Comparative analysis of cost–effectiveness between isosorbide-5-mononitrate and isosorbide: a retrospective real-world evaluation
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The cost–effectiveness of isosorbide-5-mononitrate (5-ISMN) and isosorbide dinitrate (ISDN) in real-world use in patients with coronary heart disease (CHD; either angina pectoris or myocardial infarction) was retrospectively compared. Method: In this retrospective real-world evaluation, patients with established CHD satisfying the following criteria were selected from information system of two tertiary hospitals in China: with pharmacy claiming for at least one injection of 5-ISMN or ISDN between July 2008 and May 2017; and, CHD patients. By using propensity score matching (PSM), we compared clinical aspects of efficacy, safety, length of hospital stay and cost during hospitalization between 5-ISMN and ISDN group. All data were processed by R statistical package v.2.13.1 (R Foundation for Statistical Computing, Vienna, Austria). Result: Of 5609 patients selected, 4047 received 5-ISMN and 1562 received ISDN. After PSM, we acquired 1555 pairs based on balancing of age, sex, insurance and comorbidities on admission. The frequency (4.2 ± 6.6-times vs 6.5 ± 9.5-times; p < 0.05) and total dosage (47.5 ± 153.4 vs 136.4 ± 261.0 mg; p < 0.05) of sublingual nitroglycerin use decreased and hypotension incidence lowered (8.0 vs 13.0%; p < 0.05) in 5-ISMN group compared with ISDN group. Hospital stay (16.0 ± 11.3 days vs 17.7 ± 13.2; p < 0.05) and hospitalization expenditure ([the ratio of cost in the study to the average hospitalization cost in the city] [odds ratio: 2.5 vs 2.6; p < 0.05]) were reduced in 5-ISMN group as with that of ISDN group. Moreover, the main component of hospitalization cost was medical consumables and medications in both the groups. Conclusion: In the present retrospective real-world evaluation, by using PSM analysis, we found that newer injection agent of 5-ISMN was associated with fewer use of sublingual nitroglycerin, less hypotension incidence, shorter length of hospital stay and less hospitalization expenditure related to its comparator ISDN in patients with established CHD. Further evaluation and clinical experience are need in different circumference for the usage of ISDN.
In 1990s, disability-adjusted life years (DALYs) have been proposed as the comprehensive index for the assessment of global burden of disease (GBD) by the WHO. Globally, the DALYs of noncommunicable disease (NCD) account for >60% of GBD [1]. Cardiovascular disease (CVD) represents 24% of NCD-related DALYs. Coronary heart disease (CHD) is the most common and new type of CVD [2] and is the leading cause of death worldwide, especially in Asia. Asia is rapidly becoming the epicenter for CHD in the world. It is estimated that >60% of GBD occurs in developing countries, with the majority occurring in Asia [3,4]. According to data from China Health and Family Planning Commission’s Statistical Yearbook, CHD has affected >10 million people in China [5]. In 2014, the mortality rate of CHD was 107.5 per 100,000 in urban areas and 105.37 per 100,000 in rural areas [5].
In addition, the burden of CVD remains disproportionately larger in lower- and middle-income countries (LMICs) compared with high-income countries as >80% of CVD deaths occur in LMICs [1]. The costs due to CVD in LMICs were estimated to amount to US$3.7 trillion between 2011 and 2015, representing approximately a half of the NCD economic burden and 2% of gross domestic product across LMICs [1].
Nitrates, such as sublingual nitroglycerin, isosorbide-5-mononitrate (5-ISMN) and isosorbide dinitrate (ISDN), are widely used as therapeutic agents in the treatment of CHD, not only for patients with stable angina pectoris, but also for those with unstable angina, acute myocardial infarction and heart failure [6]. These drugs act directly on the vascular smooth muscle to produce venous and arterial dilatation, reducing pre-load, after-load and oxygen demand. In addition, published meta-analyses showed that there was no significant difference in the antianginal efficacy between long-acting nitrates and β-blockers or calcium channel blockers [7,8].
