Can a biomarker triage test reduce colonoscopy burden in fecal immunochemical test screening?
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the potential of biomarker triage testing (BM-TT) in the Dutch colorectal cancer (CRC) screening program. Materials & methods: Using the Adenoma and Serrated pathway to Colorectal CAncer model, we simulated fecal immunochemical test (FIT)47-screening and various FIT plus BM-TT screening scenarios in which only individuals with both a positive FIT and BM-TT are referred to colonoscopy. Results: Adding a low polyp sensitivity BM-TT to FIT-screening reduced colonoscopy burden (89–100%) while increasing CRC mortality (27–41%) compared with FIT47-screening only. The FIT plus high polyp sensitivity BM-TT scenarios also decreased colonoscopy burden (71–89%) while hardly affecting CRC mortality (FIT47 0–4% increase, FIT15 2–7% decrease). Conclusion: Adding a BM-TT to FIT-screening considerably reduces colonoscopy burden, but could also decrease screening effectiveness. Combining FIT15 with a high polyp sensitivity BM-TT seems most promising.
Although the Dutch fecal immunochemical test (FIT) based colorectal cancer (CRC) screening program is expected to be highly effective in reducing CRC burden [1], a pressing problem remains the high number of false-positive FIT results. In 2018, over 55% of FIT-positive colonoscopies, that is 79,325 procedures, yielded no lesions or only nonadvanced lesions [2]. These colonoscopies can be considered as an unnecessary burden, putting healthy individuals at risk of complications [3,4] as well as putting a strain on limited healthcare resources. This raises the question whether the selection for colonoscopy can be improved to reduce the number of unnecessary colonoscopies.
FIT is considered positive when hemoglobin levels are above a predefined cutoff. Besides hemoglobin, also other markers for precursor lesions and CRC can be detected in stool. Presently, only the Cologuard test focuses on multiple markers, that is DNA markers and haemoglobin, in stool [5]. This test requires the collection of a whole bowel movement whereas a small stool sample is sufficient for the FIT. As the Cologuard is considerably more expensive than the FIT and the logistics of such a whole stool test in a national screening program are difficult, it is not yet considered feasible to implement Cologuard in the Dutch national screening program.
Recent efforts have been focusing on identifying biomarkers within the same stool sample as taken for FIT [6,7]. These biomarkers could be used as a primary test alternative to FIT, but also as a triage test. In such a FIT plus triage test strategy, stool samples from FIT-positive individuals will be tested for additional biomarkers. Only individuals with a positive result on both the FIT and the biomarker triage test (BM-TT) are referred for diagnostic colonoscopy. Individuals with a positive FIT but negative BM-TT result return to the screening program. Such a FIT plus triage testing screening strategy could further optimize the Dutch screening program by reducing the number of unnecessary diagnostic colonoscopies. On the other hand, adding a triage test with imperfect sensitivity to FIT-screening could potentially decrease screening effectiveness as individuals with advanced neoplasia who have a positive FIT result could have a false-negative result on a BM-TT. We therefore assessed the potential of a hypothetical BM-TT to optimize a FIT-based screening program in terms of reducing colonoscopy demand without considerably decreasing screening effectiveness.
Materials & Methods
Adenoma & Serrated pathway to Colorectal CAncer model
For all analyses, we used the Adenoma and Serrated pathway to Colorectal CAncer model which is extensively described elsewhere [8]. In short, the model simulates individuals from age 20 to age 90 or death, whichever comes first. During their life, individuals have the probability of developing up to ten adenomas and/or ten serrated polyps which have certain characteristics such as location, dysplasia and histology. Progression in terms of growth in size (diminutive <6 mm, small 6–9 mm and large ≥10 mm) and development of malignant characteristics is modeled independently for each lesion. When a lesion has progressed to advanced adenoma or arises as a sessile-serrated polyp, it can progress to CRC. We assumed that 85% of CRCs arises via the adenoma-carcinoma pathway and 15% via the serrated pathway [9]. Each year, a tumor may progress to a more advanced stage or may become detected. The natural history model satisfactorily reproduces Dutch colorectal lesion prevalence rates and Dutch CRC incidence and mortality rates in the absence of screening [10,11]. The model is externally validated by replicating several long-term CRC screening trials [12].
Reference strategy
As a reference, we simulated the Dutch national CRC screening program. In this strategy, individuals aged 55–75 are biennially invited for FIT-based screening. FIT-positive individuals (≥47 μg hemoglobin per g feces) are referred for diagnostic colonoscopy, that is colonoscopy after a positive screening test, during which all detected lesions are removed with the exception of hyperplastic polyps in the rectosigmoid. Dependent on colonoscopy findings, individuals may be referred to surveillance colonoscopy according to the Dutch surveillance guideline or return to the screening program after 10 years [13].
