Knowledge, awareness and perceptions of diabetes mellitus among the Saudi population
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: High prevalence of undiagnosed cases of diabetes mellitus (DM) has increased over the last two decades, most patients with DM only become aware of their condition once they develop a complication. Limited data are available regarding the knowledge and awareness about DM and the associated risk factors, complications and management in Saudi society. Aim: This study aimed to assess knowledge of DM in general Saudi society and among Saudi healthcare workers. Results: Only 37.3% of the participants were aware of the current DM prevalence. Obesity was the most frequently identified risk factor for DM. Most comparisons indicated better awareness among health workers. Conclusion: A significant lack of knowledge about DM in Saudi society was identified. Social media and educational curriculum can improve knowledge and awareness of DM.
Diabetes mellitus (DM) is a chronic metabolic disease that is characterized by high blood glucose levels (hyperglycemia) consequent to defective insulin action, secretion or both. Immediate symptoms of hyperglycemia usually include polyuria, polydipsia, weight loss and blurred vision, whereas chronic DM is associated with impairment, dysfunction and failure of several organs, including blood vessels, eyes, heart, kidneys and nerves [1]. In addition to etiological genetic factors, several important risk factors for DM have been identified, including eating pattern, lack of physical activity, obesity and urbanization [2].
DM can be broadly classified into two types: Type 1 diabetes, which is caused by a complete deficiency of insulin secretion, and the significantly more common Type 2 diabetes, which results from a combination of an insufficient insulin secretory response and resistance to insulin action. The International Diabetes Federation (IDF) has estimated that DM affects approximately 415 million people worldwide, among which a vast majority (90%) of cases are diagnosed as Type 2 diabetes [3]. The last two decades yielded a dramatic increase in the prevalence of DM, particularly in the Middle Eastern and North African region, which had the second-highest reported rate of DM worldwide. Furthermore, in this region, Saudi Arabia, Kuwait and Qatar were ranked among the top ten countries worldwide in terms of DM prevalence [2]. However, variability in data regarding DM prevalence in these three countries might be attributable to differences in study designs, diagnostic methods and populations [4].
Reports from Saudi Arabia have demonstrated a dramatic increase in the prevalence of DM during the last two decades, from rates of approximately 2.4–4.3% in the 1980s [5,6] to 25.4%, an approximate eightfold increase [7]. Moreover, DM was found to be more prevalent among Saudis residing in urban areas, compared with those in rural areas (25.5 vs 19.5%) [8]. A lack of health education and multiple pregnancies have also been identified as factors in the etiology of DM that may particularly affect those in the Middle Eastern and North African region [9].
It is estimated that DM will be the seventh leading cause of death worldwide by 2030 [10]. In the meantime, individuals with DM face elevated risks of heart disease, stroke, hypertension, blindness, kidney disease, nervous system disease, amputations, dental disease and gestational complications [11]. Better control of DM and a better quality of life require knowledge and awareness about DM and the associated risk factors, complications and management [12–14].
Many sufferers of DM only become aware of their disease once they have developed a life-threatening complication. Furthermore, the IDF reported that Saudi individuals and healthcare providers remain either uninformed or unconvinced about the potentially devastating complications and seriousness of DM. Consequently, in this study, we focused on three objectives: Assessment of general knowledge and awareness about DM in Saudi society; Comparison of knowledge and awareness among Saudi health and nonhealth workers; and Comparison of the perceptions of Saudi society members regarding the best awareness strategies for DM (social media and educational curriculum).
Methods
This study was approved by the Institutional Review Board at the College of Medicine, King Saud University Medical City (KSUMC), Riyadh, Saudi Arabia. After an extensive review of relevant published literature, we designed a self-reported cross-sectional questionnaire comprising 11 questions that addressed three areas. Five questions addressed socio-demographic characteristics, including age, gender, educational level, region and social media use. Three questions assessed general knowledge and awareness regarding DM risk factors and complications. Finally, three questions solicited participants’ opinions regarding DM awareness strategies, with the intent to gather data about the current roles of social media and education in improving DM awareness.
The sample size was calculated using the following formula: (Za2)(pq)/d2 = (1.96)2(21)(79)/19.4 = 329 participants, where ‘Z’ represents the z score value of a normal distribution, ‘p’ represents the prevalence of DM, ‘q’ is defined as 1-p, and ‘d’ is the accuracy of the estimate. Using simple random sampling, 50 questionnaires were distributed through a pilot study to evaluate time and suitability. Further questionnaires were distributed after a successful pilot study outcome.
This study was conducted over a period of 3 months (December 2015–February 2016). Data were collected from three Saudi areas: Riyadh, Dammam and Al-Qassim. Paper-based questionnaires were distributed in hospitals, malls and schools in the targeted areas, and an online-based questionnaire was also available. The time required to complete each questionnaire was <2 min.
Inclusion & exclusion criteria
A few limitations are associated with this study including using cities that may have a population with higher educational levels compared with other cities throughout Saudi Arabia. Also, the ‘healthcare worker’ term is general which includes a range of jobs and specialties that may not be directly related to Diabetes care management. People over the age of 60 was excluded from this study due to poor literacy rate and knowledge of DM in the Saudi society. The secondary education duration is 3 years (ages 15–18). More detailed studies that include larger numbers of participants in different regions with more detailed information is recommended, as these will provide a more thorough view about awareness of DM in Saudi Arabia.