The 5-ISMN has been used as an effective agent against angina pectoris and myocardial infarction in randomized controlled trial and clinical practice [9]. The 5-ISMN is the principal metabolite of ISDN and has no first-pass metabolism or active metabolites. The elimination half-life of 5-ISMN is 4–5 h and longer than that of ISDN, which is 30–60 min [10]. These favorable pharmacokinetic features of 5-ISMN lead to a more predictable and reproducible clinical effect compared with its parent compound [10]. However, 5-ISMN has a longer time to reach effective therapeutic concentrations than ISDN and may accumulate and predispose to the development of hypotension [9]. While the evaluation evidence from the real world is very limited, this study is to assess the effectiveness of intravenous-administered 5-ISMN and ISDN. In addition, due to big economic burden of the disease, the cost of treatments were also assessed in this study.
Methods
Design
This was a retrospective propensity score matching (PSM) study. Data collection was performed from February 2014 to November 2015 at the two hospitals in China. Data were collected from patients’ electronic medical records and retrieved for analysis in a real-world setting. The primary objective was to compare the length of stay, the frequency and dose of glycerol trinitrate between 5-ISMN and ISDN. The secondary objective was to assess the average direct medical cost during hospitalization, and to identify significant factors influencing on the direct medical cost.
Study population
The inpatients who were selected as CHD (either unstable angina pectoris or myocardial infarction) and had taken a pharmacy claiming for at least one injection of 5-ISMN or ISDN, were initially enrolled in this study. International Classification of Diseases (ICD-10) was used to identify the CHD patients. The exclusion criteria include: the patients who were selected as acute renal failure, hypertrophic obstructive cardiomyopathy, mitral stenosis, constrictive pericarditis or cardiac tamponade; systolic blood pressure <90 mmHg when enrolled; and combined modality therapy includes Sildenafil.
Effectiveness, safety & cost assessment
For the clinical effectiveness assessment in this study, use of sublingual nitroglycerin, hypotension incidence, length of hospital stay and hospitalization cost were compared between the two groups. The length of hospitalization was defined from the date of admission to discharge. In addition, the adverse events occurred during the treatment identifying with the diagnosis were also investigated, but incomplete records and missing data might exist. So we only focus on the incidence of hypotension, which can be obtained from the examination of daily blood pressure.
The direct medical cost including medication cost, examination, laboratory, treatment, surgical fees, ward bed, nursing and other costs were also compared between the two groups.
Statistical analysis
Continuous variables were expressed as mean and standard deviation in each group and compared using a t-test if variables conform to a normal distribution. Conversely, the minimum, maximum, median and interquartile ranges were calculated for each group and compared with Wilcoxon test. Categorical variables were presented as count and percentage (n, %) and compared using the Chi-square test or Fisher’s exact test.
PSM was used to balance the bias between patients’ characteristics using 1:1 pair-wise matching with a caliper of 0.05. A logistic regression model was calculated with the covariate variables (age, sex, comorbidities on admission and insurance coverage) to obtain the scores. For estimating propensity scores, one-to-one nearest neighbor matching without replacement was performed. The difference of potential confounding variables with p < 0.05 was considered to be statistically significant for each test before and after PSM.
Multiple linear regression was used to identify the influence factors on direct medical cost.
All analyses were processed by R statistical package v.2.13.1 (R Foundation for Statistical Computing, Vienna, Austria). The significant level is defined as two-sided α = 0.05.
Results
Patients characteristics
More than 20,000 patients with CHD were retrieved from the records. Finally, a total of 5609 patients were identified, 4047 patients in 5-ISMN group and 1562 patients in ISDM group. Subsequently, we carried PSM to balance the potential confounder bias in this observational research. After PSM, this matching group was comprised of 1555 pairs based on the balancing of age, sex, insurance and comorbidities on admission. The screening flow is described in Figure 1.

Figure 1. Screen flow for coronary heart disease population.
5-ISMN: Isosorbide-5-mononitrate; CHD: Coronary heart disease; ISDN: Isosorbide dinitrate; PSM: Propensity score matching.
