Safety and efficacy of GP40061 compared with originator insulin glargine (Lantus®): a randomized open-label clinical trial
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare safety (immunogenicity) and efficacy of GP40061 insulin glargine (GP-Gla) and Lantus® (Sanofi glargine, Sa-Gla) in people with diabetes mellitus. Materials & methods: This randomized open-label, 26-week clinical trial enrolled 180 Type 1 diabetes mellitus patients (HbA1c 6.5–12.0%), randomized 1:1 to once daily GP-Gla (n = 90) or Sa-Gla (n = 90). The primary end point was immune response at 26th week. Results: The frequency of immune response was similar in GP-Gla and Sa-Gla (p = 1.000). Groups were similar in terms of other safety end points. Mean HbA1c change from baseline was -0.66% for GP-Gla and -0.77% for Sa-Gla, and did not differ between groups (p = 0.326). Insulin doses, fasting plasma glucose and seven-point glucose profiles were similar between groups. Conclusion: GP-Gla and Sa-Gla demonstrated similar safety and efficacy.
ClinicalTrials.gov Identifier: NCT04022993
Diabetes mellitus (DM) is a serious medical and socioeconomic challenge that is associated with enormous economic losses in almost all countries of the world. Insulin therapy is the main method of treatment of type 1 DM (T1DM) and one of the most important options in type 2 DM (T2DM) therapy. Use of insulin products allows to achieve stable glycemic control, thereby preventing or slowing the progression of DM complications, and improving the quality of life of patients [1].
Insulin glargine was the first nonpeak long-acting human insulin analog. It is one of the most commonly used basal insulin [2]; however, it is rather expensive so there are patients and state economics that cannot afford to buy the original product. That is why pharmaceutical companies develop insulin biosimilars. A biosimilar is a biological medicine highly similar to another already approved biological medicine (the ‘reference medicine’) that is as safe and effective as the reference medicine [3]. Use of biosimilars allows reducing the economic burden without loss of treatment safety and efficacy [4]. Several biosimilar insulin glargine formulations are already available in different markets and even more formulations are currently under registration [5].
Development program of any biosimilar drug is a strictly regulated process based on a stepwise approach. In case of an insulin biosimilar studies of physical and chemical properties, in vitro pharmacodynamics studies and clinical trials are required. The goal of each step is to reveal differences between biosimilar and reference drug. Establishing biosimilarity in terms of quality characteristics and biological activity should always precede the beginning of clinical trials. Euglycemic clamp study is considered to be a pivotal efficacy study since glucose infusion rate (GIR – primary end point) is much more sensitive than HbA1c which is used as a primary end point on Phase III studies. A comparative safety (immunogenicity) and efficacy study of insulin biosimilar and reference drug is the last stage of the development program and should be considered as confirmatory (but not the pivotal) study, since the primary goal of this study is to compare immunogenicity, but not efficacy [6,7].
Russian biopharmaceutical company GEROPHARM has developed insulin glargine (GP40061 [GP-Gla]) which has the same amino acid sequence and excipients as Sanofi glargine – Lantus (Sa-Gla). Its similarity to Sa-Gla has been proved through head-to-head analytical and preclinical comparability studies. Also euglycemic clamp study had been done. All exercises had been conducted in accordance with current regulatory guidelines [6,7].
Following physiochemistry, preclinical and Phase I comparability studies, an open-label randomized active-controlled 26-week clinical trial had been run to establish similarity of GP-Gla to Sa-Gla. The aim of the study was to confirm similarity in terms of safety (immunogenicity) and to confirm similar efficacy of the drugs.
Materials & methods
Study design & treatment
This was a Phase III, randomized, multicenter, parallel group, active-controlled, open-label 26-week study, conducted in 14 centers (Supplementary Data). Eligible study participants were randomized 1:1 to once daily GP-Gla or Sa-Gla, randomization was stratified by HbA1c level at baseline (6.5–9.0% and 9.1–12.0%).
Both GP-Gla and Sa-Gla were provided to the patients in prefilled pen injectors. The initial dose of insulin glargine was determined based on previous insulin therapy. Participants were not allowed to change the type of bolus insulin they used at baseline.
The study period consisted of insulin dose titration (up to 4 weeks) and treatment period (22 weeks). During this period, the dose of both basal and bolus insulins could be changed as much as needed to achieve optimal glycemic control in patients. While daily doses were stable during treatment period. In order to keep constant blood glucose levels, participants were to measure capillary blood glucose at least four-times per day and every time they supposed to have hypoglycemic episode.
The study was registered as ClinicalTrials.gov number NCT04022993.
Study population
Eligible participants were 18–65 years old, with T1DM for at least 12 months before screening, treated with stable daily insulin doses in basal-bolus regimen for at least 30 days before screening, with HbA1c level 6.5–12.0% and body mass index (BMI) 18.5–30.0 kg/m2.
The trial included only T1DM patients since T1DM patients are considered to be a population that is more sensitive to insulin antibody formation in response to exogenous insulin administration [6,7]. Patients who were diagnosed with T1DM less than 1 year before screening were not included in the trial as their disease patterns could be different as compared with patients with longer DM duration [8].
Key exclusion criteria were history of intolerance or hypersensitivity to Sa-Gla or contraindication to it or one of its excipients previous use of any biosimilar insulin analog, severe hypoglycemia in medical history associated with seizure or loss of consciousness within the last 6 months, history of ketoacidosis or treatment for uncontrolled DM within the last 6 months. Patients with advanced stages of several DM complications (proliferative diabetic retinopathy, severe peripheral diabetic neuropathy or autonomic neuropathy, diabetic nephropathy with estimated glomerular filtration rate (eGFR) <45 ml/min/1.73-m2, diabetic foot syndrome) revealed at screening visit or earlier were not included. The full list of exclusion criteria is provided at ClinicalTrials.gov.
Immunogenicity end points
Immunogenicity outcomes were the main safety end points in this study. The primary end point was frequency of immune response development at week 26, which included:
•
An increase of anti-insulin antibody (AIA) concentration for more than 30% from baseline, for participants with AIA concentration more than 10 IU/ml at screening (positive test);
•
Any AIA concentration exceeding 10 IU/ml at week 26 for those with negative test at screening (AIA concentration of 10 IU/ml or less).
