Clinical and economic outcomes of ProGlide compared with surgical repair of large bore arterial access
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study compared real-world complication rates, hospitalization duration and costs, among patients undergoing arterial repair using the Perclose ProGlide (ProGlide) versus surgical cutdown (Cutdown). Materials & methods: Retrospective study of matched patients who underwent transcatheter aortic valve replacement/repair, endovascular abdominal aortic aneurysm repair, thoracic endovascular aortic repair or balloon aortic valvuloplasty with arterial repair by either ProGlide or Cutdown between 1 January 2013 and 24 April 2017. Results: Infections and blood transfusions were lower in the ProGlide cohort. Patients in the ProGlide cohort had a 42.5% shorter index hospitalization, which corresponded to US$14,687 lower costs. Conclusion: The use of ProGlide for arterial repair was associated with significantly lower transfusion rates, shorter index hospitalization and lower hospitalization costs compared with surgical cutdown.
Arterial procedure access-site complications, though infrequent, can increase morbidity, mortality and excess costs associated with diagnostic and interventional procedures requiring femoral catheterization [1]. Percutaneous access with use of vascular closure devices (VCDs) facilitate accelerated hemostasis when compared with surgical cutdown and repair [2,3]. Benefits include reduced time to ambulation, greater patient satisfaction and shortened hospital stays [4]. The use of the suture-mediated percutaneous VCDs, such as the Perclose ProGlide (Abbott Vascular, CA, USA), has been shown to reduce the overall risk for access-site complications compared with surgical cutdown [5,6].
Many clinical trials have demonstrated improved clinical and healthcare cost outcomes among patients treated with VCDs for closure after percutaneous large-bore arterial access [7,8]. Including the ProGlide device specifically [8–11], there is a lack of comparative effectiveness research using real-world data. This retrospective study used a nationwide, multisite database of aggregated electronic health records (EHRs) to identify, describe and match patients who underwent femoral artery repair after procedures with percutaneous large-bore arterial access using the ProGlide device to those who underwent surgical cutdown (Cutdown) without utilization of a suture-mediated repair device. Since there are no procedure codes specifically for percutaneous closure, the IBM Explorys EHR database, which contains information on medical devices used during surgical procedures, enabled us to perform an analysis that was previously not possible with claims data alone. A matched cohort design was used to compare clinical outcomes in a real-world setting and evaluate costs associated with differences in hospitalization length of stay (LOS) and complication rates.
Materials & methods
The data that support the findings of this study are available from IBM Watson Health. Restrictions apply to the availability of these data, which were used under license for this study.
Study design
Patients were selected for this retrospective study if they underwent any of the following procedures involving large-bore arterial access site closure with ProGlide device during the enrollment period of 1 January 2013 through 24 April 2017: transcatheter aortic valve replacement/repair (TAVR), endovascular abdominal aortic aneurysm repair (EVAR), thoracic endovascular aortic repair (TEVAR) or balloon aortic valvuloplasty (BAV). For patients with multiple procedures in the EHR data, the most recent procedure date was selected as the index procedure date. Patients with the ProGlide device used for vessel repair of the index procedure, the ProGlide cohort, were compared with those for whom no suture-mediated closure device was used, the Cutdown cohort. Patients with a history of VCD use for the indicated procedures were excluded from the Cutdown cohort.
Patient characteristics were measured during a 6-month pre-index baseline period. Clinical outcomes were measured during three time periods from the index date through the length of the index procedure inpatient admission, the first 30 days post-index and the first 6 months post-index. Clinical outcomes were compared between the ProGlide and Cutdown cohorts overall and within subgroups of patients undergoing each of the four procedures: TAVR, EVAR, TEVAR and BAV.
Data source
This study utilized patient-level de-identified US EHR data from the IBM Explorys Therapeutic Dataset (Explorys; IBM, NY, USA). The Explorys Dataset contains data for approximately 55 million patients (∼15% of US population), integrated from 23 large health systems comprising approximately 360 hospitals and 330,000 providers. The data, collected from EHRs, outgoing billing and adjudicated claims from both commercial and public payers, provides a full longitudinal view of a patient's medical history across the care continuum.
All study data are fully de-identified and were accessed with protocols compliant with US patient confidentiality requirements, including the Health Insurance Portability and Accountability Act of 1996 regulations; therefore, this study was exempted from Institutional Review Board approval.
Patient selection & cohort matching
Patients with at least one record for a large-bore femoral arterial access procedure (TAVR, EVAR, TEVAR or BAV) in the inpatient setting during the enrollment period were selected for analysis. The index date was set as the most recent date for any of the four procedures. The ProGlide cohort included all patients with a ProGlide model number in the EHR medical device record on the index date and no other non-ProGlide VCD recorded on the index date. The Cutdown cohort was comprised of all patients without any VCDs recorded during the entire index procedure hospitalization record or at any other time in the study period.
Model number is not a required element within Explorys; as such, model number is reported only in a minority of large-bore access arterial procedures. As not all Explorys data contributors provide implantable medical device identifiers (i.e., model numbers) to the dataset, Cutdown patients were selected from the same subset of healthcare providers (N = 419) who reported at least one record where a ProGlide device identifier was recorded. This was done to minimize the risk that Cutdown patients were originating from data providers that simply did not provide device identifiers to the database (i.e., false negatives). The result of this criteria is a substantial drop in potential sample size from all patients receiving a large-bore access arterial procedure to just those with receiving a large-bore access arterial procedure who saw a provider who definitely provided ProGlide to at least one patient. In addition, patients with the Healthcare Common Procedure Coding System procedure code C1760: Closure device, vascular (implantable/insertable) in their EHR record on the index date were excluded from either cohort because it could indicate the use of an unspecified VCD.
Patients qualifying for the ProGlide and Cutdown cohorts from the same healthcare providers were then matched in a 1:1 ratio on the following characteristics: index procedure (TAVR, EVAR, TEVAR or BAV), age at index procedure (+/− 5 years), sex, year of index procedure (+/− 1 year), blood transfusion procedure in the 6-month pre-index period (yes/no) and diagnosis of coronary artery disease in the 6-month pre-index period (yes/no).
Outcomes & explanatory variables
Patients were stratified by the procedure(s) performed on the index date based on the presence of procedure codes for TAVR, EVAR, TEVAR or BAV. Patients with more than one procedure on the index date were included in both groups.
Demographic characteristics were assessed at the index date and included age, sex, geographic region and index procedure year. Baseline clinical characteristics were measured in the 6-month pre-index period and included select comorbidities, pre-index diagnosis of clinical outcomes of interest, BMI and pre-index utilization of anticoagulants, antiplatelet medications or methicillin-resistant Staphylococcus aureus (MRSA) indicated antibiotics. BMI categories were defined based on the most recent of any BMI records in the 6-month baseline. Patients were identified as having the selected clinical comorbidity or pre-index clinical outcome of interest if they had at least one record containing an International Classification of Diseases Ninth or Tenth Revision (ICD-9 or ICD-10) diagnosis code for the condition.