Patients’ demographics and characteristics of the two groups after PSM were summarized in Table 1. The mean age between 5-ISMN and ISDN groups were 68.9 and 69.1 years old, respectively (p > 0.05). The proportion of male between the two groups was without statistical difference (54.0 vs 55.0%; p > 0.05). The most common comorbidities were hypertension (3.0 vs 3.0%; p > 0.05), lung disease (2.0 vs 2.0%; p > 0.05) and diabetes (2.0 vso 2.0%; p > 0.05). In addition, 92% patients were covered in insurance in both the groups.
| Period | Characteristics | 5-ISMN | ISDN | Difference | p-value |
|---|---|---|---|---|---|
| Before PSM | N | 4047 | 1562 | ||
| Age (mean ± SD) | 67.1 ± 11.76 | 69.1 ± 11.99 | -2 | <0.05 | |
| Sex (male, %) | 2171 (0.54) | 857 (0.55) | -0.01 | 0.428 | |
| Comorbidity (n [%]): | 0.725 | ||||
| – Lung disease | 146 (0.04) | 25 (0.02) | 0.02 | ||
| – Hypertension | 257 (0.06) | 54 (0.03) | 0.03 | ||
| – Diabetes | 131 (0.03) | 27 (0.02) | 0.01 | ||
| Insurance coverage (yes, n [%]): | 3541 (0.87) | 1425 (0.91) | -0.04 | <0.05 | |
| After PSM | – N | 1555 | 1555 | ||
| – Age (mean ± SD) | 68.9 ± 12.05 | 69.2 ± 11.96 | -0.3 | 0.52 | |
| – Sex (male, %) | 834 (0.54) | 855 (0.55) | -0.01 | 0.472 | |
| Comorbidity (n [%]): | 0.149 | ||||
| – Lung disease | 32 (0.02) | 24 (0.02) | 0 | ||
| – Hypertension | 43 (0.03) | 51 (0.03) | 0 | ||
| – Diabetes | 37 (0.02) | 24 (0.02) | 0 | ||
| Insurance coverage (yes, n [%]) | 1438 (0.92) | 1425 (0.92) | 0 | 0.426 |
5-ISMN: Isosorbide-5-mononitrate; ISDN: Isosorbide dinitrate; PSM: Propensity score matching; SD: Standard deviation.
Effectiveness
Assessment of clinical effectiveness between the two matching groups were shown in Table 2. For the frequency of sublingual nitroglycerin, the patients in 5-ISMN group claimed significantly less frequency (4.2 vs. 6.5-times; p < 0.05) and less dosage (47.5 vs 136.4 mg; p < 0.05) than those in ISDN group. For the matching pairs, the patients in 5-ISMN group had shorter length of hospital stay (16 vs. 17.7 days; p < 0.05) compared with the patients in ISDN group with statistical significance.
| Observation indicators | 5-ISMN (N = 1555) | ISDN (N = 1555) | Difference (95% CI) | p-value |
|---|---|---|---|---|
| Hospital stay (day) | 16 ± 11.3 | 17.7 ± 13.2 | -1.72 (-2.58, -0.86) | <0.05 |
| Glycerol trinitrate frequency (time) | 4.2 ± 6.6 | 6.5 ± 9.5 | -2.37 (-3.14, -1.6) | <0.05 |
| Glycerol trinitrate dosage (mg) | 47.5 ± 153.4 | 136.4 ± 261 | -88.86 (-108.77, -68.95) | <0.05 |
5-ISMN: Isosorbide-5-mononitrate; ISDN: Isosorbide dinitrate.
According to the clinical results, the incidence of hypotension in 5-ISMN group was lower than that of ISDN group (0.08 vs 0.13; p = 0.07), but the statistical significance was not achieved.
Direct medical cost assessment
The direct medical cost of CHD was considered in this study. Additionally, the different proportions of detailed cost were calculated (Figure 2). The highest component of total cost was medical consumables and medication in both the groups, which were 42.3 and 28.1%, respectively. The following ones are cost of examination, treatment, laboratory test, surgical and ward bed took majority of total cost (1–10%). In addition, nursing and the others cost <1% of the total expenditure.