Adherence to FIT-based screening and colonoscopy was set at 73 and 92% respectively, based on achieved participation rates in the Dutch CRC screening program in 2018 [2]. Test characteristics of the FIT with a cutoff of 47 μg/g (FIT47) were calibrated against the positivity rate and detection rate as reported by two Dutch trials evaluating FIT-based screening [8]. Colonoscopy detection rates for adenomas were based on a systematic review [14]. As the pale color, proximal location and flat appearance hamper visual detection of serrated polyps [15] we assumed a 10% lower colonoscopy detection rate for serrated polyps than for adenomas. Table 1 shows the test characteristics used in the model.
| Test | Specificity (per individual, %) | Sensitivity (per lesion, %) | ||||||
|---|---|---|---|---|---|---|---|---|
| CRC | Adenoma | Serrated polyp | ||||||
| Late | Early | Large | Small | Diminutive | Large | Small | ||
| FIT15 | 96 | 87 | 53 | 36 | 18 | ‡ | ‡ | ‡ |
| FIT47 | 97 | 85 | 50 | 29 | 11 | ‡ | ‡ | ‡ |
| Low polyp sensitivity BM-TT† | ||||||||
| – Sensitivity late CRC 80% | 90–100§ | 80 | 47 | 27 | 10 | ‡ | ‡ | ‡ |
| – Sensitivity late CRC 84% | 90–100§ | 84 | 49 | 29 | 11 | ‡ | ‡ | ‡ |
| – Sensitivity late CRC 88% | 90–100§ | 88 | 52 | 30 | 11 | ‡ | ‡ | ‡ |
| – Sensitivity late CRC 92% | 90–100§ | 92 | 54 | 31 | 12 | ‡ | ‡ | ‡ |
| – Sensitivity late CRC 96% | 90–100§ | 96 | 56 | 33 | 12 | ‡ | ‡ | ‡ |
| – Sensitivity late CRC 100% | 90–100§ | 100 | 59 | 39 | 13 | ‡ | ‡ | ‡ |
| High polyp sensitivity BM-TT | ||||||||
| – Sensitivity late CRC 80% | 90–100§ | 80 | 75 | 70 | 65 | 60¶ | 60 | 60¶ |
| – Sensitivity late CRC 84% | 90–100§ | 84 | 79 | 74 | 69 | 64¶ | 64 | 64¶ |
| – Sensitivity late CRC 88% | 90–100§ | 88 | 83 | 78 | 73 | 68¶ | 68 | 68¶ |
| – Sensitivity late CRC 92% | 90–100§ | 92 | 87 | 82 | 77 | 72¶ | 72 | 72¶ |
| – Sensitivity late CRC 96% | 90–100§ | 96 | 91 | 86 | 81 | 76¶ | 76 | 76¶ |
| – Sensitivity late CRC 100% | 90–100§ | 100 | 95 | 90 | 85 | 80¶ | 80 | 80¶ |
| – Sensitivity late CRC 100% | 90–100§ | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| Colonoscopy | 100 | 100 | 100 | 98 | 87 | 74 | 88 | 70 |
†
Test characteristics for the low polyp sensitivity BM-TT were determined as follows: specificity was set at either 90, 95, 97 and 100%. Sensitivity for late stage CRC varied between 80 and 100%, with 4% increments. Subsequently, we calculated the ratio with which the sensitivity for late stage CRC was changed compared with that of FIT. For example, when the sensitivity of late stage CRC was set at 92%, the relative increase in sensitivity compared with FIT is 8% (92 divided by 85%). Using the test characteristics of FIT as a reference point, sensitivity for early stage CRC, large adenomas and small adenomas was assumed to change with the same ratio as the sensitivity for late stage CRC. Sensitivity for diminutive and serrated polyps was set at 1 minus the specificity.
‡
Sensitivity is equal to 1 minus the specificity.
§
Specificity was set at 90, 95, 97 and 100%.
¶
We conducted a sensitivity analysis in which we assumed that the high polyp sensitivity BM-TT only has high sensitivity for large and small adenomas and large serrated polyps. That is, we assumed the sensitivity of the BM-TT for diminutive adenomas and small serrated polyps to be equal to 1 minus the specificity.
BM-TT: Biomarker triage test; CRC: Colorectal cancer; FIT: Faecal immunochemical test.
FIT plus biomarker triage test strategies
Besides a FIT-based screening strategy, we simulated a FIT plus BM-TT screening strategy in which we assumed that the BM-TT will only be performed in FIT-positive individuals. Thus, the BM-TT can only detect lesions in individuals with fecal hemoglobin levels that are above the cutoff. Furthermore, we assumed that the test can be applied on the same sample as the FIT. This ensures that screening participation is not affected as individuals do not have to undergo additional testing. For the FIT plus BM-TT screening strategy, we first evaluated 24 FIT47 plus BM-TT scenarios differing in sensitivity and specificity of the BM-TT (Table 1). Specificity was set either at 90, 95, 97% or 100%. Sensitivity for late stage CRC varied between 80 and 100%, with 4% increments. Subsequently, we calculated the ratio with which the sensitivity for late stage CRC was changed compared with that of FIT47. For example, when the sensitivity of late stage CRC was set at 92%, the relative increase in sensitivity compared with FIT47 is 8% (92 divided by 85%). Using FIT47 test characteristics as a reference point, sensitivity for early stage CRC, large adenomas and small adenomas was assumed to change with the same ratio as the sensitivity for late stage CRC. Sensitivity for diminutive adenomas and small and large serrated polyps was set at 1 minus the specificity. These 24 scenarios are considered the FIT47 plus low polyp sensitivity BM-TT scenarios.
