Does evidence matter? Comparative effectiveness research and prescribing of Type 2 diabetes mellitus drugs
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Comparative effectiveness research (CER) can help ascertain value of new drugs; however, limited research assesses the translation of CER into clinical practice. The objective of this study was to analyze the association between CER evidence and prescribing trends within two markets of Type 2 diabetes mellitus. Methods: A retrospective analysis to determine the prescribing trends from 2006 to 2016 and an electronic literature search to identify CER comparing different drugs was conducted. Results: In glucagon-like peptide-1 (GLP-1) agonists market, CER showed superiority of Liraglutide. Prescribing of Exenatide twice daily dropped by 50% points as Liraglutide entered the market. In dipeptidyl peptidase-4 (DPP4) inhibitors market, CER did not suggest conclusive superiority. Nevertheless, Sitagliptin, the first entrant, continued to dominate throughout. Conclusion: CER evidence appeared to be associated with prescribing trends in GLP-1 agonists market; however, no associations were found in DPP4 inhibitors market. The translation of evidence into practice can be limited by the availability of superiority trials and timing of their availability.
It is becoming increasingly challenging to ascertain the value of new drug therapies in the US healthcare system [1,2]. Real-world evidence comparing the benefits and harms of different drugs, also called comparative effectiveness research (CER), can act as a strong tool in assisting patients, providers and payers to quantify the value of healthcare and make informed clinical decisions [3]. There is a growing emphasis on generating CER [4] and integrating it into prescribing and coverage decisions [5,6]. The American Recovery and Reinvestment Act of 2009 allocated US$1.1 billion toward CER generation, which led to a rapid increase in the volume of CER evidence for various disease conditions [4,7]. However, limited knowledge exists regarding the extent to which the CER evidence is incorporated into clinical practice [3,7–9].
CER can be generated using various study designs, namely meta-analysis and systematic reviews (MA and SRs), randomized controlled trials (RCTs) and observational studies [10–12]. RCTs are considered the gold standard; however, MA and SRs conducted using RCTs are also considered high-quality evidence and currently at the top of the hierarchy [13]. With a consensus around the importance of hierarchy of CER evidence for decision making [14,15], the impact of different CER study designs proving superiority versus noninferiority and timing of their availability on prescribing has not been explored yet [16].
The Institute of Medicine has recommended diabetes as one of the high-priority disease areas for generating more CER evidence [17]. Around 9.4% of the US population (~30.3 million people) had diabetes in 2015, with an estimated 1.5 million new cases being diagnosed every year [18]. It is also the seventh leading cause of death in the USA. According to a recent report by the American Diabetes Association, the total direct and indirect cost burden of diagnosed diabetes was US$327 billion in the USA in 2017 [19]. The high economic and utilization burden of diabetes is predominantly due to Type 2 diabetes mellitus (DM), accounting for 90–95% of all the diagnosed cases [20].
To manage Type 2 DM in adults, different drugs have been approved in the USA. Two recent therapeutic categories with drugs approved as an adjunct to diet and exercise to improve glycemic control are: glucagon-like peptide-1 (GLP-1) agonists and dipeptidyl peptidase-4 (DPP4) inhibitors. GLP-1 agonists include Exenatide twice daily (BID) approved in 2005, Exenatide once weekly (QW) approved in 2012, Liraglutide approved in 2010, Albiglutide approved in 2014 (now discontinued) and Dulaglutide approved in 2014 [21]. DPP4 inhibitors include Sitagliptin approved in 2006, Saxagliptin approved in 2009, Linagliptin approved in 2011 and Alogliptin approved in 2013 [21]. Abundant CER evidence comparing the drugs has been being generated; however, the extent to which this evidence is being adopted by decision makers into clinical practice is limited. The underlying hypothesis of this study was that the presence of high-quality CER evidence proving superiority of a drug could change the prescribing trends in favor of that drug. If CER evidence is inconsequential, prescribing behavior could alter to eliminate drugs with little or no added benefit from the market [16].
Aim
The aim of this study was to assess the association between the CER evidence and drug prescribing trends within two markets of Type 2 DM: GLP-1 agonists and DPP4 inhibitors.
Methods
Data
Two kinds of data were examined: prescribing trends and CER. Prescribing trends were determined using a retrospective, longitudinal analysis of the Medical Expenditure Panel Survey (MEPS) data from January 1, 2006 to December 31, 2016. In the MEPS data, the Prescribed Medicine Event file was used to obtain the prescribed medication name, National Drug Code, unique respondents with a prescription of the medication and the Multum Lexicon therapeutic classification codes to identify ‘anti-diabetic’ drugs. This file was merged with the Household Component file of the MEPS to extract the ‘self diagnosis' variable. The sources of CER evidence were Cochrane library and MEDLINE. A comprehensive literature review was conducted to identify CER evidence published from January 1, 2006 to December 31, 2016. Based on the most widely used traditional hierarchy [11,12], this study explored MA and SRs as the first set of CER evidence, and RCTs as the next. Specific search strategies and inclusion–exclusion criteria were used to select the studies (Figures 1 & 2).

Figure 1. Selection of studies for glucagon-like peptide-1 (GLP-1) agonists market.
GLP-1: Glucagon-like peptide-1; MA: Meta-analysis; RCT: Randomized controlled trials; SR: Systematic review.