All data were entered manually into Excel data sheets (Microsoft, WA, USA), and SPSS and JMP statistical software (SPSS, Inc., IL, USA; JMP, Buckinghamshire, UK) was used to analyze the imported datasets from Excel files. Descriptive statistics, including means, standard deviations, percentages and frequencies, were calculated for socio-demographic data. The independent t-test, one-way analysis of variance and χ2 test were also used to evaluate correlations between some dependent and independent variables. A p < 0.05 was considered significant unless otherwise noted.
Results
A total of 870 questionnaires were distributed manually and via e-mail to home bound participants. After excluding 81 questionnaires that had not been completed or were completed by participants aged younger than 15 years or older than 60 years, 789 questionnaires were subjected to statistical analysis. Although most participants immediately accepted the invitation to complete the questionnaire, a few participants requested further clarification of some questions and others inquired about the future benefits of this study.
Of the 789 study participants, 628 (79.6%) were from Riyadh, 80 (10.1%) were from Dammam and 81 (10.3%) were from Al-Qassim. Most participants (95.7%) were highly educated (i.e., secondary or university students), and 73.9 and 26.1% were male and female, respectively. Social media users and nonsocial media users comprised 702 (89.0%) and 87 (11.0%) of participants, respectively (Table 1).
| Socio-demographic character | Health workers (n = 177) | Nonhealth workers (n = 612) | Overall (n = 789) |
|---|---|---|---|
| Gender | |||
| – Male | 114 (64.4%) | 469 (76.6%) | 583 (73.9%) |
| – Female | 63 (35.6%) | 143 (23.4%) | 206 (26.6%) |
| Age, years (SD) | 29.8 (7.8) | 29.1 (9.3) | 29.3 (9.5) |
| Region | |||
| – Riyadh | 121 (68.4%) | 507 (82.8%) | 628 (79.6%) |
| – Eastern | 28 (15.8%) | 52 (8.5%) | 80 (10.1%) |
| – Al-Qassim | 28 (15.8%) | 53 (8.7%) | 81 (10.3%) |
| Education level | |||
| – Less than secondary school | 3 (1.7%) | 31 (5.1%) | 34 (4.3%) |
| – Secondary school and university | 174 (98.3%) | 581 (94.9%) | 755 (95.7%) |
| Social media user | |||
| – Yes | 163 (92.1%) | 539 (88.1%) | 702 (89.0%) |
| – No | 14 (7.9%) | 73 (11.9%) | 87 |
SD: Standard deviation
Assessment of knowledge & awareness of DM in Saudi society
As reported earlier, the DM prevalence in Saudi Arabia is approximately 25%. In our survey, 294 (37.3%) participants selected the correct answer regarding DM prevalence (20–30%). The data were further reduced to 10 year of age brackets and when examined it was found that those between 20–30 years of age were most likely to correctly identify the extent of DM prevalence in Saudi Arabia society. Further examination of this data to include education level demonstrated that within the 20–30 age bracket, 34.5% of those with a secondary school education correctly identified the prevalence of DM, compared with 40.1% with a university degree, but these were not significantly different at the p < 0.05 significance level indicating that level of education on the ability to correctly identify the prevalence of DM in Saudi Arabia did not play a large role.