Secondary immunogenicity end points included mean AIA concentration at weeks 12 and 26, change in mean AIA concentration at weeks 12 and 26 from baseline (at screening), percentage of participants with neutralizing AIA formation in response to GP-Gla or Sa-Gla treatment.
AIA concentration was assessed via enzyme immunoassay method at screening and at weeks 12 and 26. Neutralizing activity was established via binding of insulin alfa-chain and CD220 receptor in samples of all study participants at screening and at week 26 regardless of clinical characteristics of insulin response and changes in AIA concentration to provide a more proper comparison of GP-Gla and Sa-Gla.
Efficacy end points
Efficacy end points were considered as secondary in accordance with regulatory guidance [4,5] and included:
•
HbA1c change at weeks 12 and 26 from baseline (at screening);
•
Percentage of participants who achieved an individual glycemic goal at week 26 based on HbA1c value;
•
Change of fasting plasma glucose (FPG) at weeks 12 and 26 from baseline (at screening);
•
Change in seven-point glucose profile (SPGP) at weeks 12 and 26 from baseline (at the end of titration period – week 4);
•
Change in body weight at week 26 from baseline (at screening);
•
Change in insulin dose at week 26 from baseline (at the end of titration period – week 4);
•
Change in Diabetes Treatment Satisfaction Questionnaire original status (DTSQs) test at week 26 from baseline (at randomization);
•
Results of Diabetes Treatment Satisfaction Questionnaire change version (DTSQc) test at week 26.
Investigators selected individual glycemic goal for each participant in accordance with national diabetes treatment guidance [9] at randomization visit. They did not change this goal during study periods.
SPGP was performed by participants with the use of glucometers they were given by Sponsor at screening. Participants performed SPGP at weeks 4, 12 and 26. They measured capillary blood glucose at fasting state, 2 h after breakfast, before lunch, 2 h after lunch, before dinner, 2 h after dinner and at 3 am.
DTSQs and DTSQc questionnaires measure patients’ satisfaction with current diabetes treatment. Both questionnaires consist of eight questions estimating absolute and relevant values of satisfaction for DTSQs and DTSQc, respectively.
Safety end points
In this study, we also assessed frequency and severity of adverse events, including adverse events of special interests such as hypoglycemic episodes, ketoacidosis, injection site reactions and any hypersensitivity reactions. Hypoglycemic episodes were assessed in terms of severity [1], time of event (nighttime hypoglycemia 00:00–05:59, daytime hypoglycemia 06:00–23:59) and presence of symptoms of hypoglycemia.
Statistical analysis
All data analyses were made using R version 3.5.0 for Windows software in accordance with approved statistical analysis plan. Here we perform the results of statistical analysis on full-analysis-set population.
All continuous variables are described as mean ± standard deviation (SD); all qualitative (categorical) variables are described as n (% of N). We also provide 95% confidence interval (CI) for immunogenicity end points.
We used ANCOVA to estimate changes of continuous variables from baseline. For each of these variables ANCOVA included the baseline variable value as covariate and treatment group and investigational center as fixed factors. In case we were not assessing changes from baseline, we used Student’s t-test or Mann–Whitney U-test to compare continuous variables, depending on normality of distribution. In case of inequality of variances in groups (evaluated using Levene’s test) we used Welch’s unequal variances t-test instead of Student’s t-test.
We have changed AIA values exceeding test quantification limit (100 IU/ml) to 100 IU/ml. We have additionally checked if AIA concentration at week 26, changed in AIA concentration from baseline and presence of neutralizing AIA affect treatment efficacy (HbA1c) using ANCOVA.
We compared qualitative (categorical) variables with X2-test (with continuity correction in case any unit contains value of 6–10) or with exact Fisher’s test (in case any unit contains value of 0–5). We analyze change of dichotomous variables from baseline with McNemar test.
p-value < 0.05 was accepted as statistically significant.
Sample size estimation
Since insulin immunogenicity is relatively low, there is no need to provide high study power in terms of frequency of immune response [6,7]. In comparative studies of insulin immunogenicity, sample size is estimated based on HbA1c values in accordance with regulatory guidance [6,7]. We used α level of 0.05, β level of 0.2, mean difference of 0, SD of 1.0% [10] and δ of 0.4% [11]. With these inputs, the total number of required participants was estimated as 180 (90 per group).
Regulatory & Independent Ethics Committee approval
The trial was conducted in accordance with the guidelines on Good Clinical Practice and with ethical standards for human experimentation established by the Declaration of Helsinki [12]. All study participants provided written informed consent before participating in the study. The trial was approved by Ministry of Health of Russian Federation (Clinical trial authorization number 282, 14 June 2018) and by each local independent ethics committees accordingly.
Results
Study participants
We have screened 194 study participants, and randomized 180 of them (90 to GP-Gla, 90 to Sa-Gla groups). Two participants withdrew from GP-Gla (one – participant’s decision, one – lost to follow-up) and one withdrew from Sa-Gla (participant’s decision). Figure 1 performs participants flowchart. Baseline participants’ characteristics are performed in Table 1. All baseline characteristics were comparable between groups.