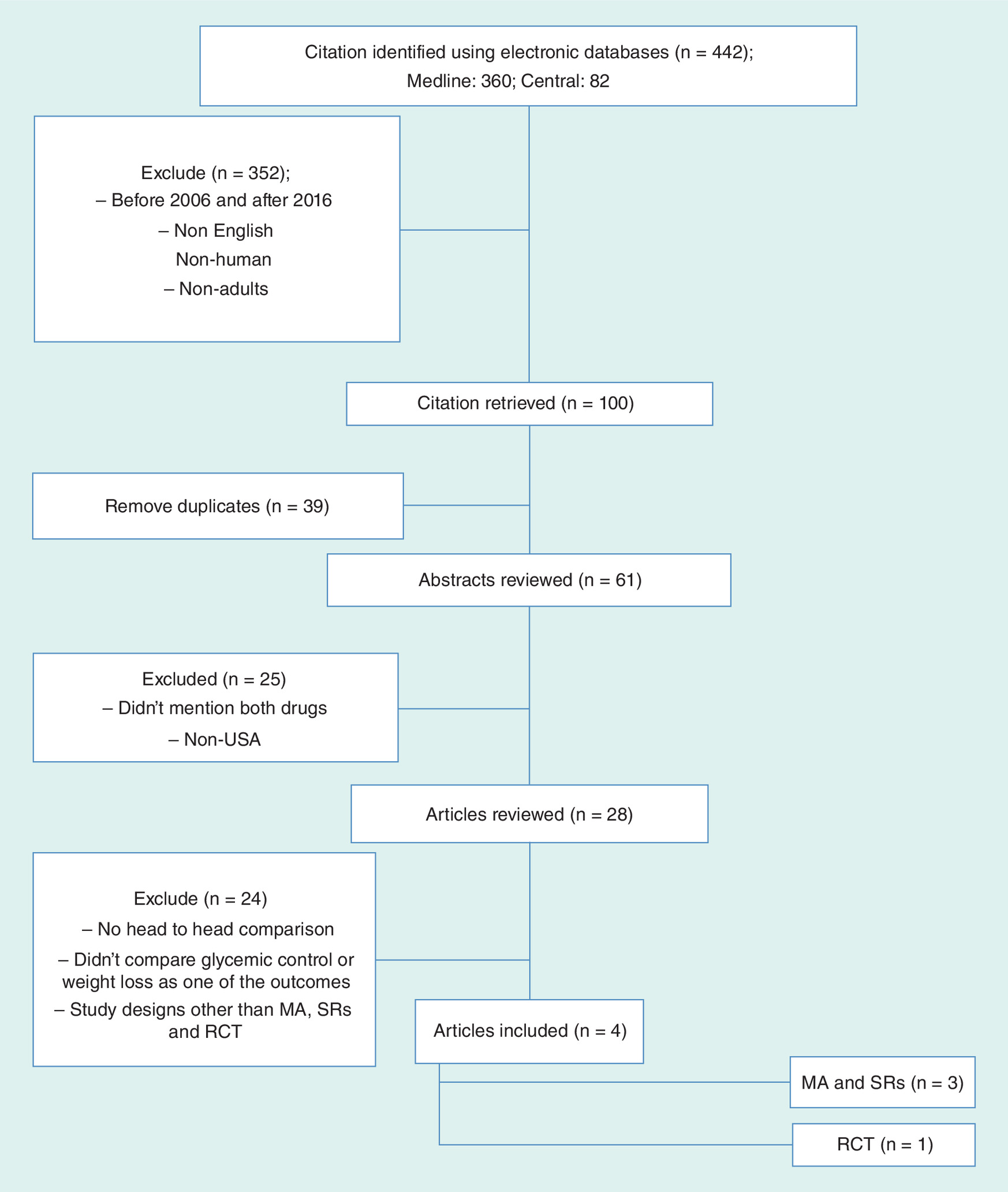
Figure 2. Selection of studies for dipeptidyl peptidase-4 (DPP4) inhibitors market.
DPP4: Dipeptidyl peptidase-4; MA: Meta-analysis; RCT: Randomized controlled trials; SR: Systematic review.
Variables
The outcome variable, annual drug prescribing, was measured as the number of unique respondents with one or more prescriptions of the drug in each year, determined separately for GLP-1 agonists and DPP4 inhibitors. The year (or time) of availability of CER evidence for each market was the intervention variable.
Statistical analysis
The outcome variable, determined using MEPS, was weighted using the survey weights and clustered standard errors to represent the US noninstitutionalized population. This part of the analysis was conducted using STATA MP 4-Core, version 15 (Stata Corporation, TX, USA). The outcome variable was plotted with time, and trends analysis was conducted with values of the slope, direction of the trends (i.e., the sign of the slope) and R-squared displayed for each market. The percentage change in the outcome variable was also determined for each year. The intervention variable was indicated on the plots for each market, representing the year of CER evidence availability.
Results
GLP-1 agonists market
Exenatide BID, Exenatide QW and Liraglutide constituted the GLP-1 agonists market, due to zero observations reported for Dulaglutide in the MEPS database and discontinuation of Albiglutide. Figure 3 shows the trends of the unique respondents being prescribed GLP-1 agonists along with the CER evidence from 2009 to 2016. Figure 3 also depicts the percentage point change from the previous year in the number of unique respondents being prescribed each GLP-1 agonists.
