Meta-analysis of short-term outcomes comparing robot-assisted and laparoscopic distal pancreatectomy
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To evaluate and compare the short-term outcomes of robotic surgery and laparoscopic approach in distal pancreatectomy (DP). Materials & methods: EMBASE, PubMed, the Cochrane Library, CNKI and Wan Fang database were retrieved from the inception of electronic databases to June 2019. All analyses were performed using Stata/SE 15.1 version (StataCorp). Results: Twenty-two papers were included, four of which were prospective studies and the rest were retrospective studies. There was significant difference in spleen preservation rate (odds ratio: 2.020; 95% CI: 1.085–3.758; p = 0.027), operation time (mean difference [MD]: 27.372; 95% CI: 8.236–47.210; p = 0.000), the length of hospital stay (MD: -0.911; 95% CI: -1.287 to -0.535; p = 0.000), conversion rate (rate difference: -0.090; 95% CI: -1.287 to -0.535; p = 0.000), operation cost (MD: 2816.564; 95% CI: 1782.028–3851.064; p = 0.000). However, no significant difference was detected in estimated blood loss, total complication, severe complication, lymph nodules harvest, blood transfusion rate, total pancreatic fistula, severe pancreatic fistula, R0 resection rate and mortality. Conclusion: Both robotic and laparoscopic DP are safe and feasible. Although robotic DP increases the operation cost, the spleen-preserving rate is much higher. Robotic surgery may be an alternative approach to DP.
Due to the complexity of the anatomical location and adjacency, distal pancreatectomy (DP) has already become one of the most challenging procedure in the abdomen, with perioperative mortality and complication rates of 2 and 30–40%, respectively [1–3]. Open DP (ODP) used to be the only choice for those patients who need DP. While Cuschieri [4] successfully applied laparoscopic surgery to DP for the first time in 1994, laparoscopic DP (LDP) has become the most widely used minimally invasive technique in pancreatic surgery. Thanks to the advance of technology, another minimally invasive technique, the robotic surgical system (Da Vinci System) was invented. Compared with ODP, minimally invasive pancreatectomy could evidently reduce intraoperative bleeding, improve spleen-preserving rate, reduce postoperative pain, accelerate postoperative recovery and shorten hospital stay [5,6]. A systematic review including 561 patients with ODP and 895 patients with LDP showed that laparoscopic resection could improve operative and postoperative outcomes [7]. Furthermore, LDP had the same rate of margin positive, lymph nodules harvested and overall survival as ODP [5,8,9]. Although achieving good clinical results, in the past 20 years, LDP also showed some limitations, such as 2D planar imaging, less freedom of movement of surgical instruments and long learning curve [10]. The emergence of robotic surgery system partly overcame the shortcomings of laparoscopic surgery through a 3D high-definition surgical view, tremor filtration and seven degrees-of-freedom manipulator arm [11–13]. Melvin et al. [14] performed the first DP with robotic surgical system in 2003. Some authors believed that compared with LDP, robotic DP (RDP) has less bleeding, lower conversion rate and higher rate of lymph node harvested and spleen preservation but has no significant differences in operation time and pancreatic fistula [4,15,16]. While other studies showed different tendencies in comparing LDP with RDP in terms of operation time, pancreatic fistula, blood loss and other outcome indicators [17,18]. Recently, a meta-analysis focusing on LDP and RDP pooled the results from studies with finite sample sizes. Therefore, we performed a more comprehensive meta-analysis concerning whether patients benefit more from RDP compared with LDP.
Materials & methods
The present study was completed according to the Preferred Reported Items for Systematic Reviews and Meta-Analyses guideline.
Literature & search strategy
Two independent researchers (Y-H Hu, Y-M Zhao) performed a systematic search of the electronic databases including EMBASE, PubMed, the Cochrane Library, CNKI and Wan Fang databases to identify randomized controlled trials (RCTs), retrospective controlled study (RCS) and prospective observational studies exploring the safety and efficacy of RDP and LDP from the inception of electronic databases to June 2019. We used a structured search strategy in combination with Boolean logic: (robotics OR robotic) AND (laparoscopy OR laparoscopic) AND (pancreatectomy OR pancreatectomies OR distal pancreatectomy). In addition, we checked the reference list of the studies to identify other trials that might potentially qualify for inclusion in the meta-analysis. The process was completed when no further studies could be determined. In case of more than one publication was available for a study, we used either the most recent publication or the one with the most relevant information.
Inclusion & exclusion criteria
If the literatures met the following criteria in accordance with PICOS, the literature was considered to be included in the present meta-analysis. Population: patients underwent surgeries for lesions in the body or tail of the pancreas; Intervention: patients who received RDP; Comparison intervention: LDP or RDP; Outcome measures: operation time, the length of hospital stay, spleen preservation rate, pancreatic fistula, estimated blood loss, conversion rate, lymph nodules harvest, operation time, blood transfusion rate, operation cost and mortality; Study design: RCTs or RCS. Exclusion criteria: abstracts, letters, editorials and expert opinions, case reports; noncomparative studies; insufficient data and unexplained results and parameters; the scores of Newcastle–Ottawa scale (NOS) <6 [19]; inadequate raw data. Diagnostic criteria for pancreatic leakage: the drainage volume of anastomotic or pancreatic residual fluid was more than 10 ml per day on the 3rd day or later after operation, and the concentration of amylase in drainage fluid was three-times higher than the upper limit of normal plasma amylase and lasted for more than 3 days [20]. Class B and Class C fistulas are thought to be severe pancreatic fistulas according to the criteria of the International Study Group on Pancreatic Surgery. Complications of grade III and IV are considered serious complications after abdominal surgery according to the Clavien–Dindo classification system [21].
Data extraction & outcome measures
We created an electronic data extraction spreadsheet that consisted of the following information: general trial parameters, demographic characteristics, diagnostic measurements, treatment regimens and outcomes. Two independent authors conducted data collection and disagreements were settled by discussion. Intraoperative outcome measures: operation time, estimated blood loss, spleen preservation rate, pancreatic fistula, lymph nodules harvest, blood transfusion rate, conversion rate and operation cost. Postoperative outcome measures: the length of hospital stay, pancreatic fistula, complication and mortality.
Quality assessment & statistical analysis
Two independent authors evaluated the methodological quality of the included RCTs and RCS, respectively, using the NOS. Evidence quality assessment using GRADEpro software Version 3.6 (https://community.cochrane.org/help/tools-and-software/gradepro-gdt). The results of continuous data (operation time, estimated blood loss, lymph nodules harvest, operation cost and the length of hospital stay) were calculated as the mean difference (MD) with 95% CIs. For dichotomous outcome variables (spleen preservation rate, pancreatic fistula, blood transfusion rate, conversion rate, complication and mortality), we used an odds ratio (OR) or rate difference (RD) with 95% CIs. All analyses were performed using Stata/SE 15.1 version (StataCorp). If there was proof of significant heterogeneity (I2 >50%), random-effects models were used. If not, fixed-effects models were used for analysis in accordance with the Cochrane Handbook for systematic reviews of Interventions (Version 5.1.0, https://training.cochrane.org/handbook). If p-value was <0.05, the difference was considered as statistically significant.
Results
Search results
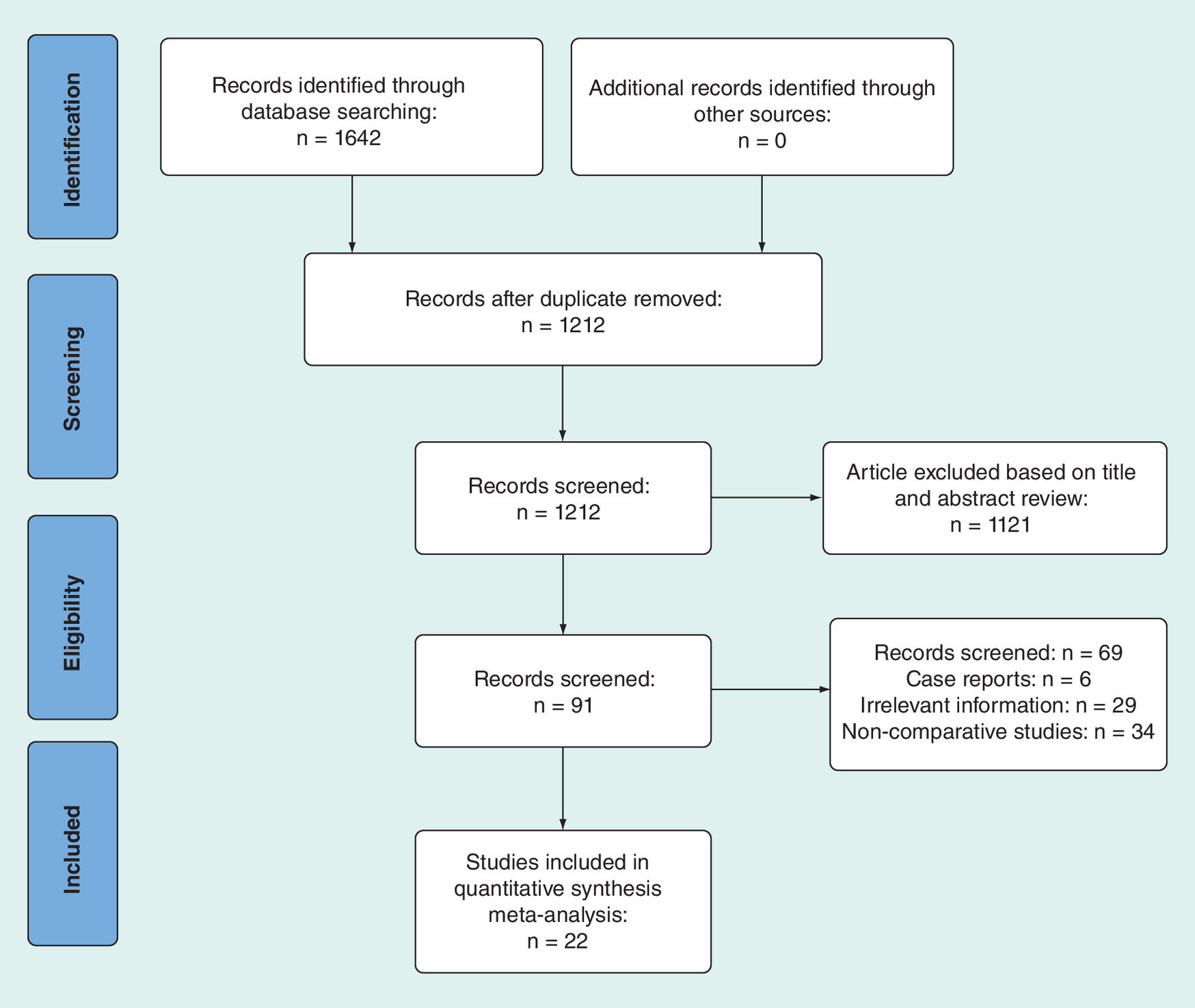
According to the proposed retrieval strategy and method, 1642 research articles were retrieved. Four hundred and thirty duplicated articles are deleted. 1121 papers were removed by reading titles and abstracts; the full text was read and the nonconforming papers were deleted; the full text was re-read and screened according to inclusion criteria, exclusion criteria and data integrity. Finally, 22 [22–43] papers were included, four of which are prospective studies and the rest were retrospective studies. The specific screening process is shown in the Figure 1.
