvalumab for locally advanced or metastatic UC [11]. Eligible patients were at least 18 years of age, had histologically or cytologically confirmed locally advanced or metastatic UC, an Eastern Cooperative Oncology Group (ECOG) performance status score of 0 or 1, adequate organ and hematologic functions, fresh tumor biopsy and/or archival tumor tissue available for PD-L1 testing. Patients were excluded if they had a history of immunodeficiency, medical conditions that required systemic immunosuppression, history of severe immune-mediated adverse reactions, untreated central nervous system metastases or human immunodeficiency virus, active tuberculosis or hepatitis B or hepatitis C infection.
Flatiron Health’s database contains processed longitudinal patient-level electronic medical record data, including patient demographics, diagnosis information (e.g., staging, histopathology and biomarkers), treatment and outcomes (e.g., mortality). The Flatiron cohort inclusion criteria were as similar as possible to the Study 1108 inclusion criteria, within the limits of real-world databases; they included the following:
•
Diagnosed with UC (International Classification of Diseases, Ninth Revision [ICD-9] 188x, 189.1, 189.2, 189.3, or International Classification of Diseases, 10th Revision [ICD-10] C65x, C66x, C67x, C68.0);
•
At least two documented clinical visits on or after 1 January 2011;
•
Pathology consistent with transitional cell (urothelial) carcinoma of the bladder;
•
Diagnosed with stage IV UC on or after 1 January 2011, or diagnosed with early stage UC and subsequently developed advanced disease on or after 1 January 2011;
•
Patients with prior systemic therapy including at least one platinum agent, who went on to receive a second line of systemic therapy no later than 30 June 2017 (6 months prior to database cutoff on 31 December 2017);
•
Patients with ECOG performance status of 0 or 1; patients with missing performance scores were excluded from the study; although, in a sensitivity analysis, patients with missing ECOG scores were included.
Patients in the Flatiron dataset were excluded if they had any of the following: histology other than transitional cell (urothelial) carcinoma, primary site of disease other than bladder, renal pelvis, ureter or urethra, lacked relevant unstructured documents in the Flatiron database that enable establishing UC status, or received treatment with any immunotherapy agents.
The Flatiron database contains data from oncology clinics in USA, while Study 1108 was conducted in USA, Belgium, Canada, France, Germany, Italy, Korea, Republic of Taiwan and the UK. Flatiron data from January 2011 to December 2017, and Study 1108 data from August 2014 to October 2017, were used in the analyses.
Exposure & baseline characteristics
In contrast to the Study 1108 UC trial population, who received treatment exclusively with durvalumab monotherapy in second line or higher, the Flatiron dataset represents patients treated with physicians’ choice of treatment post-first line including gemcitabine/cisplatin; methotrexate, vinblastine, doxorubicin and cisplatin, and gemcitabine/carboplatin for chemotherapy. Patients in the Flatiron dataset treated with any IO agent were not included in the analysis.
Baseline characteristics were selected based on their availability in both data sources and included gender, race, cancer site, cancer stage at diagnosis and each of the following at treatment start: age, body mass index (BMI), smoking status and ECOG performance score.
Outcomes
The study end point was OS. For Study 1108, OS was defined as the time between the date of first dose of durvalumab to the maximum of the last recorded date on which the patient was known to be alive or the date of death, where data are censored for patients without a known date of death. For Flatiron, OS was defined as the time between the start of second-line treatment to maximum of last visit date or the recorded death date, again censoring for patients without a known date of death. In the Flatiron database, only month and year of death are recorded; the precise day of death is not provided to protect patients’ privacy. The last day of the month was used to slightly overestimate OS for the comparator arm, being conservative for durvalumab.