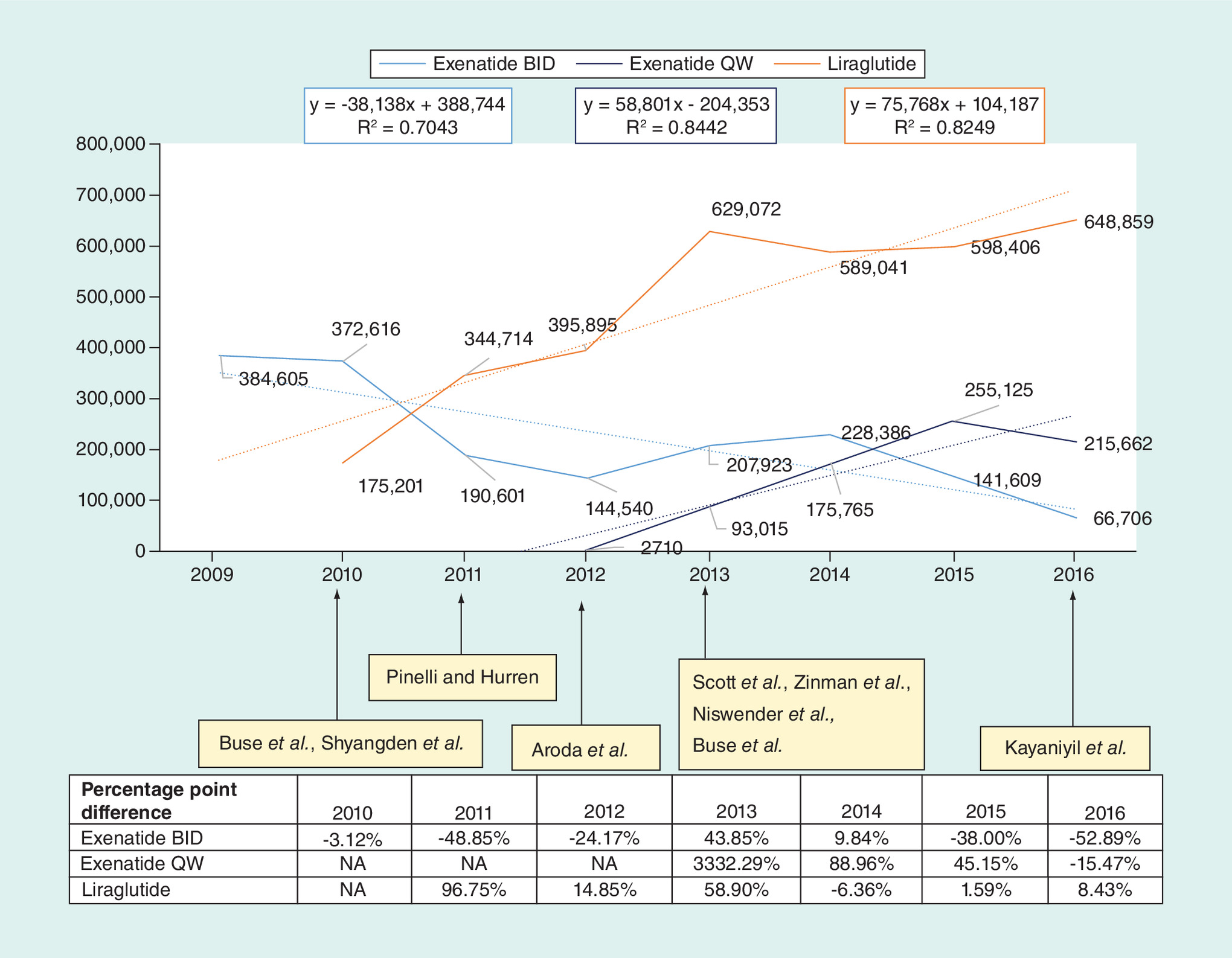
Figure 3. Yearly trends and percentage point difference in unique patients prescribed GLP-1 agonists (Exenatide twice daily, Exenatide once weekly, Liraglutide) from 2009 to 2016, plotted with CER.
Availability of CER evidence are presented on the graph, referenced with the name of the first author and arrows marking the year evidence was published.
BID: Twice daily; CER: Comparative effectiveness research; GLP-1: Glucagon-like peptide-1; NA: Not applicable; QW: Once weekly.
After the approval of Liraglutide in 2010, the number of unique patients being prescribed Exenatide BID dropped almost 50 percentage points, in other words, from 372,616 in 2010 to 190,601 in 2011 (Figure 3). The prescribing trends of Liraglutide continued to increase until 2013 and then plateaued. Prescribing trends of Exenatide BID follow a downward trend throughout the time frame. However, the new dosage of Exenatide prescribed QW follow an upward trend throughout.
CER evidence for the GLP-1 agonists market included nine studies, of which seven were MA and SRs and two were RCTs. Supplementary Material 1 summarizes the characteristics of the included studies. According to the evidence presented by the MA and SRs, both Exenatide QW and Liraglutide were clinically superior to Exenatide BID, with no meaningful differences reported between Exenatide QW and Liraglutide [22–26]. The reductions in Hemoglobin (Hb) A1c level was higher for Exenatide QW (-1.54%) and Liraglutide (-1.22%) compared with Exenatide BID (-1.08%) [22]. One study reported [24] that more patients being treated with Exenatide QW or Liraglutide achieved an HbA1c <7% compared with Exenatide BID. Another study [27] reported that the odds of achieving HbA1c <7% without weight gain or hypoglycemia were two times higher for Liraglutide compared with Exenatide BID. Similar reductions in weight were reported among the patients using Exenatide BID, Exenatide QW and Liraglutide [22–24,26,28].
According to the evidence presented by the two RCTs, Liraglutide was clinically superior to both the dosages of Exenatide [29–31]. The RCT comparing Liraglutide and Exenatide BID showed that, Liraglutide resulted in a significant reduction in HbA1c and fasting plasma glucose level with estimated treatment difference of -0.33% and -1.01 mmol/l respectively. Also, the proportion of patients achieving the HbA1c <7% goal were significantly higher with Liraglutide compared with Exenatide BID. No significant differences in weight loss or adverse events were reported for the two drugs. According to the RCT comparing Liraglutide and Exenatide QW [31], change in HbA1c at the endpoint was significantly greater in patients taking Liraglutide (-1.48%) compared with Exenatide QW (-1.28%). Also, significantly higher proportion of Liraglutide patients achieved HbA1c <7% goal and experienced higher reduction in the mean fasting serum glucose, compared with Exenatide QW. However, frequency of adverse events including nausea, diarrhea and vomiting was lower in patients using Exenatide QW compared with Liraglutide. Overall, consolidating the CER evidence presented by RCTs, Liraglutide was clinically superior to Exenatide BID and Exenatide QW.