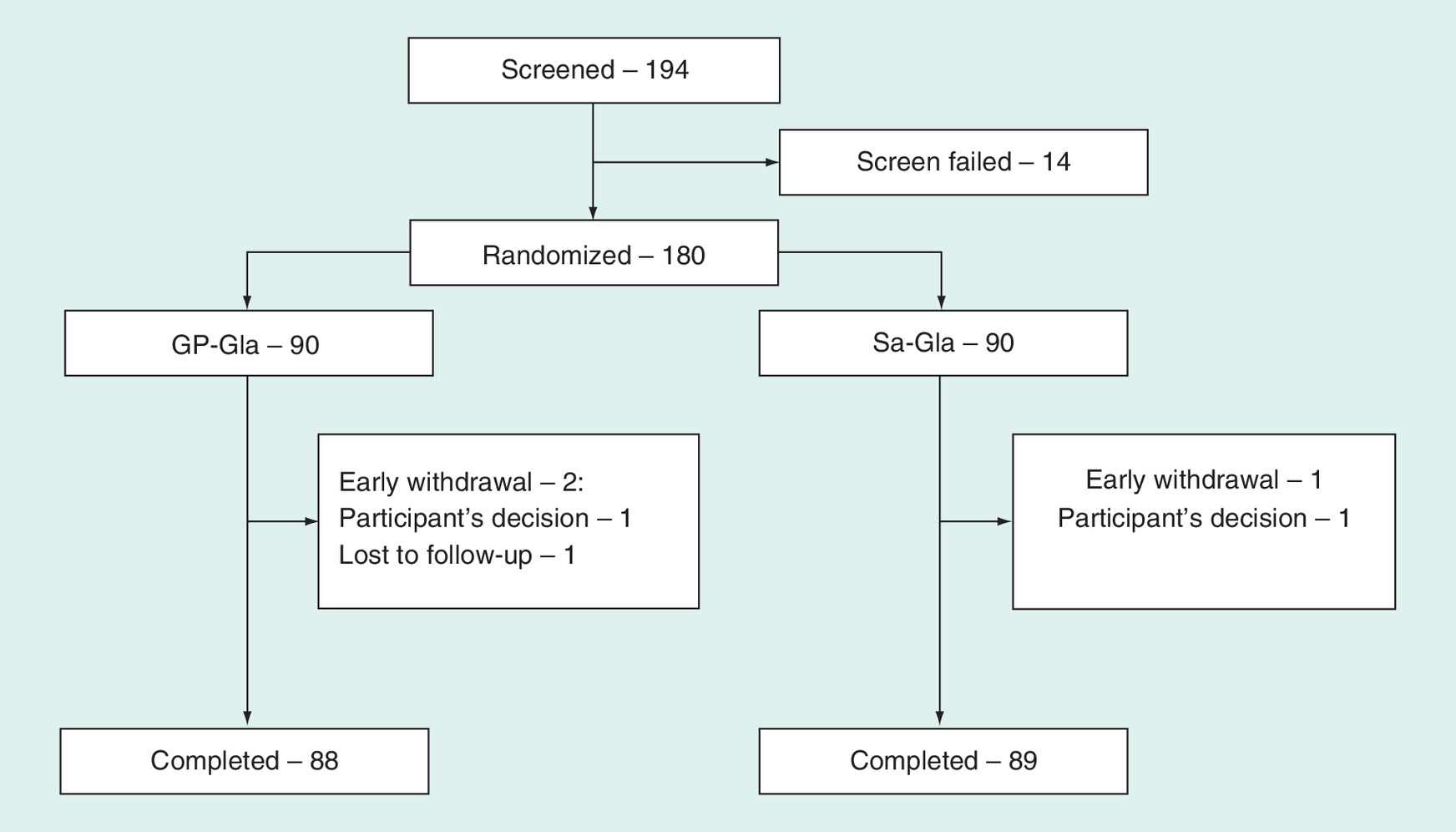
Figure 1. Participants flowchart.
GP-Gla: Insulin glargine; Sa-Gla: Sanofi glargine.
| Characteristic | GP-Gla (n = 90) | Sa-Gla (n = 90) | p-value |
|---|---|---|---|
| Age, years | 38.13 ± 10.84 | 38.90 ± 11.02 | 0.691 |
| Gender (female) | 42 (46.7%) | 43 (47.8%) | 1.000 |
| Ethnicity (Caucasian) | 90 (100%) | 90 (100%) | 1.000 |
| Bodyweight, kg | 71.52 ± 12.36 | 71.62 ± 13.01 | 0.940 |
| BMI, kg/m2 | 24.33 ± 3.11 | 24.29 ± 3.16 | 0.986 |
| Smokers • Yes • No • Previously | 12 (13.3%) 76 (84.4%) 2 (2.2%) | 20 (22.2%) 66 (73.3%) 4 (4.4%) | 0.189 |
| Duration of diabetes, years | 14.44 ± 9.85 | 13.80 ± 10.25 | 0.495 |
| HbA1c, % | 8.62 ± 1.27 | 8.68 ± 1.16 | 0.572 |
| FPG, mmol/l | 11.17 ± 4.57 | 10.62 ± 4.60 | 0.411 |
| Total insulin dose, IU/day | 48.62 ± 15.08 | 49.30 ± 15.88 | 0.769 |
| Basal insulin at screening • Glargine • Detemir • Degludec • NPH | 63 (70.0%) 9 (10.0%) 7 (7.8%) 11 (12.2%) | 71 (78.9%) 3 (3.3%) 3 (3.3%) 13 (14.4%) | 0.156 |
| Basal insulin dose, IU/day | 23.79 ± 10.25 | 24.34 ± 10.19 | 0.626 |
| Bolus insulin at screening • Lispro • Aspart • Glulisine • Human soluble | 37 (41.1%) 27 (30.0%) 18 (20.0%) 8 (8.9%) | 40 (44.4%) 28 (31.1%) 14 (15.6%) 8 (8.9%) | 0.888 |
| Bolus insulin dose, IU/day | 24.83 ± 7.79 | 24.96 ± 8.68 | 0.921 |
| AIA concentration • ≤10.0 IU/ml • >10.0 IU/ml | 86 (95.6%) 4 (4.4%) | 84 (93.3%) 6 (6.7%) | 0.747 |
| AIA concentration, IU/ml | 4.34 ± 7.66 | 5.03 ± 11.76 | 0.730 |
| Neutralizing AIA (present) | 26 (28.9%) | 27 (30.0%) | 1.000 |
| DTSQs, total score | 24.60 ± 6.98 | 25.06 ± 7.24 | 0.557 |
AIA: Anti-insulin antibody; DTSQs: Diabetes Treatment Satisfaction Questionnaire original status; FPG: Fasting plasma glucose; GP-Gla: Insulin glargine; Sa-Gla: Sanofi glargine.