Adjustment by Cohort balancing
In observational studies, propensity score (PS) methods are commonly used to obtain treatment and comparator groups whose demographic and clinical characteristics do not differ [14]. The PS is the conditional probability that each patient would receive treatment given their baseline characteristics. We estimated the PS (probability of receiving durvalumab) for each patient using a logistic regression model with treatment status (receipt of durvalumab) as the outcome and available baseline characteristics as predictors. Predictors in the PS model included age (centered at the mean age of all patients included in the analysis), square of centered age, sex (female vs male), BMI (kg/m2), smoking status (ever smoker vs never smoked), primary cancer site (renal pelvis vs other) and ECOG performance status at baseline (1 vs 0). Each patient in the durvalumab group was matched to one patient in the Flatiron group using a nearest neighbor method with a maximum difference (caliper) of 0.2-times the standard deviation of the logit of the PS [15]. Standardized differences between the means of continuous variables and proportions of categorical variables of the two groups were calculated before and after matching to assess the balance of covariate distributions between the two groups. Standardized differences of each covariate between the durvalumab and the comparison group were calculated by dividing the difference in mean values by the square root of the average sample variances:
Analysis of overall survival
Median OS time of the matched cohorts was summarized by treatment group. OS was analyzed by fitting an intention-to-treat Cox proportional hazards model on the PS-matched dataset, with durvalumab treatment status as the only predictor. The assumption of proportional hazards (PH) was tested for the treatment group indicator based on visual inspection of a plot of the log cumulative hazard curves by log of time and by assessment of Schoenfeld residuals. Because the PH assumption was violated, the Cox model was extended to include an interaction between treatment and a time-period indicator selected to reflect the changes in effect observed in the PH test. The effect of treatment was estimated as the hazard ratio (HR) obtained from the fitted Cox model and the associated 95% CI. Data management and analyses were conducted using SAS version 9.4 (NC, USA), and Stata version 13.0 (TX, USA). Statistical tests were two-sided with a significance level of 0.05.
PD-L1-stratified analysis
In Study 1108, high versus low/negative PD-L1 expression was defined as expression on ≥25% tumor cells (TC) or immune cells (IC) versus <25% TC and <25% IC, respectively. PD-L1 status was generally unavailable for the Flatiron cohort, making PD-L1 subgroups impracticable. Therefore, in the subgroup analysis, separate PS models were constructed to match high and low/negative PD-L1 subgroups from Study 1108 with all comers in Flatiron, where the PS model was based on other patient characteristics but not on PD-L1 status.
Sensitivity analyses
Many patients in Flatiron had no ECOG status available. To assess whether the exclusion of patients with missing ECOG scores may have biased the study findings, a sensitivity analysis was conducted adding these patients into the eligible Flatiron cohort. A new PS matching process was conducted, leaving out ECOG status in the estimation of PS, and the OS analyses were rerun.
Additionally, because the Flatiron database contains data only for patients in USA, while Study 1108 recruited from several countries, a sensitivity analysis removed patients from the durvalumab cohort from outside of USA. A new PS matching procedure was conducted, and the OS analyses run again.
Results
Primary analysis
For the primary analysis cohort, the durvalumab group included 181 patients and the chemotherapy group included 200 patients. Following PS matching, 158 patients from each group were retained. The baseline characteristics and standardized differences between the two groups before and after matching are presented in Table 1 [16]. Baseline variables were well balanced between groups after matching except race and stage at diagnosis.