DPP4 inhibitors market
Sitagliptin, Saxagliptin and Linagliptin constituted the DPP4 inhibitors market, due to null observations reported for Alogliptin in MEPS database. Figure 4 shows the trends of the unique respondents being prescribed DPP4 inhibitors along with the CER evidence from 2007 to 2016. Figure 4 also depicts the percentage point change from the previous year in the number of unique respondents being prescribed each DPP4 inhibitor.
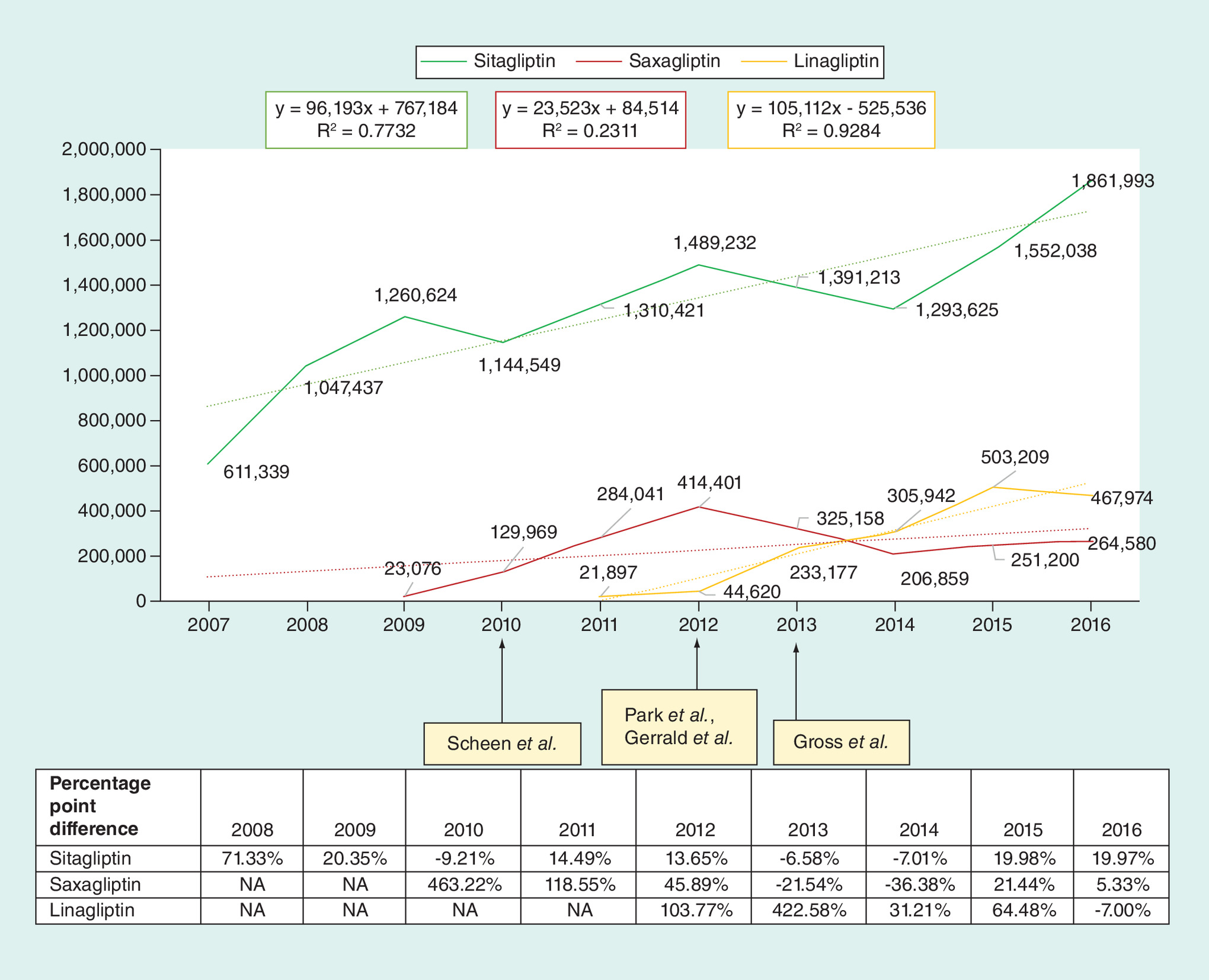
Figure 4. Yearly trends and percentage point difference in unique patients prescribed DPP4 inhibitors (Sitagliptin, Saxagliptin and Linagliptin) from 2007 to 2016, plotted with CER.
Availability of CER evidence are presented on the graph, referenced with the name of the first author and arrows marking the year evidence was published.
CER: Comparative effectiveness research; DPP4: Dipeptidyl peptidase-4; NA: Not applicable.
There was an upward trend in annual prescribing for all three DPP4 inhibitors. Prescribing of Sitagliptin followed an upward trend since its year of approval (2007). The first drop in Sitagliptin prescribing was seen in 2010, which is when Saxagliptin, was approved. The drop in the number of unique patients being prescribed Sitagliptin was similar to the number of unique patients being prescribed Saxagliptin in 2010. Prescribing of Saxagliptin follow an upward trend since its year of approval (2009). However, prescribing of both Sitagliptin and Saxagliptin drops from 2012 to 2014, which is when Linagliptin entered the market. After 2014, the prescribing trends for all DPP4 inhibitors continued to rise.