Multiple correspondence analysis plot was also used to explore the data more quickly at a glance. It may be thought of as the categorical data equivalent to multivariate analysis of continuous numerical data. In order to assess the awareness of DM in Saudi Arabia, six responses were analyzed: range of age in years, gender, levels of education, employment in the healthcare sector, province and percentage DM prevalence. The result is given in Figure 1, where the closer two points are together, greater the association between those two points. Thus, to analyze the figure in terms of general knowledge of the prevalence of DM in Saudi Arabia, the most important point to concentrate on is the point denoting the correct 20–30% response choice. Males in Riyadh are the most closely associated, as well as those in the 20–30 age bracket and those with a university education. Moreover, to improve upon this, clearly educational materials need to target those with less than a secondary school education, in all age brackets greater than 50 years old, and in the Eastern region.
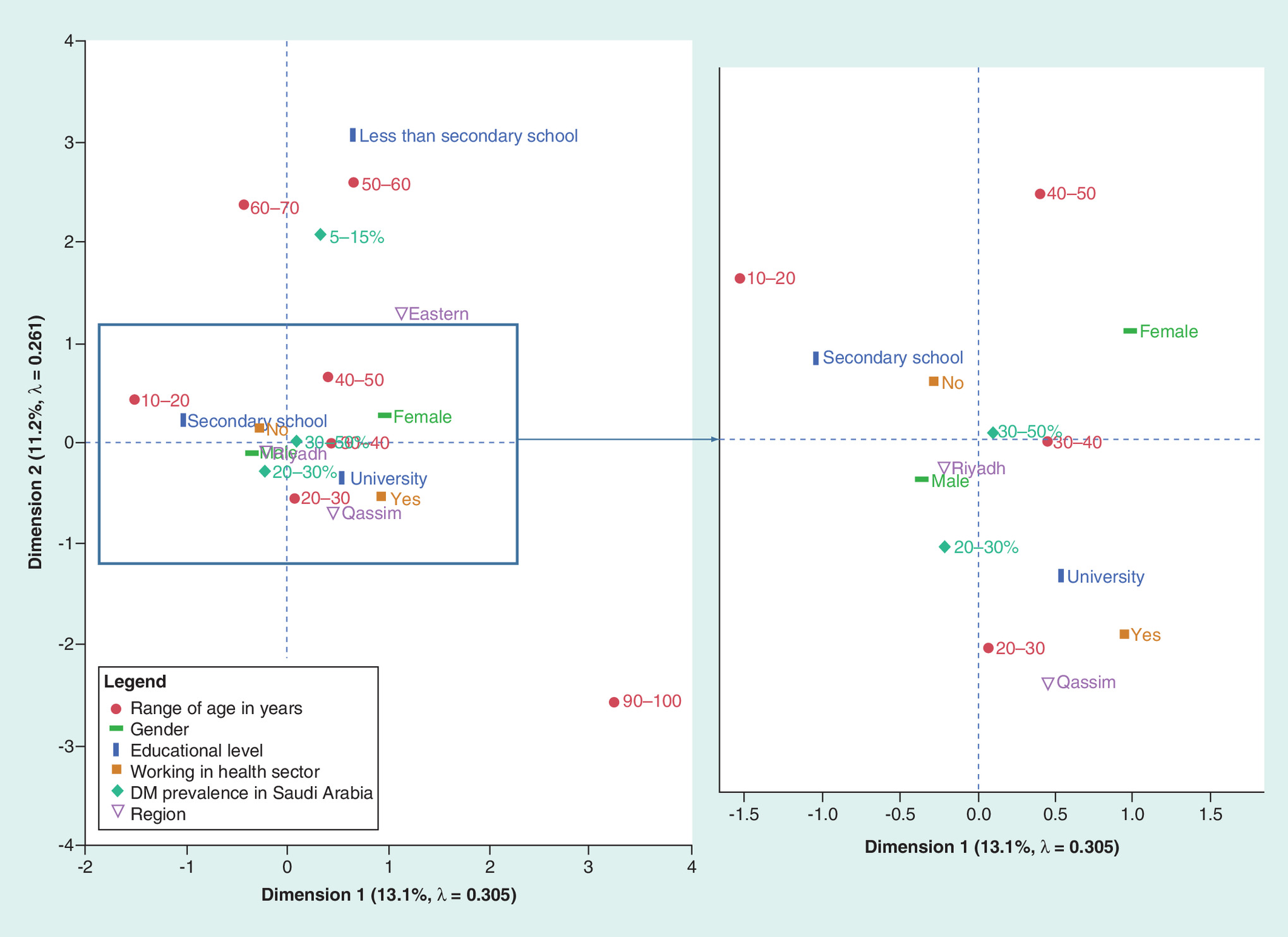
Figure 1. Multiple correspondence analysis plot summarizing the awareness of the general Saudi Arabian public to the prevalence of diabetes mellitus.
The closer two points are together, the greater the association between those two points. Thus, the most important point to consider in this instance is the 20–30% prevalence of DM. Plot on right is a zoomed version of the area outlined by the box.
DM: Diabetes mellitus.
Comparison of knowledge & awareness of DM among Saudi Arabian healthcare & nonhealthcare workers
A summary of the comparison of the knowledge and awareness of DM among healthcare and nonhealthcare workers, as well as risk factors and complications of DM, are presented in Table 2. Only 41.8% of healthcare workers were able to correctly identify the prevalence of DM in Saudi Arabia. Obesity and overweight were most frequently identified as a risk factor for DM (∼64% of the total participants), followed by physical inactivity (61.2%) and family history (55.6%). Health workers were significantly more likely to identify risk factors for DM. Amputation was most frequently identified as a complication of DM (42.0% of total participants), followed by eye complications (40.1%), heart disease (27.6%), kidney disease (26.5%) and stroke (16.7%). Moreover, health workers were significantly more likely to identify the complications of DM.
| Risk factors | Health workers | Nonhealth workers | Overall | p-value |
|---|---|---|---|---|
| Correct DM prevalence | ||||
| – 20–30% | 74 (41.8%) | 220 (35.9%) | 294 (37.3%) | 0.156 |
| Risk factors for DM development | ||||
| – Family history | 120 (67.8%) | 319 (52.1%) | 439 (55.6%) | <0.001 |
| – Obesity and overweight | 141 (79.7%) | 367 (60.0%) | 508 (64.4%) | <0.001 |
| – Physical inactivity | 116 (65.5%) | 367 (60.0%) | 483 (61.2%) | 0.181 |
| – Did not know | 5 (2.5%) | 36 (5.9%) | 41 (5.2%) | 0.107 |
| DM complications | ||||
| – Eye complications | 89 (50.3%) | 227 (37.0%) | 316 (40.1%) | 0.002 |
| – Amputation | 74 (41.8%) | 257 (42.0%) | 331 (42.0%) | 0.965 |
| – Kidney diseases | 63 (35.6%) | 146 (23.9%) | 209 (26.5%) | 0.002 |
| – Heart diseases | 69 (39.0%) | 149 (24.3%) | 218 (27.6%) | <0.001 |
| – Foot diseases | 103 (58.2%) | 252 (41.2%) | 355 (45.0%) | <0.001 |
| – Stroke | 56 (31.6%) | 76 (12.4%) | 132 (16.7%) | <0.001 |
| – Did not know | 12 (6.8%) | 85 (13.9%) | 97 (12.3%) | 0.011 |
Bold indicates statistical significance (p < 0.05).
DM: Diabetes mellitus.
The data were further analyzed to assess the awareness of the respondents of the prevalence of DM in Saudi society based on their employment in the healthcare sector and their education level. The data indicated that at the p < 0.05 significance level, no combination of education level or employment in the healthcare system led to a higher probability for the selection of the correct response.