| Variable | Durvalumab | Chemo | Std diff†, ‡ | Durvalumab | Chemo | Std diff† |
|---|---|---|---|---|---|---|
| Sample size | 181 | 200 | 158 | 158 | ||
| Age (y)§ | 66.3 (9.5) 67 (60–73) | 70.0 (9.1) 71 (64–78) | 0.396 | 66.9 (9.1) 68 (34–88) | 68.4 (8.9) 68 (63–76) | 0.168 |
| Sex (female)§ | 47 (26.0) | 53 (26.5) | 0.012 | 40 (25.3) | 44 (27.8) | 0.057 |
| Smoking status (ever vs never)§ | 102 (56.4) | 152 (76.0) | 0.425 | 98 (62.0) | 112 (70.9) | 0.189 |
| Stage 0‡, ¶ | 8 (4.4%) | 2 (1.0%) | 0.212 | 7 (4.4%) | 2 (1.3%) | 0.191 |
| Stage I‡, ¶ | 24 (13.3%) | 4 (2.0%) | 0.434 | 18 (11.4%) | 3 (1.9%) | 0.388 |
| Stage II‡, ¶ | 21 (11.6%) | 2 (1.0%) | 0.447 | 20 (12.7%) | 1 (0.6%) | 0.498 |
| Stage III‡, ¶ | 19 (10.5%) | 10 (5.0%) | 0.207 | 17 (10.8%) | 9 (5.7%) | 0.185 |
| Stage IV‡, ¶ | 94 (51.9%) | 91 (45.5%) | 0.129 | 85 (53.8%) | 78 (49.4%) | 0.089 |
| Stage unknown‡, ¶ | 15 (8.3%) | 91 (45.5%) | 0.925 | 11(7.0%) | 65 (41.1%) | 0.872 |
| Cancer site: renal pelvis¶ | 24 (13.3%) | 29 (14.5%) | 0.036 | 22 (13.9%) | 24 (15.2%) | 0.036 |
| Height (cm)‡, § | 170.7 (10.1) 172.0 (163.5–177.9) | 172.0 (9.7) 172.7 (165.1–180.3) | 0.125 | 170.4 (10.1) 171.4 (142.0–194.7) | 172.1 (10.0) 172.7 (149.9–193.0) | 0.174 |
| Weight (kg)‡, § | 76.5 (16.3) 74.0 (65.2–86.2) | 80.0 (17.8) 78.8 (68.7–89.4) | 0.209 | 76.4 (16.3) 74.0 (39.8–130.5) | 78.5 (17.5) 78.0 (38.9–151.2) | 0.122 |
| BMI (kg/m2)§ | 26.1 (4.5) 26.1 (23.2–28.9) | 26.9 (5.1) 26.5 (23.6–29.9) | 0.174 | 26.2 (4.4) 26.2 (16.2–41.1) | 26.3 (4.8) 25.8 (16.8–49.9) | 0.033 |
| Race¶: | ||||||
| – White† | 112 (61.9%) | 159 (79.5%) | 0.395 | 95 (60.1%) | 127 (80.4%) | 0.454 |
| – Asian† | 40 (22.1%) | 3 (1.5%) | 0.674 | 37 (23.4%) | 3 (1.9%) | 0.684 |
| – African American† | 5 (2.8%) | 4 (2.0%) | 0.050 | 4 (2.5%) | 3 (1.9%) | 0.043 |
| – Other† | 5 (2.8%) | 13 (6.5%) | 0.179 | 5 (3.2%) | 9 (5.7%) | 0.123 |
| – Unknown† | 18 (9.9%) | 21 (10.5%) | 0.018 | 16 (10.1%) | 16 (10.1%) | 0.000 |
| – Multiple† | 1 (0.6%) | 0 (0.0%) | 0.105 | 1 (0.6%) | 0 (0.0%) | 0.113 |
| ECOG 0¶ | 58 (32.0%) | 69 (34.5%) | 0.052 | 49 (31.0%) | 53 (33.5%) | 0.054 |
| ECOG 1¶ | 123 (68.0%) | 131 (65.5%) | 0.052 | 109 (69.0%) | 105 (66.5%) | 0.054 |
†
A standardized difference smaller than 0.25 [16] was considered to be an indication of balance between the two groups on that covariate.
‡
Variable was not included in the propensity score model.
§
Mean (SD), median, max–min.
¶
n (%).
BMI: Body mass index; ECOG: Eastern Cooperative Oncology Group; SD: Standard deviation; Std diff: Standardized difference.
In the matched groups, durvalumab demonstrated a statistically significant improvement in OS versus chemotherapy (HR: 0.63; 95% CI: 0.48–0.84) (Table 2).
| Variable | Model 1†, HR for OS (95% CI) | Model 2‡, HR for OS (95% CI) | Model 3§, HR for OS (95% CI) |
|---|---|---|---|
| Durvalumab | 0.63 (0.48–0.84); p < 0.001 | – | – |
| Durvalumab (0–5 months) | – | 1.22 (0.81–1.83); p = 0.33 | 1.30 (0.83–2.02); p = 0.25 |
| Durvalumab (>5 months) | – | 0.29 (0.16–0.52); p < 0.001 | 0.29 (0.16–0.51); p < 0.001 |
| Race (reference = white): | |||
| – Asian | – | – | 0.61 (0.32–1.16); p = 0.13 |
| – African American | – | – | 1.11 (0.45–2.72); p = 0.83 |
| – Other | – | – | 0.93 (0.47–1.84); p = 0.84 |
| – Unknown | – | – | 1.09 (0.68–1.74); p = 0.73 |
| Stage at initial diagnosis (reference = 0): | |||
| – Stage I | – | – | 0.65 (0.25–1.69); p = 0.38 |
| – Stage II | – | – | 0.74 (0.27–2.00); p = 0.55 |
| – Stage III | – | – | 0.94 (0.36–2.27); p = 0.88 |
| – Stage IV | – | – | 0.93 (0.42–2.06); p = 0.85 |
| – Stage Unknown | – | – | 0.77 (0.33–1.79); p = 0.54 |
†
Model 1: Treatment indicator only.
‡
Model 2: Time-varying treatment indicator before and after 5 months.
§
Model 3: Time-varying treatment indicator before and after 5 months, adjusting for unbalanced baseline characteristics.
CI: Confidence interval; HR: Hazard ratio; OS: Overall survival.