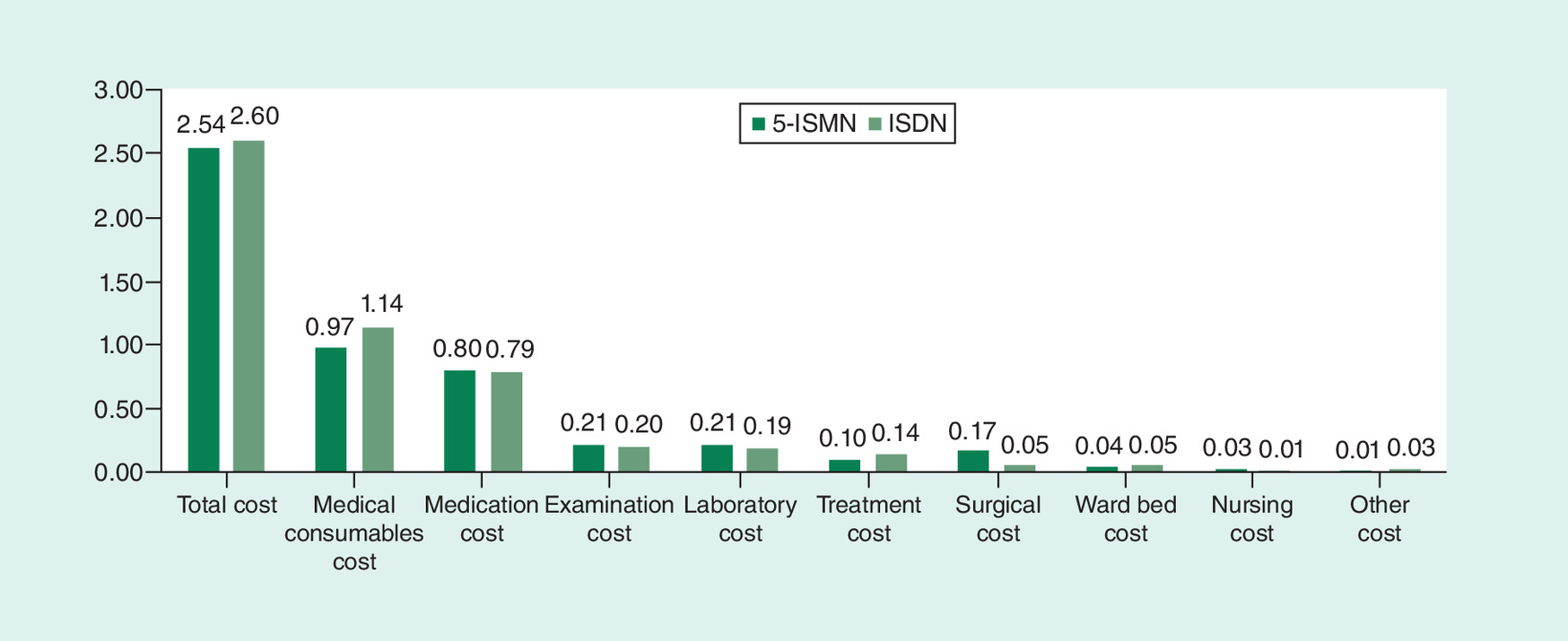
Figure 2. Comparison of hospitalization costs odds ratio between isosorbide-5-mononitrate and isosorbide dinitrate group.
The cost odds ratio was defined as the ratio of costs in the study to the average hospitalization costs in local city.
5-ISMN: Isosorbide-5-mononitrate; ISDN: Isosorbide dinitrate.
Furthermore, the summary for total cost and the detailed categories was listed in Table 3. The average hospitalization expenses of each time per patient for 5-ISMN and ISDN groups were 16,123 and 41,563 Yuan, respectively.
| Observation indicators | 5-ISMN (N = 1555) | ISDN (N = 1555) | p-value |
|---|---|---|---|
| Total cost | 16,123 | 41,563 | <0.001 |
| Medical consumable | 6157 | 18,224 | <0.001 |
| Medication cost | 5078 | 12,628 | <0.001 |
| – Western medicine | 3808 | 12,309 | <0.001 |
| – Chinese patent drug | 1269 | 319 | <0.001 |
| – Chinese herbal medicine | 0.00 | 0.00 | <0.001 |
| Examination cost | 1333 | 3197 | <0.001 |
| Laboratory test cost | 1333 | 3037 | <0.001 |
| Treatment cost | 634 | 2238 | <0.001 |
| Surgical cost | 1079 | 799 | 0.06 |
| Ward bed cost | 253 | 799 | <0.001 |
| Nursing cost | 190 | 159 | <0.001 |
| Other cost | 0.00 | 0.00 | <0.001 |
5-ISMN: Isosorbide-5-mononitrate; ISDN: Isosorbide dinitrate.