Characteristics of included studies
We summarized the characteristics of the 22 included studies as follows: 3298 individuals were incorporated into our trial of whom 2519 cases underwent an LDP and 779 cases underwent RDP. The general trial parameters, demographic characteristics, are shown in Table 1.
| Study | Year | Country | Study design | Study group | Gender | Age | |||
|---|---|---|---|---|---|---|---|---|---|
| RDP | LDP | RDP (M/F) | LDP (M/F) | RDP | LDP | ||||
| Goh et al. | 2016 | Singapore | Retrospective | 8 | 31 | 2/6 | 18/13 | NA | NA |
| Eckhardt et al. | 2015 | Germany | Retrospective | 12 | 29 | 4/8 | 12/17 | 48.5 (29–76) | 59 (17–85) |
| Lee et al. | 2016 | China | Retrospective | 18 | 6 | 9/9 | 3/3 | 58 (39–80) | 54.5 (23–80) |
| Deng et al. | 2015 | China | Retrospective | 12 | 22 | 3/9 | 6/16 | 46.5 ± 16.08 | 48.5 ± 14.8 |
| Adam et al. | 2015 | USA | Retrospective | 61 | 474 | 28/33 | 248/226 | 65 ± 14 | 64 ± 13 |
| Ryan et al. | 2015 | USA | Prospective | 18 | 16 | 9/9 | 6/10 | 67 ± 12.5 | 60 ± 17 |
| Lee et al. | 2015 | USA | Retrospective | 37 | 131 | 10/27 | 57/74 | 58 ± 11.1 | 58 ± 15.0 |
| Lai and Tang | 2015 | China | Retrospective | 17 | 18 | 10/7 | 4/14 | 61.2 ± 10.4 | 63.2 ± 17.9 |
| Chen et al. | 2015 | China | Retrospective | 69 | 50 | 23/46 | 18/32 | 56.2 ± 13.3 | 56.5 ± 15.0 |
| Butturini et al. | 2015 | Italy | Prospective | 22 | 21 | 5/17 | 6/15 | NA | NA |
| Benizri et al. | 2014 | France | Retrospective | 11 | 23 | 3/8 | 10/13 | 50.1 ± 21.1 | 52.3 ± 14.7 |
| Duran et al. | 2014 | Spain | Retrospective | 16 | 18 | 9/7 | 9/9 | 61 ± 11.6 | 58.3 ± 10.0 |
| Daouadi et al. | 2013 | USA | Retrospective | 30 | 94 | 10/20 | 33/61 | 59 ± 13 | 59 ± 16 |
| Kang et al. | 2010 | Korea | Retrospective | 20 | 25 | 8/12 | 11/14 | 44.5 ± 15.9 | 56.5 ± 13.9 |
| Waters et al. | 2010 | USA | Prospective | 17 | 18 | 6/11 | 9/9 | NA | NA |
| Balzano et al. | 2014 | Italy | Retrospective | 31 | 140 | NA | NA | NA | NA |
| Ito et al. | 2014 | Japan | Retrospective | 4 | 10 | NA | NA | 52.7 | 68.0 |
| Lin et al. | 2019 | China | Retrospective | 41 | 41 | 14/27 | 15/29 | 45.2 ± 16.4 | 47.4 ± 14.9 |
| Souche et al. | 2018 | France | Prospective | 15 | 23 | 3/12 | 9/14 | 57 (34–72) | 66 (44–83) |
| Raoof et al. | 2018 | USA | Retrospective | 99 | 605 | 45/54 | 322/283 | NA | NA |
| Zhan et al. | 2013 | China | Retrospective | 21 | 30 | 5/16 | 11/19 | 52.2 ± 9.2 | 44.0 ± 16.8 |
| Xourafas et al. | 2017 | USA | Retrospective | 200 | 694 | 83/117 | 275/419 | 62 (22–88) | 62 (19–89) |
F: Female; LDP: Laparoscopic distal pancreatectomy; M: Male; NA: Not available; RDP: Robotic distal pancreatectomy.
Study quality & risk of bias
The quality of the included studies was evaluated by the scale of NOS. The details are showed in Table 2. NOS scores for all studies were greater than 7.
| Study | Year | Selection | Comparability | Exposure | Total |
|---|---|---|---|---|---|
| Goh et al. | 2016 | 4 | 2 | 3 | 9 |
| Eckhardt et al. | 2015 | 4 | 2 | 2 | 8 |
| Lee et al. | 2016 | 3 | 1 | 3 | 7 |
| Deng et al. | 2015 | 3 | 2 | 2 | 7 |
| Adam et al. | 2015 | 4 | 2 | 2 | 8 |
| Ryan et al. | 2015 | 3 | 2 | 2 | 7 |
| Lee et al. | 2015 | 4 | 2 | 2 | 8 |
| Lai and Tang | 2015 | 4 | 2 | 3 | 9 |
| Chen et al. | 2015 | 4 | 2 | 3 | 9 |
| Butturini et al. | 2015 | 3 | 2 | 3 | 8 |
| Benizri et al. | 2014 | 4 | 2 | 3 | 9 |
| Duran et al. | 2014 | 3 | 2 | 2 | 7 |
| Daouadi et al. | 2013 | 4 | 2 | 2 | 8 |
| Kang et al. | 2010 | 3 | 2 | 3 | 8 |
| Waters et al. | 2010 | 3 | 2 | 3 | 8 |
| Balzano et al. | 2014 | 4 | 0 | 3 | 7 |
| Ito et al. | 2014 | 4 | 1 | 3 | 8 |
| Lin et al. | 2019 | 4 | 2 | 2 | 8 |
| Souche et al. | 2018 | 3 | 2 | 2 | 4 |
| Raoof et al. | 2018 | 4 | 1 | 3 | 8 |
| Zhan et al. | 2013 | 3 | 2 | 2 | 7 |
| Xourafas et al. | 2017 | 3 | 2 | 2 | 7 |
Methodological quality assessment
Table 3 indicated that the total qualities of the evidence were low for the spleen preservation rate, total pancreatic fistula, total complication, estimated blood loss and operation time.
| Robotic distal pancreatectomy compared with laparoscopy distal pancreatectomy | ||||||
|---|---|---|---|---|---|---|
| Patient or population: patients with distal pancreatectomy Settings: robotic distal pancreatectomy Intervention: laparoscopy distal pancreatectomy | ||||||
| Outcomes | Illustrative comparative risks† (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | New comparison | |||||
| Spleen preservation rate | Study population | OR: 2.06 (1.07–3.98) | 1940 (16 studies) | ⊕⊕⊝⊝ low | ||
| 184 per 1000 | 317 per 1000 (194–472) | |||||
| Moderate | ||||||
| 260 per 1000 | 420 per 1000 (273–583) | |||||
| Total pancreatic fistula | Study population | OR: 1.09 (0.84–1.4) | 1777 (17 studies) | ⊕⊕⊝⊝ low | ||
| 226 per 1000 | 241 per 1000 (197–290) | |||||
| Moderate | ||||||
| 320 per 1000 | 339 per 1000 (283–397) | |||||
| Total complication | Study population | OR: 0.88 (0.72–1.09) | 2034 (17 studies) | ⊕⊕⊝⊝ low | ||
| 417 per 1000 | 387 per 1000 (340–438) | |||||
| Moderate | ||||||
| 478 per 1000 | 446 per 1000 (397–500) | |||||
| Estimated blood loss | The mean estimated blood loss in the intervention groups was 36.25 lower (79.44 lower to 6.95 higher) | 1071 (17 studies) | ⊕⊕⊝⊝ low | |||
| Operation time | The mean operation time in the intervention groups was 27.74 higher (8.31–47.17 higher) | 2008 (19 studies) | ⊕⊕⊝⊝ low | |||
†
The basis for the assumed risk (e.g., the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
GRADE Working Group grades of evidence.
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
OR: Odds ratio.
Outcomes of meta-analysis
Spleen preservation rate
The spleen preservation rates of RDP and LDP were compared in 16 literatures. Meta-analysis showed that there was significant heterogeneity (I2 = 73.4%; p = 0.000) and the results of the random effect model showed that the RDP group had higher spleen-preserving rate (OR: 2.020; 95% CI: 1.085–3.758; p = 0.027; Figure 2).
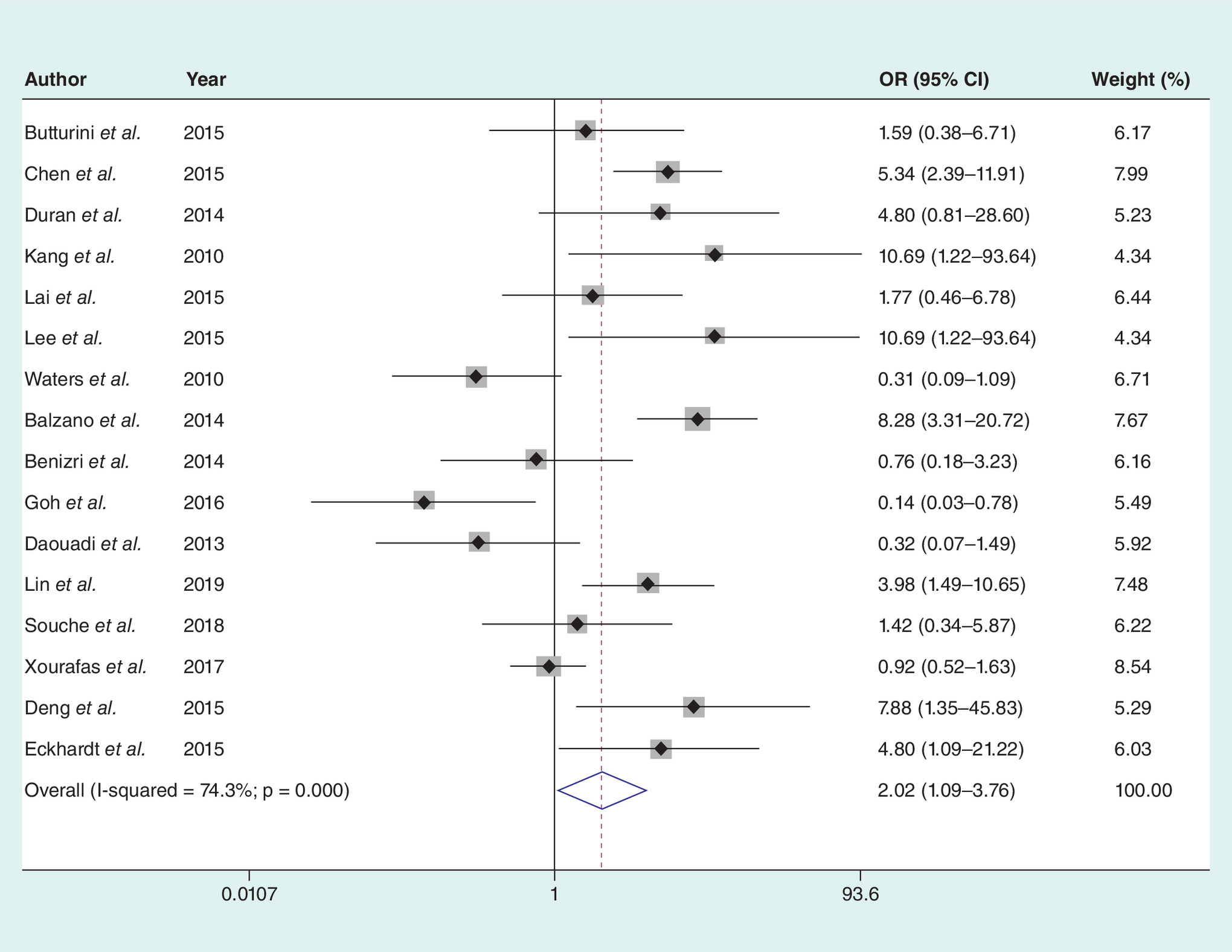
Figure 2. The spleen preservation rate.