Immunogenicity
There was no difference in frequency of immune response at week 26 (Table 2).
| Outcome | GP-Gla (n = 90) | Sa-Gla (n = 90) | p-value |
|---|---|---|---|
| Number of patients with criteria of immune response • At week 12 • At week 26 | 1 (1.1%) 1 (1.1%) | 1 (1.1%) 1 (1.1%) | 1.000 |
| Total number of patients with criteria of immune response by week 26 | 2 (2.2%) | 2 (2.2%) | 1.000 |
| Change of AIA concentration from baseline, IU/ml • At week 12 • At week 26 | -0.19 ± 2.49 (p = 0.519) -0.02 ± 2.85 (p = 0.624) | 1.38 ± 10.98 (p = 0.026) 0.30 ± 4.07 (p = 0.144) | 0.399 0.167 |
| Number of patients • With neutralizing AIA at screening • Developed neutralizing AIA during study period • Had neutralizing AIA disappeared by week 26 • Had neutralizing AIA both at screening and week 26 • Did not develop neutralizing AIA during study period | 23 (25.6%) 17 (18.9%) 18 (20.0%) 6 (6.7%) 47 (52.2%) | 24 (26.7%) 15 (16.7%) 18 (20.0%) 9 (10.0%) 48 (53.3%) | 1.000 Neutralizing AIA dynamics: 1.000 for GP-Gla 0.728 for Sa-Gla (McNemar test) |
AIA: Anti-insulin antibody; GP-Gla: Insulin glargine; Sa-Gla: Sanofi glargine.
Mean AIA concentration at week 12 was 4.16 ± 6.26 IU/ml in GP-Gla and 6.41 ± 16.30 IU/ml in Sa-Gla. By week 26 mean AIA concentration was 4.32 ± 7.12 IU/ml in GP-Gla and 5.33 ± 12.11 IU/ml in Sa-Gla. Changes of AIA levels by weeks 12 and 26 are performed in Table 2. Change of AIA concentration depended on AIA concentration at baseline (p < 0.001), and did not depend on investigational drug, center and visit number.
Neither AIA concentration at week 26, nor change in AIA concentration by week 26 from baseline affected treatment efficacy (p = 0.974 and p = 0.978, respectively).
The number of patients with neutralizing AIA was equal in both groups at screening. Seventeen and fifteen patients in GP-Gla and Sa-Gla, respectively, developed neutralizing AIA during study period, but none of them had any clinical signs of decreased insulin efficacy. The groups did not differ in terms of neutralizing AIA dynamics. More data on neutralizing AIA detection is performed in Table 2.
Presence of neutralizing AIA did not affect treatment efficacy (p = 0.900 for neutralizing AIA at screening, p = 0.885 for neutralizing AIA at week 26).
Efficacy
HbA1c significantly decreased from baseline at week 12 for 0.71 ± 1.03% in GP-Gla group (p < 0.001) and for 0.85 ± 1.15% in Sa-Gla group (p < 0.001). HbA1c significantly decreased from baseline at week 26 for 0.66 ± 1.01% in GP-Gla group (p < 0.001) and for 0.77 ± 1.06% in Sa-Gla group (p < 0.001). These changes did not differ between groups neither at week 12 (p = 0.308), nor at week 26 (p = 0.326). Fifteen (17%) and nineteen (21%) patients could achieve pre-established individual glycemic goal at week 26 (p = 0.529). HbA1c changes are shown in Figure 2.
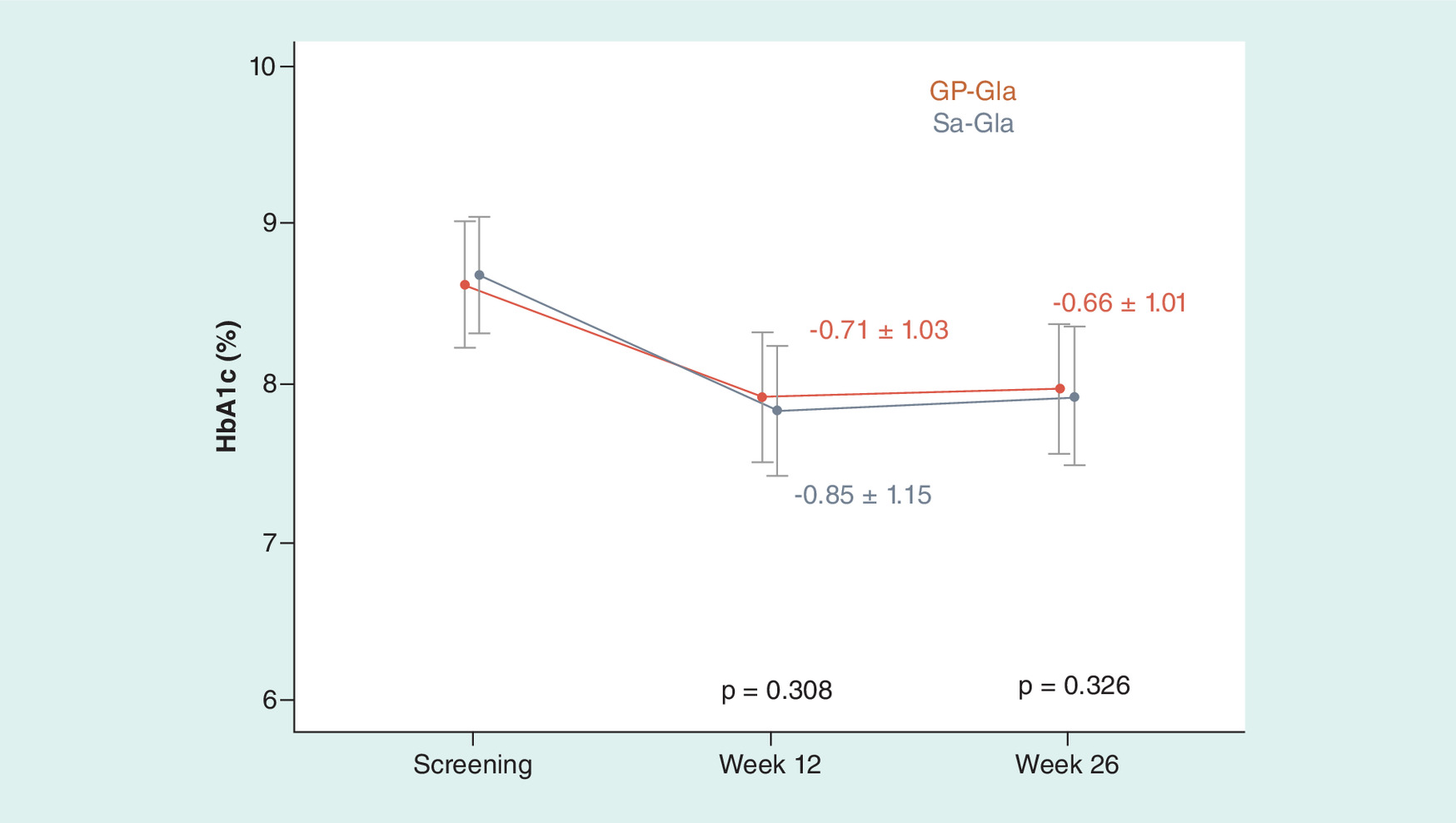
Figure 2. HbA1c changes.