The median OS in the durvalumab group was 11.2 (95% CI: 7.2–16.9) months compared with 8.2 (95% CI: 6.7–9.8) months in the matched chemotherapy patients (Table 3 & Figure 1).
| Analysis | Durvalumab (n, median OS [months], (95% CI)) | Chemotherapy (n, median OS [months], (95% CI)) |
|---|---|---|
| Primary analysis | n = 158, 11.2 (7.2–16.9) | n = 158, 8.2 (6.7–9.8) |
| Include missing ECOG status | n = 178, 10.6 (6.9–15.8) | n = 178, 7.6 (5.7–9.3) |
| US patients only | n = 82, 7.2 (3.6–20.1) | n = 82, 7.2 (5.5–8.9) |
CI: Confidence interval; ECOG: Eastern Cooperative Oncology Group; OS: Overall survival.
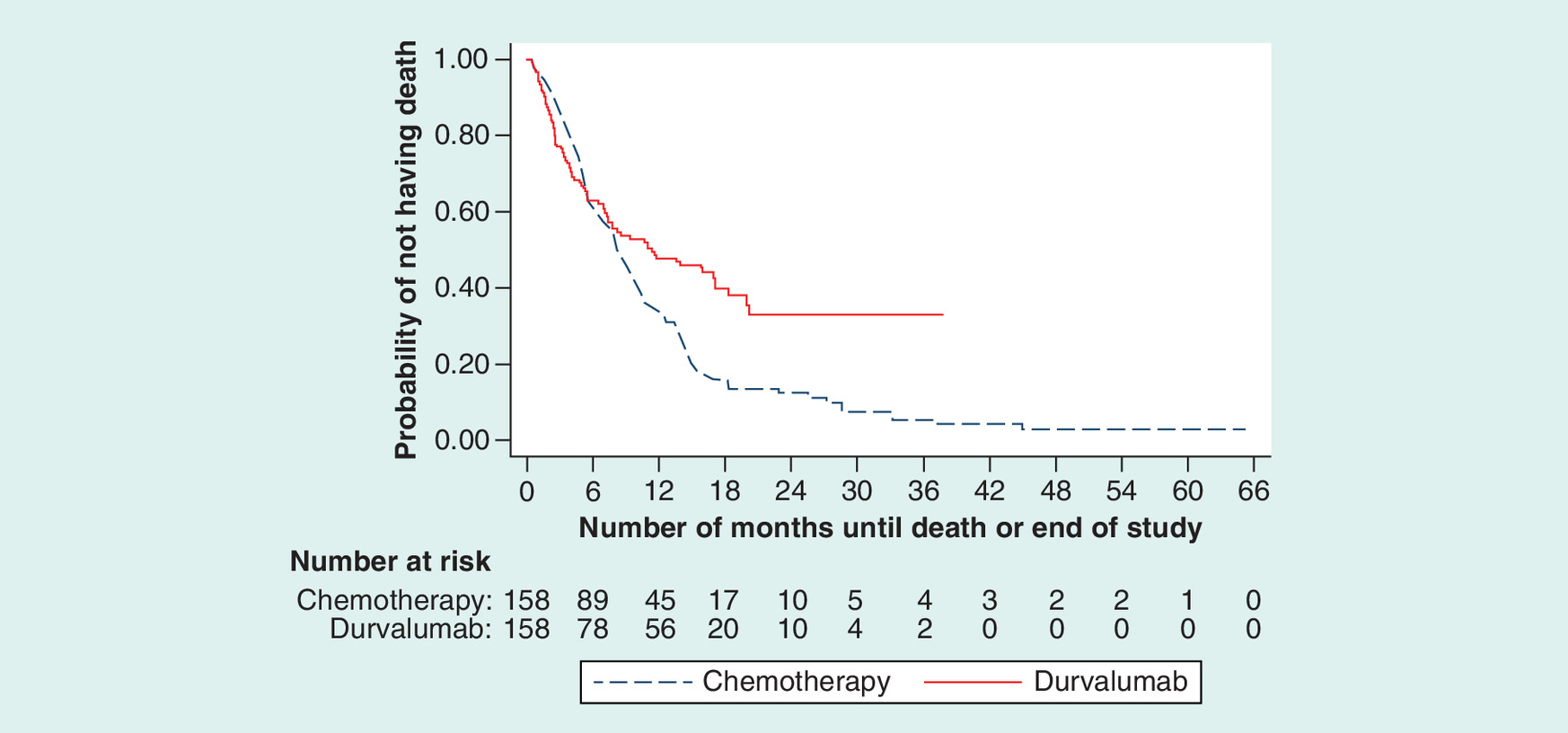
The PH assumption was violated as the Kaplan-Meier curves crossed at 5 months, by which time 48 patients (30.4%) had died in each group. Therefore, an extended Cox model was run with separate indicators for durvalumab treatment from 0 to 5 months and >5 months after the index date. In this model, the HR for durvalumab indicated no significant difference in risk in the first 5 months (p = 0.33); however, there was a 71% reduction in risk compared with chemotherapy after 5 months (HR: 0.29; 95% CI: 0.16–0.52, p < 0.001).