CER evidence for the DPP4 inhibitors market included four studies, of which three were MA and SRs and one was RCT. Supplementary Material 2 summarizes the characteristics of the included studies. Among the MA and SRs, contradictory evidence exists about the clinical superiority of the three DPP4 inhibitors. There were two MA and SR studies published in 2012 [32,33] and the third model-based MA published in 2013 [34]. One of the 2012 studies [32] suggested that Sitagliptin and Saxagliptin were not statistically significant in reducing HbA1c, and showed similar differences in weight change and rates of hypoglycemia. The other 2012 study [33] suggested that Sitagliptin versus placebo showed a HbA1c reduction of 0.74%, compared with 0.57% with Saxagliptin and 0.68% with Linagliptin. However, Sitagliptin versus placebo was associated with a higher risk of hypoglycemia compared with Saxagliptin and Linagliptin. The 2013 study [34] reported that Linagliptin was as effective as Sitagliptin in reducing the HbA1c levels by 0.81% (placebo adjusted) after 24-week of treatment.
According to the evidence presented in the RCT [35], there was no significant difference in the outcomes between Sitagliptin and Saxagliptin. The RCT showed the mean HbA1c reduction of -0.52 and -0.62% with Saxagliptin and Sitagliptin, respectively, with a between-group difference of 0.09%, demonstrating noninferiority. Both treatments were generally well tolerated, and incidence and types of adverse events were comparable between the two drugs. Overall, the CER evidence was inconclusive in establishing the superiority of any one drug, and suggest that all three DPP4 inhibitors were similar in terms of clinical outcomes.
Discussion
Our results showed that CER evidence did appear to influence physician prescribing in GLP-1 agonists market; however, the associations depend on the kind of study design proving superiority and the timing of its availability. Another past study [8] assessed the impact of four unrelated CER studies, and found an association between two of the CER trials and utilization patterns. However, it failed to ascertain the value of different study designs used to generate CER evidence and the impact of a consolidated evidence on a specific therapeutic category. Also, it was conducted using a single source of claims data, limiting its generalizability to US population. Our study attempts to address these gaps by focusing on Type 2 DM drugs and providing a comprehensive comparative effectiveness literature evaluation of MA and SRs and RCTs, important for the clinical decision making within a therapeutic market.
According to our study, Liraglutide prescribing dominated the GLP-1 agonists market throughout after 2010. Although MA and SRs did not show superiority of Liraglutide over Exenatide QW, the prescribing trends of Liraglutide appear to be associated with the RCT evidence and the year it was published. The QW dose of Exenatide might have favored its prescribing over the BID dose of Exenatide due to adherence [36], however, both the dose forms of Exenatide were dominated by Liraglutide in the GLP-1 agonists market. There have been recent arguments [37] suggesting RCTs, especially which mimic pure experimental conditions, to be considered the best quality evidence and therefore, removing MA and SRs from the top of the evidence pyramid due to their methodological flaws, heterogeneity issues and varied clinical interpretation [38,39]. Our study suggests that presence of robust well-designed RCTs proving superiority of Liraglutide in GLP-1 agonists market were translated favorably into the prescribing decisions shortly after 2010.
That being said, with newer MA and SRs being generated every day, but no steps being taken in the direction to improve their quality and value, it will remain challenging for the physicians to search and assess the best quality evidence [40]. Therefore, in addition to focusing on generating new evidence, there is also a need to establish a uniform methodology to consolidate, summarize and disseminate the CER evidence [9,41]. The Agency for Healthcare Research and Quality could allocate resources to develop an unbiased entity to generate and disseminate consolidated summaries of the CER evidence to guide decision making. Other alternatives could include building more online tools such as the CER collaborative tool, or more disease specific tools for physicians/payers to help streamline the bench to behavior translation. It is important that such tools account for the wide variety of CER generated using different study designs, populations and comparators, which would help reduce the inconsistency in evidence translation across practice.
In DPP4 inhibitors market, CER evidence proving clinical superiority of either of the drugs was inconclusive, since the only clinical trial published was designed to be a noninferiority trial. Noninferiority trials are designed not with the intent to prove superiority of one drug over another, rather to assess if the comparator drug is as safe and effective and no worse than the active drug, in other words, below a noninferiority margin. In the absence of conclusive superiority trials, prescribing behavior could be influenced by other nonmeasurable market factors.
One of the factors that could have guided the prescribing trends in the DPP4 inhibitors market is the new drug bias, in other words, every time a new drug was introduced in the market, a drop was seen in the prescribing rates of other competitors. Nevertheless, the first entrant in the market (Sitagliptin) continued to dominate the DPP4 inhibitors market throughout, without any robust evidence supporting its superiority.
CER evidence commonly guides the payer’s formulary and cost sharing decisions, which in turn impacts the prescribing trends [42–44]. However, in the absence of conclusive CER evidence, formulary and/or prescribing decisions could be guided by other factors such as rebates offered by manufactures, academic detailing and pharmaceutical marketing [45–47], thus rendering the CER evidence generation futile. Along with streamlining and prioritizing the CER evidence, there should be mandates to reduce the unnecessary trials or a larger focus on designing trials trying to prove superiority rather than noninferiority.