Furthermore, we simulated 28 FIT47 plus high polyp sensitivity BM-TT scenarios in which the sensitivity for diminutive, small and large polyps of the BM-TT was substantially increased compared with the BM-TT with low polyp sensitivity. In these scenarios, we assumed the sensitivity of the BM-TT for diminutive, small and large polyps and early stage cancer to be respectively 20, 15, 10 and 5% lower (absolute difference) than that for late stage CRC. We also included FIT47 plus BM-TT scenarios in which we assumed that the BM-TT has perfect sensitivity for all polyps and CRC.
We repeated these 52 scenarios assuming a lower FIT cutoff, that is 15 μg/g. Lowering the FIT cutoff leads to a less stringent initial selection of individuals. This may increase the added value of a BM-TT if sensitivity is sufficiently high because less advanced neoplasia is missed by the primary screening instrument.
Utilities & costs
To account for the burden of screening and CRC treatment, we calculated quality-adjusted lifeyears (QALYs). For healthy individuals, we assumed a utility of 0.84 [16]. As stool-based testing is considered as noninvasive, we assumed that this test does not lead to utility losses. Furthermore, the study of Niv et al. [17] showed that colonoscopy did not affect quality of life. Therefore, we assumed no utility loss due to colonoscopy in the base-case analysis. For complications due to colonoscopy, we assumed a disutility of 0.34 during 2 weeks [18]. Table 2 shows disutilities related to screening, surveillance and CRC treatment.
| Health state | Disutility base-case analysis | Disutility sensitivity analysis | Ref. |
|---|---|---|---|
| CRC – Stage I – Stage II – Stage III – Stage IV | 0.10 0.15 0.20 0.59 | [16] | |
| Colonoscopy | 0 | 0.34† | [17,18] |
| Colonoscopy-related complications‡ | 0.34§ | [18] | |
| Cost item | Costs (2019 Euros) | Ref. | |
| FIT – Test kit – Organization – Analysis | 1.46 15.98 5.12 | [19] | |
| BM-TT | ¶ | ||
| Colonoscopy – Without polypectomy – With polypectomy – Complications after colonoscopy | 771.71 998.15 1467.22‡ | [4,20–22] Bergman Clinics (unpublished data) | |
| CRC treatment – Stage I – Stage II – Stage III – Stage IV | 28,135 44,165 58,005 43,365 | [23] |
For healthy individuals, we assumed a utility of 0.84 [16].
†
This disutility applies for 2 days.
‡
§
This disutility applies for 2 weeks.
¶
As the costs of the BM-TT are unknown, we set the costs to 10, 25, 50, 100, 150 and 200% of the costs of colonoscopy.
BM-TT: Biomarker triage test; CRC: Colorectal cancer; FIT: Fecal immunochemical test.
Costs were determined from a healthcare payer perspective and included costs related to screening, surveillance and CRC treatment (Table 2). Costs were converted to 2019 Euros using the consumer price index for that year [24]. As costs of the BM-TT are unknown, we varied the costs using the costs of colonoscopy as a reference since the purpose of the BM-TT is to reduce the number of unnecessary colonoscopies. That is, we set the costs of the BM-TT to 10, 25, 50, 100, 150 and 200% of the costs of colonoscopy.
Analyses
For each scenario, we simulated a cohort of 20,000,000 individuals and calculated the number of CRC cases and deaths, colonoscopy burden, lifeyears, QALYs, costs and net monetary benefit. Colonoscopy burden was indicated by the number of colonoscopies (both diagnostic and surveillance) as well as the number of negative diagnostic colonoscopies for each scenario. Net monetary benefit (NMB) was calculated as (total QALYs x threshold) – total cost, using the Dutch gross domestic product per capita (€35,916) as threshold [24]. We applied a 3% discount rate to the effects and costs from age 50 onwards [25].
All FIT plus BM-TT scenarios were compared with the reference strategy consisting of FIT47-based screening with respect to CRC incidence and mortality rates, colonoscopy burden, lifeyears and QALYs. Furthermore, we calculated incremental QALYs per averted colonoscopy to simultaneously consider both screening effectiveness and colonoscopy burden as well as the incremental NMB to gain insight in the cost–effectiveness of FIT plus BM-TT scenarios compared with FIT-screening only.
Sensitivity analyses
In one-way sensitivity analyses, we set the utility loss due to colonoscopy at 0.34 during 2 days, based on previous cost–effectiveness analyses [18]. Furthermore, we evaluated scenarios in which we assumed that the high polyp sensitivity BM-TT only has high sensitivity for large and small adenomas and large serrated polyps (Table 1). Thus, sensitivity for diminutive adenomas and small serrated polyps was not increased.