To examine the impact of the remaining imbalance in race and stage at diagnosis, an additional Cox model incorporated race and stage as covariates, in addition to the separate indicators of treatment by time and interactions of race/stage and treatment. The results of this model were virtually unchanged relative to the time-varying model without the covariates, suggesting that the treatment effect did not differ across race or stage.
PD-L1-stratified analysis
Among patients on durvalumab in Study 1108, 93 had high PD-L1 expression and 76 had low/negative PD-L1 expression. After matching these patients to all patients in Flatiron, 91 and 74 patients remained in the high and low/negative PD-L1 subgroups, respectively. OS was longer for durvalumab than chemotherapy in the PD-L1 high subgroup (HR: 0.43; 95% CI: 0.29–0.64, p < 0.0001), with median OS of 19.9 (95% CI: 11.6–NA) months for durvalumab and 7.8 (95% CI: 5.5–9.8) months for chemotherapy. In the low/negative PD-L1 subgroup, no significant difference was found for OS (HR: 0.99; 95% CI: 0.68–1.44, p = .95); the median OS in the durvalumab group was 4.9 (95% CI: 3.1–8.5) compared with 7.2 (95% CI: 5.1–8.9) months for matched chemotherapy patients.
Sensitivity analyses
The Flatiron database included 456 eligible patients when the requirement of a known ECOG score was removed. In the new PS matching, an additional 20 patients per group were successfully matched compared with the primary analysis cohort, for a total of 178 patients in each treatment group. In this larger cohort, the HR for OS with durvalumab versus chemotherapy was similar to the primary analysis (HR: 0.64; 95% CI: 0.50–0.84, p = 0.001) (Table 4). Median OS was 10.6 (95% CI: 6.9–15.8) months for durvalumab and 7.6 (95% CI: 5.7–9.3) months for chemotherapy (Table 3).
| Analysis | Model 1†, HR for OS (95% CI) | Model 2‡, HR for OS (95% CI) |
|---|---|---|
| Include missing ECOG status (n = 178 for each group) | ||
| Durvalumab | 0.64 (0.50–0.84); p = 0.001 | – |
| Durvalumab (0–5 months) | – | 1.06 (0.75–1.51); p = 0.73 |
| Durvalumab (>5 months) | – | 0.37 (0.25–0.55); p < 0.001 |
| US patients only (n = 82 for each group) | ||
| Durvalumab | 0.65 (0.45–0.95); p = 0.02 | – |
| Durvalumab (0–5 months) | – | 1.60 (0.97–2.64); p = 0.06 |
| Durvalumab (>5 months) | – | 0.19 (0.1–0.37); p < 0.001 |
†
Model 1: Treatment indicator only.
‡
Model 2: Time-varying treatment indicator before and after 5 months.
CI: Confidence interval; ECOG: Eastern Cooperative Oncology Group; HR: Hazard ratio; OS: Overall survival.
Restricting the Study 1108 group to patients in USA reduced the durvalumab group to 82 patients, all of whom were matched. The point estimate comparing OS in this smaller cohort was again very similar to those of the primary analysis (HR: 0.65; 95% CI: 0.45–0.95, p = 0.02) (Table 4), although the median OS did not differ between groups, at 7.2 (95% CI: 3.6–20.1) months for durvalumab and 7.2 (95% CI: 5.5–8.9) months for chemotherapy (Table 3).
Discussion
This indirect comparison between patients with advanced/metastatic UC from a durvalumab clinical trial and real-world patients treated with physician’s choice of second-line chemotherapy, matched on baseline characteristics, suggests that OS may be longer with durvalumab than with chemotherapy. The estimated effect sizes were statistically significant and clinically meaningful (i.e., <0.85) [17].
Our findings suggest that the survival benefit with durvalumab treatment may not be immediate, but rather may only appear approximately 5 months after treatment initiation. Results in the primary cohort showed nonsignificantly lower survival in the durvalumab cohort during the first 5 months, followed by a substantial (71%) reduction in risk with durvalumab after that point. A delayed treatment effect is commonly observed in immunotherapies [18]. The increased immune and antitumor response can take several months to improve survival [19], therefore, statistical methods that account for the delay are better suited to evaluate the treatment effect. The Cox regression model that allows for a different treatment effect after 5 months better captured the separation of survival curves after the overlap in the first 5 months and did not make the assumption that hazard rates are proportional from the start of therapy.