Another factor which could influence prescribing is the timing of the availability of the comparative efficacy (CE) data (different from CER) for a new drug. More than half of the drugs approved in the USA enter the market with the presence of CE data at the time of their market approval [48]. Presence of such data that compares a new drug molecule to an active comparator in its pre-approval phase, could potentially inform the clinical decisions early on in the marketing phase. In the GLP-1 agonists market, US FDA published CE data in the approval packages of Liraglutide showing clinical superiority of Liraglutide over Exenatide BID. The presence of CE data favoring Liraglutide could explain the sudden drop in Exenatide BID with rapid uptake of Liraglutide in 2010. No CE data was published for the DPP4 inhibitors market, which might have made it challenging for the decision makers, in the early phase of marketing, to assess the superiority or comparative benefits of newly approved DPP4 inhibitors. CE evidence have been discussed in the past [48] as being the first important piece of evidence to help physicians quantify the quality of new drugs early on, thereby diminishing the influence of external nonmeasurable market factors. Although it has been argued that generating CE data could be lengthy, expensive and financially risky for the manufacturers [49], regulations around CE data might discourage the abundance of me-too drugs. Incentivizing manufacturers to generate and submit CE results, whether superior, inferior or equivalent, might be a step in the right direction. Also, devising guidelines around the choice of comparators used to generate such evidence (e.g., using the comparator which is widely prescribed in the real world) [50], are long overdue.
It has been established that incorporating CER evidence into clinical decision making would help improve health outcomes in patients, save dollars spent on prescription drugs and achieve the cost and quality balance in the US healthcare system [51–56]. This study attempts to explore the practice-based reality of evidence based medicine within specific pharmaceutical markets. Future studies could be conducted to assess and explore different markets or therapeutic conditions. With each therapeutic category being unique, the results of this study should be applied to other markets with caution. However, identifying more therapeutic areas and replicating this study in other markets would further highlight the importance of streamlining the adoption of CER evidence.
Limitations
As with most studies, this study has certain limitations. This study was not designed to determine causality, rather explore associations between CER evidence and prescribing trends in Type 2 DM, which has not been studied before. This study was limited in capturing only the self-reported prescribing in the MEPS database. However, the prescription data in MEPS are verified with pharmacy providers, and have been validated with the prescription fills reported in the Medicare Part D claims database [57]. Another limitation was that the population sample of MEPS changes every 2 years, due to which it was not possible to follow the same patients over time. However, due to the rotating panel design of MEPS, this study reports the prescribing trends representative of the US population. Another limitation of this study was the exclusion of the cross class comparison, as drugs under GLP-1 agonists were not compared with drugs under DPP4 inhibitors. Due to the different mechanism of action and route of administration for the drugs under GLP-1 agonists versus DPP4 inhibitors, it would have been clinically challenging to assess the impact of CER evidence on prescribing across classes. Lastly, this study did not account for the marketing campaigns or academic detailing efforts organized by pharmaceutical manufacturers, which could impact physician prescribing decisions.
Conclusion
According to this study, CER evidence appeared to be associated with physician prescribing in GLP-1 agonists market; however, availability of superiority trials and timing of their availability were important parameters guiding prescribing decisions. Initiatives need to be taken by the Agency for Healthcare Research and Quality and/or FDA to mandate the generation of CE evidence, devise a uniform methodology to consolidate the ever-growing CER evidence and develop disease specific CER tools for physicians/payers. In the presence of scientifically robust evidence, physicians would more likely incorporate it into practice, and payers’ formulary/cost decisions would be more uniform across the nation. Such evidence will also help quantify the value of different treatments, thereby decreasing expenditures on drugs with little or no added clinical benefit. Regulations around evidence generation and its adoption could be important steps leading to a smoother and faster bench-to behavior translation in the US healthcare system.
•
Comparative effectiveness research (CER) can act as a strong tool in assisting patients, providers and payers to quantify the value of healthcare and make informed clinical decisions.
•
There has been a rapid increase in the volume of CER being generated for various therapeutic conditions.
•
Past research assessed the impact of four unrelated clinical trials on physician prescribing within four different markets, but found no specific pattern or association.
•
According to this study, availability of superiority trials and timing of their availability seemed to be associated with the prescribing patterns of glucagon-like peptide-1 agonists for Type 2 diabetes mellitus population in the USA, however, no associations were found in dipeptidyl peptidase-4 inhibitors market.
•
Kind of study design proving superiority of a drug and timing of the evidence were important parameters affecting the translation of CER into practice.
•
With the ever-growing CER, this study emphasizes the need to establish a uniform methodology or develop disease specific tools to consolidate and summarize the evidence.
•
Regulations around evidence generation and its adoption could be important steps leading to a smoother and faster bench-to behavior translation in the US healthcare system.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Author contributions
P Arora conceived the idea for the study, P Arora, KA Look and DH Kreling were involved in developing the research design and methods of the study, P Arora conducted the analysis and wrote the manuscript. All the authors were involved in discussing the results and commenting on the manuscript.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (suppl_file.pdf)
- Download
- 701.12 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Kesselheim AS, Avorn J, Sarpatwari A. The high cost of prescription drugs in the United States: origins and prospects for reform. JAMA 316(8), 858–871 (2016).
2.
Neumann PJ, Cohen JT. Measuring the value of prescription drugs. N. Engl. J. Med. 373(27), 2595–2597 (2015).
3.
Schumock GT, Pickard AS. Comparative effectiveness and patient-centered outcomes research: enhancing uptake and use by patients, clinicians and payers. J. Comp. Eff. Res. 7(2), 177–180 (2018).
4.
Esposito D, Yong PL, Rich E, Geonnotti K, Kimmey LD. The ARRA investment in CER: a description of the midstream evaluation and how the funds were allocated and CER priorities addressed. J. Comp. Eff. Res. 3(6), 581–589 (2014).
5.
Grol R. Improving the quality of medical care: building bridges among professional pride, payer profit, and patient satisfaction. JAMA 286(20), 2578–2585 (2001).
6.
Guyatt GH, Sackett DL, Sinclair JC et al. Users’ guides to the medical literature: IX. A method for grading health care recommendations. JAMA 274(22), 1800–1804 (1995).