A similar analysis examining the combination of employment in the healthcare sector and education level on identification of risk factors for DM is examined in Table 3. The results show that university educated healthcare employees were more likely to identify family history and obesity as risks that could lead to DM at the p < 0.05 significance level compared with university educated people working in other sectors. Interestingly, there was no difference when it came to the identification of lack of physical activity as another risk that could lead to DM. At the secondary school level, those working in the healthcare industry were more likely to identify only family history as a risk compared with their counterparts working in other sectors (at p < 0.05).
| Risk factor | Educational level | ||||||
|---|---|---|---|---|---|---|---|
| Less than Secondary School | Secondary School | University | |||||
| Working in health sector | Working in health sector | Working in health sector | |||||
| No | Yes | No | Yes | No | Yes | ||
| Family history as risk for DM | No | 17 50.0% | 1 33.3% | 134 52.3% | 6 28.6% | 143 44.1% | 50 32.5% |
| Yes | 17 50.0% | 2 66.7% | 122 47.7% | 15 71.4% | 181 55.9% | 104 67.5% | |
| Total responses | 34 | 3 | 256 | 21 | 324 | 154 | |
| Obesity as risk for DM | No | 17 50.0% | 1 33.3% | 102 39.8% | 5 23.8% | 128 39.4% | 31 20.1% |
| Yes | 17 50.0% | 2 66.7% | 154 60.2% | 16 76.2% | 197 60.6% | 123 79.9% | |
| Total responses | 34 | 3 | 256 | 21 | 325 | 154 | |
| Lack of activity as risk for DM | No | 21 61.8% | 1 33.3% | 106 41.4% | 11 52.4% | 120 36.9% | 50 32.5% |
| Yes | 13 38.2% | 2 66.7% | 150 58.6% | 10 47.6% | 205 63.1% | 104 67.5% | |
| Total responses | 34 | 3 | 256 | 21 | 325 | 154 | |
Cells in bold indicate comparative responses that are significantly different at the p < 0.05 level.
DM: Diabetes mellitus.
The effect of employment in the healthcare sector and education level on identification of complications arising from DM was also examined and the results summarized in Table 4. University educated healthcare workers were able to identify vision loss, kidney disease, heart disease, feet problems and stroke at significantly higher rates than university educated nonhealthcare workers at the p < 0.05 significance level. The same is true for identification of hypertension as a risk, but only at the p < 0.1 level. However, at the secondary school level, there is practically no difference whether one works in the healthcare sector or not when identifying complications due to DM.
| DM complication | Educational level | ||||||
|---|---|---|---|---|---|---|---|
| Less than Secondary School | Secondary School | University | |||||
| Working in health sector | Working in health sector | Working in health sector | |||||
| No | Yes | No | Yes | No | Yes | ||
| DM complications: vision loss | No | 20 58.8% | 1 33.3% | 173 67.6% | 13 61.9% | 194 59.7% | 75 48.7% |
| Yes | 14 41.2% | 2 66.7% | 83 32.4% | 8 38.1% | 131 40.3% | 79 51.3% | |
| Total responses | 34 | 3 | 256 | 21 | 325 | 154 | |
| DM complications: amputation | No | 20 58.8% | 1 33.3% | 167 65.2% | 12 57.1% | 170 52.3% | 91 59.1% |
| Yes | 14 41.2% | 2 66.7% | 89 34.8% | 9 42.9% | 155 47.7% | 63 40.9% | |
| Total responses | 34 | 3 | 256 | 21 | 325 | 154 | |
| DM complications: kidney disease | No | 24 70.6% | 2 66.7% | 202 78.9% | 17 81.0% | 242 74.5% | 96 62.3% |
| Yes | 10 29.4% | 1 33.3% | 54 21.1% | 4 19.0% | 83 25.5% | 58 37.7% | |
| Total responses | 34 | 3 | 256 | 21 | 325 | 154 | |
| DM complications: heart diseases | No | 30 88.2% | 2 66.7% | 201 78.5% | 16 76.2% | 236 72.6% | 91 59.1% |
| Yes | 4 11.8% | 1 33.3% | 55 21.5% | 5 23.8% | 89 27.4% | 63 40.9% | |
| Total responses | 34 | 3 | 256 | 21 | 325 | 154 | |
| DM complications: feet problems | No | 23 67.6% | 0 0.0% | 157 61.3% | 12 57.1% | 180 55.4% | 63 40.9% |
| Yes | 11 32.4% | 3 100.0% | 99 38.7% | 9 42.9% | 145 44.6% | 91 59.1% | |
| Total responses | 34 | 3 | 256 | 21 | 325 | 154 | |
| DM complications: stroke | No | 30 88.2% | 2 66.7% | 222 86.7% | 21 100.0% | 288 88.6% | 99 64.3% |
| Yes | 4 11.8% | 1 33.3% | 34 13.3% | 0 0.0% | 37 11.4% | 55 35.7% | |
| Total responses | 34 | 3 | 256 | 21 | 325 | 154 | |
| DM complications: hypertension | No | 22 64.7% | 1 33.3% | 164 64.1% | 14 66.7% | 207 63.7% | 85 55.2% |
| Yes | 12 35.3% | 2 66.7% | 92 35.9% | 7 33.3% | 118 36.3% | 69 44.8% | |
| Total responses | 34 | 3 | 256 | 21 | 325 | 154 | |
Cells in bold indicate comparative responses that are significantly different at the p < 0.05 level. Those in bold and italics are significantly different at the p < 0.01 level.
DM: Diabetes mellitus.