GP-Gla: Insulin glargine; Sa-Gla: Sanofi glargine.
FPG changes from baseline at week 12 were insignificant: −0.26 ± 5.37 mmol/l in GP-Gla group (p = 0.583) and −0.52 ± 4.75 mmol/l in Sa-Gla group (p = 0.330). FPG decreased from baseline at week 26 for 1.30 ± 5.10 mmol/l in GP-Gla group (p = 0.023) and did not change (0.00 ± 5.71 mmol/l) in Sa-Gla group (p = 0.615). These changes did not differ between groups neither at week 12 (p = 0.330), nor at week 26 (p = 0.147). FPG changes are shown in Figure 3.
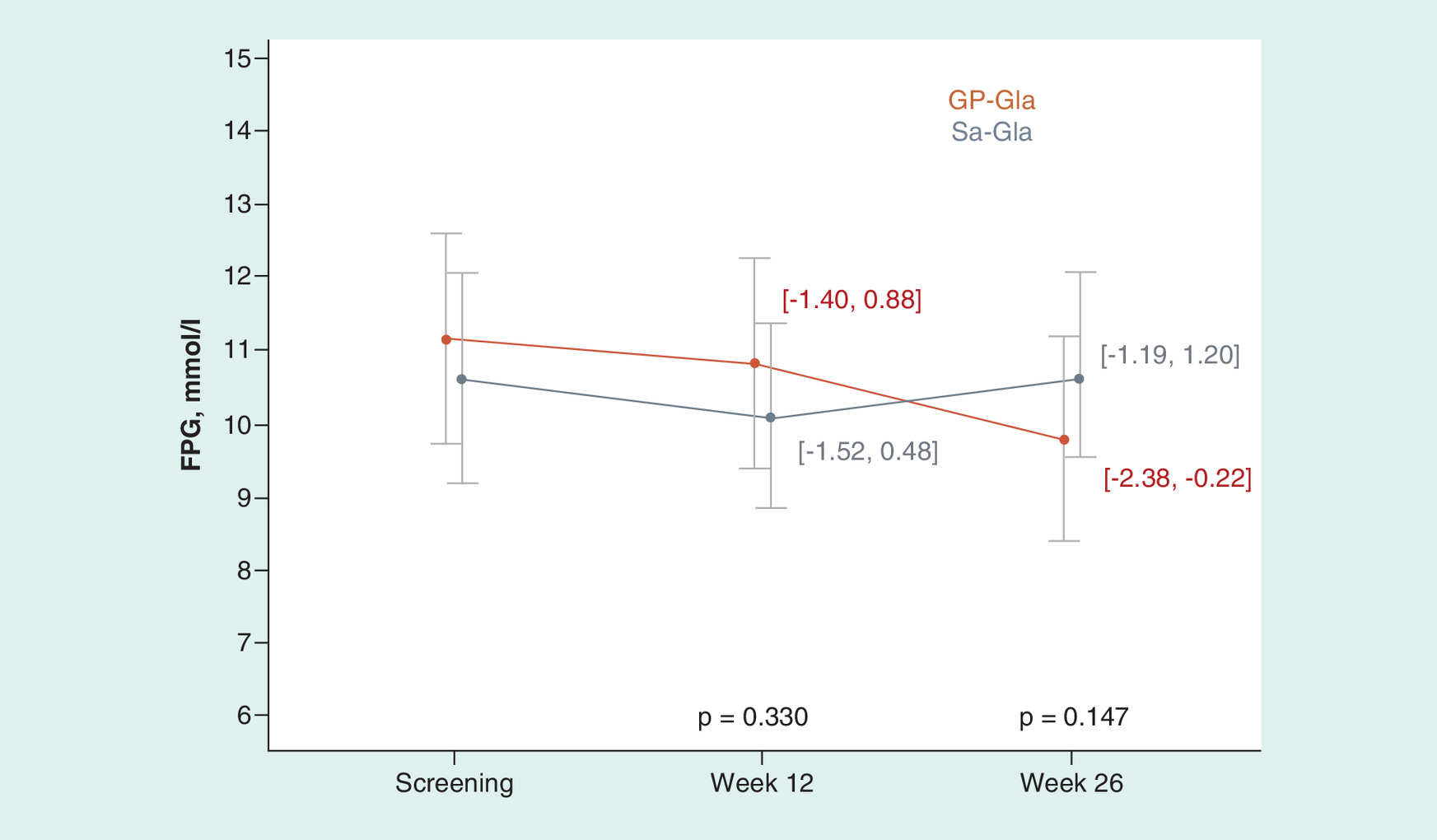
Figure 3. Fasting plasma glucose changes.
FPG: Fasting plasma glucose; GP-Gla: Insulin glargine; Sa-Gla: Sanofi glargine.
Changes in SPGP did not differ between groups neither at week 12 (p = 0.124, p = 0.063, p = 0.665, p = 0.150, p = 0.304, p = 0.658, p = 0.168 for fasting state, 2 h after breakfast, before lunch, 2 h after lunch, before dinner, 2 h after dinner and 3 am, respectively), nor at week 26 (p = 0.831, p = 0.771, p = 0.339, p = 0.315, p = 0.927, p = 0.555, p = 0.583, for above-mentioned points, respectively). Changes in SPGP are shown in Figure 4.