The primary outcomes of interest were diagnoses of access-site complications and minor ipsilateral access-site vascular complications. These included pseudoaneurysm, arteriovenous fistula, blood transfusion, hemorrhage, hematoma, lower-extremity arterial emboli/stenosis, deep vein thrombosis and infection. Complications were identified using ICD-9 or ICD-10 diagnosis codes and did not require other criteria. For example, we did not require or capture surgical treatment for hematoma. However, we did capture blood transfusion procedures separately from a bleeding diagnosis and antibiotic use separately from an infection diagnosis.
Complications were assessed during the three post-index follow-up periods: index procedure hospital admission, first 30 days post-index and first 6 months post-index. Patients were identified as having a complication if they had at least one record containing the diagnosis code. Patients were only assessed for 30-day and 6-month post-index outcomes if they had at least one record following the end of the measurement period. Also evaluated were the postsurgery inpatient LOS and hospital readmission following discharge for the index procedure. LOS was calculated as the number of days from the index procedure date through the discharge date. Evidence of death was defined by the recorded year of death and the patients’ last medical record entry occurring during the 30-day and 6-month follow-up periods. The exact death date and reason for death were not available in the database due to privacy concerns.
Healthcare cost analysis
Since the Explorys database does not include cost or charge data, the healthcare cost differences associated with observed clinical outcomes were estimated using administrative claims data from the IBM® MarketScan Commercial Claims and Encounters and Medicare Supplemental and Coordination of Benefits databases (IBM Watson Health, MA, USA). The MarketScan Research Databases comprise enrollment, demographic and inpatient medical, outpatient medical and outpatient pharmacy claims information collected from over 300 large self-insured US employers and over 25 US health plans. The administrative claims do not, however, contain information on ProGlide and other medical implantable devices at the brand level. To our knowledge, there is no database that captures both medical device brand information, which was contained in the Explorys EHR data, and the patient-level cost information found in administrative claims data. Therefore, utilizing this administrative claims database to quantify the cost of clinical outcomes associated with the device, as opposed to a direct comparison of patient costs, was the best and only feasible option for an economic analysis given the available real-world data sources.
Patients undergoing the TAVR, EVAR, TEVAR or BAV in 2016 were identified. Cost differences were applied to the Explorys clinical outcomes by first calculating the average total healthcare costs for patients with and without each complication and the costs per day of the index hospitalization. As a direct cost comparison was not possible, cost differences between ProGlide and Cutdown cohorts were indirectly quantified based on inpatient LOS. The cost-per-day of an inpatient admission for TAVR, EVAR, TEVAR or BAV patients calculated in the claims data was multiplied by LOS results for the two cohorts for use in multivariate modeling which accounts for the skewed distribution of inpatient costs.
Statistical analysis
Bivariate statistics were used to compare all baseline characteristics and outcome variables between the matched ProGlide and Cutdown cohorts. Two-tailed Student's t-tests were used to test for significant differences in the distributions of continuous variables. The χ2tests were used for significance testing of categorical variables.
Generalized linear models with a γ-distribution and log-link function were employed to evaluate LOS and healthcare costs by cohort while adjusting for baseline characteristics. Covariates included in the LOS model were index procedure type, age, sex and a subset of baseline clinical characteristics (anticoagulant use, atherosclerosis, cancer, chronic respiratory disease, myocardial infarction, stroke, blood transfusion). For the healthcare costs generalized linear model, only index procedure type, age and sex were included as covariates.
Results
Patient characteristics
During the enrollment period, a total of 44,039 patients in the Explorys database had a record of TAVR, EVAR, TEVAR or BAV. Of these, 839 patients had evidence of a ProGlide device in their procedure record and met all the selection criteria (Table 1). An additional 2569 patients, treated by the same providers, had no evidence of any VCD in their procedure record and were assigned to the manual surgical cutdown cohort. To reduce the possibility of false negatives from undercoding device usage, cutdown patients were selected only from providers who documented at least one ProGlide procedure.
| Selection criteria | Patients | |
|---|---|---|
| N | % | |
| Patients with at least one record for TAVR, EVAR, TEVAR or BAV from 1 January 2013 to 24 April 2017, the most recent of which will be considered the index date | 44,039 | |
| ProGlide cohort: | ||
| − Patients with evidence of ProGlide device on the index date | 1275 | 2.9% |
| − Patients who had no evidence for other closure devices† on the index date | 841 | 1.9% |
| − Patients with no Healthcare Common Procedure Coding System procedure code (C1760) indicating the use of a closure device | 839 | 1.9% |
| Cutdown cohort: | ||
| − Patients from the same providers identified in the ProGlide Sample (N = 419 providers) who had no evidence for ProGlide or other closure devices† at any time in the data | 2571 | 5.8% |
| − Patients with no Healthcare Common Procedure Coding System procedure code (C1760) indicating the use of a closure device | 2569 | 5.8% |
†
Other closure devices included: AngioSeal, Mynx, ExoSeal, Starclose.
BAV: Balloon aortic valvuloplasty; EVAR: Endovascular abdominal aortic aneurysm repair; TAVR: Transcatheter aortic valve replacement/repair; TEVAR: Thoracic endovascular aortic repair.
Direct 1:1 matching resulted in 757 matched pairs used in the matched ProGlide versus Cutdown analyses. Baseline demographic characteristics in prematched and postmatched cohorts are summarized in Table 2. Prior to matching, patients in the Cutdown cohort were significantly younger (73.0 ± 11.7 years Cutdown vs 76.9 ± 11.3 years ProGlide; p < 0.001) and more likely to be male (69.2 vs 65.3%; p = 0.037).
| Prematched samples | Post 1:1 matched samples | |||||
|---|---|---|---|---|---|---|
| Cutdown | ProGlide | p-value | Cutdown | ProGlide | p-value | |
| n = 2569 | n = 839 | n = 757 | n = 757 | |||
| Age† (mean, SD) | 73.0 (11.7) | 76.9 (11.3) | <0.001 | 76.8 (10.5) | 77.0 (10.7) | 0.756 |
| Male† (N, %) | 1777 (69.2%) | 548 (65.3%) | 0.0373 | 512 (67.6%) | 512 (67.6%) | 1.000 |
| Geographic region (N, %) | ||||||
| − Northeast | 246 (9.6%) | 60 (7.2%) | <0.001 | 65 (8.6%) | 52 (6.9%) | <0.001 |
| − North Central | 1820 (70.8%) | 607 (72.4%) | 552 (72.9%) | 545 (72.0%) | ||
| − South | 409 (15.9%) | 98 (11.7%) | 110 (14.5%) | 89 (11.8%) | ||
| − West | 84 (3.3%) | 71 (8.5%) | 25 (3.3%) | 68 (9.0%) | ||
| − Unknown | 10 (0.4%) | 3 (0.4%) | 5 (0.7%) | 3 (0.4%) | ||
| Index year† (n, %) | ||||||
| − 2013 | 830 (32.3%) | 85 (10.1%) | <0.001 | 137 (18.1%) | 83 (11.0%) | <0.001 |
| − 2014 | 760 (29.6%) | 236 (28.1%) | 219 (28.9%) | 232 (30.6%) | ||
| − 2015 | 601 (23.4%) | 215 (25.6%) | 208 (27.5%) | 187 (24.7%) | ||
| − 2016 | 29 (11.3%) | 236 (28.1%) | 155 (20.5%) | 197 (26.0%) | ||
| − 2017 | 86 (3.3%) | 67 (8.0%) | 38 (5.0%) | 58 (7.7%) | ||
†
Characteristics used in direct matching.