7.
Avorn J, Fischer M. ‘Bench to behavior’: translating comparative effectiveness research into improved clinical practice. Health Aff. (Millwood) 29(10), 1891–1900 (2010).
• Outlines the factors impacting the translation of comparative effectiveness research (CER) into clinical practice and was useful in interpreting the results of our current study.
8.
Gibson TB, Ehrlich ED, Graff J et al. Real-world impact of comparative effectiveness research findings on clinical practice. Am. J. Manag. Care 20(6), e208–e220 (2014).
•• Assessed the impact of four unrelated CER findings on prescribing using claims data. It was used to identify the gap in literature for our current study and recognize the need to focus on one therapeutic area.
9.
Morrato EH, Concannon TW, Meissner P, Shah ND, Turner BJ. Dissemination and implementation of comparative effectiveness evidence: key informant interviews with Clinical and Translational Science Award institutions. J. Comp. Eff. Res. 2(2), 185–194 (2013).
10.
Haidich AB. Meta-analysis in medical research. Hippokratia 14(Suppl. 1), 29–37 (2010).
11.
Murad MH, Montori VM. Synthesizing evidence: shifting the focus from individual studies to the body of evidence. JAMA 309(21), 2217–2218 (2013).
12.
Petrisor BA, Bhandari M. The hierarchy of evidence: levels and grades of recommendation. Indian J. Orthop. 41(1), 11 (2007).
13.
Paul M, Leibovici L. Systematic review or meta-analysis? Their place in the evidence hierarchy. Clin. Microbiol. Infect. 20(2), 97–100 (2014).
14.
Petrisor BA, Bhandari M. The hierarchy of evidence: levels and grades of recommendation. Indian J. Orthop. 41(1), 11–15 (2007).
15.
Evans D. Hierarchy of evidence: a framework for ranking evidence evaluating healthcare interventions. J. Clin. Nursing 12(1), 77–84 (2003).
16.
Blackstone EA, Fuhr JP, Ziernicki D. Will comparative effectiveness research finally succeed? Biotechnol. Healthc. 9(3), 22–26 (2012).
17.
Sox HC, Greenfield S. Comparative effectiveness research: a report from the Institute of Medicine. Ann. Intern. Med. 151(3), 203–205 (2009).
18.
Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2017. Centers for Disease Control and Prevention, US Department of Health and Human Services, GA, USA (2017).
19.
American Diabetes Association. Economic Costs of Diabetes in the U.S. in 2017. Diabetes Care 41(5), 917–928 (2018).
20.
Centers for Disease Control and Prevention. Division of diabetes translation at a glance (2019). https://www.cdc.gov/chronicdisease/resources/publications/aag/diabetes.htm
21.
Food and Drug Adminstration. Drugs@FDA: FDA Approved Drug Products (2019). https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm
22.
Aroda VR, Henry RR, Han J et al. Efficacy of GLP-1 receptor agonists and DPP-4 inhibitors: meta-analysis and systematic review. Clin. Therapeut. 34(6), 1247–1258 (2012).
23.
Kayaniyil S, Lozano-Ortega G, Bennett HA et al. A network meta-analysis comparing exenatide once weekly with other GLP-1 receptor agonists for the treatment of Type 2 diabetes mellitus. Diabetes Ther. 7(1), 27–43 (2016).
24.
Pinelli NR, Hurren KM. Efficacy and safety of long-acting glucagon-like peptide-1 receptor agonists compared with exenatide twice daily and sitagliptin in Type 2 diabetes mellitus: a systematic review and meta-analysis. Ann. Pharmacother. 45(7–8), 850–860 (2011).
25.
Scott DA, Boye KS, Timlin L, Clark JF, Best JH. A network meta-analysis to compare glycaemic control in patients with Type 2 diabetes treated with exenatide once weekly or liraglutide once daily in comparison with insulin glargine, exenatide twice daily or placebo. Diabetes Obes. Metabol. 15(3), 213–223 (2013).
26.
Shyangdan DS, Royle PL, Clar C, Sharma P, Waugh NR. Glucagon-like peptide analogues for Type 2 diabetes mellitus: systematic review and meta-analysis. BMC Endocrine Disord. 10, 20 (2010).
27.
Zinman B, Schmidt WE, Moses A, Lund N, Gough S. Achieving a clinically relevant composite outcome of an HbA1c of<7% without weight gain or hypoglycaemia in Type 2 diabetes: a meta-analysis of the liraglutide clinical trial programme. Diabetes Obes. Metabol. 14(1), 77–82 (2012).
28.
Niswender K, Pi-Sunyer X, Buse J et al. Weight change with liraglutide and comparator therapies: an analysis of seven Phase III trials from the liraglutide diabetes development programme. Diabetes Obes. Metabol. 15(1), 42–54 (2013).
29.
Buse JB, Rosenstock J, Sesti G et al. Liraglutide once a day versus exenatide twice a day for Type 2 diabetes: a 26-week randomised, parallel-group, multinational, open-label trial (LEAD-6). Lancet 374(9683), 39–47 (2009).
30.
Buse JB, Sesti G, Schmidt WE et al. Switching to once-daily liraglutide from twice-daily exenatide further improves glycemic control in patients with Type 2 diabetes using oral agents. Diabetes Care 33(6), 1300–1303 (2010).
31.
Buse JB, Nauck M, Forst T et al. Exenatide once weekly versus liraglutide once daily in patients with Type 2 diabetes (DURATION-6): a randomised, open-label study. Lancet 381(9861), 117–124 (2013).
32.