Results
Colonoscopy burden
Table 3 shows the summary results for the base-case analysis whereas a more detailed overview is provided in the Supplementary Material. When a BM-TT with low polyp sensitivity was added to FIT47-screening, the number of required colonoscopies decreased to 150–228 in the lifetime of a cohort of 1000 individuals (58–72% decrease compared with FIT47-screening only). The number of diagnostic colonoscopies in which no polyps were detected ranged between 0 and 11 (89–100% decrease). This decrease in colonoscopy burden was slightly lower for the FIT15 plus low polyp sensitivity BM-TT scenarios.
| Strategy | Number of colonoscopies | Number of negative diagnostic colonoscopies | CRC deaths | Discounted QALYs | Incremental QALYs per averted colonoscopy |
|---|---|---|---|---|---|
| FIT47 | 542 | 101 | 13.5 | 16,330 | Reference |
| FIT47 plus low polyp sensitivity BM-TT† | 150–228 | 0–11 | 17.1–19.1 | 16,304–16,313 | -0.066 to -0.055 |
| FIT47 plus high polyp sensitivity BM-TT‡ | 416–467 | 11–25 | 13.5–14.1 | 16,327–16,330 | -0.024 to 0.002 |
| FIT15 plus low polyp sensitivity BM-TT† | 177–269 | 1–13 | 16.2–18.4 | 16,307–16,317 | -0.062 to -0.048 |
| FIT15 plus high polyp sensitivity BM-TT‡ | 475–535 | 13–29 | 12.6–13.2 | 16,331–16,335 | 0.023–0.644 |
Outcomes are reported for the lifetime of a cohort of 1000 individuals.
†
Test characteristics for the low polyp sensitivity BM-TT were determined as follows: specificity was set at either 90, 95, 97 and 100%. Sensitivity for late stage CRC varied between 80 and 100%, with 4% increments. Subsequently, we calculated the ratio with which the sensitivity for late stage CRC was changed compared with that of FIT. For example, when the sensitivity of late stage CRC was set at 92%, the relative increase in sensitivity compared with FIT is 8% (92 divided by 85%). Using the test characteristics of FIT as a reference point, sensitivity for early stage CRC, large adenomas and small adenomas was assumed to change with the same ratio as the sensitivity for late stage CRC. Sensitivity for diminutive and serrated polyps was set at 1 minus the specificity.
‡
These scenarios assumed high polyp sensitivity for the BM-TT. Specificity was set at either 90, 95, 97 and 100%.
BM-TT: Biomarker triage test; CRC: Colorectal cancer; FIT: Faecal immunochemical test; QALY: Quality-adjusted lifeyear.
For the FIT47 plus high polyp sensitivity BM-TT scenarios, the number of lifetime colonoscopies per 1000 individuals varied between 416 and 467 (14–23% decrease) whereas the number of negative diagnostic colonoscopies ranged between 11 and 25 (75–89% decrease). The FIT15 plus high polyp sensitivity BM-TT scenarios led to slightly smaller decreases in colonoscopy burden.
Screening effectiveness
The decrease in colonoscopy burden came at the cost of a decrease in screening effectiveness for all FIT47 plus low polyp sensitivity BM-TT scenarios and the majority of the FIT47 plus high polyp sensitivity BM-TT scenarios (Table 3 & Supplementary Material). Depending on the test characteristics of the low polyp sensitivity BM-TT that was added to FIT47-screening, the number of lifetime CRC deaths ranged between 17.1 and 19.1 in a cohort of 1000 individuals. This equals to a 27–41% increase in CRC deaths compared with FIT47-screening only. FIT47-screening led to 16,330 QALYs in a cohort of 1000 individuals. This decreased to 16,304–16,313 QALYs when a BM-TT with low polyp sensitivity was added to FIT47-screening.
For the FIT47 plus high polyp sensitivity BM-TT scenarios, the increase in lifetime CRC deaths was 0–4.4% whereas QALYs decreased with 0–3 per 1000 individuals. Thus, adding a BM-TT with high polyp sensitivity to FIT47-screening led to a smaller reduction in colonoscopy burden than adding a BM-TT with low polyp sensitivity. On the other hand, screening effectiveness only slightly decreased. In fact, when the BM-TT had perfect sensitivity for polyps and CRC, screening effectiveness did not decrease.
Also for the FIT15 plus low sensitivity BM-TT scenarios, screening effectiveness decreased compared with FIT47-screening only. In contrast, the FIT15 plus high polyp sensitivity BM-TT scenarios led to a reduction in colonoscopy burden as well as an increase in screening effectiveness compared with FIT47-screening only. Depending on BM-TT test characteristics, CRC mortality decreased with 2.2–6.6% whereas QALYs increased with 1–5 per 1000 individuals.
To simultaneously consider colonoscopy burden and screening effectiveness, we calculated incremental QALYs per averted colonoscopy. For the FIT47 plus low polyp sensitivity BM-TT scenarios, each averted colonoscopy led to a 0.055–0.066 QALY decrease in screening effectiveness. For the FIT47 plus high polyp sensitivity BM-TT scenarios, incremental QALYs per averted colonoscopy ranged between -0.024 and 0.002 QALYs compared with FIT47-screening only. For the FIT15 plus low polyp sensitivity BM-TT, incremental QALYs per averted colonoscopy were comparable to the FIT47 plus low polyp sensitivity BM-TT. In contrast, incremental QALYs per averted colonoscopy were 0.023–0.644 QALYs for the FIT15 plus high polyp sensitivity BM-TT. Note that this reflects an increase in screening effectiveness per averted colonoscopy.