SD: Standard deviation.
Index procedure type and baseline clinical characteristics in prematched and postmatched cohorts are summarized in Table 3. The most commonly performed procedure on the index date was TAVR followed by EVAR. Prior to matching, pre-index procedure blood transfusions were more common in Cutdown cohort (5.2% Cutdown vs 3.5% ProGlide; p = 0.042). After matching, the distribution of index procedure types was 44.9% TAVR, 38.6% EVAR, 21.3% TEVAR and 3.4% BAV. Baseline average BMI and prevalence of clinical comorbidities and outcomes of interest were similar between cohorts after 1:1 matching with the exception of stroke (7.7% Cutdown vs 5.0% ProGlide; p = 0.035). Baseline medication utilization was different between groups after matching, with Cutdown patients have lower utilization of anticoagulants (17.8% Cutdown vs 44.9% ProGlide; p < 0.001) and higher utilization of MRSA antibiotics (27.3% Cutdown vs 11.0% ProGlide; p < 0.001).
| Prematched samples | Post 1:1 matched samples | |||||
|---|---|---|---|---|---|---|
| Cutdown | ProGlide | p-value | Cutdown | ProGlide | p-value | |
| n = 2569 | n = 839 | n = 757 | n = 757 | |||
| Index procedure type† (N, %) | ||||||
| − TAVR | 1422 (55.4%) | 403 (48.0%) | 340 (44.9%) | 340 (44.9%) | 1.000 | |
| − EVAR | 691 (26.9%) | 312 (37.2%) | 292 (38.6%) | 292 (38.6%) | 1.000 | |
| − TEVAR | 527 (20.5%) | 175 (20.9%) | 161 (21.3%) | 161 (21.3%) | 1.000 | |
| − BAV | 170 (6.6%) | 53 (6.3%) | 26 (3.4%) | 26 (3.4%) | 1.000 | |
| Clinical comorbidities (N, %) | ||||||
| − Hypertension | 2048 (79.7%) | 677 (80.7%) | 0.542 | 616 (81.4%) | 606 (80.1%) | 0.515 |
| − Type 2 diabetes | 648 (25.2%) | 200 (23.8%) | 0.420 | 175 (23.1%) | 175 (23.1%) | 1.000 |
| − Chronic respiratory disease | 759 (29.5%) | 246 (29.3%) | 0.902 | 222 (29.3%) | 223 (29.5%) | 0.955 |
| − Myocardial infarction | 164 (6.4%) | 46 (5.5%) | 0.346 | 53 (7.0%) | 38 (5.0%) | 0.105 |
| − Stroke | 205 (8.0%) | 43 (5.1%) | 0.006 | 58 (7.7%) | 38 (5.0%) | 0.035 |
| − Cancer | 262 (10.2%) | 122 (14.5%) | <0.001 | 89 (11.8%) | 110 (14.5%) | 0.110 |
| − Atherosclerosis | 1677 (65.3%) | 551 (65.7%) | 0.835 | 485 (64.1%) | 488 (64.5%) | 0.872 |
| − Coronary atherosclerosis† | 1593 (62.0%) | 515 (61.4%) | 0.746 | 451 (59.6%) | 456 (60.2%) | 0.793 |
| − Other atherosclerosis | 309 (12.0%) | 104 (12.4%) | 0.777 | 98 (12.9%) | 97 (12.8%) | 0.939 |
| − Atherosclerosis of the extremities (any) | 31 (1.2%) | 9 (1.1%) | 0.754 | 10 (1.3%) | 7 (0.9%) | 0.464 |
| − Lower extremity specified | 152 (5.9%) | 41 (4.9%) | 0.262 | 34 (4.5%) | 34 (4.5%) | 1.000 |
| − Renal dysfunction | 759 (29.5%) | 235 (28.0%) | 0.396 | 202 (26.7%) | 208 (27.5%) | 0.729 |
| BMI categories (N, %) | ||||||
| − Underweight (<18.5) | 38 (1.5%) | 16 (1.9%) | 0.646 | 16 (2.1%) | 12 (1.6%) | 0.676 |
| − Normal weight (18.5–24.9) | 643 (25.0%) | 240 (28.6%) | 187 (24.7%) | 217 (28.7%) | ||
| − Overweight (25–29.9) | 926 (36.0%) | 316 (37.7%) | 269 (35.5%) | 286 (37.8%) | ||
| − Obese (≥30) | 795 (30.9%) | 266 (31.7%) | 214 (28.3%) | 241 (31.8%) | ||
| − Unknown | 167 (6.5%) | 1 (0.1%) | 71 (9.4%) | 1 (0.1%) | ||
| Baseline diagnoses for clinical outcomes of interest (N, %) | ||||||
| − Pseudoaneurysm or arteriovenous fistula | 1270 (49.4%) | 433 (51.6%) | 0.274 | 434 (57.3%) | 408 (53.9%) | 0.179 |
| − Pseudoaneurysm or arteriovenous fistula (narrow definition‡) | 119 (4.6%) | 39 (4.6%) | 0.985 | 43 (5.7%) | 34 (4.5%) | 0.292 |
| − Pseudoaneurysm or arteriovenous fistula (broad definition§) | 1232 (48.0%) | 417 (49.7%) | 0.380 | 420 (55.5%) | 398 (52.6%) | 0.257 |
| − Arteriovenous fistula | 4 (0.2%) | 3 (0.4%) | 0.262 | 1 (0.1%) | 3 (0.4%) | 0.317 |
| − Pseudoaneurysm or aneurysm | 1230 (47.9%) | 415 (49.5%) | 0.425 | 420 (55.5%) | 396 (52.3%) | 0.216 |
| − Hemorrhage complicating a procedure | 19 (0.7%) | 3 (0.4%) | 0.230 | 3 (0.4%) | 2 (0.3%) | 0.654 |
| − Blood transfusion procedure† | 133 (5.2%) | 29 (3.5%) | 0.042 | 19 (2.5%) | 19 (2.5%) | 1.000 |
| − Deep vein thrombosis | 75 (2.9%) | 22 (2.6%) | 0.653 | 18 (2.4%) | 18 (2.4%) | 1.000 |
| − Any Infection | 759 (29.5%) | 254 (30.3%) | 0.688 | 202 (26.7%) | 216 (28.5%) | 0.421 |
| − Lower-extremity arterial emboli or stenosis | 108 (4.2%) | 37 (4.4%) | 0.797 | 33 (4.4%) | 35 (4.6%) | 0.804 |
| Baseline medication utilization (N, %) | ||||||
| − Anticoagulants | 471 (18.3%) | 393 (46.8%) | <0.001 | 135 (17.8%) | 340 (44.9%) | <0.001 |
| − Antiplatelets | 21 (0.8%) | 3 (0.4%) | 0.167 | 6 (0.8%) | 3 (0.4%) | 0.316 |
| − Methicillin-resistant Staphylococcus aureus-indicated antibiotics | 850 (33.1%) | 97 (11.6%) | <0.001 | 207 (27.3%) | 83 (11.0%) | <0.001 |
†
Characteristics used in direct matching.