OR: Odds ratio.
Operation time
The operation time between the two groups was conducted among 19 of the included studies. The result showed that the operation time of the RDP group was approximately 30 min longer than the LDP group (heterogeneity p = 0.000; I2 = 85.9%; MD: 27.372; 95% CI: 8.236–47.210; p = 0.000; Figure 3).
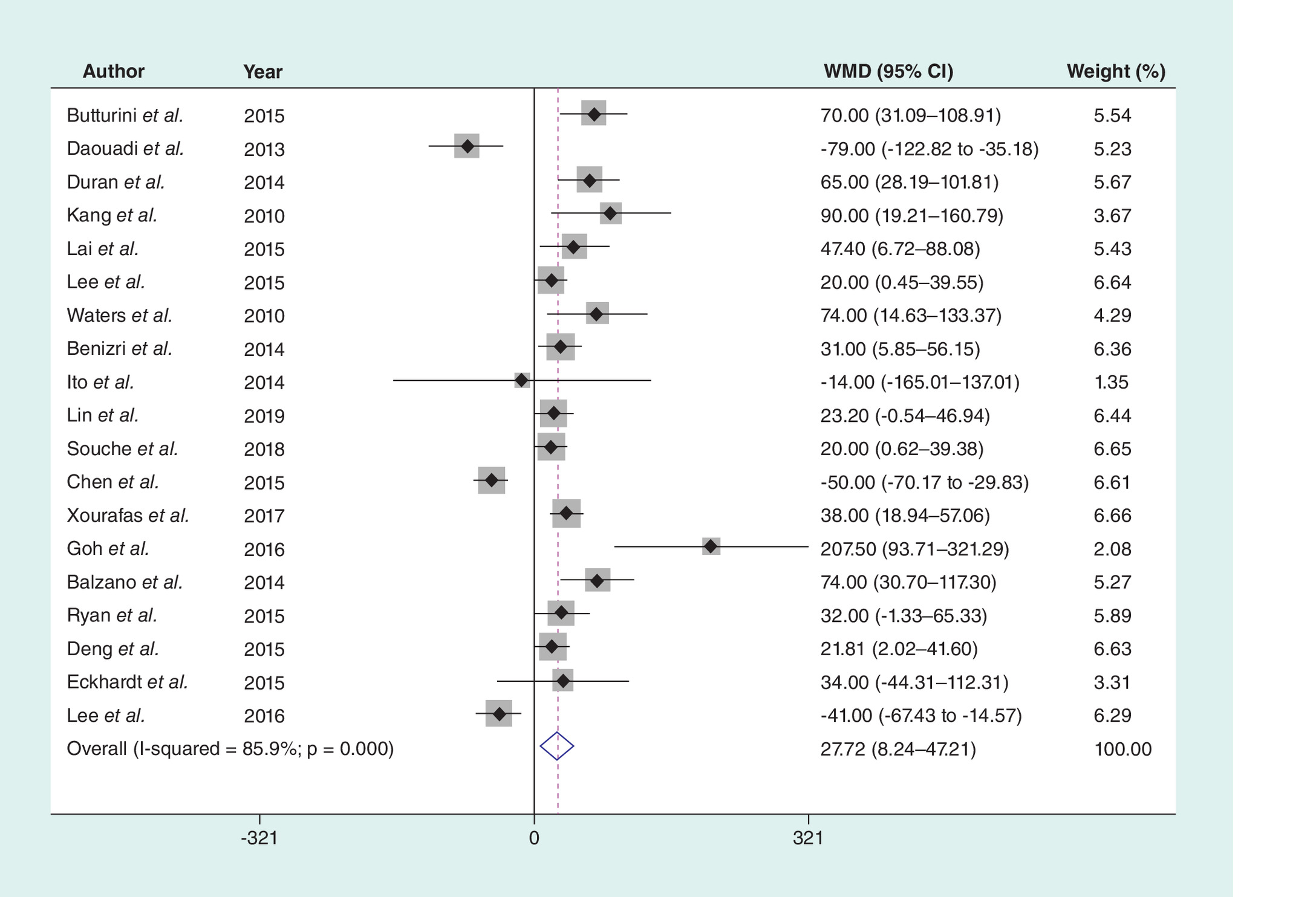
Figure 3. The operation time.
WMD: Weighted mean difference.
The length of hospital stay
Twenty-one articles published on the length of hospital stay. There is no heterogeneity in the statistical results of the pooled literatures (I2 = 44.5%, p = 0.611). The result of the fixed effect model showed that the RDP group had shorter hospital stay (MD: -0.911; 95% CI: -1.287 to -0.535; p = 0.000; Figure 4).
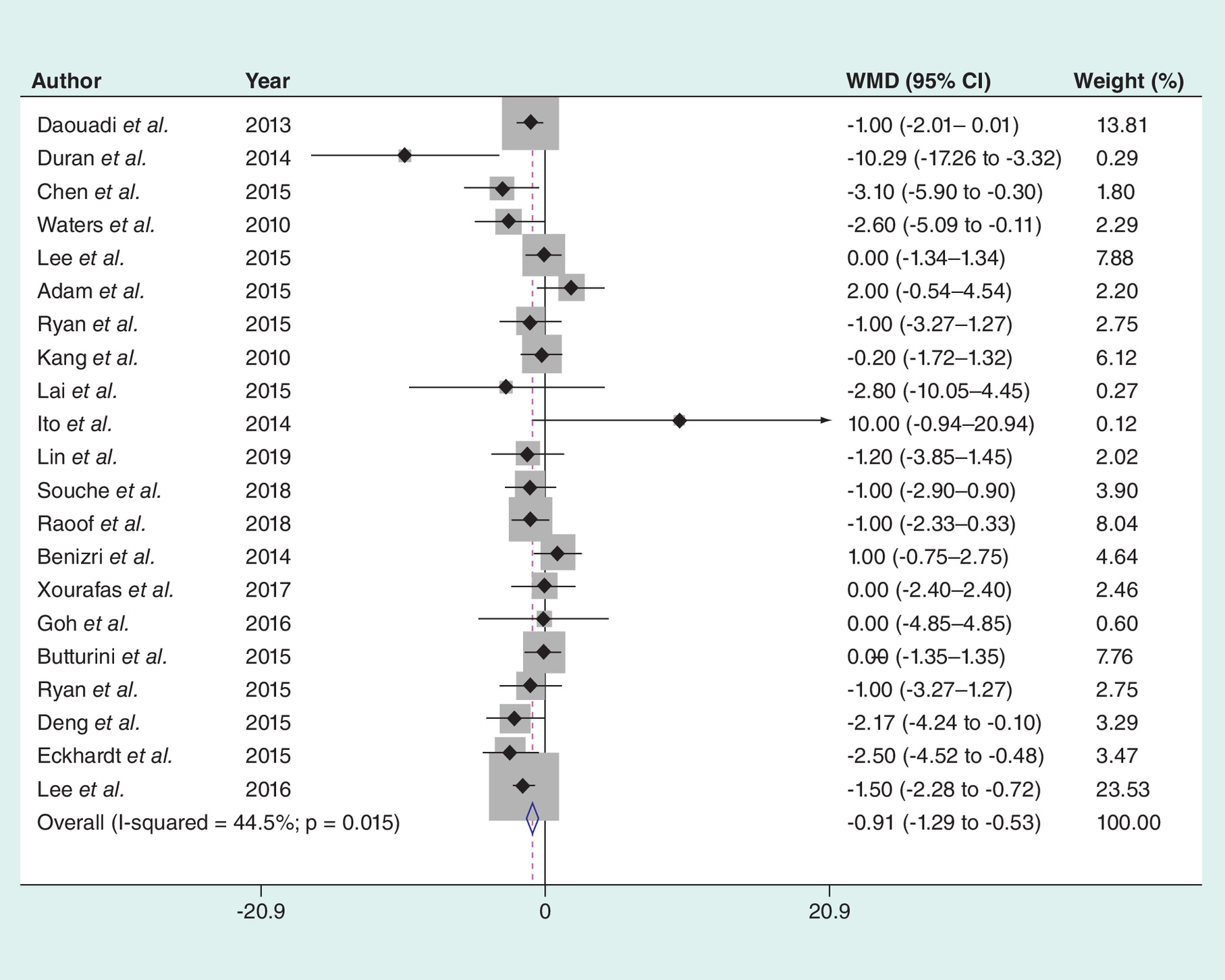
Figure 4. The length of hospital stay.
WMD: Weighted mean difference.
Conversion rate
Figure 6 showed the consequences of the conversion rate. There was a significant difference between the RDP group and the LDP group (heterogeneity p = 0.007; I2 = 51.9%; RD: -0.090; 95% CI: -1.287 to -0.535; p = 0.000; Figure 5). The conversion rate in the LDP group was significantly lower than that in the RDP group.
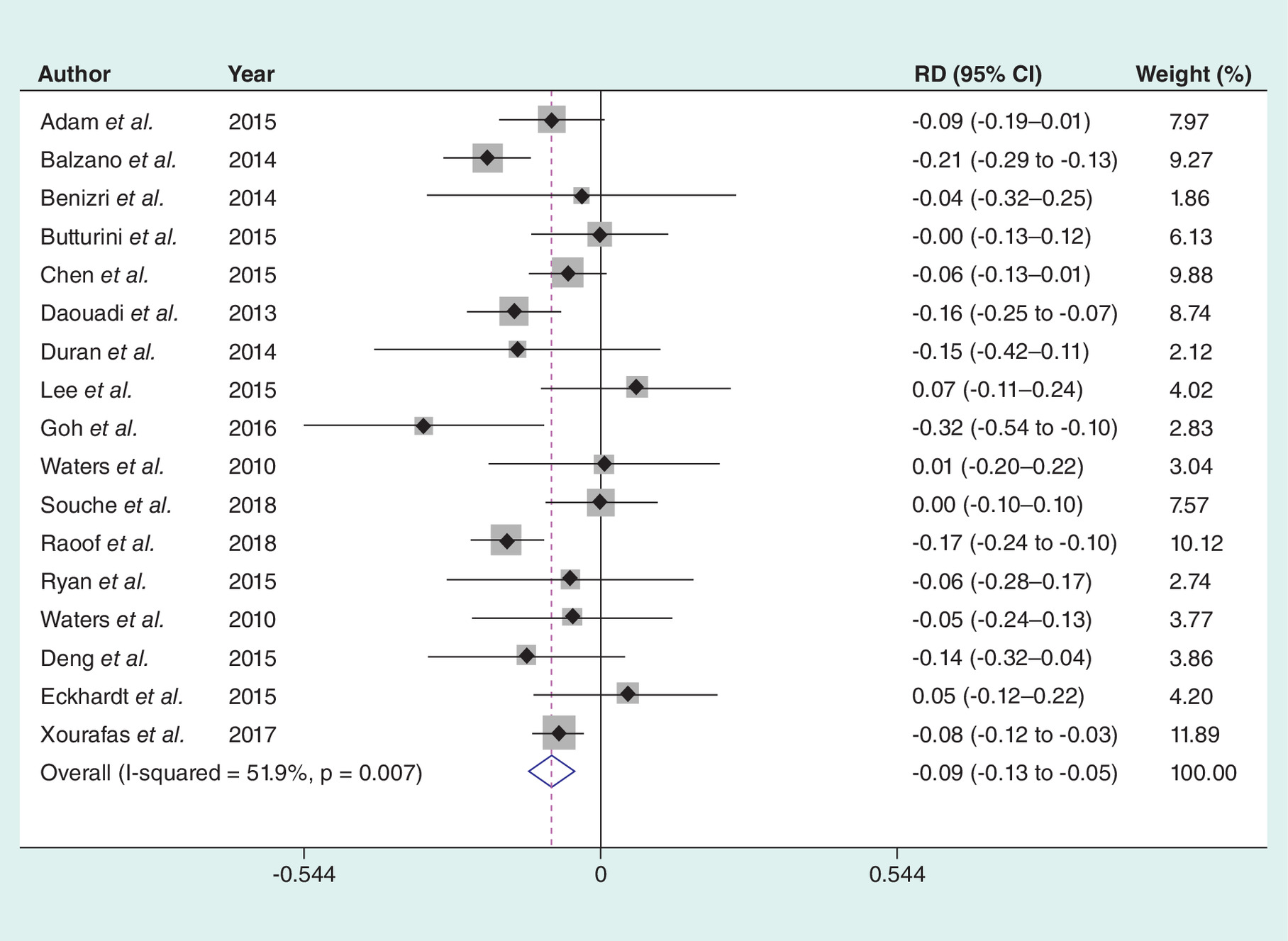
Figure 5. The conversion rate.