Cost–effectiveness
Figure 1 shows the incremental NMB for the FIT plus triage test scenarios compared with FIT47-screening only for different costs of the BM-TT. When the costs for the BM-TT are varied between 77 and 1543 Euros, that is between 10 and 200% the costs of colonoscopy, all FIT15 plus high polyp sensitivity BM-TT scenarios and some of the FIT47 plus high polyp sensitivity BM-TT scenarios led to a positive incremental NMB, indicating that these scenarios are considered cost effective at a willingness-to-pay threshold of €35,916. All scenarios in which a low-polyp sensitivity BM-TT is added to FIT-screening led to a negative incremental NMB, indicating that these scenarios are not cost effective compared with FIT47-screening only.
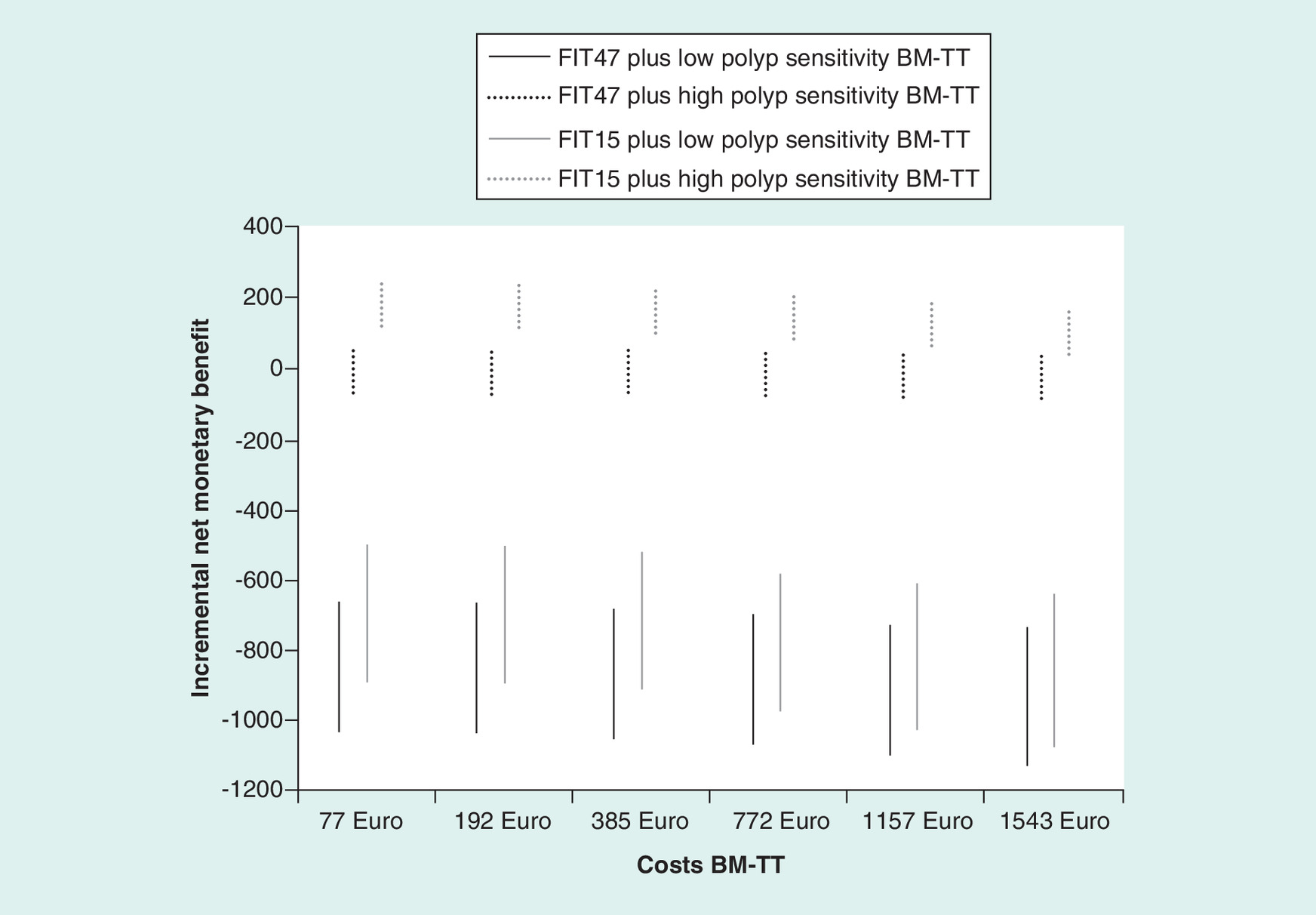
Figure 1. Incremental NMB for FIT plus BM-TT screening compared with FIT47 screening only, for different costs of the BM-TT.
As the costs of the BM-TT are unknown, we set the costs to 10, 25, 50, 100, 150 and 200% of the costs of colonoscopy. An incremental NMB >0 indicates that FIT plus BM-TT screening is considered cost effective compared with FIT47 screening only at a threshold of €35,916.
BM-TT: Biomarker triage test; FIT: Fecal immunochemical test; NMB: Net monetary benefit.