Multiple correspondence analysis plot was used to explore the data in terms of awareness of risk factors leading to DM. In this case, the variables applied were age bracket, gender, levels of education, employment in the healthcare sector, obesity as risk factor, family history as risk factor and physical inactivity as risk factor. The result is presented in Figure 2. By looking at the ‘Yes’ responses for the three risk factors for DM, we note quickly that a university education is quite closely associated, as are the 20–30 and 30–40 age brackets. Interestingly, the ‘Yes’ and ‘No’ responses for employed in the healthcare sector are almost equidistant away, indicating that the association between those working in the healthcare sector to knowledge of the risk factors is not much different than those that are employed outside of the healthcare industry. A similar analysis plot for exploring awareness those employed in the healthcare sector of complications arising from DM is given in Figure 3. All of the ‘No’ answers are highly clustered together indicating that those not working in the healthcare sector are not particularly knowledgeable of the potential complications arising from DM. On the other hand, the ‘Yes’ answers are not clustered to the same extent, and the association of a university level education is stronger than simply working in the healthcare sector.
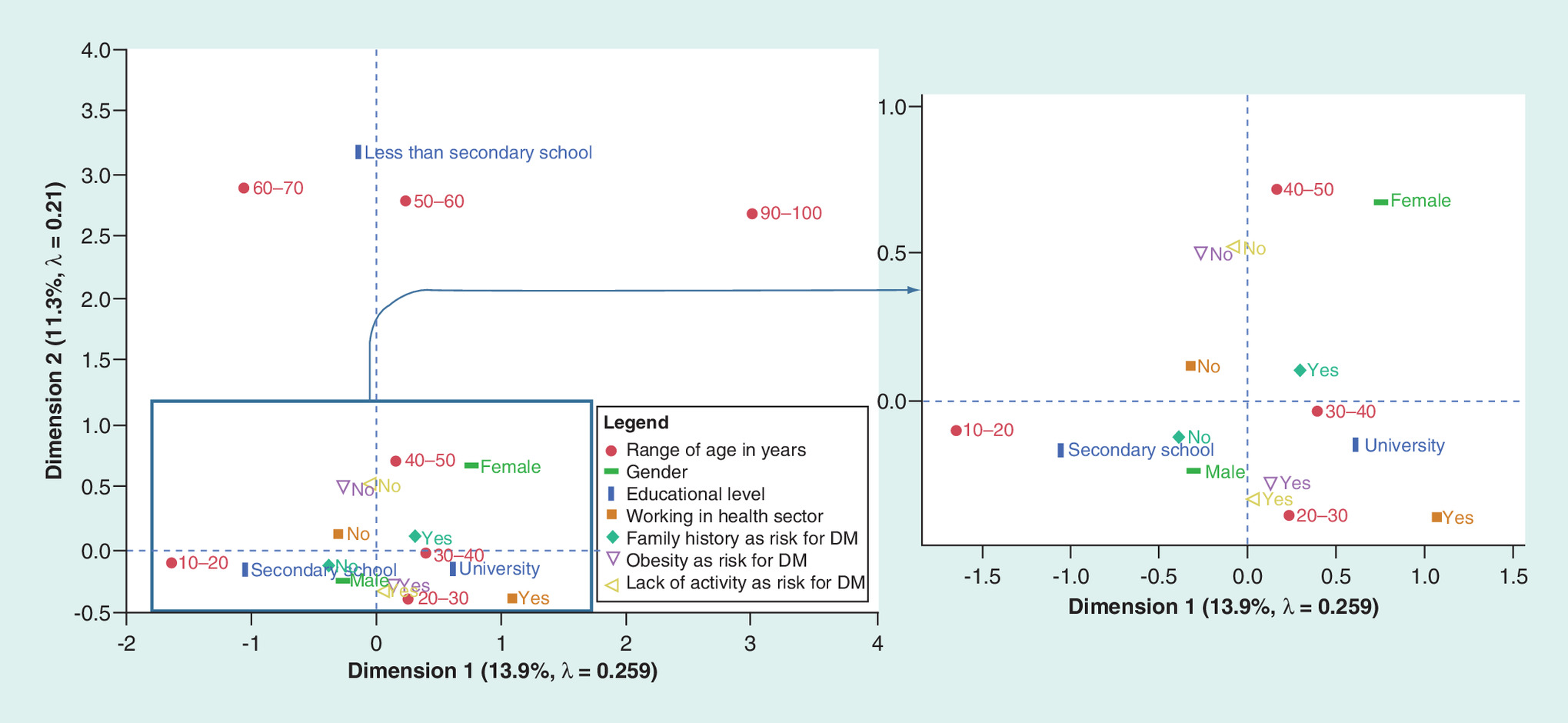
Figure 2. Multiple correspondence analysis plot summarizing the awareness of those employed in the healthcare sector to risk factors that could lead to diabetes mellitus.
The closer two points are together, the greater the association between those two points. Plot on right is a zoomed version of the area outlined by the box.
DM: Diabetes mellitus.