RD: Rate difference.
Estimated blood loss
The estimated blood loss between the two groups was conducted among 18 of the included studies. The results showed that there were no significant differences (heterogeneity p = 0.000; I2 = 74.4%; MD: -14.619; 95% CI: -58.019–28.781; p = 0.509; Figure 6).
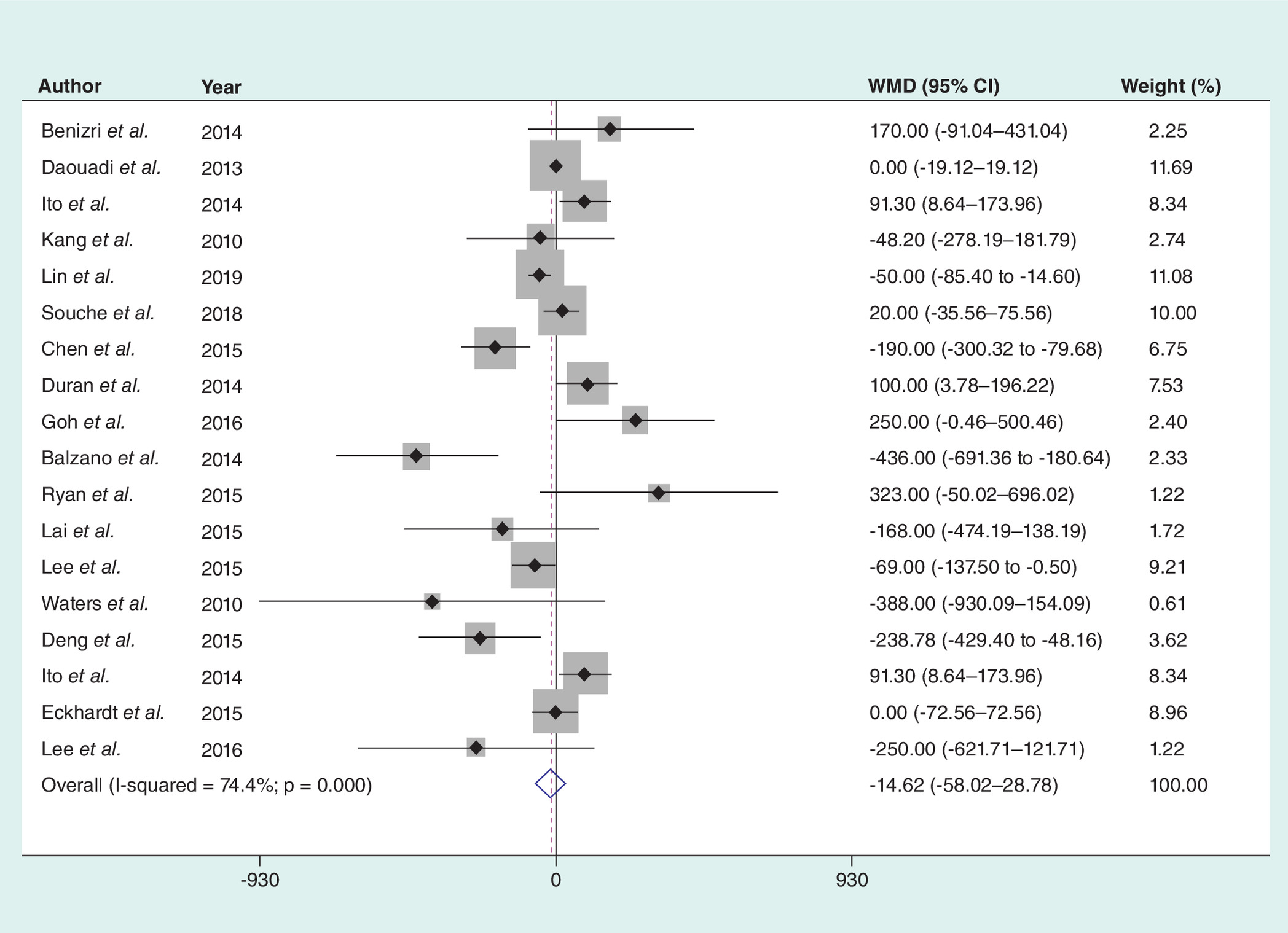
Figure 6. The estimated blood loss.
WMD: Weighted mean difference.
Total complication
Complications, including postoperative hemorrhage, biliary fistula and chylous fistula and so on, were evaluated in 17 studies. No significant differences were observed between the two groups (OR: 0.884; 95% CI: 0.716–1.092; p = 0.253; Figure 7) with no heterogeneity (p = 0.563; I2 = 0.0%).
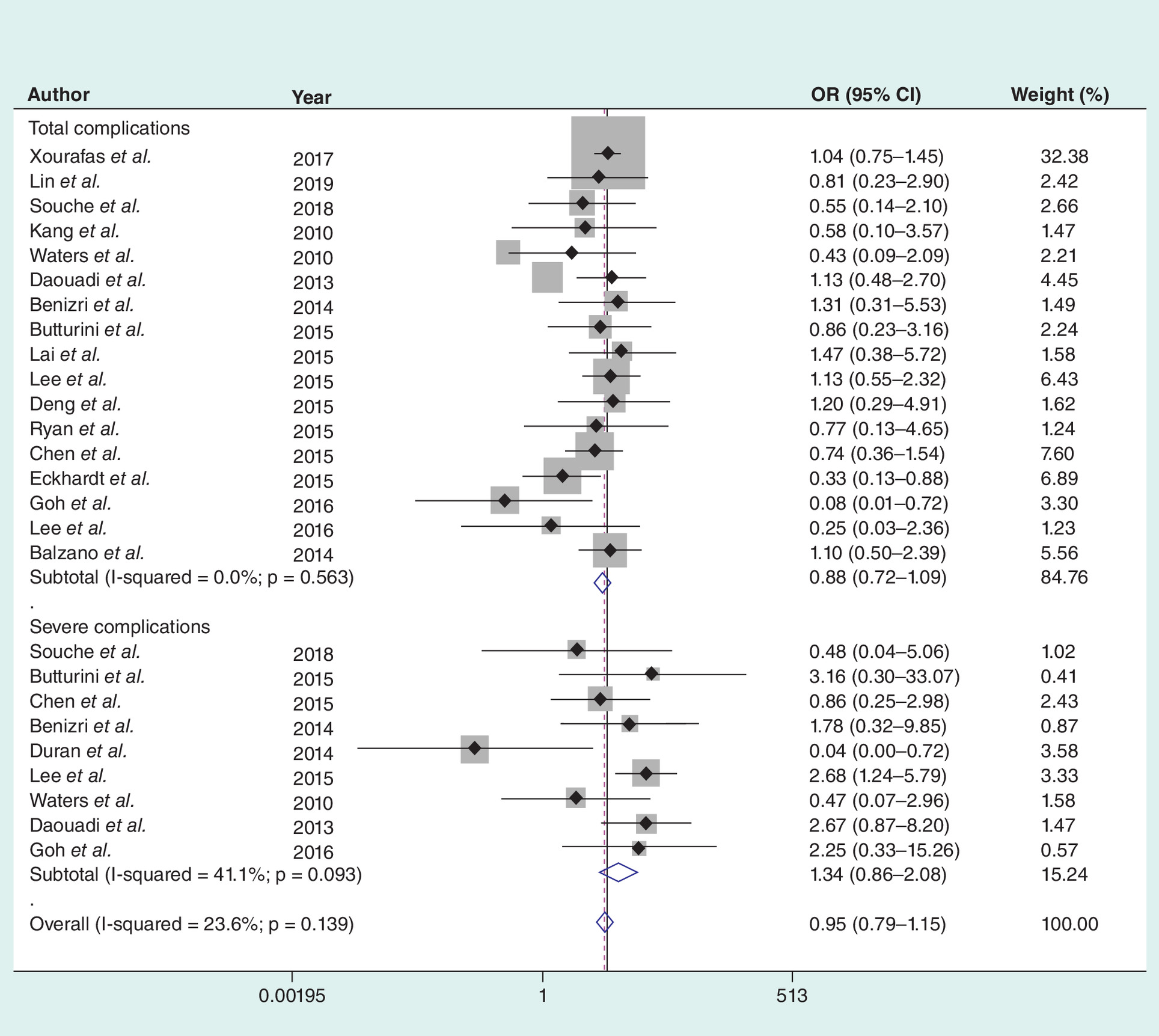
Figure 7. The complication.
OR: Odds ratio.
Severe complication
Severe complications were defined according to Clavien-Dindo classification system. No significant differences were observed between the two groups (OR: 1.337; 95% CI: 0.858–2.084; p = 0.199; Figure 7) with no heterogeneity (p = 0.093; I2 = 41.1%).
Operation cost
Only five literatures provided the adequate data about the operation cost. The result of the meta-analysis showed that there was significant difference (MD: 2816.564; 95% CI: 1782.028–3851.064; p = 0.000; Figure 8) with obvious heterogeneity (p = 0.000; I2 = 98.6%).