Sensitivity analyses
The Supplementary Material shows the results of the sensitivity analyses. Repeating the base-case analysis assuming that colonoscopy led to a utility loss did not impact the discounted QALYs per 1000 individuals. The FIT plus high polyp sensitivity BM-TT scenarios in which the BM-TT only had high sensitivity for small and large adenomas and large serrated polyps led to a greater reduction in colonoscopy burden compared with the FIT plus high polyp sensitivity BM-TT scenarios in which the BM-TT has high sensitivity for polyps of all sizes. On the other hand, screening effectiveness was more decreased. When comparing these scenarios in terms of incremental QALYs per averted colonoscopy, figures were more favourable for the FIT plus high polyp sensitivity scenarios in which the BM-TT had high sensitivity for polyps of all sizes.
Discussion
This study evaluated the potential of a hypothetical BM-TT to optimize the Dutch FIT-based CRC screening program by reducing the number of unnecessary colonoscopies without affecting screening effectiveness. According to model predictions, the number of unnecessary colonoscopies decreased considerably when a BM-TT with low polyp sensitivity was added to FIT-based screening. However, this came at the cost of lower screening program effectiveness. To fully evaluate the potential of a BM-TT in FIT-based screening, we also considered scenarios in which the polyp sensitivity of the BM-TT was substantially increased, in other words, ≥60, ≥65 and ≥70% sensitivity for diminutive, small polyps and large polyps, respectively. For these FIT plus high polyp sensitivity BM-TT scenarios, the number of unnecessary colonoscopies was markedly reduced while screening effectiveness was hardly affected (FIT47 plus high polyp sensitivity BM-TT) or even increased (FIT15 plus high polyp sensitivity BM-TT) compared with current FIT47 screening.
As per definition, adding a triage test with imperfect sensitivity will decrease screening program effectiveness in terms of mortality reduction [26], which is also shown in this study. This is due to the fact that individuals with adenomas or CRC can have a positive FIT result but a false-negative result on the BM-TT and thus, are not referred to colonoscopy. Adding a BM-TT to FIT-based screening could only be an acceptable approach to reduce the number of unnecessary colonoscopies when polyp sensitivity of the BM-TT is substantially improved compared with FIT. Adding such a high polyp sensitivity BM-TT to FIT with a low cut-off (FIT15) has the potential to reduce colonoscopy burden as well as increase screening effectiveness. However, a test with such high polyp sensitivity would have the most impact on CRC burden when used as a primary screening test.
To our knowledge, the stool test with the highest polyp sensitivities is currently the Cologuard with sensitivities varying from 20% for diminutive advanced polyps to 45% for large advanced polyps [5]. Due to the high costs of Cologuard, primary Cologuard screening is not cost effective compared with FIT-based screening [27]. The potential of Cologuard as triage test in terms of cost–effectiveness has not been studied so far. Nevertheless, our study indicates that Cologuard will not be cost-effective as the triage test as the sensitivities are considerably lower than the ≥60% polyp sensitivity we considered for the high polyp sensitivity BM-TT. To determine the optimal, most cost-effective position of new biomarker tests in a screening program, in other words, as primary test or as triage test in FIT-positive individuals, costs and effects should be carefully balanced in extensive cost–effectiveness analyses.
It could be questioned whether a biomarker test with high polyp sensitivity is desirable as it will detect numerous nonadvanced lesions, which are generally considered at low risk to progress to CRC [28]. CRC screening models, including the the Adenoma and Serrated pathway to Colorectal CAncer model, currently assume that each diminutive polyp has a probability to progress to CRC. Based on the recent studies, it is hypothesized that only a small group of polyps with specific molecular aberrations will progress to CRC [28]. If a biomarker test could only identify those polyps, this would considerably decrease overdiagnosis and overtreatment. To evaluate such tests would require detailed modeling which is beyond the scope of this study.
The BM-TT can only detect lesions in individuals with fecal hemoglobin levels that are above the cutoff, as only FIT-positive individuals will undergo triage testing. In addition, we assumed that FIT and the stool-based BM-TT are independent tests. Biomarkers can originate from exfoliated tumor cells and therefore may be tumor-specific. However, it may be hypothesized that bleeding polyps will, besides hemoglobin, also secrete other biomarkers such as blood-derived proteins. If the result of the biomarker triage test is dependent on the result of the FIT, we may have overestimated the effectiveness of a FIT plus BM-TT strategy.
It is also possible to subject FIT-positive individuals to a triage test that is not stool-based, for example, a blood-based test or computed tomography (CT) colonography. The current study shows that also for these tests, polyp sensitivity should be >60%. Preliminary findings indicate that the blood-based test developed by (CellMax Life, CA, USA) which focuses on the detection of ctDNA in blood, may reach >75% sensitivity for polyps at a 97.3% specificity [29]. High polyp sensitivities (>90%) were also reported by a study evaluating CT colonography as a triage test in FIT-positive individuals [30]. It should be kept in mind that triage testing by means of a blood-based test or CT colonography requires FIT-positive individuals to perform a separate test. It is expected that not all FIT-positive individuals will participate in additional triage testing as this means that they have to make a (substantial) effort to perform the triage test, thereby lowering screening effectiveness.