The effectiveness of durvalumab treatment appeared greater in the subgroup of patients with high PD-L1 expression. However, these results are subject to high uncertainty because of high missingness of PD-L1 status from the Flatiron database and need to be interpreted with caution. Randomized, stratified trials are ongoing [20] that will further examine the relationship between PD-L1 expression and survival in patients treated with durvalumab versus chemotherapy with known PD-L1 values.
There is no clear association between PD-L1 status and OS in patients with UC in the post-platinum setting. A review of efficacy of immune checkpoint inhibitors in the post-platinum UC setting reported that while PD-L1 positivity was associated with higher OS in a previously platinum-treated cohort of the IMvigor210 trial, it was not associated with OS in the larger randomized Phase III KEYNOTE-045 trial [21]. Results of the clinical trials of the five IO agents in the second-line setting suggest that significant ORR is observed across a range of thresholds for PD-L1 positivity [22]. A meta-analysis of 11 studies on the efficacy of PD-1 or PD-L1 inhibitors for treatment of melanoma (two trials), non-small-cell lung carcinoma (six trials), UC (one trial), head and neck cancer (one trial) and renal cell carcinoma (one trial) reported that patients with PD-L1–positive tumors had OS benefits from the PD-1/PD-L1 inhibitors regardless of PD-L1 expression level, with higher levels of PD-L1 expression showing higher OS benefits [23]. It should be noted that the meta-analysis was based on a small number of clinical trials, only one of which included patients with UC.
Because real-world oncology clinic data contain ECOG performance scores for only a subset of patients, which could represent a biased sample of all advanced/metastatic patients with UC treated with second-line chemotherapy, it was important to examine survival among a more general population of otherwise-eligible patients. The high consistency between the findings of the primary analysis and those of the sensitivity analysis adding Flatiron patients with missing ECOG data provides reassurance that the primary results are not reflecting any selection bias generated by the requirement of a recorded ECOG score.
The comparison between patients in Study 1108, who resided in any of several different countries, and those from Flatiron, who were all based in USA, creates another concern regarding potential bias, as there may be many differences between patients with UC in different countries that could potentially impact the study findings, such as different standards and quality of care. Restricting Study 1108 patients to those from USA reduced the sample size by nearly half. Despite the decrease in statistical power, the overall durvalumab treatment effect still demonstrated a significant advantage over chemotherapy, with a similar effect size to the primary analysis. Median survival duration, however, appeared the same in the durvalumab and chemotherapy groups, as result of the delayed effect of durvalumab but also suggesting some attenuation of the effect in this limited subgroup.
Limitations
There are several limitations to this analysis that should be noted. The Flatiron dataset is derived from real-world oncology practices that reflect community practice settings and hence it differs in many respects from clinical trial data. First, patients who enroll in clinical trials may differ from those treated in clinical practice, and they typically have better outcomes than patients treated in a real-world setting. Although obtaining both patient groups from the same source would be preferable, the number of patients on durvalumab in the Flatiron database at the time of data extraction was too low to permit analyses. Second, in the real-world setting, care is provided in a variety of ways decided upon by the physician and patient, rather than in the protocol-driven approach used in trials. Third, some of the information available in Study 1108 that may be important for fully balancing the groups is not consistently recorded in the real-world electronic health records. The missing information includes PD-L1 status, which could not be included for the chemotherapy patients in the stratified PD-L1 analysis, and comorbidities, which may impact survival. The PS methodology employed is designed to reduce confounding by indication. Two of the examined variables (race and stage) were not able to be balanced successfully, although analyses adding the unbalanced variables as covariates in the outcome models showed no sign of residual confounding from those factors. However, other baseline differences may have existed between patients. Thus, the potential for residual confounding due to unobserved characteristics remains.
Conclusion
Using a propensity score-matched analysis, we found that durvalumab is associated with a statistically significant improvement in OS when compared with physician’s choice of second-line chemotherapy for patients with locally advanced or metastatic UC. The treatment effect of durvalumab is more likely to translate into improved survival after 5 months. Our findings were robust to differences in race and stage at diagnosis across the two treatment groups, regional variation of patient groups and missing ECOG status. The comparative efficacy of durvalumab remains to be established in a randomized, PD-L1-stratified trial [20].
•
Platinum-based chemotherapy has been the standard of care for the treatment of metastatic urothelial carcinoma (mUC).
•
Since 2016, immunotherapies approved for the second-line treatment of mUC have improved the prognosis relative to platinum-based chemotherapy.
•
Durvalumab, a PD-L1 antibody, was approved in USA for the treatment of mUC following platinum-based chemotherapy based on the results of a single-arm, Phase I/II, open-label study (Study 1108; NCT01693562).