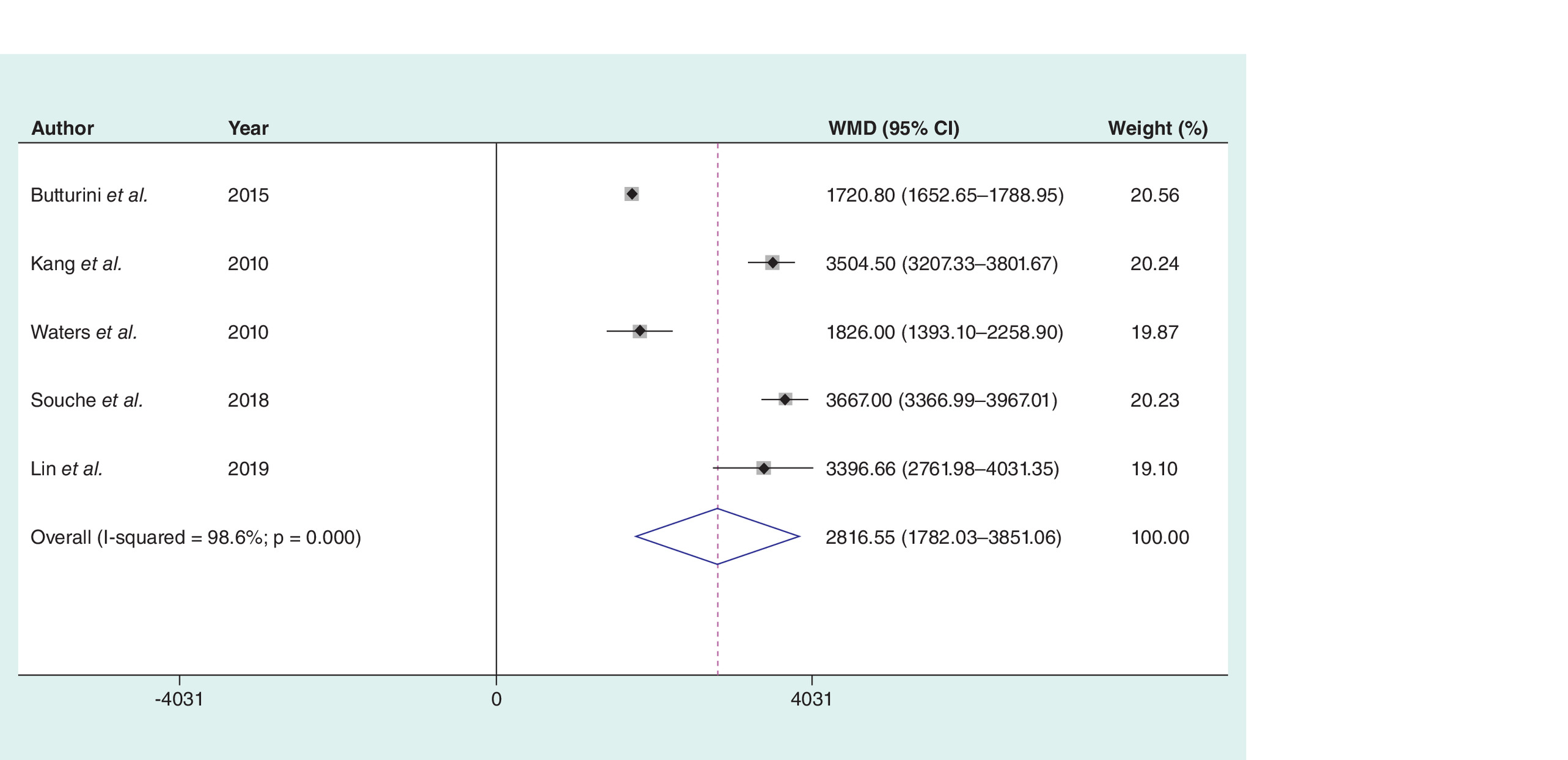
Figure 8. The operation cost.
WMD: Weighted mean difference.
Lymph nodules harvest
Ten articles published on the lymph nodules harvest. There was heterogeneity in the statistical results of the pooled literatures (I2 = 67.6%; p = 0.001). The result of the random effect model showed that the RDP group had similar lymph nodules harvest compared with the LPD group (MD: 0.826; 95% CI: -1.131–2.783; p = 0.408; Figure 9).
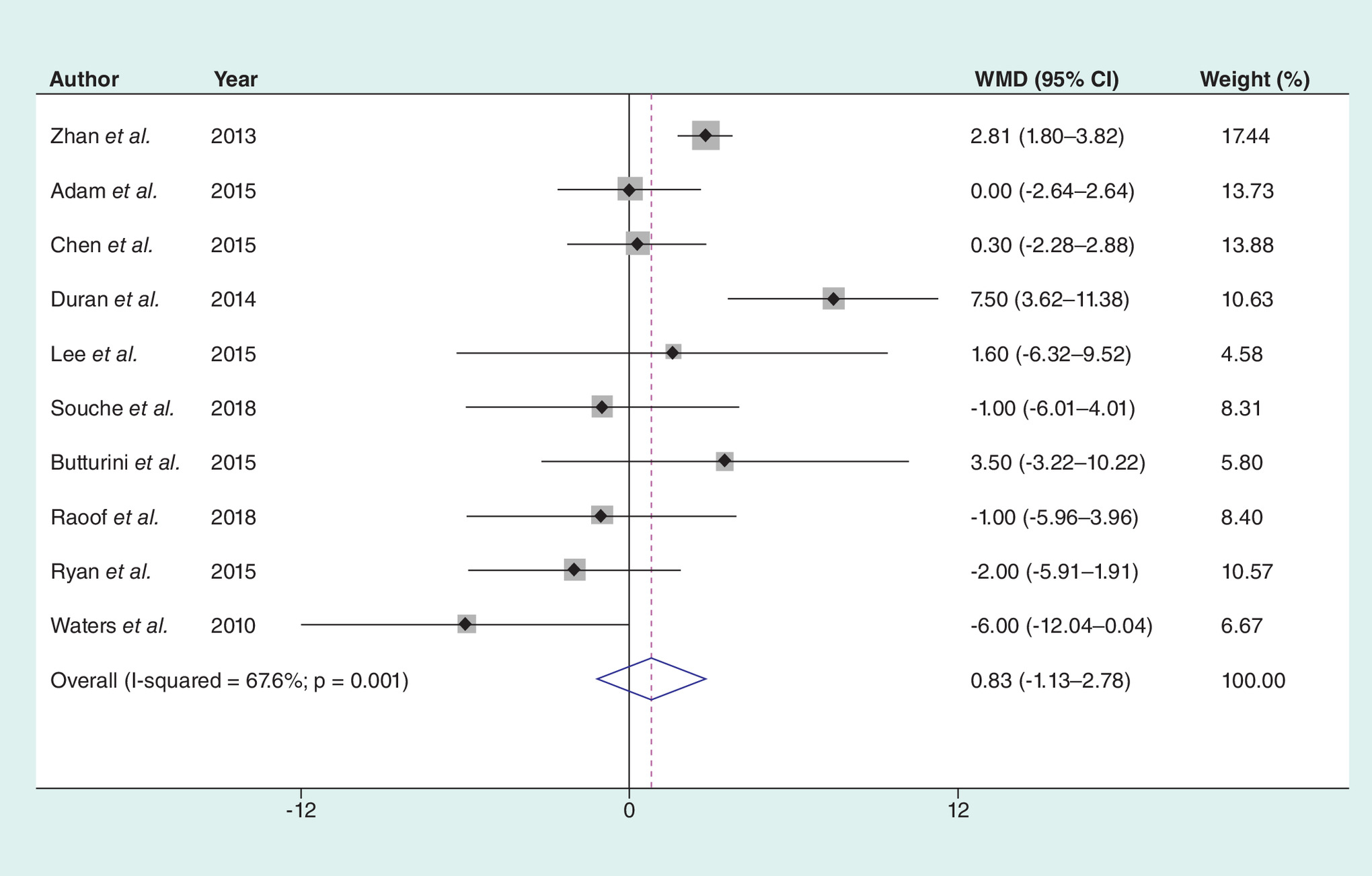
Figure 9. The lymph nodules harvest.
WMD: Weighted mean difference.
Blood transfusion rate
The blood transfusion rate was reported in 13 included studies. A fixed-effects model was performed with no heterogeneity (I2 = 0.0%; p = 0.454). There was no significant difference between the two groups (RD: 0.000; 95% CI: -0.030–0.030; p = 0.998; Figure 10).
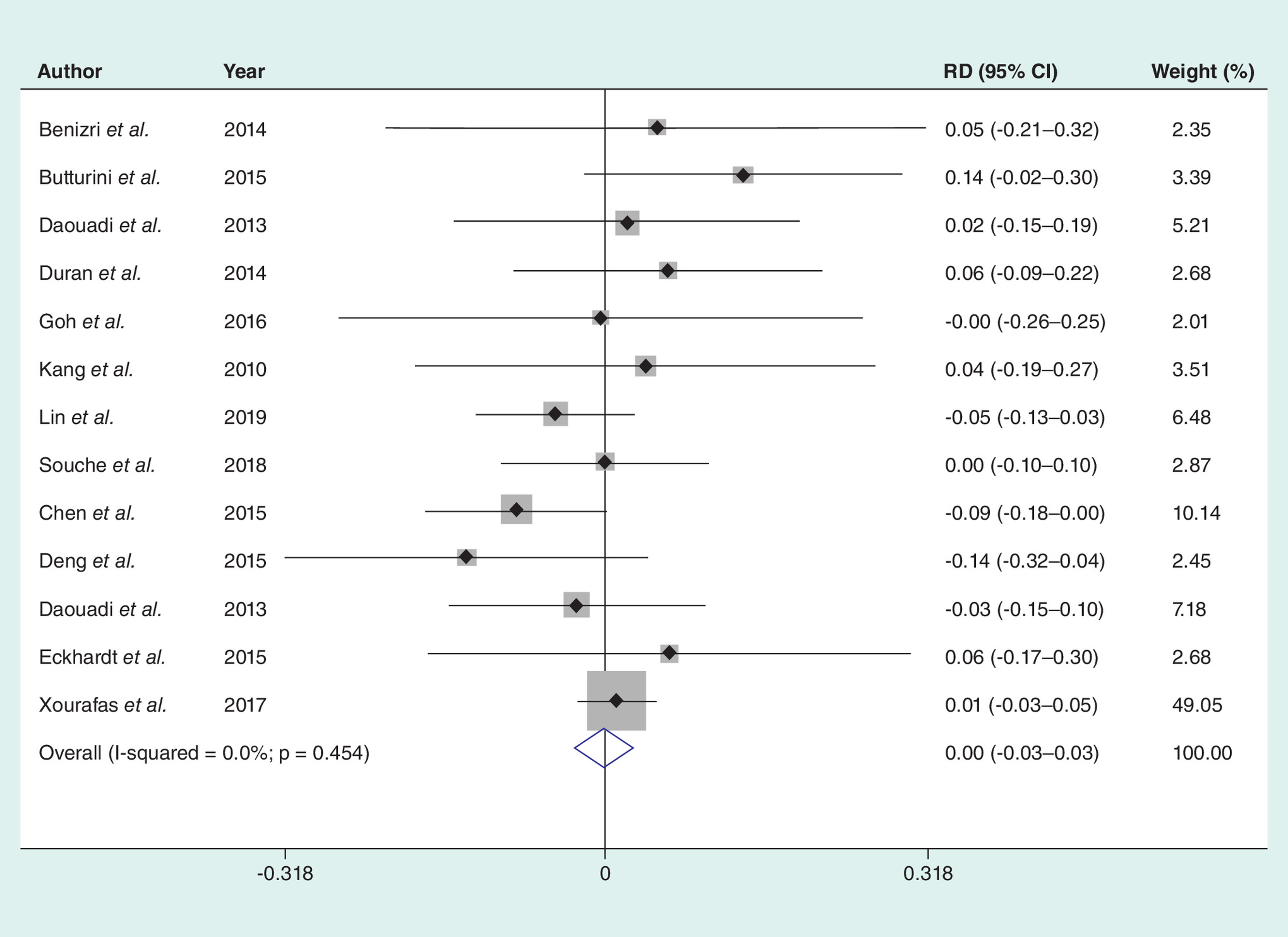
Figure 10. The blood transfusion rate.