‡
Narrow definition: codes for arteriovenous fistula, aneurysm of artery of upper extremity, aneurysm of artery of lower extremity, aneurysm of other specified site or aneurysm of unspecified site.
§
Broad definition: includes all fistula and aneurysm codes in narrow definition, plus includes aneurysms of other sites (e.g., thoracoabdominal, subclavian artery).
BAV: Balloon aortic valvuloplasty; EVAR: Endovascular abdominal aortic aneurysm repair; SD: Standard deviation; TAVR: Transcatheter aortic valve replacement/repair; TEVAR: Thoracic endovascular aortic repair.
Access-site complications in matched cohorts
During the index procedure hospitalization, patients in the ProGlide cohort were significantly less likely than matched Cutdown patients to receive a blood transfusion (35.7% Cutdown vs 9.5% ProGlide; p < 0.001) or be diagnosed with an infection (22.2% Cutdown vs 15.6% ProGlide; p < 0.001) including infections treated with MRSA-indicated antibiotics (2.6% Cutdown vs 5.0% ProGlide; p < 0.05). Other access-site complications analyzed occurred in less than 10% of patients and did not differ significantly between the matched cohorts, as seen in Figure 1A.
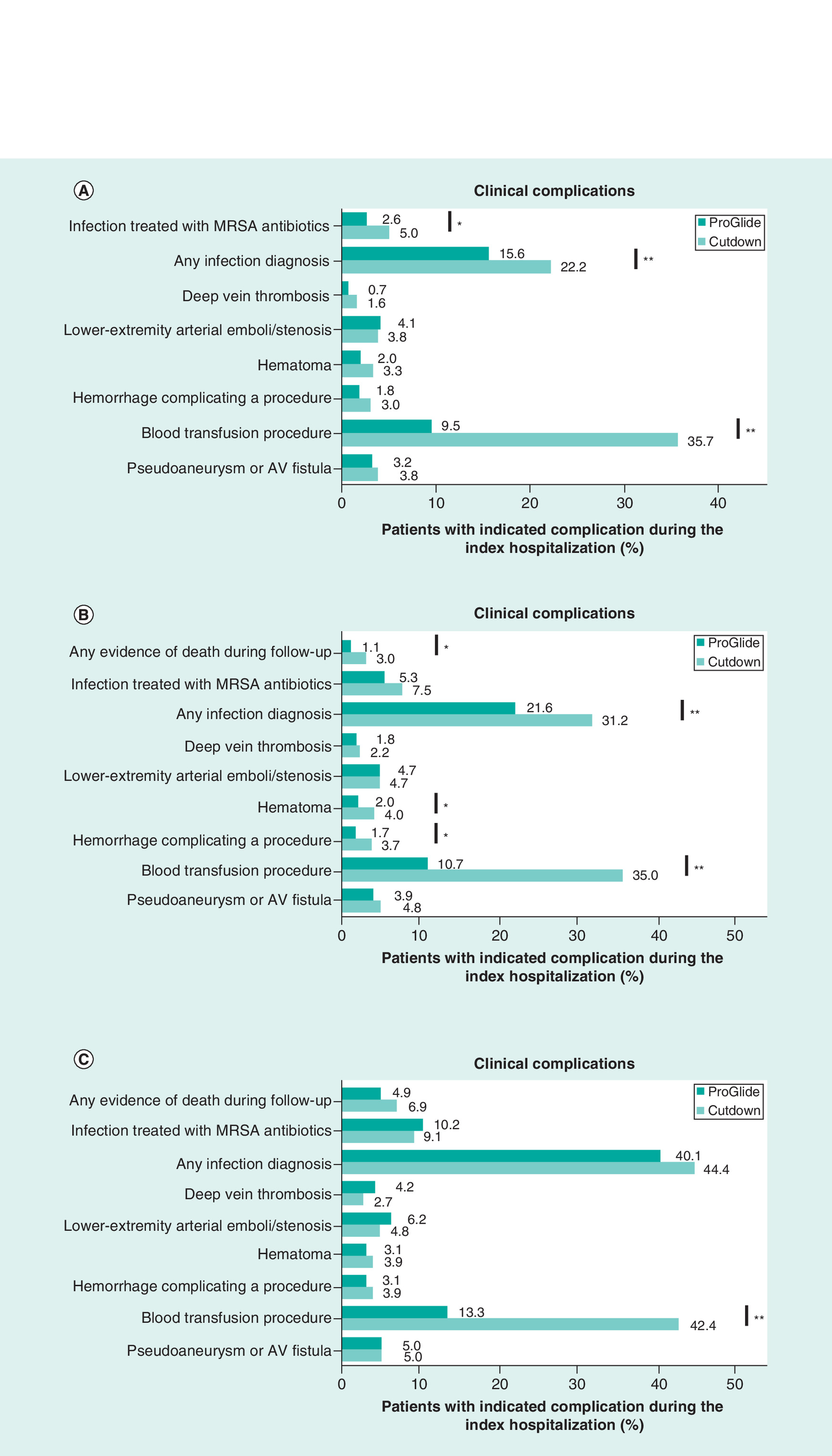
Figure 1. Comparison of prevalence of clinical complications in matched ProGlide and Cutdown cohorts.
(A) Prevalence of select clinical complications during the index hospitalization. N = 757 matched pairs. (B) Prevalence of select clinical complications during the first 30 days post-index. Matched patients with ≥30 days of follow-up: ProGlide N = 662; Cutdown N = 600. (C) Prevalence of select clinical complications during the first 6 months post-index. Matched patients with ≥6 months of follow-up: ProGlide N = 481; Cutdown N = 441.
*Statistically significant difference between cohorts, p < 0.05.
**Statistically significant difference between cohorts, p < 0.001.
AV: Arteriovenous; MRSA: Methicillin-resistant Staphylococcus aureus.