•
The present study was conducted in order to the compare overall survival (OS) of patients from Study 1108 who received durvalumab after platinum-based chemotherapy with an observational cohort of patients treated with chemotherapy.
•
In an indirect treatment comparison, patients from Study 1108 were matched to patients with mUC from the Flatiron oncology electronic medical record database who received physician’s choice of second-line chemotherapy.
•
Flatiron data from January 2011 to December 2017, and Study 1108 data from August 2014 to October 2017, were used in the analyses.
•
We estimated the propensity score (probability of receiving durvalumab) for each patient using a logistic regression model with treatment status (receipt of durvalumab) as the outcome and available baseline characteristics as predictors.
•
After matching, 158 patients from each cohort were retained with good balance on baseline characteristics except race and stage at diagnosis. OS was analyzed by fitting an intention-to-treat Cox proportional hazards model on the propensity score-matched dataset, with durvalumab treatment status as the only predictor.
•
Median OS estimated by the Cox model was 11.2 months (95% CI: 7.2–16.9) versus 8.2 months (95% CI: 6.7–9.8) for the durvalumab and chemotherapy groups, respectively (hazard ratio: 0.63; 95% CI: 0.48–0.84). Adjustment for race and stage at diagnosis did not meaningfully change the results.
•
The OS benefit of durvalumab appears more pronounced several months after the initiation of second-line therapy.
•
Our results provide evidence for the effectiveness of durvalumab compared with physician’s choice of chemotherapy as a second-line treatment for mUC.
Financial & competing interests disclosure
This study was funded by AstraZeneca. BL Nordstrom and M Oguz are employees of Evidera. BC Chu was an employee of Evidera at the time of conduct of this study (current affiliation is Gilead Sciences, Inc.). Evidera received funding from AstraZeneca for the study reported in this manuscript. M Ouwens and AB Klein are employees and shareholders of AstraZeneca. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Editorial assistance was provided by WA Pedersen and P Goodfriend of Parexel, funded by AstraZeneca.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest •• of considerable interest
1.
Fleshner NE, Herr HW, Stewart AK, Murphy GP, Mettlin C, Menck HR. The National Cancer Data Base report on bladder carcinoma. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer 78(7), 1505–1513 (1996).
2.
Powles T. Immunotherapy: the development of immunotherapy in urothelial bladder cancer. Nat. Rev. Clin. Oncol. 12(4), 193–194 (2015).
3.
American Cancer Society. Key Statistics for Bladder Cancer (2016). https://www.cancer.org/cancer/bladder-cancer/about/key-statistics.html
4.
Bellmunt J, Albiol S, Suarez C, Albanell J. Optimizing therapeutic strategies in advanced bladder cancer: update on chemotherapy and the role of targeted agents. Crit. Rev. Oncol. Hematol. 69(3), 211–222 (2009).
5.
Calabro F, Sternberg CN. State-of-the-art management of metastatic disease at initial presentation or recurrence. World J. Urol. 24(5), 543–556 (2006).
6.
Rosenberg JE, Von Der Maase H, Seigne JD et al. A Phase II trial of R115777, an oral farnesyl transferase inhibitor, in patients with advanced urothelial tract transitional cell carcinoma. Cancer 103(10), 2035–2041 (2005).
7.
Sengelov L, Kamby C, Geertsen P, Andersen LJ, Von Der Maase H. Predictive factors of response to cisplatin-based chemotherapy and the relation of response to survival in patients with metastatic urothelial cancer. Cancer Chemother. Pharmacol. 46(5), 357–364 (2000).
8.
Bellmunt J, Fougeray R, Rosenberg JE et al. Long-term survival results of a randomized Phase III trial of vinflunine plus best supportive care versus best supportive care alone in advanced urothelial carcinoma patients after failure of platinum-based chemotherapy. Ann. Oncol. 24(6), 1466–1472 (2013).
•• A Phase III study demonstrating the long-term survival of second-line chemotherapy for advanced urothelial carcinoma. The results of this study helped to establish an overall survival benchmark for second-line chemotherapy in this indication.
9.
Jiang DM, Sridhar SS. Prime time for immunotherapy in advanced urothelial cancer. Asia Pac. J. Clin. Oncol. 14(Suppl. 5), 24–32 (2018).
10.
Flaig TW, Pe Spiess PE, Agarwal N et al. NCCN Guidelines Insights: Bladder Cancer, Version 5 2018. J. Natl Compr. Canc. Netw. 16(9), 1041–1053 (2018).
11.
Powles T, O’donnell PH, Massard C et al. Efficacy and safety of durvalumab in locally advanced or metastatic urothelial carcinoma: updated results from a Phase I/II open-label study. JAMA Oncol. 3(9), e172411–e172411 (2017).