RD: Rate difference.
Total pancreatic fistula
The total pancreatic fistula could be extracted from 17 studies. There was no heterogeneity in the statistical results of the pooled literatures (I2 = 0.0%; p = 0.957). The result of the fixed effect model showed that the incidence of the total pancreatic fistula was similar between the two groups (OR: 1.086; 95% CI: 0.839–1.404; p = 0.531; Figure 11).
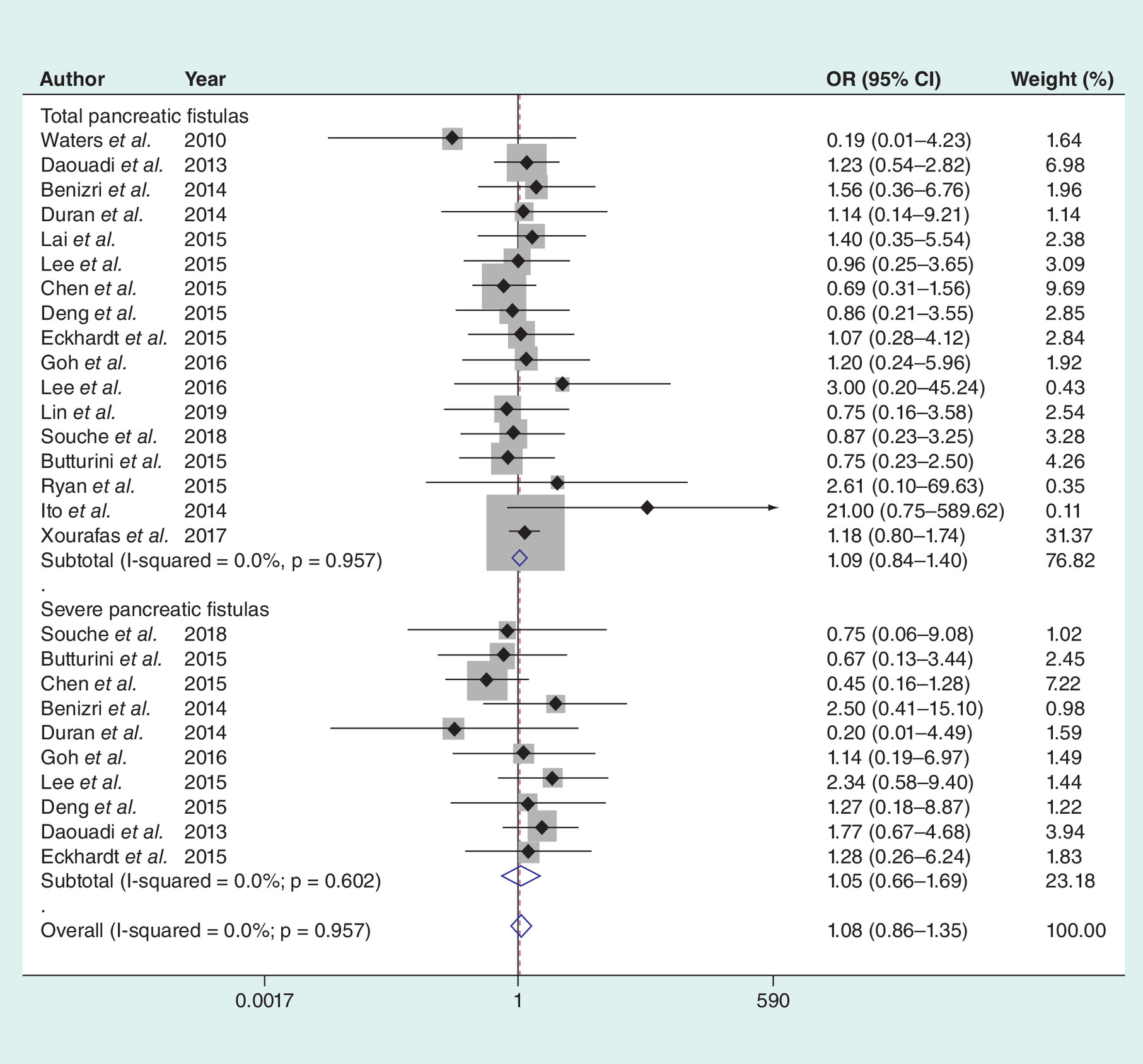
Figure 11. The pancreatic fistula.
OR: Odds ratio.
Severe pancreatic fistula
Severe pancreatic fistula including Class B and Class C fistulas was assessed in 10 articles. A fixed-effects model was performed with no heterogeneity (I2 = 0.0%; p = 0.602). There was no significant difference between the two groups (OR: 1.051; 95% CI: 0.656–1.686; p = 0.835, Figure 11).
R0 resection rate
R0 resection was evaluated in eight literatures. A random effect model was performed with significant heterogeneity (I2 = 82.7%; p = 0.000). There was no significant difference between the two groups (RD: -0.041, 95% CI: -0.151–0.096; p = 0.462; Figure 12).

Figure 12. The R0 resection rate.
RD: Rate difference.
Mortality
Seventeen articles have been published on the mortality. There was no heterogeneity in the statistical results of the pooled literatures (I2 = 0.0%; p = 1.00000). The result of the fixed effect model showed that there was no significant difference (RD: -0.007; 95% CI: -0.020–0.007; p = 0.314; Figure 13).
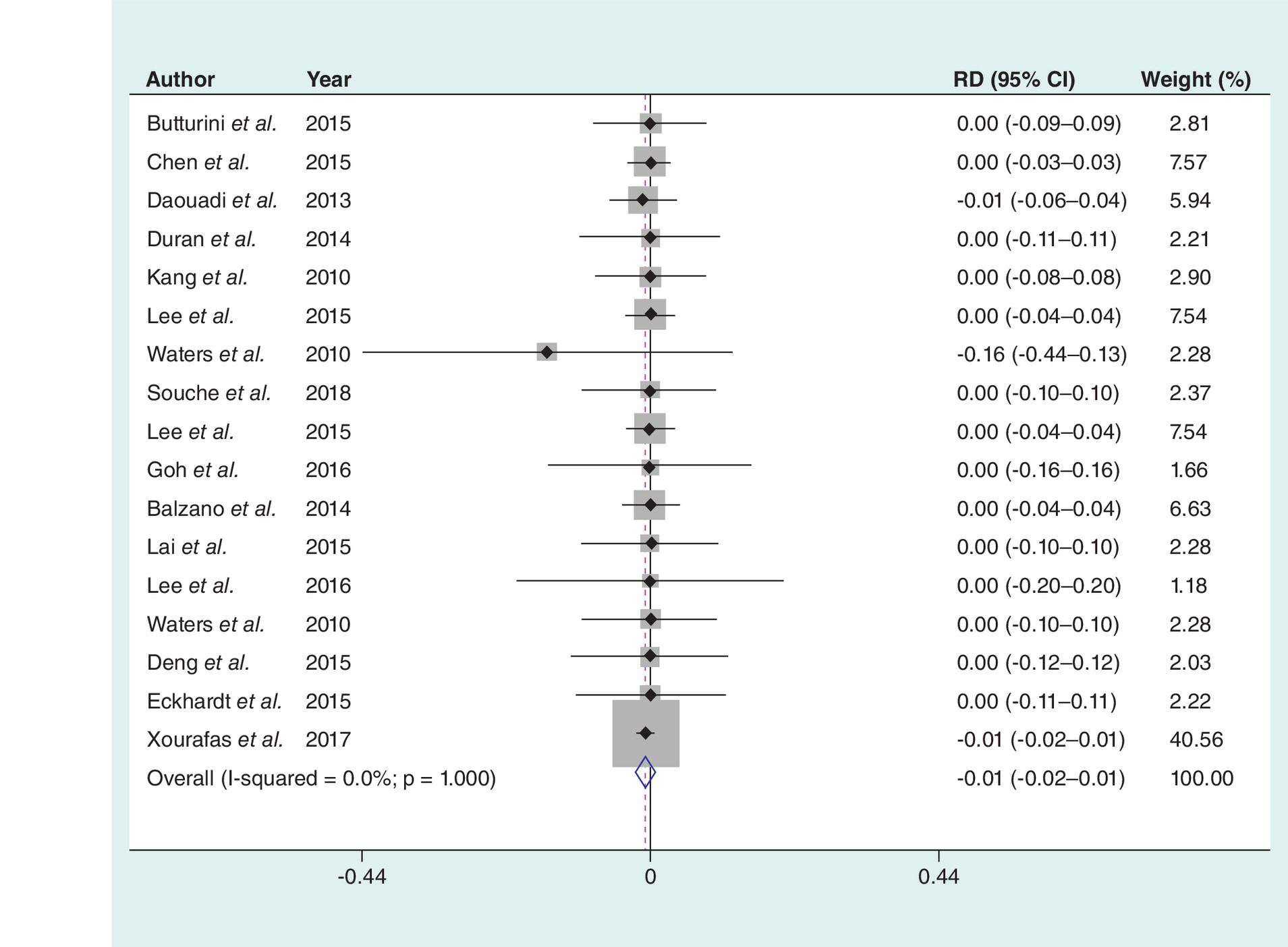
Figure 13. The mortality.
RD: Rate difference.
Discussion
The DP spleen preserving is indicated only for benign tumors, neuroendocrine tumors or borderline malignancy tumors. With the emphasis on the immune function of spleen, more and more surgeons advocate preserving the spleen while performing DP to reduce the risk of infection, thrombosis and hematological tumors after splenectomy [44–47]. There are two main types of splenic surgery: the Kimura method with preservation of splenic arteries and veins, and the Warshaw method with excision of splenic arteries and veins but preservation of gastric short vessels [48,49]. Spleen preservation and conversion rates are the key indexes for the success of minimally invasive DP. Chen et al. [24] compared the surgical effects of minimally invasive DP among matched patients scheduled for spleen preservation. It was found that the success rate of spleen preservation by RDP was significantly higher than that by LDP (95.7 vs 39.4%). In the RDP group, the Kimura method was used for spleen preservation, accounting for 75.6% (34/45). Liu et al. [50] observed that the spleen-preserving rate of the RDP group was 95.5% for nonmalignant distal pancreatic tumors with a maximum diameter of 3–5 cm and 61.9% were preserved by the Kimuma method. Both data were higher than that of the LDP group in a propensity score-matched study. In contrast, a prospective nonrandomized study of 43 patients indicated that RDP did not have a significant advantage over LDP [23]. The results of our meta-analysis showed that RDP did increase the success rate of spleen preservation (OR: 2.02; 95% CI: 1.09–3.76) and reduce the conversion rate (RD: -0.09; 95% CI: -0.13 to -3.76) compared with LDP. The incidence of splenic infarction and gastric varices after spleen-preserving operation with the Kimuma method was lower and became the first choice of many surgeons [51–53]. The RDP had a 3D high-definition field of vision and was more stable, so it was helpful for a more accurate operation. In the process of separating the pancreatic parenchyma from the splenic artery and vein, for the Kimura method, the blood vessels could be treated separately, which effectively reduced the risk of bleeding and improved the success rate of preserving the spleen [26,32].