In the first 30 days post-index procedure, fewer patients in the ProGlide cohort received a blood transfusion (35.0% Cutdown vs 10.7% ProGlide; p < 0.001) or were diagnosed with any of the following: infection (31.2% Cutdown vs 21.6% ProGlide; p < 0.001), hematoma (4.0% Cutdown vs 2.0% ProGlide; p < 0.05), bleeding complicating a procedure (3.7% Cutdown vs 1.7% ProGlide; p < 0.05) or evidence of death (3.0% Cutdown vs 1.1% ProGlide; p < 0.05; Figure 1B). At 6 months post-index procedure, the only remaining statistically significant difference in access-site complications between the two cohorts was the likelihood of having received a blood transfusion (42.4% Cutdown vs 13.3% ProGlide; p < 0.001; Figure 1C).
When comparing the subset of matched ProGlide and Cutdown patients who underwent a TAVR procedure at the index date, results remained significant for all outcomes that were significant in the overall comparison, as shown in Table 4. Among the TAVR subset, 39.4% more patients in the Cutdown cohort required a blood transfusion (p < 0.001) and 12.9% more patients were diagnosed with an infection during the index hospitalization (p < 0.001). At 30 days post-index, patients in the Cutdown cohort were more likely to be diagnosed with a hematoma (5.1% Cutdown vs 1.3% ProGlide; p ≤ 0.01), or bleeding complicating a procedure (4.7% Cutdown vs 1.0% ProGlide; p ≤ 0.01). The proportion receiving a blood transfusion during the index hospitalization, 30 days and 6 months post-index were higher among Cutdown patients in EVAR and TEVAR subsets, while other outcomes were not statistically significant.
| Overall sample (matched) | TAVR (matched) | EVAR (matched) | TEVAR (matched) | BAV (matched) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No device | ProGlide | p-value | No device | ProGlide | p-value | No device | ProGlide | p-value | No device | ProGlide | p-value | No device | ProGlide | p-value | |
| N = | 757 | 757 | 340 | 340 | 292 | 292 | 171 | 171 | 26 | 26 | |||||
| Outcomes that were significant in the overall sample | |||||||||||||||
| Index hospitalization | |||||||||||||||
| − Blood transfusion | 35.7% | 9.5% | <0.001 | 48.8% | 9.4% | <0.001 | 24.7% | 9.6% | <0.001 | 29.2% | 9.3% | <0.001 | 26.9% | 19.2% | 0.788 |
| − Infection | 22.2% | 15.6% | 0.001 | 24.4% | 11.5% | <0.001 | 13.4% | 11.3% | 0.450 | 34.8% | 34.8% | 0.695 | 30.8% | 3.8% | 0.072 |
| 30 days post-index (N) | 600 | 662 | 253 | 298 | 255 | 264 | 121 | 133 | 20 | 21 | |||||
| − Blood transfusion | 35.0% | 10.7% | <0.001 | 49.0% | 10.7% | <0.001 | 23.5% | 10.6% | <0.001 | 32.2% | 11.3% | <0.001 | 25.0% | 23.8% | 0.929 |
| − Hemorrhage† | 3.7% | 1.7% | 0.026 | 4.7% | 1.0% | 0.007 | 1.6% | 1.9% | 0.777 | 5.8% | 2.3% | 0.149 | 10.0% | 0.0% | n/a |
| − Hematoma | 4.0% | 2.0% | 0.032 | 5.1% | 1.3% | 0.010 | 2.0% | 2.3% | 0.805 | 6.6% | 3.8% | 0.303 | 10.0% | 0.0% | n/a |
| − Infection | 31.2% | 21.6% | <0.001 | 35.6% | 20.1% | <0.001 | 22.7% | 17.0% | 0.104 | 43.0% | 38.3% | 0.453 | 40.0% | 9.5% | 0.023 |
| 6 months post-index (N): | 441 | 4.81 | 202 | 2.33 | 178 | 191 | 78 | 74 | 15 | 15 | |||||
| − Blood transfusion | 42.4% | 13.3% | <0.001 | 56.4% | 11.2% | <0.001 | 28.1% | 14.7% | <0.001 | 41.0% | 17.6% | 0.002 | 33.3% | 13.3% | 0.195 |
†
Hemorrhage complicating a procedure.
BAV: Balloon aortic valvuloplasty; EVAR: Endovascular abdominal aortic aneurysm repair; SD: Standard deviation; TAVR: Transcatheter aortic valve replacement/repair; TEVAR: Thoracic endovascular aortic repair.
Hospitalization outcomes
The mean inpatient LOS for the index procedure hospitalization was on average 4 days longer for Cutdown patients than ProGlide patients (mean: 9.0 days Cutdown vs 5.1 days ProGlide; p < 0.001; median: 7.0 days Cutdown vs 3.0 days ProGlide; Figure 2). In the 30 days postdischarge, there was no difference in hospital readmissions between cohorts (11.0% Cutdown vs 10.0% ProGlide; p = 0.55). The generalized linear model, after adjusting for baseline differences in covariate, found that inpatient LOS for the ProGlide cohort was 42.5% shorter than for the matched Cutdown cohort (odds ratio [ProGlide vs Cutdown]: 0.575; 95% CI: 0.531–0.619; p < 0.001).
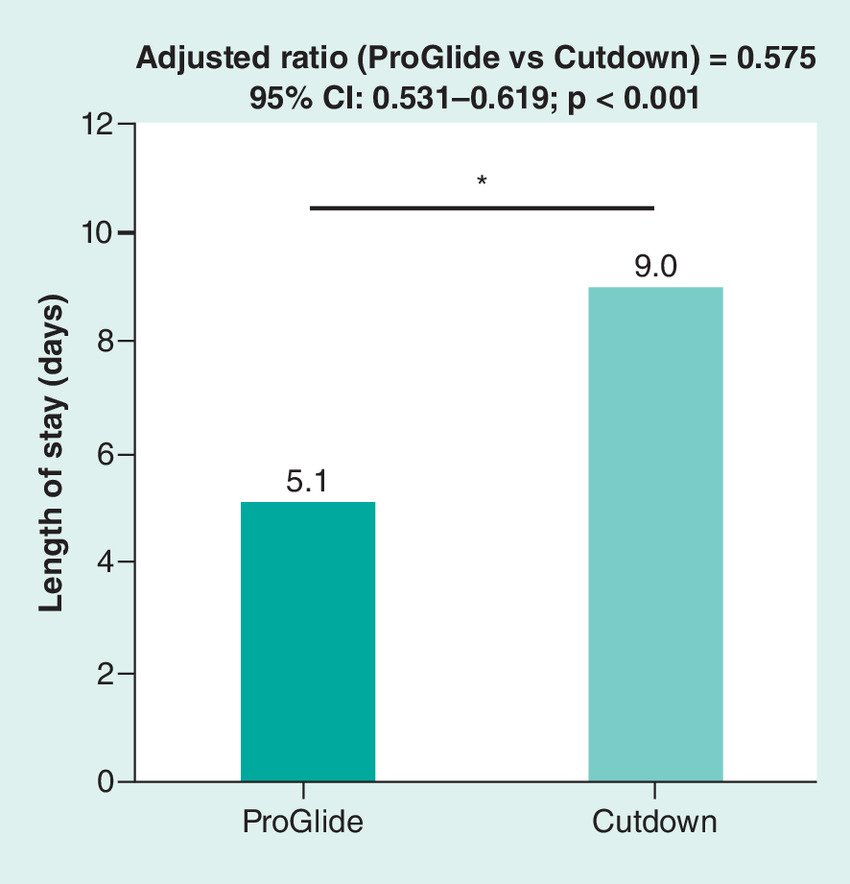
Figure 2. Length of stay of index hospitalization by cohort.