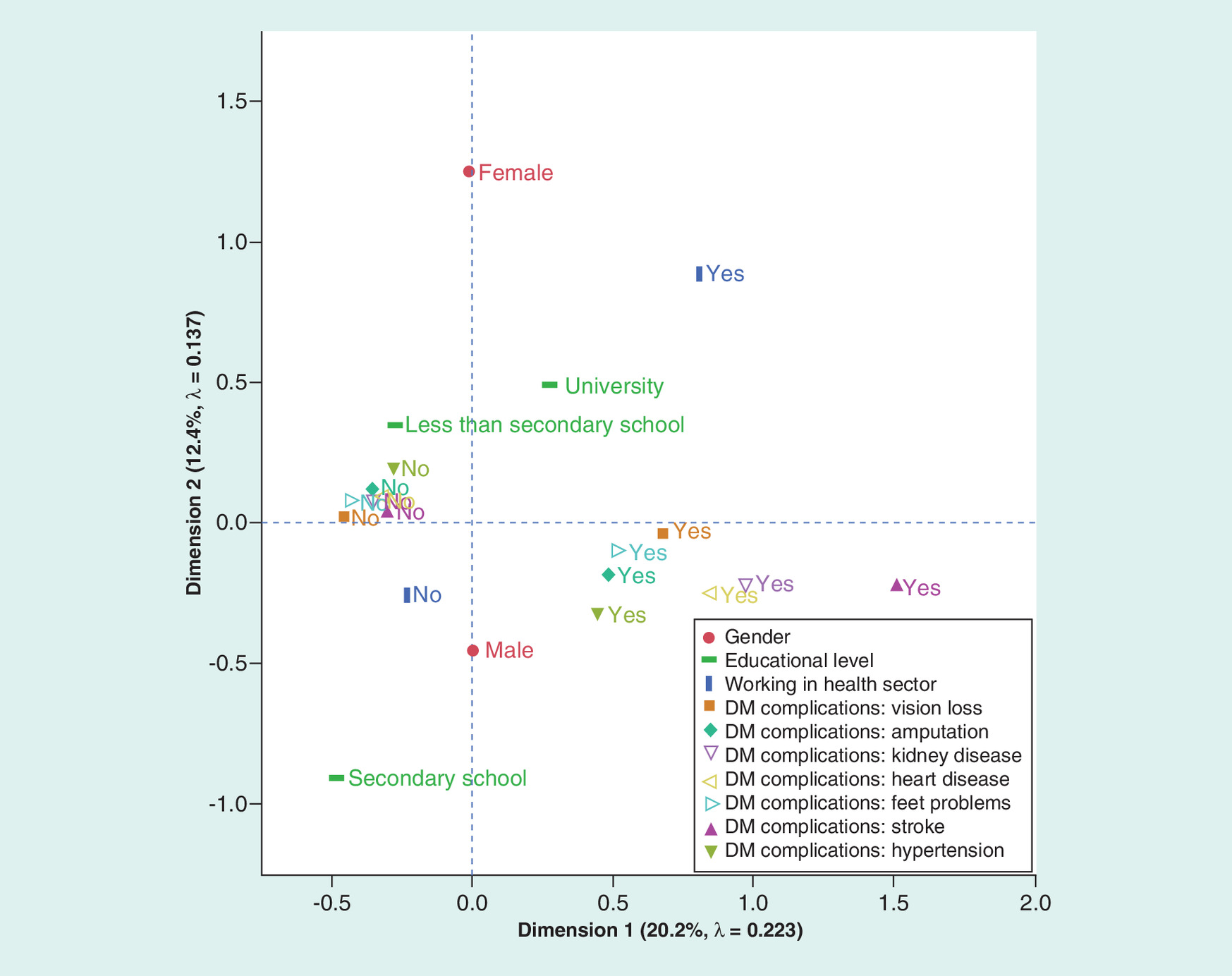
Figure 3. Multiple correspondence analysis plot summarizing the awareness of those employed in the healthcare sector complications arising from diabetes mellitus.
The closer two points are together, the greater the association between those two points.
DM: Diabetes mellitus.
Comparison of perception of Saudi Arabian society on best educational strategies for improved DM awareness: Traditional educational curriculum or social media?
Regarding strategies to increase DM knowledge, 635 (80.5%) participants believed that social media could effectively improve DM awareness, and 457 (57.9%) participants believed that educational curriculum could play a role in improving DM awareness. Initially, 48.3% of participants selected both social media and educational curriculum as effective measures for improving DM awareness. When asked about their preferred strategy (i.e., requested to select a single option), 52.2% selected social media and 47.8% selected educational curricula (Table 5).
| Opinion strategy | Health workers | Nonhealth workers | Overall | p-value |
|---|---|---|---|---|
| Promotes increased awareness | ||||
| – Social media (yes) | 150 (84.7%) | 485 (79.2%) | 635 (80.5%) | 0.104 |
| – Educational curriculum (yes) | 114 (64.4%) | 343 (56.0%) | 457 (57.9%) | 0.047 |
| – Both (yes) | 100 (56.5%) | 281 (45.9%) | 381 (48.3%) | 0.013 |
| Better strategy for DM awareness | ||||
| – Social media | 92 (52.0%) | 320 (52.3%) | 412 (52.2%) | 0.942 |
| – Educational curriculum | 85 (48.0%) | 292 (47.7%) | 377 (47.8%) | 0.942 |
Bold indicates statistical significance (p < 0.05).
DM: Diabetes mellitus.
These data can be further reduced to the age brackets defined earlier. The only age bracket where a significant propensity (at p < 0.05) to favor social media as an educational tool is in the 20–30-year range. Similarly, examination of the data showing those that believe a traditional educational curriculum is the best way to approach increased DM awareness demonstrated that the youngest age bracket, 10–20 years, were significantly against the idea, though interestingly they were not significantly in favor of social media. Other interesting data that can be extracted from the survey pertains to the education level and how it relates to a preference of either the social media or traditional educational curriculum to help increase DM awareness. In this case, it was found that education level had little influence on preferences for either educational approach to increase DM awareness. Furthermore, no regional preference over one educational approach to the other was observed.