Gerrald KR, Van Scoyoc E, Wines RC, Runge T, Jonas DE. Saxagliptin and sitagliptin in adult patients with Type 2 diabetes: a systematic review and meta-analysis. Diabetes Obes. Metabol. 14(6), 481–492 (2012).
33.
Park H, Park C, Kim Y, Rascati KL. Efficacy and safety of dipeptidyl peptidase-4 inhibitors in Type 2 diabetes: meta-analysis. Ann. Pharmacother. 46(11), 1453–1469 (2012).
34.
Gross JL, Rogers J, Polhamus D et al. A novel model-based meta-analysis to indirectly estimate the comparative efficacy of two medications: an example using DPP-4 inhibitors, sitagliptin and linagliptin, in treatment of Type 2 diabetes mellitus. BMJ Open 3(3), e001844 (2013).
35.
Scheen AJ, Charpentier G, Östgren CJ, Hellqvist A, Gause-Nilsson I. Efficacy and safety of saxagliptin in combination with metformin compared with sitagliptin in combination with metformin in adult patients with Type 2 diabetes mellitus. Diabetes Metab. Res. Rev. 26(7), 540–549 (2010).
36.
Mann KV, Raskin P. Exenatide extended-release: a once weekly treatment for patients with Type 2 diabetes. Diabetes Metab. Syndr. Obes. 7, 229–239 (2014).
37.
Villa L, Warholak TL, Hines LE et al. Health care decision makers' use of comparative effectiveness research: report from a series of focus groups. J. Manag. Care Pharm. 19(9), 745–754 (2013).
38.
Murad MH, Asi N, Alsawas M, Alahdab F. New evidence pyramid. Evid. Based Med. 21(4), 125–127 (2016).
39.
Berlin JA, Golub RM. Meta-analysis as evidence: building a better pyramid. JAMA 312(6), 603–606 (2014).
40.
Bastian H, Glasziou P, Chalmers I. Seventy-five trials and eleven systematic reviews a day: how will we ever keep up? PLoS Med. 7(9), e1000326 (2010).
41.
Westrich KD, Wilhelm JA, Schur CL. Comparative effectiveness research in the USA: when will there be an impact on healthcare decision-making? J. Comp. Eff. Res. 5(2), 207–216 (2016).
• Highlights the opinions of various elite decision makers about the impact of CER on decision making. Findings of the study by Westrich et al. (2016) suggest significant short-term impact of CER in improving the medical decision making, which helped adding credibility to the results and implications of our current study.
42.
Garber AM. Evidence-based coverage policy. Health Aff. (Millwood) 20(5), 62–82 (2001).
43.
Tunis SR, Stryer DB, Clancy CM. Practical clinical trials: Increasing the value of clinical research for decision making in clinical and health policy. JAMA 290(12), 1624–1632 (2003).
44.
Wang A, Halbert RJ, Baerwaldt T, Nordyke RJ. US payer perspectives on evidence for formulary decision making. JOP 8(3S), 22s–27s (2012).
45.
Grabowski H, Mullins CD. Pharmacy benefit management, cost–effectiveness analysis and drug formulary decisions. Social Sci. Med. 45(4), 535–544 (1997).
46.
Lyles A, Palumbo FB. The effect of managed care on prescription drug costs and benefits. PharmacoEconomics 15(2), 129–140 (1999).
47.
Prosser H, Walley T. New drug uptake: qualitative comparison of high and low prescribing GPs’ attitudes and approach. Fam. Pract. 20(5), 583–591 (2003).
48.
Goldberg NH, Schneeweiss S, Kowal MK, Gagne JJ. Availability of comparative efficacy data at the time of drug approval in the United States. JAMA 305(17), 1786–1789 (2011).
49.
Stafford RS, Wagner TH, Lavori PW. New, but not improved? Incorporating comparative-effectiveness information into FDA labeling. N. Engl. J. Med. 361(13), 1230–1233 (2009).
•• Discusses the importance of designing superiority trials as CER and its role in drug innovation. It helped guide and develop the research hypothesis of our current study.
50.
Chokshi DA, Avorn J, Kesselheim AS. Designing comparative effectiveness research on prescription drugs: lessons from the clinical trial literature. Health Affairs 29(10), 1842–1848 (2010).
51.
Fischer MA, Avorn J. Economic implications of evidence-based prescribing for hypertension: can better care cost less? JAMA 291(15), 1850–1856 (2004).
52.
Teutsch SM, Berger ML, Weinstein MC. Comparative effectiveness: asking the right questions, choosing the right method. Health Aff. (Millwood) 24(1), 128–132 (2005).
53.
Conway PH, Clancy C. Comparative-effectiveness research – implications of the Federal Coordinating Council’s report. N. Engl. J. Med. 361(4), 328–330 (2009).
54.
Conway PH, Clancy C. Charting a path from comparative effectiveness funding to improved patient-centered health care. JAMA 303(10), 985–986 (2010).
55.
Basu A, Jena AB, Philipson TJ. The impact of comparative effectiveness research on health and health care spending. J. Health Econ. 30(4), 695–706 (2011).
56.
Biskupiak JE, Dunn JD, Holtorf A-P. Implementing CER: what will it take? J. Manag. Care Pharm. 18(5), S19 (2012).
57.
Hill SC, Zuvekas SH, Zodet MW. Implications of the accuracy of MEPS prescription drug data for health services research. Inquiry 48(3), 242–259 (2011).
Information & Authors
Information
Published In
Pages: 1393 - 1403
PubMed: 31789054
Copyright
© 2019 Future Medicine Ltd.
History
Received: 22 August 2019
Accepted: 14 October 2019
Published online: 2 December 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Does evidence matter? Comparative effectiveness research and prescribing of Type 2 diabetes mellitus drugs. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0127
Export citation
Select the citation format you wish to export for this article or chapter.