*Statistically significant difference between cohorts, p < 0.001.
Cost analysis
To quantify the predicted inpatient stay cost difference between cohorts, mean and median LOS results obtained from the main analysis were compared. After controlling for index procedure, age and sex, LOS was a significant predictor of costs. (Figure 3; p < 0.05). With an observed 4-day difference in mean index hospitalization LOS, ProGlide was predicted to save $14,687 USD.
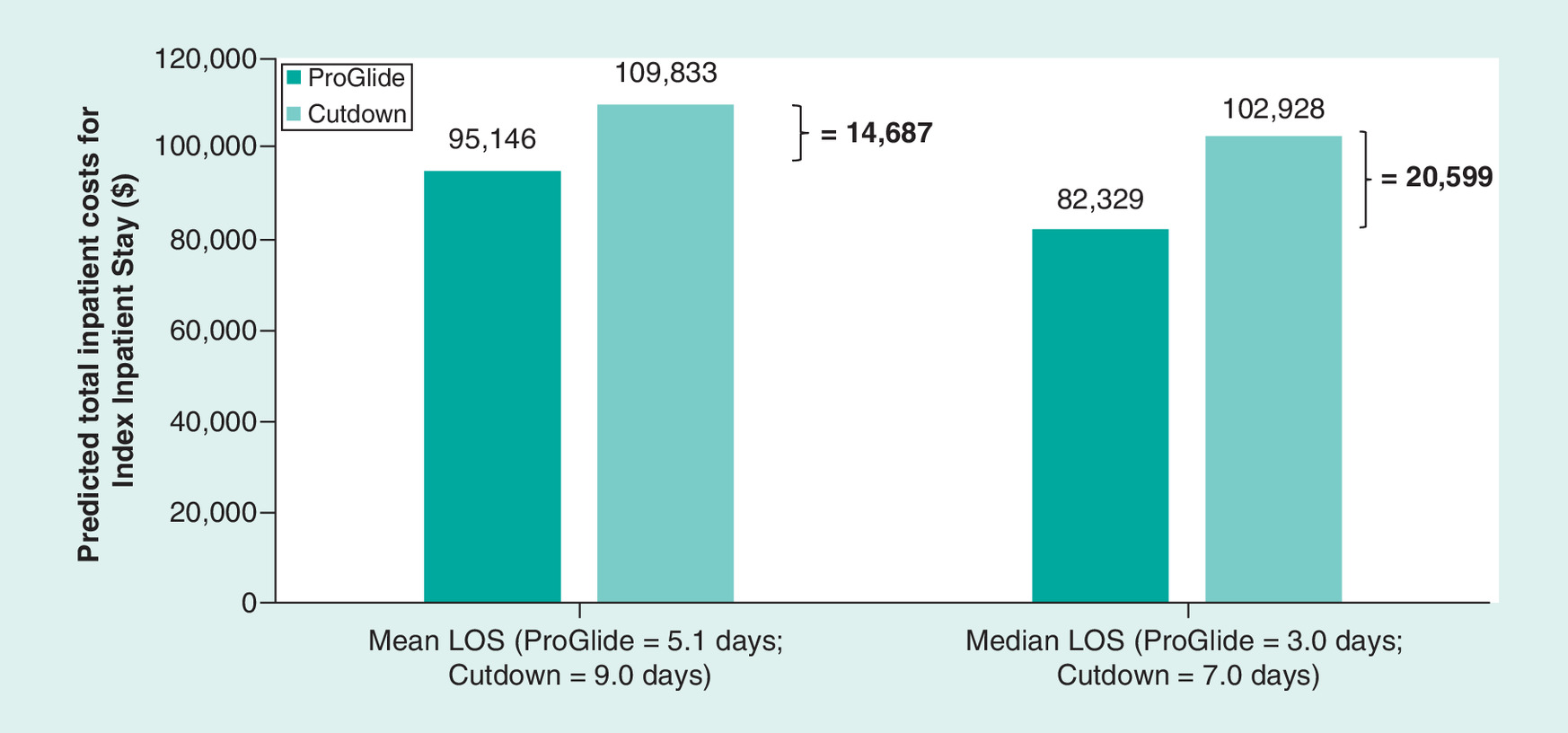
Figure 3. Predicted total inpatient costs for index hospitalization for ProGlide and Cutdown cohorts.
Statistically significant difference between cohorts, p < 0.05.
LOS: Length of stay.
Discussion
The use of ProGlide after percutaneous large-bore access compared with surgical Cutdown for arterial repair was associated with significantly fewer blood transfusions (at all time points), infections (at index and 30 days post-index), hematomas (at 30 days post-index) and bleeding complicating a procedure (at 30 days post-index). Index hospitalization LOS was 4 days shorter for those receiving ProGlide, which, according to administrative claims data, is associated with significantly lower costs for hospitalization following the index procedures. This real-world study suggests there are clinical and financial advantages to using ProGlide over manual surgical Cutdown for femoral artery repair following procedures with large bore arterial access. In particular, percutaneous access with use of VCDs such as ProGlide likely reduce access site-related complications and shorten the postprocedure LOS, thereby reducing overall costs.
In this study, only the TAVR and EVAR patient subsets were large enough to examine the effect of procedure type on complication rates. In general, procedure type did not affect the percentage of complications in the ProGlide cohort. However, consistent with a recent analysis of the National Inpatient Sample database, bleeding and infection complications were less common after EVAR than after TVAR in the cutdown cohort making it harder to detect significant differences in the EVAR subset with the available sample size [12].
The findings in this paper are consistent with those from previous clinical trials. For example, a multicenter, randomized controlled trial of closure methods after percutaneous EVAR found ProGlide mediated vessel repair to be noninferior to surgical Cutdown with a significantly shorter procedure time and time to hemostasis [8]. In a study of 146 patients who underwent EVAR, Ichihashi et al. reported similar rates of access-site complications within 30 days (4% ProGlide vs 8% Cutdown; p = 0.495) and shorter procedure-related hospital LOS (6.7 ± 6.8 days ProGlide vs 9.3 ± 4.5 days Cutdown; p < 0.001) for patients whose repair was completed with a single ProGlide device compared with surgical Cutdown [9]. In a recent study of least invasive fast-track EVAR (N = 250), ProGlide vascular closure, in combination other minimally invasive strategies, resulted in next day discharge of 216 (86%) patients with only 8 (3.2%) patients requiring conversion to surgical cutdown and 2 (0.8%) patients requiring a blood transfusion during hospitalization.