The multiple correspondence analysis plot exploring the perception of the Saudi Arabian public to use of social media or a formal educational curriculum to increase awareness of DM is given in Figure 4. Not too surprisingly, those using social media have a much closer association with the belief that a social media approach would be better to improve DM awareness. Males are also far more associated with the social media response as well. Level of education played less of a role when selecting social media or formal education curriculum.
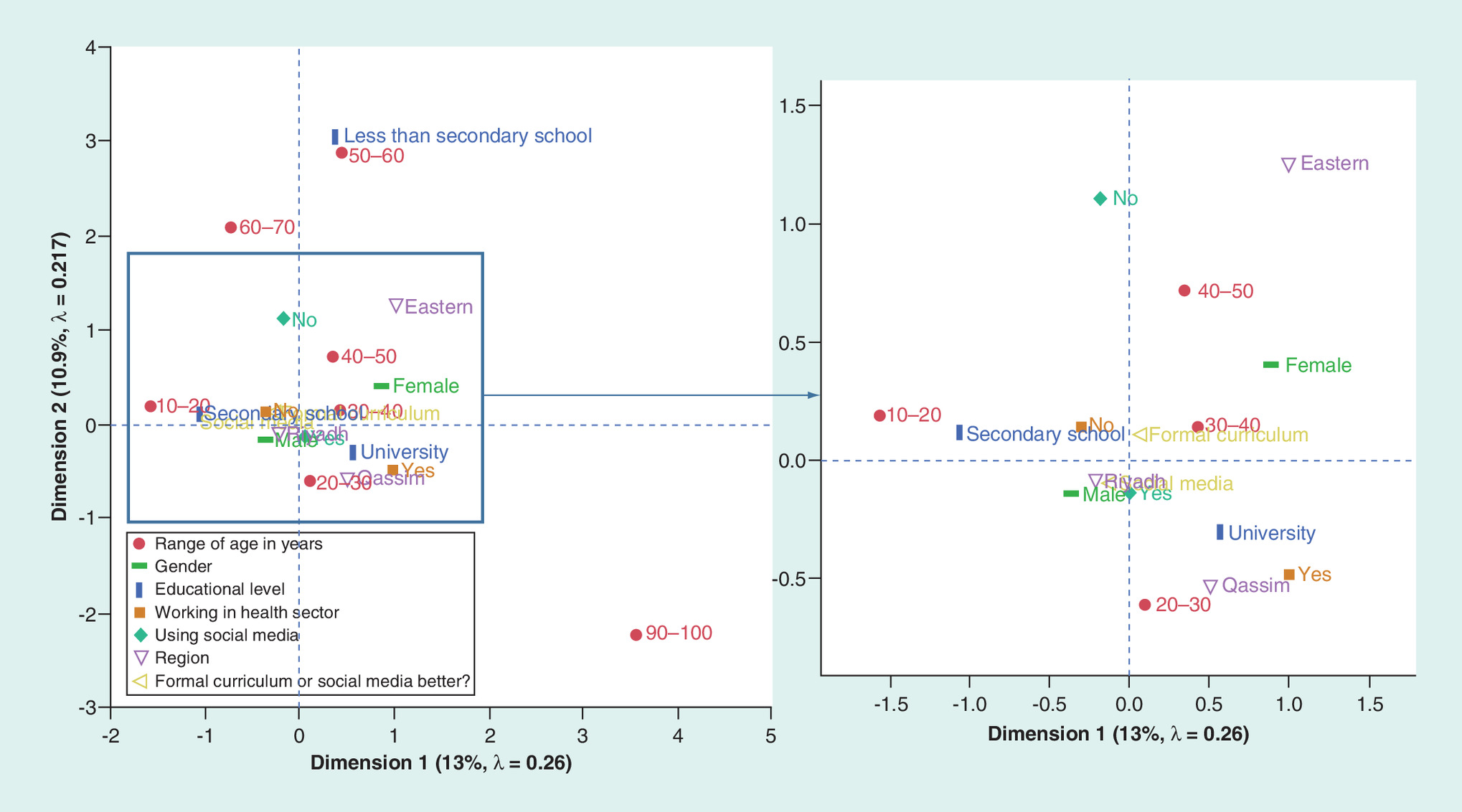
Figure 4. Multiple correspondence analysis plot showing the perception of the Saudi Arabian public to use of social media and/or a formal educational curriculum to increase awareness of diabetes mellitus.
The closer two points are together, the greater the association between those two points. Plot on right is a zoomed version of the area outlined by the box.
Discussion
The increasing prevalence and incidence of DM in Saudi Arabia provides cause for alarm. The IDF reported that approximately 4 million Saudis have DM, and an additional 1.5 million are thought to have undiagnosed DM as a consequence of the lack of awareness in this population (https://idf.org/). DM is a ‘silent’ disease, and its symptoms are often hidden until several years after disease onset. Many patients with DM have had the disease for many years before diagnosis, and many are only diagnosed once they have developed complications.
Our data demonstrate a general lack of awareness and knowledge of the prevalence of DM in Saudi society. Approximately 63% of survey participants, including health workers, could not identify the correct prevalence of DM, even though health workers would be expected to have a greater level of awareness about diseases. Furthermore, level of education was also found not to be an important factor. Those with a university degree were no more likely to identify the correct prevalence than those with a secondary school education. However, more than 64% of participants identified obesity and overweight as the most frequent risk factor for DM and health workers were significantly more likely to identify this factor, suggesting that Saudi residents possess some knowledge about potential risk factors for DM. In contrast, 42% of the participants incorrectly identified amputation as the most frequent DM complication. In Saudi Arabia, eye complications are most frequent among patients with DM, and approximately 20% of patients present with this type of complication as the first disease indicator [15,16]. Our study further demonstrated a lack of knowledge about DM complications even among health workers, as only half of the participating health workers identified eye complications as a consequence of DM. This indicates a major deficiency in awareness about DM complications in general Saudi society, including health workers.