•• Phase I/II study that established the clinical benefit of durvalumab as a second-line therapy for locally advanced or metastatic urothelial carcinoma. Results of this study supported regulatory approval of durvalumab in this indication.
12.
Imfinzi (Durvalumab). [prescribing information] AstraZeneca Pharmaceuticals LP, DE, USA (2018).
13.
Flatiron Health. Flatiron Health Database (2019). https://flatiron.com/real-world-evidence/
14.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav. Res. 46(3), 399–424 (2011).
15.
Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 10(2), 150–161 (2011).
16.
Stuart EA. Matching methods for causal inference: a review and a look forward. Stat. Sci. 25(1), 1–21 (2010).
17.
Ellis LM, Bernstein DS, Voest EE et al. American Society of Clinical Oncology perspective: raising the bar for clinical trials by defining clinically meaningful outcomes. J. Clin. Oncol. 32(12), 1277–1280 (2014).
•• A summary of recommendations by four disease-specific working groups, convened by the ASCO Cancer Research Committee, to define clinically meaningful outcomes for clinical trials of solid tumors.
18.
Hoos A, Britten C. The immuno-oncology framework: enabling a new era of cancer therapy. Oncoimmunology 1(3), 334–339 (2012).
19.
Hoos A, Eggermont AMM, Janetzki S et al. Improved endpoints for cancer immunotherapy trials. J. Natl Cancer Inst. 102(18), 1388–1397 (2010).
• A review addressing the potential for a delayed separation in Kaplan–Meier survival curves with immunotherapy agents, and how this needs to be taken into account when evaluating these agents in clinical trials (including different statistical approaches).
20.
Powles T, Galsky MD, Castellano D et al. A Phase III study of first-line durvalumab (MEDI4736) ± tremelimumab versus standard of care (SoC) chemotherapy (CT) in patients (pts) with unresectable Stage IV urothelial bladder cancer (UBC): DANUBE. J. Clin. Oncol. 34(Suppl. 15), Abst TPS4574 (2016).
• Describes an ongoing Phase III study to evaluate the efficacy and safety of durvalumab, alone or in combination with an anti-CTLA-4 agent, in patients with previously untreated, metastatic urothelial carcinoma.
21.
Tripathi A, Plimack ER. Immunotherapy for urothelial carcinoma: current evidence and future directions. Curr. Urol. Rep. 19(12), 109 (2018).
22.
Stenehjem DD, Tran D, Nkrumah MA, Gupta S. PD1/PDL1 inhibitors for the treatment of advanced urothelial bladder cancer. Onco. Targets Ther. 11, 5973–5989 (2018).
23.
Weng YM, Peng M, Hu MX, Yao Y, Song QB. Clinical and molecular characteristics associated with the efficacy of PD-1/PD-L1 inhibitors for solid tumors: a meta-analysis. Onco. Targets Ther. 11, 7529–7542 (2018).
• Describes the findings of a meta-analysis to evaluate the clinical and molecular characteristics associated with overall survival outcomes with PD-1/PD-L1 inhibitors in solid tumors, including urothelial carcinoma.
Information & Authors
Information
Published In
Pages: 191 - 199
PubMed: 31916448
Copyright
© 2020 Beth L Nordstrom. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 1 November 2019
Accepted: 16 December 2019
Published online: 9 January 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Effectiveness of durvalumab versus chemotherapy in metastatic urothelial cancer: an observational, indirect comparison. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0163
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Lishi Lin, Merel J.J. Lucassen, Vincent van der Noort, Toine C.G. Egberts, Jos H. Beijnen, Alwin D.R. Huitema, The feasibility of using real world data as external control arms in oncology trials, Drug Discovery Today, 10.1016/j.drudis.2025.104324, 30, 3, (104324), (2025).
- Bernadett Szabados, Mariano Ponz-Sarvisé, Robson Machado, Diego Saldana, Edward E. Kadel, Romain Banchereau, Fanny Bouquet, Marius Garmhausen, Thomas Powles, Carsten Schröder, Clinico-Genomic Characterization of Patients with Metastatic Urothelial Carcinoma in Real-World Practice Identifies a Novel Bladder Immune Performance Index (BIPI), Clinical Cancer Research, 10.1158/1078-0432.CCR-22-0200, 28, 18, (4083-4091), (2022).
- Jiao Wei, Aimin Hui, Review of Ribosome Interactions with SARS-CoV-2 and COVID-19 mRNA Vaccine, Life, 10.3390/life12010057, 12, 1, (57), (2022).