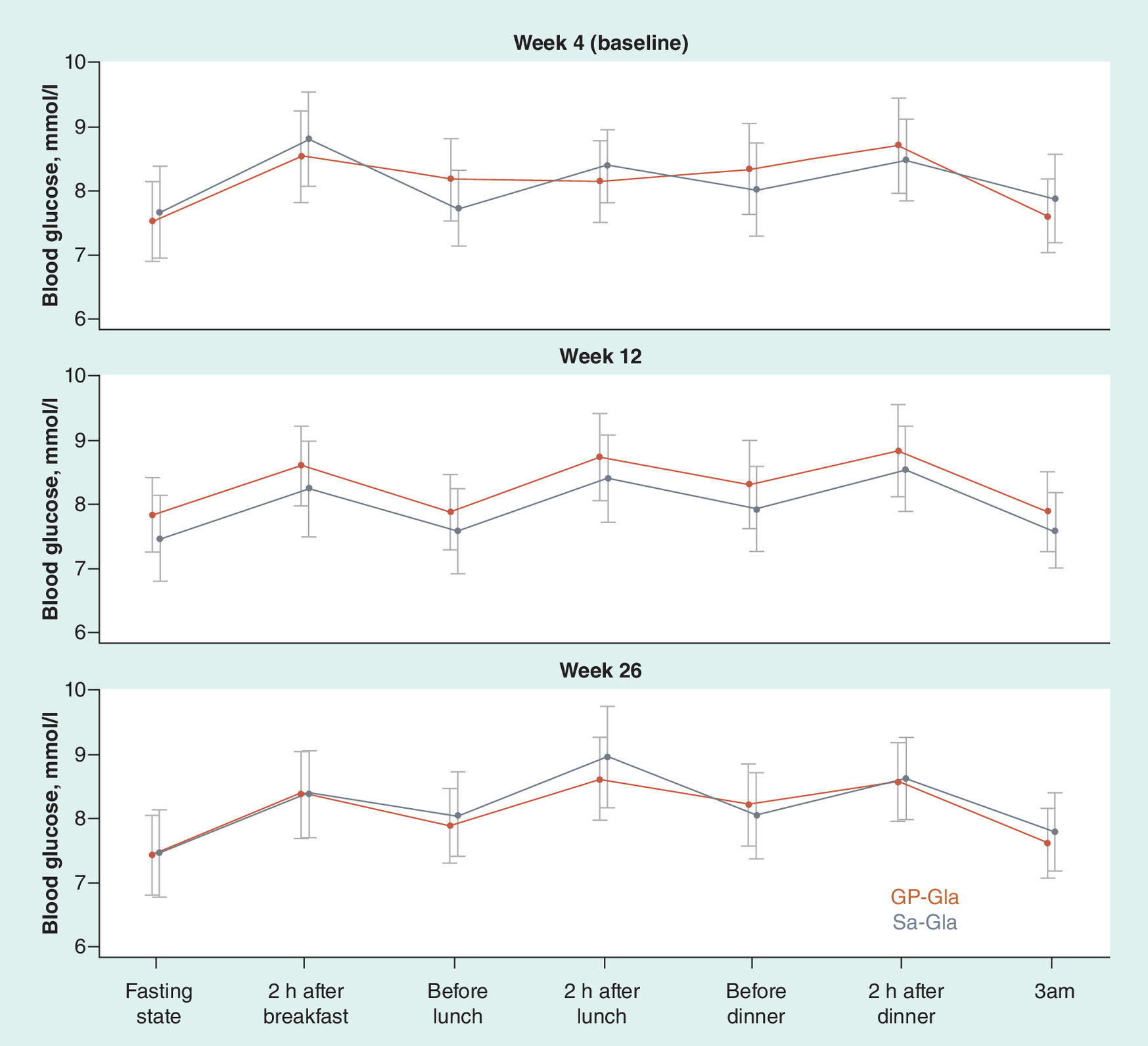
Figure 4. Seven-point glucose profile changes.
FPG: Fasting plasma glucose; GP-Gla: Insulin glargine; Sa-Gla: Sanofi glargine.
Total insulin dose did not change in both groups at week 26 as compared with week 4: 1.05 ± 5.07 IU/day in GP-Gla group (p = 0.061) and 0.18 ± 5.96 IU/day in Sa-Gla group (p = 0.774), and groups did not differ in terms of this change (p = 0.237). Changes in basal insulin dose and bolus insulin dose were also statistically insignificant and did not differ between groups (p = 0.257 and p = 0.363, respectively).
Patients in both groups had higher body weight at week 26 as compared with baseline: 0.36 ± 2.11 kg in GP-Gla group (p = 0.004) and 0.56 ± 1.99 kg in Sa-Gla group (p = 0.009). These changes did not differ between groups (p = 0.217).
Treatment satisfaction increased in both groups at week 26. The increase in DTSQs total score was 5.22 ± 7.05 points in GP-Gla group (p < 0.001) and 4.93 ± 7.18 points in Sa-Gla group (p < 0.001) and was similar between groups (p = 0.685). There was no between group difference in any questions of DTSQc.
Safety
The incidence of AEs, serious AEs, discontinuations due to AEs and adverse drug reactions reported in GP-Gla group were similar to those in the Sa-Gla group (Table 3). Relation of AEs to investigational drug exposure was assessed by investigators and was established as doubtful in all 15 cases (9 in GP-Gla group and 6 in Sa-Gla group). There was one death during the study, it occurred at screening period and was not related to study procedures or study drugs. There were four serious AEs: two in GP-Gla group and two in Sa-Gla group, all not related to study drugs. Two patients experienced three injection site reactions in GP-Gla group and one patient experienced one injection site reaction in Sa-Gla group. All these reactions were mild. No hypersensitivity reactions were observed in either group. There were no between group differences in any laboratory safety values or vital signs (data not shown).
| Adverse event | GP-Gla (n = 90) | Sa-Gla (n = 90) |
|---|---|---|
| Number of patients with one or more AEs | 16 (17.8%) | 28 (31.1%) |
| Number of AEs (total) • Mild • Intermediate • Severe | 29 21 8 0 | 41 35 6 0 |
| Number of adverse drug reactions | 9 | 6 |
| Number of serious AEs | 2 | 2 |
| Number of AEs of special interest • Injection site reactions • Hypersensitivity reactions | 3 0 | 1 0 |
AE: Adverse event; GP-Gla: Insulin glargine; Sa-Gla: Sanofi glargine.