A single-center study of ProGlide vessel repair after elective diagnostic cardiac catheterization found that ProGlide was associated with a shorter postprocedure LOS (59.6 ± 41.7 min ProGlide vs 349.9 ± 30.6 min Cutdown; p < 0.001) and an incremental per patient per procedure cost savings of US$983.6 compared with surgical Cutdown [10]. A study of TEVAR using the ProGlide preclosing technique reported LOS comparable to those found in this study (7.5 ± 5.3 days ProGlide vs 10.5 ± 5.0 days Cutdown) though total hospitalization costs were similar between cohorts in this Korean study [13]. A recent meta-analysis of randomized clinical trials and cohort studies on the use of ProGlide or ProStar VCDs in EVAR, TEVAR or TAVR found that use of a VCD was associated with lower odds of postoperative seroma, wound dehiscence and surgical site infections [14]. Overall, the results of this study are supported by the existing literature with the understanding that surgical technique and patient selection remain important factors when deciding closure strategy.
To our knowledge, Explorys is the only large-scale database in the US with implantable device model number data available to facilitate this type of analysis. ProGlide had the highest utilization of all VCDs in this database and was the only VCD with a sufficient sample size for the desired analysis. In future studies we hope to repeat this analysis when there may be sufficient counts in other VCDs for a meaningful comparison.
Limitations
Studies based on EHR data and administrative claims data have several inherent limitations. First, the EHR database does not include specific information regarding arterial anatomy (i.e., artery diameter, calcification or occlusive disease) that could influence patient selection for either VCD or Cutdown. Second, we are not able to identify or exclude patients in the ProGlide cohort who had a simultaneous cutdown procedure in the contralateral groin. Third, data collected for administrative purposes may not be collected and validated with the same rigor as data collected for researcher purposes; therefore, these datasets are subject to miss-coding and under-coding which may introduce bias or measurement error. However, there is no reason to expect systematic differences in the frequency or type of data collection errors between cohorts. Fourth, with regards to the clinical outcomes analysis, any care for complications received outside of Explorys healthcare partners would not be captured in the dataset. As a result, this study may be under-reporting the frequency of access-site complications; however, there is no reason to believe this would impact one cohort more than the other. Fifth, use of a VCD is not reported in the MarketScan administrative claims database, so cost estimates were limited to an indirect comparison based on hospitalization LOS and did not adjust for device usage. Future research using a combined dataset of EMR records and insurance claims could investigate differences in direct healthcare costs between these patient cohorts. At last, as stated above, implantable device model number is not a required field in Explorys and is, in fact, only available on a minority of Explorys patients. Because of this, the Cutdown cohort was limited to patients seen by healthcare providers who had at least one ProGlide patient (i.e., contributed data to the database with an implantable device model number). To help minimize potential confounding, we then matched this subset of patients based on parameters available into the EHR (index procedure, age, sex, index year, pre-index blood transfusion and pre-index coronary artery disease), there may be unreported factors which influence provider choice that we could not control for. For example, provider type/location (radiology, cardiology, vascular surgery) are not reported consistently across data providers there for this could not be incorporated into our matching procedure despite having a potential impact on outcomes.
Conclusion
Analysis of real-world data found an association between use of the Perclose ProGlide VCD and lower blood transfusion rates, fewer infections and shorter postsurgery index hospitalizations compared with patients who received the surgical Cutdown closure method after large-bore arterial access. Analysis of real-world administrative claims data found that shorter hospital stay after use of ProGlide was associated with significantly lower costs. This study provides novel information on cost estimates and shows beneficial cost-savings from a shortened LOS among ProGlide patients in comparison to surgical cutdown for arterial closure after procedures requiring large-bore access.
•
Perclose ProGlide and surgical cutdown are two approaches to arterial closure after a large-bore arterial access procedure.
•
Explorys electronic health records were to compare complication rates at index, 30 days and 6 months and index hospitalization duration between matched cohorts.
•
Use of ProGlide for vascular closure was associated with lower blood transfusion rates and fewer infections than surgical cutdown at index and 30 days post-index.
•
Rates of deep vein thrombosis, lower-extremity arterial emboli/stenosis, hematoma, hemorrhage complicating a procedure and pseudoaneurysm or arteriovenous fistula occurred in <5% of patients and did not differ significantly between cohorts during index hospitalization.
•
The duration of hospitalization was 42% shorter among patients who received ProGlide compared with surgical cutdown.
•
Using costs derived from the Marketscan claims database, we estimate cost savings of US$14,687–20,599 from shortened hospitalization stays.
Author contributions
The design and analysis for this study was conducted primarily at IBM Watson Health by IBM employees E Thiel and M Bonafede. E Thoma, J Hasegawa, D Scheider, Z Krajcer and P Bhounsule provided substantial intellectual support in the design, analysis and reporting of the research. All authors contributed to, reviewed and approved of the final draft of this manuscript.
Acknowledgments
Programming support was provided by B Ivanov of IBM Watson Health. Development of research plan and interpretation of results were supported by W Lee from Abbott Vascular.
Financial & competing interests disclosure
This study was funded by Abbott Vascular, CA. USA. E Thiel and M Bonafede are IBM Watson Health employees and received funding from Abbot Vascular to perform this study. E Thoma, J Hasegawa and P Bhounsule are employees of Abbott Vascular. D Scheider and Z Krajcer were paid consultants of Abbot Vascular. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing support was provided by JP Winer-Jones of IBM Watson Health. These services were paid for by Abbott Vascular.
Ethical conduct of research
All study data are fully de-identified and were accessed with protocols compliant with US patient confidentiality requirements, including the Health Insurance Portability and Accountability Act of 1996 regulations; therefore, this study was exempted from Institutional Review Board approval.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Dencker D, Pedersen F, Engstrøm T et al. Major femoral vascular access complications after coronary diagnostic and interventional procedures: a Danish register study. Int. J. Cardiol. 202, 604–608 (2016).
• Comprehensive analysis of complications from femoral access procedures.
2.
Baim DS, Knopf WD, Hinohara T et al. Suture-mediated closure of the femoral access site after cardiac catheterization: results of the Suture to Ambulate aNd Discharge (STAND I and STAND ii) trials. Am. J. Cardiol. 85(7), 864–869 (2000).
3.
Dosluoglu HH, Cherr GS, Harris LM, Dryjski ML. Total percutaneous endovascular repair of abdominal aortic aneurysms using Perclose ProGlide closure devices. J. Endovasc. Ther. 14(2), 184–188 (2007).
4.