Instead of considering the FIT result as a dichotomous outcome, it is also possible to handle the FIT result as a continuous outcome. Nielsen et al. [31] propose to subject individuals with a negative FIT result who score just below the cutoff point to a triage test. This would decrease the number of individuals with advanced neoplasia missed by screening. A similar approach could be applied to individuals who score just above the FIT cutoff point to decrease the number of unnecessary colonoscopies. This should be a topic of further research.
Conclusion
To conclude, the development of stool-based biomarker tests is of broad and current interest. Adding a biomarker triage test with low polyp sensitivity to FIT-based screening can be a means to decrease the number of unnecessary colonoscopies but comes at the cost of decreased screening effectiveness. In order to maintain current screening effectiveness at a reduced colonoscopy burden, the combination of a lower FIT cutoff with a biomarker triage test that has high polyp sensitivity (≥60% polyp sensitivity) seems most promising. Nevertheless, such a biomarker test may also hold promise as a primary screening test. A full cost–effectiveness comparison is required to determine the optimal position of new biomarker tests in the screening program.
•
Biomarker triage testing on the stool samples of fecal immunochemical test (FIT)-positive individuals and referring only those individuals with a double positive test result to colonoscopy, has the potential to substantially reduce the number of unnecessary colonoscopies.
•
However, unless the sensitivity of such a biomarker triage test is ≥60% for colorectal polyps, such a strategy leads to a decreased screening effectiveness, in other words, higher CRC incidence and mortality rates, compared with FIT-based screening only.
•
To achieve both a lower colonoscopy referral rate as well as increased screening effectiveness, a highly sensitivity biomarker triage test (≥60% polyp sensitivity) together with a lowered FIT cutoff is required.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Financial & competing interests disclosure
Financial support for this study was provided by a SU2C-DCS International Translational Cancer Research Dream Team Grant (SU2C-AACR-DT1415, MEDOCC). Stand Up To Cancer is a program of the Entertainment Industry Foundation administered by the American Association for Cancer Research. B Carvalho, M de Wit, VMH Coupé and GA Meijer have several patents pending. GA Meijer also reports grants from AACR during the conduct of the study, nonfinancial support from Exact Sciences, nonfinancial support from Sysmex, other from Royal Philips, other from GlaxoSmithKline, other from Keosys SARL, other from Open Clinica LLC, other from Roche Diagnostics Nederland BV, other from The Hyve BV, other from Open Text, other from SURFSara BV, other from Vancis BV, other from CSC Computer Sciences BV and nonfinancial support from Sentinel CH SpA outside the submitted work. E Dekker has endoscopic equipment on loan of FujiFilm and receives a research grant from FujiFilm. She has received an honorarium for consultancy from FujiFilm, Tillots and Olympus and a speakers’ fee from Olympus and Roche. Besides, she is in the supervisory board of eNose. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (suppl_file.docx)
- Download
- 38.29 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Greuter MJE, Demirel E, Lew J-B et al. Long-term impact of the Dutch colorectal cancer screening program on cancer incidence and mortality-model-based exploration of the serrated pathway. Cancer Epidemiol. Biomarkers Prev. 25(1), 135–144 (2016).
2.
Rijksintituut voor Volksgezondheid en Milieu. Monitoring evaluatie bevolkingsonderzoek darmkanker (2018). www.iknl.nl/getmedia/35d96a38-d019-4846-b7ac-b000ddff9a1a/2018_Monitor-darmkanker_definitief.pdf
3.
de Wijkerslooth TR, de Haan MC, Stoop EM et al. Burden of colonoscopy compared to non-cathartic CT-colonography in a colorectal cancer screening programme: randomised controlled trial. Gut 61(11), 1552–1559 (2012).
4.
Rex DK, Petrini JL, Baron TH et al. Quality indicators for colonoscopy. Gastrointest. Endosc. 63(Suppl. 4), S16–S28 (2006).
5.
Imperiale TF, Ransohoff DF, Itzkowitz SH et al. Multitarget stool DNA testing for colorectal-cancer screening. N. Engl. J. Med. 370(14), 1287–1297 (2014).
• Cologuard will not be cost effective the as triage test as the sensitivities are considerably lower than the ≥60% polyp sensitivity we considered for the high polyp sensitivity biomarker triage testing.
6.
Bosch LJW, de Wit M, Pham TV et al. Novel stool-based protein biomarkers for improved colorectal cancer screening: a case–control study. Ann. Intern. Med. 167(12), 855–866 (2017).
•• The development of stool-based biomarker tests is of broad and current interest.
7.
Bosch LJW, Mongera S, Terhaar Sive Droste JS et al. Analytical sensitivity and stability of DNA methylation testing in stool samples for colorectal cancer detection. Cell. Oncol. Dordr. 35(4), 309–315 (2012).
8.
Greuter MJ, Xu X-M, Lew J-B et al. Modeling the adenoma and serrated pathway to colorectal cAncer (ASCCA). Risk Anal. 34(5), 889–910 (2014).
9.
IJspeert JEG, Vermeulen L, Meijer GA, Dekker E. Serrated neoplasia-role in colorectal carcinogenesis and clinical implications. Nat. Rev. Gastroenterol. Hepatol. 12(7), 401–409 (2015).
10.