Table 4 contains summary on hypoglycemic episodes. The number of patients experienced at least one hypoglycemic episode was similar between groups for both total number of episodes and number of episodes with different glucose values. Most patients experienced mild hypoglycemia. Daytime episodes were more frequent than nighttime episodes, and most episodes were symptomatic. We registered more hypoglycemic episodes in Sa-Gla group as compared with GP-Gla group (p < 0.001), but these episodes did not differ between groups in terms of presence of symptoms (p = 0.707) or time they occurred (p = 0.505).
| Hypoglycemic event | GP-Gla (n = 90) | Sa-Gla (n = 90) | p-value (subjects) | p-value (episodes) | ||
|---|---|---|---|---|---|---|
| Number of subjects (%) | Number of episodes | Number of subjects (%) | Number of episodes | |||
| Total | 72 (80.0) | 921 | 73 (81.1) | 1361 | 0.934 | <0.001 |
| Severity • Mild • Severe • Unknown | 72 (80.0) 4 (4.4) 9 (10.0) | 873 4 44 | 72 (80.0) 9 (10.0) 7 (7.8) | 1335 15 11 | 0.387 | <0.001 |
| Glucose value, mmol/l • <3.9 • <3.3 • <2.8 • <2.2 | 72 (80.0) 54 (60.0) 34 (37.8) 13 (14.4) | 921 436 146 23 | 73 (81.1) 63 (70.0) 42 (46.7) 15 (16.7) | 1361 677 219 46 | 1.000 0.211 0.291 0.837 | <0.001 <0.001 <0.001 0.006 |
| Symptoms • Present • Absent • Unknown | 63 (70.0) 36 (40.0) 12 (13.3) | 598 274 49 | 69 (76.7) 46 (51.1) 13 (14.4) | 904 383 74 | 0.850 | 0.707 |
| Time of the episode • Night (00:00-05:59) • Day (06:00-23:59) | 31 (34.4) 72 (80.0) | 101 820 | 38 (42.2) 72 (80.0) | 162 1199 | 0.558 | 0.505 |
GP-Gla: Insulin glargine; Sa-Gla: Sanofi glargine.
Discussion & recommendations
The study was conducted to establish similarity of GP-Gla and Sa-Gla in terms of immunogenicity and safety and to confirm similar efficacy of the drugs. Similar immunogenicity was confirmed via AIA and neutralizing AIA assessment based on all pre-established immunogenicity end points. We did not register any AIA formation that would lead to altered insulin glargine efficacy or compromised safety. AIA formation did not affect insulin demand. Both GP-Gla and Sa-Gla were generally well tolerated and there was no evidence of clinically meaningful differences with regard to their safety profiles. We would not emphasize on lower hypoglycemia incidence observed in this study, because it also depends on bolus insulin use and patients’ behavior in terms of diabetes control and dose titration. However, we can conclude that GP-Gla demonstrates at least noninferior glycemic safety as compared with Sa-Gla.
Similar efficacy was confirmed based on HbA1c level at weeks 12 and 26, and it was supported by other efficacy end points, such as FPG and SPGP. However, one should notice that five of seven SPGP points depends on bolus insulin use much more than on basal insulin action. Nevertheless, 3 am and fasting points, which reflect basal insulin activity, did not differ between groups at any visit.
Doses of GP-Gla and Sa-Gla did not change a lot during treatment period, and these changes did not differ between groups. Patients’ body weight changed similarly in both treatment groups and did not rise clinically or statistically significantly by the end of the study. The results of DTSQs and DTSQc questionnaires confirm similar treatment satisfaction with GP-Gla and Sa-Gla.
Thus, this study demonstrated a high degree of clinical similarity of study drugs. GP-Gla has been proved to be biosimilar to Sa-Gla in accordance with relevant regulatory guidance.
Future perspective
Since original biologics requires an extensive investigational program, these drugs are usually rather expensive and many patients cannot afford them without insurance programs. Biosimilar products require less clinical trials because efficacy and safety of active pharmaceutical substance has already been proved by originator product, and the main goal of all biosimilar investigational program is to show that biosimilar does not differ from original biological. A cheaper investigational program leads to possibility of establishing a lower price for biosimilar products as compared with original biologicals, and it can be crucial in some countries with expensive biological drugs. Biosimilars is the opportunity for more and more people to get access to high-quality effective drugs for their better health and better future.
Study limitations
•
•
This study was open-label, and it could influence on investigator approach to insulin dose titration. However, HbA1c level was taken as a secondary end point since it is not sensitive enough to establish similar efficacy in comparison with glucose infusion rate, estimated in euglycemic clamp studies. Blinding of these studies is impossible due to specific signs on insulin delivery systems and even not required because immunogenicity end points are objective, and open-label design cannot influence it [4,5].
•
Clinical development program of biosimilars is strictly regulated.
•
Safety (immunogenicity) and efficacy study is the last stage of a biosimilar clinical development program.
•
The primary objective of the current study was to compare immunogenicity of GP-Gla (biosimilar) and Sa-Gla (original biological).
•
A pivotal efficacy study for biosimilar insulins is euglycemic clamp study, whereas the current study is confirmatory in terms of efficacy.
•
Type 1 DM patients is the most sensitive population in terms of immunogenicity, thus they were enrolled into this study.
•
GP-Gla did not differ from Sa-Gla in terms of immunogenicity, safety and efficacy based on every established end point.
•
This study demonstrated a high degree of clinical similarity of study drugs.
Acknowledgments
The authors thank DN Alpenidze, OK Khmelnitskiy, SV Vorobiev, MA Startseva, TI Rodionova, TM Parfenova, TI Kulagina, IA Karpova, EV Arefyeva, NV Kuritsina and all investigational teams for taking part in this study. The authors also thank Unimed Laboratories and Exacte Labs for laboratory testing.
Financial & competing interests disclosure
This study was funded by OOO GEROPHARM, Russia. AA Mosikyan, IE Makarenko, OA Afonkina, TM Belikova and RV Drai are current employees of OOO GEROPHARM, Russia. TL Karonova, AY Mayorov, ST Zyangirova and AG Zalevskaya were principal investigators in this study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. The data will not be made available unless it is personally requested from the principal investigator.
Supplementary Material
File (suppl_data.docx)
- Download
- 13.41 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Dedov II, Shestakova MV, Mayorov AY et al. Standards of Specialized Diabetes Care. 9th Edition. Diabetes Mellitus 22(1S1), 1–144 (2019).
2.
Siegmund T, Tentolouris N, Knudsen ST et al. A European, multicentre, retrospective, non-interventional study (EU-TREAT) of the effectiveness of insulin degludec after switching basal insulin in a population with type 1 or type 2 diabetes. Diabetes Obes. Metab. 20(3), 689–697 (2018).
3.