It is worth noting that in order to decrease the potential bias resulting from different districts, the cost odds ratio, which is defined as the ratio of costs in the study to the average hospitalization costs in local city, was compared between the two groups. According to the results in Figure 2, the odds ratio for the total cost in 5-ISMN group was significantly lower than that in ISDN group. For the detailed categories, in comparison with ISDN group, the patients in 5-ISMN group had lower costs of medical consumables, western medication, treatment and ward bed. For the other categories, the ratio of 5-ISMN group is significantly higher than that in ISDN group.
Multiple linear regression analysis
A multiple linear regression analysis was used to illustrate the associated factors for direct medical cost in this study. As presented in Table 4, the independent variable is log-transformed direct medical cost, age, insurance coverage, sex (male = 1, female = 0), surgery (yes = 1, no = 0), comorbidity on admission (yes = 1, no = 0). Sublingual nitroglycerin frequency and treatment option (5-ISMN = 1, ISDN = 0) were included into the regression model as covariates. The results indicated that patients, would take more direct medical cost with younger, male, medical insurance covered, surgery received, other diseases combined. While patients with 5-ISMN took less direct medical cost comparing with ISDN.
| Factors | Coefficients | 95% CI | p-value |
|---|---|---|---|
| Age | -0.002 | (-0.003, -0.001) | <0.05 |
| Sex (female = 0) | 0.085 | (0.058, 0.113) | <0.05 |
| Insurance coverage | 0.062 | (0.012, 0.111) | <0.05 |
| Surgery received (no = 0) | 0.551 | (0.483, 0.619) | <0.05 |
| Comorbidity (no = 0) | 0.082 | (0.026, 0.139) | <0.05 |
| Glycerol trinitrate frequency | 0.023 | (0.021, 0.026) | <0.05 |
| Treatment option (ISDN = 0) | -0.305 | (-0.332, -0.279) | <0.05 |
ISDN: Isosorbide dinitrate.
Discussion
To our knowledge, our present study is one of a few studies to investigate the difference of clinical effectiveness and pharmacoeconomics between 5-ISMN and ISDN in the real-world setting. The principal finding of the present study is as follows: first, patients who received 5-ISMN treatment showed less frequency and dosage of sublingual nitroglycerin during the treatment of CHD, which indicated statistical significance. Second, in contrast to ISDN group, the 5-ISMN group saved total direct medical cost and shortened length of hospital stay. Fourth, the main factors relevant to direct medical cost included age, length of hospital stay and troponin level.
As a widely used nitrate, 5-ISMN has been used for treatment of CHD with a long time. By releasing nitric oxide, nitrates increase the level of cyclic guanosine monophosphate in smooth muscles and dilate coronary arteries and its collateral vessels [11]. Pharmacokinetic studies demonstrated that 5-ISMN might have an advantageous effect over ISDN, considering that it has no first-pass effect, low variation, greater bioavailability, slower clearance rate, and smaller volume of distribution at steady state, compared with its parental substance [10]. Wang compared the efficacy of both nitrates in Chinese chronic heart failure patients and found 5-ISMN improved the cardiac function more rapidly, alleviated chronic heart failure symptoms and signs more effectively than ISDN [12]. Our study obtained the similar result, it was observed that patients administered with intravenous 5-ISMN had a shorter average length of hospital stay compared with patients treated with ISDN.
Although it is well recognized that 5-ISMN is related with some adverse effects like hypotension and headache [13], the present real-world study demonstrated low and comparable incidence of adverse events in both the treatment groups. Kosoglou et al. evaluated the safety of 5-ISMN and ISDN in a randomized study, found that the incidence of treatment-related adverse events including headache, dizziness and nausea was lower among the patients receiving 5-ISMN than those ISDN [10]. In addition, because severity of adverse events is not so serious and did not need to be treated, we did not collect data about headache, vomiting and circulatory shock in this study. Furthermore, most adverse events could attribute to high initial dose or fast dripping speed, which could be avoided by tailored clinical practice in hospital. Since adverse events in the present study were collected based on final diagnosis in discharge, whether there were more adverse events that had occurred but had not been recorded was unclear. This therefore contributed to the difference in length of hospital stay and average hospitalization cost and need to be confirmed further.