Stoop EM, de Haan MC, de Wijkerslooth TR et al. Participation and yield of colonoscopy versus non-cathartic CT colonography in population-based screening for colorectal cancer: a randomised controlled trial. Lancet Oncol. 13(1), 55–64 (2012).
11.
IKNL. Cijfers over kanker (2011). www.cijfersoverkanker.nl/
12.
Lew JB, Greuter MJE, Caruana M et al. Validation of microsimulation models against alternative model predictions and long-term colorectal cancer incidence and mortality outcomes of randomised-controlled trials. Submitted to Med Decis Making. [Unpublished Data, 2019].
13.
Nederlandse Vereniging van Maag-, Darm- en Leverartsen. Nederlandse Richtlijn Coloscopie Surveillance (2013). www.mdl.nl/sites/www.mdl.nl/files/richlijnen/Richtlijn_Coloscopie_Surveillance_definitief_2013.pdf
14.
van Rijn JC, Reitsma JB, Stoker J, Bossuyt PM, van Deventer SJ, Dekker E. Polyp miss rate determined by tandem colonoscopy: a systematic review. Am. J. Gastroenterol. 101(2), 343–350 (2006).
15.
Leggett B, Whitehall V. Role of the serrated pathway in colorectal cancer pathogenesis. Gastroenterology 138(6), 2088–2100 (2010).
16.
Ness RM, Holmes AM, Klein R, Dittus R. Utility valuations for outcome states of colorectal cancer. Am. J. Gastroenterol. 94(6), 1650–1657 (1999).
17.
Niv Y, Bogolavski I, Ilani S et al. Impact of colonoscopy on quality of life. Eur. J. Gastroenterol. Hepatol. 24(7), 781–786 (2012).
18.
Cenin DR, Naber SK, de Weerdt AC et al. Cost–effectiveness of personalized screening for colorectal cancer based on polygenic risk and family history. Cancer Epidemiol. Biomark. Prev. 29(1), 10–21 (2020).
19.
Health Council of the Netherlands. Population Screening Act: national population screening programme for bowel cancer. The Hague: Health Council of the Netherlands (2009). Publication no. 2009.13. www.gezondheidsraad.nl/documenten/adviezen/2009/11/17/bevolkingsonderzoek-naar-darmkanker
20.
Lüning TH, Keemers-Gels ME, Barendregt WB, Tan ACITL Rosman C. Colonoscopic perforations: a review of 30,366 patients. Surg. Endosc. 21(6), 994–997 (2007).
21.
Nederlandse Zorgautoriteit (2013). www.nza.nl/regelgeving/tarieven
22.
Whitlock EP, Lin JS, Liles E, Beil TL, Fu R. Screening for colorectal cancer: a targeted, updated systematic review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 149(9), 638–658 (2008).
23.
Tilson L, Sharp L, Usher C et al. Cost of care for colorectal cancer in Ireland: a health care payer perspective. Eur. J. Health Econ. 13(4), 511–524 (2012).
24.
Central Bureau for Statistics (2019). www.cbs.nl
25.
Siegel JE, Torrance GW, Russell LB, Luce BR, Weinstein MC, Gold MR. Guidelines for pharmacoeconomic studies. Recommendations from the panel on cost–effectiveness in health and medicine. Panel on cost–effectiveness in health and medicine. Pharmacoeconomics 11(2), 159–168 (1997).
26.
Solomon D. Chapter 14: role of triage testing in cervical cancer screening. JNCI Monogr. 2003(31), 97–101 (2003).
• Triage testing is used in other screening programs to reduce screening burden.
27.
Ladabaum U, Mannalithara A. Comparative effectiveness and cost effectiveness of a multitarget stool DNA test to screen for colorectal neoplasia. Gastroenterology 151(3), 427–439.e6 (2016).
28.
Carvalho B, Diosdado B, Terhaar Sive Droste JS et al. Evaluation of cancer-associated DNA copy number events in colorectal (advanced) adenomas. Cancer Prev. Res. 11(7), 403–412 (2018).
29.
Wen-Sy Tsai AN, Chang Gung Memorial Hospital T, Johns Hopkins Hospital B et al. Prospective clinical study of circulating tumor cells for colorectal cancer screening (2018). https://meetinglibrary.asco.org/record/155738/abstract
30.
Liedenbaum MH, van Rijn AF, de Vries AH et al. Using CT colonography as a triage technique after a positive faecal occult blood test in colorectal cancer screening. Gut 58(9), 1242–1249 (2009).
•• Computed tomography colonography is unlikely to be an efficient triage technique in fecal immunochemical test-based screening.
31.
Nielsen HJ, Christensen IJ, Andersen B et al. Serological biomarkers in triage of FIT-positive subjects? Scand. J. Gastroenterol. 52(6–7), 742–744 (2017).
•• Preliminary results of a triage test using serological biomarkers in fecal immunochemical test-positive individuals.
Information & Authors
Information
Published In
Pages: 563 - 571
PubMed: 32462913
Copyright
© 2020 Future Medicine Ltd.
History
Received: 26 August 2019
Accepted: 17 March 2020
Published online: 28 May 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Can a biomarker triage test reduce colonoscopy burden in fecal immunochemical test screening?. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0130
Export citation
Select the citation format you wish to export for this article or chapter.