Biosimilar medicines: Overview (EMA). https://www.ema.europa.eu/en/human-regulatory/overview/biosimilar-medicines-overview
4.
Mulcahy AW, Hlavka JP, Case SR. Biosimilar cost savings in the United States: initial experience and future potential. RAND Health Q. 7(4), 3 (2018).
5.
List of currently registered biosimilars in the European Union. https://www.ema.europa.eu/en/medicines/Human/ema_group_types/ema_medicine/field_ema_med_status/authorised-36/ema_medicine_types/field_ema_med_biosimilar/search_api_aggregation_ema_medicine_types/field_ema_med_biosimilar.
•• The main regulatory guidance for biosimilar insulin registration in Eurasian Economic Union.
6.
Resolution No. 89 of November 3, 2016 On Approval of the Rules for Conducting Studies of Biologicals in the Eurasian Economic Union, Chapter 15.7 Preclinical and clinical development of bioanalogous (biosimilar) medicinal products containing recombinant insulin and insulin analogues.
• The original regulatory guidance for registration of insulin biosimilars in the European Union.
7.
EMA. European Medical Agency. Guideline on non-clinical and clinical development of similar biological medicinal products containing recombinant human insulin and insulin analogues. EMEA/CHMP/BMWP/32775/2005_Rev. 1 (2015).
8.
Sokołowska M, Chobot A, Jarosz-Chobot P. The honeymoon phase - what we know today about the factors that can modulate the remission period in type 1 diabetes. Pediatr. Endocrinol. Diabetes Metab. 22(2), 66–70 (2016).
• We have provided all the medicinal features of clinical trial protocol based on the document below.
9.
Dedov II, Shestakova MV, Mayorov AYu et al. Standards of Specialized Diabetes Care. 8th Edition. Diabetes Mellitus 20(S1), 1–121 (2017).
10.
Blevins TC, Dahl D, Rosenstock J et al. Efficacy and safety of LY2963016 insulin glargine compared with insulin glargine (Lantus®) in patients with type 1 diabetes in a randomized controlled trial: the ELEMENT 1 study. Diabetes Obes. Metab. 17(8), 726–733 (2015).
11.
EMA. European Medical Agency. Guideline on clinical investigation of medicinal products in the treatment or prevention of diabetes mellitus. CPMP/EWP/1080/00 Rev. 1 (2012).
12.
World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 310, 2191–2194 (2013).
Information & Authors
Information
Published In
Pages: 263 - 273
PubMed: 32027167
Copyright
© 2020 Future Medicine Ltd.
History
Received: 10 September 2019
Accepted: 7 January 2020
Published online: 6 February 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Safety and efficacy of GP40061 compared with originator insulin glargine (Lantus®): a randomized open-label clinical trial. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0136
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Sandeep Chakravarthi Kuppirala, Somasekhar Reddy Kanala, Development and Validation of a Bridge ELISA Method for Anti-Drug Antibody Detection of Insulin Glargine, Journal of Pharmaceutical Innovation, 10.1007/s12247-026-10547-5, 21, 3, (2026).
- Xiaoxuan Xing, Lingyi Zhao, Ke Wang, Zhizhou Wang, Lan Zhang, Xianzhe Dong, Therapeutic equivalence and switching between biosimilar and reference insulins: A systematic review and meta‐analysis of randomised controlled trials, Diabetes, Obesity and Metabolism, 10.1111/dom.70328, 28, 2, (1371-1382), (2025).
- Amar D.E. van Laar, Laura Gallardo-Nuell, Sofia Pazmino Lucio, Margaretha M. Visser, Ann Mertens, Roman Vangoitsenhoven, Pieter Gillard, Ebaa Al Ozairi, Carel W. Le Roux, Jonathan Rosen, Carmen Hurtado del Pozo, Yenny Leal, José Manuel Fernández-Real, Chantal Mathieu, Nele Steenackers, Bart Van der Schueren, Trends in baseline HbA1c and body-mass index in randomised trials of people with type 1 diabetes from 1993 to 2025: an IMI2 SOPHIA systematic review and meta-analysis, eClinicalMedicine, 10.1016/j.eclinm.2025.103589, 89, (103589), (2025).
- Elena A. Christofides, Andrzej Stankiewicz, Douglas Denham, Diego Bellido, Edward Franek, Samer Nakhle, Monika Łukaszewicz, John Reed, Victoria Cózar-León, Christine Kosch, Piotr Karaś, David Fitz-Patrick, Yehuda Handelsman, Mark Warren, Priscilla Hollander, David Huffman, Philip Raskin, Tamás Oroszlán, Michael Lillestol, Fernando Ovalle, Immunogenicity, Efficacy, and Safety of Biosimilar Insulin Glargine (Gan & Lee Glargine) Compared With Originator Insulin Glargine (Lantus) in Patients With Type 1 Diabetes After 26 Weeks Treatment, Endocrine Practice, 10.1016/j.eprac.2024.06.002, 30, 9, (810-816), (2024).
- T. Yu. Demidova, V. V. Titova, Evolution of insulin therapy in the light of innovative technologies of the 21st century, Meditsinskiy sovet = Medical Council, 10.21518/ms2023-439, 23, (209-216), (2024).
- I. V. Druk, S. S. Safronova, Glycemic control and cardiovascular complications of type 2 diabetes mellitus, Meditsinskiy sovet = Medical Council, 10.21518/ms2023-222, 13, (130-140), (2023).
- S. V. Bulgakova, E. N. Saverskaya, L. A. Sharonova, Yu. A. Dolgikh, O. V. Kosareva, Biosimilar of analogue of insulin glargin: proven safety, effectiveness, interchangeability, Meditsinskiy sovet = Medical Council, 10.21518/2079-701X-2022-16-23-207-214, 23, (207-214), (2023).
- Li-Jou Yang, Ta-Wei Wu, Chao-Hsiun Tang, Tzu-Rong Peng, Efficacy and immunogenicity of insulin biosimilar compared to their reference products: a systematic review and meta-analysis, BMC Endocrine Disorders, 10.1186/s12902-022-00944-5, 22, 1, (2022).
- Thomas Danne, Lutz Heinemann, Jan Bolinder, New Insulins, Biosimilars, and Insulin Therapy, Diabetes Technology & Therapeutics, 10.1089/dia.2021.2504, 23, S2, (S-46-S-68), (2021).