It is worth mentioning that Derek et al. reported fixed-dose combination of isosorbide dinitrate and hydralazine therapy for blacks with heart failure reduced resource use and costs in African-American Heart Failure Trial (A-HeFT), long-term use of it displayed favorable cost–effectiveness [14]. In addition, one study focused on the cost comparison analysis between pentaerythrityl tetranitrate and ISDN prescribed to diabetic patients in Germany indicated that pentaerythrityl tetranitrate therapy tends to produce a saving in costs compared with ISDN therapy in diabetic patients when costs for co-medication are taken into account and after adjustment for age and co-morbidity [15]. The other cost–effectiveness study of nitrate therapy using a decision analysis demonstrated that despite a higher unit cost for ISMN, total anticipated treatment costs with this new long-acting nitrate are lower than those associated with ISDN and nitroglycerin patch therapy in patients with stable angina [16]. Moreover, a comparative study of isosorbide dinitrates and mononitrates in patients with ischemic heart disease and stable angina pectoris found that, although isosorbide dinitrate and mononitrates do not differ significantly in reduction of the anginal attacks and by an increase in exercise tolerance, but isosorbide dinitrate is more cost-effective. The results are similar with our findings, 5-ISMN could be a cost-effective treatment option for patients with CHD (either angina pectoris or myocardial infarction) comparing with ISDN. Sublingual nitroglycerin was used less frequently and with less dosage in the 5-ISMN group than that in ISDN group. Less usage of sublingual nitroglycerin may be less likely to induce the tolerance of it, which may result in a detrimental effect in the postischemic heart. Nitrate tolerance is the unavoidable outcome of continuous sublingual nitroglycerin use and remains a persistent therapeutic problem. Fan et al. [17] demonstrated that nitrate tolerance significantly exacerbated cardiac reperfusion injury as evidenced by increased cardiomyocyte apoptosis and necrosis, enlarged myocardial infarct size and decreased cardiac function recovery after reperfusion. The effect of smooth muscle relaxation induced by sublingual nitroglycerin might be mediated by changes in the activity of ALDH-2. Further studies confirmed this concept by demonstrating a marked attenuation of sublingual nitroglycerin-induced activation of the cyclic guanosine monophosphate-dependent cascade and vasodilatory potency after incubation with ALDH-2 inhibitors [18,19], so inactivation of the ALDH-2 play an important role in the sublingual nitroglycerin-induced tolerance. Conversely, ISMN and ISDN were unaffected by ALDH-2 inhibitors (or genetic ALDH-2 deletion) [19–21]. In addition, studies in clinical settings showed that chronic 5-ISMN treatment would not lead to NT. This was also proven by an experimental study which found that continuous infusion of 5-ISMN did not affect the blood pressure-lowering function of sublingual nitroglycerin [22]. By contrast, ISDN would rapidly induce nitrate tolerance at the early stage of treatment [13] and tolerance to its antianginal effects as well [23].
In brief, there are also limitations in our present study. First, this is an observational, retrospective, noninterventional, case-collection study, and the data are identified from patients’ electronic medical record database in a real-world setting, because of the limited information of the hospital information system, some of the principal clinical outcomes were not considered in this study. Second, the data included in this study came from different districts, since this is a bicentric study, the potential bias resulting from the different regions existed in this study. We used cost ratio between patients in the present study and the localized average patients to balance the bias. Third, our study focused only on direct medical costs and paid no attention to direct nonmedical and indirect costs, which may also be influential.
Conclusion
CHD patients using 5-ISMN were associated with fewer use of sublingual nitroglycerin, less hypotension incidence, shorter length of hospital stay and less hospitalization cost related to its comparator ISDN group. These findings suggested that the newer agent of 5-ISMN showed some advantages over traditional ISDN in relieving angina and myocardial ischemia. But a further study needs to be performed in the future, such as more consistent patients enrollment, and prospective study design used.
•
In this retrospective, real-world evaluation, 4047 patients were included from two tertiary hospitals. Propensity score matching was used to balance bias.