This meta-analysis showed that patients underwent RDP had a longer period of operation time than LDP (weighted mean difference [WMD]: 27.72; 95% CI: 8.24–47.21). The combined results were consistent with most clinical studies in the literatures [54,55]. The longer operation time of RDP may be related to the following reasons. First of all, the RDP relevant research is still in the learning stage, which inevitably requires a longer learning curve, including the time required to adapt to new technologies. Second, since additional settings required by robots usually take half an hour to complete, the time spent in the operating room of robotic surgery is extended. Third, most current studies do not describe surgeon proficiency clearly [56].
Pancreatic fistula is the most common abdominal complication after DP [57]. At present, most studies demonstrated that there were no significant differences in the incidence of total complications and pancreatic fistula between RDP and LDP [15,28]. No significant difference was observed in the incidence of total complications, severe complications, total pancreatic fistula and severe pancreatic fistula between RDP and LDP groups according to the results of subgroup analysis. As for transection of the pancreas, some surgeons chose to use the ultrasound scalpel [23]. The overall incidence of pancreatic fistula was 53.5%, of which the incidence of B grade and C grade pancreatic fistula is 16.3%. While other doctors who made up the majority chose to use a linear incision closure device. For those operations, the overall incidence of pancreatic fistula was 27.7–42.1%, of which the incidence of B grade and C grade pancreatic fistula was 7.9 and 9.8% [22,24,50]. It indicated that linear incision closure was more suitable for transection of pancreas than ultrasonic scalpel. The incision edge of pancreas with linear cutting stapler was smoother, the incidence of bleeding and pancreatic fistula was lower and different types of nail silos could be selected according to different thickness of the pancreas.
Kang et al. [26] considered that RDP total cost the patients about USD 8300, which was more than twice the amount for the LDP group. The results of this meta-analysis also showed that the operation cost of RDP was significantly higher than that of LDP (MD: 2816.546; 95% CI: 1782.028–3851.064). This is also one of the important reasons that restrict the application of robotic surgery at present. Studies showed that patients in the RDP group had a shorter length of hospital stay [24,50]. In our study, the hospital stay in the RDP group was nearly 1 day shorter than the LDP group (MD: -0.91; 95% CI: -1.29 to -0.53), which was consistent with previous studies.
This study had following limitations: First, there was heterogeneity in operation time, estimated blood loss, operation cost and spleen preservation rate between the two groups. Robot surgery system, including initial learning period, may lead to unequal operation quality comparison. Second, some literatures included in this meta-analysis had relative small sample size. In addition, the focus of this meta-analysis was to provide a short-term outcome to clarify the value of RDP in DP, and the long-term efficacy of surgical treatment has not been thoroughly discussed in some included studies. Therefore, further attention should be paid to long-term efficacy of RCTs to determine the potential advantages of RDP. Further studies on the long-term outcomes of two surgical techniques are warranted.
Conclusion
Both robotic and LDP are safe and feasible. Although RDP increases the operation cost, the spleen-preserving rate is higher. Robotic surgery may be an alternative approach to DP.
•
Compared with open distal pancreatectomy (ODP), minimally invasive pancreatectomy could evidently reduce intraoperative bleeding, improve spleen-preserving rate, reduce postoperative pain, accelerate postoperative recovery and shorten hospital stay.
•
The emergence of robotic surgery system partly overcame the shortcomings of laparoscopic surgery.
•
Recently, a meta-analysis focusing on laparoscopic distal pancreatectomy (LDP) and robotic distal pancreatectomy (RDP) pooled the results from studies with finite sample sizes.
•
Therefore, we performed a more comprehensive meta-analysis concerning whether patients benefit more from RDP compared with LDP.
•
There was significant difference in spleen preservation rate, operation time, the length of hospital stays, conversion rate and operation cost.
•
No significant difference was detected in estimated blood loss, total complication, severe complication, lymph nodules harvest, blood transfusion rate, total pancreatic fistula, severe pancreatic fistula, R0 resection rate and mortality.
•
Both RDP and LDP are safe and feasible.
•
Although RDP increases the operation cost, the spleen-preserving rate is much higher. Robotic surgery may be an alternative approach to distal pancreatectomy.
Author contributions
YH Hu and YF Qin conceived of the design of the study. YM Zhao, W Jin, DJ Kong and DD Yu performed and collected the data and contributed to the design of the study. X Li and H Wang prepared and revised the manuscript. All the authors read and approved the final content of the manuscript.
Financial & competing interests disclosure
This work was supported by grants to H Wang from National Natural Science Foundation of China (nos. 81273257 and 81471584), Tianjin Application Basis and Cutting-Edge Technology Research Grant (no. 14JCZDJC35700), Li Jieshou Intestinal Barrier Research Special Fund (no. LJS_201412), Natural Science Foundation of Tianjin (no. 18JCZDJC35800) and Tianjin Medical University Talent Fund. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
1.
Kleeff J, Diener MK, Z'Graggen K et al. Distal pancreatectomy: risk factors for surgical failure in 302 consecutive cases. Ann. Surg. 245(4), 573–582 (2007).
2.
Cloyd JM, Katz MH, Prakash L et al. Preoperative therapy and pancreatoduodenectomy for pancreatic ductal adenocarcinoma: a 25-year single-institution experience. J. Gastrointest. Surg. 21(1), 164–174 (2017).
3.
Winter JM, Cameron JL, Campbell KA et al. 1423 pancreaticoduodenectomies for pancreatic cancer: a single-institution experience. J. Gastrointest. Surg. 10(9), 1199–1210 (2006).
4.
Cuschieri A. Laparoscopic surgery of the pancreas. J. Royal Coll. Surg. Edin. 39(3), 178–184 (1994).
5.
Magge D, Gooding W, Choudry H et al. Comparative effectiveness of minimally invasive and open distal pancreatectomy for ductal adenocarcinoma. JAMA Surg. 148(6), 525–531 (2013).
6.
Stauffer JA, Rosales-Velderrain A, Goldberg RF, Bowers SP, Asbun HJ. Comparison of open with laparoscopic distal pancreatectomy: a single institution's transition over a 7-year period. HPB 15(2), 149–155 (2013).
7.
Jin T, Altaf K, Xiong JJ et al. A systematic review and meta-analysis of studies comparing laparoscopic and open distal pancreatectomy. HPB 14(11), 711–724 (2012).
8.
Kocaay AF, Celik SU, Goktug UU, Cakmak A. A review on the role of laparoscopy in pancreatic cancer. Acta Gastro. Enterologica Belgica. 79(2), 233–238 (2016).
9.
DiNorcia J, Schrope BA, Lee MK et al. Laparoscopic distal pancreatectomy offers shorter hospital stays with fewer complications. J. Gastrointest. Surg. 14(11), 1804–1812 (2010).
10.
Corcione F, Esposito C, Cuccurullo D et al. Advantages and limits of robot-assisted laparoscopic surgery: preliminary experience. Surg. Endosc. 19(1), 117–119 (2005).
11.
Zureikat AH, Moser AJ, Boone BA, Bartlett DL, Zenati M, Zeh HJ 3rd. 250 robotic pancreatic resections: safety and feasibility. Ann. Surg. 258(4), 554–559 (2013).
12.
Memeo R, Sangiuolo F, de Blasi V et al. Robotic pancreaticoduodenectomy and distal pancreatectomy: state of the art. J. Visceral Surg. 153(5), 353–359 (2016).
13.
Orady M, Hrynewych A, Nawfal AK, Wegienka G. Comparison of robotic-assisted hysterectomy to other minimally invasive approaches. JSLS 16(4), 542–548 (2012).
14.
Melvin WS, Needleman BJ, Krause KR, Ellison EC. Robotic resection of pancreatic neuroendocrine tumor. J. Laparoendosc. Adv. Surg. Tech. Part A 13(1), 33–36 (2003).
15.
Gavriilidis P, Lim C, Menahem B, Lahat E, Salloum C, Azoulay D. Robotic versus laparoscopic distal pancreatectomy – the first meta-analysis. HPB 18(7), 567–574 (2016).
16.
Tan-Tam C, Chung SW. Minireview on laparoscopic hepatobiliary and pancreatic surgery. World J. Gastrointest. Endosc. 6(3), 60–67 (2014).
17.
Niu X, Yu B, Yao L et al. Comparison of surgical outcomes of robot-assisted laparoscopic distal pancreatectomy versus laparoscopic and open resections: a systematic review and meta-analysis. Asian J. Surg. 42(1), 32–45 (2019).
18.
Guerrini GP, Lauretta A, Belluco C et al. Robotic versus laparoscopic distal pancreatectomy: an up-to-date meta-analysis. BMC Surg. 17(1), 105 (2017).
19.
Casadei R, Marchegiani G, Laterza M et al. Total pancreatectomy: doing it with a mini-invasive approach. JOP 10(3), 328–331 (2009).
20.
Boggi U, Palladino S, Massimetti G et al. Laparoscopic robot-assisted versus open total pancreatectomy: a case-matched study. Surg. Endosc. 29(6), 1425–1432 (2015).
21.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 240(2), 205–213 (2004).
22.
Souche R, Herrero A, Bourel G et al. Robotic versus laparoscopic distal pancreatectomy: a French prospective single-center experience and cost–effectiveness analysis. Surg. Endosc. 32(8), 3562–3569 (2018).
23.
Butturini G, Damoli I, Crepaz L et al. A prospective non-randomised single-center study comparing laparoscopic and robotic distal pancreatectomy. Surg. Endosc. 29(11), 3163–3170 (2015).
24.
Chen S, Zhan Q, Chen JZ et al. Robotic approach improves spleen-preserving rate and shortens postoperative hospital stay of laparoscopic distal pancreatectomy: a matched cohort study. Surg. Endosc. 29(12), 3507–3518 (2015).
25.
Benizri EI, Germain A, Ayav A et al. Short-term perioperative outcomes after robot-assisted and laparoscopic distal pancreatectomy. J. Robotic Surg. 8(2), 125–132 (2014).
26.
Kang CM, Kim DH, Lee WJ, Chi HS. Conventional laparoscopic and robot-assisted spleen-preserving pancreatectomy: does da Vinci have clinical advantages? Surg. Endosc. 25(6), 2004–2009 (2011).
27.
Raoof M, Nota C, Melstrom LG et al. Oncologic outcomes after robot-assisted versus laparoscopic distal pancreatectomy: analysis of the National Cancer Database. J. Surg. Oncol. 118(4), 651–656 (2018).
28.
Ielpo B, Duran H, Diaz E et al. Robotic versus laparoscopic distal pancreatectomy: a comparative study of clinical outcomes and costs analysis. Int. J. Surg. 48, 300–304 (2017).
29.
Goh BK, Chan CY, Soh HL et al. A comparison between robotic-assisted laparoscopic distal pancreatectomy versus laparoscopic distal pancreatectomy. Int. J. Med. Robot. 13(1), (2017).
30.
Balzano G, Bissolati M, Boggi U, Bassi C, Zerbi A, Falconi M. A multicenter survey on distal pancreatectomy in Italy: results of minimally invasive technique and variability of perioperative pathways. Updates Surg. 66(4), 253–263 (2014).
31.