Social media, which is among the most influential communication modalities currently available, has the power to change the attitudes, knowledge and behaviors of societies worldwide. We found that 80.5% of participants from general Saudi society thought that social media could be used effectively to improve awareness and knowledge about DM, whereas 57.9% thought that educational curriculum could also be effective with better implementation. Moreover, our study demonstrated that social media and educational curriculum were weighted similarly with regard to improving awareness of DM in Saudi society, with no regional bias toward one or the other approach.
Conclusion & recommendation
This study demonstrated a significant lack of knowledge and awareness regarding DM in Saudi society. Although health workers exhibited an increased level of awareness about DM, their level of knowledge still fell significantly short of expectations. The study further determined that both social media and educational curriculum can be major factors in improving and spreading awareness of DM. Accordingly, we recommend the design and development of DM awareness strategies, including the implementation of health subjects in educational curriculum, community educational programs and training workshops for healthcare providers. The data also suggest that educational materials need to target those with less than a secondary school education, in all age brackets greater than 50 years old, and in the Eastern provinces. It would further help if the material could address the female population as well. In addition, the establishment of an electronic website to provide health information might comprise a more attractive alternative for social media users. We further recommend more detailed studies that include larger numbers of participants in different regions, as these will provide increased awareness of DM.
•
This work aimed to assess knowledge of diabetes mellitus (DM) in general Saudi society and among Saudi healthcare workers and further compare the perceptions of using social media or educational strategies for increasing DM awareness.
•
This self-reported cross-sectional questionnaire study was conducted in different cities of Saudi Arabia.
•
This study demonstrated a significant lack of knowledge and awareness regarding DM in Saudi society. Only 37.3% of the participants were aware of the current DM prevalence.
•
Health workers exhibited an increased level of awareness about DM but their level of knowledge still fell significantly short of expectations.
•
This study determined that both social media and educational curricula can be major factors in improving and spreading awareness of DM.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 36, S67–S74 (2013).
• Highlights diabetes mellitus (DM) knowledge, risk and prevention.
2.
Abuyassin B, Laher I. Diabetes epidemic sweeping the Arab world. World J. Diabetes 7(8), 165–174 (2016).
•• Highlights the current status of DM in Arab world.
3.
Ogurtsova K, da Roacha Fernandes JD, Huang Y et al. IDF Diabetes Atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 128, 40–50 (2017).
4.
Guariguata L, Whiting DR, Hambleton I, Beagley J, Linnenkamp U, Shaw JE. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res. Clin. Pract. 103, 137–149 (2014).
5.
Bacchus RA, Bell JL, Madkour M, Kilshaw B. The prevalence of diabetes mellitus in male Saudi Arabs. Diabetologia 23, 330–332 (1982).
6.
Fatani HH, Mira SA, el-Zubier AG. Prevalence of diabetes mellitus in rural Saudi Arabia. Diabetes Care 10, 180–183 (1987).
7.
Al-Rubeaan K, Al-Manaa HA, Khoja TA et al. Epidemiology of abnormal glucose metabolism in a country facing its epidemic: SAUDI-DM study. J. Diabetes 7, 622–632 (2015).
8.
Al-Nozha MM, Al-Maatouq MA, Al-Mazrou YY, Al-Harthi SS. Diabetes mellitus in Saudi Arabia. Saudi Med. J. 25, 1603–1610 (2004).
9.
Badran M, Laher I. Type II diabetes mellitus in Arabic-speaking countries. Int. J. Endocrinol. 2012, 902873 (2012).
10.
Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 3(11), e442 (2006).
11.
World Health Organization. Global Report on Diabetes (2016). www.who.int/diabetes/global-report/en/
12.
Alanazi FK, Alotaibi JS, Paliadelis P, Alqarawi N, Alsharari A, Albagawi B. Knowledge and awareness of diabetes mellitus and its risk factors in Saudi Arabia. Saudi Med. J. 39(10), 981–989 (2018).
•• This systematic review highlights the lack of knowledge and awareness of DM among Saudis.
13.
Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 27, 1047–1053 (2004).
14.
Angeles-Llerenas A, Carbajal-Sanchez N, Allen B, Zamora-Munoz S, Lazcano-Ponce E. Gender, body mass index and socio-demographic variables associated with knowledge about Type 2 diabetes mellitus among 13,293 Mexican students. Acta Diabetol. 42, 36–45 (2005).
•• Highlights that adolescents and young adults have a low level of DM knowledge.
15.
Al-Rubeaan K, Abu El-Asrar AM, Youssef AM et al. Diabetic retinopathy and its risk factors in a society with a Type 2 diabetes epidemic: a Saudi National Diabetes Registry-based study. Acta Ophthalmol. 93(2), e140–e147 (2015).
16.
Negi A, Vernon S. An overview of the eye in diabetes. JR Soc. Med. 96, 266–272 (2003).
Information & Authors
Information
Published In
Pages: 413 - 422
PubMed: 32253916
Copyright
© 2020 Future Medicine Ltd.
History
Received: 11 September 2019
Accepted: 20 January 2020
Published online: 7 April 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Knowledge, awareness and perceptions of diabetes mellitus among the Saudi population. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0137
Export citation
Select the citation format you wish to export for this article or chapter.