•
The frequency (4.2 ± 6.6-times vs 6.5 ± 9.5-times; p < 0.05) and total dosage (47.5 ± 153.4 vs 136.4 ± 261.0 mg; p < 0.05) of sublingual nitroglycerin in the isosorbide-5-mononitrate (5-ISMN) group was apparently decreased compared with the isosorbide dinitrate (ISDN) group.
•
Hypotension incidence in the 5-ISMN group was lower (8.0 vs 13.0%; p < 0.05) than that in the ISDN group.
•
Hospital stay in the 5-ISMN group (16.0 ± 11.3 days vs 17.7 ± 13.2; p < 0.05) is less than that in the ISDN group.
•
Hospitalization expenditure in the 5-ISMN group ([the ratio of cost in the study to the average hospitalization cost in the city] [odds ratio: 2.5 vs 2.6; p < 0.05]) was reduced compared with that in the ISDN group.
Acknowledgments
The authors thank L Li, Y Lin, X Ye and H Yao who performed the statistical analysis and database support work at Palan dataRx, and all the participants in the present study for their generous contributions.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest
1.
Gheorghe A, Griffiths U, Murphy A, Legido-Quigley H, Lamptey P, Perel P. The economic burden of cardiovascular disease and hypertension in low- and middle-income countries: a systematic review. BMC Public Health 18(1), 975 (2018).
• More broadly, national-level studies with appropriate sample sizes and adequate incorporation of indirect costs need to replace small-scale, institutional and retrospective cost studies.
2.
Ding JM, Zhang XZ, Hu XJ, Chen HL, Yu M. Analysis of hospitalization expenditures and influencing factors for inpatients with coronary heart disease in a tier-3 hospital in Xi'an, China: a retrospective study. Medicine (Baltimore) 96(51), e9341 (2017).
3.
Batty GD, Jung KJ, Mok Y et al. Oral health and later coronary heart disease: cohort study of one million people. Eur. J. Prev. Cardiol. 25(6), 598–605 (2018).
4.
Meng Khoo C, Tai ES. Trends in the incidence and mortality of coronary heart disease in Asian Pacific region: the Singapore experience. J. Atheroscler. Thromb. 21(Suppl. 1), S2–S8 (2014).
5.
Chen WW, Gao RL, Liu LS et al. China cardiovascular diseases report 2015: a summary. J. Geriatr. Cardiol. 14(1), 1–10 (2017).
6.
Parker JD, Parker JO. Nitrate therapy in stable angina pectoris. New Engl. J. Med. 318(2), 119–120 (1988).
• A detailed explanation of nitrate treatment for stable angina pectoris.
7.
Heidenreich PA, McDonald KM, Hastie T et al. Meta-analysis of trials comparing β-blockers, calcium antagonists, and nitrates for stable angina. JAMA 281(20), 1927–1936 (1999).
• A meta-analysis of trials comparing β-blockers, calcium antagonists and nitrates for stable angina is reported.
8.
Heidenreich P A, Mcdonald K M, Hastie T et al. An evaluation of beta-blockers, calcium antagonists, nitrates, and alternative therapies for stable angina.[J]. Evid Rep Technol Assess (10), 1–2 (1999).
9.
Shimada K, Sunayama S, Nakazato K et al. Efficacy and safety of controlled-release isosorbide-5-mononitrate in Japanese patients with stable effort angina pectoris. Int. Heart J. 47(5), 695–705 (2006).
10.
Kosoglou T, Patrick JE, Cohen A, Radwanski E, Christopher D, Affrime MB. Pharmacokinetics of isosorbide-5-mononitrate after oral administration of an extended-release mononitrate formulation versus a standard dinitrate formulation. Clin. Ther. 17(2), 241–251 (1995).
11.
Parker JD, Parker JO. Nitrate therapy for stable angina pectoris. N. Engl. J. Med. 338(8), 12 (1998).
12.
Wang G. Comparison of the effects of intravenous administration of isosorbide dinitrate and 5-isosorbide monitrate on cardiac function in patients with chronic heart failure. World Lastest Med. Information 31, 2 (2016).
13.
Hansen EK, Olesen J. Towards a pragmatic human migraine model for drug testing: 2. Isosorbide-5-mononitrate in healthy individuals. Cephalalgia 37(1), 11–19 (2016).