Ryan CE, Ross SB, Sukharamwala PB, Sadowitz BD, Wood TW, Rosemurgy AS. Distal pancreatectomy and splenectomy: a robotic or LESS approach. JSLS 19(1), e2014.00246 (2015).
32.
Lai EC, Tang CN. Robotic distal pancreatectomy versus conventional laparoscopic distal pancreatectomy: a comparative study for short-term outcomes. Front. Med. 9(3), 356–360 (2015).
33.
Lee SY, Allen PJ, Sadot E et al. Distal pancreatectomy: a single institution's experience in open, laparoscopic, and robotic approaches. J. Am. Coll. Surg. 220(1), 18–27 (2015).
34.
Waters JA, Canal DF, Wiebke EA et al. Robotic distal pancreatectomy: cost-effective? Surgery 148(4), 814–823 (2010).
35.
Adam MA, Choudhury K, Goffredo P et al. Minimally invasive distal pancreatectomy for cancer: short-term oncologic outcomes in 1,733 patients. World J. Surg. 39(10), 2564–2572 (2015).
36.
Ito M, Asano Y, Shimizu T, Uyama I, Horiguchi A. Comparison of standard laparoscopic distal pancreatectomy with minimally invasive distal pancreatectomy using the da Vinci S system. Hepatogastroenterology 61(130), 493–496 (2014).
37.
Daouadi M, Zureikat AH, Zenati MS et al. Robot-assisted minimally invasive distal pancreatectomy is superior to the laparoscopic technique. Ann. Surg. 257(1), 128–132 (2013).
38.
Eckhardt S, Schicker C, Maurer E, Fendrich V, Bartsch DK. Robotic-assisted approach improves vessel preservation in spleen-preserving distal pancreatectomy. Digestive Surg. 33(5), 406–413 (2016).
39.
Xourafas D, Ashley SW, Clancy TE. Comparison of perioperative outcomes between open, laparoscopic, and robotic distal pancreatectomy: an analysis of 1815 patients from the ACS-NSQIP Procedure-Targeted Pancreatectomy Database. J. Gastrointest. Surg. 21(9), 1442–1452 (2017).
40.
Lee KF, Fong A, Chong C, Cheung YS, Lai P. Minimally invasive versus open approach for distal pancreatectomy: a retrospective comparative study. HPB 18(1), e438-e (2016).
41.
Lin XC, Huang HG, Chen YC et al. Robotic versus laparoscopic distal pancreatectomy: a retrospective single-center study. Chinese J. Surg. 57(2), 102–107 (2019).
42.
Zhan Q, Peng C, Deng X et al. Robot-assisted distal pancreatectomy. Chin. J. Gen. Surg. 5(28), 337–340 (2013).
43.
Deng Y, Xia A, Zhang S, Feng Y, Zhang B. Comparative analysis of clinical short term outcomes of Da Vinci robot assisted spleen preserving distal pancreatectomy and laparoscopic spleen preserving distal pancreatectomy. Int. J. Surg. 42(9), 596–599 (2015).
44.
Kristinsson SY, Gridley G, Hoover RN, Check D, Landgren O. Long-term risks after splenectomy among 8,149 cancer-free American veterans: a cohort study with up to 27 years follow-up. Haematologica 99(2), 392–398 (2014).
45.
Boyle S, White RH, Brunson A, Wun T. Splenectomy and the incidence of venous thromboembolism and sepsis in patients with immune thrombocytopenia. Blood 121(23), 4782–4790 (2013).
46.
Sinwar PD. Overwhelming post splenectomy infection syndrome – review study. Int. J. Surg. 12(12), 1314–1316 (2014).
47.
Kim H, Song KB, Hwang DW et al. A single-center experience with the laparoscopic Warshaw technique in 122 consecutive patients. Surg. Endosc. 30(9), 4057–4064 (2016).
48.
Kimura W, Yano M, Sugawara S et al. Spleen-preserving distal pancreatectomy with conservation of the splenic artery and vein: techniques and its significance. J. Hepatobiliary Pancreat. Sci. 17(6), 813–823 (2010).
49.
Warshaw AL. Distal pancreatectomy with preservation of the spleen. J. Hepatobiliary Pancreat. Sci. 17(6), 808–812 (2010).
50.
Liu R, Liu Q, Zhao ZM, Tan XL, Gao YX, Zhao GD. Robotic versus laparoscopic distal pancreatectomy: a propensity score-matched study. J. Surg. Oncol. 116(4), 461–469 (2017).
51.
Jain G, Chakravartty S, Patel AG. Spleen-preserving distal pancreatectomy with and without splenic vessel ligation: a systematic review. HPB 15(6), 403–410 (2013).
52.
Zhou ZQ, Kim SC, Song KB, Park KM, Lee JH, Lee YJ. Laparoscopic spleen-preserving distal pancreatectomy: comparative study of spleen preservation with splenic vessel resection and splenic vessel preservation. World J. Surg. 38(11), 2973–2979 (2014).
53.
Hua YF, Yadav DK, Bai X, Liang T. Laparoscopic spleen-preserving distal pancreatectomy (LSPDP) with preservation of splenic vessels: an inferior–posterior approach. Gastroenterol. Res. Pract. 2018, 1683719 (2018).
54.
Huang B, Feng L, Zhao J. Systematic review and meta-analysis of robotic versus laparoscopic distal pancreatectomy for benign and malignant pancreatic lesions. Surg. Endosc. 30(9), 4078–4085 (2016).
55.
Zhou JY, Xin C, Mou YP et al. Robotic versus laparoscopic distal pancreatectomy: a meta-analysis of short-term outcomes. PLoS ONE 11(3), e0151189 (2016).
56.
Shakir M, Boone BA, Polanco PM et al. The learning curve for robotic distal pancreatectomy: an analysis of outcomes of the first 100 consecutive cases at a high-volume pancreatic centre. HPB 17(7), 580–586 (2015).
57.
Goh BK, Wong JS, Chan CY, Cheow PC, Ooi LL, Chung AY. First experience with robotic spleen-saving, vessel-preserving distal pancreatectomy in Singapore: a report of three consecutive cases. Singapore Med. J. 57(8), 464–469 (2016).
Information & Authors
Information
Published In
Pages: 201 - 218
PubMed: 31975614
Copyright
© 2020 Future Medicine Ltd.
History
Received: 18 August 2019
Accepted: 17 December 2019
Published online: 24 January 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Meta-analysis of short-term outcomes comparing robot-assisted and laparoscopic distal pancreatectomy. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0124
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Seung Hyun Rho, Jeonghyun Lee, Jun Suh Lee, Robotic Gastrointestinal Surgery Compared to Conventional Approaches: An Umbrella Review of Clinical and Economic Outcomes, Journal of Clinical Medicine, 10.3390/jcm14238555, 14, 23, (8555), (2025).
- Yael Weksler, Guy Lifshitz, Shmuel Avital, Yaron Rudnicki, Robotic Surgery for Gastrointestinal Malignancies—A Review of How Far Have We Come in Pancreatic, Gastric, Liver, and Colorectal Cancer Surgery, Cancers, 10.3390/cancers17233802, 17, 23, (3802), (2025).
- Sorayouth Chumnanvej, Branesh M. Pillai, Jackrit Suthakorn, Siriluk Chumnanvej, Revised in-depth meta-analysis on the efficacy of robot-assisted versus traditional free-hand pedicle screw insertion, Laparoscopic, Endoscopic and Robotic Surgery, 10.1016/j.lers.2024.08.002, 7, 4, (155-165), (2024).
- María Alejandra Guerrero-Ortiz, Patricia Sánchez-Velazquez, Fernando Burdío, Marta Gimeno, Mauro Podda, Gianluca Pellino, Miguel Toledano, Javier Nuñez, Juan Bellido, María Asunción Acosta-Mérida, Emilio Vicente, Santiago Lopez-Ben, David Pacheco, Elizabeth Pando, Rosa Jorba, Juan Pablo Arjona Trujillo, Fabio Ausania, Mario Alvarez, Nair Fernandes, Sandra Castro-Boix, Amaia Gantxegi, Miquel Kraft- Carré, Pilar Pinto-Fuentes, Alejandro Bueno-Cañones, Javier Valdes-Hernandez, Luis Tresierra, Riccardo Caruso, Valentina Ferri, Berta Tio, Sonia Babiloni-Simon, David Lacasa-Martin, Carolina González-Abós, Jenny Guevara-Martinez, Eduardo Gutierrez-Iscar, Raquel Sanchez-Santos, Oscar Cano-Valderrama, Manuel Nogueira-Sixto, Nicolas Alvarez-Garrido, Sagrario Martinez-Cortijo, Manuel Alberto Lasaia, Santiago Linacero, Ana Pilar Morante, Fernando Rotellar, Jorge Arredondo, Pablo Marti, Lucas Sabatella, Gabriel Zozaya, Benedetto Ielpo, Cost-effectiveness of robotic vs laparoscopic distal pancreatectomy. Results from the national prospective trial ROBOCOSTES, Surgical Endoscopy, 10.1007/s00464-024-11109-x, 38, 11, (6270-6281), (2024).
- Sara Acciuffi, Mohammed Abu Hilal, Clarissa Ferrari, Sara Al-Madhi, Marc-Anthony Chouillard, Nouredin Messaoudi, Roland S. Croner, Andrew A. Gumbs, Study International Multicentric Pancreatic Left Resections (SIMPLR): Does Surgical Approach Matter?, Cancers, 10.3390/cancers16051051, 16, 5, (1051), (2024).
- Hester C. Timmerhuis, Christopher W. Jensen, Rejoice F. Ngongoni, Michael Baiocchi, Jonathan C. DeLong, Rika Ohkuma, Monica M. Dua, Jeffrey A. Norton, George A. Poultsides, Patrick J. Worth, Brendan C. Visser, Postoperative outcomes and costs of laparoscopic versus robotic distal pancreatectomy: a propensity-matched analysis, Surgical Endoscopy, 10.1007/s00464-024-10728-8, 38, 4, (2095-2105), (2024).
- Jyun-Ming Huang, Sheng-Hsien Chen, Te-Hung Chen, Short-Term Outcomes of Conventional Laparoscopic versus Robot-Assisted Distal Pancreatectomy for Malignancy: Evidence from US National Inpatient Sample, 2005–2018, Cancers, 10.3390/cancers16051003, 16, 5, (1003), (2024).
- Matthias Pfister, Pascal Probst, Philip C Müller, Pia Antony, Rosa Klotz, Eva Kalkum, Daniela Merz, Pietro Renzulli, Fabian Hauswirth, Markus K Muller, Minimally invasive versus open pancreatic surgery: meta-analysis of randomized clinical trials , BJS Open, 10.1093/bjsopen/zrad007, 7, 2, (2023).
- Tess M. E. van Ramshorst, Eduard A. van Bodegraven, Pietro Zampedri, Meidai Kasai, Marc G. Besselink, Mohammad Abu Hilal, Robot-assisted versus laparoscopic distal pancreatectomy: a systematic review and meta-analysis including patient subgroups, Surgical Endoscopy, 10.1007/s00464-023-09894-y, 37, 6, (4131-4143), (2023).
- Pengyu Li, Hanyu Zhang, Lixin Chen, Tiantong Liu, Menghua Dai, Robotic versus laparoscopic distal pancreatectomy on perioperative outcomes: a systematic review and meta-analysis, Updates in Surgery, 10.1007/s13304-022-01413-3, 75, 1, (7-21), (2022).