Martin JL, Pratsos A, Magargee E et al. A randomized trial comparing compression, Perclose Proglide and Angio-Seal VIP for arterial closure following percutaneous coronary intervention: the CAP trial. Catheter. Cardiovasc. Interv. 71(1), 1–5 (2008).
5.
Buck DB, Karthaus EG, Soden PA et al. Percutaneous versus femoral cutdown access for endovascular aneurysm repair. J. Vasc. Surg. 62(1), 16–21 (2015).
6.
Uhlmann ME, Walter C, Taher F, Plimon M, Falkensammer J, Assadian A. Successful percutaneous access for endovascular aneurysm repair is significantly cheaper than femoral cutdown in a prospective randomized trial. J. Vasc. Surg. 68(2), 384–391 (2018).
7.
Kerré S, Kustermans L, Vandendriessche T et al. Cost−effectiveness of contemporary vascular closure devices for the prevention of vascular complications after percutaneous coronary interventions in an all-comers PCI population. EuroIntervention 10(2), 191–197 (2014).
8.
Nelson PR, Kracjer Z, Kansal N et al. A multicenter, randomized, controlled trial of totally percutaneous access versus open femoral exposure for endovascular aortic aneurysm repair (the PEVAR trial). J. Vasc. Surg. 59(5), 1181–1193 (2014).
9.
Ichihashi T, Ito T, Kinoshita Y, Suzuki T, Ohte N. Safety and utility of total percutaneous endovascular aortic repair with a single Perclose ProGlide closure device. J. Vasc. Surg. 63(3), 585–588 (2016).
10.
Sekhar A, Sutton BS, Raheja P et al. Femoral arterial closure using ProGlide(R) is more efficacious and cost-effective when ambulating early following cardiac catheterization. Int. J. Cardiol. Heart Vasc. 13(Suppl. C), 6–13 (2016).
•• Prospective study which demonstrates potential for cost saving from early ambulation.
11.
Krajcer Z, Ramaiah VG, Henao EA et al. Perioperative outcomes from the prospective multicenter least invasive fast-track EVAR (LIFE) registry. J. Endovasc. Ther. 25(1), 6–13 (2018).
12.
Redfors B, Watson BM, Mcandrew T et al. Mortality, length of stay, and cost implications of procedural bleeding after percutaneous interventions using large-bore catheters. JAMA Cardiol. 2(7), 798–802 (2017).
13.
Ni ZH, Luo JF, Huang WH et al. Totally percutaneous thoracic endovascular aortic repair with the preclosing technique: a case−control study. Chin. Med. J. (Engl.) 124(6), 851–855 (2011).
14.
Vierhout BP, Pol RA, El Moumni M, Zeebregts CJ. Arteriotomy closure devices in EVAR, TEVAR, and TAVR: a systematic review and meta-analysis of randomised clinical trials and cohort studies. Eur. J. Vasc. Endovasc. Surg. 54(1), 104–115 (2017).
•• Comprehensive analysis and comparison of use of closure devices in large bore access procedures.
Information & Authors
Information
Published In
Pages: 1381 - 1392
PubMed: 31670598
Copyright
© 2019 Future Medicine Ltd.
History
Received: 26 June 2019
Accepted: 25 September 2019
Published online: 31 October 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Clinical and economic outcomes of ProGlide compared with surgical repair of large bore arterial access. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0082
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Masashi Kawabori, Chris A. Jackel, Jo-Ann Nugent, Anna Y. Johnson, Tony Mangino, Jamel Ortoleva, Meta-analysis: percutaneous versus surgical VA-ECMO decannulation demonstrates no clear differences in most outcomes, with a signal toward lower infection, Journal of Artificial Organs, 10.1007/s10047-026-01562-x, 29, 3, (2026).
- Kareem El Sherbiny, Natasha Hasemaki, Theodosios Bisdas, Yassine Haddad, Sallameh Al-Jamal, Konstantinos Stavroulakis, Clinical outcomes and cost analysis of plug-based versus suture-based vascular closure devices for percutaneous large bore aortic procedures, Vasa, 10.1024/0301-1526/a001278, (2026).
- Sven Ross Mathisen, Simen Tveten Berge, A seven-year single-center experience with large-bore percutaneous closure in endovascular aneurysm repair, Vascular, 10.1177/17085381261429288, (2026).
- Majd Ismail, Dilara Merve Berberoglu Aydin, Jang-Sun Lee, Markus Schönburg, Efstratios Charitos, Yeong-Hoon Choi, Oliver Joannis Liakopoulos, Femoral vessel cannulation strategies in minimally invasive cardiac surgery: single Perclose ProGlide versus open cut-down, European Journal of Cardio-Thoracic Surgery, 10.1093/ejcts/ezaf118, 67, 4, (2025).
- Li Guanqiang, Hu Bo, Sun Yuan, Chen Ming, Zhang Xicheng, Huang Xianchen, Invention of a new percutaneous closure technique for vascular haemostasis in percutaneous veno-arterial extracorporeal membrane oxygenation, European Journal of Medical Research, 10.1186/s40001-025-02307-x, 30, 1, (2025).
- Tomás Marques Pereira, Diana Martins-Fernandes, Ana Rita Ferreira, Henrique Guedes da Rocha, Mario D’Oria, João Rocha-Neves, Assessment of safety and effectiveness after percutaneous closure for decannulation of Veno-Arterial Extracorporeal Membrane Oxygenation: A systematic review and meta-analysis, The Journal of Vascular Access, 10.1177/11297298241312753, 26, 6, (1795-1805), (2025).
- Diana Martins-Fernandes, João Rocha-Neves, Ana Rita Ferreira, Hélio Martins, Sérgio Gaião, José Artur Paiva, Assessment of percutaneous closure for decannulation of veno-arterial extracorporeal membrane oxygenation: A retrospective study, The Journal of Vascular Access, 10.1177/11297298241300119, 26, 5, (1651-1660), (2024).
- Kaiyi Peng, Linhui Hu, Xiangwei Huang, Yuemei He, Xinxin Wu, Huihua Li, Wentao Zhang, Hengling Zhu, Zheng Wang, Chunbo Chen, Innovative Percutaneous 3-Stitch Suture Technique for Site Closure in Venoarterial Extracorporeal Membrane Oxygenation Decannulation Without Direct Artery Repair: A Case Series, ASAIO Journal, 10.1097/MAT.0000000000002198, 70, 9, (787-794), (2024).
- Alison Y Zhu, Charis QY Tan, Graham Meredith, Comparison of percutaneous decannulation and open surgical repair for large-bore arterial access sites of extracorporeal membrane oxygenation, Perfusion, 10.1177/02676591241241609, 40, 2, (308-316), (2024).
- Guangfeng Sun, Shan Huang, Guoming Zhang, Zhixiang Zhang, Bin Wang, Outcomes comparison between percutaneous decannulation with perclose ProGlide and surgical decannulation of veno-arterial extracorporeal membrane oxygenation, Perfusion, 10.1177/02676591231194761, (2023).