14.
Angus DC, Linde-Zwirble WT, Tam SW et al. Cost–effectiveness of fixed-dose combination of isosorbide dinitrate and hydralazine therapy for blacks with heart failure. Circulation 112(24), 3745–3753 (2005).
• Cost–effectiveness of fixed-dose combination of isosorbide dinitrate and hydralazine therapy for blacks with heart failure.
15.
Icks A, Haastert B, Rathmann W, Schroder-Bernhardi D, Giani G. Cost comparison analysis: pentaerythrithyl tetranitrate (PETN) and isosorbide dinitrate (ISDN) prescribed to diabetic patients in primary care practices in Germany. Int. J. Clin. Pharmacol. Ther. 45(9), 516–523 (2007).
• Cost comparison analysis: pentaerythrityl tetranitrate and isosorbide dinitrate prescribed to diabetic patients in primary care practices in Germany.
16.
Larrat EP. Cost–effectiveness study of nitrate therapy using a decision analysis methodology. Hosp. Formul. 29(4), 277–278 (1994).
17.
Fan Q, Gao F, Zhang L, Christopher TA, Lopez BL, Ma XL. Nitrate tolerance aggravates postischemic myocardial apoptosis and impairs cardiac functional recovery after ischemia. Apoptosis 10(6), 1235–1242 (2005).
• Nitrate tolerance aggravates postischemic myocardial apoptosis and impairs cardiac functional recovery after ischemia was revealed.
18.
Zhang J, Chen Z, Cobb FR, Stamler JS. Role of mitochondrial aldehyde dehydrogenase in nitroglycerin-induced vasodilation of coronary and systemic vessels: an intact canine model. Circulation 110(6), 750–755 (2004).
• Role of mitochondrial aldehyde dehydrogenase in nitroglycerin-induced vasodilation of coronary and systemic vessels: an intact canine model is exhibited.
19.
Sydow K, Daiber A, Oelze M et al. Central role of mitochondrial aldehyde dehydrogenase and reactive oxygen species in nitroglycerin tolerance and cross-tolerance. J. Clin. Invest. 113(3), 482–489 (2004).
20.
Daiber A, Oelze M, Coldewey M et al. Oxidative stress and mitochondrial aldehyde dehydrogenase activity: a comparison of pentaerythritol tetranitrate with other organic nitrates. Mol. Pharmacol. 66(6), 1372–1382 (2004).
21.
Chen Z, Foster MW, Zhang J et al. An essential role for mitochondrial aldehyde dehydrogenase in nitroglycerin bioactivation. Proc. Natl Acad. Sci. USA 102(34), 12159–12164 (2005).
22.
Manabe T, Yamamoto A, Satoh K, Ichihara K. Tolerance to nitroglycerin induced by isosorbide-5-mononitrate infusion in vivo. Biol. Pharm. Bull. 24(12), 3 (2001).
• Tolerance to nitroglycerin induced by isosorbide-5-mononitrate infusion in vivo is studied.
23.
MüNzel T, Steven S, Daiber A. Organic nitrates: update on mechanisms underlying vasodilation, tolerance and endothelial dysfunction. Vasc. Pharmacol. 63(3), 9 (2014).
Information & Authors
Information
Published In
Pages: 405 - 412
PubMed: 32301331
Copyright
© 2020 Future Medicine Ltd.
History
Received: 14 July 2019
Accepted: 7 February 2020
Published online: 17 April 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative analysis of cost–effectiveness between isosorbide-5-mononitrate and isosorbide: a retrospective real-world evaluation. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0099
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Hiroki Teragawa, Yu Hashimoto, Akane Tsuchiya, Shuichi Nomura, Optimal Timing of Pharmacological Spasm Provocation During Interventional Diagnostic Procedures, Journal of Coronary Artery Disease, 10.7793/jcad.31.008, 31, 4, (148-154), (2025).
- Xiaoming Fu, Haowei Lu, Meng Gao, Pinghe Li, Yan He, Yu He, Xiaojian Luo, Xiaoyong Rao, Wei Liu, Nitric oxide in the cardio-cerebrovascular system: Source, regulation and application, Nitric Oxide, 10.1016/j.niox.2024.09.005, 152, (48-57), (2024).